

Abstract
Nearly 32% of women report experiencing physical violence from an intimate partner and more than 8% report being raped by a significant other in their lifetime. Young people’s perceptions that their peers perpetrate relationship violence have been shown to increase the odds of self-reported perpetration. Yet, limited research has been conducted on this relationship as individuals begin to age out of adolescence. The present study sought to examine the link between the perception of peer perpetration of intimate partner violence (IPV) and self-reported IPV perpetration among a sample of predominately young adult (21–35 years) males. This study also explored the discordance between the perception of peer IPV behavior and self-reported perpetration. Data from 101 male peer dyads (n = 202) were taken from a study on the effects of alcohol and bystander intervention in Atlanta, Georgia. Thirty-six percent (n = 73) of men reported perpetrating physical IPV and 67% (n = 135) reported perpetrating sexual IPV in the past 12 months. Nearly 35% (n = 55) of the sample reported that none of their peers had perpetrated physical IPV, which contradicted their friend’s self-report of physical IPV perpetration. Similarly, 68% (n = 115) of the men perceived none of their peers to have perpetrated sexual IPV, which contradicted their friend’s self-report of sexual IPV perpetration. Discordance variables were significantly associated with self-reported perpetration for both physical (x2 = 152.7, p < .01) and sexual (x2 = 164.4, p < .01) IPV. These results point to an underestimation of peer IPV perpetration among young adult males. Findings suggest a traditional social norms approach to IPV prevention, which seeks to persuade individuals that negative behaviors are less common than perceived, may not be the best approach given a significant number of men believed their friends were nonviolent when they had perpetrated violence.
Keywords: intimate partner violence, peer influence, social norms theory, social learning theory
Introduction
Of women reporting sexual violence, physical violence, or stalking victimization by an intimate partner, nearly 48% are estimated to have first experienced intimate partner violence (IPV) between the ages of 18 and 24 and 20.7% between the ages of 25 and 34 (Breiding et al., 2014). Women who experience IPV are at greater risk for a number of negative health outcomes including urinary tract infections, irritable bowel syndrome, chronic pain, sexually transmitted infections, HIV, migraines, asthma, diabetes, high blood pressure, insomnia, depression, anxiety, and death (Black et al., 2011; Breiding, Black, & Ryan, 2008; Campbell, 2002; Campbell et al., 2003; Tjaden & Thoennes, 2000). Partner violence and the associated health outcomes place an enormous burden on social, medical, and criminal justice systems with estimated costs reaching more than US$8.3 billion dollars in 2003 (Max, Rice, Finkelstein, Bardwell, & Leadbetter, 2004).
A recent review and nationally representative studies have found estimates of physical IPV perpetration by young adult males (age 18–30) to range from 14% to 47% (Desmarais, Reeves, Nicholls, Telford, & Fiebert, 2012; Ramirez, Paik, Sanchagrin, & Heimer, 2012; Smith, Greenman, Thornberry, Henry, & Ireland, 2015; Whitaker, Haileyesus, Swahn, & Saltzman, 2007). Variations in estimates likely result from differing methodology—including variations in tools to measure self-report and variations in recall periods. Prevalence estimates of sexual IPV perpetration among young adult males are extremely limited, with one nationally representative study finding a 5.6% rate of sexual coersion perpetration in early adulthood (Casey, Beadnell, & Lindhorst, 2009). Among males, factors linked to IPV perpetration include younger age, lower education levels, low income, alcohol consumption, and unemployment (Capaldi, Knoble, Shortt, & Kim, 2012; Leonard, 2005). Several other factors are associated with IPV perpetration, including witnessing parental violence, experiencing child maltreatment, previous IPV victimization, hostile talk toward women, and attitudes supporting traditional gender roles (Capaldi et al., 2012; Menard, Weiss, Franzese, & Covey, 2014; Roberts, McLaughlin, Conron, & Koenen, 2011). While a significant proportion of research has identified individual-level risk factors related to IPV perpetration, considerably less evidence has been established across the socioecological spectrum including factors at the relationship level and social conditions (Capaldi et al., 2012)
Several researchers have studied the effect of peers’ attitudes and behaviors on dating violence across adolescence (e.g., Arriaga & Foshee, 2004; Reed, Silverman, Raj, Decker, & Miller, 2011); however, the examination of peer influences among young adults, specifically outside of academic settings, is limited. Largely drawing on the Social Learning Theory (Bandura, 1986), studies theorize that dating violence is learned through observing, modeling, and imitating peer behavior (Menard et al., 2014). The later iteration of this theory, known as Social Cognitive Theory, acknowledges the role of reciprocal determinism on individual behavior, that is, interactions between individuals and their environment, including peers, have a direct influence on health behaviors (Glanz, Rimer, & Viswanath, 2008). Among students 12 to 17 years old, the odds of perpetrating physical dating violence has been found to be 3 times higher among individuals who perceive their peers perpetrate dating violence compared with individuals who do not (Arriaga & Foshee, 2004). Similar research looking at a community sample of adolescents, age 14 to 20, found that perpetrating dating violence (physical, sexual, and/or emotional) was 3 times more likely among males who believe their peers had perpetrated dating violence (Reed et al., 2011). These studies also reported that 20% to 31% of adolescents perceive or were told that at least one of their peers had perpetrated dating violence (Arriaga & Foshee, 2004; Reed et al., 2011).
