

Abstract
Gingival recession is defined as an apical displacement of soft tissues to the cementoenamel junction. Various treatment options for the management of gingival recessions include laterally positioned flap, double papillae flap, coronally advanced flap (CAF) with or without guided tissue regeneration, free gingival autografts, and autogenous subepithelial connective tissue grafts. Three patients with multiple adjacent gingival recessions in the upper jaw were treated utilizing amniotic membrane (Tata memorial) with CAF. The results of this procedure show that amniotic membrane can be used in the treatment of gingival recession defects with significant root coverage and to increase the thickness of keratinized gingiva. There was an increase in height and thickness of keratinized gingiva from 3 to 3.5 mm and 1.5 to 2 mm, respectively. The present results suggest that the combined approach of CAF and amniotic membrane can be considered as a treatment option for multiple adjacent gingival recessions.
Keywords: Coronally advanced flap, gingival recession, guided tissue regeneration
Introduction
Gingival recession is defined as an apical displacement of soft tissues to the cementoenamel junction (CEJ).[1] The various treatment options for the management of gingival recessions include laterally positioned flap, double papillae flap, coronally advanced flap (CAF) with or without guided tissue regeneration (GTR), free gingival autografts, and autogenous subepithelial connective tissue grafts (CTGs).[1] CAF was introduced for the treatment of Miller's Class I gingival recession. To enhance the periodontal regeneration GTR-based membranes, growth factors, and enamel matrix proteins were used as an adjunct to CAF.[2]
A variety of nonresorbable and resorbable membranes was used for the treatment of gingival recession. GTR-based techniques resulted in similar clinical outcome to other root coverage procedures and resulted in new attachment formation.[3] Resorbable membranes including collagen and synthetic membranes were preferred to nonresorbable membranes to avoid second surgical procedure for the removal of nonresorbable membranes.[4] Collagen membranes have inherent space maintaining potential and augments the width and thickness of keratinized gingiva. Collagen membranes were harvested from tendon, dermis, placental amnion, and chorion.
The amniotic membrane used in various fields in medicine including eye surgery, burns, gynecologic surgery, orthopedics, and temporary biologic dressings for full thickness wounds, to decrease postoperative pain, reconstruction of damaged or malformed organs, and prevention of tissue adhesion.[5] Recently, the efficacy of amniotic membrane was evaluated along with CAF for root coverage. Human amniotic membrane is the innermost layer of the placenta and lines the amniotic cavity. It is composed of a single layer of epithelial cells, a basement membrane, and an avascular connective tissue matrix. The basement membrane contains collagen Types III, IV, V, and cell-adhesion bioactive factors including glycoproteins, fibronectin, and laminins (laminin-5 plays a role in the cell adhesion of gingival cells). It also contains stem cells and growth factors such as epidermal growth factor, transforming growth factor beta, fibroblast growth factor, and platelet-derived growth factor aid in the formation of granulation tissue and neovascularization. The amnion has ability to form early physiologic “seal” with the host tissue and decrease the host immunologic response through mechanisms such as localized suppression of polymorphonuclear cell migration.[6]
The present case reports utilized amniotic membrane (Tata memorial) with CAF for the treatment of adjacent multiple gingival recessions.
Case Reports
Case 1
A 35-year-old male patient presented to the Department of Periodontics, Sri Sai College of Dental Surgery, Vikarabad, Telangana, India, with a chief complaint of sensitivity and receding gums since 3 years. The case was diagnosed as Miller's Class I gingival recession in 11, 21 Class III in 22 and 23 [Figure 1a]. The patient was explained the treatment options for root coverage and signed informed consent was obtained from patient. The patient was posted for root coverage procedure 4 weeks after cause-related treatment including scaling and root planning. CAF with amnion membrane was the treatment option considered as there are multiple recession defects, with a combination of soft tissue and bone loss and the patient was not willing for subepithelial CTG, which needs a second surgical site.
