

Abstract
Background
Cytomegalovirus (CMV) is a virus that usually affects people with reduced immunity. In recent years, this virus has been thought to cause repeated inflammation in the eye, in otherwise healthy people. This form of inflammation can cause damage to the cornea (the outer layer of the eye) or to the optic nerve by causing secondary glaucoma, or to both, leading to visual loss.
Objectives
Our primary objective was to assess the effects of drug therapies for the treatment of CMV‐associated anterior segment inflammation.
Our secondary objective was to determine the optimal dose and duration of treatment with respect to recurrence and adverse effects.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (which contains the Cochrane Eyes and Vision Trials Register) (2017, Issue 2), MEDLINE Ovid (1946 to 21 March 2017), Embase Ovid (1947 to 21 March 2017), the ISRCTN registry (www.isrctn.com/editAdvancedSearch); searched 21 March 2017, ClinicalTrials.gov (www.clinicaltrials.gov); searched 21 March 2017, and the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en); searched 21 March 2017. We did not use any date or language restrictions in the electronic searches for trials. Two review authors independently reviewed the titles and abstracts.
Selection criteria
We searched for randomised controlled trials (RCTs) on the management of CMV‐associated anterior segment inflammation.
Data collection and analysis
We planned to have two review authors independently extract data from reports of included studies and analyse data based on methods expected by Cochrane.
Main results
We did not identify any RCTs that met our inclusion criteria.
Authors' conclusions
There is currently no good‐quality evidence on the management of CMV‐associated anterior segment inflammation. Ideally, a well‐designed RCT is needed to evaluate the effectiveness of different anti‐CMV medications as well as the optimal dose and duration.
Plain language summary
Treatments for the management of CMV‐associated anterior segment inflammation
What is the aim of this review? The aim of this Cochrane review was to find out what is the best way to treat inflammation of the eye due to cytomegalovirus (CMV) infection. Cochrane review authors searched for all relevant studies (randomised controlled trials) but did not find any studies that could be included in the review.
Key messages There were no randomised controlled trials of treatment of CMV‐associated inflammation of the eye.
What was studied in the review? Cytomegalovirus (CMV) is a virus that affects the front of the eye. If the CMV infection is not treated, it can cause irreversible damage to the front of the eye or damage to the optic nerve or both. This damage can cause sight loss. Untreated, this virus has a tendency to recur, and multiple recurrences can increase the chance of developing eye problems. The treatment for this virus includes the use of eyedrops as well as tablets and injections. However, the currently available medications have side effects, so that knowing the dose and duration of treatment can help reduce these side effects, as well as reducing the risk of new episodes and of further problems.
What are the main results of the review? The Cochrane review authors did not find any studies that met the inclusion criteria for the review.
How up‐to‐date is this review? The Cochrane review authors searched for studies that had been published up to 21 March 2017.
Background
Description of the condition
Cytomegalovirus (CMV) is a DNA virus from the herpes family that rarely manifests clinically in immunocompetent individuals (someone who is able to develop an immune response). However, an increasing number of cases of CMV‐associated anterior segment inflammation in otherwise healthy individuals have recently been reported (Chee 2007; Chee 2008; Chee 2012; Koizumi 2006; Koizumi 2007; Koizumi 2014). This may present in two forms: as acute recurrent anterior uveitis (multiple episodes of inflammation of the middle layer of the eye (uvea)) with high intraocular pressure (IOP), or as chronic anterior uveitis with endotheliitis (inflammation of the corneal endothelium (the innermost layer of the cornea)). This apparent increase may be due to improved diagnosis due to the availability of molecular techniques using polymerase chain reaction (PCR) or the contribution of some as yet unknown factor.
