

Abstract
Background
This is an update of a Cochrane review that was first published in 2011 of the effects of reducing dietary salt intake, through advice to reduce salt intake or low‐sodium salt substitution, on mortality and cardiovascular events.
Objectives
1. To assess the long‐term effects of advice and salt substitution, aimed at reducing dietary salt, on mortality and cardiovascular morbidity.
2. To investigate whether a reduction in blood pressure is an explanatory factor in the effect of such dietary interventions on mortality and cardiovascular outcomes.
Search methods
We updated the searches of CENTRAL (2013, Issue 4), MEDLINE (OVID, 1946 to April week 3 2013), EMBASE (OVID, 1947 to 30 April 2013) and CINAHL (EBSCO, inception to 1 April 2013) and last ran these on 1 May 2013. We also checked the references of included studies and reviews. We applied no language restrictions.
Selection criteria
Trials fulfilled the following criteria: (1) randomised, with follow‐up of at least six months, (2) the intervention was reduced dietary salt (through advice to reduce salt intake or low‐sodium salt substitution), (3) participants were adults and (4) mortality or cardiovascular morbidity data were available. Two review authors independently assessed whether studies met these criteria.
Data collection and analysis
A single author extracted data and assessed study validity, and a second author checked this. We contacted trial authors where possible to obtain missing information. We extracted events and calculated risk ratios (RRs) and 95% confidence intervals (CIs).
Main results
Eight studies met the inclusion criteria: three in normotensives (n = 3518) and five in hypertensives or mixed populations of normo‐ and hypertensives (n = 3766). End of trial follow‐up ranged from six to 36 months and the longest observational follow‐up (after trial end) was 12.7 years.
The risk ratios (RR) for all‐cause mortality in normotensives were imprecise and showed no evidence of reduction (end of trial RR 0.67, 95% confidence interval (CI) 0.40 to 1.12, 60 deaths; longest follow‐up RR 0.90, 95% CI 0.58 to 1.40, 79 deaths n=3518) or in hypertensives (end of trial RR 1.00, 95% CI 0.86 to 1.15, 565 deaths; longest follow‐up RR 0.99, 95% CI 0.87 to 1.14, 674 deaths n=3085).
There was weak evidence of benefit for cardiovascular mortality (hypertensives: end of trial RR 0.67, 95% CI 0.45 to 1.01, 106 events n=2656) and for cardiovascular events (hypertensives: end of trial RR 0.76, 95% CI 0.57 to 1.01, 194 events, four studies, n = 3397; normotensives: at longest follow‐up RR 0.84, 95% CI 0.64 to 1.10, 200 events; hypertensives: RR 0.77, 95% CI 0.58 to 1.02, 192 events; pooled analysis of six trials (RR 0.81, 95% CI 0.66 to 0.98; n = 5762). These findings were driven by one trial among retirement home residents that reduced salt intake in the kitchens of the homes, thereby not requiring individual behaviour change.
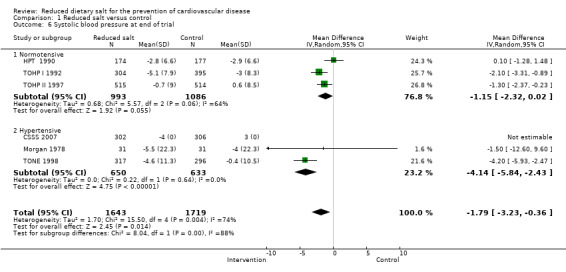
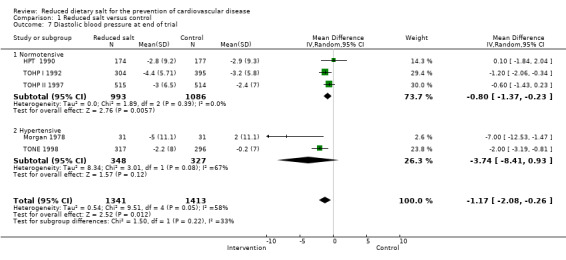
Advice to reduce salt showed small reductions in systolic blood pressure (mean difference (MD) ‐1.15 mmHg, 95% CI ‐2.32 to 0.02 n=2079) and diastolic blood pressure (MD ‐0.80 mmHg, 95% CI ‐1.37 to ‐0.23 n=2079) in normotensives and greater reductions in systolic blood pressure in hypertensives (MD ‐4.14 mmHg, 95% CI ‐5.84 to ‐2.43 n=675), but no difference in diastolic blood pressure (MD ‐3.74 mmHg, 95% CI ‐8.41 to 0.93 n=675).
Overall many of the trials failed to report sufficient detail to assess their potential risk of bias. Health‐related quality of life was assessed in one trial in normotensives, which reported significant improvements in well‐being but no data were presented.
Authors' conclusions
Despite collating more event data than previous systematic reviews of randomised controlled trials, there is insufficient power to confirm clinically important effects of dietary advice and salt substitution on cardiovascular mortality in normotensive or hypertensive populations. Our estimates of the clinical benefits from advice to reduce dietary salt are imprecise, but are larger than would be predicted from the small blood pressure reductions achieved. Further well‐powered studies would be needed to obtain more precise estimates. Our findings do not support individual dietary advice as a means of restricting salt intake. It is possible that alternative strategies that do not require individual behaviour change may be effective and merit further trials.
Plain language summary
Reduced dietary salt for the prevention of cardiovascular disease
Cardiovascular disease includes heart attacks and strokes and is a major cause of premature death and disability. This is an update of a review first published in 2011. This review sets out to assess whether intensive support and encouragement to cut down on salt in foods, and substituting low‐sodium salt, reduces the risk of death or cardiovascular disease. This update includes two new studies and eliminates one problematic study, giving a total of eight trials with 7284 participants.
Dietary advice and salt substitution did reduce the amount of salt eaten, which led to a small reduction in blood pressure by six months. There was weak evidence of benefit for cardiovascular events, but these findings were inconclusive and were driven by a single trial among retirement home residents, which reduced salt intake in the kitchens of the homes.
The findings of our review do not mean that advising people to reduce salt should be stopped. However, additional measures ‐ reducing the amount of hidden salt in processed foods, for example – will make it much easier for people to achieve a lower salt diet. Overall many of the trials failed to report sufficient detail to assess their potential risk of bias. Further evidence of the effects of different ways of reducing dietary salt on clinical events is needed from experimental and observational studies to underpin public health policies.
Background
In 2010 it was estimated that nearly 12.9 million deaths (a quarter of the global total) were due to ischaemic heart disease and stroke (Lozano 2012). Morbidity data are more difficult to collect because there are so many different measures of cardiovascular morbidity. However, in 2010 ischaemic heart disease was globally the number one cause of disability adjusted life years (DALYs) lost each year, with nearly 130 million DALYs (Allender 2008). Similarly, high blood pressure was the number one risk factor, with over 170 million DALYs lost globally each year (Murray 2013).
Globally, high blood pressure is a leading risk factor for cardiovascular disease, contributing over 7% of the global DALYs in 2010 (Lim 2012). The relationship of salt intake to blood pressure is the basis for the belief that restriction of dietary sodium intake will prevent blood pressure‐related cardiovascular events (Elliot 1996). The public health recommendations of a decade ago remain in place: to reduce salt intake by about half, i.e. from approximately 10 to 5 g/day (Dietary Guidelines for Americans 2010; He 2010; SACN 2003; Whelton 2002; Whelton 2012), and they have also been endorsed in current World Health Organization guidelines on sodium intake (WHO 2012).
Data from observational studies have indicated that a high dietary intake of salt is an important risk factor for cardiovascular disease (He 2002; He 2010). Short‐term intervention studies, including the Dietary Approaches to Stop Hypertension (DASH) trials, have shown decreases in systolic blood pressure in all groups (Sacks 2001). This was confirmed by a systematic review and meta‐analysis of 13 prospective studies including 177,000 participants, which reported a greater risk of stroke in those with higher salt intakes (relative risk 1.23, 95% CI 1.06 to 1.43) (Strarzzullo 2009). However, in this review the association between salt intake and all cardiovascular events was smaller (relative risk 1.14, 95% CI 0.99 to 1.31) and with the exclusion of one study statistical significance was achieved (relative risk 1.17, 95% CI 1.02 to 1.32), but all‐cause mortality was not reported. The interpretation of this observational evidence base is complicated by the heterogeneity in estimating sodium intake (diet or urinary salt excretion), types of participants (healthy, hypertensive, obese and non‐obese), endpoints and the definition of outcomes across studies (Alderman 2010). A more recent review of observational studies reported no strong evidence of an effect on all‐cause mortality (relative risk 1.06, 95% CI 0.94 to 1.20) and similar inconclusive effects on cardiovascular disease (relative risk 1.12, 95% CI 0.93 to 1.34), noting that the quality of evidence was generally low due to non‐randomised designs (Aburto 2013).
Following publication of the 2011 Cochrane review, commentators have put forward a view that the relationship between dietary sodium intake and cardiovascular events may be J‐shaped, suggesting that lowering sodium beyond a certain point may not be beneficial (Alderman 2011; Alderman 2012; Mente 2013). Several prospective cohort studies have been published recently that overcome the problem of dietary sodium assessment by using urinary sodium excretion as an index of dietary intake. These have shown a possible J‐shaped relationship: low sodium intake (< 3 g/day) is associated with no lower rate of cardiovascular disease, and perhaps a higher rate (Ekinci 2011; O'Donnell 2011; Stolarz‐Skrzypek 2011). In light of these studies, the US Institute of Medicine reviewed the evidence and found that it supported population‐based efforts to lower excessive dietary salt intake, but not the lowering of intakes to < 2.3 g sodium/day (Institute of Medicine 2013). Commentary on the new recommendations has suggested that the scientific debates, our earlier Cochrane review and difficulties in interpreting the evidence only provide opportunities for the food industry to avoid regulation of salt in their products (Neal 2013). Others consider that we still have insufficient evidence to decide whether to advise people to reduce their salt intake below current average levels (Mente 2013). A recent review of four decades of the salt and health debate concludes that the evidence available from different eras has been unable to resolve the debate satisfactorily (Bayer 2012).
A number of meta‐analyses of randomised controlled trials of salt reduction and blood pressure have been undertaken (He 2004; Jürgens 2004). Whilst these analyses consistently report a reduction in the level of blood pressure with reduced salt intake, the level of blood pressure reduction achieved is less impressive in the longer term. The 2004 Cochrane review of dietary salt restriction intervention studies of at least six months' duration found that intensive support and encouragement to reduce salt intake lowered blood pressure at 13 to 60 months, but only by a small amount (systolic by 1.1 mmHg, 95% CI 1.8 to 0.4; diastolic by 0.6 mmHg, 95% CI 1.5 to ‐0.3) (Hooper 2004). These findings of small blood pressure reductions among normotensive people were confirmed in a recent Cochrane review, which demonstrated much smaller blood pressure reductions in normotensives (about 1% in systolic blood pressure) and greater reductions in hypertensive people (around 3.5%) (Graudal 2011). Certainly the very large estimated effects of salt reduction using both trial and observational data are no longer considered plausible (Law 1991). The most recent review has continued the questionable practice of combining both short and longer duration trials: among 34 trials of 3230 participants with four or more weeks (median four to five weeks) of follow‐up, the mean change in blood pressure was ‐4 mmHg for systolic and ‐2 mmHg for diastolic blood pressure, although heterogeneity was marked with I² estimates of between 68% and 75% (He 2013a; He 2013b). Such estimates are unlikely to reflect the reductions in blood pressure that can be obtained in the general normotensive population in practice. However, even small sustained reductions in mean blood pressure of 2 to 3 mmHg would be sufficient for important population reductions in cardiovascular events (Elliot 1991).
In a previous version of this review a trial of salt restriction in patients with heart failure was included (Paterna 2008). We have now excluded this trial following the retraction by the editors of Heart journal of a meta‐analysis including this paper (Editor's Note 2013). Trials of salt restriction in heart failure are no longer within the scope of this review.
Whilst our earlier Cochrane review also sought to assess the impact of dietary salt restriction advice on mortality and cardiovascular events, across the 11 randomised controlled trials included there were only 17 deaths spread evenly across groups and 46 cardiovascular events in the controls compared with 36 in the low‐sodium diet groups (Hooper 2004). The small number of events limited the ability of this earlier review to detect small to moderate reductions in the risk of cardiovascular events.
Given that the effect of interventions to reduce dietary salt on blood pressure is well established and health policy in the area of salt reduction has advanced, the primary focus of this review is to confirm whether reducing dietary salt through advice or substitution is associated with improvements in mortality and cardiovascular events.
Objectives
To assess the long‐term effects of advice and salt substitution, aimed at reducing dietary salt, on mortality and cardiovascular morbidity.
To investigate whether a reduction in blood pressure is an explanatory factor in the effect of such dietary interventions on mortality and cardiovascular outcomes.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs), individual or cluster level, with follow‐up of at least six months.
Types of participants
Studies in adults (18 years or older), irrespective of gender or ethnicity. We excluded studies in patients with heart failure, children or pregnant women.
Types of interventions
Reducing dietary salt intake, either by advice from health professionals or provision of low‐sodium salt substitution. The comparison group could include usual, control or placebo diet, or no intervention.
Types of outcome measures
Primary outcomes
All‐cause mortality.
Cardiovascular mortality.
Cardiovascular morbidity (including fatal and non‐fatal myocardial infarction, stroke, angina, heart failure, peripheral vascular events, sudden death, revascularisation (coronary artery bypass surgery or angioplasty with or without stenting) and cardiovascular‐related hospital admissions).
We assessed primary outcomes at study end and also at the latest trial follow‐up, where participants had been followed observationally after the end of the original trial.
Secondary outcomes
In studies that reported the primary outcomes we also sought the following secondary outcomes:
Changes in systolic and diastolic blood pressure.
Urinary salt excretion (or other method of estimation of salt intake).
Health‐related quality of life using a validated outcome measure (e.g. Short Form 36, McHorney 1993).
Search methods for identification of studies
Electronic searches
We updated the searches, initially run in 2008 (Appendix 1), and re‐ran these on 1 May 2013 (Appendix 2). We searched the following databases:
Cochrane Central Register of Controlled Trials (CENTRAL) (2013, Issue 4);
MEDLINE (OVID, 1946 to April week 3 2013);
EMBASE Classic + EMBASE (OVID, 1947 to 30 April 2013);
CINAHL Plus with Full Text (EBSCO, to 1 April 2013);
PsycINFO (OVID, 1806 to October 2008 ‐ not updated as resources were limited);
Health Technology Assessment (HTA) on The Cochrane Library (2008, Issue 4 ‐ not updated as resources were limited);
Database of Abstracts of Reviews of Effects (DARE) on The Cochrane Library (2008, Issue 4 ‐ not updated as resources were limited).
Searches conducted in MEDLINE, EMBASE, CINAHL and PsycINFO included a controlled trials filter in 2008. We updated this in 2013 to the Cochrane sensitivity‐maximising RCT filter for MEDLINE and adaptations of it for EMBASE and CINAHL (Lefebvre 2011). We limited the searches in MEDLINE, EMBASE and CINAHL by entry dates/weeks to identify only newly added records since the last search. We limited the CENTRAL search by publication dates.
We applied no language restrictions.
Searching other resources
We searched reference lists of all eligible trials and relevant systematic reviews for additional studies.
Data collection and analysis
Selection of studies
Two authors (KA and RST) independently screened the titles and abstracts of studies identified by the original search and discarded clearly irrelevant studies. In order to be selected, abstracts had to identify clearly the study design, an appropriate population and a relevant intervention/exposure, as described above. We obtained the full‐text reports of all potentially relevant studies and two authors (KA and RST) assessed these independently for eligibility, based on the defined inclusion criteria. We resolved any disagreement by discussion or where agreement could not be reached, by consultation with an independent third person (LH). For the update, two authors (AJA, FCT or NM) independently screened half the abstracts. A third author (NM) checked 10% of all studies. Two authors (AJA and FCT) checked full‐text articles of potentially relevant studies. A third author (NM) checked all excluded studies.
Data extraction and management
We used standardised data extraction forms. We extracted relevant data regarding inclusion criteria (study design, participants, intervention/exposure and outcomes), risk of bias (see below) and outcome data. A single author (KA or RST) carried out data extraction and a second author (RST or KA) checked this. We resolved disagreements by discussion or, if necessary, with a third author (LH). We extracted outcomes at the latest follow‐up point within the trial, and also at the latest follow‐up after the trial where this was available, as we reasoned this would maximise the number of events reported. We contacted all included study authors to clarify any missing outcome data or issues of 'Risk of bias' assessment. For the update, two authors (AJA or FCT and SE) carried out data extraction independently.
Assessment of risk of bias in included studies
Factors considered included random sequence generation and allocation concealment, description of drop‐outs and withdrawals, blinding (participants, personnel and outcome assessment) and selective outcome reporting. In addition we sought evidence that the groups were balanced at baseline, that intention‐to‐treat analysis was undertaken and that the period over which the salt intervention lasted and follow‐up of outcome were equivalent. A single author (KA) assessed the risk of bias of the included studies and a second author (RST) checked this. We resolved disagreements by discussion or if necessary with a third author (LH). Two authors (AJA and FCT) independently checked risk of bias in the update.
Data synthesis
We processed data as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). For mortality and cardiovascular events, we calculated the risk ratio and 95% confidence interval (CI) for each trial. For blood pressure and urinary sodium excretion, we calculated mean group differences and 95% CI using the mean difference. We explored heterogeneity amongst included studies qualitatively (by comparing the characteristics of included studies) and quantitatively (using the Chi² test of heterogeneity and the I² statistic). We combined results from included studies for each outcome to give an overall estimate of treatment effect at the latest point available within the randomised trial and, as a secondary analysis, at the latest point available (including where participants were followed up after the end of the randomisation period). We used a fixed‐effect meta‐analysis except where statistical heterogeneity was identified (Chi² P value ≤ 0.05 and I² value ≥ 50%), in which case we considered methodological and clinical reasons for heterogeneity and used a random‐effects model.
Subgroup analysis and investigation of heterogeneity
We planned to use stratified meta‐analysis to explore the differential effects that might occur as a result of: individual advice versus group advice, salt substitution versus advice and baseline risk of cardiovascular disease. We used meta‐regression to assess the effects of the level of salt reduction achieved, baseline blood pressure and change in blood pressure on mortality and cardiovascular event outcomes.
Sensitivity analysis
We conducted sensitivity analysis of the primary outcomes to determine whether cluster and individually randomised trial designs influenced the effects observed.
Results
Description of studies
Results of the search
The searches in 2013 retrieved 2439 references and 1861 remained after de‐duplication. We excluded 1737 references based on screening the title and abstract. We retrieved the remaining 124 references in full text, two of which met the inclusion criteria (two reports) (CSSS 2007; Kwok 2012). We also identified three additional reports for previously included studies.
The searches in 2008 identified a total of 2649 titles, of which we excluded 2605 on title and abstract. After examining the full texts of the remaining 44 papers, we included six trials (26 reports) (Chang 2006; HPT 1990; Morgan 1978; TOHP I 1992; TOHP II 1997; TONE 1998).
Five studies from an earlier Cochrane review, Hooper 2004, met the inclusion criteria (HPT 1990; Morgan 1978; TOHP I 1992 (18 months); TOHP II 1997; TONE 1998). We excluded the other six included studies from Hooper 2004, as they did not report mortality or cardiovascular events (Alli 1992; Arroll 1995; Costa 1981; Morgan 1987; Silman 1983; Thaler 1982).
In total, we included eight trials (reported in 31 papers) and one ongoing study (Aung 2012).
We obtained responses to our requests for additional details from four of the included trial authors (Kwok 2012; TOHP I 1992; TOHP II 1997; TONE 1998).
The study selection process is summarised in the flow diagram shown in Figure 1.
1.
