

Abstract
Background
Surgical site infection rates in the month following clean surgery vary from 0.6% (knee prosthesis) to 5% (limb amputation). Due to the large number of clean surgical procedures conducted annually the costs of these surgical site infections (SSIs) can be considerable in financial and social terms. Preoperative skin antisepsis using antiseptics is performed to reduce the risk of SSIs by removing soil and transient organisms from the skin where a surgical incision will be made. Antiseptics are thought to be toxic to bacteria and therefore aid their mechanical removal. The effectiveness of preoperative skin preparation is thought to be dependent on both the antiseptic used and the method of application, however, it is unclear whether preoperative skin antisepsis actually reduces postoperative wound infection, and, if so, which antiseptic is most effective.
Objectives
To determine whether preoperative skin antisepsis immediately prior to surgical incision for clean surgery prevents SSI and to determine the comparative effectiveness of alternative antiseptics.
Search methods
For this third update we searched just the Cochrane Wounds Group Specialised Register (searched 27 January 2015); The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2014, Issue 12).
Selection criteria
Randomised controlled trials evaluating the use of preoperative skin antiseptics applied immediately prior to incision in clean surgery. There was no restriction on the inclusion of reports based on language of publication, date or publication status.
Data collection and analysis
Data extraction and assessment of risk of bias were undertaken independently by two review authors.
Main results
There were no new studies added to the review in the third update
Thirteen studies were included in this review (2,623 participants). These evaluated several different types of skin antiseptics ‐ leading to 11 different comparisons being made. Although the antiseptics evaluated differed between studies, all trials involved some form of iodine. Iodine in alcohol was compared to alcohol alone in one trial; one trial compared povidone iodine paint (solution type not reported) with soap and alcohol. Six studies compared different types of iodine‐containing products with each other and five compared iodine‐containing products with chlorhexidine‐containing products.
There was evidence from one study suggesting that preoperative skin preparation with 0.5% chlorhexidine in methylated spirits led to a reduced risk of SSI compared with an alcohol based povidone iodine solution: RR 0.47 (95% CI 0.27 to 0.82). However, it is important to note that the trial does not report important details regarding the interventions (such as the concentration of povidone iodine paint used) and trial conduct, such that risk of bias was unclear.
There were no other statistically significant differences in SSI rates in the other comparisons of skin antisepsis. Overall the risk of bias in included studies was unclear.
A mixed treatment comparison meta‐analysis was conducted and this suggested that alcohol‐containing products had the highest probability of being effective ‐ however, again the quality of this evidence was low.
Authors' conclusions
A comprehensive review of current evidence found some evidence that preoperative skin preparation with 0.5% chlorhexidine in methylated spirits was associated with lower rates of SSIs following clean surgery than alcohol‐based povidone iodine paint. However this single study was poorly reported. Practitioners may therefore elect to consider other characteristics such as costs and potential side effects when choosing between alternatives.
The design of future trials should be driven by the questions of high priority to decision makers. It may be that investment in at least one large trial (in terms of participants) is warranted in order to add definitive and hopefully conclusive data to the current evidence base. Ideally any future trial would evaluate the iodine‐containing and chlorhexidine‐containing solutions relevant to current practice as well as the type of solution used (alcohol vs. aqueous).
Keywords: Humans; Preoperative Care; Anti‐Infective Agents, Local; Anti‐Infective Agents, Local/therapeutic use; Chlorhexidine; Chlorhexidine/therapeutic use; Ethanol; Ethanol/therapeutic use; Iodine Compounds; Iodine Compounds/therapeutic use; Povidone‐Iodine; Povidone‐Iodine/therapeutic use; Randomized Controlled Trials as Topic; Surgical Wound Infection; Surgical Wound Infection/prevention & control
Plain language summary
Preoperative skin antiseptic for prevention of surgical wound infections after clean surgery
Patients' skin at the operation site is routinely cleansed with antiseptic solutions in the operating theatre before surgical incisions are made. This skin cleansing with an antiseptic aims to reduce the microorganisms present on the skin and therefore reduce the risk that the surgical wound will become infected. It is not known whether one antiseptic treatment is better than any other(s) at preventing infection, so our team examined the evidence for antiseptic skin preparation prior to clean surgery (i.e. surgery that does not involve the breathing system, gut, genital or urinary tract or any part of the body with an existing infection) to see if there are differences between preoperative antiseptic treatments. Unfortunately there is very little good quality research around skin cleansing before surgery and we cannot say whether one antiseptic is better than another at preventing wound infections. More research is required to show whether one antiseptic is better than the others at preventing wound infection after clean surgery.
Background
Description of the condition
Surgical site infections (SSIs) can occur following an invasive surgical procedure (NICE 2008). An SSI can be diagnosed by the presence of clinical signs and symptoms alone, e.g. pus, redness, pain, heat, or based on the presence of one or more clinical symptoms along with a quantitative measurement of more than 106 colony forming units per mm³ tissue (Mangram 1999). Surgical procedures and their resulting surgical wounds are classified as either clean, clean‐contaminated, contaminated or dirty‐infected, depending upon the area of the body operated upon and the level of infection and inflammation present (Table 1). A surgical wound is less likely to become infected postoperatively if it is classified as clean. Leaper 1995 suggested expected infection rates of less than 2% in clean surgery and less than 10% in contaminated surgery.
1. Classifications of surgical procedures.
| Classification | Description |
| Clean | Non‐infective surgical wounds in which no inflammation is encountered, and neither the respiratory, alimentary, genitourinary tract nor the oro‐pharyngeal cavity is entered. In addition these cases are elective, primarily closed, and drained with closed drainage system when required. |
| Clean/ Contaminated | Surgical wounds in which respiratory, alimentary, genital or urinary tract is entered under controlled conditions and without unusual contamination. Specifically, surgeries involving the biliary tract, appendix, vagina and oropharynx are included in this category, provided no evidence of infection or a major break in sterile technique is encountered. |
| Contaminated | Fresh, accidental wounds, operations with major breaks in sterile technique or gross spillage from the gastrointestinal tract, and incisions in which acute, non‐purulent inflammation is encountered. |
| Dirty | Old traumatic wounds with retained devitalised tissue and those that involve existing clinical infection or perforated viscera. This definition suggests that organisms causing postoperative infection were present in the operative field before the operation. |
In the UK the Health Protection Agency (HPA) collects ongoing SSI data nationally although only data collection following orthopaedic surgery is mandatory. From April 2006 to March 2011, the HPA collected data in 237 NHS hospitals on 438,679 surgical procedures (Health Protection Agency 2011). They report clean SSI rates of: 0.6% for knee prosthesis; 1% for cardiac surgery (non‐coronary artery bypass graft); 0.8% for hip prosthesis and 5% for limb amputation. This is in contrast to the HPA‐reported incidence (2006 to 2011) of SSI following surgery on the large bowel (contaminated) of 10%. Whilst the incidence of SSI in clean surgery can be low relative to other surgical procedures, there are tens of thousands of clean procedures performed annually world‐wide and the frequency of these procedures raises the overall numbers at risk for SSI in this group. Addtionally, since for clean surgery there is, arguably, a lower risk of infection from 'internal' contamination, it may be that skin cleansing plays, relatively, a more important role in terms of SSI prevention compared to non‐clean surgeries.
The costs incurred when a patient contracts an SSI can be considerable in financial, as well as social, terms. It has been estimated that patients with SSIs require, on average, an additional hospital stay of 6.5 days, and that hospital costs are doubled. When extrapolated to all acute hospitals in England, it is estimated that the annual cost is approximately GBP 1 billion (Plowman 2000). NICE 2006 identified that an SSI increased the costs of surgery by two to five times (NICE 2008).
Description of the intervention
The removal of transient bacteria and reduction of the number of commensal organisms by an antiseptic is recommended prior to surgery by several organisations including the Royal College of Surgeons of England (Leaper 2001), the Centers for Disease Control and Prevention (CDC) (Mangram 1999), the Association of Perioperative Registered Nurses (AORN) (AORN 2006), and the Association for Perioperative Practice (AfPP 2007). Therefore, it has become routine preoperative practice to cleanse the skin at the operation site with an antiseptic (McCluskey 1996). The effectiveness of preoperative skin preparation is thought to depend on both the antiseptic used and the method of application.
CDC guidance states:
the size of the area prepared should be sufficient to include any potential incision sites divorced from the main incision site e.g. abdominal preparation for laparoscopic surgery (Mangram 1999);
the solution should be applied in concentric circles;
a dedicated instrument may be used, e.g. a sponge, or X‐ray detectable swab, adapted for the purpose; this applicator should be discarded once the periphery has been reached;
time should be allowed for the solution to dry, especially when alcoholic solutions are used, as these are flammable (MHRA 2000).
AORN guidelines stipulate the following (AORN 2006):
that the applicator used should be sterile;
the solution should be applied using friction, and extend from the incision site to the periphery.
For the purposes of this review skin preparation antiseptic agents are referred to as "antiseptics" and can be applied in the form of liquids, solutions or powders. Leclair 1990 described an antiseptic as "a chemical agent that reduces the microbial population on the skin". It is suggested that the ideal agent would:
kill all bacteria, fungi, viruses, protozoa, tubercle bacilli and spores;
be non toxic;
be hypoallergenic;
be safe to use in all body regions;
not be absorbed;
have residual activity;
be safe for repetitive use (Hardin 1997).
Several antiseptic agents are available for preoperative preparation of skin at the incision site.
Iodine/iodophors
Iodine/iodophors are iodine solutions which are effective against a wide range of Gram‐positive and Gram‐negative bacteria, the tubercle bacillus, fungi and viruses. These penetrate cell walls, then oxidise and substitute the microbial contents with free iodine (Hardin 1997; Mangram 1999; Warner 1988). Iodophors contain a surfactant/stabilising agent that liberates the free iodine (Wade 1980). Iodophor has largely replaced iodine as the active ingredient in antiseptics. Iodophor comprises free iodine molecules bound to a polymer such as polyvinyl pyrrolidine (i.e. povidone), so is often termed povidone iodine (PI) (Larson 1995). Typically, 10% PI formulations contain 1% available iodine (Larson 1995; Reichman 2009). PI is soluble in both water and alcohol, and available preparations include: aqueous iodophor scrub and paint, aqueous iodophor one‐step preparation with polymer (3M), and alcoholic iodophor with water‐insoluble polymer (DuraPrep).
Alcohol
Alcohol denatures the cell wall proteins of bacteria (Hardin 1997; Mangram 1999; Warner 1988). Alcohol is active against Gram‐positive and Gram‐negative bacteria, the tubercle bacillus and many fungi and viruses. Concentration, rather than type, of alcohol is important in determining its effectiveness (Larson 1995; Leclair 1990).
Chlorhexidine gluconate
Chlorhexidine gluconate (aqueous or alcoholic) is an antiseptic thought to be effective against a wide range of Gram‐positive and Gram‐negative bacteria, yeasts and some viruses (Reichman 2009)
How the intervention might work
The aim of preoperative skin antisepsis is to reduce the risk of SSIs by removing soil and transient organisms from the skin (AORN 2006). The skin is not a sterile surface, but is colonised by a large number of bacteria, with up to three million microorganisms on each square centimetre of skin (Hinchliffe 1988). Antiseptics have the ability to bind to the stratum corneum, resulting in persistent chemical activity on the skin (Larson 1988). Primary action of antiseptics includes the mechanical removal, and chemical killing and inhibition, of contaminating and colonising flora (Larson 1988). As micro‐organisms tend to colonise the deeper layers of the stratum corneum (the layer of dead cells on the outside of the body), they are not shed with desquamation (loss of dead cells). There are two types of micro‐organisms on the skin; commensals, which are normally resident, and transients, which are not consistently present and are easily exchanged between individuals. The transient organisms are easily removed, whereas, it has been suggested, the commensals are difficult to remove completely (Larson 1988). The commensals include Staphylococci, diptheroid organisms, Pseudomonas and Propionibacterium species which can lead to harmful infections if they are allowed to multiply. An SSI occurs when the number of bacteria in the incision overcome the host's defences. Most commonly these bacteria are commensals from the patient's skin (Malangoni 1997).
Why it is important to do this review
It has become routine preoperative practice to cleanse the surgical site with an antiseptic (McCluskey 1996), however, it is important to assess the comparative effectiveness of alternative antiseptics to inform clinical practice. The current National Institue of Health and Clinical Excellence (NICE) guidelines recommendation regarding skin preparation across surgeries is to: "Prepare the skin at the surgical site immediately before incision using an antiseptic (aqueous or alcohol‐based) preparation: povidone‐iodine or chlorhexidine are most suitable" (NICE 2008). However, a recent trial undertaken in 849 participants undergoing clean‐contaminated surgery compared chlorhexidine in alcohol with PI‐aqueous and reported that the chlorhexidine solution was more effective in terms of SSI prevention for superficial incisional infection (4.2% developed an SSI in the chlorhexidine group compared to 8.6% in the PI group: p‐value 0.08) and deep incisional infection (1.0% developed an SSI in the chlorhexidine group compared with 3.0% in the PI group p‐value 0.05) (Darouiche 2010). A further recent systematic review meta‐analysed five RCTs that compared chlorhexidine‐alcohol with PI‐aqueous in skin antiseptics for the prevention of SSI and included Darouiche 2010, (this was the largest included study in the analysis). The authors report that there was evidence that chlorhexidine‐alcohol reduces risk of SSI following surgery compared with PI: risk ratio (RR) of 0.65, 95% CI 0.50 to 0.85 (Maiwald 2012). However, this review goes on to raise the important issue of whether there is potential for the alcohol in the chlorhexidine‐alcohol solution to have a role in SSI prevention that is not being acknowledged when PI‐aqueous solutions are compared with chlorhexidine‐alcohol solutions (Maiwald 2012; Maiwald 2014). Given the inclusion of RCTs evaluating clean/contaminated wounds in this review it is not clear how its results relate to clean surgical wounds.
Objectives
To determine whether preoperative skin antisepsis immediately prior to incision prevents SSI and to determine the comparative effectiveness of alternative antiseptics.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) comparing use of preoperative skin antiseptics with no skin antiseptics and those comparing different skin antiseptics.
Types of participants
People of any age undergoing clean surgery. For the purposes of this review the CDC definition of a clean surgical wound was applied (Mangram 1999). Settings were not limited to a specific clinical area as clean surgery can take place in a variety of environments.
Types of interventions
Studies in which antiseptic solutions or powders were applied to the participant's skin at the specific site of surgery, under sterile conditions and prior to surgical incision in the immediate preoperative period. The following comparisons were eligible for inclusion:
One or more antiseptics (solution, powder) compared with a control.
One type of antiseptic compared with another type of antiseptic.
One antiseptic applied more than once compared with the same antiseptic applied in a single application.
One antiseptic applied more than once compared with another antiseptic applied more than once.
The review did not compare different cleansing techniques, e.g. antiseptic showers or body washes and did not compare the use of incise drapes as these are considered by other reviews (Webster 2011; Webster 2012).
Types of outcome measures
Primary outcomes
Occurance of postoperative SSI as defined by the CDC criteria (Horan 2008), or the authors' definition of SSI. We did not differentiate between superficial and deep‐incisional infection.
Secondary outcomes
Participant health‐related quality of life / health status (measured using a standardised generic questionnaire such as EQ‐5D (Dolan 1995), SF‐36, SF‐12 or SF‐6 (Ware 2001) or wound‐specific questionnaires such as the Cardiff wound impact schedule (Price 2004). We did not include ad hoc measures of quality of life which are likely not to be validated and will not be common to multiple studies.
Other adverse events including death (measured using survey/questionnaire/data capture process or visual analogue scale).
Resource use (including measurements of resource use such as length of hospital stay and re‐operation/intervention).
Search methods for identification of studies
Electronic searches
The databases searched and CENTRAL search strategies used in the first and second update of the review can be found in Appendix 1. For this third update we searched the following electronic databases:
Cochrane Wounds Group Specialised Register (searched 27 January 2015); The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2014, Issue 12).
