

Abstract
Background
This is an update of a previous Cochrane review published in Issue 1, 2010 and updated in Issue 9, 2015. The role of lymphadenectomy in surgical management of endometrial cancer remains controversial. Lymph node metastases can be found in approximately 10% of women who before surgery are thought to have cancer confined to the womb. Removal of all pelvic and para‐aortic lymph nodes (lymphadenectomy) at initial surgery has been widely advocated, and pelvic and para‐aortic lymphadenectomy remains part of the FIGO (International Federation of Gynaecology and Obstetrics) staging system for endometrial cancer. This recommendation is based on data from studies that suggested improvement in survival following pelvic and para‐aortic lymphadenectomy. However, these studies were not randomised controlled trials (RCTs), and treatment of pelvic lymph nodes may not confer a direct therapeutic benefit, other than allocating women to poorer prognosis groups. Furthermore, the Cochrane review and meta‐analysis of RCTs of routine adjuvant radiotherapy to treat possible lymph node metastases in women with early‐stage endometrial cancer found no survival advantage. Surgical removal of pelvic and para‐aortic lymph nodes has serious potential short‐term and long‐term sequelae. Therefore, it is important to investigate the clinical value of this treatment.
Objectives
To evaluate the effectiveness and safety of lymphadenectomy for the management of endometrial cancer.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE and Embase to June 2009 for the original review, updated the search to June 2015 for the last updated version and further extended the search to March 2017 for this version of the review. We also searched registers of clinical trials, abstracts of scientific meetings, and reference lists of included studies, and we contacted experts in the field.
Selection criteria
RCTs and quasi‐RCTs that compared lymphadenectomy versus no lymphadenectomy in adult women diagnosed with endometrial cancer.
Data collection and analysis
Two review authors independently extracted data and assessed risk of bias. Hazard ratios (HRs) for overall and progression‐free survival and risk ratios (RRs) comparing adverse events in women who received lymphadenectomy versus those with no lymphadenectomy were pooled in random‐effects meta‐analyses. We assessed the quality of the evidence using the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) approach.
Main results
978 unique references were identified via the search strategy. All but 50 were excluded by title and abstract screening. Three RCTs met the inclusion criteria; for one small RCT, data were insufficient for inclusion in the meta‐analysis. The two RCTs included in the analysis randomly assigned 1945 women, reported HRs for survival adjusted for prognostic factors and based on 1851 women and had an overall low risk of bias, as they satisfied four of the assessment criteria. The third study had an overall unclear risk of bias, as information provided was not adequate concerning random sequence generation, allocation concealment, blinding, or completeness of outcome reporting.
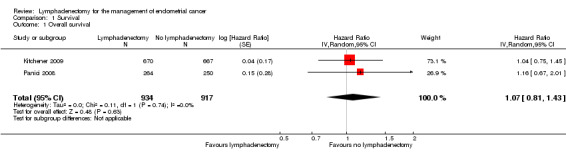
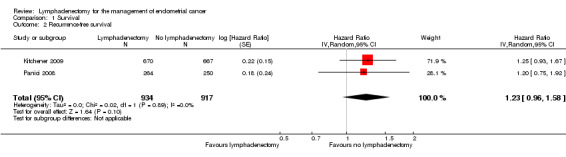
Results of the meta‐analysis remained unchanged from the previous versions of this review and indicated no differences in overall and recurrence‐free survival between women who underwent lymphadenectomy and those who did not undergo lymphadenectomy (pooled hazard ratio (HR) 1.07, 95% confidence interval (CI) 0.81 to 1.43; HR 1.23, 95% CI 0.96 to 1.58 for overall and recurrence‐free survival, respectively) (1851 participants, two studies; moderate‐quality evidence).
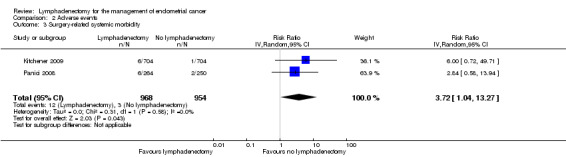
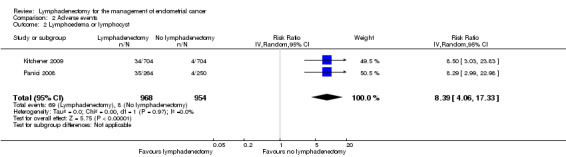
We found no difference in risk of direct surgical morbidity between women who underwent lymphadenectomy and those who did not undergo lymphadenectomy. However, women who underwent lymphadenectomy had a significantly higher risk of surgery‐related systemic morbidity and lymphoedema/lymphocyst formation than those who did not undergo lymphadenectomy (RR 3.72, 95% CI 1.04 to 13.27; RR 8.39, 95% CI 4.06 to 17.33 for risk of surgery‐related systemic morbidity and lymphoedema/lymphocyst formation, respectively) (1922 participants, two studies; high‐quality evidence).
Authors' conclusions
This review found no evidence that lymphadenectomy decreases risk of death or disease recurrence compared with no lymphadenectomy in women with presumed stage I disease. Evidence on serious adverse events suggests that women who undergo lymphadenectomy are more likely to experience surgery‐related systemic morbidity or lymphoedema/lymphocyst formation. Currently, no RCT evidence shows the impact of lymphadenectomy in women with higher‐stage disease and in those at high risk of disease recurrence.
Plain language summary
The role of removing lymph nodes as part of standard surgery for endometrial cancer
The issue Cancer of the lining of the womb (endometrial cancer) is now the most common gynaecological cancer among women in western Europe and North America. Most of these women (75%) have tumours confined to the body of the womb at the time of diagnosis, and three‐quarters of women will survive for 10 years after diagnosis. Lymph node metastases can be found in one in 10 women who appear to have cancer confined to the womb at the time of diagnosis, and removal of all pelvic and para‐aortic lymph nodes has been advocated, even for women with presumed early‐stage cancer. This recommendation is based on non‐randomised studies that suggested improvement in survival following removal of pelvic and para‐aortic lymph nodes. However, treatment of pelvic lymph nodes may not be beneficial, and additional treatment to lymph nodes might not necessarily be better treatment, especially as surgical removal of lymph nodes has serious potential short‐term and long‐term harmful effects.
The aim of the review To evaluate the safety and efficacy of lymphadenectomy in the management of endometrial cancer.
What are the main findings? We found only three trials that compared lymphadenectomy with no lymphadenectomy among women with endometrial cancer. One of these trials could not be included in the meta‐analysis of this review, as it provided insufficient information about outcomes for women. When we combined findings from the two remaining trials, which included 1945 women, we found no evidence that women who received lymphadenectomy were less likely to die or have a relapse of their cancer. In addition, severe adverse events experienced as a consequence of lymphadenectomy outnumbered those reported when no lymphadenectomy was performed.
Quality of the evidence The overall quality of the evidence for lymphadenectomy versus standard surgery was moderate for survival outcomes and adverse events (other than evidence for presence or absence of lymphoedema or lymphocyst, which was of high quality). The quality of evidence for quality of life was very low, as this outcome was not reported.
What are the conclusions? The uncertainty of whether lymphadenectomy or no lymphadenectomy is best in the management of early‐stage endometrial cancer probably reflects the fact that evidence shows no reduction in death or in disease relapse when lymphadenectomy is performed, rather than lack of evidence. In addition, women undergoing lymphadenectomy experienced more severe adverse events than those who did not undergo lymphadenectomy.
Summary of findings
Summary of findings for the main comparison. Summary of findings table.
| Lymphadenectomy for the management of endometrial cancer | |||||||
|
Patient or population: women with stage I endometrial cancer Settings: inpatient or outpatient Intervention: lymphadenectomy | |||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | ||
| Assumed risk | Corresponding risk | ||||||
| Control | Lymphadenectomy | ||||||
| Overall survival Follow‐up: median 37 to 49 monthsa | HR 1.07 (0.81 to 1.43) | 1851 (2 studies) | ⊕⊕⊕⊝ Moderateb | As a result of the way HRs are calculated, assumed and corresponding risks were not estimated | |||
| Recurrence‐free survival Follow‐up: median 37 to 49 monthsa | HR 1.23 (0.96 to 1.58) | 1851 (2 studies) | ⊕⊕⊕⊝ Moderateb | As a result of the way HRs are calculated, assumed and corresponding risks were not estimated | |||
| Direct surgical morbidity | Study population | RR 1.93 (0.79 to 4.71) | 1922 (2 studies) | ⊕⊕⊕⊝ Moderateb | |||
| 17 per 1000 | 33 per 1000 (13 to 80) | ||||||
| Moderate‐risk population | |||||||
| 19 per 1000 | 37 per 1000 (15 to 89) | ||||||
| Surgery‐related systemic morbidity | Study population | RR 3.72 (1.04 to 13.27) | 1922 (2 studies) | ⊕⊕⊕⊝ Moderateb | |||
| 3 per 1000 | 11 per 1000 (3 to 40) | ||||||
| Moderate‐risk population | |||||||
| 5 per 1000 | 19 per 1000 (5 to 66) | ||||||
| Lymphoedema or lymphocyst | Study population | RR 8.39 (4.06 to 17.33) | 1922 (2 studies) | ⊕⊕⊕⊕ High | |||
| 8 per 1000 | 67 per 1000 (32 to 139) | ||||||
| Moderate‐risk population | |||||||
| 11 per 1000 | 92 per 1000 (45 to 191) | ||||||
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; HR: Hazard ratio; RR: Risk ratio. | |||||||
| GRADE Working Group grades of evidence. High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | |||||||
aMedian follow‐up was 37 months (interquartile range (IQR) 24 to 58 months) in the Kitchener trial and 49 months (IQR 27 to 79 months) in the trial of Panici.
bEstimate is imprecise, as a fair degree of uncertainty can be seen in the pooled estimate, as indicated by a 95% confidence interval.
Background
Description of the condition
Endometrial cancer affects the lining of the womb and is the fifth most common cancer among women worldwide (Ferlay 2012). The disease occurs predominantly in postmenopausal women (91% of cases are reported in women over 50 years old) (Parkin 2005). Global incidences vary as a result of differences in risk factors, with higher risk associated with a 'western' lifestyle; the age‐standardised incidence is 14.7 per 100,000 women per year in more developed countries, compared with 5.5 per 100,000 per year in less developed countries (Ferlay 2012). One of the main risk factors for endometrial cancer is unopposed oestrogen, which may come from exogenous (from outside of the body) sources, such as oestrogen‐only hormone replacement therapy (HRT), or endogenous (from within the body) overproduction, as is seen with polycystic ovarian syndrome, oestrogen‐producing tumours and excessive adipose tissue in obese women (Park 2010; Renehan 2008).
Most women present with symptoms of abnormal vaginal bleeding. This typically is reported as postmenopausal bleeding, as most cases occur in those over the age of 50, although younger women may present with intermenstrual bleeding, menorrhagia (heavy periods), or a change in bleeding pattern, and in those over 45 years, changes in menstruation should be investigated (NICE 2007). Less common symptoms include low pelvic pain and vaginal discharge. Most women (75% to 80%) with postmenopausal bleeding present with early‐stage disease (International Federation of Gynaecology and Obstetrics (FIGO) stage I), in which the disease is confined to the womb (Shepherd 1989 ‐Table 2), (Siegel 2015 ‐ Figure 1). It should be noted that FIGO staging was changed in 2009, following publication of the main studies included in this analysis (Pecorelli 2009 ‐ Table 3). The 2009 staging system will be used in this review, unless otherwise stated.
1. Pre‐2009 FIGO staging.
| Stage | Extent of disease | |
| I | Tumour limited to uterine body | |
| IA | Limited to endometrium | |
| IB | < 1/2 myometrial depth invaded | |
| IC | > 1/2 myometrial depth invaded | |
| II | Tumour limited to uterine body and cervix | |
| IIA | Endocervical invasion only | |
| IIB | Invasion into cervical stroma | |
| III | Extension to uterine serosa, peritoneal cavity and/or lymph nodes | |
| IIIA | Extension to uterine serosa, adnexae or positive peritoneal fluid (ascites or washings) | |
| IIIB | Extension to vagina | |
| IIIC | Pelvic or para‐aortic lymph nodes involved | |
| IV | Extension beyond true pelvis and/or involvement of bladder/bowel mucosa | |
| IVA | Extension to adjacent organs | |
| IVB | Distant metastases or positive inguinal lymph nodes | |
1.
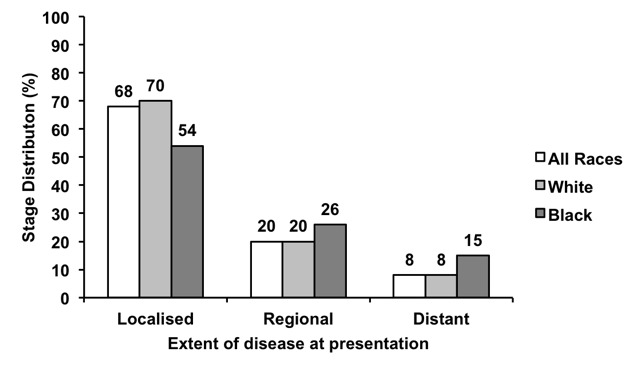
Distribution of stage of endometrial cancer at presentation, USA 2004‐2010. Adapted from Siegel 2015.
2. FIGO staging (2009).
| Stage | Extent of disease | |
| 1 | Tumour confined to corpus uteri | |
| IA | No or less than half myometrial invasion | |
| IB | Invasion equal to or greater than half of the myometrium | |
| II | Tumour invasion into cervical stroma but not extending beyond uterus | |
| III | Local and/or regional spread of tumour | |
| IIIA | Tumour invasion into serosa of corpus uteri and/or adnexae | |
| IIIB | Vaginal and/or parametrial involvement | |
| IIIC | Metastases to pelvic and/or para‐aortic lymph nodes | |
| IIIC1 | Positive pelvic nodes | |
| IIIC2 | Positive para‐aortic lymph nodes with or without positive pelvic lymph nodes | |
| Stage IV tumour invasion into bladder and/or bowel mucosa, and/or distant metastases | ||
| IVA | Tumour invasion into bladder and/or bowel mucosa | |
| IVB | Distant metastases, including intra‐abdominal metastasis and/or inguinal nodes | |
Pelvic washings/cytology should be recorded separately and now does not change the stage.
Histologically most endometrial cancers are endometrioid adenocarcinomas. Other histological subtypes tend to have a poorer prognosis, as they typically are more aggressive (high grade = G3) and present at a more advanced FIGO stage. These include adenosquamous, clear cell and serous carcinomas.