CMV corneal endotheliitis has been reported in people with Fuchs' heterochromic iridocyclitis (chronic unilateral inflammation of the middle layer of the eye that is associated with iris discolouration), Posner‐Schlossman syndrome (inflammation of the middle layer of the eye that is associated with raised IOP and tends to recur), idiopathic corneal endotheliitis as well as endotheliitis in herpes simplex virus (HSV) and herpes zoster virus (HZV) (both HSV and HZV are viruses that cause infection in the eye), associated keratouveitis (inflammation of the cornea and the middle layer of the eye) (Chee 2007; Chee 2008; Koizumi 2006; Koizumi 2007; Markomichelakis 2002; Suzuki 2007; Van Boxtel 2007). It is characterised by the presence of corneal swelling and Descemet's membrane folds (folds in the inner layer of the cornea), often accompanied by keratic precipitates (white blood cells deposited on the inner layer of the cornea in inflammation of the eye). The endothelial lesions are heterogeneous and can be curvilinear or coin‐shaped. They may be associated with anterior uveitis and raised IOP. IOP may be raised without the presence of active anterior chamber inflammation.
A prior history of intraocular surgery may also be a risk factor for CMV‐associated anterior segment inflammation, for example previous cataract surgery, penetrating keratoplasty (full thickness corneal transplant), or Descemet stripping automated endothelial keratoplasty (partial thickness corneal transplant for treating conditions that affect the innermost layer of the cornea, known as the endothelium) (Ang 2013; Anshu 2009; Koizumi 2007; Sonoyama 2010; Suzuki 2007). It is commonly believed that trauma to the corneal nerves can lead to activation of the latent virus in the adjacent tissue. Failure to recognise and properly treat severe cases of endotheliitis following cataract surgery and keratoplasty can lead to irreversible corneal decompensation and graft failure, respectively. However, early and specific antiviral therapy can potentially reverse corneal oedema and prevent permanent endothelial damage, obviating the need for a corneal transplant.
Endotheliitis has classically been associated more often with HSV and HZV than with other viruses.
In people who have endotheliitis without corneal stromal involvement and are unresponsive to acyclovir and its analogues (drugs that are used to treat HSV/HZV), CMV may be suspected.
Description of the intervention
The diagnosis of CMV‐associated anterior segment inflammation requires PCR of aqueous fluid obtained by an anterior chamber tap. Confocal microscopy has also been used to detect owl's eye morphology (a specific cell type seen in CMV‐positive cases) in infected cells (Kobayashi 2012; Shiraishi 2007). Therapy requires systemic or topical ganciclovir, or both, or systemic valganciclovir. However, recurrences have been reported once the drug is suspended, and the length of treatment needed remains unresolved (De Schryver 2006; Mietz 2000).
How the intervention might work
Once the diagnosis of CMV is established following PCR analysis of the anterior chamber tap, treatment may be required in order to prevent irreversible complications of corneal decompensation (irreversible corneal oedema) and glaucoma (optic nerve damage resulting from raised IOP). The treatment options currently available include systemic medications in the form of valganciclovir and ganciclovir and topical ganciclovir. The optimal duration of therapy is largely unknown, and recurrences can occur when the medications have been stopped, with some people requiring long‐term therapy (especially those who are on immunosuppressive drugs like oral/topical steroids).
If the dose and duration of therapy can be determined, treatment may help the resolution of anterior segment inflammation associated with CMV and secondarily prevent corneal decompensation and glaucoma. Currently the available treatment for irreversible corneal decompensation is a corneal transplant. However, adequate and early treatment may help prevent corneal decompensation and hence a corneal transplant. Glaucoma in these people can be severe and recalcitrant to medical therapy alone, sometimes requiring surgery in the form of trabeculectomy (a type of glaucoma surgery that helps to relieve high IOP); early and aggressive treatment of CMV endotheliitis may obviate the need for glaucoma surgery.
Why it is important to do this review
Corneal and anterior segment inflammation secondary to CMV have recently been described in healthy adults with an increasing incidence, particularly in Asian populations. Currently there is uncertainty as to the best way to treat this condition, in particular what are the relative benefits and harms of systemic versus topical treatment, and the optimal dose and duration of treatment.
Objectives
Our primary objective was to assess the effects of drug therapies for the treatment of CMV‐associated anterior segment inflammation.