The following search strategy was used in the Cochrane Central Register of Controlled Trials (CENTRAL):
#1 MeSH descriptor Skin explode all trees #2 MeSH descriptor Antisepsis explode all trees #3 (#1 AND #2) #4 "skin antisepsis" #5 MeSH descriptor Anti‐Infective Agents, Local explode all trees #6 MeSH descriptor Iodine explode all trees #7 MeSH descriptor Iodophors explode all trees #8 MeSH descriptor Povidone‐Iodine explode all trees #9 MeSH descriptor Chlorhexidine explode all trees #10 MeSH descriptor Alcohols explode all trees #11 iodophor* or povidone‐iodine or betadine or chlorhexidine or alcohol or alcohols or antiseptic* #12 MeSH descriptor Detergents explode all trees #13 (#1 AND #12) #14 skin NEAR detergent* #15 MeSH descriptor Disinfectants explode all trees #16 (#1 AND #15) #17 skin NEAR disinfect* #18 (#3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #13 OR #14 OR #16 OR #17) #19 MeSH descriptor Surgical Wound Infection explode all trees #20 MeSH descriptor Surgical Wound Dehiscence explode all trees #21 (surgical NEAR/5 infection):ti,kw,ab #22 (surgical NEAR/5 wound*):ti,ab,kw #23 ((post‐operative or postoperative) NEAR (wound NEXT infection*)):ti,ab,kw #24 MeSH descriptor Preoperative Care explode all trees #25 (preoperative or pre‐operative):ti,ab,kw #26 (#19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25) #27 (#18 AND #26)
As part of the updating process modifications were made to the CENTRAL search string (the MeSH heading Surgical Wound Dehiscence was included). All other database strings were modified accordingly and searches were re‐run over all years. The search strategies for Ovid MEDLINE, Ovid EMBASE and EBSCO CINAHL used in the first and second update can be found in Appendix 2; Appendix 3 and Appendix 4 respectively. The Ovid MEDLINE search was combined with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐ and precision‐maximizing version (2008 revision); Ovid format (Lefebvre 2011). The EMBASE and CINAHL searches were combined with the trial filters developed by the Scottish Intercollegiate Guidelines Network (SIGN 2011). No date or language restrictions were applied.
Searching other resources
We also searched the bibliographies of all retrieved and relevant publications identified by the above strategies for further studies.
Data collection and analysis
Selection of studies
Two review authors independently assessed titles and abstracts of citations identified by the search strategy against the selection criteria. The review authors obtained copies of articles and studies that appeared to satisfy these criteria. If it was unclear from the title or abstract whether the paper fulfilled the criteria, or when there was disparity between the review authors, a copy of the full article was obtained. All review authors decided independently whether to include or exclude a study. Disagreements were resolved by discussion or referred to another party.
Data extraction and management
The review authors used a piloted data extraction sheet to extract and summarise details of the studies. Where data were missing from a study, the review authors attempted to contact the trial authors to obtain the missing information. The review authors undertook data extraction independently, and then compared their results.
Assessment of risk of bias in included studies
All review authors independently assessed each included study using the Cochrane Collaboration tool for assessing risk of bias (Higgins 2011). This tool addresses up to six specific domains, namely sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other issues (see Appendix 5 for details of criteria on which the judgement was based). We discussed any disagreement amongst all review authors to achieve a consensus.
We presented our assessment of risk of bias using a 'Risk of bias' summary figure, which presents all of the judgements in a cross‐tabulation of study by entry. This display of internal validity indicates the weight the reader may give the results of each study. The risk of bias graph gives review authors' judgements about each risk of bias item presented as percentages across all included studies.
Data synthesis
We considered both clinical and statistical heterogeneity. Wherever appropriate data were pooled using meta‐analysis (conducted using RevMan 5.3 (RevMan 2014)), that is where studies appeared similar in terms of wound type, intervention type, duration and outcome type. We assessed statistical heterogeneity using the chi² test (a significance level of P < 0.1 was considered to indicate heterogeneity) and the I² estimate (Higgins 2003). The I² estimate examines the percentage of total variation across studies due to heterogeneity rather than to chance. Values of I² over 50% indicate a high level of heterogeneity. In the absence of clinical heterogeneity and in the presence of statistical heterogeneity (I² over 50%), we used a random‐effect model, however, we did not pool studies at all where heterogeneity was very high (I² over 75%). Where there was no clinical or statistical heterogeneity we used a fixed‐effects model.
Measures of treatment effect
We entered data into Cochrane Review Manager Version 5 software (RevMan 2014), and used this program for the analysis. We presented effect measures for dichotomous outcomes (e.g. rates of infection) as risk ratio (RR) with 95% confidence intervals (CI). For continuous outcomes, we planned to use the mean difference (MD), or, if the scale of measurement differed across trials, standardised mean difference (SMD), each with 95% CI
Subgroup analysis and investigation of heterogeneity
Because of on‐going interest regarding whether possible differences in SSI prevention rates for peri‐operative skin antiseptics are due to the carrier solutions (alcohol‐based vs. aqueous‐based), we compared studies comparing aqueous and alcohol solutions regardless of active ingredient (e.g. chlorhexidine or PI).
Mixed Treatment Comparison Meta‐analysis
To maximise the use of all available RCT data and to facilitate decision making regarding antiseptic choice, in addition to a standard meta‐analysis, we conducted a mixed treatment comparison meta‐analysis (sometimes called a network meta‐analysis). This approach links head‐to‐head comparison data from trials, via common comparators, into a network which can then be used to calculate indirect estimates of relative treatment effect. In a simple example where there are three treatments A, B and C compared in two head‐to‐head trials, A vs B and B vs C, as B is a common comparator the network of A—B—C can be formed. These data can then be used to obtain an indirect estimate of the relative effects of A vs C. In networks where direct and indirect data exist for some or all links, both are used to generate relative treatment effect estimates, with direct evidence given more ‘weight’ in the final estimate. The mixed treatment comparison was conducted from a Bayesian perspective using Winbugs and results summarised in this review. Fixed and random effects models were fitted to these data and model fit was assessed using residual deviance and deviance information criterion (DIC).
The treatment with the highest relative effect estimate in the mixed treatment comparison meta‐analysis is expected to confer the highest likelihood of preventing SSIs. However, it is important to fully comprehend the uncertainty around such estimates. In addition to presenting credible interval (CrIs), a Bayesian equivalent of confidence intervals, we represented uncertainty regarding treatment choice as the probability that each dressing was the ‘best’ treatment in terms of being the most likely to heal diabetic foot ulcers (when compared to all other evaluated treatments).
Quality assessment of mixed treatment comparison meta‐analysis estimates
We wanted to reflect the quality of the evidence provided by the mixed treatment comparison meta‐analysis so that any conclusions made could reflect the quality of the data being drawn on as occurs in other forms of evidence synthesis. Whilst there is no recognised system to undertake such quality assessment for mixed treatment comparison meta‐analysis we have previously published a modified GRADE approach (we called this iGRADE) to allow us to access and communicate the quality of mixed treatment comparison meta‐analysis‐derived evidence (Dumville 2012). The iGRADE approach uses the five GRADE categories that allow the quality of evidence to be decreased, with the focus of some categories modified so they are relevant when assessing a mixed treatment comparison meta‐analysis (Appendix 6). We conducted a cautious application of iGRADE to the mixed treatment comparison meta‐analysis where estimates could be graded as very low quality evidence, low evidence; moderate evidence and high quality evidence. No formal down‐weighting of evidence was undertaken.
Results
Description of studies
Results of the search
The initial search and searches for the three updates yielded a total of 856 citations which were screened for potential relevance. A total of 34 papers were retrieved for full examination and were classified as follows:
original review, six studies included (Alexander 1985; Berry 1982; Roberts 1995; Segal 2002; Dewan 1987; Lorenz 1988); 12 studies ineligible (not RCTs or ineligible outcome measures);
first update,one further study included (Ellenhorn 2005);
second update, three further studies included (Paocharoen 2009; Saltzman 2009, Sistla 2010) (with authors for Paocharoen 2009 and Saltzman 2009 responding to requests for further information to confirm eligibility. In this current update, the inclusion criteria have been narrowed so only studies of antiseptic solutions or powders (applied to the patient in the immediate preoperative period) are included: this is in response to the publication of a Cochrane Review considering the use of plastic adhesive drapes during surgery for preventing SSI (Webster 2011). This reclassification of plastic adhesive drapes resulted in two previously included studies (Dewan 1987; Lorenz 1988) being excluded as they evaluated drapes and not skin cleansers per se; additionally, the fourth arm of the Segal 2002 study was not considered. Studies considering film‐forming solutions are still included in this review;
third update, it was decided that Bibbo 2005; Gilliam 1990; Howard 1991; Meier 2001; and Shirahatti 1993 should be moved from excluded studies into included studies as they were deemed to be randomised controlled trials based on the information provided. No further eligible studies were identified. Two studies were obtained as full text and both were excluded at this stage. Two studies are 'awaiting assessment' whilst we contact the trial authors for further information (Nentwich 2012; Taneja 2012).
No further eligible unpublished studies were identified. (See Characteristics of excluded studies)
Included studies
See Characteristics of included studies
A summary is presented in Table 2. Thirteen studies are included in this third update; one four‐arm study (Segal 2002), one three‐arm (Saltzman 2009) and eleven two arm studies (Alexander 1985; Berry 1982; Ellenhorn 2005; Paocharoen 2009; Roberts 1995; Sistla 2010; Bibbo 2005; Gilliam 1990; Howard 1991; Meier 2001; Shirahatti 1993). All studies took place in hospital operating theatres.
2. Summary of Studies.
| Study ID | Group A | n (Group A) | Group B | n (Group B) | Group C | n (Group C) | Duration of follow‐up | SSI outcome data available |
| Alexander 1985 | 70% alcohol (1‐minute scrub) and polyester antimicrobial incise drape | 76 | 2% iodine in 90% alcohol (1‐minute scrub) and polyester antimicrobial incise drape | 81 | n/a | one month | Yes | |
| Berry 1982 | 10% PI in alcohol | 256 | 0.5% Chlorhexidine in methylated spirit (Hibitane) | 286 | n/a | Until hospital discharge | Yes | |
| Bibbo 2005 | 7.5% PI scrub (7‐minutes) followed by 10% aqueous PI paint | 67 | 4% Chlorhexidine in 70% isopropyl alcohol scrub (7‐minutes) | 60 | n/a | Not reported | Yes | |
| Ellenhorn 2005 | 0.75% (available iodine) PI soap scrub (5 minute) followed by 1% (available iodine) aqueous PI paint | 33 | 1% (available iodine) aqueous PI paint | 37 | n/a | 30 days | Yes | |
| Gilliam 1990 | Aqueous iodophor scrub (5‐minute) followed by application of iodophor paint | 30 | Water insoluble iodophor‐in‐alcohol solution | 30 | n/a | Not reported | Yes | |
| Howard 1991 | Aqueous iodophor scrub (5‐minute) followed by iodophor paint | 75 | Water insoluble iodophor‐in‐alcohol solution | 84 | n/a | At least 30 days post‐op | Yes | |
| Meier 2001 | Scrub with standard (shop‐brought) soap (5‐minute) followed by methylated spirit | 98 | PI paint (n=102) | 102 | n/a | 4 to 8 weeks post operatively | Yes | |
| Paocharoen 2009 | 5‐minute scrub with PI followed by aqueous 10% PI paint | 87 | 4% chlorhexidine in 70% isopropyl alcohol scrub (5 minute)(Hibitane) followed by Hibitane paint | 96 | n/a | one month | Yes | |
| Roberts 1995 | Aqueous iodophor scrub (5‐10 minutes) followed by iodophor paint | 96 | Iodophor‐in‐alcohol, film‐forming, water insoluble antiseptic | 104 | n/a | 30 days | Yes | |
| Saltzman 2009 | 0.75% PI scrub followed by 1% PI paint | 50 | 2% chlorhexidine gluconate and 70% alcohol | 50 | Water insoluble iodophor‐in‐alcohol solution | 50 | 10 months | Yes |
| Segal 2002 | 7.5% PI scrub (5‐minute) followed by 10% aqueous PI paint | 52 | 10% aqueous PI paint | 56 | Water insoluble iodophor‐in‐alcohol solution | 50 | 6 weeks post‐op. | Yes |
| Shirahatti 1993 | 0.75% Cholorhexidine and 1.5% cetrimide scrub (10 minutes) followed by application of 1% iodine in 70% spirit | 46 | Application of 0.75% Chlorhexidine and 1.5% cetrimide followed by application of 1% iodine in 70% spirit | 45 | n/a | Not reported | Yes | |
| Sistla 2010 | 10% PI aqueous paint | 285 | 2.5% chlorhexidine with 70% ethanol | 271 | n/a | 30 days | Yes |
Participants
Four studies did not specify types of surgery undertaken on trial participants, simply providing separate data on clean and non‐clean surgery (Alexander 1985; Howard 1991; Paocharoen 2009; Shirahatti 1993). One study recruited participants reported to be undergoing elective abdominal procedures (Ellenhorn 2005). Other studies were classified as: 'hernia, genitalia, veins' and other 'clean' operations (Berry 1982); elective foot and ankle surgery (Bibbo 2005) and clean total joint surgery (Gilliam 1990). Five studies were based on a single procedures: shoulder surgery (Saltzman 2009); coronary artery bypass graft (Roberts 1995; Segal 2002) and elective hernia repair (Meier 2001; Sistla 2010).
Interventions
Although the antiseptics studied differed between studies, all trials involved some form of iodine. Iodine in alcohol was compared with alcohol alone in one trial (Alexander 1985); one trial compared PI paint (solution type not reported) with soap and alcohol (Meier 2001). Six studies compared different types of iodine‐containing products with each other (Ellenhorn 2005; Gilliam 1990; Howard 1991; Roberts 1995; Saltzman 2009; Segal 2002) and five compared iodine‐containing products with chlorhexidine‐containing products (Berry 1982; Bibbo 2005; Paocharoen 2009; Saltzman 2009; Sistla 2010). One included study used antimicrobial incise drapes on all patients (Alexander 1985) and one used iodophor‐impregnated incise drapes on all chest wounds, but not leg wounds (Roberts 1995).
Excluded studies
In total, 21 studies were excluded; data for clean surgery could not be extracted from six of the studies (Brooks 2001; Brown 1984; Geelhoed 1983; Hibbard 2002; Silva 1985; Zdeblick 1986), Nine studies were not RCTs (Eiselt 2009; Hagen 1995; Kalantar‐Hormozi 2005; Lee 2013; Ostrander 2005; Polk 1967; Swenson 2009; Vos 2010; Yoshimura 2003 ), two studies did not involve clean surgery (Culligan 2005; Shindo 2002); three studies had no systematic difference in skin antiseptics (as defined by review) used between groups (Dewan 1987; Lewis 1984; Lorenz 1988) and in one study the antiseptic was applied post‐operatively (Becerro de Bengoa 2013). Full details are given in the Characteristics of excluded studies.
Risk of bias in included studies
(See Characteristics of included studies for details and risk of bias summary figures Figure 1; Figure 2)
1.
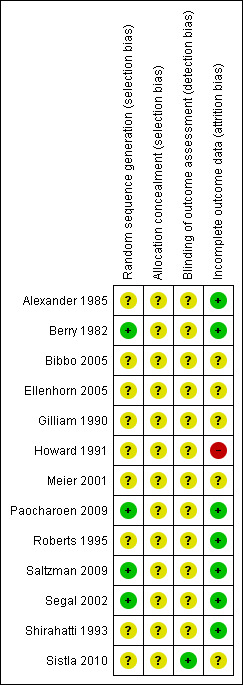
Risk of Bias summary of Included Studies.
2.
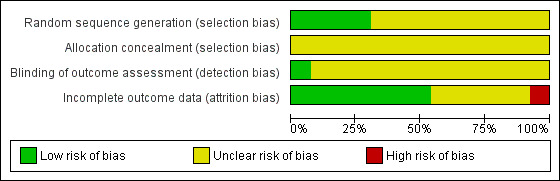
Risk of Bias Graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Method of randomisation
The generation of the randomisation sequence was classed as adequate in four studies (Ellenhorn 2005; Roberts 1995; Saltzman 2009; Segal 2002). The remaining studies were classed as being at unclear risk of bias for this domain.
Allocation concealment
The risk of bias associated with the method of allocation concealment was considered unclear for all studies. Whilst a number of studies provided some detail about the allocation concealment process there was insufficient information to confidently classify the studies as at high or low risk of bias: e.g. Meier 2001 states that "Randomisation was performed using a card drawing system" but it is not clear what this refers to or who conducted this process. Likewise Alexander 1985 states "randomisation was carried out by drawing a card from a sealed envelope" but there is no detail about who randomised participants and whether other features were used to protect against the introduction of bias ‐ e.g. envelopes being numbered and opaque.
