

Abstract
Background
Chronic exposure to stress has been linked to several negative physiological and psychological health outcomes. Among employees, stress and its associated effects can also result in productivity losses and higher healthcare costs. In‐person (face‐to‐face) and computer‐based (web‐ and mobile‐based) stress management interventions have been shown to be effective in reducing stress in employees compared to no intervention. However, it is unclear if one form of intervention delivery is more effective than the other. It is conceivable that computer‐based interventions are more accessible, convenient, and cost‐effective.
Objectives
To compare the effects of computer‐based interventions versus in‐person interventions for preventing and reducing stress in workers.
Search methods
We searched CENTRAL, MEDLINE, PubMed, Embase, PsycINFO, NIOSHTIC, NIOSHTIC‐2, HSELINE, CISDOC, and two trials registers up to February 2017.
Selection criteria
We included randomised controlled studies that compared the effectiveness of a computer‐based stress management intervention (using any technique) with a face‐to‐face intervention that had the same content. We included studies that measured stress or burnout as an outcome, and used workers from any occupation as participants.
Data collection and analysis
Three authors independently screened and selected 75 unique studies for full‐text review from 3431 unique reports identified from the search. We excluded 73 studies based on full‐text assessment. We included two studies. Two review authors independently extracted stress outcome data from the two included studies. We contacted study authors to gather additional data. We used standardised mean differences (SMDs) with 95% confidence intervals (CIs) to report study results. We did not perform meta‐analyses due to variability in the primary outcome and considerable statistical heterogeneity. We used the GRADE approach to rate the quality of the evidence.
Main results
Two studies met the inclusion criteria, including a total of 159 participants in the included arms of the studies (67 participants completed computer‐based interventions; 92 participants completed in‐person interventions). Workers were primarily white, Caucasian, middle‐aged, and college‐educated. Both studies delivered education about stress, its causes, and strategies to reduce stress (e.g. relaxation or mindfulness) via a computer in the computer‐based arm, and via small group sessions in the in‐person arm. Both studies measured stress using different scales at short‐term follow‐up only (less than one month). Due to considerable heterogeneity in the results, we could not pool the data, and we analysed the results of the studies separately. The SMD of stress levels in the computer‐based intervention group was 0.81 standard deviations higher (95% CI 0.21 to 1.41) than the in‐person group in one study, and 0.35 standard deviations lower (95% CI ‐0.76 to 0.05) than the in‐person group in another study. We judged both studies as having a high risk of bias.
Authors' conclusions
We found very low‐quality evidence with conflicting results, when comparing the effectiveness of computer‐based stress management interventions with in‐person stress management interventions in employees. We could include only two studies with small sample sizes. We have very little confidence in the effect estimates. It is very likely that future studies will change these conclusions.
Plain language summary
Computer‐based versus in‐person stress management programmes for workers
What is the aim of this review?
We wanted to find out if stress management programmes at work had a different effect if they were given via a computer, compared to being given in person. We collected and analysed all relevant studies to answer this question. We found two studies that studied the effect of the delivery method on stress reduction in workers.
Key messages
The effects of the delivery method on stress reduction were unclear. More research should be conducted to directly compare equivalent stress management programmes delivered via a computer and in‐person. Any future studies will likely affect the conclusions of this review.
What was studied in the review? Many employers wish to reduce stress in their employees and are willing to invest in stress management programmes. It has been shown that workplace stress management programmes can reduce stress in employees, either when delivered by a computer or mobile device, or by a live person. However, it is unclear if the delivery method itself impacts how effective the programme is. Therefore, we evaluated the effect of the intervention delivery method (computer or in person) to reduce stress in workers.
What are the results of the review?
We found two studies, involving 159 employees, that looked at stress levels in workers after completing stress management programmes on a computer, compared to workers receiving that same programme content from a live person. Both studies taught participants, individually or in small groups, how to recognise and reduce stress, but had conflicting results.
How up to date is this review?
We searched for studies that had been published up to February 2017.
Summary of findings
Summary of findings for the main comparison. Computer‐based interventions compared to in‐person interventions for reducing stress in employees, less than 3 month follow‐up.
| Computer‐based (CB) interventions compared to in‐person (IP) interventions for reducing stress in employees, less than 3 month follow‐up | ||||||
|
Population: employees Settings: any workplace Intervention: computer‐based stress management intervention, less than 3 month follow‐up Comparison: in‐person stress management intervention | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk with in‐person stress management intervention | Corresponding risk with computer‐based stress management intervention | |||||
| Stress Various Measurement Instruments |
0.81 standard deviations higher (0.21 higher to 1.41 higher) in one study and 0.35 standard deviations lower (0.76 lower to 0.05 higher) in another study | data not pooled1 | 159 (2 studies) | ⊕⊝⊝⊝ very low2 | 0.2 standard deviations indicates a small effect 0.5 standard deviations indicates a medium effect 0.8 standard deviations and beyond indicates a large effect |
|
| Burnout | ‐ | ‐ | ‐ | ‐ | ‐ | none of the studies reported this outcome |
| *The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; SMD: standard mean difference | ||||||
| GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate. 1. Pooling of data not appropriate due to considerable heterogeneity (I² > 75%). 2. We downgraded the level of evidence once due to small sample size and underpowered studies. We also downgraded once due to high risk of bias due to incomplete outcome data (high and unequal attrition between interventions). Finally we downgraded once more because of inconsistency, due to considerable heterogeneity precluding meta‐analysis. | ||||||
Background
Description of the condition
Stress can be defined as a relationship between a person and his or her environment that is perceived by the person as taxing, exceeding his or her resources, or endangering his or her well‐being (Lazarus 1984). Consequently, stress depends on environmental factors, an individual’s perception of the environment, and the interaction of the two. Stress elicits short‐term responses, including elevated blood pressure (Backé 2012), and unhealthy behaviours, such as smoking, as coping mechanisms (Conway 1981). Chronic exposure to stress is associated with both physiological and psychological adverse health outcomes, including cardiovascular problems (Brotman 2007; Kivimäki 2013), musculoskeletal problems (Van Rijn 2009), anxiety (Ding 2014; Acquadro 2015; Lee 2015), depression (Hammen 2005), alcoholism (Grunberg 1999), and increased mortality (Levi 1989; Nilsen 2016; Rueppell 2017).
Stress in employees can originate from workplace or work‐related stressors, such as excessive workload or an effort‐reward imbalance (French 1982; Siegrist 1996). It can also originate from individual sources, such as inadequate coping skills (Laranjeira 2012), or from the interaction of work‐related and individual stressors, such as work‐family conflict (Greenhaus 1985). This means that it can be difficult to distinguish stress that originates solely from work‐related stressors from that originating from individual factors or stressors outside the workplace. As such, work‐related or occupational stress can be considered a subset of all stress experienced by employees.
In any case, stress and its associated health effects in employees lead to direct and indirect costs for employers, including higher healthcare costs and reduced productivity from absenteeism and presenteeism (Moreau 2004; Cooper 2008; Ahola 2009). The British Labour Force Survey reported that 1510 per 100,000 workers experienced work‐related stress, depression, or anxiety, resulting in an average of 23.9 days lost per case (HSE 2016). An American survey cited anxiety and stress as the cause of 25 days of absence every year (U.S. Department of Labor 2001). Total costs to society from stress in employees, including related legal and insurance costs, are generally estimated to be around 1% to 3% of Gross Domestic Product (GDP; Rosch 2001; EU‐OSHA 2014).
Description of the intervention
Stress management interventions in the workplace are programmes organized by an employer to reduce the presence of stressors or reduce the negative impact of exposure to these stressors on employees (Ivancevich 1990). They can be categorised according to: 1) their level of focus, and 2) their target (De Jonge 2002; Richardson 2008; Bhui 2012).
First, stress management interventions in the workplace differ in their level of focus. Commonly, workplace stress management programmes are classified as organizational‐level, individual‐organizational‐level, or individual‐level interventions (DeFrank 1987; Jordan 2003). Organizational‐level stress management interventions can include changing the physical and environmental characteristics of the workplace or restructuring the job and its responsibilities (Bergerman 2009). Individual‐organizational‐level stress management interventions can include adding coworker support groups and implementing regular appraisals that try to match employee and employer expectations. Individual‐level stress management interventions can include relaxation, biofeedback, cognitive behavioural therapy (CBT), and time management techniques, among others (Richardson 2008).
Secondly, workplace stress management interventions differ in their target. Often interventions can be classified as targeting primary factors (i.e. stressors), secondary factors (i.e. individual factors), or tertiary factors (i.e. symptoms (Bergerman 2009)).
Traditionally, stress management interventions have been delivered live by a trainer, therapist, or similar expert individual, who personally takes his or her client or clients through the programme. However, the promulgation of technology, and focus on efficient use of resources, has introduced several computer‐based (web and mobile) alternatives to deliver the same interventions without a person physically present to lead the process (Andersson 2009; Carey 2009; Andrews 2010; Mohr 2010). Consequently, stress management interventions can also be classified a third way, according to their delivery method.
Computer‐based stress management interventions in the workplace
The term 'computer‐based' is used here to refer to any delivery method that uses technology and is not delivered live and in‐person (face‐to‐face). As such, self‐taught methods using books or print material would not fall into either of the groups defined in this review. In general, any computer‐based intervention (e.g. to address health promotion or mental health) is more commonly text‐based, and aimed at education and goal setting, using modules with a fixed order. In some cases, the content has been developed earlier for an offline programme, and has been made available on an easily accessible electronic platform, such as a website or software (Ludden 2015). Computer‐based interventions can be delivered by or accessed via a computer, text message, email, mobile phone application, CD player, or web browser (Zetterqvist 2003; Griffiths 2006; Ruwaard 2007). They can also vary according to the media used (e.g. text, audio recording, video, or game), and degree of therapist involvement (e.g. from entirely self‐help to remote client‐therapist interaction (Proudfoot 2011)).
A key characteristic of computer‐based interventions is whether or not the intervention is guided or unguided (self‐guided). Guided interventions have some kind of human support, which can come in the form of email reminders, counsellor support, or peer support groups (Brouwer 2011; Baumeister 2014). Furthermore, the guidance can be classified by whether or not it is synchronous, by the qualifications of the one giving guidance (e.g. trained therapist or non‐clinical support), by the mode of guidance (e.g. email reminders or live chat), and the dosage or frequency of guidance (Baumeister 2014).
Computer‐based stress management interventions are generally focused on the individual level. They can use a variety of theoretical bases, such as CBT, mindfulness, or physical activity. Unguided or self‐paced interventions are more common for computer‐based stress management interventions (Heber 2017). The duration of computer‐based stress management interventions in the workplace generally vary from two to 12 weeks (Heber 2017). Employees can access the intervention via work‐provided devices or their personal devices. Interventions can be either self‐paced or have a regular schedule.
In‐person stress management interventions in the workplace
In‐person stress management interventions in the workplace can be delivered by a trained instructor, counsellor, practitioner, or teacher, and they can occur in small groups or in one‐on‐one sessions. The sessions can be as short as 15 minutes or as long as one day. Similar to computer‐based methods, they generally focus on the individual level. The duration of workplace in‐person stress management interventions is usually similar to computer‐based stress management interventions, ranging from two to 12 weeks (Richardson 2008).
How the intervention might work
In general, workplace stress management interventions aim to reduce stressors, improve reactions to stressors, or mitigate physiological or psychological effects from stress. Both computer‐based and in‐person delivery methods can use these mechanisms. However, only certain interventions, usually directly targeting workers, can be transposed into computer‐based ones (e.g. CBT, mindfulness, problem solving training).
Computer‐based workplace stress management interventions most commonly ‐ but not exclusively ‐ operate on the individual level and target secondary prevention. Secondary prevention stress management interventions aim to modify an employee’s perception of, or ability to cope with, or respond to, existing stressors. Often, the interventions use cognitive behavioural techniques, meditation or relaxation, exercise, or time management techniques. Cognitive behavioural techniques educate employees about the roles of their thoughts and emotions in stressful events to provide new ways to feel, think, and act in stressful situations. Meditation and relaxation divert attention away from stress. Exercise provides a physical release from tension, increases endorphins, or provides an outlet for anger. Time management techniques allow an employee to reduce the work‐demand imbalance.
While the theoretical mechanisms of stress management interventions' effect on stress should be dependent on the level (i.e. primary, secondary, tertiary) and technique, the delivery method may affect the outcome by facilitating or mitigating exposure and adherence. Computer‐based interventions are known to commonly suffer from higher attrition, reduced exposure, and less adherence, compared to in‐person interventions (Kelders 2012). While in‐person interventions can be more responsive to participants, computer‐based interventions are more prone to a mismatch between the goals of the intervention and the goals of the participants, and are less flexible in adjusting to situations and user characteristics, which have been associated with higher attrition (Kelders 2011; Postel 2011; Ludden 2015). Consequently, some computer‐based interventions add a guidance component (i.e. a form of human support) or adherence‐facilitating component, such as automated prompts (Baumeister 2014). Guided interventions have been shown to be significantly more effective at symptom reduction and increased intervention completion than unguided interventions (Baumeister 2014; Heber 2017). Guidance in the form of peer support, counsellor support, and email contact may increase exposure, which may increase adherence, and thus, the efficacy (Brouwer 2011; Baumeister 2014).
Why it is important to do this review
In‐person interventions have been shown to be effective in reducing stress in employees, when compared to a control (Van der Klink 2001; Richardson 2008; Bhui 2012; Ruotsalainen 2015). Computer‐based interventions have also been shown to be effective in reducing stress in employees, when compared to a control (Heber 2017). However, computer‐based interventions offer many advantages to employers: they are easily accessible at any time or place; greater anonymity is possible; workers can follow the course whenever and wherever they wish; they may reach workers earlier than traditional health services; they can cost less; and computer‐based interventions are easily scalable (Griffiths 2006; Ebert 2017).
However, a systematic review directly comparing computer‐based and in‐person stress management interventions among workers has not yet been completed. Such a review could provide the necessary evidence to help employers and occupational health services choose the best method for reducing stress in their employees. This Cochrane review aims to fill this gap in the evidence base.
Objectives
To compare the effects of computer‐based interventions to in‐person interventions for preventing and reducing stress in employees.
Methods
Criteria for considering studies for this review
Types of studies
We included only randomised controlled trials (RCTs).
Types of participants
We included studies in which participants were full‐time, part‐time, or self‐employed working individuals over 18 years of age.
Types of interventions
We considered for inclusion all studies assessing the effectiveness of any type of worker‐focused web‐based stress management intervention, aimed at preventing or reducing work‐related stress with techniques such as CBT, relaxation, time management, or problem‐solving skills training. These interventions had to be delivered via email, a website, or a stand‐alone computer programme, and they had to be compared to a face‐to‐face stress management intervention with the same content (e.g. web‐based CBT versus face‐to‐face CBT). Interventions could vary by the device providing access (e.g. computer, laptop, or mobile device), the type of multimedia used (e.g. text, graphics, animations, audio, video), and the degree of therapist involvement (from entirely self‐help to remote client‐therapist interaction).
The in‐person comparator interventions could be delivered by a trained instructor, counsellor, practitioner, or teacher, and they could occur in small groups or in one‐on‐one sessions.
Types of outcome measures
Primary outcomes
We included studies that measured the effect of the interventions on stress or burnout in employees. We included studies measuring:
stress with Perceived Stress Scale (PSS (Cohen 1983)), Occupational Stress Inventory (OSI (Osipow 1998)), or similar; or
burnout with Maslach Burnout Inventory (MBI (Maslach 1996)) or similar.