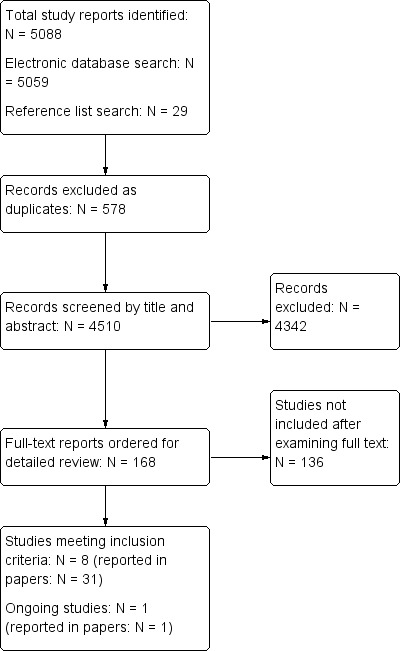
578Study flow diagram for review and update
Included studies
The eight included studies are described in the Characteristics of included studies table.
We included three trials in people with normotension (n = 3518) (HPT 1990; TOHP I 1992; TOHP II 1997), two in people with hypertension (n = 748) (Morgan 1978; TONE 1998), and three in a mixed population of people with normo‐ and hypertension (n = 3018) (Chang 2006; CSSS 2007; Kwok 2012). For the purposes of analysis, we included studies in mixed normo‐ and hypertensive individuals with the hypertensive studies.
Post‐randomisation follow‐up varied from up to six to nine months (Morgan 1978), to around three‐years (Chang 2006; HPT 1990), and long‐term post‐trial end follow‐up of 10 to 15 years (TOHP I 1992; TOHP II 1997; TONE 1998).
The three normotensive trials were in healthy people (predominantly white (> 75%), male (75%), median age 40) and were conducted in the USA. Entry criteria varied between trials, but included those with diastolic blood pressure from 78 mmHg to 89 mmHg, with a narrow range of means from 83 mmHg to 86 mmHg diastolic and 124 mmHg to 127 mmHg systolic. The number of participants included ranged from 392 to 2382.
All three trials in normotensives (as well as TONE 1998, below) aimed to reduce salt by comprehensive dietary and behaviour change programmes led by experienced personnel, including regular group counselling sessions over several months, with newsletters between sessions, self assessment, goal setting, food tasting and recipes. For example, the Hypertension Prevention Trial (HPT) ran 10 weekly group counselling sessions on food selection, food preparation and behaviour management skills, followed by semi‐monthly and then bi‐monthly meetings throughout the trial (with newsletters in the months where no meetings occurred) (HPT 1990). Sessions were run by nutritionists and behavioural scientists and individual counselling was provided, where participants missed sessions or had special needs. Techniques used in the sessions included group discussions, instructions for dietary record keeping, goal setting, individual diet analysis for each participant, cooking demonstrations, provision of recipe books and tasting of new foods. The intervention duration ranged from seven months (TONE 1998) to 36 months (TOHP II 1997). Control groups received no active intervention. Sodium excretion goals were set at less than 70 to 80 mmol/24 hours. Only two studies used salt substitution; one gradually increased the use of a potassium‐enriched salt substitute over several weeks, although this was done in kitchens by cooks without requiring participants to alter their behaviours (Chang 2006), and the other advised participants to use a low‐sodium salt substitute (CSSS 2007).
The five trials that included hypertensives included one trial in treated hypertensive participants (TONE 1998), two that included participants with untreated hypertension (Chang 2006; Morgan 1978), one study with a proportion of treated participants (CSSS 2007) and one unspecified (Kwok 2012). In the mixed studies, the per cent with hypertension ranged from 40% (Chang 2006) to 60% (Kwok 2012). Studies were carried out in Australia, China, Hong Kong,Taiwan and the USA and ranged in size from 77 to 1981 participants. Between 15% and 100% of participants were male, with a median age of 60 years.Most studies did not report ethnicity. At study entry mean diastolic blood pressure ranged from 71 mmHg (Chang 2006; TONE 1998, on treatment) to 97 mmHg (Morgan 1978, untreated) and systolic blood pressure ranged from approximately 131 mmHg (Chang 2006, untreated; TONE 1998, on treatment) to 162 mmHg (Morgan 1978, untreated).
Sodium goals varied from < 80 mmol/day (TONE 1998) to 70 to 100 mmol/day and unspecified sodium intake (Chang 2006).
Excluded studies
Studies that were close to meeting but did not meet our inclusion criteria are listed in the Characteristics of excluded studies table.
Risk of bias in included studies
A number of studies failed to give sufficient detail to assess their potential risk of bias.
Details of the generation and concealment of the random allocation sequence were particularly poorly reported (Figure 2; Figure 3). However, in all cases there was objective evidence of balance in the baseline characteristics of the intervention and control participants.
2.
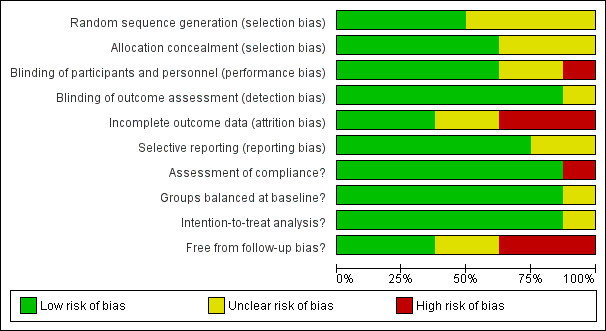
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
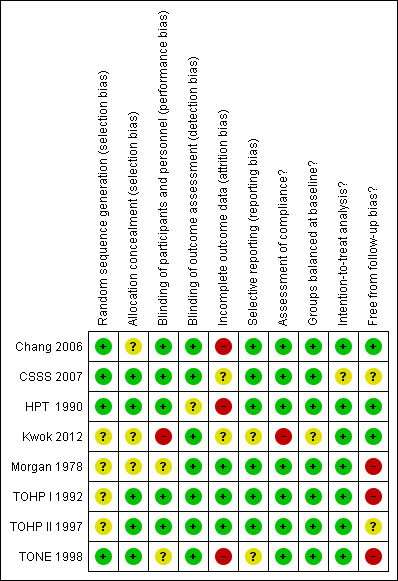
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
For blinding of outcome assessment we assumed there to be low risk of bias, as the primary outcomes of mortality and major cardiovascular disease morbidity are unlikely to be wrongly assessed based on participant allocation.
While studies reported loss to follow‐up and reasons for loss to follow‐up, only a few undertook a sensitivity or imputation analysis to assess the impact of these losses, followed up participants for event outcomes and described reasons for loss to follow‐up for other outcomes. In the Trial of Nonpharmacologic Intervention in the Elderly (TONE) trial, the authors stated that data were collected via psychological questionnaires at randomisation and a number of the follow‐up visits (TONE 1998). However, none of these data were found in the trial reports. Although often not stated, all studies appeared to undertake an intention‐to‐treat analysis in that groups were analysed according to initial random allocation.
All studies assessed compliance with the salt reduction intervention using diet diaries or monitoring of use. However, in the longer‐term post‐trial end follow‐up of the TOHP I (11.5 years), TOHP II (eight years) and TONE (12.7 years) trials, such compliance data were not reported beyond the official end of the study (TOHP I 1992; TOHP II 1997; TONE 1998). Therefore it was unclear whether intervention groups were encouraged to continue their low‐salt diets long‐term, or returned to their pre‐trial diet. Similarly, in the control groups it is not clear whether they were left to continue with their usual diet or advised to reduce their salt at the end of the trial.
Effects of interventions
Given the heterogeneity of populations and the likelihood that normotensives and hypertensives would differ in their adherence to dietary interventions, the results are presented and pooled separately for studies of people with normotension and hypertension. We pooled outcomes at end of trial and at the longest follow‐up point unless otherwise indicated.
Primary outcomes
All‐cause mortality
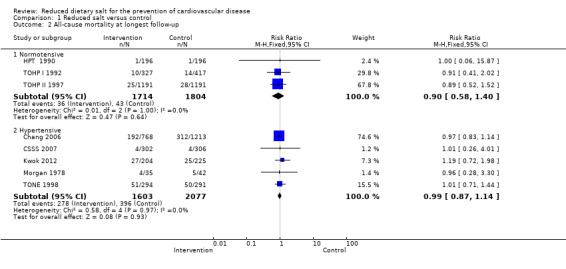
All‐cause mortality was reported at the end of the trial in seven of the included studies (Chang 2006; CSSS 2007; HPT 1990; Kwok 2012; Morgan 1978; TOHP I 1992; TOHP II 1997). Trials were homogeneous and therefore we pooled them using a fixed‐effect model. There was no strong evidence of a reduction in the number of deaths in the reduced salt group relative to controls for the normotensive (fixed‐effect risk ratio (RR) 0.67, 95% confidence interval (CI) 0.40 to 1.12, 60 deaths in total, I² = 0%) or hypertensive populations (fixed‐effect RR 1.00, 95% CI 0.86 to 1.15, 565 deaths in total, I² = 0%) (Analysis 1.1).
1.1. Analysis.
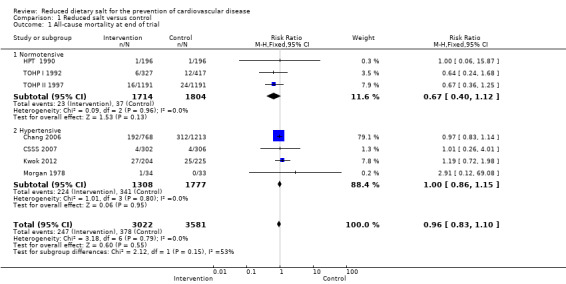
Comparison 1 Reduced salt versus control, Outcome 1 All‐cause mortality at end of trial.
A longer observational follow‐up following the end of the randomised trial period was reported for the Trials of Hypertension Prevention (TOHP) I (11.5 years) and TOHP II (eight years) trials (Cook 2007). We were also able to obtain longer observational unpublished data from the authors from the Trial of Nonpharmacologic Intervention in the Elderly (TONE) study (12.7 years) (TONE 1998). Trials remained homogeneous. At longest follow‐up, there was still no evidence of a reduction in the number of deaths in the reduced salt group relative to controls, for the normotensive (fixed‐effect RR 0.90, 95% CI 0.58 to 1.40, 79 deaths in total, I² = 0%) or hypertensive populations (fixed‐effect RR 0.99, 95% CI 0.87 to 1.14, 674 deaths; I² = 0%) (Analysis 1.2).
1.2. Analysis.
Comparison 1 Reduced salt versus control, Outcome 2 All‐cause mortality at longest follow‐up.
Cardiovascular mortality
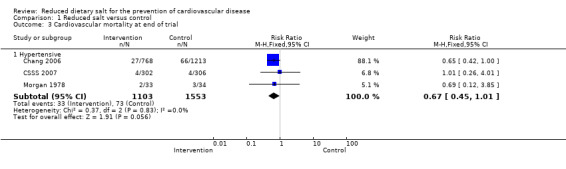
Cardiovascular mortality was reported in three studies including hypertensive patients. Chang 2006 reported a lower proportion of cardiovascular deaths in the intervention group than in the control group (27 versus 66) and contributed 90% weight to this analysis. Importantly, dietary salt was substituted gradually with a potassium‐rich, low‐salt product in the kitchens used by residents in retirement homes. Morgan 1978 reported only one cardiovascular death in the intervention group and none in the control group, but in a subsequent publication two cardiovascular deaths were reported in each of the intervention and control groups (Morgan 1980). There was no difference in the other study (CSSS 2007). The pooled risk ratio shows weak, inconclusive evidence of benefit (fixed‐effect RR 0.67, 95% CI 0.45 to 1.01, 106 cardiovascular deaths, I² = 0%) (Analysis 1.3).
1.3. Analysis.
Comparison 1 Reduced salt versus control, Outcome 3 Cardiovascular mortality at end of trial.
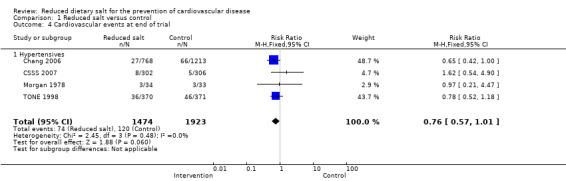
Cardiovascular morbidity
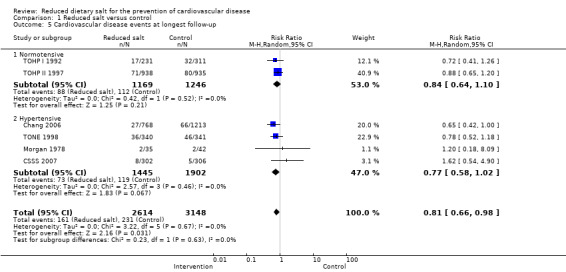
We assessed cardiovascular events (both fatal and non‐fatal) at end of trial. The definition of non‐fatal cardiovascular events varied from trial to trial, although it broadly consisted of a composite of myocardial infarction, stroke, coronary artery bypass and percutaneous transluminal coronary angioplasty. Data at end of trial were only available in trials of hypertensives (Chang 2006; CSSS 2007; Morgan 1978; TONE 1998), and demonstrated weak evidence of a reduction in events (fixed‐effect RR 0.76, 95% CI 0.57 to 1.01, 192 events, I² = 0%) (Analysis 1.4). Cardiovascular events at longest follow‐up were also examined to maximise the number of events available for analysis and gain data for normotensives. Data were available from six trials (Chang 2006; CSSS 2007; HPT 1990; Morgan 1978; TOHP I 1992; TOHP II 1997). Following long‐term observational follow‐up, TOHP I and II reported no strong evidence of risk reduction, with heterogeneity of effect between the two trials in normotensive participants (random‐effects RR 0.84, 95% CI 0.64 to 1.10). We found weak evidence of benefit in hypertensive individuals (fixed‐effect RR 0.77, 95% CI 0.58 to 1.02; I2 = 0%). Pooling across normotensive and hypertensive trials gives modest evidence of benefit for cardiovascular events at longest follow‐up (random‐effects RR 0.81, 95% CI 0.66 to 0.98; I2 = 0%) (Analysis 1.5).
1.4. Analysis.
Comparison 1 Reduced salt versus control, Outcome 4 Cardiovascular events at end of trial.
1.5. Analysis.
Comparison 1 Reduced salt versus control, Outcome 5 Cardiovascular disease events at longest follow‐up.
Secondary outcomes
Changes in systolic and diastolic blood pressure
End of trial blood pressure was reported by five studies (HPT 1990; Morgan 1978; TOHP I 1992; TOHP II 1997; TONE 1998). CSSS 2007 reported end of trial blood pressure but did not provide standard deviations (SD), so we imputed the median SD of the other studies to include the findings in the pooled analysis using the methodology outlined in section 7.7.3.3 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Kwok 2012 did not report end of trial blood pressure but stated that there was no difference between intervention and control groups. For systolic blood pressure there was evidence of substantial statistical heterogeneity in the normotensive groups, but not the hypertensive studies. Systolic blood pressure was reduced in all intervention arms: normotensives (random‐effects mean difference (MD) ‐1.15 mmHg, 95% CI ‐2.32 to 0.02, I² = 64%) and hypertensives (random‐effects MD ‐4.14 mmHg, 95% CI ‐5.84 to ‐2.43, I² = 0%). Combining normotensives and hypertensives resulted in substantial heterogeneity (I² = 74%) and moderate evidence of benefit (random‐effects MD ‐1.79 mmHg, 95% CI ‐3.23 to ‐0.36). Diastolic blood pressure was also reduced in normotensives (random‐effects MD ‐0.80 mmHg, 95% CI ‐1.37 to ‐0.23, I² = 0%), but not in hypertensives (random‐effects MD ‐3.74 mmHg, 95% CI ‐8.41 to 0.93, I² = 67%). In this analysis there was no heterogeneity in normotensives, but substantial heterogeneity in hypertensives. Pooled analysis of normotensives and hypertensives showed moderate evidence of an effect (random‐effects MD ‐1.17 mmHg, 95% CI ‐2.08 to ‐0.26) (Analysis 1.6; Analysis 1.7).
1.6. Analysis.
Comparison 1 Reduced salt versus control, Outcome 6 Systolic blood pressure at end of trial.
1.7. Analysis.
Comparison 1 Reduced salt versus control, Outcome 7 Diastolic blood pressure at end of trial.
Urinary salt excretion (or other method of estimation of salt intake)
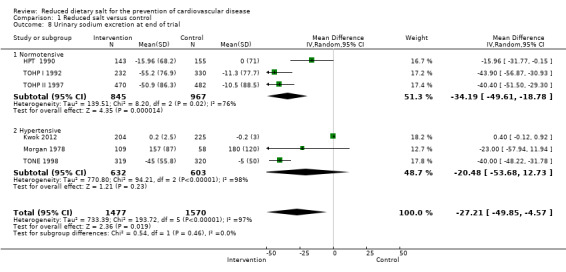
Changes in urinary sodium excretion at the end of trial were reported by six studies (HPT 1990; Kwok 2012; Morgan 1978; TOHP I 1992; TOHP II 1997; TONE 1998). There was substantial evidence of statistical heterogeneity, which may reflect different approaches to the assessment of 24‐hour urinary sodium excretion. In the study by Morgan, results were only reported as samples and therefore comprised repeated observations for a number of patients (Morgan 1978). As for blood pressure, in a number of studies the last urinary sodium excretion value available was at a time point much preceding the timing of the reported mortality or cardiovascular events (blood pressure follow‐up time: six months (Morgan 1978); 30 months (TONE 1998); 18 months (TOHP I 1992); 36 months (TOHP II 1997)). Urinary 24‐hour sodium excretion was reduced by a similar amount across the study subgroups: normotensives (random‐effects MD ‐34.19 mmol/24 hours, 95% CI ‐49.61 to ‐18.78, I² = 76%); hypertensives (random‐effects MD ‐20.48 mmol/24 hours, 95% CI ‐53.68 to 12.73, I² = 98%) and pooled analysis (random‐effects MD ‐27.21 mmol/24 hours, 95% CI ‐49.85 to ‐4.57, I² = 97%) (Analysis 1.8).
1.8. Analysis.
Comparison 1 Reduced salt versus control, Outcome 8 Urinary sodium excretion at end of trial.
Health‐related quality of life
One study in normotensives reported that significant improvements on the Psychological General Well‐Being scale were observed at six and 18 months, but no data were presented (TOHP I 1992).
Subgroup analyses and investigation of heterogeneity
In order to take to take account of the heterogeneity in populations and cardiovascular baseline risk, we stratified meta‐analyses according to whether studies were undertaken in normotensive or hypertensive populations. As one of the studies involved a kitchen salt substitution rather than requiring participants to change their behaviours, we conducted a subgroup analysis excluding this trial (Chang 2006). This resulted in reductions in the pooled effects observed (cardiovascular mortality at end of trial: RR 0.87, 95% CI 0.30 to 2.55; cardiovascular events at end of trial: RR 0.86, 95% CI 0.57 to 1.30; cardiovascular events at longest follow‐up: RR 0.81, 95% CI 0.63 to 1.03). As this trial did not measure blood pressure or urinary sodium excretion we were not able to explore its effects on these outcomes.
Small study bias
Given the small number of included studies it was not possible to assess small study bias either statistically or using a funnel plot.
Sensitivity analysis
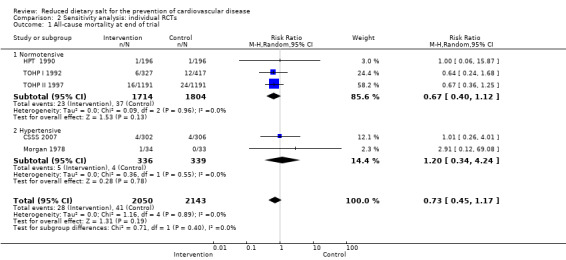
We conducted sensitivity analysis for the primary outcomes by removing the Kwok 2012 and Chang 2006 studies as they were cluster‐randomised trials. Both studies were carried out in hypertensives, so results for normotensives remained unchanged. Chang 2006 was the largest study conducted in hypertensives, so the overall result of removing it was to reduce the sample size and considerably decrease the precision of the estimate. For the primary outcome all‐cause mortality at end of trial, the two removed trials had accounted for 86.9% of the weight, thus the sensitivity analysis increased the relative weight of the TOHP I 1992 and TOHP II 1997 trials. As a result, even though the pooled estimate for hypertensives was higher in sensitivity analysis, the pooled estimate was lower than the main analysis but with less precision (RR 0.73, 95% CI 0.45 to 1.17, 69 events, 4193 participants) (Analysis 2.1). For cardiovascular mortality, removing the cluster‐randomised trials decreased the effect estimate and decreased the precision (RR 0.87, 95% CI 0.29 to 2.64, 13 events, 675 participants) (Analysis 2.2). For cardiovascular disease events at end of trial, removing Chang 2006 resulted in TONE 1998 increasing in weight to 84.5% of the estimate, and resulted in salt reduction showing less evidence of an effect (RR 0.86, 95% CI 0.57 to 1.30, 101 events, 1416 participants) (Analysis 2.3).
