

Abstract
Evidence of prior autoerotic asphyxia is often difficult to establish due to the decedent's efforts to hide the activity from others. In this case report, we suggest that a healed fracture of the thyroid cartilage is indicative of prior autoerotic asphyxia activity.
The decedent was a 45-year-old man who was found unclothed on the floor of his bedroom with a belt ligature around the neck. A second rope ligature was loosely wrapped around the decedent's wrists, scrotum, and penis. A definitive escape mechanism was not identified, but a nearby towel and barbell weight may have comprised a possible escape mechanism. There was no known history of depression or prior autoerotic activity. Autopsy was notable for the presence of a healed fracture of the right superior horn of the thyroid cartilage.
Three-dimensional (3D) surface scanning and 3D printing was utilized to preserve the anatomical findings prior to histologic sampling. To our knowledge, this is the first reported use of 3D surface scanning and 3D printing for the purpose of documenting a forensic finding prior to alteration of the anatomical specimen for histologic sampling.
Acute fractures of the superior horns of the thyroid cartilage are not infrequently seen in ligature hanging. Therefore, the presence of a healed fracture in the setting of autoerotic asphyxia likely indicates prior activity. Histologic sampling of the laryngeal cartilages to detect occult healed fractures in autoerotic asphyxia may be useful. Three-dimensional scanning and printing may alleviate concerns for specimen alteration due to histology sampling.
Keywords: Forensic pathology, Autoerotic asphyxia, Healed neck fracture, 3D surface scanning, 3D printing, Autopsy
Introduction
Evidence of prior autoerotic asphyxia is often difficult to establish during a death investigation due to the decedent's efforts to hide the activity from others. In this case report, we suggest that a healed fracture of the thyroid cartilage is indicative of prior autoerotic asphyxia activity. Acute fractures of the superior horns of the thyroid cartilage are sometimes seen in ligature hangings. Therefore, the presence of a healed fracture of a superior horn, in the setting of an autoerotic asphyxial death, is likely indicative of prior autoerotic asphyxial activity.
Case Report
Scene Investigation
The decedent was a 45-year-old man who was found unclothed on his bedroom floor with a belt ligature around his neck. He was found by his father who opened the door and noticed that something was preventing it from completely opening. The father did not recall hearing any unusual activity in the room before-hand. There appeared to be an area of the upper door frame that was clean of dust and was thought to represent the attachment point for the ligature. A second ligature was loosely wrapped around the decedent's scrotum and connected to his wrists.
Other nearby items at the scene included a cellphone with a dead battery, a mirror on the bed, and a barbell with an adjacent towel. The cellphone was locked with a code so it could not be ascertained whether the phone was being used at the time of death.
A definitive escape mechanism was not identified but the nearby barbell and towel may have represented components of an escape mechanism. The towel may also have been used to protect the neck from bruising as a means of concealment of the activity. Escape mechanisms and concealment efforts are often, but not always, present at autoerotic asphyxia death scenes.
The decedent did not have a known history of depression, suicidal ideation, substance abuse, or autoerotic activity. The father, who was nearby in the next room, did not hear any unusual activity in the room during the day.
Autopsy
At autopsy, external examination revealed fixed lividity of the lower extremities in a “stocking-pattern,” consistent with the body initially being in an upright position. An incomplete ligature furrow surrounded the neck, with a ligature abrasion pattern that matched that of the overlying belt. There were no petechial hemorrhages of the face, gingiva, or conjunctivae. Internally, an anterior layered neck dissection revealed only minimal hemorrhage of the strap muscles and focal hemorrhages of the anterior surfaces of the thyroid cartilage ala. There were no recent fractures of the hyoid bone, thyroid cartilage, cricoid cartilage, tracheal cartilages, or cervical vertebrae. However, there was a healed, displaced fracture of the right superior horn of the thyroid cartilage with fracture callus (Image 1). The fractured tip was displaced anteriorly and medially. Gross photography and postmortem radiography of the thyroid cartilage were performed, which confirmed the presence of a healed fracture with callus (Image 2). Histology of the fracture showed a displaced fracture in an advanced stage of healing with well-formed lamellar bone and central medullary cavity, and only focal periosteal fibrous callus (Image 3). Prior to disrupting the anatomical structures for histologic examination, images of the formalin-fixed larynx specimen were acquired with a handheld three-dimensional (3D) Artec (Luxembourg City, Luxembourg) Space Spider surface scanner. Three-dimensional printing was undertaken in the 3D Laboratory within the Department of Radiology at a major academic medical center affiliated with the medical examiner office. Postmortem toxicology was negative.
