

Summary
Background
Few studies focus on the role training has on rescue workers who are active as volunteers or actual workers in emergency situations such as an earthquake. In October 2016, a strong earthquake hit Central Italy and in particular the province of Macerata in the Marche region. Lots of rescuers were called to deal with the emergency. The aim of this study was, therefore, to examine their preparation, studying resilience and coping strategies, as these qualities can protect against complications brought on by traumatic situations (post traumatic stress disorder).
Study design
An observational study on 70 rescue workers who active in the area affected by the disaster within the province of Macerata was carried out.
Materials and methods
The questionnaire proposed by the Coping Inventory for Stressful situations (CISS) was used, while individual resilience levels were measured with the Resilience Scale. Both methods were employed in two separate interviews conducted before and after their intervention in the disaster area. To verify a possible difference between the resilience and coping values before and after the activity of rescue effort, the paired Student t test was applied.
Results
The sample showed medium to high levels of coping (91.6%) and resilience (89.6%) were present in both interviews and not significant statistical differences was observed for the resilience (among females t = 1.63, p-value = 0.179, and among males (t = -0.76; p-value = 0.487). In contrast, CISS scores before and after the rescue effort showed significant statistical differences both among females (t = 4.81; p-value = 0.009) and males (t = 10.06; p-value = 0.001).
Some areas relative to coping mechanisms, such as social avoidance and distraction are preferred by women, while men prefer avoidance and task-oriented activity. Results for resilience show a slight difference for perseverance in men.
Conclusions
The ability to use mechanisms of self-preservation like coping and resilience helps rescue workers to better respond in emergency situations. Surely one of the most appropriate ways to reach this result is provided by their preparation.
Key words: Coping, Resilience, Earthquake, Rescue
Introduction
In October 2016, Central Italy was struck by a magnitude 6.5 earthquake affecting the Marche region, Abruzzo and Lazio. The extent of the event resulted in an unprecented migration of inhabitants from the mountainous areas towards the coast. Relief efforts were immediate and hundreds of rescue workers were mobilized by the Italian Civil Protection department. Rescue workers perform their role as volunteers or paid workers and offer out-of-hospital medical aid [1-4].
In view of this type of complex activity, rescue workers can be more exposed to stressful situations that can give rise to disturbances such as Post Traumatic Stress Sindrome (PTSD), which increase with the frequency of traumatic events [5-10]. Studies carried out in connection with separate disasters on people involved in rescue efforts suggest that the symptoms associated with post traumatic stress disorder are stronger depending on the magnitude of the event, exposure to corpses, failure to save survivors, identifying with victims, stress, fatigue and potential first-person exposure to danger [11, 12]. Some categories, such as maritime search and rescue workers, associate the stress of a particularly tough training period (although inevitable for that particular mission) with work-related stress. Factors which, when combined, can increase the frequency of PTSD and adjustment disorders (ADS) [13, 14].
Adjustment disorders, though more frequent, are generally not given the same importance as PTSD. Characterized by milder symptoms which are actually treacherous as they are more easily hidden or disguised, and perhaps not even fully understood by the rescue workers themselves, leading them to ignore their unease and aggravate existing problems [15].
Therefore, it is central to investigate methods which can best help rescue workers to identify and use individual, interpersonal, medical and environmental resources to reduce levels of stress and encourage adjustment in this high-risk group. For example, resilience and coping are important factors in the development of strategies to prevent and cure psychological distress (depression, anxiety and stress), allowing the person to overcome difficult situations.
Resilience, generally associated with low levels of psychological stress, should be taken into consideration when evaluating protection and risk factors. To face internal and external needs associated with the task at hand, the rescue worker has to be able to marshal and make use of all his/her resources [16, 17]. Given the above, training is fundamentally important for rescue workers and should increase their knowledge on subjects which are not limited to organisational management but include items such as Emergency Response Psychology, Public Healthcare, Hygiene and Preventive Medicine [18-24]. In the light of events connected to the latest earthquake in Central Italy and in view of the lack of knowledge on the relationship between specific training and resilience/coping strategies adopted by emergency rescue workers, we thought it would be interesting to take a closer look at their psychological well-being in relation to the sort of training they had received [25, 26].