2.1. Analysis.
Comparison 2 Sensitivity analysis: individual RCTs, Outcome 1 All‐cause mortality at end of trial.
2.2. Analysis.

Comparison 2 Sensitivity analysis: individual RCTs, Outcome 2 Cardiovascular mortality at end of trial.
2.3. Analysis.
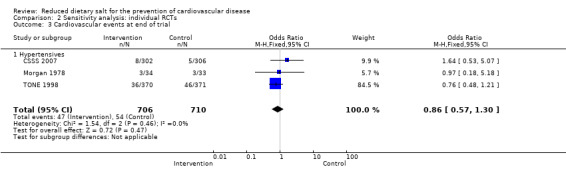
Comparison 2 Sensitivity analysis: individual RCTs, Outcome 3 Cardiovascular events at end of trial.
Discussion
Summary of main results
This Cochrane review identified eight randomised controlled trials that assessed the long‐term (more than six months) effects of interventions aimed at reducing dietary salt on mortality and cardiovascular morbidity. Three trials were in normotensives (HPT 1990; TOHP I 1992; TOHP II 1997, n = 3518 participants), two in hypertensives (Morgan 1978; TONE 1998, n = 748 participants) and three in mixed populations of normo‐ and hypertensives (Chang 2006; CSSS 2007; Kwok 2012, n = 3018 participants).
We found no strong evidence that dietary advice or substitution to reduce salt intake reduced all‐cause mortality in normotensives (end of trial risk ratio (RR) 0.67, 95% confidence interval (CI) 0.40 to 1.12, 60 deaths, 3518 participants; longest follow‐up RR 0.90, 95% CI 0.58 to 1.40, 79 deaths, 3518 participants), or in hypertensives (end of trial RR 1.00, 95% CI 0.86 to 1.15, 565 deaths, 3085 participants; longest follow‐up RR 0.99, 95% CI 0.87 to 1.14, 674 deaths, 3680 participants).
There was weak evidence that cardiovascular mortality and cardiovascular events were reduced among hypertensives (cardiovascular mortality: end of trial RR 0.67, 95% CI 0.45 to 1.01, 106 deaths, 2656 participants; cardiovascular events: end of trial RR 0.76, 95% CI 0.57 to 1.01, 194 deaths, 3397 participants), however these results were strongly driven by the Chang 2006 study, which accounted for 88% of the weight in the cardiovascular mortality analysis and 49% of the weight in cardiovascular events analysis. There was no strong evidence that cardiovascular events (fatal and non‐fatal combined) were reduced in people with normal blood pressure (longest follow‐up RR 0.71, 95% CI 0.42 to 1.20, 200 events, 2505 participants), but in hypertensives there was weak evidence of benefit (longest follow‐up RR 0.77, 95% CI 0.57 to 1.02, 192 events, 3407 participants). Maximising the available data by pooling across normotensive and hypertensive groups and using the data collected by some trials after the trial end date gave a 'significant' result (RR 0.77, 95% CI 0.63 to 0.95, P value < 0.01). This result was driven by the trial of residents in institutions where salt reduction was achieved by changes in salt used in the institution kitchens (Chang 2006). Excluding this trial from the analysis gave an overall effect of RR 0.81 (95% CI 0.63 to 1.03) for cardiovascular events at longest follow‐up. Both TOHP I 1992 and TOHP II 1997 were carried out in overweight individuals (average body mass index (BMI) in TOHP I 27.1, mean BMI in TOHP II 30.9 in both intervention and control), so the effects of dietary advice to reduce salt found in this trial may not be applicable to non‐overweight people.
Although no data were published on participant's health‐related quality of life, in one trial among normotensives it was reported that there were significant improvements in quality of life in the intervention group (TOHP I 1992).
The interventions reduced urinary sodium excretion and indicated that participants continued to comply with sodium restriction in the long term, at least to some degree, although, as noted in a previous Cochrane review, the degree of sodium restriction is likely to attenuate over time (Hooper 2004). End of trial systolic and diastolic blood pressure were reduced by an average of 1 mmHg in normotensives and by an average of 2 to 4 mmHg in hypertensives.
Sustained long‐term reductions of diastolic blood pressure of 1 mmHg and 4 mmHg would be predicted to reduce cardiovascular disease mortality by 5% and 20% respectively (MacMahon 1990). Our point estimates among hypertensives are consistent with effects of this size, but have wide confidence intervals owing to the relatively small number of events. Among normotensives our point estimate of benefit is rather larger (about a 30% risk reduction in cardiovascular events), which probably reflects the use of the long‐term follow‐up data from the TOHP I and II trials These provide the only relevant data but they may be biased by losses to follow‐up for non‐fatal events and no data on blood pressure or urinary sodium excretion were available to assess the extent to which participants had maintained trial values (Cook 2007). The systolic blood pressure reduction in the TOHP I and II trials was between 1 mmHg and 2 mmHg, which would not be expected to produce such a large reduction in cardiovascular events.
Findings from sensitivity analysis excluding cluster‐randomised trials are less precise, but overall are consistent with the main analysis.
Overall completeness and applicability of evidence
A previous Cochrane review was limited by the lack of reported events (17 deaths, 93 cardiovascular events) (Hooper 2004). In this review, because of longer observational follow‐up (up to 10 to 15 years) of three of the trials included in the previous Cochrane review (TOHP I 1992; TOHP II 1997 (eight years); TONE 1998 (12.7 years)) and inclusion of one more recent randomised controlled trial (RCT) (Chang 2006), we have gathered more evidence on mortality and cardiovascular outcomes (approximately 7200 participants, 753 deaths and 392 cardiovascular events). Nevertheless, the total amount of evidence on events remains limited. The question arises of how much more evidence would be required to give a conclusive answer on the benefits of advice to reduce salt intake. Assuming a 15% risk of suffering a cardiovascular event over 10 years (consistent with mild hypertension at age 60 in a man), a trial with 80% power and a significance level of 5% would require randomisation of about 25,000 people to intervention and control arms with follow‐up for 10 years to detect a 10% reduction in cardiovascular events. However, targeting a 20% reduction in cardiovascular events ‐ similar to the effects of antihypertensives or statins in primary prevention of cardiovascular disease ‐ and a shorter follow‐up of five years would require a more feasible trial of 12,000 participants. The randomised evidence to support antihypertensive drug treatment comprises over 120,000 participants followed for about five years and provides conclusive evidence of benefit. Despite over a decade of advocacy for salt reduction as a major public health strategy, it is remarkable that an evidence base a 10th of the size of the equivalent pharmacological database has been produced. Doing better than this is considered impracticable because of logistic, financial and ethical issues (He 2011).
More recently, the US Institute of Medicine, in its review of the evidence on salt and health, has recommended further trials to examine the effects of a range of sodium levels on the risk of cardiovascular events, stroke and mortality among patients in controlled environments, where randomised trials may be more feasible, and in natural experiments (Institute of Medicine 2013). In response to this the TOHP I and II trial investigators reported long‐term observational findings from the control groups of these trials, which did not show a J‐shaped association but indicated that urinary sodium excretion is linearly associated with cardiovascular events, although only 10% of the participants had urinary sodium excretions of below 2300 mg/24 hours (Cook 2014), a little higher than the level of 2000 mg/24 hours recommended by the World Health Organization (WHO 2012). In contrast, an observational cohort analysis was unable to demonstrate a clear linear relationship between urinary sodium excretion and coronary heart disease events, although a weak interaction between urinary sodium excretion and plasma N‐terminal pro‐B‐type natriuretic peptide on coronary heart disease events was reported (Joosten 2014). Reviewing these new studies, Whelton stated that "... the potential for reverse causality, bias in assessment of sodium intake, absent or insufficient adjustment for confounding variables, and random error" all contribute to inconsistent findings (Whelton 2014).
Quality of the evidence
Although all included studies were RCTs, only two of the eight included studies provided sufficient detail to be judged as having adequate random sequence generation, allocation concealment and outcome blinding. One cluster‐randomised trial was analysed as if it was individually randomised (Chang 2006). Nevertheless, all trials provided evidence of baseline balance. Although lack of blinding is unlikely to alter outcome assessment when outcomes include mortality and cardiovascular events, failure to blind participants may have led to a positive change in the lifestyle and dietary behaviours of control participants, leading to a reduction in the difference between groups.
Most trials appeared to be free from dietary changes in the intervention and control groups, apart from dietary sodium. The one major exception was the trial by Chang where sodium was replaced by a high‐potassium substitute (Chang 2006). Potassium has beneficial effects on blood pressure but may have adverse effects in individuals with renal disease (Cappuccio 2000). Two studies in hypertensives allowed changes in antihypertensive medication during the period of the trial (Morgan 1978; TONE 1998). In both trials, lower levels of hypertensive medication in the intervention group compared to control may have reduced the blood pressure‐lowering effect of reduced dietary sodium and therefore offset mortality and cardiovascular morbidity benefits.
Potential biases in the review process
We searched comprehensively for randomised controlled trials of dietary sodium reduction, with a duration of six months or more and which reported mortality or cardiovascular events. We attempted to contact all authors of included studies to verify events. Nevertheless, we were unable to report all relevant outcomes for all trials. The small number of included studies prevented us from being able to assess the presence of small study or publication bias.
By incorporating data from the longest follow‐up point, we sought to maximise the number of deaths and cardiovascular events that might be affected by alterations in dietary salt. However, in doing so we may have introduced a source of bias as not all trials conducted long‐term follow‐up. For three large studies (TOHP I 1992, TOHP II 1997 (eight years), TONE 1998 (12.7 years)), the longest follow‐up was considerably beyond the official end of the trial and therefore can no longer be assumed to represent a randomised comparison. It was unclear if the intervention groups continued their low‐salt diets and whether control groups were left to continue with dietary advice or advised to reduce their salt. For this reason we consider the trial end findings to be a more robust, albeit less precise, source of evidence.
In common with previous systematic reviews of dietary interventions, we observed marked heterogeneity across studies in terms of their population, sample size and follow‐up. Whilst we stratified meta‐analysis by differing sub‐populations (normotensives and hypertensives) and pooled studies using weighting based on sample size, we did not account for the duration of follow‐up. A previous Cochrane review suggests that over time the sodium reduction achieved is greatly reduced, as is the effect on blood pressure and therefore the effect on events is potentially diminished (Hooper 2004). In a systematic review of trials of dietary salt reduction, sodium excretion was about half that in the two trials of over one‐year duration compared with the other trials with a median duration of four to five weeks (He 2013a; He 2013b), indicating that long‐term blood pressure reductions would be smaller with commensurate reductions in clinical benefit.
Agreements and disagreements with other studies or reviews
Our finding of a lack of strong evidence of an effect of dietary sodium reduction advice on mortality and cardiovascular events in our 2011 Cochrane review was strongly contested on the grounds that we failed to consider the totality of the epidemiological, animal and short‐duration trials of blood pressure reduction, and that if we had pooled across people with and without hypertension our findings would have achieved statistical significance (He 2011). The effects of dietary salt advice are greater in people with hypertension (possibly because of greater adherence) and underlying risks of cardiovascular disease are higher, which was our rationale for providing separate analyses. Indeed, the 'significant' effect that He and MacGregor achieved becomes 'non‐significant' depending on whether the odds ratio (0.78, 95% CI 0.61 to 0.99, P value =0.045) or rate ratio (0.88, 95% CI 0.77 to 1.00, P value = 0.054) is estimated, indicating the limitations of the available evidence and the problem of basing decisions on arbitrary thresholds of statistical significance (Taylor 2011). Another Cochrane review examining the physiological effects of dietary salt reduction in a 167 trials found a 1% decrease in blood pressure in normotensives, a 3.5% decrease in hypertensives, a significant increase in plasma renin, plasma aldosterone, plasma adrenaline and plasma noradrenaline, a 2.5% increase in cholesterol and a 7% increase in triglyceride. The authors concluded, "There were increases in some hormones and lipids which could be harmful if persistent over time. However, the studies were not designed to measure long‐term health effects. Therefore we do not know if low‐salt diets improve or worsen health outcomes." (Graudal 2011). In a further Cochrane review, restricted to 34 trials of at least four weeks duration, there was no strong evidence of these hormonal and lipid effects, suggesting that they may not be long‐term problems (He 2013a; He 2013b).
In light of the limited randomised evidence, non‐randomised observational evidence has been reviewed and meta‐analysed. In a review of prospective observational studies that examined the relationship between dietary sodium and cardiovascular events (Strarzzullo 2009), 13 cohort studies (177,025 participants) with follow‐up of 3 to 17 years were included. Higher salt intake was associated with a greater risk of stroke (pooled relative risk 1.23, 95% CI 1.06 to 1.43, 5161 events) and cardiovascular events (pooled relative risk 1.14, 95% CI 0.99 to 1.32, 5346 events). Total and cardiovascular mortality were not reported. A more recent update of this review reported inconclusive findings for all‐cause mortality and cardiovascular events, but did report an increased risk of coronary mortality (pooled relative risk 1.32, 95% CI 1.13 to 1.53) and stroke events (pooled relative risk 1.24, 95% CI 1.08 to 1.43) in those with high salt intakes (Aburto 2013). The inherent limitation of both of these reviews is the observational nature of the evidence on clinical outcomes, i.e. the studies describe the life course of persons who follow a self selected diet, unlike in randomised trials where allocation is at random and not self selected. People who choose a lower‐salt diet are likely also to eat a diet of fresh foods, lower in fats and refined carbohydrate, take more exercise and be less likely to smoke, so that their lower levels of deaths and disease may not relate to salt intake at all.
Dietary advice appears to be only modestly effective at reducing salt intake and consequently has only small effects on blood pressure, particularly in the general population. Alternative means of reducing dietary salt intake include salt substitution, which may be relatively easy to implement in institutional and workplace kitchens as indicated in the one trial of an institutional kitchen intervention in this review (Chang 2006). Experience in the United Kingdom and elsewhere has demonstrated that voluntary regulation, with the threat of government legislation, by the food industry has resulted in reductions in dietary sodium intake, although the effects have been small (a reduction from 9.5 g/day to 8.6 g/day but remaining a long way from a target of 6 g/day (Cappuccio 2011; Millett 2012). Evidence from other countries suggests that regulatory approaches are needed (Webster 2011), and are cost‐saving compared with dietary advice, which is not cost‐effective in Australian scenarios (Cobiac 2010). In a recent review of the evidence, Whelton considered that "... a gradual decrease in the addition of Na to food products represents the easiest "lifestyle" change for the general population and the intervention option with the greatest potential for success" (Whelton 2014). In most countries, establishing means of monitoring progress, both in terms of population levels of dietary salt intake and blood pressure, will be essential.
Authors' conclusions
Implications for practice.
Despite collating more event data than previous systematic reviews of randomised controlled trials, there is insufficient power to confirm clinically important effects of dietary advice and salt substitution on cardiovascular mortality in normotensive or hypertensive populations. The methods of achieving salt reduction (advice and salt substitution) in the trials included in our review, and other systematic reviews, were relatively modest in their impact on sodium excretion and on blood pressure levels. They generally required considerable efforts to implement and would not be expected to have an effect on the burden of cardiovascular disease commensurate with their costs. The challenge for clinical and public health practice is to find more effective interventions for reducing salt intake that are both practicable and inexpensive.
Many countries have national authoritative recommendations, often sanctioned by government, which call for reduced dietary sodium. In the UK, the National Institute of Health and Care Excellence (NICE) has recently called for an acceleration of the reduction in salt intake of the general population from a maximum intake of 6 g per day per adult by 2015 to 3 g by 2025 (NICE 2010).
Implications for research.
Further long‐term follow‐up of existing trials (as done by Trials of Hypertension Prevention (TOHP) I, TOHP II and Trial of Nonpharmacologic Intervention in the Elderly (TONE)) may contribute further events to allow assessment of the long‐term effects of reduced dietary salt advice on mortality, cardiovascular morbidity and hormonal and lipid outcomes, although the intensive dietary advice interventions evaluated in trials over the last three decades are of less relevance to current policy initiatives. Our findings support the recent US Institute of Medicine recommendation for further rigorous, large, long‐term studies, capable of demonstrating the cardiovascular benefit of dietary salt reduction beyond reasonable doubt using a range of plausible interventions. Such trials need to assess population level (e.g. workplace, institutional, regulatory) interventions that might be more likely to lead to sustained reductions in salt intake and which would provide evidence relevant to current public health guidelines. It will also be important to evaluate the effects of voluntary and regulatory salt reduction by food industries (such as the UK's reduction of salt in processed foods) on dietary salt intake and blood pressure, as these may hold greater opportunities for practicable and inexpensive means of reducing salt intake in the population at large.
Feedback
Analysis queries, 27 February 2017
Summary
My first two points are mainly based on a paper by O’Donnell et al (1) which drew my attention to some of the numbers used in the Cochrane review by Adler et al (2). The focus is on Analysis 1.5 (Cardiovascular disease events at longest follow‐up) in the Cochrane review.
1) A total number of patients is 321 for TOHP I in the reduced salt group in Analysis 1.5. However, there were 17 events among 231 patients in the intervention group versus 32 events among 311 patients in the control group considering cardiovascular disease as shown in Table 2 in BMJ (3).
2) The authors indicate in “Characteristics of included studies” that in TONE trial 340 and 341 patients were randomized into intervention and control group, respectively. However, these respective numbers are 370 and 371 in Analysis 1.5. The number of patients randomized into sodium reduction and usual care were 340 and 341, respectively, based on Figure 1 and Table 1 in Whelton et al (4). In Table 3, however, the numbers are 370 and 371 (4).
Interestingly, from Table 3 one gets a total of 1035 (370+147+147+371) patients randomized not 975 as stated in the abstract (4). However, one gets a total of 975 patients with the use of Figure 1 and Table 1 from Whelton et al (4).
The number of patients with end‐point known were 332 and 331 in sodium reduction and usual care, respectively, based on Figure 1 (4). The numbers (events/total) were 36/332 for salt reduction and 46/331 for control group in O’Donnell et al (1). Evidently, the patients with end‐point known were used as denominators (i.e. available case‐analysis as per Cochrane Handbook Chapter 16).
3) There is a slight discrepancy between number of patients shown in “Characteristics of included studies” and in Analysis 1.5 (33 versus 35 patients allocated to intervention) considering Morgan et al (5). However, 35 patients seems to be in line with Table 2 (5).
In addition, there are 2 events in both salt reduction and control group in Analysis 1.5. However, there are 3 events in both groups in Analysis 1.4. In other words, there are fewer events with longer (Analysis 1.5) compared to shorter (Analysis 1.4) follow‐up period which seems, at least to me, counterintuitive.
References
O’Donnell MJ, et al. Salt intake and cardiovascular disease: why are the data inconsistent? Eur Heart J 2013;34:1034‐40.
Adler AJ, et al. Reduced dietary salt for the prevention of cardiovascular disease. Cochrane Database Syst Rev 2014;12:CD009217.
Cook NR, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow‐up of the trials of hypertension prevention (TOHP). BMJ 2007;334:885‐8.
Whelton PK, et al. Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of nonpharmacologic interventions in the elderly (TONE). JAMA 1998;279:839‐46.
Morgan TO, et al. Failure of therapy to improve prognosis in elderly males with hypertension. Med J Aust 1980;2:27‐31.
