

Abstract
The explosive effects of lightning have been known to exist for some time; however the precise risks associated with it have been generally unknown. This curious injury phenomenon has existed historically under many different names in the literature: “lightning's pressure blast wave,” “arc blast,” “shattering effects of lightning,” “pressures developed by arcs,” “thunder generation of shock waves,” and “the sixth mechanism of lightning injury” are but a few of the many divergent and disparate terminologies used in the past to describe this invisible blast phenomenon. Blunt force trauma injuries and barotrauma injuries are often identified on lightning strike victims. Lightning's pressure blast wave and its associated overpressure does appear to have significant injury implications associated with it. This paper takes an in-depth look at the explosive effects of lightning and the main blast-related pathologies seen on lightning strike victims. Knowledge and insight into this phenomenon may help forensic pathologists and those working in the fields of lightning injury and lightning protection. A general literature search of the medical, the electrical engineering, and the mechanical engineering literature was conducted. By looking exclusively at the pathology of barotrauma in the human body, forensic pathologists may now get a relatively good idea as to the possible overpressures and distances involved with regards to lightning's explosive effects.
Keywords: Forensic pathology, Arc blast, Barotrauma, Explosive barotrauma, Explosive effect, Lightning, Pressure blast wave, Shock wave, Thermobaric effect, Risks
Introduction
Lightning may be defined as a transient, high-current electric discharge whose path length is generally measured in kilometers. The electric current involved in lightning strikes is direct current (DC) on the order of 30 000 to 50 000 Amps (1).
Lightning's pressure blast wave has been known to exist since the time of Gaius Plinius Secundus, better known as Pliny the Elder (AD 23 – August 25, AD 79). Pliny's dictum was that “the man who sees the lightning flash and hears the thunder, is not the one to be struck” (2).
One can hear thunder from as far away as 25 km, which means that there is a tremendous amount of energy involved in the generation of thunder (3). However, before thunder exists, there is a pressure blast wave. This pressure blast wave is caused by the superheating of the air around the lightning channel, which travels at supersonic speeds. It is this supersonic blast wave which decays, within meters, and transforms into thunder. Many people think that lightning injures humans chiefly due to its electricity and heat. While this is true for the vast majority of lightning-related deaths and injuries, the accompanying pressure blast wave (overpressure) can also do serious harm. Lightning causes an instantaneous superheating and expansion of the air close to the victim's body, followed almost immediately by an implosion as the air rapidly cools.
The lightning channel is a narrow channel containing ionized air molecules. The previously neutral air molecules split into positive ions (molecules missing electrons) and negative free electrons. The presence of the positive ions and negative free electrons makes the channel conductive and current can flow along the channel and the charged cloud is able to discharge through the channel to the earth, which is what we see as lightning.
During a lightning strike, the channel temperature will be raised to about 25 000 K in a few microseconds and the pressure in and around the channel may increase above atmospheric pressure as a result of Charles' Law (Figure 1). The resulting rapid expansion of the air creates a shock wave. This shock wave may injure a human being located in the close vicinity of the lightning flash. The overpressure generated by thunder at the source may approach 1470 pounds of force per square inch (psi) (4).
Figure 1:
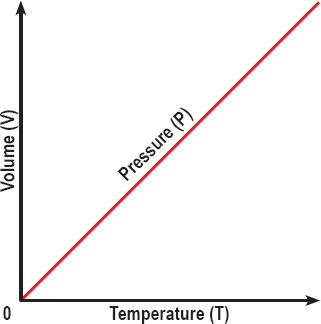
Charles Law is an experimental gas law which describes how gases tend to expand when heated. When the pressure on a sample of a dry gas is held constant, the temperature and the volume will be directly related.
Hill's work for a 30 000 Amp lightning strike shows the following: 588 psi at 0.75 cm radius from the stroke channel, 426 psi at 1.1 cm radius from the stroke channel, 279 psi at 2 cm radius from the stroke channel, and 132 psi at 4.1 cm radius from the channel (5). This shows a near inverse relationship between the pressure and the distance. Calculations by Hill therefore show that the overpressure within a few centimeters of the lightning channel may reach about 147 psi to 294 psi.
Cooray et al. reported that injuries can be caused by shock waves created by the lightning channel, although they did not commit to a specific distance within which a victim would be at risk from blast wave injury. In addition to causing damage in the ears and eyes, this shock wave may also cause damage to other internal organs such as the spleen, liver, the lungs, and the gastrointestinal tract. Moreover, it may displace the victim suddenly from one place to another, causing head and other traumatic injuries (6).