Materials and methods
The study was carried out in the province of Macerata, in areas affected by the Central Italian earthquake of 2016, and was conducted in accordance with the latest version of the Declaration of Helsinki. The sample consisted of volunteers who came to the aid of victims, randomly selected from lists provided by voluntary associations that had taken part in the rescue effort, trying to include an equal sample of women and men. During the emergency phase, volunteers were interviewed after being informed about the study by specifically trained personnel under the supervision of psychologists. During the first phase of testing, before the rescue effort, a questionnaire was administered to measure general levels of resilience and coping, and the results were reported as percentage. This had previously been evaluated by submitting it to a sample of 100 volunteers who were involved in the earlier Aquila earthquake (2009), a fact which also allowed us to investigate the socio-demographic characteristics of the sample. Afterwards, in order to evaluate aspects related to resilience and coping levels in rescue workers prior to and after their participation in the rescue effort, two approved questionnaires were administered. The Coping Inventory for Stressful Situation (CISS) for adults was used to investigate various coping strategies such as task-oriented, emotion-oriented, avoidance-oriented, distraction and social diversion [27]. The questionnaire is composed of 48 questions to which responders choose an answer from 1 (not at all) to 5 (very much). The “standard score” is calculated (T scale) as well as the percentile rank (% ile). Results are “lower than average” to “higher than average” and the cut-off has been set at 50. Individual resilience was measured using the “Resilience Scale” (US English version of the Resilience Scale, di Gail M, Wagnild RN - Resilience Center Worden, Montana, USA) which assesses self reliance, meaning, equanimity, perseverance and existential aloneless [28]. The resilience scale is composed of 25 questions, to which the responder must give an answer ranging from 1 (strongly disagree) to 7 (strongly agree); results are interpreted on a total RS score and values are confronted with the following scores in the manual: 25-100 (very low degree of resilience), 101-115 (low degree of resilience), 116-130 (moderately low degree of resilience), 131-144 (moderate degree of resilience), 145-160 (high resilience degree), 161-175 (very high degree of resilience) [29]. A second interview was administered after their participation in the rescue effort to measure any changes in their coping and resilience levels. Data were gathered by first obtaining informed consent from the interviewee and asking the participant to sign it to signify willingness to take part in the study.
STATISTICAL ANALYSIS
To verify a possible difference between the resilience and coping values before and after the activity of rescue effort, the paired Student t test was applied, processing the data with the XLStat software at a significant level (%): 5 [30].
Results
A total of 70 questionnaires was handed out and 52 of these were completed, bringing compliance up to 74%. The percentage of males and females in the sample is almost equal. Most survey respondents are aged between 21 and 60 (90.4%) with the most common group aged 21-30 (48%) (Tab. I).
Tab. I.
Sample characteristics.
| Gender | n. | % |
|---|---|---|
| Males | 24 | 46.00 |
| Females | 28 | 54.00 |
| Total | 52 | |
| Age | ||
| < = 20 | 0 | 0 |
| 21-30 | 25 | 48.00 |
| 31-40 | 8 | 15.40 |
| 41-50 | 6 | 11.50 |
| 51-60 | 8 | 15.40 |
| > = 61 | 5 | 9.60 |
| Total | 52 | |
| Level of education | ||
| Primary school certificate | 3 | 5.80 |
| Middle school certificate | 2 | 3.90 |
| Secondary school certificate | 29 | 55.80 |
| Bachelor’s degree | 12 | 23.00 |
| Master’s degree | 5 | 9.60 |
| n.r. | 1 | 1.90 |
| Total | 52 | |
| Employment | ||
| Student | 10 | 19.20 |
| Worker | 20 | 38.50 |
| Student and worker | 12 | 23.00 |
| Housewife | 1 | 1.90 |
| Unemployed | 3 | 5.70 |
| Pensioner | 5 | 9.50 |
| n.r. | 1 | 1.90 |
| Total | 52 |
Generally speaking, the sample shows a medium/high coping level (91.6%) and a low level of 8.4% (Fig. 1a).
Fig. 1.
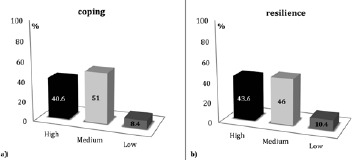
a) Coping level (%), b) Resilience level (%), calculated on the whole sample, during the first phase of testing.
Regarding individual resilience, results are in line with values associated with coping, with 89.6% of the sample displaying high/medium levels of resilience; on the contrary, only 10.4% display low levels (Fig. 1b).
Results for the single items measured by the CISS obtained in the first and second interviews show levels above 50 %ile (the cut-off point between below average coping levels and above average coping levels) in all subscales, with the exception of the emotion-oriented scale. For task-oriented coping mechanisms, women are on the cut-off point, while men have higher scores (Fig. 2).