Research looking at the peer influence on dating violence among young adults is limited to a few studies among college students. The evidence of this relationship among college students is mixed. The perception that peers are sexually aggressive toward a female dating partner has been found to increase the likelihood of self-reported forced sex behaviors among college students, yet the perception of peer physical IPV was not associated with self-reported perpetration (Gwartney-Gibbs, Stockard, & Bohmer, 1987; Schwartz & DeKeseredy, 2000). This research has yet to be replicated among young adults outside a college setting. The limited amount of research on this relationship may be due to researchers theorizing that violent peers have a greater effect during the adolescent period, when norms and behaviors are established (Capaldi, Dishion, Stoolmiller, & Yoerger, 2001). Many of the constructs that support social learning’s effect on dating violence, however, may still apply to young adults, including the observation of peer behavior and discussion of dating norms. Understanding the influence of peers on young adults as they transition between adolescence and adulthood, more recently described as the period of emerging adulthood (ages 18–29), may help to inform the prevention of IPV behaviors (Arnett, 2000, 2015).
Social Learning Theory and the aforementioned studies do not account for the misperception of peer behavior. As described by Social Norms Theory, inaccurate perceptions of peer behaviors and/or attitudes can influence individuals to change their health behaviors to match the misperceived norm (Berkowitz, 2004). Understanding whether or not perceptions of peer IPV behaviors are accurate is particularly important to informing prevention strategies as “… overestimation of problem behavior will increase these problem behaviors while underestimations of healthy behaviors will discourage individuals from engaging in them” (Berkowitz, 2004, p. 5). Inaccurate perceptions of peers’ engagement in IPV can be addressed through a social norms approach, where misperceptions of peers’ behaviors are corrected to influence individual behaviors (Berkowitz, 2004). Social Norms Theory has a significant presence within nonpartner sexual violence research and programming, but its contribution in understanding partner specific violence is not well documented. For example, a recent study found that college males who reported perpetrating nonpartner sexual violence were 3 times more likely to inaccurately perceive their peers’ sexually aggressive behaviors (Dardis, Murphy, Bill, & Gidycz, 2016). It is currently unknown if young adults accurately estimate, overestimate, or underestimate their peers’ perpetration of IPV, and it is important to understand whether or not misperceptions exist to develop tailored prevention messaging. This study aims to address several gaps in the current literature on peer influence of young adult male IPV behavior.
Guided by Social Learning Theory, we first examined the influence of perceiving peer IPV behavior on IPV perpetration among a sample of predominately young adult males. We then applied the Social Norms Theory to assess whether or not males misperceive their peers’ IPV behavior. We tested three hypotheses:
Hypothesis 1: A positive association between the perceptions of peer IPV and self-report IPV exists among the sample of predominately young adult males.
Hypothesis 2: Young adult males overestimate their peers’ engagement in IPV behaviors based on the report of their dyad peer.
Hypothesis 3: A positive association exists between young adult males overestimating their peers’ violent behaviors and self-reported IPV perpetration.
Method
Participants
The distinct set of hypotheses tested herein used data that were drawn from a larger investigation on the effects of alcohol, peers, and bystander intervention on sexual aggression (Parrott et al., 2012). Although the focus of the present study did not examine alcohol-related effects, participants were required to meet eligibility criteria for an alcohol administration study (see below), and all nondrinkers were excluded. The larger investigation received approval from the institution’s institutional review board (IRB) prior to data collection.
Researchers recruited 261 males between the ages of 21 and 35 in the metro-Atlanta area through Internet-based advertisements and local newspapers. Participants were told the study was on “Alcohol and Views About the Media.” Initial phone screening was utilized to ascertain participants’ selfreported alcohol consumption and exclude individuals who reported no regular alcohol use, alcohol- or drug-related problems, or a medical condition in which alcohol is medically contraindicated. Participants were required to present to the laboratory with a “good friend,” and each participant completed study questionnaires separately. Measures were not employed to confirm the nature of the relationship between the participant and their dyad partner. Only friend dyads in which both individuals met the required eligibility criteria, self-identified as heterosexual, and reported being in an intimate relationship in the past year were included in this analysis.
The final sample included 202 men (101 dyads), and the average age of participants was 25 years (SD = 3.4). The sample consisted of 62% African Americans, 27% Caucasians, 9% multiracial, 1% American Indian or Alaska Native, 0.5% Asian, and 0.5% did not identify. On average, participants reported 14 years of education (SD = 2.4) and a median annual income of US$15,000 (range = US$2,500-US$70,000). Of the individuals in the study, 82% identified as never married and reported an average of eight drinks per day (SD = 1.1), on days they drank, in the past 12 months. All participants received US$10 an hour for their participation.
Measures
Demographic form.
Demographic characteristics included age, race, relationship status, years of education, and yearly income. Age provided by respondents was categorized into groups of 21 to 25, 26 to 30, and 31 to 35. Respondent’s race was categorized to White, Black or African American, or Other—other included American Indian or Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, and multi-racial. Marital status was categorized to single (never married, divorced, widowed, and separated) and committed (married and not married but living with intimate partner). Respondents provided their completed years of education (including kindergarten) and responses were categorized into (1) less than or equal to high school degree or (2) greater than high school degree. Average yearly income was reported on a 7-answer scale ranging from US$0 to US$70,000 (e.g., US$0-US$5,000, US$5,000-US$10,000), and responses were categorized to <US$20,000 and >US$20,000.
Alcohol consumption.
Respondents’ alcohol consumption during the past 12 months was assessed using the National Institute on Alcohol Abuse and Alcoholism’s (NIAAA; 2003) recommended set of questions. To measure participants’ average consumption of alcohol per day, the following question was asked, “During the last 12 months, how many alcoholic drinks did you have on a typical day when you drank alcohol?” Categorical responses were provided on a scale from 1 to 25 or more drinks per day (e.g., 1 drink, 2 drinks, 3–4 drinks, etc.). As recommended by NIAAA (2003), final scores were computed by averaging the number of drinks in each range. For example, if a respondent reported “9–11” drinks per day, then their average drinks per day would be “10.” This method reliably measures a respondent’s average consumption of alcoholic drinks per day over a period of time.
