

Abstract
Background
This review is an update of a previously published review in The Cochrane Database of Systematic Reviews Issue 3, 2009 on single dose oral dexibuprofen (S(+)‐ibuprofen) for acute postoperative pain in adults.
Dexibuprofen is a non‐steroidal anti‐inflammatory drug (NSAID) licensed for use in rheumatic disease and other musculoskeletal disorders in the UK, and widely available in other countries worldwide. It is an active isomer of ibuprofen. This review sought to evaluate the efficacy and safety of oral dexibuprofen in acute postoperative pain, using clinical studies in patients with established pain, and with outcomes measured primarily over four to six hours, using standard methods. This type of study has been used for many decades to establish that drugs have analgesic properties.
Objectives
To assess the efficacy and adverse effects of single dose oral dexibuprofen for acute postoperative pain using methods that permit comparison with other analgesics evaluated in standardised studies using almost identical methods and outcomes.
Search methods
Searches were run for the original review in 2009 and subsequent searches have been run in August 2013. We did not find any new published studies as a result of the updated search.
We searched for randomised studies of dexibuprofen in acute postoperative pain in MEDLINE, EMBASE, and CENTRAL (The Cochrane LIbrary), and for clinical trial reports and synopses of published and unpublished studies from Internet sources.
Selection criteria
Randomised, double blind, placebo‐controlled clinical studies of oral dexibuprofen for relief of acute postoperative pain in adults.
Data collection and analysis
Two review authors independently assessed study quality and extracted data. We extracted pain relief or pain intensity data and converted it into the dichotomous outcome of number of participants with at least 50% pain relief over four to six hours, from which relative risk and number needed to treat to benefit (NNT) were calculated. Numbers of participants using rescue medication over specified time periods, and time to use of rescue medication, were sought as additional measures of efficacy. We collected information on adverse events and withdrawals.
Main results
New data were identified for this update in one unpublished trial synopsis (BR1160 1995) in addition to the single study (Dionne 1998) that was included in the original review. In both studies dexibuprofen gave high levels of response, with 51/96 (53%) participants experiencing at least 50% pain relief with dexibuprofen 200 mg and 35/50 (70%) with dexibuprofen 400 mg, compared with 75/147 (51%) with racemic ibuprofen 400 mg, and 12/62 (13%) with placebo. The numbers of participants was too small to calculate NNTs with any meaning. The median time to additional analgesic use was greater than four hours for all active therapies, but about two hours for placebo.
Adverse events were generally of mild or moderate intensity and consistent with events normally associated with anaesthesia and surgery. There were no serious adverse events or deaths.
Additional data did not alter the conclusions from the earlier review.
Authors' conclusions
The information from these two studies in acute postoperative pain suggested that dexibuprofen may be a useful analgesic, but at doses not very different from racemic ibuprofen, for which considerably more evidence exists.
Plain language summary
Single dose oral dexibuprofen for acute postoperative pain in adults
Acute pain is often felt soon after injury. Most people who have surgery have moderate or severe pain afterwards. People with pain are used to test pain killers. They have often had wisdom teeth removed. The pain is often treated with pain killers given by mouth. Results can be applied to other forms of acute pain.
A series of reviews looks at how good pain killers are. This review looks at a drug called dexibuprofen. This is a form of ibuprofen. It is thought to give the same pain relief at a lower dose.
We found two clinical trials with 313 people. Dexibuprofen at 200 mg or 400 mg single doses probably produced useful pain relief. The small number of studies, and of people in them, meant that no sensible results about benefit or harm after taking the drug were available.
Summary of findings
for the main comparison.
| Dexibuprofen compared with placebo for acute postoperative pain | ||||||
|
Patient or population: Adults with moderate or severe acute postoperative pain Settings: Community or hospital Intervention: Dexibuprofen 200 mg or 400 mg Comparison: Placebo | ||||||
| Outcomes | Probable outcome with |
NNT or NNH and/or relative effect (95% CI) |
No of studies, attacks, events |
Quality of the evidence (GRADE) |
Comments | |
| comparator | intervention | |||||
| At least 50% of maximum pain relief over 4 to 6 hours | Insufficent data | Very low | Quality of evidence very low because of small numbers of studies and participants | |||
| Participants with at least 1 adverse event | No data | Very low | ||||
| Participants with a serious adverse event | No serious adverse events | Very low | ||||
| Deaths | No deaths | Very low | ||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
Background
Description of the condition
This review is an update of a previously published review in The Cochrane Database of Systematic Reviews Issue 3, 2009 on Single dose oral dexibuprofen [S(+)‐ibuprofen] for acute postoperative pain in adults (Moore 2009).
Acute pain occurs as a result of tissue damage either accidentally due to an injury or as a result of surgery. Acute postoperative pain is a manifestation of inflammation due to tissue injury and/or nerve injury. The management of postoperative pain and inflammation is a critical component of patient care.
This is one of a series of reviews whose aim is to increase awareness of the range of analgesics that are potentially available, and present evidence for relative analgesic efficacy through indirect comparisons with placebo, in very similar studies performed in a standard manner, with very similar outcomes, and over the same duration. Such relative analgesic efficacy does not in itself determine choice of drug for any situation or patient, but guides policy‐making at the local level. The series covers all analgesics licensed for acute postoperative pain in the UK, and dipyrone, which is commonly used in Spain, Portugal, and Latin‐American countries. The results have been examined in an overview (Moore 2011a), and important individual reviews include ibuprofen (Derry 2009), paracetamol (Toms 2008), codeine (Derry 2010), and etoricoxib (Clarke 2012).
Description of the intervention
Acute pain studies
Single dose studies in acute pain are commonly short in duration, rarely lasting longer than 12 hours. The numbers of participants are small, allowing no reliable conclusions to be drawn about safety. To show that the analgesic is working, it is necessary to use placebo (McQuay 2005). There are clear ethical considerations in doing this. These ethical considerations are answered by using acute pain situations where the pain is expected to go away, and by providing additional analgesia, commonly called rescue analgesia, if the pain has not diminished after about an hour. This is reasonable, because not all participants given an analgesic will have significant pain relief. Approximately 18% of participants given placebo will have significant pain relief (Moore 2006), and up to 50% may have inadequate analgesia with active medicines. The use of additional or rescue analgesia is hence important for all participants in the studies.