Reply
The number of participants in the intervention group for TOHP I has been corrected to 231 which changes the RR from 0.77 (95% 0.63 to 0.95) to 0.81 (95% CI 0.66 to 0.98) but does not change the conclusions (Analysis 1.5). The questions raised about TONE reflect a “per‐protocol” vs “intention to treat (ITT)” analysis debate. Whelton et al seem to have chosen an ITT analysis and this is what was used for Analysis 1.5. This does not change the result (and changes the subgroup results only minutely). O’Donnell uses an available‐case analysis which is another option. Both ways are acceptable according to Cochrane. The discrepancy between number of patients shown in “Characteristics of included studies” and in Analysis 1.5 may be because at the longest follow‐up 1 participants in each group with previous cardiovascular events are now counted as deaths.
Contributors
Feedback submitted by: Jesper M Kivelä, Institute of Clinical Medicine, University of Helsinki, Finland
Response composed by: Bill Cayley (Cochrane Heart Feedback Editor) and Nicole Martin
What's new
| Date | Event | Description |
|---|---|---|
| 3 July 2017 | Feedback has been incorporated | Feedback and response incorporated. |
History
Review first published: Issue 7, 2011
| Date | Event | Description |
|---|---|---|
| 1 May 2014 | New citation required but conclusions have not changed | Two new studies included. Conclusions not changed. |
| 1 May 2014 | New search has been performed | Searches re‐run in May 2013. |
| 6 June 2013 | Amended | The Paterna trial has now been retracted and we have removed the data from this trial from the review. |
| 13 March 2013 | Amended | Doubts have been raised about the integrity of research from the Paterna group. The previously published results should be discounted for now. |
| 1 September 2011 | Amended | Amended 'Plain language summary'. |
| 6 July 2011 | Amended | Corrected typo error in 'Abstract ‐ Results' section. |
Notes
Following doubts raised about the integrity of research from the Paterna group and retraction of a publication by this group (Heart 2013), we have now removed this trial and its data from this review.
Acknowledgements
This review was supported by a UK NIHR Cochrane Collaboration Programme grant: 'Cochrane Heart Public Health and Prevention Reviews' CPGS10. We would like to acknowledge the work of previous authors on this review: Kate Ashton, Tiffany Moxham and Lee Hooper.
Appendices
Appendix 1. Search strategies 2008
The Cochrane Library (2008, Issue 4)
Results for CENTRAL, Health Technology Assessment (HTA) and Database of Abstracts of Reviews of Effect (DARE)
Search date: 3 November 2008
#1 MeSH descriptor Heart Arrest explode all trees #2 (cardiac NEAR/3 arrest*):ti,ab,kw #3 (heart NEAR/3 arrest*):ti,ab,kw #4 (cardiopulmonary NEAR/3 arrest*):ti,ab,kw #5 (sudden NEAR/3 death):ti,ab,kw #6 asystole*:ti,ab,kw #7 (myocard* NEAR/2 contract*):ti,ab,kw #8 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7) #9 (death* or died or dead or fatal*):ti,ab #10 mortality:ti,ab. #11 (#9 OR #10) #12 MeSH descriptor Cerebrovascular Disorders explode all trees #13 (stroke* or poststroke* or cva*):ti,ab #14 (cerebrovascular* or (cerebral adj vascular)):ti,ab #15 (cerebral or cerebellar or brain* or vertebrobasilar):ti,ab #16 (infarct* or isch*emi* or thrombo* or emboli* or apoplexy):ti,ab #17 (cerebral or intracerebral or intracranial or brain* or parenchymal or intraventricular or cerebellar or infratentorial or supratentorial or subarachnoid):ti,ab #18 (haemorrhage or hemorrhage or bleed* or haematoma or hematoma or aneurysm):ti,ab #19 (#15 AND #16) #20 (#17 AND #18) #21 (trans* isch*emic attack*):ti,ab #22 brain attack:ti,ab #23 MeSH descriptor Hemiplegia explode all trees #24 (hemipleg* or hemipar* or post NEXT stroke):ti,ab #25 (#21 OR #22 OR #23 OR #24) #26 (#12 OR #13 OR #14 OR #19 OR #20 OR #25) #27 MeSH descriptor Intermittent Claudication explode all trees #28 claudica*:ti,ab #29 MeSH descriptor Peripheral Vascular Diseases explode all trees #30 MeSH descriptor Vascular Diseases, this term only #31 (peripher* NEAR/3 (occlu* or arteri* or vascular)):ti,ab #32 (arterial NEAR/3 (obstruct* or occlus*)):ti,ab #33 MeSH descriptor Arteriosclerosis Obliterans, this term only #34 MeSH descriptor Atherosclerosis, this term only #35 MeSH descriptor Arterial Occlusive Diseases, this term only #36 ((leg or limb) NEAR/3 (isch*emia or occlusi*)):ti,ab #37 (arteriosclerosis or atherosclerosis):ti,ab #38 MeSH descriptor Femoral Artery, this term only #39 MeSH descriptor Popliteal Artery, this term only #40 MeSH descriptor Iliac Artery, this term only #41 ((femoral or renal or iliac) NEAR/3 artery):ti,ab #42 (occlu* or obstruct*):ti,ab #43 (#38 OR #39 OR #40 OR #41) #44 (#42 AND #43) #45 (#27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37) #46 (#44 OR #45) #47 MeSH descriptor Heart Failure explode all trees #48 MeSH descriptor Myocardial Ischemia explode all trees #49 angina:ti,ab #50 (angor pectoris):ti,ab #51 myocard*:ti,ab #52 MeSH descriptor Ventricular Dysfunction explode all trees #53 (ventricular NEAR/2 failure):ti,ab #54 revascular*:ti,ab #55 (isch*mi* NEAR/3 heart):ti,ab,kw #56 coronary:ti,ab,kw #57 MeSH descriptor Angioplasty explode all trees #58 MeSH descriptor Angioplasty, Transluminal, Percutaneous Coronary, this term only #59 (PTCA or angioplast*):ti,ab #60 MeSH descriptor Myocardial Revascularization, this term only #61 stenocardia*:ti,ab #62 (heart NEAR/3 decompensation):ti,ab #63 MeSH descriptor Myocardial Infarction explode all trees #64 (heart NEAR/3 infarc*):ti,ab #65 (heart NEAR/3 failure):ti,ab,kw #66 cardiac*:ti,ab #67 CABG:ti,ab #68 MeSH descriptor Coronary Artery Bypass explode all trees #69 (heart NEAR/3 bypass):ti,ab,kw #70 (#47 OR #48 OR #49 OR #50 OR #51 OR #52 OR #53 OR #54 OR #55 OR #56 OR #57 OR #58 OR #59 OR #60) #71 (#61 OR #62 OR #63 OR #64 OR #65 OR #66 OR #67 OR #68 OR #69) #72 (#70 OR #71) #73 (cardiovascular NEAR/3 (outcome* or morbidity or event*)):ti,ab,kw #74 (hospital* or admission*):ti,ab #75 (#73 OR #74) #76 (#8 OR #11 OR #26 OR #46 OR #72 OR #75) #77 MeSH descriptor Sodium, Dietary explode all trees #78 MeSH descriptor Diet, Sodium‐Restricted explode all trees #79 MeSH descriptor Sodium, this term only #80 MeSH descriptor Sodium Chloride explode all trees #81 (#79 OR #80) #82 (restrict* or low* or reduc* or intak* or added or diet):ti,ab #83 (consum* or excess* or increas* or high*):ti,ab #84 (#82 OR #83) #85 (#84 AND #81) #86 (urin* or excret*):ti,ab #87 (#80 AND #86) #88 (restrict* NEAR/3 (salt or sodium)):ti,ab,kw #89 (low* NEAR/3 (salt or sodium)):ti,ab,kw #90 (reduc* NEAR/3 (salt or sodium)):ti,ab,kw #91 (intak* NEAR/3 (salt or sodium)):ti,ab,kw #92 (change NEAR/3 (salt or sodium)):ti,ab,kw #93 (consum* NEAR/3 (salt or sodium)):ti,ab,kw #94 (excess* NEAR/3 (salt or sodium)):ti,ab,kw #95 (sodium NEAR/3 (urin* or excret*)):ti,ab,kw #96 (increas* NEAR/3 (salt or sodium)):ti,ab,kw #97 (high* NEAR/3 (salt or sodium)):ti,ab,kw #98 (added NEAR/3 (salt or sodium or food)):ti,ab,kw #99 (diet* and (salt or sodium)):ti,ab,kw #100 (#77 OR #78 OR #85 OR #87 OR #88 OR #89 OR #90 OR #91 OR #92 OR #93 OR #94 OR #95 OR #96 OR #97 OR #98 OR #99) #101 (#76 AND #100)
Ovid MEDLINE(R) 1950 to October Week 4 2008
Search date: 29 October 2008
1 Randomized controlled trial.pt. 2 randomized controlled trial/ 3 (random$ or placebo$).ti,ab,sh. 4 ((singl$ or double$ or triple$ or treble$) and (blind$ or mask$)).tw,sh. 5 or/1‐4 6 "controlled clinical trial".pt. 7 (retraction of publication or retracted publication).pt. 8 6 or 7 or 5 9 exp Sodium, Dietary/ 10 exp Diet, Sodium‐Restricted/ 11 Sodium/ 12 Sodium Chloride/ 13 11 or 12 14 (restrict* or low* or reduc* or intak* or added).tw. or diet*.mp. 15 (consum* or excess* or increas* or high*).tw. 16 14 or 15 17 13 and 16 18 (urin* or excret*).tw. 19 12 and 18 20 (restrict* adj3 (salt or sodium)).mp. 21 (low* adj3 (salt or sodium)).mp. 22 (reduc* adj3 (salt or sodium)).mp. 23 (intak* adj3 (salt or sodium)).mp. 24 (change adj3 (salt or sodium)).mp. 25 (consum* adj3 (salt or sodium)).mp. 26 (excess* adj3 (salt or sodium)).mp. 27 (sodium adj3 (urin* or excret*)).mp. 28 (increas* adj3 (salt or sodium)).mp. 29 (high* adj3 (salt or sodium)).mp. 30 (added adj3 (salt or sodium or food)).mp. 31 (diet* and (salt or sodium)).tw. 32 9 or 10 or 17 or 19 or (or/20‐31) 33 exp Heart Arrest/ 34 (cardiac adj3 arrest*).mp. 35 (heart adj3 arrest*).mp. 36 (cardiopulmonary adj3 arrest*).mp. 37 (sudden adj3 death).mp. 38 asystole*.mp. 39 (myocard* adj2 contract*).mp. 40 or/33‐39 41 (death* or died or dead or fatal*4).ti,ab. 42 mortality.ti,ab. 43 41 or 42 44 exp Cerebrovascular Disorders/ 45 (stroke* or poststroke* or cva*).tw. 46 (cerebrovascular* or (cerebral adj vascular)).tw. 47 (cerebral or cerebellar or brain* or vertebrobasilar).tw. 48 (infarct* or isch?emi* or thrombo* or emboli* or apoplexy).tw. 49 (cerebral or intracerebral or intracranial or brain$ or parenchymal or intraventricular or cerebellar or infratentorial or supratentorial or subarachnoid).tw. 50 (haemorrhage or hemorrhage or bleed$ or haematoma or hematoma or aneurysm).tw. 51 48 and 47 52 49 and 50 53 trans* isch?emic attack*.tw. 54 brain attack.tw. 55 hemiplegia/ 56 (hemipleg* or hemipar* or post‐stroke).tw. 57 54 or 55 or 56 or 53 58 51 or 44 or 52 or 46 or 57 or 45 59 Intermittent Claudication/ 60 claudica*.ti,ab. 61 exp Peripheral Vascular Diseases/ 62 Vascular Diseases/ 63 (peripher* adj3 (occlu* or arteri* or vascular)).ti,ab. 64 (arterial adj3 (obstruct* or occlus*)).ti,ab. 65 Arteriosclerosis Obliterans/ 66 Atherosclerosis/ 67 ARTERIAL OCCLUSIVE DISEASES/ 68 ((leg or limb) adj3 (isch?emia or occlusi*)).ti,ab. 69 (arteriosclerosis or atherosclerosis).ti,ab. 70 Femoral Artery/ 71 POPLITEAL ARTERY/ 72 ILIAC ARTERY/ 73 ((femoral or renal or iliac) adj3 artery).ti,ab. 74 (occlu* or obstruct*).ti,ab. 75 73 or 72 or 71 or 70 76 75 and 74 77 or/59‐69 78 76 or 77 79 40 or 43 or 58 or 78 80 exp Heart Failure/ 81 exp Myocardial Ischemia/ 82 angina.tw. 83 angor pectoris.tw. 84 myocard*.tw. 85 Ventricular Dysfunction/ 86 (ventricular adj2 failure).tw. 87 revascular*.ti,ab. 88 (isch?mi* adj3 heart).ti,ab,sh. 89 coronary.ti,ab,sh. 90 exp Angioplasty/ 91 Angioplasty, Transluminal, Percutaneous Coronary/ 92 (PTCA or angioplast*).tw. 93 Myocardial Revascularization/ 94 stenocardia*.tw. 95 (heart adj3 decompensation).tw. 96 exp Myocardial Infarction/ 97 (heart adj3 infarc*).tw. 98 (heart adj3 failure).ti,ab,sh. 99 cardiac*.tw. 100 CABG.tw. 101 exp coronary artery bypass/ 102 (heart adj3 bypass).tw,sh. 103 or/80‐102 104 (cardiovascular adj3 (outcome* or morbidity or event*)).mp. [mp=title, original title, abstract, name of substance word, subject heading word] 105 (hospital* or admission*).tw. 106 104 or 105 107 103 or 106 or 58 or 78 or 43 or 40 108 32 and 107 109 (animals not humans).sh. 110 exp Case Reports/ 111 letter.pt. 112 (news or editorial).pt. 113 111 or 110 or 112 114 108 not 113 115 114 not 109 116 8 and 115
EMBASE OVID SP <1980 to 2008 Week 43>
Search date: 30 October 2008
1 sodium intake/ 2 sodium restriction/ 3 Sodium/ 4 Sodium Chloride/ 5 3 or 4 6 (restrict* or low* or reduc* or intak* or added).tw. or diet*.mp. 7 (consum* or excess* or increas* or high*).tw. 8 6 or 7 9 5 and 8 10 (urin* or excret*).tw. 11 4 and 10 12 (restrict* adj3 (salt or sodium)).mp. 13 (low* adj3 (salt or sodium)).mp. 14 (reduc* adj3 (salt or sodium)).mp. 15 (intak* adj3 (salt or sodium)).mp. 16 (change adj3 (salt or sodium)).mp. 17 (consum* adj3 (salt or sodium)).mp. 18 (excess* adj3 (salt or sodium)).mp. 19 (sodium adj3 (urin* or excret*)).mp. 20 (increas* adj3 (salt or sodium)).mp. 21 (high* adj3 (salt or sodium)).mp. 22 (added adj3 (salt or sodium or food)).mp. 23 (diet* and (salt or sodium)).tw. 24 1 or 2 or 9 or 11 or (or/12‐23) 25 exp Heart Arrest/ 26 (cardiac adj3 arrest*).mp. 27 (heart adj3 arrest*).mp. 28 (cardiopulmonary adj3 arrest*).mp. 29 (sudden adj3 death).mp. 30 asystole*.mp. 31 (myocard* adj2 contract*).mp. 32 or/25‐31 33 (death* or died or dead or fatal*4).ti,ab. 34 mortality.ti,ab. 35 33 or 34 36 exp Cerebrovascular Disease/ 37 (stroke* or poststroke* or cva*).tw. 38 (cerebrovascular* or (cerebral adj vascular)).tw. 39 (cerebral or cerebellar or brain* or vertebrobasilar).tw. 40 (infarct* or isch?emi* or thrombo* or emboli* or apoplexy).tw. 41 (cerebral or intracerebral or intracranial or brain$ or parenchymal or intraventricular or cerebellar or infratentorial or supratentorial or subarachnoid).tw. 42 (haemorrhage or hemorrhage or bleed$ or haematoma or hematoma or aneurysm).tw. 43 40 and 39 44 41 and 42 45 trans* isch?emic attack*.tw. 46 brain attack.tw. 47 hemiplegia/ 48 (hemipleg* or hemipar* or post‐stroke).tw. 49 46 or 47 or 48 or 45 50 43 or 36 or 44 or 38 or 49 or 37 51 Intermittent Claudication/ 52 claudica*.ti,ab. 53 exp Peripheral Vascular Disease/ 54 Vascular Disease/ 55 (peripher* adj3 (occlu* or arteri* or vascular)).ti,ab. 56 (arterial adj3 (obstruct* or occlus*)).ti,ab. 57 Arteriosclerosis Obliterans/ 58 Atherosclerosis/ 59 Peripheral Occlusive Artery Disease/ 60 ((leg or limb) adj3 (isch?emia or occlusi*)).ti,ab. 61 (arteriosclerosis or atherosclerosis).ti,ab. 62 Femoral Artery/ 63 POPLITEAL ARTERY/ 64 ILIAC ARTERY/ 65 ((femoral or renal or iliac) adj3 artery).ti,ab. 66 (occlu* or obstruct*).ti,ab. 67 65 or 64 or 63 or 62 68 67 and 66 69 or/51‐61 70 68 or 69 71 exp Heart Failure/ 72 exp Heart Muscle Ischemia/ 73 angina.tw. 74 angor pectoris.tw. 75 myocard*.tw. 76 Heart Ventricle Function/ 77 (ventricular adj2 failure).tw. 78 revascular*.ti,ab. 79 (isch?mi* adj3 heart).ti,ab,sh. 80 coronary.ti,ab,sh. 81 exp Angioplasty/ 82 exp Transluminal Coronary Angioplasty/ 83 (PTCA or angioplast*).tw. 84 exp Heart Muscle Revascularization/ 85 stenocardia*.tw. 86 (heart adj3 decompensation).tw. 87 exp Heart Infarction/ 88 (heart adj3 infarc*).tw. 89 (heart adj3 failure).ti,ab,sh. 90 cardiac*.tw. 91 CABG.tw. 92 exp Coronary Artery Bypass Graft/ 93 (heart adj3 bypass).tw,sh. 94 or/71‐93 95 (cardiovascular adj3 (outcome* or morbidity or event*)).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer name] 96 (hospital* or admission*).tw. 97 95 or 96 98 94 or 97 or 50 or 70 or 35 or 32 99 24 and 98 100 ((animal$ or Nonhuman$) not human$).sh,hw. 101 letter.pt. 102 editorial.pt. 103 102 or 101 or 100 104 99 not 103 105 Randomized Controlled Trial/ 106 Single Blind Procedure/ 107 Double Blind Procedure/ 108 Crossover Procedure/ 109 105 or 106 or 107 or 108 110 (random$ or factorial$ or crossover$ or placebo$ or (cross adj over) or assign$).ti,ab. 111 ((singl$ or double$ or triple$ or treble$) and (blind$ or mask$)).ti,ab. 112 controlled clinical trial*.ti,ab. 113 112 or 110 or 111 or 109 114 104 and 113
PsycINFO (OVID) 1806 to October Week 4 2008
1 (random$ or placebo$ or rct).tw,sh. 2 ((singl$ or double$ or triple$ or treble$) and (blind$ or mask$)).tw,sh. 3 ("2000" or treatment outcome clinical trial).md. 4 ((retract$ or withdraw$) adj (public$ or article$)).tw. 5 or/1‐4 6 Sodium/ 7 (diet and (salt or sodium)).mp. 8 (restrict* adj3 (salt or sodium)).mp. 9 (low* adj3 (salt or sodium)).mp. 10 (reduc* adj3 (salt or sodium)).mp. 11 (intak* adj3 (salt or sodium)).mp. 12 (change adj3 (salt or sodium)).mp. 13 (consum* adj3 (salt or sodium)).mp. 14 (excess* adj3 (salt or sodium)).mp. 15 (sodium adj3 (urin* or excret*)).mp. 16 (increas* adj3 (salt or sodium)).mp. 17 (high* adj3 (salt or sodium)).mp. 18 (added adj3 (salt or sodium or food)).mp. 19 or/6‐18 20 exp Heart Arrest/ 21 exp heart disorders/ 22 (cardiac adj3 arrest*).mp. 23 (heart adj3 arrest*).mp. 24 (cardiopulmonary adj3 arrest*).mp. 25 (sudden adj3 death).mp. 26 asystole*.mp. 27 (myocard* adj2 contract*).mp. 28 or/20‐27 29 (death* or died or dead or fatal*4).ti,ab. 30 mortality.ti,ab. 31 29 or 30 32 exp Cerebrovascular Disorders/ 33 (stroke* or poststroke* or cva*).tw. 34 (cerebrovascular* or (cerebral adj vascular)).tw. 35 (cerebral or cerebellar or brain* or vertebrobasilar).tw. 36 (infarct* or isch?emi* or thrombo* or emboli* or apoplexy).tw. 37 (cerebral or intracerebral or intracranial or brain$ or parenchymal or intraventricular or cerebellar or infratentorial or supratentorial or subarachnoid).tw. 38 (haemorrhage or hemorrhage or bleed$ or haematoma or hematoma or aneurysm).tw. 39 36 and 35 40 37 and 38 41 32 or 33 or 34 or 39 or 40 42 trans* isch?emic attack*.tw. 43 brain attack.tw. 44 hemiplegia/ 45 (hemipleg* or hemipar* or post‐stroke).tw. 46 43 or 44 or 45 or 42 47 claudica*.ti,ab. 48 (peripher* adj3 (occlu* or arteri* or vascular)).ti,ab. 49 (arterial adj3 (obstruct* or occlus*)).ti,ab. 50 Atherosclerosis/ 51 ((leg or limb) adj3 (isch?emia or occlusi*)).ti,ab. 52 (arteriosclerosis or atherosclerosis).ti,ab. 53 ((femoral or renal or iliac) adj3 artery).ti,ab. 54 (occlu* or obstruct*).ti,ab. 55 or/47‐54 56 Heart Failure.mp. 57 ischemia/ and myocard$.tw. 58 angina.tw. 59 angor pectoris.tw. 60 myocard*.tw. 61 Ventricular Dysfunction/ 62 (ventricular adj2 failure).tw. 63 revascular*.ti,ab. 64 (isch?mi* adj3 heart).ti,ab,sh. 65 coronary.ti,ab,sh. 66 heart surgery/ 67 (PTCA or angioplast*).tw. 68 stenocardia*.tw. 69 (heart adj3 decompensation).tw. 70 exp Myocardial Infarction/ 71 (heart adj3 infarc*).tw. 72 (heart adj3 failure).ti,ab,sh. 73 cardiac*.tw. 74 CABG.tw. 75 (heart adj3 bypass).tw,sh. 76 or/56‐75 77 (cardiovascular adj3 (outcome* or morbidity or event*)).mp. [mp=title, abstract, heading word, table of contents, key concepts] 78 (hospital* or admission*).tw. 79 77 or 78 80 editorial.dt. 81 letter.dt. 82 80 or 81 83 28 or 31 or 41 or 46 or 55 or 76 or 79 84 83 and 19 85 84 and 5 86 85 not 82 87 86 88 limit 87 to human
