

Abstract
Objective:
People’s views regarding autopsy vary according to their cultural and religious beliefs. This paper aims to determine the opinions towards this procedure among Muslims resident in Libya and Muslims and non-Muslims resident in the UK. Our long-term goal is to improve autopsy rates; whether conventional or through the use of post-mortem imaging.
Methods:
400 questionnaires were distributed to the three communities, interrogating belief about post-mortem investigations. Descriptive statistics and non-parametric statistics were used to analyse the data.
Results:
Of the 400 distributed questionnaires, there was a high return rate of 320 (80%). All groups felt that children should be buried sooner than adults(p < 0.001), but 77% of Libyan Muslims thought that children should be buried within 12 h of death compared to 16% of UK Muslims and only 7% of UK non-Muslims (p < 0.001). More non-Muslims were unconcerned about a negative impact of traditional autopsy on the dignity of the corpse than Muslims (p < 0.001) and more Muslims responded that autopsy has a negative emotional effect on the family (p < 0.001). Type of death altered what sort of investigations were desired. In the case of homicide, Libyan Muslims were less likely to prefer CT (p < 0.001) or MRI (p = 0.001). Sex had no effect on the results of the survey.
Conclusion:
Post-mortem imaging is acceptable to both Muslims and non-Muslims in Libya and the UK, but Muslims have a significant preference for post-mortem imaging compared to autopsy, except in homicidal cases.
Advances in knowledge:
(1) The ability of post-mortem imaging to preserve the dignity of the corpse is independent of religion, however, significantly more Muslims feel that autopsy has a negative emotional effect on the family of the deceased. (2) A significant majority of Muslims in Libya prefer to bury children within 12 h of death, while a delay of up to a week is acceptable in UK. (3) Muslims resident in UK have an attitude closer to that of the indigenous (non-Muslim) population and therefore, educational programmes may be successful in changing attitudes of Muslims in Libya and other predominantly Muslim countries.
Introduction
Autopsy is regarded as the gold-standard for determining cause of death.1 Clinically important information is discovered in up to 46% of neonatal and infant autopsies and the procedure is important for eliminating abuse as a cause of death.2 In the last three decades, however, autopsy rates across the world have declined by 40–50%.3 This decline has been influenced by religious, cultural and emotional factors.4 Furthermore, fewer parents are willing to consent and fewer clinicians are asking for permission to perform the autopsy.2, 5 Other reasons given for this decline include administrative bottlenecks when requesting an autopsy and delays in providing the autopsyreport.6
Muslims teach that Allah stressed the importance of maintaining the dignity of the body before and after death. Islam, therefore, calls for respect for the body and recommends that the body should not be disfigured, based on the Hadith, “The breaking of the bone of a dead person is like breaking the bone of a live person”.7 Furthermore, Islam requires that the body be buried soon after death, and that there be no cremation.8 An Islamic fatwa (opinion), issued in 1982, however, states that the benefits of autopsy may be greater than its disadvantages, if it serves justice.9
Over the last three decades, post-mortem imaging has been increasingly used as part of the forensic examination and provides significant information. Post-mortem CT (PMCT) or MRI (PMMRI) scans can be used to detect some causes of death as an addition to, or instead of, a conventional autopsy.1 Medical imaging is particularly useful when consent for conventional autopsy has been withheld. PMCT offers a rapid method of scanning the whole body (including inside a body bag)2 and is now widely used in forensic medicine in adults.
Currently, however, neither MRI nor CT are sufficiently accurate to replace an autopsy as the post-mortem (PM) investigation of choice. In recent studies of PMCT, misinterpretation of PM change and/or poor imaging have led to the cause of death being misdiagnosed.10, 11 Caution and the development of expertise in interpretation are therefore required. In their study, Sieswerda-Hoogendoorn et al5 state that CT identifies bone fractures more reliably than autopsy, including sites such as the face, which might be overlooked during an autopsy examination.3 MRI has been shown to be more acceptable to some parents than conventional autopsy for identifying the cause of death of their child.12, 13 Recently, some UK healthcare centres have begun issuing death certificates which include reports of PMMRI findings that are accepted as medicolegal documents.14
PM imaging has the advantages of being non-invasive and less time consuming than conventional autopsy. Data storage offer the chance to review cases in later years and the ability to highlight areas of interest before (and thereby guiding) the forensic pathology investigation.1 Despite these advantages, conventional autopsy is still the only modality available in Libya for both children and adults. A search of the literature in PubMed, Medline and the Cochrane Systematic Review databases was conducted to identify studies related to the opinion of Muslims on the use of PM imaging to diagnose cause of death; no relevant publications were identified. Prior to the (potentially widespread) introduction of PM imaging to Libya, we aimed to ascertain the opinions and preferences of Muslims and non-Muslims regarding PM imaging (PMCT and PMMRI).