Fig. 2.

Coping Inventory for Stressful Situations (CISS) scores in percentile rank (% ile; CUT OFF = 50%ile) in males, females and total sample for Task: task-oriented coping factor, Emotion: emotion-oriented coping factor, Avoidance: avoidance-oriented coping factor in a) first interview and in b) second interview. (Student t test between the first and second interview among females t = 4.81; p-value = 0.009, and among males t = -10.06; p-value = 0.001).
Avoidance seems most used by men, while distraction and social diversion is preferred by women.
Levels of resilience do not seem to have undergone significant changes between the first and second interview, though a higher score was noticed for men (total value of resilience). Considering the fact that scores for very low resilience go from 25-100, 101-115 for low resilience, 116-130 for moderately low resilience, 131-144 for moderate resilience, 145-160 for moderately high resilience, 161-175 for high resilience, both men and women show moderate levels (Fig. 3).
Fig. 3.
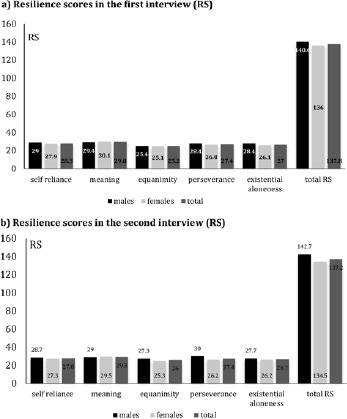
Resilience Score (RS) in a) first interview, and b) second interview in males, females and total sample. Resilience Scale: 25-100 (very low resilience), 101-115 (low resilience), 116-130 (moderately low resilience), 131-144 (moderate resilience), 145-160 (moderately high resilience), 161-175 (high resilience) for self reliance, meaning, equanimity, perseverance and existential aloneness. (Student t test between the first and second interview among females t = 1.63; p-value = 0.179, and among males t = -0.76; p-value = 0.487).
An analysis of the individual items that make up the Resilience Scale shows the only difference can be seen for Perseverance, that is to say a person’s continued effort to reach his or her personal or family goals in spite of obstacles. More specifically, a slight increase was seen in the second interview which was conducted after the rescue effort.
STATISTICAL ANALYSIS
No significant statistical differences was observed for the resilience before and after the rescue effort activity among females (t = 1.63; p-value = 0.179), and among males (t = -0.76; p-value = 0.487).
In contrast, the p-values computed for CISS before and after the rescue effort showed significant statistical differences both among females (t = 4.81; p-value = 0.009) and males (t = 10.06; p-value = 0.001).
Discussion and conclusions
The current study has addressed the issue of emergency from a medical standpoint, focusing in particular on the psychological well-being of emergency medical responders who are faced with the problems and tragedies experienced by the victims of a catastrophe such as an earthquake. This study shows medium/high levels of coping and resilience in participants and identifies a link between coping strategies and individual resilience. This is probably due to the fact that the training and preparation received outside of the emergency situation is adequate.
Training plays a part in minimizing factors that lead to the development of problems and enables responders to adapt to highly stressful logistical and emotional situations. Rescue workers are thus able to help people in need in an appropriate manner. In relation to coping and resilience, the medium/high levels can be explained by the fact that the people who participated in the study belong to responder teams who are prepared from a practical point of view, but who are also made aware of their emotional setup; without a doubt, training contributes to being better equipped to face situations with the right degree of involvement.
More specifically, the CISS scores show some differences among females and males, before and after the rescue effort, confirmed by paired Student t test. In particular, scores for “Avoidance” might depend on the fact that women feel the need to share their experiences and build a wider network of interpersonal relationships.
Concerning resilience, the basic correlation between the two scores, measured before and after the rescue effort, could be caused by a number of elements such as: theoretical and practical training; turn-over (from 4 to 8 days); ability of individuals and community to promote and build resilience up all-round; support and sharing between peers and through one’s organisation in support of the network provided by family and friends.
Even if not statically significant, a slight difference can be seen in the results of the Resilience Scale too, in particular between the first and second interviews relating to perseverance scores. This difference could depend on having processed the experience, reinforced by feelings of self-esteem. Results show that a majority of participants adopt mechanisms of self-preservation such as coping and resilience, which come to their aid and help them face emergency situations. In fact, it should be noted that trauma in volunteers is mainly due to their contact with victims who are in a state of shock; this intensifies when an emotional link with victims is present.
