

Abstract
Background
Physical exercise training may form an important part of regular care for people with cystic fibrosis. This is an update of a previously published review.
Objectives
To assess the effects of physical exercise training on exercise capacity by peak oxygen consumption, pulmonary function by forced expiratory volume in one second, health‐related quality of life and further important patient‐relevant outcomes in people with cystic fibrosis.
Search methods
We searched the Cochrane Cystic Fibrosis and Genetic Disorders Group Trials Register which comprises references identified from comprehensive electronic database searches and handsearches of relevant journals and abstract books of conference proceedings.
Date of the most recent search: 04 May 2017.
We searched ongoing trials registers (clinicaltrials.gov and the WHO ICTRP). Date of most recent search: 10 August 2017.
Selection criteria
All randomised and quasi‐randomised controlled clinical trials comparing exercise training of any type and a minimum duration of two weeks with conventional care (no training) in people with cystic fibrosis.
Data collection and analysis
Two authors independently selected studies for inclusion, assessed methodological quality and extracted data. The quality of the evidence was assessed using the GRADE system.
Main results
Of the 83 studies identified, 15 studies which included 487 participants, met the inclusion criteria. The numbers in each study ranged from nine up to 72 participants; two studies were in adults, seven were in children and adolescents and six studies included all age ranges. Four studies of hospitalised participants lasted less than one month and 11 studies were outpatient‐based, lasting between two months and three years. The studies included participants with a wide range of disease severity and employed differing levels of supervision with a mixture of types of training. There was also wide variation in the quality of the included studies.
This systematic review shows very low‐ to low‐quality evidence from both short‐ and long‐term studies that in people with cystic fibrosis aerobic or anaerobic physical exercise training (or a combination of both) has a positive effect on aerobic exercise capacity, pulmonary function and health‐related quality of life. No study reported on mortality; two studies reported on adverse events (moderate‐quality evidence); one of each study reported on pulmonary exacerbations (low‐quality evidence) and diabetic control (very low‐quality evidence). Although improvements were not consistent between studies and ranged from no effects to clearly positive effects, the most consistent effects of the heterogeneous exercise training modalities and durations were found for maximal aerobic exercise capacity (in four out of seven studies) with unclear effects on forced expiratory volume in one second (in two out of 11 studies) and health‐related quality of life (in two out of seven studies).
Authors' conclusions
Evidence about the efficacy of physical exercise training in cystic fibrosis from 15 small studies with low to moderate methodological quality is limited. Exercise training is already part of regular outpatient care offered to most people with cystic fibrosis, and since there is some evidence for beneficial effects on aerobic fitness and no negative side effects exist, there is no reason to actively discourage this. The benefits from including physical exercise training in an individual's regular care may be influenced by the type and duration of the training programme. High‐quality randomised controlled trials are needed to comprehensively assess the benefits of exercise programmes in people with cystic fibrosis and the relative benefits of the addition of aerobic versus anaerobic versus a combination of both types of physical exercise training to the care of people with cystic fibrosis.
Plain language summary
Physical training to improve exercise capacity in people with cystic fibrosis
Review question
We reviewed the evidence about whether physical exercise training improves low aerobic fitness, improves health‐related quality of life and slows the decline in lung function in people with cystic fibrosis (CF). This is an update of a previously published review.
Background
CF affects many systems in the body, but mainly the lungs. It causes shortness of breath and limits the amount of exercise people with the condition can tolerate. The progress of lung disease leads to a low ability to exercise and physical inactivity, which in turn affects health and health‐related quality of life. We looked for studies where people with CF of any age did aerobic training (continuous activity at a low to moderate intensity, such as jogging, cycling, swimming or walking) or anaerobic training (weight or resistance training or sprinting at a high intensity for a short duration) or a combination of both compared to no training.
Search date
The evidence is current to: 04 May 2017.
Study characteristics
This review includes 15 studies with a total of 487 people with CF; the numbers in each study ranged from just nine people up to 72 people in the largest study. Two studies were in adults, seven were in children and adolescents and six studies included all age ranges. Four studies lasted less than one month and took place while the participants were in hospital; 11 studies were outpatient‐based and lasted from two months up to three years. The studies included people with a wide range of severity of CF lung disease. There were differing levels of supervision in the studies and a mixture of types of training.
The outcome most often reported in the studies was the change in lung function; other commonly reported outcomes included peak oxygen consumption, health‐related quality of life, change in muscle strength and change in body composition (e.g. muscle and fat).
Key results
Due to different study designs (type of exercise training, duration, etc.), we could not combine results from different studies. The short‐term studies did not show differences between treatments. The longer studies showed that physical exercise training can improve aerobic capacity, there were some improvements in lung function and health‐related quality of life, but these were not consistent across all studies. No study reported the number of deaths; two studies reported on side effects; one study reported on pulmonary exacerbations and another on diabetic control.
Quality of the evidence
We included a number of small studies and thought the quality of these studies was moderate at best (only for side effects). Overall, there was only low‐ to very low‐quality evidence that aerobic or anaerobic physical exercise training (or a combination of both) has a positive effect on aerobic exercise capacity, pulmonary function and health‐related quality of life in people with CF. In four of the studies the participant characteristics at the start of the studies were different between groups, despite being put into the different treatment groups at random. It is not possible for people not to know which treatment group they are in when comparing exercise training to no exercise. However, we do not think the fact that people knew which treatment they were receiving would affect the results for lung function as long as the assessments were done properly. In contrast, there may be bias when the people assessing an individual's cardiopulmonary fitness are not blinded to which group the volunteer is in. In less than half of the included studies, the investigators tried to prevent the outcome assessors from knowing which groups the participants were in; and in only one study was the lead researcher blinded. The studies did not routinely measure health‐related quality of life and where it was measured, different measurement tools were used. Selective reporting of results maybe an issue, especially as most of the included studies were not listed in trial registries, which give advance details of the outcomes being measured. We are uncertain about the effects and further better quality studies will likely change these findings.
Summary of findings
Background
Description of the condition
Cystic fibrosis (CF) is the most common life‐limiting autosomal recessively inherited disease in populations of Northern European descent. The incidence of CF has been estimated as 1 in 3500 live births in the USA (CF Foundation 2009; CF Trust 2010). The prevalence in the European countries varies widely and was recently estimated as 0.840 per 10,000 (Farrell 2008). Although CF is a multisystem disease, the primary cause of death is respiratory failure (CF Trust 2010). Progressive respiratory disease results in an abnormal ventilatory response to exercise in CF, which contributes to dyspnoea (shortness of breath) and is a major limiting factor to exercise tolerance in this population (O'Neill 1987). In addition, a sedentary lifestyle contributes to the progression of physical and functional impairment in CF (Schneiderman 2014). A consequence of this is low aerobic fitness that is associated with reduced life expectancy (Nixon 1992).
Description of the intervention
Physical exercise training is defined as participation in a programme of regular vigorous physical activity designed to improve physical performance, cardiovascular function, muscle strength or any combination of these three (Shephard 1994). There are basically two different types of physical exercise training: aerobic training or anaerobic training, but none can be considered purely 'aerobic' or 'anaerobic' with respect to energy supply. Aerobic training usually involves periods of continuous training (e.g. cycling or running) for a length of time at a target intensity below the anaerobic threshold. Anaerobic training involves training (e.g. weight or resistance training or sprinting) at a high intensity for a short duration above the anaerobic threshold.
How the intervention might work
Physical exercise training has multiple beneficial effects. It contributes to the alleviation of dyspnoea and improves exercise tolerance in people with CF (Cerny 2013). Physical exercise training maintains pulmonary function by improving sputum clearance through a combination of hyperventilation, mechanical vibration, coughing and changes in sputum rheology leading to facilitated and increased sputum expectoration (Dwyer 2011; Dwyer 2017; Hebestreit 2001) and possibly training of respiratory muscles (Houston 2013).
Physical exercise training may also be an important part of the management of diabetes in CF, as exercise improves glycaemic control in type 1 diabetes mellitus by improving insulin sensitivity and reducing systemic inflammation (Galassetti 2013). Regular exercise may delay the onset of osteoporosis by preventing a reduction in bone mineral density (Tejero García 2011). Other postulated benefits of any physical exercise training may be decreased anxiety and depression, enhanced feelings of well‐being and health‐related quality of life (HRQoL) (Hebestreit 2014) and enhanced performance at work, recreational and sport activities (ACSM 2010). It is not clear how many weeks training are required to achieve these benefits or what combination of aerobic and anaerobic training is required. Non‐adherence to prescribed physical training may contribute to worsening signs and symptoms of respiratory disease, more frequent respiratory infections and a reduced ability to perform activities of daily living and thus ultimately have a detrimental effect on the individual's prognosis. Side effects of physical exercise training are extremely rare so that exercise can be considered safe in CF (Ruf 2010).
Why it is important to do this review
This review aims to provide evidence for the inclusion of physical exercise training in regular care for people with CF. This version of the review is an update of previous versions (Bradley 2002; Bradley 2008; Radtke 2015a).
Objectives
To assess the effects of physical exercise training on exercise capacity by peak oxygen consumption (VO2 peak), pulmonary function by forced expiratory volume at one second (FEV1), HRQoL and further important patient‐relevant outcomes in people with CF.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCT) or quasi‐RCTs.
Types of participants
People with CF, of any age, and any degree of disease severity, diagnosed on the basis of clinical criteria and sweat testing or genotype analysis.
Types of interventions
Any type of prescribed physical exercise training delivered to people with CF compared to usual care. Studies which involved pure respiratory muscle training were excluded. In a post hoc change it was stipulated that studies must have a duration of at least two weeks.
Types of outcome measures
Primary outcomes
Exercise capacity (VO2 peak reported either as L, mL per kg body weight or fat‐free mass or as per cent (%) predicted)
Pulmonary function (FEV1 reported either as L or % predicted and as absolute values or change from baseline)
HRQoL (measured by generic or disease‐specific instruments, or both using validated instruments or patient reports)
In a post hoc change, the fourth primary outcome 'mortality' was moved to secondary outcomes in line with Cochrane guidance to limit the number of primary outcomes to three.
Secondary outcomes
CF‐related mortality
Muscle strength and anaerobic exercise capacity, measured by muscle force tests (isokinetic or non‐isokinetic tests), a Wingate Anaerobic Test (WaNT) or by a supramaximal sprint test on a cycle ergometer measured by e.g. aerobic capacity as power in absolute values (Watt), adjusted for body weight, fat‐mass; fat‐free mass, or as % predicted), or muscle strength as kg or Nm or anaerobic capacity as peak power, mean power and fatigue index during a WaNT
Additional indices of exercise capacity (such as peak work capacity, peak heart rate, minute ventilation, lactate and functional capacity tests (six‐and 12‐minute walk tests; shuttle tests; three‐minute step test; sit‐to‐stand test); oxygenation; effort and fatigue)
Additional indices of pulmonary function, pulmonary diffusing capacity, ventilation inhomogeneity and respiratory muscle strength (such as forced vital capacity, forced expiratory flows between 25% and 75% of expirated volume, total lung capacity, functional residual capacity, residual volume, pulmonary diffusing capacity for carbon monoxide, pulmonary diffusing capacity for nitric oxide, lung clearance index and maximum inspiratory and expiratory pressures)
Physical activity, measured by self report (diary), validated questionnaires or objectively with pedometers (e.g. number of steps) or accelerometers (counts per min; time spent in different exercise intensities, e.g. light, moderate, vigorous physical activity)
Body composition, measured by weight (kg), body mass index (kg/m² or z scores), skinfolds (mm), bioelectrical impedance analysis or whole body air‐displacement plethysmography or dual‐energy X‐ray absorptiometry (e.g. fat mass, fat‐free mass in kg, % or % predicted)
-
Acute exacerbations
number of exacerbations
time to first exacerbation
Antibiotic use (including oral, intravenous or inhaled antibiotics)
Bone health (measured by dual X‐ray energy absorptiometry or peripheral quantitative computed tomography)
Diabetic control, measured by fasting blood glucose levels (mmol/L or mg/dL), insulin levels (mmol/L or mg/dL) or homeostasis model assessment (HOMA) or oral glucose tolerance test (blood glucose in mmol/L or mg/dL)
Compliance with physical exercise training, assessed by questionnaires, (online) diaries, or with exercise monitoring devices such as heart rate monitors
Adverse events related to the exercise intervention or exercise testing as part of intervention
Search methods for identification of studies
There are no restrictions regarding language or publication status.
Electronic searches
Relevant studies were identified from the Cystic Fibrosis and Genetic Disorders Group's Cystic Fibrosis Trials Register using the term: exercise. The Cystic Fibrosis Trials Register is compiled from electronic searches of the Cochrane Central Register of Controlled Trials (CENTRAL) (updated each new issue of the Cochrane Library), weekly searches of MEDLINE, a search of Embase to 1995 and the prospective handsearching of two journals ‐ Pediatric Pulmonology and the Journal of Cystic Fibrosis. Unpublished work is identified by searching through the abstract books of three major cystic fibrosis conferences: the International Cystic Fibrosis Conference; the European Cystic Fibrosis Conference and the North American Cystic Fibrosis Conference. For full details of all searching activities for the register, please see the relevant sections of the Cystic Fibrosis and Genetic Disorders Group website. Date of the most recent search of the Group's Cystic Fibrosis Trials Register: 04 May 2017.
We searched the ongoing trials database clinicaltrials.gov (https://clinicaltrials.gov/) using the terms: "physical activity" AND "cystic fibrosis". A further search was run using the terms "exercise" AND "physical activity" AND "training" AND "cystic fibrosis". Date of most recent search: 01 June 2017.
We also searched the WHO ICTRP (http://apps.who.int/trialsearch/) using the terms: "physical activity and cystic fibrosis". Date of the most recent search: 09 August 2017.
Searching other resources
The reference lists of each RCT and of review articles were searched for additional publications that may contain RCTs. Authors of studies included in this review and other experts in the field were contacted and asked for information on other published and unpublished studies.
Data collection and analysis
Selection of studies
Two authors (for the original review JB, FM; from the 2015 update onwards SK, TR) independently assessed the titles and abstracts of identified citations and selected the studies to be included in the review. They excluded non‐RCTs, those studies involving respiratory muscle training exclusively, those which did not have a programme of exercise training and those that did not meet the inclusion criteria, based on screening the abstracts or full text articles. If disagreement arose on the suitability of a study for inclusion in the review, the authors reached a consensus by discussion. The authors recorded any areas of disagreement. The studies that did not fulfil all of the inclusion criteria were excluded and their details listed with the reason for exclusion. A third review author solved all the discrepancies if disagreement or uncertainty of the two authors persisted.
Data extraction and management
Each author (SK, TR) independently extracted data using standard data acquisition forms containing details about: study design (parallel versus multi‐arm; single‐centre versus multicentre, participants and trial characteristics for baseline equality between groups, details on the number of participants screened for eligibility, randomised, analysed, excluded, lost to follow up and dropped out, method of randomisation and allocation concealment, blinding of personnel and outcome assessors, use of stratification, incomplete outcome data, selective reporting, use of intention‐to‐treat analysis); the detailed intervention (aerobic training versus no training; anaerobic training versus no training and a combination of both versus no training; duration of studies, i.e. short term (less than one month) and long term (more than one month) and whether the study was supervised, partially supervised or not supervised); and outcome measures (continuous and dichotomous). If disagreement arose on the quality of a study, the authors reached a consensus by discussion. If disagreement persisted, they contacted a third author. The authors recorded any areas of disagreement. One author (for the original review JB, from the 2015 update onwards TR) entered the data into the Cochrane software Review Manager (Review Manager 2014) and a second author (from the 2015 update onwards SK) reviewed it. The review authors contacted the authors of the included studies in case of unclear or missing data and information.
Assessment of risk of bias in included studies
For the original review two authors judged the methodological quality of the review (JB, FM). From the 2015 update onwards, two authors (SK, TR) independently assessed the risk of bias for each included study according to the Cochrane risk of bias tool (Higgins 2011). In particular, the authors examined details of the randomisation method with sequence generation, allocation concealment, degree of blinding, inclusion and exclusion criteria, dropouts or withdrawals, intention‐to‐treat and detailed statistical analysis. Authors also examined for selective reporting and any other potential sources of bias. The authors judged the risk of bias as low, unclear or high. Unexplained dropouts or an unequal number of dropouts across treatment groups was considered as a potential risk of bias. Likewise, a lack of important information, e.g. on adverse effects, missing data, statistical methods etc., was also considered as potential risk of bias.
Measures of treatment effect
The authors have currently only been able to report continuous outcome data and have calculated the mean differences (MD) with 95% confidence intervals (CIs) where between‐group differences in the mean change from baseline were recorded. When data on the standard deviation (SD) for an individual group were not available, but instead standard error (SE) of the difference was available they used the available calculator within the Review Manager software (Review Manager 2014). Where possible, the published standard error of the mean (SEM) was used, or alternatively, published CIs were taken to estimate SE. If in future updates of this review, different measurement scales are used for an outcome, e.g. different HRQoL scales, the authors plan to analyse the data using the standardised mean difference (SMD) with 95% CIs.
Also, if in future updates of this review, the authors are able to present data for dichotomous outcomes, e.g. mortality or adverse events, they plan to record the number of participants experiencing an event and the total number of participants by group. They will analyse the data and report the odds ratio (OR) (the odds that an outcome will occur given a particular treatment, compared to the odds of the outcome occurring in the absence of that treatment) with 95% CIs.
Unit of analysis issues
The authors have not included any cross‐over studies in this latest version of the review. If future versions of this review include cross‐over studies and if data are presented in published papers from paired statistical analyses or if available information is available to allow us to adjust for within‐patient correlation using the methods described by Elbourne (Elbourne 2002), we will use the generic inverse variance method for data analysis. If appropriate data are not presented to allow adjustment for within‐patient correlation, we will contact study investigators to request these data. If we are unable to make the necessary adjustments, we will describe data from cross‐over studies narratively in the review.
Dealing with missing data
The review authors contacted the investigators of studies included in this review for further study details and data and 12 investigators responded. The investigators of four studies stated that the requested data were not available (Klijn 2004; Michel 1989; Schneiderman‐Walker 2000; Selvadurai 2002). The investigator of a further study confirmed that the extracted data were correct and that no further data were available (Cerny 1989). The investigators of the Hebestreit study stated that they were in the process of writing up the abstract for publication ‐ the review authors have now included this study in the updated review (Hebestreit 2010). One investigator involved in the Phillips study, currently listed under Studies awaiting classification, confirmed that the study has been completed and the review authors updated the information in the table (Phillips 2008). In both publications by Santana‐Sosa, the means and SEs were reported for all variables; the review authors contacted the investigators for additional data (Santana‐Sosa 2012; Santana‐Sosa 2014). Finally, investigators of six studies provided additional raw data for this review update (Beaudoin 2017; Hebestreit 2010; Kriemler 2013; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014).