Our secondary objective was to determine the optimal dose and duration of treatment with respect to recurrence and adverse effects.
Methods
Criteria for considering studies for this review
Types of studies
We sought randomised controlled trials.
Types of participants
We planned to include all adults with a positive anterior chamber tap for CMV DNA. We planned to exclude the following groups of participants:
Pregnant women
Children
People who are allergic to the systemic drugs
People who have neutropenia (reduction in white blood cells) or are predisposed to it due to a systemic medical condition
Types of interventions
We planned to include studies that compare:
oral valganciclovir to oral ganciclovir;
topical ganciclovir to systemic valganciclovir/ganciclovir therapy;
oral/topical antiviral therapy to placebo treatment;
intravitreal ganciclovir injections to ganciclovir implant;
different doses of the same drug;
different duration of the same drug.
Types of outcome measures
Primary outcomes
Clinical resolution of inflammation at three months after randomisation (i.e. start of treatment).
Secondary outcomes
Confirmation of resolution of clinical inflammation by aqueous PCR showing undetectable CMV DNA (if possible)
Number of recurrences
Time to recurrence (mean number of days)
Corneal decompensation
Glaucoma
Mean final best‐corrected visual acuity
Quality of life measured using a validated questionnaire
We planned to assess secondary outcome measures at post‐randomisation visits at 3, 12, and 24 months.
Adverse events
These may include diarrhoea, dizziness and tremors, neutropenia, anaemia (reduction in haemoglobin), allergic reaction in the form of rash, and breathing difficulties.
Search methods for identification of studies
Electronic searches
The Cochrane Eyes and Vision Information Specialist conducted systematic searches in the following databases for randomised controlled trials and controlled clinical trials. There were no language or publication year restrictions. The date of the search was 21 March 2017.
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 2) (which contains the Cochrane Eyes and Vision Trials Register) in the Cochrane Library (searched 21 March 2017) (Appendix 1);
MEDLINE Ovid (1946 to 21 March 2017) (Appendix 2);
Embase Ovid (1980 to 21 March 2017) (Appendix 3);
ISRCTN registry (www.isrctn.com/editAdvancedSearch; searched 21 March 2017) (Appendix 4);
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; searched 21 March 2017) (Appendix 5);
World Health Organization International Clinical Trials Registry Platform (www.who.int/ictrp; searched 21 March 2017) (Appendix 6).
Searching other resources
We planned to screen the reference lists of potentially relevant studies to identify further trials for this review. We planned also to contact investigators and experts in the field to help identify unpublished data or ongoing studies. We did not handsearch conference proceedings or journals specifically for the purposes of this review.
Data collection and analysis
Selection of studies
Two review authors (AA, JM) independently assessed the titles and abstracts obtained from the electronic and manual searching. Once we had screened the titles and abstracts, we had 'yes', 'no', and 'unclear' lists. The two review authors planned also to independently conduct all relevant full‐copy assessments for all 'yes' and 'unclear' studies, to decide which studies we would include and to document excluded studies in a 'Characteristics of excluded studies' table. We planned to contact authors for further clarification where studies lacked the required information and when we could not agree on them.
Data extraction and management
We planned to extract the following study characteristics: methods, participants, interventions, and outcomes, including type of chart used for measuring vision. To measure our primary outcome, clinical resolution of inflammation would include one or more of the following: absence of cells in the anterior chamber, resolution of corneal oedema or keratic precipitates or both. We planned to analyse logMAR (log of the minimum angle of resolution) score, converting from letters as appropriate, following guidance given in Chaper 18 of the Cochrane Handbook for Systematic Reviews of Interventions (Stewart 2011). Following identification of relevant studies, two review authors (AA, JM) planned to independently extract the relevant data using a simple form that would be piloted.
