

Massachusetts' abortion parental consent law is associated with clinically significant delays, which may constrain options available for the clinical management of minors undergoing abortion.
Abstract
OBJECTIVE:
To describe individual-level delay in obtaining abortion associated with use of the Massachusetts judicial bypass system, which legal minors (aged 17 years or younger) use to obtain abortion without consent of a parent or legal guardian in the setting of Massachusetts' parental consent law for abortion.
METHODS:
We conducted a retrospective cohort study of 2,026 abortions among minors at a large, statewide network of abortion clinics between 2010 and 2016. Delay was defined as the number of calendar days between the minor's first call to the clinic to schedule an abortion, and the day the abortion was received.
RESULTS:
In the study population, 1,559 (77%) abortions were obtained with parental consent and 467 (23%) using judicial bypass. Abortions after judicial bypass were more common among minors identifying as Hispanic, non-Hispanic black, or other race, those of low socioeconomic status (as indicated by having Medicaid insurance) and those with a prior birth or prior abortion (all P<.05). Minors with parental consent received their abortion a mean of 8.6 days after initial contact, compared with 14.8 days for minors with judicial bypass, for an unadjusted difference of 6.1 days. In multivariable linear regression modeling adjusting for demographic differences between groups, this difference persisted: minors who obtained abortions after judicial bypass had a significantly greater delay compared with those with parental consent (adjusted mean difference = 5.2 days; 95% CI 4.3 to 6.2). Using multivariable logistic regression modeling, minors with judicial bypass also had higher odds of becoming ineligible for medication abortion between the day of first call and the day of procedure (adjusted odds ratio 1.57; 95% CI 1.09 to 2.26).
CONCLUSION:
Massachusetts' parental consent law for abortion is associated with delay among minors and thereby may constrain the clinical options available to them.
Thirty-seven states currently mandate parental consent or notification before provision of abortion care to minors.1 Among the oldest of these laws is Massachusetts' parental consent law, the subject of the 1979 Supreme Court case Bellotti v Baird, which found parental involvement laws are permissible under the U.S. Constitution so long as parental involvement can be bypassed through some mechanism, for example, a petition to a judge (“judicial bypass”).2 Though a significant majority of minors prefer to inform their parents about their abortions, and do so even in the absence of a legal mandate, some do not involve parents owing to poor relationship quality, family stressors, fear of abuse, or are unable to involve parents owing to logistical barriers.3–6 Currently, these minors may use judicial bypass hearings to circumvent the parental involvement requirement in 36 states.1
The 2018 National Academies of Sciences, Engineering and Medicine report, “The Safety and Quality of Abortion Care in the United States,” named timeliness as one of six key components of quality abortion care.7 The effects of parental involvement laws, and in particular the effect of the judicial bypass process on timeliness of abortion, are unclear. Parental involvement laws do not appear to reduce minors' overall pregnancy rates or birth rates but may lead to delay in accessing abortion.8–13 Several ecologic studies found an increase in second trimester abortion rates after the implementation of parental involvement laws; however, owing to lack of individual-level data, it is not clear whether this delay is associated specifically with judicial bypass utilization.11,13 The few studies on parental involvement laws that use individual-level data are primarily limited to vital statistics records with few demographic variables collected, leaving potential for unmeasured confounding.14,15 Therefore, any delay in obtaining abortion owing to use of the judicial bypass process remains poorly described in the literature.
We set out to fill this gap through a retrospective cohort study documenting individual-level abortion delay associated with using Massachusetts' judicial bypass system for minors receiving abortion care without parental consent.
METHODS
We conducted a retrospective observational cohort study of abortions among minors 17 years or younger at three Planned Parenthood League of Massachusetts clinics in the Eastern, Central, and Western regions of the state, between September 2010 and June 2016. Massachusetts law requires the consent of one parent or legal guardian for all never-married legal minors before obtaining abortion. No other adults are permitted to provide consent. The statute itself does not elucidate how consent may be given.16 The standard procedure at Planned Parenthood League of Massachusetts clinics in this study is for the minor patient and the accompanying parent to each sign a form signifying informed consent (for the parent) or assent (for the minor) in person on the day of the abortion procedure. The state of Massachusetts does not have any other major abortion restrictions, including no mandatory waiting period before abortion. MassHealth, the state Medicaid program, routinely reimburses abortion care.