Endometrial cancer directly invades surrounding tissues, most commonly the myometrium and the cervix. Lymphatic spread also occurs, primarily to the pelvic lymph nodes, including external and common iliac lymph nodes, and then to the para‐aortic lymph nodes. Results of histopathological studies have demonstrated spread to pelvic and para‐aortic lymph nodes in up to 10% of cases of early‐stage disease (Creasman 1987). Metastasis to more distant organs is typically haematological.
Description of the intervention
Standard treatment for early‐stage endometrial cancer consists of total hysterectomy, bilateral salpingo‐oophorectomy (BSO) and washings. This may be performed via a laparotomy or by a laparoscopic approach. For patients with risk factors for spread beyond the womb, adjuvant radiotherapy (and increasingly chemotherapy) is administered to reduce the risk of recurrence.
Randomised controlled trials (RCTs) have demonstrated that adjuvant radiotherapy does not improve overall survival In early‐stage disease (FIGO stage I without G3 disease or without evidence of invasion into the lymphovascular space), although it does reduce the number of pelvic recurrences (Kong 2012). Reducing the number of pelvic recurrences does not affect survival rates, probably because pelvic recurrences usually can be treated effectively with radiotherapy in women who have not previously received pelvic radiotherapy.
Lymphadenectomy can be considered as clearance of all lymph nodes or sampling of a few lymph nodes from an anatomical area. Lymphadenectomy is used to drain the site of cancer when cancers have spread to the lymph nodes, for example, in breast cancer surgery. Lymphadenectomy often refers to the systematic removal of all lymph nodes within a defined area, as opposed to lymph node sampling, which refers to removal of a few representative lymph nodes or removal of suspiciously enlarged nodes. Use of sentinel lymph node biopsy in the management of endometrial carcinoma is a topic of increasing interest, and studies assessing the diagnostic accuracy of this procedure have yielded promising results (Ansari 2013; Kang 2011).
How the intervention might work
Knowledge of cancer spread gives prognostic information and guides the decision to provide adjuvant treatment in the form of radiotherapy and chemotherapy. Lymphadenectomy can be directly therapeutic, as surgery removes involved lymph nodes, which may be the source of pelvic recurrences. However, lymph node involvement is rare if the tumour is of low grade (G1) or is confined to the inner half of the myometrium (FIGO stage IA). Hence, surgical staging involving a lymphadenectomy may be recommended only for women who are at increased risk of pelvic lymph node involvement (e.g. those with higher‐grade tumours identified by biopsy) (Kim 1993).
Nevertheless, lymphadenectomy is not performed without serious short‐term and long‐term morbidity. Many women with endometrial cancer are elderly or obese and have serious comorbidities, and the increase in operative time required to perform a full lymphadenectomy may increase risks of surgery and anaesthesia. Complications associated with lymphadenectomy include damage to blood vessels and nerves during the operation; development of a deep vein thrombosis or pulmonary embolus during the postoperative period; and lymphoedema and/or pelvic lymphocyst formation. These complications can be severe and disabling, and lymphoedema and lymphocyst formation may be under‐reported or under‐recognised, especially in studies focusing on short‐term outcomes.
Why it is important to do this review
Debate is ongoing regarding lymphadenectomy for the treatment of endometrial cancer. Lymphadenectomy may not be routinely performed, and if it is, the extent of lymphadenectomy can range from taking a few lymph nodes for sampling to performing complete pelvic and para‐aortic lymphadenectomy.
The extent of disease, as assessed by preoperative imaging (such as magnetic resonance imaging (MRI)) and the grade of tumour as identified through biopsies, may influence the decision whether to undertake lymphadenectomy. The ongoing MAPPING study aims to determine whether MRI, diffusion‐weighted MRI, fluorodeoxyglucose positron emission tomography (FDGPET)/computed tomography (CT) and fluoro‐ethyl‐choline PET/CT can identify lymph node metastasis and facilitate minimally invasive or non‐invasive lymph node staging (ISRCTN84527805). Results of this study may further influence the decision to perform lymphadenectomy.
Evidence from one retrospective, non‐randomised study suggested that multiple‐site lymph node sampling may increase survival over procedures that do not include lymph node sampling (Kilgore 1995). In this retrospective review of 649 participants with endometrial cancer, women who underwent multiple‐site lymph node sampling had improved five‐year survival (extrapolated from survival curves) compared with women who underwent no pelvic node sampling (five‐year survival ˜90% vs ˜75%; P = 0.002). Furthermore, one study found that patients who undergo extensive lymph node sampling may have increased survival as compared with those who have fewer lymph nodes removed (Chan 2006). This retrospective analysis of 12,333 participants with endometrioid endometrial cancer demonstrated that participants with high‐risk disease (pre‐2009 FIGO stage IB, grade 3 or greater) appeared to have improved five‐year survival rates following extensive lymph node removal (75.3% with one node removed vs 86.8% with 20 or more nodes removed; P = 0.001). Another large, population‐based study of 9185 women with stage I and 881 women with stage II endometrial cancer compared outcomes stratified by whether lymph node sampling had been performed (Trimble 1998). Overall investigators reported no significant differences in five‐year survival for women with stage I and II disease who did or did not undergo lymph node sampling. In contrast, a retrospective study of 671 women with endometrial cancer demonstrated improvement in overall survival for those at intermediate or high risk of disease recurrence among women who had undergone para‐aortic lymphadenectomy in addition to pelvic lymphadenectomy compared with women treated with pelvic lymphadenectomy alone (hazard ratio (HR) 0.44, 95% confidence interval (CI) 0.30 to 0.64) (Todo 2010).
However, lymphadenectomy, similar to pelvic radiotherapy (Kong 2012), is not beneficial for most women with endometrial cancer, as most are unlikely to have lymph node involvement. Therefore, the additional surgery would make no difference to their chance of cure or need for further treatment and would benefit only a minority of women to the detriment of the majority, who would be cured by hysterectomy and BSO alone. The previous version of this review did not demonstrate that lymphadenectomy improved survival or reduced disease recurrence compared with no lymphadenectomy in women with presumed stage I disease (May 2010). However, knowledge of lymph node status does provide prognostic information and may reduce the need for adjuvant radiotherapy in women found to have negative lymph nodes (Look 2004).
As these data demonstrate, clinical controversy surrounds the role of lymphadenectomy in endometrial cancer. This procedure carries significant long‐term morbidity for a large minority of patients and should be performed only if good evidence demonstrating improvements in survival and quality of life (QOL) supports its use.
This review aimed to address the value of lymphadenectomy in endometrial cancer. This included the effects of routine removal of all pelvic lymph nodes (pelvic lymphadenectomy) and effects of routine removal of para‐aortic lymph nodes. This review also assessed evidence for the value of removing clinically suspicious (enlarged) lymph nodes.
Objectives
To evaluate the effectiveness and safety of lymphadenectomy for the management of endometrial cancer.
Methods
Criteria for considering studies for this review
Types of studies
RCTs and quasi‐RCTs. We excluded cross‐over trials and cluster‐randomised trials.
Types of participants
Adult women diagnosed with endometrial cancer. We excluded women with other concurrent malignancies.
Types of interventions
We included the following comparisons.
Pelvic lymphadenectomy versus no lymphadenectomy.
Pelvic lymphadenectomy versus pelvic lymph node sampling.
Pelvic and para‐aortic lymphadenectomy versus no lymphadenectomy.
Pelvic and para‐aortic lymphadenectomy versus pelvic lymphadenectomy.
Removal of bulky pelvic lymph nodes versus no removal of lymph nodes.
Types of outcome measures
Primary outcomes
Overall survival (OS).
Secondary outcomes
Progression‐free survival (PFS).
QOL measured by a validated scale.
Adverse events, for example,
direct surgical morbidity (e.g. injury to bladder, ureter, vascular, small bowel (or colon); presence and complications of adhesions; febrile morbidity; intestinal obstruction; haematoma; local infection);
surgery‐related systemic morbidity (chest infection, thromboembolic events (deep vein thrombosis and pulmonary embolism), cardiac events (cardiac ischaemia and cardiac failure), cerebrovascular accident;
recovery: delayed discharge, unscheduled re‐admission;
lymphoedema and lymphocyst formation; and
other side effects not categorised above.
Search methods for identification of studies
Electronic searches
See the Cochrane Gynaecological Cancer Group methods used in reviews. We searched the following electronic databases.
Original review ‐ 2010
Cochrane Central Register of Controlled Trials (CENTRAL; 2009, Issue 2).
MEDLINE ‐ 1966 to June 2009.
Embase ‐ 1966 to June 2009.
Updated review ‐ 2015
Cochrane Central Register of Controlled Trials (CENTRAL; 2015, Issue 5).
MEDLINE ‐ June 2009 to June 2015.
Embase ‐ June 2009 to June 2015.
Updated review ‐ 2017
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 3).
MEDLINE ‐ June 2015 to March 2017.
Embase ‐ June 2015 to March 2017.
We developed a search strategy based on terms related to the review topic (for CENTRAL, MEDLINE and EMBASE search strategies, see Appendix 1, Appendix 2, and Appendix 3).
All relevant articles found were identified on PubMed, and, using the 'related articles' feature, we carried out a further search for newly published articles.
Searching other resources
Unpublished and grey literature
We searched metaregister, Physicians Data Query, www.controlled‐trials.com/rct, www.clinicaltrials.gov and www.cancer.gov/clinicaltrials for ongoing trials. We contacted the main investigators of relevant ongoing trials, along with the major co‐operative trials groups active in this area, to ask for further information..
Handsearching
We handsearched the reference lists of all relevant trials obtained by this search to look for further trials.
Correspondence
We contacted authors of relevant trials to ask if they knew of additional data that may or may not have been published.
Language
We sought papers in all languages and carried out translations when necessary.
Data collection and analysis
Selection of studies
Original review ‐ 2010
We downloaded all titles and abstracts retrieved by electronic searching to the reference management database Endnote and removed duplicates. At least two review authors (a combination of KW, JM, and AB) independently examined the remaining references. We excluded studies that clearly did not meet the inclusion criteria and obtained copies of the full text of potentially relevant references. Two review authors (JM and KW) independently assessed the eligibility of retrieved papers and resolved disagreements by discussion between them and, if necessary, with a third review author (AB). We documented reasons for exclusion.
Updated review ‐ 2015
We downloaded all titles and abstracts retrieved by electronic searching to the reference management databases Endnote and Mendeley and removed duplicates. At least two review authors (of KW, JF, and JM) independently examined the remaining references. We excluded studies that clearly did not meet the inclusion criteria and obtained copies of the full text of potentially relevant references. Two review authors (KW and JF) independently assessed the eligibility of retrieved papers and, when necessary, requested additional information from study authors. These two review authors resolved disagreements by discussion between them and, if necessary, with a third review author (JM). We documented reasons for exclusion.
Update review ‐ 2017
We downloaded all titles and abstracts (MEDLINE: June 2015 to March week 4 2017 – 61 refs; Embase: June 2015 to 2017 week 13 – 135 refs; Central: Issue 3 of 12 2017 – 54 refs) to the RCT classifier for de‐duplication and identification of possible RCTs. 76 unique references were identified and 20 were identified as possible clinical trials by the classifier. These 76 references were uploaded to Covidence and the 20 potential clinical trials screened independently by two reviewers (JM and JF). There were no disagreements and no additional studies were identified.
Data extraction and management
We extracted data from the included studies as recommended in Chapter 7 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). These data consisted of characteristics of participants (inclusion criteria, age, stage, comorbidity, previous treatment, number enrolled in each arm), interventions (extent of lymphadenectomy, number of lymph nodes removed, use of radiotherapy or chemotherapy), study quality, duration of follow‐up, outcomes, any variables used to adjust HRs, and deviations from the protocol. Two review authors (a combination of JM, KW and JF) independently extracted data. When possible, all data extracted were those relevant to an intention‐to‐treat (ITT) analysis. Review authors resolved differences by discussion or by appeal to a third review author (JM), if necessary.
Assessment of risk of bias in included studies
We assessed risk of bias in included RCTs by using the Cochrane 'risk of bias' tool and the criteria specified in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). This included assessment of:
sequence generation;
allocation concealment;
blinding (assessment of blinding was restricted to blinding of outcome assessors, as generally it is not possible to blind participants and personnel to surgical interventions);
incomplete outcome data;
selective reporting of outcomes; and
other possible sources of bias.
Two review authors (KW and JF) independently applied the 'risk of bias' tool and resolved differences by discussion or by appeal to a third review author (JM). We have presented results in the 'risk of bias' table, the 'risk of bias' graph and the 'risk of bias' summary section. We interpreted results of meta‐analyses in the light of the 'risk of bias' assessment.
Measures of treatment effect
For time‐to‐event data (overall survival, progression‐free survival), we extracted the HR and its variance from trial reports; if these were not presented, we would have attempted to abstract the data required to estimate them using Parmar's methods (Parmar 1998) (e.g. number of events in each arm and log‐rank P value comparing relevant outcomes in each arm, or relevant data from Kaplan‐Meier survival curves).
For dichotomous outcomes (adverse events), we extracted the number of participants in each treatment arm who experienced the outcome of interest to estimate a risk ratio (RR).
We also extracted the number of participants assessed at endpoint.
Dealing with missing data
We attempted to extract data on outcomes only for participants who were assessed at endpoint. We did not impute missing outcome data; if only imputed outcome data were reported, we contacted trial authors to request data on outcomes only among participants who were assessed.
Assessment of heterogeneity
We assessed heterogeneity between studies by visually inspecting forest plots, by estimating the percentage of heterogeneity between trials that could not be ascribed to sampling variation (Higgins 2003), by conducting a formal statistical test of the significance of the heterogeneity (Deeks 2001) and, if possible, by performing subgroup analyses (see below). If we found evidence of substantial heterogeneity, we investigated and reported possible reasons for this.
Assessment of reporting biases
We were unable to assess reporting bias, as only three studies met our inclusion criteria.
Data synthesis
We pooled the findings of two of the three included trials in meta‐analyses.
For time‐to‐event data (overall survival and progression‐free survival), we pooled HRs using the generic inverse variance facility of RevMan 5. We used adjusted HRs, if available; otherwise we used unadjusted results.
For dichotomous outcomes (adverse events), we pooled RRs.
We used random‐effects models with inverse variance weighting for all meta‐analyses (DerSimonian 1986).
