

Abstract
The fatal maltreatment of people that are detained against their will, such as political prisoners and suspected terrorists, can occur in unstable countries. The death of such detainees is often controversial and debated in the media, legal tribunals, and communities. Therefore, there is a need for nonpartisan information about the cause of death of prisoners due to the implications that the data may have about a conclusion that human rights were abused. Autopsies are the only scientific way to prove the cause of death of detainees and to ascertain the truth behind how injuries may have occurred. On this basis, all forensic pathologists ought to be able to interpret the basic injury patterns commonly encountered in torture. The injuries are similar to those found in child abuse, but also include trauma from suspension and “homicide by heart attack” during interrogation. This paper will review the postmortem findings in cases of torture.
Keywords: Forensic pathology, Postmortem, Torture, Autopsy
Introduction
People who are detained can be tortured, maltreated, injured, executed, or die unexpectedly during interrogation. Torture is a key form of custodial maltreatment and can be defined as the infliction of pain to obtain a confession, or to punish. If death occurs during torture or detention, questions will often be asked about if the death was caused by the actions of the people who detained the prisoner. In the cases of the death of political prisoners, or people detained as suspected terrorists, the international community may demand to know what happened. To seek the truth in such cases is among the greatest duties of the forensic pathologist (1-3). This is because at times of political instability and war, a statement of what is considered to be true is subjected to variable interpretations, often determined by ideology. On this basis, the autopsy is a powerful scientific method to seek the actual truth about custodial deaths. Sometimes it is the only way to ascertain what actually happened to a person, if they died while detained by state actors, or hostile agents.
Only a few people who die in prisons, interrogation centers, or after a political “disappearance”, in the international setting, will undergo autopsy. This is because the bodies of these people are often concealed so that the truth of their deaths is also hidden. However, every forensic pathologist ought to be able to document and interpret the basic injury patterns observed in cases of torture. This is akin to the recognition of child abuse at the autopsy table. The main postmortem findings in cases of torture will be explained in this paper.
Discussion
Regional Injury
Multiple blunt impact trauma is the most common form of violence in torture (Image 1). Patterned injuries either as tram-line bruises or similarly shaped scars are often present in whipping or related trauma (Image 2). Body regions are often preferentially targeted. Head injuries are common and organizing subdural hemorrhage is frequently observed in long-term prisoners who are repeatedly tortured. Extensive soft tissue injury, especially subcutaneous and intramuscular hematoma formation, is frequently encountered in cases of delayed death following interrogation. The bruising may be minimal or invisible on the skin surface. On this basis, it is essential to conduct complete musculocutaneous dissections of the anterior and posterior torso and the limbs (Images 3 and 4). Otherwise, the extent of injury can be grossly underestimated.
Image 1.

Recent bruises on thigh.
Image 2.

Wounds from lashing of buttocks.
Image 3.

Subcutaneous bruising of lateral torso.
Image 4.

Subcutaneous bruising of upper arm.
A common form of regional blunt injury is falanga, also known as felaka in Arabic. This is repeated impacts on the soles of the feet (4). In many cases, the sole of the foot appears normal externally. However, dissection of the foot reveals subcutaneous and sub-plantar fascial hemorrhage (Image 5). In some cases of fatal torture with chronic heart disease (see below), the only injury that may be present at autopsy is internal bruising in the foot. Thus, the forensic pathologist may unknowingly attribute death to natural causes, unless the foot is dissected at autopsy. Other injuries can include damage to the fingernails and toenails (Image 6).
Image 5.

Falanga injuries.
Image 6.

Healing avulsion of toenail.
Injuries from Heat and Electricity
A thermal burn is a common method of torture (Image 7). Burns from cigarettes or other heated objects tend to be the most frequently seen, and are usually small round second-degree burns. Often, there is a collapsed blister on the surface of the injury. Cigarette burns are often multiple, grouped, and symmetrically distributed (e.g., hands and feet). The main pitfall in the diagnosis of cigarette burns is that round perimortem abrasions with postmortem drying can often resemble cigarette burns. In addition, in tropical climates with abundant insect activity, postmortem insect feeding on the epidermis can often resemble a burn. Thus, the diagnosis of a cigarette burn must be approached with great care, particularly if it is the main basis for the conclusion that someone has been tortured.
Image 7.