Secondary outcomes
Sick leave
Absenteeism
Return to work
We considered self‐reported stress and burnout scales to be subjective outcome measures, while sick leave, absenteeism, and return to work could be objective outcome measures, as long as the employer, rather than the worker, supplied the data.
Studies could measure time until partial RTW as:
number of days of sick leave until partial RTW;
total number of days of partial sick leave during follow‐up; or
rate of partial RTW at follow‐up measurements.
They could measure time until full RTW as:
number of days of sick leave until full RTW;
total number of days of full‐time sick leave during follow‐up; or
rate of full RTW at follow‐up measurements.
We did not include the reporting of one or more of the secondary outcomes listed here as an inclusion criterion for the review.
Search methods for identification of studies
Electronic searches
We conducted a systematic literature search to identify all published and unpublished trials eligible for inclusion. We adapted the search strategy developed for MEDLINE to use in the other electronic databases. We did not impose any limitation on the language of publication. In future updates, if we identify any potentially eligible papers in languages other than those spoken by the review team, we will either arranged for the translation of key sections prior to assessment, or arrange for their full assessment by people who are proficient in the publications' language(s).
We searched the following electronic databases from inception to 27 February 2017 to identify potential studies (i.e. no date restrictions):
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 2) in the Cochrane Library (searched 27 February 2017; Appendix 1);
MEDLINE Ovid (1946 to 27 February 2017; Appendix 2);
PubMed (Appendix 3);
Embase Ovid (1974 to 27 February 2017; Appendix 4);
PsycINFO Ovid (1806 to 27 February 2017; Appendix 5);
NIOSHTIC, NIOSHTIC‐2, HSELINE, CISDOC (OSH‐UPDATE; Appendix 6);
ClinicalTrials.gov and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP; Appendix 7).
Searching other resources
We checked reference lists of all articles that we retrieved as full‐text articles, related systematic, and narrative reviews in order to identify additional potentially eligible studies. We contacted other researchers, but they did not identify any unpublished studies.
Data collection and analysis
Selection of studies
Three review authors (AA, TD, YLT) independently screened the titles and abstracts of all the potentially eligible studies we identified during the search, and coded them as 'retrieve' (eligible, potentially eligible, or unclear) or 'do not retrieve'. We coded studies as 'do not retrieve' if the title and abstract provided sufficient information to decide that the study did not fulfil our inclusion criteria. We excluded studies in this phase only if the study clearly was not randomised or clearly had no computer‐based stress management intervention.
We retrieved the full‐text study reports or publications, and three review authors (AK, YLT, QDM) independently screened these for inclusion, also noting the reasons for excluding the ineligible studies in the 'Characteristics of excluded studies' table. From full‐text review, we were able to identify and exclude duplicates (e.g. study protocols or conference presentations of included studies) and multiple reports of the same study, so that each study, rather than each report, was the unit of interest in the review. We resolved any disagreement through discussion, or if required, we consulted one of the remaining two authors (AA, TD).
Data extraction and management
Three review authors (AK, YLT, QDM) independently extracted the following study characteristics, using a standard data collection form.
Methods: study design, total duration of study, study location (country), study setting, and date of study.
Participants: number of participants and allocation to intervention groups, method of analysis ('as‐treated' or 'intention‐to‐treat'), demographic data, inclusion criteria, and exclusion criteria.
Interventions: description of intervention, comparison, duration, intensity, content of both intervention and control condition, and co‐interventions.
Outcomes: description of primary and secondary outcomes specified and collected, and time points reported.
Notes: funding for trial, notable conflicts of interest of trial authors, and other sources of information (e.g. communication with author or another publication of same study).
We noted in the 'Characteristics of included studies' table if outcome data were not reported in a usable way. We resolved disagreements by consensus or by involving a fourth review author (TD). One review author (AK) transferred data into the Review Manager 5 file (RevMan 2014). We double‐checked that data were entered correctly by comparing the data presented in the systematic review with the study reports.
Assessment of risk of bias in included studies
Two review authors (TD, AK) independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We resolved any disagreements by discussion or by involving a third author (QDM). We assessed the risk of bias according to the following domains:
Random sequence generation.
Allocation concealment.
Blinding of participants and trial personnel.
Blinding of outcome assessment.
Incomplete outcome data.
Selective outcome reporting.
Other sources of bias.
In addition to evaluating risk of bias in these standard domains, we added two domains: the presence or absence of co‐interventions (and if included, their degree of similarity to the intervention), and treatment fidelity. The idea was that these two additional domains would shed light on theory failure or programme failure pertinent to the intervention being evaluated.
We graded each potential source of bias as high, low, or unclear and provided a justification in the 'Risk of bias' table in RevMan 5 (RevMan 2014). We considered random sequence generation, allocation concealment, selective outcome reporting, and incomplete outcome data to be key domains. We judged a study to have a high overall risk of bias when we judged one or more key domains to have a high risk of bias. For instance, a study with substantial variation in attrition between treatment and comparison groups, which had not been appropriately accounted for, warranted a high risk of bias assessment for incomplete outcome data, and as a result, for the overall study. Conversely, if a future study is identified in which we judge all key domains to be at low risk of bias, we will judge the study to have low overall risk of bias. We summarised the risk of bias judgements across different studies for each of the domains listed. Where information on risk of bias related to unpublished data or correspondence with a study author, we noted this in the 'Risk of bias' table.
Assessment of bias in conducting the systematic review
We conducted the review according to the methods reported in our published protocol (Kuster 2015). We reported all deviations from the published protocol in the Differences between protocol and review section of the review.
Measures of treatment effect
The included studies measured stress with self‐report instruments that yielded continuous data. We put means, standard deviations, and the number of participants for each arm of the study, from the latest available reporting time, into the data tables in RevMan 5 (RevMan 2014). Because the included studies used different instruments, we calculated the standardised mean difference (SMD) with a 95% confidence interval (CI) between groups as the summary effect measure. The included studies did not report any dichotomous outcomes.
We considered whether the computer‐based delivery mode was equivalent to the in‐person delivery mode. We defined equivalence to mean that the difference in effect size between the two interventions was 0.2 SMD or less. Since there is no generally accepted minimal clinically important difference for measures of stress (i.e. an amount of change that on average would be perceived as improvement by a participant), we believe this approach provides a reasonable approximation.
Unit of analysis issues
The included studies' interventions aimed to achieve changes at the individual level (in thinking, feelings, behaviour, or all three) in order to reduce the level of stress. Hence, the unit of analysis was the individual. For studies that used a cluster‐randomised design and did not consider the design effect in the analyses, we had planned to calculate the design effect by following the methods stated in the Cochrane Handbook for Systematic Reviews of Interventions for the calculations, using a fairly large assumed intra cluster correlation of 0.10 (Campbell 2001; Higgins 2011). However, we found no cluster‐randomised studies to include in this review, and thus did not need to consider design effects.
Dealing with missing data
If the SDs were not presented in the publication, we contacted the authors with a request to provide these data. Whenever authors were unable or unwilling to provide this information, we calculated SDs from available information following the instructions of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Assessment of heterogeneity
We assessed clinical heterogeneity based on the degree of similarity in the population, interventions, outcomes, and follow‐up periods. Due to the nature of the interventions and the narrowness of our inclusion criteria (i.e. adult workers), we did not expect to find study populations with significant differences, and we did not.
We considered follow‐up times of less than three months, three months to one year, and more than one year to be different. Our included studies only provided short‐term follow‐up data.
If we include sufficiently similar studies in future updates of this review to conduct meta‐analyses, we will assess heterogeneity by visual inspection of forest plots, and by using the I² statistic. We will then quantify the degree of heterogeneity as follows (Higgins 2011).
0% to 40% might not be important
30% to 60% may represent moderate heterogeneity.
50% to 90% may represent substantial heterogeneity.
75% to 100% equals considerable heterogeneity.
In the presence of substantial heterogeneity and a sufficient number of studies, we will conduct subgroup analyses as described below in Subgroup analysis and investigation of heterogeneity.
When we found considerable heterogeneity (I² > 75%), we did not pool the data, and downgraded the quality of the evidence because of inconsistency, according to the GRADE system (see Data synthesis and Quality of the evidence for details).
Assessment of reporting biases
We tried to prevent location bias by searching across multiple databases, and language bias by including all eligible articles, regardless of publication language. When we detected multiple articles on the same study, we extracted data only once. If we can include a sufficient number of studies in future updates of this review, we will assess publication bias using funnel plots, and we will test for funnel plot asymmetry (Higgins 2011).
Data synthesis
We judged both included studies to be sufficiently clinically homogeneous to be reported in a single comparison. However, because the I² value of their pooled numerical results exceeded 75%, we refrained from reporting the pooled results, and we analysed the results for each study separately using Review Manager 5 software (RevMan 2014). If future updates of this review identify studies that are less statistically heterogeneous, such that results can be pooled in one or more meta‐analyses, we will use a random‐effects model and combine effect sizes using the general inverse variance method. In such a case, we will conduct a sensitivity check by using the fixed‐effect model to compare differences in results. However, if the heterogeneity might not be important (I² ≤ 40%), we will use a fixed‐effect model. We included a 95% confidence interval (CI) for the intervention effect of studies.
When studies reported multiple trial arms, we only included the relevant arms. Had we needed to include two comparisons from one study (e.g. intervention A versus face‐to‐face intervention and intervention B versus the same face‐to‐face intervention) in the same meta‐analysis, we would have halved the number of participants in the control group to avoid double‐counting.
Quality of the evidence
We used the GRADE approach, as described in the Cochrane Handbook for Systematic Reviews of Interventions, to assess the quality of the body of evidence for the primary outcomes (Higgins 2011). The quality of a body of evidence for a specific outcome is based on five factors: 1) limitations of the study designs; 2) indirectness of evidence; 3) inconsistency of results; 4) imprecision of results; and 5) publication bias.
The GRADE approach specifies four levels of quality (high, moderate, low, and very low), incorporating the factors noted above. Quality of evidence by GRADE should be interpreted as follows:
High‐quality: We are very confident that the true effect lies close to that of the estimate of the effect;
Moderate‐quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different;
Low‐quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect;
Very low‐quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
Subgroup analysis and investigation of heterogeneity
Given the limited number of studies included in this review, we could not perform subgroup analyses. If there are sufficient data in future updates of this review, we will undertake subgroup analyses based on type of workers (e.g. salaried versus hourly, or blue‐ versus white‐collar workers), techniques used in the computer‐based intervention (e.g. CBT versus relaxation), and level of human support (e.g. guided versus unguided). Since our criteria for inclusion were limited to studies involving a face‐to‐face intervention comparator, we would not require further analyses by comparator arm.
If future updates of this review include studies that report a return‐to‐work outcome in multiple ways (e.g. full‐time, part‐time), we will conduct a subgroup analysis to see if there is a difference.
We will use the Chi² statistic to test for subgroup interactions in Review Manager 5 (RevMan 2014).
Sensitivity analysis
We explored the impact of including studies with missing data and multiple reports of the primary outcome, which could introduce bias, with a sensitivity analysis. We used the sensitivity analysis (and the inherent estimates) to understand how the conclusions were affected by the choice of data used in the comparison.
We had also planned to perform a sensitivity analysis to test the robustness of our results by omitting studies with a high overall risk of bias. However, we could not conduct this sensitivity analysis, because we judged both included studies to have a high risk of bias.
'Summary of findings' table
We created a 'Summary of findings' table that reported on the primary outcomes, stress and burnout. The table omits secondary outcomes (sick leave, absenteeism, and return to work) because none of the included studies reported these outcomes. If future studies are identified to warrant multiple comparisons (e.g. different follow‐up times), we will add additional 'Summary of findings' tables. We used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to assess the quality of the body of evidence for each outcome. We used the methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions, and used GRADEpro GDT software to develop the 'Summary of findings' table (Higgins 2011; GRADEpro GDT 2015). We were transparent, and justified all decisions to downgrade the quality of evidence in the footnotes.
Results
Description of studies
Results of the search
We ran the original search in February 2016, which identified 2037 unique records for review. We updated the search strategy to use consistent keywords across databases and to be more sensitive, and then we re‐ran it in February 2017. Figure 1 displays a PRISMA study flow chart of the inclusion process from the updated February 2017 search, which identified 5004 records. After removing duplicates, we identified 3431 unique reports to assess against our inclusion and exclusion criteria. We assessed the titles and abstracts of these 3431 reports, and identified 89 reports to be read as full text. After identifying duplicates (e.g. study protocols or conference presentations of included studies) and multiple reports of the same study, we considered 75 unique studies for inclusion. We excluded 73 of those and included two studies in this Cochrane review.
1.
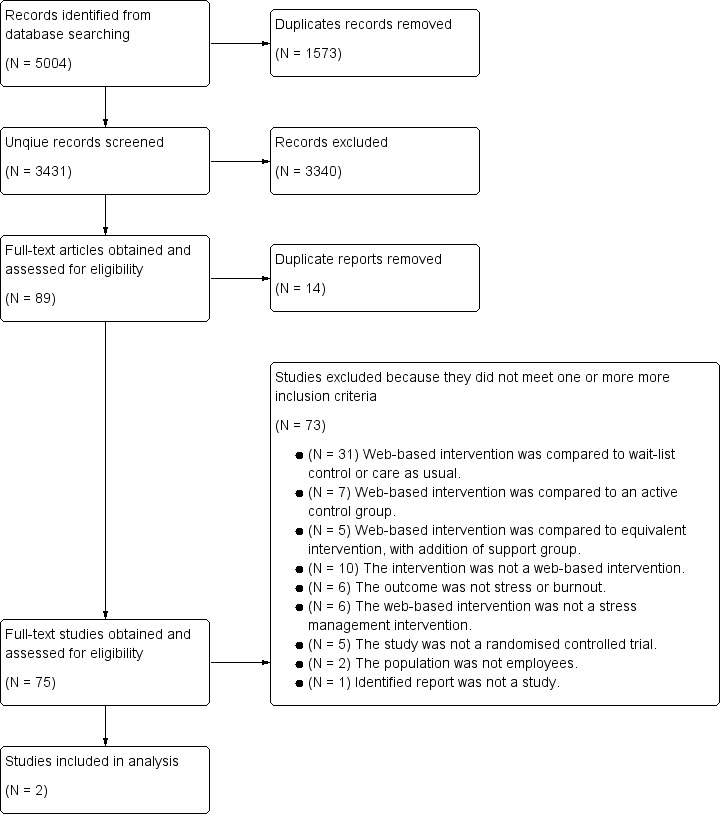
PRISMA study flow diagram
Included studies
Study design
We included two randomised controlled trials (Eisen 2008; Wolever 2012). Both used a parallel group design with three arms. We only analysed the data from the two arms that compared computer‐based interventions to equivalent in‐person interventions. Details can be found in the 'Characteristics of included studies' table.
Country and time period
Both trials were set in the USA, between 2000 and 2010.
Type of settings and participants
In the Eisen 2008 study, the 63 included participants were a mix of hourly workers and salaried workers from three different manufacturing sites of a single corporation. In the Wolever 2012 study, the 96 included participants were almost entirely full‐time employees from two different sites of a single national insurance company. In both studies, the majority of participants were white, Caucausian, married, and had at least a college education.