We have presented the overall quality of the evidence for each outcome according to the GRADE approach, which takes into account issues not only related to internal validity (risk of bias, inconsistency, imprecision, publication bias) but also to external validity such as directness of results (Langendam 2013). We have created a 'Summary of findings' table based on the methods described the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) and GRADEpro GDT. We used the GRADE checklist and GRADE Working Group quality of evidence definitions (Meader 2014). We downgraded the evidence from 'high' quality by one level for serious (or by two for very serious) concerns for each limitation.
Subgroup analysis and investigation of heterogeneity
We performed no subgroup analyses, as only three trials met our inclusion criteria. The two trials included in the meta‐analysis showed no heterogeneity (I2 = 0).
Sensitivity analysis
We performed no sensitivity analyses, as both of the studies included in the analysis were at low risk of bias.
'Summary of findings' table
Results
Description of studies
Results of the search
Original review ‐ 2010
The search yielded 349 unique references. Three review authors independently read the abstracts of these articles and at this stage excluded articles that obviously did not meet the inclusion criteria. We retrieved 18 articles in full text and translated them into English, when appropriate; we identified updated versions of relevant studies. Through full‐text screening of these 18 studies, we excluded 11 trials. However, we identified two completed RCTs that met our inclusion criteria and five references that provided preliminary results of the two included studies. See Figure 2 for a study flow diagram.
2.
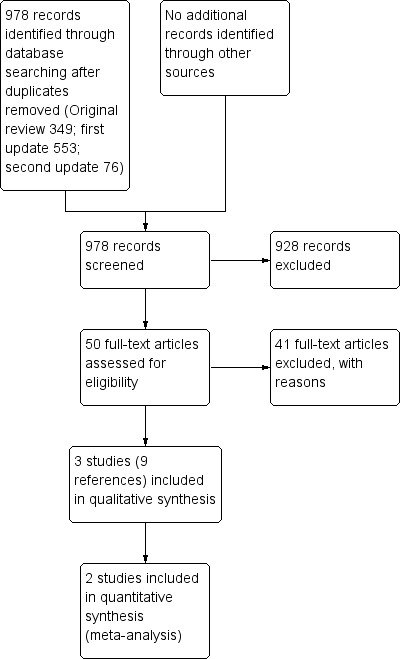
Study flow diagram.
Updated review ‐ 2015
The search yielded 553 additional unique references. At least two review authors (of KW, JF and JM) independently read the abstracts of these articles and excluded 521 articles that obviously did not meet the inclusion criteria. We retrieved 32 articles in full and subjected them to full‐text screening. We subsequently excluded 30 of these. One additional RCT met the inclusion criteria, and one article provided additional data from a previously included RCT.
Searches of the grey literature revealed no additional relevant studies.
Therefore, in this updated version of the review, we excluded 41 of the articles reviewed in full text for the reasons given in the Characteristics of excluded studies table and included nine articles reporting results from three RCTs, as described in the Characteristics of included studies table.
Updated review ‐ 2017
The search yielded 76 additional unique references. On screening, all articles were excluded and no articles were retrieved in full text.
Included studies
Three studies met the inclusion criteria (Fayallah 2011; Kitchener 2009; Panici 2008). One of these was a small RCT of 38 participants (Fayallah 2011) designed to assess the role of pretreatment detection of P53 overexpression in the selection of women with clinical stage I disease for pelvic lymphadenectomy. We excluded this study from the meta‐analysis, as it was not possible to estimate hazard or risk ratios for the outcomes of interest in this review using the data provided. We contacted authors of the Fayallah 2011 study via their published contact details to ask for additional information, but none has been forthcoming. We also contacted the publishers of the Fayallah 2011 study to ask for further information, but we have received no response.
The two remaining included trials (Kitchener 2009; Panici 2008) randomly assigned 1945 women, of whom 1923 (99%) were assessed at the end of the trial and 1851 (95%) were assessed in multivariate survival analyses using Cox models.
Kitchener 2009 reported 191 (13.6%) deaths and 173 (12.3%) disease recurrences; Panici 2008 reported 53 (10.3%) deaths and 78 (15.1%) disease recurrences; Kitchener 2009 reported 38 (2.7%) instances of direct surgical morbidity, seven (0.5%) cases of surgery‐related systemic morbidity, 12 (0.9%) cases of lymphocyst formation and 26 (1.8%) cases of lymphoedema; Panici 2008 reported 13 (2.5%) instances of direct surgical morbidity, eight (1.6%) cases of surgery‐related systemic morbidity and 39 (7.6%) cases of lymphoedema/lymphocyst formation.
Fayallah 2011 randomly assigned 38 women and reported four (10.5%) deaths; seven (18.4%) disease recurrences; five (13.2%) instances of direct surgical morbidity, one (2.6%) case of surgery‐related systemic morbidity and one (2.6%) case of lymphorrhoea.
The Kitchener 2009 trial (ASTEC)
Design
Between 1998 and 2005, 1408 women with preoperative endometrial cancer thought clinically to be confined to the uterus (womb) (pre‐2009 FIGO stage I) from 85 centres in four countries were randomly assigned preoperatively to standard surgery (n = 704) (total hysterectomy, bilateral salpingo‐oophorectomy and palpation of para‐aortic lymph nodes) or standard surgery plus systematic pelvic lymphadenectomy (n = 704) (iliac and obturator lymph nodes). Women with enlarged lymph nodes in the standard surgery arm could have these removed at the discretion of the surgeon. All operations were performed by specialist gynaecological surgeons with experience in pelvic lymphadenectomy, and the operation was performed by the same surgeon, regardless of to which arm the participant was randomly assigned. After surgery, women with early‐stage disease at intermediate or high risk of recurrence were randomly assigned (independent of lymph node status) to the ASTEC radiotherapy trial, to control for adjuvant treatment.
Participants
Women were well matched between the two arms in terms of clinico‐pathological features, although slightly more poor prognosis histopathological types were assigned to the lymphadenectomy arm (clear cell 10 (1%) versus 17 (2%); serous 21 (3%) versus 32 (5%)). In the lymphadenectomy arm, 58 (8%) women had no nodes removed for reasons including anaesthetic concerns, obesity, obvious late‐stage disease or participant request. For those in the lymphadenectomy arm who did undergo lymphadenectomy, a median of 12 nodes (range one to 59) were removed. Thirty‐five (5%) women in the standard surgery arm underwent lymph node sampling with removal of a median of two nodes (range one to 27). Lymph nodes were invaded by cancerous cells in nine participants in the standard surgery arm (27% of the 35 women who had suspicious nodes removed at the time of surgery) and in 54 (9%) of the 686 women in the lymphadenectomy arm who had lymph nodes removed.
Interventions
This study pre‐dated routine use of laparoscopic surgery, and most study participants underwent open surgery. Median operating time was shorter in the standard surgery group: 60 minutes (10 to 255) for standard surgery and 90 minutes (10 to 390) for lymphadenectomy. Median hospital stay was six days (range two to 120 days) for standard surgery and six days (range two to 106 days) for lymphadenectomy. Women in the lymphadenectomy arm were more likely to have a vertical than a transverse (Pfannenstiel) abdominal incision (287 (45%) vertical incisions for standard surgery versus 384 (60%) vertical incisions for lymphadenectomy).
One‐third of women in each group received adjuvant radiotherapy (standard surgery 227 (33%); lymphadenectomy 228 (33%)), and similar numbers received external beam radiotherapy plus vault brachytherapy (173 (25%) versus 165 (23%)) or brachytherapy only (54 (8%) versus 63 (9%)).
Median follow‐up was 37 months (interquartile range (IQR) 24 to 58 months).
The Panici 2008 trial
Design
Over 9½ years, 514 participants with endometrial cancer clinically confined to the uterus preoperatively (pre‐2009 FIGO stage I) from 31 centres (30 in Italy and 1 in Chile) were randomly assigned to undergo pelvic systematic lymphadenectomy (n = 264) or no lymphadenectomy (n = 250). All eligible women had frozen section performed on the uterus to confirm the presence of endometrioid or adenosquamous carcinoma and grade of disease, and to evaluate the depth of myometrial invasion. Women without myometrial invasion (pre‐2009 FIGO stage IA) and those with a well‐differentiated tumour and less than 50% myometrial invasion (G1, pre‐2009 FIGO stage IB) were excluded. All other women were randomly assigned intraoperatively to one of the two trial arms by a block arrangement that balanced treatment assignments at each site. Women randomly assigned to the pelvic lymphadenectomy arm had lymphatic tissue removed from the external iliac, superficial and common iliac regions. Dissection was considered appropriate only if 20 or more lymph nodes were removed for histopathological examination. Para‐aortic node sampling or lymphadenectomy was performed at the discretion of the surgeon. In the no‐lymphadenectomy group, no lymphatic tissue in the retroperitoneal region was removed other than bulky (> 1 cm) lymph nodes detected at gross intraoperative inspection by palpation of lymph node sites.
Participants
Women were well matched between the two arms in terms of clinico‐pathological features, except for a higher proportion of pre‐2009 FIGO stage IIIC participants in the lymphadenectomy arm, following examination of lymph node status. All women allocated to the lymphadenectomy arm underwent lymphadenectomy, with a median of 26 pelvic lymph nodes removed (range 21 to 35). In the no‐lymphadenectomy arm, 56 (22%) women had enlarged lymph nodes and underwent pelvic lymph node sampling or lymphadenectomy: 28 (11%) had more than 10 lymph nodes removed. Of these 56 women with bulky lymph nodes, only eight (15% of those who had lymph nodes removed) had positive lymph nodes on histological examination. Aortic lymphadenectomy was performed in 69 (26%) of the 264 women in the lymphadenectomy arm and in five (2%) of the 250 women in the no lymphadenectomy arm.
Interventions
Median operating time (180 minutes versus 120 minutes, P < 0.001) and hospital in‐patient stay (6 days versus 5 days; P value < 0.001) were greater in the lymphadenectomy arm than in the no lymphadenectomy arm.
Rates of adjuvant therapy (pelvic external beam, brachytherapy, chemotherapy, or combination of chemotherapy and radiotherapy) were similar between the two arms. Most participants received no adjuvant therapy (69% in the lymphadenectomy arm and 65% in the no‐lymphadenectomy arm; P = 0.07).
Median follow‐up was 49 months (IQR 27 to 79 months).
The Fayallah 2011 trial
Design
Between April 2005 and October 2008, 38 women with preoperative clinical stage I endometrial carcinoma from a single hospital were preoperatively randomly assigned to extrafascial hysterectomy, bilateral salpingo‐oophorectomy with pelvic lymphadenectomy (n = 21) (iliac and obturator lymph nodes) or extrafascial hysterectomy and bilateral salpingo‐oophorectomy alone (n = 17). Before surgery, immunohistochemistry was carried out on endometrial tissue for detection of P53 over‐expression. After surgery, the decision to provide adjuvant radiotherapy was made at the discretion of tumour board meeting members. Women were followed up every three months with clinical assessment and ultrasound and underwent MRI every six months.
Participants
No significant difference was noted between the two arms in terms of age, medical status, surgical stage, histological type, or grade of tumour. The number of nodes removed from women in either arm was not reported.
Interventions
Operating time, route of surgery, and use of adjuvant therapy were not reported in the trial.
Mean follow‐up after treatment was 21.5 months (range six to 40 months).
Outcomes reported
Both the Panici 2008 trial and the Kitchener 2009 trial reported overall and recurrence‐free survival rates and used appropriate statistical techniques (HRs to correctly allow for censoring). Investigators adjusted for prognostic factors in the analysis of survival outcomes in each trial.
The Fayallah 2011 trial reported survival rate and recurrence rate as percentages based on participants who were known to have died or were known to experience disease progression. Hazard ratios and risk ratios were not reported and could not be estimated from available data. Study authors provided no additional data.
In the trial of Kitchener 2009, investigators adjusted HR for age (continuous), World Health Organization (WHO) performance status (0, 1, 2, 3, or 4), weeks between diagnosis and randomisation (six weeks or longer vs less than six weeks), surgical technique intended (open vs laparoscopic), type of incision (vertical vs Pfannenstiel vs other transverse), extent of tumour (confined vs spread), histology (endometrioid/adenocarcinoma vs other), depth of invasion (inner half vs endometrium, outer half vs endometrium), differentiation (grade 1, 2, or 3) and centre (dummy variables and centres with fewer than five women were grouped as one new centre). Seventy‐one women were not included (37 standard surgery group, 34 lymphadenectomy group): 39 with no disease and 32 with differentiation not applicable (histology mixed epithelial stromal sarcoma).
In the trial of Panici 2008, researchers adjusted the HR for age (65 or older, younger than 65 years), tumour grade (grade 1, 2 or 3), myometrial invasion (50% or more, less than 50%) and tumour stage (stage I to II, stage III to IV).
A secondary analysis from the Panici 2008 trial assessed survival in women who underwent lymphadenectomy compared with those who did not undergo lymphadenectomy in relation to age (older than 65 years and 65 years or younger).
For distribution of these factors at baseline in each trial by treatment arm, see the Characteristics of included studies table.
The two trials included in the analysis reported adverse events (direct surgical morbidity, surgery‐related systemic morbidity, and lymphoedema or lymphocyst formation).
Excluded studies
After obtaining the full text, we excluded 41 articles for the following reasons.
21 studies were non‐RCTs, including retrospective reviews, in which results were compared between women who underwent systematic lymphadenectomy and those who did not.
11 articles were reviews on the role of lymphadenectomy in endometrial cancer; none identified any RCT‐level evidence.
9 studies were RCTs but provided no outcome information based on randomisation for lymphadenectomy.
For further details on all excluded studies, see the Characteristics of excluded studies table.
Risk of bias in included studies
The Panici 2008 and Kitchener 2009 trials were at low risk of bias: They satisfied four of the criteria that we used to assess risk of bias (see Figure 3 and Figure 4). The Fayallah 2011 trial had an overall unclear risk of bias, as adequate information was not available concerning random sequence generation, allocation concealment, blinding, or completeness of outcome reporting. It was likely that the Fayallah 2011 study had high risk of attrition bias, as follow‐up of women was limited (see the Characteristics of included studies table).
3.
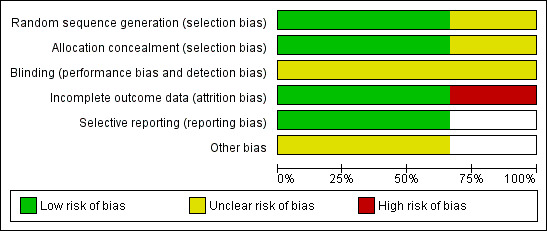
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
4.