CINAHL
WEB 2.0
Search date: 3 November 2008
1 SODIUM CHLORIDE, DIETARY/ OR DIET, SODIUM‐RESTRICTED/ 2 SODIUM/ 3 SODIUM CHLORIDE/ 4 ((restrict* OR low* OR reduc* OR intak* OR added) OR diet*).ti,ab 5 ((consum* OR excess* OR increas* OR high*)).ti,ab 6 4 OR 5 7 6 AND (2 or 3) 8 ((urin* OR excret*)).ti,ab 9 3 AND 8 12 ((restrict* AND (salt OR sodium))).ti,ab 13 ((low* AND (salt OR sodium))).ti,ab 14 ((reduc* AND (salt OR sodium))).ti,ab 15 ((intak* AND (salt OR sodium))).ti,ab 16 ((change AND (salt OR sodium))).ti,ab 17 ((consum* AND (salt OR sodium))).ti,ab 18 ((excess* AND (salt OR sodium))).ti,ab 19 ((sodium AND (urin* OR excret*))).ti,ab 20 ((increas* AND (salt OR sodium))).ti,ab 21 ((high* AND (salt OR sodium))).ti,ab 22 ((added AND (salt OR sodium OR food))).ti,ab 23 ((diet* AND (salt OR sodium))).ti,ab 24 1 OR 7 OR 9 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 25 24 [Limit to: (Publication Type Clinical Trial or Systematic Review)] 26 ((placebo* OR random* OR rct)).ti,ab 27 (((singl* OR double* OR triple* OR treble*) AND (blind* OR mask*))).ti,ab 28 ((controlled clinical trial)).ti,ab 29 26 OR 27 OR 28 30 24 AND 29 31 25 OR 30 [Limit to: (Publication Type Clinical Trial or Systematic Review)]
Appendix 2. Search strategies 2013
CENTRAL
#1 MeSH descriptor: [Sodium, Dietary] explode all trees #2 MeSH descriptor: [Diet, Sodium‐Restricted] this term only #3 (restrict* near/3 (salt or sodium)) #4 (low* near/3 (salt or sodium)) #5 (reduc* near/3 (salt or sodium)) #6 (intak* near/3 (salt or sodium)) #7 (change near/3 (salt or sodium)) #8 (consum* near/3 (salt or sodium)) #9 (excess* near/3 (salt or sodium)) #10 (high* near/3 (salt or sodium)) #11 (diet* and (salt or sodium)) #12 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 #13 MeSH descriptor: [Cardiovascular Diseases] explode all trees #14 cardio* or cardia* or heart* or coronary* or angina* or ventric* or myocard* #15 pericard* or isch?em* or emboli* or arrhythmi* or thrombo* or atrial next fibrillat* #16 tachycardi* or endocardi* or sick near/3 sinus #17 MeSH descriptor: [Stroke] explode all trees #18 stroke or stokes or cerebrovasc* or apoplexy or cerebral next vascular #19 brain near/2 accident* #20 ((brain* or cerebral or lacunar) near/2 infarct*) #21 MeSH descriptor: [Hypertension] explode all trees #22 hypertensi* or peripheral next arter* next disease* #23 ((high or increased or elevated) near/2 blood pressure) #24 MeSH descriptor: [Hyperlipidemias] explode all trees #25 hyperlipid* or hyperlip?emia* or hypercholesterol* or hypercholester?emia* or hyperlipoprotein?emia* or hypertriglycerid?emia* #26 MeSH descriptor: [Arteriosclerosis] explode all trees #27 MeSH descriptor: [Cholesterol] explode all trees #28 cholesterol #29 "coronary risk factor*" #30 MeSH descriptor: [Blood Pressure] this term only #31 blood pressure #32 #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 #33 #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31 #34 #32 or #33 #35 #12 and #34
MEDLINE
1. exp Sodium, Dietary/ 2. Diet, Sodium‐Restricted/ 3. (restrict* adj3 (salt or sodium)).tw. 4. (low* adj3 (salt or sodium)).tw. 5. (reduc* adj3 (salt or sodium)).tw. 6. (intak* adj3 (salt or sodium)).tw. 7. (change adj3 (salt or sodium)).tw. 8. (consum* adj3 (salt or sodium)).tw. 9. (excess* adj3 (salt or sodium)).tw. 10. (high* adj3 (salt or sodium)).tw. 11. (diet* and (salt or sodium)).tw. 12. or/1‐11 13. exp Cardiovascular Diseases/ 14. cardio*.tw. 15. cardia*.tw. 16. heart*.tw. 17. coronary*.tw. 18. angina*.tw. 19. ventric*.tw. 20. myocard*.tw. 21. pericard*.tw. 22. isch?em*.tw. 23. emboli*.tw. 24. arrhythmi*.tw. 25. thrombo*.tw. 26. atrial fibrillat*.tw. 27. tachycardi*.tw. 28. endocardi*.tw. 29. (sick adj sinus).tw. 30. exp Stroke/ 31. (stroke or stokes).tw. 32. cerebrovasc*.tw. 33. cerebral vascular.tw. 34. apoplexy.tw. 35. (brain adj2 accident*).tw. 36. ((brain* or cerebral or lacunar) adj2 infarct*).tw. 37. exp Hypertension/ 38. hypertensi*.tw. 39. peripheral arter* disease*.tw. 40. ((high or increased or elevated) adj2 blood pressure).tw. 41. exp Hyperlipidemias/ 42. hyperlipid*.tw. 43. hyperlip?emia*.tw. 44. hypercholesterol*.tw. 45. hypercholester?emia*.tw. 46. hyperlipoprotein?emia*.tw. 47. hypertriglycerid?emia*.tw. 48. exp Arteriosclerosis/ 49. exp Cholesterol/ 50. cholesterol.tw. 51. "coronary risk factor* ".tw. 52. Blood Pressure/ 53. blood pressure.tw. 54. or/13‐53 55. 12 and 54 56. randomized controlled trial.pt. 57. controlled clinical trial.pt. 58. randomized.ab. 59. placebo.ab. 60. drug therapy.fs. 61. randomly.ab. 62. trial.ab. 63. groups.ab. 64. 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 65. exp animals/ not humans.sh. 66. 64 not 65 67. 55 and 66 68. (200810* or 200811* or 200812* or 2009* or 2010* or 2011* or 2012* or 2013*).ed. 69. 67 and 68
EMBASE
1. salt intake/ 2. sodium restriction/ 3. (restrict* adj3 (salt or sodium)).tw. 4. (low* adj3 (salt or sodium)).tw. 5. (reduc* adj3 (salt or sodium)).tw. 6. (intak* adj3 (salt or sodium)).tw. 7. (change adj3 (salt or sodium)).tw. 8. (consum* adj3 (salt or sodium)).tw. 9. (excess* adj3 (salt or sodium)).tw. 10. (high* adj3 (salt or sodium)).tw. 11. (diet* and (salt or sodium)).tw. 12. or/1‐11 13. exp cardiovascular disease/ 14. cardio*.tw. 15. cardia*.tw. 16. heart*.tw. 17. coronary*.tw. 18. angina*.tw. 19. ventric*.tw. 20. myocard*.tw. 21. pericard*.tw. 22. isch?em*.tw. 23. emboli*.tw. 24. arrhythmi*.tw. 25. thrombo*.tw. 26. atrial fibrillat*.tw. 27. tachycardi*.tw. 28. endocardi*.tw. 29. (sick adj sinus).tw. 30. exp cerebrovascular disease/ 31. (stroke or stokes).tw. 32. cerebrovasc*.tw. 33. cerebral vascular.tw. 34. apoplexy.tw. 35. (brain adj2 accident*).tw. 36. ((brain* or cerebral or lacunar) adj2 infarct*).tw. 37. exp hypertension/ 38. hypertensi*.tw. 39. peripheral arter* disease*.tw. 40. ((high or increased or elevated) adj2 blood pressure).tw. 41. exp hyperlipidemia/ 42. hyperlipid*.tw. 43. hyperlip?emia*.tw. 44. hypercholesterol*.tw. 45. hypercholester?emia*.tw. 46. hyperlipoprotein?emia*.tw. 47. hypertriglycerid?emia*.tw. 48. exp Arteriosclerosis/ 49. exp Cholesterol/ 50. cholesterol.tw. 51. "coronary risk factor*".tw. 52. Blood Pressure/ 53. blood pressure.tw. 54. or/13‐53 55. 12 and 54 56. random$.tw. 57. factorial$.tw. 58. crossover$.tw. 59. cross over$.tw. 60. cross‐over$.tw. 61. placebo$.tw. 62. (doubl$ adj blind$).tw. 63. (singl$ adj blind$).tw. 64. assign$.tw. 65. allocat$.tw. 66. volunteer$.tw. 67. crossover procedure/ 68. double blind procedure/ 69. randomized controlled trial/ 70. single blind procedure/ 71. 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 or 64 or 65 or 66 or 67 or 68 or 69 or 70 72. (animal/ or nonhuman/) not human/ 73. 71 not 72 74. 55 and 73 75. (20084* or 20085* or 2009* or 2010* or 2011* or 2012* or 2013*).em. 76. 74 and 75 77. limit 76 to embase
CINAHL
S54 S52 AND S53 S53 EM 20081101‐20130401 S52 S33 AND S51 S51 S34 or S35 or S36 or S37 or S38 or S39 or S40 or S41 or S42 or S43 or S44 or S45 or S46 or S47 or S48 or S49 or S50 S50 TX cross‐over* S49 TX crossover* S48 TX volunteer* S47 (MH "Crossover Design") S46 TX allocat* S45 TX control* S44 TX assign* S43 TX placebo* S42 (MH "Placebos") S41 TX random* S40 TX (doubl* N1 mask*) S39 TX (singl* N1 mask*) S38 TX (doubl* N1 blind*) S37 TX (singl* N1 blind*) S36 TX (clinic* N1 trial?) S35 PT clinical trial S34 (MH "Clinical Trials+") S33 S12 AND S32 S32 S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 S31 blood pressure S30 (MH "Blood Pressure") S29 "coronary risk factor*" S28 cholesterol S27 (MH "Cholesterol+") S26 (MH "Arteriosclerosis+") S25 hyperlipid* or hyperlip?emia* or hypercholesterol* or hypercholester?emia* or hyperlipoprotein?emia* or hypertriglycerid?emia* S24 (MH "Hyperlipidemia+") S23 ((high or increased or elevated) N2 blood pressure) S22 hypertensi* or peripheral arter* disease* S21 (MH "Hypertension+") S20 ((brain* or cerebral or lacunar) N2 infarct*) S19 brain N2 accident* S18 stroke or stokes or cerebrovasc* or apoplexy or cerebral next vascular S17 (MH "Stroke+") S16 tachycardi* or endocardi* or sick N3 sinus S15 pericard* or isch?em* or emboli* or arrhythmi* or thrombo* or atrial fibrillat* S14 cardio* or cardia* or heart* or coronary* or angina* or ventric* or myocard* S13 (MH "Cardiovascular Diseases+") S12 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 S11 (diet* and (salt or sodium)) S10 (high* N3 (salt or sodium)) S9 (excess* N3 (salt or sodium)) S8 (consum* N3 (salt or sodium)) S7 (change N3 (salt or sodium)) S6 (intak* N3 (salt or sodium)) S5 (reduc* N3 (salt or sodium)) S4 (low* N3 (salt or sodium)) S3 (restrict* N3 (salt or sodium)) S2 (MH "Diet, Sodium‐Restricted") S1 (MH "Sodium, Dietary+")
Data and analyses
Comparison 1. Reduced salt versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 All‐cause mortality at end of trial | 7 | 6603 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.83, 1.10] |
| 1.1 Normotensive | 3 | 3518 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.40, 1.12] |
| 1.2 Hypertensive | 4 | 3085 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.86, 1.15] |
| 2 All‐cause mortality at longest follow‐up | 8 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Normotensive | 3 | 3518 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.58, 1.40] |
| 2.2 Hypertensive | 5 | 3680 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.87, 1.14] |
| 3 Cardiovascular mortality at end of trial | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Hypertensive | 3 | 2656 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.45, 1.01] |
| 4 Cardiovascular events at end of trial | 4 | 3397 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.57, 1.01] |
| 4.1 Hypertensives | 4 | 3397 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.57, 1.01] |
| 5 Cardiovascular disease events at longest follow‐up | 6 | 5762 | Risk Ratio (M‐H, Random, 95% CI) | 0.81 [0.66, 0.98] |
| 5.1 Normotensive | 2 | 2415 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.64, 1.10] |
| 5.2 Hypertensive | 4 | 3347 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.58, 1.02] |
| 6 Systolic blood pressure at end of trial | 6 | 3362 | Mean Difference (IV, Random, 95% CI) | ‐1.79 [‐3.23, ‐0.36] |
| 6.1 Normotensive | 3 | 2079 | Mean Difference (IV, Random, 95% CI) | ‐1.15 [‐2.32, 0.02] |
| 6.2 Hypertensive | 3 | 1283 | Mean Difference (IV, Random, 95% CI) | ‐4.14 [‐5.84, ‐2.43] |
| 7 Diastolic blood pressure at end of trial | 5 | 2754 | Mean Difference (IV, Random, 95% CI) | ‐1.17 [‐2.08, ‐0.26] |
| 7.1 Normotensive | 3 | 2079 | Mean Difference (IV, Random, 95% CI) | ‐0.80 [‐1.37, ‐0.23] |
| 7.2 Hypertensive | 2 | 675 | Mean Difference (IV, Random, 95% CI) | ‐3.74 [‐8.41, 0.93] |
| 8 Urinary sodium excretion at end of trial | 6 | 3047 | Mean Difference (IV, Random, 95% CI) | ‐27.21 [‐49.85, ‐4.57] |
| 8.1 Normotensive | 3 | 1812 | Mean Difference (IV, Random, 95% CI) | ‐34.19 [‐49.61, ‐18.78] |
| 8.2 Hypertensive | 3 | 1235 | Mean Difference (IV, Random, 95% CI) | ‐20.48 [‐53.68, 12.73] |
Comparison 2. Sensitivity analysis: individual RCTs.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 All‐cause mortality at end of trial | 5 | 4193 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.45, 1.17] |
| 1.1 Normotensive | 3 | 3518 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.40, 1.12] |
| 1.2 Hypertensive | 2 | 675 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [0.34, 4.24] |
| 2 Cardiovascular mortality at end of trial | 2 | 675 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.29, 2.64] |
| 2.2 Hypertensive | 2 | 675 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.29, 2.64] |
| 3 Cardiovascular events at end of trial | 3 | 1416 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.57, 1.30] |
| 3.1 Hypertensives | 3 | 1416 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.57, 1.30] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Chang 2006.
| Methods | Cluster‐RCT (5 kitchens) | |
| Participants |
N randomised: 1981 (N = 768 intervention, 2 kitchens; N = 1213 control, 3 kitchens) Baseline blood pressure: intervention: SBP mean 131.3 (SD 19.7), DBP mean 71.2 (SD 10.8); control: SBP mean 130.7 (SD 20.4), DBP mean 71.4 (SD 10.8) Case mix: intervention: 40.2% hypertension; control: 40.4% hypertension Age: mean 75.6 (SD 7.7), 74.8 (7.0), in kitchens 2 and 3 (intervention group) 74.8 (7.3), 74.6 (6.7), 74.6 (6.1) in kitchens 1, 4 and 5 (control group) respectively Cardiovascular diagnoses: none reported Percentage male: 100% Percentage white: not reported Inclusion/exclusion criteria: Inclusion: veterans registered in a retirement home in Northern Taiwan Exclusion: bed‐ridden veterans, high serum creatinine (i.e. >= 3.5 mg/dL) Funder: Taiwan Salt Work, Tainan, Taiwan, ROC |
|
| Interventions |
Intervention Total duration: average of 31 months Salt reduction/advice component: ate food prepared by the cook of the kitchen to which they were assigned, using salt containing 49% sodium chloride, 49% potassium chloride and 2% other additives. The 'potassium enriched salt' replaced the regular salt in the selected kitchens in a gradual manner. It was mixed with regular salt in a 1:3 ratio for the first week; it was then increased to 1:1 for the second week and 3:1 for the third week. By the 4th week the cooks solely used the potassium‐enriched salt Other dietary component: other condiments and spices such as soy sauce and monosodium glutamate were not limited because reasonably priced low‐sodium soy sauce and monosodium glutamate were not available at the time of the trial Comparator Dietary: ate food prepared by the cook of the kitchen to which they were assigned using 'regular salt' containing 99.6% sodium chloride and 0.4% other additives at all times. Other condiments and spices such as soy sauce and monosodium glutamate were not limited because reasonably priced low‐sodium soy sauce and monosodium glutamate were not available at the time of the trial |
|
| Outcomes | Deaths (all‐cause and CVD); costs of CVD health care | |
| Follow‐up | Average 31 months | |
| Country and setting | Taiwan ‐ veterans' retirement home | |
| Notes | Outcomes are not reported by kitchen so not possible to quantify the effect of clustering The authors reported the number of deaths due to cardiovascular disease and elsewhere in the table of number of deaths due to other heart problems. In the most current update we included these deaths under cardiovascular mortality. Also, the authors included deaths due to diabetes under deaths due to cardiovascular disease. We emailed the authors to ask about this inclusion and they replied, "As to diabetes, we included it in CVD because we knew locally at the time our coders coded death to be due to diabetes as long as diabetes is related and diabetes occurred earlier. For example, if a person has diabetes and stroke, the code would be diabetes. That is why we grouped diabetes in the CVD category which can be viewed as the cardiometabolic death. A large proportion of dm death is due to CVD" |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The simplest randomisation method, i.e., drawing lots, was used." |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "The veterans were told about the trial, but were not told to which salt they were assigned." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not stated, however primary outcomes are clinical and unlikely to be affected by outcome assessors |
| Incomplete outcome data (attrition bias) All outcomes | High risk | It appears that all subjects were followed up for the deaths outcome. A consort diagram and reasons for losses to follow‐up for other outcomes are given. No sensitivity analysis or imputation was carried out to assess the impact of missing data |
| Selective reporting (reporting bias) | Low risk | All outcomes described in the methods are reported in the results |
| Assessment of compliance? | Low risk | Subjects ate food that was prepared for them |
| Groups balanced at baseline? | Low risk | Quote: "The ages of persons in different kitchens were not significantly [different] at entry (P=0.24). The results also indicated that weight, height, body mass index, blood pressure, and electrolytes for a subsamples of persons in the experimental and control groups were not significantly different at baseline. Persons in [the experimental kitchens] had slightly longer follow‐up times than did their counterparts [in the control kitchens]; however, the difference did not reach statistical significance (P=0.11)." |
| Intention‐to‐treat analysis? | Low risk | Not specifically reported, but on the basis of the consort diagram, subjects did appear to be analysed according to the groups to which they were originally allocated |
| Free from follow‐up bias? | Low risk | The dietary intervention was applied over the period of event outcome follow‐up |
CSSS 2007.