IPV perpetration.
For the purpose of this study, we created two dichotomous variables from the Revised Conflict Tactics Scale (CTS-2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) to measure intimate partner physical violence and sexual violence perpetration. The CTS-2 is a self-report instrument consisting of 78 questions measuring both perpetration and victimization of physical, sexual, and emotional violence in an intimate relationship. Participants were instructed to report frequency of behaviors in the past 12 months on a 7-point scale, ranging from never (0) to more than 20 times (6). While the full scale was administered, only a subset of the 18 items that assessed physical violence perpetration and the seven items that assessed sexual violence perpetration were included in this study (see Straus et al., 1996, for scale items). The physical violence measure included questions ranging from less severe physical violence (e.g., slapping a partner) to violence resulting in an injury (e.g., needing medical attention). Questions asking about both forced sex (e.g., using a weapon to force a partner to have sex) and sexually coercive behaviors (e.g., using threats to make a partner have sex) were included in the sexual violence measure. Responses were dichotomized to 0 (never) or 1 (at least once in past 12 months).
Perception of peer IPV.
We created two dichotomized variables to measure the perception of peer physical violence and sexual violence perpetration from the Attachment to Abusive Male Peers subscale of the Male Peer Support questionnaire (DeKeseredy, 1988). The Male Peer Support questionnaire asks participants to answer based on “friends or people you hang around with” and has been previously correlated with IPV perpetration (e.g., DeKeseredy, 1988; Schwartz & DeKeseredy, 2000). The Full Attachment to Abusive Male Peers subscale measures the number of peers who had perpetrated dating violence perpetration on a 4-point scale—asking participants to identify how many of their male peers they believed to have perpetrated physical violence, sexual violence, and psychological abuse against a dating partner. Questions pertaining to physical and sexual violence asked the participant to describe, to the best of their knowledge, how many of their male friends had (a) ever made physically forceful attempts at sexual activity with women they were dating which were disagreeable and offensive enough that the women responded in an offended manner such as crying, fighting, screaming, or pleading, and (b) ever used physical force, such as hitting or beating, to resolve conflicts with their girlfriends and/or dating partners to make them fulfill some demand. The response scale included four categories regarding how many friends they believed had exhibited these behaviors (none, 1 or 2, 3 to 5, and 6 to 10) and were dichotomized to “none” or “at least 1 peer” for the analysis. This variable measures participants’ perceptions about all of their peers rather than only their friend in the study. We used the measure as a proxy to assess the index respondent’s (participant’s) perception of the behavior of their study partner (friend in the study). Both the participant and their friend in the study completed the same questionnaire; thus, each individual’s responses were counted as both an “index respondent” and the “study partner.”
Peer IPV supportive attitudes.
To measure peer IPV supportive attitudes, we created three dichotomized measures from the Male Peer Support’s Informational Support subscale (DeKeseredy, 1988). To assess peer IPV supportive attitudes on physical violence perpetration, forced sex, and expecting sex, we collapsed responses from the two questions asked for each of the three topics.
The full Informational Support subscale includes seven dichotomous questions that assess peer advice received by the respondent regarding physical violence perpetration, emotional abuse, forced sex behaviors, and expecting sex from women. We did not use the item on emotional abuse because that was not the focus of our study. Questions used to assess peer IPV supportive attitudes are shown in Table 1.
Table 1.
Male Peer Supporta Informational Support Subscale Questions by Topic.
| Did any of your male friends tell you that … |
| Physical violence perpetration |
| 1. You should respond to your dates’ or girlfriends’ challenges to your authority by using physical force, such as hitting or slapping? |
| 2. It is alright for a man to hit his date or girlfriend in certain situations? |
| Sexual violence perpetration |
| 1. You should respond to your dates’ or girlfriends’ sexual rejections by physically forcing them to have sex? |
| 2. It is alright for a man to physically force a woman to have sex with him in certain situations? |
| Expecting sex |
| 1. Your dates or girlfriends should have sex with you when you want? |
| 2. If a man spends money on a date, she should have sex with him in return? |
Procedure
The research team greeted participating dyads upon arrival to the study location and led each participant to separate rooms where they provided consent for the study. Participants then completed the questionnaire battery, including measures described above, on a computer using MediaLab 2006 software (Jarvis, 2006). Other study instruments were also completed but are unrelated to this study and are not reported here. Researchers answered questions throughout the session and debriefed participants after completion of the questionnaire.
Data Analysis
We used chi-square analyses to test all three hypotheses. For Hypothesis 1, we examined the association between the perception of peer IPV and selfreport IPV. To explore this relationship further and to provide context for the results of Hypothesis 1, we also examined the relationship between having peers with IPV supportive attitudes and self-reported IPV behaviors.
To test our second hypothesis, we created discordance variables to assess whether males in our sample overestimated their peers’ engagement in IPV behaviors. As described in Figure 1, discordance was measured by comparing perceived peer IPV behaviors with the study partner’s self-report of IPV perpetration. We operationalized concordance as the dyad having matching responses (i.e., no IPV or IPV behaviors) and discordance as having mismatched responses. We used participant’s responses to assess their own IPV behavior and the perception of their peers’ behavior. Discordance variables were created for physical and sexual IPV separately.
Figure I.