Blinding
Blinded outcome assessment is important in wound care studies for outcomes that have a subjective element to their assessment like healing and SSI. The risk of bias associated with outcome assessment was rated as unclear in twelve of the thirteen included studies. The study by Berry 1982 aimed to conduct blinded outcome assessment, but reported that wounds were assessed by those who had been present during surgery for some participants and thus it was classed as being at unclear risk of bias. Saltzman 2009 stated that the study was double blind, but provided no further details. Only Sistla 2010 was classed at low risk of bias for this domain stating that "information regarding the antiseptic used was not available to the investigators or the patients during the assessment of wounds for SSI".
Effects of interventions
Very limited information on secondary outcomes was given in the trial reports and thus only the primary outcome incidence of SSIs are reviewed here. In all comparisons the first treatment is considered the 'intervention' and the second the 'control'. RR point estimates less than one favour the intervention and those over one favour the control.
1. Iodine in alcohol compared with alcohol
Comparison 1: 2% iodine in 90% alcohol compared with 70% alcohol (one trial; 157 participants)
Alexander 1985 recruited 157 participants undergoing elective clean surgery, randomising them to skin preparation using an iodine in alcohol solution (2% iodine in 90% alcohol) or skin preparation using an alcohol solution (70%) ‐ both applications were reported to be 1‐minute scrubs. Both study arms were also treated with an antimicrobial incise drape and participants were followed up for one month.
Primary outcome: SSI
There was no statistically significant difference in the number of SSIs in the iodine‐alcohol treated group (1/81; 1.2%) compared with the alcohol‐only treated group (1/76; 1.3%): RR 0.94, 95% CI 0.06 to 14.74 (Analysis 1.1). The study was classed as being at unclear risk of bias.
1.1. Analysis.
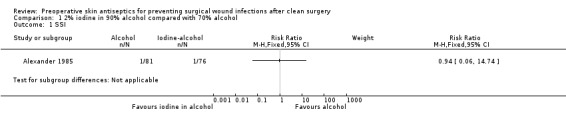
Comparison 1 2% iodine in 90% alcohol compared with 70% alcohol, Outcome 1 SSI.
Summary: 2% iodine in 90% alcohol compared with 70% alcohol
Limited data from one small study at unclear risk of bias found no statistically significant difference in the number of SSIs following skin preparation with 2% iodine in 90% alcohol compared with 70% alcohol alone.
2. Iodophor compared with alcohol
Comparison 2: PI paint compared with soap (shop bought) scrub/methylated spirit (one trial; 200 participants)
Meier 2001 recruited 200 participants undergoing elective hernia repair and compared skin preparation using a PI‐paint solution (concentration or base not specified) compared with skin preparation using shop‐bought soap (described as 5‐minute scrub) followed by application of methylated spirits. Participants were followed up for 4 to 8 weeks post‐operatively.
Primary outcome: SSI
There was no evidence of a difference in the number of SSIs in the PI paint‐treated group (6/102; 5.9%) compared with the soap/methylated spirit‐treated group (5/98; 5.1% ): RR 1.15, 95% CI 0.36 to 3.66 (Analysis 2.1). The study was classed as being at unclear risk of bias.
2.1. Analysis.
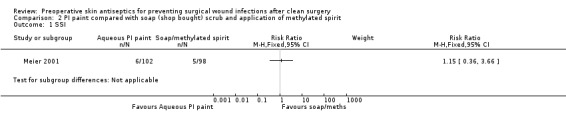
Comparison 2 PI paint compared with soap (shop bought) scrub and application of methylated spirit, Outcome 1 SSI.
Summary: PI paint compared with soap (shop bought) scrub and application of methylated spirit
Limited data from one small study at unclear risk of bias found no statistically significant difference in the number of SSIs following skin preparation with PI paint when compared with skin preparation with soap followed by application of methylated spirits.
3. Iodopher compared with iodophor
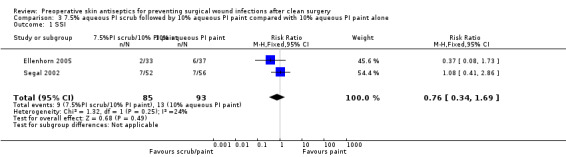
Comparison 3: 7.5% aqueous PI scrub/10% aqueous PI paint compared with 10% aqueous PI paint (two trials; 178 participants)
Ellenhorn 2005 randomised 70 oncology participants undergoing clean elective abdominal procedures and had 30 days follow up. Segal 2002 was a three‐arm trial randomising 209 participants all undergoing a coronary artery bypass graft and had 6 weeks post‐operative follow‐up.
Primary outcome: SSI
Ellenhorn 2005: there was no evidence of a difference in the number of SSIs in the PI scrub/paint‐treated group (2/33; 6%) compared with the PI paint‐treated group (6/37; 16%): RR 0.37, 95% CI 0.08 to 1.73 (Analysis 3.1). This study was classed as being at unclear risk of bias. Segal 2002: there was no statistically significant difference in the number of SSIs in the PI scrub/paint‐treated group (7/52; 14%) compared with the PI paint‐treated group (7/56; 13%): RR 1.08, 95% CI 0.41 to 2.86 (Analysis 3.1). This study was classed as being at unclear risk of bias.
3.1. Analysis.
Comparison 3 7.5% aqueous PI scrub followed by 10% aqueous PI paint compared with 10% aqueous PI paint alone, Outcome 1 SSI.
Data from these two studies were pooled using a fixed effects model (I2 = 24%). Results showed no statistically significant difference in number of SSIs following skin preparation with 7.5% aqueous scrub (5‐minute) followed by an application of 10% aqueous PI paint compared with an application of 10% aqueous paint alone: RR 0.76, 95% CI 0.34 to 1.69 (Analysis 3.1).
Summary: 7.5% aqueous PI scrub/10% aqueous PI paint compared with 10% aqueous PI paint alone
Data from two small studies found no strong evidence for a difference in the number of SSIs following skin preparation with 7.5% aqueous PI scrub (5‐minute) followed by application of 10% aqueous PI paint compared with application of 10% aqueous paint alone. The studies were judged to generally be at unclear risk of bias.
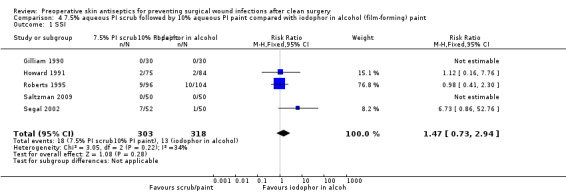
Comparison 4: 7.5% aqueous PI scrub/10% aqueous PI paint compared with iodophor in alcohol (film‐forming) paint (5 trials; 561 participants)
Five studies were included in this comparison (Gilliam 1990; Howard 1991; Roberts 1995; Saltzman 2009; Segal 2002). Gilliam 1990 randomised 60 participants undergoing clean total joint surgery ‐ length of follow‐up was not reported. Howard 1991 reported that 240 participants undergoing clean and clean‐contaminated surgery were randomised. We have used the reported outcome data for the 159 participants undergoing clean surgery. The study authors reported that outcome data from 55 study participants was excluded because of the high infection rates associated with the operating surgeons. It was not possible to obtain these excluded data and this study was classed as being at high risk of bias for incomplete outcome data. Roberts 1995 randomised 200 participants all undergoing a coronary artery bypass graft and had 30 days follow‐up. Saltzman 2009 was a three‐arm trial that randomised 150 participants all undergoing shoulder surgery and had 10 months follow‐up. Segal 2002 was a three‐arm trial recruiting 209 patients all undergoing a coronary artery bypass graft and had 6 weeks post‐operative follow‐up.
Primary outcome: SSI
Gilliam 1990 and Saltzman 2009 reported no SSI events in either group in this study (Analysis 4.1). Howard 1991: there was no statistically significant difference in the number of SSIs in the scrub/paint group (2/75; 2.6%) compared with the iodophor in alcohol group (2/84; 2.4%): RR 1.12, 95% CI 0.16 to 7.76 (Analysis 4.1). Roberts 1995: there was no statistically significant difference in the number of SSIs in the scrub/paint group (9/96; 9.4%) compared with the iodophor in alcohol group (10/104; 9.6%): RR 0.97, 95% CI 0.41 to 2.30. (Analysis 4.1). Segal 2002: there was no statistically significant difference in the number of SSIs in the scrub/paint group (7/52; 13.5%) compared with the iodophor in alcohol group (1/50; 2%): RR 6.73, 95% CI 0.86 to 52.75 (Analysis 4.1).
4.1. Analysis.
Comparison 4 7.5% aqueous PI scrub followed by 10% aqueous PI paint compared with iodophor in alcohol (film‐forming) paint, Outcome 1 SSI.
Data from the three studies reporting outcome data were pooled using a fixed effects model (I2 = 34%). Results showed no evidence of a difference in number of SSIs following skin preparation with 7.5% aqueous scrub (5‐minute) and application of 10% aqueous PI paint compared with application of iodophor in alcohol alone: RR 1.47, 95% CI 0.73 to 2.94 (Analysis 4.1).
Summary: 7.5% aqueous PI scrub/10% aqueous PI paint compared with iodophor in alcohol (film‐forming) paint
Data from five studies (one classed as being at high risk of bias) found no statistically significant difference in the number of SSIs following skin preparation with 7.5% PI aqueous scrub (5‐minute) followed by application of 10% aqueous PI paint compared with application of iodophor in alcohol.
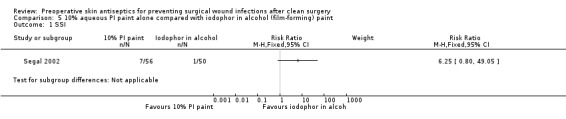
Comparison 5: 10% aqueous PI paint compared with iodophor in alcohol (film‐forming) paint (1 trial; 106 participants)
Segal 2002 was a three‐arm trial recruiting 209 patients all undergoing a coronary artery bypass graft and had 6 weeks post‐operative follow‐up.
Primary outcome: SSI
Segal 2002: there was no evidence of a difference in the number of SSIs in the PI paint alone group (7/56; 12.5%) compared with the iodophor in alcohol group (1/50; 2%): RR 6.25, 95%CI 0.80 to 49.05 (Analysis 5.1).
5.1. Analysis.
Comparison 5 10% aqueous PI paint alone compared with iodophor in alcohol (film‐forming) paint, Outcome 1 SSI.
Summary: 10% aqueous PI paint compared with iodophor in alcohol (film‐forming) paint
One small study at low risk of bias for outcome assessment but unclear for other domains found no statistically significant difference in the number of SSIs following skin preparation with 10% aqueous PI paint alone compared with iodophor in alcohol paint.
4. Iodophor compared with chlorhexidine
Comparison 6: 7.5% aqueous PI scrub/10% aqueous PI paint compared with 2% chlorhexidine in 70% alcohol paint (one trial; 100 participants)
Saltzman 2009 was a three arm trial that randomised 150 participants all undergoing shoulder surgery and had 10 months follow‐up.
Primary outcome: SSI
Saltzman 2009: there were no reported SSI events in either group for this comparison: (0/50; 0%) reported for both study arms (Analysis 6.1).
6.1. Analysis.
Comparison 6 7.5% aqueous PI scrub followed by 10% aqueous PI paint compared with 2% chlorhexidine in 70% alcohol paint, Outcome 1 SSI.
Summary: 7.5% aqueous PI scrub/10% aqueous PI paint compared with 2% chlorhexidine in 70% alcohol paint
One small, underpowered, study did not reported any SSI events in post‐operative surgical wounds randomised to either 7.5% aqueous PI scrub/10% aqueous PI paint or 2% chlorhexidine in 70% alcohol paint over a 10 month follow‐up period.
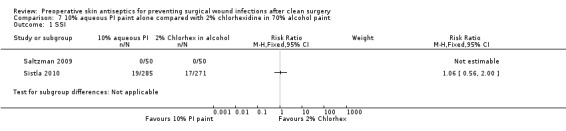
Comparison 7: 10% aqueous PI paint compared with 2% chlorhexidine in 70% alcohol paint (2 trials; 656 participants)
Two studies were included in this comparison (Saltzman 2009; Sistla 2010). Saltzman 2009 was a three ‐arm trial that randomised 150 participants all undergoing shoulder surgery and had 10 months follow‐up. Sistla 2010 randomised 556 participants undergoing elective inguinal hernia repair and had 30 days follow‐up.
Primary outcome: SSI
Saltzman 2009: there were no reported SSI events in either group for this comparison: (0/50; 0%) reported for both study arms (Analysis 7.1). Sistla 2010: there was no statistically significant difference in the number of SSIs in the PI paint group (19/285; 6.7%) compared with the 2% chlorhexidine group (17/271; 6.3%): RR 1.06, 95%CI 0.56 to 2.00. (Analysis 7.1).
7.1. Analysis.
Comparison 7 10% aqueous PI paint alone compared with 2% chlorhexidine in 70% alcohol paint, Outcome 1 SSI.
Summary: 10% aqueous PI paint compared with 2% chlorhexidine in 70% alcohol paint
Data from one study found no evidence of a difference in the number of SSIs following skin preparation with 10% aqueous PI paint alone compared with 2% chlorhexidine in 70% alcohol paint.
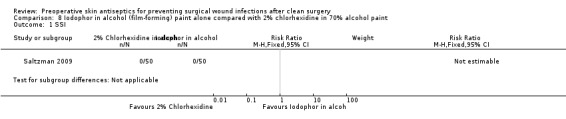
Comparison 8: Iodophor in alcohol (film‐forming) paint compared with 2% chlorhexidine in 70% alcohol paint (1 trial; 100 participants)
Saltzman 2009 was a three‐arm trial that randomised 150 participants all undergoing shoulder surgery and had 10 months follow‐up.
Primary outcome: SSI
Saltzman 2009: there were no reported SSI events in either group for this comparison: (0/50; 0%) reported for both study arms (Analysis 8.1).
8.1. Analysis.
Comparison 8 Iodophor in alcohol (film‐forming) paint alone compared with 2% chlorhexidine in 70% alcohol paint, Outcome 1 SSI.
Summary: Iodophor in alcohol (film‐forming) paint compared with 2% chlorhexidine in 70% alcohol paint
One small, underpowered, study judged to be at unclear risk of bias did not report any SSI events in post‐operative surgical wounds randomised to either Iodophor in alcohol compared with 2% chlorhexidine in 70% alcohol paint.
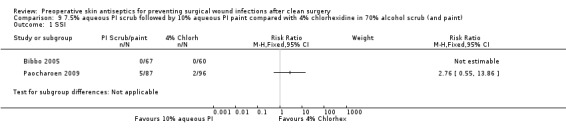
Comparison 9: 7.5% aqueous PI scrub/10% aqueous PI paint compared with 4% chlorhexidine in 70% alcohol scrub and paint (2 trials; 683 participants)
Two studies were included in this comparison (Bibbo 2005; Paocharoen 2009). Bibbo 2005 randomised 127 participants under‐going elective foot and ankle surgery: no duration of follow‐up was reported. Paocharoen 2009 randomised 500 participants undergoing a range of surgeries resulting in clean, clean‐contaminated and contaminated wounds. In total, 183 participants underwent clean surgery (as defined by the author) and the authors provided outcome data for this sub‐set of participants on request.
Primary outcome: SSI
Bibbo 2005: there were no reported SSI events in either group for this comparison: (0/67; 0%) in the scrub/paint arm and (0/60; 0%) in the chlorhexidine arm. Paocharoen 2009: there was no evidence of a difference in the number of SSIs in the PI paint group (5/87; 5.7%) compared with the 2% chlorhexidine group (2/96; 2.1%): RR 2.76, 95% CI 0.55 to 13.86 (Analysis 9.1).
9.1. Analysis.
Comparison 9 7.5% aqueous PI scrub followed by 10% aqueous PI paint compared with 4% chlorhexidine in 70% alcohol scrub (and paint), Outcome 1 SSI.
Summary: 7.5% aqueous PI scrub/10% aqueous PI paint compared with 4% chlorhexidine in 70% alcohol scrub and paint
Data from one study found no evidence of a difference in the number of SSIs following skin preparation with 7.5% aqueous PI scrub/10% aqueous PI paint compared with 4% chlorhexidine in 70% alcohol scrub and paint.