Healing burn.
Joule burns from the application of an electrode are often easier to recognize than cigarette burns, however, there is an overlap in macroscopic appearance. Histologic examination can be helpful in distinguishing an electrical or thermal burn from an artifact. However, it can often be difficult to definitely distinguish between an electrical and thermal burn by histology. In addition to blister formation, the histological appearance of electrical burns is characterized by epithelial nuclear streaming (Image 8). In many cases, a crater-like lesion composed of thermally-altered collagen can be stained by the Masson's trichrome stain. This is because heat-altered collagen appears red rather than green (5). The presence of epidermal nuclear streaming, a blister, and tinctorial changes in dermal collagen are helpful guides to the histologic determination of a burn.
Image 8.
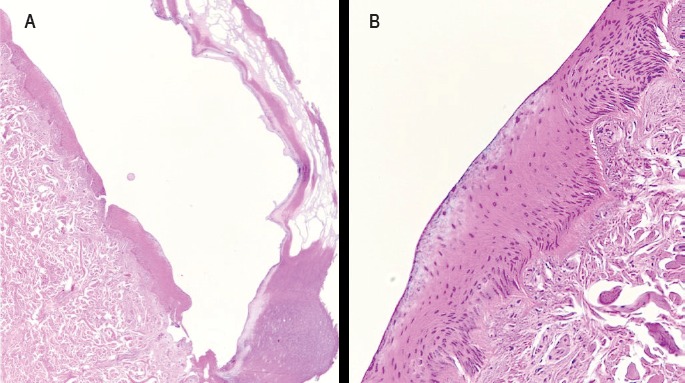
Electrical burn. A) Epidermal blistering (H&E, x40); B) Epithelial nuclear streaming (H&E, x200).
Image courtesy of Dr. Nicholas Batalis.
Delayed Death from Hemorrhage, Sepsis, and Renal Failure
Injuries to the head, such as subdural hemorrhage, can lead to death by raised intracranial pressure over days. Similarly, rupture of subcapsular hematomas of the liver and spleen may cause hemorrhagic shock over a time course of hours to days after injury. Peritonitis from ruptured seromuscular intestinal injuries, infected skin wounds and burns (Images 9 and 10), pneumonia after disability, and neglect following injury can all be immediate causes of death. In fatal cases of musculocutaneous injury, mostly involving the back, buttocks, thighs, and legs, death may occur by myoglobinuric renal failure (6). In these cases, a compartment syndrome may have developed due to hemorrhage and edema around neurovascular bundles. This is disclosed by dissection of the limbs, which may only show minor external injury. The lower leg, ankle, and foot can swell to enormous proportions due to hematoma formation due to pooling of blood in avulsion pockets. Indeed, in severe cases of falanga, the feet may harbor enough blood to cause hemorrhagic shock, but the feet are obviously enlarged and bruised on external examination in such cases.
Image 9.

Subscalpular abscesses complicating burns of head.
Image 10.