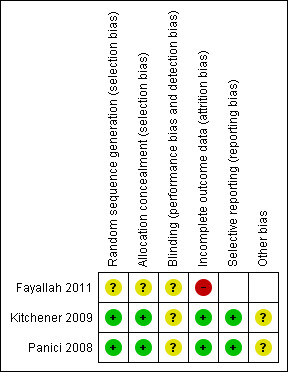
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
The Panici 2008 and Kitchener 2009 trials reported the method of generation of the sequence of random numbers used to allocate women to treatment arms and concealment of this allocation sequence from participants and healthcare professionals involved in the trials. Neither trial reported whether outcome assessors were blinded. It is highly likely that both trials reported all outcomes that they assessed, but it is not clear whether any other bias may have been present. At least 95% of women who were enrolled were assessed at endpoint in both trials.
Effects of interventions
See: Table 1
All meta‐analyses pooled data from two trials (Kitchener 2009; Panici 2008).
Meta‐analyses of survival were based on HRs that were adjusted for prognostic variables.
Overall survival
Meta‐analysis, assessing 1851 women, showed no differences in risk of death among women who underwent lymphadenectomy and those who did not undergo lymphadenectomy, after adjustment for important prognostic factors including age and tumour grade (HR 1.07, 95% CI 0.81 to 1.43; Analysis 1.1). The percentage of variability in effect estimates that was due to heterogeneity rather than to sampling error (chance) was not important (I2 = 0%). The Panici 2008 study reported no differences in five‐year overall survival among women who underwent lymphadenectomy and those who did not undergo lymphadenectomy in relation to age (HR 1.17, 95% CI 0.56 to 2.46 in those older than 65 years; HR 1.21, 95% CI 0.54 to 2.72 in those 65 years of age or younger), although no adjustment was made for other prognostic factors.
1.1. Analysis.
Comparison 1 Survival, Outcome 1 Overall survival.
The Fayallah 2011 study also reported no differences in overall survival between those who underwent pelvic lymphadenectomy and those who did not.
Recurrence‐free survival
Meta‐analysis, assessing 1851 women, showed no differences in risk of disease recurrence between women who underwent lymphadenectomy and those who did not undergo lymphadenectomy, after adjustment for important prognostic factors including age and tumour grade (HR 1.23, 95% CI 0.96 to 1.58; Analysis 1.2). The percentage of variability in effect estimates that was due to heterogeneity rather than to chance was not important (I2 = 0%).
1.2. Analysis.
Comparison 1 Survival, Outcome 2 Recurrence‐free survival.
Adverse events
Direct surgical morbidity
Meta‐analysis, assessing 1922 women, showed no differences in risk of direct surgical morbidity between women who underwent lymphadenectomy and those who did not undergo lymphadenectomy (RR 1.93, 95% CI 0.79 to 4.71; Analysis 2.1). The percentage of variability in effect estimates that was due to heterogeneity rather than to chance may represent moderate heterogeneity (I2 = 50%).
2.1. Analysis.

Comparison 2 Adverse events, Outcome 1 Direct surgical morbidity.
Surgery‐related systemic morbidity
Meta‐analysis of both trials, assessing 1922 women, showed that women given lymphadenectomy had higher risk of surgery‐related systemic morbidity than those not given lymphadenectomy (RR 3.72, 95% CI 1.04 to 13.27; Analysis 2.3). The percentage of variability in effect estimates that was due to heterogeneity rather than to chance was not important (I2 = 0%).
2.3. Analysis.
Comparison 2 Adverse events, Outcome 3 Surgery‐related systemic morbidity.
Lymphoedema or lymphocyst
Meta‐analysis, assessing 1922 women, revealed that women given lymphadenectomy had higher risk of lymphoedema or lymphocyst formation than those not given lymphadenectomy (RR 8.39, 95% CI 4.06 to 17.33; Analysis 2.2). The percentage of variability in effect estimates that was due to heterogeneity rather than to chance was not important (I2 = 0%).
2.2. Analysis.
Comparison 2 Adverse events, Outcome 2 Lymphoedema or lymphocyst.
Discussion
Summary of main results
We found three studies that met our inclusion criteria, but we were able to include only two of these in the meta‐analysis. The two studies included in the analysis (Kitchener 2009; Panici 2008) enrolled a total of 1945 women. These studies compared lymphadenectomy versus no lymphadenectomy in women with endometrial cancer that was thought on clinical grounds to be confined to the womb.
When we combined the findings from these two studies and adjusted for important prognostic factors, we found that risks of death and disease recurrence were no different among women who underwent lymphadenectomy than among those who did not (hazard ratio (HR) 1.07, 95% confidence interval (CI) 0.81 to 1.43; HR 1.23, 95% CI 0.96 to 1.58 for overall and recurrence‐free survival, respectively). Risk of adverse events was significantly higher in women who underwent lymphadenectomy (lymphoedema and lymphocyst formation; risk ratio (RR) 8.39, 95% CI 4.06 to 17.33).
The two studies included in the meta‐analysis had many strengths; HRs correctly allowed for censoring and provided information about adverse events. Both studies recruited a substantial number of women, and investigators observed a reasonably large number of events in the two survival outcomes and in the number of women with lymphoedema. Researchers reported no differences in overall or recurrence‐free survival in the two groups of women, but the risk of adverse events was consistently higher among women who underwent lymphadenectomy.
Overall completeness and applicability of evidence
We found no studies that randomly assessed pelvic lymph node sampling, sentinel lymph node biopsy, pelvic and para‐aortic lymphadenectomy, or removal of bulky pelvic lymph nodes.
Although we specified quality of life (QOL) as an outcome of interest, none of the trials reported this. QOL after treatment for cancer is an extremely important outcome, as treatment‐related morbidity very often degrades the quality of the time that patients continue to live. This is especially important for a condition that has relatively good survival rates.
Surgical treatment of endometrial cancer varies among hospitals, and before the Panici 2008 and Kitchener 2009 studies were published, no clear evidence indicated whether lymphadenectomy has a role in management at early stages of the disease. However, evidence from these RCTs suggests no clear benefit of radical treatment for women with early‐stage endometrial cancer.
Additional trials undertaken to assess lymphadenectomy for the management of endometrial cancer may test the robustness of the findings of this review, but evidence from two large included trials suggests that the true effect for the primary outcome (overall survival) may be close to the estimated effect, so it is questionable whether additional trials are justified in this area. A higher proportion of women appeared to be disease‐free in the lymphadenectomy group compared with the control group, but this finding was not statistically significant. Meta‐analyses in the review found no differences between lymphadenectomy and standard surgery in risk of death (HR 1.07, 95% CI 0.81 to 1.43; Analysis 1.1) or disease recurrence (HR 1.23, 95% CI 0.96 to 1.58; Analysis 1.2), and no differences in direct surgical morbidity (RR 1.93, 95% CI 0.79 to 4.71; Analysis 2.1), but more women experienced surgery‐related systemic morbidity (RR 3.72, 95% CI 1.04 to 13.27; Analysis 2.3) and lymphoedema or lymphocyst (RR 8.39, 95% CI 4.06 to 17.33; Analysis 2.2). According to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (GRADE Working Group 2004), the evidence summarised by this review is potentially adequate, and we are moderately confident in the effect estimates, but they could be substantially different (especially for recurrence‐free survival and adverse event outcomes).
Quality of the evidence
Overall, the evidence appears to be of moderate quality (GRADE Working Group 2004) for all outcomes of comparisons of lymphadenectomy versus control, with the exception of the presence or absence of lymphoedema or lymphocyst, which was graded as high‐quality evidence (Table 1). The quality of the evidence for primary outcomes overall and for recurrence‐free survival was moderate and was mainly downgraded from high‐quality evidence because of concerns regarding the degree of uncertainty in the pooled estimates, as indicated by the 95% confidence intervals and the imprecise estimates. Two trials (Kitchener 2009; Panici 2008) were at low overall risk of bias, and one trial (Fayallah 2011) was at unclear risk of bias but contributed no weight to the meta‐analyses and main findings of this review.
Both of the studies included in the meta‐analysis (Kitchener 2009; Panici 2008) had low risk of bias for concealment of the randomisation sequence from healthcare providers and participants. Inadequate concealment of allocation is often associated with overestimation of the effects of treatment (Moher 1998; Schulz 1995). However, blinding of outcome assessors was not reported in either study. Evidence on overall survival therefore is more robust than that for recurrence‐free survival, as blinding of outcome assessors is of less relevance for death than for disease progression.
Both trials reported the hazard ratio (HR), which is the best statistic for summarising differences in risk between two treatment groups over the duration of a trial when time to death or disease progression is 'censored' or unknown for some women, as they were still alive (or disease‐free) at the end of the trial.
The two studies provided consistent evidence about all outcomes, with the exception of direct surgical morbidity, for which the trial of Kitchener 2009 reported higher risk of direct surgical morbidity for women who underwent lymphadenectomy than for those who did not, whereas the trial of Panici 2008 found no differences.
Both studies randomly assigned women who were thought on clinical evidence to have disease confined to the uterus. However, the timing of randomisation varied: one was randomly assigned preoperatively (Kitchener 2009), and one following examination of the uterus at the time of surgery (Panici 2008). Another difference between the two studies was the median number of lymph nodes removed: 12 (range one to 59) in the Kitchener 2009 study and 26 (range 21 to 35) in the Panici 2008 study. However, despite this, five‐year disease‐free survival rates were similar, and a predefined subgroup analysis within Kitchener 2009 found a trend toward poorer survival when more lymph nodes were removed. One major difference between the studies was that Kitchener 2009 included low‐risk early‐stage participants (49% of the standard surgery group and 42% of the lymphadenectomy group), who were specifically excluded from Panici 2008, following examination of the uterus by frozen section intraoperatively. However, a predefined subgroup analysis within Kitchener 2009 revealed no evidence of a difference in the relative effect of lymphadenectomy (P = 0·55 for overall survival; P = 0·35 for recurrence‐free survival) when groups were stratified into low‐risk early‐stage disease, intermediate‐risk and high‐risk early‐stage disease, and advanced disease. From a clinical management perspective, routine use of whole uterine frozen section is not universally available and is resource‐intensive; in addition, as the two studies had similar outcomes in their high‐risk groups, this is unlikely to have had a major influence on the results.
Both trials permitted removal of suspicious lymph nodes in women allocated to no lymphadenectomy, at the discretion of the surgeon. Relatively small numbers of women in the control groups of each study had lymph nodes removed (35 women in Kitchener 2009; 56 women in Panici 2008), and this may cause some difficulty in interpretation of study results, but it would reflect clinical practice if lymphadenectomy was not standard treatment in the absence of suspicious lymph nodes.
Quality of life (QOL) was not reported in any of the trials, so we could not assess the quality of the evidence, which was very low for this outcome, but we could not report pertinent adverse events comprehensively.
We are moderately confident in the effect estimates in all analyses, but they could be substantially different (especially for recurrence‐free survival and adverse event outcomes).
Potential biases in the review process
We conducted a comprehensive search, including a thorough search of the grey literature, and three review authors independently sifted all studies and extracted data. We restricted included studies to randomised controlled trials (RCTs), as they provide the strongest level of evidence available. Hence, we have attempted to reduce bias in the review process.
The greatest threat to the validity of the review is likely to be the possibility of publication bias (i.e. studies that did not find the treatment to have been effective may not have been published). We were unable to assess this possibility, as we found only three included studies. However, as none of the studies reported differences between lymphadenectomy and no lymphadenectomy, publication bias seems unlikely.
Agreements and disagreements with other studies or reviews
A pooled HR for overall survival in the Kitchener 2009 and Panici 2008 studies was reported as 1.17 (95% CI 0.91 to 1.50) (Kitchener 2009a), which differs from the findings of this meta‐analysis (HR 1.07, 95% CI 0.81 to 1.43), in which combined data were adjusted for prognostic factors.
Previous studies and reviews have been based on data from non‐randomised studies. As discussed, some retrospective studies have demonstrated benefit from pelvic lymphadenectomy (Chan 2006; Kilgore 1995), whereas other studies have not (Trimble 1998; Van Lankveld 2006). Similarly, some retrospective studies have demonstrated benefit from pelvic and para‐aortic lymphadenectomy compared with pelvic lymphadenectomy alone (Todo 2010), whilst others have not (Tong 2011).
One retrospective review of 649 women with endometrial cancer found that women who underwent multiple‐site lymph node sampling had improved five‐year survival (extrapolated from survival curves) compared with women who underwent no pelvic node sampling (five‐year survival ˜90% vs ˜75%; P = 0.002) (Kilgore 1995). However, only disease‐specific survival was recorded, non‐endometrial cancer deaths were censored and no details were provided on participant characteristics, which are known to have a major influence on endometrial cancer survival (e.g. age, diabetes, cardiac comorbidity). Furthermore, retrospective population‐based studies demonstrated no survival advantage of lymphadenectomy (Van Lankveld 2006), or showed such an advantage only for women in high‐risk subgroups (high‐grade (G3) stage I disease who did undergo lymph node sampling) (five‐year relative survival for no node sampling 0.83 ± 0.05 (n = 497) versus 0.92 ± 0.04 (n = 553) for node sampling; P = 0.0110) (Trimble 1998).
Authors' conclusions
Implications for practice.
This review update does not alter the conclusions of the original review (May 2010); data do not support routine use of pelvic lymphadenectomy in the treatment of endometrial cancer thought to be confined to the uterus at presentation (presumed stage I disease). We found no differences in survival between groups, and, in relation to harmful effects of treatment, women who did not undergo lymphadenectomy showed clear benefit. We found no good quality data that assessed the role of para‐aortic lymphadenectomy, or removal of grossly enlarged lymph nodes. The two trials that contributed to the meta‐analyses were at low risk of bias, and the other trial was at unclear risk of bias.
Results demonstrating no benefit of routine lymphadenectomy in presumed early‐stage endometrial cancer are of interest and reflect results of RCTs that have examined the role of pelvic radiotherapy in treatment of these women (Kong 2012). In addition, we found no differences in patterns of recurrence between pelvic lymphadenectomy groups and standard surgery groups in the Kitchener 2009 study, which further supports the survival evidence that lymphadenectomy yields prognostic information only, rather than showing a direct therapeutic benefit. Although prognostic information is useful, these data reveal the real costs to patients associated with gathering this information and show that studies that do not look at the long‐term sequelae of lymphadenectomy do not allow women to make fully informed decisions about their health care.