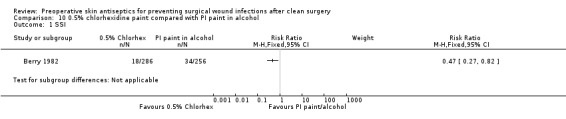
Comparison 10: 0.5% chlorhexidine in methylated spirit compared with PI paint (in alcohol) (1 trial; 542 participants)
Berry 1982 randomised 866 participants undergoing elective surgery, however, of these only 542 participants were undergoing clean surgery (results were presented separately for this group) and are considered here. These were those surgical procedures classed in the study as 'hernia, genitalia, veins' and other 'clean' operations. Duration of follow‐up was recorded to be until hospital discharge. The strength of PI paint used was not reported in this study.
Primary outcome: SSI
Berry 1982: there was a statistically significant difference in the number of SSIs in the chlorhexidine group (18/286; 6.3%) compared with the PI (in alcohol) paint treatment group (34/256; 13%): RR 0.47, 95% CI 0.27 to 0.82 (Analysis 10.1). Thus, over the duration of follow‐up there was a 53% reduction in the risk of getting an SSI in the chlorhexidine group compared to the PI (in alcohol) paint group. The 95% CI suggest that the true population reduction in risk of SSI from using 0.5% chlorhexidine (compared to PI paint in alcohol) is likely to lie somewhere between a 73% reduction in risk of SSI and an 18% reduction, with a 53% reduction being the best estimate based on the data we have.
10.1. Analysis.
Comparison 10 0.5% chlorhexidine paint compared with PI paint in alcohol, Outcome 1 SSI.
Summary: 0.5% chlorhexidine paint in methylated spirit compared with PI (in alcohol) paint
There is evidence from one study that suggests that clean wounds treated with 0.5% chlorhexidine in methylated spirits have a reduced risk of SSI compared with PI (in alcohol) treated wounds. However, it is important to note that the trial does not report important details regarding the interventions ‐ such as the concentration of PI paint used. The study was classed as being at low risk of bias for the randomisation sequence domain but unclear for allocation concealment and blinded outcome assessment.
5. Chlorhexidine compared with Chlorhexidine
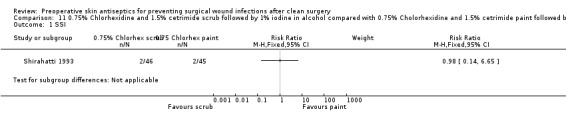
Comparison 11: 0.75% Cholorhexidine and 1.5% cetrimide scrub compared with 0.75% chlorhexidine and 1.5% cetrimide paint (1 trial; 91 participants)
Shirahatti 1993 randomised 135 participants undergoing a range of surgical procedures of which 91 were classed as clean by the trial authors. In both arms the scrub or paint was followed by an application of 1% iodine in 70% spirit. Duration of follow‐up was not reported.
Primary outcome: SSI
Shirahatti 1993: there was evidence of a difference in the number of SSIs in the chlorhexidine/cetrimide scrub group (2/46; 4.3%%) compared with the chlorhexidine/cetrimide paint group (2/45; 4.4%): RR 0.98, 95% CI 0.14 to 6.65 (Analysis 11.1).
11.1. Analysis.
Comparison 11 0.75% Chlorhexidine and 1.5% cetrimide scrub followed by 1% iodine in alcohol compared with 0.75% Cholorhexidine and 1.5% cetrimide paint followed by 1% iodine in 70% spirit, Outcome 1 SSI.
Summary: 0.75% Cholorhexidine and 1.5% cetrimide scrub compared with 0.75% chlorhexidine and 1.5% cetrimide paint
Data from one study found no evidence of a difference in the number of SSIs following skin preparation with 0.75% chlorhexidine and 1.5% cetrimide scrub compared with 0.75% chlorhexidine and 1.5% cetrimide.
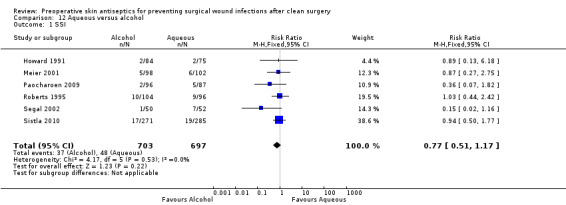
6. Alcoholic solutions compared with aqueous solutions (six trials; 1400 participants)
Six studies were included in this comparison, all having been included in at least one of the comparisons 1 to 11 above.
Meier 2001 compared soap in methylated spirit with aqueous PI. Howard 1991; Roberts 1995 and Segal 2002 compared iodophor in alcohol with aqueous PI. Sistla 2010 and Paocharoen 2009 compared chlorhexidine in 70% alcohol with aqueous PI.
Primary outcome: SSI
Study outcome data are as reported above for relevant comparisons. For this analysis data were pooled using a fixed effects meta‐analysis (I2 = 0%). Results showed evidence of a difference in number of SSIs following skin preparation with alcoholic solutions compared with aqueous solutions: RR 0.77, 95% CI 0.51 to 1.17 (Analysis 12.1).
12.1. Analysis.
Comparison 12 Aqueous versus alcohol, Outcome 1 SSI.
Summary: Alcoholic solutions compared with aqueous solutions
Data from six studies showed no statistically significant difference in the number of SSIs following skin preparation with alcoholic or aqueous solutions.
Mixed treatment comparison meta‐analysis
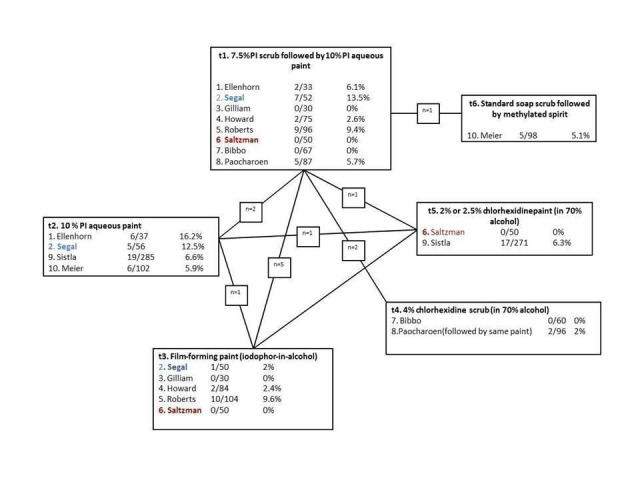
In total, ten of the included studies were formed into a mixed treatment comparison meta‐analysis ‐ Alexander 1985; Berry 1982; Shirahatti 1993 ‐ could not be linked into the network (Figure 3). A fixed effects model was found to be the be best fit and was employed ‐ results in the form of odds ratios (OR) are presented in Table 3. When considering all direct and indirect comparisons for available comparisons ‐ there was no statistically significant difference between any two interventions included in the network. It is important to note that the study with a significant finding reported above (Berry 1982) could not be included in the network as it did not form any link.
3.
Mixed treatment comparison meta‐analysis
3. Mixed Treatment comparison results (including summary of iGrade estimate quality ‐ high, moderate, low or very low).
|
Control |
|||||||
| Intervention |
Odds Ratios (95%CIs) |
7.5% PI Scrub/ 10% PI aqueous paint |
10% PI aqueous paint | Film‐forming paint |
4% Chlorhexidine scrub in 70% alcohol |
2% or 2.5% Chlorhexidine paint |
Soap scrub/followed by methylated spirits |
|
7.5% PI Scrub/10% PI aqueous paint |
|||||||
|
10% PI aqueous paint |
2.04 (0.73 to 5.64) VERY LOW |
||||||
|
Film‐forming paint |
0.73 (0.31 to 1.41) LOW |
0.43 (0.13 to 1.05) LOW |
|||||
| 4% Chlorhexidine scrub in 70% alcohol | 0.44 (0.04 to 1.63) LOW |
0.27 (0.02 to 1.13) LOW |
0.69 (0.05 to 2.84) VERY LOW |
||||
|
2% or 2.5% Chlorhexidine paint |
2.02 (0.53 to 5.48) VERY LOW |
0.99 (0.46 to 1.85) LOW |
3.08 (0.72 to 9.41) VERY LOW |
11.74 (0.74 to 58.29) VERY LOW |
|||
| Soap scrub/followed by methylated spirits | 2.16 (0.33 to 7.43) VERY LOW |
1.06 (0.23 to 2.95) VERY LOW |
3.30 (0.44 to 11.87) VERY LOW |
12.46 (0.49 to 65.95) VERY LOW |
1.20 (0.21 to 3.91) VERY LOW |
||
Effect estimates (the evidence) were judged as being at low or very low quality. This was driven by the unclear risk of bias for most studies and the imprecision due to the limited number and size of studies.
When considered in terms of probability of a treatment being the best (the most effective in preventing SSI), analysis suggested that 4% chlorhexidine scrub (in 70% alcohol) has a 78% probability of being the best treatment in terms of preventing SSI, followed by iodophor in alcohol with a 16% probability of being the best and standard soap scrub followed by methylated spirit with 4% probability of being the best. We note that all the treatments that were estimated as having the highest probability of being effective were all alcohol‐containing products (Table 4). Again it is important to note the low quality of this evidence.
4. Probability of treatment being the best in terms of preventing SSI.
| Treatment | % being the best in terms of preventing SSI |
| 4% Chlorhexidine scrub (in 70% alcohol) | 78% |
| Film‐forming paint (iodophor in alcohol) | 16% |
| Standard soap scrub followed by Methylated spirit | 4% |
| 2% or 2.5% Chlorhexidine paint (in 70% alcohol) | 1% |
| 7.5% PI scrub followed by 10% PI aqueous paint | 0.8% |
| 10 % PI aqueous paint | 0.2% |
Discussion
Summary of main results
We included thirteen studies involving a total of 2,623 participants in this review. We did not find any studies that compared skin antisepsis with no skin antisepsis. A large number of different skin cleansing products were evaluated across these 13 trials resulting in 11 comparisons. It is unclear whether the array of products used reflects changes in practice over time or differing practice at local, national or international levels.
One study, classed as being at unclear risk of bias, demonstrated a significant reduction in rates of SSI when skin was prepared with 0.5% chlorhexidine in methylated spirit compared with povidone iodine (in alcohol) paint (Berry 1982). Further interpretation of this study data was limited by the lack of detailed description of the interventions evaluated i.e. the concentration of povidone iodine. However, the study does suggest that a chlorhexidine‐containing treatment solution was more effective than alcohol‐based povidone iodine paint. No other comparisons yielded statistically significant differences.
Ten out of thirteen studies were linked in a mixed treatment comparison meta‐analysis ‐ Alexander 1985; Berry 1982 and Shirahatti 1993 could not be linked to the network. This analysis suggested that 4% chlorhexidine scrub (in 70% alcohol) had the highest probability of being effective and that overall alcohol‐based solutions had the higher probabilities of being effective than aqueous‐based solutions.
Quality of the evidence
Whilst only one study demonstrated a statistically significant difference in the rate of SSI between antiseptics, it is important to note that many studies randomised relatively small numbers of participants and therefore had low statistical power to detect a difference even if it existed. Indeed it is notable that of the 13 included studies three (23%) reported no SSI outcomes in either arm and thus contribute no outcome data to the analysis. The universally limited quality of the studies also impacts on the quality of, and thus confidence in, the effect estimates derived from the mixed treatment comparison meta‐analysis.
Agreements and disagreements with other studies or reviews
There has been some suggestion in the literature that perhaps the 'active ingredient' of skin antiseptics is the alcohol solution as it has antimicrobial properties (Kamel 2012; Maiwald 2012; Maiwald 2014). Whilst not significant, our comparison of trials comparing alcohol‐based vs. aqueous based solutions showed an potentially interesting signal towards alcohol which was also observed in the mixed treatment comparison meta‐analysis findings ‐ however, no firm conclusions can be drawn based on the current evidence in this area.
Authors' conclusions
Implications for practice.
A comprehensive review of current evidence found evidence from a single study that preoperative skin preparation with 0.5% chlorhexidine solution in methylated spirits was more effective in preventing SSIs following clean surgery than alcohol‐based povidone iodine paint. However poor reporting of this trial makes this finding difficult to act upon. Practitioners may therefore elect to consider other characteristics such as costs and potential side effects when choosing between alternatives.
Implications for research.
There are 13 RCTs included in this review presenting data from over 2,000 participants who have agreed to contribute data for clinical research. However, the range of antiseptics evaluated (resulting in the 11 different study‐related comparisons), the sometimes limited description of interventions and the relative small sample sizes of the trials make the evidence difficult to interpret and have confidence in. Yet, whilst relatively rare, SSIs following clean surgery are an important issue given the large number of people undergoing surgery annually world‐wide.
Given the large number of treatment options, the design of future trials should be driven by the questions of high priority to decision makers. It may be that investment in at least one large trial (in terms of participants) is warranted in order to add definitive and hopefully conclusive data to the current evidence base. Ideally any future trial would evaluate the iodine‐containing and chlorhexidine‐containing solutions relevant to current practice as well as the type of solution used (alcohol vs. aqueous). Finally, current trials report very limited data on secondary outcomes. Outcomes such as adverse events and resource use may have an important role in influencing decision making regarding the use of different pre‐operative skin cleaning products and thus should be assessed.
What's new
| Date | Event | Description |
|---|---|---|
| 2 March 2015 | New search has been performed | Third update. New search, two additional studies were excluded (Becerro de Bengoa 2013; Lee 2013). |
| 2 March 2015 | New citation required but conclusions have not changed | No change to conclusions. Edited the use of term no statistically significant difference in the results to terms like no evidence of a difference which are more appropriate. Slight edit of 'Agreements and disagreements with other studies or reviews' section in light of author feedback. |
History
Protocol first published: Issue 1, 2003 Review first published: Issue 1, 2004
| Date | Event | Description |
|---|---|---|
| 7 August 2012 | New citation required and conclusions have changed | Three new included studies added to review (Paocharoen 2009; Saltzman 2009; Sistla 2010). Five trials previously excluded were included in this update (Bibbo 2005; Gilliam 1990; Howard 1991; Meier 2001; Shirahatti 1993). Two trials (Dewan 1987; Lorenz 1988) previously included were excluded in this update. Mixed treatment comparison meta‐analysis included. |
| 7 August 2012 | New search has been performed | Second update, new search. Two authors joined the team. |
| 1 July 2008 | New search has been performed | This review was originally published in the Cochrane library in 2004. For this first update, new searches were carried out in July 2008, 1 new study was included. The reviewers' conclusions remain unchanged |
| 16 April 2008 | Amended | Converted to new review format. |
| 22 April 2004 | New citation required and conclusions have changed | Publication of review, Issue 3 2004. |
Acknowledgements
Review authors thank Pedro Saramago for his advice regarding the conduct of the mixed treatment comparison meta‐analysis.
Review authors (original review) would like to acknowledge the support of their employers (Peggy Edwards ‐ Welsh Risk Pool; Allyson Lipp ‐ University of Glamorgan; Alex Holmes ‐ University of Glamorgan).
The review authors would like to thank the following people: Wounds Group Editors (David Margolis, Andrea Nelson) and Peer Referees (Vickie Arrowsmith, Anne‐Marie Bagnall, Chris Booth, Anne Humphreys, Judith Tanner and Vicky Whittaker). In addition thanks to Elizabeth Royle who copy‐edited the review update and we would also like to thank the support of the editorial base of the Wounds Group.
