

Abstract
Hypertension, the leading risk factor for cardiovascular disease, originates from combined genetic, environmental, and social determinants. Environmental factors include overweight/obesity, unhealthy diet, excessive dietary sodium, inadequate dietary potassium, insufficient physical activity, and consumption of alcohol. Prevention and control of hypertension can be achieved through targeted and/or population-based strategies. For control of hypertension, the targeted strategy involves interventions to increase awareness, treatment, and control in individuals. Corresponding population-based strategies involve interventions designed to achieve a small reduction in blood pressure (BP) in the entire population. Having a usual source of care, optimizing adherence, and minimizing therapeutic inertia are associated with higher rates of BP control. The Chronic Care Model, a collaborative partnership among the patient, provider, and health system, incorporates a multilevel approach for control of hypertension. Optimizing the prevention, recognition, and care of hypertension requires a paradigm shift to team-based care and the use of strategies known to control BP.
Keywords: antihypertensive agents, dietary sodium, exercise, medication adherence, lifestyle, telemedicine
CONDENSED ABSTRACT:
Hypertension is the world’s leading risk factor for cardiovascular disease and originates from a combination of genetic, environmental, and social determinants. Prevention and control of hypertension can be achieved by application of targeted and/or population-based strategies. The Chronic Care Model, a collaborative partnership among the patient, provider, and health system, incorporates a multilevel approach to the control of hypertension. Optimizing prevention, recognition and care of high blood pressure will require a paradigm shift to team-based care and use of strategies known to control blood pressure.
INTRODUCTION
High blood pressure (BP) is the leading risk factor for cardiovascular disease (CVD), and hypertension ranks first as a cause of disability-adjusted life years worldwide (1,2). Suboptimal BP control is the most common attributable risk factor for CVD and cerebrovascular disease, including hemorrhagic (58%) and ischemic (50%) stroke, ischemic heart disease (55%), and other forms of CVD (58%), including heart failure and peripheral arterial disease (1,2). In addition, hypertension is a leading cause of chronic kidney disease, kidney disease progression, and end-stage kidney disease, as well as dementia due to cerebral small vessel disease (3–6).
Large-scale epidemiological studies have provided definitive evidence that high BP, at all ages and in both sexes, maintains a continuous graded association with the risk of fatal and nonfatal stroke, ischemic heart disease, heart failure, and noncardiac vascular disease, without heterogeneity due to ethnicity, down to a BP nadir of 115/75 mm Hg (7–9) Each 20-mm Hg increment of systolic blood pressure (SBP) or 10-mm Hg increment of diastolic blood pressure (DBP) is associated with a doubling of the risk of a fatal cardiovascular event (7).
The prevalence of hypertension globally is high and continues to increase (1,10). Defined at the SBP/DBP cutoff of >140/90 mm Hg, the worldwide prevalence of hypertension is 31%, translating to approximately 1.4 billion adults (1,10). The prevalence of hypertension in the adult U.S. population is similar to the worldwide prevalence at 31.9% (72.2 million people) using the >140/90 mm Hg BP cutoff; the U.S. prevalence is projected to increase to 45.6% (103.3 million people) using the 2017 American College of Cardiology/American Heart Association (ACC/AHA) hypertension clinical practice guideline definition of BP >130/80 mm Hg (10–12).
In this review, we first describe the current state of knowledge regarding pathophysiological determinants of high BP. We then describe strategies for, and barriers to, prevention and control of hypertension, and suggest multilevel and population health actions to improve BP control.
PATHOPHYSIOLOGICAL DETERMINANTS OF HIGH BP
Hypertension can be divided into primary and secondary forms. Primary (essential) hypertension accounts for the vast majority (>90%) of cases, and poor diet and insufficient physical activity seem to be important and potentially reversible environmental causes. A specific, sometimes remediable cause of hypertension can be identified in approximately 10% of adults with hypertension, termed secondary hypertension (Table 1) (11). If the cause can be accurately diagnosed and treated, patients with secondary hypertension can achieve normalization of BP or marked improvement in BP control, with concomitant reduction in CVD risk (11). The majority of patients with secondary hypertension have primary aldosteronism or renal parenchymal or renal vascular disease, whereas the remainder may have more unusual endocrine disorders or drug- or alcohol-induced hypertension.
Table 1.
Causes of Secondary HT
| Disorder | Major Clinical Findings | Prevalence* |
|---|---|---|
| Primary aldosteronism | RH; HT with hypokalemia; HT with muscle cramps or weakness; HT and incidentally discovered adrenal mass; HT and FH of early-onset HT or stroke | 8–20 |
| Renovascular disease | RH; HT with abrupt onset, worsening or increasingly difficult to control; flash pulmonary edema (ASCVD); early-onset HT, especially in women (FMH) | 5–34 |
| Renal parenchymal disease | UTIs; obstruction; hematuria; urinary frequency/nocturia; analgesic abuse; FH of polycystic kidney disease; increased serum creatinine; abnormal urinalysis | 1–2 |
| Drug- or alcohol-induced | Sodium-containing antacids; nicotine (smoking); alcohol; NSAIDs; OCs; cyclosporine or tacrolimus; sympathomimetic agents; cocaine, amphetamines, other illicit drugs; neuropsychiatric agents; EPO; clonidine withdrawal | 2–4 |
| Pheochromocytoma/paraganglioma | RH; paroxysmal HT or crisis superimposed on sustained HT; “spells,” BP lability; headache, sweating, palpitations, pallor; FH of pheochromocytoma/paraganglioma; incidentally discovered adrenal mass | 0.1–0.6 |
| Cushing’s syndrome | Rapid weight gain with central distribution; proximal muscle weakness; depression; hyperglycemia | <0.1 |
| Hypothyroidism | Dry skin, cold intolerance, constipation, hoarseness, weight gain | <1 |
| Hyperthyroidism | Warm, moist skin; heat intolerance; nervousness; tremulousness; insomnia; weight loss; diarrhea; proximal muscle weakness | <1 |
| Hypercalcemia and primary hyperparathyroidism | Hypercalcemia | Rare |
| Congenital adrenal hyperplasia (excess DOC) | HT and hypokalemia; virilization (Π-β-hydroxylase deficiency [Π-β-OH]) incomplete masculinization in men and primary amenorrhea in women (17-α-hydroxylase deficiency [17-α-OH]) | Rare |
| Other mineralocorticoid excess syndromes due to DOC | Early-onset HT; hypokalemia or hyperkalemia | Rare |
| Acromegaly | Acral features, enlarging shoe, glove, or hat size; headache, visual disturbances; diabetes mellitus | Rare |
| Coarctation of the aorta | Young patient with HT (<30 years of age) | 0.1 |
Estimated percent prevalence among adults with hypertension.
ASCVD = atherosclerotic cardiovascular disease; BP = blood pressure; DOC = deoxycorticosterone; FH = family history; EPO = erythropoietin-stimulating agents; FMH = fibromuscular hyperplasia; HT = hypertension; MAO = monoamine oxidase; NSAIDs = nonsteroidal anti-inflammatory drugs; OCs = oral contraceptives; OH = hydroxylase; RH = resistant hypertension; UTI = urinary tract infection.
Figure 1 depicts the major pathophysiological determinants of BP in primary hypertension. Primary hypertension originates from a combination of genetic and environmental factors. The heritability of BP is 30% to 50% (13–18), reflecting the degree of phenotypic resemblance among family kin, and depends both upon shared genetic background contributing to BP as well as environmental factors and their interactions with the genome.
Figure 1: Schematic Depiction of the Major Determinants of BP in Primary Hypertension and Their Interactions in Adults.
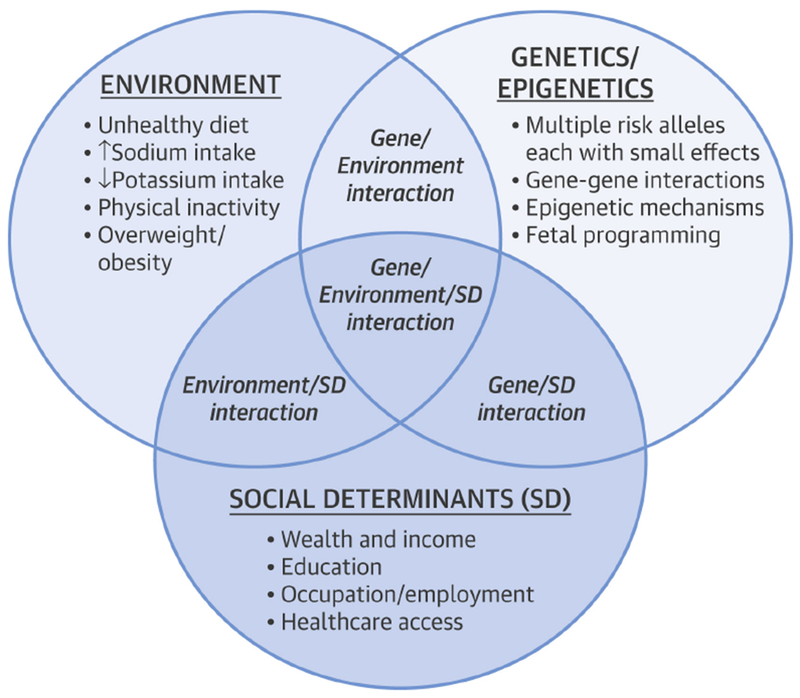
Genetic/epigenetic, environmental, and social determinants interact to increase BP in virtually all hypertensive individuals and populations. BP = blood pressure. SD = social determinants.
GENETIC AND EPIGENETIC PREDISPOSITION
Hypertension is a complex polygenic disorder in which many genes and/or combinations of genes influence BP (19,20). Although several monogenic forms of hypertension have been identified, such as glucocorticoid-remediable aldosteronism, Liddle’s and Gordon’s syndromes, and others, in which single-gene mutations completely explain the pathophysiology of the hypertension, these disorders are rare (21). Common genetic variants influencing BP have been identified at over 300 independent genetic loci. However, these genetic variants typically have effects on the order of only 1.0 mm Hg SBP and 0.5 mm Hg DBP per BP-raising allele. Individually, these genetic variants each explain <0.1% of BP phenotype and collectively <3.5% of total BP variance (20,22,23).