In addition to being Massachusetts' largest abortion provider, Planned Parenthood League of Massachusetts hosts a statewide care navigation program that connects minors seeking judicial bypass with pro bono legal counsel.17–22 This program is available free of charge to minors seeking abortion at any provider anywhere in the state, and serves all minors who use judicial bypass for abortion at Planned Parenthood League of Massachusetts. Care navigators based at Planned Parenthood League of Massachusetts maintain standardized intake records that query minors on their pregnancy and abortion plans and document the location of the court to which the minor plans to travel for the bypass hearing. Within one business day, the care navigators obtain all necessary information and assign legal counsel. The state of Massachusetts does not provide consent for minors in its custody (such as incarcerated individuals or those in the foster care system), and never-married legally emancipated minors may not consent for themselves under the parental involvement statute.16 Therefore, the following groups must use judicial bypass: 1) never-married minors not involving their parents or guardians in the abortion decision or whose parents or guardians refuse to provide consent, 2) never-married minors whose parents or guardians support the abortion but are unable to provide documented consent for logistical reasons, 3) never-married minors who are in foster care or incarcerated, and 4) never-married emancipated minors with no legal guardian.
Using scheduling and billing data, as well as a database maintained by the care navigation program, we identified 2,073 instances of minors seeking abortion at Planned Parenthood League of Massachusetts over the study period, of whom four were excluded because they were married minors not subject to the parental consent law. For the remaining 2,069, we were able to track outcomes both for individuals who received abortions at Planned Parenthood League of Massachusetts, which had an institutional gestational age limit of 18 weeks 6 days for abortions during the study period, and for those who were referred from Planned Parenthood League of Massachusetts to outside providers owing to a gestational age of 19 weeks or later. Data on minors who required an external referral were abstracted both from the Planned Parenthood League of Massachusetts medical record and from a patient referral database maintained by care-navigation staff. From the initial cohort, we excluded 33 records from the analysis either because the minor continued the pregnancy after initially requesting abortion (n=22, 1.1%), or because they were lost to follow up after initially requesting an abortion (n=11, 0.5%). Additionally, we excluded 10 records (0.5%) with missing values for key variables. This resulted in a final sample size of 2,026 abortions corresponding to 1,909 minors as some minors had multiple abortion procedures in the study period. We obtained public records from the Massachusetts Department of Public Health Registry of Vital Records and Statistics, including total abortions provided by patient age, for the study period. Based on these records, we calculate the Planned Parenthood League of Massachusetts cohort examined here includes 60% of all abortions provided to minors in Massachusetts over the study period.17–22
All data were dual-entered. Data from the electronic medical record (EMR) were exported by a computer programmer using a SQL query from the NextGen EMR that was in use at Planned Parenthood League of Massachusetts from September 2010 through June 2016. Every variable was also manually abstracted by a research assistant, and the manually entered dataset was compared with the SQL-exported dataset to check for discrepancies using a merging function in a REDCap (Research Electronic Data Capture) database hosted by Partners Healthcare.23 Additionally, all variables from the judicial bypass care navigation team's paper records and electronic referral database were manually abstracted and dual-entered independently by two research assistants and merged in REDCap to check for discrepancies. All discrepancies were reviewed by investigators and reconciled through manual record review. All study procedures were approved by the Partners Human Research Committee (institutional review board).