Assessment of heterogeneity
Due to the low number of included studies and variability of interventions, the authors were unable to combine data for any of the listed outcomes; however, if for future updates of this review the authors are able to combine any data, they will measure heterogeneity between studies using the the Chi² test and the I² statistic (Higgins 2003). The Chi² test measures the deviation of observed effect sizes from the underlying overall effect. A low P value (or a large Chi² statistic relative to its degree of freedom) provides evidence of heterogeneity of intervention effects (variation in effect estimates beyond chance). The authors will use a P value of 0.10, rather than the conventional level of 0.05, to determine statistical significance. The I² statistic, as defined by Higgins (Higgins 2011), measures heterogeneity as a percentage where a value:
• 0% to 40%: might not be important; • 30% to 60%: may represent moderate heterogeneity; • 50% to 90%: may represent substantial heterogeneity; • 75% to 100%: considerable heterogeneity. The importance of the observed value of I² depends on: (i) magnitude and direction of effects; and (ii) strength of evidence for heterogeneity (e.g. P value from the Chi² test, or a CI for I²).
Assessment of reporting biases
The authors assessed relevant bias and selective reporting by comparing the 'Methods' and 'Results' sections from the included papers and trial registries, if available. They have documented this information in the risk of bias tables and figures. If, for future updates of the review, they are able to include and combine a sufficient number of studies (n = 10), the authors will assess publication bias initially by visual inspection of a funnel plot, although they are aware that an asymmetrical funnel plot is not necessarily due to publication bias.
Data synthesis
The review authors used a fixed‐effect model for all outcome parameters using the Review Manager software (Review Manager 2014). The authors were unable to pool studies due to the low number of available studies, the use of different exercise types and different study durations. For future updates, the authors will use a random‐effects model if substantial or considerable heterogeneity exists. The random‐effects model incorporates any between‐study heterogeneity into a meta‐analysis if the number of studies is sufficient. The authors will select the MD when combining data and use forest plots to compare results across studies.
Subgroup analysis and investigation of heterogeneity
If the authors are able to include a sufficient number of studies (about n = 10) and they observe at least moderate heterogeneity in the pooled analyses, they will undertake subgroup analyses of children versus adults, supervised versus unsupervised training and disease severity.
Sensitivity analysis
If the authors are able to include a sufficient number of studies (n = 10) and in order to investigate whether heterogeneity impacted upon the overall pooled effect estimate, the authors plan to apply random‐effects modelling, and compare this with a fixed‐effect model. They also plan a sensitivity analysis with and without quasi‐randomised studies and based on the quality of the studies. The authors will exclude studies with a high risk of bias from the analysis.
Summary of findings tables and quality of the evidence (GRADE)
In a post hoc change in line with current Cochrane guidance, at the 2017 update we added a summary of findings table for each comparison presented in the review (Table 1; Table 2; Table 3). We selected the following seven outcomes to report (chosen based on relevance to clinicians and consumers):
Summary of findings for the main comparison. Summary of findings ‐ Aerobic training versus no physical training.
| Aerobic training compared with no physical training for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: Outpatients Intervention: Aerobic training Comparison: No physical training | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| No physical training | Aerobic training | |||||
|
Exercise capacity: change in VO2 peak during maximal exercise (mL/min per kg body weight) Follow‐up: from hospital discharge up to 3 years |
Short‐term improvements in exercise tolerance during aerobic training were significantly greater than with no physical training at hospital discharge and 1 month after hospital discharge. One study showed no difference between groups at 3 months and 1 study showed a significant improvement in exercise tolerance following aerobic training at 6 months compared to no physical training. No significant longer‐term differences between groups were observed. |
NA | 170 (4 studies) |
⊕⊝⊝⊝ very low1,2,3 | ||
|
Pulmonary function: change in FEV1 (% predicted) Follow‐up: from hospital discharge up to 3 years |
There were no short‐term differences between groups at hospital discharge or one month after hospital discharge. Two studies showed a significant improvement in pulmonary function during and following aerobic training at 3 months, 6 months and 18 months post‐training compared to no physical training. However, 1 study showed no significant differences in annual change of pulmonary function between groups were observed over 36 months. |
NA | 187 (5 studies) |
⊕⊕⊝⊝ low1,2 | ||
|
HRQoL: CFQ Quality of Well‐being Scale and perceived 'positive effects.' Follow‐up: one month after hospital discharge up to three years |
No significant differences between the groups were shown according to the CFQ. A significant improvement in HRQoL according to the Quality of Well‐being Scale was observed in the aerobic exercise group compared to the no physical training group at 1 month after hospital discharge, MD 0.10 (95% CI 0.03 to 0.17). Positive effects were reported by 43 out of 49 participants (not reported by treatment group). |
NA | 143 (3 studies) |
⊕⊕⊝⊝ low1,4 | ||
|
CF‐related mortality Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Pulmonary exacerbations: number of hospitalisations and number of days in hospital Follow‐up: up to three years |
There were no between‐group differences reported for the mean number of hospitalisations or mean number of days in hospital at year 1, 2 and 3. | NA | 65 (1 study) |
⊕⊕⊝⊝ low1,5 | ||
|
Diabetic control Follow‐up:NA |
Outcome not reported. | NA | ||||
|
Adverse events Follow‐up: up to two years |
One study reported that no adverse effects occurred. In the other study, 1 participant in the aerobic training group injured her ankle and missed 2 days of aerobic training. One participant from the control group developed haemoptysis and withdrew from the study. | NA | 71 (2 studies) |
⊕⊕⊕⊝ moderate1 | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CFQ: Cystic Fibrosis Questionnaire; CI: confidence interval; FEV1 : forced expiratory volume in 1 second; HRQoL: health‐related quality of life;MD: mean difference; NA: not applicable; VO2 peak: peak oxygen consumption. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
1. Downgraded once due to risk of bias: Methodological details of the studies relating to randomisation and allocation concealment were unclear; one study used an inadequate method of randomisation and allocation concealment which may have introduced bias. 2. Downgraded once due to applicability: the no physical training group of one study deteriorated more than expected, this should be taken into account when interpreting results. 3. Downgraded once due to applicability: in one study, the method of measuring VO2 was not validated and likely underestimates the true VO2 peak of the study participants. 4. Downgraded once due to imprecision and applicability: very limited numerical data reported and unclear if the measures and questionnaires used were validated in this population. 5. Downgraded once due to imprecision: very limited numerical data reported.
Summary of findings 2. Summary of findings ‐ Anaerobic training versus no physical training.
| Anaerobic training compared with no physical training for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: outpatients Intervention: anaerobic training Comparison: no physical training | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| No physical training | Anaerobic training | |||||
|
Exercise capacity: change in VO2 peak during maximal exercise (mL/min per kg BW) Follow‐up: from hospital discharge up to 3 years |
One study showed a significant improvement in exercise capacity following anaerobic training at 6 months compared to no physical training. No significant differences between groups were observed at any other time points. |
NA | 86 (3 studies) |
⊕⊕⊝⊝ low1,2 | ||
|
Pulmonary function: change in FEV1 (% predicted) Follow‐up: from hospital discharge up to 3 years |
Two studies showed a significant improvement in pulmonary function during and following anaerobic training at hospital discharge, 1 month after discharge, 3 months, 6 months and 18 months post‐training compared to no physical training. The second study showed no significant differences in lung function at any time point. |
NA | 86 (3 studies) |
⊕⊕⊝⊝ low1,2 | ||
|
HRQoL: Quality of Well‐being Scale or HRQoL scale physical function Follow‐up: up to 2 years |
No significant differences between groups were observed according to the Quality of Well‐being Scale or HRQoL scale physical function. | NA | 64 (2 studies) |
⊕⊕⊝⊝ low1,3 | ||
|
CF‐related mortality Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Pulmonary exacerbations Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Diabetic control Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Adverse events Follow‐up: 2 years |
One study reported that no adverse effects occurred. | NA | 22 (1 study) |
⊕⊕⊕⊝ moderate1 | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; FEV1 : forced expiratory volume in 1 second; HRQoL: health‐related quality of life; NA: not applicable; VO2 peak: peak oxygen consumption. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
1. Downgraded once due to risk of bias: methodological details of the studies relating to randomisation and allocation concealment were unclear; one study used an inadequate method of randomisation and allocation concealment which may have introduced bias. 2. Downgraded once due to applicability: the no physical training group of one study deteriorated more than expected, this should be taken into account when interpreting results. 3. Downgraded once due to applicability: unclear if the measures and questionnaires used were validated in this population.
Summary of findings 3. Summary of findings ‐ Combined aerobic and anaerobic training versus no training.
| Combined aerobic and anaerobic training compared with no physical training for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: outpatients Intervention: combined aerobic and anaerobic training Comparison: no physical training | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| No physical training | Combined aerobic and anaerobic training | |||||
|
Exercise capacity: change in VO2 peak during maximal exercise (mL/min per kg body weight) Follow‐up: 12 weeks to two years |
A significantly higher VO2 peak was found in the combined training compared to the no physical training group after 12 to 18 months in 1 study. No significant difference between groups was found at any other time point. |
NA | 52 (2 studies) |
⊕⊕⊝⊝ low1,2 | Two additional studies recruiting 42 participants showed significant group x time interactions for VO2 peak; however, these results are not included in this review due to concerns over inconsistencies in the data provided to us by the original trial authors. | |
|
Pulmonary function: change in FEV1 (% predicted) or mL Follow‐up: 12 weeks to two years |
No significant differences in pulmonary function were observed between treatment groups at any time point. | NA | 103 (3 studies) |
⊕⊕⊝⊝ low1,2 | ||
|
HRQoL: CFQ, Medical Outcomes Study‐36 Item Short‐Form Health Survey, SF‐36 Follow‐up: 12 weeks to 2 years |
Two studies showed no significant differences in any HRQoL scale. One study showed a significant improvement in subjective health perception in the combined training group after 3 to 6 months and after 12 to 18 months (but not between 6 and 12 months). |
NA | 93 (3 studies) |
⊕⊝⊝⊝ very low1,2,3 | ||
|
CF‐related mortality Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Pulmonary exacerbations Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Diabetic control Follow‐up: 12 weeks |
Significant differences in some of the parameters were observed in the no physical training group compared to the combined training group and vice versa. Also no significant differences were observed for some parameters. |
NA | 14 (1 study) |
⊕⊝⊝⊝ very low1,2,3 | The study reported a range of metabolic parameters (HbA1c(%), Glucose AUC, Total Insulin AUC, Insulin Sensitivity Index) Plasma Glucose and Plasma Insulin. | |
|
Adverse events Follow‐up: NA |
Outcome not reported. | NA | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). AUC: area under the curve; CFQ: Cystic Fibrosis Questionnaire; CI: confidence interval; FEV1 : forced expiratory volume in 1 second; HRQoL: health‐related quality of life; NA: not applicable; VO2 peak: peak oxygen consumption. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
1. Downgraded once due to risk of bias: methodological details of the studies relating to randomisation and allocation concealment were unclear; one study used an inadequate method of randomisation and allocation concealment which may have introduced bias. 2. Downgraded once due to risk of bias: one study had many methodological inadequacies including early termination and low statistical power. These inadequacies are likely to have impacted on results. 3. Downgraded once due to imprecision: wide CIs around effect estimates due to small numbers of participants analysed.
Exercise capacity
Pulmonary function
HRQoL
CF‐related mortality
Pulmonary exacerbations
Diabetic control
Adverse events
We determined the quality of the evidence using the GRADE approach; and downgraded evidence in the presence of a high risk of bias in at least one study, indirectness of the evidence, unexplained heterogeneity or inconsistency, imprecision of results, high probability of publication bias. We downgraded evidence by one level if they considered the limitation to be serious and by two levels if very serious.
Results
Description of studies
See Characteristics of included studies; Characteristics of excluded studies; Characteristics of studies awaiting classification.
Results of the search
Please see the study flow chart for details (Figure 1). The combined searches to date have identified 123 individual references to 83 unique studies. A total of 15 studies (30 references) are included, 51 studies (73 references) have been excluded (for further details, see Excluded studies),13 studies (15 references) are currently awaiting assessment and four studies (five references) are ongoing.
1.
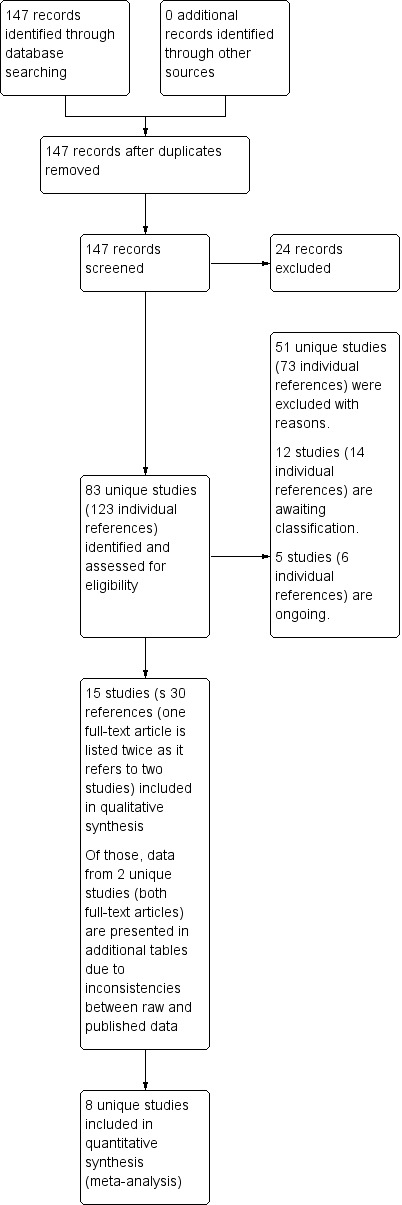
Study flow diagram.
Included studies
Of the 83 studies identified, 15 studies with a total of 487 participants met the inclusion criteria (Beaudoin 2017; Cerny 1989; Douglas 2015; Hebestreit 2010; Hommerding 2015; Klijn 2004; Kriemler 2013; Michel 1989; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002; Schneiderman‐Walker 2000; Turchetta 1991).
Trial characteristics
All included studies were of a randomised parallel group design. The study by Beaudoin was registered as randomised cross‐over study (ClinicalTrials.gov) but results were reported as randomised parallel group design in the final publication (Beaudoin 2017). Thirteen studies were single‐centre studies (Beaudoin 2017; Cerny 1989; Douglas 2015; Hommerding 2015; Klijn 2004; Michel 1989; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002; Schneiderman‐Walker 2000; Turchetta 1991) and two studies were national multicentre studies conducted in Germany and Switzerland (Hebestreit 2010; Kriemler 2013). The size of trials varied from a minimum number of nine participants (Michel 1989) to a maximum of 72 participants (Schneiderman‐Walker 2000). In one study the number of participants in each group was not reported and the MD between the treatment and control groups could not be calculated (Michel 1989).
There was wide heterogeneity in study designs with eight studies using a supervised training approach (Cerny 1989; Douglas 2015; Klijn 2004; Michel 1989; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002; Turchetta 1991); six studies a partially‐supervised approach (Beaudoin 2017; Hebestreit 2010; Hommerding 2015; Kriemler 2013; Rovedder 2014; Schneiderman‐Walker 2000) and one an unsupervised training approach (Moorcroft 2004).
Four studies were of short duration (less than one month) and were carried out during hospitalisations (Cerny 1989; Michel 1989; Selvadurai 2002; Turchetta 1991). In one study the hospital admission was for routine assessment (Turchetta 1991); in two further studies, the hospital admission was due to an acute exacerbation requiring intravenous antibiotic treatment (Cerny 1989; Selvadurai 2002); and in the fourth study, the reason for and the duration of admission were not reported (Michel 1989). The remaining 11 longer‐term studies (more than one month) were outpatient‐based (Hebestreit 2010; Hommerding 2015; Klijn 2004; Kriemler 2013; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Schneiderman‐Walker 2000). Both Santana‐Sosa studies used a two‐month training period including a one‐month detraining period, during which the participants did not engage in supervised exercise training (Santana‐Sosa 2012; Santana‐Sosa 2014). Three studies were home‐based training studies lasting three months (Beaudoin 2017; Hommerding 2015; Rovedder 2014). The Klijn study was a three‐month study with a three‐month follow up (Klijn 2004). The Hebestreit and Kriemler studies were both of six months duration including a six‐ and 18‐month follow‐up period (Hebestreit 2010; Kriemler 2013). The Moorcroft study was a 12‐month study (Moorcroft 2004), the Douglas study is a 24‐month intervention study (Douglas 2015) and the Schneiderman‐Walker study lasted three years (Schneiderman‐Walker 2000).
Follow‐up studies off training were undertaken in seven studies (Hebestreit 2010; Klijn 2004; Kriemler 2013; Michel 1989; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002).
Participants
Two studies included adults only (Beaudoin 2017; Moorcroft 2004); seven studies included children and adolescents only (Douglas 2015; Hommerding 2015; Klijn 2004; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002; Turchetta 1991) and six studies included both adults and children (Cerny 1989; Hebestreit 2010; Kriemler 2013; Michel 1989; Rovedder 2014; Schneiderman‐Walker 2000). Overall, the studies included participants with a broad range of disease severity.
The vast majority of studies included participants of both sexes (Beaudoin 2017; Douglas 2015; Hebestreit 2010; Hommerding 2015; Klijn 2004; Kriemler 2013; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002; Schneiderman‐Walker 2000; Turchetta 1991); however, no information was available for two studies (Cerny 1989, Michel 1989). Eight studies provided detailed information about the proportion of male and female participants at baseline (Hebestreit 2010; Hommerding 2015; Kriemler 2013; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002; Turchetta 1991).
In seven of the 11 studies published as full‐text articles, FEV1 % predicted values were used as exclusion criteria (Beaudoin 2017; Hebestreit 2010; Klijn 2004; Kriemler 2013; Santana‐Sosa 2012; Santana‐Sosa 2014, Schneiderman‐Walker 2000); this was also true of the study only available from ClinicalTrials.gov (Douglas 2015). The remaining five studies published as full‐text articles did not specify disease severity based on FEV1 or other outcomes (Cerny 1989; Hommerding 2015; Moorcroft 2004; Rovedder 2014; Selvadurai 2002), but no information was available in the remaining two studies (Michel 1989; Turchetta 1991).
In four of the studies, the baseline characteristics of the participants were different between groups despite randomisation (Cerny 1989; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014). In the Cerny study, FEV1 and FEF25‐75 were significantly lower in the control compared to the training group at admission (Cerny 1989). In both Santana‐Sosa studies, the training groups had a lower aerobic exercise capacity (VO2 peak) and lower muscle strength (most but not all strength measures) (Santana‐Sosa 2012, Santana‐Sosa 2014). In the study by Rovedder, a significantly lower body mass index (BMI) was observed in the intervention group compared to the control group (Rovedder 2014).
In the study by Kriemler, the control group experienced an unusual deterioration of physical health during the study and the results should be interpreted with caution (Kriemler 2013).
Interventions
As the aim of this review was to assess the efficacy of physical exercise training, studies which involved respiratory muscle training exclusively were excluded. All 15 studies included a control group which did not receive a prescribed exercise programme. Two studies compared two different types of exercise training programmes (aerobic training or anaerobic training) with a control group (Kriemler 2013; Selvadurai 2002). One study compared anaerobic training alone to a control group (Klijn 2004). Five studies compared aerobic training alone to a control group (Cerny 1989; Hommerding 2015; Michel 1989; Schneiderman‐Walker 2000; Turchetta 1991). Five studies compared the effects of a combined training programme (a mixture of aerobic and anaerobic exercise training) to a control group (Beaudoin 2017; Douglas 2015; Moorcroft 2004; Rovedder 2014, Santana‐Sosa 2012). One study used a home‐based exercise training with aerobic and strengthening exercises without training supervision (Rovedder 2014). The later Santana‐Sosa study compared a combined programme (aerobic and strength) including additional inspiratory muscle training with a control group (Santana‐Sosa 2014). In a further study, an individualised exercise programme including endurance type or strengthening exercises or a combination of both regimens was compared with a control group (Hebestreit 2010). The Santana‐Sosa and the Hebestreit studies were added to the section combined aerobic and anaerobic training (Hebestreit 2010; Santana‐Sosa 2014).
