

Abstract
Imaging technologies play an integral role in forensic anthropology cases. Advances in digital photography allow the anthropologist to photo-document the scene and skeletal remains in exceptional detail. Traditionally, radiographs have been used to document remains, potential trauma, and any individualizing characteristics such as healing trauma and frontal sinus morphology. Given technological advances, some forensic anthropologists have begun to incorporate more advanced imaging methods in their case analyses and research, such as computed tomography and three-dimensional (3D) surface scans. These advanced imaging technologies provide a means to document skeletal remains and trauma, and can be used to create 3D replicas of the elements for archival and illustrative purposes. Researchers have begun to develop novel methods for estimating biological parameters from these 3D virtual models, using new variables such as surface areas and volumes, and advanced statistical methods (e.g., geometric morphometric analyses) to quantitatively analyze skeletal variation for sex and ancestry estimation. The use of these technologies in forensic anthropology remains somewhat limited, however, due to required costs, expertise, and the time involved in collecting and processing the data. Newly developed methods require further validation, and some areas of advanced imaging, such as photogrammetry, remain relatively unexplored in the field. Interdisciplinary collaborations between forensic anthropologists and other medicolegal professionals can help alleviate some of these resource constraints and facilitate advancements in forensic case analysis and research.
Keywords: Forensic pathology, Computed tomography, Radiography, Photogrammetry, Surface scans, 3D models
Introduction
Technological advances, particularly in medical and engineering fields, have resulted in a wide array of advanced imaging techniques, such as computed tomography and three-dimensional (3D) surface scans. As these imaging techniques become more commonplace and the costs associated with them begin to decrease, we are seeing them more frequently incorporated into the field of forensic anthropology. Beyond the traditional use of photographs and radiographs, forensic anthropologists are now using virtual 3D models of skeletal material for case analyses, documentation, and research. This paper reviews the types of traditional and advanced imaging technologies that are currently incorporated into forensic anthropological analyses in order to familiarize professionals in associated disciplines with these recent advancements and their utility to the field. Despite their potential benefit, not all forensic anthropologists employ these technologies, and the current limitations with regards to cost, access, and utilization of advanced imaging will be discussed. One way to alleviate many of these limitations involves interdisciplinary collaborations between researchers and professionals, particularly with forensic pathologists. Through such collaborations, advanced imaging can be a valuable tool not only for case documentation, but may also be used to help identify the deceased and provide insight regarding circumstances surrounding their death.
Discussion
Photography
All professionals within forensic disciplines understand the importance of photography for the purpose of case documentation. Forensic anthropologists and forensic pathologists each work with human remains. Those remains are expected to be returned to family members in a timely fashion, at which point any evidence is lost if it is not thoroughly documented through written notes and photography. For this reason, forensic anthropologists are trained to document everything photographically. If the forensic anthropologist is called to the scene to search for and recover human remains, the photographic documentation begins immediately at scene arrival. The entire search and recovery procedure is photo-documented by a member of the team and thus can be used to reconstruct the actions and timeline of the search and recovery. These photographs can be useful when describing the recovery procedures in the report, as well as in courtroom testimony. In addition, any discovered material or biological evidence is photographed in situ, before it is collected. In this manner, the original position of the remains and evidence and their context to the scene are preserved. The context of the remains may provide information regarding the position of the body, time since death, whether it is a primary or secondary depositional site, and whether the remains have been moved by taphonomic agents. Once the remains are transported to the laboratory, they are photographed again in order to document their initial condition (e.g., amount and condition of soft tissue). Any suspicious defects are also photographed at this point so that it can be shown that the defects were present upon arrival to the lab and are not an artifact of any subsequent processing procedures. Of course, scales are included in all photographs so that size is documented. After the remains are processed and cleaned, another round of photographs is taken to capture the postprocessing condition of the remains. Any individualizing features, traumatic defects, or taphonomic modifications are thoroughly documented photographically. It is standard operating procedure (SOP) to also photograph all six views of the skull, the dentition, and all skeletal features used in sex, age, and ancestry estimation. A well-equipped laboratory may have a microscope from which digital microscopic or macroscopic images can be captured. These images may be used to document sharp force trauma (e.g., cut marks and characteristics of those cut marks such as striations and kerf floor), characteristics of compression and tension on fracture surfaces, periosteal reactions, or characteristics of taphonomic modifications (e.g., rodent and carnivore damage) (Image 1). Given that digital photographs are easy to take, can be reviewed immediately, and stored easily, it is not uncommon to take over 100 photographs of a single case. All photographs, even those of poor quality or those taken erroneously, are saved in order to show the continuity in the sequence of photograph numbers and illustrate that no photographs had been deleted (either mistakenly or intentionally). Of course, all photographs must have a backup file and be stored in a secure location. Photographs taken throughout the case may be used to support written documentations in case reports, although the amount of detail provided in forensic anthropology case reports varies by institution. If questions arise about the case after the remains have been returned, the forensic anthropologist can refer back to the photographs. If a case goes to court, the photographs can be used in conjunction with the report to refresh the anthropologist's memory of the case and provide useful visualizations during testimony so that judges and jurors can see for themselves the recovery procedures or skeletal characteristics being described by the forensic anthropologist. Images can, and arguably should, be shared between the medical examiner and forensic anthropologist. In forensic anthropological cases in which a prior autopsy was performed, photographs from the autopsy will help the anthropologist understand the original condition of the remains and identify any skeletal modifications which may have occurred during or post-autopsy. Skeletal regions associated with any soft tissue defects can also be identified and closely evaluated by the forensic anthropologist. By sharing photographs of the findings, forensic anthropologists and pathologists can also continue to learn from one another. The body acts as a single functional unit, with the soft tissues and skeleton closely integrated, and as such, both the soft and hard tissues should be considered, as well as their relationship, when interpreting human skeletal variation and trauma.
Image 1.

Example of photo-documentation of sharp force trauma (and associated blunt force trauma) to right radius and ulna. Insets A-D were taken with a Leica MZ16A stereo microscope.
Radiographs
Although radiography may no longer be considered a form of advanced imaging given current technological advancements, it is the most highly utilized imaging modality in forensic anthropology besides basic photography. Most forensic anthropology laboratories are equipped with some type of X-ray machine, although the type of equipment may vary. Some laboratories are equipped with a closed, cabinet system, such as a Faxitron, while others have open X-ray systems similar to those used clinically in hospitals. If the laboratory is fortunate, then they have a digital X-ray system, which can result in immediate viewing of the radiographs, allowing the anthropologist to quickly assess whether the settings and position of the remains are optimal.
Documentation and Trauma
In many respects, the forensic anthropologist uses radiography in much of the same way as a forensic pathologist. In cases of suspected gunshot wounds, radiographs are taken not only to search for any potential bullets or bullet fragments, but also to identify any other areas of lead transfer. We have seen cases where even in completely skeletonized crania that have been exposed to the elements for a prolonged period of time, lead can still be observed radiographically around entrance and exit wounds, or on other endocranial surfaces impacted by the bullet. Thus, documentation of the lead transfer can help the forensic anthropologist decipher the bullet trajectory.
Radiographs are also used to search for and document other forms of trauma, such as fracture patterns. It should be part of every forensic anthropology laboratory's SOPs to radiograph all remains upon receipt, regardless of their condition. Not all of the cases received by forensic anthropologists are completely skeletonized. There may be mummified or decomposing tissue adhering to the remains, and in some cases the bodies may be mostly fleshed. By radiographing all remains upon receipt, the forensic anthropologist can later show that fractures or other skeletal trauma were present and documented prior to any processing. In other words, the anthropologist can empirically demonstrate that the trauma observed is not a result of maceration or other processing procedures. By radiographing any large masses of decomposing tissue, the anthropologist can confirm that all skeletal elements or potential evidence is recovered.
Even when remains are completely skeletonized, all elements should be radiographed. As mentioned previously, lead transfer has been found in cases in which the remains are completely skeletonized. In addition, the radiographs may reveal useful characteristics in the internal bone structures. For example, epiphyseal lines of fusion may be visible radiographically, supplying information about the age of the individual. Radiographs may reveal signs of bony remodeling or disruption in the trabecular bone pattern, which could be indicative of antemortem trauma, which in turn may be helpful in identifying the decedent or recognizing signs of potential abuse.