Methods and materials
Study design
This study used a non-validated questionnaire (Supplementary Figure 1) divided into three sections, the first being related to respondents’ demographics. The second section addressed respondents’ knowledge of PM examinations (autopsy, CT and MRI). The third and final section explored reasons why PM examinations might be unacceptable to respondents. A total of 400 questionnaires were distributed to adult volunteers as follows: Group 1: 75 Muslim adults attending an outpatient clinic at Assafwa International Hospital, which is one of the main hospitals in the central region of Libya and 75 Muslim students and teaching staff at Misurata University in Libya. The completed questionnaires were distributed and collected by a colleague in Libya, who then scanned and emailed them to MBT; Group 2: 50 Muslim Libyans self-selected from those attending a regular monthly Libyan community meeting in Sheffield, UK. Participants in Group 2 returned their completed questionnaires to MBT at the Libyan community centre; Group 3: 200 non-Muslims (110 distributed to members of a community centre in Sheffield and 90 to staff and students at the University of Sheffield). Participants in Group 3 also returned their completed questionnaires directly to MBT. The questionnaire was in Arabic for all respondents in Libya and in English for respondents who were resident in the UK.
Ethical approval and consent process
Distributed with the questionnaire was a participant information sheet detailing the nature of the research, the rules governing research and the research objectives, assuring participants that their anonymity would be protected and that responses would be treated with the utmost confidentiality and used only for the purposes of this project. The information sheet also gave a short background to traditional autopsy, CT and MRI. Return of the completed questionnaire was taken as informed consent. The above process was granted ethical approval by the University of Sheffield (Reference Number 007234). Separate ethical approval was also obtained from Misurata University in Libya.
Statistical analysis
Descriptive statistics summarise respondents’ demographics and non-parametric tests were used to compare between groups and methods of investigation. Comparison between groups was by the Χ2 test. Monte-Carlo significances were calculated rather than the traditional asymptotic analysis approach; this removed the need to worry over small sample sizes. For age, a Kruskal-Wallis test was used and a Mann–Whitney for sex. Cochrane-W was used to compare the differences between the different investigations. Statistical analyses were performed using the Statistical Package for the Social Sciences, v. 24 (IBM, Armonk, NY). Statistical significance was set at p < 0.05.
Results
Of the 400 distributed questionnaires, there was a high return rate of 320 (80%) (Table 1 and Figure 1). There was a significant difference in the age of the three groups (KW = p < 0.01) with median (90% CI) for groups 1, 2 and 3 being 30 (27–32), 38 (35–41) and 27 (24–28) years respectively. Equally, there was a significant relationship between education level and the three analysis groups (p = 0.004) with 91.1% of UK Muslims having higher education; however, as there was very little evidence of a separate education effect, this was ignored in the further analyses.
Table 1.
Respondents’ demographics
| Analysis groups a | |||||||||
| Religion | Group 1 | Group 2 | Group 3 | Total | |||||
| Age | ≤25 | 43 | 31% | 0 | 0% | 63 | 46% | 106 | 33% |
| 26–30 | 35 | 25% | 6 | 13% | 28 | 20% | 69 | 22% | |
| 31–40 | 24 | 17% | 21 | 47% | 21 | 15% | 66 | 21% | |
| 41–65 | 34 | 25% | 18 | 40% | 23 | 17% | 75 | 23% | |
| 66+ | 2 | 1% | 0 | 0% | 2 | 2% | 4 | 1% | |
| Sex | Male | 88 | 64% | 31 | 69% | 73 | 53% | 192 | 60% |
| Female | 50 | 36% | 14 | 31% | 64 | 47% | 128 | 40% | |
| Ethnicity | Mixed | 138 | 100% | 45 | 100% | 1 | 1% | 184 | 58% |
| White | 0 | 0% | 0 | 0% | 86 | 63% | 86 | 27% | |
| African | 0 | 0% | 0 | 0% | 18 | 13% | 18 | 6% | |
| Black | 0 | 0% | 0 | 0% | 7 | 5% | 7 | 2% | |
| Asian | 0 | 0% | 0 | 0% | 24 | 18% | 24 | 8% | |
| Other | 0 | 0% | 0 | 0% | 1 | 1% | 1 | 0% | |
| Income | Less than £250 | 30 | 2% | 4 | 9% | 1 | 1% | 35 | 11% |
| £250–500 | 14 | 10% | 2 | 4% | 0 | 0% | 16 | 5% | |
| £500–750 | 30 | 22% | 4 | 9% | 16 | 12% | 50 | 16% | |
| £750–1000 | 45 | 33% | 11 | 24% | 37 | 27% | 93 | 29% | |
| £1000–2000 | 15 | 11% | 14 | 31% | 16 | 12% | 45 | 14% | |
| £2000–3000 | 2 | 1% | 5 | 11% | 48 | 35% | 55 | 17% | |
| More than £ 3000 | 2 | 1% | 5 | 11% | 19 | 14% | 26 | 8% | |
aGroup 1, Muslims in Libya; Group 2, UK Muslims; Group 3, UK non-Muslims.