In two studies, all participants additionally received intravenous antibiotic treatment (Cerny 1989; Selvadurai 2002).
Outcomes
The most commonly reported outcome measure was the change in FEV1 which was reported in all studies except one (Michel 1989). The change in VO2 peak was documented in nine studies (Beaudoin 2017; Hebestreit 2010; Hommerding 2015; Klijn 2004; Kriemler 2013; Santana‐Sosa 2012; Santana‐Sosa 2014; Schneiderman‐Walker 2000; Selvadurai 2002). The change in HRQoL was also reported in nine studies (Beaudoin 2017; Hebestreit 2010; Hommerding 2015; Klijn 2004; Kriemler 2013; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002), the change in muscle strength was reported in eight studies (Beaudoin 2017; Hebestreit 2010; Klijn 2004; Kriemler 2013; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002). The change in body composition was reported in 11 studies (Beaudoin 2017; Hebestreit 2010; Hommerding 2015; Klijn 2004; Kriemler 2013; Michel 1989; Moorcroft 2004; Santana‐Sosa 2012; Santana‐Sosa 2014; Schneiderman‐Walker 2000; Selvadurai 2002). The change in physical activity was reported in six studies (Beaudoin 2017; Hebestreit 2010; Hommerding 2015; Kriemler 2013; Schneiderman‐Walker 2000; Selvadurai 2002) and the change in other indices of exercise capacity (other than cardiopulmonary exercise testing) in four studies (Cerny 1989; Hommerding 2015; Moorcroft 2004; Rovedder 2014). Only one study reported on changes in diabetic control after an exercise training intervention (Beaudoin 2017).
Excluded studies
We excluded 51 studies for the reasons which follow: 16 studies were not RCTs (Andreasson 1987; Asher 1982; Balfour 1998; Barry 2001; Bongers 2015; de Jong 1994; Edlund 1986; Heijerman 1992; NCT02277860; NCT02715921; NCT03117764; Orenstein 1981; Petrovic 2013; Salh 1989; Stanghelle 1998; Tuzin 1998); 24 studies did not include a physical training programme as per our protocol (Alarie 2012; Albinni 2004; Amelina 2006; Aquino 2006; Balestri 2004; Bieli 2017; Bilton 1992; Chang 2015; Chatham 1997; Dwyer 2008; Falk 1988; Giacomodonato 2015; Haynes 2016; Irons 2012; Lannefors 1992; NCT02821130; NCT02875366; Ozaydin 2010; Patterson 2004; Rand 2012; Reix 2012; Salonini 2015; Vallier 2016; Vivodtzev 2013); eight studies did not use a control arm with 'no physical training' (Calik‐Kutukcu 2016; del Corral Nunez‐Flores 2011; Gruet 2012; Kuys 2011; Lima 2014; Lowman 2012; Orenstein 2004; Shaw 2016); and three studies were acute exercise studies and of insufficient duration (less than 14 days) to be included in this review (Dwyer 2017; Kriemler 2016; Wheatley 2015).
Studies awaiting classification
There are 13 studies awaiting classification (ACTRN12617001009303; Almajan 2011; Housinger 2015; Johnston 2004; Lorenc 2015; Mandrusiak 2011; NCT00609050; NCT00792194; NCT02552043; NCT03100214; NCT03109912; Oliveira 2010; Phillips 2008). One author of the study informed us that the trial has been terminated prematurely due to recruitment problems and that no paper will be published from this study (NCT00792194).
Trial characteristics
Nine of the 13 studies awaiting classification were of a randomised parallel group design (ACTRN12617001009303; Almajan 2011; Johnston 2004; Lorenc 2015; Mandrusiak 2011; NCT00792194; NCT02552043; NCT03100214; NCT03109912; Phillips 2008). One study was described as a modified RCT (Housinger 2015) and one study used a cross‐over design (NCT00609050). The study by Phillips (published as abstract only) was described as controlled, prospective clinical trial (Phillips 2008), but is it not clear from the abstract whether the two study groups were randomly allocated. We contacted one author of this study, but we did not receive an answer. All studies were single‐centre studies and the study size ranged from 12 to 150 participants (ACTRN12617001009303; Almajan 2011; Housinger 2015; Johnston 2004; Lorenc 2015; Mandrusiak 2011; NCT00609050; NCT00792194; NCT02552043; NCT03100214; NCT03109912; Oliveira 2010; Phillips 2008).
Inclusion and exclusion criteria were reported in five studies (ACTRN12617001009303; NCT00792194; NCT02552043; NCT03100214; NCT03109912). Six studies included children (Almajan 2011; Johnston 2004; Mandrusiak 2011; NCT00609050; NCT02552043; Oliveira 2010); seven studies included children, adolescents and adults (ACTRN12617001009303; Housinger 2015; Lorenc 2015; NCT00792194; NCT03100214; NCT03109912; Phillips 2008).
Interventions
There was a great variety between studies with respect to exercise training modalities and approaches. Three studies were of a combined aerobic and anaerobic home‐based exercise training (NCT00792194; NCT03109912; NCT00609050). One study focused on aerobic type exercises during a six‐week supervised programme followed by a 16‐week home‐based programme (Johnston 2004). Four exercise training studies were conducted with participants hospitalised for treatment of a pulmonary exacerbation (ACTRN12617001009303; Housinger 2015; NCT03100214; Phillips 2008); one of these was a web‐based intervention to promote physical activity participation (ACTRN12617001009303). One study was conducted in hospital followed by a 8‐ to 12‐week home‐based exercise training programme (Mandrusiak 2011). One study investigated the effects of active video games during a six‐week domiciliary pulmonary rehabilitation programme (NCT02552043) and another study investigated the feasibility and effectiveness of Tai Chi as exercise intervention (Lorenc 2015). Two studies did not report on the type of exercises included in their training study (Almajan 2011; Oliveira 2010).
Outcomes
Five studies reported on changes in FEV1 after exercise training (ACTRN12617001009303; Almajan 2011; NCT00609050; NCT03100214; NCT03109912); in one of these it was a secondary outcome (ACTRN12617001009303). Eight studies report on changes in exercise capacity measured with cardiopulmonary exercise testing (VO2 peak) (NCT00609050; NCT00792194) or exercise capacity measured by field exercise tests such as the six‐minute walk test (Housinger 2015; NCT03100214; NCT02552043); shuttle test (NCT03109912; Phillips 2008) or three‐minute step test (Oliveira 2010). One study did not specify the exercise test to measure aerobic capacity (Johnston 2004). Eight studies report on changes in HRQoL (ACTRN12617001009303; Housinger 2015; Lorenc 2015; NCT00609050; NCT02552043; NCT03100214; NCT03109912; Oliveira 2010) and three studies on changes in muscle strength after exercise training (Housinger 2015; NCT02552043; Phillips 2008). Four studies also report on changes in physical activity (ACTRN12617001009303; Almajan 2011; Johnston 2004; NCT03109912).
Ongoing studies
Four studies are listed as ongoing (Donadio 2017; Gupta 2017; Hebestreit 2016; NCT02700243).
Trial characteristics
All four studies are of a randomised parallel group design (Donadio 2017; Gupta 2017; Hebestreit 2016; NCT02700243) and registered with clinicaltrials.gov (https://clinicaltrials.gov/) or WHO ICTRP (http://apps.who.int/trialsearch/). Three studies are single‐centre studies (Donadio 2017; Gupta 2017; NCT02700243) and one study in an international, multi‐centre study (Hebestreit 2016). The studies range in duration, from three months (Donadio 2017), over one year (Gupta 2017; Hebestreit 2016) to two years (NCT02700243). Inclusion and exclusion criteria are specified for all studies (Donadio 2017; Gupta 2017; Hebestreit 2016; NCT02700243). All four studies include both genders and focus on either children and adults (Donadio 2017; Hebestreit 2016), only children and adolescents (Gupta 2017) or only adults (over 18 years) (NCT02700243). In two studies, participation in the exercise trial is restricted to participants with an FEV1 ≥ 20% predicted (Gupta 2017) and ≥ 35% predicted (Hebestreit 2016) and in one of these participants must additionally have access to the Internet (Hebestreit 2016). The target sample size in the studies ranges from a minimum of 30 to a maximum of 292 study participants (Donadio 2017; Gupta 2017; Hebestreit 2016; NCT02700243).
Interventions
There is a great variety in interventions with respect to the study designs. One study provides participants with a written manual with instructions regarding physical activity and investigates the effects of the programme on posture and balance (Donadio 2017). In the study by Gupta, study participants take part in a one‐year resistance exercise and plyometric jumping exercise training programme to improve bone mineral density (Gupta 2017). In the third study, participants take part in a partially supervised exercise training intervention using step counters and online diaries as motivational elements over a period of six months; in the second part of the study (also six months), supervision by exercise experts is withdrawn (Hebestreit 2016). The remaining study aims to evaluate whether the use of a fitness tracker (Fitbit®) and an exercise prescription is associated with increased daily physical activity and exercise tolerance in young adults with CF over a period of two years (NCT02700243).
Outcomes
The primary outcome measures of the studies are: changes in posture (Donadio 2017); bone mineral density (Gupta 2017); FEV1, % predicted (Hebestreit 2016) and submaximal exercise capacity (NCT02700243). All studies included HRQoL (Donadio 2017; Gupta 2017; Hebestreit 2016; NCT02700243) as secondary outcome and three studies included changes in FEV1 as secondary outcomes (Donadio 2017; Gupta 2017; NCT02700243). Several other secondary endpoints will be considered, listed under characteristics of ongoing studies.
Risk of bias in included studies
A risk of bias of each study was assessed according to the Cochrane risk of bias tool, which categorises studies into low, high or unclear risk of bias (Higgins 2011). The results are displayed graphically in the figures (Figure 2; Figure 3).
2.
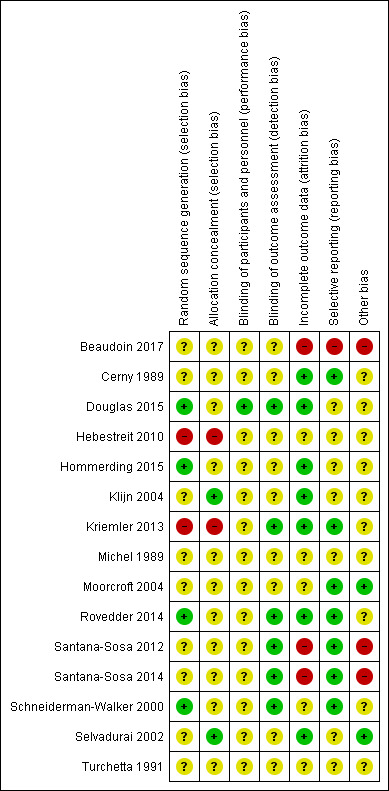
Methodological quality summary: review authors' judgments about each methodological quality item for each included study.
3.
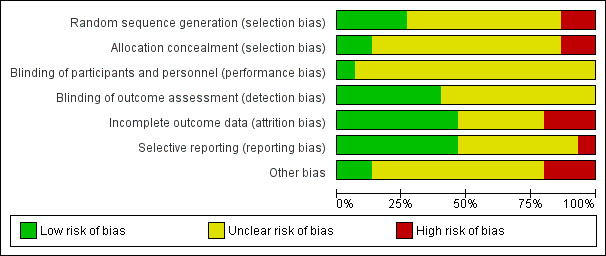
Methodological quality graph: review authors' judgments about each methodological quality item presented as percentages across all included studies.
Allocation
Sequence generation
Three studies described the methods used for generation of the randomisation sequence and were judged to have a low risk of bias (Hommerding 2015; Rovedder 2014; Schneiderman‐Walker 2000). A total of 10 studies were described as randomised, but did not give details of the methods used; these were deemed to have an unclear risk of bias (Beaudoin 2017; Cerny 1989; Douglas 2015; Klijn 2004; Michel 1989; Moorcroft 2004; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002; Turchetta 1991). In two studies, information on the generation of the random sequence was provided, but the method used in the studies can potentially introduce selection bias and lacks reproducibility; these were judged as having a high risk of bias (Hebestreit 2010; Kriemler 2013).
Allocation concealment
Only four studies described how allocation was adequately concealed. Two of these studies were judged to have a low risk of bias (Klijn 2004; Selvadurai 2002). The other two studies were judged as high risk of bias because allocation concealment is no longer given when the investigator is aware of the number of lots in the bag and if for one group all available lots have already been drawn out (Hebestreit 2010; Kriemler 2013). A total of 11 studies did not give any details of the method of allocation concealment (Beaudoin 2017; Cerny 1989; Douglas 2015; Hommerding 2015; Michel 1989; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Schneiderman‐Walker 2000; Turchetta 1991).
Blinding
None of the studies was obviously blinded for group assignment, as it is impossible to blind exercise training compared to no exercise training.
Blinding of participants and personnel (performance bias)
In two of the 13 included studies, one researcher of the study team was blinded to the participants group allocation (Rovedder 2014; Klijn 2004). Klijn reported that the primary researcher was blinded to group allocation, but their role in the study is not clear (Klijn 2004). In the Rovedder study , one researcher was blinded for randomisation, the intervention and was responsible for database entries (Rovedder 2014). We judged all included studies to have an unclear risk of bias.
Blinding of outcome assessment (detection bias)
In five of 15 studies, outcome assessors were blinded to group allocation (Kriemler 2013; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Schneiderman‐Walker 2000). These studies were deemed to have a low risk of bias. It is unclear whether outcome measures were assessed by blinded investigators in nine of the studies (Beaudoin 2017; Cerny 1989; Douglas 2015; Hebestreit 2010; Hommerding 2015; Michel 1989; Moorcroft 2004; Selvadurai 2002; Turchetta 1991) and one study reported that the primary researcher was blinded but is is not clear whether this person was responsible for outcome assessment (Klijn 2004).
Incomplete outcome data
We evaluated risk of bias for incomplete outcome data with respect to:
the use of an intention‐to‐treat analysis including appropriate methods for imputing data;
the dropout rate (balanced or unbalanced between groups) including a description of reasons for dropouts; and
the differentiation of the dropout rate between short‐term (less than one month) and long‐term studies (over one month).
Information about dropouts was provided in 12 studies (Beaudoin 2017; Cerny 1989; Hebestreit 2010; Hommerding 2015; Klijn 2004; Kriemler 2013; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Schneiderman‐Walker 2000; Selvadurai 2002). Three studies were published only in abstract form and did not give any details about dropouts (Douglas 2015; Michel 1989; Turchetta 1991).
Six studies were rated as having a low risk of bias for incomplete outcome data (Cerny 1989; Hommerding 2015; Klijn 2004; Kriemler 2013; Rovedder 2014, Selvadurai 2002). Two short‐term studies (Cerny 1989; Selvadurai 2002) and one long‐term study (Hommerding 2015) reported no dropouts. In three long‐term studies the dropout rate was balanced among groups and reasons for dropout were clearly reported (Klijn 2004; Kriemler 2013, Rovedder 2014). Additionally, Rovedder used multiple imputation to account for missing data in the statistical analysis (Rovedder 2014).
Three long‐term studies were rated as having a high risk of bias (Beaudoin 2017; Santana‐Sosa 2012; Santana‐Sosa 2014). In two studies, dropout rates were high and not balanced between groups. The use of intention‐to‐treat was reported in both studies, while in one study the last value carried forward method was applied (Santana‐Sosa 2012); in the second study, the method used for data imputation was not reported (Santana‐Sosa 2014). In the study by Beaudoin, the dropout rate (post‐randomisation) was 18% (n = 3) and the group allocation of two study participants was not reported (Beaudoin 2017). This study was registered as randomised cross‐over study (ClinicalTrials.gov), but the results were only reported for the first phase and the original publication described it as a parallel design study (Beaudoin 2017).
The remaining studies were rated as having an unclear risk of bias for incomplete outcome data (Douglas 2015; Hebestreit 2010; Michel 1989; Moorcroft 2004; Schneiderman‐Walker 2000; Turchetta 1991). Three of these studies were published only in abstract form and did not give any details about dropouts (Douglas 2015; Michel 1989; Turchetta 1991). In one long‐term study, dropouts were reported and balanced between groups, but reasons for dropouts were not described and intention‐to‐treat was not used (Hebestreit 2010). One study reported the reasons for participants dropping out and that an intention‐to‐treat analysis produced similar results for pulmonary function outcomes; however, data were only reported for 65 participants excluding dropouts (Schneiderman‐Walker 2000). Another study reported the use of an intention‐to‐treat analysis, but missing data were treated by omission rather than imputation and reasons for dropout were not clearly described (Moorcroft 2004).
Selective reporting
We judged seven studies to have a low risk of bias since they reported all outcomes detailed in the 'Methods' sections for all time points in the 'Results' section (Cerny 1989; Kriemler 2013; Moorcroft 2004, Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Schneiderman‐Walker 2000). One of these studies mentioned in the original publication that data for HRQoL would be addressed separately (Kriemler 2013). Data from this study were published together with data from another study which used similar methods (Hebestreit 2010); the combined data are presented in a separate paper (Hebestreit 2014).
Six studies did not report all outcomes and were deemed to have an unclear risk of bias (Hebestreit 2010; Hommerding 2015; Klijn 2004; Michel 1989; Selvadurai 2002; Turchetta 1991). Three of these studies were in abstract format and selective reporting could not be assessed (Douglas 2015; Michel 1989; Turchetta 1991); even so, we would expect the most common measure of lung function (FEV1) to be mentioned which it is not in one of these studies (Michel 1989). Three studies did not report all outcomes for HRQoL (Klijn 2004; Hebestreit 2010; Hommerding 2015) and anaerobic exercise capacity (Hebestreit 2010). Two studies did not report all variables for cardiopulmonary exercise testing as mentioned in the methods section (Hommerding 2015; Selvadurai 2002).
The study by Beaudoin was judged as high risk of bias for selective reporting, because the study was registered as randomised cross‐over study, but reported as a parallel‐design study. The second part of the study was not reported in the original publication. Moreover, oxygen saturation and heart rate were measured during cardiopulmonary exercise testing, but results were not reported in the full‐text publication (Beaudoin 2017).
Other potential sources of bias
Description of inclusion or exclusion criteria
Three studies are only available in abstract format and do not state inclusion or exclusion criteria, nor do they describe the methods of statistical analysis used which could be a source of bias (Douglas 2015; Michel 1989; Turchetta 1991). Six studies clearly stated inclusion and exclusion criteria which limits the potential for bias (Beaudoin 2017; Hebestreit 2010; Hommerding 2015; Kriemler 2013; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Selvadurai 2002). Three studies described the inclusion criteria but not the exclusion criteria, which could be a potential source of bias (Cerny 1989; Klijn 2004; Schneiderman‐Walker 2000).