Clinical studies measuring the efficacy of analgesics in acute pain have been standardised over many years (McQuay 2012). They have to be randomised and double‐blind. Typically, in the first few hours or days after an operation, patients develop pain that is moderate to severe in intensity, and will then be given the test analgesic or placebo. Pain is measured using standard pain intensity scales immediately before the intervention, and then using pain intensity and pain relief scales over the following four to six hours for shorter‐acting drugs, and up to 12 or 24 hours for longer‐acting drugs. Pain relief of half the maximum possible pain relief or better (at least 50% pain relief) is typically regarded as a clinically useful outcome. For patients given rescue medication it is usual for no additional pain measurements to be made, and for all subsequent measures to be recorded as initial pain intensity or baseline (zero) pain relief (baseline observation carried forward). This process ensures that analgesia from the rescue medication is not wrongly ascribed to the test intervention. In some studies the last observation is carried forward, which gives an inflated response for the test intervention compared to placebo, but the effect has been shown to be negligible over four to six hours (Moore 2005). Participants usually remain in the hospital or clinic for at least the first six hours following the intervention, with measurements supervised, although they may then be allowed home to make their own measurements in studies of longer duration.
Knowing the relative efficacy of different analgesic drugs at various doses can be helpful.
Dexibuprofen
Dexibuprofen is a non‐steroidal anti‐inflammatory drug (NSAID), sporadically available in different countries, and with no consistent licensed indications. In England in 2012 only 4500 prescriptions were issued in primary care, for 300 mg and 400 mg tablets. This compares with almost 5.7 million prescriptions for naproxen and 4.6 million prescriptions for ibuprofen in the same period (PACT 2013).
Dexibuprofen (trade names Deltaran and Seractil) is the single pharmacologically active enantiomer of racemic ibuprofen. Half doses of dexibuprofen are not entirely equivalent to full doses of ibuprofen (Gabard 1995), since there is hepatic conversion of some of the inactive enantiomer to the active form when the racemic mixture is given (Lee 1985). In general, the dexibuprofen dose given is half that of ibuprofen, although this may not be the case in some ethnic groups, particularly the Chinese (Zheng 2008). In arthritis, daily doses of 800 mg dexibuprofen produced as much analgesia as 200 mg celecoxib (Hawel 2003), and 1200 mg dexibuprofen as much as 2400 mg ibuprofen (Singer 2000). A review by Phleps 2001 reported clinical efficacy in rheumatoid arthritis, ankylosing spondylitis, osteoarthritis of the hip, osteoarthritis of the knee, lumbar vertebral syndrome, distortion of the ankle joint and dysmenorrhoea.
How the intervention might work
NSAIDs reversibly inhibit cyclooxygenase (prostaglandin endoperoxide synthase), the enzyme mediating production of prostaglandins and thromboxane A2 (FitzGerald 2001). Prostaglandins mediate a variety of physiological functions such as maintenance of the gastric mucosal barrier, regulation of renal blood flow, and regulation of endothelial tone. They also play an important role in inflammatory and nociceptive processes. Ibuprofen, like most NSAIDs, causes reversible inhibition of the cyclooxygenases, which interferes with thromboxane and prostaglandin synthesis, and increases production of anti‐inflammatory lipoxins.
Why it is important to do this review
We could find no systematic review on the efficacy of dexibuprofen in acute pain. While a number of studies have reported equivalent efficacy for reduced doses of dexibuprofen compared with racemic ibuprofen (or other NSAIDs) in chronic musculoskeletal pain, it is not known whether the same is found in acute pain. Lower doses of NSAIDs may result in better tolerability. This update was prompted by the availability of an unpublished clinical trial synopsis.
Objectives
To assess the efficacy and adverse effects of single dose oral dexibuprofen for acute postoperative pain using methods that permit comparison with other analgesics evaluated in standardised studies using almost identical methods and outcomes.
Methods
Criteria for considering studies for this review
Types of studies
We included double blind studies of single dose oral dexibuprofen compared with placebo for the treatment of moderate to severe postoperative pain in adults, with at least 10 participants randomly allocated to each treatment group. We included multiple dose studies if appropriate data from the first dose were available, and cross‐over studies provided that data from the first phase were presented separately.
We excluded:
review articles, case reports, and clinical observations;
studies of experimental pain;
studies where pain relief is assessed only by clinicians, nurses or carers (i.e. not patient‐reported);
studies of less than four hours duration or studies that fail to present data over four to six hours post‐dose.
For postpartum pain, we included studies if the pain investigated was due to episiotomy or Caesarean section irrespective of the presence of uterine cramps; we excluded studies investigating pain due to uterine cramps alone.
Types of participants
We included studies of adult participants (> 15 years) with established postoperative pain of moderate to severe intensity following day surgery or in‐patient surgery. For studies using a visual analogue scale (VAS), pain of at least moderate intensity would be equated to greater than 30 mm (Collins 1997).
Types of interventions
Dexibuprofen administered as a single oral dose, compared with matched placebo or racemic ibuprofen, given for relief of postoperative pain.
Types of outcome measures
We collected the following data where available:
participant characteristics;
patient reported pain at baseline (physician, nurse or carer reported pain were not included in the analysis);
patient reported pain relief expressed at least hourly over four to six hours using validated pain scales (pain intensity and pain relief in the form of VAS or categorical scales, or both);
patient global assessment of efficacy (PGE), using a standard categorical scale;
time to use of rescue medication;
number of participants using rescue medication;
number of participants with one or more adverse events;
number of participants with serious adverse events;
number of withdrawals (all cause, adverse event).
Search methods for identification of studies
Electronic searches
We searched the following electronic databases:
The Cochrane Central Register of Controlled Trials (CENTRAL) on The Cochrane Library, (Issue 2, 2009 for the original review and Issue 7, 2013 for this update);
MEDLINE via Ovid (to May 2009 for the original review and from 2008 to 19 August 2013 for this update);
EMBASE via Ovid (to May 2009 for the original review and from 2008 to 19 August 2013 for this update).
Oxford Pain Relief Database (Jadad 1996a).
Please see Appendix 1 for the MEDLINE search strategy, Appendix 2 for the EMBASE search strategy, and Appendix 3 for the CENTRAL search strategy.