Figure 1.

Distribution of questionnaires/response rate The figure summarises distribution of the questionnaire and response rate from the various groups of respondents.
Asked whether they had previously heard about post-mortem imaging, the percentage of positive responses for PMCT and PMMRI respectively were Group 1: 16 and 14%, Group 2: 7 and 6% and Group 3: 31 and 80% (p < 0.001).
For both adult and child burials, differences in opinion concerning an acceptable delay in burial were significant when comparing the three respondent groups and when comparing all Muslims to non-Muslims (p ranged from < 0.001 to < 0.011, Table 2). Muslims in Libya preferred more rapid burial, particularly for children; 77% of Group 1, 16% of Group 2 and only 7% of Group 3 preferring to bury a child within 12 h of death(p < 0.001).
Table 2.
Acceptable time before burial of children and adults
|
Religion/
residence a |
Time to burial (Child) | Time to burial (Adult) | |||||||||
| <12 h | 12–24 h | 1–3 days | 4–7 days | >7 days | <12 h | 12–24 h | 1–3 days | 4–7 days | >7 days | ||
| Group 1 | 101 | 37 | 0 | 0 | 0 | 62 | 54 | 22 | 0 | 0 | |
| Group 2 | 21 | 13 | 11 | 0 | 0 | 12 | 17 | 16 | 0 | 0 | |
| Group 3 | 9 | 18 | 43 | 34 | 33 | 4 | 11 | 43 | 29 | 50 | |
| p-values:a | |||||||||||
| Child burials | Adult burials | Child vs adult burials | |||||||||
| Group 1 vs Group 2: p < 0.001 | Group 1 vs Group 2: p < 0.011 | Group 1: Χ2 test was statistically significant at p < 0.001 | |||||||||
| Group 2 vs Group 3: p < 0.001 | Group 2 vs Group 3: p < 0.001 | Group 2: Χ2 test was statistically significant at p < 0.001 | |||||||||
| Muslims (All) vs Group 3: p < 0.001 | Muslims (All) vs Group 3 p < 0.001 | Group 3: Χ2 test was statistically significant at p < 0.001 | |||||||||
aGroup 1, Muslims in Libya; Group 2, UK Muslims; Group 3, UK non-Muslims.
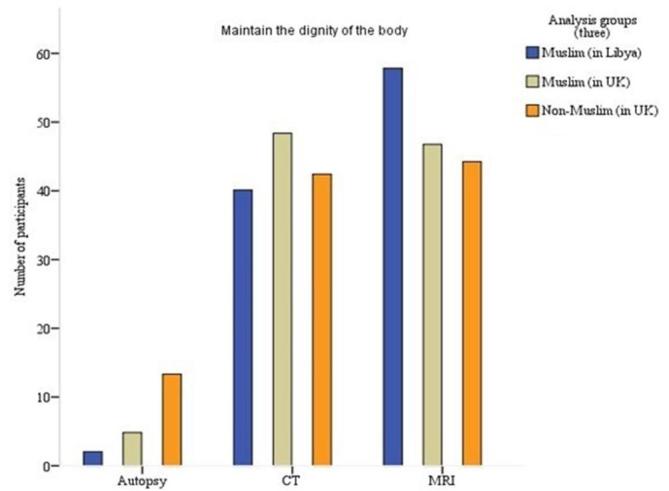
More of Groups 1 and 2 (88% and 91% respectively) than Group 3 (72%) felt that autopsy leads to an unnecessary delay in burial (p < 0.001, Table 3). More non-Muslims were unconcerned about the impact of traditional autopsy on the dignity of the corpse than Muslims (Table 3, Figure 2). The ability of post-mortem imaging to preserve the dignity of the corpse was independent of religion, however Muslims felt differently about the emotional impact of autopsy, with 93, 98 and 64% of groups 1, 2 and 3 respectively, responding that autopsy has a negative emotional effect on the family (p < 0.001, Figure 3).