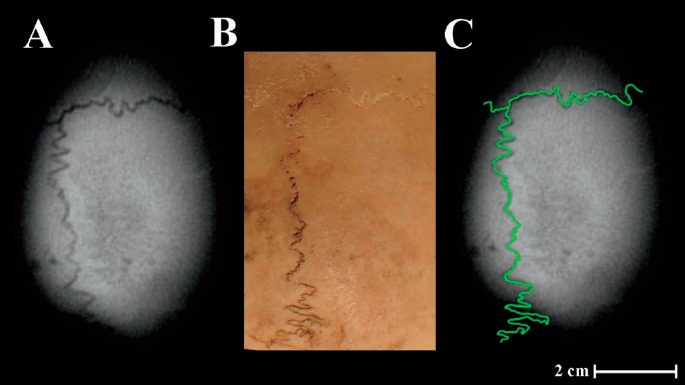
In cases of suspected child abuse, we recommend radiographing (and photographing) the remains on three separate occasions: 1) upon receipt, 2) after removal of the majority of soft tissue (but prior to any maceration or removal of the epiphyses), and 3) after processing. This is done regardless of whether clinical radiographs were taken, as we find that in many cases the anthropological radiographs may reveal additional evidence of trauma (1). The sequence of radiographs are important in illustrating that the trauma, such as periosteal reactions and metaphyseal fractures, was visible prior to any processing, especially given the fragility of infant and child remains (Image 2). Once the soft tissue is removed, the remains can be oriented in various positions to optimally capture any potential trauma, which is not always possible in clinical settings. For example, clinically there is a large amount of overlap in regions of the ribs. Once disarticulated, however, the ribs may be radiographed individually or spaced in such a manner that any potential antemortem or perimortem trauma can be easily evaluated.
Image 2.

Evidence of antemortem trauma to infant left humerus. A) Post-processing photograph illustrating a large bony callus (orange arrow) and abnormal remodeling to the distal metaphysis (yellow arrow). B) Mid-processing radiograph taken once the majority of soft tissue was removed but before the removal of the epiphyses. A healing metaphyseal corner fracture is evident (green arrow) which attributes to the metaphyseal remodeling, and an additional layer of bone has been laid down over the distal portion of the lateral diaphysis (blue arrow), suggesting additional trauma. Both the osteological and radiographic examinations corroborate one another, but each provides unique information.
Biological Profile and Identification
Forensic anthropologists may also use radiographs to help assess the age of an unknown individual. This is particularly true for infant or subadult individuals. The pattern of presence or absence of primary and secondary ossification centers and epiphyseal fusion can be used to age fetal, infant, and subadult remains (2–6). Partially fused epiphyses may appear fused macroscopically, but when viewed radiographically, a radiopaque line of fusion remains evident. Patterns of dental formation and eruption, which are also used for juvenile age estimation (7), are best evaluated radiographically in order to assess any unerupted dentition. In adults, where age estimation is predominantly based on deterioration of the skeleton instead of growth and development, the utility of radiographs for age estimation is more limited. Radiographic analysis of laryngeal and costal cartilage ossification may provide broad age estimates (8–10), and signs of osteoporosis and osteoarthritis may evaluated. Many of the traditional areas of the skeleton used for adult age estimation (i.e., cranial sutures, sternal rib ends, auricular surface, and pubic symphysis), however, undergo morphological changes that are not easily captured with conventional radiographs.
There is also a potential to use radiographs in cases of fleshed remains to estimate sex, ancestry, and stature. For example, previous studies have shown that costal cartilage ossification, as examined radiographically, may also be useful in estimating the sex of an individual (8, 10,11). In general, however, radiographic methods in estimating biological profile parameters have yet to be thoroughly researched. Theoretically, most of the skeletal features that forensic anthropologists use to estimate these biological parameters should be visible in radiographs (e.g., greater sciatic notch or nasal aperture shape) and if these features could be evaluated radiographically, then it could possibly eliminate the need for more invasive methods such as maceration in certain situations. In order to develop and apply such methods, however, radiographic procedures would have to be standardized. In a radiograph, a three-dimensional object is projected into a two-dimensional (2D) space; thus, there are problems with superimposition of structures, which may obscure some features. Any variation in the positioning of the remains during the X-ray process will result in different angles in the features, making shape evaluation and any type of measurement collection problematic. Scales are also required if any type of measurements are to be collected and analyzed. Forensic anthropologists and pathologists may be able to work together to develop such protocols and potentially develop new radiographic methods to create a preliminary biological profile from radiographs in a fleshed individual. There is also the potential for distortion in radiographs caused by parallax and magnification error (12–14). There is a radiographic system called Lodox Statscan that uses a slot-scanning technology opposed to the normal cone-beam technology, thereby alleviating distortion issues (15–17). While this technology is becoming more common in medical examiner's offices (MEOs), it still cannot address the superimposition issues.
Forensic anthropologists have also utilized radiographs to assist with positive identifications. Just as forensic odontologists use comparisons of antemortem and postmortem dental radiographs to make an identification, forensic anthropologists can radiographically compare other regions of the skeleton. For example, a number of studies have illustrated that frontal sinus morphology, as viewed radiographically, is unique among individuals and can be reliably used for forensic identifications (18–21). Other radiographic studies have used unique bone shapes and features (22–31), suture patterns (32) or even trabecular bone patterns (33–35) to assist with identification. This can be particularly useful in mass disaster settings, where antemortem information can be gathered from the finite pool of potential victims (36). Arguably, skeletal variations in any region of the body may be useful for presumptive or positive identification, and thus it is important to provide copies of any antemortem radiographs to the forensic anthropologist along with the skeletal remains so that they might evaluate any unique morphologies.
Research
Given the ease of collection and availability of radiographs, they also provide an opportunity to create large radiographic databases for research purposes. For example, the Denver Growth Study (37, 38) and the Fels Longitudinal Study (39) consist of series of radiographs taken at regular intervals from infancy through adulthood in a sample of individuals. These studies provide a valuable opportunity for longitudinal studies in growth and development. Another database, known as PATRICIA (40) consists of pediatric radiographs from more than 9000 subadults collected from U.S. medical examiner's offices. A similar database, consisting of adult and juvenile radiographs acquired from the North Carolina Office of the Chief Medical Examiner, is available online through North Carolina State University (NCSU) (41). This database includes individuals with trauma, thus providing a comparative learning tool. Unlike with the Fels data, which was collected specifically for research purposes following specific research protocols, the radiographs in PATRICIA and the NCSU databases were collected retrospectively from MEOs. Typically in a MEO, radiographs are taken to best capture a specific region of interest (e.g., potential trauma defects), with the body positioned however will best elucidate that feature. This limits their utility somewhat, given that there is no standardization in subject positioning or radiographic settings even within an MEO, not to mention variation between MEOs. The creation of SOPs for radiographic procedures within and between MEOs, under consultation with radiologists, technicians, and forensic anthropologists, could lead to larger databases with greater utility for forensic research.
Computed Tomography
More advanced technologies have recently been, and continue to be, incorporated in the forensic anthropologist's arsenal of imaging techniques. One such technique, computed tomography (CT) scanning, was originally developed for use in the clinical setting, and is primarily used as a medical diagnostic procedure. Computed tomography scans essentially take a series of radiographs from a full complement of angles and the resultant images are then combined using digital algorithms to produce tomographic (i.e., cross-sectional) images that can be stacked to create a virtual 3D reconstruction of the object scanned. This procedure constitutes an essentially noninvasive and nondestructive method for visualization of both the external and internal structures of materials and organisms. Since CT scanning's introduction to the mainstream medical community, major advances in safety and resolution have occurred, and along with a concomitant reduction in cost, these factors have resulted in the increasing prevalence of patients receiving CT scans. For these reasons, CT scans are also gaining traction in the worlds of research and education, bolstered by a robust and growing body of scholarly work.