Image 1.
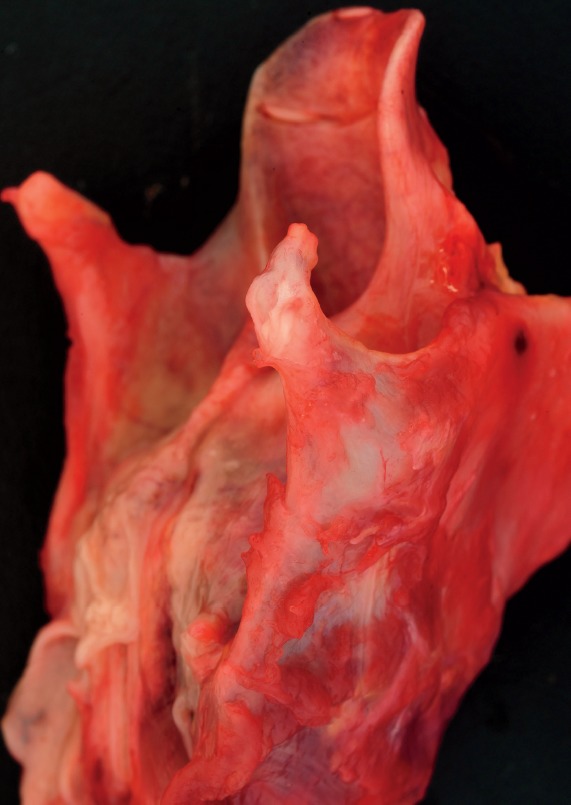
Anteriorly and medially displaced healed fracture of right superior horn of thyroid cartilage.
Image 2.

Radiograph of larynx demonstrating fracture of right superior horn of thyroid cartilage (arrow).
Image 3.
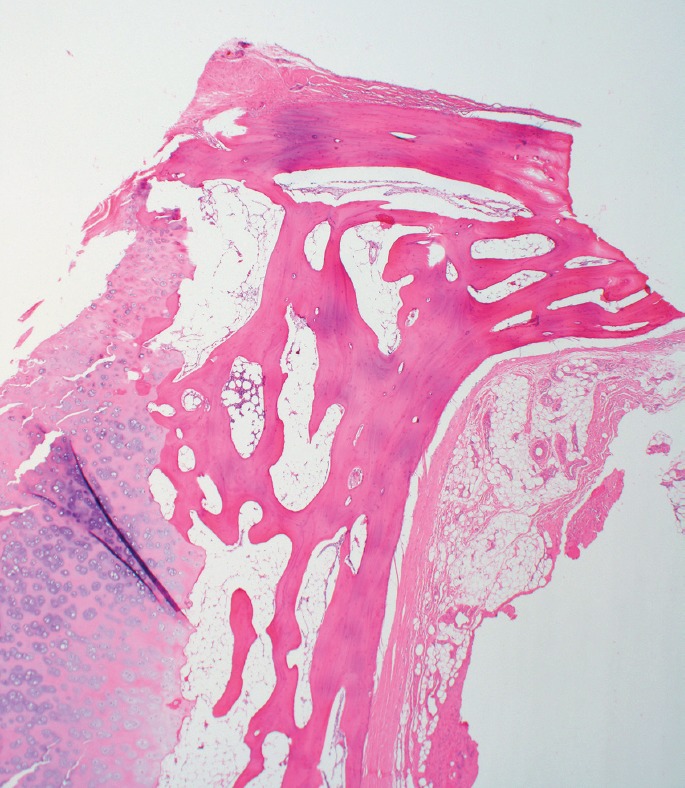
Histology of fracture showing displaced fracture site in an advanced stage of healing with well-formed lamellar bone and medullary cavity (H&E, x20).
Discussion
Autoerotic death is defined as an unanticipated death in the course of solo sexual activity in which an arousal-enhancing device is employed along with an apparent safety or escape mechanism (1). The most common method employed to increase arousal is asphyxia in which a device is designed to lower the brain's oxygen supply to achieve heightened sexual pleasure. This is most commonly done with a ligature, although cases of inhalation of chemicals and the use of a plastic bag have also been identified as alternative means of achieving the same effect. Rarer forms of autoerotic death have been documented and include electrocution and drowning (aquaeroticum) (2, 3).