Searching other resources
We searched for additional studies in reference lists of retrieved articles and reviews. We also searched the PhRMA clinical study results database (www.clinicaltrials.gov) and the WHO International Clinical Trials Registry Platform (apps.who.int/trialsearch/) for otherwise unpublished trial results and information about ongoing studies.
The unpublished clinical trial synopsis included in this update was made available by Reckitt Benckiser.
Data collection and analysis
Selection of studies
Two review authors independently assessed and agreed the search results for studies to be included in the review. Disagreements would be resolved by consensus or referral to a third review author.
Data extraction and management
Two review authors extracted data and recorded them on a standard data extraction form. One review author entered data into RevMan 5.2 (RevMan 2012).
Assessment of risk of bias in included studies
Two review authors independently assessed each study for methodological quality using a three‐item, five‐point scale (Jadad 1996b), and agreed a consensus score.
We also completed a Risk of bias in included studies table, using methods adapted from those described by the Cochrane Pregnancy and Childbirth Group. Two authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) with any disagreements resolved by discussion. The following were assessed for each study.
Random sequence generation (checking for possible selection bias). The method used to generate the allocation sequence was assessed as: low risk of bias (any truly random process, e.g. random number table; computer random number generator); high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number) ‐ these studies would be excluded; unclear risk of bias.
Allocation concealment (checking for possible selection bias). The method used to conceal allocation to interventions prior to assignment assessed whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment. The methods were assessed as: low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes); high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth) ‐ theses studies would be excluded; unclear risk of bias.
Blinding of outcome assessment (checking for possible detection bias). The methods used to blind study participants and outcome assessors from knowledge of which intervention a participant received were assessed. Studies were considered to be at low risk of bias if they stated that they were blinded and described the method used to achieve blinding (e.g. identical tablets; matched in appearance and smell), or at unknown risk if they stated that they were blinded, but did not provide an adequate description of how it was achieved. Single blind and open studies would be excluded.
Size (checking for possible biases confounded by small size). Small studies have been shown to overestimate treatment effects, probably due to methodological weaknesses (Nuesch 2010). Studies were considered to be at low risk of bias if they had ≥ 200 participants, at unknown risk of they had 50 to 200 participants, and at high risk if they had < 50 participants.
Measures of treatment effect
We used relative risk (or 'risk ratio', RR) to establish statistical difference. We used numbers needed to treat (NNT) and pooled percentages as absolute measures of benefit or harm.
We used the following terms to describe adverse outcomes in terms of harm or prevention of harm.
When significantly fewer adverse outcomes occur with treatment than with control (placebo or active) we use the term the number needed to treat to prevent one event (NNTp).
When significantly more adverse outcomes occur with treatment compared with control (placebo or active) we use the term the number needed to harm or cause one event (NNH).
Unit of analysis issues
We accepted only randomisation to the individual participant.
Assessment of heterogeneity
We planned to examine heterogeneity visually using L'Abbé plots (L'Abbé 1987), a visual method for assessing differences in results of individual studies.
Data synthesis
We followed QUOROM guidelines (Moher 1999). For efficacy analyses we used the number of participants in each treatment group who were randomised, received medication, and provided at least one post‐baseline assessment. For safety analyses we used number of participants randomised to each treatment group who took the study medication. We planned to analyse for different doses separately.
For each study we converted the mean TOTPAR, SPID, VAS TOTPAR, or VAS SPID (Appendix 4) values for active and placebo to %maxTOTPAR or %maxSPID by division into the calculated maximum value (Cooper 1991), and calculated the proportion of participants in each treatment group who achieved at least 50%maxTOTPAR using verified equations (Moore 1996; Moore 1997a; Moore 1997b). We then converted these proportions into the number of participants achieving at least 50%maxTOTPAR by multiplying by the total number of participants in the treatment group. We used this information on the number of participants with at least 50%maxTOTPAR for active and placebo to calculate relative benefit or relative risk, and number needed to treat to benefit (NNT) or harm (NNH). Because adverse events with ibuprofen/paracetamol combinations were less frequent than with placebo, this is described as an NNTp, the number needed to treat to prevent an adverse event. NNTp was also used to describe differences in remedication rates, where remedication rates were lower with active treatment than control.
We accepted the following pain measures for the calculation of TOTPAR or SPID:
five‐point categorical pain relief (PR) scales with comparable wording to 'none, slight, moderate, good or complete';
four‐point categorical pain intensity (PI) scales with comparable wording to 'none, mild, moderate, severe';
VAS for pain relief;
VAS for pain intensity.
If none of these measures was available, we would use the number of participants reporting 'very good or excellent' on a five‐point categorical global scale with the wording 'poor, fair, good, very good, excellent' for the number of participants achieving at least 50% pain relief (Collins 2001).
For each treatment group we extracted the number of participants reporting treatment‐emergent adverse effects, and calculated relative benefit and risk estimates with 95% confidence intervals (CI) using a fixed‐effect model (Morris 1995). We calculated NNT and NNH with 95% CIs using the pooled number of events using the method devised by Cook and Sackett (Cook 1995). We assumed a statistically significant difference from control when the 95% CI of the relative risk or relative benefit did not include the number one.
Subgroup analysis and investigation of heterogeneity
We planned no subgroup analysis as the data set was known to be small. We required a minimum of two studies and 200 participants to be available in any subgroup analysis (Moore 1998).
Sensitivity analysis
We planned no sensitivity analysis as the data set was known to be small. We required a minimum of two studies and 200 participants to be available in any sensitivity analysis (Moore 1998).
Results
Description of studies
This is an update of a review first published in 2009 (Moore 2009).
Results of the search
No new studies were found through an updated search. Reckitt Benckiser provided a clinical trial synopsis of a previously unpublished study (BR1160 1995) that did not appear on any search, including clinicaltrials.gov or the WHO portal. Figure 1 shows the flow diagram for included studies.
1.
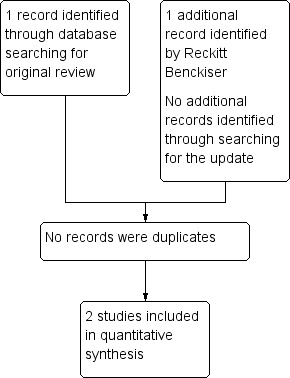
Study flow diagram.
Included studies
Two studies satisfied inclusion criteria. One study (Dionne 1998) was published in a peer review journal and included in the earlier review. The other (BR1160 1995) was available only as a clinical trial synopsis; this new study increased the total number of participants by 137.