In this spirit, it appears essential to make sure that the training received by volunteers not be limited to organisational and emotional aspects, but be enriched by new types of knowledge which acknowledge our aging populations, and the likelihood of assisting people who are elderly, disabled or ill, and therefore depend on specific drug therapies or diets (diabetes, heart disease etc.) [31-36].
Training before a disaster is the first step towards guaranteeing survival, above all for the more vulnerable subgroups, allowing communities to prioritize disaster preparation. Training for emergency rescue workers and the development of support programmes for the community could provide important sources of assistance, especially as it becomes essential to change normal habits during evacuation and the post-disaster phase [37]. Everything contributes to avoid harmful lifestyle choices (change of diet, alcohol consumption, smoking etc.) which effect the individual’s health [38-43].
Acknowledgements
Funding sources: this research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Participant consent
The completion of questionnaires was absolutely anonymous and voluntary. All participants provided written informed consent.
Conflict of interest statement
None declared.
Authors’ contributions
SS conducted the statistical data analyses and wrote the manuscript. NTTC contributed to the study design and interpretation of results, PF participated in designing the study protocol and wrote the manuscript. GI designed the study, built the questionnaire, and made the critical review of the manuscript. All authors gave substantial contribution to manuscript revising and editing.
References
- [1].WHO/HPR/HEP/98.1. Health Promotion Glossary. 1998. http://www.who.int/healthpromotion/about/HPR%20Glossary%201998.pdf
- [2].Siracusa M, Grappasonni I, Petrelli F. The pharmaceutical care and the rejected constitutional reform: what might have been and what is. Acta Biomed 2017;88(3):352-9. doi: 10.23750/abm.v88i3.6376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Signorelli C, Odone A, Gozzini A, Petrelli F, Tirani M, Zangrandi A, Zoni R, Florindo N. The missed Constitutional Reform and its possible impact on the sustainability of the Italian National Health Service. Acta Biomed 2017;88(1):91-4. doi: 10.23750/abm.v88i1.6408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Petrelli F, Contratti CM, Tanzi E, Grappasonni I. Vaccine hesitancy, a public health problem. Ann Ig 2018;30(2):86-103. doi: 10.7416/ai.2018.2200. [DOI] [PubMed] [Google Scholar]
- [5].American Psychiatric Association. Diagnostic Criteria from DSMIV-TR. Washington, DC: 2000. [Google Scholar]
- [6].Pearlman LA, Mac Ian PS. Vicarious traumatization: an empirical study of the effects of trauma work on trauma therapists. Professional Psychology Research and Practice 1995;26:558-65. [Google Scholar]
- [7].Noda Y, Asano K, Shimizu E, Hirano Y. Assessing subgroup differences in posttraumatic stress disorder among rescue workers in Japan with the impact of event scale-revised. Disaster Med Public Health Prep 2018:1-10. doi:10.1017/dmp.2018.62. [DOI] [PubMed] [Google Scholar]
- [8].Kim Y, Patel N, Diehl G, Richard P. The association between service members’ participation in humanitarian aid and disaster relief and mental health symptoms and treatments. Mil Med 2017;182(9):e1849-e55. doi:10.7205/MILMED-D-17-00023. [DOI] [PubMed] [Google Scholar]
- [9].Grappasonni I, Petrelli F, Traini E, Grifantini G, Mari M, Signorelli C. Psychological symptoms and quality of life among the population of L’Aquila’s “new towns” after the 2009 earthquake. Epidem Biostat Pub Health 2017;14(2):e11690-1-13. doi: 10.2427/11690. [Google Scholar]
- [10].Priebe S, Grappasonni I, Mari M, Dewey M, Petrelli F, Costa A. Posttraumatic stress disorder six months after an earthquake: findings from a community sample in a rural region in Italy. Soc Psychiatry Psychiatr Epidemiol 2009;44(5):393-7. doi: 10.1007/s00127-008-0441-y. [DOI] [PubMed] [Google Scholar]
- [11].Leffler CT, Dembert M. Posttraumatic Stress Symptoms among U.S. Navy Divers Recovering TWA Flight 800. J Nerv Ment Dis 1998;186:574-7. [DOI] [PubMed] [Google Scholar]