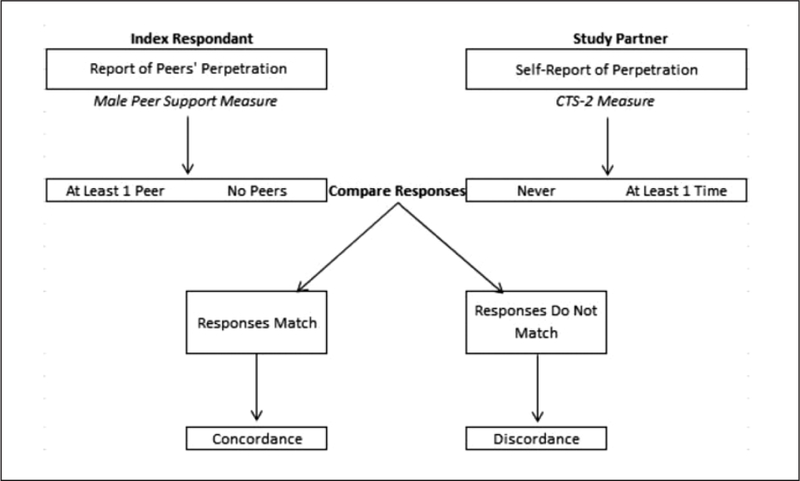
Dyad discordance variable.
Note. CTS-12 = Revised Conflict Tactics Scale.
Finally, to test Hypothesis 3, we examined the association between discordance (i.e., the misperception of peers’ IPV behavior) and self-report IPV perpetration for both physical and sexual IPV. Using the discordance variable created and self-report IPV perpetration, we examined the association between misperceiving peer IPV behaviors and self-reported IPV perpetration.
The computerized administration of the study questionnaires resulted in limited missing data on the relevant questionnaires. Missing data from the Male Peer Support subscales were removed via listwise deletion for the descriptive analysis of the measures and the discordance analysis. There were no missing data from the Conflicts Tactics Scale (self-report IPV perpetration) questionnaire. Those with missing data were not significantly different to those with complete data.
Results
Of the total sample, 36% of men (n = 73) reported perpetrating physical IPV in the last 12 months and 67% (n = 135) reported perpetrating sexual IPV (results not presented in table). Of the men reporting physical IPV, nearly 70% reported perpetrating between 1 to 5 times in the past 12 months (results not presented in table). Ninety-two percent reported perpetrating less severe behaviors (e.g., slapping partner, twisting a partner’s arm) and 38% reported more severe behaviors (e.g., choking a partner; results not presented in table). A smaller minority (7%) of the total sample reported perpetrating physical violence that resulted in an injury (e.g., breaking a bone). Twenty-seven percent of the men reporting sexual IPV reported perpetrating more than 20 times in the past year (results not presented in table). The majority of sexual IPV reported at a high frequency were sexual coercive behaviors (e.g., making a partner have sex without a condom), while a smaller minority were forced sex behaviors. All of the men who reported perpetrating sexual IPV reported engaging in sexual coercive behaviors, with only 6% of the men also reporting physically forcing sex on a partner (results not presented in table). The majority of men who reported perpetrating either type of IPV were between the ages of 21 and 25, single, non-Hispanic/Latino, African American, with an income less than US$20,000, and reported consuming an average of one to four alcoholic drinks per day. Of men reporting physical IPV perpetration, 51% (n = 37) had less than a high school degree while 54% (n = 73) of those reporting sexual IPV had greater than a high school degree. None of the demographic variables were significantly associated with IPV perpetration.
Hypothesis I
A positive association between the perceptions of peer IPV and self-report IPV was not found, for either physical (χ2 = 1.87; p = .171) or sexual violence (χ2 = 1.05; p = .305) (Table 2). Only one participant (0.5% of the total sample) perceived that at least one of their peers had engaged in physical IPV perpetration, and only two participants (1% of the total sample) stated they had at least one peer who had perpetrated sexual violence (results not presented in table).
Table 2.
Association Between Peer Influence Variables and Self-Reported IPV.
| Physical Violence Perpetration |
Sexual Violence Perpetration |
|
|---|---|---|
| Peer Influence Variables | χ2 (p) | χ2 (p) |
| Perception of peer IPV | ||
| Physical violence | 1.87 (.171) | — |
| Sexual violence | — | 1.05 (.305) |
| Peer IPV supportive attitudes | ||
| Physical violence | 2.97 (.084) | — |
| Sexual violence | — | 2.49 (.115) |
| Expecting sex | — | 9.53 (.002)* |
Note. IPV = intimate partner violence.
p < .01.
To explore the results of Hypothesis 1 further, we then examined the relationship between peer IPV supportive attitudes and self-reported IPV perpetration (Table 2). Participants reporting that their peers held supportive attitudes for IPV perpetration was not found to be associated with selfreported physical IPV (χ2 = 2.97; p = .084) or sexual violence IPV (χ2 = 2.49; p = .115). Eight percent (n = 16) of participants reported being told by a male peer to use physical violence when a date or girlfriend challenged authority or in “certain situations” (results not presented in table). And, 5% (n = 10) reported that their male friends had verbally shared that physically forcing sex was appropriate either when they were sexually rejected by a date/girlfriend or under “certain situations” (results not presented in table). However, none of the participants who reported having a peer who held supportive attitudes for IPV perpetration also reported having peers who actually engaged in IPV perpetration for both physical and sexual violence. Having peers who held supportive attitudes for expecting sex was significantly associated with self-reported sexual IPV perpetration (χ2 = 9.53;p < .05; Table 2). Nearly one fourth of the sample (n = 48) reported that their peers told them either a date/girlfriend should have sex with a man when he wants or if he spent money on a date (results not presented in table).