| Methods | RCT | |
| Participants |
N randomised: 608; intervention: 302, control: 306 Baseline blood pressure: intervention: 159/93 (25/14), control: 159/93 (26/14) Case mix: mixed Age: mean 60 years; intervention: 59 (10), control: 61 (9.7) Cardiovascular diagnoses: history of vascular diseases, intervention: 62%, control: 66% Percentage male: 44% male; intervention: 48%, control: 42% Percentage white: not reported Inclusion/exclusion criteria: Inclusion: individuals with a high risk of future vascular disease based on a doctor's diagnosis of any of the following: coronary, cerebral or peripheral vascular disease, diabetes and aged 55 years or older or a systolic blood pressure of 160 mmHg or higher. In addition, all participants were required to have an estimated daily sodium intake of 260 mmol/day or more and an expectation that at least half of the dietary salt could be replaced with the study salt or salt substitute. Participants were required to have no established clear indication for, or contra‐indication to, the use of the study salt substitute, such as use of a potassium‐sparing medication or significant renal impairment Exclusion: any individual with a blood test result considered to be possibly abnormal. Any patient with a family member who had a contra‐indication to the salt substitute Funding: the George Institute for International Health (Australia), the Clinical Trials Research Unit (New Zealand), the Capital Medical Science Development Fund (China) and the National Health and Medical Research Council of Australia |
|
| Interventions |
Salt reduction/advice component: salt substitute. The salt substitute was 65% sodium chloride, 25% potassium chloride and 10% magnesium sulphate Comparison: 100% sodium chloride |
|
| Outcomes | Death, BP, urinary sodium excretion | |
| Follow‐up | 1, 2, 3, 6, 9 and 12 months after randomisation | |
| Country and setting | China; 39 sites in 6 regional co‐ordinating centres | |
| Notes | 2 lost to follow‐up in the control group; 6 lost to follow‐up and 1 withdrew in the intervention group. Do not report enough data for us to calculate standard deviations for MD in SBP and DBP | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation done using a central, computerised randomisation service accessed by centre physicians via the study website with a back‐up phone and fax service. The service was maintained by the Clinical Trials Research Unit at the University of Auckland, New Zealand |
| Allocation concealment (selection bias) | Low risk | The randomisation service provided a unique number for each individual corresponding to a treatment pack held at the centre |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Treatment allocation was blinded to study investigators, participants and centre physicians until the study database was unlocked. Randomised treatment was delivered in 1 kg bags identical except for a 3‐digit code corresponding to the randomisation number, with up to 3 kg a month salt substitute/salt available to each randomised participant to cover all cooking, pickling and other uses within the household. Double‐blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Treatment allocation was blinded to study investigators and centre physicians until the study database was unlocked |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Data not provided for hypertensives (61%) or those with diabetes (16% to 19%); values for urinary sodium excretion and BP not given |
| Selective reporting (reporting bias) | Low risk | No evidence of selective reporting |
| Assessment of compliance? | Low risk | Participants that were randomised reported very good adherence to study salt substitute/salt with 99% of individuals stating that they used study salt substitute/salt for all or nearly all of their day‐to‐day food preparation with no difference between randomised groups (P value = 0.40) |
| Groups balanced at baseline? | Low risk | Appeared similar at baseline |
| Intention‐to‐treat analysis? | Unclear risk | No (5% missing data so no imputations were made for missing data). Final follow‐up visit attended by 96% of randomised participants and overall 98% of all post‐randomisation visits completed as scheduled |
| Free from follow‐up bias? | Unclear risk | Follow‐up very high, with no evidence of differences between groups |
HPT 1990.
| Methods | Individual RCT | |
| Participants |
N randomised: 392 (N = 196 intervention, N = 196 control) Baseline blood pressure: intervention: SBP mean 124.0 (SD NR), DBP mean 82.6 (SD NR); control: mean SBP 123.9 (SD NR), DBP mean 83.0 (SD NR) Case mix: normotensives Age: intervention: mean 39.0 (SD NR); control: mean 38.5 (SD NR) Cardiovascular diagnoses: none Percentage male: 65% Percentage white: 82% Inclusion/exclusion criteria: Inclusion: men and women aged 25 to 49 years; DBP 78 to 89 mmHg Exclusion: use of antihypertensive medication, evidence of CVD, BMI >= 0.0035 kg/cm², dietary requirements incompatible with any of the interventions, drank 21 or more alcoholic drinks per week, pregnant women, unable to comply with the protocol requirements |
|
| Interventions |
Intervention Total duration: 36 months Salt reduction/advice component: dietary counselling (in groups) aimed at sodium restriction. The groups met once a week for the first 10 weeks, once every 2 weeks for the next 4 weeks, and then once every month for the rest of treatment and follow‐up. The group goal was a 50% reduction (<= 70 mmol) in mean urine sodium. Personnel delivering the interventions were trained and experienced in effecting behaviour change. Counselling included a mixture of didactic presentations and demonstrations, token incentives, telephone calls and newsletters Other dietary component: none stated Comparator Dietary: no dietary counselling |
|
| Outcomes | BP, urinary Na excretion, deaths (all‐cause) | |
| Follow‐up | 36 months | |
| Country and setting | USA; 4 clinics | |
| Notes | ‐ Factorial design (calorie restriction and potassium supplementation not reported here ‐ 841 participants in total in study) ‐ No difference in proportion of individuals in each group who began hypertensive medication (8.4% intervention versus 9.0% control) over 36 months |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The randomisation procedure involved a fixed assignment ratio design that provided for equal numbers of assignments within clinic and weight strata in blocks (randomly ordered) of size 3, 6, or 9 for the normal weight stratum and of size 5 to 10 for the high‐weight stratum." "Randomisations were performed on demand at the individual clinic centers (using a pseudo‐random number generator provided with the S/23 BASIC language) with schedules and software for issuing assignments generated by the DCC." |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomisations were performed on demand at the individual clinic centers (using a pseudo‐random number generator provided with the S/23 BASIC language) with schedules and software for issuing assignments generated by the DCC. Clinic personnel had to key all [Baseline 1 and Baseline 2 visit] data and those contained on part I of the [Baseline 3 visit] data before an assignment could be obtained (via the S/23)" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "In order to reduce observer bias, data collection and treatment visits for dietary counselling were not held in the same week for a given participant, and data collection (i.e., interviews, measurements, food record review, and the like) were carried out by personnel not involved in treatment." "Participants were asked not to [...] divulge or discuss their dietary counselling with data collection personnel." |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated, but as primary outcomes are clinical they are unlikely to be affected by outcome assessor's risk of bias |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Numbers in each group at each assessment time point were reported. The only reasons given for losses to follow‐up were non‐attendance at follow‐up visits or death. No sensitivity analysis or imputation undertaken to assess the impact of loss to follow‐up |
| Selective reporting (reporting bias) | Low risk | All outcomes described in methods are reported in results |
| Assessment of compliance? | Low risk | Quote: "Attendance during the first 12 counselling sessions ranged from a high of 86.5% for the Na treatment group in the sodium‐calorie component at session 1 to a low of 46.8% for that same treatment group at session 12. Attendance for all counselling groups declined with time (test for linear decline, P<.001). Generally, attendance over the 12 sessions was better for the two treatment groups involving calorie restriction [...] than for the other two dietary treatment groups [including the sodium reduction group]." "For the purposes of this article, we use progress toward or attainment of dietary treatment goals as indices of compliance. [...] As a first level of exploratory analysis, univariate and multiple linear regressions were conducted comparing 34 baseline and process variables with urine sodium excretion [....] as [one of the] dependent variables. [ ....] In the second level of analysis, compliance was defined in terms of achieving treatment goals. For the sodium reduction groups, compliance was defined as having a 24‐hr urine excretion of less than or equal to 70mEq." |
| Groups balanced at baseline? | Low risk | Quote: "Except for sex there were no marked baseline differences among the treatment groups." |
| Intention‐to‐treat analysis? | Low risk | Quote: "All results are presented by original treatment assignment." |
| Free from follow‐up bias? | Low risk | Duration of intervention same as follow‐up time for event outcomes |
Kwok 2012.
| Methods | Cluster‐RCT | |
| Participants |
N randomised: 429 (14 hostels); intervention: 204 (6 hostels), control: 225 (8 hostels) Baseline blood pressure: intervention: SBP 139.2 (16.6), DBP 78.9 (9.3); control: SBP 141.0 (18.5), DBP 78.4 (8.7) Case mix: intervention: 55.4%, control: 64.4% Age: 75+, average age intervention: 83.1 (5.7), control: 83.3 (5.5) Cardiovascular diagnoses: none Percent male: intervention: 22.1%, control: 9.3% Percent white: not stated Inclusion/exclusion criteria: Inclusion: men and women 75 years and older in old age hostels run by 2 non‐government organisations Exclusion: tube‐fed residents, individuals on a special diet due to chronic renal failure Funding: Tung Wah group and private donations |
|
| Interventions |
Total duration: 33 months Salt reduction/advice component: 1) Research dietician gave a 1‐hour talk to residents and staff on the prevention of dementia and promoted the 'brain preservation diet' with the following targets including avoidance of salty foods 2) Trained dietician conducted dietary support groups to reinforce the brain preservation diet (group size ranged from 10 to 15 subjects), totalling 20 times in the first year, each group session lasting 45 minutes. In the subsequent 21 months, the frequency of dietary groups was reduced to once in 6 weeks to reinforce the intervention 3) The dietician also liaised closely with the hostel staffs and kitchen staff on the hostel menu and cooking methods. Instead of using salt or other salty seasoning like fermented tofu and oyster sauce, they suggested using peppers, ginger, onion, spring onion, garlic, coriander and Chinese 5 spices powder. The hostel staff also helped to promote the 'brain preservation diet' in their homes Comparator 1) Research dietician gave a 1‐hour talk to residents and staff on the prevention of dementia and promoted the 'brain preservation diet' with the following targets including avoidance of salty foods 2) In the control hostels, the dietician gave advice on menus at the beginning of the trial only |
|
| Outcomes | Mortality, BP, urinary sodium excretion, health‐related quality of life | |
| Follow‐up | 12 months, 24 months, 33 months | |
| Country and setting | Hong Kong: 14 old age hostels | |
| Notes | Did not provide information on BP and health‐related quality of life; only said that there were no significant differences at 33 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated; "randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not possible for patients and caregivers to be blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not possible for outcome assessors to be blinded, however as primary outcomes all clinical, unlikely to be affected by risk of bias |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not stated |
| Selective reporting (reporting bias) | Unclear risk | Appeared to report on all outcomes, although did not give data for some of the outcomes, only stating that there were no differences |
| Assessment of compliance? | High risk | Stated that "The dietary intervention was not successful in reducing salt intake. Although salty foods in the menu of the intervention homes were reduced significantly, the residents had the option of adding salty flavouring, for example, soya sauce to their foods." |
| Groups balanced at baseline? | Unclear risk | More males in the treatment group, slightly higher BP in the control group |
| Intention‐to‐treat analysis? | Low risk | Done |
| Free from follow‐up bias? | Low risk | Yes |
Morgan 1978.
| Methods | Individual RCT | |
| Participants |
N randomised: 4‐arm trial. 2 arms were of drug treatments and not considered here. The dietary sodium restriction arm and control arm are used here. 67 (N = 34 intervention, N = 33 control). Morgan 1980 reports on a longer follow‐up and gives 42 allocated to control and 33 to intervention arms Baseline blood pressure: intervention: SBP mean 160 (SD 23), DBP 97 (SD 8); control: SBP mean 165 (SD 17), DBP mean 97 (SD 8) Case mix: untreated hypertensives Age: intervention: mean 57.1 (SD NR); control: mean 58.6 (SD NR) Cardiovascular diagnoses: borderline hypertensives (DBP 95 to 109 mmHg) and hypertensives (DBP 110+ mmHg) Percentage male: 100% Percentage white: not reported Inclusion/exclusion criteria: Inclusion: males with borderline hypertension on admission to hospital or outpatient visit Exclusion: malignant disease, severe psychiatric disturbances, severe physical incapacity or a disease likely to be fatal in the next 2 years, serum‐creatinine levels > 0.18 mmol/l, abnormal liver function tests, in cardiac failure or on diuretic therapy Funding: Australian Department of Veterans' Affairs, the Australian National Heart Foundation, Merck, Sharp & Dohme (Aust), Pty Ltd and ICI Australia Ltd |
|
| Interventions |
Intervention Total duration: 24 months Salt reduction/advice component: patients were instructed to reduce their sodium chloride intake and were given a diet that should have reduced their sodium intake to 70 to 100 mmol/day. The advice about diet was repeated at 6 months. No details on who gave advice Other dietary component: at each 6‐month review visit, if serum potassium levels < 3.4 mmol/L, potassium supplements were given Comparator No treatment, reviewed at 6 months (as intervention) Other: not given any treatment, but reviewed at 6‐monthly intervals and if DBP rose above 115 mmHg treatment was started |
|
| Outcomes | Deaths (all‐cause and CVD); BP; urinary Na excretion | |
| Follow‐up | BP at 24 months; clinical outcomes at 24 months (end of trial) and at extra follow‐up to 70 months | |
| Country and setting | Australia ‐ single hospital | |
| Notes | Cardiovascular morbidity and mortality data taken from review of Morgan 1978 and Morgan 1980 Taking antihypertensive medication (at 6 months): intervention 4/10 versus control 9/10 (RR 0.44, 95% CI 0.20 to 0.98) Longer‐term follow‐up reported in Med J Australia 1980. Note that denominators for long‐term findings are taken from this report |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "[patients] were randomly divided into 4 subgroups" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not reported but as primary outcomes clinical unlikely to be affected by risk of bias |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "Information regarding life or death was not known for two patients, who were excluded from the study. All patients included in the study were seen at the initial visit, and at a subsequent six‐month visit. Patients who did not report back on at least one occasion have not been analysed. Five patients died in the first six months; these have been included in the analysis. There were no other known deaths in this time interval in the patients who did not report back. More than 90% of initially allocated patients reported back at the end of the first six‐month period." The only reason given for losses to follow‐up was patients not reporting back. No sensitivity analysis or imputation undertaken to assess the impact of loss to follow‐up |
| Selective reporting (reporting bias) | Low risk | All outcomes described in the methods are reported at some point in the results |
| Assessment of compliance? | Low risk | Urinary sodium is measured and although it is not specifically stated that this was used to assess compliance, it is implied. Quote: "Patients in the dietary therapy group who continued to have a high sodium excretion were advised about their diet." |
| Groups balanced at baseline? | Low risk | Quote: "At the start of the study the groups were similar in age, weight, height, pulse‐rate, and serum electrolytes, urea, creatinine, uric acid, glucose, and cholesterol. The initial systolic and diastolic blood‐pressures, supine and standing, did not differ among the groups". |
| Intention‐to‐treat analysis? | Low risk | Although the term ITT is not used by the authors it appears that groups were analysed as randomised. Quote: "[Morgan et al's (1980)] report does not exclude patients who changed therapy or ceased therapy. It evaluates the proposition: 'Did the decision to implement therapy alter the mortality rate in patients with mild hypertension'?" |
| Free from follow‐up bias? | High risk | Longest event follow‐up for mortality was 71 months but last stated diet advice stated as 6 months. No urinary sodium excretion data available at longest follow‐up |
TOHP I 1992.
| Methods | Individual RCT | |
| Participants |
N randomised: 744 (intervention: 327 and control: 417) Baseline blood pressure: intervention: SBP mean 124.8 (SD 8.5), DBP mean 83.7 (SD 2.7); control: SBP mean 125.1 (SD 8.1), DBP mean 83.9 (SD 2.8) Case mix: normotensives Age: intervention: 43.4 (SD 6.6); control: 42.6 (SD 6.5) Cardiovascular diagnoses: none Percentage male: 71.4% Percentage white: 77.2% Inclusion/exclusion criteria: Inclusion: aged 30 to 54: mean DBP 80 to 89 mmHg without antihypertensive medication; ability to complete and return a satisfactory 24‐hour urine collection and food frequency questionnaire Exclusion: long list of exclusion criteria, generally designed to eliminate patients with: evidence of medically diagnosed hypertension (DBP >= 90 mmHg or use of BP medications within 2 months of first evaluation), cardiovascular or other life‐threatening or disabling diseases, gross obesity (BMI > 36.14), a contraindication to any of the phase I interventions, or might have difficulty complying with the treatment or follow‐up requirements of the trial |
|
| Interventions |
Intervention Total duration: 18 months Salt reduction/advice component: dietary and behavioural counselling on how to identify sodium in the diet, self monitor intake and select or prepare low‐sodium foods and condiments suited to personal preferences. Individual and weekly group counselling sessions were provided during the first 3 months, with additional less frequent counselling and support for the remainder of follow‐up. Sessions were provided by nutritionists, psychologists, or other experienced counsellors. The objective was to reduce urinary sodium excretion in the intervention group to 80 mmol/24 hours Comparator Dietary: usual diet. General guidelines for healthy eating were given |
|
| Outcomes | All‐cause mortality, cardiovascular morbidity, BP and 24‐hour urinary sodium excretion | |
| Follow‐up | 11.5 years ("additional ˜10 yrs observational follow up") | |
| Country and setting | USA; 6 clinics | |
| Notes | TOHP I design included allocation to other interventions (weight loss, stress management and supplements, e.g. fish oil) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Low risk | Quote: "the clinic notified the coordinating center [of participant eligibility] by telephone and obtained a randomisation assignment. Clinics were also provided with sealed envelopes containing randomization assignments for use when telephone contact with the coordinating center was not possible." "adherence to the appropriate assignment sequence was monitored by the coordinating center." |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "To minimize bias, [BP] observers were blinded to treatment allocation. Persons certified to measure BP were not involved with intervention aspects of the trial, nor were they allowed access to data that would reveal group assignment. When possible, separate facilities or entrances were used for data collection visits as compared to intervention visits." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "In order to reduce observer bias, data collectors were blinded to the treatment assignment of the participants." Primary outcomes all clinical and are unlikely to be affected by risk of bias |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "In the analyses shown, participants with no follow‐up visits [...] were assigned a zero value for BP change ("intention‐to‐treat" analysis). These results did not differ appreciably from those in which missing BP values were treated as missing at random and excluded from the analysis." "The effect of missing urinary sodium excretion data at follow‐up on estimates of the absolute change from baseline was assessed by assuming no change (the baseline sodium excretion value was imputed). To reduce the likelihood that estimates of treatment group differences were influenced by the inclusion of incomplete samples, mean differences in urinary sodium excretion at 6, 12, and 18 months were recalculated excluding urine values associated with a volume less than 500g or, in separate analyses, associated with creatinine or creatinine per kilogram of body weight less than 85% of the within‐person average. Mean treatment group differences with these exclusions were very similar to each other and to those calculated when all samples were included." |
| Selective reporting (reporting bias) | Low risk | All outcomes described in methods are reported in results |
| Assessment of compliance? | Low risk | Quote: "Twenty‐four‐hour urine samples were used to monitor sodium reduction" [....] In addition, food frequency questionnaire and 24‐hour dietary recall estimates of sodium intake were obtained from all life‐style participants." "Compliance with the three life‐style interventions was satisfactory, both in terms of attendance at counselling sessions and in reaching specific goals. [...] The group difference [in urinary Na excretion] was maximal (58mmol/24h) at 6 months, [...] the mean reduction [in urinary Na excretion] was well‐maintained." "The Data Coordinating Center provided guidelines for estimating adherence to the counselling goal of 60mmol sodium /24hr from the average sodium excretion in two 8‐hour urine samples collected at least 2 days apart." |
| Groups balanced at baseline? | Low risk | Quote: "Baseline characteristics were evenly distributed, except for age, which was higher in the sodium reduction intervention group" |
| Intention‐to‐treat analysis? | Low risk | Quote: "In a sensitivity analysis using logistic regression we performed an intention to treat analysis treating non‐responders as non‐events. Because mortality follow‐up was virtually complete, we included all randomised participants in analyses of mortality alone in a full intention to treat analysis." |
| Free from follow‐up bias? | High risk | Longest event follow‐up for mortality and cardiovascular morbidity was approximately 11.5 years but last stated diet advice stated as 18 months. No urinary sodium excretion data available at longest follow‐up |
TOHP II 1997.