Paraspinal pyomyositis complicating burns of back.
Suspension Torture
A common form of torture is suspension of the detainee by the wrist from handcuffs. This gives rise to classical injuries on the wrists including abrasions, bruises, and lacerations. Chronic and recurrent shackling also produces lacerations with varying stages of healing (Image 11). Suspension by the wrists can cause radial and ulnar artery thrombosis and ischemic necrosis of the digits or the entire hand. At autopsy, it is essential to dissect the wrists to explore and histologically sample the ulnar and radial arteries.
Image 11.
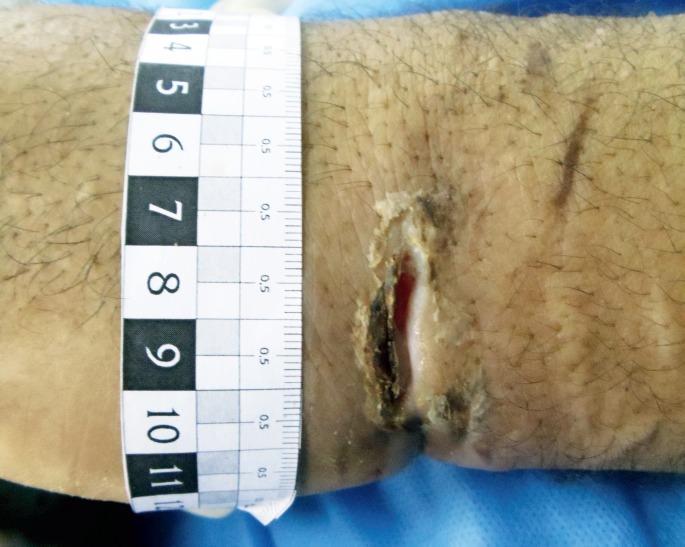
Injuries from chronic handcuffing.
Another common variation of suspension torture is reverse hanging or Palestinian hanging (Figure 1). This is suspension by the wrists or forearms by hyper-extending the upper limbs at the shoulder joint. This position concentrates the body weight on the shoulder and may cause dislocation, hemoarthrosis, avulsive brachial plexus injury, and damage to muscles of the shoulder girdle. Prolonged suspension can cause skeletal muscle necrosis of the pectoralis major, deltoids, and other regional muscles (Image 12). This can lead to fatal myoglobinuric renal failure (7). At autopsy, it is essential to dissect the shoulder joint in cases of possible reverse hanging. Otherwise, this form of torture will escape detection. In the author's experience, this is the most underrecognized form of torture because autopsies seldom involve dissection of the shoulders.
Figure 1:
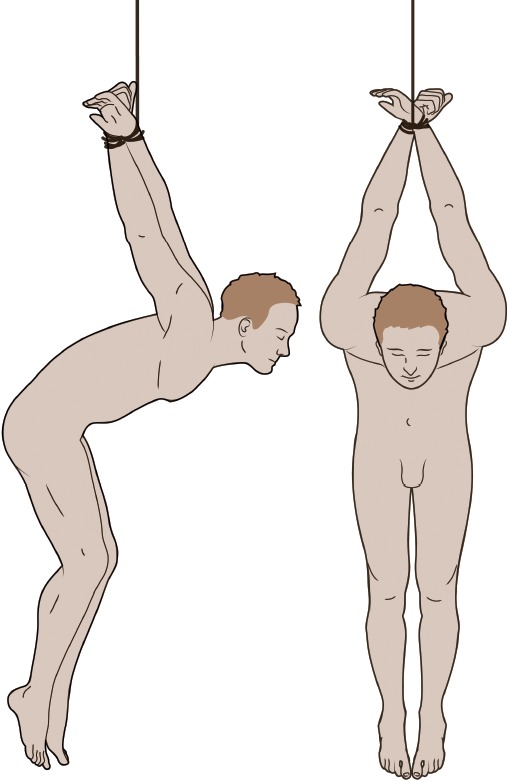
Reverse hanging. Created under contract by professional medical illustrator Diana Kryski.
Image 12.