Hypothesis 2
Results of the discordance analysis are summarized in Table 3. The majority of participants underestimated or accurately estimated their peers’ IPV behavior based on the report of their study partner. The majority of index respondents’ (n = 102) perceptions of peer physical IPV were concordant, meaning they mirrored that of their study partner’s self-report of IPV perpetration. Thirty-five percent (n = 55) of the index respondents’ responses were discordant with their study partner’s self-report of physical IPV perpetration. All of the discordance reflects the index respondent perceiving that none of their peers had perpetrated physical IPV while their study partner reported perpetration at least once in the past 12 months. This means that over a third of participants underestimated their peers’ engagement in physical IPV (Table 3).
Table 3.
Discordance Between the Index Respondent’s Prediction of Peers’ IPV Perpetration and Their Study Partner’s Self-Report of IPV Perpetration.
| Physical Violence Perpetration |
Sexual Violence Perpetration |
|
|---|---|---|
| Discordance | % (n) | % (n) |
| Concordance | 65.0 (102) | 32.0 (54) |
| Index respondent “No” and study 2003partner “No” | 99.0 (101) | 98.1 (53) |
| Index respondent “Yes” and study partner “Yes” | 1.0 (1) | 1.9 (1) |
| Discordance | 35.0 (55) | 68.0 (115) |
| Index respondent “No” and study partner “Yes” | 100.0 (55) | 100.0 (115) |
| Index respondent “Yes” and study partner “No” | 0.0 (0) | 0.0 (0) |
Note. IPV = intimate partner violence.
Thirty-two percent (n = 54) of index respondents’ responses were concordant with their study partner’s self-report of sexual IPV perpetration. Sixty-eight percent of the index respondents’ perception of their peers’ sexual IPV perpetration responses were discordant. All discordant responses (n = 115) reflected the index respondent perceiving that none of their peers engaged in sexual IPV perpetration, while their study partner self-reported perpetration at least once in the past 12 months. This means that the majority of participants underestimated their peers’ engagement in sexual IPV perpetration, based on the report of one peer.
Hypothesis 3
A positive association was found between the misperception of peers’ violent behaviors and self-reported IPV perpetration (results not presented in table). This relationship was significant for both physical IPV (χ2 = 152.7; p < .01) and sexual IPV (χ2 = 164.4; p < .01). Of those who self-reported perpetrating physical IPV in the past 12 months, 98% (n = 55) misperceived their peers’ engagement in physical IPV. Similarly, 99% (n = 115) of participants who self-reported perpetrating sexual IPV in the past year also misperceived their peers’ sexual IPV behaviors. Only data from participants who reported their perceptions of peer behavior were included in this analysis. Missing data from the Male Peer Support subscales assessing both peer physical IPV (n = 18) and sexual IPV (n = 20) were removed via listwise deletion. For both physical and sexual IPV, less than 2% of participants who reported perpetrating violence in the past year accurately perceived their peers’ engagement in IPV, based on the report of one peer. These findings indicate that index participants who misperceived and underestimated their peers’ perpetration of IPV, based on the report of one peer, were more likely to self-report IPV perpetration compared with index participants who did not misperceive their peers’ behavior.
Discussion
To our knowledge, this is one of the only studies to examine peer influence on IPV from a sample of young adults drawn from outside a college setting. Specifically, this study aimed to assess if perceived peer IPV behaviors and peer IPV supportive attitudes influenced self-reported IPV perpetration, and if the perception of peers’ IPV perpetration was accurately estimated based on the report of a good friend. As the majority of the men included in this study fell between the ages of 21 and 25, this research explored the influence of peers during young adulthood. We found no association between the perception of peers’ IPV perpetration and self-reported perpetration among our sample of young adults, contrary to our first hypothesis and previous research of adolescents ages 12 to 20 (Arriaga & Foshee, 2004; Reed et al., 2011). The perception of peers’ IPV perpetration was extremely low in this sample compared with the previous studies of adolescents. Only 1% or less of participants perceived their peers to have perpetrated physical or sexual IPV, compared with adolescent estimates ranging from 20% to 31% (Arriaga & Foshee, 2004; Reed et al., 2011). Some of the variation between the results of our study and that of previous work on adolescents may be due to differences in measurement tools. In addition, variations may be related to the age of the respondent. While the majority of our sample falls within the lower range of young adulthood (21–25), this is still distinct from the previously mentioned studies where the average age of respondents was considerably younger, 13 to 17 years old. As adolescents begin to age into adulthood, they may be less influenced by their perceptions of peer behaviors or tuned into their peers’ behaviors.
The posteriori analysis to explore peer attitudes and self-report of IPV found that only peer supporting attitudes on expecting sex were documented as related to self-report on sexual violence perpetration. Almost 24% of the sample reported having a friend who verbally shared they should expect sex from a woman either on a date or when a man wants. The report of peer supportive attitudes for expecting sex and self-report sexual violence perpetration was found to be associated in this sample. This is consistent with previous literature, as individuals with dominant male gender role ideologies have been shown to be more likely to perpetrate sexual coercion (e.g., Santana, Raj, Decker, La Marche, & Silverman, 2006). The expectation of sex may be a more socially acceptable position to disclose among male peers compared with other IPV supportive attitudes (e.g., forced sex) and may account for some of the differences in our findings.
Similar to previous findings among college students from Schwartz and DeKeseredy (2000), our study found an association between peer supportive attitudes for physically forcing a partner to engage in sex and self-reported sexual violence perpetration. Varying from Schwartz and DeKeseredy’s results, we found no association between peer supportive attitudes for physical IPV and self-reported physical violence perpetration. However, we collapsed responses for the physical violence and sexual violence measures separately to compare against the outcomes of physical IPV and sexual IPV, while Schwartz and DeKeseredy used the accumulative assessment of peer IPV supportive attitudes (physical violence, sexual violence, expecting sex, and emotional abuse), which may help to explain differences in results.