Sample sizes
A total of 159 participants completed the interventions in the included arms of the included studies. A total of 92 participants completed the in‐person interventions, and a total of 67 participants completed the computer‐based interventions. The sample sizes were generally small. One study's computer‐based arm had fewer than 20 participants, while all other arms had between 20 and 60 participants.
Interventions
Both studies delivered education ‐ broken into eight to 12 modules ‐ about stress and its causes, together with strategies to reduce stress or its causes, to employees via a computer. In the Eisen 2008 study, the video was prerecorded, and delivered via computer software, and the modules could be completed at any time. In the Wolever 2012 study, the education was delivered live on a computer via a virtual classroom with bi‐directional communication between teacher and participants. However, if participants missed the online class, they could watch a video recording of it. Thus, we judged the Eisen 2008 study to have provided an unguided intervention, and the Wolever 2012 study to have provided a guided intervention.
In Eisen 2008, the total education time was one and one‐half to two hours, completed over a two‐week period; in Wolever 2012, it was 14 hours completed over a 12‐week period.
Both studies compared the computer‐based intervention to an in‐person intervention with the same educational content. A teacher delivered the in‐person intervention to small groups of up to 28 people.
Outcomes
Both studies measured stress as an outcome. The Wolever 2012 study used the 10‐item Perceived Stress Scale (PSS). The Eisen 2008 study used two stress outcomes: Subjective Units of Distress Scale (SUDS), and a 12‐item Stress Survey (composite of stress‐related items from Johnson & Johnson Health Care System Insight combined with Health Risk Appraisal survey and Occupational Stress Inventory ‐ Revised Edition). We used the latest available outcome measurement for which sufficient information was available.
Neither of the included studies measured burnout as an outcome, which we had defined as our second primary outcome.
Neither of the included studies measured any of our secondary outcomes.
Follow‐Up
Both studies used short‐term follow‐up (less than one month). The Eisen 2008 study had a one‐month follow‐up but the authors did not report the data from that follow‐up. Thus we used the post‐intervention data in our quantitative analysis. The Wolever 2012 study had a two‐week follow‐up.
Missing information
We sought and obtained additional information on study details and statistical data from the authors of both included studies. One author of the Eisen 2008 study provided a PhD thesis published in 2005 that reported SDs for outcomes at post‐intervention, and answered questions about study details for assessing risk of bias. However, the authors were unable to provide missing SDs for the Stress Survey instrument at one‐month follow‐up. One author of the Wolever 2012 study answered questions about study details for assessing risk of bias, but was unable to provide SDs. We reported all information obtained via correspondence with authors in the 'Characteristics of included studies' table.
Excluded studies
We read 91 reports as full‐text, and excluded 89 of them because they did not meet our inclusion criteria (see 'Characteristics of excluded studies' table). In some cases, studies could have been excluded for more than one reason. In those cases, we listed the highest priority reason for exclusion.
Most commonly, we excluded studies because they compared a computer‐based stress management intervention against a wait‐list control only (e.g. Ruwaard 2007; Billings 2008; Heber 2016; Hammer 2015), or they compared a computer‐based intervention to an active control group that contained different content than the computer‐based intervention (e.g. Cook 2007; Rose 2013; ACTRN12615000574549; Erdman 2015). In other cases, we excluded studies because the computer‐based intervention was not a stress management intervention (e.g. Kawakami 2005; Van Drongelen 2013), or the outcome of the study was not stress or burnout (e.g. Prochaska 2008; Schell 2008; Hasson 2010).
Other, less common reasons for exclusion were: the study was not a randomised controlled trial (e.g. Mackenzie 2014; Zarski 2016); the population was not employees (Wiegand 2010; Drozd 2013); the intervention was not web‐ or computer‐based (e.g. Bragard 2009; Noordik 2013; Baker 2015), or it was not actually a study at all (Hughes 2013).
Risk of bias in included studies
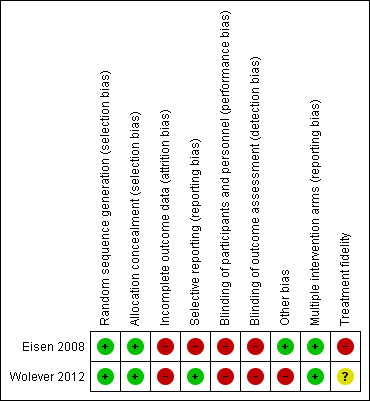
We judged both included studies as being at low risk of bias for random sequence generation and allocation concealment. On the other hand, we judged both included studies as being at high risk of bias due to incomplete outcome data, which was caused by attrition. We also judged the Eisen 2008 study as being at high risk of bias due to selective reporting.
We judged a study to have an overall high risk of bias when we assessed one of the key domains (random sequence generation, allocation concealment, selective outcome reporting and incomplete outcome) as being at high risk of bias. Consequently, we considered the overall risk of bias to be high in both included studies (Eisen 2008; Wolever 2012).
Figure 2 reports the 'Risk of bias' assessments for the two studies. Details for the judgments can be found in the 'Characteristics of included studies' tables.
2.
Allocation
While the publications only reported that they 'randomised participants', personal communications with the authors provided evidence that they used adequate randomisation methods, including both the random sequence generation and allocation concealment, to warrant a judgment of low risk of bias in this domain.
Blinding
Both Eisen 2008 and Wolever 2012 measured stress by means of self‐reported questionnaires. Such outcome measures could be biased by knowledge and expectations of the intervention. This could create an overestimation of the effect of the intervention. The authors of neither included study mentioned that blinding could be an issue. We judged both studies as being at high risk of performance and detection bias due to their use of self‐reported outcome measures.
Incomplete outcome data
We judged both included studies as having a high risk of bias due to incomplete data caused by attrition. In both studies, attrition proportions were statistically significantly different between the two intervention arms analysed in this review (P < 0.05). Both studies had at least one study arm with more than 20% attrition. The study by Eisen 2008 suffered significant dropouts. In that study, 64% of participants from the in‐person group and 88% from the computer‐based group did not complete the intervention, with the majority of the dropouts occurring between randomisation and the start of the intervention. These high dropout rates reduced the effectiveness of randomisation and introduced potential confounding that may explain differences in the intervention effect more than the delivery method variable.
Selective reporting
The authors of the Wolever 2012 study had published a protocol that they provided to us upon request, and the outcomes reported in their study matched the ones in the protocol and their stated study objectives. Therefore, we judged the risk of bias from selective reporting as low. However, in the Eisen 2008 study, the authors collected data for two stress outcome measures, but we could not calculate an effect size from one of the measures, because the authors did not publish SDs, nor could they provide them when queried. The authors did not report the results that were not statistically significant, which were possibly more appropriate than the statistically significant results they chose to publish. Our sensitivity analysis confirmed different conclusions based on the selection of outcome measure. Consequently, we judged the study as being at high risk of bias due to selective reporting.
Other potential sources of bias
We judged the Wolever 2012 study as being at a high risk of bias because the study was funded by the owner of the software used in the intervention, which is a clear conflict of interest. We could not identify any other sources of bias in the Eisen 2008 study. Thus, we judged it as being at low risk of bias for this domain.
Presence of co‐interventions
Neither of the two included studies reported that their participants receiving any other interventions in addition to either the in‐person or computer‐based stress management intervention. Therefore, we judged both studies as being at low risk of bias for this domain.
Treatment fidelity
We judged the Wolever 2012 study as having an unclear risk of bias due to treatment fidelity, because we could not determine if sufficient measures were implemented to ensure the intervention was delivered as planned. We judged the Eisen 2008 study as being at high risk of bias due to problems in treatment fidelity that were caused by technological issues and inadequate monitoring of adherence in the computer‐delivered group.
Effects of interventions
See: Table 1
Both included studies reported stress outcomes such that a higher number indicated a higher amount of stress. To compare results produced with different scales, we used the standardised mean difference (SMD) with a 95% confidence interval (CI) between the intervention and comparison groups as the summary effect measure. Thus, a negative effect measure indicated a lower stress outcome in the intervention group (computer‐based stress management interventions) compared to the comparator group (in‐person stress management interventions with equivalent content) ‐ that is, favouring the computer‐based intervention.
1. Web‐based interventions versus in‐person interventions for reducing stress in workers
1.1 Any stress outcome, follow‐up less than three months
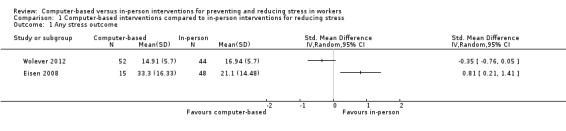
Two studies (159 participants) compared stress levels in employees after a stress management intervention delivered via computer‐based means to equivalent interventions delivered in‐person. Both studies had follow‐up times shorter than one month. Heterogeneity between the results obtained by the two studies was very high (I² = 90%) and the confidence intervals did not overlap. Thus, we did not pool the data in a meta‐analysis. Instead, we reported the results of the studies individually. Eisen 2008 found that stress levels were statistically significantly lower in the in‐person group (0.81 standard deviations, 95% CI 0.21 to 1.41) immediately after the intervention, while Wolever 2012 did not find a clear difference between the groups (‐0.35 standard deviations, 95% CI ‐0.76 to 0.05) one month after the intervention (Analysis 1.1). Table 2 reports the results of the two studies in their original scales.
1.1. Analysis.
Comparison 1 Computer‐based interventions compared to in‐person interventions for reducing stress, Outcome 1 Any stress outcome.
1. Effect estimates of included studies reported in original outcome scales.
| Study, outcome scale | Assumed risk, in‐person stress management intervention | Corresponding risk, computer‐based stress management intervention | Effect estimate (95% CI) | ||
| Mean (SD) | No. of participants | Mean (SD) | No. of participants | ||
| Eisen 2008, SUDS | 21.1 (14.48) | 48 | 33.3 (16.33) | 15 | +12.2 (+2.98 to +21.4) |
| Wolever 2012, PSS‐10 | 16.94 (5.7) | 44 | 14.91 (5.7) | 57 | ‐2.03 (‐4.32 to +0.26) |
| SD = standard deviation CI = confidence interval SUDS = Subjecive Units of Distress Scale PSS‐10 = Perceived Stress Scale | |||||
1.2 Any burnout outcome
Neither of the included studies evaluated the effectiveness of their interventions using a burnout measure.
1.3 Sensitivity analysis: effect of selective outcome reporting and missing data
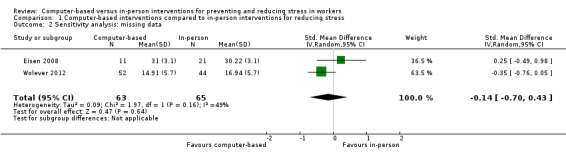
We conducted a sensitivity analysis to simultaneously assess the impact of two potential sources of bias: 1) the availability of more than one outcome measure for the primary outcome and, correspondingly, 2) selective reporting of data. Eisen 2008 reported the means for a second stress outcome measure (sum of Likert‐type items on Stress Survey) without SDs. This measure of stress was more clinically similar to the Wolever 2012 study in content and follow‐up time. Without SDs, this outcome measure could not be used in a meta‐analysis. However, the authors did report that ANOVAs between the items were non‐significant (P > 0.05). Therefore, we assumed P values from 0.1 to 0.7 (see Analysis 1.2 for an illustration of the results assuming P = 0.50). This led to an estimate range from 1.2 to 5.4 of the SD of the outcomes for each intervention, when we used the calculator tool provided in Review Manager 5 (RevMan 2014; see Table 3). This significantly changed the conclusion of the study from 95% CI not inclusive of no effect (as presented in Analysis 1.1) to 95% CI inclusive of no effect. The results of our sensitivity analysis showed that the choice of outcome measure and missing data significantly impacted the heterogeneity of results when pooled in meta‐analysis. Taking the Stress Survey results from Eisen 2008, instead of the SUDS scores reported in our Analysis 1.1, and combining these data with the PSS data obtained from Wolever 2012, led to I² values ranging from 26% to 80%.
1.2. Analysis.
Comparison 1 Computer‐based interventions compared to in‐person interventions for reducing stress, Outcome 2 Sensitivity analysis: missing data.
2. Sensitivity analysis results: effect of selective outcome reporting by assuming P value to impute missing data.
| Assumed P value | t value1 | SE1 | SD1 | I² (Meta‐analysis)2 | SMD (95% CI), Eisen 20082 |
| 0.1 | 1.7 | 0.46 | 1.23 | 80% | 0.62 (‐0.13 to 1.37) |
| 0.3 | 1.05 | 0.74 | 1.99 | 66% | 0.38 (‐0.35 to 1.12) |
| 0.5 | 0.68 | 1.15 | 3.08 | 49% | 0.25 (‐0.49 to 0.98) |
| 0.7 | 0.39 | 2.00 | 5.37 | 26% | 0.14 (‐0.59 to 0.87) |
| Comparison to meta‐analysis (post‐intervention SUDS), Analysis 1.1 | |||||
| N/A | 90% | 0.81 (0.21, 1.41) | |||
| SD = standard deviation, SE = standard error, SMD = standard mean difference, SUDS = Subjecive Units of Distress Scale 1. Imputed using RevMan 5 for estimating SDs from P values, entering n1 = 11, n2 = 21, difference in means = 0.78 2. Computed using RevMan | |||||
Discussion
Summary of main results
We included two RCTs with a total of 159 participants in this Cochrane review. Both studies evaluated interventions consisting of education about stress and its causes, as well as strategies to reduce stress, delivered via a computer. Both studies compared computer‐based intervention delivery to interventions with the same content provided to another group of employees by a live instructor. The results were substantially heterogeneous and could not be pooled in a single meta‐analysis. Considering the studies independently, one study found no evidence of a difference between a computer‐based method or an in‐person method. The other study found that a computer‐based method was significantly less effective than an in‐person method. However, another more appropriate measure of stress from that same study, which could not be used in this review due to missing data, would most likely have found a similar result of no evidence of a difference between a computer‐based method or an in‐person method. We judged both studies as being at high risk of bias overall. According to our judgment, the quality of the evidence produced by these two studies was very low.
Overall completeness and applicability of evidence
We found two studies comparing computer‐based and in‐person stress management interventions at the workplace. Both studies were conducted in the USA and they covered only a narrow range of occupations. Therefore, the generalisibility of these findings to other countries and other occupations is limited. While our inclusion criteria aimed to capture studies from any location or any occupation, research directly comparing computer‐based and in‐person stress management interventions has not been extensively conducted. In addition, the limited number of studies conducted to date was insufficient to adequately answer our review's objective.
We found studies that used cognitive behavioural and relaxation techniques. There are many other techniques for workplace stress management, such as exercise, goal‐setting, or journaling. The included studies used computers and video. However, now there is a broader range of delivery technologies, such as mobile devices. Therefore, it is unclear if any conclusions from this study would apply to other techniques and delivery technologies. The included studies were either completely unguided or guided. Other forms of guidance and adherence support exist, such as reminders or peer support groups. It is unclear from this review what difference the level of guidance makes when compared to in‐person versions.
Because we limited our review objective to comparing the effectiveness of computer‐based and in‐person interventions, we could not include organizational‐level interventions to reduce stress.
The follow‐up in both included studies was short, so it is uncertain what long‐term effects these interventions may have.