Despite the obvious benefits of this technology and its potential utility for both forensic casework and research, CT scanning remains limited in use within the forensic anthropological community. Many practitioners do not have access to facilities with the necessary equipment to perform CT scanning, and even for those who do, the relatively high cost of scanning may in itself be prohibitive. Furthermore, working with CT images requires access to specialized (and expensive) computer software as well as experience with manipulating 3D datasets.
Documentation and Trauma
In forensic anthropology, CT scans can be used in variety of different ways. When performing casework, CT scanning facilitates the documentation of human remains when the soft tissue is still present and the skeletal elements remain in articulation, as opposed to post-processing, which entails disarticulation of the skeleton and removal of all soft tissue. The ability to visualize the remains nondestructively is especially important in cases where trauma is suspected, and can be especially helpful in recognizing and analyzing fractures in situ (Image 3). As discussed, remains are often radiographed in forensic anthropological laboratories to facilitate the recognition of healing antemortem fractures, gunshot wounds and perimortem fracture patterns. CT scanning can accomplish these same goals, although perhaps with even better resolution and appreciation of the spatial relationships of the object in question given CTs' three-dimensionality and depth of field.
Image 3.

Comparison of a postmortem computed tomography scan (A) and the post-processing osteological specimen (B), with a linear occipital fracture illustrated in each.
Once a CT scan is completed, the resulting data constitutes a 3D replica of the remains in question, which can then be saved and archived by the forensic anthropologist and/or forensic pathologist even once the remains have been returned to family members. This persisting digital documentation allows practitioners to refer back to a 3D digital model of the remains if any analyses are called into question, or if they testify in court. 3D printouts of the virtual skeletal models can also be created, allowing the forensic anthropologist to create a tangible example to illustrate points in court testimony as well as in the classroom. All of this can be done without extensive processing of the remains.
This idea that postmortem analyses can be completed with CT scans without invasive procedures, eventually led to the concept of virtual autopsies. Virtual autopsies, or Virtopsies, combine CT technology with magnetic resonance imaging (MRI), allowing forensic pathologists to perform a digital investigation to help determine cause and manner of death. CT scanning excels at discriminating between tissues of different densities (i.e., hard versus soft tissue) and MRI complements this with its proficiency at discerning between different soft tissue structures. The noninvasive character of Virtopsies make it beneficial, especially when cultural or religious concerns preclude a traditional autopsy. Although some pathologists have begun implementing virtual autopsies, there is still debate about its feasibility due to both the high requisite cost and level of technological expertise, as well as the scans' inability to discern coloration, which can play an important role in postmortem examinations (42–49). While U.S. MEOs have not begun to implement the full CT/MRI Virtopsy methods, many have begun to use CT scans as part of their autopsy procedure, given that costs and required expertise for CT technology has decreased considerably. Although such virtual autopsies fall under the purview of the forensic pathologist, the forensic anthropologist's skeletal expertise may still be required. Given that the data are digital, the forensic pathologist may be able to seek consultation from a forensic anthropologist anywhere on the globe.
Biological Profile and Identification
Any radiographic methods for estimating an individual's biological profile, such as the appearance of ossification centers, epiphyseal fusion, and dental eruptions patterns used in subadult analyses, can also be applied to CT data. Recent studies have also extended adult age methods in costal cartilage ossification to CT scans (50, 51). In addition, many of the skeletal analyses typically performed by forensic anthropologists on defleshed bone can also be performed on CT scans. From the 3D models created with the CT scans, standard osteometric landmarks and interlandmark distances traditionally taken with calipers on dry bone can be collected virtually. A number of studies have evaluated measurement errors when collecting craniometric landmarks and distances from CT data (52–58). Depending on the resolution of the CT scans, some researchers have found certain landmarks difficult to locate precisely, particularly those at suture intersections. CT scans do not preserve the color or texture of the objects, so suture location can only be discerned if the slice thickness is thin enough to pick up the slight indentation in those regions. Other measurements, such as maximum cranial breadth, can actually be taken semi-automatically in various software programs, removing a certain level of human error and potentially making them more accurate. Overall, results vary slightly between studies, but the general consensus is that measurements and landmark data collected from CT scans are reliable; however, many researchers advise caution when combining osteological and CT data as scan settings (e.g., slice thickness), measurement techniques (e.g., using slices versus 3D renderings), postprocessing methods (e.g., thresholds and smoothing), and even the software used to collect the virtual data may all result in measurement discrepancies (52, 54,57). Studies combining CT and osteological data are typically required to include an error study, in order to document errors using those specific scanning and measurement parameters.
Although further validation studies are required, if these landmarks and measurements are accurate, then they can be used in forensic anthropological metric analyses of sex, ancestry, and stature as well as age at death in subadults (based on long bone lengths) just as any standard measurements would be. At present, forensic anthropologists remain cautious when it comes to using virtual measurements in software programs and equations derived from standard osteometric measurements, such as using CT measurements in Fordisc 3.1 (59). Given that a number of variables can affect error rates in landmarks and distances collected from CT scans (e.g., scan settings, processing methods, software, landmarks/measurements utilized), the impact of these errors on results obtained from osteologically derived equations will also vary. Further validation studies are required to evaluate whether the differences between CT and osteological data are great enough to impact forensic outcomes. At present, the osteological measurements are generally considered the gold standard, and the forensic anthropologist is presented with few scenarios in which virtual data are available and osteometric data are not. This is likely to change as forensic anthropologists take on a larger role in MEOs and the use of CT scanners during postmortem examinations continue to increase, creating a greater need for validation studies incorporating virtual data. As large samples of virtual 3D models are accumulated, we may see the creation of virtual-specific data collection methods, analyses, and databases of measurements, alongside the development of virtual skeletal collections.
With an increase in research and validation studies using new technology, it may also be possible to apply nonmetric methods for estimating biological profile parameters that were originally designed for dry bone to CT scans. The pubic symphysis, a joint surface of the pelvis that forensic anthropologists commonly use to assess age at death, has been evaluated for age estimation purposes from CT scan models, and recent research has proved promising for these methods (60–62). Studies have also investigated the use of the auricular surface in CT scans for age estimation and found that although some of the traditional traits are difficult to score from CT scans, by modifying the traits scored or including new criteria they were able to obtain decent estimations (63, 64). Recent work has also demonstrated that estimating sex from nonmetric traits in the pelvis and skull from rendered CT models produce good results with low associated error rates (61, 65,66). In particular, Phenice-derived traits of the pubis and the standard nonmetric traits for evaluating sex in the skull (including glabella, supraorbital margin, mastoid process, nuchal area and mental eminence) perform well when scored from CT scans (65, 66). These qualitative traits are not easily captured by simple landmarks or linear measurements, and therefore researchers are using more advanced geometric morphometric methods to 3D CT and surface scans in order to begin quantifying and statistically analyzing these traits. Geometric morphometric methods of analysis can be used to quantitatively capture and analyze the shape of object outlines, curves, and surfaces, eliminating the subjectivity involved in visual interpretation and ordinal scoring methods. For example, Garvin and Ruff use 3D models (created from surface scans) to isolate and quantitatively analyze sex and ancestry differences in brow ridge and chin shapes (67). Some researchers are even exploring automating data collection and analysis procedures using entire 3D models of the skull (68). As researchers continue to explore new methods of skeletal analysis using CT scan data, appropriate validation studies are required before use of these methods become mainstream. It is also worth noting that unless the CT-derived methods are also applicable on dry bone specimens, then their use is restricted to individuals with access to similar CT technology.
However, even with advances in resolution and the creation of sophisticated quantitative analytical techniques, there are still aspects of skeletal biology that are difficult to appreciate from digital models, including age indicators like cranial suture closure and subtle pathological signals such as periosteal bone reactions. This situation leads many forensic anthropologists to prefer physically examining remains themselves, rather than only having access to 3D scans or models, and this often means fully processing of the remains to better visualize the bones, even if advanced imaging techniques are available.