Assessment of risk of bias in included studies
We planned to use the Cochrane tool for assessing risk of bias as described in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a). We will assess the following six parameters for each included study:
sequence generation
allocation concealment
blinding (masking)
incomplete outcome data
selective reporting
other potential sources of bias
Measures of treatment effect
We planned to use risk ratios with 95% confidence intervals as the measure of effect for dichotomous variables (resolution of inflammation, glaucoma, corneal decompensation, and adverse events). We planned to use the mean difference (with a 95% confidence interval) as the measure of effect for continuous variables (visual acuity, quality of life).
We planned to analyse time to recurrence as a hazard ratio, as outlined in Chapter 7 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011b). We also planned to investigate adjustments for repeated measures (summary effect over all time points).
We planned to measure visual acuity in logMAR scale. Where visual acuity is measured on different scales, we planned to convert it into logMAR before analysis.
Unit of analysis issues
Trials may randomise one or both eyes to the intervention or comparator. If people are randomly allocated to treatment, but only one eye per person is included in the trial, then there will not be a unit‐of‐analysis issue. In these cases, we planned to document how the eye was selected. If people are randomly allocated to treatment, but both eyes are included and reported, we planned to analyse as "clustered data", that is to adjust for within‐person correlation as summarised in Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011). We planned to contact the trial investigators for further information in order to do this.
We excluded studies that had allocated different eyes to different treatments, as there may be a confounding cross‐over effect due to systemic absorption.
Dealing with missing data
We planned to follow the general recommendations for dealing with missing data as outlined in Chapter 16 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011c).
We planned to report follow‐up for each treatment group for each individual study, and collect data on reasons for missingness, where available.
Whenever possible, we planned to contact the original investigators to request missing data, in particular where review outcomes have not been reported.
We planned to make explicit the assumptions of any methods used to address missing data, for example that the data are assumed missing at random, or that missing values were assumed to have a particular value such as a poor outcome.
We planned to address the potential impact of missing data on the findings of the review in the 'Discussion' section.
We planned not to use missing summary data (for example no usable data) as a reason to exclude a study from the review. We planned to include the study in the review, and discuss the potential implications of its absence from a meta‐analysis.
Assessment of heterogeneity
We planned to check for heterogeneity by examining the:
characteristics of the study;
forest plot of results of the study;
results of the Chi2 test for statistical heterogeneity;
results of the I2 statistic to quantify inconsistencies between study results.
We planned to use the following guide to interpret the I2 statistic, following guidance given in Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011):
0% to 40%: may not be important;
30% to 60%: may represent moderate heterogeneity;
50% to 90%: may represent substantial heterogeneity;
75% to 100%: considerable heterogeneity.
Assessment of reporting biases
If there are 10 or more studies contributing to a meta‐analysis, we planned to prepare a funnel plot. An asymmetric funnel plot is possible evidence of publication bias, although there may be other explanations for the asymmetry (Sterne 2011).
We planned to check for selective outcome reporting bias by checking that the individual trials have reported all the outcomes that they collected data for; where possible, we planned to look at the trial protocol to check this.
Data synthesis
We planned to pool data using a random‐effects model, unless there are three or fewer trials, in which case we planned to use a fixed‐effect model.
There is likely to be some clinical or methodical diversity in a meta‐analysis, therefore heterogeneity is inevitable. If we identify heterogeneity, we planned to check that the data are correct. If there is evidence of substantial heterogeneity, for example, I2 greater than 50%, Chi2 less than 0.1 and different direction of effects, we planned not to pool data, as the pooled effect may not be a good summary of the individual trial results.
Multiplicity
Adjustments for multiple tests are not recommended in systematic reviews (Higgins 2011c).
To avoid problems with multiplicity, we planned to emphasise estimating intervention effects rather than testing for them. We have prespecified the outcomes to appear in the 'Summary of findings' table, and it is these outcomes that we planned to discuss in the abstract. We planned not to select results for emphasis on the basis of a statistically significant P value, particularly in the abstract. We planned to interpret any post hoc findings cautiously.
Subgroup analysis and investigation of heterogeneity
We did not plan any subgroup analyses.
Sensitivity analysis
We planned to compare all analyses with different models, that is random‐effects compared to fixed‐effect.