Quality of the evidence
We judged the overall quality of the evidence provided by the included studies to be very low. We downgraded the quality of evidence due to high risk of bias caused by study limitations (serious attrition bias), imprecision (limited sample size and wide confidence intervals), and substantial statistical heterogeneity. Due to heterogeneity, we were unable to combine the results of the two studies in a meta‐analysis. Significant statistical heterogeneity does not necessarily suggest that the true intervention effect is very different. Instead, it may arise from methodological diversity or differences in outcome assessments. One significant form of bias affecting the results of this review arose from incomplete data due to attrition and selective reporting (see 'Characteristics of included studies' table). Our sensitivity analysis also revealed that the choice of outcome measure and selective reporting in one study significantly influenced the overall estimated effect size.
Due to the small number of included studies, we could not assess publication bias.
The overall outcome of very low‐quality evidence means that there is substantial room for improvement in future studies.
Potential biases in the review process
We used a search strategy that was very broad and put very few restrictions on inclusion (e.g. any language, any workplace, any country, any stress intervention type, any date), which was reflected in the large number of reports identified by our search strategy. We also assessed similar systematic reviews for any mention of possible studies, and did not uncover any studies outside our search. Therefore, we believe it is unlikely we missed any published studies that would meet our inclusion criteria.
We could not obtain some relevant data requested from authors. One study did not publish enough data to compute an effect size for its most relevant outcome. The study authors' conclusion was very different from the one based on our sensitivity analysis in which we computed results from available data. With such a limited number of studies included, one study can have a major influence on the overall conclusions. The addition of future studies will allow us to have a clearer picture of intervention effects.
Finally, this Cochrane review evaluated the effectiveness of a range of interventions aiming to reduce stress in workers, rather than one specific intervention. While we believe this is appropriate for a complex and multifactorial outcome such as stress, it fails to differentiate between the many approaches to stress management in the workplace. We will conduct subgroup analyses in future updates of this review to consider differences in workers or approaches, provided that more data become available. However, any future categorization of techniques in subgroup analyses would be subject to bias from our categorization choices.
Agreements and disagreements with other studies or reviews
While this Cochrane review could not reasonably conclude that the delivery modes were equivalent, a conclusion of no clear differences between computer‐based and face‐to‐face methods in stress management in employees would have agreed with another review that examined internet‐based psychotherapeutic interventions to address any psychological problem in any population (Barak 2008). In that review, a subgroup analysis showed no significant difference in effect size when directly comparing equivalent Internet‐based and face‐to‐face therapies.
Other evidence shows that stress management interventions given via computer‐based technologies can be effective in employees (Heber 2017). Similarly, stress management interventions given in the traditional face‐to‐face way have been shown to be effective as well (Richardson 2008; Bhui 2012). However, it is still unclear how strongly the delivery method alone impacts the effectiveness of the programme. The body of evidence that currently directly compares these two delivery methods is weak. The very low‐quality evidence from this review suggests the differences in effects between the two may be small or non‐significant. Moreover, these differences may be due to other factors.
A key factor in the effectiveness of stress management interventions is the level of engagement and participation (i.e. adherence), which is also dependent on exposure. An effective stress management technique cannot induce change if participants do not engage with, and practice the technique. Computer‐based stress management interventions offer greater accessibility by allowing more employees to access the programme remotely. They also offer greater flexibility and convenience. However, that flexibility and convenience (e.g. a self‐paced programme without a fixed schedule) can reduce engagement and participation as employees choose to put off the programme for other, higher priorities with immediate deadlines (as reported in one included study, Eisen 2008). One key difference in the computer‐based interventions given in the two studies included in this review was that Wolever 2012 employed a predetermined schedule, while the intervention in Eisen 2008 was pre‐recorded and fully self‐paced. In addition, the Wolever 2012 intervention had a form of human support (i.e. it was guided), whereas the Eisen 2008 intervention was unguided. Attrition was lower and reductions in stress were greater in the Wolever 2012 version of a computer‐based stress management intervention. This result agrees with similar observations that by adding support or guidance to an online stress management intervention, participation, engagement, practice, and stress outcomes all improved relative to the online stress management intervention alone (Baumeister 2014; Allexandre 2016; Zarski 2016). A systematic review in the field of depression supports this conclusion as well (Richards 2012). Thus, the inclusion of guidance may be an explanatory factor in the differences between the two included studies, and should be investigated further when more research becomes available.
Authors' conclusions
Implications for practice.
We found very low‐quality evidence with conflicting results of the effectiveness of computer‐based stress management interventions compared to in‐person stress management interventions in employees. We could only include two studies with small sample sizes. We have very little confidence in the effect estimates. It is very likely that future studies will change these conclusions. The true effect may likely be substantially different from the estimate of effect.
Implications for research.
More research is needed that directly compares computer‐based and face‐to‐face stress management programmes, so that the impact of the delivery method can be better understood. The research should randomise employees into equivalent computer‐based and face‐to‐face interventions, as well as a control group. However, future studies must be cognisant of the risk from attrition in computer‐based interventions. In particular, efforts must be made to address attrition, and to account for differences between intervention arms from dropouts (e.g. by using an intention‐to‐treat approach). Adherence in computer‐based health interventions is often around 50% (Kelders 2012; Ludden 2015). Therefore, efforts to monitor adherence (e.g. logging online activity or measuring frequency of practice) are also critical, since adherence seems to be a significant factor in determining outcomes. In addition, researchers should be aware of, and measure possible differences, in characteristics of employees between groups, in particular their ability and propensity to use technology.
Assuming a difference in standard deviations between the two groups of two and a standard deviation of six on the commonly‐used Perceived Stress Scale, at 80% statistical power and with a 95% significance level, the required minimum sample size to detect a meaningful difference would be 141 participants in each study arm. Assuming 50% attrition, we recommend recruiting and allocating at least 300 participants for each intervention arm to avoid future studies from being underpowered.
Furthermore, while research has examined the impact of support systems (both technical and clinical) among computer‐based systems, it has not compared them with in‐person delivery methods. The level of support may be a critical factor associated with adherence, and thus we recommend that future research that compares computer‐based and in‐person stress management interventions in employees also varies the level of support (e.g. completely self‐guided versus self‐guided with online support group). Creating this gradation of human support in separate study arms may provide insight on the direction of the effect size.
Acknowledgements
We thank Katie Eisen, George Allen, and Ruth Wolever for providing additional information on their studies.
We thank Jani Ruotsalainen, Managing Editor, Cochrane Work Review Group for providing administrative and logistical support for the conduct of the current review, and Kaisa Neuvonen, Information Specialist, Cochrane Work Review Group for developing and testing the search strategies.
We would also like to thank the Cochrane Work Review Group Coordinating Editor Jos Verbeek, Editors Karen Nieuwenhuijsen and Consol Serra, and external peer referees Johan Sigveland, Kim Jinnett, Kirsi Ahola, and Renzo Bianchi for their comments. We thank Meggan Harris for copy editing the protocol and Anne Lethaby, Jani Ruotsalainen, and Victoria Pennick for copy editing the review.
Appendices
Appendix 1. CENTRAL search strategy
Searched via Cochrane Library. Date of search: 22 February 2017 Search hits: 1563 mh = MeSH subject heading exploded mh ^=MeSH subject heading unexploded
| #1 [mh "Stress, Psychological"] | 4640 |
| #2 [mh "Burnout, Professional"] | 170 |
| #3 stress or burnout* or "burn‐out" | 33201 |
| #4 [mh "Return to Work"] | 119 |
| #5 [mh "Sick Leave"] | 515 |
| #6 [mh Absenteeism] | 500 |
| #7 "return to work" or "back to work" or (sick* next leave*) or (sick* next day*) or (sick* next absen*) or absenteeism | 3828 |
| #8 {or #1‐#7} | 36545 |
| #9 [mh ^Workplace] | 698 |
| #10 [mh ^Work] | 209 |
| #11 work* or occupation* or job* or employ* or personnel* or staff | 82649 |
| #12 [mh "occupational groups"] | 8562 |
| #13 [mh "occupational health"] | 570 |
| #14 {or #9‐#13} | 86274 |
| #15 [mh Telemedicine] | 1821 |
| #16 telemedicine or (tele next medicine) or ehealth* or (e next health*) or telehealth* or (tele next health*) or (e next mental next health*) or (emental next health*) or (e next therapy) or etherapy or (e next treatment*) or etreatment* or (e next counsel*) or ecounsel* or teletherapy or (tele next therapy) or telecounsel* or (tele next counsel*) or (tele next treatment*) or teletreatment* or cyber* or mhealth* or (m next health*) or (mobile next health*) | 4519 |
| #17 [mh Internet] | 2885 |
| #18 internet* or web or webbased or website* or webinar* or online or (technology next based) or technologybased or (tele next psychology*) or telepsychology* | 22135 |
| #19 [mh "Electronic Mail"] | 270 |
| #20 e next mail* | 97417 |
| #21 [mh ^software] or [mh ^"mobile applications"] or [mh ^"user‐ computer interface"] or [mh ^Computers] or [mh "Cell Phones"] | 3330 |
| #22 software or app or apps or application* or computer* or laptop* or (cell* next phone*) or (smart next phone*) or pad or ipad | 74102 |
| #23 [mh "Remote consultation"] or [mh ^Multimedia] | 589 |
| #24 multimedia* or video or remote | 10767 |
| #25 eCBT | 6 |
| #26 {or #15‐#25} | 180859 |
| #27 #8 and #14 and #26 | 3996 |
| #28 #8 and #14 and #26 in Trials | 1563 |
Appendix 2. MEDLINE search strategy
The search was first performed February 2016 and again with revisions February 2017. Below are the revised search strategies from February 2017.
Searched via Ovid.
Date of search: 27 February 2017
Ovid MEDLINE(R) Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE(R) Daily, Ovid MEDLINE and Versions(R)
Search hits: 1622
| Searches | Results | |
| 1 | Stress, Psychological/ | 101571 |
| 2 | Burnout, Professional/ | 8777 |
| 3 | (stress or burnout* or burn‐out*).tw. | 574967 |
| 4 | Return to Work/ | 1238 |
| 5 | Sick Leave/ | 4815 |
| 6 | Absenteeism/ | 8226 |
| 7 | (return to work or back to work or sick* leave* or sick* day* or sick* absen* or absenteeism).tw. | 17567 |
| 8 | or/1‐7 | 646678 |
| 9 | Workplace/ | 17304 |
| 10 | Work/ | 19273 |
| 11 | (work* or occupation* or job* or employ* or personnel* or staff).tw. | 1775132 |
| 12 | exp occupational groups/ or exp occupational health/ | 536177 |
| 13 | or/9‐12 | 2173378 |
| 14 | exp Telemedicine/ | 20399 |
| 15 | (telemedicine or tele‐medicine or ehealth or e‐health or telehealth* or tele‐health* or e‐mental health* or emental health* or e‐therapy or etherapy or e‐treatment* or etreatment* or e‐counsel* or ecounsel* or teletherapy or tele‐therapy or telecounsel* or tele‐counsel* or tele‐treatment* or teletreatment* or cyber* or mhealth* or m‐health* or mobile health*).tw. | 21969 |
| 16 | exp Internet/ | 63271 |
| 17 | (internet* or web or webbased or website* or webinar* or online or technology‐based or technologybased or tele‐psychology* or telepsychology*).tw. | 174444 |
| 18 | Electronic Mail/ or e‐mail*.tw. | 8119 |
| 19 | software/ or mobile applications/ or user‐computer interface/ or Computers/ or exp Cell Phones/ | 168253 |
| 20 | (software or app or apps or application* or computer* or laptop* or cell* phone* or smart phone* or pad or ipad).tw. | 1268661 |
| 21 | Remote consultation/ or Multimedia/ | 5861 |
| 22 | (multimedia* or video or remote).tw. | 122484 |
| 23 | eCBT.tw. | 14 |
| 24 | or/14‐23 | 1622307 |
| 25 | (randomized controlled trial or controlled clinical trial).pt. or Randomized Controlled Trials as Topic/ or Controlled Clinical Trials as Topic/ or Pragmatic clinical trial/ or Random Allocation/ or Double‐Blind Method/ or Single‐Blind Method/ or clinical trial.pt. or Placebos/ or Comparative Study/ or evaluation studies.pt. or Evaluation Studies As Topic/ or (clinical trial or ((singl* or doubl* or trebl* or tripl*) adj3 (mask* or blind*)) or latin square or placebo* or random*).tw. or trial.ti. | 3273273 |
| 26 | 8 and 13 and 24 and 25 | 1712 |
| 27 | Animals/ not Humans/ | 4292389 |
| 28 | 26 not 27 | 1622 |
Appendix 3. PubMed search strategy
Searched via pubmed.com. Simple search to find publications not indexed in MEDLINE(Ovid).
Date of search: 02.22.2017 Search hits: 22
(stress or burnout or sick* leave* or absent* or "back to work" or "return to work") AND (web* or online or internet* or computer*) AND (work* or job* or occupation* or employ* or personnel*) AND (trial or rct or random*) AND (pubstatusaheadofprint OR publisher[sb] OR pubmednotmedline[sb])
Appendix 4. EMBASE Search Strategy
Embase Ovid (1980 to 2017 Week 09)
Search hits: 996
| Searches | Results | |
| 01 | (((stress/ or burnout/ or emotional stress/ or interpersonal stress/ or life stress/ or mental stress/ or exp chronic stress/) and (exp work/ or employee/)) or job stress/) and (telemedicine/ or teleconsultation/ or telemonitoring/ or telepsychiatry/ or teletherapy/ or telehealth/ or telenursing/ or internet/ or e‐mail/ or exp computer/ or mobile phone/) and ("randomized controlled trial"/ or controlled clinical trial/ or random*.tw.) | 91 |
| 2 | ((stress or burnout* or burn‐out* or return to work or back to work or sick* leave* or sick* day* or sick* absen* or absenteeism) and (work* or occupation* or job* or employ* or personnel* or staff) and (telemedicine or tele‐medicine or ehealth or e‐health or telehealth* or tele‐health* or e‐mental health* or emental health* or e‐therapy or etherapy or e‐treatment* or etreatment* or e‐counsel* or ecounsel* or teletherapy or tele‐therapy or telecounsel* or tele‐counsel* or tele‐treatment* or teletreatment* or cyber* or mhealth* or m‐health* or mobile health* or internet* or web or webbased or website* or webinar* or online or technology‐based or technologybased or tele‐psychology* or telepsychology* or software or app or apps or application* or computer* or laptop* or cell* phone* or smart phone* or pad or ipad or multimedia* or video or remote or eCBT)).tw. and ((clinical trial or ((singl* or doubl* or trebl* or tripl*) adj3 (mask* or blind*)) or latin square or placebo* or random*).tw. or trial.ti.) | 993 |
| 3 | 1 or 2 | 1034 |
| 4 | (exp animals/ or exp invertebrate/ or animal experiment/ or animal model/ or animal tissue/ or animal cell/ or nonhuman/) not (human/ or normal human/ or human cell/) | 5837226 |
| 5 | 3 not 4 | 996 |
Appendix 5. PsycINFO search strategy
PsycINFO Ovid (1806 to 2017 February Week 3)
Search hits: 426
| Searches | Results | |
| 1 | (stress or burnout* or burn‐out*).tw. | 185400 |
| 2 | exp stress/ | 93037 |
| 3 | stress management/ | 4534 |
| 4 | employee leave benefits/ | 887 |
| 5 | reemployment/ | 1172 |
| 6 | employee absenteeism/ | 2032 |
| 7 | (return to work or back to work or sick* leave* or sick* day* or sick* absen* or absenteeism).tw. | 7351 |
| 8 | or/1‐7 | 207253 |
| 9 | work related illnesses/ or exp occupational health/ | 2834 |
| 10 | exp Personnel/ or exp Working Conditions/ or exp Working Space/ | 374723 |
| 11 | (work* or occupation* or job* or employ* or personnel* or staff).tw. | 886249 |
| 12 | or/9‐11 | 1072444 |
| 13 | exp telemedicine/ or exp computer assisted therapy/ or exp computer mediated communication/ or exp telecommunications media/ | 24495 |
| 14 | telecommunications media/ or online therapy/ | 3390 |
| 15 | internet/ or exp electronic communication/ | 38128 |
| 16 | exp Computers/ | 17279 |
| 17 | exp Computer Software/ | 13206 |
| 18 | cellular phones/ or exp mobile devices/ | 4446 |
| 19 | cellular phones/ or exp mobile devices/ | 4446 |
| 20 | (telemedicine or tele‐medicine or ehealth or e‐health or telehealth* or tele‐health* or e‐mental health* or emental health* or e‐therapy or etherapy or e‐treatment* or etreatment* or e‐counsel* or ecounsel* or teletherapy or tele‐therapy or telecounsel* or tele‐counsel* or tele‐treatment* or teletreatment* or cyber* or mhealth* or m‐health* or mobile health*).tw. | 10694 |
| 21 | (internet* or web or webbased or website* or webinar* or online or technology‐based or technologybased or tele‐psychology* or telepsychology*).tw. | 99011 |
| 22 | (software or app or apps or application* or computer* or laptop* or cell* phone* or smart phone* or pad or ipad).tw. | 250573 |
| 23 | (multimedia* or video or remote or eCBT).tw. | 42393 |
| 24 | or/13‐23 | 388659 |
| 25 | experimental design/ or clinical trials/ or "Treatment Outcome/Clinical Trial".md. or (clinical trial or ((singl* or doubl* or trebl* or tripl*) adj3 (mask* or blind*)) or latin square or placebo* or random*).tw. or trial.ti. | 208386 |
| 26 | 8 and 12 and 24 and 25 | 426 |
Appendix 6. NIOSHTIC, NIOSHTIC‐2, HSELINE, CISDOC (OSH‐UPDATE)
Date of search: 08 August 2017 Search hits: 61 All databases were searched simultaneously in OSH‐UPDATE.