- [12].Martarelli D, Cocchioni M, Scuri S, Spataro A, Pompei P. Cold exposure increases exercise-induced oxidative stress. J Sports Med Phys Fitness 2011;51(2):299-304. [PubMed] [Google Scholar]
- [13].Kamiyama K, Yamami N, Sato K, Aoyagi M, Kyoya M, Mizuno E, Uemura M, Kawamoto Y, Okuda M, Togawa S, Shibayama M, Hosaka T, Mano Y. Effetcs of a structured stress management program on psychological and physiological indicators among marine hazard rescues. J Occup Health 2004;46:497-99. [DOI] [PubMed] [Google Scholar]
- [14].Grappasonni I, Petrelli F, Amenta F. Deaths on board ships assisted by the Centro Internazionale Radio Medico in the last 25 years. Travel Med Infect Dis 2012;10(4):186-91. doi: 10.1016/j.tmaid.2012.06.006. [DOI] [PubMed] [Google Scholar]
- [15].Giannantonio M, Cusano M. Lo stress post-traumatico nel personale di soccorso. IV° Forum Internazionale sull’EBN (Evidence Based Nursing). L’assistenza infermieristica basata sull’evidenza. Promuovere l’eccellenza nelle scienze infermieristiche 2003. [Google Scholar]
- [16].Tsuno K, Oshima K, Kubota K, Kawakami N. Personal resilience and post-traumatic stress symptoms of local government employees: six months after the 2011 magnitude 9.0 East Japan Earthquake. Sangyo Eiseigaku Zasshi 2014;56(6):245-58. doi: 10.1539/sangyoeisei.B14006. [DOI] [PubMed] [Google Scholar]
- [17].Yasien S, Abdul Nasir J, Shaheen T. Relationship between psychological distress and resilience in rescue workers. Saudi Med J 2016;37(7):778-82. doi: 10.15537/smj.2016.7.15004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Pedersen MJ, Gjerland A, Rund BR, Ekeberg Ø, Skogstad L. Emergency preparedness and role clarity among rescue workers during the terror attacks in Norway July 22, 2011. PLoS One 2016;11(6):e0156536. doi: 10.1371/journal.pone.0156536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Vippiani M. Il disturbo post traumatico da stress (PTSD): rischio per vittime e soccorritori. 112 Emergencies pp. 20-24. [Google Scholar]
- [20].Perry RW, Lindell MK. Preparedness for emergency response: guidelines for the emergency planning process. Disasters 2003;27(4):336-50. [DOI] [PubMed] [Google Scholar]
- [21].Schulberg HC, Block MR, Madonia MJ, Scott CP, Rodriguez E, Imber SD, Perel J, Lave J, Houck PR, Coulehan JL. Treating major depression in primary care practice. Eight-month clinical outcomes. Arch Gen Psychiatry 1996;53(10):913-9. [DOI] [PubMed] [Google Scholar]
- [22].Grappasonni I, Petrelli F, Scuri S, Mahdi SS, Sibilio F, Amenta F. Knowledge and attitudes on food hygiene among food services staff on board ships. Ann Ig 2018;30(2):162-72. doi: 10.7416/ai.2018.2207. [DOI] [PubMed] [Google Scholar]
- [23].Grappasonni I, Petrelli F, Klusoňová H, Kračmarová L. Level of understanding of medical terms among italian students. Ceska Slov Farm Winter 2016;65(6):216-20. [PubMed] [Google Scholar]
- [24].Spacilova L, Klusonova H, Petrelli F, Signorelli C, Visnovsky P, Grappasonni I. Substance use and knowledge among Italian high school students. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2009;153(2):163-8. [DOI] [PubMed] [Google Scholar]
- [25].Pedersen MJ, Gjerland A, Rund BR, Ekeberg Ø, Skogstad L. Emergency preparedness and role clarity among rescue workers during the terror attacks in Norway July 22, 2011. PLoS One 2016;11(6):e0156536 doi:10.1371/journal.pone.0156536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Berger W, Coutinho ES, Figueira I, Marques-Portella C, Luz MP, Neylan TC, Marmar CR, Mendlowicz MV. Rescuers at risk: a systematic review and meta-regression analysis of the worldwide current prevalence and correlates of PTSD in rescue workers. Soc Psychiatry Psychiatr Epidemiol 2012;47(6):1001-11. doi: 10.1007/s00127-011-0408-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Sirigatti S, Stefanile C. Coping Inventory for Stressful situation (CISS). Italian standardization Giunti O.S. 2009. [Google Scholar]
- [28]. https://www.futureacademy.org.uk/files/menu_items/other/6_icc_2899_4134_fullText_0_5693.pdf.
- [29]. https://www.dovepress.com/reliability-and--validity-of-the-italian-version-of-the-14-item-resili-peer-reviewed-fulltext-article-PRBM.
