

Abstract
Introduction
The Summit County Medical Examiner's Office (SCMEO) observed 52 unexplained deaths during the month of July 2016 in which drug overdose was suspected. A fentanyl screening immunoassay performed on autopsy specimens was positive, but gas chromatograph/mass spectrometry (GC/MS) failed to confirm its presence. Carfentanil, a large wildlife tranquilizer, was later identified through reference lab testing as the cause of the sudden increase in overdoses.
Methods
Due to the large volume of cases which followed, a method for identifying carfentanil was developed utilizing in-house instrumentation. In addition, a retrospective analysis for all drug overdose cases was conducted through the SCMEO database from January 2009 through December 2016.
Results
Assessment of the data revealed a 277% increase in yearly overdose-related fatalities when comparing 2009 to 2016. Carfentanil was not identified in any other fatal drug overdoses in the area before the first appearance in Akron in July of 2016. There was an initial spike of 35 deaths in both July and August, which then decreased to 12 deaths in December. There was an almost equal distribution of carfentanil as a single agent and carfentanil mixed with multiple other illicit drugs.
Discussion
Current observations suggest carfentanil concentrations in overdose cases are decreasing; however, it may be present in combination with other drugs, especially other fentanyl analogs. The lower concentrations of carfentanil are much more difficult to detect in urine and peripheral blood, therefore making the testing of scene paraphernalia, central blood, and organ tissue more of a necessity.
Keywords: Forensic pathology, Carfentanil, Overdose, Opioids, Ohio
Introduction
Ohio has become one of the focal points of the opioid epidemic sweeping the nation since 2014, with fentanyl and its analogs being the main reported cause of overdose deaths. From 2010 to 2015, the number of unintentional drug overdose deaths increased 98% (1). Ohio reported 514 fentanyl-related fatal overdoses in 2014, compared to 92 in 2013 (2). Illicitly manufactured synthetic opioids and opioid analogues are not detected in the commercially available routine screening tests utilized at most medical examiner's offices (1, 2). Therefore, some suspected overdoses may remain unconfirmed or undiagnosed. This may cause inaccurate statistics and underestimate the growing trend of drug overdose-related fatalities.
The Summit County Medical Examiner's Office (SCMEO) in Akron, Ohio experienced an unprecedented surge of unexplained deaths in July 2016 for which drug overdose was suspected. Previous reports in other areas of Ohio and neighboring Midwestern states led to the erroneous assumption that these deaths might be related to heroin adulterated with fentanyl or acetyl fentanyl (3). One of the two screening immunoassays utilized at the SCMEO was positive for fentanyl, but testing utilizing gas chromatograph/mass spectrometry (GC/MS) was unable to confirm the presence of fentanyl in the specimen. The drug in question was later confirmed as carfentanil by reference lab testing.
Carfentanil is a synthetic opioid that is 10 000 times more potent than morphine and 100 times more potent than fentanyl. Carfentanil is legally approved in the United States only for veterinary use, under the trade name Wildnil, to rapidly tranquilize large wildlife (1, 3–10). Only two documented human exposures to carfentanil were found in the literature dating before the initial cases identified in Akron. One case was a veterinarian with unintentional exposure due to a splash from a tranquilizing dart, who survived due to his quick acting colleagues administering 100 mg of naltrexone in the field (3, 4). The other report discusses carfentanil residue found on clothing and norcarfentanil identified in urine toxicology testing from victims exposed to an unidentified gas released in a Moscow theater by the Russian military (4–6). Prior to July 8th of 2016, there had never been a reported outbreak of the magnitude of illicit carfentanil overdose deaths that were seen in Summit County, Ohio (7).
Methods
A retrospective analysis for all drug overdose cases was conducted through the SCMEO database from January 2009 through December 2016. The database included the case number, date of death, age, sex, race, manner of death, location of death, place of residence, cause of death, and the corresponding toxicology results. A specific database query was run for carfentanil from January 2016 through December 2016. Standard autopsies with microscopic analysis and toxicology testing were performed for each case, as per office protocol. Matrices collected commonly for toxicology studies included peripheral blood and urine. These specimens were tested as required by the circumstances of the case. Most often, peripheral blood was obtained from the femoral vein. Other collection sites included the heart and great vessels, defined as central collection sites. When blood and/or urine were not available, for instance in decomposed cases, other fluids or tissues were collected for testing.