Evidence of barotrauma (Figures 2 and 3) does exist on lightning strike victims. Lightning's pressure blast wave has been known to tear and tatter clothing, fracture long bones, rupture eardrums and damage lungs. The blast causes a pocket of air behind the sternum (pneumomediastinum) and it may cause injury to the chest wall and lungs. These findings are similar to what one would expect to find in bomb explosion victims. Lightning has even been known to cause secondary missile injury. One victim had multiple small fragments of exploded concrete embedded within her skin, after the lightning struck the pavement (7).
Figure 2:
Lightning explosive barotrauma, imagined as a “pressure shockwave” immediately surrounding lightning's luminous channel.
Figure 3:

Proposed appearance of lightning's “pressure shockwave.” Please keep in mind that the lightning channel is three-dimensional.
As forensic pathologists we would need to know within what range a human would be at risk and the risk of lightning's pressure blast wave. A general literature search of the medical, electrical engineering, and mechanical engineering literature was conducted.
Keywords were difficult to locate as this curious injury phenomenon has existed historically under many different names in the literature: “lightning's pressure blast wave,” “arc blast,” “shattering effects of lightning,” “pressures developed by arcs,” “thunder generation of shock waves,” and “the sixth mechanism of lightning injury” are but a few of the many divergent and disparate terminologies used in the past to describe this invisible blast phenomenon (3, 8-10).
Discussion
Overpressure (or blast overpressure) is the pressure caused by a shockwave over and above normal atmospheric pressure. Overpressures in this paper have been presented in the same format as they have been presented in previous papers. None of the previous literature took into consideration the “rate of change” of overpressure. Using standard conversion tables, all findings have been expressed in pound-force per square inch (psi).
One psi is the equivalent of 0.068046 atmospheres, which is the equivalent of 6.89476 kilopascals.
There exists a relatively large literature which addresses damage approximations from high explosive overpressures, human injury in proximity to a small bomb, and the predicted injuries and fatalities from direct blast effect of explosions (11,12).
The Otorhinological Medical Literature
There is evidence in the literature supporting the fact that lightning can rupture eardrums (13-22). By looking exclusively at the pathology of trauma of tympanic membrane rupture, forensic pathologists may now get a relatively good idea as to the possible overpressures and distances involved with regards to lightning explosive barotrauma in the field (8,23). The medical ear, nose and throat (otorhinological) literature sometimes describes the tympanic membrane following lightning strike as “a large tympanic membrane perforation with ossicular chain disruption” (19). Proposed mechanisms of injury have included concussive “blast” effect on the ear, “direct” effect of electrical conduction, “splash” effect, “cylindrical shock wave of electrons,” and/or direct “thermal burn” (13-21, 24, 25). The human tympanic membrane is able to withstand a limited amount of overpressure before failure. Overpressures are required to produce minor, moderate, and major eardrum ruptures.
Rupture of the normal eardrum is a function of age as well as of the effective blast pressure. Tympanic membranes may, for example, rupture more easily in the young. Failures have been reported at overpressures as low as 5 psi ranging up to 40 or 50 psi. As mentioned earlier, calculations by Hill showed that the overpressure within a few centimeters of the lightning channel can reach about 147 psi to 294 psi (5). A study by Richmond suggests a minimum threshold of about 29 psi to produce minor eardrum ruptures (Table 1) (26).
Table 1:
| Overpressure (or blast overpressure) | Predicted Injuries |
|---|---|
| 29 psi | Minimum threshold required to produce minor eardrum ruptures |
| 40 to 50 psi | Rupture of the normal eardrum |
| 29 psi to 72.5 psi | Chest and/or lung trauma |
| 40 psi (30 psi – 50 psi) | Minimum threshold for lethality |
| 62 psi (50 psi – 75 psi) | Fifty percent lethality |
| 92 psi (75 psi – 115 psi) | One-hundred percent lethality |
| 100 psi | Possible disruption and/or disfigurement |
One can therefore deduce from human victims with tympanic membrane rupture, that lightning's blast wave must have had a minimum overpressure of approximately 29 psi.