For the analysis of the primary outcome, we planned to examine the effect of excluding the following types of trials:
Trials graded as high risk of bias on any parameter
Unpublished trials
Industry‐funded studies
Summary of findings table
We planned to present absolute and relative risks for the outcomes listed below. We will grade the overall certainty of the evidence for each outcome using GRADEpro (GRADEpro 2014).
Resolution of inflammation
Number of recurrences
Time to recurrence (days)
Corneal decompensation
Glaucoma
Best‐corrected visual acuity
Adverse effects
Follow‐up: 12 months
Results
Description of studies
Results of the search
The electronic searches yielded 537 references (Figure 1). The Cochrane Information Specialist removed 146 duplicate records and we screened the remaining 391 reports. Two review authors (AA, JM) independently screened for potentially eligible studies, namely RCTs looking at treatment options for the management of CMV‐associated anterior segment inflammation. We found no trials that met the inclusion criteria. There was no disagreement between the review authors regarding eligibility of any of the search results. We are not aware of any individuals or organisations who have conducted or may be conducting relevant RCTs.
1.
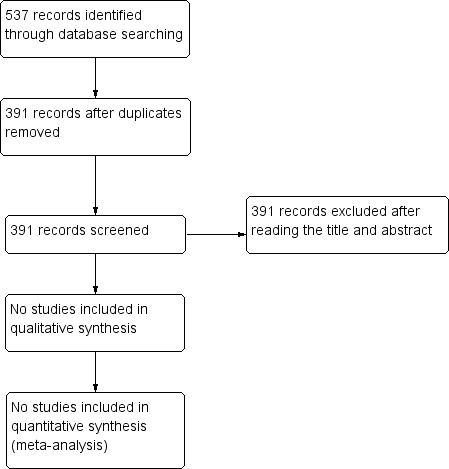
Study flow diagram.
Included studies
We did not find any published or ongoing studies that met the study inclusion criteria.
Excluded studies
We did not exclude any trials after obtaining the full‐text report.
Risk of bias in included studies
We have included no trials in this review for reasons stated previously.
Effects of interventions
None of the citations identified by the search were reports of RCTs on the management of CMV‐associated anterior segment inflammation.
Discussion
Summary of main results
All the reviewed studies were either case series or case reports and therefore could not be included in the review. The search did not identify any RCTs on the management of CMV‐associated anterior segment inflammation.
Overall completeness and applicability of evidence
We performed a thorough search of the available evidence on CMV‐associated anterior segment inflammation and therefore believe that our conclusions are valid. We also looked at registered trials but found no ongoing studies. A lack of ongoing trials could be because of the small numbers seen and the lack of sensitive testing techniques to detect the virus; treatment is often empirical, based on suspected clinical findings, and treatment dose and duration are based on clinical response to treatment and the occurrence of side effects, as well as the patient's capacity to pay for these expensive medications. The dose, duration and therapeutic effect of currently available treatment options need to be established for optimal management of CMV‐associated anterior segment inflammation and to avoid potential complications.
Quality of the evidence
We did not identify any RCTs for inclusion in this review.
Potential biases in the review process
The review authors may not be aware of individuals or organisations who have conducted or may be conducting relevant RCTs, so it is possible that we have missed relevant RCTs.
Agreements and disagreements with other studies or reviews
Jap 2011 reviewed the treatment of viral anterior uveitis. The evidence for treatment of CMV‐related uveitis was limited to a retrospective chart review of patients treated with systemic or ocular ganciclovir, or both. Although participants responded to treatment, the relapse rate was high. They suggested that the use of topical ganciclovir was at lower cost with similar effectiveness but without the systemic side effects. However, the review did not address the dose and duration of therapy or alternative treatments.
Authors' conclusions
Implications for practice.
There is a lack of high‐quality evidence on the management of CMV‐associated anterior segment inflammation. Ophthamologists need to bear this in mind when managing people with CMV‐associated anterior segment inflammation.
Implications for research.