Postmortem CT scans may be compared to antemortem scans of potential decedents if they are available, enabling analysts to assess the morphology of internal individualizing characteristics such as the frontal sinuses. Postmortem radiography is much more accessible and widespread among forensic anthropologists, but because of the superimposition inherent in radiographs, it is not difficult to compare a 2D slice from a CT scan to a traditional radiograph. Because of issues with superimposition, orientation, and distortion, any comparison between a radiograph and CT scan may not be definitive enough for positive identification. Luckily, however, scout images that commonly accompany CT scans may allow for an analogous comparison. Given the advantages of CT scans over traditional radiography and the fact that more individuals are receiving CT scans during their life, we may find antemortem and postmortem comparisons of CT data becoming a more popular means of positive identification.
If any antemortem CT scans are available or postmortem CT scans are taken during autopsy, the forensic pathologist should share that data with the forensic anthropologist. The forensic anthropologist's trained eye may identify certain skeletal features from the scans that can be useful for identification or assist in reconstructing the circumstances surrounding their death. Because the CT scans essentially represent a 3D virtual replication of the skeleton, individualizing skeletal traits and morphologies evident on antemortem CT scans can be compared to the bone specimens to assist with positive identification (Image 4). In addition, the forensic anthropologist can review those scans prior to any processing, noting regions of interest (e.g., potential trauma) that may need to be processed with additional care and documentation.
Image 4.
Comparison of an antemortem computed tomography slice illustrating sagittal and coronal suture patterns (A) to a photograph of the sutures post-processing (B). An overlay of the suture patterns was used to help corroborate the identity of the individual (C).
Although it is not generally part of the role of forensic anthropologists, it is worth noting that 3D models created from the CT scans can also be utilized in facial reconstructions. Forensic artists can either create a virtual facial reconstruction, allowing certain features such as eye and hair color to be easily exchanged, or they may use a 3D printout of the skull to build their reconstruction (69–72). In this manner, the actual skull does not need to be retained in custody during the reconstruction.
Research
In the realm of forensic anthropological research, CT scans are playing a growing role for data collection purposes. Not only are digital scans more easily accessible for researchers, but they also constitute a more appropriate data source for forensic research. Unlike radiographs, CT scans do not suffer from issues of 2D superimposition or parallactic distortion. Individual decedents scanned for inclusion in CT scan samples also come from more modern and diverse populations than are available at the majority of skeletal collections, allowing a greater appreciation of human intraspecific variation as well as mitigating the effects of secular change. Furthermore, modern digital skeletal collections are generally accompanied by thorough demographic and life-history data, which many (pre) historical skeletal collections lack, however this greater access to information must also be tempered by ethical concerns about privacy.
On the other hand, robust digital skeletal collections are difficult to acquire due to the time and cost constraints associated with producing the scans. Therefore, when forensic anthropologists conduct research using CT scans, they have almost always been taken for other reasons, such as diagnostic imaging in the clinical setting or postmortem for medicolegal purposes. Protecting decedents' privacy is also a concern, especially when CT scans are used for research purposes, and therefore methods for deidentifying scans are becoming commonplace, although additional funding must be sought, usually by the anthropologist, in order to cover the cost of scan anonymization. Collaboration and partnerships between MEOs and forensic anthropologists are beginning to form in order to create these types of digital database collections (73), which constitute a valuable step forward for this type of research and advances in the field.
Surface Scans
Three-dimensional models of skeletal material can also be produced using surface scanners. There are a variety of 3D scanners currently on the market. These surface scanners use either lasers or structured light patterns to capture and reconstruct the 3D surface of an object. Unlike with CT scans, where X-rays are involved, the 3D surface scanners can only capture the external surfaces, and those surfaces must be in the line of sight of the scanner. It is impossible to capture the internal structures or surfaces and complex surfaces with large projections or deep crevasses can be challenging or at times unfeasible to capture with a surface scanner. If the goal is to create 3D models of skeletal remains, all soft-tissue must first be removed.
Some surface scanners are hand-held and can be moved freely around the object of interest, while with other scanners, the object must be moved. Automated turntables, which rotate a specified number of degrees between scans, simplify this process, and are commonly included with stationary 3D surface scanners. Most 3D surface scanners will also take photographs of the object, which are then overlaid on top of the 3D model, replicating the original coloration of the object (referred to as “texture”) (Image 5). Because the laser or light source can only capture the exposed surfaces, multiple scans must be taken from different orientations, which are then aligned and merged (either manually or automatically using the scanning software) to create a complete 3D model. The benefit of using 3D surface scanners over CT scanners to create 3D models is that 3D surface scanners are cheaper, more accessible, more mobile, and have resolutions higher than the CT slice thickness used by most clinical institutions, even during postmortem examinations. Keep in mind, however, that surface scanners cannot collect any information about internal structures, only the external surfaces that the lasers or light can reach.
Image 5.
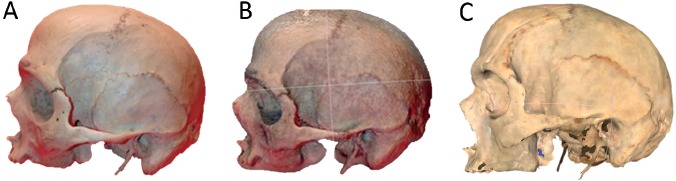
A photograph A), screenshot of a 3D model created using digital photos and photogrammetry software B), and screenshot of a 3D model created using a NextEngine desktop surface scanner C) of the same cranium. Note that the photogrammetry model was created using only 15 photographs and represents the authors' first trial with the software.
Of the 3D surface scanners utilized by researchers, the NextEngine Desktop 3D scanner is the most widely used and is owned by numerous academic, research, and medicolegal institutions. Its popularity is, in part, due to its affordability (∼$3000), user-friendly interface, and overall accuracy (up to 0.13 mm in macro mode) (74). The NextEngine can collect up to 29 000 points per square inch in the wide mode, and up to 268 000 in the macro mode. It is also fairly small (∼28 cm x 22 cm x 9 cm), making it relatively portable. Although the act of creating a 3D scan using the NextEngine and associated ScanStudio software is fairly simple, there are a number of settings and preferences that can be adjusted in order to obtain scans of varying quality and file size. At present, there are no published standards for scanning forensic anthropological skeletal material, and preferred methods and scanner settings utilized vary amongst researchers. There are also a number of more expensive 3D scanners available (e.g., Breuckmann SmartScan, DEIOS Prototype, Descam Model Maker). These scanners can run upwards of $200 000. A few studies have compared NextEngine scan results to those of higher-end scanners (75, 76) and found that for most purposes, the NextEngine scanner provides high enough resolution.
Documentation and Trauma
Essentially, 3D surface scans can be used in much of the same manner as CT scans. The 3D scans can be used to create a 3D replica of a skeletal element for documentation and archival purposes. A 3D virtual model of the skull, os coxae, and any other region of interest can be created and stored. Even after the remains are returned, the anthropologist can refer to the 3D model, should new information arise or previous information come into question. Because the surface scanners also capture the texture and coloration of the surface, taphonomic modifications such as sun bleaching and soil staining can also be preserved. The scan resolution is generally high enough to be able to accurately document most fracture patterns (especially those displaying plastic deformation or separation at the fracture margins) and gunshot wounds. It is generally more difficult to capture evidence of sharp force trauma using 3D scans, unless the defects are a couple of millimeters wide. Narrower incisive wounds and shallow cuts might be able to be captured using higher-end scanners, but will depend on the resolution and settings. Overall, the utility of 3D surface scans in documenting and analyzing trauma defects has not been thoroughly explored and requires further experimentation. As with the CT scans, any virtual models created from 3D surface scans can then be printed with a 3D printer, providing a tangible replica. The 3D print may then be used for illustrative purposes in court testimony or when teaching in the classroom and training the next generation of forensic anthropologists.