Because primary hypertension is a highly heritable condition but genetic variants only explain a miniscule fraction of phenotypic variation and disease risk, the term missing heritability has been introduced. Missing heritability is the difference between estimated and observed phenotypic variance (24). Recent studies have suggested that missing heritability in hypertension may be due, in part, to pathological events during embryonic, fetal, and early postnatal life (e.g., nutritional deprivation of the fetus during pregnancy leading to low birth weight) having persistent effects on CVD homeostasis and thereby increasing CVD risk, including hypertension, with advancing age. These fetal programming events may be mediated by epigenetic mechanisms (i.e., alterations in gene expression in the absence of changes in DNA sequence, including post-translational histone modification, DNA methylation, and noncoding microRNAs) (25). During early life, epigenetic mechanisms seem to be strongly influenced by the environment, and environmentally induced epigenetic modification is heritable through multiple generations (26).
ENVIRONMENTAL (LIFESTYLE) FACTORS
Although the genetic predisposition to hypertension is nonmodifiable and conveys lifelong CVD risk, the risk for hypertension is modifiable and largely preventable due to a strong influence by key environmental/lifestyle factors. The most important of these factors, which often are gradually introduced in childhood and early adult life, are weight gain leading to overweight/obesity, unhealthy diet, excessive dietary sodium and inadequate potassium intake, insufficient physical activity, and consumption of alcohol (11). The greatest impact can be achieved by targeting lifestyle areas of highest deficiency and combining more than one of these lifestyle modifications, as the individual BP reductions are often additive. Nevertheless, only a minority of adults change their lifestyle after a diagnosis of hypertension (27) and sustainability is difficult, posing a substantial challenge for successful implementation of lifestyle modification (28). The evidence underlying each of the environmental/lifestyle factors that promote elevation of BP and hypertension will be briefly reviewed.
Heart-healthy diet
Consuming a healthful diet lowers BP. The Dietary Approaches to Stop Hypertension (DASH) eating plan is especially effective for lowering BP (29,30). The DASH diet is rich in fruits, vegetables, whole grains, nuts, legumes, lean protein, and low-fat dairy products and is markedly reduced in refined sugar, saturated fat, and cholesterol (29). The combination of low sodium intake and the DASH diet provides substantially greater BP reduction than sodium restriction or the DASH diet alone (30,31). Both the DASH diet and sodium reduction, therefore, are recommended in adults with elevated BP and hypertension (11,32).
Excess sodium intake
Sodium is an essential nutrient and dietary requirement for all humans (33). However, excessive sodium intake is an important determinant of hypertension (33,34). Sodium intake is positively correlated with BP in cross-sectional and prospective cohort studies and accounts substantially for the age-related rise in BP (35–41).
In the United States, most (>70%) of the sodium intake results from addition during processing of foods, including breads, salted meats, canned goods, cereals, pastries, and food preparation (fast-food and sit-down restaurants) (42–44). Modeling studies suggest that even a small reduction in population sodium intake would prevent thousands of deaths attributable to hypertension (e.g., heart disease and stroke) and save billions of dollars in health care costs annually (45).
Inadequate potassium intake
Increasing potassium intake lowers BP in hypertensive adults (46–50), especially among those who are black, older, or consuming a high intake of dietary sodium (51). Because of its BP-lowering effects, increased potassium intake would be expected to prevent CVD events, and several studies have demonstrated an inverse relationship of potassium intake to stroke as well as other forms of CVD (52). Increased potassium intake can be achieved either by augmenting dietary potassium intake or by use of potassium supplements. The former approach is preferable, with the DASH diet providing the recommended daily consumption of 4,700 mg for a 2,000-calorie intake (29).
Inadequate physical activity
Observational studies have consistently demonstrated a protective effect of physical activity in preventing hypertension and controlling BP among those with hypertension (53). Even moderate levels of physical activity have been associated with a reduction in the risk of incident hypertension (54). Randomized trials suggest that the best form of physical activity conveying BP-lowering benefits is aerobic exercise (5- to 7-mm Hg reduction), but dynamic and isometric resistance exercise are also effective (4- to 5-mm Hg reduction) (55,56). The mechanisms of physical activity in preventing hypertension are unclear but may include decreased cardiac output, diminution of sympathetic nervous system and renin-angiotensin system activity, decreased total peripheral vascular resistance and insulin resistance, and improved endothelial function (57).
Overweight and obesity
Studies in various populations demonstrate a direct, nearly linear association of body mass index (BMI) with BP (58). The risk of hypertension increases continuously with increasing anthropomorphic measurements (waist circumference, waist-to-hip ratio, and waist-to-height ratio) in parallel with BMI (59). About 40% of adults with hypertension in the United States are obese (BMI >30 kg/m2), and over one-third of the obese population has hypertension (SBP/DBP >140/90 mmHg or treatment with antihypertensive medication), compared to less than one-fifth of normal-weight individuals (60,61). Clinical studies have repeatedly demonstrated that weight loss reduces the risk for hypertension and BP in adults with hypertension (62,63).
Several pathophysiological mechanisms seem to contribute to the development of hypertension in obesity, including insulin resistance, chronic low-grade inflammation, oxidative stress, adipokine abnormalities (e.g., high leptin, reduced adiponectin), increased sympathetic nervous system and renin-angiotensin-aldosterone system activity, endothelial dysfunction, intestinal microbiota, and increased renal sodium reabsorption with volume expansion (64,65).
SOCIAL DETERMINANTS
Although hypertension is a consequence of a combination of environmental and genetic risk factors, social determinants of health are also risk factors for hypertension (66). Social determinants of health are broadly defined as “the circumstances in which people are born, grow, live, work, and age, and the systems put in place to deal with illness” (66). Socioeconomic status signifies socially defined economic factors that influence the positions that individuals or groups hold within the stratified structure of a society (66). Socioeconomic status includes wealth and income, education, employment/occupation status, access to health care, and other factors. Although social determinants are most often invoked in discussions of inequalities or disparities, social factors affect cardiovascular health in virtually all people (66).
In the United States, a strong association exists between social determinants of health and hypertension, especially in minority populations (blacks and Hispanics) (67). Hypertension is more prevalent in blacks than in whites, and hypertension increases the risk of stroke and end-stage kidney disease disproportionately in blacks (67,68). Blacks are more likely to have uncontrolled hypertension, largely due to lower BP control rates while taking antihypertensive medication (69,70).
Neighborhood characteristics may impact hypertension prevalence. Individuals residing in the most economically deprived neighborhoods have greater odds of having high BP (71). An association also exists between residence in certain geographic areas, such as the southeastern United States, and the prevalence of hypertension (72). Taken together, these and other social determinants of BP are critically important to the prevention and control of hypertension in the population.
OVERALL STRATEGIES FOR PREVENTION AND CONTROL OF HYPERTENSION
Prevention and control of hypertension can be achieved by application of targeted and/or population-based strategies. The targeted approach is the traditional strategy used in health care practice and seeks to achieve a clinically important reduction in BP for individuals at the upper end of the BP distribution. The targeted approach is used in the management of patients with hypertension, but the same approach is well-proven as an effective strategy for prevention of hypertension in those at high risk of developing hypertension (11). The population-based strategy is derived from public health mass environmental control experience (73). It aims to achieve a smaller reduction in BP that is applied to the entire population, resulting in a small downward shift in the entire BP distribution (74).
An appeal of the population-based approach is that modeling studies have consistently suggested that it provides greater potential to prevent CVD compared with the targeted strategy (75,76). This finding is based on the principle that a large number of people exposed to a small increased CVD risk may generate many more cases than a small number of people exposed to a large increased risk (75). For example, a general population DBP-lowering of as little as 2 mm Hg would be expected to result in a 17% reduction in the incidence of hypertension, a 14% reduction in stroke risk, and a 6% reduction in the risk of coronary heart disease (77). Because they use the same interventions, the targeted and population-based strategies are complementary and mutually reinforcing.
FACTORS PREVENTING/INTERFERING WITH HYPERTENSION CONTROL
In adults with hypertension, controlling BP to nonhypertensive levels through nonpharmacological and pharmacological treatment reduces the risk for CVD events and all-cause mortality by 20% to 40% (7,78). It has been estimated that approximately 46,000 deaths annually can be prevented through improved BP control among U.S. adults, more deaths than can be averted through modification of any other major risk factor (79). However, BP control can only be achieved if those with hypertension are identified, diagnosed, and treated. The first step in this cascade is the diagnosis of hypertension. Once hypertension is diagnosed, effective nonpharmacological and pharmacological approaches need to be implemented to lower BP. Finally, treatment must be adhered to and titrated to optimize BP and CVD risk reduction. Factors associated with hypertension awareness, treatment, and control, as well as the components of a systems-level algorithm designed to increase BP control rates, are schematically depicted in the Central Illustration.
Central Illustration. Prevention and Control of Hypertension.
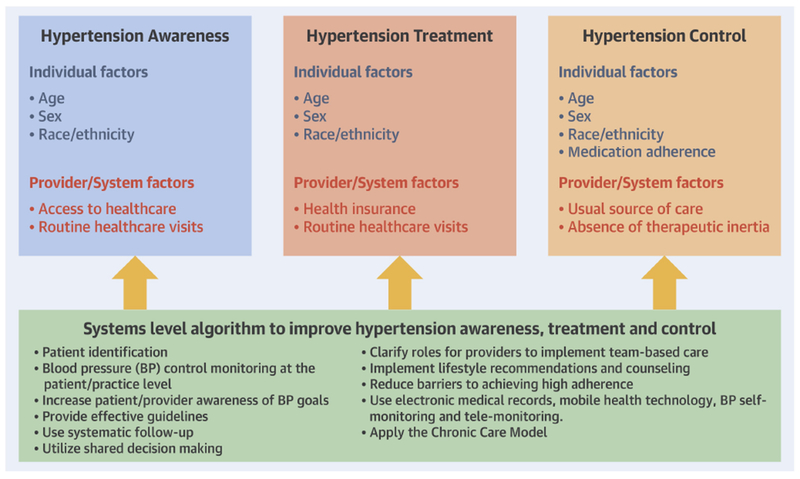
Factors associated with hypertension awareness, treatment, and control, and the components of a systems-level algorithm designed to increase blood pressure (BP) control.