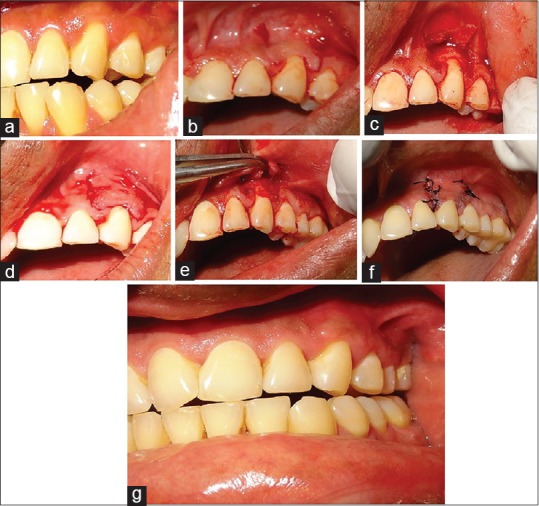
Figure 1.

(a) Miller's Class I gingival recession in 11, 21 and Class III in 22, 23. (b and c) Operative view showing two beveled oblique vertical releasing incisions online angle of distal teeth without involving the adjacent papilla extending into the alveolar mucosa. (d and e) Amnion Membrane and Placement. (f) Placement of interrupted sutures to close the vertical incisions and sling sutures at the interdental papillae with 5-0 mersilk. (g) Superficial releasing incision to release the lip pull. (h) One-year postoperative view showing near complete root coverage in relation to 11, 21 and partial root coverage in relation to 22 and 23 in case 1
Case 2
A 39-year-old male patient of presented to the Department of Periodontics, Sri Sai College of Dental Surgery, Vikarabad, Telangana, India, with a chief complaint of sensitivity and receding gums since 2 years. The case was diagnosed as Miller's Class I gingival recession in 23 [Figure 2a]. Patients were explained the treatment options for root coverage and signed informed consent was obtained from the patient. The patient was posted for root coverage procedure 4 weeks after cause-related treatment including scaling and root planning [Figure 2b-2f]. CAF with amnion membrane was the treatment option considered, and the patient was not willing for subepithelial CTG, which needs a second surgical site.
Figure 2.
(a) Photograph showing Miller's Class I gingival recession in 23. (b-d) Operative view showing two beveled vertical releasing incisions on line angle of distal teeth without involving the adjacent papilla extending into the alveolar mucosa. (e) Placement of amnion membrane the root surface. (f) Placement of interrupted sutures to close the vertical incisions. (g) One-year postoperative view showing near complete root coverage in relation to 23 in case 2
Case 3
A 37-year-old male patient presented to the Department of Periodontics, Sri Sai College of Dental Surgery, Vikarabad, Telangana, India, with a chief complaint of sensitivity and receding gums since 2 years. The case was diagnosed as Miller's Class I gingival recession in 21, Class II in 22 and 23 [Figure 3a]. The patient was explained the treatment options for root coverage and signed informed consent was obtained from the patient. The patient was posted for root coverage procedure 4 weeks after cause-related treatment including scaling and root planning. As the patient was not willing for subepithelial CTG, which needs a second surgical site CAF with amnion membrane was the treatment option considered as there are multiple recession defects.
Figure 3.