Surface scanners can also be utilized to document the crime scene in forensic cases. This technology has been utilized by various agencies in indoor crime scenes, outdoor crime scenes, and in crash reconstructions. The surface scanner can be used to create a 3D replica of a crime scene, thereby digitally preserving the scene. Besides obvious archival and evidentiary purposes, the 3D crime scene may be used for scene reconstructions and analyses. Measurements and angles can be collected from the 3D models to aid in such analyses as blood spatter and bullet trajectories. They also cut down on scene processing time, as much of the traditional information collected from the scene can be collected virtually after the fact, allowing agencies to clear scenes in a more timely manner. Finally, the 3D crime scenes can be used for explanatory purposes in the courtroom. Most forensic anthropologists, however, have not had the opportunity to work with this technology. Laser scanners utilized for scene documentations (such as the popular Leica ScanStation) cost upwards of $115 000, which is typically outside the forensic anthropologist's budget. These scanners can create a 360 degree reconstruction of a scene with up to 3 mm accuracy at a distance of 50 m. The National Institute of Justice recently published the results of a study entitled “Landscape Study on 3D Crime Scene Scanning Devices”, in which various 3D scene scanning devices are compared (77). Overall, the results of the study emphasize the utility of 3D scanning devices at crime scenes, but also stresses the time requirements in post-processing the data and required funds and resources for analysts, as well as the maintenance and upkeep of the equipment and software. Given these limitations, it may be best for forensic anthropologists to identify where the closest regional access to such technology may be and collaborate with those agencies if 3D scanning of an outdoor scene is required.
Biological Profile and Identification
At this point, 3D surface scans do not contribute much directly to forensic anthropological case analyses. Although landmarks and measurements can be collected from the surface scans and have been shown to be accurate (78), there is not much point in taking them from the surface scans when the actual element is available and can be measured directly. This is also true when applying traditional age, sex, and ancestry estimation techniques. However, as mentioned previously, 3D virtual models provide an opportunity to use new variables, such as surface areas, volumes, outlines, surface relief, and semilandmarks (i.e., landmarks placed along curves or surfaces in order to capture shape) in skeletal variation analyses. Because surface scans are generally more accessible than CT scans, many of the novel quantitative methods are being developed from samples of surface scans (67, 79–82).
Research
The research potential for 3D surface scans mirrors that of CT scans. The use of craniometric landmarks from 3D surface scans has been approached a little more cautiously than those from CT scans, as the quality and resolution of the surface scans have been known to vary. Experimentation with various scanning equipment and software should be systematically conducted, the results of which may be used to create SOPs for scanning skeletal elements for forensic purposes. Statistical advances in the field of geometric morphometrics are also allowing researchers to explore new variables in skeletal analyses, and this new research is well-represented in the literature. A cursory literature search reveals over 100 articles in the Journal of Forensic Sciences, Forensic Science International, and the American Journal of Physical Anthropology in which 3D models (from surface or CT scans) were used in some form of skeletal analysis since 2001. Forensic skeletal analyses will continue to advance as researchers investigate new methods of analyzing features which could not be easily quantified in the past.
Unlike CT scans, which are commonly collected and archived at medical institutions and therefore are theoretically accessible for research purposes, we have yet to reach the point where there are large repositories of modern human 3D surface scans available for researchers. It is anticipated that this will change in the near future as 3D scanning becomes more affordable and practical and data analysis software continues to improve. Instead of travelling to skeletal collections to physically take measurements and landmarks for research, 3D scans of skeletal elements can be sent over the internet or uploaded onto servers. Three-dimensional surface scans thus offer another opportunity for researchers to share data and the potential for growing virtual skeletal collections if the time and resources can be allocated to collecting and processing those scans. Before this can occur; however, SOPs need to be developed for scanning processes and ethics for data sharing of such sensitive material should be considered.
Photogrammetry
Another affordable option for the production of 3D models is the use of photogrammetry. Although the concept of photogrammetry was developed well before 3D surface scanning and CT scans were available, photogrammetry methods have recently become increasingly popular as camera technology has advanced. Recent publications demonstrate its versatility in several fields, including applications to biological anthropology (83, 84). Essentially, photogrammetry allows for the reconstruction of the position, orientation, shape, and size of an object from digital photographs and thus requires no expensive hardware other than a decent digital camera (84). A number of fee-based and free software programs are currently available (e.g., Agisoft PhotoScan, 123DCatch, 3DFlow, Acute3D) that use algorithms to more or less automatically align multiple photographs of an object into a 3D model. Theoretically, the outcome would be equivalent to a 3D surface scan; however, the accuracy of the 3D photogrammetry reconstructions has not yet been evaluated for forensic use. Given that the reconstruction is built from a series of photographs (which do not even need to be taken in a particularly systematic order), instead of the lasers or structured light source in a 3D surface scanner, it may be assumed that photogrammetry methods will result in less accurate models. Overall, photogrammetry is a new area for forensic anthropologists to explore for use both in the laboratory and at the scene. This is particularly true for laboratories or agencies that may not have the funds for more advanced technology.
Conclusion
Over the last decade, the use of advanced imaging in forensic research and case analyses has exponentially increased. That being said, these technologies are not yet commonplace and their full potential is not yet being exploited in the field of forensic anthropology. One of the major limiting factors is cost. Computed tomography scanners and high-end laser scanners will likely be outside the forensic anthropologist's budget. Some forensic anthropology labs may not even have access to digital X-ray systems. Even affordable imaging options, such as the NextEngine scanner, may require additional software to perform certain analyses. Programs such as AMIRA, GeoMagic, and Polyworks which are commonly used to view, collect, and analyze 3D data, cost thousands of dollars, with annual maintenance fees. The use of the advanced imaging equipment and associated software is also a limiting factor as these require expertise, and postprocessing of CT or surface scan data is time consuming. Despite these limitations, those with access to advanced imaging technologies have begun to incorporate them into forensic anthropological analyses and research. As there are continued advances in 3D technologies, we should expect to see the continued development of novel, more quantitative methods, including movements towards automating data collection, processing, and analyzing procedures. Given the high monetary and time cost of traveling to collections to physically collect data and the ease of accessing digital data, we should also expect to see growing trends of institutions using these advanced imaging techniques to create virtual collections for research and teaching purposes. The formation of these virtual collections is already proving time-consuming, and therefore it may take years to render even modest collections fully digital, but despite these drawbacks, several museums and other institutions are forging ahead and steadily adding specimens to their virtual collections. The real key to promote the continued implementation and improvement of advanced imaging techniques is to increase collaboration between forensic anthropologists, law enforcement, and forensic pathologists and other clinicians. Open communication and the sharing of information, data, and resources will facilitate these interdisciplinary collaborations, ultimately supporting our common goals in medicolegal investigations.