| Methods | Individual RCT | |
| Participants |
N randomised: 2382 (intervention: 1191; control: 1191) Baseline blood pressure: intervention: mean SBP 127.5 (SD 6.6), DBP mean 86.0 (SD 1.9); control: SBP mean 127.4 (SD 6.2), DBP SD 85.9 (SD 1.9) Case mix: normotensives Age: intervention: mean 43.9 (SD 6.2); control: mean 43.3 (SD 6.1) Cardiovascular diagnoses: none Percentage male: 65.7% Percentage white: 79.3% Inclusion/exclusion criteria: Inclusion: 30 to 54‐year old adults with no evidence of medically diagnosed hypertension, who were moderately overweight (men: between 26.1 and 37.4 kg/m²; women: between 24.4 and 37.4 kg/m²), and had average DBP between 83 to 89 mmHg, and a SBP < 140 mmHg. Participants also had to demonstrate compliance with the more difficult data collection tasks Exclusion: evidence of current hypertension. History of CVD, diabetes mellitus, malignancy other than non‐melanoma skin cancer during the past 5 years, or any other serious life‐threatening illness that requires regular medical treatment. Current use of prescription medications that affect BP, as well as non‐prescription diuretics. Serum creatinine level >= 1.7 mg/dL for men or 1.5 mg/dL for women, or casual serum glucose >= 200mg/dL. Current alcohol intake > 21 drinks/week. Pregnancy, or intent to become pregnant during the study. Plans to move or inability to co‐operate |
|
| Interventions |
Intervention Total duration: 36 months Salt reduction/advice component: individual and weekly group counselling sessions were provided initially followed by additional less intensive counselling and support for the remainder of follow‐up. Mini‐modules to reinforce the content of the counselling session were offered in the later years of the intervention. The content of sessions included sodium information, self management and social support components. Sessions were provided by registered dieticians mainly, plus a few psychologists, or other experienced counsellors. The objective was to reduce urinary sodium excretion in the intervention group to 80 mmol/24 hours Other: the salt reduction intervention was combined with a weight loss intervention or alone Comparator Dietary: no advice Other: usual care or weight loss intervention alone |
|
| Outcomes | All‐cause mortality, cardiovascular morbidity (a composite of myocardial infarction, stroke, coronary revascularisation or cardiovascular death), BP, urinary excretion | |
| Follow‐up | 36 months | |
| Country and setting | USA; 9 clinics | |
| Notes | This study had a 2 x 2 factorial design in which the groups were: weight loss alone, sodium reduction alone, a combination of weight loss and sodium reduction, and a usual care group. The long‐term effects of the sodium reduction intervention were analysed by grouping data for the 2 sodium reduction interventions (alone or with weight loss) and for the 2 non‐sodium reduction groups (usual care and weight loss alone) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Low risk | Quote: "The clinic then notified the coordinating center [of participant eligibility] by telephone and obtained a randomisation assignment. In those cases where random assignment was not done by phone, clinics also were provided with sealed randomization envelopes for use when contact with the coordinating center was not possible." |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "With respect to the determination of categorical end points, in order to minimize bias in the ascertainment of hypertension, an Endpoints Subcommittee conducts a blind review of study forms, and as necessary, the medical records of participants who are considered to have had hypertensive events. Potential hypertensive end points identified are either confirmed or refuted by the subcommittee." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "[Data collectors] were masked to participants' intervention assignments." Primary outcomes all clinical and are unlikely to be affected by risk of bias |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "For those with BP measurements but without urinary sodium excretion data at the corresponding follow‐up visit, a 0 change in urinary sodium excretion was imputed in a secondary analysis." "For the small number of participants with no useable BP readings after randomisation (n=99, of whom 57% were treated early with BP medications by their physicians), measures from a randomly selected participant in the usual care group were imputed under the assumption that having little or no exposure to the intervention programs would produce similar results to that of the usual care group." |
| Selective reporting (reporting bias) | Low risk | All outcomes described in methods are reported in results |
| Assessment of compliance? | Low risk | Quote: "Intervention attendance also is collected for participants within each of the active intervention groups. The dietary data are collected on random samples of equal numbers of participants across the treatment groups. The 24‐hour urine specimens for sodium, potassium and creatinine measurements are collected from all participants at 18 and 36 months. An additional 24‐hour urine specimen, collected on a 25% sample of trial participants at 6 months, was added to more fully assess sodium intakes at this time as compared to baseline levels." "Urinary sodium excretion and weight change are collected as intermediate end points for all participants. These intermediate end points were selected to evaluate compliance to specific interventions" |
| Groups balanced at baseline? | Low risk | Quote: "Baseline characteristics were evenly distributed, except for age, which was higher in the sodium reduction intervention group" |
| Intention‐to‐treat analysis? | Low risk | Quote: "In a sensitivity analysis using logistic regression we performed an intention to treat analysis treating non‐responders as non‐events. Because mortality follow‐up was virtually complete, we included all randomised participants in analyses of mortality alone in a full intention to treat analysis." |
| Free from follow‐up bias? | Unclear risk | Longest event follow‐up for mortality and cardiovascular morbidity was approximately 8 years but last stated diet advice stated as 36 months. No urinary sodium excretion data available at longest follow‐up |
TONE 1998.
| Methods | Individual RCT | |
| Participants |
N randomised: 681 (N = 340 intervention, N = 341 control) ‐ part of a factorial design study Baseline blood pressure: SBP 128.0 (9.4), DBP 71.3 (7.3) mmHg Case mix: treated hypertensives Age: 65.8 (SD 4.6) Cardiovascular diagnoses: none Percentage male: 53% Percentage white: 76% Inclusion/exclusion criteria: Inclusion: healthy, aged 60 to 80 years, SBP < 145 mmHg and DBP < 85 mmHg while taking a single antihypertensive medication or a single combination regimen consisting of a diuretic agent and a non‐diuretic agent. Individuals taking 2 antihypertensive medications were also eligible if they were successfully weaned off one of them during the screening phase. Independence in activities of daily living. Capacity to alter diet and physical activity in accordance with the requirements of any TONE intervention Exclusion: diagnosis or treatment of cancer within the last 5 years; treatment with diuretics, ACE inhibitors, or digitalis for CHF or unknown reason; drug therapy with nitrates, beta‐blockers or calcium channel blockers for CHD or reason other than hypertension; MI or stroke within 6 months; "active" CHD (e.g. angina pectoris); CHF; atrial fibrillation; second‐ or third‐degree heart block without permanent pacemaker; drug therapy for ventricular arrhythmias; self report of heart valve replacement; clinically important valvular heart disease; insulin‐dependent diabetes mellitus; severe hypertension; current or recent (within 6 months) drug therapy for asthma or chronic obstructive lung disease; use of corticosteroid therapy for > 1 month; serious mental or physical illness; unexplained or involuntary weight loss (>= 4.5 kg) during the previous year; BMI < 21 in men or women, or > 33 in men or > 37 in women; serum creatinine > 2 mg/dL; non‐fasting blood glucose level of > 260 mg/dL; hyperkalaemia (> 5.5 mmol/L); anaemia (Hb level < 110 g/L); > 14 alcoholic drinks per week (assessed by self report); severe visual or hearing impairment; other reason making it difficult for the participant to comply fully with any part of the study protocol |
|
| Interventions |
Intervention Total duration: 4‐month "intensive" phase, plus 3‐month "extended" phase, and then a maintenance phase (duration of this phase is unclear) Salt reduction/advice component: individual and group sessions with an interventionist (typically a registered dietician) who provided information using both centrally and locally prepared materials, motivated participants to make and sustain long‐term lifestyle changes, and frequently monitored progress of groups and individuals. Individualised feedback was provided. Participants learned about sources of sodium, in particular those foods with a high salt content, and they learned about possible alternatives. They also learned how to adapt the recommendations for a low‐salt diet to their own lifestyle. The goal of this intervention for the group was to achieve and maintain a 24‐hour dietary sodium intake of 80 mmol (1800 mg) or less (as measured by 24‐hour urine collection) Other: attempt to withdraw hypertensive therapy began 3 months post‐randomisation Comparator Dietary: in order to enhance retention of control participants, meetings were held on a regular basis with speakers on subjects unrelated to BP, CVD or nutrition Other: drug withdrawal began at a comparable time to the intervention group |
|
| Outcomes | Mortality (all‐cause and cardiovascular), cardiovascular morbidity (a composite of myocardial infarction, stroke, coronary artery bypass graft (CABG)), BP, urinary sodium | |
| Follow‐up | 30 months | |
| Country and setting | USA; 4 clinical academic centres | |
| Notes | Unpublished all‐cause mortality data at 12.7 years obtained from authors No data specifically reported on number of individuals who stopped antihypertensive medication in 2 groups Multifactorial design. Only used sodium reduction without weight loss. Used in both overweight and non‐overweight groups |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Overweight participants were randomly assigned, in a 2x2 factorial design [...] Nonoverweight participants were randomly assigned [...]" "We used a variable block length randomization algorithm." (from investigators) |
| Allocation concealment (selection bias) | Low risk | Quote: "Assignments were made via computers at the clinic sites, after eligibility criteria were confirmed. The sequences were concealed from clinic staff?only known to statisticians at the coordinating center." (from investigators) |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "To facilitate masking of the data collectors, intervention visits were conducted at separate times and places from the data collection visits." "An end point committee, masked to intervention assignment, made final decisions concerning the end point status of each participant." "Outcome information was obtained by staff members who were blind to the participants’ intervention assignment, at different times and different locations from those used for the intervention visits. Participants were instructed not to reveal their intervention assignment to the data collection staff." "Intervention staff members were masked with respect to the participants’ BP and drug withdrawal status." "When questioned at the final follow‐up visit, the data collectors guessed the correct treatment assignment in 31% of the obese participants (compared with an expected rate of 25% on the basis of chance) and in 45% of the nonobese participants (compared with and expected rate of 50% on the basis of chance)." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Primary outcomes all clinical and are unlikely to be affected by risk of bias |
| Incomplete outcome data (attrition bias) All outcomes | High risk | The only reason given for losses to follow‐up was non‐attendance at follow‐up visits. No sensitivity analysis or imputation undertaken to assess the impact of loss to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | The authors report that data were collected via psychological questionnaires at randomisation and a number of the follow‐up visits, but none of the data from these appear to be reported, unless they are in a separate publication |
| Assessment of compliance? | Low risk | Quote: "Monitoring adherence (Reduced sodium life‐style): Attendance; urinary data; food and behaviour records; adherence‐related incentives. Monitoring adherence (Usual (control) life‐style): Attendance." |
| Groups balanced at baseline? | Low risk | Quote: "There was no evidence of a substantial imbalance between the reduced sodium and UL [usual lifestyle] groups [at baseline]" |
| Intention‐to‐treat analysis? | Low risk | Quote: "Analyses were conducted on an intention‐to‐treat basis." |
| Free from follow‐up bias? | High risk | Mortality outcome provided by authors at 12.7 years average follow‐up. No urinary sodium excretion data available at longest follow‐up |
ACE: angiotensin‐converting enzyme BMI: body mass index BP: blood pressure CHF: coronary heart failure CHD: coronary heart disease CSSS: China Salt Substitute Study CVD: cardiovascular disease DBP: diastolic blood pressure Hb: haemoglobin HPT: Hypertension Prevention Trial ITT: intention‐to‐treat MD: mean difference MI: myocardial infarction Na: sodium NR: not reported RCT: randomised controlled trial ROC: Republic of China RR: risk ratio SBP: systolic blood pressure SD: standard deviation TOHP: Trials of Hypertension Prevention TONE: Trial of Nonpharmacologic Intervention in the Elderly
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bentley 2006 | Inadequate follow‐up duration |
| Knuist 1998 | Pregnant women |
| Koopman 1997 | No appropriate outcomes |
| Licata 2003 | Not dietary salt reduction intervention |
| Tobari 2010 | No cardiovascular events |
| van der Post 1997 | Pregnant women |
| Velloso 1991 | Inadequate follow‐up duration |
Characteristics of ongoing studies [ordered by study ID]
Aung 2012.
| Trial name or title | RESIP‐CVD Study |
| Methods | Cluster‐randomised trial |
| Participants | High CVD risk patients stratified by the Framingham general CVD risk scoring system (> 15%) |
| Interventions | Education regarding salt content in foods, subsequent cooking classes |
| Outcomes | BP, CVD events, CVD mortality |
| Starting date | Not stated |
| Contact information | — |
| Notes | — |
BP: blood pressure CVD: cardiovascular disease
Differences between protocol and review
Given the small number of trials included in this review it was not possible to undertake exploration of heterogeneity using stratified meta‐analysis or meta‐regression.
Contributions of authors
All the authors were involved in the design of the review.
In the original review:
TM developed the search strategy.
KA and RT selected studies for inclusion, extracted data, carried out data synthesis/analysis and wrote the first draft of the review.
For this update:
NM conducted the searches.
FCT, NM and AJA screened abstracts and selected studies for analysis.
FCT and AJA extracted trial data.
AJA did the analysis and wrote the review.
SE reviewed the data extraction, did the analysis and wrote the review.
Sources of support
Internal sources
No sources of support supplied
External sources
-
NIHR programme grant, UK.
Original review funded by a NIHR programme grant
Declarations of interest
Dr. Gottlieb owns the trademark "Greens, Beans, and Leans (R)", a registered trademark in the United States, for a diet that is high in fibre and polyunsaturated fats, low in simple carbohydrates, saturated fats and sodium.
Shah Ebrahim's research is supported by grants from the Wellcome Trust, IDRC, ESRC and the National Institute of Health Research.
Alma Adler, Fiona Taylor, Nicole Martin and Rod Taylor have no known conflict of interest.
