

Abstract
Breast undergoes hormonal changes, especially during pregnancy and postpartum period and may be associated with benign and malignant lesions. These lesions can arise either de novo or can be an exacerbated change occurring in a preexisting breast lesion. The benign lesion in the lactating breast can show some degree of atypia due to the high levels of progesterone and prolactin which can mimic malignant features microscopically and can be overdiagnosed with breast cancer. On the other hand, breast cancer in the lactating breast can be underdiagnosed when the atypical cytological features are considered as hormonal changes. A few case reports are published in the literature regarding lactating adenoma undergoing malignant transformation. We present a case in 23 years postpartum lactating female with mass in bilateral breasts. Initially, the lesions were diagnosed with hormonal changes on cytology. On follow-up by fine-needle aspiration cytology and biopsy, it was diagnosed with infiltrating ductal carcinoma in both breasts. As far as our knowledge goes, this is the first-case report in the English literature of ductal carcinoma in the bilateral lactating breast arising de novo.
Keywords: Breast cancer, fine-needle aspiration cytology of breast, lactating breast
Introduction
Breast undergoes changes due to estrogen and progesterone, especially during menarche, pregnancy, lactation, and postpartum periods. Lactation changes in the breast are common in women during pregnancy and lactation period due to an increase in serum levels of estrogen, progesterone, and prolactin. The benign or malignant lesions in the lactating breast can arise either de novo or can be an exacerbated change in a preexisting breast lesion.[1,2] Lactational adenoma and breast carcinoma in lactation adenoma are reported.[3,4] However, bilateral breast carcinoma in the lactating breast arising de novo is very rare.
Diagnosis of breast lump in the lactating breast is a challenge, especially by fine-needle aspiration cytology (FNAC) as the changes in ductal epithelial cells often mimics malignancy. On the other hand, the cytological diagnosis of breast carcinoma can be delayed considering the cellular changes is due to hormonal change.[5]
Case Report
A 23-year lactating woman presented with painful mass in both breasts and the left axilla for 8 months. The left breast examination revealed a diffuse and mobile mass in the upper inner quadrant measuring 3 cm × 2 cm. The skin over the lump was normal, and the lump was not fixed either to the skin or the chest wall. On examination of the left axilla, a mobile mass was palpated which was firm in consistency and measured 3 cm × 3 cm. On examination of the right breast, an ill-defined mobile and firm lump was noticed in the upper inner quadrant measuring 6 cm × 5 cm. The skin over the lump was normal, and the lump was not fixed either to the skin or the chest wall. No palpable lymph nodes were found in the right axilla.
Ultrasound of the left breast revealed two well-circumscribed oval-shaped hypoechoic lesions measuring 4.1 cm × 2 cm and 2.4 cm × 2 cm in the upper inner quadrant and in the axillary tail region, respectively. BI-RADS III was considered, and a diagnosis of fibroadenoma was offered. Ultrasound of the right breast revealed a heterogeneous hypoechoic ill-defined area in the subareolar region measuring 3.5 cm × 3 cm. BI-RADS II was considered, and differential diagnosis of inflammatory phlegmon and early evolving abscess were offered.
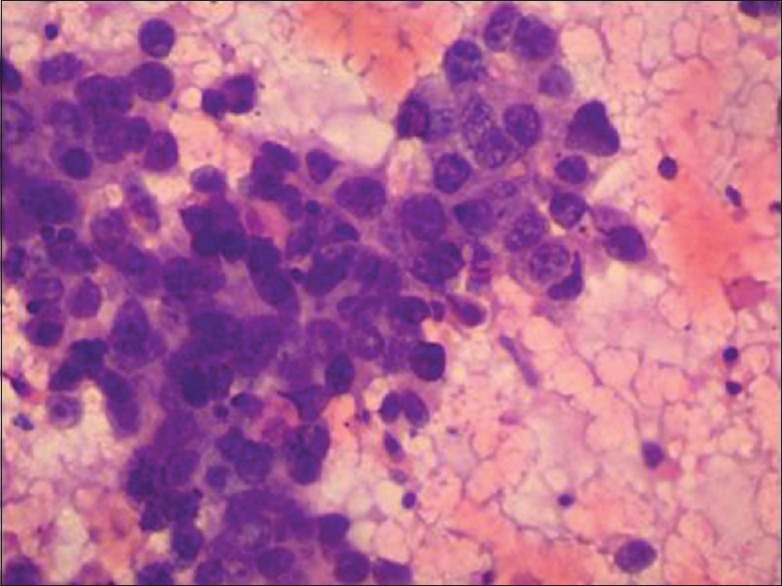
Smears studied from FNAC of the left breast mass was highly cellular consisting of ductal epithelial cell having vesicular nucleus, increased nuclear-cytoplasmic ratio, finely granular chromatin with prominent nucleoli, and moderate to abundant amount of pale eosinophilic/vacuolated fragile cytoplasm having ill-defined borders. These cells were arranged in loose cohesive clusters, in singles, and some in glandular pattern. Background showed bare nuclei, erythrocytes, and lipid droplets [Figure 1]. Smears studied from aspirate of the right breast mass and left axillary lump also showed similar features. A cytological diagnosis of a benign lesion with hormonal changes due to lactation was considered. The patient was followed up.