Footnotes
Disclosures
The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript
ETHICAL APPROVAL
As per Journal Policies, ethical approval was not required for this manuscript
STATEMENT OF HUMAN AND ANIMAL RIGHTS
This article does not contain any studies conducted with animals or on living human subjects
STATEMENT OF INFORMED CONSENT
No identifiable personal data were presented in this manuscsript
DISCLOSURES & DECLARATION OF CONFLICTS OF INTEREST
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest
References
- 1).Garvin H.M., Symes S.A. A comparison of radiographic and osteological findings in suspected infant abuse cases. Proc Am Acad Forensic Sci. 2015; 21: 177. [Google Scholar]
- 2).Scheuer L., Black S.M. Developmental juvenile osteology. San Diego: Academic Press; 2000. 587 p. [Google Scholar]
- 3).Crowder C., Austin D. Age ranges of epiphyseal fusion in the distal tibia and fibula of contemporary males and females. J Forensic Sci. 2005. Sep; 50(5): 1001–07. PMID: 16225203. 10.1520/jfs2004542. [DOI] [PubMed] [Google Scholar]
- 4).Cardoso H.F.V. Epiphyseal union at the innominate and lower limb in a modern Portuguese skeletal sample, and age estimation in adolescent and young adult male and female skeletons. Am J Phys Anthropol. 2008. Feb; 135(2): 161–70. PMID: 18044694. 10.1002/ajpa.20717. [DOI] [PubMed] [Google Scholar]
- 5).Cardoso H.F.V. Age estimation of adolescent and young adult male and female skeletons II, epiphyseal union at the upper limb and scapular girdle in a modern Portuguese skeletal sample. Am J Phys Anthropol. 2008. Sep; 137(1): 97–105. PMID: 18553494. 10.1002/ajpa.20850. [DOI] [PubMed] [Google Scholar]
- 6).O'Connor J.E., Bogue C., Spence L.D., Last J. A method to establish the relationship between chronological age and stage of union from radiographic assessment of epiphyseal fusion at the knee: An Irish population study. J Anat. 2008. Feb; 212(2): 198–209. PMID: 18179475. PMCID: PMC2408977. 10.1111/j.1469-7580.2007.00847.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7).AlQahtani S.J., Hector M.P., Liversidge H.M. Accuracy of dental age estimation charts: Schour and Massler, Ubelaker, and the London Atlas. Am J Phys Anthropol. 2014. May; 154(1): 70–8. PMID: 24470177. 10.1002/ajpa.22473. [DOI] [PubMed] [Google Scholar]
- 8).McCormick W.F. Mineralization of the costal cartilages as an indicator of age: preliminary observations. J Forensic Sci. 1980. Oct; 25(4): 736–41. PMID: 7430987. 10.1520/jfs11287j. [DOI] [PubMed] [Google Scholar]
- 9).Garvin H.M. Ossification of laryngeal structures as indicators of age. J Forensic Sci. 2008. Sep; 53(5): 1023–7. PMID: 18624888. 10.1111/j.1556-4029.2008.00793.x. [DOI] [PubMed] [Google Scholar]
- 10).Garvin H.M. Age estimation of the human skeleton. Springfield (IL): Charles C Thomas; c2010. Chapter 8, Limitations of cartilage ossification as an indicator of age at death; p. 118–33. [Google Scholar]
- 11).Middleham H.P., Boyd L.E., McDonald S.W. Sex determination from calcification of costal cartilages in a Scottish sample. Clin Anat. 2015. Oct; 28(7): 888–95. PMID: 25534066. 10.1002/ca.22491. [DOI] [PubMed] [Google Scholar]
- 12).Schroeder C.F., Schmidtke S.Z., Bidez M.W. Measuring the human pelvis: a comparison of direct and radiographic techniques using a modern United States-ased sample. Am J Phys Anthropol. 1997. Aug; 103(4): 471–9. PMID: 9292165. . [DOI] [PubMed] [Google Scholar]
- 13).Bontrager K. Textbook of radiographic positioning and related anatomy. 5th ed. Philadelphia: Mosby; 2001. 826 p. [Google Scholar]
- 14).Mantini S., Ripani M. Modern morphometry: new perspectives in physical anthropology. N Biotechnol. 2009. Jun; 25(5): 325–30. PMID: 19491048. 10.1016/j.nbt.2009.03.009. [DOI] [PubMed] [Google Scholar]
- 15).Beningfield S., Potgieter H., Nicol A. et al. Report on a new type of trauma full-body digital x-ray machine. Emer Radiol. 2003. Apr; 10(1): 23–9. PMID: 15290526. 10.1007/s10140-003-0271-x. [DOI] [PubMed] [Google Scholar]
- 16).Deyle S., Wagner A., Benneker L.M. et al. Could full-body X-ray (LODOX-Statscan) screening in trauma challenge conventional radiography? J Trauma. 2009. Feb; 66(2): 418–22. PMID: 19204516. 10.1097/TA.0b013e31818a5d1a. [DOI] [PubMed] [Google Scholar]
- 17).Douglas T., Pitcher R., van As A. Full-body digital radiographic imaging of the injured child. Contin Med Educ. 2010; 28(3): 108–112. [Google Scholar]
- 18).Yoshino M., Miyasaka S., Sato H., Seta S. Classification system of frontal sinus patterns by radiography. Its application to identification of unknown skeletal remains. Forensic Sci Int. 1987. Aug; 34(4): 289–99. PMID: 3623370. 10.1016/0379-0738(87)90041-7. [DOI] [PubMed] [Google Scholar]
- 19).Marlin D.C., Clark M.A., Standish S.M. Identification of human remains by comparison of frontal sinus radiographs: a series of four cases. J Forensic Sci. 1991. Nov; 36(6): 1765–72. PMID: 1770345. 10.1520/jfs13202j. [DOI] [PubMed] [Google Scholar]
- 20).Kirk N.J., Wood R.E., Goldstein M. Skeletal identification using the frontal sinus region: a retrospective study of 39 cases. J Forensic Sci. 2002. Mar; 47(2): 318–23. PMID: 11908601. 10.1520/jfs15250j. [DOI] [PubMed] [Google Scholar]
- 21).Christensen A.M. Testing the reliability of frontal sinuses in positive identification. J Forensic Sci. 2005. Jan; 50(1): 18–22. PMID: 15830992. 10.1520/jfs2004145. [DOI] [PubMed] [Google Scholar]
- 22).Jablonski N.G., Shum B.S. Identification of unknown human remains by comparison of antemortem and postmortem radiographs. Forensic Sci Int. 1989. Aug; 42(3): 221–30. PMID: 2792981. 10.1016/0379-0738(89)90089-3. [DOI] [PubMed] [Google Scholar]
- 23).Ubelaker D.H. Positive identification of American Indian skeletal remains from radiograph comparison. J Forensic Sci. 1990. Mar; 35(2): 466–72. PMID: 2329337. 10.1520/jfs12848j. [DOI] [PubMed] [Google Scholar]
- 24).Rhine S., Sperry K. Radiographic identification by mastoid sinus and arterial pattern. J Forensic Sci. 1991. Jan; 36(1): 272–9. PMID: 2007877. 10.1520/jfs13029j. [DOI] [PubMed] [Google Scholar]
- 25).Owsley D.W., Mann R.W. Positive personal identity of skeletonized remains using abdominal and pelvic radiographs. J Forensic Sci. 1992. Jan; 37(1): 332–6. PMID: 1545209. 10.1520/jfs13238j. [DOI] [PubMed] [Google Scholar]
- 26).Adams B.J., Maves R.C. Radiographic identification using the clavicle of an individual missing from the Vietnam conflict. J Forensic Sci. 2002. Mar; 47(2): 369–373. PMID: 11908610. 10.1520/jfs15259j. [DOI] [PubMed] [Google Scholar]
- 27).Kahana T., Goldin L., Hiss J. Personal identification based on radiographic vertebral features. Am J Forensic Med Pathol. 2002. Mar; 23(1): 36–41. PMID: 11953491. 10.1097/00000433-200203000-00007. [DOI] [PubMed] [Google Scholar]
- 28).Kuehn C.M., Taylor K.M., Mann F.A. et al. Validation of chest x-ray comparisons for unknown decedent identification. J Forensic Sci. 2002. Jul; 47(4): 725–9. PMID: 12136980. 10.1520/jfs15450j. [DOI] [PubMed] [Google Scholar]