Carey, R.M. et al. J Am Coll Cardiol. 2018;72(11):1278-93.
DIAGNOSIS OF HYPERTENSION: BP MEASUREMENT
Accurate BP measurement
The science underpinning prevention and treatment of high BP has progressively become stronger, but much remains to be done to ensure that this knowledge is translated to clinical practice. A fundamental need is to improve the quality of the BP measurements used for diagnosis and management of hypertension. Estimation of BP is highly prone to systematic and random error, but simple guideline-recommended approaches (11) minimize these errors. Unfortunately, the quality of BP assessments in clinical practice is very poor (80). Improvements in the quality of office-based measurements through training of clinicians or designated staff members is essential to translation of clinical practice recommendations for detection and management of hypertension. An important complement or alternative is to train patients in accurate measurement of BP. Initiatives such as Million Hearts (81) and Target BP (82) are important steps in reaching this goal.
BP self-monitoring/telemonitoring
Several randomized controlled trials, systematic reviews, and meta-analyses have shown that self-monitoring of BP (especially as a part of a multifaceted intervention) can lead to slightly improved BP control, possibly as a result of better adherence to treatment (83–86). The most effective approaches use telemonitoring (discussed later), whereby readings made at home are relayed to a health care professional who can take appropriate action. These studies showed that home telemonitoring for hypertension can produce reliable and accurate data and is well-accepted by patients (87,88). Self-monitoring with self-titration of antihypertensive medication compared with usual care resulted in lower SBP at 12 months among individuals with high CVD risk in the TASMIN2 trial (89).
Ambulatory BP monitoring
The United States Preventive Services Task Force and the 2017 ACC/AHA BP guideline recommend conducting out-of-office BP measurements, preferably with ambulatory BP monitoring (ABPM), to confirm the diagnosis of hypertension among patients with high BP in the clinic and to identify masked hypertension (11,90). Between 15% and 30% of adults with SBP > 140 mm Hg or DBP > 90 mm Hg, based on measurements obtained in the clinic, have white-coat hypertension, defined by mean awake SBP < 135 mm Hg and DBP < 85 mm Hg based on ABPM (91). Although white-coat hypertension has been associated with only a modestly increased risk for CVD compared with sustained normotension (nonhypertensive BP in the clinic and outside of the clinic on ABPM), a recent large observational study indicates that white-coat hypertension may not be benign (92,93). Additionally, between 15% and 30% of adults without hypertension, based on BP measured in the clinic (SBP < 140 mm Hg and DBP < 90 mm Hg), have masked hypertension, mean awake SBP > 135 mm Hg or DBP > 85 mm Hg on ABPM (94). In observational studies, masked hypertension has consistently been associated with a 2 times higher risk for CVD (95). Patients with clinic BP that is 10 mm Hg above or below the threshold for hypertension are the groups most likely to have white-coat hypertension and masked hypertension, respectively. Despite the potential value of ABPM for accurately diagnosing hypertension, it is not commonly performed in clinical practice in the United States. Barriers limiting the use of ABPM include the lack of knowledge among clinicians in how to conduct the procedure, limited access to specialists to conduct the test, and low reimbursement (96). Addressing these barriers and increasing the use of ABPM should be a high priority for ensuring antihypertensive medication is appropriately initiated and intensified.
HYPERTENSION AWARENESS
Awareness of hypertension has increased markedly over the past half-century in the United States. For example, according to the National Health and Nutrition Examination Survey (NHANES), the percentage of U.S. adults with hypertension (SBP >140 mm Hg, DBP >90 mm Hg, or treatment with antihypertensive medication) who were aware of having this condition increased from 70% in 1999 to 2000 to 84% in 2011 to 2014 (97).
A number of programs have been implemented to increase awareness of hypertension (81). Many of these programs have been directed toward populations with a high prevalence of hypertension, including blacks and individuals with low socioeconomic status. These programs appear to have been effective in raising hypertension awareness and subsequent hypertension screening. There are currently no clear patterns in disparities in hypertension awareness by poverty level or education, representing a marked change from the late 1980s and early 1990s, when hypertension awareness was less common among individuals with lower income and less education (98). Additionally, data from NHANES 2011 to 2014 report that a similar proportion of non-Hispanic blacks and whites are aware they have hypertension (86% and 85% for non-Hispanic, respectively) (97). In contrast, hypertension awareness is lower among Hispanics (80%) and non-Hispanic Asians (75%).
Lack of access to health care remains a barrier to increasing hypertension awareness. U.S. adults without health insurance are substantially less likely to be aware of having hypertension than their counterparts with health insurance (70% vs. 86%) (99). However, 82% of U.S. adults with hypertension but unaware of this diagnosis report having health insurance, 83% report having a usual source of care, and 62% report having had 2 or more health care visits in the previous year (97). Additionally, there is a graded association, with a progressively higher percentage of U.S. adults not aware of having hypertension among individuals with fewer health care visits per year.
Hypertension awareness differs around the world. Based on a systematic review of 90 studies, 46.5% of adults with hypertension worldwide in 2010 were aware they had this condition (100). Between 2000 and 2010, awareness of hypertension increased to a greater degree in high-income versus low- or medium-income countries. In 2010, awareness of hypertension was substantially more common in high-income countries compared with low- or middle-income countries (67.0% vs. 37.9%) (100).
HYPERTENSION TREATMENT
Following the diagnosis of hypertension, initiation of treatment is the next step toward achieving control of BP and reducing the risk for CVD. The 2017 ACC/AHA BP guideline recommends nonpharmacological treatment for all adults with hypertension (11). According to NHANES 1999 to 2004, 84% of U.S. adults who are aware of their diagnosis of hypertension report having been advised by a health care provider to make lifestyle modification changes to lower their BP (101). Most U.S. adults with hypertension report being advised to reduce their dietary sodium intake (82%), increase their physical activity (79%), and lose weight (66%), whereas only 31% were advised to reduce their alcohol consumption. Of those with hypertension who were advised to undertake nonpharmacological approaches to lower their BP, 88% reported adhering to these recommendations.
The 2017 ACC/AHA BP guideline recommends pharmacological antihypertensive treatment for adults with SBP > 140 mm Hg or DBP > 90 mm Hg (11). Additionally, adults with SBP between 130 and 139 mm Hg or DBP between 80 and 89 mm Hg are recommended pharmacological antihypertensive treatment if they have high CVD risk, defined by a history of CVD, diabetes, chronic kidney disease, a 10-year predicted CVD risk > 10%, or are 65 years of age or older. Among all U.S. adults with hypertension according to the Seventh Joint National Committee (JNC7) definition (SBP > 140 mm Hg and/or DBP > 90 mm Hg and/or antihypertensive medication use), 75% were taking pharmacological antihypertensive medication in 2013 to 2014 (102). Among those aware that they had hypertension, 89% were taking antihypertensive medication (102). In the United States, treatment with pharmacological therapy is more common among older versus younger adults, women (80.6%) compared with men (70.9%), and among non-Hispanic black (77.4%) and white (76.7%) adults compared with non-Hispanic Asians and Hispanics (73.5% and 65.2%, respectively) (103).
Similar to hypertension awareness, the use of antihypertensive medication differs by world region (100). Overall, 36.9% of adults with hypertension worldwide were taking antihypertensive medication in 2010. Use of antihypertensive medication was more common in high-income versus medium- or low-income regions (55.6% vs. 29.0%).
HYPERTENSION CONTROL
All adults with hypertension are recommended to use nonpharmacological approaches to lower their BP, and the use of these interventions is associated with a higher likelihood of having controlled BP (11). According to the NHANES 2011 to 2014, among adults taking antihypertensive medication, 39.0% of the U.S. population has BP above the goal defined in the JNC7 guideline (SBP > 140 mm Hg or DBP > 90 mm Hg) and 53.4% have SBP or DBP above the goal defined in the 2017 ACC/AHA guideline (SBP > 130 mm Hg or DBP > 80 mm Hg) (12). The percentage of U.S. adults taking antihypertensive medication with above-goal BP, whether using the JNC7 or 2017 ACC/AHA guideline, is higher at older age, among men compared with women, and among non-Hispanic blacks, non-Hispanic Asians, and Hispanics compared with non-Hispanic whites. The reasons for uncontrolled BP (Table 2) are multifactorial and include patient, provider, and health system factors (11), which are often intertwined.
Table 2.
Causes of Failure to Normalize BP
| Lack of health insurance |
| Lack of access to health care |
| Absence of a usual source of care |
| Failure to diagnose HT |
| Failure to screen for high BP |
| Inaccurate BP measurement |
| Failure to recognize masked HT |
| Clinician therapeutic inertia |
| Failure to treat masked HT |
| Failure to initiate treatment when HT is present |
| Failure to intensify therapy in a treated patient when BP is above goal |
| Inadequate patient education |
| Absence of shared decision-making |
| Inadequate lifestyle recommendations and counseling |
| Low adherence to lifestyle modification and/or prescribed antihypertensive medication |
| Absence of home or ambulatory BP monitoring and reporting |
| Low patient and/or provider awareness of BP target |
| Absence of systematic follow-up |
Abbreviations as in Table 1.
Having a usual source of care is strongly associated with BP control. Among U.S. adults in NHANES 2007 to 2012, 55% of those with a usual source of care had an SBP/DBP < 140/90 mm Hg, compared with 14% of their counterparts without a usual source of care (104). It is worth noting that 89% of U.S. adults without controlled BP report having a usual source of health care, and 82% reported having health insurance. This highlights challenges to achieving BP goals beyond just access to health care.