Appendices
Appendix 1. Databases searched and CENTRAL search strategy
The following search strategy was used in the Cochrane Central Register of Controlled Trials (CENTRAL):
#1 MeSH descriptor Skin explode all trees #2 MeSH descriptor Antisepsis explode all trees #3 (#1 AND #2) #4 "skin antisepsis" #5 MeSH descriptor Anti‐Infective Agents, Local explode all trees #6 MeSH descriptor Iodine explode all trees #7 MeSH descriptor Iodophors explode all trees #8 MeSH descriptor Povidone‐Iodine explode all trees #9 MeSH descriptor Chlorhexidine explode all trees #10 MeSH descriptor Alcohols explode all trees #11 iodophor* or povidone‐iodine or betadine or chlorhexidine or alcohol or alcohols or antiseptic* #12 MeSH descriptor Detergents explode all trees #13 (#1 AND #12) #14 skin NEAR detergent* #15 MeSH descriptor Disinfectants explode all trees #16 (#1 AND #15) #17 skin NEAR disinfect* #18 (#3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #13 OR #14 OR #16 OR #17) #19 MeSH descriptor Surgical Wound Infection explode all trees #20 (surgical NEAR/5 infection):ti,kw,ab #21(surgical NEAR/5 wound*):ti,ab,kw #22 ((post‐operative or postoperative) NEAR (wound NEXT infection*)):ti,ab,kw #23 MeSH descriptor Preoperative Care explode all trees #24 (preoperative or pre‐operative):ti,ab,kw #25 (#19 OR #20 OR #21 OR #22 OR #23 OR #24) #26(#18 AND #25)
The Ovid MEDLINE search strategy can be viewed in Appendix 2 and was adapted as appropriate for the EMBASE and CINAHL searches. The MEDLINE search was combined with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐ and precision‐maximizing version (2008 revision); Ovid format. The EMBASE and CINAHL searches were combined with the trial filters developed by the Scottish Intercollegiate Guidelines Network.
The authors also searched web based resources in January 2008: Guideline Finder Specialist Library, Research Findings Register, Centre for Reviews and Dissemination web site, National Electronic Library for Health (Surgery, Theatres and Anaesthetic Specialist Library).
In addition we also searched the bibliographies of all retrieved and relevant publications identified by these strategies for further studies. We placed no specific date restriction upon study inclusion. We also contacted manufacturers and distributors of antiseptic agents as well as professional organisations, for example Association for Perioperative Practice, AORN, Royal College of Surgeons of England, and The Association of Operating Department Practitioners, for details of unpublished and ongoing studies. We did not restrict the search by language or publication status.
Appendix 2. Ovid MEDLINE search strategy
1 exp Skin/ 2 exp Antisepsis/ 3 and/1‐2 4 skin antisepsis.mp. 5 exp Anti‐Infective Agents, Local/ 6 exp Iodine/ 7 exp Iodophors/ 8 exp Povidone‐Iodine/ 9 exp Chlorhexidine/ 10 exp Alcohols/ 11 (iodophor$ or povidone‐iodine or betadine or chlorhexidine or alcohol or alcohols or antiseptic$).mp. 12 exp Detergents/ 13 1 and 12 14 (skin adj5 detergent$).mp. 15 exp Disinfectants/ 16 1 and 15 17 (skin adj5 disinfect$).mp. 18 or/3‐11,13‐14,16‐17 19 exp Surgical Wound Infection/ 20 exp Surgical Wound Dehiscence/ 21 (surgical adj5 infection).mp. 22 (surgical adj5 wound$).mp. 23 ((post‐operative or postoperative) adj wound infection$).mp. 24 exp Preoperative Care/ 25 (preoperative or pre‐operative).mp. 26 or/19‐25 27 18 and 26
Appendix 3. Ovid EMBASE search strategy
1 exp Skin/ 2 exp Antisepsis/ 3 and/1‐2 4 skin antisepsis.mp. 5 exp Topical Antiinfective Agent/ 6 exp Iodine/ 7 exp Iodophors/ 8 exp Povidone‐Iodine/ 9 exp Chlorhexidine/ 10 exp Alcohols/ 11 (iodophor$ or povidone‐iodine or betadine or chlorhexidine or alcohol or alcohols or antiseptic$).mp. 12 exp Detergents/ 13 1 and 12 14 (skin adj5 detergent$).mp. 15 exp Disinfectants/ 16 1 and 15 17 (skin adj5 disinfect$).mp. 18 or/3‐11,13‐14,16‐17 19 exp Surgical Infection/ 20 exp Surgical Wound Dehiscence/ 21 (surgical adj5 infection).mp. 22 (surgical adj5 wound$).mp. 23 ((post‐operative or postoperative) adj wound infection$).mp. 24 exp Preoperative Care/ 25 (preoperative or pre‐operative).mp. 26 or/19‐25 27 18 and 26
Appendix 4. EBSCO CINAHL search strategy
S26 S16 and S25 S25 S17 or S18 or S19 or S20 or S21 or S22 or S23 or S24 S24 TI ( preoperative or pre‐operative ) or AB ( preoperative or pre‐operative ) S23 (MH "Preoperative Care+") S22 TI post‐operative wound infection* or AB post‐operative wound infection* S21 TI postoperative wound infection* or AB postoperative wound infection* S20 TI surgical N5 wound* or AB surgical N5 wound* S19 TI surgical N5 infection* or AB surgical N5 infection* S18 (MH "Surgical Wound Dehiscence") S17 (MH "Surgical Wound Infection") S16 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S11 or S12 or S14 or S15 S15 TI skin N5 disinfect* or AB skin N5 disinfect* S14 S10 and S13 S13 (MH "Disinfectants") S12 TI skin N5 detergent* or AB skin N5 detergent* S11 S9 and S10 S10 (MH "Skin+") S9 (MH "Detergents+") S8 TI ( iodophor* or povidone‐iodine or betadine or chlorhexidine or triclosan or hexachlorophene or benzalkonium or alcohol or alcohols or antiseptic* ) or AB ( iodophor* or povidone‐iodine or betadine or chlorhexidine or triclosan or hexachlorophene or benzalkonium or alcohol or alcohols or antiseptic* ) S7 (MH "Alcohols+") S6 (MH "Chlorhexidine") S5 (MH "Alcohols") S4 (MH "Povidone‐Iodine") S3 (MH "Iodine") S2 (MH "Antiinfective Agents, Local+") S1 TI skin antisepsis or AB skin antisepsis
Appendix 5. Risk of bias definitions
1. Was the allocation sequence randomly generated?
Low risk of bias
The investigators describe a random component in the sequence generation process such as: referring to a random number table; using a computer random number generator; coin tossing; shuffling cards or envelopes; throwing dice; drawing of lots.
High risk of bias
The investigators describe a non‐random component in the sequence generation process. Usually, the description would involve some systematic, non‐random approach, for example: sequence generated by odd or even date of birth; sequence generated by some rule based on date (or day) of admission; sequence generated by some rule based on hospital or clinic record number.
Unclear
Insufficient information about the sequence generation process to permit judgement of either Yes or No (as above) to be made.
2. Was the treatment allocation adequately concealed?
Low risk of bias
Participants and investigators enrolling participants could not foresee assignment either because one of the following, or an equivalent method, was used to conceal allocation: central allocation (including telephone, web‐based and pharmacy‐controlled randomisation); sequentially‐numbered drug containers of identical appearance; sequentially‐numbered, opaque, sealed envelopes.
High risk of bias
Participants or investigators enrolling participants could possibly foresee assignments and thus introduce selection bias, i.e. when allocation used: an open random allocation schedule (e.g. a list of random numbers); assignment envelopes without appropriate safeguards (e.g. if envelopes were unsealed or nonopaque or not sequentially numbered); alternation or rotation; date of birth; case record number; any other explicitly unconcealed procedure.
Unclear
Insufficient information to permit judgement of either Yes or No to be made. This is usually the case if the method of concealment is not described, or is not described in sufficient detail to allow a definite judgement, for example if the use of assignment envelopes is described, but it remains unclear whether envelopes were sequentially numbered, opaque and sealed.
3. Blinding: was knowledge of the allocated interventions adequately prevented during the study?
Low risk of bias
Any one of the following:
No blinding, but the review authors judge that the outcome and the outcome measurement are not likely to be influenced by lack of blinding.
Blinding of participants and key study personnel ensured, and unlikely that the blinding could have been broken.
Either participants or some key study personnel were not blinded, but outcome assessment was blinded and the non‐blinding of others unlikely to introduce bias.
High risk of bias
Any one of the following:
No blinding or incomplete blinding, and the outcome or outcome measurement is likely to be influenced by lack of blinding.
Blinding of key study participants and personnel attempted, but likely that the blinding could have been broken.
Either participants or some key study personnel were not blinded, and the non‐blinding of others likely to introduce bias.
Unclear
Any one of the following:
Insufficient information to permit judgement of Yes or No to be made.
The study did not address this outcome.
4. Were incomplete outcome data adequately addressed?
Low risk of bias
Any one of the following:
No missing outcome data.
Reasons for missing outcome data unlikely to be related to true outcome (for survival data, censoring unlikely to be introducing bias).
Missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups.
For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically relevant impact on the intervention effect estimate.
For continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes not enough to have a clinically relevant impact on observed effect size.
Missing data have been imputed using appropriate methods.
High risk of bias
Any one of the following:
Reason for missing outcome data likely to be related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups.
For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk enough to induce clinically relevant bias in intervention effect estimate.
For continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes enough to induce clinically relevant bias in observed effect size.
As‐treated analysis done with substantial departure of the intervention received from that assigned at randomisation.
Potentially inappropriate application of simple imputation.
Unclear
Any one of the following:
Insufficient reporting of attrition/exclusions to permit judgement of Yes or No (e.g. number randomised not stated, no reasons for missing data provided).
The study did not address this outcome.
5. Are reports of the study free of suggestion of selective outcome reporting?
Low risk of bias
Any of the following:
The study protocol is available and all of the pre‐specified (primary and secondary) outcomes that are of interest in the review have been reported in the pre‐specified way.
The study protocol is not available but it is clear that the published reports include all expected outcomes, including those that were pre‐specified (convincing text of this nature may be uncommon).
High risk of bias
Any one of the following:
Not all of the study's pre‐specified primary outcomes reported.
One or more primary outcomes is reported using measurements, analysis methods or subsets of the data (e.g. subscales) that were not pre‐specified.
One or more reported primary outcomes were not pre‐specified (unless clear justification for their reporting is provided, such as an unexpected adverse effect).
One or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis.
The study report fails to include results for a key outcome that would be expected to have been reported for such a study.
Unclear
Insufficient information to permit judgement of Yes or No to be made. It is likely that the majority of studies will fall into this category.
6. Other sources of potential bias:
Low risk of bias
The study appears to be free of other sources of bias.
High risk of bias
There is at least one important risk of bias. For example, the study:
Had a potential source of bias related to the specific study design used; or
Stopped early due to some data‐dependent process (including a formal‐stopping rule); or
Had extreme baseline imbalance; or
Has been claimed to have been fraudulent; or
Had some other problem.
Unclear
There may be a risk of bias, but there is either:
Insufficient information to assess whether an important risk of bias exists; or
Insufficient rationale or evidence that an identified problem will introduce bias.
Appendix 6. Igrade: Quality assessments of mixed treatment comparison estimates using iGRADE: comparison with the GRADE tool.
| GRADE CATEGORY | GRADE Definition and guidance | iGRADE CATEGORY | iGRADE Definitions and guidance | iGRADE ISSUES |
| Limitations in design |
Risk of Bias ‐If you think any limitations were negligible choose no ‐If you think there were serious limitations choose serious ‐If you think there were very serious limitations choose very serious |
Limitations in design |
Use GRADE limitations in design rating for DIRECT links to assess the mixed treatment comparison meta‐analysis estimates these links clearly contributed to. No: GRADE limitations in design category recorded as ‘no’ for all links identified as informing the mixed treatment comparison meta‐analysis estimate. Serious: GRADElimitations in design category recorded as serious for one or more links identified as informing the mixed treatment comparison meta‐analysis estimate, but none identified as very serious. Very serious: GRADElimitations in design category recorded as very serious for one or more links identified as informing the mixed treatment comparison meta‐analysis estimate. |
Qualitative assessment of risk of bias difficult for indirect evidence. When direct and indirect evidence are available, this assessment may be subjective. |
| Inconsistency |
Unexplained heterogeneity of results ‐If you think any inconsistency was negligible choose no ‐If you think there was serious inconsistency choose serious ‐If you think there was very serious inconsistency choose very serious |
Sensitivity of results |
Judgement based on the impact of sensitivity analysis on the mixed treatment meta‐analysis and thus estimates (e.g. removing each trial where there are two or more informing a link, or sensitivity to alternative priors in random effect analysis) No: No or small change in estimate and intervals Serious: Some notable change in estimate and intervals Very serious: Large change in estimate and intervals |
Does not address unexplained heterogeneity per se |
| Indirectness |
Indirect comparison ‐If you think the evidence is direct choose no ‐If you have serious doubts about directness choose serious ‐If you have very serious doubts about directness choose very serious |
Indirectness/Inconsistency Within GRADE the term inconsistency is used to refer to unexplained heterogeneity. Within mixed treatment comparison meta‐analysis inconsistency has meaning specific to agreement between direct and indirect data. Furthermore, in GRADE the presence of indirectness is taken as a reason to downgrade evidence – however in the context of an mixed treatment comparison meta‐analysis where indirect data is expected and ideally adds value such an approach does not make sense. Thus we merged these categories resulting in joint assessment of unexplained heterogeneity and/or assessment of inconsistency where possible. |
Define the type of data available for each mixed treatment comparison meta‐analysiscomparison as follows: 1. Direct or indirect only: No heterogeneity 2. Direct, indirect or mixed (direct and indirect): heterogeneity 3. Mixed:No heterogeneity: statistical inconsistencies 4. Mixed: No heterogeneity; No statistical inconsistencies No: 1 and 4 Serious: 2, 3 Very serious: n/a |
Assessment of heterogeneity based on INDIRECT links is challenging Cannot always assess for inconsistencies |
| Imprecision |
CIs around estimates of treatment effect ‐If you think the results were precise choose no ‐If there was serious imprecision choose serious ‐If there was very serious imprecision choose very serious |
Imprecision | Judged by the size of CIs around ORs. As ORs were used to analyse data with relative high number of events a more conservative interval width used than would have been employed were data presented using risk ratios. No: uncertainty judged to be reasonable (upper interval < 2·5) Serious: judged to be inadequate (upper interval > 2·5<5) Very serious: (upper interval > 5) |
|
|
Publication bias |
‐If you think there is no evidence of publication bias choose unlikely ‐If there is high probability of publication bias choose likely ‐If there is very high probability of publication bias choose very likely |
Publication bias |
Use GRADE limitations in design rating for DIRECT links to assess the mixed treatment comparison meta‐analysisestimates these links clearly contributed to. Unlikely: GRADE publication bias category recorded as unlikely for links identified as informing the mixed treatment comparison meta‐analysis estimate. Likely: GRADE publication bias category recorded as likely for one or more links identified as informing the mixed treatment comparison meta‐analysis estimate and none identified as very likely. Very likely: for GRADE publication bias category recorded as very likely for one or more link identified as informing the mixed treatment comparison meta‐analysis estimate. |
Qualitative assessment of publication bias difficult for indirect evidence Again, in the presence of both direct and indirect evidence there is the need to consider potential publication bias in the indirect links as well as the direct links informing the same comparison. Yet, outlined in the discussion of limitations, assessing potential bias in indirect comparison is complex. If, for example, AC is biased (missing studies) favouring A and BC is biased (missing studies) favouring B, then the AB indirect estimate will be unbiased if the bias in AC is similar to the bias in BC. |
Data and analyses
Comparison 1. 2% iodine in 90% alcohol compared with 70% alcohol.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 2. PI paint compared with soap (shop bought) scrub and application of methylated spirit.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 3. 7.5% aqueous PI scrub followed by 10% aqueous PI paint compared with 10% aqueous PI paint alone.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 2 | 178 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.34, 1.69] |
Comparison 4. 7.5% aqueous PI scrub followed by 10% aqueous PI paint compared with iodophor in alcohol (film‐forming) paint.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 5 | 621 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.47 [0.73, 2.94] |
Comparison 5. 10% aqueous PI paint alone compared with iodophor in alcohol (film‐forming) paint.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 6. 7.5% aqueous PI scrub followed by 10% aqueous PI paint compared with 2% chlorhexidine in 70% alcohol paint.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 7. 10% aqueous PI paint alone compared with 2% chlorhexidine in 70% alcohol paint.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 8. Iodophor in alcohol (film‐forming) paint alone compared with 2% chlorhexidine in 70% alcohol paint.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 9. 7.5% aqueous PI scrub followed by 10% aqueous PI paint compared with 4% chlorhexidine in 70% alcohol scrub (and paint).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 10. 0.5% chlorhexidine paint compared with PI paint in alcohol.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 11. 0.75% Chlorhexidine and 1.5% cetrimide scrub followed by 1% iodine in alcohol compared with 0.75% Cholorhexidine and 1.5% cetrimide paint followed by 1% iodine in 70% spirit.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 12. Aqueous versus alcohol.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SSI | 6 | 1400 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.51, 1.17] |
Comparison 13. Trial data.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Trial data | Other data | No numeric data |
13.1. Analysis.
Comparison 13 Trial data, Outcome 1 Trial data.