The Chest and the Lung Medical Literature
There appears to be relatively good data for chest and lung damage by blast waves in the literature. Lightning has also been known to cause damage to the chest and lungs. Pneumomediastinum and hemorrhage from a lung in a tracheostomized patient have both been reported (24, 27-29). The bomb blast literature shows that the threshold for lung damage is in the range of 12 psi (8 to 15 psi) and the range for severe lung damage is in the range of 25 psi (20 to 30 psi) (11). Posttraumatic pneumomediastinum is not a cause for alarm amongst clinicians (28). Pneumomediastinum is therefore generally not considered a fatal injury. The literature suggests that lung damage requires approximately 29.0 to 72.5 psi barotrauma.
Other Medical Literature
Lightning has also been implicated in the fractures of bones and rupture of internal organs (30,31). Bowel contusion has been reported in the direct transmission of a detonation Shockwave (32). No associated overpressure data could be found in the bomb blast and explosive literature in this regard.
In addition to causing damage in the ear and eyes, this shock wave can also cause damage to other internal organs such as the spleen, liver, and the bowel tract (33). Moreover, it may displace the victim suddenly from one place to another causing head and other traumatic injuries (6). No associated overpressure data could be found in the literature in regard to these injuries.
The human body can survive relatively high blast overpressures without experiencing barotrauma (32). There is no evidence to suggest that lightning victims suffer severe blast-related disfigurement. There is no evidence to suggest that lightning would rip a cavity in human flesh, for example.
When looking at tentative criteria for direct (primary) blast effects in man from fast-rising, long-duration pressure pulses (such as a bomb explosion), the threshold for lethality would be in the 40 psi (30 to 50 psi) range. Fifty percent lethality would be in the 62 psi (50 to 75 psi) range. One-hundred percent lethality would be in the 92 psi (75 to 115 psi) range. About 100 psi is the minimum threshold for serious damage (with possible disruption) to humans (11, 12, 32, 34).
In summary, a 35 to 45 psi overpressure may cause 1% fatalities, and 75 to 115 psi overpressure may cause 99% fatalities in bomb blasts (11).
Should a forensic pathologist find a human barotrauma victim with disfiguring barotrauma (in other words, disruption), he/she could theoretically deduce that the blast wave must have had a minimum overpressure of approximately 100 psi. Halldorsson et al. believed that this explosion/implosion phenomenon surrounding the lightning channel may cause trauma which may mimic the patterns of blast injuries seen in bomb blast victims (29).
Conclusion
Review articles of tympanic membrane rupture in humans in relation to various blast pressure-time patterns suggest that the tympanic membrane can withstand a limited amount of pressure. Overpressures are required to produce minor, moderate and major eardrum ruptures. Tympanic membranes tend to rupture more easily in the young for example. The eardrum may rupture at pressures above 29.0 psi. We can therefore deduce from the otolaryngological literature that lightning's blast wave must have a minimum overpressure of approximately 29.0 psi.
The literature shows that posttraumatic pneumomediastinum is not a cause for alarm amongst our clinical colleagues (28). Pneumomediastinum is not generally considered a fatal injury. It would appear that lung damage requires approximately 29.0 to 72.5 psi to induce.
We know that lightning victims do not suffer severe blast-related disfigurement. To be fatally injured by a bomb blast, one has to be in the immediate vicinity of the explosion, within about a meter or so (the “kill zone”). About 100 psi is the minimum estimated threshold for serious damage (disruption) to humans (34).
From the aforementioned results of the literature review, it is now possible to estimate at what range a human would possibly be at risk from lightning's pressure blast wave. A 10 lb (4.5 kg) trinitrotoluene or TNT equivalent bomb would rupture an eardrum (of a 70 kg male) within about 10 meters; lung damage would occur at about 5 meters, and the body would be injured at about 3 meters (11).
If one knew the initial conditions of the lightning strike (the thermodynamics and flow parameters as a function of radius at selected instants of time) then one could possibly calculate a numerical solution to this thermobaric phenomenon; however there are always varying initial conditions, for example, the magnitude and strength of the lightning discharge.
In conclusion, it is therefore possible to estimate, based exclusively on the victim's pathology of barotrauma, the minimum overpressure to which a lightning victim was exposed and the possible distance from the lightning channel.