Low adherence to antihypertensive medication is common and a major contributing factor to uncontrolled BP (105). For example, in 1 study, 21.3% of 6,627 older U.S. adults initiating antihypertensive medication in 2012 discontinued treatment within 1 year (106). Also, 31.7% of patients who had not discontinued their antihypertensive medication had low treatment adherence, defined by having medication available to take for <80% of days in the year following treatment initiation. Barriers to achieving high medication adherence are multifactorial and include complex medication regimens (e.g., multi-pill regimens), convenience factors (e.g., dosing frequency), behavioral factors, and issues with treatment of asymptomatic diseases (e.g., treatment side effects) (106). Additional factors commonly associated with low antihypertensive medication adherence and uncontrolled BP include younger age, depressive symptoms, lack of lifestyle modification, and limited access to care (107–109). Methods to assess and improve adherence from a patient, clinician, and health system perspective are shown in Table 3.
Table 3.
Methods to Assess and Improve Adherence
| Assessment of Adherence |
|---|
| Indirect |
| Patient self-report; lacks accuracy |
| Adherence scales (e.g., Hill-Bone Compliance Scale); slight accuracy improvement |
| Prescription refill data, slight accuracy improvement |
| Direct |
| Medication Event Monitoring System*; increased accuracy over indirect methods |
| Witnessed medication intake; increased accuracy over indirect methods |
| Drug monitoring in blood or urine†; most accurate method currently available |
| Drug monitoring using drug fluorometry, accurate but experimental |
| Drug sensor, accurate but experimental |
| Improvement in Adherence |
| Educate patients, their families and caregivers about hypertension, its consequences and the possible adverse effects of antihypertensive medications |
| Address patient health literacy |
| Collaborate with patients to establish goals of therapy and the plan of care |
| Use antihypertensive agents dosed once daily and fixed-dose combinations |
| Use low-cost and generic medications whenever possible |
| Consolidate refill schedule to obtain all prescribed medication at a single pharmacy visit |
| Use motivation adherence scales to identify barriers |
| Assess for medication nonadherence regularly and systematically |
| Use team-based care |
| Maintain contact with patient via telehealth technology |
Uses an electronic pillbox or pill bottle that records each time the cap is opened.
Uses high-pressure liquid chromatography with tandem mass spectrometry
Clinician therapeutic inertia is another barrier preventing patients from achieving guideline-recommended BP goals. Data from the U.S. National Ambulatory Medical Care Survey indicate that there were 41.7 million primary care visits in the United States annually between 2005 and 2012 wherein a patient had SBP > 140 mm Hg or DBP > 90 mm Hg (110). However, a new antihypertensive medication was initiated in only 7 million (16.8%) of these visits. Several reasons may underlie clinicians not initiating or intensifying antihypertensive medication, including workflow constraints and insufficient time to conduct a patient evaluation, concern about side effects, lack of knowledge to make dosing decisions, and uncertainty regarding a patient’s out-of-office BP (112–115).
One approach available to clinicians to help overcome therapeutic inertia may be to prescribe a fixed-dose combination when initiating antihypertensive medication (116). Initiating treatment with 2 drug classes simultaneously can reduce the number of follow-up visits needed and has been shown to achieve a higher rate of BP control (117–119).
In 2014, the ACC/AHA and Clinical Disease Center (CDC) published a Scientific Advisory focused on approaches to control high BP (120). Effective system-level solutions to guide BP management include using the best scientific evidence, keeping algorithms simple and modifiable for when new evidence becomes available, creating a feasible strategy for implementation, giving patients information on how their BP should be managed, taking into account costs of diagnosis, treatment, and monitoring, and including a disclaimer to ensure that the algorithm is not used to contradict clinical judgement. Systems-level algorithms to increase the percentage of people with controlled BP include patient identification, monitoring BP control at the patient and practice levels, increasing patient and provider awareness of BP goals, providing effective diagnosis and treatment guidelines, having systematic follow-up for patients to ensure treatment is initiated and intensified when appropriate, clarifying roles of health care providers to implement a team-based approach, reducing barriers to achieve high medication adherence, encouraging nonpharmacological treatment, and using electronic medical records to support these steps. Evidence that these approaches can be effective has been demonstrated in several health systems that provide care for adults with health care insurance, including the Kaiser Permanente (121) and the Veterans Affairs health care systems (122).
Between 2000 and 2010, the percentage of those with hypertension who had controlled BP increased in high-income countries but declined in low- or middle-income countries (100). In 2010, 28.4% of adults with hypertension in high-income countries had controlled BP compared with only 7.7% among their counterparts in low- and middle-income countries. These data highlight the need for efforts to increase the control of BP in all world regions, with a focus on low- and middle-income countries.
MULTILEVEL AND POPULATION HEALTH INTERVENTIONS TO IMPROVE BP CONTROL
The pursuit of detecting and improving BP control has uncovered multifactorial barriers, including cultural norms, insufficient attention to health education by health care practitioners, lack of reimbursement for health education services, lack of access to sites to engage in physical activity, larger servings of food in restaurants, lack of availability of healthy food choices in many schools, worksites, and restaurants, lack of exercise programs in schools, large amounts of sodium added to foods during processing and preparation in fast-food and sit-down restaurants, and higher cost of food products that are lower in sodium and calorie content (74). These challenges to prevention, detection, awareness, and management of hypertension will require a multipronged approach directed not only to high-risk populations, but also to communities, schools, worksites, and the food industry.
To date, most interventions have been focused on improving hypertension-selfmanagement behaviors including BP self-monitoring, lifestyle changes (e.g., eating, exercise habits, and abstinence or moderation in alcohol consumption), improving adherence to medications (Table 3), and shared medical decision-making (i.e., patients playing an active role in decisions about their hypertension care with clinicians). These behaviors represent a cornerstone of recommended care for hypertension and have been associated with substantial improvements in hypertension control among treated patients (11,84,86,123–127). However, few interventions have effects at multiple sites in the system: patients; clinicians; health care organizations; and communities. Thus, when applied in real-world settings, interventions may ultimately fail if: they are not well-adapted to the organization where they are to be implemented; clinicians do not endorse the intervention; patients and their families are not actively engaged; or the communities in which patients live pose so many challenges to successful implementation of interventions that patients cannot be consistently adherent over time.
THE CHRONIC CARE MODEL
Strategies for overcoming barriers at the health system, physician, patient, and community levels (128,129) may be framed within the context of the Chronic Care Model (CCM). The CCM was developed as a framework for redesigning health care and addressing deficiencies in the care of chronic conditions, such as hypertension. Its 6 domains are decision support, self-management support, delivery design, information systems, community resources, and health care systems (Figure 2). Optimizing and integrating these domains has been shown to lead to activated patients, responsive health care teams, improved health services and treatment outcomes, and cost-effectiveness. (130–136) The CCM emphasizes the role of patients with hypertension as being their own principal caregivers and underscores the importance of health care providers, family, and community support in self-management (130,137). In effect, patients are at the center of the care model with providers, family, and community interacting in different ways to influence and support health decisions. Collaborative care can be categorized as: 1) collaborative definition of problems; 2) goal-setting, planning, and action plans; 3) a continuum of self-management training and support services; and 4) active and sustained follow-up (130–138). This model of care recognizes a collaborative partnership between the patient, provider, and the care team, each with their own expertise in managing that person’s health and sharing in the decision-making process. This collaborative partnership between patient and provider is important in supporting the patient’s management of their hypertension over multiple encounters and adjustments in the treatment plan, with the goal of achieving optimal care.
Figure 2: Schematic Illustration of the CCM, Including Multilevel Interventions to Prevent and Control Hypertension.
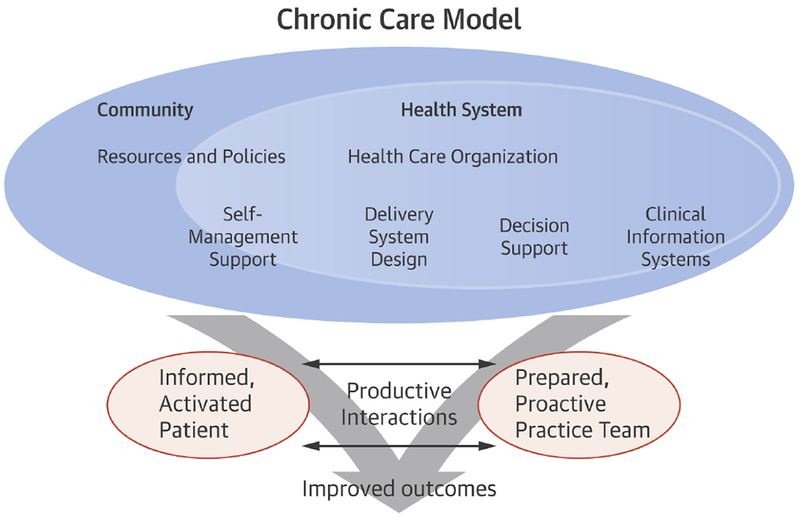
Adapted with permission from Wagner (132). CCM = chronic care model; HT = hypertension.
Team-based care
Team-based care incorporates a multidisciplinary team, centered on the patient, to optimize the quality of hypertension care and includes the patient, the primary care clinician, and other professionals such as nurses, pharmacists, physician assistants, dieticians, social workers, and community health workers, each with predefined responsibilities in care (11). These professionals complement the primary care clinician by providing process support and sharing the responsibilities of hypertension care. When the primary care provider can delegate routine matters to the team, more time is available to manage complex and critical patient-care problems. A recent systematic review and meta-analysis of 100 randomized trials determined that team-based care, involving medication titration by either nonphysicians or physicians, is highly effective compared with other implementation strategies for BP control in hypertensive patients (84).
Community involvement
Beyond the confines of the individual and the health system, the community is a significant partner and a vital point of intervention for attaining health goals and outcomes. Partnerships with community groups, such as civic, philanthropic, religious, and senior citizen organizations, provide locally focused orientation to the health needs of diverse populations. The probability of success increases as interventional strategies more aptly address the diversity of racial, ethnic, cultural, linguistic, religious, and social factors in the delivery of medical services. Community service organizations can promote the prevention of hypertension by providing culturally sensitive educational messages and lifestyle support services and by establishing CVD risk factor screening and referral programs (139).