While the results from our first hypothesis found that the perception of peers’ IPV behaviors was not associated with self-reported IPV perpetration, some peer supportive attitudes for IPV were found to be associated with selfreported IPV. These findings, although mixed, suggest that peers may continue to influence IPV behaviors following adolescence. These data also suggest that the constructs of Social Learning Theory may continue to influence IPV perpetration during emerging adulthood. Future research is needed to fully explore and understand the relevance of Social Learning Theory to IPV perpetration among this population.
When examining our second hypothesis, the perceptions of peer IPV behaviors, we found high levels of discordance between the perceptions of peers’ IPV behavior and self-report of IPV perpetration by one peer. While we hypothesized that discordance would exist, we anticipated that the respondents would overestimate their peers’ behavior, when in fact our results indicated they underestimated their peers’ violent behavior (Hypothesis 2). Nearly one third of the sample reported having no peers who had perpetrated physical IPV, yet their study partner self-reported perpetration in the past year. Similarly, 68% of participants reported having no peers who had perpetrated sexual violence while their study partner self-reported perpetration.
If these findings reflect the true discordance of the perceptions of peer IPV behaviors, then the results would suggest that a traditional social norms prevention approach, based on Social Norms Theory, in which perceived overestimations of a peer’s negative behavior are corrected, may not be as appropriate as males transition from adolescence into adulthood (Berkowitz, 2004). Misperceptions have been shown to differ among various populations (e.g., athletes, college Greek life members), and some researchers suggest that social norms interventions may not be suitable for subpopulations underestimating negative peer behaviors (Berkowitz, 2004). This sample greatly underestimated their peers’ engagement in dating violence rather than overestimated IPV behaviors, based a proxy measure of one friend. Correcting for the underestimation of IPV in educational messaging may impede positive behavior changes as the correction would inform individuals that more people than they thought are violent toward a partner, which could unintentionally create a new norm for acceptance of IPV. However, this approach could also increase awareness of the issue of IPV; thus, some researchers emphasize including both descriptive norms (i.e., typical behaviors) and injunctive norms (i.e., individual’s morals or beliefs) in interventions, as the reported injunctive norms often oppose the reported behaviors (Dardis et al., 2016; Paul & Gray, 2011). Injunctive norms, and other factors such as knowledge of laws against IPV or lack of social acceptance for violent behaviors, may play more of a key role in the underestimation of peer IPV behaviors. While little research has examined how the influence of social norms change, and the continued relevance of Social Norms Theory throughout the life span, future studies should explore whether a social norms approach may be more relevant among adolescents, or individuals in a school setting, as they might be more likely to display or boast about negative behaviors among peers to fit in socially.
When testing our last hypothesis, we found that individuals whose perception of their peers’ perpetration of IPV did not match their study partner’s self-report of perpetration were more likely to report IPV perpetration for both physical and sexual violence. This does not directly align with our hypothesis, where we predicted that overestimating peers’ violent behavior would increase the likelihood of self-reported IPV perpetration, and underestimating peers’ violent behavior would decrease the likelihood of self-reported perpetration. Our results contradicted this hypothesis, as we found that the underestimation of peers’ violent behavior increased the likelihood of self-reported IPV perpetration. These findings may indicate that an adult male’s perpetration of IPV is not driven by the perception that their peers’ perpetrate violence and that other factors may play a more powerful role influencing violent behavior, such as norms about women or general aggressiveness.
It is necessary to comment on a number of limitations. First, perpetration estimates were collected via self-report measures and may not accurately represent the true prevalence of behavior. However, the respondents believed the study was on alcohol and the media, and thus, their responses on dating measures might not have been subject to an increase in reporting bias. We also focused on whether or not perpetration occurred, rather than how many times it occurred. While this allowed us to conduct the discordance analysis, it did not allow us to assess differences among men reporting a higher frequency of perpetration. Further work could be conducted to assess the frequency of perpetration in relation to peer influences. It is also important to note that while our study drew on a community sample of predominately young adults (21–35), the average age of participants is similar to previous research among college students (e.g., Schwartz & DeKeseredy, 2000). While we cannot ascertain how many participants in our sample were currently enrolled in college, the average age and reported years of education suggest our sample is more similar rather than distinct from previous studies among college students. Nevertheless, the majority of research looking at peer influences on IPV is among adolescents (e.g., Arriaga & Foshee, 2004). This research provides novel contribution to the limited evidence of how peers influence IPV among young adults.
Additional limitations relate to how peer influence was assessed in this study. First, perception measures did not ask specifically about the study partner but rather the perception of all their peers. This measure was used as a proxy to assess their perceptions of their good friend in the study; therefore, the accuracy of the perception of their dyad peer’s behavior was not directly ascertained. The index respondents may have estimated their answer(s) based on the average behavior exhibited in their peer group rather than by individual peers. Thus, their response may not accurately reflect the level of violence perpetrated by their peers. Furthermore, the index respondents may not have included their study partner when reporting the perception of their peers’ IPV behaviors and, as such, the results may not accurately reflect the respondent’s perceptions of their good friend in the study. The term “good friend” was not operationalized in this study and no methods were employed to validate the relationship, as such it is possible that the good friend was not a significant peer. This further points to the possibility that the index respondent may not have considered their study partner when reporting their perception of their peers’ behaviors. The results of this analysis may not accurately reflect the level of discordance between the perceptions of peers’ IPV behaviors and self-reported IPV perpetration. In addition, responses may have included reports based on knowledge rather than perceptions, as it asked respondents to report peer behavior to the best of their knowledge. While answers could have included both perceptions and knowledge of peer behavior, findings indicated a high level of discordance which suggests either the majority of responses were based on perceptions or the friend was not a significant peer.