Both studies recruited participants with pain following third molar extraction, aged 16 years or older (mean age 22 and 25 years), and the majority were female (65%). There was a washout period for analgesics or other drugs likely to influence pain perception of 24 or 48 hours. Study medication was administered when pain was of moderate or severe intensity. Dionne 1998 used standard pain intensity (4‐point) and pain relief (5‐point) scales, but BR1160 1995 measured only pain intensity using a non‐standard 9‐point scale.
There were 318 participants in total, of whom 313 provided data for analysis; 97 received dexibuprofen (S(+) ibuprofen) 200 mg, 50 received dexibuprofen 400 mg, 101 received racemic ibuprofen 400 mg, and 65 received placebo.
Full details are in the Characteristics of included studies table.
Excluded studies
One study excluded in the original review was a pharmacokinetic study without pain measures (Jamali 1999). Details are in Characteristics of excluded studies table.
Risk of bias in included studies
Included studies were both randomised and double‐blind and provided information about withdrawals and dropouts. The methodological quality of the studies was determined using the Oxford Quality Scale. BR1160 1995 scored 5/5 points whereas Dionne 1998 only scored 4/5 as it did not adequately describe sequence generation. Details for individual studies are provided in the Characteristics of included studies table.
In addition we created a Risk of bias in included studies table which considered random sequence generation, allocation concealment, blinding, and study size (Figure 2; Figure 3).
2.
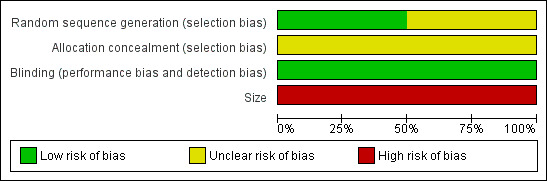
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
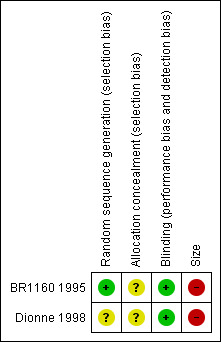
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Both studies reported that they were randomised. Only one (BR1160 1995) adequately described the method used to generate the sequence and to conceal the random allocation.
Blinding
Both studies were double blind and adequately described how this was achieved.
Other potential sources of bias
Treatment group size was an issue. Small studies are thought to be at increased risk of bias, probably because the conduct of small studies is more likely to be less rigorous, allowing critical criteria such as blinding to be compromised. Both studies had treatment group sizes that put them at high risk of bias.
Effects of interventions
See: Table 1
Number of participants achieving at least 50% pain relief
Dexibuprofen 200 mg vs placebo
Both studies reported on this dose; 51/96 (53%) participants achieved this outcome with dexibuprofen 200 mg compared with 12/62 (13%) with placebo. There were insufficient data for statistical analysis.
Dexibuprofen 400 mg vs placebo
One study (Dionne 1998) reported on this dose; 35/50 (70%) achieved this outcome with dexibuprofen 400 mg compared with 12/62 (13%) with placebo. There were insufficient data for statistical analysis.
Dexibuprofen 200 mg vs racemic ibuprofen 400 mg
Both studies reported on this dose; 51/96 (53%) achieved this outcome with dexibuprofen 200 mg compared with 49/97 (51%) with racemic ibuprofen 400 mg. There were insufficient data for statistical analysis.
Dexibuprofen 400 mg vs racemic ibuprofen 400 mg
One study reported on this dose (Dionne 1998); 35/50 (70%) achieved this outcome with dexibuprofen 400 mg compared with 26/50 (52%) with racemic ibuprofen 400 mg. There were insufficient data for statistical analysis.
Rescue medication
Median time to use of rescue medication
One study (Dionne 1998) reported a median time to remedication of 5.8 hours with dexibuprofen 200 mg, 6.1 hours with dexibuprofen 400 mg, and 5.4 hours with racemic ibuprofen compared with 1.8 hours with placebo.
The other study (BR1160 1995) reported median time to remedication in excess of 4.0 hours for dexibuprofen 200 mg and racemic ibuprofen compared to 2.5 hours with placebo.
Number of participants using rescue medication
One study (BR1160 1995) reported that 16/45, 17/47, 24/37 participants used rescue medication with dexibuprofen 200 mg, racemic ibuprofen 400 mg, and placebo respectively.
Adverse events
The adverse events most commonly reported in Dionne 1998 were drowsiness, nausea and headache with ibuprofen, and headache with placebo. In BR1160 1995 nausea with racemic ibuprofen 400 mg and vomiting with dexibuprofen 200 mg and placebo were reported. These events are commonly associated with surgery and anaesthesia and there were no obvious differences between treatment groups. All adverse events were reported as mild to moderate in intensity, and were most likely to be related to the anaesthetic or surgical procedure.
Neither study reported the number of participants who experienced one or more adverse event. There were no serious adverse events reported in either study.
Withdrawals
Withdawal due to lack of efficacy is considered under use of rescue medication. Withdrawals for other reasons were infrequent and balanced across treatment arms. Two adverse event withdrawals were reported, both in the study BR1160 1995, in the placebo group, both due to vomiting. Dionne 1998 reported no withdrawals due to adverse events but four participants were excluded as impaction was neither partial nor bony at the time of surgery. One further participant was excluded as remedication was administered within one hour of the study drug. Eleven participants were excluded from BR1160 1995 due to protocol violation and a further eight due to loss to follow‐up.
Discussion
Dexibuprofen is not a widely available NSAID, and there is no large literature describing its use in clinical pain conditions, although in a review by Phleps 2001 clinical efficacy of dexibuprofen was reported in rheumatoid arthritis, ankylosing spondylitis, osteoarthritis of the hip, osteoarthritis of the knee, lumbar vertebral syndrome, distortion of the ankle joint and dysmenorrhoea. The information from the two studies in acute postoperative pain suggests it to be a useful analgesic, but at doses not very different from racemic ibuprofen. Published randomised trials indicate reasonable efficacy of dexibuprofen in relatively short studies in osteoarthritis (Hawel 2003; Singer 2000), and in single doses in dysmenorrhoea (Kollenz 2009).