The primary outcome of this analysis was mean delay in time to abortion defined as the number of days from the date of first telephone contact by the minor to Planned Parenthood League of Massachusetts requesting to schedule an abortion, and the date abortion care was ultimately received. For minors who initiated cervical dilation the day before uterine evacuation (eg, through the placement of osmotic dilators), the date of cervical dilation was considered the date of abortion procedure. The secondary outcomes were the odds of passing specific gestational age thresholds during the delay period; that is, of being eligible for a particular abortion procedure on the date of first contact but becoming ineligible by gestational age before actually receiving care. We examined individual odds of passing three clinically significant gestational thresholds corresponding to changes in clinical care: 1) becoming ineligible for medication abortion per institutional protocol at 64 days (9 weeks) of gestation or more (before April 1, 2015) or 71 days (10 weeks) of gestation or more (on or after April 1, 2015, in accordance with a change in clinical protocol by Planned Parenthood League of Massachusetts); 2) having routine same-day cervical ripening recommended, prolonging the procedure day at 85 days (12 weeks) of gestation or more; or 3) having cervical ripening required, which, for a majority of minors, required a 2-day procedure at 99 days (14 weeks) of gestation or more. To create these variables, we first calculated gestational age at first contact as gestational age using ultrasound scan on the day of procedure minus the number of days since first contact. Abortions were coded as passing through a threshold if gestational age at first contact was less than the threshold and the gestational age at procedure was greater than the threshold.
The exposure of interest was consent type coded as parental or guardian consent (hereafter, “parental consent”) or judicial bypass. Based on prior literature documenting demographic factors associated with later presentation to abortion care among adult or mixed-age populations, we considered the following patient characteristics as potential confounding variables for the relationship between the exposure and the primary and secondary outcomes: age, Hispanic ethnicity and race category, being Medicaid insured (as a proxy for socioeconomic status), residential distance to clinic, parity (none vs any prior births), prior abortion (none vs any), and patient-reported gestational age at first call to Planned Parenthood League of Massachusetts, which is recorded by appointment schedulers as part of standard preprocedure phone screening.24–27 In Massachusetts, Medicaid routinely reimburses abortions and many patients use this coverage. However, because we considered Medicaid a proxy for socioeconomic status, we coded any patient recorded as having Medicaid insurance anywhere within the EMR within 60 days of the abortion procedure as Medicaid-insured, irrespective of abortion payment type. We computed the distance to clinic as the mileage from the centroid of residential ZIP code to the exact address of the Planned Parenthood League of Massachusetts clinic where the patient sought care using the geodist package in Stata. For the patient-reported gestational age at first phone call variable, there were missing values for 379 (19%) abortions. We imputed based on the mean value from abortions in the same gestational age at procedure category (at or before 9 0/7 weeks, 9 1/7–12 0/7 weeks, 12 1/7–13 6/7 weeks, 14 0/7–15 6/7 weeks, 16 0/7–18 6/7 weeks, 19 0/7 weeks or more). We investigated differences in demographic and clinical characteristics by consent type using χ2 tests for categorical variables and two-sample t-tests for continuous variables.
For the primary analysis, we built a multivariable linear regression model to compare the mean delay in abortion care by consent type adjusting for multiple confounders. For the secondary analysis, we built three multivariable logistic regression models for each gestational age threshold to compare the odds of passing a gestational age threshold during the delay period by consent type. For each model, only abortions at risk of passing the threshold were included; that is, gestational age at first contact was less than the outcome threshold being assessed. For all analyses, we accounted for multiple abortions per minor by use of generalized estimating equations—a common technique to estimate the parameters from the regression mean model while adjusting the variance for clustering.28–30 Before building the logistic regression models, we confirmed there were at least five events for each categorical variable included in the analysis for all three cutpoints.31 The abortion was the unit of analysis in all presented analyses. All statistical analyses were performed in Stata 15.
RESULTS
During the study period, there were 2,026 abortions provided to minors. Of these, 1,559 (77%) abortions were provided with parental consent and 467 (23%) abortions followed judicial bypass. Further, 97% (n=1,964) of abortions occurred at Planned Parenthood League of Massachusetts and 3% (n=62) were referred to other providers. We found significant differences (P<.05) by consent type for all demographic and social characteristics (Table 1). The distributions of race and ethnicity categories and of age categories were significantly different between the judicial bypass and parental consent groups (P<.001). Additionally, Medicaid insurance was more prevalent among abortions after judicial bypass (75%, 348/467) than among those with parental consent (59%, 925/1,559) (P<.001). Ten percent (46/467) of the judicial bypass group reported a prior birth, compared with 6% (97/1,559) of the parental consent group (P=.010). Twelve percent (56/467) of the judicial bypass group reported a prior abortion, compared with 9% (136/1,559) of the parental consent group (P=.034).