It is also important to note that the demographics of the study population are not reflective of the general population, and thus, our findings cannot be generalized. The men in our sample were predominately African American, which is novel for research examining IPV perpetration, specifically sexual assault; however, our results cannot be generalized to this population. Further analysis with a larger sample of men is needed to examine race and ethnic differences related to IPV perpetration. This is important as the rates of IPV perpetration were found to be higher for both physical and sexual violence compared with previous studies (e.g., Santana et al., 2006). The high rates of IPV perpetration found in this study may be related to the respondents’ reports of several risk factors for IPV including high frequency of alcohol use and low socioeconomic status. None of the demographic variables were found to be associated with IPV. However, we did not test the combined effect of the demographic variables on IPV perpetration which may help to explain the high rate of perpetration.
Despite these limitations, our study begins to explore several gaps in the literature and supports further research on the influence of peers on IPV among young adults. Our findings pose the hypothesis that the level of influence of peers on the perpetration of IPV in younger adults may not be as significant as evidenced in adolescents (e.g., Reed et al., 2011) or in nonpartner sexual violence research (e.g., Swartout, 2013). Future research is needed to explore the true nature and the level to which peers influence these behaviors among this population. Our study was also the first to our knowledge to explore the level of concordance between perceived peer norms and actual IPV behaviors from a peer among young adults. As our results found a high level of misperception of peer IPV behaviors, based on a proxy measure, additional research expanding this work to better understand the accuracy of peer perceptions of IPV behaviors is needed.
Acknowledgments
The authors thank Kimberley Freire, PhD, Division of Violence Prevention, Centers for Disease Control and Prevention, for her valuable suggestions and edits in review of the article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Biographies
Marissa McKool is an ORISE fellow at the Centers for Disease Control and Prevention (CDC) in the Division of Violence Prevention. Her work focuses on evaluation and translation of sexual violence prevention strategies.
Rob Stephenson is a professor in the Department of Health Behavior and Biological Sciences in the School of Nursing at the University of Michigan, where he also directs the Center for Sexuality and Health Disparities.
Kate Winskell is an associate professor in the Hubert Department of Global Health of Rollins School of Public Health at Emory University. She specializes in communication for social and behavioral change, particularly as it relates to HIV, gender, and sexual and reproductive health.
Andra Teten Tharp is a special consultant with the Division of Violence Prevention at the CDC. She works in the areas of dating and sexual violence prevention.
Dominic Parrott is an associate professor of psychology (Clinical) at Georgia State University. His research uses laboratory and survey methods to examine risk factors and mechanisms for aggression perpetration, with a particular emphasis on the effects of alcohol on intimate partner violence, aggression toward sexual minorities, and sexual aggression. An end goal of his research program is to inform directly the development of interventions that prevent or reduce alcohol-related violence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Arnett JJ (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55, 469–480. [PubMed] [Google Scholar]
- Arnett JJ (2015). Emerging adulthood: The winding road from the late teens through the twenties New York, NY: Oxford University Press. [Google Scholar]
- Arriaga XB, & Foshee VA (2004). Adolescent dating violence: Do adolescents follow in their friends’, or their parents’, footsteps? Journal of Interpersonal Violence, 19, 162–184. doi: 10.1177/0886260503260247 [DOI] [PubMed] [Google Scholar]
- Bandura A (1986). Social foundations of thought and action: A social cognitive theory Englewood Cliffs, NJ: Prentice-Hall. [Google Scholar]
- Berkowitz A (2004). The social norms approach: Theory, research, and annotated bibliography Retrieved from http://www.alanberkowitz.com/articles/social_norms.pdf
- Black MC, Basile KC, Breiding MJ, Smith SG, Walters ML, Merrick MT, … Stevens MR (2011). The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 summary report (pp. 1–106). Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. [Google Scholar]
- Breiding MJ, Black MC, & Ryan GW (2008). Chronic disease and health risk behaviors associated with intimate partner violence—18 U.S. states/territories, 2005. Annals of Epidemiology, 18, 538–544. [DOI] [PubMed] [Google Scholar]
- Breiding MJ, Smith SG, Basile KC, Walter ML, Chen J, & Merrick MT (2014). Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization—National Intimate Partner and Sexual Violence Survey, United States, 2011. Morbidity and Mortality Weekly Report, 63 (SS08), 1–18. [PMC free article] [PubMed] [Google Scholar]
- Campbell JC (2002). Health consequences of intimate partner violence. The Lancet, 359, 1331–1336. doi: 10.1016/s0140-6736(02)08336-8 [DOI] [PubMed] [Google Scholar]
- Campbell JC, Webster D, Koziol-McLain J, Block C, Campbell D, Curry M,… Wilt S (2003). Assessing risk factors for intimate partner homicide. National Institute of Justice, 250, 14–19. [Google Scholar]