- 29).Koot M.G., Sauer N.J., Fenton T.W. Radiographic human identification using bones of the hand: a validation study. J Forensic Sci. 2005. Mar; 50(2): 263–8. PMID: 15813535. 10.1520/jfs2004229. [DOI] [PubMed] [Google Scholar]
- 30).Mundorff A.Z., Vidoli G., Melinek J. Anthropological and radiographic comparison of vertebrae for identification of decomposed human remains. J Forensic Sci. 2006. Sep; 51(5): 1002–4. PMID: 17018076. 10.1111/j.1556-4029.2006.00233.x. [DOI] [PubMed] [Google Scholar]
- 31).Campobasso C.P., Dell'Erba A.S., Belviso M., Di Vella G. Craniofacial identification by comparison of antemortem and postmortem radiographs: two case reports dealing with burnt bodies. Am J Forensic Med Pathol. 2007. Jun; 28(2): 182–6. PMID: 17525575. 10.1097/PAF.0b013e31806195cb. [DOI] [PubMed] [Google Scholar]
- 32).Rogers T.L., Allard T.T. Expert testimony and positive identification of human remains through cranial suture patterns. J Forensic Sci. 2004. Mar; 49(2): 203–7. PMID: 15027532. 10.1520/jfs2003095. [DOI] [PubMed] [Google Scholar]
- 33).Kahana T., Hiss J. Positive identification by means of trabecular bone pattern comparison. J Forensic Sci. 1994. Sep; 39(5): 1325–30. PMID: 7964570. 10.1520/jfs13720j. [DOI] [PubMed] [Google Scholar]
- 34).Kahana T., Hiss J., Smith P. Quantitative assessment of trabecular bone pattern identification. J Forensic Sci. 1998. Nov; 43(6): 1144–7. PMID: 9846391. 10.1520/JFS14377J. [DOI] [PubMed] [Google Scholar]
- 35).Mann R.W. Use of bone trabeculae to establish positive identification. Forensic Sci Int. 1998. Nov 30; 98(1-2): 91–9. PMID: 10036762. 10.1016/s0379-0738(98)00138-8. [DOI] [PubMed] [Google Scholar]
- 36).Kahana T., Ravioli J.A., Urroz C.L., Hiss J. Radiographic identification of fragmentary human remains from a mass disaster. Am J Forensic Med Pathol. 1997. Mar; 18(1): 40–4. PMID: 9095299. 10.1097/00000433-199703000-00007. [DOI] [PubMed] [Google Scholar]
- 37).McCammon R.W. Human growth and development. Sprinfield (IL): Charles C. Thomas; 1970. 295 p. [Google Scholar]
- 38).Ruff C.B. Body size prediction from juvenile skeletal remains. Am J Phys Anthropol. 2007. May; 133(1): 698–716. PMID: 17295297. 10.1002/ajpa.20568. [DOI] [PubMed] [Google Scholar]
- 39).Roche A.F. Growth, maturation and body composition: the Fels longitudinal study 1929-1991. New York: Cambridge University Press; 1992. 282 p. [Google Scholar]
- 40).Ousley S., Daly S., Frazee K., Stull K. A radiographic database for estimating biological parameters in modern subadults. Washington: National Institute of Justice; 2013. 59 p. [Google Scholar]
- 41).Ross A.H., Lanfear A.K., Maxwell A.B. Testing the validity of radiographic comparisons in positive identifications, final technical report. Washington: National Institute of Justice; 2015. 50 p. [Google Scholar]
- 42).Jackowski C., Schweitzer W., Thali M. et al. Virtopsy: postmortem imaging of the human heart in situ using MSCT and MRI. Forensic Sci Int. 2005. Apr 20; 149(1): 11–23. PMID: 15734105. 10.1016/j.forsciint.2004.05.019. [DOI] [PubMed] [Google Scholar]
- 43).Thali M.J., Braun M., Buck U. et al. 2005. VIRTOPSY—scientific documentation, reconstruction and animation in forensic: individual and real 3D data based geo-metric approach including optical body/object surface and radiological CT/MRI scanning. J Forensic Sci. 2005. Mar; 50(2): 428–42. PMID: 15813556. 10.1520/jfs2004290. [DOI] [PubMed] [Google Scholar]
- 44).Thali M.J., Jackowski C., Oesterhelweg L. et al. VIRTOPSY–the Swiss virtual autopsy approach. Leg Med (Tokyo). 2007. Mar; 9(2): 100–4. PMID: 17275386. 10.1016/j.legalmed.2006.11.011. [DOI] [PubMed] [Google Scholar]
- 45).Dirnhofer R., Jackowski C., Vock P. et al. VIRTOPSY: minimally invasive, imaging-guided virtual autopsy. Radiographics. 2006. Sep-Oct; 26(5): 1305–33. PMID: 16973767. 10.1148/rg.265065001. [DOI] [PubMed] [Google Scholar]
- 46).Sidler M., Jackowski C., Dirnhofer R. et al. Use of multislice computed tomography in disaster victim identification—advantages and limitations. Forensic Sci Int. 2007. Jul 4; 169(2-3): 118–28. PMID: 16997522. 10.1016/j.forsciint.2006.08.004. [DOI] [PubMed] [Google Scholar]
- 47).Bolliger S.A., Thali M.J., Ross S. et al. Virtual autopsy using imaging: bridging radiologic and forensic sciences. A review of the Virtopsy and similar projects. Eur Radiol. 2007. Feb; 18(2): 273–82. PMID: 17705044. 10.1007/s00330-007-0737-4. [DOI] [PubMed] [Google Scholar]
- 48).Verhoff M.A., Ramsthaler F., Krähahn J. et al. Digital forensic osteology–possibilities in cooperation with the Virtopsy project. Forensic Sci Int. 2008. Jan 30; 174(2-3): 152–6. PMID: 17451898. 10.1016/j.forsciint.2007.03.017. [DOI] [PubMed] [Google Scholar]
- 49).Christe A., Flach P., Ross S. et al. Clinical radiology and postmortem imaging (Virtopsy) are not the same: Specific and unspecific postmortem signs. Leg Med (Tokyo). 2010. Sep; 12(5): 215–22. PMID: 20630787. 10.1016/j.legalmed.2010.05.005. [DOI] [PubMed] [Google Scholar]
- 50).Milenkovic P., Djuric M., Milovanovic P. et al. The role of CT analyses of the sternal end of the clavicle and the first costal cartilage in age estimation. Int J Legal Med. 2014. Sep; 128(5): 825–9. PMID: 24957198. 10.1007/s00414-014-1026-9. [DOI] [PubMed] [Google Scholar]
- 51).Oldrini G., Harter V., Witte Y. et al. Age estimation in living adults using 3D volume rendered CT images of the sternal plastron and lower chest. J Forensic Sci. 2016. Jan; 61(1): 127–33. PMID: 27092960. 10.1111/1556-4029.12990. [DOI] [PubMed] [Google Scholar]
- 52).Richtsmeier J.T., Paik C.H., Elfert P.C. et al. Precision, repeatability, and validation of the localization of cranial landmarks using computed tomography scans. Cleft Palate Craniofac J. 1995. May; 32(3): 217–27. PMID: 7605789. . [DOI] [PubMed] [Google Scholar]
- 53).Barbeito-Andrés J., Anzelmo M., Ventrice F., Sardi M.L. Measurement error of 3D cranial landmarks of an ontogenetic sample using computed tomography. J Oral Biol Craniofac Res. 2012. May-Aug; 2(2): 77–82. PMID: 25737840. PMCID: PMC3942138. 10.1016/j.jobcr.2012.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54).Guyomarc'h P., Santos F., Dutailly B. et al. Three-dimensional computer-assisted craniometrics: A comparison of the uncertainty in measurement induced by surface reconstruction performed by two computer programs. Forensic Sci Int. 2012. Jun 10; 219(1): 221–7. PMID: 22297143. 10.1016/j.forsciint.2012.01.008. [DOI] [PubMed] [Google Scholar]
- 55).Franklin D., Cardini A., Flavel A. et al. Concordance of traditional osteometric and volume-rendered MSCT interlandmark cranial measurements. Int J Legal Med. 2013. Mar; 127(2): 505–20. PMID: 23052442. 10.1007/s00414-012-0772-9. [DOI] [PubMed] [Google Scholar]
- 56).Katkar R.A., Kummet C., Dawson D. et al. Comparison of observer reliability of three-dimensional cephalometric landmark identification on subject images from Galileos and i-CAT cone beam CT. Dentomaxillofac Radiol. 2013; 42(9): 20130059 PMID: 23833319. PMCID: PMC3828023. 10.1259/dmfr.20130059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57).Hale A.R., Honeycutt K.K., Ross A.H. A geometric morphometric validation study of computed tomography–extracted craniofacial landmarks. J Craniofac Surg. 2014. Jan; 25(1): 231–7. PMID: 24406584. 10.1097/SCS.0000000000000460. [DOI] [PubMed] [Google Scholar]