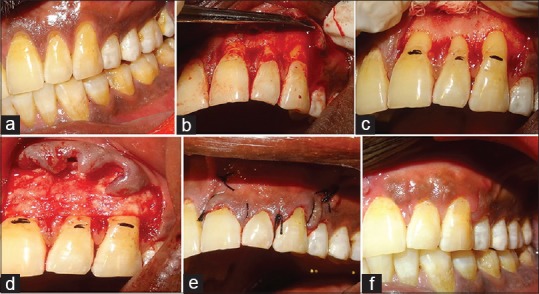
(a) Photograph showing Miller's Class I gingival recession in 21, Class II in 22 and 23. (b and c) Operative view showing two beveled oblique vertical releasing incisions on line angle of distal teeth without involving the adjacent papilla extending into the alveolar mucosa. (d) Placement of amnion membrane the root surface. (e) Placement of interrupted sutures to close the vertical incisions on line angle of distal teeth without involving the adjacent papilla extending into the alveolar mucosa. (f) One-year postoperative view showing near complete root coverage in relation to 21, 22, 23 in case 3
Manufacturing criteria for amniotic membrane
Donor screening
Amniotic membranes are retrieved postdelivery; consent is obtained and screened for infectious diseases and diseases of unknown origin. Donor blood samples are tested for Hepatitis B surface antigen, Hepatitis C antibodies, syphilis, and HIV 1 and 2 antibodies. To eliminate the risk inherent in the serodiagnostic window for HIV, all donated tissues are processed.[7]
Processing
The amnion is cleaned of blood, pasteurized at 60°C in saline, treated with 70% alcohol, washed, lyophilized using a dose of 25 kGy.
Clinical procedure
After the administration of local anesthesia (2% xylocaine with 1:80,000 epinephrine) thickness of keratinized gingiva apical to the recession was measured with a reamer with stopper. The width of keratinized tissue was 3 mm and thickness was 1.5 mm. Split-thickness horizontal incisions were performed at the interdental papillae of teeth with the recession. Two beveled oblique vertical releasing incisions extending into the alveolar mucosa were given online angle of distal teeth without involving the adjacent papilla [Figures 1b and c, 2d, 3b and c]. The flap was elevated with split-full-split approach in the coronal-apical direction [Figure 1c]. Split-thickness reflection was performed at interdental papilla and 3–4 mm apical to the base of the recession defect to facilitate coronal advancing of the flap. The facial interdental papilla coronal to the horizontal incisions was de-epithelized to create vascular beds for the surgical papilla of CAF. Root surface was instrumented with curettes; root conditioning [Figure 1c] was done along with decortication of the bone surface to increase vascularization to the surgical area. The amnion membrane [Figures 1e, 2e, and 3d] was placed over the root surface and adjacent bone and it self-adhered to the underlying surfaces, eliminating the need for sutures to the membrane. The reflected flap was coronally advanced and positioned 1 mm coronal to the CEJ to compensate the postoperative soft-tissue shrinkage and interrupted sutures were given to close the vertical incisions and sling sutures at the interdental papillae with 5-0 mersilk sutures [Figures 1f, 2f and 3e]. The superficial releasing incision was given to release the lip pull on the gingiva as this incision maintains adequate blood supply [Figure 1g]. The patient was evaluated and the Coe-pack was placed over the treated area.
Postsurgical care
Analgesics (Ibuprofen 400 mg) and antibiotics (Amoxicillin 500 mg thrice a day) were given for 5 days. 0.12% chlorhexidine mouthwash and postoperative instructions were given. Suture removal was done at 1 week after evaluation. No postoperative adverse effects were observed. The patient recalled at 3 weeks, 1 month, and 6-month period intervals.
Near complete root coverage in relation to 11, 21 and partial root coverage in relation to 22 and 23 [Figure 1h] was achieved in case 1, Near complete root coverage in relation to 23 was achieved in case 2 [Figure 2g], Near complete root coverage in relation to 21, 22, 23 was achieved in case 3 [Figure 3f]. As root coverage procedures are aimed only to achieve full coverage in Miller's Class I recession defects. There was an increase in height and thickness of keratinized gingiva from 3 to 3.5 mm and 1.5 to 2 mm, respectively.
Discussion
The results of this procedure show that amniotic membrane can be used in the treatment of gingival recession defects with significant root coverage and to increase the thickness of keratinized gingiva. Amniotic membrane closely mimics the basement membrane of human mucosa, and it contains laminin-5, plays a role in the cellular adhesion of gingival cells.[5]
It has several clinical advantages, such as excellent handling properties, reduction in operatory time as it does not require second surgical site, availability of unlimited barrier material with uniform thickness and postoperative maintenance.