| Trial data | |||
|---|---|---|---|
| Study | Groups | Number/timing of applications (n.b. assumed one application unless stated) | Primary outcome SSI: |
| Alexander 1985 | Group A: 2% iodine in 90% alcohol (1‐minute scrub) and polyester antimicrobial incise drape (n=81) Group B 70% alcohol (1‐minute scrub) and polyester antimicrobial incise drape (n=76) | Group A: One application Group B: One application |
Group A: 1/81 Group B: 1/76 |
| Berry 1982 | Group A: 0.5% Chlorhexidine in methylated spirit (Hibitane). (n=286) Group B: 10% PI (in alcohol) paint (n=256) | Group A: Two applications Group B: Two applications |
At time of discharge Group A: 18/286 Group B: 34/256 3 to 4 days post‐operation (if not discharged before this point) Group A: 15/222 Group B: 22/200 |
| Bibbo 2005 | Group A: 7.5% PI scrub (7‐minutes) followed by 10% aqueous PI paint (n=67) Group B: 4% Chlorhexidine scrub (7‐minute) in 70% isopropyl alcohol (n=60) |
Group A: 7‐minute scrub then one application Group B: 7‐minute scrub then one application |
Group A: 0/67 Group B: 0/60 |
| Ellenhorn 2005 | Group A: 0.75% PI soap scrub (5‐minute) followed by 1% (available iodine) aqueous PI paint (n=33)* Group B: 1% aqueous PI paint (n=37) *10% PI and 1% PI treated as same solution since it is 10% PI solution with 1% free iodine and thus has been reported inconsistently between trials. Likewise 0.75% and 7.5% assumed to be same treatment described differently. |
Group A: 5‐minute scrub then one application Group B:One application |
Group A: 2/33 Group B: 6/37 |
| Gilliam 1990 | Group A: Aqueous iodophor scrub (5‐minute) followed by iodophor paint (n=30) Group B: Iodophor‐in‐alcohol solution (n=30) |
Group A: 5‐minute scrub then one application Group B: One application |
Group A: 0/30 Group B: 0/30 |
| Howard 1991 | Group A: Aqueous iodophor scrub (10‐minute) followed by iodophor paint (n=75) Group B: Iodophor‐in‐alcohol, film‐forming, water insoluble antiseptic (n=84) |
Group A: 10‐minute scrub then one application Group B: One application |
Group A: 2/75 Group B: 2/84 |
| Meier 2001 | Group A: PI paint (n=102) Group B: Standard (shop‐brought) soap scrub (5 minute) followed by methylated spirit (n=98) |
Group A: 5 minute scrub then one application Group B: One application |
Group A: 6/102 Group B: 5/98 |
| Paocharoen 2009 | Group A: PI scrub (5‐minute) followed by aqueous PI paint (n=87). Group B: 4% chlorhexidine in 70% isopropyl alcohol scrub (5 minute) (Hibitane) followed by Hibitane paint (n=96). |
Group A:5 minute scrub then one application Group B:5 minute scrub then one application |
Group A: 5/87 Group B: 2/96 |
| Roberts 1995 | Group A: Aqueous iodophor scrub (5‐10 minutes) followed by iodophor paint (n=96). Group B: Iodophor‐in‐alcohol, film‐forming, water insoluble antiseptic (DuraPrep Surgical Soltion, 3M) St Paul, Minn) (n=104) |
Group A: 5‐10 minute scrub then one application Group B:One application |
Group A: 9/96 Group B: 10/104 |
| Saltzman 2009 | Group A: 0.75% PI scrub followed by 1% PI paint (n= 50)* Group B: 2% chlorhexidine gluconate and 70% alcohol (n= 50) Group C: Iodophor‐in‐alcohol film‐forming antiseptic (n= 50) *10% PI and 1% PI treated as same solution since it is 10% PI solution with 1% free iodine and thus has been reported inconsistently between trials. Likewise 0.75% and 7.5% assumed to be same treatment described differently. |
Group A: Scrub (timing not reported). One application Group B:One application Group C:One application |
Group A: 0/50 Group B: 0/50 Group C: 0/50 |
| Segal 2002 | Group A: PI scrub (5‐minute) followed by PI aqueous paint (n=52) Group B: Aqueous 10% PI paint (n=56) Group C: Iodophor‐in‐alcohol film‐forming antiseptic (50) |
Group A:5 minute scrub then one application Group B:One application Group C:One application |
Group A: 7/52 Group B: 7/56 Group C: 1/50 |
| Shirahatti 1993 | Group A: 10‐minute scrub with 0.75% chlorhexidine and 1.5% cetrimide followed by 1% iodine in 70% spirit (n=46) Group B: 0.75% Chlorhexidine and 1.5% cetrimide followed by 1% iodine in 70% spirit (both paint) (n= 45) |
Group A: 10‐minute scrub then one application Group B: One application of each |
Group A: 2/46 Group B: 2/45 |
| Sistla 2010 | Group A: 10% PI aqueous paint (N=285). Group B: 2.5% chlorhexidine with 70% ethanol (n=271). |
Group A:One application Group B:One application |
Group A: 19/285* Group B: 17/271* *missing denominator data in these group ‐ this analysis assumed that those missing did not have the event of interest i.e. included in the denominator but not the numerator. |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Alexander 1985.
| Methods | 3‐arm RCT; undertaken in the USA. | |
| Participants | 480 patients undergoing elective surgery. Of these 480 participants only 234 were undergoing clean surgery (results reported separately) and are considered here. Inclusion: ability to apply incise drape and informed consent. Exclusion: allergy to iodine, dirty wounds and areas difficult to drape (perineum, genitalia, feet, upper extremities, head and neck). | |
| Interventions | Group A: 1‐minute scrub 2% iodine in 90% alcohol and polyester antimicrobial incise drape (n=81).
Group B: 1‐minute scrub 70% alcohol and polyester antimicrobial incise drape (n=76).
Group C:10‐minute scrub Betadine soap, two applications Betadine paint and no incise drape (n=77) (not considered further). Stated that all participants received a Phisohex scrub to the operative area the night before the surgery. |
|
| Outcomes | Primary outcome: SSI defined as discharge of pus, with or without positive culture. | |
| Notes | Trial data: Analysis 13.1 The published paper incorporated three separate studies, only one of which could be used within the review. In turn this study contained three‐arms, however only two groups (Groups A and B) had a skin preparation treatment as the only systematic difference between groups. The third group (Group C) used a different skin preparation treatment AND no drape. Length of follow‐up: one month. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomisation was carried out by drawing a card from a sealed envelope" Unclear if and how cards/envelopes were 'put' into a random sequence. Further information on this particular method is required to make a clear judgement. |
| Allocation concealment (selection bias) | Unclear risk | "randomisation was carried out by drawing a card from a sealed envelope" No detail about who randomised participants and whether other features were used to protect against the introduction of bias ‐ e.g. envelopes being numbered and opaque. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not discussed. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "Eight were unavailable for follow up after hospital discharge and four participants died". Total of 5%. |
Berry 1982.
| Methods | 2‐arm RCT; undertaken in the UK. | |
| Participants | 866 participants undergoing elective surgery. Of these 866 participants only 542 were undergoing clean surgery (results presented separately) and are considered here. These were those surgeries classed in the study as 'hernia, genitalia, veins' and other 'clean' operations. Inclusion: all elective cases. Exclusion: sensitivity to solutions. |
|
| Interventions | Group A: Two applications of 0.5% chlorhexidine in methylated spirit (Hibitane) (n=286).
Group B: Two applications of 10% PI (alcohol) paint (n=256). Skin shaving was routinely performed on hairy skin 18 to 24 hours prior to surgery. For each group the allocated intervention was used for both skin preparation of the participant and was also used for surgical scrub (7.5% PI or 0.5% chlorhexidine in methylated spirit (Hibitane)). |
|
| Outcomes | Primary outcome: SSI defined as presence of a wound abnormality: erythematous, oedematous, discharging or purulent. It is not clear whether this assessment also included significant bacterial growth . | |
| Notes | Trial data: Analysis 13.1 The wound healing data extracted from this report was for wound infection assessed on day of discharge and agreed by two assessors. Data were presented for assessment at 3 to 4 days after operation, again agreed by two assessors. The study also presented number of wound abnormalities but these data were not extracted. It was not clear how an abnormal wound differed from an infected wound and these data were not presented for clean surgical cases alone. Length of follow‐up: Until hospital discharge. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "the regime to be used in each successive (operating) session (allocated from a table of random numbers) was recorded on a card and each card was put in a sealed envelope. The sequence of randomisation was known to only one of us (MG)". |
| Allocation concealment (selection bias) | Unclear risk | 'the regime to be used for the operating theatre session was determined by means of drawing a card from a sealed envelope prior to the start of the operating list." No detail about who randomised participants and whether other features were used to protect against the introduction of bias ‐ e.g. envelopes being numbered and opaque. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "When possible the wound was assessed by a member of staff who had no knowledge of the regimen used although, on occasion, wounds had to be assessed by staff who were present during the operating session." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants included in analysis. |
Bibbo 2005.
| Methods | 2‐arm RCT; Undertaken in USA. | |
| Participants | 127 participants undergoing clean, elective foot and ankle surgery. Inclusion: Elective clean foot and ankle surgery. Exclusion:Patients with open wounds, skin ulcers and/or sores, an active acute or chronic infection or on active anti microbial therapy. |
|
| Interventions | Group A: 7‐minute scrub with 7.5% PI scrub followed by application of 10% aqueous PI paint (n=67). Group B: 7‐minute scrub with 4% Chlorhexidine in 70% isopropyl alcohol (n=60). Participants followed their usual personal hygiene routine on the day of surgery. Each extremity was allowed to dry after the skin preparation. |
|
| Outcomes | Primary outcome: SSI not defined. | |
| Notes | Trial data: Analysis 13.1 Length of follow‐up: Not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Whilst described as a prospective randomised study there is no description of how patients were randomised. |
| Allocation concealment (selection bias) | Unclear risk | No method of allocation concealment is reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported. |
Ellenhorn 2005.
| Methods | 2‐arm RCT; undertaken in the USA. | |
| Participants | 234 oncology patients having elective abdominal procedures. Of these 234 participants only 70 were undergoing clean surgery (as defined by authors ‐ no further details) and are considered here using outcome data supplied from authors on request. Inclusion: elective abdominal procedures with informed consent. Exclusion: active infection, neutropenia, skin reaction to iodine or the anticipated use of a prosthetic. | |
| Interventions | Group A: 5‐minute scrub with 0.75% (available iodine) PI soap followed by application of 1% (available iodine) aqueous PI paint (n=33). Group B: Application of 1% (available iodine) aqueous PI paint (n=37). All participants had all gross foreign material removed from the skin using a dry sponge and tape remover, if necessary. A razor was used to remove hair from the operative site. |
|
| Outcomes | Primary outcome: SSI defined by clinical criteria as presence of wound erythema or purulence requiring intervention within the first 30 days after the surgical procedure. | |
| Notes | Trial data: Analysis 13.1 The study authors provided data concerning the infection rates for clean surgery. Review author note: Study authors have analysed as an equivalency trial and employed a one‐sided analysis ‐ however analyses in this review were two‐sided. Length of follow‐up: 30 days. 10% PI and 1% PI treated as same solution since it is 10% solution of PI with 1% free iodine and thus has been reported inconsistently between trials. Likewise 0.75% and 7.5% assumed to be same treatment described differently. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomised in blocks with equal allocation to the two preoperative preparation arms". No description about the method used for randomising in blocks is provided. |
| Allocation concealment (selection bias) | Unclear risk | Randomisation occurred immediately prior to preoperative preparation. No details were provided about who performed this. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information reported regarding blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ‘Randomisation slots were not reused, which resulted in a slight imbalance between the two arms from ineligible patients or patients who withdrew consent’. Not clear from study how many patients undergoing clean surgery withdrew consent. |
Gilliam 1990.
| Methods | 2 arm RCT: undertaken in USA. | |
| Participants | 60 participants undergoing clean total joint surgery. No other information. | |
| Interventions | Group A: 5‐minute aqueous iodophor scrub followed by application of iodophor paint (n=30). Group B: Water insoluble iodophor‐in‐alcohol solution (0.7% iodophor and 74% isopropyl alcohol) (Duraprep, 3M Healthcare) (n = 30). All hair was removed by dry shave just prior to preparing the skin. In both groups non antimicrobial plastic incise drape used. All participants showered before with a chlorhexidine gluconate soap. |
|
| Outcomes | Primary outcome: SSI not defined. | |
| Notes | Trial data: Analysis 13.1 Length of follow‐up: Not reported. Group A: assumed to be 7.5% PI scrub and 10% PI paint (not confirmed by author). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Whilst the study notes that patients were 'randomly' divided there is no further description of how patients were randomised. |
| Allocation concealment (selection bias) | Unclear risk | No method of allocation concealment is reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported. |
Howard 1991.
| Methods | 2 arm RCT: undertaken in USA. | |
| Participants | 240 general surgery patients. Of these 240 participants an unknown number received clean surgery. Data are reported for 159 participants undergoing clean surgery but it is clear there have been some exclusions (see notes). | |
| Interventions | Group A: 10‐min aqueous iodophor scrub followed by iodophor paint (n=75)*. Group B: Iodophor‐in‐alcohol, film‐forming, water insoluble antiseptic (DuraPrep Surgical Soltion, 3M, St Paul, Minn) (n=84)*. |
|
| Outcomes | Primary outcome: SSI defined as drainage of pus, significant erythema at wound margins; wound drained serous fluid and was opened by surgeon; wound was felt by the operating surgeon to be infected. | |
| Notes | Trial data: Analysis 13.1 Length of follow‐up: at least thirty days post‐operatively. Group A: Assumed to be 7.5% PI scrub and 10% PI paint not confirmed by author *240 participants were randomised, some having clean and some clean‐contaminated surgery. Of the 240 randomised, 55 participants (from across the two groups) who were operated on by two surgeons were excluded because of their high infection rates. It was not possible to obtain these excluded data so only report data are presented. Specific participants excluded from the analysis ‐ increases risk of bias. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Whilst patients were noted to be randomised into two groups there is no further description of how randomisation was conducted. |
| Allocation concealment (selection bias) | Unclear risk | No details provided. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details provided. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 55 participants excluded from analysis. Unclear how many had clean surgery. |
Meier 2001.
| Methods | 2‐arm RCT: undertaken in Nigeria. | |
| Participants | 200 participants undergoing elective hernia repair. No other information. | |
| Interventions | Group A: PI paint (n=102). Group B: 5‐minute scrub with standard (shop‐brought) soap followed by application of methylated spirit (n=98). All skin preparations we performed by the same investigator. The incisional area was shaved, if needed, using a wet razor immediately before skin preparation. |
|
| Outcomes | Primary outcome: SSI defined as any redness of the wound or purulent discharge from the wound that resulted in early removal of skin sutures, operative drainage or treatment with antibiotics. | |
| Notes | Trial data: Analysis 13.1. Length of follow up: 8 to10 days post‐operatively and 4 to 8 weeks post‐operatively. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomisation was performed using a card drawing system" Not clear what this refers to. |
| Allocation concealment (selection bias) | Unclear risk | "Randomisation was performed using a card drawing system" Not clear what this refers to or who conducted this process. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No details reported. |
Paocharoen 2009.