Advanced search:
All Fields: stress or burnout or burn‐out or sick* leave* or absen* or back to work or return to work AND All Fields: work* or employ* or occupation* or job* AND All Fields: web* or www or online or on‐line or internet* or computer* AND All Fields: random* or trial* or controlled study or control group*
Appendix 7. Trials registries search strategies
Total search hits: 314 Search hits after duplicate removal: 210
WHO ICTRP (International Clinical Trials Registry Platform) Date: 02 November 2016
Search 1: Advanced search: 41 hits Condition: stress OR burnout AND Intervention: web* OR internet* Recruitment status: ALL
Search 2: Simple search: 29 hits stress AND web‐based
Search 3: Simple search: 2 hits burnout AND web‐based
Search 4: Advanced search: 22 hits Condition: stress OR burnout AND Intervention: online Recruitment status: ALL
clinicaltrials.gov Date: 02 November 2016
Search 1: Advanced search: 73 hits Conditions: stress OR burnout AND Interventions: web* OR internet
Search 2: Simple search: 98 hits stress AND web‐based
Search 3: Simple search: 5 hits burnout AND web‐based
Search 4: Advanced search: 44 hits Conditions: stress OR burnout AND Interventions: online
Data and analyses
Comparison 1. Computer‐based interventions compared to in‐person interventions for reducing stress.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Any stress outcome | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Sensitivity analysis: missing data | 2 | 128 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.70, 0.43] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Eisen 2008.
| Methods | Randomised controlled trial with 3 arms (in‐person intervention, computer‐based intervention, and wait‐list control). The wait‐list control was not analysed. Total study duration: 8 months. Study location: USA. Study setting: 3 manufacturing sites within a single corporation. Date of study: 2003 to 2004 (personal communication with author). | |
| Participants | Recruitment: written and electronic advertisements to over 13,000 employees at 3 sites. Randomisation of 288 volunteers resulted in 134 in in‐person group (48 (36%) completed intervention), 123 in computer‐based group (15 (12%) completed intervention), 31 in wait‐list‐control (WLC) group. Demographics of the 134 participants that started the interventions (13 of whom declined to provide data): Mean age: 44.4 (SD = 9.61) Male: 64.7% Caucasian: 83.3% Married: 64.2% At least a college education: 74.1% |
|
| Interventions | 'Stress to Success Workshop' with content identical for individuals in computer‐based and in‐person groups. Each session contained four 10‐minute psycho‐education modules. After each module (8 total), employees were led through a two‐minute 'mini‐relaxation'. In‐person group led by instructor in groups (ranging from 1 to 28 in size, median = 4) during the lunch period over two weeks. Iterations of the workshop were held on 11 separate occasions over the course of 8 months. The computer‐based group could complete modules any time, but encouraged to complete 8 modules over a period of 2 weeks (some completed all at once, others over more than 2 weeks). |
|
| Outcomes | Stress: Subjecive Units of Distress Scale (SUDS) measured 10 times for each session (each session intended to cover 1 week): before the session, before and after each of the 4 'mini‐relaxations', and at the end of the session. SUDS after the end of Session 2 used for analysis (post‐test data, follow‐up = 0 months). In addition, authors used a 'Stress Survey' with 8 items selected from Johnson & Johnson Health Care System Insight + Health Risk Appraisal survey and 4 items selected from Occupational Stress Inventory ‐ Revised Edition (OSI‐R). This outcome could not be quantitatively analysed because SD/SEs could not be retrieved. AK contacted authors of the study, and they were unable to retrieve data. |
|
| Notes | Additional details of methodology and results were obtained from publication of a PhD thesis (Eisen 2005). AK contacted the authors of the study for additional information. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Personal communication with the authors: random numbers table used from statistics textbook |
| Allocation concealment (selection bias) | Low risk | Personal communication with the authors: "Participants would have had no way of knowing how they were randomised – the participants were employees at a large manufacturing plan who expressed interest in participating in this study. They were simply informed that they would be participating in a web‐based stress management programme, or that they were being assigned to a stress management group." Researcher was not blinded to assignment, but risk was assessed as low. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Baseline characteristics between the two comparison groups were reported as significantly different in sex and wage type: the in‐person group had more male, hourly workers; the computer‐based group more female, salaried workers; likely due to the unavailability of computers among hourly wage workers, causing pre‐intervention drop out, resulting in systematic differences between baseline characteristics of the groups. Furthermore, both groups experienced high dropout rates, with a statistically significantly higher attrition in the computer‐based group. Results were analysed 'as‐treated'. Very few participants turned up for 1‐month follow‐up (16%, 9%) and only 'Stress Survey' results were reported. |
| Selective reporting (reporting bias) | High risk | The available publications did not report Subjective Units of Distress Scale (SUDS) results from 1‐week or 1‐month follow‐up times, but did report SUDS from immediately after interventions, which were statistically significantly lower than pre‐intervention. The selective reporting may have favoured the results that showed significant differences post‐intervention, rather than the no‐effect results found at 1‐month follow‐up. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding, self‐reported outcome. |
| Other bias | Low risk | No other sources of bias were identified. |
| Multiple intervention arms (reporting bias) | Low risk | While there were more than two arms of the interventions in the study, the stated objective of the study was to compare a computer‐based version of their stress management intervention to an in‐person version, thus there was a low risk of bias for this domain. |
| Treatment fidelity | High risk | Differences in exposure and timing: "Although [CB] participants were encouraged to complete the module over a two‐week time period, some individuals went through the entire program over a period of a single week, while others took longer than the two week time period to complete all material." (Eisen 2005, p. 15) Technological difficulties: "Twenty‐one percent of respondents described such problems to be the main reason for their decision not to continue the program. Several respondents described having difficulty logging into the course, or finding that the program would freeze up part‐way through. One respondent described his aggravation with the technological problems he was having with the Stress to Success program and his inability to connect with a live person at the computer help desk, writing that he had been "hoping to reduce my level of stress from frustrating issues like this." Thus, we assessed the risk that the intervention was not delivered as intended as high. |
Wolever 2012.
| Methods | Randomized controlled trial, parallel group, 3 arms (only two arms used in this review, the yoga group was not analysed). Total study duration: 12 weeks. Study location: USA. Study setting: 2 sites within a single insurance corporation. Date of study: 2010 | |
| Participants | 683 potential participants were recruited via email from a single national insurance corporation from two states (CA and CT) in USA for screening. Inclusion criteria: 16 or higher on 10‐item PSS Exclusion criteria: heart arrhythmia, pregnancy, heavy tobacco or nicotine use, heart rate medication, any major medical condition After screening, 239 eligible participants were randomised into yoga (N = 90, not analysed), mindfulness‐online (N = 52, 50 completed (96%)), mindfulness‐in‐person (N = 44, 32 completed 73%)), and wait‐list control (N = 53, not analysed). The demographics of the mindfulness groups, collectively, were: Mean age: 44.3 (SD = 9.4) Male: 22.9% White: 85.4% Married: 66.7% At least a college education: 75.0% |
|
| Interventions | Mindfulness at Work programme, 12 weeks (14 hours total) Within 12 weekly hour‐long classes, the programme taught mindfulness practices (each practice from 5 to 15 minutes) targeting work‐related stress, work‐life balances, and self‐care. An additional 2‐hour mindfulness practice intensive occurred at week 10. The in‐person group was taught in classes of around 20 participants each. The computer‐based group had the same teacher as the in‐person group, giving the same instructions, but via an online classroom with real‐time bi‐directional communication. Same assignments and homework. |
|
| Outcomes | Perceived Stress Scale (PSS) Follow‐up 2 weeks after the 12‐week intervention |
|
| Notes | Aetna, Inc. and eMindful funded the study. Mindfulness at Work is owned by eMindful and contracted for use by Aetna for delivery through eMindful. AK contacted the first author for additional information. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Personal communication with the first author: independent statisticians generated blocks of random numbers |
| Allocation concealment (selection bias) | Low risk | Personal communication with the first author: "Sealed envelopes were created with the allocation inside. As participants enrolled and went through baseline, they were given a study number. After collection of baseline data, randomisation sequences were disclosed to participants individually." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | While a comparison of attrition was reported as not having any statistically significant differences in primary outcomes compared to completers, and a comparison of ITT and 'as‐completed' groups did not reveal significant differences in primary outcomes, the loss to follow‐up in the computer‐based group was 4% (2/52), and 27% (18/44) in the in‐person group. Thus, due to the statistically significant difference in the proportion lost to attrition in the two groups (P < 0.001), which did not occur in any other inter group comparisons of this study, and because one group had greater than 20% attrition, we assessed the risk of attrition bias as high. |
| Selective reporting (reporting bias) | Low risk | The study appeared to be free of any selective reporting. The main outcome of stress was measured and reported according to protocols provided by the author. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding, Self‐reported outcome |
| Other bias | High risk | The study was funded by the software company that developed the intervention being tested. |
| Multiple intervention arms (reporting bias) | Low risk | While multiple arms of interventions were randomised in the study, one of the stated objectives of the study was to compare the online version of their stress management intervention to the in‐person version, thus, assessed as low risk of bias for selective reporting. |
| Treatment fidelity | Unclear risk | No evidence was available to support or refute that the interventions were delivered as planned. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abbott 2009 | Web‐based intervention was compared to wait‐list control or care as usual |
| ACTRN12611001114932 | Web‐based intervention was compared to wait‐list control or care as usual |
| ACTRN12615000574549 | Web‐based intervention was compared to attention or active control group that was not in‐person with equivalent content to intervention group |
| ACTRN12615001015538 | Web‐based intervention was compared to wait‐list control or care as usual |
| Aikens 2014 | Web‐based intervention was compared to wait‐list control or care as usual |
| Alexopoulos 2014 | Web‐based intervention was compared to wait‐list control or care as usual |
| Allexandre 2012 | Web‐based intervention was compared to equivalent intervention with addition of in‐person support group |
| Allexandre 2016 | Web‐based intervention was compared to equivalent intervention with addition of in‐person support group. A computer‐based stress management intervention was compared to the equivalent computer‐based intervention with the addition of in‐person group support. While the group meeting facilitated and supported the weekly assignments, it did not deliver them. Therefore, the comparator could not be considered an in‐person intervention. |
| Baker 2015 | Web‐based intervention was compared to wait‐list control or care as usual |
| Bakker 2007 | Intervention was not web‐ or computer‐based |
| Beauchamp 2005 | Web‐based intervention was compared to wait‐list control or care as usual |
| Billings 2008 | Web‐based intervention was compared to wait‐list control or care as usual |
| Blonk 2006 | Intervention was not web‐ or computer‐based |
| Bolier 2014 | Web‐based intervention was compared to wait‐list control or care as usual |
| Borness 2013 | Web‐based intervention was not a stress management intervention |
| Bragard 2009 | Intervention was not web‐ or computer‐based |
| Carissoli 2015 | Web‐based intervention was compared to wait‐list control or care as usual |
| Cook 2007 | Web‐based intervention was compared to attention or active control group that was not in‐person with equivalent content to intervention group |
| Deitz 2014 | Web‐based intervention was not a stress management intervention |
| Dreusicke 2016 | Study was not a randomised trial |
| Drozd 2013 | Population was not employees |
| Ebert 2014 | Web‐based intervention was compared to wait‐list control or care as usual |
| Ebert 2014a | Web‐based intervention was compared to equivalent intervention with addition of online support. A computer‐based stress management intervention was compared to the equivalent computer‐based intervention with the addition of human support to increase adherence and provide feedback. While the in‐person component in the comparator was supportive it did not deliver the intervention entirely. Therefore, the comparator could not be considered an in‐person intervention. |
| Erdman 2015 | Web‐based intervention was compared to attention or active control group that was not in‐person with equivalent content to intervention group |
| Eriksen 2002 | Intervention was not web‐ or computer‐based |
| Feicht 2013 | Web‐based intervention was compared to wait‐list control or care as usual |
| Franco 2010 | Intervention was not web‐ or computer‐based |
| Geraedts 2014 | Web‐based intervention was compared to wait‐list control or care as usual |
| Giardina 2006 | Web‐based intervention was compared to attention or active control group that was not in‐person with equivalent content to intervention group |
| Grime 2004 | Web‐based intervention was compared to wait‐list control or care as usual |
| Hammer 2015 | Web‐based intervention was compared to wait‐list control or care as usual |
| Hasson 2005 | Web‐based intervention was compared to attention or active control group that was not in‐person with equivalent content to intervention group |
| Hasson 2010 | Outcome was not stress or burnout |
| Heber 2016 | Web‐based intervention was compared to wait‐list control or care as usual |
| Hedman 2015 | Outcome was not stress or burnout |
| Hersch 2016 | Web‐based intervention was compared to wait‐list control or care as usual |
| Hinman 1997 | Web‐based intervention was compared to wait‐list control or care as usual |
| Hirokawa 2012 | Intervention was not web‐ or computer‐based |
| Hughes 2013 | Identified report was not a study; publication was a comment on another study |
| Huibers 2004 | Intervention was not web‐ or computer‐based |
| ISRCTN14881571 | Web‐based intervention was compared to wait‐list control or care as usual |
| Kawakami 2005 | Web‐based intervention was not a stress management intervention |
| Kawakami 2006 | Web‐based intervention was not a stress management intervention |
| Ly 2014 | Web‐based intervention was compared to wait‐list control or care as usual |
| Mackenzie 2014 | Study was not a randomised trial |
| Manas 2011 | Intervention was not web‐ or computer‐based |
| Mino 2006 | Web‐based intervention was compared to wait‐list control or care as usual |
| Mori 2014 | Intervention was not web‐ or computer‐based |
| NCT01595555 | Web‐based intervention was compared to equivalent intervention with addition of online support |
| NCT01661569 | Web‐based intervention was compared to wait‐list control or care as usual |
| NCT01796054 | Web‐based intervention was compared to equivalent intervention with addition of in‐person support group |
| NCT02173626 | Study was not a randomised trial |
| NCT02240082 | Outcome was not stress or burnout |
| NCT02540317 | Web‐based intervention was compared to wait‐list control or care as usual |
| NCT02614443 | Study was not a randomised trial |
| Noordik 2013 | Intervention was not web‐ or computer‐based |
| Phillips 2014 | Web‐based intervention was compared to attention or active control group that was not in‐person with equivalent content to intervention group |
| Prochaska 2008 | Outcome was not stress or burnout |
| Rose 2013 | Web‐based intervention was compared to attention or active control group that was not in‐person with equivalent content to intervention group |
| Ruwaard 2007 | Web‐based intervention was compared to wait‐list control or care as usual |
| Schell 2008 | Outcome was not stress or burnout |
| Shimazu 2005 | Web‐based intervention was compared to wait‐list control or care as usual |
| Spanier 2015 | Web‐based intervention was not a stress management intervention |
| Stansfeld 2015 | Web‐based intervention was compared to wait‐list control or care as usual |
| Stetz 2011 | Web‐based intervention was compared to wait‐list control or care as usual |
| Thiart 2015 | Outcome was not stress or burnout |
| Umanodan 2014 | Web‐based intervention was compared to wait‐list control or care as usual |
| Van Drongelen 2013 | Web‐based intervention was not a stress management intervention |
| Volker 2015 | Web‐based intervention was compared to wait‐list control or care as usual |
| Wiegand 2010 | Population was not employees |
| Yamagishi 2008 | Web‐based intervention was compared to wait‐list control or care as usual |
| Yuan 2014 | Web‐based intervention was compared to wait‐list control or care as usual |
| Zarski 2016 | Study was not a randomised trial |
Differences between protocol and review
We changed the title from 'Web‐based stress management for preventing stress and reducing sick leave in workers' to 'Computer‐based versus in‐person interventions for preventing and reducing stress in workers'. The title of the protocol did not clearly express our comparator group (in‐person interventions) and erroneously referred to sick leave, which is a secondary outcome.