The SCMEO utilizes two urine based immunoassays for routine screening tests: one for drugs of abuse and the other for fentanyl and its analogs. A fentanyl screen was not part of routine testing prior to June 2014 when the nation was experiencing an opioid epidemic, mostly due to heroin and illicit fentanyl. Quantitation and confirmation of all positive drug screens are performed by GC/MS.
During the routine work-up of these initially unexplained deaths, multiple cases were encountered with a positive fentanyl screening test by the Immunalysis Fentanyl Urine Enzyme Immunoassay, but confirmation testing by GS/MS was negative. Specimens were sent to another forensic toxicology lab (Franklin County Coroner's Office, Columbus, OH), as well as to a forensic reference lab (Axis Forensic Toxicology, Indianapolis, IN) for qualitative and more sensitive testing with liquid chromatography/mass spectrometry/mass spectrometry (LC/MS/MS). These labs were able to identify the presence of carfentanil as the cause of the reactive screening assay.
Due to the large volume of cases and costs associated with reference lab referrals, we developed a method to identify and quantify carfentanil by utilizing our current GC/MS testing platform. A standard curve with concentrations at 5 ng/mL, 2.5 ng/mL, and 1.0 ng/mL was set up from a 3 mg/mL stock standard acquired from the Cleveland Zoo. A 1 ng/mL cut-off level is currently used for all cases of carfentanil as standard protocol, due to the less sensitive method of GC/MS. When suspicious cases are negative for carfentanil testing on autopsy samples, paraphernalia from the scene is tested using the “dilute and shoot” method. If this fails to confirm carfentanil, the specimens are then sent for reference lab testing.
Results
From January 2009 through December 2016, the SCMEO reported a total of 1065 drug overdose deaths, averaging about 11 deaths per month. The caseload of overdoses rose from 70 in 2009 to 264 through 2016. This signifies a 277% increase in overdose deaths in a seven year period. Starting July 8th 2016, Summit County became one of the epicenters in Ohio for carfentanil overdoses. Three-hundred and two total overdoses, with 52 deaths, not exclusive to opioids, were reported specifically for the city of Akron (the largest city in Summit County) from the Department of Planning and Research in the Akron City Police Department (11). There were 140 presumed carfentanil deaths in 2016, with 135 cases being confirmed by toxicology testing at the time of this submission. Carfentanil quickly overtook fentanyl as the leading cause of opioid overdose deaths in 2016, when heroin and fentanyl levels started to decline. Cocaine and methamphetamine had a significant increase in 2016 as well (Figure 1).
Figure 1.
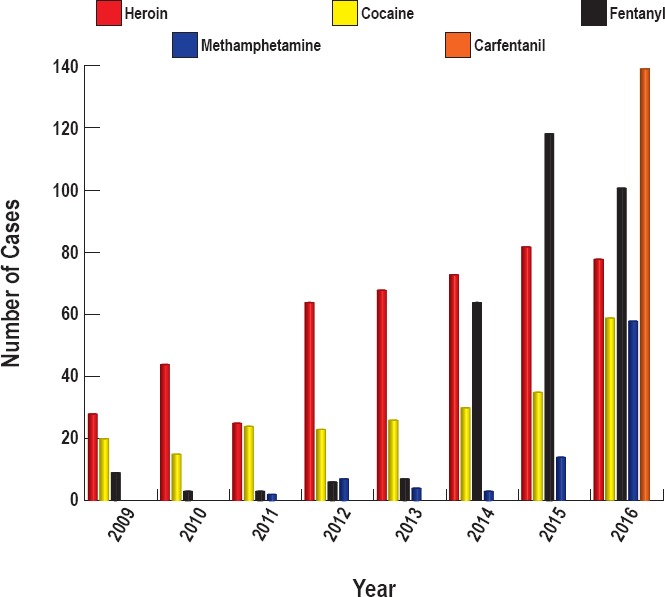
Overdose cases per year by drug.