Statistical analysis
A total of 11 studies clearly described the methods of statistical analysis, thus eliminating a potential source of bias (Cerny 1989; Hebestreit 2010; Hommerding 2015; Klijn 2004; Kriemler 2013; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014; Schneiderman‐Walker 2000; Selvadurai 2002).
In one study, the MD between the treatment and control groups could not be calculated, as the number of participants in each group was not reported (Michel 1989).
In one study, information on sample size and recruitment goals differ between the information provided on the trial registry and the final publication (Beaudoin 2017). The study aimed to recruit 24 participants (12 in each group) but the recruitment goal was not achieved (18 were recruited and only 17 randomised), but according to the power calculation provided in the original publication, 18 participants (nine per group) were required for the analysis. Only 14 participants actually completed the study (Beaudoin 2017).
Group characteristics
In five studies, significant between‐group differences existed at baseline despite randomisation (Cerny 1989; Kriemler 2013; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014). In one study, FEV1 and FEF25‐75 were significantly lower in the control compared to the training group at admission (Cerny 1989). In a second study, differences in exercise capacity (peak power was higher in the strength training group compared to the control group) and in vigorous physical activity (lower in the aerobic training group compared to controls) were evident at baseline (Kriemler 2013). In both Santana‐Sosa studies, the training groups had a lower aerobic exercise capacity (VO2 peak) and lower muscle strength (most but not all strength measures) (Santana‐Sosa 2012; Santana‐Sosa 2014). In the fifth study, BMI was significantly lower in the intervention group compared to the control group (Rovedder 2014). It is uncertain whether these factors could be a potential source of bias so we judged the risk to be unclear for significant between‐group differences at baseline.
In six of the 12 studies published as full‐text articles, FEV1 % predicted values were used as exclusion criteria (Beaudoin 2017; Hebestreit 2010; Klijn 2004; Kriemler 2013; Santana‐Sosa 2012; Santana‐Sosa 2014, Schneiderman‐Walker 2000). We accept that studies which exclude participants on the basis of one of our outcomes may cause a risk of bias to the review. However, the risk of exercise‐induced adverse effects is likely to be higher in people with severe CF lung disease and many researchers tend to exclude those people because of this. In one study, financial support was provided to the training group participants to foster the activity plan; this study was judged as having an unclear risk of bias (Hebestreit 2010).
Intervention
In the original publication, no information was provided on the control intervention. We noticed discrepancies between the registered (clinicaltrials.gov) and published trial design (cross‐over versus parallel‐group design) (Beaudoin 2017).
Data discrepancies
Three studies were rated as having a high risk of bias (Beaudoin 2017; Santana‐Sosa 2012; Santana‐Sosa 2014). Two studies for which we received some raw data from the authors were rated as high risk of bias, due to inconsistencies between the raw data files and the data reported in the original publications (Santana‐Sosa 2012; Santana‐Sosa 2014). Furthermore, Beaudoin reported within‐group changes from baseline and not between‐group differences, as would be appropriate for a RCT (Beaudoin 2017). We calculated between‐group differences using raw data provided by the authors and our results suggest no between‐group differences for the primary endpoint. When considered alongside the fact that the stated power calculation requiring 18 participants to demonstrate a difference was not achieved (see above), there is a high risk of bias that the reported effects are not sound.
Effects of interventions
See: Table 1; Table 2; Table 3
Where primary studies reported differences between groups but did not provide adequate data (means and SD) that could be presented in the Review Manager software (Review Manager 2014), the information from the primary (original) study has been included in the results. It was not possible to pool data for any outcomes due to variations in the type and duration of studies, the times at which outcomes were measured, the different methods of reporting outcomes, the omission of data relating to either mean change from baseline for each group and the SD or SE.
We present the effects of the interventions according to training modalities, i.e. aerobic training, anaerobic training and combined aerobic and anaerobic training, these are further differentiated by length of training. There are four short‐term (less than one month) aerobic studies (Cerny 1989; Michel 1989; Selvadurai 2002; Turchetta 1991); three longer‐term aerobic studies ranging from six months to three years (Kriemler 2013; Hommerding 2015; Schneiderman‐Walker 2000); one short‐term anaerobic study (Selvadurai 2002); two longer‐term anaerobic studies ranging from three (Klijn 2004) to 24 months (Kriemler 2013); and five longer‐term combined aerobic and anaerobic training studies ranging from three to 24 months (Beaudoin 2017; Douglas 2015; Hebestreit 2010; Moorcroft 2004, Rovedder 2014).
In the two studies by Santana‐Sosa, means and SE were reported for baseline, post‐training and detraining and we were not able to calculate the MD (Santana‐Sosa 2012; Santana‐Sosa 2014). We received incomplete raw data files from the authors and due to inconsistencies in the provided data sets, we were unable to reproduce all data. Due to the review authors' concerns about data quality, both studies were excluded from the formal analysis in the review and data are provided in two additional tables at the end of the review (Table 4; Table 5). Two studies comparing aerobic exercise training with no training were published as abstracts (Michel 1989; Turchetta 1991) and no information on relevant outcomes for this review was available.
1. Study results for Santana‐Sosa 2012.
| Variable | Group | Pre‐training | Post‐training | Detraining | P value (group x time) | Comments |
| Age (mean (SE)) years | Intervention | 11 (3) | ‐ | ‐ | ‐ | |
| Control | 10 (2) | ‐ | ‐ | ‐ | ||
| Sex (% boys) | Intervention | 55 | ‐ | ‐ | ‐ | |
| Control | 64 | ‐ | ‐ | ‐ | ||
| VO2 peak (mean (95% CI)) ml/min per kg body weight | Intervention | n.a. | 3.9 (1.8 to 6.1) | ‐3.4 (‐5.7 to 1.7) | 0.036 | Significantly higher in controls at baseline (P = 0.023). Data were presented in a figure in the original publication. |
| Control | n.a. | ‐2.2 (‐5.3 to 0.1) | ‐0.7 (‐4.4 to 5.9) | |||
| Leg press (mean (95% CI)) kg | Intervention | n.a. | 24.9 (14.3 to 34.4) | ‐1.0 (‐4.1 to 3.3) | < 0.001 | Data are reported in a figure in the original publication. Significantly higher in controls at baseline (P = 0.014). |
| Control | n.a. | n.a. | n.a. | |||
| Bench press (mean (95% CI)) kg | Intervention | n.a. | 10.5 (7.0 to 14.0) | ‐1.2 (‐3.6 to 3.0) | < 0.001 | Significantly higher in controls at baseline (P = 0.007). Data presented in a figure in the original publication. |
| Control | n.a. | n.a. | n.a. | |||
| Seated row (mean (95% CI)) kg | Intervention | n.a. | 12.7 (9.2 to 16.0) | ‐0.2 (‐3.6 to 3.2) | < 0.001 | Significantly higher in controls at baseline (P = 0.009). Data presented in a figure in the original publication. |
| Control | n.a. | n.a. | n.a. | |||
| Oxygen saturation at peak exercise (mean (SE)) | Intervention | 94.9 (0.9)% | 95.6 (0.8)% | 94.5 (1.2)% | n.a. | |
| Control | 95.7 (0.5)% | 96.4 (0.4)% | 96.1 (0.5)% | |||
| FEV1 (mean (SE)) litres | Intervention | 1.87 (0.24) | 1.94 (0.23) | 1.90 (0.25) | 0.769 | |
| Control | 1.77 (0.17) | 1.87 (0.15) | 1.79 (0.19) | |||
| FVC (mean (SE)) litres | Intervention | 2.41 (0.24) | 2.49 (0.25) | 2.56 (0.29) | 0.920 | |
| Control | 2.29 (0.19) | 2.36 (0.20) | 2.40 (0.24) | |||
| PImax (mean (SE)) cm H2O | Intervention | 64.0 (5.5) | 69.8 (6.8) | 75.2 (6.2) | 0.797 | |
| Control | 61.5 (6.9) | 72.2 (7.2) | 76.4 (7.5) | |||
| HRQoL score ‐ children's report (median (range)) | Intervention | 696 (495 ‐ 741) | 719 (550 ‐ 734) | ‐ | 0.257 | HRQoL was assessed before and after the intervention. P value for comparison pre versus post‐training. |
| Control | 649 (578 ‐ 768) | 638 (461 ‐ 791) | ‐ | |||
| HRQoL score ‐ parents' report (median (range)) | Intervention | 896 (688‐1011) | 889 (811 ‐ 973) | ‐ | 0.143 | HRQoL was assessed before and after the intervention. |
| Control | 911 (842 ‐ 1028) | 978 (684 ‐ 1059) | ‐ | |||
| Weight (mean (SE)) kg | Intervention | 39.9 (3.5) | 40.5 (3.4) | 41.4 (3.4) | 0.723 | |
| Control | 34.0 (2.6) | 35.1 (2.8) | 36.2 (3.0) | |||
| BMI (mean (SE)) kg/m² | Intervention | 18.4 (1.0) | 18.3 (0.7) | 18.5 (0.7) | 0.959 | |
| Control | 17.2 (0.8) | 17.1 (0.8) | 17.4 (0.9) | |||
| Fat‐free mass (mean (SE)) % | Intervention | 78.1 (2.7) | 79.4 (2.8) | 78.8 (2.9) | 0.115 | |
| Control | 81.1 (2.5) | 80.9 (2.1) | 81.1 (2.2) | |||
| Body fat (mean (SE)) % | Intervention | 21.9 (2.7) | 20.6 (2.8) | 21.2 (2.9) | 0.115 | |
| Control | 18.9 (2.5) | 19.1 (2.1) | 18.9 (2.2) | |||
| Compliance with physical training (mean (SE)) % | Intervention | ‐ | 95.1 (7.4) | ‐ | ‐ ‐ |
73% of children completed all training sessions. |
| Control | ‐ | ‐ | ‐ | |||
| Adverse effects | Intervention | ‐ | ‐ | ‐ | ‐ | No adverse effects occurred during training or maximal exercise testing. |
| Control | ‐ | ‐ | ‐ |
BMI: body mass index CI: confidence interval FEV1: forced expiratory volume in one second FVC: forced vital capacity HRQoL: health‐related quality of life n.a.: not applicable PImax: maximum inspiratory mouth pressure SE: standard error VO2 peak: peak oxygen consumption
2. Study results for Santana‐Sosa 2014.
| Variable | Group | Pre‐training | Post‐training | Detraining | P value (group x time) | Comments |
| Age (mean (SE)) years | Intervention | 11 (1) | ‐ | ‐ | ‐ | |
| Control | 10 (1) | ‐ | ‐ | ‐ | ||
| Sex (% boys) | Intervention | 60 | ‐ | ‐ | ‐ | |
| Control | 60 | ‐ | ‐ | ‐ | ||
| VO2 peak (mean (95% CI) ml/min per kg body weight | Intervention | n.a. | 6.9 (3.4 to 10.5) | ‐1.5 (‐2.7 to ‐0.4) | < 0.001 | Significantly higher in controls at baseline (P = 0.034). |
| Control | n.a. | n.a. | n.a. | |||
| Leg press (mean (SE)) kg | Intervention | 62.5 (6.5) | 89.5 (9.3) | 88.6 (9.2) | < 0.001 | Significantly higher in controls at baseline (P = 0.046). |
| Control | 45.2 (4.7) | 43.9 (5.1) | 43.9 (5.4) | |||
| Bench press (mean (SE)) kg | Intervention | 26.4 (2.7) | 38.4 (3.2) | 35.9 (2.9) | < 0.001 | |
| Control | 23.2 (2.9) | 21.6 (3.2) | 21.7 (3.6) | |||
| Lateral row (mean (SE)) kg | Intervention | 30.5 (3.6) | 43.0 (4.2) | 35.9 (2.9) | < 0.001 | |
| Control | 23.2 (3.0) | 22.0 (3.1) | 21.7 (3.6) | |||
| Oxygen saturation at peak exercise (mean (SE)) % | Intervention | 94.7 (0.7) | 94.5 (0.7) | 93.1 (0.8) | n.a. | |
| Control | 96.4 (0.4) | 96.2 (0.5) | 96.1 (0.6) | |||
| FEV1 (mean (SE)) L | Intervention | 1.65 (0.19) | 1.74 (0.23) | 1.69 (0.24) | 0.486 | |
| Control | 1.57 (0.26) | 1.55 (0.26) | 1.59 (0.26) | |||
| FVC (mean (SE)) L | Intervention | 2.23 (0.27) | 2.34 (0.29) | 2.28 (0.28) | 0.156 | |
| Control | 1.90 (0.33) | 1.85 (0.32) | 1.92 (0.32) | |||
| PImax (mean (SE)) cm H2O | Intervention | 68.3 (6.3) | 107.6 (8.4) | 103.2 (8.1) | < 0.001 | |
| Control | 69.5 (9.7) | 71.8 (10.0) | 66.7 (9.4) | |||
| HRQoL score (median (min ‐ max)) | Intervention | 629 (505 ‐ 701) | 688 (609 ‐ 791) | ‐ | 0.071 | HRQoL was assessed before and after the intervention. |
| Control | 636 (626 ‐ 745) | 638 (626 ‐ 737) | ‐ | |||
| Weight (mean (SE)) kg | Intervention | 36.4 (3.1) | 37.8 (3.2) | 38.3 (3.1) | 0.342 | |
| Control | 31.5 (4.6) | 32.4 (4.7) | 32.7 (4.5) | |||
| Fat‐free mass (mean (SE)) % of total | Intervention | 81.6 (1.3) | 82.6 (1.0) | 82.5 (1.0) | 0.001 | |
| Control | 82.9 (1.8) | 82.8 (1.8) | 82.5 (1.9) | |||
| Body fat (mean (SE)) % of total | Intervention | 18.4 (1.3) | 17.4 (1.2) | 17.5 (1.1) | 0.023 | |
| Control | 17.1 (1.8) | 17.2 (1.8) | 17.5 (1.9) | |||
| Compliance with physical training (mean (SE)) % | Intervention | ‐ | 97.5 (1.7) | ‐ | 70% of children completed all training sessions. | |
| Control | ‐ | ‐ | ‐ | |||
| Adverse effects | Intervention | ‐ | ‐ | ‐ | No adverse effects occurred during training or exercise testing. | |
| Control | ‐ | ‐ | ‐ |
CI: confidence interval FEV1: forced expiratory volume in one second FVC: forced vital capacity HRQoL: health‐related quality of life n.a.: not applicable PImax: maximum inspiratory mouth pressure SE: standard error VO2 peak: peak oxygen consumption
Aerobic training versus no physical training
Five studies with 197 participants are included in this comparison (Cerny 1989; Hommerding 2015; Kriemler 2013; Schneiderman‐Walker 2000; Selvadurai 2002). In the study by Kriemler, the control group experienced an unusual deterioration of physical health during the study and the results should be interpreted with caution (Kriemler 2013).
Primary outcomes
1. Exercise capacity by VO2 peak
This outcome was reported in four studies (n = 180) (Hommerding 2015; Kriemler 2013; Schneiderman‐Walker 2000; Selvadurai 2002). Results are presented in the analysis (very low‐quality evidence) (Analysis 1.1).
1.1. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 1 Change in VO2 peak during maximal exercise (ml/min per kg BW).
In the short‐term study by Selvadurai, exercise capacity was measured by VO2 peak during a treadmill exercise test (Selvadurai 2002). Improvements in exercise tolerance during aerobic training were significantly greater than with no specific training after hospital discharge, MD 8.53 mL/min per kg body weight (95% CI 4.85 to 12.21). One month after hospital discharge VO2 peak remained significantly higher in the aerobic training group compared to the control group, MD 4.91 mL/min per kg body weight (95% CI 1.13 to 8.69) (Selvadurai 2002).
Two studies reported on this outcome after three months (Hommerding 2015; Kriemler 2013). In the study by Hommerding, exercise capacity was measured during cycle ergometry. No between‐group differences in VO2 peak (mL/min per kg body weight) were observed after three months, MD ‐1.20 mL/min per kg body weight (95% CI ‐7.26 to 4.86) (Hommerding 2015). In the study by Kriemler, VO2 peak (mL/min per kg body weight) was measured during cycle ergometry (Kriemler 2013). After three months, a significant difference in VO2 peak between the aerobic training group and the control group was observed, MD 9.71 mL/min per kg body weight (95% CI 0.86 to 18.56). When combined, the data from both studies showed no difference in VO2 peak between the exercise and control groups, pooled MD 2.29 (95% CI ‐2.71 to 7.29). Heterogeneity between these studies was high (I² = 75%); most likely due to the unusual deterioration of the control group.
In the Kriemler study, VO2 peak was significantly higher in the training compared to the control group after six months, MD 18.33 mL/min per kg body weight (95% CI 8.95 to 27.71). No differences between groups were observed at six and 18 months off training, MD 9.51 mL/min per kg body weight (95% CI ‐1.32 to 20.34) and 2.86 mL/min per kg body weight (95% CI ‐9.70 to 15.42), respectively.
In the study by Schneiderman‐Walker, VO2 peak was measured during cycle ergometry (Schneiderman‐Walker 2000). No significant difference between groups was found in the annual rate of decline in VO2 peak, MD 0.05 mL/min per kg body weight (95% CI ‐1.15 to 1.25) (Schneiderman‐Walker 2000).
2. Pulmonary function (FEV1)
This outcome was reported in five studies (n = 197) (Cerny 1989; Hommerding 2015; Kriemler 2013; Schneiderman‐Walker 2000; Selvadurai 2002). Results are presented in the analysis (low‐quality evidence) (Analysis 1.2).
1.2. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 2 Change in FEV1(% predicted).
Two short‐term aerobic training studies reported on change in FEV1 (Cerny 1989; Selvadurai 2002). In the study by Cerny, there was no difference in the change in FEV1 % predicted (Cerny 1989). In the study by Selvadurai there was no significant difference between the groups in FEV1 % predicted at hospital discharge, MD 2.03% (95% CI ‐2.31 to 6.37) and one month after discharge, MD 1.53% (95% CI ‐2.93 to 5.99) (Selvadurai 2002).
Three long‐term studies reported on changes in FEV1 after aerobic training compared to no exercise training (Hommerding 2015; Kriemler 2013; Schneiderman‐Walker 2000). In the study by Hommerding, no between‐group differences were observed in FEV1 % predicted after three months, MD ‐2.80% (95% CI ‐10.69 to 5.09). In the Kriemler study, the aerobic training group had significantly higher values for FEV1 % predicted compared to control group after three months, MD 12.81% (95% CI 6.91 to 18.71). When combined, the data from both studies showed a significant increase in favour of the exercise group, pooled MD 7.21% (95% CI 2.49 to 11.94). Heterogeneity between these studies was high (I² = 90%); most likely due to the unusual deterioration of the control group.
Also after six months, FEV1 % predicted was higher in the exercise compared to the control group, MD 17.17% (95% CI 8.59 to 25.75) (Kriemler 2013). At the six and 18 months off‐training period, a difference was found between the training and control group for FEV1, MD 16.92% (95% CI 6.07 to 27.77) and MD 12.45% (95% CI 1.27 to 23.63).