Implications for research.
Important questions remain to be answered about the role of lymphadenectomy in endometrial cancer. However, neither this meta‐analysis of pelvic lymphadenectomy in early‐stage endometrial cancer nor the Cochrane review on radiotherapy for early‐stage endometrial cancer (Kong 2012) supports routine adjuvant treatment to pelvic nodes for early‐stage disease. The overall quality of the evidence was moderate across all outcomes (high‐quality evidence for the presence or absence of lymphoedema or lymphocyst outcome) and was downgraded because of concerns over imprecision of estimates.
Studies identified in this review examined pelvic lymphadenectomy. We were not able to identify any RCTs that assessed lymph node sampling or sentinel lymph node sampling, rather than systematic lymphadenectomy. Likewise, we found no RCTs that looked at differences between pelvic and para‐aortic lymph node removal. These interventions have been assessed by cohort studies but have yet to be assessed by RCTs. It is not known whether pelvic and para‐aortic lymph node dissection confers any benefit over pelvic lymphadenectomy alone, and the benefit demonstrated in the SEPAL study (Todo 2010) has yet to be replicated by an RCT. It is important to note that Kitchener 2009 and Panici 2008 data caution against the assumption that even more surgery will result in improved survival.
The studies included in this review primarily evaluated the impact of lymphadenectomy in early‐stage disease with low risk of recurrence; the role of lymphadenectomy in women with intermediate and high risk of disease recurrence has yet to be established by RCTs. Further research is underway to investigate the role of imaging technologies in the detection of lymph node metastasis in endometrial cancer (ISRCTN84527805); findings of this research may aid future researchers in evaluating the impact of lymphadenectomy among women with intermediate and high risk of disease recurrence.
The studies included in this review did not assess use of sentinel lymph node biopsy, which has the potential to improve staging whilst minimising surgical morbidity. When lymphadenectomy or lymph node sampling is not performed, use of adjuvant therapies is based on the pathological findings derived from surgical specimens. This may lead to inappropriate use, or omission, of adjuvant therapies. Use of sentinel lymph node biopsy may have a role in surgical staging. We recommend that data should be assessed by a Cochrane Diagnostic Test Accuracy review to determine whether the sentinel lymph node approach is valid in endometrial cancer. In addition, future versions of protocols for this review should include an assessment of the role of sentinel lymph node biopsy, if this is shown to be adequately sensitive to be used in an intervention trial.
Studies conducted to determine the role of adjuvant treatment in early‐stage cancer have highlighted that, for most women, simple surgery alone is sufficient to provide cure. Further research is needed to allow more individualised treatment strategies, ensuring that women with later‐stage or more aggressive cancers receive appropriate treatment, whilst not exposing women with a good prognosis to potentially serious lifelong side effects. In addition, the impact of any intervention on quality of life must be examined in future studies, particularly for cancer types with good survival rates.
What's new
| Date | Event | Description |
|---|---|---|
| 2 October 2017 | Amended | Author contact details amended. |
| 25 September 2017 | New search has been performed | New search March 2017 ‐ no new studies identified. |
| 25 September 2017 | New citation required but conclusions have not changed | Review revised but conclusions not changed. |
History
Protocol first published: Issue 1, 2009 Review first published: Issue 1, 2010
| Date | Event | Description |
|---|---|---|
| 29 June 2015 | New citation required but conclusions have not changed | Review updated |
| 23 June 2015 | New search has been performed | New study identified. Results unchanged as no data available to be added to the meta‐analysis |
Acknowledgements
We thank Chris Williams for providing clinical and editorial advice on the original protocol and review, Jane Hayes and Jo Platt for designing the search strategy and running the searches, Gail Quinn and Clare Jess for contributing to the editorial process, and the reviewers for providing helpful comments. We are grateful to Sean Kehoe and Heather Dickinson for providing assistance with the original version of this review.
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure, Cochrane Programme Grant or Cochrane Incentive funding to the Cochrane Gynaecological, Neuro‐oncology and Orphan Cancer Group. The views and opinions expressed therein are those of the review authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS, nor the Department of Health.
Appendices
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor Lymph Node Excision explode all trees #2 lymphadenectom* #3 (lymph NEAR node) NEAR/5 excision* #4 (lymph NEAR node) NEAR/5 dissection* #5 (lymph NEAR node) NEAR/5 surg* #6 (lymph NEAR node) NEAR/5 removal #7 (lymph NEAR node) NEAR/5 clearance #8 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7) #9 MeSH descriptor Endometrial Neoplasms explode all trees #10 endometr* NEAR/5 neoplas* #11 endometr* NEAR/5 carcinom* #12 endometr* NEAR/5 malignan* #13 endometr* NEAR/5 cancer* #14 endometr* NEAR/5 tumor* #15 endometr* NEAR/5 tumour* #16 (#9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15) #17 (#8 AND #16)
Appendix 2. MEDLINE search strategy
1 exp Lymph Node Excision/ 2 (lymph adj node adj5 (excision* or dissection* or surg* or removal or clearance)).mp. 3 lymphadenectom*.mp. 4 1 or 2 or 3 5 exp Endometrial Neoplasms/ 6 (endometr* adj5 (neoplas* or carcinom* or malignan* or cancer* or tumor* or tumour*)).mp. 7 5 or 6 8 randomized controlled trial.pt. 9 controlled clinical trial.pt. 10 randomized.ab. 11 randomly.ab. 12 trial.ab. 13 groups.ab. 14 8 or 9 or 10 or 11 or 12 or 13 15 4 and 7 and 14
Key:
mp=title, original title, abstract, name of substance word, subject heading word, pt=publication type, ab=abstract
Appendix 3. EMBASE search strategy
1 exp lymphadenectomy/ 2 (lymph adj node adj5 (excision* or dissection* or surg* or removal or clearance)).mp. 3 lymphadenectom*.mp. 4 1 or 2 or 3 5 exp endometrium tumor/ 6 (endometr* adj5 (neoplas* or carcinom* or malignan* or cancer* or tumor* or tumour*)).mp. 7 5 or 6 8 exp controlled clinical trial/ 9 randomized.ab. 10 randomly.ab. 11 trial.ab. 12 groups.ab. 13 8 or 9 or 10 or 11 or 12 14 4 and 7 and 13
Key
mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer name, ab=abstract
Appendix 4. Data abstraction form
Lymphadenectomy for the management of endometrial cancer
Paper ID:
Reviewer:
THE DATA COLLECTION CHECKLIST
April 2009
DATA COLLECTION
Once potentially relevant studies have been identified for a review, the following data should be extracted independently by two reviewers.
Please record your name and the Study ID (first author and year of publication) in the space provided on this page and on any page(s) that may be separated from the main checklist (e.g. Results section).
For all items, review authors should mark an X against the appropriate response in each case. In addition, it will be helpful if you cut and paste relevant supporting text and state its original location in the paper (page/column/paragraph). This facilitates later comparisons of extracted data. Any other comments can also be recorded in the right‐hand side boxes.
Data that are missing or ‘UNCLEAR’ in a published report should be marked clearly on the data collection form.
Items on the data extraction sheet that clearly are not applicable to the study in question should be marked accordingly (i.e. N/A).
After data extraction, review authors should compare their completed data extraction sheets and attempt to reach agreement for each item on the checklist before submitting their completed data records.
SCOPE OF REVIEW: INCLUSION/EXCLUSION CRITERIA
| Inclusion criteria | Yes/No/Unclear | Relevant supporting text and location (page/column/paragraph) |
| Were participants adult women diagnosed with endometrial cancer? | ||
Did the trial include at least 1 of the following comparisons?
|
||
|
Was the type of study design as described by the authors: Randomised controlled trial (RCT) Quasi‐randomised controlled trial (quasi‐RCT) |
||
| Exclusion criteria | ||
| Did the trial not include women with other concurrent malignancies? | ||
| Was the trial not cluster‐randomised, or was it not a cross‐over trial? | ||
| If any of the inclusion criteria are not satisfied andthe answer to any of the questions above is “NO”, the study should be excluded from the review. COLLECT NO FURTHER DATA | ||
| STUDY DETAILS | Relevant supporting text and location (page/column/paragraph) | |
|
Country: If multi‐centre, please give details Please state UNCLEAR if information is not available |
||
|
Setting: |
||
|
Duration: Indicate N/A as appropriate |
||
| Median length of follow‐up: | ||
| Mean length of follow‐up: | ||
| Min length of follow‐up: | ||
| Max length of follow‐up: | ||
| Additional information: |
| Baseline characteristics of participants | Relevant supporting text and location (page/column/paragraph) | |
| Age | Mean = Years SD = Median = Years Range: | |
| FIGO stage | Number (%) stage I: Number (%) stage II: Number (%) stage III: Number (%) stage IV: Number (%) unknown: |
|
| Grade | Number (%) grade I: Number (%) grade II: Number (%) grade III: Number (%) unknown: |
|
| Comorbidities | ||
| Previous treatment | |
|
| Additional information | |
ASSESSMENT OF RISK OF BIAS
|
Sequence generation Was the allocation sequence adequately generated? Describe in sufficient detail the method used to generate the allocation sequence to allow assessment of whether it should produce comparable groups |
Tick one row | Relevant supporting text and location (page/column/paragraph) |
| Yes e.g. a computer‐generated random sequence or a table of random numbers | ||
| No e.g. non‐randomised or quasi‐randomised (participants allocated on basis of date of birth, clinic ID number or surname) | ||
| Unclear insufficient information about the sequence generation | ||
|
ALLOCATION CONCEALMENT Was the randomisation sequence for allocating participants to different arms of the trial adequately concealed, to prevent both participants and clinicians providing treatment from predicting in advance to which arm of the trial a women would be assigned? |
||
| Yes e.g. when the allocation sequence could not be foretold | ||
| No e.g. allocation sequence could be foretold by participants, investigators or treatment providers | ||
| Unclear e.g. if use of assignment envelopes is described, but it remains unclear whether envelopes were sequentially numbered, opaque and sealed | ||
|
BLINDING OF OUTCOME ASSESSORS Were the clinicians who assessed disease progression at the end of follow‐up prevented from knowing to which arm of the trial the women were assigned? |
||
| Yes Outcome assessors were blinded | ||
| No No blinding or incomplete blinding of outcome assessors | ||
| Unclear Information was insufficient to permit judgement of ‘yes’ or ‘no’ |
| LOSS TO FOLLOW‐UP | Enter numbers below | Relevant supporting text and location (page/column/paragraph) |
| How many participants were enrolled in each treatment arm? Intervention group: Comparison group: | ||
| How many participants were assessed at the end of follow‐up in each treatment arm? Intervention group: Comparison group: | ||
| What % of participants were lost to follow‐up?
Intervention group:
Comparison group: Overall: |
||
| Now code satisfactory level of loss‐to‐follow‐up as Yes/No/Unclear: | Tick one row below | |
| Yes: if fewer than 20% of participants were lost to follow‐up and reasons for loss to follow‐up were similar in both treatment arms | ||
| No: if more than 20% of participants were lost to follow‐up or reasons for loss to follow‐up were different in different treatment arms | ||
| Unclear: If loss to follow‐up was not reported | ||
|
Selective reporting of outcomes: Are reports of the study free of the suggestion of selective outcome reporting? |
||
| Yes e.g. if review reports all outcomes specified in the protocol | ||
| No | ||
| Unclear | ||
|
Other potential threats to validity: Was the study apparently free of other problems that could put it at high risk of bias? |
||
| Yes | ||
| No | ||
| Unclear |
CHARACTERISTICS OF THE INTERVENTIONS
| Describe the intervention(s) for each study group. Report this in the words of the paper and give specific details if they are provided e.g. type of surgeon (gynaeoncologist, gynaecologist, general surgeon) and experience of surgeon, etc. | Location of text (page/column/paragraph) |
|
Intervention details: |
|
|
Comparison details: |
|
|
Did any women receive a different intervention from the one to which they were assigned? Yes/No/Unclear |
|
| If the answer to the question above is YES, record any reported changes in assigned treatment | |
|
Intervention: |
|
|
Comparison: |
|
|
If women received treatments different from those to which they were assigned, were outcomes reported in the groups to which they were assigned? Yes/No/Unclear |
| OUTCOMES | ||
| Overall survival | ||
| If the following were reported, record the value | Value | Relevant supporting text and location (page/column/paragraph) |
| Unadjusted hazard ratio (HR) Was the comparison group the reference group for the estimate of the HR? | Yes/No/Unclear | |
| 95% confidence on unadjusted HR Lower 95% confidence limit Upper 95% confidence limit | ||
| Adjusted hazard ratio (HR) Was the comparison group the reference group for the estimate of the HR? List the factors for which the HR was adjusted: | Yes/No/Unclear | |
| 95% confidence on adjusted HR Lower 95% confidence limit Upper 95% confidence limit | ||
| If an HR was reported, record the number of women in each treatment arm on whom the estimated HR was based: Number of women in intervention arm: Number of women in comparison arm: |
||
| If an HR was reported, and if the study was based on a prespecified protocol for assigning women to intervention group or comparison group, was the HR based on an intention‐to‐treat (ITT) analysis? i.e. were women analysed in the groups to which they were assigned, regardless of which treatment they received? | Yes/No/Unclear | |
| SE(HR) | ||
| SE(ln(HR)) | ||
| Var(HR) | ||
| Var(ln(HR)) | ||
| Kaplan‐Meier plots | Yes/No | |
| Minimum follow‐up time | ||
| Maximum follow‐up time | ||
| Log rank P value | ||
| Was Cox regression reported? | Yes/No | |
| Cox P value |
| OUTCOMES | ||
| Progression‐free survival | ||
| If the following were reported, record the value | Value | Relevant supporting text and location (page/column/paragraph) |
| Unadjusted hazard ratio (HR) Was the comparison group the reference group for the estimate of the HR? | Yes/No/Unclear | |
| 95% confidence on unadjusted HR Lower 95% confidence limit Upper 95% confidence limit | ||
| Adjusted hazard ratio (HR) Was the comparison group the reference group for the estimate of the HR? List the factors for which the HR was adjusted: | Yes/No/Unclear | |
| 95% confidence on adjusted HR Lower 95% confidence limit Upper 95% confidence limit | ||
| If an HR was reported, record the number of women in each treatment arm on whom the estimated HR was based Number of women in intervention arm: Number of women in comparison arm: |
||
| If an HR was reported, and if the study was based on a prespecified protocol for assigning women to intervention group or comparison group, was the HR based on an intention‐to‐treat (ITT) analysis? i.e. were women analysed in the groups to which they were assigned, regardless of which treatment they received? | Yes/No/Unclear | |
| SE(HR) | ||
| SE(ln(HR)) | ||
| Var(HR) | ||
| Var(ln(HR)) | ||
| Kaplan‐Meier plots | Yes/No | |
| Minimum follow‐up time | ||
| Maximum follow‐up time | ||
| Log rank P value | ||
| Was Cox regression reported? | Yes/No | |
| Cox P value |
| Intervention group | Comparison group | Location of text (page/column/paragraph) | |
| Total number of women enrolled in study | |||
| For women enrolled in comparison of intervention/comparison treatment | |||
| Number of women enrolled | |||
| Number (%) of women who died | |||
| Number of women whose vital status was known | |||
| Time point at which death was recorded e.g. 1 year/5 years/end of study/not reported | |||
| Median time to death: | |||
| Mean (SD) time to death: | |||
| Intervention group | Comparison group | Location of text (page/column/paragraph) | |
| Number (%) of women with disease progression | |||
| Number of women whose disease was assessed | |||
| Time point at which disease progression was recorded e.g. 1 year/5 years/end of study/not reported | |||
| Median time to disease progression: | |||
| Mean (SD) time to disease progression: | |||
|
Quality of life outcome State ‘not reported’ if not given |
Response | Relevant supporting text and location (page/column/paragraph) |
| Validated scale Yes/No | ||
| Name of scale | ||
| Intervention group: Mean QOL at end of follow‐up SD of QOL at end of follow‐up Number of women assessed for QOL at end of follow‐up |
||
| Comparison group: Mean QOL at end of follow‐up SD of QOL at end of follow‐up Number of women assessed for QOL at end of follow‐up |
| Adverse events | Number | ||
| Intervention group | Comparison group | Location of text (page/column/paragraph) | |
|
Direct surgical morbidity (e.g. injury to bladder, ureter, vascular, small bowel or colon), presence and complications of adhesions, febrile morbidity, intestinal obstruction, haematoma, local infection) List below the specific types and numbers of adverse events reported | |||
|
Surgery‐related systemic morbidity (chest infection, thromboembolic events (deep vein thrombosis and pulmonary embolism), cardiac events (cardiac ischaemias and cardiac failure), cerebrovascular accident List below the specific types and numbers of adverse events reported | |||
|
Recovery: delayed discharge, unscheduled re‐admission List below the specific types and numbers of adverse events reported | |||
|
Lymphoedema and lymphocyst formation List below the specific types and numbers of adverse events reported | |||
|
Other side effects not categorised above List below the severity of bleeding and numbers of adverse events reported | |||
| Does the number of adverse events reported above refer to the number of women who experienced adverse events or to the number of episodes of adverse events? | Number of women/Number of episodes | ||
Data and analyses
Comparison 1. Survival.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall survival | 2 | 1851 | Hazard Ratio (Random, 95% CI) | 1.07 [0.81, 1.43] |
| 2 Recurrence‐free survival | 2 | 1851 | Hazard Ratio (Random, 95% CI) | 1.23 [0.96, 1.58] |
Comparison 2. Adverse events.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Direct surgical morbidity | 2 | 1922 | Risk Ratio (IV, Random, 95% CI) | 1.93 [0.79, 4.71] |
| 2 Lymphoedema or lymphocyst | 2 | 1922 | Risk Ratio (IV, Random, 95% CI) | 8.39 [4.06, 17.33] |
| 3 Surgery‐related systemic morbidity | 2 | 1922 | Risk Ratio (IV, Random, 95% CI) | 3.72 [1.04, 13.27] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Fayallah 2011.