As with many other analgesics in acute and chronic pain, dexibuprofen produces good pain relief in some but not all patients (Moore 2013a). With NSAIDs, formulations that produce faster absorption (soluble salts, or liquigel, for example) also produce faster and often better overall pain relief, as with ibuprofen (Moore 2013b). For dexibuprofen in this review, only standard formulations were reported upon.
Summary of main results
Data from one new study synopsis were available for this updated review in addition to the original study but the conclusions remained unchanged. Incuded studies involved 313 participants of whom 97 received dexibuprofen 200 mg, 50 received dexibuprofen 400 mg, 101 received racemic ibuprofen 400 mg, and 76 received placebo. Dexibuprofen at 200 mg and 400 mg single doses produced more participants with good pain relief than did placebo, and roughly the same proportion as with the same or double doses (in mg) of racemic ibuprofen. No analyses of the available data were sensible given the small numbers, and the high likelihood of false conclusions being arrived at by chance (Moore 1998).
It was also unclear if the median time to rescue medication varied between studies because there was a difference in study duration. Dionne 1998 lasted six hours; the median time to remedicate was five or six hours for active therapies (dexibuprofen and ibuprofen). BR1160 1995) lasted only for four hours; the median time to remedicate was over four hours for both active treatments (dexibuprofen and ibuprofen). Therefore no pooling of results was possible.
Neither study reported serious adverse events, including death.
Overall completeness and applicability of evidence
Both studies included in this update enrolled participants with dental pain following extraction of at least one impacted third molar. These individuals are generally in their early 20s, and are otherwise fit and healthy. They are not representative of the range of individuals who might need analgesia for acute postoperative pain. Although there is no reason why analgesic response in these individuals should differ in any systematic way from a more generalised population, it is entirely possible that adverse events (gastrointestinal in particular) may be more frequent, intense, or severe in older patients, and those with comorbidities. Neither study provided information on numbers of participants experiencing adverse events, but it was unlikely to be a significant problem as both were single‐dose studies.
Quality of the evidence
The studies were of adequate methodological quality with (Dionne 1998) scoring 4/5 and (BR1160 1995) scoring 5/5 on the Oxford Quality Scale, although they were both judged to be at high risk of bias from the small sizes of their treatment groups. Both studies administered the medication when pain levels were moderate or severe, ensuring that the study was sensitive to detect a 50% reduction (Moore 2013a).
Potential biases in the review process
We are unaware of any potential biases in the review process.
Agreements and disagreements with other studies or reviews
We are not aware of any other systematic reviews of dexibuprofen in treating acute postoperative pain.
Authors' conclusions
Implications for practice.
Additional information has not changed the conclusions. There are no implications for practice because there is insufficient information at present to draw conclusions about efficacy or harm of dexibuprofen, or to make any sensible comparisons with racemic ibuprofen or other analgesics.
Implications for research.
A considerable additional body of clinical trial results would be needed to know whether dexibuprofen has any advantages in efficacy, or faster analgesic onset, or safety over racemic ibuprofen. There seems little need for this research, as emerging evidence is that formulation is likely to be more important than chirality for NSAIDs in acute pain.
What's new
| Date | Event | Description |
|---|---|---|
| 29 May 2019 | Amended | Contact details updated. |
| 11 October 2017 | Review declared as stable | No new studies likely to change the conclusions are expected. |
History
Protocol first published: Issue 1, 2009 Review first published: Issue 3, 2009
| Date | Event | Description |
|---|---|---|
| 26 February 2014 | Review declared as stable | This review will be assessed for updating in 2018. |
| 20 August 2013 | New search has been performed | New data identified in one unpublished trial synopsis and included in review (BR1160 1995) with 137 participants. New searches carried out for published studies on the 19 August 2013. |
| 20 August 2013 | New citation required but conclusions have not changed | Additional data do not alter the conclusions from the previous publication. There are still too few data to determine whether dexibuprofen has any advantages in efficacy or safety over racemic ibuprofen. No clinical trials have been published since 1998, and this review can probably be made stable for 5 to 10 years. |
| 10 November 2010 | Review declared as stable | The authors declare that there is unlikely to be any further studies to be included in this review and so it should be published as a 'stable review'. |
| 24 September 2010 | Amended | Contact details updated. |
Notes
The authors believe that there are unlikely to be any further studies for inclusion in this review, so it should be published as a 'stable review'.
Acknowledgements
Henry McQuay was an author on the original review. The earlier review was supported by an NHS Cochrane Collaboration Grant and NIHR Biomedical Research Centre Programme. We thank Reckitt Benckiser for making available data from the unpublished study.