CMV‐associated anterior segment inflammation can result in significant ocular morbidity in the form of irreversible corneal oedema and glaucoma, necessitating corneal transplant surgery or glaucoma surgery, or both. Properly‐designed RCTs are therefore needed to provide information on effective management strategies for CMV‐associated anterior segment inflammation. These RCTs should address treatment options that can best treat this condition, with minimal ocular and systemic side effects. Future studies should also focus on the dose and duration of treatment necessary to reduce ocular complications from CMV endotheliitis.
Acknowledgements
Cochrane Eyes and Vision created the electronic searches. We thank Catey Bunce and Vishal Jhanji for their comments on the protocol, Augusto Azuara‐Blanco for his comments on the review and Jennifer Evans and Anupa Shah for their assistance with the review process.
Appendices
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor: [Cytomegalovirus] explode all trees #2 MeSH descriptor: [Cytomegalovirus Infections] explode all trees #3 Cytomegalovirus #4 CMV #5 #1 or #2 or #3 or #4 #6 MeSH descriptor: [Uveitis, Anterior] explode all trees #7 (acute or recurrent or chronic or anterior) near/3 (uveitis) #8 endotheliitis #9 MeSH descriptor: [Iridocyclitis] explode all trees #10 Fuchs' heterochromic iridocyclitis #11 #6 or #7 or #8 or #9 or #10 #12 #5 and #11
Appendix 2. MEDLINE Ovid search strategy
1. randomised controlled trial.pt. 2. (randomised or randomised).ab,ti. 3. placebo.ab,ti. 4. dt.fs. 5. randomly.ab,ti. 6. trial.ab,ti. 7. groups.ab,ti. 8. or/1‐7 9. exp animals/ 10. exp humans/ 11. 9 not (9 and 10) 12. 8 not 11 13. Cytomegalovirus/ 14. exp cytomegalovirus infections/ 15. Cytomegalovirus.tw. 16. CMV.tw. 17. or/13‐16 18. exp Uveitis, Anterior/ 19. ((acute or recurrent or chronic or anterior) adj3 uveitis).tw. 20. endotheliitis.tw. 21. Iridocyclitis/ 22. Fuchs' heterochromic iridocyclitis.tw. 23. or/18‐22 24. 17 and 23 25. 12 and 24
The search filter for trials at the beginning of the MEDLINE strategy is from the published paper by Glanville 2006.
Appendix 3. Embase Ovid search strategy
1. exp randomized controlled trial/ 2. exp randomization/ 3. exp double blind procedure/ 4. exp single blind procedure/ 5. random$.tw. 6. or/1‐5 7. (animal or animal experiment).sh. 8. human.sh. 9. 7 and 8 10. 7 not 9 11. 6 not 10 12. exp clinical trial/ 13. (clin$ adj3 trial$).tw. 14. ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw. 15. exp placebo/ 16. placebo$.tw. 17. random$.tw. 18. exp experimental design/ 19. exp crossover procedure/ 20. exp control group/ 21. exp latin square design/ 22. or/12‐21 23. 22 not 10 24. 23 not 11 25. exp comparative study/ 26. exp evaluation/ 27. exp prospective study/ 28. (control$ or prospectiv$ or volunteer$).tw. 29. or/25‐28 30. 29 not 10 31. 30 not (11 or 23) 32. 11 or 24 or 31 33. Cytomegalovirus/ 34. exp cytomegalovirus infection/ 35. Cytomegalovirus.tw. 36. CMV.tw. 37. or/33‐36 38. exp uveitis/ 39. ((acute or recurrent or chronic or anterior) adj3 uveitis).tw. 40. endotheliitis.tw. 41. Iridocyclitis/ 42. Fuchs' heterochromic iridocyclitis.tw. 43. or/38‐42 44. 37 and 43 45. 32 and 44
Appendix 4. ISRCTN search strategy
(cytomegalovirus OR CMV) AND (uveitis OR endotheliitis OR iridocyclitis)
Appendix 5. ClinicalTrials.gov search strategy
(cytomegalovirus OR CMV) AND (uveitis OR endotheliitis OR iridocyclitis)
Appendix 6. WHO ICTRP search strategy
cytomegalovirus uveitis
cytomegalovirus endotheliitis
cytomegalovirus iridocyclitis
Differences between protocol and review
The primary outcome "Clinical resolution of inflammation at three months after randomisation (i.e. start of treatment); confirmed by aqueous PCR showing undetectable CMV DNA (if possible)" was modified, by moving "Confirmation of resolution of clinical inflammation by aqueous PCR showing undetectable CMV DNA (if possible)" to Secondary outcomes.