We added Ingvild Kirkehei to the author team after the publication of the protocol because of her assistance in designing and performing the search strategy.
We removed the terms 'burnout' and 'sick leave' from the objectives to clarify that our primary outcome was stress and that we would examine sick leave, absenteeism, and return to work as secondary outcomes, when available.
We rewrote the Background section for the review to give a more robust explanation of the characteristics of stress management interventions (e.g. target level, technique, delivery method, and media used).
For studies that used a cluster‐randomised design and did not consider the design effect in the analyses, we had planned to calculate the design effect by following the methods stated in the Cochrane Handbook for Systematic Reviews of Interventions for the calculations, using a fairly large assumed intra cluster correlation of 0.10. However, we did not include any cluster‐randomised studies in the review, and thus, did not need to take design effects into account in meta‐analyses.
We had planned to conduct a sensitivity analysis by omitting studies that we assessed as having an overall high risk of bias. However, we judged both included studies to have a high risk of bias. Therefore, we could not conduct the sensitivity analysis.
In cases where we could pool data into a meta‐analysis, we had planned to use a fixed‐effect model if there was statistical heterogeneity. Otherwise, we had planned to use the random‐effects model. However, because the data could not be pooled (heterogeneity too high), we did not use any model. In addition, we specified in this review that the cut‐off point for moderate heterogeneity was defined as I² > 40%. We had not specified this exact cut‐off point in the protocol.
We defined equivalence of effects between the two intervention delivery modes to mean that difference in the effect size was less than or equal to 0.2 SMD. We had not provided this definition in the protocol.
There was a mistake in the Secondary outcomes section of our protocol where we stated: "Although sick leave is covered under return to work (RTW), we will consider studies for inclusion when they have measured either one". The mistake is that we did not actually intend to use return to work or any of the other secondary outcomes as inclusion criteria. This was explicitly stated later on in the same section: "Reporting one or more of the secondary outcomes listed here in the trial is not an inclusion criterion for the review". Consequently we removed the erroneous sentence from the Methods section of the review.
We added one additional subgroup analysis (i.e. among different levels of human support) to be conducted if enough data becomes available in future updates of this review. This subgroup analysis was not conceived in the protocol.
Contributions of authors
Anootnara Talkul Kuster (AK) conceived the protocol.
AK, Quentin Durand‐Moreau (QDM), Arnav Agarwal (AA), Therese Dalsbø (TD), and Yen Luong Thanh (YLT) drafted the protocol.
AK, QDM, AA, TD, and YLT approved the final version of the protocol.
Ingvild Kirkehei (IK) performed searches.
AA, TD, YLT screened the titles and abstracts.
AK, YLT, QDM reviewed full‐text articles.
AK, QDM, YLT extracted data.
AK, TD conducted data analysis and 'Risk of bias' assessment.
AK, QDM, AA, and TD wrote the first submission of the review.
AK took the lead in writing the second submission of the review, with input from QDM, TD, and YLT.
All review authors approved the final version.
Sources of support
Internal sources
-
Khon Kaen University, Thailand.
Salary for Anootnara Kuster
-
Norwegian Institute of Public Health, Norway.
Salary for Therese Dalsbø and Ingvild Kirkehei
-
Hue University of Medicine and Pharmacy, Vietnam.
Salary for Bao Yen Luong Thanh
-
University Hospital of Brest, France.
Salary for Quentin Durand‐Moreau
External sources
-
Thailand Research Fund (TRF), Thailand.
Grant to Anootnara Kuster under New Scholar Program (grant number MRG5980017) to complete first review
Declarations of interest
Anootnara Kuster: None known.
Therese Dalsbø: None known.
Yen Luong Thanh: None known.
Arnav Agarwal: None known.
Quentin Durand‐Moreau: None known.
Ingvild Kirkehei: None known.
New
References
References to studies included in this review
Eisen 2008 {published and unpublished data}
- Eisen KP. Stress management in the workplace: a comparison of a computer‐based and a group‐based stress management intervention [dissertation]. Paper AAI3193737. Doctoral Dissertations, 2005. [Google Scholar]
- Eisen KP, Allen GJ, Bollash M, Pescatello LS. Stress management in the workplace: a comparison of a computer‐based and an in‐person stress‐management intervention. Computers in Human Behavior 2008;24:486‐96. [Google Scholar]
Wolever 2012 {published data only}
- Wolever R, Bobinet K, McCabe K, MacKenzie L, Fekete E, Kusnick C, et al. Effective and viable mind‐body stress reduction in the workplace: two RCTs. BMC Complementary and Alternative Medicine 2012;12(Suppl 1):87. [DOI] [PubMed] [Google Scholar]
- Wolever RQ, Bobinet KJ, McCabe K, Mackenzie ER, Fekete E, Kusnick CA, et al. Effective and viable mind‐body stress reduction in the workplace: a randomized controlled trial. Journal of Occupational Health Psychology 2012; Vol. 17, issue 2:246‐58. [DOI] [PubMed]
References to studies excluded from this review
Abbott 2009 {published data only}
- Abbott J, Klein B, Hamilton C, Rosenthal AJ. The impact of online resilience training for sales managers on wellbeing and performance. Journal of Applied Psychology 2015;5(1):89‐95. [DOI: ] [Google Scholar]
ACTRN12611001114932 {published data only}
- ACTRN12611001114932. An examination of the relationship between self‐compassion, emotion regulation, happiness and stress in practising psychotherapists, and an a randomized controlled trial of a web‐based self‐compassion training program for postgraduate psychology trainees. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=347588 (first received 12 October 2011). [https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=347588]
ACTRN12615000574549 {published data only}
- ACTRN126150000574549. The resilience at work mindfulness program: the development and evaluation of an online mindfulness based cognitive therapy program aimed at enhancing psychological resilience among emergency workers. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=368296 (first received 9 April 2015).
ACTRN12615001015538 {published data only}
- ACTRN12615001015538. A randomised controlled trial and consumer characteristics of iChooseWell eHealth: a comprehensive biopsychosocial online wellbeing program to decrease stress. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=369295 (first received 13 September 2015).
Aikens 2014 {published data only}
- Aikens KA, Astin J, Pelletier KR, Levanovich K, Baase CM, Park YY, et al. Mindfulness goes to work: impact of an online workplace intervention. Journal of Occupational and Environmental Medicine 2014;56(7):721‐31. [DOI] [PubMed] [Google Scholar]
Alexopoulos 2014 {published data only}
- Alexopoulos EC, Zisi M, Manola G, Darviri C. Short‐term effects of a randomized controlled worksite relaxation intervention in Greece. Annals of Agricultural and Environmental Medicine 2014;21(2):382‐7. [DOI] [PubMed] [Google Scholar]
Allexandre 2012 {published data only}
- Allexandre D, Neuman A, Hunter J, Morledge T, Roizen M. Efficacy of an 8‐week online mindfulness stress management program in a corporate call center. BMC Complementary and Alternative Medicine 2012;12(Suppl 1):119. [Google Scholar]
Allexandre 2016 {published data only}
- Allexandre D, Bernstein AM, Walker E, Hunter J, Roizen MF, Morledge TJ. A web‐based mindfulness stress management program in a corporate call center: A randomized clinical trial to evaluate the added benefit of onsite group support. Journal of Occupational and Environmental Medicine / American College of Occupational and Environmental Medicine 2016;58(3):254‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT02087891. Stress free now in a corporate call center (SFN). clinicaltrials.gov/ct2/show/NCT02087891. The Cleveland Clinic, (first received 26 February 2014).
Baker 2015 {published data only}
- Baker C, Huxley P, Dennis M, Islam S, Russell I. Alleviating staff stress in care homes for people with dementia: protocol for stepped‐wedge cluster randomised trial to evaluate a web‐based mindfulness ‐ stress reduction course. BMC Psychiatry 2015;15(1):317. [DOI: 10.1186/s12888-015-0703-7] [DOI] [PMC free article] [PubMed] [Google Scholar]
- ISRCTN80487202. Improving staff stress, job satisfaction and staff turnover rates in care homes for people living with dementia. www.isrctn.com/search?q=ISRCTN80487202 (first received 12 April 2013).
Bakker 2007 {published data only}
- Bakker IM, Terluin B, Marwijk HWJ, Windt DAWM, Rijmen F, Mechelen W, et al. A cluster‐randomised trial evaluating an intervention for patients with stress‐related mental disorders and sick leave in primary care. PLOS Clinical Trials 2007;2(6):e26. [DOI: 10.1371/journal.pctr.0020026] [DOI] [PMC free article] [PubMed] [Google Scholar]
Beauchamp 2005 {published data only}
- Beauchamp N, Irvine AB, Seeley J, Johnson B. Worksite‐based internet multimedia program for family caregivers of persons with dementia. Gerontologist 2005;45(6):793‐801. [DOI] [PubMed] [Google Scholar]
Billings 2008 {published data only}
- Billings DW, Cook RF, Hendrickson A, Dove DC. A web‐based approach to managing stress and mood disorders in the workforce. Journal of Occupational and Environmental Medicine 2008;50(8):960‐8. [DOI: 10.1097/JOM.0b013e31816c435b] [DOI] [PMC free article] [PubMed] [Google Scholar]
Blonk 2006 {published data only}
- Blonk RWB, Brenninkmeijer V, Lagerveld SE, Houtman ILD. Return to work: a comparison of two cognitive behavioural interventions in cases of work‐related psychological complaints among the self‐employed. Work and Stress 2006;20(2):129‐44. [DOI: 10.1080/02678370600856615] [DOI] [Google Scholar]
Bolier 2014 {published data only}
- Bolier L, Ketelaar SM, Nieuwenhuijsen K, Smeets O, Gartner FR, Sluiter JK. Workplace mental health promotion online to enhance well‐being of nurses and allied health professionals: a cluster‐randomized controlled trial. Internet Interventions 2014;1(4):196‐204. [DOI: 10.1016/j.invent.2014.10.002] [DOI] [Google Scholar]
Borness 2013 {published data only}
- Borness C, Proudfoot J, Crawford J, Valenzuela M. Putting brain training to the test in the workplace: a randomized, blinded, multisite, active‐controlled trial. PLoS One 2013;8(3):e59982. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bragard 2009 {published data only}
- Bragard I, Etienne AM, Libert Y, Merckaert I, Lienard A, Meunier J, et al. Efficacy of a communication and stress management training on residents' stress to communicate, self‐efficacy and burnout level: a randomized controlled study. Psycho‐oncology 2009;18(Suppl 2):S252‐3. [Google Scholar]
Carissoli 2015 {published data only}
- Carissoli C, Villani D, Riva G. Does a meditation protocol supported by a mobile application help people reduce stress? Suggestions from a controlled pragmatic trial. Cyberpsychology, Behavior and Social Networking 2015;18(1):46‐53. [DOI: 10.1089/cyber.2014.0062] [DOI] [PubMed] [Google Scholar]
Cook 2007 {published data only}
- Cook RF, Billings DW, Hersch RK, Back AS, Hendrickson A. A field test of a web‐based workplace health promotion program to improve dietary practices, reduce stress, and increase physical activity: randomized controlled trial. Journal of Medical Internet Research 2007;9(2):e17. [DOI] [PMC free article] [PubMed] [Google Scholar]
Deitz 2014 {published data only}
- Deitz D, Cook RF, Hersch RK, Leaf S. Heart Healthy Online: an innovative approach to risk reduction in the workplace. Journal of Occupational and Environmental Medicine 2014;56(5):547‐53. [DOI: 10.1097/JOM.0000000000000148] [DOI] [PMC free article] [PubMed] [Google Scholar]
Dreusicke 2016 {published data only}
- Dreusicke M, Ruff KM, Wolever R. Mindfulness program delivered virtually in the workplace shows correlation between decreased stress and increased productivity. Journal of Alternative and Complementary Medicine 2016;22(6):A2‐3. [Google Scholar]
Drozd 2013 {published data only}
- Drozd F, Raeder S, Kraft P, Bjorkli CA. Multilevel growth curve analyses of treatment effects of a web‐based intervention for stress reduction: randomized controlled trial. Journal of Medical Internet Research 2013;15(4):e84. [DOI: 10.2196/jmir.2570] [DOI] [PMC free article] [PubMed] [Google Scholar]
- ISRCTN25619675. A fully automated and web‐based intervention for stress management. www.isrctn.com/ISRCTN25619675 (first received 30 August 2012).