Table 3.
Unacceptable delay in burial and preservation of the corpse’s dignity
| Causes an unacceptable delay in burial n (%) | ||||
| Post-mortem method |
Muslims in Libya
(Group 1) |
UK Muslims
(Group 2) |
UK non-Muslims
(Group 3) |
p- value |
| CT | 6 (4%) | 0 (0%) | 27 (20%) | <0.001 |
| MRI | 11 (8%) | 4 (9%) | 32 (23%) | 0.001 |
| Autopsy | 122 (88%) | 41 (91%) | 99 (72%) | <0.001 |
| Dignity of the corpse | ||||
| CT | 59 (43%) | 30 (67%) | 70 (51%) | 0.019 |
| MRI | 85 (62%) | 29 (64%) | 73 (53%) | 0.264 |
| Autopsy | 3 (2%) | 3 (7%) | 22 (16%) | <0.001 |
Figure 2.
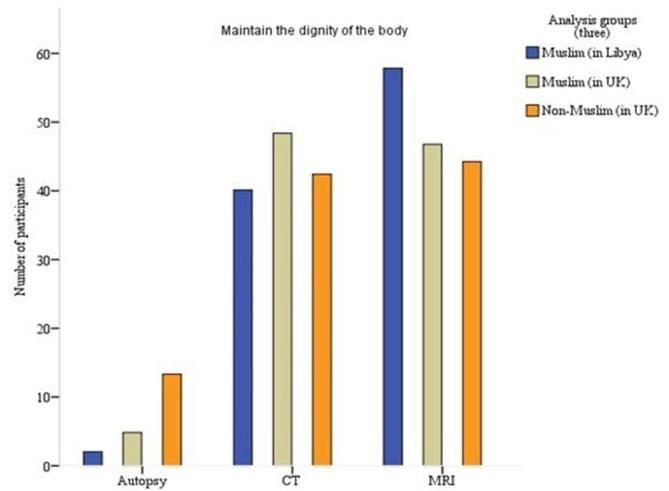
Post-mortem methods investigations that preserve the dignity.
Figure 3.
Post-mortem methods lead to a negative emotional effect on the family.
In terms of identifying the cause of homicidal deaths, 58% of Group 1, 64% of Group 2 and 52% of Group 3 felt that autopsy should be used (p = 0.289). In contrast, 42% of Group 1, 47% of Group 2 and 26% of Group 3 preferred the use of CT to investigate the causes of natural and unexplained death (p = 0.004), while no respondent from Group 1, 2% of Group 2 and 16% of Group 3 preferred conventional autopsy to investigate natural expected deaths (p < 0.001). Finally, 31% of Group 1, 51% of Group 2 and 52% of Group 3 (p = 0.001) preferred the use of MRI over autopsy to investigate the causes of suspicious deaths (Table 4).
Table 4.
PM imaging vs conventional autopsy
| Mode of death | ||||
| Homicide/suicide n (%) | ||||
| Religion | Group 1 | Group 2 | Group 3 | p-value |
| CT | 29 (21%) | 15 (33%) | 66 (48%) | < 0.001 |
| MRI | 30 (22%) | 19 (42%) | 56 (41%) | 0.001 |
| Autopsy | 80 (58%) | 29 (64%) | 71 (52%) | 0.289 |
| Natural but unexplained | ||||
| Religion | Group 1 | Group 2 | Group 3 | p-value |
| CT | 58 (42%) | 21 (47%) | 35 (26%) | 0.004 |
| MRI | 55 (40%) | 29 (64%) | 54 (39%) | 0.008 |
| Autopsy | 27 (20%) | 4 (9%) | 73 (53%) | < 0.001 |
| Natural and expected | ||||
| Religion | Group 1 | Group 2 | Group 3 | p-value |
| CT | 89 (65%) | 33 (73%) | 21 (15%) | < 0.001 |
| MRI | 51 (37%) | 17 (38%) | 36 (26%) | 0.119 |
| Autopsy | 0(0%) | 1 (2%) | 22 (16%) | < 0.001 |
| Suspicious | ||||
| Religion | Group 1 | Group 2 | Group 3 | p-value |
| CT | 52 (38%) | 18 (40%) | 50 (37%) | 0.903 |
| MRI | 43 (31%) | 23 (51%) | 71 (52%) | 0.001 |
| Autopsy | 45 (33%) | 16 (36%) | 44 (32%) | 0.935 |
aGroup 1, Muslims in Libya; Group 2, UK Muslims; Group 3, UK non-Muslims.