Table 1.
Characteristics of the Study Population by Consent Type (N=2,026)

The mean delay in time to abortion was 6.1 days longer for minors using judicial bypass (8.6 vs 14.8 days, P<.001, Table 1). This finding is corroborated in Figure 1, where the mean of the distribution of delay in time to abortion with parental consent is closer to no delay compared with the mean of the distribution among the judicial bypass group. The overall greater amount of delay in the judicial bypass group is also evident when examined categorically: whereas 47% (732/1,559) of minors obtaining abortion with parental consent accessed care within 6 days, only 8% (37/467) of those with judicial bypass did so; conversely, 7% (105/1,559) of the parental consent group was delayed 21 days or more, compared with 19% (88/467) of the bypass group (P<.001, Table 1). There was no significant difference in the proportions of abortion procedures requiring two visits to achieve adequate cervical dilation (“2-day procedures”) between the judicial bypass and parental consent groups. In the parental consent group, 93% (1,450/1,559) of procedures were 1-day and 7% (109/1,559) were 2-day, compared with 90.8% (424/467) 1-day and 9.2% (42/467) 2-day in the bypass group (P=.11).
Fig. 1. Distribution of delay in time to abortion by consent type (N=2,026).
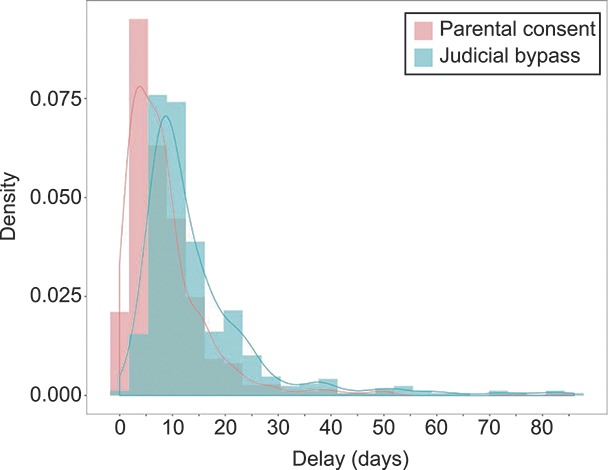
Janiak. Massachusetts’ Abortion Parental Consent Law. Obstet Gynecol 2019.
A significant difference in mean delay persisted when adjusting for demographic factors (adjusted mean difference 5.2 days; 95% CI 4.29 to 6.20, P<.001, Table 2). In the multivariable linear regression model, we also found that minors with a prior birth (adjusted mean difference=2.3; 95% CI 0.79 to 3.89) and prior abortion (adjusted mean difference=1.9; 95% CI 0.51 to 3.20) experienced a statistically significantly longer delay in time to abortion (Table 2). Minors with higher self-reported gestational age (weeks) at first contact also had a significantly longer delay (adjusted mean difference=0.9; 95% CI 0.79 to 1.05). There were no significant differences in delay in time to abortion by age category, Hispanic ethnicity and race category, Medicaid insurance (as a proxy for socioeconomic status), or residential distance from the clinic.
Table 2.