The underlying mechanism of autoerotic asphyxia by ligature involves constriction of the neck, producing hypoxia due to diminished cerebrovascular circulation as well as retention of carbon dioxide with resulting hypercapnia (4). This state produces a light-headed sensation which enhances sexual pleasure in the practitioners.
There are between 500 and 1000 deaths attributed to autoerotic activity in the United States and Canada each year (4). The decedent is typically a single, young to middle aged, Caucasian man who is solitary in nature. There is typically no history of depression or suicidal ideation. Individuals will go to great lengths to hide their activities, most being found in their private residence behind closed doors.
The scene usually displays an element of fetishism, bondage, and/or cross dressing being the most common. A pornographic element may also be present. As the practitioner does not want others to know of their practices, there is usually an effort made to hide bruises caused by the ligature through means of some padding. Evidence of prior autoerotic asphyxia may be found at the scene, including worn areas that served as an anchor for repeated suspensions. An escape mechanism, or fail-safe device, is also often found. Escape mechanisms involve a way to automatically release pressure when the practitioner becomes unconscious. In autoerotic death, the escape mechanism fails resulting in death. In some instances, a definitive escape mechanism is not identified. In such cases, the individual relies upon maintaining consciousness as a safety measure.
Autoerotic deaths are accidental deaths because the intent of the individual is enhanced sexual gratification, not death. However, during the initial stages of a suspected autoerotic death investigation, it is important to search for alternative causes and manners of death such as an accidental drug overdose, suicide by ligature strangulation, or homicide by ligature or manual strangulation. Because the scene typically involves an undressed body with evidence of recent sexual activity and presence of ligatures, a sex-related homicide must be considered. Suicide can be difficult or impossible to distinguish from autoerotic asphyxia if there is a history of depression, prior suicide attempt, or absence of an escape mechanism. An argument may also be made that some types of autoerotic asphyxia carry such a high risk of death that suicide would be an appropriate classification, similar to the reasoning for classifying “Russian Roulette”-type of deaths as suicide. However, manner of death classification should not be based on simplistic categorizations of deaths, but rather on the specific features of each individual case. Nonetheless, most, if not all, instances of bona fide autoerotic asphyxia deaths should fall in the accident category. As with all types of cases, the cause and manner of death should only be determined after consideration of all available information obtained through a complete death investigation including record review, scene investigation, law enforcement investigation, complete postmortem examination, toxicology, and other relevant studies.
In the case presented, the decedent ft the typical profile of someone who engages in autoerotic asphyxia: a single, young to middle-aged, Caucasian man. At the scene, there was evidence of fetishism including the ligature around the genitalia and the mirror on the bed. The ligature around the wrists and genitals was loosely wrapped and would have allowed the decedent to free himself at will, reducing suspicion for a sex-related homicide. Law enforcement investigation determined that no other individuals could have entered the son's room because the father was home the entire day and no unusual activity was heard. No evidence of pornographic material was found; however, it could be postulated that the cellphone was used for this purpose. While no definitive escape mechanism could be determined, the barbell and towel found in close proximity to the decedent could have been components of a release mechanism. The towel may have also initially been used as padding between the belt ligature and the neck to prevent visible neck injury. Petechial hemorrhages were not identified, but the ligature furrow of the neck with patterned abrasions as well as focal hemorrhages of the strap muscles and soft tissue overlying the thyroid cartilage ala all support asphyxial neck compression as the cause of death. No other cause of death or significant trauma was identified and the toxicology screen was negative. The presence of a “stocking-distribution” lividity pattern on the lower extremities with Tardieu spots indicates that the body was initially in an upright position leaned against the door prior to the father opening it. There was also no history of depression or expression of suicidal intent. Finally, the remote fracture with healing of the right superior horn of the thyroid cartilage was suggestive of prior autoerotic asphyxial activity involving neck compression. Given the overall findings, the cause of death was certified as ligature hanging (autoerotic asphyxia) and the manner of death as accident.