There was a significant difference in annual income between Muslim and non-Muslim respondents (p < 0.001), however, there was no difference in salary between those who approved of conventional autopsy and those who did not (p = 0.894).
Discussion
The recent Arab uprising has been associated with considerable damage to infrastructure and a significant number of people have been killed;15 a total of 21,490 persons were killed in Libya between February 2011 and February 2012. Due to the high number of criminal offences and the limited number of consultant pathologists in Libya, there are difficulties with investigating and explaining the circumstances of death.16 Post-mortem imaging may play an important role.
As far as we are aware, this study is the first to formally evaluate the acceptability of PMCT and PMMRI of Libyan Muslims and UK Muslims of Libyan descent with that of non-Muslim UK residents.
This study shows that both Muslims and non-Muslims perceive conventional autopsy to have a negative emotional effect on family members due to its invasiveness and (for Muslims) the delay to burial that it causes.
Most non-Muslim participants had heard about post-mortem imaging compared to only a small minority of Muslims (mainly doctors and/or those resident in the UK). By comparison, most Muslim and non-Muslim participants were aware of conventional autopsy as an investigational procedure. These differences in awareness between Muslim and non-Muslim participants may be attributed to the fact that several UK healthcare providers now routinely offer post-mortem MRI in children and PMCT in adults and that some families may have participated in or have been aware of previous/ongoing diagnostic accuracy studies of PM imaging. In Libya on the other hand, conventional autopsy is the only available means of PM investigation. We pre-empted this lack of awareness when distributing the questionnaires by providing a short background to conventional autopsy, PMCT and PMMRI as an introduction to the questionnaire.
The time to burial of the body is important in the Libyan culture and is an essential issue for the Muslim family of the deceased, since the culture enforces the religious belief that the body should be buried as soon as possible to reduce the emotional effect on the family and to respect the deceased. It is clearly demonstrated in this study that Muslim participants in Libya support this view, with a significant number feeling that burial should occur within 12 h of death. This contrasts with the views of non-Muslims, for which no respondent felt that burial was necessary within 24 h of death and that delays of up to a week were acceptable. Age appears to be negatively related to time of burial but is best interpreted as an artefact of the data collection, where UK Muslims tended to be older than Libyan Muslims and UK non-Muslims, i.e. there is a lack of mature non-Muslims in our study population. These views were irrespective of sex. Of interest, more Muslims in the UK had no concerns if burial was delayed for up to 3 days following death. This might be due to differences in the process of obtaining approval for burial and/or due to their living in the UK and assimilating the views of that population. Our results support those of Gatrad et al, that Muslims prefer to bury the body immediately or as soon as possible after death.17, 18 Another study showed that 3 days is generally considered the maximum delay before burial of a body in the Muslim world,7 which is in keeping with the attitudes of the Muslims we surveyed in the UK. Lishimpi et al19 who studied the guardians and parents of deceased children in Zambia, also found that concerns about time delay before burial had an influence on decisions to refuse an autopsy, although the religion of their study participants was not provided.19 Only a small number of Muslim participants in our study thought (perhaps incorrectly) that CT and MRI could lead to unnecessary delay to burial.
“Mutilation” of the body is an important reason that might lead a family to refuse a PM examination9 along with a fear that organs might be sold for transplantation.19 Less invasive methods such as medical imaging can help maintain the body’s dignity, which Muslim and non-Muslim participants of this study also believe. On the other hand, non-Muslim participants were more prepared to accept that a conventional autopsy would not violate the body’s dignity and here, the influence of religion is clearly seen. This result is supported by Ben‐Sasi et al who pointed out that generally, traditional autopsy was perceived comparatively favourably (scored 8 out of 10), with certain demographic factors affecting the overall autopsy acceptability, including ethnicity (more Caucasian and African individuals preferred autopsy compared to Asian or Arabic individuals) and religion (Christians and those with no religious beliefs found autopsy more acceptable than did those of Muslim or Sikh faiths).20 Other studies supporting our results include: (1) Lynch, who found that Hindus and those of other religions are considered to have a less intrinsic objection to autopsy than Muslims.21 (2) Cox et al who reported from Uganda, that 59% of relatives (Muslim and non-Muslim) were opposed to autopsy for reasons including delayed burial, body mutilation and associated reasons of a religious nature. Furthermore, the rate of autopsies decreased by approximately 9% due to cultural beliefs and fears that it might lead to infertility among females.22 (3) Loughrey who showed that relatives and parents might not consider the benefits of an autopsy and may prefer to “maintain the physical dignity” of their loved one, rather than define the precise cause of death23 and (4) Parmar and Rathod, most of whose study participants refused conventional autopsy due to the delay in burial and concern about the cutting of the body or removal of organs.24 Furthermore, consenting to post-mortem examination, especially for infants or children, is psychologically distressing for all guardians involved.