Univariable and Multivariable Linear Model Results: Mean Delay in Time to Abortion (Days) by Consent Type, Demographic, and Medical Variables Among Minors Undergoing Abortion in Massachusetts (N=2,026)

For the secondary analysis, the unadjusted odds of reaching or passing the medication abortion, 84-day, or 98-day thresholds were greater among judicial bypass abortions compared with parental consent abortions (Table 3). Among minors with parental consent, 15% (n=164) first called the clinic before the medication abortion threshold but ultimately presented to care when they were too advanced in gestation for that method compared to 28% (n=96) among minors who used judicial bypass. Figure 2 provides an additional illustration for this finding as the proportion of judicial bypass abortions, 33% (141/428), passing any of the three thresholds is significantly larger than that among parental consent abortions, 19% (268/1,441) (P<.001). In the adjusted analysis (Table 4), the odds of becoming ineligible for medication abortion were significantly greater among judicial bypass abortions compared with parental consent abortions (adjusted odds ratio [aOR] 1.57; 95% CI 1.09 to 2.26). However, the associations between consent type and passing gestational age thresholds were not significant for the 84-day (aOR 1.34; 95% CI 0.83 to 2.16) and 98-day (aOR 1.43; 95% CI 0.76 to 2.69) multivariable logistic regression models.
Table 3.
Prevalence of Passing a Gestational Age Threshold Between the Initial Scheduling Call and Procedure by Consent Type Among Minors Undergoing Abortion in Massachusetts

Fig. 2. Passing a gestational age threshold between the initial scheduling call and procedure by consent type (n=1,869*): (A) Judicial bypass (n=428) and (B) parental consent (n=1,441). Horizontal lines represent the gestational age at first contact to gestational age at procedure in days for each abortion by consent type. The length of each horizontal line can be interpreted as the delay in days from first contact to procedure. The vertical lines correspond to gestational age thresholds. *Includes only pregnancies with gestational age at first contact before the 98-day threshold.
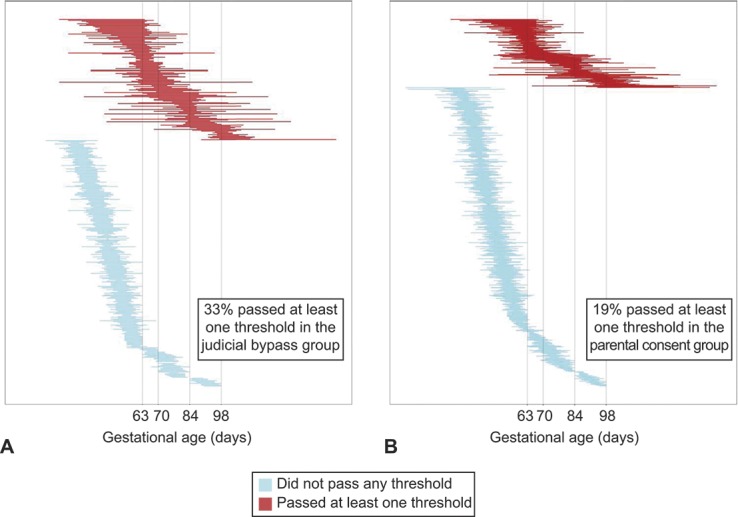
Janiak. Massachusetts’ Abortion Parental Consent Law. Obstet Gynecol 2019.
Table 4.
Multivariable Logistic Model Results: Odds of Passing a Gestational Age Threshold Between the Initial Scheduling Call and Procedure by Consent Type Among Minors Undergoing Abortion in Massachusetts

DISCUSSION
Within this large retrospective cohort, we found judicial bypass of Massachusetts' parental consent law disproportionately involves minors who identify as racial or ethnic minorities, and who are of low socioeconomic status. Adolescents who sought judicial bypass were also more likely to have prior births and abortions. Some adolescents may choose judicial bypass because their familiarity with pregnancy imbues them with the confidence to make the abortion decision without the involvement of a parent; conversely, some may know from prior experience that parents will react poorly to the pregnancy. On average, the parental consent group experienced approximately a 9-day lapse from first scheduling call to abortion care, roughly comparable with the 10-day wait documented in a 2004 national survey of abortion patients.25 By contrast, the judicial bypass group experienced a 15-day wait. We did not find any difference in delay related to residential distance to the clinic. All three Planned Parenthood League of Massachusetts clinics that provide abortion care are in major cities located near highways and accessible by bus and rail. Distance may affect time to abortion in larger states with less transit infrastructure.