One challenge associated with the investigation and certification of deaths associated with autoerotic activity is the frequent absence of a known history of such activity. Individuals who engage in autoerotic activity often hide their activity from family members and friends. In fact, the presence of materials at the scene that are specifically intended to prevent the formation of visible injuries, such as a towel around the neck to prevent the formation of neck abrasions, is one of the characteristic hallmarks of an autoerotic death scene. This absence of history can lead to refusal by the family to accept the death as an accidental death but instead suspect a homicidal death. Therefore, it is important to search for evidence of prior autoerotic activity, even though such evidence has usually been deliberately hidden by the decedent and therefore can be difficult to find. Rarely, video or audio recordings of prior activity may be found. Very few studies have attempted to find autopsy markers of prior autoerotic asphyxial activity. One study examined whether intra-alveolar hemosiderin was indicative of prior asphyxial episodes, but no significant difference was found between autoerotic asphyxial deaths and control groups (5).
To our knowledge, this case report is the first to suggest that a healed fracture of a superior horn of the thyroid cartilage is indicative of prior autoerotic asphyxial activity. In this particular case, the healed fracture was displaced anteriorly and medially allowing easy identification, but a nondisplaced fracture without callus formation would be difficult to detect without careful dissection and histologic examination. Therefore, histologic sampling of the superior horns of the thyroid cartilage may be useful in suspected autoerotic asphyxia.
Acute fractures of the thyroid cartilage or hyoid bone in the setting of hanging are seen with variably reported frequency ranging from less than 10% to as high as 68% (6, 7). Fractures of the superior horns of the thyroid cartilage are the most commonly reported fractures in hanging deaths (7). The amount of weight required to fracture the superior horns of the thyroid cartilage has been estimated to be approximately 3 kg, compared to the amount of force required to fracture the thyroid cartilage laminae (15.8 kg) and the cricoid cartilage (20.8 kg) (8). However, it is important to note that these studies typically use isolated specimens without attached musculature and tendons, and therefore may not reflect the true amount of force required to cause fracture. Fractures of the superior horns of the thyroid cartilage may also be artifactually induced during the removal of neck organs. Therefore, careful removal is required, and the presence of hemorrhage in the adjacent soft tissue is supportive of a true fracture.
Histologic examination may also assist in confirming the presence of an acute or healed fracture, or it may also reveal the presence of an occult fracture. Healed fractures of the superior horns of the thyroid cartilage are thought to be less common and are difficult to detect. One study, in which careful examination of the thyroid cartilage was performed in 1160 adult forensic autopsies, found 43 healed thyroid horn fractures (3.7%) in a variety of cases involving neck trauma, though histologic confirmation was not performed (9).
Conclusion
Medical examiners may be reluctant to perform histology on laryngeal specimens, especially in homicidal strangulation deaths, due to the necessary disruption of the specimen for histology. In most situations, histologic confirmation of a laryngeal fracture is not necessary because the fracture is readily apparent on gross examination. However, histology may be necessary to demonstrate an occult fracture. Furthermore, in homicidal strangulation deaths, histologic confirmation of an acute or subacute laryngeal fracture may be performed to demonstrate intracartilaginous hemorrhage (in order to distinguish from an artifactual fracture caused during removal of the neck organs). In these situations, disruption of the laryngeal specimen is unavoidable. With the use of 3D imaging technology in conjunction with 3D printing, the anatomical findings can be permanently documented in a highly accurate, 3D model (Image 4) The use of this technology in forensic pathology has been previously described (10). These models may serve as useful tools for the demonstration of anatomic findings to other investigators, law enforcement officers, attorneys, and jury members. To our knowledge, this is the first reported use of 3D surface scanning and printing to document a laryngeal fracture discovered at autopsy in the setting of autoerotic asphyxia.
Image 4.
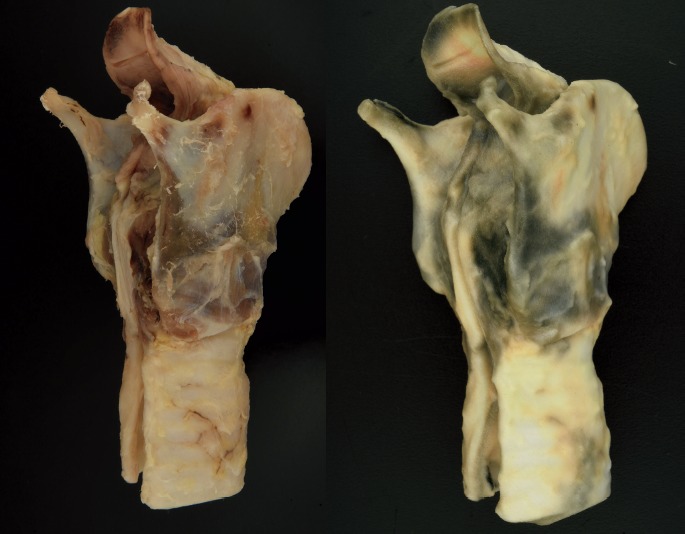
Side-by-side comparison of actual larynx specimen (left) and three-dimensional printed model (right) demonstrating highly accurate reproduction.