Health care policy
Policy decisions play an important role when considering potential levels at which to apply hypertension interventions. An understanding of current policies related to reimbursement is essential to ensure implementation of any effective program. For example, the Centers for Medicare & Medicaid Services has a goal to link 50% of fee-for-service payments by 2018 to alternative payment and population-based care models such as accountable care organizations and patient-centered medical homes. These changes will affect hypertension management. Strong evidence suggests that team-based, coordinated care with shared decision making improves outcomes and reduces costs, particularly for hypertension (140,141).
Examples of multilevel interventions for hypertension
The Heart Health Lenoir Study was a multilevel Quality Improvement intervention to improve BP control in patients cared for K000 in rural primary care practices in eastern North Carolina. Results suggest that a practice-based multilevel intervention designed using the principles of health literacy can help lower SBP for up to 2 years in patients with low and higher health literacy (142).
Another recent study examined a nontraditional multilevel BP control intervention in which health promotion by barbers was linked to drug treatment by pharmacists and the resultant efficacy was evaluated in a cluster-randomized trial (143). At 6 months, the mean SBP reduction was 21.6 mm Hg greater in the intervention versus the control group (95% confidence interval: 14.7 to 28.4; p < 0.001).
There is also increasing work demonstrating the impact of community health worker-led interventions, a potentially more affordable and sustainable approach for low-income settings (144). In 1 study, low-income patients in Argentina with uncontrolled hypertension who participated in a community health worker-led multicomponent intervention experienced a greater decrease in SBP/DBP over 18 months than patients who received usual care (145).
CONNECTED HEALTH FOR HYPERTENSION CONTROL
Improving patients’ hypertension management behaviors, and medication adherence, although critically important, can be complex and time-consuming. In a typical primary care setting, time limitations, competing demands, and the burden of comorbid illness, along with inadequate mechanisms for follow-up constitute barriers to effective hypertension risk factor management. Many aspects of hypertension risk reduction, however, do not require a physical examination, and BP can be measured at home; thus, much of the care for hypertension could be accomplished outside of the traditional confines of office-based clinical care.
Advances in health information technology, including electronic health records and high-speed communications, provide new opportunities for improving the care of chronic conditions, including hypertension. Additionally, the Institute of Medicine’s blueprint for meeting the Crossing the Quality Chasm (146) goals for delivering of state-of-the-art health care suggests that patients should “receive care when they need it and in many forms, have unfettered access to their own medical information and that there should be active collaboration and information exchange between clinicians.”
Telemedicine
Telemedicine refers to interactive communications, which can be as simple as telephone-based care or interactive video and digital technologies, enabling direct communication between patients and their care team from remote sites. Automated interactive voice response uses computer technology to telephone patients, collect data, and provide tailored interventions based on their responses. Telemedicine or remote monitoring in patients’ homes has been offered as a plausible solution to improving ambulatory medical care. However current reimbursement models do not encourage these in-person and remote primary care interventions.
Telephone interventions
Clinic visits are primarily focused on symptom management, leaving little time for comprehensive risk factor management. An intervention that is delivered in patients’ homes may be more successful in nonsymptom-based approaches to health care. Telephone contact has been shown to be effective in changing multiple patient behaviors (147–150). Telephone interventions also allow more patients to be reached and these interventions may be more acceptable and convenient than in-person interventions (151). Delivering an intervention by telephone may enhance the interventions’ cost-effectiveness, primarily due to reduced intervention costs and reduced visit rates, coupled with the clinicians’ ability to follow a much larger panel over which to spread fixed intervention costs than would be possible with an in-person intervention. Thus, the use of telephones to implement the intervention allows individualized, personal interaction at minimal cost and without the time and transportation barriers that accompany in-person programs. This personal interaction allows the intervention to be adapted and tailored to participants’ current concerns, health goals, and specific barriers to achieving these goals.
Mobile health interventions
Mobile health interventions, such as smartphone applications (apps), have been advocated as promising strategies to assist in the self-management of hypertension. (152,153). These tools have the potential to address nonadherence by providing reminders for medication taking and refilling, tracking biometric results, offering education, and facilitating social interactions that provide support and motivation (154). From 2012 to 2015, there was a 515% increase in adherence apps available for download (155) and an estimated 107 unique apps have been evaluated for hypertension (156). However, rigorous evaluation of these technologies is still warranted, as indicated by a recent study among those with poorly controlled hypertension, in which patients randomized to the use of a stand-alone smartphone app had a small improvement in self-reported medication adherence but no change in SBP at 12 weeks of follow-up compared with controls (157).
Lifestyle counseling/monitoring
Clinicians would benefit from help in other areas as well, especially in counseling and monitoring recommendations for lifestyle change. This can be achieved by designation of a practice-based champion for lifestyle change who is sufficiently knowledgeable in behavior change techniques to be effective in patient counseling. Policy changes resulting in financial support for such endeavors would greatly enhance the opportunity for patients to improve their lifestyles and reduce the burden for busy clinicians.
SUMMARY
Remarkable progress has been made in the understanding of BP as a CVD risk factor and optimal approaches to the prevention and treatment of hypertension. Major clinical, societal, and research questions still remain to be answered (Table 4), which will require more and better research evidence. In addition to the importance of accuracy in measurement of BP, team-based care with shared decision-making, maximizing adherence by use of once-daily medications and combination pills when feasible, promotion of lifestyle strategies proven to be effective in lowering BP, active use of the electronic health record and telehealth strategies, and use of performance measures as a component of quality improvement initiatives and financial incentives can improve hypertension management and control rates. Optimizing prevention, recognition, and care of high BP is achievable but is predicated on the assumption that BP can be measured with greater accuracy, there is a progressive shift to team-based care and use of other strategies known to improve BP control, and the capacity to assist patients in adopting a healthier lifestyle is substantially strengthened.
Table 4:
Remaining Questions and Research Needs
| What are the optimal methods of BP measurement that balance accuracy with acceptability? |
| What are the most effective methods of engaging patients and the public in beneficial |
| lifestyle modification to lower BP? |
| What are the optimal BP treatment thresholds and goals that maximize CVD benefit while minimizing harm? |
| What is the optimal approach to management of white coat and masked HT? |
| How can we best detect and reverse antihypertensive medication nonadherence? |
| How can we successfully incorporate health information technology into the routine care of HT? |
| As a medical community, how can we most effectively use the CCM in the care of HT? |
| As a society, how can we encourage, promote and support community engagement in HT control in partnership with health systems, clinicians, patients, and the public? |
CCM = Chronic Care Model; CVD = cardiovascular disease. Other abbreviations as in Table 1.
Acknowledgments:
Dr. Carey has received grant support from the National Heart, Lung and Blood Institute (R01-HL-128189 and P01-HL-074940). Dr. Muntner has received grant support from the American Heart Association (15SFRN2390002). Dr. Bosworth has received grant funding from the Veterans Affairs Health Services Research and Development (VAHSR&D 08027) and from the National Institutes of Health (NIH K12-HL-138030, R01-DK093938, and R34-DK-102166). Dr. Whelton has received grant support from the National Institute of General Medical Sciences (P20GM109036).