In both raw and adjusted analyses, minors who sought judicial bypass experienced statistically and clinically significant delays. Although the risk of death from abortion is low in absolute terms (0.6/100,000 abortions), mortality increases exponentially by 38% with each week of additional gestation.32,33 Additionally, procedures at later gestational ages require additional cervical priming, increasing time spent at the clinic, patient discomfort, and for some patients, financial burden. Because young age is an independent risk factor for difficult dilation and for cervical laceration, advancing gestational age increases the risk for procedural complications among minors in particular.34 Thus, the time required to comply with the judicial bypass process may increase the risks of medical complications for some minors in Massachusetts. Additionally, clinical management options change as gestational age at time of abortion advances. Within our cohort, minors who received judicial bypass were significantly more likely to lose the option of a medication abortion as they waited for their abortion care, compared with those with parental consent. Prior literature has demonstrated that some patients have strong preferences for medication abortion.35,36
These results have several limitations. First, the study cohort represents approximately two-thirds of minors who obtained abortions in Massachusetts over the study period. It is possible that the one third of minors who did not seek abortion at Planned Parenthood League of Massachusetts differ from those who did, and in particular that they received abortion care at hospitals or private doctors' offices, which could be associated with greater disease burden or higher overall socioeconomic status. Because Planned Parenthood League of Massachusetts has clinics throughout the state, we do not suspect that area of residence systematically differs between minors who were or were not included. Additionally, we do not suspect that gestational age at abortion systematically differs between individuals in the cohort and those we did not capture, because the presence of a care-navigation program within Planned Parenthood League of Massachusetts enabled us to track outcomes for minors referred out of the source clinics at 19 weeks of gestation or greater. Additionally, our proxy variable for socioeconomic status is imperfect. Although we are certain that every person with Medicaid is low-income, it is also possible that some individuals who are uninsured or have private insurance are also low-income. Further, the race–ethnicity category was either unknown or refused to answer for 17% of abortions. Finally, by design, our clinic-based cohort study was not able to capture any minors who desired but ultimately chose not to attempt to receive abortion care owing to the parental consent law.
Our findings may not be generalizable to other states with parental consent laws, particularly those with additional legal barriers to obtaining abortion. Many states have additional abortion regulations that do not exist in Massachusetts, such as laws prohibiting Medicaid (in 33 states) or private (in 11 states) insurance from reimbursing abortion care,37 mandated counseling and waiting periods (in 27 states),38 or regulations on clinic infrastructure that have resulted in closures of freestanding abortion clinics (6% drop nationally from 2011 to 2014).39 In states with additional legal restrictions, the effect of obtaining judicial bypass on procedural timing may be amplified by the presence of additional barriers. Importantly, poor quality information provision40–42 and a lack of robust infrastructure to connect minors with attorneys and courts for judicial bypass hearings—each of which have been documented in several states—could also introduce delays that do not exist in Massachusetts. At the bypass hearing, denials and the need for legal appeals could result in additional delay or ultimate denial of abortion care for some minors. Nationally representative data on the frequency of denials are currently lacking.
Massachusetts' parental involvement law for abortion is associated with significant delays, thereby potentially increasing medical risks and constraining the clinical options available to patients. Because racial and ethnic minority youth, as well as those of lower socioeconomic status, are overrepresented in the judicial bypass group, the law may accordingly worsen reproductive health inequities among these populations. The full effect of parental involvement requirements has not yet been documented in most U.S. states with such laws. Future research should describe both the population-level effects of these policies, as well as any disparate effect on subpopulations of vulnerable youth.
Footnotes
Supported by the Society of Family Planning (SFP) Research Fund (grant number SFPRF10-1). The findings and conclusions in this article are those of the authors and do not necessarily reflect the views of the SFP Research Fund or of Planned Parenthood Federation of America, Inc.
Financial Disclosure The authors did not report any potential conflicts of interest.
Presented at the North American Forum on Family Planning, October 20–22, 2018, New Orleans, Louisiana.
The authors thank TJ McAndrew for assistance with EMR queries and Souci Rollins and Cale Stoeffler for assistance accessing study data.
Peer reviews and author correspondence are available at http://links.lww.com/AOG/B339.