Despite the overall preference for PM imaging over conventional autopsy, it was interesting to find that Muslim participants preferred conventional autopsy for the investigation of homicides and PM imaging for the investigation of unsuspicious deaths. This might imply more belief, by Muslims, in the intrinsic superiority of conventional autopsy to identify the cause of any death. This might not be a misguided belief, since Hussain et al showed that autopsy explained 78% of cases of homicidal deaths.11 On the other hand, PMMRI has been shown to be accurate in detecting abnormal pathology in foetuses (sensitivity 77%, specificity 95%), with slightly lower specificity and sensitivity in children,25 while PMCT identified the main pathologic process leading to death in 39 of 40 adults,26 such that in certain instances, PM imaging is not inferior to conventional autopsy.
Our survey included 15 physicians (all Muslim) who did not respond significantly differently to the non-physicians. It has been shown that some physicians find the request from relatives for PM examination of a loved one, to be one of the most difficult and unpleasant quarters of paediatric medical practice.22 Interestingly, in their survey of general practitioners and clinicians, Midelfart and Aase showed that the number of doctors participating in their study who found that the value of autopsy had decreased due to improvements in CT and MRI techniques was 81 and 71% for each modality respectively.27 We disagree that the value of autopsy has decreased and do not perceive it as a case of performing one or the other technique, but rather we believe that PM imaging should be viewed as an adjunct to conventional autopsy and a replacement only when consent for conventional autopsy is withheld. This is a view we have previously expressed and that is held by others.28, 29
Roberts et al pointed out that the cost implications of PM imaging may be a concern; MRI in particular is more expensive than traditional autopsy.30 In Group 1, the average salary was particularly low and in Libya, healthcare is paid for by the individual. It might be expected that in Libya, caution over the cost of MRI would be a concern, which is congruent with over half of the people in Group 1 being cautious of using this technique. A similar caution may be applied to CT. Healthcare in the UK is free at the point of delivery and therefore, cost is not necessarily of personal concern to the individual. Sex had no effect on the results of the survey. As far as we know, there are no published studies that have previously measured the impact of variables such as sex and income on the acceptance rate of autopsies.
This study has several limitations. Firstly, although there were high response rates of 94% from Muslims and 70% from non-Muslims, the precise reasons for those who received but did not return their questionnaires are not available, since we did not attempt to contact the relevant individuals. There may therefore be self-selection bias (particularly amongst non-Muslims), which the study design has not allowed us to ascertain. However, response rate does not necessarily determine the validity of a survey.31 Even if response rates are low, with careful planning questionnaire surveys may provide high quality data. The anonymous nature may encourage participants to give more frank and credible answers than (for example) interviews, thus helping to reduce bias.32 Probably of more significance than determining reasons why some did not respond, is the fact that we used a non-validated questionnaire. Although the process of validating a questionnaire is time-consuming, it does improve the reliability and accuracy of the collected data.33 As part of the validation process, it is also recommended that a pilot study of the questionnaire be conducted. The utility of both validated and non-validated questionnaires is improved when the following conditions are met (as in the current study): the target audience, even if geographically spread apart, can be easy defined and identified; the majority of participants understand what is being asked of them; and the focus of the analysis is numerical, i.e. the questionnaire provides quantitative data.34 A final limitation of the study is that the questionnaire was distributed to Libyan Muslims in only two countries; Muslims from (or living in) other countries might have responded differently (as indeed might non-Muslims from or living in other countries). Future steps include validating the questionnaire and repeating the study in other populations.
In conclusion, religious beliefs and age of the deceased (child vs adult) affect individual preference for PM investigational methods. The preference amongst Muslims for PM imaging is mainly related to the perception that it leads to less delay to burial and is less invasive. Interestingly, conventional autopsy is preferred by Muslims when the cause of death is suspicious. Muslims resident in the UK have an attitude closer to that of the indigenous (non-Muslim) population and therefore, in conjunction with developing expertise in performing and reporting on post-mortem imaging investigations, educational programmes may be successful in changing attitudes of Muslims in Libya and other predominantly Muslim countries.
Contributor Information
Mohamed Ben Taher, Email: mbentaher1@sheffield.ac.uk.
Jean Pearson, Email: j.russell@sheffield.ac.u.
Marta Cohen, Email: Marta.Cohen@sch.nhs.uk.
Amaka C Offiah, Email: a.offiah@sheffield.ac.uk.