Appendices
Appendix 1. MEDLINE search strategy (via OVID)
(dexibuprofen).mp. (15)
(deltaran or seractil).mp. (2)
1 or 2 (17)
Pain, Postoperative/ (6191)
exp Surgical Procedures, Operative/ (399388)
((postoperative adj4 pain*) or (post‐operative adj4 pain*) or post‐operative‐pain* or (post* adj4 pain*) or (postoperative adj4 analgesi*) or (post‐operative adj4 analgesi*) or "post‐operative analgesi*").mp. (10296)
((post‐surgical adj4 pain*) or ("post surgical" adj4 pain*) or (post‐surgery adj4 pain*)).mp. (100)
("pain‐relief after surg*" or "pain following surg*" or "pain control after").mp. (132)
(("post surg*" or post‐surg*) and (pain* or discomfort)).mp. (388)
((pain* adj4 "after surg*") or (pain* adj4 "after operat*") or (pain* adj4 "follow* operat*") or (pain* adj4 "follow* surg*")).mp. (650)
((analgesi* adj4 "after surg*") or (analgesi* adj4 "after operat*") or (analgesi* adj4 "follow* operat*") or (analgesi* adj4 "follow* surg*")).mp. (97)
or/4‐11 (402335)
randomized controlled trial.pt. (82601)
controlled clinical trial.pt. (7435)
randomized.ab. (74425)
placebo.ab. (27937)
drug therapy.fs. (320336)
randomly.ab. (49540)
trial.ab. (74386)
groups.ab. (27566)
or/13‐20 (65141)
3 and 12 and 21 (2)
Appendix 2. Search strategy for EMBASE (via Ovid)
Dexibuprofen/ (102)
(dexibuprofen).mp. (104)
(deltaran or seractil).mp. (15)
1 or 2 or 3 (105)
Pain, Postoperative/ (16657)
exp Surgical Procedures, Operative/ (1089731)
((postoperative adj4 pain*) or (post‐operative adj4 pain*) or post‐operative‐pain* or (post* adj4 pain*) or (postoperative adj4 analgesi*) or (post‐operative adj4 analgesi*) or "post‐operative analgesi*").mp. (34142)
((post‐surgical adj4 pain*) or ("post surgical" adj4 pain*) or (post‐surgery adj4 pain*)).mp. (371)
("pain‐relief after surg*" or "pain following surg*" or "pain control after").mp. (330)
(("post surg*" or post‐surg*) and (pain* or discomfort)).mp. (1140)
((pain* adj4 "after surg*") or (pain* adj4 "after operat*") or (pain* adj4 "follow* operat*") or (pain* adj4 "follow* surg*")).mp. (1558)
((analgesi* adj4 "after surg*") or (analgesi* adj4 "after operat*") or (analgesi* adj4 "follow* operat*") or (analgesi* adj4 "follow* surg*")).mp. (225)
or/5‐12 (1098653)
clinical trials.sh. (219621)
controlled clinical trial.sh. (95337)
randomized controlled trial.sh. (127951)
double‐blind procedure.sh. (33503)
(clin* adj25 trial*).mp (374809)
((doubl* or trebl* or tripl*) adj25 (blind* or mask*)).mp (55272)
placebo*.mp (120870)
random*.mp (425810)
or/14‐21 (678206)
4 and 13 and 22 (11)
Appendix 3. Search strategy for Cochrane CENTRAL
(Dexibuprofen or Deltaran or Seractil):ti,ab,kw (26)
MeSH descriptor: [Pain, Postoperative] this term only (8842)
MeSH descriptor: [Surgical Procedures, Operative] explode all trees (89806)
2 or 3 (91999)
4 and 6 (3)
Limit 5 to Trials (1)
Appendix 4. Glossary
Categorical rating scale:
The commonest is the five category scale (none, slight, moderate, good or lots, and complete). For analysis numbers are given to the verbal categories (for pain intensity, none=0, mild=1, moderate=2 and severe=3, and for relief none=0, slight=1, moderate=2, good or lots=3 and complete=4). Data from different subjects is then combined to produce means (rarely medians) and measures of dispersion (usually standard errors of means). The validity of converting categories into numerical scores was checked by comparison with concurrent visual analogue scale measurements. Good correlation was found, especially between pain relief scales using cross‐modality matching techniques. Results are usually reported as continuous data, mean or median pain relief or intensity. Few studies present results as discrete data, giving the number of participants who report a certain level of pain intensity or relief at any given assessment point. The main advantages of the categorical scales are that they are quick and simple. The small number of descriptors may force the scorer to choose a particular category when none describes the pain satisfactorily.
VAS:
Visual analogue scale: lines with left end labelled "no relief of pain" and right end labelled "complete relief of pain", seem to overcome this limitation. Patients mark the line at the point which corresponds to their pain. The scores are obtained by measuring the distance between the no relief end and the patient's mark, usually in millimetres. The main advantages of VAS are that they are simple and quick to score, avoid imprecise descriptive terms and provide many points from which to choose. More concentration and coordination are needed, which can be difficult post‐operatively or with neurological disorders.
TOTPAR:
Total pain relief (TOTPAR) is calculated as the sum of pain relief scores over a period of time. If a patient had complete pain relief immediately after taking an analgesic, and maintained that level of pain relief for six hours, they would have a six‐hour TOTPAR of the maximum of 24. Differences between pain relief values at the start and end of a measurement period are dealt with by the composite trapezoidal rule. This is a simple method that approximately calculates the definite integral of the area under the pain relief curve by calculating the sum of the areas of several trapezoids that together closely approximate to the area under the curve.
SPID:
Summed pain intensity difference (SPID) is calculated as the sum of the differences between the pain scores over a period of time. Differences between pain intensity values at the start and end of a measurement period are dealt with by the trapezoidal rule.
VAS TOTPAR and VAS SPID are visual analogue versions of TOTPAR and SPID.
See "Measuring pain" in Bandolier's Little Book of Pain, Oxford University Press, Oxford. 2003; pp 7‐13 (Moore 2003).
Appendix 5. Summary of outcomes in individual studies: efficacy
| Analgesia | Rescue medication | ||||
| Study ID | Treatment | PI or PR | Number with 50% PR | Median time to use (h) | Number using |
| Dionne 1998 | 1) Ibuprofen (s(+)‐) 200mg n= 51 2) Ibuprofen (s(+)‐) 400mg n=50 3) Ibuprofen (racemic) 400mg n=50 4) Placebo n= 25 | TOTPAR 6: 1) 12.96 2) 14.85 3) 11.52 4) 3.45 | 1) 31/51 2) 35/50 3) 26/50 4) 2/25 |
1) 5.8 2) 6.1 3) 5.4 4) 1.8 |
No data |
| BR1160 1995 | 1)Ibuprofen s(+) 200mg n=46 2)racemic ibuprofen 400mg n=51 3)Placebo n=40 | This was converted to 100mm for 4 hours. SPID 4 1) 86.66 2) 91.51 3) 58.04 | 1) 20/45 2) 23/47 3) 10/37 | 1) >4 2) >4 3) 2.5 |
1) 16/45 2) 17/47 3) 24/37 |
| PI = pain intensity; PR = pain relief; TOTPAR = total pain relief; SPID = summed pain intensity difference | |||||
Characteristics of studies
Characteristics of included studies [ordered by study ID]
BR1160 1995.
| Methods | RCT, DB, single oral dose, parallel groups Medication administered when pain was of moderate or severe intensity Pain assessed at 0, 15, 30, 45, 60 minutes, then hourly to 4 hours |
|
| Participants | Third molar extraction N = 137 M = 55, F = 82 Mean age 25 years |
|
| Interventions | Dexibuprofen (S(+)‐Ibuprofen) 200 mg, n = 46 Racemic ibuprofen 400 mg, n = 51 Placebo, n = 40 |
|
| Outcomes | PI: non‐std 9 point scale Use of rescue medication Withdrawals |
|
| Notes | Oxford Quality Score: R2, DB2, W1 Rescue medication permitted after 1 hour |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomisation list generated by the Statistics Section of Boots Pharmaceuticals" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding (performance bias and detection bias) All outcomes | Low risk | "Double‐dummy method" |
| Size | High risk | < 50 participants per treatment group |
Dionne 1998.