REFERENCES
- 1.Guttmacher Institute. Parental involvement in minors' abortions. Available at: https://www.guttmacher.org/state-policy/explore/parental-involvement-minors-abortions. Retrieved August 17, 2018. [Google Scholar]
- 2.Bellotti v. Baird, 443 U.S. 622; 1979. [PubMed] [Google Scholar]
- 3.Webster RD, Neustadt AN, Whitaker AK, Gilliam ML. Parental involvement laws and parent-daughter communication: policy without proof. Contraception 2010;82:310–13. [DOI] [PubMed] [Google Scholar]
- 4.Ralph L, Gould H, Baker A, Foster DG. The role of parents and partners in minors' decisions to have an abortion and anticipated coping after abortion. J Adolesc Health 2014;54:428–34. [DOI] [PubMed] [Google Scholar]
- 5.Kavanagh EK, Hasselbacher LA, Betham B, Tristan S, Gilliam ML. Abortion-seeking minors' views on the Illinois parental notification law: a qualitative study. Perspect Sex Reprod Health 2012;44:159–66. [DOI] [PubMed] [Google Scholar]
- 6.Ehrlich JS. Who decides? The abortion rights of teens. Westport (CT): Prager; 2003. [Google Scholar]
- 7.National Academies of Sciences, Engineering, and Medicine. The safety and quality of abortion care in the United States. Washington, DC: The National Academies Press; 2018. [PubMed] [Google Scholar]
- 8.Cartoof VG, Klerman LV. Parental consent for abortion: impact of the Massachusetts law. Am J Public Health 1986;76:397–400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.MacAfee L, Castle J, Theiler RN. Association between the New Hampshire parental notification law and minors undergoing abortions in northern New England. Obstet Gynecol 2015;125:170–4. [DOI] [PubMed] [Google Scholar]
- 10.Dennis A, Henshaw SK, Joyce TJ, Finer LB, Blanchard K. The impact of laws requiring parental involvement for abortion: a literature review. New York (NY): Guttmacher Institute; 2009. [Google Scholar]
- 11.Henshaw SK. The impact of requirements for parental consent on minors’ abortions in Mississippi. Fam Plann Perspect 1995;27:120–2. [PubMed] [Google Scholar]
- 12.Colman S, Joyce T. Minors' behavioral responses to parental involvement laws: delaying abortion until age 18. Perspect Sex Reprod Health 2009;41:119–26. [DOI] [PubMed] [Google Scholar]
- 13.Rogers JL, Boruch RF, Stoms GB, DeMoya D. Impact of the Minnesota parental notification law on abortion and birth. Am J Public Health 1991;81:294–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Colman S, Joyce T, Kaestner R. Misclassification bias and the estimated effect of parental involvement laws on adolescents' reproductive outcomes. Am J Public Health 2008;98:1881–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Joyce T. Parental consent for abortion and the judicial bypass option in Arkansas: effects and correlates. Perspect Sex Reprod Health 2010;42:168–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Consent to abortion, forms, persons less than 18 years of age. Massachusetts General Laws Chapter 112, Section 12s; 1977. [Google Scholar]
- 17.Massachusetts Department of Public Health. Registry of vital records and statistics. Abortion tables, 2010. Boston (MA): Massachusetts Department of Public Health; 2011. [Google Scholar]
- 18.Massachusetts Department of Public Health. Registry of vital records and statistics. Abortion tables, 2011. Boston (MA): Massachusetts Department of Public Health; 2012. [Google Scholar]
- 19.Massachusetts Department of Public Health. Registry of vital records and statistics. Abortion tables, 2012. Boston (MA): Massachusetts Department of Public Health; 2013. [Google Scholar]
- 20.Massachusetts Department of Public Health. Registry of vital records and statistics. Abortion tables, 2013. Boston (MA): Massachusetts Department of Public Health; 2014. [Google Scholar]
- 21.Massachusetts Department of Public Health. Registry of vital records and statistics. Abortion tables, 2014. Boston (MA): Massachusetts Department of Public Health; 2015. [Google Scholar]