Figure 1.

Microphotograph of fine-needle aspiration cytology from the left breast lump showing ductal epithelial cells with increased N:C ratio and prominent nucleoli (H and E, ×400)
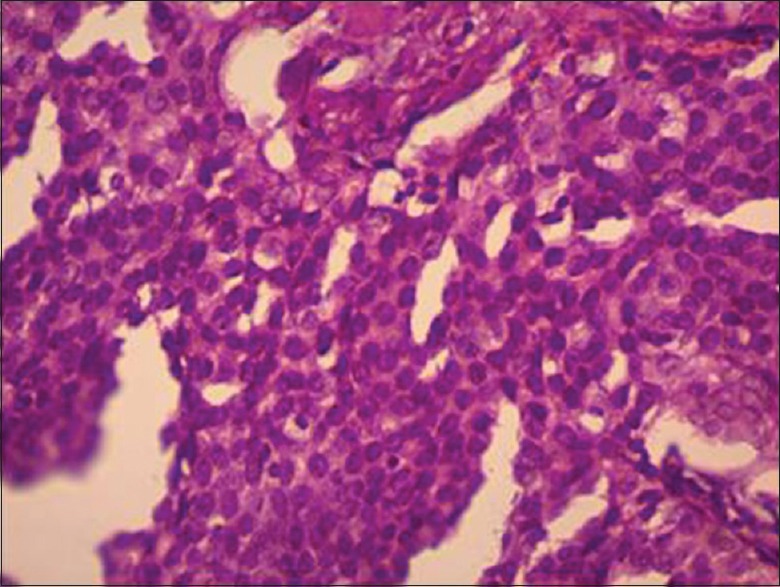
After 7 months, the patient presented with an increase in the size of all the three mass of both the breasts. A repeat FNAC of the left breast lump revealed highly cellular smears composed of highly pleomorphic cells arranged in loose cohesive clusters, sheets, and ductal pattern with irregular nuclear membrane, prominent nucleoli, and moderate amount of cytoplasm. The background showed stripped tumor nuclei and hemorrhage [Figure 2]. Smears studied from the left axillary lymph node showed similar cells with lymphocytes in the background. The features were consistent with ductal carcinoma of the left breast with ipsilateral axillary lymph node deposits. A repeat FNAC of the right breast lump showed cellular smear consisting of ductal epithelial cell having vesicular nucleus, fine granular chromatin with prominent nucleoli, and moderate amount of pale eosinophilic/vacuolated fragile cytoplasm. These cells were arranged in cohesive clusters and in the glandular pattern. Focal areas showed the ductal epithelial cells with the increased nuclear and cytoplasmic ratio, irregular nuclear border, and coarse irregularly distributed chromatin. The background showed bare nuclei and erythrocytes cytological feature of lactational changes with a few ductal epithelial cells showing atypical features was offered.
Figure 2.
Microphotograph of repeat fine-needle aspiration cytology from the left breast lump showing pleomorphic cells with prominent nucleoli and atypia (H and E, ×400)
The patient was referred to the nearest cancer institute where the patient underwent left modified radical mastectomy with axillary clearance. Grossly, the specimen measured 15 cm × 12 cm × 5 cm. Skin and nipple appeared normal. Cut section showed gray-white tumor in the upper and inner quadrant, measuring 5.2 cm × 4 cm. The resected margins were free from the tumor. Twelve lymph nodes were retrieved from the axillary clearance. Microscopy showed highly pleomorphic ductal epithelial cells having hyperchromatic nucleus, irregular nuclear border, many with prominent nucleoli, and moderate amount of eosinophilic cytoplasm. These cells were arranged in sheets and in ductular pattern with features of infiltration into dense fibro-collagenous tissue [Figure 3]. Lymphovascular invasion was noted. Similar tumor cells were seen in four lymph nodes of axillary clearance. A diagnosis of infiltrating ductal carcinoma of the left breast with tumor deposits in axillary lymph nodes with T3N2Mx stage was offered. The tumor was negative for estrogen receptor, progesterone receptor, and HER2neu on immunohistochemistry. The patient was subjected to four cycles of chemotherapy. Meanwhile, the right breast mass had increased in size considerably with the presence of nipple retraction (Clinical stage T4bN1Mx). Mammography showed BIRADS IVB. Core-needle biopsy of the right breast showed ductal epithelial cells with marked nuclear pleomorphism, prominent nucleoli, and irregular nuclear margin with moderate amount of cytoplasm arranged in sheets and ductular pattern amidst dense fibro-collagenous tissue. Features were consistent with infiltrating ductal carcinoma.
Figure 3.