ABBREVIATIONS AND ACRONYMS
- ABPM
ambulatory blood pressure monitoring
- BMI
body mass index
- BP
blood pressure
- CCM
Chronic Care Model
- CVD
cardiovascular disease
- DBP
diastolic blood pressure
- SBP
systolic blood pressure
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclosures: The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
REFERENCES
- 1.Forouzanfar MH, Liu P, Roth GA, et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015. JAMA 2017;317:165–82. [DOI] [PubMed] [Google Scholar]
- 2.GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2016;390:1345–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fox CS, Larson MG, Leip EP, Culleton B, Wilson PW, Levy D. Predictors of new-onset kidney disease in a community-based population. JAMA 2004;291:844–50. [DOI] [PubMed] [Google Scholar]
- 4.Klag MJ, Whelton PK, Randall BL, et al. Blood pressure and end-stage renal disease in men. N Engl J Med 1996;334:13–8. [DOI] [PubMed] [Google Scholar]
- 5.Hsu CY, McCulloch CE, Darbinian J, Go AS, Iribarren C. Elevated blood pressure and risk of end-stage renal disease in subjects without baseline kidney disease. Arch Intern Med 2005;165:923–8. [DOI] [PubMed] [Google Scholar]
- 6.Hwang S, Jayadevappa R, Zee J, et al. Concordance between clinical diagnosis and medicare claims of depression among older primary care patients. Am J Geriatr Psychiatry 2015;23:726–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies [Published correction appears in Lancet 2003;361:1060]. Lancet 2002;360:1903–13. [DOI] [PubMed] [Google Scholar]
- 8.Rapsomaniki E, Timmis A, George J, et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people. Lancet 2014;383:1899–911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lawes CMM, Rodgers A, Bennett DA, et al. Blood pressure and cardiovascular disease in the Asia Pacific region. J Hypertens 2003;21:707–16. [DOI] [PubMed] [Google Scholar]
- 10.Mills KT, Bundy JD, Kelly TN, et al. Global Disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation 2016;134:441–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018;71:e127–e248. [DOI] [PubMed] [Google Scholar]
- 12.Muntner P, Carey RM, Gidding S, et al. Potential US population impact of the 2017 ACC/AHA high blood pressure guideline. Circulation 2018;137:109–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bochud M, Bovet P, Elston RC, et al. High heritability of ambulatory blood pressure in families of East African descent. Hypertension 2005;45:445–50. [DOI] [PubMed] [Google Scholar]
- 14.Havlik RJ, Garrison RJ, Feinleib M, Kannel WB, Castelli WP, McNamara PM. Blood pressure aggregation in families. Am J Epidemiol 1979;110:304–12. [DOI] [PubMed] [Google Scholar]
- 15.Hottenga JJ, Boomsma DI, Kupper N, et al. Heritability and stability of resting blood pressure. Twin Res Hum Genet 2005;8:499–508. [DOI] [PubMed] [Google Scholar]
- 16.Kupper N, Willemsen G, Riese H, Posthuma D, Boomsma DI, de Geus EJ. Heritability of daytime ambulatory blood pressure in an extended twin design. Hypertension 2005;45:80–5. [DOI] [PubMed] [Google Scholar]
- 17.Snieder H, Harshfield GA, Treiber FA. Heritability of blood pressure and hemodynamics in African- and European-American youth. Hypertension 2003;41:1196–201. [DOI] [PubMed] [Google Scholar]
- 18.Frazer KA, Murray SS, Schork NJ, Topol EJ. Human genetic variation and its contribution to complex traits. Nat Rev Genet 2009;10:241–51. [DOI] [PubMed] [Google Scholar]
- 19.Padmanabhan S, Caulfield M, Dominiczak AF. Genetic and molecular aspects of hypertension. Circ Res 2015;116:937–59. [DOI] [PubMed] [Google Scholar]
- 20.Dominiczak AF, Kuo D. Hypertension: update 2017. Hypertension 2017;69:3–4. [DOI] [PubMed] [Google Scholar]
- 21.Lifton RP, Gharavi AG, Geller DS. Molecular mechanisms of human hypertension. Cell 2001;104:545–56. [DOI] [PubMed] [Google Scholar]
- 22.Ehret GB, Ferreira T, Chasman DI, et al. The genetics of blood pressure regulation and its target organs from association studies in 342,415 individuals. Nat Genet 2016;48:1171–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Surendran P, Drenos F, Young R, et al. Trans-ancestry meta-analyses identify rare and common variants associated with blood pressure and hypertension. Nat Genet 2016;48:1151–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zuk O, Hechter E, Sunyaev SR, Lander ES. The mystery of missing heritability: genetic interactions create phantom heritability. Proc Natl Acad Sci U S A 2012;109:1193–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kato N, Loh M, Takeuchi F, et al. Trans-ancestry genome-wide association study identifies 12 genetic loci influencing blood pressure and implicates a role for DNA methylation. Nat Genet 2015;47:1282–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lane M, Robker RL, Robertson SA. Parenting from before conception. Science 2014;345:756–60. [DOI] [PubMed] [Google Scholar]
- 27.Ineke Neutel C, Campbell NRC. Changes in lifestyle after hypertension diagnosis in Canada. Can J Cardiol 2008;24:199–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hinderliter AL, Sherwood A, Craighead LW, et al. The long-term effects of lifestyle change on blood pressure: one-year follow-up of the ENCORE study. Am J Hypertens 2014;27:734–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Appel LJ, Moore TJ, Obarzanek E, et al. ; DASH Collaborative Research Group. A clinical trial of the effects of dietary patterns on blood pressure. N Engl J Med 1997;336:1117–24. [DOI] [PubMed] [Google Scholar]
- 30.Sacks FM, Svetkey LP, Vollmer WM, et al. ; DASH-Sodium Collaborative Research Group. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med 2001;344:3–10. [DOI] [PubMed] [Google Scholar]
- 31.Juraschek SP, Miller ER III, Weaver CM, Appel LJ. Effects of sodium reduction and the DASH diet in relation to baseline blood pressure. J Am Coll Cardiol 2017;70:2841–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Van Horn L, Carson JAS, Appel LJ, et al. ; American Heart Association Nutrition Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Stroke Council. Recommended dietary pattern to achieve adherence to the American Heart Association/American College of Cardiology (AHA/ACC) Guidelines: a scientific statement from the American Heart Association [Published correction appears in: Circulation 2016;134:e534]. Circulation 2016;134:e505–e529.27789558 [Google Scholar]
- 33.O’Donnell M, Mente A, Yusuf S. Sodium intake and cardiovascular health. Circ Res 2015;116:1046–57. [DOI] [PubMed] [Google Scholar]
- 34.Whelton PK, Appel LJ, Sacco RL, et al. Sodium, blood pressure, and cardiovascular disease: further evidence supporting the American Heart Association sodium reduction recommendations. Circulation 2012;126:2880–9. [DOI] [PubMed] [Google Scholar]
- 35.Klag MJ, He J, Coresh J et al. The contribution of urinary cations to the blood pressure differences associated with migration. Am J Epidemiol 1995;142:295–303. [DOI] [PubMed] [Google Scholar]
- 36.Intersalt Cooperative Research Group. Intersalt: an international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. BMJ 1988;297:319–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Mente A, O’Donnell MJ, Rangarajan S, et al. ; PURE Investigators. Association of urinary sodium and potassium excretion with blood pressure. N Engl J Med 2014;371:601–11. [DOI] [PubMed] [Google Scholar]
- 38.Elliott P, Stamler J, Nichols R, et al. ; Intersalt Cooperative Research Group. Intersalt revisited: further analyses of 24 hour sodium excretion and blood pressure within and across populations. BMJ 1996;312:1249–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Takase H, Sugiura T, Kimura G, Ohte N, Dohi Y. Dietary sodium consumption predicts future blood pressure and incident hypertension in the Japanese normotensive general population. J Am Heart Assoc 2015;4:e001959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Stamler J The INTERSALT Study: background, methods, findings, and implications [Published correction appears in: Am J Clin Nutr 1997;66:1297]. Am J Clin Nutr 1997;65:626S–642S. [DOI] [PubMed] [Google Scholar]
- 41.Jackson SL, Cogswell ME, Zhao L, et al. Association between urinary sodium and potassium excretion and blood pressure among adults in the United States: National Health and Nutrition Examination Survey, 2014. Circulation 2018;137:237–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Institute of Medicine (US) Committee on Strategies to Reduce Sodium Intake; Henney JETC, Boon CS, editors. Strategies to reduce sodium intake in the United States. National Academies Press: Washington, DC, 2010. [PubMed] [Google Scholar]
- 43.Draft Guidance for Industry: Voluntary Sodium Reduction Goals: Target Mean and Upper Bound Concentrations for Sodium in Commercially Processed, Packaged, and Prepared Foods. Silver Spring, MD: U.S. Department of Health and Human Services Food and Drug Administration, Center for Food Safety and Applied Nutrition, June 2016. Available at: https://www.fda.gov/downloads/Food/GuidanceRegulation/GuidanceDocumentsRegulatoryInformation/UCM503798.pdf. Accessed July 9, 2018. [Google Scholar]
- 44.Harnack LJ, Cogswell ME, Shikany JM, et al. Sources of sodium in US adults from 3 geographic regions. Circulation 2017;135:1775–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bibbins-Domingo K, Chertow GM, Coxson PG, et al. Projected effect of dietary salt reductions on future cardiovascular disease. N Engl J Med 2010;362:590–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Whelton PK, He J, Cutler JA, et al. Effects of oral potassium on blood pressure. Metaanalysis of randomized controlled clinical trials. JAMA 1997;277:1624–32. [DOI] [PubMed] [Google Scholar]
- 47.Geleijnse JM, Kok FJ, Grobbee DE. Blood pressure response to changes in sodium and potassium intake: a metaregression analysis of randomised trials. J Hum Hypertens 2003;17:471–80. [DOI] [PubMed] [Google Scholar]
- 48.Aburto NJ, Ziolkovska A, Hooper L, Elliott P, Cappuccio FP, Meerpohl JJ. Effect of lower sodium intake on health: systematic review and meta-analyses. BMJ 2013;346:f1326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Filippini T, Violi F, D’Amico R, Vinceti M. The effect of potassium supplementation on blood pressure in hypertensive subjects: a systematic review and meta-analysis. Int J Cardiol 2017;230:127–35. [DOI] [PubMed] [Google Scholar]
- 50.Poorolajal J, Zeraati F, Soltanian AR, Sheikh V, Hooshmand E, Maleki A. Oral potassium supplementation for management of essential hypertension: a meta-analysis of randomized controlled trials. PLoS ONE 2017;12:e0174967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Brancati FL, Appel LJ, Seidler AJ, Whelton PK. Effect of potassium supplementation on blood pressure in African Americans on a low-potassium diet. A randomized, double-blind, placebo-controlled trial. Arch Intern Med 1996;156:61–7. [PubMed] [Google Scholar]
- 52.Vinceti M, Filippini T, Crippa A, de Sesmaisons A, Wise LA, Orsini N. Meta-analysis of potassium intake and the risk of stroke. J Am Heart Assoc 2016;5:e004210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Huai P, Xun H, Reilly KH, Wang Y, Ma W, Xi B. Physical activity and risk of hypertension: a meta-analysis of prospective cohort studies. Hypertension 2013;62:1021–6. [DOI] [PubMed] [Google Scholar]