| Methods | Single‐centre RCT randomly assigning participants from a university hospital in Egypt | |
| Participants | 38 women with histologically proven endometrial carcinoma thought to be International Federation of Gynecology and Obstetrics stage I Women recruited between April 2005 and October 2008 were randomly assigned preoperatively to undergo extra fascial hysterectomy, bilateral salpingo‐oophorectomy with pelvic lymphadenectomy (iliac and obturator lymph nodes) (n = 21) or extrafascial hysterectomy and bilateral salpingo‐oophorectomy alone (n = 17). Before surgery, immunohistochemistry was carried out on endometrial tissue for detection of P53 overexpression. A total of 30 (79%) women had FIGO surgical stage I disease, four (11%) had stage II and four (11%) stage III disease. Depth of invasion was as follows: endometrium only 6 (16%); inner half of myometrium 17 (45%); and outer half of myometrium or further 15 (39%). Histological cell types were as follows: endometrioid 29 (80%); adenocarcinoma NOS 4 (11%); and papillary serous 5 (13%). Tumour grade was as follows: 14 (37%) had tumour grade 1; 16 (42%) grade 2; and 8 (21%) grade 3 No significant difference was noted between arms in terms of age, medical status, surgical stage, histological type, or grade of tumour. The number of nodes removed from participants in either arm was not reported, although the overall number of nodes removed on each pelvic side was reported as ranging from 6 to 14 After surgery, adjuvant radiotherapy was provided at the discretion of tumour board members. Women were followed up every 3 months with clinical assessment and ultrasound and underwent an MRI every 6 months |
|
| Interventions |
Intervention Extrafascial hysterectomy with bilateral salpingo‐oophorectomy combined with pelvic lymphadenectomy involving common iliac, external iliac and obturator lymph node dissection Comparison Extrafascial hysterectomy with bilateral salpingo‐oophorectomy alone |
|
| Outcomes | Overall survival Recurrence rate |
|
| Notes | Mean duration of follow‐up was 21.5 months (range 6 to 40) Outcomes of overall survival and recurrence rate were based on the number of participants known to have died or in whom the disease was known to have progressed, rather than knowledge of survival and recurrence status among study participants |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Mean follow‐up duration from treatment was 21.5 months (range 6 to 40 months); no other information regarding attrition was given |
Kitchener 2009.
| Methods | Multi‐centre RCT randomly assigning participants from 85 centres in 4 countries (UK, South Africa, Poland, and New Zealand) | |
| Participants | 1408 women with histologically proven endometrial carcinoma thought preoperatively to be confined to the corpus Median age at the time of randomisation was 63 years (range 36 to 89) for standard surgery and 63 years (range 34 to 93) for lymphadenectomy Time from diagnosis to random assignment was ≤ 6 weeks for 576 (82%) women in the standard surgery group vs 588 (84%) in the lymphadenectomy arm and > 6 weeks for 128 (18%) women in the standard surgery group vs 116 (16%) in the lymphadenectomy arm 1057 participants (75%) had WHO performance status 0; 295 (21%) had status 1; 45 (3%) status 2; 9 (1%) status 3; and 2 (0%) status 4, similarly spread between the 2 groups 650 (92%) women underwent open surgery and 54 (8%) underwent laparoscopic surgery in the standard surgery group vs 659 (94%) open and 45 (6%) laparoscopic in the lymphadenectomy group Baseline characteristics below excluded participants whose pathology details did not confirm endometrial cancer: 39 women (21 standard surgery group, 18 lymphadenectomy group) who had no other tumour in the surgical specimen; atypical hyperplasia; or cervical, ovarian, or colorectal cancer Tumour was confined to the corpus uteri in 1091 (80%) women and spread beyond the corpus in 274 (20%) women: 553 (81%) standard surgery; 538 (79%) lymphadenectomy Depth of invasion was as follows for standard surgery: endometrium only 96 (14%); inner half of myometrium 369 (55%); outer half of myometrium 212 (31%): unknown 6 (0.9%) Depth of invasion was as follows for lymphadenectomy: endometrium only 89 (13%); inner half of myometrium 310 (46%); outer half of myometrium 274 (41%): unknown 13 (1.9%) FIGO staging (pre‐2009): Stage IIIC was not included, and women with positive lymph nodes were classified irrespective of nodal status. In the standard surgery group, 553 participants (81%) were stage I according to FIGO, 86 (13%) were stage II and 38 (5.6%) were stage III or IV. FIGO stage was unknown in 6 (0.9%) participants. In the lymphadenectomy group, 532 participants (78%) were stage I according to FIGO, 91 (13%) were stage II and 52 (7.5%) were stage III or IV. FIGO stage was unknown in 11 (1.6%) participants Histological cell types were as follows for standard surgery vs lymphadenectomy: endometrioid 545 (80%) vs 541 (79%); adenocarcinoma NOS 46 (7%) vs 37 (5%); clear cell 10 (1%) vs 17 (2%); serous 21 (3%) vs 32 (5%); squamous 6 (1%) vs 5 (1%); mucinous 1 (< 1%) vs 4 (1%); mixed epithelial stromal 7 (1%) vs 8 (1%); sarcoma 10 (1%) vs 9 (1%); other epithelial 4 (1%) vs 6 (1%); mixed epithelial 31 (5%) vs 25 (4%); unknown 2 (0.5%) in both groups Tumour grade was as follows for standard surgery vs lymphadenectomy: 225 women (33%) vs 213 (31%) had tumour grade 1; 300 (44%) vs 290 (43%) grade 2; 139 (20%) vs 158 (23%) grade 3; and in 19 (3%) vs 25 (4%) women, tumour grade was unknown or was not applicable Of the 1403 women who completed surgery, surgical technique used in the standard surgery group was as follows: laparoscopic 42 (6%); vertical incision 287 (45%); Pfannenstiel incision 311 (49%); other transverse 43 (7%); unknown 6. Surgical technique used in the lymphadenectomy group was as follows: laparoscopic 45 (6%); vertical incision 384 (60%); Pfannenstiel incision 208 (32%); other transverse 49 (8%); unknown 7. Five women (2 standard surgery; 3 lymphadenectomy) did not undergo completed surgery |
|
| Interventions |
Intervention Lymphadenectomy: Women in the lymphadenectomy group had standard surgery plus a systematic dissection of the iliac and obturator nodes. If the nodes could not be dissected thoroughly because of obesity or anaesthetic concerns, sampling of suspect nodes was recommended and para‐aortic node sampling was done at the discretion of the surgeon Comparison Standard surgery: Women in the standard surgery group had a hysterectomy and BSO, peritoneal washings and palpation of para‐aortic nodes. Nodes that were suspicious could be sampled if the surgeon believed this to be in the woman’s best interest |
|
| Outcomes | Overall survival Recurrence‐free survival Surgical complications |
|
| Notes | Median duration of follow‐up was 37 months (IQR 24 to 58 months) Specialist gynaecological surgeons who were experienced in pelvic lymphadenectomy undertook all surgical procedures 69 women in the lymphadenectomy group received a different intervention from the intervention to which they were assigned: 3 women had no surgery, 2 had subtotal hysterectomy, 6 women were given unknown intervention and 58 (8%) had no nodes taken In the standard surgery group, 2 had no surgery, 6 had subtotal hysterectomy, 11 were given unknown intervention and 35 (5%) had nodes taken No adjuvant radiotherapy was received by 471 (67%) in the standard surgery group and by 469 (67%) in the lymphadenectomy group |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “We used a method of minimisation. Stratification factors were centre, WHO performance status (0‐1 versus 2 to 4), time since diagnosis (<= 6 weeks versus > 6 weeks), and planned surgical approach (open versus laparoscopic)” Minimisation is a method that attempts to randomly assign while at the same time balancing groups for several prognostic variables, so the method of sequence generation was adequate in this trial |
| Allocation concealment (selection bias) | Low risk | “Randomisation was done by a telephone call to the Medical Research Council Clinical Trials Unit (MRC CTU)” |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | For multivariate Cox model: % analysed: 1337/1408 (95%) |
| Selective reporting (reporting bias) | Low risk | All important survival and adverse event outcomes have been reported. Survival outcomes have been analysed using appropriate statistical techniques to account for censoring |
| Other bias | Unclear risk | Information was insufficient for assessment of whether an important risk of bias existed |
Panici 2008.