- 22.Massachusetts Department of Public Health. Registry of vital records and statistics. Abortion tables, 2015. Boston (MA): Massachusetts Department of Public Health; 2016. [Google Scholar]
- 23.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42:377–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jones RK, Finer LB. Who has second-trimester abortions in the United States? Contraception 2012;85:544–51. [DOI] [PubMed] [Google Scholar]
- 25.Finer LB, Frohwirth LF, Dauphinee LA, Singh S, Moore AM. Timing of steps and reasons for delays in obtaining abortions in the United States. Contraception 2006;74:334–44. [DOI] [PubMed] [Google Scholar]
- 26.Drey EA, Foster DG, Jackson RA, Lee SJ, Cardenas LH, Darney PD. Risk factors associated with presenting for abortion in the second trimester. Obstet Gynecol 2006;107:128–35. [DOI] [PubMed] [Google Scholar]
- 27.Janiak E, Kawachi I, Goldberg A, Gottlieb B. Abortion barriers and perceptions of gestational age among women seeking abortion care in the latter half of the second trimester. Contraception 2014;89:322–7. [DOI] [PubMed] [Google Scholar]
- 28.Zeger SL, Liang KY, Albert PS. Models for longitudinal data: a generalized estimating equation approach. Biometrics 1988;44:1049–60. [PubMed] [Google Scholar]
- 29.Hibbs AM, Black D, Palermo L, Cnaan A, Luan X, Truog WE, et al. Accounting for multiple births in neonatal and perinatal trials: systematic review and case study. J Pediatr 2010;156:202–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Yelland LN, Sullivan TR, Pavlou M, Seaman SR. Analysis of randomised trials including multiple births when birth size is informative. Paediatr Perinat Epidemiol 2015;29:567–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Vitinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol 2007;165:710–8. [DOI] [PubMed] [Google Scholar]
- 32.Raymond EG, Grimes DA. The comparative safety of legal induced abortion and childbirth in the United States. Obstet Gynecol 2012;119:215–9. [DOI] [PubMed] [Google Scholar]
- 33.Bartlett LA, Berg CJ, Shulman HB, Zane SB, Green CA, Whitehead S, et al. Risk factors for legal induced abortion-related mortality in the United States. Obstet Gynecol 2004;103:729–37. [DOI] [PubMed] [Google Scholar]
- 34.Allen RH, Goldberg AB. Society of Family Planning clinical guidelines: cervical dilation before first-trimester surgical abortion (14 weeks' gestation). Contraception 2016;93:277–91. [DOI] [PubMed] [Google Scholar]
- 35.Crandell L. Psychological outcomes of medical versus surgical elective first trimester abortion. Nurs Womens Health 2012;16:296–307. [DOI] [PubMed] [Google Scholar]
- 36.Ho PC. Women’s perceptions on medical abortion. Contraception 2006;74:11–15. [DOI] [PubMed] [Google Scholar]
- 37.Henry J. Kaiser Family Foundation Interactive: how state policies shape access to abortion coverage. Available at: https://www.kff.org/interactive/abortion-coverage/. Retrieved November 11, 2018. [Google Scholar]
- 38.Guttmacher Institute. Counseling and waiting periods for abortion. Available at: https://www.guttmacher.org/print/state-policy/explore/counseling-and-waiting-periods-abortion. Retrieved November 11, 2018. [Google Scholar]
- 39.Jones RK, Jerman J. Abortion incidence and service availability in the United States, 2014. Perspect Sex Reprod Health 2017;49:17–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Dodge LE, Haider S, Hacker MR. Knowledge of state-level abortion laws and policies among front-line staff at facilities providing abortion services. Womens Health Issues 2012;22:415–20. [DOI] [PubMed] [Google Scholar]
- 41.Coleman-Minahan K, Stevenson AJ, Obront E, Hays S. Young women’s experiences obtaining judicial bypass for abortion in Texas. J Adol Health 2019;64:20–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Silverstein H. Girls on the stand: how courts fail pregnant minors. New York (NY): New York University Press; 2009. [Google Scholar]