Schneiderman‐Walker reported on the effects of aerobic physical training on lung function at three years (Schneiderman‐Walker 2000). The control group was not significantly different from the intervention group in annual decline in FEV1 % predicted, MD 2.01% (95% CI ‐0.06 to 4.08) (Schneiderman‐Walker 2000).
3. Health‐related quality of life
This outcome was reported in three studies (n = 143) (low‐quality evidence) (Hommerding 2015; Schneiderman‐Walker 2000; Selvadurai 2002). No detailed results were presented for HRQoL scales in the study by Hommerding (Hommerding 2015).
Hommerding assessed HRQoL with the Cystic Fibrosis Questionnaire (Hommerding 2015). No effects of physical exercise training were found for HRQoL scales after the intervention. Selvadurai assessed HRQoL using the generic 'Quality of Well‐being Scale'. Since this scale was validated in an outpatient setting, assessment was undertaken on the participants' admission to hospital and during the follow‐up one month after their discharge, at which time there was a significant difference between the groups in favour of the intervention group for the change in HRQoL, MD 0.10 (95% CI 0.03 to 0.17) (Selvadurai 2002) (Analysis 1.3). Schneiderman‐Walker reported on attitudes toward physical activity and perceived feasibility of a regular aerobic exercise programme (Schneiderman‐Walker 2000). Positive effects, reported by 43 out of 49 participants, included generally feeling better about themselves, having more energy and less chest congestion. A small number of participants reported no differences. Both groups stated it would be feasible to meet aerobic exercise targets, if requested to do so by doctors (Schneiderman‐Walker 2000).
1.3. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 3 Change in health‐related quality of life.
Secondary outcomes
1. CF‐related mortality
No data were reported from any of the studies.
2. Muscle strength and anaerobic exercise capacity
This outcome was reported in two studies (n = 71) (Kriemler 2013; Selvadurai 2002).
In the Kriemler study, no significant differences in muscle strength measured by a leg Wingate anaerobic test (WAnT) (change in mean power in watt (W) per kg body weight) were observed between the study groups after three months, MD 0.28 W/kg body weight (95% CI ‐0.53 to 1.09) and six months, MD ‐0.09 (95%CI ‐0.92 to 0.74) (Analysis 1.4). No significant differences in leg muscle strength between the training and control group were found at the six months off‐training time point, MD 0.23 W/kg body weight (95% CI ‐0.65 to 1.11) and 18 months off training period, MD 0.28 W/kg body weight (95% CI ‐0.72 to 1.28) (Kriemler 2013).
1.4. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 4 Change in mean power during WAnT (W per kg BW).
In the study by Selvadurai, the aerobic training group had a significantly greater increase in lower limb muscle strength than the control group at hospital discharge, MD 8.13 Newton metres (Nm) (95% CI 4.49 to 11.77). This increase remained significant one month after discharge, MD 6.13 Nm (95% CI 2.47 to 9.79) (Selvadurai 2002) (Analysis 1.5).
1.5. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 5 Change in strength (Newton metres).
3. Additional indices of exercise capacity
These outcomes were reported in five studies (n = 187) (Cerny 1989; Hommerding 2015; Kriemler 2013; Schneiderman‐Walker 2000; Selvadurai 2002).
Three studies reported on peak exercise capacity (Cerny 1989; Kriemler 2013; Schneiderman‐Walker 2000). In the study by Cerny, results were presented in figures but raw data were not available for this study. Cerny reported no differences between groups in peak work capacity (Watt (W) per kg body weight) (Cerny 1989). In the Kriemler study, a significant difference between the training and control group was observed for peak work capacity after three months, MD 0.52 W/kg body weight (95% CI 0.17 to 0.87) and after six months, MD 0.81 W/kg body weight (95% CI 0.52 to 1.10) (Analysis 1.6). No between‐group differences existed after the six months off‐training period, MD 0.25 W/kg body weight (95% CI ‐0.11 to 0.61) and 18 months off‐training period, MD 0.13 W/kg body weight (95% CI ‐0.46 to 0.72).
1.6. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 6 Change in peak work capacity during maximal exercise (W per kg BW).
Schneiderman‐Walker reported on the annual rate of decline in peak work capacity (Schneiderman‐Walker 2000); no significant difference was found between groups, MD 0.82% (95% CI ‐1.91 to 3.55) (Analysis 1.7).
1.7. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 7 Annual rate of change in peak work capacity during maximal exercise over 36 month (%).
One study reported on treadmill speed (km/h) and treadmill exercise time (min) after three months (Hommerding 2015). In this study, no differences between groups were found in treadmill speed, MD ‐0.60 km/h (95% CI ‐2.03 to 0.83) or treadmill exercise time, MD ‐0.50 min (95% CI ‐2.06 to 1.06) (Analysis 1.8; Analysis 1.9).
1.8. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 8 Change in treadmill speed (km/h).
1.9. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 9 Change in treadmill exercise time (min).
Three studies reported on heart rate (Cerny 1989; Hommerding 2015; Schneiderman‐Walker 2000). In the study by Hommerding, no differences between groups were found for resting heart rate, MD 7.00 beats per min (bpm) (95% CI ‐5.35 to 19.35) or peak exercise heart rate, MD 4.00 bpm (95% CI ‐17.03 to 25.03) after three months (Hommerding 2015). The study by Schneiderman‐Walker reported that there was no significant difference in the annual rate of decline in peak heart rate between groups, MD 1.10 bpm (95% CI ‐0.85 to 3.05) (Analysis 1.10). Cerny did not present any data that we could analyse, but reported that there was no significant difference between control and treatment arms in change in peak heart rate or the ratio of peak heart rate to peak load (Cerny 1989).
1.10. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 10 Change in heart rate (beats per min).
One study measured oxygen saturation at rest (Hommerding 2015) and two studies reported on oxygenation during exercise (Hommerding 2015; Selvadurai 2002). In the study by Hommerding, no differences between the training and control groups were found in either resting oxygen saturation, MD ‐0.70% (95% CI ‐2.53 to 1.13) or peak oxygen saturation during maximal exercise, MD 9.60% (95% CI ‐5.20 to 24.40). The reasons for the large changes in peak oxygen saturation in the control group (about 10% change in peak oxygen saturation) are unclear to the authors of this review. In the study by Selvadurai, the aerobic training group demonstrated less desaturation following training compared to control, MD 0.62% (95% CI 0.32 to 0.92) (Analysis 1.11). These differences did not reach statistical significance in the original study (Selvadurai 2002).
1.11. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 11 Change in oxygen saturation (%).
Two studies reported on minute ventilation at peak exercise (Cerny 1989; Schneiderman‐Walker 2000). In the study by Schneiderman‐Walker, there was no significant difference in the annual rate of decline in maximum minute ventilation between groups, MD 2.09 L/min (95% CI ‐1.60 to 5.78) (Analysis 1.12). The study by Cerny again did not present any data we were able to analyse, but stated that there were no differences between groups in the ratio change of peak minute ventilation to peak load (Cerny 1989).
1.12. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 12 Annual rate of change in peak VE over 36 months (L/min).
Finally, in the study by Hommerding breathlessness and fatigue was measured with a 0 to 10 Borg scale. Data were presented as medians (interquartile range) in the original publication and could not be analysed in this review. Hommerding reported no differences in either variable between groups after the three‐month intervention (Hommerding 2015).
4. Additional indices of pulmonary function and respiratory muscle strength
Changes in pulmonary function in addition to FEV1 were reported in five studies (Cerny 1989; Hommerding 2015; Kriemler 2013; Schneiderman‐Walker 2000; Selvadurai 2002). No study reported on respiratory muscle strength.
All five studies reported on FVC % predicted (n = 187) (Cerny 1989; Hommerding 2015; Kriemler 2013; Schneiderman‐Walker 2000; Selvadurai 2002). In the short‐term study by Selvadurai, there was no significant difference between the groups in change of FVC % predicted at hospital discharge, MD 0.06% (95% CI ‐2.55 to 2.67) and one month after discharge, MD ‐0.11% (95% CI ‐2.64 to 2.42) (Selvadurai 2002) (Analysis 1.13). In the second short‐term study (by Cerny), there was no difference reported in the change in FVC % predicted among groups (Cerny 1989). In the longer‐term study by Hommerding, there was no difference between the study groups in FVC % predicted after the three‐month intervention, MD ‐1.60% (95% CI ‐8.22 to 5.02) (Hommerding 2015). In the Kriemler study, significant differences were observed in the training group compared to the control group for FVC % predicted at three and six months, MD 9.24% (95% CI 3.82 to 14.66) and MD 12.51% (95% CI 5.90 to 19.12), respectively (Kriemler 2013). When combined, the data from both studies showed a significant difference in FVC % predicted between the exercise and control groups at three months, pooled MD 4.89% (95% CI 0.69 to 9.08) (Analysis 1.13). Heterogeneity between these studies was high (I² = 84%); most likely due to the unusual deterioration of the control group. Further, differences between groups were found in favour for the exercise group after six months off‐training, MD 15.09% (95% CI 6.01 to 24.17). No differences between groups were observed after 18 months off‐training, MD 9.10% (95% CI ‐0.94 to 19.14) (Kriemler 2013).
1.13. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 13 Change in FVC (% predicted).
Schneiderman‐Walker reported on the effects of aerobic physical training on lung function at three years (Schneiderman‐Walker 2000). The control group demonstrated a significantly greater mean rate of annual decline in FVC % predicted than the exercise group, MD 2.17% (95% CI 0.47 to 3.87) (Analysis 1.13).
Two longer‐term studies reported on changes in FEF25‐75 % predicted (Hommerding 2015; Schneiderman‐Walker 2000). No between‐group differences in FEF25‐75 % predicted were found in the study by Hommerding after three months, MD ‐9.00% (95% CI ‐23.29 to 5.29) (Hommerding 2015). Schneiderman‐Walker also reported that the control group demonstrated a significantly greater mean rate of annual decline in FEF25‐75 % predicted, MD 0.80% (95% CI ‐2.20 to 3.80), although this was not statistically significant (Schneiderman‐Walker 2000) (Analysis 1.14).
1.14. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 14 Change in FEF25‐75 (% predicted).
The Kriemler study additionally reported on the ratio of residual volume to total lung capacity (RV/TLC) in % predicted (Kriemler 2013). Compared to the control group, no differences were observed for this outcome at either three, MD ‐3.93 (95% CI ‐9.53 to 1.67) or six months, MD ‐0.73 (95% CI ‐7.60 to 6.14) (Analysis 1.15). Results remained non‐significant after six, MD 3.19 (95% CI ‐4.02 to 10.40) and 18 months off‐training, MD ‐1.98 (95% CI ‐8.82 to 4.86).
1.15. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 15 Change in RV/TLC (%).
Hommerding also reported on FEV1/FVC as % predicted (Hommerding 2015). They found no differences in FEV1/FVC between the training and control group after the intervention, MD ‐1.40% (95% CI ‐8.66 to 5.86) (Hommerding 2015) (Analysis 1.16).
1.16. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 16 Change in FEV1/FVC (% predicted).
5. Physical activity
Physical activity was reported in three studies (n = 105) (Hommerding 2015; Kriemler 2013, Selvadurai 2002).
Hommerding assessed physical activity levels by self‐report (diary) and reported an increase in self‐reported physical activity in the intervention compared to the control group after three months. However, in the original publication, data were presented as N (%) and could not be included in our analysis (Hommerding 2015).
Kriemler measured physical activity levels using accelerometry (Kriemler 2013). At three months, total physical activity (counts per min) was higher in the aerobic training group compared to the control group, MD 121.00 counts per min (95% CI 29.90 to 212.10) (Analysis 1.17). There were no differences in this outcome at six months, MD ‐86.00 counts per min (95% CI ‐375.51 to 203.51); after six months off‐training, MD ‐20.00 counts per min (95% CI ‐309.67 to 269.67) and after 18 months off‐training, MD ‐13.00 counts per min (95% CI ‐362.46 to 336.46) (Analysis 1.17).
1.17. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 17 Change in total physical activity (counts per min).
Kriemler also reported on moderate to vigorous physical activity (hours per week) but found no differences between the aerobic training group and the control group at any time point reported during the study: at three months, MD ‐0.50 hours per week (95% CI ‐2.30 to 1.30); at six months, MD ‐0.20 hours per week (95% CI ‐2.28 to 1.88); after six months off‐training, MD 0.55 hours per week (95% CI ‐1.09 to 2.19); and after 18 months off‐training, MD 1.20 hours per week (95% CI ‐1.05 to 3.45) (Analysis 1.18).
1.18. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 18 Change in moderate‐to‐vigorous physical activity (hours per week).
Selvadurai measured physical activity levels with a combination of accelerometry and activity diaries in a sub‐sample of study participants (Selvadurai 2002). No between‐group differences in physical activity levels were reported at hospital discharge, MD 1.20 mega joules (MJ) per day (95% CI ‐0.20 to 2.60) (Analysis 1.19).
1.19. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 19 Change in total physical activity (MJ/day).
6. Body composition
Changes in body composition were reported in five studies (n = 187) (Hommerding 2015; Kriemler 2013; Michel 1989; Schneiderman‐Walker 2000; Selvadurai 2002).
Selvadurai reported on change in weight (Selvadurai 2002). There was no difference between groups at hospital discharge, MD ‐0.23 kg (95% CI ‐0.59 to 0.13) and one month after discharge, MD 0.10 kg (95% CI ‐0.33 to 0.53) (Analysis 1.20). Michel also reported on weight at one‐month follow up, the mean (SD) increase in weight in the aerobic exercise group, 6.4 (4.8) lb was greater than in the non‐exercise group 3.8 (3.4) lb (Michel 1989). These data cannot be entered into the data tables, as the number of participants assigned to each treatment group was not reported. We have contacted the authors for further information, but there is none available.
1.20. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 20 Change in body weight (kg).
In the study by Kriemler, no changes were observed in BMI after three and six months, MD 0.30 kg/m² (95% CI ‐0.13 to 0.73) and MD 0.40 kg/m² (95% CI ‐0.00 to 0.80), respectively (Analysis 1.21). At six months off‐training, BMI was significantly higher in the training compared to the control group, MD 0.50 kg/m² (95% CI 0.01 to 0.99), but at 18 months off‐training no significant difference was observed between groups, MD 0.40 kg/m² (95% CI ‐0.37 to 1.17). Hommerding reported BMI z scores and found no differences between the training and the control group at three months, MD 0.10 (95% CI ‐0.16 to 0.36) (Hommerding 2015) (Analysis 1.22).
1.21. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 21 Change in BMI (kg/m2).
1.22. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 22 Change in BMI z score.
Selvadurai reported no difference in fat‐free mass between the the aerobic training group and the control group at hospital discharge, MD 0.01 kg (95% CI ‐0.19 to 0.21) and one month after discharge MD 0.04 kg (95% CI ‐0.19 to 0.27) (Selvadurai 2002) (Analysis 1.23). Kriemler also reported on fat‐free mass, for which there were no significant differences between the aerobic training and the control groups at three months MD ‐0.30 kg (95% CI ‐1.05 to 0.45) and six months MD 0.30 kg (95% CI ‐0.95 to 1.55) (Analysis 1.23). This was also the case at six and 18 months off‐training, MD 0.90 kg (95% CI ‐0.39 to 2.19) and MD 0.50 kg (95% CI ‐0.75 to 1.75).
1.23. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 23 Change in fat‐free mass (kg).
The change in % of body fat reported in the study by Kriemler was higher in the training compared to the control group after three months, MD 1.60 % (95% CI 0.36 to 2.84) (Kriemler 2013). No between group differences were observed after six months, MD 1.40 % (95% CI ‐0.40 to 3.20) and at six and 18 months off‐training, MD 1.00% (95% CI ‐1.66 to 3.66) and MD 1.20% (95% CI ‐1.64 to 4.04), respectively (Analysis 1.24).
1.24. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 24 Change in body fat (%).
The study by Schneiderman‐Walker reported on the annual rate of decline in % of ideal weight for height (Schneiderman‐Walker 2000). There was there was no significant difference between groups at after 36 months, MD 0.52% (95% CI ‐0.76 to 1.80) (Analysis 1.25).
1.25. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 25 Annual rate of change of ideal weight for height (%).
Hommerding measured triceps skinfold thickness and arm muscle circumference (Hommerding 2015). No between‐group differences were observed in either triceps skinfold thickness, MD 0.39 mm (95% CI ‐0.39 to 1.17) or arm muscle circumference, MD 0.16 cm (95% CI ‐0.05 to 0.37) (Analysis 1.26; Analysis 1.27). Michel also reported skinfold thickness and stated that there was a trend towards a greater increase in the sum of four skin folds in the exercise group and mid‐arm muscle circumference than the non‐exercise group (Michel 1989).
1.26. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 26 Change in triceps skinfold thickness (mm).
1.27. Analysis.
Comparison 1 Aerobic training versus no physical training, Outcome 27 Change in arm muscle circumference (cm).
7. Acute exacerbations
One study reported on this outcome (Schneiderman‐Walker 2000). There were no between‐group differences reported for the mean number of hospitalisations or mean number of days in hospital at year one, two and three (low‐quality evidence) (Schneiderman‐Walker 2000).
8. Antibiotic use
No data were reported in any of the studies.
9. Bone health
No data were reported in any of the studies.
10. Diabetic control
No data were reported in any of the studies.
11. Compliance with physical exercise training
Two studies reported on this outcome (n = 92) (Kriemler 2013; Schneiderman‐Walker 2000).
The Kriemler study reported on training compliance for the overall study groups, but not separately for the different training groups. Altogether, the training groups fulfilled at least 65% of all training sessions (i.e. two out of three sessions per week) and 80% of all participants performed the requested three training sessions per week (Kriemler 2013).
In the Schneiderman‐Walker study, mean (SD) scores for compliance with exercise were reported, where the possible scores ranged from zero to two indicating poor, partial or full compliance, respectively. These scores within the exercise group for year 1 (1.51), year 2 (1.51) and year 3 (1.49) were not significantly different, but they were always higher than the scores for compliance with airway clearance techniques. Compliance with airway clearance was not statistically different between the groups (Schneiderman‐Walker 2000).
12. Adverse events
Two studies specifically reported on adverse events (n = 71) (moderate‐quality evidence) (Kriemler 2013; Selvadurai 2002). The Kriemler study reported that no adverse effects (e.g. injuries, pneumothorax, asthma attacks, hypoglycaemia) occurred during the study (Kriemler 2013). In the study by Selvadurai, one participant in the aerobic training group injured her ankle and missed two days of aerobic training. One participant from the control group developed haemoptysis and withdrew from the study (Selvadurai 2002). No other study reported on adverse events.
Anaerobic training versus no physical training
Three studies with 86 participants are included in this comparison (Klijn 2004; Kriemler 2013; Selvadurai 2002). In the study by Kriemler, the control group experienced an unusual deterioration of physical health during the study and the results should be interpreted with caution (Kriemler 2013).
Primary outcomes
1. Exercise capacity by VO2 peak
This outcome was reported in three studies (n = 86) (Klijn 2004; Kriemler 2013; Selvadurai 2002). Results are presented in the analysis (low‐quality evidence) (Analysis 2.1).
2.1. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 1 Change in VO2 peak during maximal exercise (ml/min per kg BW).