Although healing by long junctional epithelium was an effective barrier for local inflammatory processes, the recreation of natural attachment apparatus by GTR-based root coverage provide better long-term stability.[8] The previous histologic evaluation of tooth treated with a polymer-based bioabsorbable membrane extracted 6 months' postoperatively found significant connective tissue attachment, new bone formation, and cementum regeneration.[9]
According to a systematic review, there was no significant difference between the CTG and GTR groups in studies followed up for <12 months, although the CTG data implied a slightly larger weighted mean difference in recession depth reduction.[10]
A meta-analysis of GTR-based root coverage showed that both conventional mucogingival surgery and GTR could produce similar clinical attachment gains.[3]
Conclusion
The present results suggest that the combined approach of CAF and amniotic membrane can be considered as a treatment option for multiple adjacent gingival recessions.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Pradeep K, Rajababu P, Satyanarayana D, Sagar V. Gingival recession: Review and strategies in treatment of recession. Case Rep Dent. 2012;2012:563421. doi: 10.1155/2012/563421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cairo F, Pagliaro U, Nieri M. Treatment of gingival recession with coronally advanced flap procedures: A systematic review. J Clin Periodontol. 2008;35:136–62. doi: 10.1111/j.1600-051X.2008.01267.x. [DOI] [PubMed] [Google Scholar]
- 3.Al-Hamdan K, Eber R, Sarment D, Kowalski C, Wang HL. Guided tissue regeneration-based root coverage: Meta-analysis. J Periodontol. 2003;74:1520–33. doi: 10.1902/jop.2003.74.10.1520. [DOI] [PubMed] [Google Scholar]
- 4.Kimble KM, Eber RM, Soehren S, Shyr Y, Wang HL. Treatment of gingival recession using a collagen membrane with or without the use of demineralized freeze-dried bone allograft for space maintenance. J Periodontol. 2004;75:210–20. doi: 10.1902/jop.2004.75.2.210. [DOI] [PubMed] [Google Scholar]
- 5.Niknejad H, Peirovi H, Jorjani M, Ahmadiani A, Ghanavi J, Seifalian AM, et al. Properties of the amniotic membrane for potential use in tissue engineering. Eur Cell Mater. 2008;15:88–99. doi: 10.22203/ecm.v015a07. [DOI] [PubMed] [Google Scholar]
- 6.Robson MC, Krizek TJ. The effect of human amniotic membranes on the bacteria population of infected rat burns. Ann Surg. 1973;177:144–9. doi: 10.1097/00000658-197302000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kothiwale SV, Anuroopa P, Gajiwala AL. A clinical and radiological evaluation of DFDBA with amniotic membrane versus bovine derived xenograft with amniotic membrane in human periodontal grade II furcation defects. Cell Tissue Bank. 2009;10:317–26. doi: 10.1007/s10561-009-9126-3. [DOI] [PubMed] [Google Scholar]
- 8.Wang HL, Modarressi M, Fu JH. Utilizing collagen membranes for guided tissue regeneration-based root coverage. Periodontol 2000. 2012;59:140–57. doi: 10.1111/j.1600-0757.2011.00438.x. [DOI] [PubMed] [Google Scholar]
- 9.Windisch P, Sculean A, Klein F, Tóth V, Gera I, Reich E, et al. Comparison of clinical, radiographic, and histometric measurements following treatment with guided tissue regeneration or enamel matrix proteins in human periodontal defects. J Periodontol. 2002;73:409–17. doi: 10.1902/jop.2002.73.4.409. [DOI] [PubMed] [Google Scholar]
- 10.Ko HY, Lu HK. Systematic review of the clinical performance of connective tissue graft and guided tissue regeneration in the treatment in the treatment of gingival recessions of Miller's classification grades I and II. J Exp Clin Med. 2010;2:63–71. [Google Scholar]