Edited (no change to conclusions), comment added to review
References
References to studies included in this review
Chang 2006 {published data only}
- Chang HY, Hu YW, Yue CS, Wen YW, Yeh WT, Hsu LS, et al. Effect of potassium‐enriched salt on cardiovascular mortality and medical expenses of elderly men. American Journal of Clinical Nutrition 2006;83:1289‐96. [DOI] [PubMed] [Google Scholar]
CSSS 2007 {published data only}
- The China Salt Substitute Study Collaborative Group. Salt substitution: a low‐cost strategy for blood pressure control among rural Chinese. A randomized, controlled trial. Journal of Hypertension 2007;25:2011‐8. [DOI] [PubMed] [Google Scholar]
HPT 1990 {published and unpublished data}
- Borhani NO, Tonascia J, Schlundt DG, Prineas RJ, Jefferys JL. Recruitment in the hypertension prevention trial. Controlled Clinical Trials 1989;10(Suppl 3):30‐9S. [DOI] [PubMed] [Google Scholar]
- Brown KM, Oberman A, Natta ML, Forster JL. Baseline characteristics in the hypertension prevention trial. Controlled Clinical Trials 1989;10(Suppl 3):40‐64S. [DOI] [PubMed] [Google Scholar]
- Forster JL, Jeffery RW, VanNatta M, Pirie P. Hypertension prevention trial: do 24‐h food records capture usual eating behavior in a dietary study?. American Journal of Clinical Nutrition 1990;51:253‐7. [DOI] [PubMed] [Google Scholar]
- Hypertension Prevention Trial Research Group. The Hypertension Prevention Trial: three‐year effects of dietary changes on blood pressure. Archives of Internal Medicine 1990;150:153‐62. [PubMed] [Google Scholar]
- Jeffery RW, French SA, Schmid TL. Attributions for dietary failures: problems reported by participants in the Hypertension Prevention Trial. Health Psychology 1990;9:315‐29. [DOI] [PubMed] [Google Scholar]
- Jeffery RW, Tonascia S, Bjornson BW, Schlundt DG, Sugars C for the Hypertension Prevention Trial Research Group. Treatment in the Hypertension Prevention Trial. Controlled Clinical Trials 1989;10(Suppl 3):65‐83S. [DOI] [PubMed] [Google Scholar]
- Meinert CL, Borhani NO, Langford HG. Design, methods, and rationale in the Hypertension Prevention Trial. Controlled Clinical Trials 1989;10(Suppl 3):1‐29S. [DOI] [PubMed] [Google Scholar]
- Prudhomme GJ, Canner PL, Cutler JA. Quality assurance and monitoring in the Hypertension Prevention Trial. Controlled Clinical Trials 1989;10(Suppl 3):84‐94S. [DOI] [PubMed] [Google Scholar]
- Schmid TL, Jeffery RW, Onstad L, Corrigan SA. Demographic, knowledge, physiological, and behavioral variables as predictors of compliance with dietary treatment goals in hypertension. Addictive Behaviors 1991;16:151‐60. [DOI] [PubMed] [Google Scholar]
- Shah M, Jeffery RW, Laing B, Savre SG, Van NM, Strickland D. Hypertension Prevention Trial (HPT): food pattern changes resulting from intervention on sodium, potassium, and energy intake. Journal of the American Dietetic Association 1990;90:69‐76. [PubMed] [Google Scholar]
Kwok 2012 {published data only}
- Kwok TCY, Lam LCW, Sea MMM, Goggins W, Woo J. A randomized controlled trial of dietetic interventions to prevent cognitive decline in old age hostel residents. European Journal of Clinical Nutrition 2012;66:1135‐40. [DOI] [PubMed] [Google Scholar]
Morgan 1978 {published data only}
- Morgan T, Adam W, Gillies A, Wilson M, Morgan G, Carney S. Hypertension treated by salt restriction. Lancet 1978;1(8058):227‐30. [DOI] [PubMed] [Google Scholar]
- Morgan TO, Adams WR, Hiodgson M, Giverd RW. Failure to improve prognosis in elderly males with hypertension. Medical Journal Australia 1980;2:27‐31. [PubMed] [Google Scholar]
TOHP I 1992 {published data only}
- Cook NR, Cutler JA, Obarzanek E, Buring JE, Rexrode KM, Kumanyika SK. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow‐up of the trials of hypertension prevention (TOHP). BMJ 2007;334:885‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Trials of Hypertension Prevention Collaborative Research Group. The effects of nonpharmacologic interventions on blood pressure of persons with high normal levels: results of the Trials of Hypertension Prevention, Phase I. JAMA 1992;267:1213‐20. [DOI] [PubMed] [Google Scholar]
TOHP II 1997 {published data only}
- Appel LJ, Hebert PR, Cohen JD, Obarzanek E, Yamamoto M, Buring J, et al. Baseline characteristics of participants in phase II of the Trials of Hypertension Prevention (TOHP II). Annals of Epidemiology 1995;5:149‐55. [DOI] [PubMed] [Google Scholar]
- Hebert PR, Bolt RJ, Borhani NO, Cook NR, Cohen JD, Cutler JA, et al. Design of a multicenter trial to evaluate long‐term life‐style intervention in adults with high‐normal blood pressure levels. Trials of Hypertension Prevention (Phase II). Annals of Epidemiology 1995;5:130‐9. [DOI] [PubMed] [Google Scholar]
- Hollis JF, Satterfield S, Smith F, Fouad M, Allender PS, Borhani N, et al. Recruitment for phase II of the Trials of Hypertension Prevention. Effective strategies and predictors of randomization. Annals of Epidemiology 1995;5:140‐8. [DOI] [PubMed] [Google Scholar]
- Hunt SC, Cook NR, Oberman A, Cutler JA, Hennekens CH, Allender PS, et al. Angiotensinogen genotype, sodium reduction, weight loss, and prevention of hypertension. Trials of Hypertension Prevention Phase II. Hypertension 1998;32:393‐401. [DOI] [PubMed] [Google Scholar]
- Hypertension Prevention Collaborative Research Group. Effects of weight loss and sodium reduction intervention on blood pressure and hypertension incidence in overweight people with high‐normal blood pressure. The Trials of Hypertension Prevention, phase II. Archives of Internal Medicine 1997;157:657‐67. [PubMed] [Google Scholar]
- Lasser VI, Raczynski JM, Stevens VJ, Mattfeldt‐Beman M, Kumanyika S, Evans M, et al. Trials of Hypertension Prevention, phase II. Structure and content of the weight loss and dietary sodium reduction interventions. Annals of Epidemiology 1995;5:156‐64. [DOI] [PubMed] [Google Scholar]
TONE 1998 {published data only}
- Appel LJ, Espeland M, Whelton PK, Dolecek T, Kumanyika S, Applegate WB, et al. Trial of Nonpharmacologic Intervention in the Elderly (TONE). Design and rationale of a blood pressure control trial. Annals of Epidemiology 1995;5:119‐29. [DOI] [PubMed] [Google Scholar]
- Appel LJ, Espeland MA, Easter L, Wilson AC, Folmar S, Lacy CR. Effects of reduced sodium intake on hypertension control in older individuals. Results from the Trial of Nonpharmacological Interventions in the Elderly (TONE). Archives of Internal Medicine 2001;161:685‐93. [DOI] [PubMed] [Google Scholar]
- Bahnson JL, Whelton PK, Appel LJ, Espeland MA, Wofford JL, Rosen R, et al. Baseline characteristics of randomized participants in the trial of nonpharmacologic intervention in the elderly (TONE). Disease Management and Clinical Outcomes 1997;1:61‐8. [Google Scholar]
- Espeland MA, Whelton PK, Kostis JB, Bahnson JL, Ettinger WH, Cutler JA, et al. Predictors and mediators of successful long‐term withdrawal from antihypertensive medications. Archives of Family Medicine 1999;8:228‐36. [DOI] [PubMed] [Google Scholar]
- Kostis JB, Espeland MA, Appel LJ, Johnson KC, Pierce J, James L. Does withdrawal of antihypertensive medication increase the risk of cardiovascular events?. American Journal of Cardiology 1998;82:1501‐8. [DOI] [PubMed] [Google Scholar]
- Shea MK, Nicklas BJ, Houston DK, Miller ME, Davis CC, Kitzman DW, et al. The effect of intentional weight loss on all‐cause mortality in older adults: results of a randomized controlled weight‐loss trial. American Journal of Clinical Nutrituion 2011;94:839‐46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whelton PK, Appel LJ, Espeland MA, Applegate WB, Ettinger WH Jr, Kostis JB, et al. Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of nonpharmacologic interventions in the elderly (TONE). JAMA 1998;279:839‐46. [DOI] [PubMed] [Google Scholar]
- Whelton PK, Bahnson J, Appel LJ, Charleston J, Cosgrove N, Espeland MA, et al. Recruitment in the Trial of Nonpharmacologic Intervention in the Elderly (TONE). Journal of the American Geriatric Society 1997;45:185‐93. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Bentley 2006 {unpublished data only}
- Bentley BB. Dietary Sodium in Heart Failure. USA: University of Kentucky, 2006. [Google Scholar]
Knuist 1998 {published data only}
- Knuist M, Bonsel GJ, Zondervan HA, Treffers PE. Low sodium diet and pregnancy‐induced hypertension: a multi‐centre randomised controlled trial. British Journal of Obstetrics and Gynaecology 1998;105:430‐4. [DOI] [PubMed] [Google Scholar]
Koopman 1997 {published data only}
- Koopman H, Deville W, Eijk J, Donker AJM, Spreeuwenberg C. Diet or diuretic? Treatment of newly diagnosed mild to moderate hypertension in the elderly. Journal of Human Hypertension 1997;11:807‐12. [DOI] [PubMed] [Google Scholar]
Licata 2003 {published data only}
- Licata G, Pasquale P, Parrinello G, Cardinale A, Scandurra A, Follone G, et al. Effects of high‐dose furosemide and small‐volume hypertonic saline solution infusion in comparison with a high dose of furosemide as bolus in refractory congestive heart failure: long‐term effects. American Heart Journal 2003;145:459‐66. [DOI] [PubMed] [Google Scholar]
Tobari 2010 {published data only}
- Tobari H, Arimoto T, Shimojo N, Yuhara K, Noda H, Yamagishi K, et al. Physician–pharmacist cooperation program for blood pressure control in patients with hypertension: a randomized‐controlled trial. American Journal of Hypertension 2010;23(10):1144‐52. [DOI] [PubMed] [Google Scholar]
van der Post 1997 {published data only}
- Post JA, Buul BJ, Hart AA, Heerikhuize JJ, Pesman G, Legros JJ, et al. Vasopressin and oxytocin levels during normal pregnancy: effects of chronic dietary sodium restriction. Journal of Endocrinology 1997;152:345‐54. [DOI] [PubMed] [Google Scholar]
Velloso 1991 {published data only}
- Velloso LG, Alonso RR, Ciscato CM, Barretto AC, Bellotti G, Pileggi F. Diet with usual quantity of salt in hospital treatment of congestive heart insufficiency. Arquivos Brasileiros de Cardiologia 1991;57:465‐8. [PubMed] [Google Scholar]
References to ongoing studies
Aung 2012 {published data only}
- Aung MY, Yuasa M, Moolphate S, Nedsuwan S, Yokokawa H, Kitajima T, et al. Reducing salt intake for prevention of cardiovascular disease in high‐risk patients by advanced health education intervention (RESIP‐CVD study), Northern Thailand: study protocol for a cluster randomised trial. Trials 2012;13:158. [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Aburto 2013
- Aburto NJ, Ziolkovska A, Hooper L, Elliott P, Cappuccio F, Meerphol JJ. Effect of lower sodium intake on health: systematic review and meta‐analyses. BMJ 2013;346:f1326. [DOI] [PMC free article] [PubMed] [Google Scholar]
Alderman 2010
- Alderman MH. Reducing dietary sodium. The case for caution. JAMA 2010;303:448‐9. [DOI] [PubMed] [Google Scholar]
Alderman 2011
- Alderman MH. The Cochrane review of sodium and health. American Journal of Hypertension 2011;24:854‐6. [DOI] [PubMed] [Google Scholar]
Alderman 2012
- Alderman MH, Cohen HW. Dietary sodium intake and cardiovascular mortality: controversy resolved?. American Journal of Hypertension 2012;25:727‐34. [DOI] [PubMed] [Google Scholar]
Allender 2008
- Allender S, Scarborough P, Peto V, Rayner M, Leal J, Luengo‐Fernandez R, et al. European Cardiovascular Disease Statistics 2008. 3rd Edition. European Heart Network, 2008. [Google Scholar]
Alli 1992
- Alli C, Avanzini F, Bettelli G, Bonati M, Colombo F, Corso R, et al. Feasibility of a long‐term low‐sodium diet in mild hypertension. Journal of Human Hypertension 1992;6:281‐6. [PubMed] [Google Scholar]
Arroll 1995
- Arroll B, Beaglehole R. Salt restriction and physical activity in treated hypertensives. New Zealand Medical Journal 1995;108:266‐8. [PubMed] [Google Scholar]
Bayer 2012
- Bayer R, Johns DM, Galea S. Salt and public health: contested science and the challenge of evidence‐based decision making. Health Affairs 2012;31:2738‐46. [DOI] [PubMed] [Google Scholar]
Cappuccio 2011
- Cappuccio F, Capewell S, Lincoln P, McPherson K. Policy options to reduce population salt intake. BMJ 2011;343:d4995. [DOI] [PubMed] [Google Scholar]
Cappuccio 2000
- Cappuccio FP. Sodium, potassium, calcium and magnesium and cardiovascular risk. Journal of Cardiovascular Risk 2000;7:1‐3. [DOI] [PubMed] [Google Scholar]
Cobiac 2010
- Cobiac LJ, Vos T, Veerman JL. Cost‐effectiveness of interventions to reduce dietary salt intake. Heart 2010;96:1920‐5. [DOI] [PubMed] [Google Scholar]
Cook 2007
- Cook NR, Cutler JA, Obarzanek E, Buring JE, Rexrode KM, Kumanyika SK. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow‐up of the trials of hypertension prevention (TOHP). BMJ 2007;334:885‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cook 2014
- Cook NR, Appel LJ, Whelton PK. Lower levels of sodium intake and reduced cardiovascular risk. Circulation 2014;129(9):981‐9. [DOI: 10.1161/CIRCULATIONAHA.113.006032] [DOI] [PMC free article] [PubMed] [Google Scholar]
Costa 1981
- Costa FV, Ambrosioni E, Montebugnoli L, Paccaloni L, Vasconi L, Magnani B. Effects of low‐salt diet and of acute salt loading on blood pressure and intralymphatic sodium concentration in young subjects with borderline hypertension. Clinical Science 1981;61(Suppl 7):21‐3S. [DOI] [PubMed] [Google Scholar]
Dietary Guidelines for Americans 2010
- U.S. Department of Agriculture and U.S. Department of Health & Human Services. Dietary Guidelines for Americans, 2010. Washington DC: US Government Printing Office, December 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
Editor's Note 2013
- Note of Retraction. Heart Online first: 12 March 2013; Vol. 10.1136/heartjnl‐2012‐302337.
Ekinci 2011
- Ekinci E, Clarke S, Thomas M, Moran JL, Cheong K, Maclsaac RJ, et al. Dietary sodium intake and mortality in patients with type 2 diabetes. Diabetes Care 2011;34:703‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elliot 1991
- Elliot P. Sodium and blood pressure: a review of the evidence from controlled trials of sodium reduction and epidemiological studies. Klinische Wochenschrift 1991;69(Suppl 25):3‐10. [PubMed] [Google Scholar]
Elliot 1996
- Elliott P, Stamler J, Nichols R, Dyer AR, Stamler R, Kesteloot H, Marmot M. Intersalt revisited: further analyses of 24 hour sodium excretion and blood pressure within and across populations. Intersalt Cooperative Research Group. BMJ 1996;312(7041):1249‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Graudal 2011
- Graudal NA, Hubeck‐Graudal T, Jurgens G. Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride. Cochrane Database of Systematic Reviews 2011, Issue 11. [DOI: 10.1002/14651858.CD004022.pub3] [DOI] [PubMed] [Google Scholar]
He 2002
- He J, Whelton PK. Commentary: Salt intake, hypertension and risk of cardiovascular disease: an important public health challenge. International Journal of Epidemiology 2002;31:327‐31. [PubMed] [Google Scholar]
He 2004
- He FJ, MacGregor GA. Effect of longer‐term modest salt reduction on blood pressure. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD004937] [DOI] [PubMed] [Google Scholar]
He 2010
- He FJ, MacGregor GA. Reducing population salt intake worldwide: from evidence to implementation. Progress in Cardiovascular Diseases 2010;52(5):363‐82. [DOI] [PubMed] [Google Scholar]
He 2011
- He FJ, MacGregor GA. Salt reduction lowers cardiovascular risk: meta‐analysis of outcome trials. Lancet 2011;378:380‐2. [DOI] [PubMed] [Google Scholar]
He 2013a
- He F, Li J, MacGregor G A. Effect of longer‐term modest salt reduction on blood pressure. Cochrane Database of Systematic Reviews 2013, Issue 4. [DOI: 10.1002/14651858.CD004937.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
He 2013b
- He FJ, Li J, MacGregor GA. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta‐analysis of randomized trals. BMJ 2013;346:f1325. [DOI] [PubMed] [Google Scholar]
Heart 2013
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hooper 2004
- Hooper L, Bartlett C, Davey Smith G, Ebrahim S. Advice to reduce dietary salt for prevention of cardiovascular disease. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD003656.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Institute of Medicine 2013
- IOM (Institute of Medicine). Sodium Intake in Populations: Assessment of Evidence. Washington DC: The National Academies Press, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
Joosten 2014
- Joosten MM, Gansevoort RT, Mukamal KJ, Lambers Heerspink HJ, Geleijnse M, Feskens EJM, et al for the PREVEND Study Group. Sodium excretion and risk of developing coronary heart disease. Circulation 2014;129(10):1121‐8. [DOI: 10.1161/CIRCULATIONAHA.113.004290] [DOI] [PubMed] [Google Scholar]
Jürgens 2004
- Jürgens G, Graudal NA. Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterols, and triglyceride. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD004022.pub2] [DOI] [PubMed] [Google Scholar]
Law 1991
- Law MR, Frost CD, Wald NJ. By how much does dietary salt reduction lower blood pressure? I‐‐Analysis of observational data among populations. BMJ 1991;302:811‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Lim 2012
- Lim S, Vos T, Flaxman A, Danaei G, Shibuya K, Adair‐Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990—2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2224‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lozano 2012
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2095‐128. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mackay 2004
- Mackay J, Mensah G (editors). Atlas of Heart Disease and Stroke. World Health Organization, 2004. [Google Scholar]
MacMahon 1990
- MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J, et al. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990;335:765‐74. [DOI] [PubMed] [Google Scholar]
McHorney 1993
- McHorney CA, Ware Jr JE, Raczek AE. The MOS 36‐item Short‐Form Health Survey (SF‐36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Medical Care 1993;31:247‐63. [DOI] [PubMed] [Google Scholar]
Mente 2013
- Mente A, O'Donnell MJ, Yusuf S. Extreme sodium reductions for the entire population: zealotry or evidence based?. American Journal of Hypertension 2013;26:1187‐90. [DOI] [PubMed] [Google Scholar]
Millett 2012
- Millett C, Laverty AA, Stylianou N, Bibbins‐Domingo K, Pape UJ. Impacts of a national strategy to reduce population salt intake in England: serial cross sectional study. PloS One 2012;7:e29836. [DOI] [PMC free article] [PubMed] [Google Scholar]
Morgan 1980
- Morgan TO, Adams WR, Hiodgson M, Giverd RW. Failure to improve prognosis in elderly males with hypertension. Medical Journal Australia 1980;2:27‐31. [PubMed] [Google Scholar]
Morgan 1987
- Morgan T, Anderson A. Sodium restriction can delay the return of hypertension in patients previously well‐controlled on drug therapy. Canadian Journal of Physiology and Pharmacology 1987;65:1720‐5. [DOI] [PubMed] [Google Scholar]
Murray 2013
- Murray CJL, Lopez AD. Measuring the global burden of disease. New England Journal of Medicine 2013;369:448‐57. [DOI] [PubMed] [Google Scholar]
Neal 2013
- Neal B, Land M‐A, Woodward M. An update on the salt wars ‐ genuine controversy, poor science, or vested interest. Current Hypertension Reports 2013;15(6):687‐93. [DOI] [PubMed] [Google Scholar]
NICE 2010
- National Institute for Health & Clinical Excellence (NICE). Prevention of cardiovascular disease at population level. Public health guidance 25. www.nice.org.uk/guidance/PH25 (accessed 31 May 2011).
O'Donnell 2011
- O'Donnell MJ, Yusuf S, Mente A, Gao P, Mann JF, Teo K, et al. Urinary sodium and potassium excretion and risk of cardiovascular events. JAMA 2011;306:2229‐38. [DOI] [PubMed] [Google Scholar]
Paterna 2008
- Paterna S, Gaspare P, Fasullo S, Sarullo FM, Pasquale P. Normal‐sodium diet compared with low‐sodium diet in compensated congestive heart failure: is sodium an old enemy or a new friend?. Clinical Science 2008;114:221‐30. [DOI] [PubMed] [Google Scholar]
Sacks 2001
- Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH‐Sodium Collaborative Research Group. New England Journal of Medicine 2001;344(1):3‐10. [DOI] [PubMed] [Google Scholar]
SACN 2003
- Scientific Advisory Committee on Nutrition (SACN). Salt and health. https://www.gov.uk/government/publications/sacn‐salt‐and‐health‐report (assessed 31 May 2011).
Silman 1983
- Silman AJ, Locke C, Mitchell P, Humpherson P. Evaluation of the effectiveness of a low sodium diet in the treatment of mild to moderate hypertension. Lancet 1983;1(8335):1179–82. [DOI] [PubMed] [Google Scholar]
Stolarz‐Skrzypek 2011
- Stolarz‐Skrzypek K, Kuznetsova T, Thijs L, Tikhonoff V, Seidlerova J, Richart T, et al. Fatal and non‐fatal outcomes, incidence of hypertension and blood pressure changes in relation to urinary sodium excretion. JAMA 2011;305(1777‐85). [DOI] [PubMed] [Google Scholar]
Strarzzullo 2009
- Strazzullo P, D'Elia L, Kandala NB, Cappuccio FP. Salt intake, stroke, and cardiovascular disease: meta‐analysis of prospective studies. BMJ 2009;339:b4567. [DOI] [PMC free article] [PubMed] [Google Scholar]
Taylor 2011
- Taylor R, Hooper L, Ebrahim S. Dietary salt and cardiovascular disease. Lancet 2011;378:1993. [DOI] [PubMed] [Google Scholar]
Thaler 1982
- Thaler BI, Paulin JM, Phelan EL, Simpson FO. A pilot study to test the feasibility of salt restriction in a community. New Zealand Medical Journal 1982;95:839‐42. [PubMed] [Google Scholar]
Webster 2011
- Webster JL, Dunford EK, Hawkes C, Neal BC. Salt reduction initiatives around the world. Journal of Hypertension 2011;29:1043‐50. [DOI] [PubMed] [Google Scholar]
Whelton 2002
- Whelton PK, He J, Appel LJ, Cutler JA, Havas S, Kotchen TA, et al. Primary prevention of hypertension: clinical and public health advisory from The National High Blood Pressure Education Program. JAMA 2002;288:1882‐8. [DOI] [PubMed] [Google Scholar]
Whelton 2012
- Whelton PK, Appel LJ, Sacco RL, Anderson CAM, Antman EM, Campbell N, et al. Sodium, blood pressure and cardiovascular disease: further evidence supporting the American Heart Association sodium reduction recommendations. Circulation 2012;126(24):2880‐9. [DOI] [PubMed] [Google Scholar]
Whelton 2014
- Whelton PK. Sodium, blood pressure and cardiovascular disease: a compelling scientific case for improving the health of the public. Circulation 2014;129(10):1085‐7. [DOI: 10.1161/CIRCULATIONAHA.114.008138] [DOI] [PubMed] [Google Scholar]
WHO 2012
- World Health Organization. Guideline: Sodium intake for adults and children. Geneva: WHO, 2012. [PubMed] [Google Scholar]