The number of overdose deaths due to carfentanil decreased each month, starting with 35 deaths each in July and August, steadily decreasing to 22 in September, 20 in October, 16 in November, down to the lowest number of deaths in December with 12 (Figure 2). Of the carfentanil deaths, the median age was 38, with ages ranging from 17 to 64 years. One-hundred and eighteen of the 140 decedents were white and 21 were black (84% vs 15%); 90 were male and 50 were female (64% vs 36%). In 91 cases, the decedent was found at a residence and in 32 cases death was pronounced at a hospital. The remaining 17 cases were as follows: 6 in a hotel, 5 in a grassy area/side of a street, 3 in a vehicle, and 3 in a parking lot.
Figure 2.
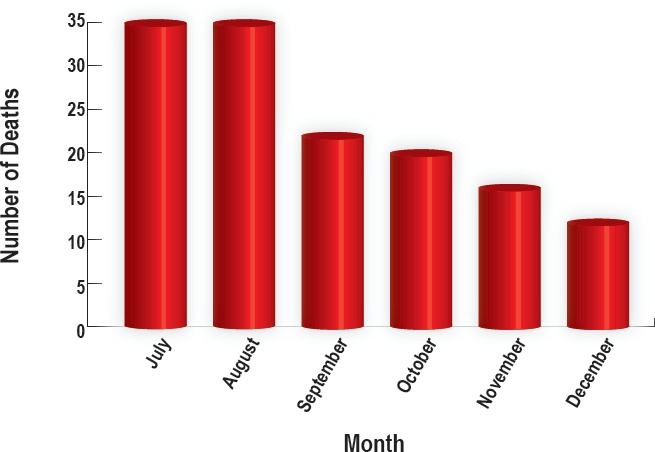
Carfentanil deaths per month in Summit County in 2016.
Reference lab testing was requested for a total of 66 cases. Strictly qualitative analysis was performed in 56 of these cases. Of the cases where quantitative analysis was completed, ten reference cases resulted in blood carfentanil levels that ranged 22.0 pg/mL to 0.1 ng/mL. The 0.1 ng/mL concentration was seen in July when carfentanil was first encountered.
Paraphernalia was tested in 40 cases with the “dilute and shoot” method. For paraphernalia with minimal residue, like straws, bindle bags, and spoons, five drops of methanol were used to pick up and dissolve any residue and then directly injected into the GC/MS for analysis. Ten drops of methanol were used to dissolve a small portion of any powder or unknown substances found at scenes and then directly “shot” into the GC/MS.
We also analyzed specimens from the carfentanil cases for the presence or absence of other drugs. This sub-categorization shows that 53% of carfentanil overdose cases were found to have other drugs present on toxicology. The majority of the combination cases were found to have carfentanil and methamphetamine. The “other” category, which comprised 13% of carfentanil overdoses, included marijuana, benzodiazepines, alcohol, and selective serotonin reuptake inhibitors (SSRIs) (Figure 3). Carfentanil was found to be the only drug reported in 75 cases, comprising 47% of all carfentanil-related overdose deaths.
Figure 3.
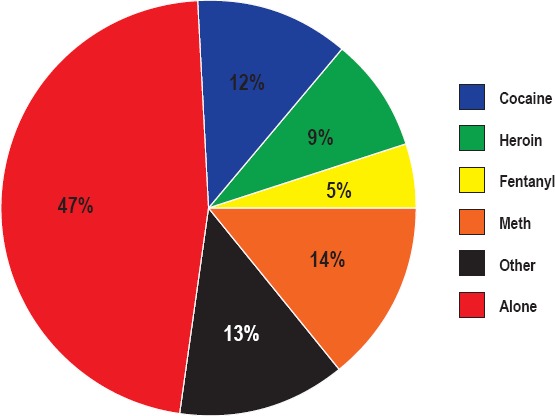
Breakdown of carfentanil cases in 2016.
Discussion
Fentanyl and fentanyl analog adulteration of heroin represents a significant change in the environmental risks for heroin users (3). The state of Ohio reported the total drug overdose cases for 2016 and showed an increase of 1000 cases from the previous year (12). Fentanyl and more potent fentanyl analogues, including carfentanil, were involved in 58% of the 4050 reported deaths (12). Ohio reported 340 total carfentanil overdoses in 2016. The unintentional overdose deaths in Ohio, with the declining presence of heroin and pharmaceutical opioids, indicate a rapidly emerging, substantial role of illicit, laboratory created fentanyls among drug users in our state (1).