Necrosis of deltoid after reverse hanging.
Sudden Cardiac Death during Interrogation
Death during interrogation can be sudden and unexpected. In many cases, the only conspicuous postmortem finding is chronic atherosclerotic and/or hypertensive cardiovascular disease. In some of these cases, recent sublethal injuries may be present. The injuries may be nonspecific or appear as regional bruising. In some cases, the injuries can be clearly related to a specific form of torture such as falanga. The question that emerges in these cases is whether the sublethal injuries have caused death by provoking a fatal arrhythmia from marked physiologic stress of a chronically diseased heart. This is exactly analogous to the commonly and widely understood concept of “homicide by heart attack” (8). These cases can often be challenging because the opinion of the forensic pathologist often results in polarizing views of the case. Prison authorities and government officials may claim that the primary cause of death was heart disease and advocates for the detainee will claim that death was due to injury. Therefore, the forensic pathologist must explain how, mechanistically, both cofactors have causal relevance in the fatal pathophysiological cascade. Unless this is understood by interlocutors, the death will remain controversial, rather than being attributed to the consequences of torture (i.e., but-for causation).
Histopathology
Histologic examination is an important element of injury evaluation. The main utility is assessing timing of the injury and secondary complications such as infection. Furthermore, histologic examination provides a permanent reviewable record that can assist in controversial or debated cases. On this basis, histologic examination is strongly recommended in all cases. In some cases, if the autopsy is done under exigent conditions in the field (e.g., conflict zones, at the grave side), the lack of access to formalin, or laboratory facilities can prevent histologic preparation.
Exigent Photographs
In some cases of death during detention, the body will be released to the family without proper investigation by a credible authority. The family members, human right's defenders, and other members of civil society may use that opportunity to take photographs of the body. These photographs are usually obtained with personal electronic devices and can be easily shared electronically and posted on the Internet. The photographs are often valuable sources of information that can be reviewed and interpreted by forensic pathologists, even if an autopsy is not conducted. However, there are two main pitfalls with reviewing these opportunistic photographs. First, the photographs are often biased by what the photographer thinks represents an injury (i.e., selection bias). Therefore, the photographs are often not representative and under-represent body regions that are not easily accessible. Second, lay observers often confuse postmortem artifacts with injuries; for example livor mortis is mistaken for bruising, postmortem drying of the scrotum is mistaken for burns, and decomposition is mistaken for injury.
Conclusion
The autopsy in a case of torture often proves the cause of death and can provide the scientific basis to determine how injuries occurred. Such data are often helpful in international criminal prosecutions. In addition, there is considerable historical and humanitarian value in knowing how people die during times of sociopolitical unrest when human rights are often abused. Furthermore, families are often deeply committed to seeking truth and justice about the fate of their loved ones, particularly if detained by oppressive regimes. The postmortem findings may form part of the critical evidence that underpins the legal determination of torture, crimes committed against humanity, or genocide. Therefore, the role of the forensic pathologist cannot be overemphasized. Indeed, well written descriptions of injuries, high-quality photographs of wounds, and histologic slides of damaged tissues form the incontrovertible basis of the truth, for all to see.
Acknowledgements
The author thanks many courageous collaborators in various countries for ongoing efforts in this domain of forensic pathology.
Footnotes
ETHICAL APPROVAL
As per Journal Policies, ethical approval was not required for this manuscript
STATEMENT OF HUMAN AND ANIMAL RIGHTS
This article does not contain any studies conducted with animals or on living human subjects
STATEMENT OF INFORMED CONSENT
No identifiable personal data were presented in this manuscsript
DISCLOSURES & DECLARATION OF CONFLICTS OF INTEREST
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest
FINANCIAL DISCLOSURE The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript
References
- 1.Thomsen J.L. Helweg-Larsen K. Rasmussen O.V.. Amnesty International and the forensic sciences. Am J Forensic Med Pathol. 1984. Dec; 5(4): 305–11. PMID: 6524593. 10.1097/00000433-198412000-00005. [DOI] [PubMed] [Google Scholar]
- 2.Thomsen J.L. Voigt J.. Forensic medicine and human rights. Forensic Sci Int. 1988. Jan; 36(1-2): 147–51. PMID: 3338686. 10.1016/0379-0738(88)90228-9. [DOI] [PubMed] [Google Scholar]
- 3.Thomsen J.L.. The role of the pathologist in human rights abuses. J Clin Pathol. 2000. Aug; 53(8): 569–72. PMID: 11002757. PMCID: PMC1762934. 10.1136/jcp.53.8.569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Byard R.W. Singh B.. Falanga torture: characteristic features and diagnostic issues. Forensic Sci Med Pathol. 2012. Sep; 8(3): 320–2. PMID: 22105805. 10.1007/s12024-011-9298-6. [DOI] [PubMed] [Google Scholar]
- 5.Brans T.A. Dutrieux R.P. Hoekstra M.J. et al. Histopathological evaluation of scalds and contact burns in the pig model. Burns. 1994; 20 Suppl 1: S48–51. PMID: 8198744. 10.1016/0305-4179(94)90090-6. [DOI] [PubMed] [Google Scholar]
- 6.Malik G.H. Sirwal I.A. Reshi A.R. et al. Acute renal failure following physical torture. Nephron. 1993; 63(4): 434–7. PMID: 8459879. 10.1159/000187248. [DOI] [PubMed] [Google Scholar]
- 7.Pollanen M.S.. Fatal rhabdomyolysis after torture by reverse hanging. Forensic Sci Med Pathol. 2016. Jun; 12(2): 170–3. PMID: 26888609. 10.1007/s12024-016-9752-6. [DOI] [PubMed] [Google Scholar]
- 8.Turner S.A. Barnard J.J. Spotswood S.D. Prahlow J.A.. “Homicide by heart attack” revisited. J Forensic Sci. 2004. May; 49(3): 598–600. PMID: 15171183. 10.1520/jfs2003343. [DOI] [PubMed] [Google Scholar]