- 54.Hayashi T, Tsumura K, Suematsu C, Okada K, Fujii S, Endo G. Walking to work and the risk for hypertension in men: the Osaka Health Survey. Ann Intern Med 1999;131:21–6. [DOI] [PubMed] [Google Scholar]
- 55.Dimeo F, Pagonas N, Seibert F, Arndt R, Zidek W, Westhoff TH. Aerobic exercise reduces blood pressure in resistant hypertension. Hypertension 2012;60:653–8. [DOI] [PubMed] [Google Scholar]
- 56.Blumenthal JA, Siegel WC, Appelbaum M. Failure of exercise to reduce blood pressure in patients with mild hypertension. Results of a randomized controlled trial. JAMA 1991;266:2098–104. [PubMed] [Google Scholar]
- 57.Arakawa K Antihypertensive mechanism of exercise. J Hypertens 1993; 11:223–9. [DOI] [PubMed] [Google Scholar]
- 58.Hall JE. The kidney, hypertension, and obesity. Hypertension 2003;41:625–33. [DOI] [PubMed] [Google Scholar]
- 59.Jayedi A, Rashidy-Pour A, Khorshidi M, Shab-Bidar S. Body mass index, abdominal adiposity, weight gain and risk of developing hypertension: a systematic review and dose-response meta-analysis of more than 2.3 million participants. Obes Rev 2018;19:654–67. [DOI] [PubMed] [Google Scholar]
- 60.Egan BM, Li J, Hutchison FN, Ferdinand KC. Hypertension in the United States, 1999 to 2012: progress toward Healthy People 2020 goals. Circulation 2014;130:1692–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Saydah S, Bullard KM, Cheng Y, et al. Trends in cardiovascular disease risk factors by obesity level in adults in the United States, NHANES 1999–2010. Obesity (Silver Spring) 2014;22:1888–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Jones DW, Miller ME, Wofford MR, et al. The effect of weight loss intervention on antihypertensive medication requirements in the Hypertension Optimal Treatment (HOT) study. Am J Hypertens 1999;12:1175–80. [DOI] [PubMed] [Google Scholar]
- 63.Stevens VJ, Obarzanek E, Cook NR, et al. ; Trials of Hypertension Prevention Research Group. Long-term weight loss and changes in blood pressure: results of the Trials of Hypertension Prevention, phase II. Ann Intern Med 2001;134:1–11. [DOI] [PubMed] [Google Scholar]
- 64.Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res 2015;116:991–1006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.DeMarco VG, Aroor AR, Sowers JR. The pathophysiology of hypertension in patients with obesity. Nat Rev Endocrinol 2014;10:364–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Havranek EP, Mujahid MS, Barr DA, et al. ; American Heart Association Council on Quality of Care and Outcomes Research, Council on Epidemiology and Prevention, Council on Cardiovascular and Stroke Nursing, Council on Lifestyle and Cardiometabolic Health, and Stroke Council. Social determinants of risk and outcomes for cardiovascular disease: a scientific statement from the American Heart Association. Circulation 2015;132:873–98. [DOI] [PubMed] [Google Scholar]
- 67.Rodriguez F, Ferdinand KC. Hypertension in minority populations: new guidelines and emerging concepts. Adv Chronic Kidney Dis 2015;22:145–53. [DOI] [PubMed] [Google Scholar]
- 68.Howard G, Lackland DT, Kleindorfer DO, et al. Racial differences in the impact of elevated systolic blood pressure on stroke risk. JAMA Intern Med 2013;173:46–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999–2000. JAMA 2002;288:1723–7. [DOI] [PubMed] [Google Scholar]
- 70.Howard G, Prineas R, Moy C, et al. Racial and geographic differences in awareness, treatment, and control of hypertension: the REasons for Geographic And Racial Differences in Stroke study. Stroke 2006;37:1171–8. [DOI] [PubMed] [Google Scholar]
- 71.Keita AD, Judd SE, Howard VJ, Carson AP, Ard JD, Fernandez JR. Associations of neighborhood area level deprivation with the metabolic syndrome and inflammation among middle- and older-age adults. BMC Public Health 2014;14:1319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Kershaw KN, Roux AV Diez, Carnethon M, et al. Geographic variation in hypertension prevalence among blacks and whites: the Multi-Ethnic Study of Atherosclerosis. Am J Hypertens 2010;23:46–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Rose G Sick individuals and sick populations. Int J Epidemiol 1985;14:32–8. [DOI] [PubMed] [Google Scholar]
- 74.Whelton PK, He J, Appel LJ, et al. ; National High Blood Pressure Education Program Coordinating Committee. Primary prevention of hypertension: clinical and public health advisory from the National High Blood Pressure Education Program. JAMA 2002;288:1882–8. [DOI] [PubMed] [Google Scholar]
- 75.Rose G The strategy of preventive medicine. Oxford, U.K.: Oxford University Press, 1992. [Google Scholar]
- 76.Emberson J, Whincup P, Morris R, Walker M, Ebrahim S. Evaluating the impact of population and high-risk strategies for the primary prevention of cardiovascular disease. Eur Heart J 2004;25:484–91. [DOI] [PubMed] [Google Scholar]
- 77.Cook NR, Cohen J, Hebert PR, Taylor JO, Hennekens CH. Implications of small reductions in diastolic blood pressure for primary prevention. Arch Intern Med 1995;155:701–9. [PubMed] [Google Scholar]
- 78.Tajeu GS, Booth JN III, Colantonio LD, et al. Incident cardiovascular disease among adults with blood pressure <140/90 mm Hg. Circulation 2017;136:798–812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Farley TA, Dalal MA, Mostashari F, Frieden TR. Deaths preventable in the U.S. by improvements in use of clinical preventive services. Am J Prev Med 2010;38:600–9. [DOI] [PubMed] [Google Scholar]
- 80.Myers MG. The great myth of office blood pressure measurement. J Hypertens 2012;30:1894–8. [DOI] [PubMed] [Google Scholar]
- 81.Frieden TR, Berwick DM. The “Million Hearts” initiative-preventing heart attacks and strokes. N Engl J Med 2011;365:e27. [DOI] [PubMed] [Google Scholar]
- 82.Target: BP. BP guideline. Top 5 takeaways for your practice. 2016. American Heart Association, American Medical Association; Available at: https://targetbp.org/guidelines17/. Accessed July 9, 2018. [Google Scholar]
- 83.Reboussin DM, Allen NB, Griswold ME, et al. Systematic review for the 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018;71:2176–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Mills KT, Obst KM, Shen W, et al. Comparative effectiveness of implementation strategies for blood pressure control in hypertensive patients: a systematic review and meta-analysis. Ann Intern Med 2018; 168:110–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Bray EP, Holder R, Mant J, McManus RJ. Does self-monitoring reduce blood pressure? Meta-analysis with meta-regression of randomized controlled trials. Ann Med 2010;42:371–86. [DOI] [PubMed] [Google Scholar]
- 86.Ogedegbe G, Schoenthaler A. A systematic review of the effects of home blood pressure monitoring on medication adherence. J Clin Hypertens (Greenwich) 2006;8:174–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Pare G, Jaana M, Sicotte C. Systematic review of home telemonitoring for chronic diseases: the evidence base. J Am Med Inform Assoc 2007;14:269–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Bosworth HB, Powers BJ, Olsen MK, et al. Home blood pressure management and improved blood pressure control: results from a randomized controlled trial. Arch Intern Med 2011;171:1173–80. [DOI] [PubMed] [Google Scholar]
- 89.McManus RJ, Mant J, Haque MS, et al. Effect of self-monitoring and medication selftitration on systolic blood pressure in hypertensive patients at high risk of cardiovascular disease: the TASMIN-SR randomized clinical trial. JAMA 2014;312:799–808. [DOI] [PubMed] [Google Scholar]
- 90.Siu AL U.S. Preventive Services Task Force. Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2015;163:778–86. [DOI] [PubMed] [Google Scholar]
- 91.Piper MA, Evans CV, Burda BU, Margolis KL, O’Connor E, Whitlock EP. Diagnostic and predictive accuracy of blood pressure screening methods with consideration of rescreening intervals: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 2015;162:192–204. [DOI] [PubMed] [Google Scholar]
- 92.Banegas JR, Ruilope LM, de la Sierra A, et al. Relationship between clinic and ambulatory blood-pressure measurements and mortality. N Engl J Med 2018;378:1509–20. [DOI] [PubMed] [Google Scholar]
- 93.Muntner P, Booth JN III, Shimbo D, Schwartz JE. Is white-coat hypertension associated with increased cardiovascular and mortality risk? J Hypertens 2016;34:1655–8. [DOI] [PubMed] [Google Scholar]
- 94.Booth JN III, Diaz KM, Seals SR, et al. Masked hypertension and cardiovascular disease events in a prospective cohort of blacks: the Jackson Heart Study. Hypertension 2016;68:501–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Palla M, Saber H, Konda S, Briasoulis A. Masked hypertension and cardiovascular outcomes: an updated systematic review and meta-analysis. Integr Blood Press Control 2018;11:11–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Kronish IM, Kent S, Moise N, et al. Barriers to conducting ambulatory and home blood pressure monitoring during hypertension screening in the United States. J Am Soc Hypertens 2017;11:573–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Paulose-Ram R, Gu Q, Kit B. Characteristics of U.S. adults with hypertension who are unaware of their hypertension, 2011–2014. NCHS Data Brief 2017;(278): 1–8. [PubMed] [Google Scholar]
- 98.Burt VL, Cutler JA, Higgins M, et al. Trends in the prevalence, awareness, treatment, and control of hypertension in the adult US population. Data from the health examination surveys, 1960 to 1991. Hypertension 1995;26:60–9. [DOI] [PubMed] [Google Scholar]
- 99.Egan BM, Li J, Small J, Nietert PJ, Sinopoli A. The growing gap in hypertension control between insured and uninsured adults: National Health and Nutrition Examination Survey 1988 to 2010. Hypertension 2014;64:997–1004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: A systematic analysis of population-based studies from 90 countries. Circulation 2016;134:441–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Lopez L, Cook EF, Horng MS, Hicks LS. Lifestyle modification counseling for hypertensive patients: results from the National Health and Nutrition Examination Survey 1999–2004. Am J Hypertens 2009;22:325–31. [DOI] [PubMed] [Google Scholar]
- 102.Zhang Y, Moran AE. Trends in the prevalence, awareness, treatment, and control of hypertension among young adults in the United States, 1999 to 2014. Hypertension 2017;70:736–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS Data Brief 2013;(133): 1–8. [PubMed] [Google Scholar]
- 104.Dinkler JM, Sugar CA, Escarce JJ, Ong MK, Mangione CM. Does age matter? Association between usual source of care and hypertension control in the US population: Data from NHANES 2007–2012. Am J Hypertens 2016;29:934–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Peacock E, Krousel-Wood M. Adherence to antihypertensive therapy. Med Clin North Am 2017;101:229–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Tajeu GS, Kent ST, Kronish IM, et al. Trends in antihypertensive medication discontinuation and low adherence among Medicare beneficiaries initiating treatment from 2007 to 2012. Hypertension 2016;68:565–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Krousel-Wood M, Hyre A, Muntner P, Morisky D. Methods to improve medication adherence in patients with hypertension: current status and future directions. Curr Opin Cardiol 2005;20:296–300. [DOI] [PubMed] [Google Scholar]