Footnotes
Financial Disclosure
The author has indicated that he does not have financial relationships to disclose that are relevant to this manuscript
ETHICAL APPROVAL
As per Journal Policies, ethical approval was not required for this manuscript
STATEMENT OF HUMAN AND ANIMAL RIGHTS
This article does not contain any studies conducted with animals or on living human subjects
STATEMENT OF INFORMED CONSENT
No identifiable personal data were presented in this manuscsript
DISCLOSURES & DECLARATION OF CONFLICTS OF INTEREST
This work was presented at the 2015 NAME Annual Meeting. The author, reviewers, editors, and publicationstaff do not report any relevant conflicts of interest
References
- 1.Uman M.A. Lightning. New York: McGraw-Hill; 1969. 264 p. [Google Scholar]
- 2.Critchley M. Neurological effects of lightning and of electricity. Lancet. 1934. Jan; 223(5759): 68–72. 10.1016/s0140-6736(01)03101-4 [DOI] [Google Scholar]
- 3.Rakov V.A., Uman M.A. Lightning: physics and effects. Cambridge (UK): Cambridge University Press; 2003. 687 p. [Google Scholar]
- 4.Ritenour A.E., Morton M.J., McManus J.G. et al. Lightning injury: a review. Burns. 2008. Aug; 34(5): 585–94. PMID: 18395987. 10.1016/j.burns.2007.11.006. [DOI] [PubMed] [Google Scholar]
- 5.Hill R.D. Channel heating in return-stroke lightning. J Geophys Res. 1971. Jan; 76(3): 637–45. 10.1029/jc076i003p00637. [DOI] [Google Scholar]
- 6.Cooray V., Cooray C., Andrews C.J. Lightning caused injuries in humans. J Electrostatics. 2007. May; 65(5-6): 386–94. 10.1016/j.elstat.2006.09.016. [DOI] [Google Scholar]
- 7.Blumenthal R. Secondary missile injury from lightning strike. Am J Forensic Med Pathol. 2012. Mar; 33(1): 83–5. PMID: 22104330. 10.1097/paf.0b013e31823a8c96. [DOI] [PubMed] [Google Scholar]
- 8.Lee R.H. The shattering effect of lightning-pressure from heating of air by stroke current. IEEE Trans Ind Appl. 1986. May-Jun; IA-22(3): 416–9. 10.1109/tia.1986.4504735. [DOI] [Google Scholar]
- 9.Lee R.H. Pressures developed by arcs. IEEE Trans Ind Appl. 1987. Jul-Aug; IA-23(4): 760–3. 10.1109/tia.1987.4504977. [DOI] [Google Scholar]
- 10.Blumenthal R., Jandrell I.R., West N.J. Does a sixth mechanism exist to explain lightning injuries?: investigating a possible new injury mechanism to determine the cause of injuries related to close lightning flashes. Am J Forensic Med Pathol. 2012. Sep; 33(3): 222–6. PMID: 21952103. 10.1097/paf.0b013e31822d319b. [DOI] [PubMed] [Google Scholar]
- 11.Glasstone S., Dolan P.J. The effects of nuclear weapons. 3rd ed. Washington: U.S. Department of Defence and U.S. Department of Energy; US Government Printing Office; 1977. 653 p. [Google Scholar]
- 12.Kinney G.F., Graham K.J. Explosive shocks in air. 2nd ed. New York: Springer Verlag; 1985. 269 p. [Google Scholar]
- 13.Bergstrom L., Neblett L.W., Sando I. et al. The lightning-damaged ear. Arch Otolaryngol. 1974. Aug; 100(2): 117–21. PMID: 4843111. 10.1001/archotol.1974.00780040123008. [DOI] [PubMed] [Google Scholar]
- 14.Wright J.W. Jr., Silk K.L. Acoustic and vestibular defects in lightning survivors. Laryngoscope. 1974. Aug; 84(8): 1378–87. PMID: 4411819. 10.1288/00005537-197408000-00013. [DOI] [PubMed] [Google Scholar]
- 15.Weiss K.S. Otologic lightning bolts. Am J Otolaryngol. 1980. Aug; 1(4): 334–7. PMID: 7446850. 10.1016/s0196-0709(80)80036-6. [DOI] [PubMed] [Google Scholar]
- 16.Bellucci R.J. Traumatic injuries of the middle ear. Otolaryngol Clin North Am. 1983. Aug; 16(3): 633–50. PMID: 6634185. [PubMed] [Google Scholar]