Contributions of authors
JM; AA; HMT: helped with writing the protocol/review and responding to peer review/editorial base comments. DT, CSP: helped in responding to peer review and editorial base comments.
Sources of support
Internal sources
No sources of support supplied
External sources
-
National Institute for Health Research (NIHR), UK.
- Richard Wormald, Co‐ordinating Editor for Cochrane Eyes and Vision (CEV) acknowledges financial support for his CEV research sessions from the Department of Health through the award made by the National Institute for Health Research to Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology for a Specialist Biomedical Research Centre for Ophthalmology.
- This review was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to the CEV UK editorial base.
The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Declarations of interest
JM: none known AA: none known HMT: none known DT: none known CSP: none known
New
References
Additional references
Ang 2013
- Ang M, Sng CC, Chee SP, Tan DT, Mehta JS. Outcomes of corneal transplantation for irreversible corneal decompensation secondary to corneal endotheliitis in Asian eyes. American Journal of Ophthalmology 2013;156(2):260‐6. [DOI] [PubMed] [Google Scholar]
Anshu 2009
- Anshu A, Chee SP, Mehta J, Tan DT. CMV endotheliitis in Descemet's stripping endothelial keratoplasty. Ophthalmology 2009;116(4):624‐30. [DOI] [PubMed] [Google Scholar]
Chee 2007
- Chee SP, Bacsal K, Jap A, Se‐Thoe SY, Cheng CL, Tan BH. Corneal endotheliitis associated with evidence of cytomegalovirus infection. Ophthalmology 2007;114(4):798‐803. [DOI] [PubMed] [Google Scholar]
Chee 2008
- Chee SP, Bacsal K, Jap A, Se‐Thoe SY, Cheng CL, Tan BH. Clinical features of cytomegalovirus anterior uveitis in immunocompetent patients. American Journal of Ophthalmology 2008;145(5):834‐40. [DOI] [PubMed] [Google Scholar]
Chee 2012
- Chee SP, Jap A. Treatment outcome and risk factors for visual loss in cytomegalovirus endotheliitis. Graefe's Archive for Clinical and Experimental Ophthalmology 2012;250(3):383‐9. [DOI] [PubMed] [Google Scholar]
De Schryver 2006
- Schryver I, Rozenberg F, Cassoux N, Michelson S, Kestelyn P, Lehoang P, et al. Diagnosis and treatment of cytomegalovirus iridocyclitis without retinal necrosis. British Journal of Ophthalmology 2006;90(7):852‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JP, Altman DG, editor(s). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Glanville 2006
- Glanville JM, Lefebvre C, Miles JN, Camosso‐Stefinovic J. How to identify randomized controlled trials in MEDLINE: ten years on. Journal of the Medical Library Association 2006;94(2):130‐6. [PMC free article] [PubMed] [Google Scholar]
GRADEpro 2014 [Computer program]
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed 30 March 2017. Hamilton (ON): GRADE Working Group, McMaster University, 2014.