- 108.Krousel-Wood MA, Muntner P, Islam T, Morisky DE, Webber LS. Barriers to and determinants of medication adherence in hypertension management: perspective of the Cohort Study of Medication Adherence Among Older Adults. Med Clin North Am 2009;93:753–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Krousel-Wood M, Islam T, Muntner P, et al. Association of depression with antihypertensive medication adherence in older adults: cross-sectional and longitudinal findings from CoSMO. Ann Behav Med 2010;40:248–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Krousel-Wood M, Joyce C, Holt E, et al. Predictors of decline in medication adherence: results from the cohort study of medication adherence among older adults. Hypertension 2011;58:804–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Mu L, Mukamal KJ. Treatment intensification for hypertension in US ambulatory medical care. J Am Heart Assoc 2016;5:e004188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Willock R Josiah, Miller JB, Mohyi M, Abuzaanona A, Muminovic M, Levy PD. Therapeutic inertia and treatment intensification. Curr Hypertens Rep 2018;20:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Levy PD, Willock RJ, Burla M, et al. Total antihypertensive therapeutic intensity score and its relationship to blood pressure reduction. J Am Soc Hypertens 2016;10:906–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Faria C, Wenzel M, Lee KW, Coderre K, Nichols J, Belletti DA. A narrative review of clinical inertia: focus on hypertension. J Am Soc Hypertens 2009;3:267–76. [DOI] [PubMed] [Google Scholar]
- 115.Holland N, Segraves D, Nnadi VO, Belletti DA, Wogen J, Arcona S. Identifying barriers to hypertension care: implications for quality improvement initiatives. Dis Manag 2008;11:71–7. [DOI] [PubMed] [Google Scholar]
- 116.Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2013;31:1281–357. [DOI] [PubMed] [Google Scholar]
- 117.Mancia G, Parati G, Bilo G, Choi J, Kilama MO, Ruilope LM. Blood pressure control by the nifedipine GITS-telmisartan combination in patients at high cardiovascular risk: the TALENT study. J Hypertens 2011;29:600–9. [DOI] [PubMed] [Google Scholar]
- 118.Egan BM, Bandyopadhyay D, Shaftman SR, Wagner CS, Zhao Y, Yu-Isenberg KS. Initial monotherapy and combination therapy and hypertension control the first year. Hypertension 2012;59:1124–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Brown MJ, Mclnnes GT, Papst CC, Zhang J, MacDonald TM. Aliskiren and the calcium channel blocker amlodipine combination as an initial treatment strategy for hypertension control (ACCELERATE): a randomised, parallel-group trial. Lancet 2011;377:312–20. [DOI] [PubMed] [Google Scholar]
- 120.Go AS, Bauman MA, King SM Coleman, et al. An effective approach to high blood pressure control: a science advisory from the American Heart Association, the American College of Cardiology, and the Centers for Disease Control and Prevention. J Am Coll Cardiol 2014;63:1230–8. [DOI] [PubMed] [Google Scholar]
- 121.Jaffe MG, Lee GA, Young JD, Sidney S, Go AS. Improved blood pressure control associated with a large-scale hypertension program. JAMA 2013;310:699–705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Fletcher RD, Amdur RL, Kolodner R, et al. Blood pressure control among US veterans: a large multiyear analysis of blood pressure data from the Veterans Administration health data repository. Circulation 2012;125:2462–8. [DOI] [PubMed] [Google Scholar]
- 123.Wright JT Jr., Probstfield JL, Cushman WC, et al. ; ALLHAT Collaborative Research Group. ALLHAT findings revisited in the context of subsequent analyses, other trials, and meta-analyses. Arch Intern Med 2009;169:832–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women. The Women’s Health Initiative (WHI). Arch Intern Med 2004;164:289–98. [DOI] [PubMed] [Google Scholar]
- 125.Chobanian AV, Bakris GL, Black HR, et al. ; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003;289:2560–72. [DOI] [PubMed] [Google Scholar]
- 126.Pickering TG, Miller NH, Ogedegbe G, et al. Call to action on use and reimbursement for home blood pressure monitoring: executive summary: a joint scientific statement from the American Heart Association, American Society Of Hypertension, and Preventive Cardiovascular Nurses Association. Hypertension 2008;52:1–9. [DOI] [PubMed] [Google Scholar]
- 127.Schoenthaler A, Chaplin WF, Allegrante JP, et al. Provider communication effects medication adherence in hypertensive African Americans. Patient Educ Couns 2009;75:185–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.He J, Muntner P, Chen J, Roccella EJ, Streiffer RH, Whelton PK. Factors associated with hypertension control in the general population of the United States. Arch Intern Med 2002;162:1051–8. [DOI] [PubMed] [Google Scholar]
- 129.Odedosu T, Schoenthaler A, Vieira DL, Agyemang C, Ogedegbe G. Overcoming barriers to hypertension control in African Americans. Cleve Clin J Med 2012;79:46–56. [DOI] [PubMed] [Google Scholar]
- 130.Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness. JAMA 2002;288:1775–9. [DOI] [PubMed] [Google Scholar]
- 131.McCulloch DK, Price MJ, Hindmarsh M, Wagner EH. A population-based approach to diabetes management in a primary care setting: early results and lessons learned. Eff Clin Pract 1998;1:12–22. [PubMed] [Google Scholar]
- 132.Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Eff Clin Pract 1998;1:2–4. [PubMed] [Google Scholar]
- 133.Wagner EH. The role of patient care teams in chronic disease management. BMJ 2000;320:569–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Wagner EH, Glasgow RE, Davis C, et al. Quality improvement in chronic illness care: a collaborative approach. Jt Comm J Qual Improv 2001;27:63–80. [DOI] [PubMed] [Google Scholar]
- 135.Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q 1996;74:511–44. [PubMed] [Google Scholar]
- 136.Coleman EA, Grothaus LC, Sandhu N, Wagner EH. Chronic care clinics: a randomized controlled trial of a new model of primary care for frail older adults. J Am Geriatr Soc 1999;47:775–83. [DOI] [PubMed] [Google Scholar]
- 137.Scisney-Matlock M, Bosworth HB, Giger JN, et al. Strategies for implementing and sustaining therapeutic lifestyle changes as part of hypertension management in African Americans. Postgrad Med 2009;121:147–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Grumbach K, Bodenheimer T. Can health care teams improve primary care practice? JAMA 2004;291: 1246–51. [DOI] [PubMed] [Google Scholar]
- 139.National High Blood Pressure Education Program. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Bethesda, MD: National Heart Lung, and Blood Institute; 2004. [PubMed] [Google Scholar]
- 140.David G, Gunnarsson C, Saynisch PA, Chawla R, Nigam S. Do patient-centered medical homes reduce emergency department visits? Health Serv Res 2015;50:418–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Jacob V, Chattopadhyay SK, Thota AB, et al. Economics of team-based care in controlling blood pressure: a community guide systematic review. Am J Prev Med 2015;49:772–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Halladay JR, Donahue KE, Cene CW, et al. The association of health literacy and blood pressure reduction in a cohort of patients with hypertension: the Heart Healthy Lenoir trial. Patient Educ Couns 2017;100:542–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Victor RG, Lynch K, Li N, et al. A cluster-randomized trial of blood-pressure reduction in black barbershops. N Engl J Med 2018;378:1291–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Santschi V, Chiolero A, Colosimo AL, et al. Improving blood pressure control through pharmacist interventions: A meta-analysis of randomized controlled trials. J Am Heart Assoc 2014;3:e000718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.He J, Irazola V, Mills KT, et al. ; HCPIA Investigators. Effect of a community health worker-led multicomponent intervention on blood pressure control in low-income patients in Argentina: a randomized clinical trial. JAMA 2017;318:1016–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press, 2001. [PubMed] [Google Scholar]
- 147.Bosworth HB, Olsen MK, Gentry P, et al. Nurse administered telephone intervention for blood pressure control: a patient-tailored multifactorial intervention. Patient Educ Couns 2005;57:5–14. [DOI] [PubMed] [Google Scholar]
- 148.Friedman RH, Kazis LE, Jette A, et al. A telecommunications system for monitoring and counseling patients with hypertension. Impact on medication adherence and blood pressure control. Am J Hypertens 1996;9:285–92. [DOI] [PubMed] [Google Scholar]
- 149.Pinto BM, Friedman R, Marcus BH, Kelley H, Tennstedt S, Gillman MW. Effects of a computer-based, telephone-counseling system on physical activity. Am J Prev Med 2002;23:113–20. [DOI] [PubMed] [Google Scholar]
- 150.Resnicow K, Jackson A, Wang T, et al. A motivational interviewing intervention to increase fruit and vegetable intake through Black churches: results of the Eat for Life trial. Am J Public Health 2001;91:1686–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Friedman RH. Automated telephone conversations to assess health behavior and deliver behavioral interventions. J Med Syst 1998;22:95–102. [DOI] [PubMed] [Google Scholar]
- 152.Rehman H, Kamal AK, Morris PB, Sayani S, Merchant AT, Virani SS. Mobile health (mHealth) technology for the management of hypertension and hyperlipidemia: slow start but loads of potential. Curr Atheroscler Rep 2017;19:12. [DOI] [PubMed] [Google Scholar]
- 153.Buis LR, Artinian NT, Schwiebert L, Yarandi H, Levy PD. Text messaging to improve hypertension medication adherence in African Americans: BPMED Intervention Development and Study Protocol. JMIR Res Protoc 2015;4:e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Dayer L, Heldenbrand S, Anderson P, Gubbins PO, Martin BC. Smartphone medication adherence apps: potential benefits to patients and providers. J Am Pharm Assoc (2003) 2013;53:172–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Dayer LE, Shilling R, Van Valkenburg M, et al. Assessing the medication adherence app marketplace from the health professional and consumer vantage points. JMIR Mhealth Uhealth 2017;5:e45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Kumar N, Khunger M, Gupta A, Garg N. A content analysis of smartphone-based applications for hypertension management. J Am Soc Hypertens 2015;9:130–6. [DOI] [PubMed] [Google Scholar]
- 157.Morawski K, Ghazinouri R, Krumme A, et al. Association of a smartphone application with medication adherence and blood pressure control: the MedlSAFE-BP randomized clinical trial. JAMA Intern Med 2018;178:802–9. [DOI] [PMC free article] [PubMed] [Google Scholar]