Microphotograph of the left breast mass showing ductal cells showing nuclear atypia and prominent nucleoli (H and E, ×400)
Discussion
Breast cancer is the most common cancer in females. The etiological factors are many which include hormones. Estrogen and progesterone have a role in the development and changes in the breast in different stages of life in females. The role of these hormones in carcinogenesis of the breast is well-documented. Recent studies have shown the association of prolactin in the development of malignancy in the lactating breast and also reported an increased number of receptors for prolactin in the ductal epithelial cells.[6] Excess prolactin was used in an experimental study to induce breast carcinoma in mice which showed the positive association between prolactin and breast cancer.[7] Breast cancer in preexisting lactational adenoma is reported[3,4] Probably, similar hormonal mechanism must be the cause of breast cancer in the present case without the evidence of preexisting lesion (arising de novo).
Cytological smears of the aspirates from the lactating breast are usually cellular and are composed of cells arranged in loose cohesive clusters or in singles. The cells are large and have abundant, fragile, and vacuolated/granular cytoplasm. The nuclei are centrally located, round, and larger than the normal ductular cells. The presence of distinct small nucleoli is often noted. Single bipolar nuclei are rarely seen. The characteristic finding in the lactating breast is the background which shows abundant milky secretion and numerous lipid droplets as vacuoles.[8,9] Similar features were observed in our case in the first FNAC of both the breast.
The cytological features of aspirates obtained from the lactating breast that are most often misinterpreted as an atypical or carcinomatous change are high cellularity, lack of cell cohesion, the absence of bimodal population of cells, lack of bipolar nuclei, and the presence of prominent nucleoli. The differential diagnoses which can be considered are alveolar variant of lobular carcinoma and secretory carcinoma. The clinical and radiological correlation is required to avoid a false-positive diagnosis of malignancy. However, the points favoring the benign nature of lactating breast tissue are the bland nuclear features and the lipid droplets in the background.[3,8,9] In the present case, the cells showed lactation changes along with atypia in the first aspirate for which the case was followed up closely to avoid the false negative diagnosis.
On the contrary, the apprehension of over-diagnosing a lactational change as carcinoma may lead to the false positive diagnosis. Therefore, a mass in a pregnant or lactating breast is a challenge on FNAC. Such cases warrant the need for clinical and radiological correlation to avoid under or overdiagnosis. Core-needle biopsy followed by histopathological diagnosis can be done in ambiguous lesions.[3,8,9]
In the present case, the diagnosis of breast cancer was delayed or masked by lactational changes. The cancer progressed rapidly in the later phase of the disease with the involvement of both breast and immunohistochemistry for hormonal markers showed triple negative. As far as our knowledge goes, this is the first-case report in the English literature of bilateral breast cancer in the lactating female arising de novo.
Conclusion
Lactational or hormonal changes are rarely associated with carcinomas. It may be difficult to distinguish between hormonal changes and ductal carcinoma on cytology. In cases where nuclear atypia is seen, the clinician should be cautioned and regular follow-up along with radiological investigation should be advised. FNAC diagnosis should be correlated with tru-cut biopsy findings and radiological studies to reach a consensus preoperatively. Ours is a unique case where patient presented with ductal carcinoma in both lactating breasts simultaneously. We have not found similar case report in the English literature.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Prasaad PR. Fine needle aspiration cytologic diagnosis of lactating adenoma: Report of two cases. J Clin Diagn Res. 2013;7:2417–8. doi: 10.7860/JCDR/2013/5260.3544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Faupel-Badger JM, Duggan MA, Sherman ME, Garcia-Closas M, Yang XR, Lissowska J, et al. Prolactin receptor expression and breast cancer: Relationships with tumor characteristics among pre- and post-menopausal women in a population-based case-control study from Poland. Horm Cancer. 2014;5:42–50. doi: 10.1007/s12672-013-0165-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khanna M, Manjari M, Khanna A. Lactating adenoma with infiltrating ductal carcinoma breast in a pregnant woman. Indian J Cancer. 2015;52:585–6. doi: 10.4103/0019-509X.178391. [DOI] [PubMed] [Google Scholar]
- 4.Hertel BF, Zaloudek C, Kempson RL. Breast adenomas. Cancer. 1976;37:2891–905. doi: 10.1002/1097-0142(197606)37:6<2891::aid-cncr2820370647>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 5.Geschicker CF, Lewis D. Pregnancy and lactational changes in fibroadenoma of breast. BMJ. 1938;1:499–503. doi: 10.1136/bmj.1.4026.499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yu JH, Kim MJ, Cho H, Liu HJ, Han SJ, Ahn TG, et al. Breast diseases during pregnancy and lactation. Obstet Gynecol Sci. 2013;56:143–59. doi: 10.5468/ogs.2013.56.3.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wennbo H, Gebre-Medhin M, Gritli-Linde A, Ohlsson C, Isaksson OG, Törnell J, et al. Activation of the prolactin receptor but not the growth hormone receptor is important for induction of mammary tumors in transgenic mice. J Clin Invest. 1997;100:2744–51. doi: 10.1172/JCI119820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Harendra Kumar ML, Narasimha A, Bhaskaran A, Divya MN. Concurrent lactating adenoma and infiltrating ductal carcinoma: A case report. J Clin Diag Res. 2015;9:14–5. doi: 10.7860/JCDR/2015/12786.6326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Saria MA, Mirza MR. Breast diseases presenting during pregnancy and lactation. J Surg Pak. 2010;15:147–50. [Google Scholar]