| Methods | RCT, DB, single oral dose, 4 parallel groups Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 15, 30, 45, 60 minutes, then hourly to 6 hours |
|
| Participants | Third molar extraction N = 181 (176 analysed for efficacy) M = 50, F = 126 Mean age 22 years |
|
| Interventions | Dexibuprofen (S(+)‐Ibuprofen) 200 mg, n = 51 Dexibuprofen (S(+)‐Ibuprofen) 400 mg, n = 50 Ibuprofen (racemic) 400 mg, n = 50 Placebo, n = 25 |
|
| Outcomes | PI: std 4 point scale and 100 mm VAS PR: std 5 point scale and 100 mm VAS Time to use of rescue medication Withdrawals |
|
| Notes | Oxford Quality Score: R1, DB2, W1 Rescue medication permitted ‐ no further details |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not specified |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding (performance bias and detection bias) All outcomes | Low risk | "Double‐dummy method" |
| Size | High risk | < 50 participants per treatment group |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Jamali 1999 | Fewer than 10 per group Pharmacokinetic study ‐ no pain measures |
Differences between protocol and review
For the update we have added a Risk of bias table and Summary of findings table.
Contributions of authors
For the original review, SD and RAM performed searching, data extraction, and analysis, including assessment of study quality. HJM helped with analysis and acted as arbitrator. All review authors contributed to writing.
For the update, JB and SD carried out searching, data extraction and analysis, and risk of bias assessments. All review authors were involved with writing.
Sources of support
Internal sources
Oxford Pain Research Funds, UK.
External sources
NHS Cochrane Collaboration Grant, UK.
-
NIHR Biomedical Research Centre Programme, UK.
RAM Funding
Declarations of interest
SD and RAM have received research support from charities, government and industry sources at various times. RAM has consulted for various pharmaceutical companies and received lecture fees from pharmaceutical companies related to analgesics and other healthcare interventions. JB has no interests to declare.
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
BR1160 1995 {unpublished data only}
- Lancaster L, Goulder MA. A double blind, singe‐dose, parallel‐group study comparing the analgesic effect of S(+) ibuprofen with racemic ibuprofen and placebo following unilateral or bilateral extraction of third molars. Boots healthcare international, trial synopsis 1995:1‐79.
Dionne 1998 {published data only}
- Dionne RA, McCullagh L. Enhanced analgesia and suppression of plasma B‐endorphin by the S(+)‐isomer of ibuprofen. Clinical Pharmacology and Therapeutics 1998;63(5):694‐701. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Jamali 1999 {published data only}
- Jamali F, Kunz‐Dober CM. Pain‐mediated altered absorption and metabolism of ibuprofen: an explanation for decreased serum enantiomer concentration after dental surgery. British Journal of Clinical Pharmacology 1999;47(4):391‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Clarke 2012
- Clarke R, Derry S, Moore RA. Single dose oral etoricoxib for acute postoperative pain in adults. Cochrane Database of Systematic Reviews 2012, Issue 4. [DOI: 10.1002/14651858.CD004309.pub3] [DOI] [PubMed] [Google Scholar]
Collins 1997
- Collins SL, Moore RA, McQuay HJ. The visual analogue pain intensity scale: what is moderate pain in millimetres?. Pain 1997;72:95‐7. [DOI] [PubMed] [Google Scholar]
Collins 2001
- Collins SL, Edwards J, Moore RA, Smith LA, McQuay HJ. Seeking a simple measure of analgesia for mega‐trials: is a single global assessment good enough?. Pain 2001;91(1‐2):189‐94. [DOI] [PubMed] [Google Scholar]
Cook 1995
- Cook RJ, Sackett DL. The number needed to treat: a clinically useful measure of treatment effect. BMJ 1995;310(6977):452‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cooper 1991
- Cooper SA. Single‐dose analgesic studies: the upside and downside of assay sensitivity. The Design of Analgesic Clinical Trials. Advances in Pain Research Therapy 1991;18:117‐24. [Google Scholar]
Derry 2009
- Derry C, Derry S, Moore RA, McQuay HJ. Single dose oral ibuprofen for acute postoperative pain in adults. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD001548.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Derry 2010
- Derry S, Moore RA, McQuay HJ. Single dose oral codeine, as a single agent, for acute postoperative pain in adults. Cochrane Database of Systematic Reviews 2010, Issue 4. [DOI: 10.1002/14651858.CD008099.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
FitzGerald 2001
- FitzGerald GA, Patrono C. The coxibs, selective inhibitors of cyclooxygenase‐2. New England Journal of Medicine 2001;345(6):433‐42. [DOI: 10.1056/NEJM200108093450607] [DOI] [PubMed] [Google Scholar]
Gabard 1995
- Gabard B, Nirnberger G, Schiel H, Mascher H, Kikuta C, Mayer JM. Comparison of the bioavailability of dexibuprofen administered alone or as part of racemic ibuprofen. European Journal of Clinical Pharmacology 1995;48(6):505‐11. [DOI] [PubMed] [Google Scholar]
Hawel 2003
- Hawel R, Klein G, Singer F, Mayrhofer F, Kahler ST. Comparison of the efficacy and tolerability of dexibuprofen and celecoxib in the treatment of osteoarthritis of the hip. International journal of Clinical Pharmacology and Therapeutics 2003;41(4):153‐64. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Altman DG, Antes G, Gøtzsche P, Higgins JPT, Jüni P, Lewis S, et al. Assessing risk of bias in included studies. In: Higgins JPT, Altman DG, Sterne JAC editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. www.cochrane‐handbook.org. The Cochrane Collaboration, 2011. [Google Scholar]
Jadad 1996a
- Jadad AR, Carroll D, Moore RA, McQuay H. Developing a database of published reports of randomised clinical trials in pain research. Pain 1996;66(2‐3):239‐46. [DOI] [PubMed] [Google Scholar]