From July 2016 through until the time of publication, over 140 carfentanil-related deaths have occurred in Summit County. The data regarding the carfentanil epidemic show an almost even distribution of carfentanil being used alone versus being used in combination with other drugs. The largest percentage of cases had carfentanil detected as a single agent, illustrated in Figure 3. These data indicate that users were likely supplied a pure product of carfentanil. There were approximately 14% of cases in which either fentanyl or heroin metabolites were detected. These findings might imply that, in these cases, carfentanil could represent a cutting agent resulting in an adulterated product.
The strong potency of carfentanil leads to rapid and sudden respiratory depression when the presumed heroin is injected or ingested. Opioids, such as fentanyl, cause respiratory depression in a dose-dependent manner. When an overdose victim becomes unconscious, their breathing may decelerate so that adequate oxygen levels cannot be attained in the blood and provided to the rest of the body. Fentanyls also cause the neck and tongue muscles to relax, leading to airway obstruction. However, when delivered rapidly, fentanyls can cause muscle rigidity, also causing a disruption of breathing (5, 8).
Carfentanil is 10 000 times more potent than morphine due to its ease of crossing the blood-brain barrier, its high affinity for the μ-opioid receptors and its high lipophilicity. Carfentanil is also tightly bound to plasma proteins, giving it a large volume of distribution. The elimination of a drug as lipophilic as fentanyl is limited to the volume of distribution (5, 7). These factors also cause this potent fentanyl analog to have a very high risk of renarcotization, where the agonist/drug has a longer duration of effects than the reversal agent (7, 8). The liver's CYP enzymes, especially CYP3A4, metabolize fentanyl, sufentanyl, and alfentanyl. Carfentanil is structurally similar to fentanyl (Figure 4), and is broken down in the same way into its main two metabolites, norcarfentanil and M8 (8–9). Norcarfentanil is a good indicator of carfentanil exposure; however, it is not specific and possibly unlikely to be encountered due to the abrupt onset of respiratory depression and death (8).
Figure 4.
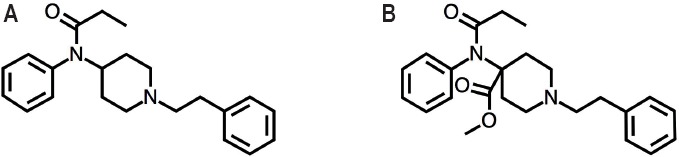
Chemical structures of A) fentanyl and B) carfentanil.
After the initial months of July and August, deaths due to carfentanil started to decrease. Sofalyi et al. recently found that sub-nanogram per milliliter concentrations of carfentanil in the blood may not be lethal for an individual (7). Currently, confirmation testing by GC/MS shows carfentanil concentrations decreasing. These lower concentrations are being seen in combination with other drugs, especially other fentanyl analogs. These lower carfentanil levels in urine and blood may be below the detection limits of our present-day instrumentation. Due to the potency of carfentanil, less drug is needed to obtain the desired effect and it is difficult to detect using GC/MS methods (9, 10). Targeted analysis should ideally be performed using liquid chromatography with tandem mass spectrometry due to its increased sensitivity. The testing of residues from paraphernalia located at the scenes, as well as organ tissue, might need to become routine when toxicology results are negative and carfentanil is suspected (10).
Conclusion
Multiple state and county-wide initiatives have been implemented to combat this dangerous epidemic. The need for up to date and highly sensitive testing is crucial for the detection of drugs, which are lethal at low concentrations, such as carfentanil and other fentanyl analogs. States without centralized medical examiner systems are less likely to be able to identify the specific drug involved in an overdose than states with a centralized system (3). Synthetic illicit opioids produced in chemistry laboratories have become a recurrent aspect of the heroin supply. They are easy to produce and cheap for users to obtain, but have created an urgent need for updated, sensitive toxicology methods for treatment centers, criminal justice labs, and especially medical examiner's offices.