Footnotes
ETHICAL APPROVAL
As per Journal Policies, ethical approval was not required for this manuscript
STATEMENT OF HUMAN AND ANIMAL RIGHTS
This article does not contain any studies conducted with animals or on living human subjects
STATEMENT OF INFORMED CONSENT
No identifiable personal data were presented in this manuscsript
DISCLOSURES & DECLARATION OF CONFLICTS OF INTEREST
This work was presented at the 2017 NAME Annual Meeting. The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest
FINANCIAL DISCLOSURE The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript
References
- 1).Shields L.B., Hunsaker D.M., Hunsaker JC 3rd. Autoerotic asphyxia: part I. Am J Forensic Med Pathol. 2005. Mar; 26(1): 45–52. PMID: 15725776. 10.1097/01.paf.0000153998.44996.fd. [DOI] [PubMed] [Google Scholar]
- 2).Schott J.C., Davis G.J., Hunsaker JC 3rd. Accidental electrocution during autoeroticism: a shocking case. Am J Forensic Med Pathol. 2003. Mar; 24(1): 92–5. PMID: 12605007. 10.1097/01.PAF.0000052754.37280.10. [DOI] [PubMed] [Google Scholar]
- 3).Sauvageau A., Racette S. Aqua-eroticum: an unusual autoerotic fatality in a lake involving a home-made diving apparatus. J Forensic Sci. 2006; 51(1): 137–139. PMID: 16423240. 10.1111/j.1556-4029.2005.00031.x. [DOI] [PubMed] [Google Scholar]
- 4).Shields L.B., Hunsaker D.M., Hunsaker JC 3rd et al. Atypical autoerotic death: part II. Am J Forensic Med Pathol. 2005. Mar; 26(1): 53–62. PMID: 15725777. 10.1097/01.paf.0000153995.07817.9f. [DOI] [PubMed] [Google Scholar]
- 5).Byard R.W., Masoumi H., Haas E. et al. Could intra-alveolar hemosiderin deposition in adults be used as a marker for previous asphyxial episodes in cases of autoerotic death? J Forensic Sci. 2011. May; 56(3): 627–9. PMID: 21361942. 10.1111/j.1556-4029.2011.01716.x. [DOI] [PubMed] [Google Scholar]
- 6).Feigin G. Frequency of neck organ fractures in hanging. Am J Forensic Med Pathol. 1999. Jun; 20(2): 128–30. PMID: 10414650. 10.1097/00000433-199906000-00004. [DOI] [PubMed] [Google Scholar]
- 7).Nikolic S., Micic J., Atanasijevic T. et al. Analysis of neck injuries in hanging. Am J Forensic Med Pathol. 2003. Jun; 24(2): 179–82. PMID: 12773858. 10.1097/01.PAF.0681069550.31660.f5. [DOI] [PubMed] [Google Scholar]
- 8).Bockholdt B., Hempelmann M., Maxeiner H. Experimental investigations of fractures of the upper thyroid horns. Leg Med (Tokyo). 2003. Mar; 5 Suppl 1: S252–5. PMID: 12935603. 10.1016/s1344-6223(02)00142-6. [DOI] [PubMed] [Google Scholar]
- 9).Maxeiner H. [Healed fractures of the larynx and lingual bone in forensic autopsy]. Arch Kriminol. 1999. May-Jun; 203(5-6): 175–83. German. PMID: 10418669. [PubMed] [Google Scholar]
- 10).Ebert L.C., Thali M.J., Ross S. Getting in touch–3D printing in forensic imaging. Forensic Sci Int. 2011. Sep 10; 211(1-3): e1–6. PMID: 21602004. 10.1016/j.forsciint.2011.04.022. [DOI] [PubMed] [Google Scholar]