Selvadurai reported that anaerobic training was not associated with improvements in VO2 peak compared with control at hospital discharge, MD 1.95 mL/min per kg BW (95% CI ‐1.61 to 5.51) and one month after hospital discharge, MD ‐0.40 mL/min per kg BW (95% CI ‐4.03 to 3.23). Two studies reported on this outcome at three months (Klijn 2004; Kriemler 2013). In the study by Klijn, the change in VO2 peak was not significantly greater in the anaerobic training versus control group, MD 3.95 mL/min per kg body weight (95% CI ‐2.95 to 10.85). Kriemler also reported there was no difference in VO2 peak in the training group compared to the control group after three months, MD 9.34 mL/min per kg body weight (95% CI ‐1.31 to 19.99). When combined, the data from both studies showed no between group differences, pooled MD 5.54 (95% CI ‐0.25 to 11.34). Klijn reported no significant changes in VO2 peak in the training group after three months off training, while VO2 peak significantly decreased in the control group by ‐1.5 (1.7) mL/min per kg body weight. No data were available in the original paper to calculate the mean difference (Klijn 2004). Kriemler reported significant differences in VO2 peak in the training group compared to the control group after six months, MD 17.70 mL/min per kg body weight (95% CI 5.98 to 29.42). No significant differences between the groups was found at six and 18 months off training, MD 11.59 mL/min per kg body weight (95% CI ‐1.02 to 24.20) and MD 9.26 mL/min per kg body weight (95% CI ‐4.26 to 22.78), respectively.
2. Pulmonary function by FEV1
This outcome was reported in three studies (n = 86) (Klijn 2004; Kriemler 2013; Selvadurai 2002). Results are presented in the analysis (Analysis 2.2).
2.2. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 2 Change in FEV1 (% predicted).
In the study by Selvadurai, the anaerobic training group showed a significantly greater mean increase in FEV1 % predicted at hospital discharge, MD of 5.58% (95% CI 1.34 to 9.82) (Selvadurai 2002). This increase was maintained one month after hospital discharge, MD 5.08% (95% CI 0.66 to 9.50). In the study by Kriemler, significant differences in FEV1 % predicted in favour for the anaerobic training group were seen for all study time points: at three months, MD 11.11% (95% CI 5.16 to 17.06); at six months, MD 19.51% (95% CI 10.57 to 28.45); at six months off‐training, MD 16.09% (95% CI 4.95 to 27.23) and at 18 months off‐training, MD 17.01% (95% CI 6.27 to 27.75) (Kriemler 2013). The Klijn study reported that there were no significant between group differences in lung function parameters, but no data were reported which could be entered into the analysis (Klijn 2004).
3. Health‐related quality of life
This outcome was reported in two studies (n = 64) (low‐quality evidence) (Klijn 2004; Selvadurai 2002).
Selvadurai assessed HRQoL with the 'Quality of Well‐being Scale' (Selvadurai 2002). Since this scale was previously only validated in an outpatient setting, assessment was undertaken on the participants' admission to hospital and one month after their discharge. There was no significant difference between the groups in the change in HRQoL, MD 0.03 (95% CI ‐0.04 to 0.10) (Analysis 2.3).
2.3. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 3 Change in HRQoL.
In the Klijn study no significant difference in the HRQoL scale physical function between the groups was found at the end of the anaerobic training period, MD 1.30 (95% CI ‐11.55 to 14.15) (Analysis 2.4). No other difference was found in any other HRQoL domain (Klijn 2004). Klijn reported that there were significantly higher values for the domain of physical functioning in the training group after the follow‐up period (Klijn 2004). No data were available in the paper to calculate the MD.
2.4. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 4 Change in HRQoL physical function (CF questionnaire).
Secondary outcomes
1. CF‐related mortality
No data were reported from any of the studies.
2. Muscle strength and anaerobic exercise capacity
These outcomes were reported in three studies (n = 86) (Klijn 2004; Kriemler 2013; Selvadurai 2002).
In two studies (n = 42), a WAnT was performed, but due to differences in outcome measures, we are not able to combine any data (Klijn 2004; Kriemler 2013). The Klijn study reported a significantly greater change in peak power and mean power during WAnT in the anaerobic training versus control group: peak power, MD 70.30 W (95% CI 32.50 to 108.10) (Analysis 2.5); and mean power, MD 43.30 W (95% CI 22.56 to 64.04) (Analysis 2.6). Klijn reported a higher peak power and mean power in the training groups after three months off training; however, no data were available for analysis from the original publication. The Kriemler study reported no significant differences in mean power among the groups after three and six months of anaerobic training, MD ‐0.63 W/kg body weight (95% CI ‐1.30 to 0.04) and MD 0.30 W/kg body weight (95% CI ‐0.34 to 0.94), respectively (Analysis 2.7). This remained the case at six and 18 months off training, MD ‐0.15 W/kg body weight (95% CI ‐0.97 to 0.67) and 0.10 kg body weight (95% CI ‐0.94 to 1.14), respectively (Analysis 2.7).
2.5. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 5 Change in peak power during WAnT (W).
2.6. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 6 Change in mean power during WAnT (W).
2.7. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 7 Change in mean power during WAnT (W per kg BW).
In the study by Selvadurai, the anaerobic training group had a significantly greater increase in lower limb strength than the control group at discharge, MD 24.62 Nm (95% CI 20.73 to 28.51). The increase remained significant between groups one month after hospital discharge, MD 19.23 Nm (95% CI 15.24 to 23.22) (Analysis 2.8) (Selvadurai 2002).
2.8. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 8 Change in lower limb strength (Newton metres).
3. Additional indices of exercise capacity
This outcome was reported in three studies (n = 86) (Klijn 2004; Kriemler 2013; Selvadurai 2002).
In the study by Klijn, peak work capacity was significantly higher in the anaerobic training versus control group, MD 13.00 W (95% CI 4.11 to 21.89) (Analysis 2.9). In the study by Kriemler, peak work capacity was significantly lower in the training compared to the control group after three months, MD ‐0.50 W/kg body weight (95% CI ‐0.84 to ‐0.16) (Analysis 2.10). However, in the original study by Kriemler, no between‐group difference in peak work capacity was reported after three months training (Kriemler 2013). Our analysis showed significant between‐group differences in favour for the training group in peak work capacity after six months of training, MD 0.31 W/kg body weight (95% CI 0.01 to 0.61). However, the differences were not significant at six months and 18 months off‐training, MD 0.10 W/kg body weight (95% CI ‐0.26 to 0.46) and MD, 0.00 W/kg body weight (95% CI ‐0.79 to 0.79), respectively (Analysis 2.10).
2.9. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 9 Change in peak work capacity during maximal exercise (W).
2.10. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 10 Change in peak work capacity during maximal exercise (W per kg body weight).
Klijn also reported on lactate levels (Klijn 2004). At three months the anaerobic training group showed significant improvements in serum lactate levels compared to the control group, MD 3.40 mmol/L (95% CI 1.33 to 5.47) (Analysis 2.11).
2.11. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 11 Change in lactate during maximal exercise (mmol/L).
One study reported on desaturation during exercise (Selvadurai 2002). The anaerobic training group demonstrated significantly less desaturation following training compared to the control group at hospital discharge, MD 0.33% (95% CI 0.04 to 0.62) (Analysis 2.12). These differences did not reach statistical significance in the original study for an unknown reason (Selvadurai 2002).
2.12. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 12 Change in peak oxygen saturation during maximal exercise (%).
4. Additional indices of pulmonary function and respiratory muscle strength
Changes in pulmonary function measures were reported in three studies (n = 86) (Klijn 2004; Kriemler 2013; Selvadurai 2002). No study reported on respiratory muscle strength.
Two studies reported on FVC % predicted (Kriemler 2013; Selvadurai 2002). In the study by Selvadurai, there was no significant difference in FVC % predicted in the anaerobic training group compared to control at hospital discharge, MD 0.17% (95% CI ‐2.31 to 2.65) and one month after discharge, MD 0.06% (95% CI ‐2.42 to 2.54) (Analysis 2.13). Kriemler reported significant differences between the training and control group at all study time points: at three months, MD 7.37% (95% CI 1.89 to 12.85); at after six months, MD 14.05% (95% CI 7.16 to 20.94); at six months off‐training, MD 13.66% (95% CI 4.38 to 22.94) and 18 months off‐training, MD 13.63% (95% CI 4.13 to 23.13) (Kriemler 2013) (Analysis 2.13).
2.13. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 13 Change in FVC (% predicted).
Kriemler also reported RV/TLC % predicted (Kriemler 2013). The results show significant differences between the anaerobic training and the control group at three months, MD ‐6.42% (95% CI ‐10.87 to ‐1.97); six months, MD ‐14.86% (95% CI ‐21.36 to ‐8.36); six month off‐training, MD ‐6.86% (95% CI ‐13.47 to ‐0.25), but not at 18 months off‐training, MD ‐4.77% (95% CI ‐10.61 to 1.07) (Analysis 2.14).
2.14. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 14 Change in RV/TLC (%).
In the Klijn study there were no significant differences reported between groups in lung function parameters, but no data were available for analysis (Klijn 2004).
5. Physical activity
This outcome was reported in three studies (n = 86) (Klijn 2004; Kriemler 2013; Selvadurai 2002).
One study assessed physical activity levels using accelerometry (Kriemler 2013); a second study used a combination of accelerometry and activity diary (Selvadurai 2002); and the third study used the habitual activity estimation scale to assess physical activity levels (Klijn 2004).
Kriemler observed no between‐group differences in total physical activity after three or six months of training, MD 17.00 counts per min (95% CI ‐81.59 to 115.59) and MD 17.00 counts per min (95% CI –58.95 to 92.95), respectively (Analysis 2.15). This was also true at six months off‐training, MD 10.00 counts per min (95% CI ‐98.04 to 118.04) and at 18 months off‐training, MD 105.00 (95% CI ‐34.90 to 244.90) (Analysis 2.15) (Kriemler 2013).
2.15. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 15 Change in total physical activity (counts per min).
Kriemler also reported on moderate to vigorous physical activity (Kriemler 2013). No differences existed in the hours of moderate to vigorous physical activity undertaken per week for the anaerobic training and the control groups after three and six months, MD ‐1.40 hours per week (95% CI ‐2.93 to 0.13) and MD 0.20 hours per week (95% CI ‐1.58 to 1.98), respectively (Analysis 2.16). No differences were observed at six months off‐training, MD ‐1.10 hours per week (95% CI ‐2.56 to 0.36) and at 18 months off‐training, MD 1.10 hours per week (95% CI ‐0.85 to 3.05) (Analysis 2.16).
2.16. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 16 Change in moderate to vigorous physical activity (hours per week).
Selvadurai measured physical activity levels in a subgroup of 18 participants in the anaerobic training group and 16 participants in the control group (Selvadurai 2002). No differences in physical activity levels (MJ per day) were observed between the intervention and control group at hospital discharge, MD 0.65 MJ per day (95% CI ‐0.86 to 2.16) (Analysis 2.17).
2.17. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 17 Change in physical activity (MJ/day).
Klijn reported no differences between the anaerobic training and control group in habitual physical activity levels after 12 weeks (Klijn 2004). A subgroup of participants (anaerobic n = 18; control n = 16) who completed an activity diary and wore an activity accelerometer showed no significant differences for between group comparisons in habitual activity at follow‐up (Klijn 2004).
6. Body composition
Outcomes related to changes in body composition were reported in three studies (n = 86) (Klijn 2004; Kriemler 2013; Selvadurai 2002).
Selvadurai reported a significantly greater change in weight at hospital discharge in the training group compared to the control group, MD 1.73 kg (95% CI 1.35 to 2.11) and one month after discharge, MD 1.65 kg (95% CI 1.24 to 2.06) (Analysis 2.18).
2.18. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 18 Change in weight (kg).
Kriemler reported had lower values for BMI in the control group at all time points during the study: at three months, MD 0.50 kg/m² (95% CI 0.07 to 0.93); after six months, MD 0.70 kg/m² (95% CI 0.27 to 1.13); after six months off‐training, MD 1.10 kg/m² (95% CI 0.45 to 1.75); and after 18 months off‐training, MD 1.30 kg/m² (95% CI 0.34 to 2.26) (Analysis 2.19).
2.19. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 19 Change in BMI (kg/m2).
Kriemler and Selvadurai both reported fat‐free mass (Kriemler 2013; Selvadurai 2002). Selvadurai reported a significant difference favouring the training group at hospital discharge, MD 1.80 kg (95% CI 1.57 to 2.03) and again one month after discharge MD 1.71 kg (95% CI 1.46 to 1.96). Kriemler observed no significant differences in fat‐free mass between groups after three months, MD 0.70 kg (95% CI ‐0.34 to 1.74). However, significantly higher values for fat‐free mass favouring the exercise group were found after six months, MD 1.50 kg (95% CI 0.08 to 2.92); after six months off‐training, MD 2.00 kg (95% CI 0.14 to 3.86) and after 18 months off‐training, MD 3.20 kg (95% CI 1.02 to 5.38) (Analysis 2.20).
2.20. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 20 Change in fat‐free mass (kg).
Only one study reported on body fat as a % of the whole (Kriemler 2013). No differences between groups in % body fat were reported after three and six months, MD 1.20% (95% CI ‐0.26 to 2.66) and MD 0.80% (95% CI ‐0.85 to 2.45), respectively. This was also true after six months off‐training, MD 1.70% (95% CI ‐0.14 to 3.54) and 18 months off‐training, MD 1.10% (95% CI ‐1.65 to 3.85), respectively (Analysis 2.21).
2.21. Analysis.
Comparison 2 Anaerobic training versus no physical training, Outcome 21 Change in body fat (%).
Klijn reported that there was no significant difference in change in body composition between the groups at end of the training period, but no data were available for analysis (Klijn 2004).
7. Acute exacerbations
No data were reported for this outcome in any of the studies.
8. Antibiotic use
No data were reported for this outcome in any of the studies.
9. Bone health
No data were reported for this outcome in any of the studies.
10. Diabetic control
No data were reported for this outcome in any of the studies.
11. Compliance with physical exercise training
Two studies reported on compliance (n = 42) (Klijn 2004; Kriemler 2013). In the study by Klijn, the mean (SD) attendance rate at exercise sessions was 98.1% (4.3) with reasons for absence being holidays or sickness (Klijn 2004).
The Kriemler study reported on overall training compliance for the study groups, but not separately for the different groups. Overall, the training groups fulfilled at least 65% of all training sessions (i.e. two out of three sessions per week) and 80% of all participants performed the requested three training sessions per week (Kriemler 2013).
12. Adverse events
The Kriemler study (n = 22) reported that no adverse effects (e.g. injuries, pneumothorax, asthma attacks, hypoglycaemia) occurred during the study (moderate‐quality evidence) (Kriemler 2013).
Combined aerobic and anaerobic training versus no training
Seven studies with 257 participants are included in this comparison (Beaudoin 2017; Douglas 2015; Hebestreit 2010; Moorcroft 2004; Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014).
Additional data were provided by the authors of the two Santana‐Sosa studies, which included 42 participants (Santana‐Sosa 2012; Santana‐Sosa 2014). However, due to inconsistencies between the data provided and the published results, the results for these studies are not formally included in this review. Published results of the two studies are summarised in the additional tables (Table 4; Table 5). These results showed significant group x time interactions for VO2 peak and muscle strength in the training compared to the control group after eight weeks of training. In one study, during a four‐week detraining period, when no exercise training was performed, VO2 peak decreased to pre‐training values but muscle strength was maintained (Santana‐Sosa 2012). In the second study, which combined aerobic and anaerobic training with respiratory muscle training, the improvements in VO2 peak and muscle strength were largely preserved during the four‐week detraining period (Santana‐Sosa 2014). In this later study, respiratory muscle strength (PImax) improved in the intervention group after eight weeks (Santana‐Sosa 2014), while the earlier study without respiratory muscle training did not show any effects on PImax (Santana‐Sosa 2012). One of the studies showed a group x time interaction effect for fat mass and fat‐free mass (% of total) (Santana‐Sosa 2014). In both studies, exercise training did not have any effect on pulmonary function or HRQoL.
The study by Beaudoin published within‐group changes for the exercise and control group from baseline to 12 weeks (Beaudoin 2017). The investigators provided us with participant‐level data allowing us to calculate values for the change from baseline measurements for all relevant outcomes by intervention group. We note that, for this reason, the results presented in the review are different from the results presented in the published report (Beaudoin 2017). There were several methodological inadequacies in this study (see Characteristics of included studies for further details), including that the study was originally designed as a cross‐over study but the authors present only the first period as if it was a parallel study. The study also did not reach the target sample size so is likely to be underpowered. For these reasons, we have not combined results from the Beaudoin study with any other results and we encourage that the results from this study should be interpreted with caution (Beaudoin 2017).
Primary outcomes
1. Exercise capacity by VO2 peak
These outcomes were reported in two studies (n = 52) using a maximal cardiopulmonary exercise test on a cycle ergometer (low‐quality evidence) (Hebestreit 2010; Beaudoin 2017).
Hebestreit reported the change from baseline to the three‐month to six‐month assessment period and observed significantly higher values for VO2 peak, in the training compared to the control group, MD 2.04 mL/min per kg body weight (95% CI 0.08 to 4.00). During the follow‐up period, no differences between groups were observed six months off‐training, MD 0.70 mL/min per kg body weight (95% CI ‐1.61 to 3.01), but a significantly higher VO2 peak was found in the training compared to the control group after 12 to 18 months off‐training, MD 3.73 mL/min per kg body weight (95% CI 1.32 to 6.14) (Analysis 3.1) (Hebestreit 2010).
3.1. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 1 Change in VO2 peak during maximal exercise (ml/min per kg BW).
In the Beaudoin study, no between group differences were found for VO2 peak after 12‐weeks, MD ‐2.13 mL/min per kg body weight (95% CI ‐4.93 to 0.67) (Analysis 3.1) (Beaudoin 2017).
2. Pulmonary function (FEV1)
This outcome was reported in four studies (n = 144) (low‐quality evidence) (Beaudoin 2017; Hebestreit 2010; Moorcroft 2004; Rovedder 2014). Results on FEV1 were not reported in detail in the original paper by Hebestreit (Hebestreit 2010).
Three studies (n = 100) reported FEV1 % predicted (Beaudoin 2017; Hebestreit 2010; Rovedder 2014). At three months, Rovedder observed no between‐group differences after three months, MD ‐4.00% (95% CI ‐11.86 to 3.86) (Analysis 3.2). Our calculations using the data from the Beaudoin study, also showed no differences between groups for FEV1 % predicted at this time point, MD ‐0.75% (95% CI ‐5.62 to 4.12) (Analysis 3.2). After three to six months, Hebestreit also reported no between‐group differences in FEV1 % predicted, MD 2.00% (95% CI ‐5.31 to 9.31). Hebestreit also found no differences in FEV1 % predicted at six months and 12 to 18 months off‐training, MD ‐1.10% (95% CI ‐8.69 to 6.49) and MD 3.60 (95% CI ‐4.37 to 11.57), respectively (Analysis 3.2) (Hebestreit 2010).
3.2. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 2 Change in FEV1 (% predicted).
Moorcroft reported the annual change in FEV1 (mL) (Moorcroft 2004). This study showed no significant change in FEV1 after one year of training compared to the control group, MD 107.00 mL (95% CI ‐73.98 to 287.98) (Analysis 3.3).