Ebert 2014 {published data only}
- Ebert DD, Lehr D, Bos L, Riper H, Cuijpers P, Andersson G, et al. Efficacy of an internet‐based problem‐solving training for teachers: results of a randomized controlled trial. Scandinavian Journal of Work, Environment & Health 2014;40(6):582‐96. [DOI] [PubMed] [Google Scholar]
Ebert 2014a {published data only}
- DRKS00005687. Comparative efficacy and cost‐effectiveness of internet‐based stress management with and without guidance. www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00005687 (first received 6 June 2014).
- Ebert DD, Lehr D, Smit F, Zarski AC, Riper H, Heber E, et al. Efficacy and cost‐effectiveness of minimal guided and unguided internet‐based mobile supported stress‐management in employees with occupational stress: a three‐armed randomised controlled trial. BMC Public Health 2014;14:807. [DOI] [PMC free article] [PubMed] [Google Scholar]
Erdman 2015 {published data only}
- Erdman R. Increasing worker engagement and alleviating Teacher Burnout Syndrome (TBS) [Dissertation]. ProQuest Dissertations Publishing, 2014. [Google Scholar]
Eriksen 2002 {published data only}
- Eriksen HR, Ihlebaek C, Mikkelsen A, Grønningsaeter H, Sandal GM, Ursin H. Improving subjective health at the worksite: a randomized controlled trial of stress management training, physical exercise and an integrated health programme. Occupational Medicine 2002;52(7):383‐91. [DOI] [PubMed] [Google Scholar]
Feicht 2013 {published data only}
- Feicht T, Wittmann M, Jose G, Mock A, Hirschhausen E, Esch T. Evaluation of a seven‐week web‐based happiness training to improve psychological well‐being, reduce stress, and enhance mindfulness and flourishing: a randomized controlled occupational health study. Evidence‐Based Complementary and Alternative Medicine 2013; Vol. 2013:676953. [DOI] [PMC free article] [PubMed]
Franco 2010 {published data only}
- Franco C, Manas i, Cangas A J, Moreno E, Gallego J. Reducing teachers' psychological distress through a mindfulness training program. Spanish Journal of Psychology 2010;13(2):655. [DOI] [PubMed] [Google Scholar]
Geraedts 2014 {published data only}
- Geraedts AS, Kleiboer AM, Twisk J, Wiezer NM, Mechelen W, Cuijpers P. Long‐term results of a web‐based guided self‐help intervention for employees with depressive symptoms: randomized controlled trial. Journal of Medical Internet Research 2014;16(7):11‐25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geraedts AS, Kleiboer AM, Wiezer NM, Mechelen W, Cuijpers P. Short‐term effects of a web‐based guided self‐help intervention for employees with depressive symptoms: randomized controlled trial. Journal of Medical Internet Research 2014; Vol. 16, issue 5:3‐17. [DOI] [PMC free article] [PubMed]
- Geraedts AS, Kleiboer AM, Wiezer NM, Mechelen W, Cuijpers P. Web‐based guided self‐help for employees with depressive symptoms (Happy@Work): design of a randomized controlled trial. BMC Psychiatry 2013;13:61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Giardina 2006 {published data only}
- Giardina TD. Evaluation of a web‐based writing intervention as a means of preventing distress and job burnout among professional helpers [Dissertation/Thesis]. Dissertations & Theses @ SUNY Buffalo,ProQuest Dissertations & Theses Global, 2006. [hdl.handle.net/10477/49609] [Google Scholar]
Grime 2004 {published data only}
- Grime PR. An open, randomised study, to compare the effects of a computerised cognitive behavioural therapy programme (beating the blues) plus conventional care, vs. conventional care alone, on absence from work due to anxiety, depression or stress. http://research.bmh.manchester.ac.uk/epidemiology/COEH/postgraduate/msc/abstracts/Paul_Grime.pdf (accessed prior to 5 July 2017).
- Grime PR. Computerized cognitive behavioural therapy at work: a randomized controlled trial in employees with recent stress‐related absenteeism. Occupational Medicine 2004;54(5):353‐9. [DOI] [PubMed] [Google Scholar]
Hammer 2015 {published data only}
- Hammer LB, Truxillo DM, Bodner T, Rineer J, Pytiovany AC, Richman A. Effects of a workplace intervention targeting psychosocial risk factors on safety and health outcomes. BioMed Research International 2015;2015:836967. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hasson 2005 {published data only}
- Hasson D, Anderberg UM, Theorell T, Arnetz BB. Psychophysiological effects of a web‐based stress management system: a prospective, randomized controlled intervention study of IT and media workers. BMC Public Health 2005;5:78. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hasson 2010 {published data only}
- Hasson H, Brown C, Hasson D. Factors associated with high use of a workplace web‐based stress management program in a randomized controlled intervention study. Health Education Research 2010;25(4):596. [DOI] [PubMed] [Google Scholar]
Heber 2016 {published data only}
- DRKS00004749. Internet‐based occupational stress management program. www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00004749 (first received 21 February 2013).
- DRKS00005112. Internet‐based occupational stress management program with feedback on demand. www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00005112 (first received 26 July 2013).
- DRKS00005384. Online self‐help training for work‐related stress. www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00005384 (first received 5 November 2013).
- DRKS00005990. Online‐based stress‐management training ‐ also effective under unfavourable working conditions? Randomized controlled trial. www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00005990 (first received 16 December 2014).
- Heber E, Ebert DD, Lehr D, Nobis S, Berking M, Riper H. Efficacy and cost‐effectiveness of a web‐based and mobile stress‐management intervention for employees: design of a randomized controlled trial. BMC Public Health 2013;13:655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heber E, Lehr D, Ebert DD, Berking M, Riper H. Web‐based and mobile stress management intervention for employees: a randomized controlled trial. Journal of Medical Internet Research 2016;18(1):e21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hedman 2015 {published data only}
- Hedman E, Andersson E, Lekander M, Ljótsson B. Predictors in Internet‐delivered cognitive behavior therapy and behavioral stress management for severe health anxiety. Behaviour Research and Therapy 2015;64:49‐55. [DOI] [PubMed] [Google Scholar]
Hersch 2016 {published data only}
- Hersch RK, Cook RF, Deitz DK, Kaplan S, Hughes D, Friesen MA, et al. Reducing nurses' stress: a randomized controlled trial of a web‐based stress management program for nurses. Applied Nursing Research 2016;32:18‐25. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hinman 1997 {published data only}
- Hinman M, Ezzo L, Hunt D, Mays A. Computerized exercise program does not affect stress levels of asymptomatic VDT users. Journal of Occupational Rehabilitation 1997;7(1):45‐51. [Google Scholar]
Hirokawa 2012 {published data only}
- Hirokawa K, Taniguchi T, Tsuchiya M, Kawakami N. Effects of a stress management program for hospital staffs on their coping strategies and interpersonal behaviors. Industrial Health 2012;50(6):487‐98. [DOI] [PubMed] [Google Scholar]
Hughes 2013 {published data only}
- Hughes JW, Goldstein CM. Lower the cost, extend the reach, expand the opportunities: a comment on Morledge et al. Annals Of Behavioral Medicine 2013;46(2):129‐30. [DOI] [PubMed] [Google Scholar]
Huibers 2004 {published data only}
- Huibers MJH, Beurskens AJHM, Schayck CP, Bazelmans E, Metsemakers JFM, Knottnerus JA, et al. Efficacy of cognitive‐behavioural therapy by general practitioners for unexplained fatigue among employees. British Journal of Psychiatry 2004;184(3):240. [DOI] [PubMed] [Google Scholar]
ISRCTN14881571 {published data only}
- ISRCTN14881571. The effectiveness of the internet 'Self‐Examination Therapy (SET)' on anxiety, depression and burn‐out: a randomised trial. www.isrctn.com/ISRCTN14881571 (first received 9 January 2006).
Kawakami 2005 {published data only}
- Kawakami N, Kobayashi Y, Takao S, Tsutsumi A. Effects of web‐based supervisor training on supervisor support and psychological distress among workers: a randomized controlled trial. Preventive Medicine 2005;41:471‐8. [DOI] [PubMed] [Google Scholar]
Kawakami 2006 {published data only}
- Kawakami N, Takao S, Kobayashi Y, Tsutsumi A. Effects of web‐based supervisor training on job stressors and psychological distress among workers: a workplace‐based randomized controlled trial. Journal of Occupational Health 2006;48(1):28‐34. [DOI] [PubMed] [Google Scholar]
Ly 2014 {published data only}
- Ly KH, Asplund K, Andersson G. Stress management for middle managers via an acceptance and commitment‐based smartphone application: a randomized controlled trial. Internet Interventions 2014;1:95‐101. [Google Scholar]
Mackenzie 2014 {published data only}
- Mackenzie A, Harvey S, Mewton L, Andrews G. Occupational impact of internet‐delivered cognitive behaviour therapy for depression and anxiety: reanalysis of data from five Australian randomised controlled trials. Medical Journal of Australia 2014;201(7):417‐9. [DOI] [PubMed] [Google Scholar]
Manas 2011 {published data only}
- Israel MM, Clemente FJ, Eduardo JM. Reducing levels of teacher stress and the days of sick leave in secondary school teachers through a mindfulness training programme. Clínica y Salud 2011;22(2):121. [Google Scholar]
Mino 2006 {published data only}
- Mino Y, Babazono A, Tsuda T, Yasuda N. Can stress management at the workplace prevent depression? A randomized controlled trial. Psychotherapy and Psychosomatics 2006;75(3):177. [DOI] [PubMed] [Google Scholar]
Mori 2014 {published data only}
- Mori M, Tajima M, Kimura R, Sasaki N, Somemura H, Ito Y. A web‐based training program using cognitive behavioral therapy to alleviate psychological distress among employees: randomized controlled pilot trial. JMIR Research Protocols 2014;3(4):e70. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT01595555 {published data only}
- NCT01595555. Effectiveness of Stress Free Now: an internet‐based mindfulness program for stress management. clinicaltrials.gov/ct2/show/NCT01595555 (first received 8 May 2012).
NCT01661569 {published data only}
- NCT01661569. A randomised controlled trial to investigate the effects of the headspace mindfulness smartphone app on psychological well‐being and biological indicators of stress in the workplace. clinicaltrials.gov/ct2/show/NCT01661569 (first received 7 August 2012).
NCT01796054 {published data only}
- NCT01796054. Stress Free Now, a mind‐body reduction program for nurses (SFN‐Nurses). clinicaltrials.gov/ct2/show/NCT01796054. National Library of Medicine (US), (first received 15 February 2013). [https://clinicaltrials.gov/ct2/show/NCT01796054]
NCT02173626 {published data only}
- NCT02173626. Effect of video‐module based mindfulness training on physician stress and well being. clinicaltrials.gov/ct2/show/NCT02173626 (first received 20 June 2014).
NCT02240082 {published data only}
- NCT02240082. COPing with shift work ‐ web based program for police officers. clinicaltrials.gov/ct2/show/NCT02240082 (accessed prior to 9 July 2017).
NCT02540317 {published data only}
- NCT02540317. Internet‐based cognitive behavior therapy for stress disorders: a randomized trial. clinicaltrials.gov/ct2/show/NCT02540317 (first received 1 September 2015).
NCT02614443 {published data only}
- NCT02614443. Effectiveness and acceptability of internet‐delivered treatment for depression, anxiety and stress (EAITDAS). clinicaltrials.gov/ct2/show/NCT02614443 (first received 19 November 2015).
Noordik 2013 {published data only}
- Noordik E, Klink JJ, Geskus RB, Boer MR, Dijk FJH, Nieuwenhuijsen K. Effectiveness of an exposure‐based return‐to‐work program for workers on sick leave due to common mental disorders: a cluster‐randomized controlled trial. Scandinavian Journal of Work, Environment & Health 2013;39(2):144‐54. [DOI] [PubMed] [Google Scholar]
Phillips 2014 {published data only}
- Phillips R, Schneider J, Molosankwe I, Leese M, Foroushani PS, Grime P, et al. Randomized controlled trial of computerized cognitive behavioural therapy for depressive symptoms: effectiveness and costs of a workplace intervention. Psychological Medicine 2014;44(4):741‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Prochaska 2008 {published data only}
- Prochaska JO, Butterworth S, Redding CA, Burden V, Perrin N, Leo M, et al. Initial efficacy of MI, TTM tailoring and HRIs with multiple behaviors for employee health promotion. Preventive Medicine 2008;46:226‐31. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rose 2013 {published data only}
- Rose RD, Buckey JC, Zbozinek TD, Motivala SJ, Glenn DE, Cartreine JA, et al. A randomized controlled trial of a self‐guided, multimedia, stress management and resilience training program. Behaviour Research and Therapy 2013;51:106‐12. [DOI] [PubMed] [Google Scholar]
Ruwaard 2007 {published data only}
- Ruwaard J, Lange A, Bouwman M, Broeksteeg J, Schrieken B. E‐mailed standardized cognitive behavioural treatment of work‐related stress: a randomized controlled trial. Cognitive Behaviour Therapy 2007;36(3):179‐92. [DOI] [PubMed] [Google Scholar]
Schell 2008 {published data only}
- Schell E, Theorell T, Hasson D, Arnetz B, Saraste H. Impact of a web‐based stress management and health promotion program on neck‐shoulder‐back pain in knowledge workers? 12 month prospective controlled follow‐up. Journal of Occupational and Environmental Medicine 2008;6:667. [DOI] [PubMed] [Google Scholar]
Shimazu 2005 {published data only}
Spanier 2015 {published data only}
- Spanier K, Streibelt M, Ünalan F, Bethge M. A web‐based intervention to promote applications for rehabilitation: a study protocol for a randomized controlled trial. Trials 2015;16:436. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stansfeld 2015 {published data only}
- Stansfeld SA, Kerry S, Chandola T, Russell J, Berney L, Hounsome M. Pilot study of a cluster randomised trial of a guided e‐learning health promotion intervention for managers based on management standards for the improvement of employee well‐being and reduction of sickness absence: GEM Study. BMJ Open 2015;5(10):e007981. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stetz 2011 {published data only}
- Stetz MC, Kaloi‐Chen JY, Turner DD, Bouchard S, Riva G, Wiederhold BK. The effectiveness of technology‐enhanced relaxation techniques for military medical warriors. Military Medicine 2011;9:1065‐70. [DOI] [PubMed] [Google Scholar]
Thiart 2015 {published data only}
- Thiart H, Lehr D, Ebert DD, Berking M, Riper H. Log in and breathe out: internet‐based recovery training for sleepless employees with work‐related strain ‐ results of a randomized controlled trial. Scandinavian Journal of Work,Environment and Health 2015;41(2):164‐74. [DOI] [PubMed] [Google Scholar]
- Thiart H, Lehr D, Ebert DD, Sieland B, Berking M, Riper H. Log in and breathe out: efficacy and cost‐effectiveness of an online sleep training for teachers affected by work‐related strain ‐ study protocol for a randomized controlled trial. Trials 2013;14:169. [DOI] [PMC free article] [PubMed] [Google Scholar]
Umanodan 2014 {published data only}
- Umanodan R, Shimazu A, Minami M, Kawakami N. Effects of computer‐based stress management training on psychological well‐being and work performance in Japanese employees: a cluster randomized controlled trial. Industrial Health 2014; Vol. 52, issue 6:480‐91. [DOI] [PMC free article] [PubMed]
Van Drongelen 2013 {published data only}
- Drongelen A, Beek AJ, Hlobil H, Smid T, Boot CRL. Development and evaluation of an intervention aiming to reduce fatigue in airline pilots: design of a randomised controlled trial. BMC Public Health 2013;13:776. [DOI] [PMC free article] [PubMed] [Google Scholar]
Volker 2015 {published data only}
- Volker D, Zijlstra‐Vlasveld MC, Anema JR, Beekman AT, Brouwers EP, Emons WH, et al. Effectiveness of a blended web‐based intervention on return to work for sick‐listed employees with common mental disorders: results of a cluster randomized controlled trial. Journal of Medical Internet Research 2015;17(5):e116. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wiegand 2010 {published data only}
- Wiegand B, Luedtke K, Friscia D, Nair M, Aleles M, McCloskey R. Efficacy of a comprehensive program for reducing stress in women: a prospective, randomized trial. Current Medical Research and Opinion 2010;26(4):991‐1002. [DOI] [PubMed] [Google Scholar]
Yamagishi 2008 {published data only}
- Yamagishi M, Kobayashi T, Nakamura Y. Effects of web‐based career identity training for stress management among Japanese nurses: a randomized control trial. Journal of Occupational Health 2008;50(2):191‐3. [DOI] [PubMed] [Google Scholar]
Yuan 2014 {published data only}
- Yuan Q, Liu S, Tang S, Zhang D. Happy@Work: protocol for a web‐based randomized controlled trial to improve mental well‐being among an Asian working population. BMC Public Health 2014;14:685. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zarski 2016 {published data only}
- Zarski AC, Lehr D, Berking M, Riper H, Cuijpers P, Ebert DD. Adherence to internet‐based mobile‐supported stress management: a pooled analysis of individual participant data from three randomized controlled trials. Journal of Medical Internet Research June 2016;18(6):e146. [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Acquadro 2015
- Acquadro Maran D, Varetto A, Zedda M, Ieraci V. Occupational stress, anxiety and coping strategies in police officers. Occupational medicine (Oxford, England) 2015;65(6):466‐73. [PUBMED: 26048331] [DOI] [PubMed] [Google Scholar]
Ahola 2009
- Ahola K, Gould R, Virtanen M, Honkonen T, Aromaa A, Lönnqvist J. Occupational burnout as a predictor of disability pension: a population‐based cohort study. Occupational and Environmental Medicine 2009;66:284‐90. [DOI] [PubMed] [Google Scholar]
Andersson 2009
- Anderrson G. Using the Internet to provide cognitive behaviour therapy. Behaviour Research and Therapy 2009;47:175‐80. [DOI] [PubMed] [Google Scholar]
Andrews 2010
- Andrews G, Cuijpers P, Craske MG, McEvoy P, Titov N. Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: a meta‐analysis. PLoS ONE 2010;5(10):e13196. [DOI] [PMC free article] [PubMed] [Google Scholar]
Backé 2012
- Backé EM, Seidler A, Latza U, Rossnagel K, Schumann B. The role of psychosocial stress at work for the development of cardiovascular diseases: a systematic review. International Archives of Occupational and Environmental Health 2012;85(1):67‐79. [DOI] [PMC free article] [PubMed] [Google Scholar]
Barak 2008
- Barak A, Hen L, Boniel‐Nissim M, Shapira N. A comprehensive review and a meta‐analysis of internet‐based pyschotherapeutic interventions. Journal of Technology in Human Services 2008;26(2/4):109‐60. [Google Scholar]
Baumeister 2014
- Baumeister H, Reichler L, Munzinger M, Lin J. The impact of guidance on Internet‐based mental health interventions ‐ a systematic review. Internet Interventions 2014;1(4):205‐15. [Google Scholar]
Bergerman 2009
- Bergerman L, Corabian P, Harstall C. Effectiveness of organizational interventions for the prevention of workplace stress (Report). www.ihe.ca/documents/Interventionsforpreventionofworkplace_stress.pdf (accessed 10 February 2015).