| Methods | 2‐arm RCT; undertaken in Thailand. | |
| Participants | 500 patients undergoing a range of surgeries resulting in clean, clean‐contaminated and contaminated wounds. Of these 183 were undergoing clean surgery (as defined by the author ‐ no further details) and are considered here using outcome data supplied from authors on request. Inclusion criteria: 18‐60 year‐old surgical patients, ASA grades 1 & 2. Exculsion criteria: patient refusal, dirty wound, uncontrolled diabetes, on immunosuppressive drugs, serum albumin less than 3.0 mg/dl, or history of allergy to agent. |
|
| Interventions | Group A: 5‐minute scrub with PI followed by aqueous 10% PI paint (aqueous ‐ from author) (n=87). Group B: 5‐minute scrub with 4% chlorhexidine in 70% isopropyl alcohol (Hibitane) followed by Hibitane paint (n=96). |
|
| Outcomes | Primary outcome: SSI defined as occurring when the surgical wound was draining purulent material, or if the surgeon judged it to be infected and opened it. | |
| Notes | Trial data: Analysis 13.1 The study authors provided data concerning the infection rates for clean surgery. Length of follow‐up: one month. Group A: Assumed to be 7.5% PI scrub ‐ not confirmed by author. 10% PI and 1% PI treated as same solution since it is 10% PI solution with 1% free iodine and thus has been reported inconsistently between trials |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number table used to generate sealed envelopes (correspondence with author). |
| Allocation concealment (selection bias) | Unclear risk | Drawn from a sealed envelope, but no detail of who performed this (correspondence with author). |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All data reported, no dropouts. |
Roberts 1995.
| Methods | 2‐arm RCT; undertaken in the USA. | |
| Participants | 200 participants all undergoing a coronary artery bypass graft (CABG) which is a clean surgery. Inclusion: consecutive consenting patients undergoing CABG. Exclusion: allergy to iodine. | |
| Interventions | Group A: Aqueous iodophor scrub (5‐10 minutes) followed by iodophor paint (E‐Z Scrub Detergent and Paint, Parke Davis, Sandy Utah) (n=96). Group B: Iodophor‐in‐alcohol, film‐forming, water insoluble antiseptic (DuraPrep Surgical Soltion, 3M, St Paul, Minn) (n=104). All patients had antimicrobial (iodophor) preoperative showers on the night prior to surgery. Prophylactic antibiotics with cefuroxime were started in the operating theatre approximately 30 minutes prior to surgical incision and continued every 6 hours for 36 hours post‐op in all participants. Hair removal was performed on all participants. Iodophor‐impregnated incise drape on all chest wounds, but not leg wounds. |
|
| Outcomes | Primary outcome: SSI defined when purulent material drained from the incision site. | |
| Notes | Trial data: Analysis 13.1 Length of follow‐up: 30 days. As both the chest and legs were operated on it was possible for participants to have more than one wound infection and in two cases (both Group A) patients had both a chest wound infection and a leg wound infection. However, figures reported in this review were for numbers of patients with infections, and not wounds infected so these data were extracted and presented in the review. Group A: Assumed to be 7.5% scrub and 10% aqueous PI paint ‐ not confirmed by author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Consenting adults were randomly assigned by a table of random numbers". Not clear how the table of random numbers was used to generate a sequence. |
| Allocation concealment (selection bias) | Unclear risk | Randomised "immediately prior to the CABG procedure". No detail was given on who performed this process or how it was conducted. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All data reported, no dropouts. |
Saltzman 2009.
| Methods | 3 arm RCT; undertaken in India | |
| Participants | 150 patients all undergoing shoulder surgery. Inclusion: adults undergoing shoulder surgery. Exclusion: open wounds, concurrent infection or chronically immunosuppressed. | |
| Interventions | Group A: 0.75% PI scrub followed by 1% PI paint (n= 50). Group B: 2% chlorhexidine gluconate and 70% alcohol (Chloroprep, Enturia, El Paso Texas) (n= 50). Group C: 0.7% iodophor and 74% isopropyl alcohol (iodophor‐in‐ alcohol (Duraprep, 3M Healthcare) (n= 50). Each shoulder was prepared according to the manufacturers instructions by the attending surgeon. The participants were instructed to shower the day before surgery. Pre‐operative antibiotics were administered to all 150 participants. Participants who had prosthetic components implanted received the same protocol with the addition of 1g vancomycin and use of antibacterial impregnated barriers. |
|
| Outcomes | Primary outcome: SSI defined as any wound erythema or drainage that occurred that either required local wound care, antibiotics, or debridement in the operating room (definition obtained from author) | |
| Notes | Trial data: Analysis 13.1 Length of follow‐up: 10 months. 10% PI and 1% PI treated as same solution since it is 10% solution with 1% free iodine. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The agent used for each patient was chosen by opening a sealed, randomly assigned envelope". |
| Allocation concealment (selection bias) | Unclear risk | "sealed, randomly assigned envelope that indicated the agent to be used" Opened immediately before surgery. No detail was given about approaches used to ensure concealment (such as sequentially numbered envelopes). |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All data reported, no dropouts. |
Segal 2002.
| Methods | 4‐arm RCT; undertaken in the USA | |
| Participants | 209 patients all undergoing a coronary artery bypass graft (CABG) which is a clean surgery. Inclusion: CABG, one or more high risk predictive factor. Exclusion: pre‐existing infection, allergy to iodine, CPR in progress. | |
| Interventions | Group A: 5‐minute scrub with aqueous PI paint (scrub 7.5% and paint 10% both aqueous ‐ from author) (n=52).
Group B: Aqueous PI paint (10% aqueous ‐ from author). (n=56).
Group C: iodophor‐in‐alcohol film‐forming antiseptic (50).
Group D: iodophor‐in‐alcohol film‐forming antiseptic with iodine‐impregnated incise drape ‐ not considered further. No further details about solution strength. All participants were instructed to take an antimicrobial shower the evening before and the morning of surgery. If hair removal was necessary this was undertaken. All participants received a prophylactic preoperative antibiotic. |
|
| Outcomes | Primary outcome: SSI defined according to CDC criteria | |
| Notes | Trial data: Analysis 13.1 Length of follow‐up: 6 weeks post‐op. Assumed to be 10% PI with 1% free iodine (not confirmed by author) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Perioperative nurses initiated a data collection sheet and chose the prep method by drawing from a closed sack". Further detailed was supplied by the author: ....a bag with 120 pieces of paper (30 for each of the four methods). Once the patient was identified, the charge nurse...drew from the sack. The staff had been trained and knew which method each letter identified. Comment: Adequate method. |
| Allocation concealment (selection bias) | Unclear risk | "The study group selection was determined 10‐15 minutes prior to the incision". Further detail was supplied (as noted above) but safeguards to ensure allocation concealment were not mentioned specifically in the process as described. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All data reported, no dropouts. |
Shirahatti 1993.
| Methods | 2‐arm RCT: undertaken in India. | |
| Participants | 135 participants undergoing a range of surgeries, of which 91 were classed as clean by the authors. Exclusion: Anorectal operations, abscesses and day care procedures were excluded from the study. |
|
| Interventions | Group A: 10 minute scrub with 0.75% Cholorhexidine and 1.5% cetrimide followed by application of 1% iodine in 70% spirit (n=46) Group B: Application of 0.75% Cholorhexidine and 1.5% cetrimide followed by application of 1% iodine in 70% spirit (n= 45) Antibiotic policy in both groups was identical (no antibiotic in clean cases). All participants undergoing clean surgery did not need intravenous fluids. |
|
| Outcomes | Primary outcome: SSI defined as wound showing redness or swelling of surrounding area or had a discharge irrespective of whether any organisms were grown in the discharge. | |
| Notes | Trial data: Analysis 13.1 Length of follow‐up: Not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Whilst described as a prospective randomised trial, the method of randomisation was not reported. |
| Allocation concealment (selection bias) | Unclear risk | Method of randomisation not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported ‐ no details on blinding in the report. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Appears all randomised participants undergoing clean surgery were considered. |
Sistla 2010.
| Methods | 2‐arm trial: undertaken in India. | |
| Participants | 556 adult patients undergoing elective inguinal hernia repair. Inclusion: Over 18 and undergoing inguinal hernia repair. Exclusion: Patients with recurrent or complicated inguinal hernia and patients with a history of allergy to the antiseptics. |
|
| Interventions | Group A: 10% PI aqueous paint (aqueous ‐ from author) (N=285). Group B: 2.5% chlorhexidine in 70% ethanol paint (n=271). |
|
| Outcomes | Primary outcome: SSI defined according to CDC criteria . | |
| Notes | Trial data: Analysis 13.1 Length of follow‐up: 30 days. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomised by the sealed envelope method" Not enough detail to make judgement. |
| Allocation concealment (selection bias) | Unclear risk | "Randomised by the sealed envelope method" Not enough detail to make judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Whilst the surgeon was not blind to the type of antiseptic used information "regarding the antiseptic used was not available to the investigators or the patients during the assessment of wounds for SSI" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | "Of the 556 patients 72% returned their completed questionnaires for 30 days post‐op". 85 (30%) participants did not provide SSI data in Group A and 71 (26%) participants did not provide SSI data for Group B. Unclear if attrition was differential and thus introduced bias. |
Abbreviations
< = less than > = more than ASA = American Association of Anethetists CABG = coronary artery bypass graft CNS = Clinical Nurse Specialist CPR = cardiopulmonary resuscitation h = hour(s) OR = operating room PI = povidone iodine RCT = randomised controlled trial
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Becerro de Bengoa 2013 | Antisepsis applied post‐operatively |
| Brooks 2001 | No systematic difference in skin antiseptics used between groups. |
| Brown 1984 | Unable to extract data for clean surgery only. Authors responded to request for information, but were unable to provide clean surgery data. |
| Culligan 2005 | Not clean surgery. |
| Dewan 1987 | No systematic difference in skin antiseptics (as defined by review) used between groups. |
| Eiselt 2009 | Not a RCT (before‐and‐after study). |
| Geelhoed 1983 | Unable to obtain data for clean surgery. |
| Hagen 1995 | Not a RCT. A retrospective chart review. Two groups were treated 1 year apart with a lack of baseline comparability. |
| Hibbard 2002 | Unable to obtain data for clean surgery. |
| Kalantar‐Hormozi 2005 | Not a RCT. Quasi‐ randomised study ‐ allocation based on day of admission (even and odd days). |
| Lee 2013 | Not an RCT: Cohort study |
| Lewis 1984 | No systematic difference in skin antiseptics (as defined by review) used between groups. |
| Lorenz 1988 | No systematic difference in skin antiseptics (as defined by review) used between groups. |
| Ostrander 2005 | Not a RCT. Quasi randomisation. |
| Polk 1967 | Not a RCT. Quasi randomisation. |
| Shindo 2002 | Not clean surgery. |
| Silva 1985 | Unable to obtain data for clean surgery. |
| Swenson 2009 | Not a RCT. |
| Vos 2010 | Not a RCT. Summary of published RCT regarding pre‐operative skin anti‐septics in clean‐contaminated surgery. |
| Yoshimura 2003 | Not a RCT. |
| Zdeblick 1986 | Unable to obtain data for clean surgery. No response from author contact. |
Characteristics of studies awaiting assessment [ordered by study ID]
Nentwich 2012.
| Methods | RCT |
| Participants | Undergoing cataract surgery |
| Interventions | 10% PI pre‐operatively vs. no PI |
| Outcomes | Positive cultures ‐ SSI not measured |
| Notes |
Taneja 2012.
| Methods | RCT |
| Participants | Undergoing total joint arthoplasty |
| Interventions | Standard skin preparation with additional application of iodophor‐in‐alcohol (Duraprep) following draping but prior to incise draping. |
| Outcomes | SSI |
| Notes |
Differences between protocol and review
In response to the publication of a Cochrane review considering the use of plastic adhesive drapes during surgery for preventing SSI (Webster 2011) in this update the inclusion criteria was narrowed to include only studies of antiseptic solutions or powders (applied to the patient in the immediate preoperative period). This reclassification of plastic adhesive drapes resulted in two previously included studies (Dewan 1987; Lorenz 1988) being excluded as they evaluated drapes and not skin cleansers per se; additionally, the fourth arm of the Segal 2002 study was not considered.
In this update it was decided that Bibbo 2005; Gilliam 1990; Howard 1991; Meier 2001; and Shirahatti 1993 should be moved from excluded studies into included studies as we took a less conservative view and deemed them to be randomised controlled trials based on the information provided e.g. being described as a prospective randomised study or noting that patients were randomised but with no further details provided about how this was undertaken. Further information regarding unclear reporting was captured using risk of bias assessment.
Contributions of authors
Jo Dumville: took the lead in developing and writing this second review update. Performed independent screening, data extraction and risk of bias assessment of included trials. Responded to the peer referee feedback. Approved the final version of the review. Emma McFarlane: Contributed to writing this second review update. Performed independent screening, data extraction and risk of bias assessment of included trials. Responded to the peer referee feedback. Approved the final version of the review. Peggy Edwards: took the lead in writing the protocol and original review, provided overall methodological and clinical expertise, contacted manufacturers and performed independent data extraction and quality assessment of included trials. Responded to the peer referee feedback. Approved the final version of the original review. Contributed to the first and second updates of the review by performing searches, retrieving studies, contacting authors, performing independent data extraction and quality assessment of included trials, and amending the review where required. Allyson Lipp: assisted in writing the protocol and original review, performed searches of databases and retrieved all studies, provided methodological expertise contacted authors, was involved in selecting trials for the review and performed independent data extraction and quality assessment of included trials. Approved the final version of the review. Contributed to, and proof‐read, the first and second updates of the review. Alex Holmes: assisted in writing the protocol, and confirmed and commented upon the original review content, provided clinical expertise, contacted manufacturers, was involved in selecting trials for the review and performed independent data extraction and quality assessment of included trials. Approved the final version of the review. Contributed to the first update by performing independent data extraction and quality assessment of included trials. Zhenmi Liu: assisted with the third update ‐ screening citations and obtaining full texts, making decisions regarding inclusion, amended the review as required and approved the update.
Contributions of editorial base:
Nicky Cullum: edited the review, advised on methodology, interpretation and review content. Approved the final review and review updates prior to submission. Joan Webster, Editor: approved the second review update prior to submission. Sally Bell‐Syer: co‐ordinated the editorial process. Advised on methodology, interpretation and content. Edited the review and the updated reviews. Ruth Foxlee: designed the search strategy and edited the search methods section for the updates.
Sources of support
Internal sources
Welsh Risk Pool, UK.
University of Glamorgan, UK.
External sources
3M Clinical Fellowship Award/NATN, UK.
NIHR/Department of Health (England), (Cochrane Wounds Group), UK.
NIHR Programme Grants for Applied Research, UK.
Declarations of interest
Allyson Lipp, Peggy Edwards and Alex Holmes received sponsorship from 3M/NATN clinical fellowship to undertake the original version of this review. The findings of the review were not constrained by the sponsoring body. Allyson Lipp has received a consultancy fee for work with an antiseptics manufacturer. The work was unrelated to this systematic review.
Jo Dumville received funding from the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research funding scheme. This study presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research funding scheme (RP‐PG‐0407‐10428). The views expressed in this review are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Emma McFarlane: none known. Zhenmi Liu: none known.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Alexander 1985 {published data only}
- Alexander J, Aerni S, Plettner J. Development of a safe and effective one‐minute preoperative skin preparation. Archives of Surgery 1985;120(12):1357‐61. [DOI] [PubMed] [Google Scholar]
Berry 1982 {published data only}
- Berry A, Watt B, Goldacre M, Thomson J, McNair T. A comparison of the use of povidone‐iodine and chlorhexidine in the prophylaxis. Journal of Hospital Infection 1982;3(1):55‐63. [DOI] [PubMed] [Google Scholar]
Bibbo 2005 {published data only}
- Bibbo C, Patel DV, Gehrmann RM, Lin SS. Chlorhexidine provides superior skin decontamination in foot and ankle surgery. Clinical Orthopaedics and Related Research September 2005;438:204‐8. [DOI] [PubMed] [Google Scholar]
Ellenhorn 2005 {published and unpublished data}
- Ellenhorn JD. Clean Surgery Data Set June 2007.