REFERENCES
- 1. Underwood J. Post-mortem imaging and autopsy: rivals or allies? The Lancet 2012; 379: 100–2. doi: 10.1016/S0140-6736(11)61584-5 [DOI] [PubMed] [Google Scholar]
- 2. Thayyil S, Chitty LS, Robertson NJ, Taylor AM, Sebire NJ. Minimally invasive fetal postmortem examination using magnetic resonance imaging and computerised tomography: current evidence and practical issues. Prenat Diagn 2010; 30: 713–8. doi: 10.1002/pd.2534 [DOI] [PubMed] [Google Scholar]
- 3. Stawicki S, Aggrawal A, Dean A, Bahner D, Steiberg S, Stehly C. Postmortem use of advanced imaging techniques: is autopsy going digital. OPUS 2008; 12: 17–26. [Google Scholar]
- 4. Noda Y, Yoshimura K, Tsuji S, Ohashi A, Kawasaki H, Kaneko K, et al. Postmortem computed tomography imaging in the investigation of nontraumatic death in infants and children. Biomed Res Int 2013; 2013: 1–5. doi: 10.1155/2013/327903 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Sieswerda-Hoogendoorn T, van Rijn RR. Current techniques in postmortem imaging with specific attention to paediatric applications. Pediatr Radiol 2010; 40: 141–52. doi: 10.1007/s00247-009-1486-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Oluwasola OA, Fawole OI, Otegbayo AJ, Ogun GO, Adebamowo CA, Bamigboye AE. The autopsy: knowledge, attitude, and perceptions of doctors and relatives of the deceased. Arch Pathol Lab Med 2009; 133: 78–82. doi: 10.1043/1543-2165-133.1.78 [DOI] [PubMed] [Google Scholar]
- 7. Mohammed M, Kharoshah MA. Autopsy in Islam and current practice in Arab Muslim countries. J Forensic Leg Med 2014; 23: 80–3. doi: 10.1016/j.jflm.2014.02.005 [DOI] [PubMed] [Google Scholar]
- 8. Gatrad AR. Muslim customs surrounding death, bereavement, postmortem examinations, and organ transplants. BMJ 1994; 309: 521–3. doi: 10.1136/bmj.309.6953.521 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Puranik R, Gray B, Lackey H, Yeates L, Parker G, Duflou J, et al. Comparison of conventional autopsy and magnetic resonance imaging in determining the cause of sudden death in the young. J Cardiovasc Magn Reson 2014; 16: 44. doi: 10.1186/1532-429X-16-44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Oyake Y, Aoki T, Shiotani S, Kohno M, Ohashi N, Akutsu H, et al. Postmortem computed tomography for detecting causes of sudden death in infants and children: retrospective review of cases. Radiat Med 2006; 24: 493–502. doi: 10.1007/s11604-006-0061-y [DOI] [PubMed] [Google Scholar]
- 11. Hussain Z, Shah MM, Afridi HK, Arif M, Ayub J. Homicidal deaths by firearms in Peshawar: an autopsy study. J Ayub Med Coll Abbottabad 2006; 18: 44–7. [PubMed] [Google Scholar]
- 12. Cannie M, Votino C, Moerman P, Vanheste R, Segers V, Van Berkel K, et al. Acceptance, reliability and confidence of diagnosis of fetal and neonatal virtuopsy compared with conventional autopsy: a prospective study. Ultrasound Obstet Gynecol 2012; 39: 659–65. doi: 10.1002/uog.10079 [DOI] [PubMed] [Google Scholar]
- 13. Wichmann D, Obbelode F, Vogel H, Hoepker WW, Nierhaus A, Braune S, et al. Virtual autopsy as an alternative to traditional medical autopsy in the intensive care unit: a prospective cohort study. Ann Intern Med 2012; 156: 123–30. doi: 10.7326/0003-4819-156-2-201201170-00008 [DOI] [PubMed] [Google Scholar]
- 14. Thayyil S. Less invasive autopsy: an evidenced based approach. Arch Dis Child 2011; 96: 681–7. doi: 10.1136/adc.2009.165704 [DOI] [PubMed] [Google Scholar]
- 15. Daw MA, El-Bouzedi A, Dau AA. Libyan armed conflict 2011: Mortality, injury and population displacement. Afr J Emerg Med 2011; 2015: 101–7. [Google Scholar]
- 16. Araby OA. 55 thousand criminal offences in Libya and experts accuse the militias 2016. 2018. Available from: http://ara.tv/zcdz5 [updated 2018 July 13; cited 2018Jul 9].