- [30].XLSTAT. Statistical software & data analysis add-on for Excel. Addinsoft (2017). [Google Scholar]
- [31].Mignini F, Sabbatini M, Pascucci C, Petrelli F, Grappasonni I, Vanacore N. Pharmaco-epidemiological description of the population of the Marche Region (central Italy) treated with the antipsychotic drug olanzapine. Ann Ist Super Sanita 2013;49(1):42-9. doi: 10.4415/ANN_13_01_08. [DOI] [PubMed] [Google Scholar]
- [32].Cioffi P, Laudadio L, Nuzzo A, Belfiglio M, Petrelli F, Grappasonni I. Gemcitabine-induced posterior reversible encephalopathy syndrome: a case report. J Oncol Pharm Pract 2012;18(2):299-302. doi: 10.1177/1078155211424628. [DOI] [PubMed] [Google Scholar]
- [33].Grappasonni I, Marconi D, Mazzucchi F, Petrelli F, Scuri S, Amenta F. Survey on food hygiene knowledge on board ships. Int Marit Health 2013;64(3):160-7. [PubMed] [Google Scholar]
- [34].Personal Preparedness for Older Adults and Their Caregivers. Disaster planning tips for older adults and their families. CDC website. http://www.cdc.gov/aging/emergency/preparedness.htm. Last updated March 17, 2015. Accessed June 21, 2016.
- [35].Grappasonni I, Scuri S, Tanzi E, Kracmarova L, Petrelli F. The economic crisis and lifestyle changes: a survey on frequency of use of medications and of preventive and specialistic medical care, in the Marche Region (Italy). Acta Biomed 2018;89(1):87-92. doi: 10.23750/abm.v89i1.7068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Scuri S, Tesauro M, Petrelli F, Peroni A, Kracmarova L, Grappasonni I. Implications of modified food choices and food-related lifestyles following the economic crisis in the Marche Region of Italy. Ann Ig 2018;30(2):173-9. doi: 10.7416/ai.2018.2208. [DOI] [PubMed] [Google Scholar]
- [37].Wakui T, Agree EM, Saito T, Kai I. Disaster preparedness among older japanese adults with long-term care needs and their family caregivers. Disaster Med Public Health Prep 2017;11(1):31-8. doi:10.1017/dmp.2016.53. [DOI] [PubMed] [Google Scholar]
- [38].Siracusa M, Petrelli F. Trade of food supplement: food or drug supplement? Recenti Prog Med 2016;107(9):465-71. doi: 10.1701/2354.25224. [DOI] [PubMed] [Google Scholar]
- [39].Petrelli F, Grappasonni I, Peroni A, Kracmarova L, Scuri S. Survey about the potential effects of economic downturn on alcohol consumption, smoking and quality of life in a sample of Central Italy population. Acta Biomed 2018;89(1):93-8. doi: 10.23750/abm.v89i1.7059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Yabe H, Suzuki Y, Mashiko H, Nakayama Y, Hisata M, Niwa S, Yasumura S, Yamashita S, Kamiya K, Abe M, Mental Health Group of the Fukushima Health Management Survey Psychological distress after the great East Japan earthquake and Fukushima Daiichi nuclear power plant accident: results of a mental health and lifestyle survey through the Fukushima Health Management Survey in FY2011 and FY2012. Fukushima J Med Sci 2014;60(1):57-67. [DOI] [PubMed] [Google Scholar]
- [41].Kračmarová L, Klusočová H, Petrelli F, Grappasonni I. Tobacco, alcohol and illegal substances: experiences and attitudes among Italian university students. Rev Assoc Med Bras (1992). 2011;57(5):523-8. [DOI] [PubMed] [Google Scholar]
- [42].Scuri S, Petrelli F, Tesauro M, Carrozzo F, Kracmarova L, Grappasonni I. Energy drink consumption: a survey in high school students and associated psychological effects. J Prev Med Hyg 2018;59(1):E75-9. doi: 10.15167/2421-4248/jpmh2018.59.1.898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Petrelli F, Grappasonni I, Evangelista D, Pompei P, Broglia G, Cioffi P, Kracmarova L, Scuri S. Mental and physical effects of energy drinks consumption in an Italian young people group: a pilot study. J Prev Med Hyg 2018;59(1):E80-7. doi: 10.15167/2421-4248/jpmh2018.59.1.900. [DOI] [PMC free article] [PubMed] [Google Scholar]