- Ellenhorn JD, Smith DD, Schwarz RE, Kawachi MH, Wilson TG, McGonigle KF, et al. Paint‐only is equivalent to scrub‐and‐paint in preoperative preparation of abdominal surgery sites. Journal of the American College of Surgeons 2005;201(5):737‐41. [DOI] [PubMed] [Google Scholar]
Gilliam 1990 {published data only}
- Gilliam D, Nelson C. Comparison of a one‐step iodophor skin preparation versus traditional preparation in total joint surgery. Clinical Orthopaedics and Related Research 1990;250:258‐60. [PubMed] [Google Scholar]
Howard 1991 {published data only}
- Howard R. Comparison of a 10 minute aqueous iodophor and 2 minute water‐insoluble iodophor in alcohol preoperative skin preparation. Complications in Surgery 1991;10(7):43‐5. [Google Scholar]
Meier 2001 {published data only}
- Meier D, Nkor S, Aasa D, OlaOlorun D, Tarpley J. Prospective randomized comparison of two preoperative skin preparation techniques in a developing world country. World Journal of Surgery 2001;25(4):441‐3. [DOI] [PubMed] [Google Scholar]
Paocharoen 2009 {published data only}
- Paocharoen V, Mingmalairak C, Apisarnthanarak A. Comparison of surgical wound infection after preoperative skin preparation with 4% chlorhexidine and povidone iodine: a prospective randomised trial. Journal of the Medical Association of Thailand 2009;92(7):898‐902. [PubMed] [Google Scholar]
Roberts 1995 {published data only}
- Roberts A, Wilcox K, Devineni R, Harris R, Osevala M. Skin preparation in CABG surgery: A prospective randomized trial. Complications in Surgery 1995;14(6):724,741‐4,747. [Google Scholar]
Saltzman 2009 {published data only}
- Saltzman MD, Nuber GW, Gryzlo SM, Marecek GS, Koh JL. Efficacy of surgical preparation solutions in shoulder surgery. Journal of Bone and Joint Surgery 2009;91:1949‐53. [DOI] [PubMed] [Google Scholar]
Segal 2002 {published data only}
- Segal C, Anderson J. Preoperative skin preparation of cardiac patients. AORN journal 2002;76(5):821‐8. [DOI] [PubMed] [Google Scholar]
Shirahatti 1993 {published data only}
- Shirahatti R, Joshi R, Vishwanath Y, Shinkre N, Rao S, Sankpal J, Govindrajulu N. Effect of pre‐operative skin preparation on post‐operative wound infection. Journal of Postgraduate Medicine 1993;39(3):134‐6. [PubMed] [Google Scholar]
Sistla 2010 {published data only}
- Sistla SC, Prabhu G, Sistla S, Sadasivan J. Minimizing wound contamination in a ‘clean’ surgery: comparison of chlorhexidine‐ethanol and povidone‐iodine. Chemotherapy 2010;56:261‐7. [DOI: 10.1159/000319901] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Becerro de Bengoa 2013 {published data only}
- Becerro de Bengoa Vallejo R, Losa Iglesias ME, Alou Cervera L, Sevillano Fernández D, Prieto Prieto J. Efficacy of intraoperative antiseptic scrub after nail removal surgery. Journal of the European Academy of Dermatology and Venereology 2013;27:925‐927. [DOI] [PubMed] [Google Scholar]
Brooks 2001 {published data only}
- Brooks RA, Hollinghurst D, Ribbans WJ, Severn M. Bacterial recolonization during foot surgery: a prospective randomized study of toe preparation techniques. Foot and Ankle International 2001;22(4):347‐50. [DOI] [PubMed] [Google Scholar]
Brown 1984 {published data only}
- Brown T, Ehrlich C, Stehman F, Golichowski A, Madura J, Eitzen H. A clinical evaluation of chlorhexidine gluconate spray as compared with iodophor. Surgery, Gynecology and Obstetrics 1984;158(4):363‐6. [PubMed] [Google Scholar]
Culligan 2005 {published data only}
- Culligan PJ, Kubik K, Murphy M, Blackwell L, Snyder J. A randomized trial that compared povidone iodine and chlorhexidine as antiseptics for vaginal hysterectomy. American Journal of Obstetrics and Gynecology 2005;192(2):422‐5. [DOI] [PubMed] [Google Scholar]
Dewan 1987 {published data only}
- Dewan PA, Rij AM, Robinson RG, Skeggs GB, Fergus M. The use of an iodophor‐impregnated plastic incise drape in abdominal surgery‐‐a controlled clinical trial.. Australian and New Zealand Journal of Surgery 1987;57(11):859‐63. [DOI] [PubMed] [Google Scholar]
Eiselt 2009 {published data only}
- Eiselt D. Presurgical skin preparation with a novel 2% chlorhexidine gluconate cloth reduces rates of surgical site infection in orthopaedic surgical patients. Orthopaedic Nursing 2009;28(3):141‐5. [DOI] [PubMed] [Google Scholar]
Geelhoed 1983 {published data only}
- Geelhoed GW, Sharpe K, Simon GL. A comparative study of surgical skin preparation methods. Surgery, Gynecology and Obstetrics 1983;157(3):265‐8. [PubMed] [Google Scholar]
Hagen 1995 {published data only}
- Hagen K, Treston‐Aurand J. A comparison of two skin preps used in cardiac surgical procedures. AORN journal 1995;62(3):393‐402. [DOI] [PubMed] [Google Scholar]
Hibbard 2002 {published data only}
- Hibbard JS, Mulberry GK, Brady AR. A clinical study comparing the skin antisepsis and safety of ChloraPrep, 70% isopropyl alcohol, and 2% aqueous chlorhexidine. Journal of Infusion Nursing 2002;25(4):244‐9. [DOI] [PubMed] [Google Scholar]
Kalantar‐Hormozi 2005 {published data only}
- Kalantar‐Hormozi AJ, Davami B. No need for preoperative antiseptics in elective outpatient plastic surgical operations: a prospective study. Plastic and Reconstructive Surgery 2005 August;116(2):529‐31. [DOI] [PubMed] [Google Scholar]
Lee 2013 {published data only}
- Lee AS, Cooper BS, Malhotra‐Kumar S, Chalfine A, Daikos GL, Fankhauser C, et al. Comparison of strategies to reduce meticillin‐resistant Staphylococcus aureus rates in surgical patients: A controlled multicentre intervention trial. BMJ open 2013;3:9 e003126. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lewis 1984 {published data only}
- Lewis DA, Leaper DJ, Speller DC. Prevention of bacterial colonization of wounds at operation: comparison of iodine‐impregnated ('Ioban') drapes with conventional methods. Journal of Hospital Infection 1984;5(4):431‐7. [DOI] [PubMed] [Google Scholar]
Lorenz 1988 {published data only}
- Lorenz RP, Botti JJ, Appelbaum PC, Bennett N. Skin preparation methods before cesarean section. A comparative study. Journal of Reproductive Medicine 1988;33(2):202‐4. [PubMed] [Google Scholar]
Ostrander 2005 {published data only}
- Ostrander RV, Botte MJ, Brage ME. Efficacy of surgical preparation solutions in foot and ankle surgery. Journal of Bone and Joint Surgery 2005;87A(5):980‐5. [DOI] [PubMed] [Google Scholar]
Polk 1967 {published data only}
- Polk HC, Jr. Surgical skin preparation. A clinical comparison of two methods. American Surgery 1967;33(3):209‐12. [PubMed] [Google Scholar]
Shindo 2002 {published data only}
- Shindo K, Funai S, Kuroda K, Wakano T, Nishimura K. Clinical study on the antiseptic effect of povidone‐iodine solution for the surgical field of digestive tract operations. Dermatology (Basel Switzerland) 2002;204(Suppl 1):47‐51. [DOI] [PubMed] [Google Scholar]
Silva 1985 {published data only}
- Silva JJ, Schmidt A, Rappoport J. Effect of povidone‐iodine vs. iodine on the prevention of surgical wound infection [Efecto de povidona yodada versus yodo en la prevencion de la infeccion de la herida operatoria]. Revista Médica de Chile 1985;113:103‐5. [PubMed] [Google Scholar]
Swenson 2009 {published data only}
- Swenson BR, Hedrick TL, Metzger R, Bonatti H, Pruett TL, Sawyer RG. Effects of preoperative skin preparation on postoperative wound infection rates: A prospective study of 3 skin preparation protocols. Infection Control and Hospital Epidemiology October 2009;30(10):964‐971. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vos 2010 {published data only}
- Vos CGJ, Hartemink K. Prevention of surgical site infections: chlorhexidine better than povidone iodine. Nederlands Tijdschrift Voor Geneeskunde 2010;154:A1826. [Google Scholar]
Yoshimura 2003 {published data only}
- Yoshimura Y, Kubo S, Hirohashi K, Ogawa M, Morimoto K, Shirata K, et al. Plastic iodophor drape during liver surgery operative use of the iodophor‐impregnated adhesive drape to prevent wound infection during high risk surgery. World Journal of Surgery 2003;27(6):685‐8. [DOI] [PubMed] [Google Scholar]
Zdeblick 1986 {published data only}
- Zdeblick TA, Lederman MM, Jacobs MR, Marcus RE. Preoperative use of povidone‐iodine. A prospective, randomized study. Clinical Orthopaedics and Related Research 1986;213:211‐5. [PubMed] [Google Scholar]
References to studies awaiting assessment
Nentwich 2012 {published data only}
- Nentwich MM, Rajab M, Ta CN, He L, Grueterich M, Haritoglou C, et al. Application of 10% povidone iodine reduces conjunctival bacterial contamination rate in patients undergoing cataract surgery. Euroepan Journal of Ophthalmology 2012;22(4):541‐6. [DOI] [PubMed] [Google Scholar]
Taneja 2012 {published data only}
- Taneja M, Purtill J, Rothman R, Austin M, Parvizi J. Can surgical site infection after joint arthroplasty be reduced?. Surgical infections 2012;13:S10. [Google Scholar]
Additional references
AfPP 2007
- Association for Perioperative Practice. Standards and Recommendations for Safe Perioperative Practice. Harrogate, North Yorkshire: Association for Perioperative Practice, 2007. [Google Scholar]
AORN 2006
- Association of peri‐Operative Registered Nurses (AORN). Standards, Recommended Practices and Guidelines. 1st Edition. Denver: AORN, 2006. [Google Scholar]
Darouiche 2010
- Darouiche RO, Wall MJ Jr, Itani KM, Otterson MF, Webb AL, Carrick MM, et al. Chlorhexidine‐alcoholversus povidone‐iodine for surgical‐site antisepsis. New England Journal of Medicine 2010;362(1):18‐26. [DOI] [PubMed] [Google Scholar]
Dolan 1995
- Dolan P, Gudex C, Kind P, Williams A. A social tariff for EuroQol: results from a UK general population survey. University of York Centre for HealthEconomics Discussion Paper Series (no 138) 1995.
Dumville 2012
- Dumville JC, Soares MO, O'Meara S, Cullum N. Systematic review and mixed treatment comparison: dressings to heal diabetic foot ulcers. Diabetologia 212;55(7):1902‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hardin 1997
- Hardin W, Nichols R. Handwashing and patient skin preparation. In: Malangoni MA editor(s). Critical Issues in Operating Room Management. Philadelphia: Lippincott‐Raven, 1997:133‐49. [Google Scholar]
Health Protection Agency 2011
- Health Protection Agency. Surveilance of Surgical Site Infections in NHS hospitals in England, 2010/2011. London: Health Protection Agency December 2011:Available from: www.hpa.org.uk.
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG, on behalf of the Cochrane Statistical Methods Group and the Cochrane Bias Methods Group (Editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org. 2011.
Hinchliffe 1988
- Hinchliffe S, Montague S. Physiology for Nursing Practice. Physiology for Nursing Practice. Bailliere Tindall, 1988. [Google Scholar]
Horan 2008
- Horan TC, Andrus M, Dudeck MAC. DC/NHSN surveillance definition of healthcare‐associated infection and criteria for specific types of infections in the acute care setting. American Journal of Infection Control 2008;36(5):309‐32. [DOI] [PubMed] [Google Scholar]
Kamel 2012
- Kamel C, McGahan L, Polisena J, Mierzwinski‐Urban M, Embil JM. Preoperativeskin antiseptic preparations for preventing surgical site infections: asystematic review. Infection Control and Hospital Epidemiology 2012;33:608‐17. [DOI] [PubMed] [Google Scholar]
Larson 1988
- Larson E. Guideline for use of topical antimicrobial agents. American Journal of Infection Control 1988;16(6):253‐66. [DOI] [PubMed] [Google Scholar]
Larson 1995
- Larson E. APIC guideline for handwashing and hand antisepsis in health‐care settings. American Journal of Infection Control 1995;23(4):251‐69. [DOI] [PubMed] [Google Scholar]
Leaper 1995
- Leaper DJ. Risk factors for surgical infection. Journal of Hospital Infection 1995;30(Suppl):127‐39. [DOI] [PubMed] [Google Scholar]
Leaper 2001
- Leaper D, Orr K. Step: Inflammation and Infection. Royal College of Surgeons of England, 2001. [Google Scholar]
Leclair 1990
- Leclair J. A review of antiseptics. Cleansing agents. Todays OR Nurse 1990;12(10):25‐8. [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J, on behalf of the Cochrane Information Retrieval Methods Group. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org..
Maiwald 2012
- Maiwald M, Chan ES. The Forgotten Role of Alcohol: A Systematic Review and Meta‐Analysis of the Clinical Efficacy and Perceived Role of Chlorhexidine in Skin Antisepsis. PLoS One 2010;7:e44277. [DOI] [PMC free article] [PubMed] [Google Scholar]
Maiwald 2014
- Maiwald M, Chan ES. Pitfalls in evidence assessment: the case of chlorhexidine and alcohol in skin antisepsis. Journal of Antimicrobial Chemotherapy 2014;69:2017‐21. [DOI] [PubMed] [Google Scholar]
Malangoni 1997
- Malangoni M. Perioperative antimicrobial prophylaxis. Critical Issues in Operating Room Management. Philadelphia: Lippincott ‐ Raven Publishers, 1997:115‐32. [Google Scholar]
Mangram 1999
- Mangram A, Horan T, Pearson M, Silver L, Jarvis W. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infection Control and Hospital Epidemiology 1999;20(4):250‐78. [DOI] [PubMed] [Google Scholar]
McCluskey 1996
- McCluskey F. Does wearing a face mask reduce bacterial wound infection:a literature review. British Journal Theatre Nursing 1996;6(5):18‐20,29. [PubMed] [Google Scholar]
MHRA 2000
- Medicines and Healthcare products Regulatory Agency. SN 2000(17) ‐ Use of spirit‐based solutions during surgical procedures requiring the use of electrosurgical equipment. http://www.mhra.gov.uk/Publications/Safetywarnings/MedicalDeviceAlerts/Safetynotices/CON008859 (accessed 30 April 2008).
NICE 2008
- National Institute for Health and Clinical Excellence. Prevention and treatment of surgical site infection. NICE 2008.
Plowman 2000
- Plowman R, Graves N, Griffin M. The Socio‐economic Burden of Hospital Acquired Infection. London: Public Health Services Laboratory, 2000. [Google Scholar]
Price 2004
- Price PE, Harding KG. Cardiff Wound Impact Schedule: the development of a condition‐specific questionnaire to assess health‐related quality of life in patients with chronic wounds of the lower limb. International Wound Journal 2004;1(1):10‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
Reichman 2009
- Reichman DE, Greenberg JA. Reducing Surgical Site Infections:A Review. Reviews in Obstetrics and Gynecology 2009;2(4):212‐21. [PMC free article] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan) [Computer program]. Version 5.3. The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
SIGN 2011
- Scottish Intercollegiate Guidelines Network (SIGN). Search filters. http://www.sign.ac.uk/methodology/filters.html#random 2011.
Wade 1980
- Wade A. Pharmaceutical Handbook. 19th Edition. London: Pharmaceutical Press, 1980. [Google Scholar]
Ware 2001
- Ware JE, Koninski M. SF‐36. Physical and mental health summary scores: a manual for users of version 1.2. Rhode Island: Qualitymetric, 2001. [Google Scholar]
Warner 1988
- Warner C. Skin preparation in the surgical patient. Journal of the National Medical Association 1988;80(8):899‐904. [PMC free article] [PubMed] [Google Scholar]
Webster 2011
- Webster J, Alghamdi AA. Use of plastic adhesive drapes during surgery for preventing surgical site infection. Cochrane Database of Systematic Reviews 2007, Issue 4. [DOI: 10.1002/14651858.CD006353.pub2] [DOI] [PubMed] [Google Scholar]
Webster 2012
- Webster J, Osborne S. Preoperative bathing or showering with skin antiseptics to prevent surgical site infection. Cochrane Database of Systematic Reviews 2012, Issue 9. [DOI: 10.1002/14651858.CD004985.pub4] [DOI] [PubMed] [Google Scholar]