3.3. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 3 Annual change in FEV1 (mL).
3. Health‐related quality of life
This outcome was reported in three studies (n = 93) (very low‐quality evidence). All studies used the disease‐specific questionnaire the Cystic Fibrosis Questionnaire (CFQ) to assess HRQoL (Beaudoin 2017; Hebestreit 2010; Rovedder 2014); the Rovedder study applied an additional questionnaire (Medical Outcomes Study‐36 Item Short‐Form Health Survey, SF‐36) (Rovedder 2014).
In the Beaudoin study, no differences were observed in any single HRQoL scale between the training and control group after 12 weeks (Beaudoin 2017): physical functioning, MD ‐0.04 (95% CI ‐4.35 to 4.27); vitality, MD 0.38 (95% CI ‐0.78 to 1.53); emotional state, MD ‐1.17 (95% CI ‐2.78 to 0.45); treatment burden, MD ‐0.50 (95% CI ‐2.17 to 1.17); health perception, MD ‐0.50 (95% CI ‐1.93 to 0.93); social limitations, MD ‐1.38 (95% CI ‐3.28 to 0.53); body image, MD ‐0.54 (‐1.88 to 0.80); role limitations, MD 0.54 (95% CI ‐1.13 to 2.21); respiratory symptoms, MD ‐0.58 (95% CI ‐3.51 to 2.35); digestion symptoms, MD 1.33 (95% CI ‐0.49 to 3.16) (Analysis 3.5). Effect estimates (MD and 95% CIs) are not estimable for the scales eating disturbances and weight problems as mean (SD) change values for all participants in the control group were zero.
3.5. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 5 Change in Quality of Life: CFQ‐R.
In the study by Hebestreit, the HRQoL subscale of "subjective health perception" was higher in the training compared to the control group after three to six months, MD 9.91 (95% CI 0.89 to 18.93) (Hebestreit 2010). No differences between groups were found six months off‐training, MD ‐2.31 (95% CI ‐15.46 to 10.84), while there were significant between group differences at 12 to 18 months off‐training, MD 9.89 (95 % CI 0.64 to 19.14). No other HRQoL scales were significantly different between groups (Analysis 3.4). Results for the other HRQoL scales were reported as non‐significant for all time points in the original paper (Hebestreit 2010).
3.4. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 4 Change in subjective health perception (CFQ‐R).
In the study by Rovedder, no differences were found in any single HRQoL scale between the training and control group in either the CFQ‐R or the SF‐36 questionnaire after three months (Rovedder 2014). Data for each single HRQoL scale were reported for both questionnaires in the original publication. The data were presented as medians (interquartile range) in the publication and could not be analysed in the review. Data are presented in additional tables (Table 6).
3. HRQoL results for Rovedder 2014.
| Health‐related quality of life | Exercise group (n = 19) | Control group (n = 22) | P value |
| HRQoL scale ‐ physical (median (interquartile range)) | 6.1 (‐4 to 8) | 2.4 (‐10 to 13) | 0.742 |
| HRQoL scale ‐ body image (median (interquartile range)) | 3.3 (‐11 to 22) | 3.0 (‐2 to 11) | 0.915 |
| HRQoL scale ‐ digestive (median (interquartile range)) | ‐1.0 (‐4 to 0) | ‐0.5 (0 to 0) | 0.953 |
| HRQoL scale ‐ respiratory (median (interquartile range)) | 3.8 (0 to 11) | ‐4.7 (‐1 to 7) | 0.925 |
| HRQoL scale ‐ emotional (median (interquartile range)) | 1.2 (‐6 to 6) | ‐4.3 (‐13 to 6) | 0.458 |
| HRQoL scale ‐ social (median (interquartile range)) | ‐1.1 (‐11 to 5) | ‐1.7 (‐5 to 11) | 0.822 |
| HRQoL scale ‐ food (median (interquartile range)) | ‐0.3 (‐11 to 6) | ‐2.0 (‐11 to 0) | 0.913 |
| HRQoL scale ‐ treatment (median (interquartile range)) | ‐2.0 (‐11 to 0) | ‐2.5 (‐11 to 11) | 0.850 |
| HRQoL scale ‐ vitality (median (interquartile range)) | ‐1.2 (‐16 to 8) | 2.6 (‐8 to 10) | 0.579 |
| HRQoL scale ‐ health (median (interquartile range)) | 1.7 (‐11 to 16) | ‐3.0 (‐11 to 0) | 0.382 |
| HRQoL scale ‐ weight (median (interquartile range)) | 4.6 (0 to 33) | 12.1 (0 to 11) | 0.410 |
| HRQoL scale ‐ social role (median (interquartile range)) | 0.8 (‐8 to 8) | 1.8 (‐2 to 0) | 0.935 |
| SF‐36 ‐ functional capacity (median (interquartile range)) | 2.8 (‐10 to 15) | 2.0 (‐11 to 10) | 0.916 |
| SF‐36 ‐ physical aspects (median (interquartile range)) | 11.8 (‐25 to 50) | 6.8 (‐6 to 31) | 0.705 |
| SF‐36 ‐ pain (mean (median (interquartile range)) | ‐7.2 (‐28 to 11) | 8.0 (7 to 17) | 0.100 |
| SF‐36 ‐ general health (median (interquartile range)) | 3.7 (‐5 to 10) | ‐3.5 (‐11 to 5) | 0.197 |
| SF‐36 ‐ vitality (median (interquartile range)) | 1.2 (‐15 to 20) | 7.5 (‐1 to 21) | 0.416 |
| SF‐36 ‐ social aspects (median (interquartile range)) | 15.2 (0 to 33) | 21.2 (0 to 66) | 0.989 |
| SF‐36 ‐ emotional aspects (median (interquartile range)) | 4.7 (‐12 to 37) | 4.5 (‐12 to 25) | 0.914 |
| SF‐36 ‐ mental health (median (interquartile range)) | ‐0.8 (‐12 to 12) | 0.9 (‐9 to 13) | 0.752 |
Pre‐post changes in HRQoL measured by the CFQ and the SF‐36
CFQ: Cystic Fibrosis Questionnaire HRQoL: health‐related quality of life SF‐36: Medical Outcomes Study‐36 Item Short‐Form Health Survey
Secondary outcomes
1. CF‐related mortality
No data were reported for this outcome in any of the studies.
2. Muscle strength and anaerobic exercise capacity
These outcomes were reported in the publications of two studies (n = 55) (Beaudoin 2017; Rovedder 2014); Data on anaerobic capacity were not reported in detail in the original paper by Hebestreit (n = 32), but additional data have been made available by the study investigators (Hebestreit 2010).
Beaudoin measured muscle strength (leg press, chest press, latpull down and biceps curl) using the 1RM test; muscle endurance was assessed using different exercises (push‐up, sit‐up, flexibility and handgrip‐strength) (Beaudoin 2017). After 12 weeks, there were no between‐group differences in leg press, MD 19.26 kg (95% CI ‐7.33 to 45.85) (Analysis 3.9); chest press, MD 3.14 (95% CI ‐5.64 to 11.91) (Analysis 3.10); latpull down, MD 1.95 kg (95% CI ‐2.80 to 6.70) (Analysis 3.11) and biceps curl, MD ‐1.09 kg (95% CI ‐3.20 to 1.03) (Analysis 3.12). Moreover, no between‐group differences were found for the number of push ups, MD 7.18 (95% CI ‐13.7 to 15.73) (Analysis 3.13); the number of sit‐ups, MD 6.07 (95% CI ‐2.26 to 14.41) (Analysis 3.14); flexibility, MD ‐1.96 cm (95% CI ‐15.64 to 11.71) (Analysis 3.15) and handgrip strength, MD ‐5.92 kg (95% CI ‐18.48 to 6.63) (Analysis 3.16). In the original study, Beaudoin reported significantly higher values for leg press, chest press and the number of push‐ups in the exercise group after 12 weeks of training (Beaudoin 2017).
3.9. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 9 Change in muscular strength ‐ leg press (kg; 1 RM test).
3.10. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 10 Change in Muscular Strength ‐ Chest press (kg; 1 RM test).
3.11. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 11 Change in Muscular Strength ‐ Latpull down (kg; 1 RM test).
3.12. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 12 Change in Muscular Strength ‐ Biceps curl (kg; RM test).
3.13. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 13 Change in Muscular Endurance ‐ Number of push ups.
3.14. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 14 Change in Muscular Endurance ‐ Number of sit ups.
3.15. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 15 Change in Muscular Endurance ‐ Flexibility (cm).
3.16. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 16 Change in Muscular Endurance ‐ hand grip strength (kg).
Hebestreit measured anaerobic capacity measured by a WAnT (Hebestreit 2010). After three to six months, no differences were observed for peak power, MD ‐0.44 W per kg body weight (95% CI ‐0.98 to 0.10); there were also no differences between groups found during the follow‐up period at six months and 12 to 18 months off‐training, MD ‐0.43 W per kg body weight (95% CI ‐2.23 to 1.37) and MD 0.37 W per kg body weight (95% CI ‐0.66 to 1.40), respectively (Analysis 3.6). The results reported for mean power were also not significant between the training and control group at three to six months, MD ‐0.22 W per kg body weight (95% CI ‐0.58 to 0.14); six months off‐training, MD ‐0.08 W per kg body weight (95% CI ‐0.94 to 0.78) and 12 to 18 months off‐training, MD 0.17 W per kg body weight (95% CI ‐0.34 to 0.68) (Analysis 3.7).
3.6. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 6 Change in peak power during WAnT (W per kg body weight).
3.7. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 7 Change in mean power during WAnT (W per kg body weight).
Rovedder measured muscle strength of elbow flexors and knee extensors using the one repetition maximum (1RM) strength test (Rovedder 2014). After three months, the training group had significantly higher values compared to the control group for right upper limb muscle strength, MD 1.00 kg (95% CI 0.15 to 1.85) and left upper limb muscle strength, MD 1.40 kg (95% CI 0.33 to 2.47) (Analysis 3.8). A significant difference between groups was also observed for left lower limb muscle strength, MD 1.60 kg (95% CI 0.15 to 3.05), but not for right lower limb muscle strength, MD 1.10 kg (95% CI ‐0.51 to 2.71) (Analysis 3.8). In the original paper by Rovedder, differences of left lower limb muscle strength among groups did not reach statistical significance (P value > 0.05) (Rovedder 2014).
3.8. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 8 Change in muscle strength (all limbs) (1RM test).
3. Additional indices of exercise capacity
Peak work capacity
One study reported changes in peak work capacity (n = 38) (Hebestreit 2010). This study found significantly higher values for peak work capacity in the training compared to the control group after three to six months, MD 0.25 W/kg body weight (95% CI 0.03 to 0.47) (Analysis 3.17). During the follow‐up period, no differences were found six months off‐training, MD 0.19 W/kg body weight (95% CI ‐0.03 to 0.41), but significantly higher values in favour for the exercise training group were observed between 12 and 18 months off‐training, MD 0.37 W/kg body weight (95% CI 0.15 to 0.59) (Analysis 3.17).
3.17. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 17 Change in peak work capacity during maximal exercise (W per kg BW).
Functional exercise capacity
Rovedder (n = 41) assessed changes in functional exercise capacity after physical training using a six‐minute walk test (6MWT) (Rovedder 2014). After three months of combined aerobic and strength training no differences were observed in walk distance, MD ‐0.80 m (95% CI ‐24.59 to 22.99) or the change in % predicted walking distance, MD 1.90% (95% CI ‐3.01 to 6.81) (Analysis 3.18).
3.18. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 18 Change in functional exercise capacity.
Heart rate
Two studies (n = 92) reported on heart rate (Moorcroft 2004; Rovedder 2014). Rovedder did not observe any between group differences in peak heart rate at the end of the 6MWT, MD 4.70 bpm (95% CI ‐9.17 to 18.57) (Rovedder 2014) (Analysis 3.19). Moorcroft reported on the heart rate response which was measured at the end of an identical constant work rate of 55% of participants' maximal workload at baseline on an incremental arm and bicycle ergometry (Moorcroft 2004). The study showed a significant reduction in heart rate in favour of the training group at the pre‐defined cycling intensity, MD ‐8.20 bpm (95% CI ‐15.61 to ‐0.79), but not during arm ergometry, MD ‐1.40 bpm (95% CI ‐10.20 to 7.40) (Analysis 3.20).
3.19. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 19 Change in peak heart rate during 6MWT (beats/min).
3.20. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 20 Annual change in peak heart rate (beat/min).
Ventilation
Moorcroft (n = 51) also reported the annual change in peak ventilation (VE) (Moorcroft 2004). There was no significant reduction in VE in the training group compared to the control group during during whole body cycle ergometry, MD ‐2.50 L/min (95% CI ‐6.11 to 1.11), but a significant reduction during arm ergometry, MD ‐3.30 L/min (95% CI ‐6.40 to ‐0.20) (Analysis 3.21).
3.21. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 21 Annual change in VE (L/min).
Beaudoin reported VE during maximal cardiopulmonary exercise testing (Beaudoin 2017). After 12 weeks, there were no between‐group differences in VE, MD ‐6.74 L/min (95% CI ‐17.35 to 3.87) (Analysis 3.22).
3.22. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 22 Change in peak ventilation (VE) during maximal exercise.
Lactate levels
Only Moorcroft (n = 51) reported on lactate levels (Moorcroft 2004). Lactate levels decreased significantly during whole body ergometry, MD ‐0.83 mmol/L (95% CI ‐1.54 to ‐0.12), but not during arm ergometry, MD ‐0.32 mmol/L (95% CI ‐1.14 to 0.50) (Analysis 3.23).
3.23. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 23 Annual change in lactate (mmol/l).
Respiratory rate and respiratory exchange ratio
Two studies (n = 92) reported on respiratory rate (Moorcroft 2004; Rovedder 2014). At three months Rovedder reported no significant difference in respiratory rate during the 6MWT, MD ‐1.00 (95% CI ‐5.56 to 3.56) (Analysis 3.24). Moorcroft also reported no significant changes in respiratory rate at one year either for whole body bicycle ergometry, MD ‐0.80 (95% CI ‐4.90 to 3.30), or arm ergometry, MD 1.50 (95% CI ‐3.11 to 6.11) (Analysis 3.25).
3.24. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 24 Change in RR during 6MWT (breaths/min).
3.25. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 25 Annual change in RR (breaths/min).
Only Moorcroft presented data for the annual change in respiratory exchange ratio (RER) (Moorcroft 2004). No significant differences were identified for either testing modalities; whole body, MD 0.02 (95% CI ‐0.02 to 0.06) and arm ergometry, MD 0.00 (95% CI ‐0.04 to 0.04) (Analysis 3.26).
3.26. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 26 Annual change in RER.
Oxygen saturation
One study measuring oxygenation at rest and at the end of a 6MWT report on oxygen saturation by ear or finger oximetry (n = 41) (Rovedder 2014). After the three‐month intervention no differences in resting oxygen saturations (SaO2) were found between the exercise and control group, MD 0.90 % (95% CI ‐0.15 to 1.95); or at the end of the 6MWT, MD 2.60 % (95% CI ‐0.11 to 5.31) (Analysis 3.27).
3.27. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 27 Change in oxygen saturation (%).
Breathlessness and fatigue
Two studies reported on breathlessness and fatigue using the Borg scales (n = 92) (Moorcroft 2004; Rovedder 2014).
Rovedder reported on breathlessness and fatigue after a three‐month intervention (Rovedder 2014). No differences between the exercise and control groups were observed either at rest, MD 0.00 (95% CI ‐0.38 to 0.38) and during the 6MWT, MD ‐0.10 (95% CI ‐1.31 to 1.11) (Analysis 3.28). Moorcroft reported on the annual change in breathlessness score (Moorcroft 2004). No significant reduction was shown by the Moorcroft study data for Borg scale scores between the training compared to the control groups either during bicycle ergometry, MD 0.00 (95% CI ‐1.00 to 1.00) or during arm ergometry, MD ‐0.90 (95% CI ‐1.90 to 0.10) (Analysis 3.29).
3.28. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 28 Change in Borg breathlessness score.
3.29. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 29 Annual change in Borg breathlessness score.
Furthermore, Rovedder found no differences between groups in Borg fatigue scale either at rest, MD 0.02 (95% CI ‐0.50 to 0.54) or during the 6MWT, MD ‐0.60 (95% CI ‐1.87 to 0.67) (Analysis 3.30). Moorcroft also found no difference between the training group compared to the control group in the change scores for muscle fatigue during bicycle ergometry, MD ‐0.30 (95% CI ‐1.50 to 0.90) or during arm ergometry, MD 0.30 (95% CI ‐0.99 to 1.59) (Analysis 3.31).
3.30. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 30 Change in Borg fatigue score.
3.31. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 31 Annual change in Borg muscle effort.
4. Additional indices of pulmonary function and respiratory muscle strength
This outcome was reported in four studies (n = 144) (Beaudoin 2017; Hebestreit 2010; Moorcroft 2004; Rovedder 2014);. Data for RV/TLC were not reported in detail in the original paper by Hebestreit, but the data were made available by the investigators (Hebestreit 2010).
Three studies reported FVC % predicted (n = 93) (Beaudoin 2017; Hebestreit 2010; Rovedder 2014). In the study by Beaudoin, there were no differences in FVC % predicted between the exercise and control group after 12 weeks, MD 3.29 % (95% CI ‐4.36 to 10.94) (Analysis 3.32); for the reasons already stated above, we have not combined the data from this study with other studies. In the study by Rovedder, no between‐group differences were observed after three months, MD ‐3.30 (95% CI ‐11.73 to 5.13) (Analysis 3.32) Hebestreit, too, found no difference between training and control group after three to six months, MD 0.50% (95% CI ‐4.30 to 5.30); and six months off‐training, MD 2.71 (95% CI ‐4.37 to 9.79). However, the difference between groups was significant at 12 to 18 months off‐training, MD 6.06 (95% CI 0.43 to 11.69) (Analysis 3.32).
3.32. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 32 Change in FVC (% predicted).
The study by Moorcroft showed a significant improvement in the annual change in FVC (mL) in the training group compared to the control group, MD 213.00 mL (95% CI 3.01 to 422.99) (Moorcroft 2004) (Analysis 3.33).
3.33. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 33 Annual change in FVC (mL).
Additionally, Hebestreit measured RV/TLC; there was no observed difference between groups after three to six months, MD ‐0.90% (95% CI ‐6.73 to 4.93), six months off‐training, MD ‐2.20% (95% CI ‐11.33 to 6.93) and 12 to 18 months off‐training, MD ‐4.90% (95% CI ‐13.68 to 3.88) (Hebestreit 2010) (Analysis 3.34).
3.34. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 34 Change in RV/TLC (%).
5. Physical activity
This outcome was reported in one study using accelerometry (n = 38) (Hebestreit 2010) and in another study using a combination of a physical activity monitor (SenseWear armband) and a physical activity questionnaire (n = 14) (Beaudoin 2017). The instrument used by Beaudoin is available at www.ircm.qc.ca/CLINIQUE/educoeur/Documents/questionnaire.pdf; however, the authors of this review are not aware of any study that has validated this physical activity questionnaire in the CF population.