| Methods | Multicentre RCT randomly assigning participants from Italy and Chile | |
| Participants | Women with preoperative International Federation of Gynecology and Obstetrics stage I endometrial carcinoma Median age at time of random assignment was 62 years (IQR 56 to 68): standard surgery 63 (IQR 55 to 68); lymphadenectomy 63 (IQR 56 to 68) 386 participants (75%) were stage I according to FIGO (standard surgery 195 (78%); lymphadenectomy 191 (72%)); 43 (8%) were stage II (standard surgery 21 (8%); lymphadenectomy 22(8%)); 71 (14%) were stage III (standard surgery 27 (11%); lymphadenectomy 44 (17%)); and 6 (1%) were stage IV (standard surgery 3 (1%); lymphadenectomy 3 (1%)). FIGO stage was unknown in 8 (2%) participants (2 in each group) Histological cell types were similar between the 2 groups and were as follows: endometrioid 474 (92%); adenosquamous 33 (6.4%); clear cell 1 (0%); serous 3 (0.6%); mullerian mixed malignant tumour 2 (0.4); tumour not found 1 (0%) 38 women (7%) had tumour grade 1 (standard surgery 19 (8%); lymphadenectomy 19 (7%)); 298 (58%) grade 2 (standard surgery 148 (59%); lymphadenectomy 150 (57%)); 169 grade 3 (33%) (standard surgery 78 (31%); lymphadenectomy 91 (35%)); and in 9 (2%) women, tumour grade was unknown (standard surgery 5 (2%); lymphadenectomy 4 (1.5%)) |
|
| Interventions | For both lymphadenectomy and no‐lymphadenectomy arms, primary surgery included standard hysterectomy with bilateral salpingo‐oophorectomy Intervention Lymphadenectomy group underwent external/common iliac and superficial obturator node dissection. Systematic/para‐aortic lymphadenectomy was performed at surgeon's discretion Comparison Removal of bulky (> 1 cm) nodes at surgeon's discretion in no lymphadenectomy arm |
|
| Outcomes | Overall survival Disease‐free survival (defined as time from random assignment to earliest occurrence of relapse or death from any cause) Severe intraoperative complications Postoperative complications |
|
| Notes | Median duration of follow‐up was 49 months (IQR 27 to 79 months) 38 women in the lymphadenectomy group had fewer than 20 nodes resected In the standard surgery group, 56 women (22%) underwent lymph node sampling/removal, and 17 had 20 or more pelvic lymph nodes resected Para‐aortic lymphadenectomy was performed in 69 (26%) of the 264 participants in the lymphadenectomy group and in 5 (2%) in the standard surgery group Adjuvant treatment (chemotherapy and radiotherapy) did not vary significantly between the 2 arms (no adjuvant therapy in 182 (69%) of the lymphadenectomy group and in 162 (65%) of the standard surgery group) (P = 0.07) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Patients were randomly assigned to one of the two trial arms by a block arrangement that balanced the treatment assignment within each site” |
| Allocation concealment (selection bias) | Low risk | “Intraoperative random assignment was performed centrally by telephone at the Mario Negri Institute, Milan” |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | For all outcomes: % analysed: 514/537 (96%) By treatment arm: Intervention: 264/273 (97%) Comparison: 250/264 (95%) |
| Selective reporting (reporting bias) | Low risk | All important survival and adverse event outcomes have been reported. Survival outcomes have been analysed using appropriate statistical techniques to account for censoring |
| Other bias | Unclear risk | Information was insufficient for assessment of whether an important risk of bias existed |
BSO ‐ IQR ‐ interquartile range FIGO ‐ International Federation of Gynaecology and Obstetrics MRI ‐ Magnetic resonance imaging NOS ‐ Not otherwise stated RCT ‐ Randomised controlled trial WHO ‐ World Health Organization
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Angoli 2013 | Retrospective review; comparison of lymphadenectomy vs no lymphadenectomy; quality of life assessment |
| Ansari 2013 | Systematic review and meta analysis ‐ no additional RCT evidence found |
| Babilonti 1989 | Retrospective review; comparison of lymphadenectomy vs no lymphadenectomy; examination of short‐term complications |
| Barton 2009 | Narrative review article only ‐ no additional RCT evidence found |
| Bogani 2014 | Narrative review article ‐ no additional RCT evidence found |
| Chan 2006 | Retrospective case review |
| Crosbie 2012 | Incorrect comparator ‐ analysis by body mass index only |
| Fujimoto 2009 | Narrative evaluation of RCT only; no primary data |
| Gao 2013 | Retrospective case review |
| Havrilesky 2013 | Review of study methods only |
| Hofstetter 2014 | Retrospective case review |
| Huh 2008 | All participants underwent lymph node dissection. Study randomly assigned processing of samples |
| Kang 2009 | Retrospective study ‐ no lymphadenectomy randomly assigned |
| Kim 2012 | Systematic review ‐ no additional RCT evidence found |
| Kitchener 2011 | No additional information by relevant comparator |
| Kitchener 2013 | Narrative review article ‐ no additional RCT evidence found |
| Kyrgiou 2013 | Incorrect interventional comparator |
| Kyrgiou 2013a | Incorrect interventional comparator |
| Lamela 2013 | Incorrect interventional comparator |
| Look 2004 | Systematic review ‐ no additional RCT evidence found |
| Mannel 1989 | Retrospective study ‐ no lymphadenectomy randomly assigned |
| Mariani 2000 | Retrospective study |
| Mosgaard 2013 | Incorrect study intervention |
| Nahhas 1980 | Retrospective review of treatment of individuals with stage II endometrial cancer with no randomisation |
| Obermair 2012 | Incorrect study intervention |
| Poll‐Franse 2012 | Retrospective non‐randomised study assessing health‐related quality of life |
| Puente 2011 | Retrospective non‐randomised study |
| Quinn 1993 | Randomised controlled trial of progesterone therapy for high‐risk endometrial cancer ‐ no surgical randomisation. Comparison of outcomes of 238 women who underwent pelvic lymphadenectomy vs 774 women who did not under pelvic lymphadenectomy. Women who underwent lymphadenectomy were younger and showed less myometrial invasion. Longer overall survival in women with lymphadenectomy. No differences in patterns of recurrence |
| Rodolakis 2012 | Retrospective non‐randomised study |
| Rossi 2013 | Incorrect study design |
| Rossi 2014 | Incorrect study intervention |
| Rubin 1990 | Retrospective non‐randomised study |
| Salvesen 2001 | Systematic review of role of lymphadenectomy in gynaecological malignancies ‐ no RCT or endometrial cancer found |
| Schulz 1986 | RCT of adjuvant hormonal therapy after surgery for endometrial cancer |
| Shan 2013 | Incorrect study design |
| Tinelli 2009 | Narrative review article ‐ no additional RCT evidence found |
| Tong 2011 | Retrospective case review |
| Trovik 2013 | Incorrect study intervention |
| Turkler 2013 | Retrospective non‐randomised study |
| Watari 2014 | Narrative review article ‐ no additional RCT evidence found |
| Zapico 2013 | Incorrect study intervention |
Differences between protocol and review
In addition to methods described in the protocol, we used the GRADE approach to define the quality of the evidence and the extent to which we can be confident that an estimate of effect or association is free from bias.
In the most recent update of the review in 2017, as the first step of screening, we applied the machine learning classifier (RCT model) available in the Cochrane Register of Studies (CRS‐web; Wallace 2017). The classifier assigns a probability (from 0 to 100) to each citation for being a true RCT. For citations that are assigned a probability score of less than 10, the machine learning classifier currently has a specificity/recall of 99.987% (James Thomas, personal communication). For citations assigned a score from 10 to 100, we screened them independently and in duplicate using Covidence on‐line software (Covidence).
The following methods were specified in the protocol but were not implemented, as we found only three trials that met our inclusion criteria, only two of which could be included in the meta‐analysis. Both trials included in the meta‐analysis reported HRs, so we did not need to estimate RRs. Neither trial reported continuous outcomes such as quality of life and neither included multiple treatment groups. Both trials were at low risk of bias, so we did not conduct sensitivity analysis around quality. However, the methods specified below may be required when this review is next updated.
Measures of treatment effect
If it is not possible to estimate the HR, we will abstract the number of participants in each treatment arm who experienced the outcome of interest and the number of participants assessed, to estimate a risk ratio (RR).
For continuous outcomes (QOL measures), we will abstract the final value and the standard deviation of the outcome of interest in each treatment arm at the end of follow‐up for each study, if available.
For dichotomous and continuous data, we will extract the number of participants assessed at endpoint.
Assessment of reporting biases
We will examine funnel plots corresponding to meta‐analyses of the primary outcome to assess the potential for small‐study effects such as publication bias. If these plots suggest that treatment effects may not be sampled from a symmetrical distribution, as assumed by the random‐effects model, we will perform further meta‐analyses using the fixed‐effect model.
Data synthesis
For continuous outcomes (e.g. QOL measures), we will pool mean differences between treatment arms at the end of follow‐up, if all trials measured outcomes on the same scale; otherwise we will pool standardised mean differences.
If any trials include multiple treatment groups, we will divide the ‘shared’ comparison group into single treatment groups, and we will treat comparisons between treatment groups and the split comparison group as independent comparisons.
If possible, we will synthesise studies making different comparisons by using the subgroup methods of Bucher 1997.
Subgroup analysis and investigation of heterogeneity
We will perform subgroup analyses by grouping the trials by:
early‐stage disease low‐risk participants (stage IA‐B, G1 or G2) versus high‐risk participants (stage IB, G3 or stage IC or higher, any grade); or
no obvious lymph node enlargement versus lymph node enlargement.
We will consider factors such as age, stage, type of intervention, length of follow‐up, and adjusted/unadjusted analysis when interpreting any heterogeneity.
Sensitivity analysis
We will perform sensitivity analyses that exclude studies at high risk of bias.
Contributions of authors
JF and JM contributed equally to the review update. The protocol was originally developed by JM, KW, HD, and AB. JF, KW, AB, and JM sifted references, and KW, JF, and AB extracted data, which were checked by JM. AB, JF, and JM co‐wrote the results and conclusions of the review with input from KW.
Sources of support
Internal sources
No sources of support supplied
External sources
-
Department of Health, UK.
NHS Cochrane Collaboration programme Grant Scheme CPG‐506
Declarations of interest
Jonathan Frost ‐ none known Katie Webster ‐ none known Jo Morrsion ‐ none known Andrew Bryant ‐ none known
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Fayallah 2011 {published data only}
- Fayallah EA, Hemida RA, Gamal AM, Abd Elhady E, Anwar KI, Nada NA, et al. Pretreatment study of P53 overexpression for selection of candidates for pelvic lymphadenectomy in clinical stage I endometrial carcinoma: a randomized‐controlled study. Archives of Gynecology and Obstetrics 2011;283(3):617‐22. [DOI] [PubMed] [Google Scholar]
Kitchener 2009 {published data only}
- Kitchener H. ASTEC ‐ A study in the treatment of endometrial cancer: a randomised trial of lymphadenectomy in the treatment of endometrial cancer. Gynecologic Oncology 2006;101(1 Suppl 1):S21‐2, Abstract 45. [Google Scholar]
- Kitchener H, Swart AM, Qian Q, Amos C, Parmar MK. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): a randomised study. Lancet 2009;373(9658):125‐36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kitchener HC, Redman CW, Swart AMC, Amos CL. Astec (Surgery Component): a study in the treatment of endometrial cancer: a randomised trial of lymphadenectomy in the treatment of endometrial cancer (ISRCTN 16571884): 00094. International Journal of Gynecological Cancer 2005;15:77. [Google Scholar]
Panici 2008 {published data only}
- Panici PB, Basile S, Maneschi F, Alberto Lissoni A, Signorelli M, Scambia G, et al. Systematic pelvic lymphadenectomy vs. no lymphadenectomy in early‐stage endometrial carcinoma: randomized clinical trial. Journal of the National Cancer Institute 2008;100(23):1707‐16. [DOI] [PubMed] [Google Scholar]
- Panici PB, Basile S, Salerno MG, Donato V, Marchetti C, Perniola G, et al. Secondary analyses from a randomized clinical trial: age as the key prognostic factor in endometrial carcinoma. American Journal of Obstetrics & Gynecology 2014;210:363e1‐363e10. [DOI] [PubMed] [Google Scholar]
- Panici PB, Frigerio L, Sardi J, Campagnutta E, Scambia G, Tateo S, et al. Feasibility and complications of systematic lymphadenectomy in endometrial cancer. preliminary results of a prospective randomized multicentric clinical trial. International Journal of Gynecological Cancer 1999;9:88‐9. [Google Scholar]
- Panici PB, Maneschi F, Cutillo G. Pelvic and aortic lymphadenectomy. Surgical Clinics of North America 2001;81(4):841‐58. [DOI] [PubMed] [Google Scholar]
- Panici PB, Tateo S, Mangili G, Scambia G, Garozzo G, Pelusi G, et al. Complications of lymphadenectomy in endometrial cancer. results of a prospective randomized multicentric clinical trial. International Journal of Gynecological Cancer 2004;14:6. [Google Scholar]
References to studies excluded from this review
Angoli 2013 {published data only}
- Angoli R, Plotti F, Cafa E, Dugo N, Caprigione S, Corrado T, et al. Quality of life in patients with endometrial cancer treated with or without systematic lymphadenectomy. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2013;170:539‐43. [DOI] [PubMed] [Google Scholar]
Ansari 2013 {published data only}
- Ansari M, Ghodsi Rad MA, Hassanzadeh M, Gholami H, Yousefi Z, Dabbagh VR, et al. Sentinel node biopsy in endometrial cancer: systematic review and meta‐analysis of the literature. European Journal of Gynaecological Oncology 2013;34:387‐401. [PubMed] [Google Scholar]
Babilonti 1989 {published data only}
- Babilonti L, Pietro G, Fianza A, Beretta P, Franchi M. Complications of pelvic lymphadenectomy in patients with endometrial adenocarcinoma. European Journal of Gynaecological Oncology 1989;10(2):131‐3. [PubMed] [Google Scholar]
Barton 2009 {published data only}
- Barton DP, Naik R, Herod J. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC Trial): a randomized study. International Journal of Gynaecological Cancer 2009;19(8):1465. [DOI] [PubMed] [Google Scholar]
Bogani 2014 {published data only}
- Bogani G, Dowdy SC, Cliby WA, Ghezzi F, Rossetti D, Mariani A. Role of pelvic and para‐aortic lymphadenectomy in endometrial cancer: current evidence. Journal of Obstetrics and Gynaecology Research 2014;40:301‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chan 2006 {published data only}