- 17. Gatrad AR. Muslim customs surrounding death, bereavement, postmortem examinations, and organ transplants. BMJ 1994; 309: 521–3. doi: 10.1136/bmj.309.6953.521 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Black J. Broaden your mind about death and bereavement in certain ethnic groups in Britain. Br Med J 1987; 295: 536–539. doi: 10.1136/bmj.295.6597.536 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Lishimpi K, Chintu C, Lucas S, Mudenda V, Kaluwaji J, Story A, et al. Necropsies in African children: consent dilemmas for parents and guardians. Arch Dis Child 2001; 84: 463–7. doi: 10.1136/adc.84.6.463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Ben-Sasi K, Chitty LS, Franck LS, Thayyil S, Judge-Kronis L, Taylor AM, et al. Acceptability of a minimally invasive perinatal/paediatric autopsy: healthcare professionals' views and implications for practice. Prenat Diagn 2013; 33: n/a–12. doi: 10.1002/pd.4077 [DOI] [PubMed] [Google Scholar]
- 21. Lynch M. Forensic pathology: redefining medico-legal death investigation. Journal of Law and Medicine 1999; 7: 67–74. [Google Scholar]
- 22. Cox JA, Lukande RL, Kateregga A, Mayanja-Kizza H, Manabe YC, Colebunders R. Autopsy acceptance rate and reasons for decline in Mulago Hospital, Kampala, Uganda. Trop Med Int Health 2011; 16: 1015–8. doi: 10.1111/j.1365-3156.2011.02798.x [DOI] [PubMed] [Google Scholar]
- 23. Loughrey MB, McCluggage WG, Toner PG. The declining autopsy rate and clinicians' attitudes. Ulster Med J 2000; 69: 83. [PMC free article] [PubMed] [Google Scholar]
- 24. Parmar P, Rathod GB. Study of knowledge, attitude and perception regarding medico-legal autopsy in general population. Int J Med Pharm Sci 2013; 3: 1–6. [Google Scholar]
- 25. Arthurs OJ, Thayyil S, Owens CM, Olsen OE, Wade A, Addison S, et al. Diagnostic accuracy of post mortem MRI for abdominal abnormalities in foetuses and children. Eur J Radiol 2015; 84: 474–81. doi: 10.1016/j.ejrad.2014.11.030 [DOI] [PubMed] [Google Scholar]
- 26. Ross S, Ebner L, Flach P, Brodhage R, Bolliger SA, Christe A, et al. Postmortem whole-body MRI in traumatic causes of death. AJR Am J Roentgenol 2012; 199: 1186–92. doi: 10.2214/AJR.12.8767 [DOI] [PubMed] [Google Scholar]
- 27. Midelfart J, AASE S. The value of autopsy from a clinical point of view. APMIS 1998; 106: 693–8. doi: 10.1111/j.1699-0463.1998.tb00213.x [DOI] [PubMed] [Google Scholar]
- 28. Cohen MC, Whitby E, Fink MA, Collett JM, Offiah AC. Running a postmortem service-a business case and clinical experience. Pediatr Radiol 2015; 45: 501–8. doi: 10.1007/s00247-014-3156-0 [DOI] [PubMed] [Google Scholar]
- 29. Whitby EH, Offiah AC, Cohen MC. Initial experiences of a minimally invasive autopsy service. A report of the techniques and observations in the first 11 cases. Pediatr Dev Pathol 2015; 18: 24–9. doi: 10.2350/14-06-1503-OA.1 [DOI] [PubMed] [Google Scholar]
- 30. Roberts ISD, Benamore RE, Benbow EW, Lee SH, Harris JN, Jackson A, et al. Post-mortem imaging as an alternative to autopsy in the diagnosis of adult deaths: a validation study. The Lancet 2012; 379: 136–42. doi: 10.1016/S0140-6736(11)61483-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Morton SM, Bandara DK, Robinson EM, Carr PE. In the 21st Century, what is an acceptable response rate? Aust N Z J Public Health 2012; 36: 106–8. doi: 10.1111/j.1753-6405.2012.00854.x [DOI] [PubMed] [Google Scholar]
- 32. Williams A. How to..write and analyse a questionnaire. J Orthod 2003; 30: 245–252. doi: 10.1093/ortho/30.3.245 [DOI] [PubMed] [Google Scholar]
- 33. Smit PR, de Jong RR, Bijleveld CC. Homicide data in Europe: definitions, sources, and statistics. Handbook of European homicide research. The British Institute of Radiology.; 2012. 5–23. [Google Scholar]
- 34. Jack B, Clarke AM. The purpose and use of questionnaires in research. Prof Nurse 1998; 14: 176–9. [PubMed] [Google Scholar]