- Capaldi DM, Dishion TJ, Stoolmiller M, & Yoerger K (2001). Aggression toward female partners by at-risk young men: The contribution of male adolescent friendships. Developmental Psychology, 37, 61–73. doi: 10.1037/0012-1649.37.1.61 [DOI] [PubMed] [Google Scholar]
- Capaldi DM, Knoble NB, Shortt JW, & Kim HK (2012). A systematic review of risk factors for intimate partner violence. Partner Abuse, 3, 231–280. doi: 10.1891/1946-6560.3.2.231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Casey EA, Beadnell B, & Lindhorst TP (2009). Predictors of sexually coercive behavior in a nationally representative sample of adolescent males. Journal of Interpersonal Violence, 24, 1129–1147. [DOI] [PubMed] [Google Scholar]
- Dardis CM, Murphy MJ, Bill AC, & Gidycz CA (2016). An investigation of the tenets of social norms theory as they relate to sexually aggressive attitudes and sexual assault perpetration: A comparison of men and their friends. Psychology of Violence, 6, 163–171. doi: 10.1037/a0039443 [DOI] [Google Scholar]
- DeKeseredy W (1988). Women abuse in dating relationships: The role of male peer support Toronto, Ontario, Canada: Canadian Scholars’ Press. [Google Scholar]
- Desmarais SL, Reeves KA, Nicholls TL, Telford RP, & Fiebert MS (2012). #2 Prevalence of physical violence in intimate relationships, part 2: Rates of male and female perpetration. Partner Abuse, 3(2), 1–10. [Google Scholar]
- Glanz K, Rimer BK, & Viswanath K (2008). Health behavior and health education: Theory, research, and practice San Francisco, CA: Jossey-Bass. [Google Scholar]
- Gwartney-Gibbs PA, Stockard J, & Bohmer S (1987). Learning courtship aggression: The influence of parents, peers, and personal experiences. Family Relations: An Interdisciplinary Journal of Applied Family Studies, 36, 276–282. doi: 10.2307/583540 [DOI] [Google Scholar]
- Jarvis BG (2006). MediaLab (version 2006.1.41) New York, NY: Empirisoft Corporation. [Google Scholar]
- Leonard KE (2005). Alcohol and intimate partner violence: When can we say that heavy drinking is a contributing cause of violence? Addiction, 100, 422–425. doi: 10.1111/j.1360-0443.2005.00994.x [DOI] [PubMed] [Google Scholar]
- Max W, Rice DP, Finkelstein E, Bardwell RA, & Leadbetter S (2004). The economic toll of intimate partner violence against women in the United States. Violence and Victims, 19, 259–272. [DOI] [PubMed] [Google Scholar]
- Menard S, Weiss AJ, Franzese RJ, & Covey HC (2014). Types of adolescent exposure to violence as predictors of adult intimate partner violence. Child Abuse & Neglect, 38, 627–639. doi: 10.1016/j.chiabu.2014.02.001 [DOI] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism. (2003). National Council on Alcohol Abuse and Alcohol recommended sets of alcohol consumption questions Bethesda, MD. [Google Scholar]
- Parrott DJ, Tharp AL, Swartout KM, Miller CA, Hall GCN, & George WH (2012). Validity for an integrated laboratory analogue of sexual aggression and bystander intervention. Aggressive Behavior, 38, 309–321. [DOI] [PubMed] [Google Scholar]
- Paul LA, & Gray MJ (2011). Sexual assault programming on college campuses: Using social psychological belief and behavior change principles to improve outcomes. Trauma, Violence, & Abuse, 12, 99–109. doi: 10.1177/1524838010390710 [DOI] [PubMed] [Google Scholar]
- Ramirez M, Paik A, Sanchagrin K, & Heimer K (2012). Violent peers, network centrality, and intimate partner violence perpetration by young men. Journal of Adolescent Health, 51, 503–509. doi: 10.1016/j.jadohealth.2012.02.016 [DOI] [PubMed] [Google Scholar]
- Reed E, Silverman JG, Raj A, Decker MR, & Miller E (2011). Male perpetration of teen dating violence: Associations with neighborhood violence involvement, gender attitudes, and perceived peer and neighborhood norms. Journal of Urban Health, 88, 226–239. doi: 10.1007/s11524-011-9545-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts AL, McLaughlin KA, Conron KJ, & Koenen KC (2011). Adulthood stressors, history of childhood adversity, and risk of perpetration of intimate partner violence. American Journal of Preventive Medicine, 40, 128–138. doi: 10.1016/j.amepre.2010.10.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Santana MC, Raj A, Decker MR, La Marche A, & Silverman JG (2006). Masculine gender roles associated with increased sexual risk and intimate partner violence perpetration among young adult men. Journal of Urban Health, 83, 575585. doi: 10.1007/s11524-006-9061-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz MD, & DeKeseredy WS (2000). Aggregation bias and woman abuse: Variations by male peer support, region, language and school type. Journal of Interpersonal Violence, 15, 555–565. doi: 10.1177/088626000015006001 [DOI] [Google Scholar]
- Smith CA, Greenman SJ, Thornberry TP, Henry KL, & Ireland TO (2015). Adolescent risk for intimate partner violence perpetration. Prevention Science, 16, 862–872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Straus MA, Hamby SL, Boney-McCoy S, & Sugarman DB (1996). The Revised Conflict Tactics Scales (CTS2): Development and preliminary psychometric data. Journal of Family Issues, 17, 283–316. doi: 10.1177/019251396017003001 [DOI] [Google Scholar]
- Swartout KM (2013). The company they keep: How peer networks influence male sexual aggression. Psychology of Violence, 3, 157–171. [Google Scholar]
- Tjaden P, & Thoennes N (2000). Extent, nature, and consequences of intimate partner violence: Findings from the National Violence Against Women Survey (Publication No. NCJ 181867) Washington, DC: U.S. Department of Justice. Retrieved from https://www.ncjrs.gov/pdffiles1/nij/181867.pdf [Google Scholar]
- Whitaker DL, Haileyesus T, Swahn M, & Saltzman LS (2007). Differences in frequency of violence and reported injury between relationships with reciprocal and nonreciprocal intimate partner violence. Research and Practice, 9, 941–947. [DOI] [PMC free article] [PubMed] [Google Scholar]