Jadad 1996b
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17:1‐12. [DOI] [PubMed] [Google Scholar]
Kollenz 2009
- Overview on clinical data of dexibuprofen. ADIDAC trial: analgesia with dexibuprofen versus ibuprofen in patients suffering from primary dysmenorrhea: a crossover trial. Gynecologic and Obstetric Investigation 2009;67(1):25‐31. [DOI: 10.1159/000158648] [DOI] [PubMed] [Google Scholar]
L'Abbé 1987
- L'Abbé KA, Detsky AS, O'Rourke K. Meta‐analysis in clinical research. Annals of Internal Medicine 1987;107:224‐33. [DOI] [PubMed] [Google Scholar]
Lee 1985
- Lee EJ, Williams K, Day R, Graham G, Champion D. Stereoselective disposition of ibuprofen enantiomers in man. British Journal of Clinical Pharmacology 1985;19(5):669‐74. [DOI: 10.1111/j.1365-2125.2004.02288.x] [DOI] [PMC free article] [PubMed] [Google Scholar]
McQuay 2005
- McQuay HJ, Moore RA. Placebo. Postgraduate Medical Journal 2005;81:155‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
McQuay 2012
- McQuay HJ, Derry S, Eccleston C, Wiffen PJ, Moore RA. Evidence for analgesic effect in acute pain ‐ 50 years on. Pain 2012;153(7):1364‐7. [DOI: 10.1016/j.pain.2012.01.024] [DOI] [PubMed] [Google Scholar]
Moher 1999
- Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of meta‐analyses of randomised controlled trials: the QUOROM statement. Lancet 1999;354:1896‐900. [DOI: 10.1016/S0140-6736(99)04149-5] [DOI] [PubMed] [Google Scholar]
Moore 1996
- Moore A, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics. Pain 1996;66(2‐3):229‐37. [DOI: 10.1016/0304-3959(96)03032-1] [DOI] [PubMed] [Google Scholar]
Moore 1997a
- Moore A, Moore O, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics: use of pain intensity and visual analogue scales. Pain 1997;69(3):311‐5. [DOI: 10.1016/S0304-3959(96)03306-4] [DOI] [PubMed] [Google Scholar]
Moore 1997b
- Moore A, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics: verification from independent data. Pain 1997;69(1‐2):127‐30. [DOI: 10.1016/S0304-3959(96)03251-4] [DOI] [PubMed] [Google Scholar]
Moore 1998
- Moore RA, Gavaghan D, Tramer MR, Collins SL, McQuay HJ. Size is everything-large amounts of information are needed to overcome random effects in estimating direction and magnitude of treatment effects. Pain 1998;78(3):209‐16. [DOI: 10.1016/S0304-3959(98)00140-7] [DOI] [PubMed] [Google Scholar]
Moore 2003
- Moore RA, Edwards J, Barden J, McQuay HJ. Bandolier's Little Book of Pain. Oxford: Oxford University Press, 2003. [ISBN: 0‐19‐263247‐7] [Google Scholar]
Moore 2005
- Moore RA, Edwards JE, McQuay HJ. Acute pain: individual patient meta‐analysis shows the impact of different ways of analysing and presenting results. Pain 2005;116(3):322‐31. [DOI: 10.1016/j.pain.2005.05.001] [DOI] [PubMed] [Google Scholar]
Moore 2006
- Moore A, McQuay H. Bandolier's Little Book of Making Sense of the Medical Evidence. Oxford: Oxford University Press, 2006. [ISBN: 0‐19‐856604‐2] [Google Scholar]
Moore 2011a
- Moore RA, Derry S, McQuay HJ, Wiffen PJ. Single dose oral analgesics for acute postoperative pain in adults. Cochrane Database of Systematic Reviews 2011, Issue 9. [DOI: 10.1002/14651858.CD008659.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2013a
- Moore A, Derry S, Eccleston C, Kalso E. Expect analgesic failure; pursue analgesic success. BMJ 2013;346:f2690. [DOI: 10.1136/bmj.f2690] [DOI] [PubMed] [Google Scholar]
Moore 2013b
- Moore RA, Derry S, Straube S, Ireson‐Pain J, Wiffen PJ. Faster, higher, stronger? Evidence for formulation and efficacy for ibuprofen in acute pain. Pain 2013;epub 14 August. [DOI: 10.1016/j.pain.2013.08.013] [DOI] [PubMed] [Google Scholar]
Morris 1995
- Morris JA, Gardner MJ. Calculating confidence intervals for relative risk, odds ratio and standardised ratios and rates. In: Gardner MJ, Altman DG editor(s). Statistics with Confidence ‐ Confidence Intervals and Statistical Guidelines. London: British Medical Journal, 1995:50‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nuesch 2010
- Nüesch E, Trelle S, Reichenbach S, Rutjes AW, Tschannen B, Altman DG, et al. Small study effects in meta‐analyses of osteoarthritis trials: meta‐epidemiological study. BMJ 2010;341:c3515. [DOI: 10.1136/bmj.c3515] [DOI] [PMC free article] [PubMed] [Google Scholar]
PACT 2013
- Prescription Cost Analysis, England 2012. London: Health and Social Care Information Centre, 2013. [ISBN: 978‐1‐84‐636859‐2]
Phleps 2001
- Phleps W. Overview on clinical data of dexibuprofen. Clinical Rheumatology 2001;20(Suppl 1):S15‐2. [DOI] [PubMed] [Google Scholar]
RevMan 2012 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Singer 2000
- Singer F, Mayrhofer F, Klein G, Hawel R, Kollenz CJ. Evaluation of the efficacy and dose‐response relationship of dexibuprofen (S(+)‐ibuprofen) in patients with osteoarthritis of the hip and comparison with racemic ibuprofen using the WOMAC osteoarthritis index. International Journal of Clinical Pharmacology and Therapeutics 2000;38(1):15‐24. [DOI] [PubMed] [Google Scholar]
Toms 2008
- Toms L, McQuay HJ, Derry S, Moore RA. Single dose oral paracetamol (acetaminophen) for postoperative pain in adults. Cochrane Database of Systematic Reviews 2008, Issue 4. [DOI: 10.1002/14651858.CD004602] [DOI] [PMC free article] [PubMed] [Google Scholar]
Zheng 2008
- Zheng C, Hao H, Wang G, Sang G, Sun J, Li P, et al. Chiral separation of ibuprofen and chiral pharmacokinetics in healthy Chinese volunteers. European Journal of Drug Metabolism and Pharmacokinetics 2008;33(1):45‐51. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Moore 2009
- Moore RA, Derry S, McQuay HJ. Single dose oral dexibuprofen [S(+)‐ibuprofen] for acute postoperative pain in adults. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD007550.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]