- 17.Kristensen S., Tveterås K. Lightning-induced acoustic rupture of the tympanic membrane: (a report of two cases). J Laryngol Otol. 1985. Jul; 99(7): 711–3. PMID: 4020264. 10.1017/s0022215100097528. [DOI] [PubMed] [Google Scholar]
- 18.Jones D.T., Ogren F.P., Roh L.H., Moore G.F. Lightning and its effects on the auditory system. Laryngoscope. 1991. Aug; 101(8): 830–4. PMID: 1865731. 10.1288/00005537-199108000-00006. [DOI] [PubMed] [Google Scholar]
- 19.Redleaf M.I., McCabe B.F. Lightning injury of the tympanic membrane. Ann Otol Rhinol Laryngol. 1993. Nov; 102(11): 867–9. PMID: 8239348. 10.1177/000348949310201108. [DOI] [PubMed] [Google Scholar]
- 20.Gordon M.A., Silverstein H., Willcox T.O., Rosenberg S.I. Lightning injury of the tympanic membrane. Am J Otol. 1995. May; 16(3): 373–6. PMID: 8588633. [PubMed] [Google Scholar]
- 21.Gluncić I., Roje Z., Gluncić V., Poljak K. Ear injury caused by lightning: report of 18 Cases. J Laryngol Otol. 2001. Jan; 115(1): 4–8. PMID: 11233621. 10.1258/0022215011906858. [DOI] [PubMed] [Google Scholar]
- 22.Modayil P.C., Lloyd G.W., Mallik A., Bowdler D.A. Inner ear damage following electric current and lightning injury: a literature review. Eur Arch Otorhinolaryngol. 2014. May; 271(5): 855–61. PMID: 23649510. 10.1007/s00405-013-2544-7. [DOI] [PubMed] [Google Scholar]
- 23.Malan D.J. Physics of lightning. London: English Universities Press; 1963. 176 p. [Google Scholar]
- 24.Soltermann B., Frutiger A., Kuhn M. Lightning injury with lung bleeding in a tracheotomized patient. Chest. 1991. Jan; 99(1): 240–2. PMID: 1984964. 10.1378/chest.99.1.240. [DOI] [PubMed] [Google Scholar]
- 25.Andrews C.J., Darveniza M. Further study of the functional and structural changes after lightning strike with special emphasis on special sense orifices as portals of entry. Paper presented at: Proceedings of the 9th International Conference on Atmospheric Electricity; 1992. Jun 15-19; St Petersburg, Russia. [Google Scholar]
- 26.Richmond D.R., Yelverton J.T., Fletcher E.R., Phillips Y.Y. Physical correlates of eardrum rupture. Ann Otol Rhinol Laryngol Suppl. 1989. May; 140: 35–41. PMID: 2497697. [DOI] [PubMed] [Google Scholar]
- 27.Moulson A.M. Blast injury of the lungs due to lightning. Br Med J (Clin Res Ed). 1984. Nov 10; 289(6454): 1270–1. PMID: 6437514. PMCID: PMC1443487. 10.1136/bmj.289.6454.1270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bouwen L., Bosmans E. Posttraumatic pneumomediastinum: not always a cause for alarm. Acta Chir Belg. 1997. Jun; 97(3): 145–7. PMID: 9224521. [PubMed] [Google Scholar]
- 29.Halldorsson A., Couch M.H. Pneumomediastinum caused by a lightning strike. J Trauma. 2004. Jul; 57(1): 196–7. PMID: 15284576. 10.1097/01.ta.0000119167.63219.11. [DOI] [PubMed] [Google Scholar]
- 30.Graber J., Ummenhofer W., Herion H. Lightning accident with eight victims: case report and brief review of the literature. J Trauma. 1996. Feb; 40(2): 288–90. PMID: 8637081. 10.1097/00005373-199602000-00020. [DOI] [PubMed] [Google Scholar]
- 31.Kannan R.Y., Chester D.L., Titley O.G. Combined Bennett's fracture subluxation and scapho-trapezio-trapezoidal dislocation secondary to lightning strike. J Trauma. 2004. Dec; 57(6): 1351–3. PMID: 15625477. 10.1097/01.ta.0000151251.58008.9a. [DOI] [PubMed] [Google Scholar]
- 32.Mason J.K., Purdue B.N. The pathology of trauma. 3rd ed. London: Hodder Arnold; 2000. 516 p. [Google Scholar]
- 33.Barmate N.S., Tumram N.K., Singh R.K., Shrigiriwar M.B. A rare case of blast effect by lightning. J Forensic Res. 2014. Nov; 5(6): 248 10.4172/2157-7145.1000248. [DOI] [Google Scholar]
- 34.Saukko P., Knight B. Knight's forensic pathology. 3rd ed. London: Hodder Arnold; 2004. 720 p. [Google Scholar]