- Chan JK, Cheung MK, Huh WK, Osann K, Husain A, Teng NN, et al. Therapeutic role of lymph node resection in endometrioid corpus cancer: a study of 12,333 patients. Cancer 2006;107(6):1823‐30. [DOI] [PubMed] [Google Scholar]
Crosbie 2012 {published data only}
- Crosbie EJ, Roberts C, Qian W, Swart AM, Kitchener HC, Renehan AG. Body mass index does not influence post‐treatment survival in early stage endometrial cancer: results from the MRC ASTEC trial. European Journal of Cancer 2012;48(6):853–64. [DOI] [PubMed] [Google Scholar]
Fujimoto 2009 {published data only}
- Fujimoto T, Tanaka T. Evaluation of the efficacy of systematic pelvic lymphadenectomy in endometrial cancer. Future Oncology 2009;5(4):459‐63. [DOI] [PubMed] [Google Scholar]
Gao 2013 {published data only}
- Gao M, Gao YN, Yan X, Zheng H, Jiang GQ, Wang W, et al. Evaluation of complications of different operation modes in endometrial cancer. Chinese Journal of Oncology 2013;35:932‐5. [PubMed] [Google Scholar]
Havrilesky 2013 {published data only}
- Havrilesky LJ, Chino JP, Myers ER. How much is another randomized trial of lymph node dissection in endometrial cancer worth? A value of information analysis. Gynecologic Oncology 2013;131:140‐6. [DOI] [PubMed] [Google Scholar]
Hofstetter 2014 {published data only}
- Hofstetter G, Alektiar K, Leitao MM, Hensley ML, Soslow RA, Zivanovic O, et al. Does removal of a positive sentinel node without lymphadenectomy impact pelvic sidewall control in endometrial cancer?. Gynecologic Oncology 2014;Suppl 1:193‐4. [Google Scholar]
Huh 2008 {published data only}
- Huh WK, Crim A, Petro KN, Irons AE, Samples KL, Alvarez RD, et al. Specimen labelling and processing impacts pelvic lymph node yield: results of a randomized controlled trial. Gynecologic Oncology 2008;108(3 Suppl 1):S64, Abstract 143. [Google Scholar]
Kang 2009 {published data only}
- Kang WD, Kim CH, Cho MK, Kim JW, Kim YH, Choi HS, et al. Lymphadenectomy for low‐risk endometrial cancer based on preoperative and intraoperative assessments. International Journal of Gynecological Cancer 2009;19(4):657‐61. [DOI] [PubMed] [Google Scholar]
Kim 2012 {published data only}
- Kim HS, Suh DH, Kim MK, Chung HH, Park NH, Song YS. Systematic lymphadenectomy for survival in patients with endometrial cancer: a meta‐analysis. Japanese Journal of Clinical Oncology 2012;42(5):405‐12. [DOI] [PubMed] [Google Scholar]
Kitchener 2011 {published data only}
- Kitchener H. The effect of incision in the surgical treatment of endometrial cancer and long‐term follow‐up of a randomized trial of lymphadenectomy: results of the MRC ASTEC trial. Journal of Clinical Oncology 2011;29(Suppl):e15583. [Google Scholar]
Kitchener 2013 {published data only}
- Kitchener H. Lymphadenectomy for endometrial cancer. Why we still need a trial. International Journal of Gynecological Cancer 2013;23(Suppl 1):19. [Google Scholar]
Kyrgiou 2013 {published data only}
- Kyrgiou M, Warwick J, Swart AM, Qian W, Ghaem‐Maghami S, Kitchener H. Laparoscopic versus open hysterectomy for endometrial cancer: the ASTEC trial. Reproductive Sciences 2013:339A. [Google Scholar]
Kyrgiou 2013a {published data only}
- Kyrgiou M, Warwick J, Swart AM, Qian W, Ghaem‐Maghami S, Kitchener H. Laparoscopic versus open hysterectomy for endometrial cancer: the ASTEC trial. Reproductive Sciences 2013;20(3 Suppl):339A. [Google Scholar]
Lamela 2013 {published data only}
- Lamela EM, Jesus MV, Veronica SM, Carmen GP, Yolanda EL, Teresa RR. Complications and long‐term results after laparoscopy for stage endometrial cancer. Gynecological Surgery 2013;10(Suppl 1):S57. [Google Scholar]
Look 2004 {published data only}
- Look KY. Role of lymphadenectomy in management of adenocarcinoma of the endometrium. European Journal of Gynaecological Oncology 2004;25(5):545‐51. [PubMed] [Google Scholar]
Mannel 1989 {published data only}
- Mannel RS, Berman ML, Walker JL, Disaia PJ. Initial surgical therapy in the management of clinical stage II endometrial cancer. Gynecologic Oncology 1989;32(1):105. [Google Scholar]
Mariani 2000 {published data only}
- Mariani A, Webb MJ, Galli L, Podratz KC. Potential therapeutic role of para‐aortic lymphadenectomy in node‐positive endometrial cancer. Gynecologic Oncology 2000;76(3):348‐56. [DOI] [PubMed] [Google Scholar]
Mosgaard 2013 {published data only}
- Mosgaard BJ, Skovlund VR, Hendel HW. Promising results using sentinel node biopsy as a substitute for radical lymphadenectomy in endometrial cancer staging. Danish Medical Journal 2013;60(7):A4665. [PubMed] [Google Scholar]
Nahhas 1980 {published data only}
- Nahhas WA, Whitney CW, Stryker JA, Curry SL, Chung CK, Mortel R. Stage II endometrial carcinoma. Gynecologic Oncology 1980;10(3):303‐11. [DOI] [PubMed] [Google Scholar]
Obermair 2012 {published data only}
- Obermair A, Janda M, Baker J, Kondalsamy‐Chennakesavan S, Brand A, Hogg R, et al. Improved surgical safety after laparoscopic compared to open surgery for apparent early stage endometrial cancer: results from a randomised controlled trial. European Journal of Cancer 2012;48:1147‐53. [DOI] [PubMed] [Google Scholar]
Poll‐Franse 2012 {published data only}
- Poll‐Franse LV, Pijnenborg JM, Boll D, Vos MC, Berg H, Lybeert ML, et al. Health related quality of life and symptoms after pelvic lymphadenectomy or radiotherapy vs. no adjuvant regional treatment in early‐stage endometrial carcinoma: a large population‐based study. Gynecologic Oncology 2012;127:153‐60. [DOI] [PubMed] [Google Scholar]
Puente 2011 {published data only}
- Puente R, Schneider E, Carpio D, Benavides T. It's important the surgery performed in low‐risk and intermediate‐risk of endometrial cancer in relation to relapsed disease and recurrence sites?. International Journal of Gynecological Cancer 2011;21(Suppl 3 12):S1184. [Google Scholar]
Quinn 1993 {published data only}
- Quinn MA. Complete pelvic lymphadenectomy in 'high‐risk' endometrial carcinoma. International Journal of Gynecological Cancer 1993;3(Suppl 1):28. [Google Scholar]
Rodolakis 2012 {published data only}
- Rodolakis A, Thomakos N, Vlachos G, Haidopoulos D, Sarris K, Sotiropoulou M, et al. Lymphadenectomy in apparent early‐stage endometrial cancer – clinical utility and cost effectiveness. Gynecologic Oncology 2012;125(Suppl 1):S150. [Google Scholar]
Rossi 2013 {published data only}
- Rossi EC, Jackson A, Ivanova A, Boggess JF. Detection of sentinel nodes for endometrial cancer with robotic assisted fluorescence imaging: cervical versus hysteroscopic injection. International Journal of Gynecological Cancer 2013;23:1704‐11. [DOI] [PubMed] [Google Scholar]
Rossi 2014 {published data only}
- Rossi EC, Jackson AL, Kowalski LD, Ivanova A, Boggess JF. The sensitivity of sentinel lymph nodes identified with robotic fluorescence imaging for detecting metastatic endometrial cancer: interim results from the FIRES trial. Gynecologic Oncology 2014;133:22‐3. [Google Scholar]
Rubin 1990 {published data only}
- Rubin SC, Hoskins WJ, Nori D, Mychalczak B, Almadrones L, Chapman D, et al. Management of stage II endometrial adenocarcinoma. Gynecologic Oncology 1990;36(2):294. [DOI] [PubMed] [Google Scholar]
Salvesen 2001 {published data only}
- Salvesen HB. Role of lymphadenectomy in the surgery of gynecologic cancer. Tidsskr Nor Laegeforen 2001;121(10):1240‐5. [PubMed] [Google Scholar]
Schulz 1986 {published data only}
- Schulz KD. Adjuvant treatment of endometrial carcinoma. Journal of Cancer Research & Clinical Oncology 1986;111 Suppl 1:S6. [Google Scholar]
Shan 2013 {published data only}
- Shan B, Ren Y, Tu X, Jiang Z, Sun M, Cheng X, et al. Sentinel lymph nodes mapping and micrometastases detection in patients with early‐stage endometrial cancer. International Journal of Gynecological Cancer 2013;23(Suppl 1):333. [Google Scholar]
Tinelli 2009 {published data only}
- Bijen CB, Bock GH, Mourits MJ. Total laparoscopic versus abdominal hysterectomy with lymphadenectomy for early stage endometrial cancer: a prospective randomized study: author reply. Gynecologic Oncology 2009;113(2):295‐6. [DOI] [PubMed] [Google Scholar]
Tong 2011 {published data only}
- Tong SY, Lee JM, Lee JK, Kim JW, Cho CH, Kim SM, et al. Efficacy of para‐aortic lymphadenectomy in early‐stage endometrioid uterine corpus cancer. Annals of Surgical Oncology 2011;18(5):1425‐30. [DOI] [PubMed] [Google Scholar]
Trovik 2013 {published data only}
- Trovik J, Wik E, Werner HM, Krakstad C, Helland H, Vandenput I, et al. Hormone receptor loss in endometrial carcinoma curettage predicts lymph node metastasis and poor outcome in prospective multicentre trial. European Journal of Cancer 2013;49(16):3431‐41. [DOI] [PubMed] [Google Scholar]
Turkler 2013 {published data only}
- Turkler C, Gokcu M, Ozeren M, Sanci M. Role of lymphadenectomy in disease‐free and overall survival on low risk endometrium cancer patients. International Journal of Gynecological Cancer 2013;23(Suppl 1):422. [DOI] [PubMed] [Google Scholar]
Watari 2014 {published data only}
- Watari H, Todo Y, Kang S, Odagiri T, Sakuragi N. Proposal of a concept and design of a randomized phase III trial investigating the survival effect of para‐aortic lymphadenectomy in endometrial cancer. Journal of Obstetrics and Gynaecology Research 2014;40(2):312‐6. [DOI] [PubMed] [Google Scholar]
Zapico 2013 {published data only}
- Zapico A, Pedro V, Aldina C, Irene H, Victoria M, Pedro F, et al. Sentynel lymph node biopsy and endometrial cancer. Gynecological Surgery 2013;10(Suppl 1):S53. [Google Scholar]
Additional references
Bucher 1997
- Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta‐analysis of randomized controlled trials. Journal of Clinical Epidemiology 1997;50:683‐91. [DOI] [PubMed] [Google Scholar]
Creasman 1987
CRS‐web [Computer program]
- Cochrane. CRS‐web. Cochrane, accessed prior to 8 September 2017.
Deeks 2001
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic Reviews in Health Care: Meta‐Analysis in Context. 2nd Edition. London: BMJ Publication Group, 2001. [Google Scholar]
DerSimonian 1986
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7:177‐88. [DOI] [PubMed] [Google Scholar]
Ferlay 2012
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. GLOBOCAN 2012 v1.0. Lyon: IARC Press, 2013. [Google Scholar]
GRADE Working Group 2004
- GRADE Working Group. Grading quality of evidence and strength of recommendations. British Medical Journal 2004;328:1490‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
ISRCTN84527805
- ISRCTN84527805. Diagnostic accuracy of MRI, diffusion‐weighted MRI, FDGPET/CT and Fluoro‐ethyl‐choline PET/CT in the detection of lymph node metastases in surgically staged endometrial and cervical carcinoma. www.isrctn.com/search?q=ISRCTN84527805 (first received 14 December 2011); Vol. ISRCTN 84527805; UKCRN ID 10984.
Kang 2011
- Kang S, Yoo HJ, Hwang JH, Lim MC, Seo SS, Park SY. Sentinel lymph node biopsy in endometrial cancer: meta‐analysis of 26 studies. Gynecologic Oncology 2011;123(3):522‐7. [DOI] [PubMed] [Google Scholar]
Kilgore 1995
Kim 1993
- Kim YB, Niloff JM. Endometrial carcinoma: analysis of recurrence in patients treated with a strategy minimizing lymph node sampling and radiation therapy. Obstetrics and Gynecology 1993; Vol. 82, issue 2:175‐80. [PubMed]
Kitchener 2009a
- Kitchener H, Swart AM, Qian W, Parmar M. Lymphadenectomy in endometrial cancer ‐ Authors' reply. Lancet 2009;373(9670):1170‐1. [DOI] [PubMed] [Google Scholar]
Kong 2012
- Kong A, Johnson N, Kitchener HC, Lawrie TA. Adjuvant radiotherapy for stage I endometrial cancer. Cochrane Database of Systematic Reviews 2012, Issue 4. [DOI: 10.1002/14651858.CD003916.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Langendam 2013
- Langendam MW, Akl EA, Dahm P, Glasziou P, Guyatt G, Schunemann HJ. Assessing and presenting summaries of evidence in Cochrane Reviews. Systematic Reviews 2013;23(2):81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Meader 2014
- Meader N, King K, Llewellyn A, Norman G, Brown J, Rodgers M, et al. A checklist designed to aid consistency and reproducibility of GRADE assessments: development and pilot validation. Systematic Reviews 2014;3:82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moher 1998
- Moher D, Pham D, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta‐analyses?. Lancet 1998;352:609‐13. [DOI] [PubMed] [Google Scholar]
NICE 2007
- NICE. NICE Clinical Guideline: Heavy menstrual bleeding. www.nice.org.uk/guidance/cg44 (accessed prior to 8 September 2017); Vol. CG44.
Park 2010
- Park SL, Goodman MT, Zhang ZF, Kolonel LN, Henderson BE, Setiawan VW. Body size, adult BMI gain and endometrial cancer risk: the multiethnic cohort. International Journal of Cancer 2010;126:490‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Parkin 2005
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA: A Cancer Journal for Clinicians 2005;55(2):74‐108. [DOI] [PubMed] [Google Scholar]
Parmar 1998
Pecorelli 2009
- Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. International Journal of Gynecology & Obstetrics 2009;105(2):103‐4. [DOI] [PubMed] [Google Scholar]
Renehan 2008
- Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body‐mass index and incidence of cancer: a systematic review and meta‐analysis of prospective observational studies. Lancet 2008;371:569‐78. [DOI] [PubMed] [Google Scholar]
Schulz 1995
- Schulz KF, Chalmers I, Hayes RJ, Altman D. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273:408‐12. [DOI] [PubMed] [Google Scholar]
Shepherd 1989
- Shepherd JH. Revised FIGO staging for gynaecological cancer. British Journal of Obstetrics and Gynaecology 1989;96(8):889‐92. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Siegel 2015
- Siegel R, Miller K, Jemal A. Cancer Statistics, 2015. CA: A Cancer Journal for Clinicians 2015;65(1):5‐29. [DOI] [PubMed] [Google Scholar]
Todo 2010
- Todo Y, Kato H, Kaneuchi M, Watari H, Takeda M, Sakuragi N. Survival effect of para‐aortic lymphadenectomy in endometrial cancer (SEPAL study): a retrospective cohort analysis. Lancet 2010;375:1165‐72. [DOI] [PubMed] [Google Scholar]
Trimble 1998
Van Lankveld 2006
- Lankveld MA, Koot NC, Peeters PH, Leeuwen JS, Jurgenliemk‐Schulz IM. Compliance to surgical and radiation treatment guidelines in relation to patient outcome in early stage endometrial cancer. Journal of Evaluation in Clinical Practice 2006;12(2):196‐201. [DOI] [PubMed] [Google Scholar]
Wallace 2017
- Wallace BC, Noel‐Storr A, Marshall IJ, Cohen AM, Smalheiser NR, Thomas J. Identifying reports of randomized controlled trials (RCTs) via a hybrid machine learning and crowdsourcing approach.. Journal of the American Medical Informatics Association 2017;May 25:1‐4. [DOI: 10.1093/jamia/ocx053] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Frost 2015
- Frost JA, Webster KE, Bryant A, Morrison J. Lymphadenectomy for the management of endometrial cancer. Cochrane Database of Systematic Reviews 2015, Issue 9. [DOI: 10.1002/14651858.CD007585.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
May 2010
- May K, Bryant A, Dickinson HO, Kehoe S, Morrison J. Lymphadenectomy for the management of endometrial cancer. Cochrane Database of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/14651858.CD007585.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]