Footnotes
ETHICAL APPROVAL
As per Journal Policies, ethical approval was not required for this manuscript
STATEMENT OF HUMAN AND ANIMAL RIGHTS
This article does not contain any studies conducted with animals or on living human subjects
STATEMENT OF INFORMED CONSENT
No identifiable personal data were presented in this manuscsript
DISCLOSURES & DECLARATION OF CONFLICTS OF INTEREST
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest
FINANCIAL DISCLOSURE The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript
References
- 1.Daniulaityte R., Juhascik M.P., Strayer K.E. et al. Overdose deaths related to fentanyl and its analogs — Ohio, January–February 2017. MMWR Morb Mortal Wkly Rep. 2017. Sep 1; 66(34): 904–8. PMID: 28859050. 10.15585/mmwr.mm6634a3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Centers for Disease Control and Prevention [Internet]. Atlanta: Centers for Disease Control and Prevention; c2017. Increases in fentanyl drug confiscations and fentanyl-related overdose fatalities; 2015. Oct 26 [cited 2017 Sep 5]. Available from: https://emergency.cdc.gov/han/han00384.asp. [Google Scholar]
- 3.Ciccarone D. Fentanyl in the US heroin supply: a rapidly changing risk environment. Int J Drug Policy. 2017. Aug; 46: 107–11. PMID: 28735776. 10.1016/j.drugpo.2017.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.George A.V., Lu J.J., Pisano M.V. et al. Carfentanil—an ultra potent opioid. Am J Emerg Med. 2010. May; 28(4): 530–2. PMID: 20466249. 10.1016/j.ajem.2010.03.003. [DOI] [PubMed] [Google Scholar]
- 5.Riches J.R., Read R.W., Black R.M. et al. Analysis of clothing and urine from Moscow theatre siege casualties reveals carfentanil and remifentanil use. J Anal Toxicol. 2012. Nov-Dec; 36(9): 647–56. PMID: 23002178. 10.1093/jat/bks078. [DOI] [PubMed] [Google Scholar]
- 6.Cole J.B., Nelson L.S. Controversies and carfentanil: We have much to learn about the present state of opioid poisoning. Am J Emerg Med. 2017. Nov; 35(11): 1743–5. PMID: 28851500. 10.1016/j.ajem.2017.08.045. [DOI] [PubMed] [Google Scholar]
- 7.Sofalvi S., Schueler H.E., Lavins E.S. et al. An LC–MS-MS method for the analysis of carfentanil, 3-methylfentanyl, 2-furanyl fentanyl, acetyl fentanyl, fentanyl and norfentanyl in postmortem and impaired-driving cases. J Anal Toxicol. 2017. Jul 1; 41(6): 473–83. PMID: 28830122. 10.1093/jat/bkx052. [DOI] [PubMed] [Google Scholar]
- 8.Feasel M.G., Wohlfarth A., Nilles J.M. et al. Metabolism of carfentanil, an ultra-potent opioid, in human liver microsomes and human hepatocytes by high-resolution mass spectrometry. AAPS J. 2016. Nov; 18(6): 1489–99. PMID: 27495118. 10.1208/s12248-016-9963-5. [DOI] [PubMed] [Google Scholar]
- 9.Wang L., Bernert J.T. Analysis of 13 fentanils, including sufentanil and carfentanil, in human urine by liquid chromatographyatmospheric-pressure ionization-tandem mass spectrometry. J Anal Toxicol. 2006. Jun; 30(5): 335–41. PMID: 16839472. 10.1093/jat/30.5.335. [DOI] [PubMed] [Google Scholar]
- 10.Swanson D.M., Hair L.S., Rivers S.R. et al. Fatalities involving carfentanil and furanyl fentanyl: two case reports. J Anal Toxicol. 2017. Jul 1; 41(6): 498–502. PMID: 28575422. 10.1093/jat/bkx037. [DOI] [PubMed] [Google Scholar]
- 11.Wiles Erika. Summit County drug overdose data [Internet]. Message to: Kristy Waite. 30 Mar. 2017. [cited 2017 Sep 25]. [Google Scholar]
- 12.Fentanyl, carfentanil and cocaine drive increase in drug overdose deaths in 2016 [Internet]. Columbus (OH): Ohio Department of Health; 2017. Aug 30 [cited 2017 Oct 26]. 2 p. Available from: https://www.odh.ohio.gov/-/media/ODH/ASSETS/Files/health/injury-prevention/ODH-News-Release—-2016-Ohio-Drug-Overdose-Report.pdf?la=en. [Google Scholar]