Higgins 2011a
- Higgins JP, Altman DG, Sterne JAC, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011b
- Higgins JP, Deeks JJ, editor(s). Chapter 7: Selecting studies and collecting data. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011c
- Higgins JP, Deeks JJ, Altman DG, editor(s). Chapter 16: Special topics in statistics. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Jap 2011
- Jap A, Chee SP. Viral anterior uveitis. Current Opinion in Ophthalmology 2011;22(6):483‐8. [DOI] [PubMed] [Google Scholar]
Kobayashi 2012
- Kobayashi A, Yokogawa H, Higashide T, Nitta K, Sugiyama K. Clinical significance of owl eye morphologic features by in vivo laser confocal microscopy in patients with cytomegalovirus corneal endotheliitis. American Journal of Ophthalmology 2012;153(3):445‐53. [DOI] [PubMed] [Google Scholar]
Koizumi 2006
- Koizumi N, Yamasaki K, Kawasaki S, Sotozono C, Inatomi T, Mochida C, et al. Cytomegalovirus in aqueous humor from an eye with corneal endotheliitis. American Journal of Ophthalmology 2006;141(3):564‐5. [DOI] [PubMed] [Google Scholar]
Koizumi 2007
- Koizumi N, Suzuki T, Uno T, Chihara H, Shiraishi A, Hara Y, et al. Cytomegalovirus as an etiologic factor in corneal endotheliitis. Ophthalmology 2008;115(2):292‐7. [DOI] [PubMed] [Google Scholar]
Koizumi 2014
- Koizumi N, Inatomi T, Suzuki T, Shiraishi A, Ohashi Y, Kandori M, et al. Clinical features and management of cytomegalovirus corneal endotheliitis: analysis of 106 cases from the Japan corneal endotheliitis study. British Journal of Ophthalmology 2015;99(1):54‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Markomichelakis 2002
- Markomichelakis NN, Canakis C, Zafirakis P, Marakis T, Mallias I, Theodossiadis G. Cytomegalovirus as a cause for anterior uveitis with sectorial iris atrophy. Ophthalmology 2002;109(5):879‐88. [DOI] [PubMed] [Google Scholar]
Mietz 2000
- Mietz H, Aisenbrey S, Ulrich Bartz‐Schmidt K, Bamborschke S, Krieglstein GK. Ganciclovir for the treatment of anterior uveitis. Graefe's Archive for Clinical and Experimental Ophthalmology 2000;238(11):905‐9. [DOI] [PubMed] [Google Scholar]
Shiraishi 2007
- Shiraishi A, Hara Y, Takahashi M, Oka N, Yamaguchi M, Suzuki T, et al. Demonstration of "owl's eye" morphology by confocal microscopy in a patient with presumed cytomegalovirus corneal endotheliitis. American Journal of Ophthalmology 2007;143(4):715‐7. [DOI] [PubMed] [Google Scholar]
Sonoyama 2010
- Sonoyama H, Araki‐Sasaki K, Osakabe Y, Nakamura M, Amano S, Koizumi N, et al. Detection of cytomegalovirus DNA from cytomegalovirus corneal endotheliitis after penetrating keratoplasty. Cornea 2010;29(6):683‐5. [DOI] [PubMed] [Google Scholar]
Sterne 2011
- Sterne JAC, Egger M, Moher D, editor(s). Chapter 10: Addressing reporting biases. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Stewart 2011
- Stewart LA, Tierney JF, Clarke M. Chapter 18: Reviews of individual patient data. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Suzuki 2007
- Suzuki T, Hara Y, Uno T, Ohashi Y. DNA of CMV detected by PCR in aqueous of patient with corneal endothelialitis after penetrating keratoplasty. Cornea 2007;26(3):370‐2. [DOI] [PubMed] [Google Scholar]
Van Boxtel 2007
- Boxtel LA, Lelij A, Meer J, Los LI. Cytomegalovirus as a cause of anterior uveitis in immunocompetent patients. Ophthalmology 2007;114(7):1358‐62. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Anshu 2015
- Anshu A, Tan D, Chee SP, Mehta JS, Htoon HM. Interventions for the management of CMV‐associated anterior segment inflammation. Cochrane Database of Systematic Reviews 2015, Issue 10. [DOI: 10.1002/14651858.CD011908] [DOI] [PMC free article] [PubMed] [Google Scholar]