Bhui 2012
- Bhui S, Bino S, Stansfeld S, White P. A synthesis of the evidence for managing stress at work: a review of the reviews reporting on anxiety, depression, and absenteeism. Journal of Environmental and Public Health 2012;2012:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brotman 2007
- Brotman DJ, Golden SH, Wittstein IS. The cardiovascular toll of stress. Lancet 2007;370(9592):22‐8. [DOI] [PubMed] [Google Scholar]
Brouwer 2011
- Brouwer W, Kroeze W, Crutzen R, Nooijer J, Vries NK, Brug J, et al. Which intervention characteristics are related to more exposure to Internet‐delivered healthy lifestyle promotion interventions: a systematic review. Journal of Medical Internet Research 2011;13(1):e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Campbell 2001
- Campbell MK, Mollison J, Grimshaw JM. Cluster trials in implementation research: estimation of intracluster correlation coefficients and sample size. Statistics in Medicine 2001;20(3):391‐9. [DOI] [PubMed] [Google Scholar]
Carey 2009
- Carey KB, Scott‐Sheldon LA, Elliott JC, Bolles JR, Carey MP. Computer‐delivered interventions to reduce college student drinking: a meta‐analysis. Addiction 2009;104(11):1807‐19. [PUBMED: 19744139] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cohen 1983
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of Health and Social Behavior 1983;24(4):385‐96. [PubMed] [Google Scholar]
Conway 1981
- Conway TL, Vickers RR Jr, Ward HW, Rahe RH. Occupational stress and variation in cigarette, coffee, and alcohol consumption. Journal of Health and Social Behavior 1981;22(2):155‐65. [PubMed] [Google Scholar]
Cooper 2008
- Cooper C, Dewe P. Well‐being—absenteeism, presenteeism, costs and challenges. Occupational Medicine 2008;58(8):522‐4. [DOI] [PubMed] [Google Scholar]
De Jonge 2002
- Jonge J, Dollard MF. Stress in the Workplace: Australian Master OHS and Environment Guide. Sydney, Australia: CCH, 2002. [Google Scholar]
DeFrank 1987
- DeFrank RS, Cooper CL. Worksite stress management interventions: their effectiveness and conceptualisation. Journal of Managerial Psychology 1987;2(1):4‐10. [Google Scholar]
Ding 2014
- Ding Y, Qu J, Yu X, Wang S. The mediating effects of burnout on the relationship between anxiety symptoms and occupational stress among community healthcare workers in China: a cross‐sectional study. PLoS One 2014;9(9):e107130. [PUBMED: 25211025] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ebert 2017
- Ebert DD, Heber E, Berking M, Riper H, Cuijpers P, Funk B, et al. Self‐guided internet‐based and mobile‐based stress management for employees: Results of a randomised controlled trial. Occupational and Environmental Medicine 2016;73:315‐23. [DOI] [PubMed] [Google Scholar]
EU‐OSHA 2014
- Hassard J, Teoh K, Cox T, Dewe P, Cosmar M, Gründler R, et al. Calculating the cost of work‐related stress and psychosocial risks ‐ European risk observatory literature review. Available from osha.europa.eu/en/tools‐and‐publications/publications/literature_reviews/calculating‐the‐cost‐of‐work‐related‐stress‐and‐psychosocial‐risks 2014, issue accessed prior to 9 July 2017.
French 1982
- French JR, Caplan RD, Harrison R. The mechanisms of job stress and strain. John Wiley & Son, Inc, 1982. [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed prior to 9 July 2017. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Greenhaus 1985
- Greenhaus JH, Beutell NJ. Sources of conflict between work and family roles. Academy of Management Review 1985;10(1):76‐88. [Google Scholar]
Griffiths 2006
- Griffiths KM, Christensen H. Review of randomised controlled trials of internet interventions for mental disorders and related conditions. Clinical Psychologist 2006;10(1):16‐29. [Google Scholar]
Grunberg 1999
- Grunberg L, Moore S, Anderson‐Connolly R, Greenberg E. Work stress and self‐reported alcohol use: the moderating role of escapist reasons for drinking. Journal of Occupational Health Psychology 1999;4(1):29‐36. [PUBMED: 10100111] [DOI] [PubMed] [Google Scholar]
Hammen 2005
- Hammen C. Stress and depression. Annual Review of Clinical Psychology 2005;1:293‐319. [DOI] [PubMed] [Google Scholar]
Heber 2017
- Heber E, Ebert DD, Lehr D, Cuijpers P, Berking M, Nobis S, et al. The benefit of web‐and computer‐based interventions for stress: a systematic review and meta‐analysis. Journal of Medical Internet Research 2017;19:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
HSE 2016
- Health and Safety Executive. Work related stress, anxiety, and depression statistics in Great Britain 2016. Available from www.hse.gov.uk/statistics/causdis/stress/stress.pdf (accessed prior to 9 July 2017).
Ivancevich 1990
- Ivancevich JM, Matteson MT, Freedman SM, Phillips JS. Worksite stress management interventions. The American Psychologist 1990;45(2):252‐61. [PUBMED: 2178505] [DOI] [PubMed] [Google Scholar]
Jordan 2003
- Jordan J, Gurr E, Tinline G, Giga S, Faragher B, Cooper C. Beacons of excellence in stress prevention. Research Report No. 133. Available from www.hse.gov.uk/research/rrpdf/rr133.pdf 2003, issue accessed prior to 9 July 2017. [funded by the Health and Safety Executive (HSE)]
Kelders 2011
- Kelders SM, Gemert‐Pijnen JE, Werkman A, Nijland N, Seydel ER. Effectiveness of a Web‐based intervention aimed at healthy dietary and physical activity behavior: a randomized controlled trial about users and usage. Journal of Medical Internet Research 2011;13(2):e32. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kelders 2012
- Kelders S, Kok R, Ossebaard H, Gemert‐Pijnen J. Persuasive System design does matter: a systematic review of adherence to web‐based interventions. Journal of Medical Internet Research 2012;14(6):e152. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kivimäki 2013
- Kivimäki M, Nyberg ST, Fransson EI, Heikkilä K, Alfredsson L, Casini A, et al. Associations of job strain and lifestyle risk factors with risk of coronary artery disease: a meta‐analysis of individual participant data. Canadian Medical Association Journal 2013;185(9):763‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Laranjeira 2012
- Laranjeira CA. The effects of perceived stress and ways of coping in a sample of Portuguese health workers. Journal of Clinical Nursing 2012;21(11‐12):1755‐62. [PUBMED: 22151103] [DOI] [PubMed] [Google Scholar]
Lazarus 1984
- Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York: Springer, 1984. [Google Scholar]
Lee 2015
- Lee KH, Ho Chae C, Ouk Kim Y, Seok Son J, Kim JH, Woo Kim C, et al. Anxiety symptoms and occupational stress among young Korean female manufacturing workers. Annals of Occupational and Environmental Medicine 2015;27:24. [PUBMED: 26568830] [DOI] [PMC free article] [PubMed] [Google Scholar]
Levi 1989
- Levi L. Occupational stressors, biological stress and workers' health. Journal of UOEH 1989;11(2):229‐45. [PUBMED: 2672225] [DOI] [PubMed] [Google Scholar]
Ludden 2015
- Ludden G, Rompay T, Kelders S, Gemert‐Pijnen J. How to increase reach and adherence of web‐based interventions: a design research viewpoint. Journal of Medical Internet Research 2015;17(7):e172. [DOI] [PMC free article] [PubMed] [Google Scholar]
Maslach 1996
- Maslach C, Jackson SE, Leiter MP. MBI: The Maslach Burnout Inventory: Manual. Palo Alto: Consulting Psychologists Press, 1996. [Google Scholar]
Mohr 2010
- Mohr DC, Siddique J, Ho J, Duffecy J, Jin L, Fokuo JK. Interest in behavioral and psychological treatments delivered face‐to‐face, by telephone, and by Internet. Annals of Behavioral Medicine 2010;40(1):89‐98. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moreau 2004
- Moreau M, Valente F, Mak R, Pelfrene E, Smet P, Backer G, et al. Occupational stress and incidence of sick leave in the Belgian workforce: the Belstress study. Journal of Epidemiology and Community Health 2004;58(6):507‐16. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nilsen 2016
- Nilsen C, Andel R, Fritzell J, Kareholt I. Work‐related stress in midlife and all‐cause mortality: can sense of coherence modify this association?. European Journal of Public Health 2016;26(6):1055‐61. [PUBMED: 27335331] [DOI] [PubMed] [Google Scholar]
Osipow 1998
- Osipow SH, Spokane AR. Occupational stress inventory ‐ revised (OSI‐R). Psychological 1998:1‐15.
Postel 2011
- Postel M, Haan HA, Ter Huurne ED, Becker ES, Jong CA. Characteristics of problem drinkers in e‐therapy versus face‐to‐face treatment. American Journal of Drug and Alcohol Abuse 2011;37(6):537‐42. [DOI] [PubMed] [Google Scholar]
Proudfoot 2011
- Proudfoot J, Klein B, Barak A, Carlbring P, Cuijpers P, Lange A, et al. Establishing guidelines for executing and reporting Internet intervention research. Cognitive Behaviour Therapy 2011;40(2):82‐97. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Richards 2012
- Richards D, Richardson T. Computer‐based psychological treatments for depression: a systematic review and meta‐analysis. Clinical Pyschology Review 2012;32(4):329‐42. [DOI] [PubMed] [Google Scholar]
Richardson 2008
- Richardson KM, Rothstein HR. Effects of occupational stress management intervention programs: a meta‐analysis. Journal of Occupational Health Psychology 2008;13(1):69‐93. [PUBMED: 18211170] [DOI] [PubMed] [Google Scholar]
Rosch 2001
- Rosch RJ. The quandary of job stress compensation. Health and Stress 2001;3:1‐4. [Google Scholar]
Rueppell 2017
- Rueppell O, Yousefi B, Collazo J, Smith D. Early life stress affects mortality rate more than social behavior, gene expression or oxidative damage in honey bee workers. Experimental Gerontology 2017;90:19‐25. [PUBMED: 28122251] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ruotsalainen 2015
- Ruotsalainen JH, Verbeek JH, Mariné A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews 2015, Issue 4. [DOI: 10.1002/14651858.CD002892.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Siegrist 1996
- Siegrist J. Adverse health effects of high‐effort/low reward conditions. Journal of Occupational Health Psychology 1996;1(1):27‐41. [DOI] [PubMed] [Google Scholar]
U.S. Department of Labor 2001
- U.S. Department of Labor. Report on the American workforce 2001. Available from www.bls.gov/opub/rtaw/pdf/rtaw2001.pdf. U.S. Department of Labor, 2001, issue accessed prior to 9 July 2017.
Van der Klink 2001
- Klink JJL, Blonk RWB, Schene AH, Dijk FJH. The benefits of interventions for work‐related stress. American Journal of Public Health 2001;91(2):270‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Van Rijn 2009
- Rijn RM, Huisstede BM, Koes BW, Burdof A. Associations between work‐related factors and specific disorders at the elbow: a systematic literature review. Rheumatology 2009;48(5):528‐36. [DOI] [PubMed] [Google Scholar]
Zetterqvist 2003
- Zetterqvist K, Maanmies J, Ström L, Andersson G. Randomized controlled trial of Internet‐based stress management. Cognitive Behaviour Therapy 2003;32(3):151‐60. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Kuster 2015
- Kuster AT, Dalsbø TK, Luong Thanh YB, Agarwal A, Durand‐Moreau QV. Web‐based stress management for preventing stress and reducing sick leave in workers. Cochrane Database of Systematic Reviews 2015, Issue 10. [DOI: 10.1002/14651858.CD011899] [DOI] [PMC free article] [PubMed] [Google Scholar]