- 58).Stull K.E., Tise M.L., Ali Z., Fowler D.R. Accuracy and reliability of measurements obtained from computed tomography 3D volume rendered images. Forensic Sci Int. 2014. May; 238: 133–40. PMID: 24713466. 10.1016/j.forsciint.2014.03.005. [DOI] [PubMed] [Google Scholar]
- 59).Jantz R.L., Ousley S.D. FORDISC 3.1: computerized forensic discriminant functions. Knoxville: University of Tennessee; 2010. [Google Scholar]
- 60).Telmon N., Gaston A., Chemla P. et al. Application of the Suchey-Brooks method to three-dimensional imaging of the pubic symphysis. J Forensic Sci. 2005. May; 50(3): 507–12. PMID: 15932079. 10.1520/jfs2004326. [DOI] [PubMed] [Google Scholar]
- 61).Grabherr S., Cooper C., Ulrich-Bochsler S. et al. Estimation of sex and age of “virtual skeletons”–a feasibility study. Eur Radiol. 2008. Feb; 19(2): 419–29. PMID: 18766348. 10.1007/s00330-008-1155-y [DOI] [PubMed] [Google Scholar]
- 62).Lottering N., Macgregor D.M., Meredith M. et al. Evaluation of the Suchey-Brooks method of age estimation in an Australian subpopulation using computed tomography of the pubic symphyseal surface. Am J Phys Anthropol. 2013. Mar; 150(3): 386–99. PMID: 23283754. 10.1002/ajpa.22213. [DOI] [PubMed] [Google Scholar]
- 63).Barrier P., Dedouit F., Braga L. et al. Age at death estimation using multislice computed tomography reconstructions of the posterior pelvis. J Forensic Sci. 2009. Jul; 54(4): 773–8. PMID: 19486247. 10.1111/j.1556-4029.2009.01074.x. [DOI] [PubMed] [Google Scholar]
- 64).Ferrant O1, Rougé-Maillart C., Guittet L. et al. Age at death estimation of adult males using coxal bone and CT scan: a preliminary study. Forensic Sci Int. 2009. Apr 15; 186(1-3): 14–21. PMID: 19201560. 10.1016/j.forsciint.2008.12.024. [DOI] [PubMed] [Google Scholar]
- 65).Ramsthaler F., Kettner M., Gehl A., Verhoff M. Digital forensic osteology: morphological sexing of skeletal remains using volume-rendered cranial CT scans. Forensic Sci Int. 2010. Feb 25; 195(1-3): 148–52. PMID: 20074879. 10.1016/j.forsciint.2009.12.010. [DOI] [PubMed] [Google Scholar]
- 66).Decker S.J., Davy-Jow S.L., Ford J.M., Hilbelink D.R. Virtual determination of sex: metric and nonmetric traits of the adult pelvis from 3D computed tomography models. J Forensic Sci. 2011. Sep; 56(5): 1107–14. PMID: 21595690. 10.1111/j.1556-4029.2011.01803.x. [DOI] [PubMed] [Google Scholar]
- 67).Garvin H.M., Ruff C.B. Sexual dimorphism in skeletal browridge and chin morphologies determined using a new quantitative method. Am J Phys Anthropol. 2012. Apr; 147(4): 661–70. PMID: 22371071. 10.1002/ajpa.22036. [DOI] [PubMed] [Google Scholar]
- 68).Fatah E.E.A., Shirley N.R., Jantz R.L., Mahfouz M.R. Improving sex estimation from crania using a novel three-dimensional quantitative method. J Forensic Sci. 2014. May; 59(3): 590–600.PMID: 24502609. 10.1111/1556-4029.12379. [DOI] [PubMed] [Google Scholar]
- 69).De Greef S., Willems G. Three-dimensional cranio-facial reconstruction in forensic identification: latest progress and new tendencies in the 21st century. J Forensic Sci. 2005. Jan; 50(1): 12–7. PMID: 15830991. 10.1520/jfs2004117. [DOI] [PubMed] [Google Scholar]
- 70).Lee W.J., Wilkinson C.M., Hwang H.S. An accuracy assessment of forensic computerized facial reconstruction employing cone-beam computed tomography from live subjects. J Forensic Sci. 2012. Mar; 57(2): 318–27. PMID: 22073932. 10.1111/j.1556-4029.2011.01971.x. [DOI] [PubMed] [Google Scholar]
- 71).Lee W.J., Wilkinson C.M., Hwang H.S., Lee S.M. Correlation between average tissue depth data and quantitative accuracy of forensic craniofacial reconstructions measured by geometric surface comparison method. J Forensic Sci. 2015. May; 60(3): 572–80. PMID: 25739646. 10.1111/1556-4029.12726. [DOI] [PubMed] [Google Scholar]
- 72).Short L.J., Khambay B., Ayoub A. et al. Validation of a computer modelled forensic facial reconstruction technique using CT data from live subjects: a pilot study. Forensic Sci Int. 2014. Apr; 237: 147.e1–147.e8. PMID: 24529418. 10.1016/j.forsciint.2013.12.042. [DOI] [PubMed] [Google Scholar]
- 73).Stull K., Garvin H. and Klales A. Development of modern subadult standards: improved age and sex estimation in U.S. forensic practice. Washington: National Institute of Justice; 2015. [Google Scholar]
- 74).NextEngine [Internet]. Santa Monica: NextEngine, Inc.; 2016. [cited 2016 Jul 6]. Available from: http://www.nextengine.com. [Google Scholar]
- 75).Slizewski A., Semal P. Experiences with low and high cost 3D surface scanner. Quartär. 2009; 56: 131–8. [Google Scholar]
- 76).Friess M. Scratching the surface? The use of surface scanning in physical and paleoanthropology. J Anthropol Sci. 2012; 90: 7–31. PMID: 22781581. 10.4436/jass.90004. [DOI] [PubMed] [Google Scholar]
- 77).Ropero-Miller J., Bailey M., Bushman M.H. et al. Landscape study on 3D crime scene scanning devices. Washington: National Institute of Justice; 2016. 14 p. [Google Scholar]
- 78).Sholts S., Flores L., Walker P., Wärmländer S. Comparision of coordinate measurement precision of different landmark types on human crania using a 3D laser scanner and a 3D digitiser: implications for applications of digital morphometrics. Int J Osteoarch. 2010. Feb; 21(5): 535–43. 10.1002/oa.1156. [DOI] [Google Scholar]
- 79).Sholts S.B., Wärmländer S.K., Flores L.M. et al. Variation in the measurement of cranial volume and surface area using 3D laser scanning technology. J Forensic Sci. 2010. Jul; 55(4): 871–6. PMID: 20384925. 10.1111/j.1556-4029.2010.01380.x. [DOI] [PubMed] [Google Scholar]
- 80).Shearer B.M., Sholts S.B., Garvin H.M., Wärmländer S.K. Sexual dimorphism in human browridge volume measured from 3D models of dry crania: a new digital morphometrics approach. Forensic Sci Int. 2012. Oct 10; 222(1): 400.e1–5. PMID: 22776689. 10.1016/j.forsciint.2012.06.013. [DOI] [PubMed] [Google Scholar]
- 81).Sholts S.B., Wärmländer S.K. Zygomaticomaxillary suture shape analyzed with digital morphometrics: reassessing patterns of variation in American Indian and European populations. Forensic Sci Int. 2012. Apr 10; 217(1): 234.e1–6. PMID: 22154439. 10.1016/j.forsciint.2011.11.016. [DOI] [PubMed] [Google Scholar]
- 82).Villa C., Buckberry J., Cattaneo C. et al. Quantitative analysis of the morphological changes of the pubic symphyseal face and the auricular surface and implications for age at death estimation. J Forensic Sci. 2015. May; 60(3): 556–65. PMID: 25613520. 10.1111/1556-4029.12689. [DOI] [PubMed] [Google Scholar]
- 83).Katz D., Friess M. Technical note: 3D from standard digital photography of human crania-a preliminary assessment. Am J Phys Anthropol. 2014. May; 154(1): 162–8. PMID: 24711122. 10.1002/ajpa.22468. [DOI] [PubMed] [Google Scholar]
- 84).Kraus K. Photogrammetry: geometry from images and laser scans. Vienna: Walter de Gruyter; 2007. 459 p. [Google Scholar]