No differences between groups were found in total energy expenditure in the Beaudoin study, MD ‐108.92 k/cal (95% CI ‐360.20 to 142.37) (Analysis 3.35); the same was true for the number of daily steps, MD ‐110.58 (95% CI ‐2260.72 to 2039.56) (Analysis 3.36). However, after 12 weeks questionnaire‐assessed physical activity was significantly higher in the training group compared to the control group, MD 19.85 % (1.92 to 37.80) (Analysis 3.37) (Beaudoin 2017).
3.35. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 35 Change in Total Energy Expenditure (k/cal).
3.36. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 36 Change in the Number of Steps.
3.37. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 37 Change in Physical Activity (%).
In the study by Hebestreit, after three to six months, no differences were observed in vigorous physical activity (hours per week) between the training and control group, MD 1.05 hours per week (95% CI ‐0.66 to 2.76) or after six months off training, MD 2.08 (95% CI ‐1.84 to 6.00); however, a significant difference favouring the training group was seen after 12 to 18 months off training, MD 1.63 (95% CI 0.02 to 3.24) (Analysis 3.38).
3.38. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 38 Change in vigorous physical activity (hours per week).
6. Body composition
Changes in body composition were reported in three studies (n = 103) (Beaudoin 2017; Hebestreit 2010; Moorcroft 2004). Data on body weight, BMI, body fat and fat‐free mass were not reported in detail in the original paper by Hebestreit, but were additionally provided and analysed for this review (Hebestreit 2010).
Beaudoin reported on body weight and found no differences between groups after 12 weeks, MD ‐0.27 kg (95% CI ‐1.76 to 1.22) (Analysis 3.39) (Beaudoin 2017). Hebestreit also reported on total body weight and found no differences between the groups at three to six months, MD 1.10 kg (95% CI ‐0.42 to 2.62); after six months off training, MD 0.20 (95% CI ‐2.52 to 2.92); and after 12 to 18 months off training, MD 0.00 (95% CI ‐3.78 to 3.78) (Analysis 3.39) (Hebestreit 2010).
3.39. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 39 Change in body weight (kg).
Three studies reported on the change in BMI, but none of the results were significant (Beaudoin 2017; Hebestreit 2010; Moorcroft 2004). In the study by Beaudoin no between group differences were found after 12 weeks, MD 0.10 kg/m² (95% CI ‐0.61 to 0.80) (Analysis 3.40). Hebestreit reported at three to six months, MD 0.40 kg/m² (95% CI ‐0.17 to 0.97); after six months off‐training, MD 0.00 kg/m² (95% CI ‐0.78 to 0.78); and after 12 to 18 months off‐training, MD ‐0.10 kg/m² (95% CI ‐1.12 to 0.92); Moorcroft reported the change at one year, MD 0.54 kg/m² (95% CI ‐0.09 to 1.17) (Analysis 3.40).
3.40. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 40 Change in BMI (kg/m2).
Hebestreit additionally reported on the sum of four skin folds, which was not significantly different between groups at three to six months, MD ‐1.19 mm (95% CI ‐4.95 to 2.57); however, there were significant differences favouring the control group both after six months off‐training, MD ‐5.68 mm (95% CI ‐10.83 to ‐0.53) and after 12 to 18 months off‐training, MD ‐7.10 mm (95% CI ‐13.37 to ‐0.83) (Analysis 3.41).
3.41. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 41 Change in sum of four skinfolds (mm).
Hebestreit and Beaudoin further analysed the changes in body fat and fat‐free mass (Beaudoin 2017; Hebestreit 2010). In the study by Beaudoin, after 12 weeks significantly lower values for body fat (%) and fat mass (kg) were found in the exercise group compared to the control group, MD ‐1.21% (95% CI ‐2.38 to ‐0.05) (Analysis 3.42) and 1.09 kg (95% CI ‐1.80 to ‐0.39), respectively (Analysis 3.43); however, no difference was found between the two groups for fat‐free mass, MD ‐0.15 kg (95% CI ‐1.55 to 1.26) (Analysis 3.44) (Beaudoin 2017).
3.42. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 42 Change in body fat (%).
3.43. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 43 Change in fat‐mass (kg).
3.44. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 44 Change in fat‐free mass (kg).
In the study by Hebestreit, there were no significant differences at any time point in % body fat: at three to six months, MD 1.30% (95% CI ‐2.35 to 4.95); after six months off‐training, MD ‐0.50% (95% CI ‐4.77 to 3.77); and after 12 to 18 months off‐training, MD 2.20% (95% CI ‐3.90 to 8.30) (Analysis 3.42). Likewise, there were no differences between groups in fat‐free mass: at three to six months, MD 0.90 kg (95% CI ‐4.76 to 6.56); after six months off‐training, MD 0.70 kg (95% CI ‐2.08 to 3.48); or after 12 to 18 months off‐training, MD ‐1.40 kg (95% CI ‐6.86 to 4.06) (Analysis 3.44).
7. Acute exacerbations
No data were reported for this outcome in any of the studies.
8. Antibiotic use
No data were reported for this outcome in any of the studies.
9. Bone health
No data were reported for this outcome in any of the studies.
10. Diabetic control
Only Beaudoin reported on this outcome and the investigators have provided additional raw data from the study (Beaudoin 2017). The outcomes measured were HbA1c and the plasma glucose and insulin response to a two‐hour oral glucose tolerance test before and after 12 weeks (very low‐quality evidence) (Beaudoin 2017).
No differences in the change in HbA1c were observed between the exercise and control groups, MD ‐0.00 % (95% CI ‐0.01 to 0.00) (Analysis 3.45). In our analysis, this was also true for area under the curve for plasma glucose, MD ‐5.59 (95% CI ‐13.51 to 2.33) (Analysis 3.46) (in the original publication the authors reported a significant improvement in this outcome for the training group) and area under the curve for plasma insulin, MD ‐20.02 (95% CI ‐52.90 to 12.85) (Analysis 3.47). However, after 12 weeks the insulin sensitivity index was significantly higher in the exercise compared to the control group, MD 0.02 (95% CI 0.00 to 0.04) (Analysis 3.48).
3.45. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 45 Change in metabolic parameters (HbA1c (%)).
3.46. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 46 Change in metabolic parameters (Glucose AUC).
3.47. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 47 Change in metabolic parameters (Total Insulin AUC).
3.48. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 48 Change in metabolic parameters (Insulin Sensitivity Index).
The authors of this review further analysed data for plasma glucose and plasma insulin at different time points during the oral glucose tolerance test (time point 0 and 30, 60, 90 and 120 minutes after the oral glucose load). The authors presented these data in figures in the original publication (Beaudoin 2017).
Plasma glucose values were not different between groups at time points 0 minutes, MD 0.44 mmol/L (95% CI ‐0.41 to 1.28); 60 minutes, MD ‐1.86 mmol/L (95% CI ‐4.11 to 0.40); and 90 minutes, MD ‐1.69 mmol/L (95% CI ‐5.09 to 1.71). Significant differences in favour of the intervention group were noted for the time points 30 minutes after ingestion of the glucose solution, MD ‐1.96 mmol/L (95% CI ‐3.58 to ‐0.33) and at 120 minutes after ingestion of the glucose solution, MD ‐3.24 mmol/L (95% CI ‐6.41 to ‐0.06) (Analysis 3.49). Plasma insulin values were not different between groups at 0 minutes, MD ‐2.10 µU/mL (95% CI ‐5.46 to 1.26); at 90 minutes, MD 6.20 µU/mL (95% CI ‐17.05 to 29.45); and at 120 minutes, MD 2.23 µU/mL (95% CI ‐13.98 to 18.45). Significant differences in favour for the intervention group were noted for the time points 30 and 60 minutes after the ingestion of the glucose solution, MD ‐13.90 µU/mL (95% CI ‐19.47 to ‐8.33) and MD ‐12.39 µU/mL (95% CI ‐22.14 to ‐2.65), respectively (Analysis 3.50).
3.49. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 49 Change in Plasma Glucose (mmol/L).
3.50. Analysis.
Comparison 3 Combined aerobic and anaerobic training versus no physical training, Outcome 50 Change in Plasma Insulin (µU/mL).
The results presented herein are different to the results reported in the original publication by Beaudoin (Beaudoin 2017). Beaudoin reported within‐group changes for plasma glucose and plasma insulin at different time points (Figure 1 A‐D in the original publication) during the oral glucose tolerance test for the exercise and control group separately (Beaudoin 2017). The results presented herein should be interpreted with caution due to the low sample size and high chance for type II error.
11. Compliance with physical exercise training
This outcome was reported in two studies (Beaudoin 2017; Douglas 2015).
Beaudoin reported that over 80% (n = 8) were compliant to the exercise programme; this information was available from the study diary (Beaudoin 2017). Beaudoin excluded one participant from the exercise group due to non‐compliance based on self‐report and information derived from the study diary; but a definition of "compliance" and "non‐compliance" was not provided in the original publication.
In an interim analysis of the INSPIRE‐CF study, Douglas reported on participation and attendance and non‐attendance (%) in the physical exercise programme (Douglas 2015). Results were only reported for intervention group participants (n = 34) and between‐group differences can not be computed for this outcome. Narrative results from the abstract state that overall the mean (SD) attendance was 53.5 (23)% of 52 potential weeks in the first 12 months. Individual attendance ranged between 0% and 92% of sessions. Boys attended more often than girls (58% versus 49%). Major reasons for non‐attendance were: no membership with a fitness centre in place (6.4%), family (5.8%) or trainer holidays (6.3%) and unexplained non‐attendance (4.5%). Minor reasons were recorded as child illness (3%), hospital admissions or clinic appointments (2.8%), public holidays (2.5%), school events (1.9%), family events (1.7%), staff training (2.3%), with other reasons less than 1% accounting for the remaining missed sessions (3.5%).
12. Adverse events
No data were reported for this outcome in any of the studies.
Discussion
Summary of main results
This systematic review shows limited evidence from both short‐ and long‐term studies that in people with CF aerobic or anaerobic physical exercise training or a combination of both has a positive effect on exercise capacity, pulmonary function and HRQoL. Although improvements are not consistent between studies and ranged from no effects to clearly positive effects the most consistent effects of the heterogeneous exercise training modalities and durations were found for maximal aerobic exercise capacity measured by VO2 peak (in four out of seven studies) with unclear effects on FEV1 (in two out of 11 studies) and HRQoL (in two out of seven studies).
Also, the length of training required to obtain any physiological benefits in CF cannot be defined based on this review, but it is unlikely that training for short periods of less than one month would achieve physiological benefit (Casaburi 1992). Lung function as measured by FEV1 was not responsive of change, except in two studies (Kriemler 2013; Selvadurai 2002). Whether this finding is an indication of true non‐responsiveness or rather explained by poor exercise adherence, insufficient exercise training (sub‐optimal modality, insufficient frequency, intensity, duration) or by the inappropriate methodology of the current literature (i.e. insufficient power) has to be determined.
Overall completeness and applicability of evidence
The improvement of VO2 peak is of clinical relevance as exercise training addresses low exercise capacity as an important risk factor and strong predictor of mortality in CF (Nixon 1992). In order to have any measurable beneficial effect on exercise capacity, exercise training should be performed for at least six weeks, with exercises for an initially tolerable time, but progressing to at least 20 to 30 minutes of exercise at an intensity of 55% to 64% of maximum heart rate, for three to five days a week (ACSM 2010). Although many of the included studies were sufficient to achieve a training effect, this condition was not always fulfilled. Yet, no data are available on the minimal important difference of VO2 peak in CF that would provide us with some information about the clinical relevance of improvement in aerobic capacity.
Nevertheless, as the studies in this review recruited mixed populations with regard to age, gender, disease severity and stability, the results have some applicability to the general CF population. Due to the small number and heterogeneity of included studies, we were unable to tease out effects of different length, types (aerobic versus anaerobic versus a combination of both), level of supervision of training, and whether effects were different for subgroups by age, gender, genetical constellation, or severity of disease.
It is possible that more sophisticated functional measures such as pulmonary diffusing capacity and multiple‐breath washout may be more sensitive to document subtle, but clinically relevant effects of exercise training on pulmonary function than FEV1. Furthermore, in the included studies, HRQoL was rarely assessed and if so, mostly by non‐validated or generic questionnaires.
Quality of the evidence
Overall, there is very low‐ to low‐quality of evidence that aerobic or anaerobic physical exercise training or a combination of both has positive effects on VO2 peak, FEV1 and HRQoL. We are uncertain about the estimates and further research will very likely have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
It should be highlighted that considerable caution is indicated when interpreting the results of this review. The training modalities and durations were heterogenous, sometimes of very short duration and combined with additional treatments such as intensive physiotherapy, nutritional rehabilitation and intravenous antibiotic treatment in the short‐term in‐hospital studies (Cerny 1989; Selvadurai 2002). Further, most studies showed considerable methodological shortcomings based on the Cochrane risk of bias tool that was used (Higgins 2011); this may also reflect the inappropriate methodology of the current literature (i.e. insufficient power) in general. All studies had small sample sizes, which puts them at risk of imprecision and lack of power which can work in two ways, i.e. under‐ or overestimation of intervention effects (Ellis 2010).This phenomenon can at least in part be explained by a publication bias, as small studies are unlikely be published if they present negative results (Hopewell 2009).
A lack of effectiveness does not necessarily mean that the treatment was ineffective; especially in longer‐term studies, poor adherence to training, which requires precise monitoring, could be a reason for lack of treatment effects. Although standard outcome measures were used in the included studies to assess efficacy of physical exercise training, estimates for the minimal clinically important differences of these outcome measures were not available. Although the effect sizes for some of the outcome measures in this review were statistically significant, the clinical significance of these results remains open to interpretation.
Potential biases in the review process
There are some potential biases in the review process that need to be addressed. One important issue is participant selection bias which limits external validity. In 64% of the included full‐text articles (where inclusion and exclusion criteria were reported) participants were excluded based on disease severity expressed by FEV1, which is one of our primary outcome measures. We acknowledge that study investigators are ethically bound to keep potential exercise‐induced adverse reactions at a minimum; however, this limits the generalisability of findings to people with mild to moderate CF lung disease and may not be representative to the overall population of people with CF. We have chosen FEV1 and VO2 peak as primary outcomes measures because both are clinically relevant and predictive for mortality in people with CF. Moreover, HRQoL was chosen as important patient‐reported outcome. Overall, FEV1 was measured in all and VO2 peak and HRQoL in about half of the included studies, but results were mostly inconclusive. Despite extensive searches it is theoretically possible that we failed to identify studies. However, since the field of researchers publishing on physical exercise training in CF is relatively small and close‐knit, we are quite confident that we did not miss any potentially relevant study. In summary, this review includes a limited number of mostly small studies with low to moderate quality and predominantly unclear risk of bias.
Agreements and disagreements with other studies or reviews
To the best of the authors' knowledge, there are no other published systematic reviews on physical exercise training in people with CF. Due to the low number of included studies and the inability to pool study results in this review update, the overall conclusions have not substantially changed compared to the previously published versions of this Cochrane physical training review despite a larger number of included studies (Bradley 2002; Bradley 2008; Radtke 2015a).
Authors' conclusions
Implications for practice.
Conclusions about the efficacy of physical exercise training in cystic fibrosis (CF) are limited by the small size, duration and incomplete reporting of most of the studies included in this review. However, there is limited evidence that physical exercise training is beneficial.
The benefits obtained from including physical exercise training in a package of care may be influenced by the type of training programme and the inclusion of aerobic and anaerobic training. Physical exercise training is already part of the regular care offered to most people with CF and there is no evidence to actively discourage this.
In conclusion, the limited number of available studies with low to moderate quality does not allow us to make firm conclusions about the efficacy of physical exercise training on peak oxygen consumption (VO2 peak), forced expiratory volume in one second (FEV1) and health‐related quality of life (HRQoL) (primary outcomes) and other (secondary) outcomes.
Implications for research.
Further research is needed to comprehensively assess the benefits of exercise programmes in people with CF and the relative benefits of the addition of aerobic versus anaerobic versus a combination of both types of physical training to the care of people with CF. There is a need for high‐quality randomised controlled studies with sufficient numbers of study participants and well‐chosen, objectively measurable, reproducible and sensitive primary outcome measures. Physical exercise training components (type, intensity, duration, and frequency) should be sufficient to elicit beneficial adaptations and should be clearly reported and monitored. There is a lack of studies investigating the effects of physical exercise training on important and clinically relevant outcomes such as bone health, diabetic control and exacerbations, which could be a focus of future work. Investigators should also consider adherence to the training regimens. Moreover, the use of more sophisticated diagnostic techniques such as multiple‐breath washout and the measurement of pulmonary diffusing capacity during exercise may improve our understanding about the effects of physical exercise training on pulmonary function in CF. For all outcomes, meaningful and patient‐relevant changes of the outcomes need to be determined.
To draw firm conclusions, larger high‐quality studies are clearly needed to assess whether exercise training is safe, effective and well‐tolerated by people with CF. While exercise training appears to be safe in CF (Ruf 2010), safety measures should be implemented in exercise training studies and include the documentation of any (exercise‐related) adverse events, pulmonary function, exacerbations and oxygen saturation. Other important outcomes which should be used to measure effectiveness are improved (functional) exercise capacity and HRQoL.
The optimal training components (e.g. type, frequency, intensity, duration) need to be determined in the future by large high‐quality studies. Study investigators should carefully select the number and type of study endpoints as a high number of outcomes requiring time‐consuming assessments may decrease participants' compliance and on the other hand increase the risk of false‐positive results by chance. Besides selecting the clinically relevant and participant‐oriented outcomes, testing of the interrelationship of the outcome measures would ascertain whether, for instance, changes in HRQoL correlate with changes in exercise capacity (Hebestreit 2014).
What's new
| Date | Event | Description |
|---|---|---|
| 1 November 2017 | Amended | Formatting issues resolved |
History
Protocol first published: Issue 4, 2000 Review first published: Issue 2, 2002
| Date | Event | Description |
|---|---|---|
| 19 October 2017 | New citation required but conclusions have not changed | Despite the inclusion of two new studies our conclusions remain the same. |
| 19 October 2017 | New search has been performed | A search of the Cystic Fibrosis and Genetic Disorders Review Group's Cystic Fibrosis Trials Register identified 38 new references which were potentially eligible for inclusion in the review. There was one additional reference to an already included study (Schneiderman‐Walker 2000) and six additional references to five already excluded studies (Amelina 2006; del Corral Nunez‐Flores 2011; Kuys 2011; Lima 2014; Salonini 2015). Six references to two new studies has been included (Beaudoin 2017; Douglas 2015) and seven references to five new studies are listed as 'Awaiting classification' (Housinger 2015; Johnston 2004; Lorenc 2015; Mandrusiak 2011; Oliveira 2010). One study with two references is ongoing (Hebestreit 2016) and a total of 16 references to 13 new studies have been excluded (Bieli 2017; Bongers 2015; Calik‐Kutukcu 2016; Chang 2015; Dwyer 2017; Giacomodonato 2015; Haynes 2016; Kriemler 2016; Ozaydin 2010; Patterson 2004; Shaw 2016; Vallier 2016; Wheatley 2015). A search of clinicaltrials.gov identified 11 additional studies. Five studies were added to 'Awaiting classification' (NCT00609050; NCT00792194; NCT02552043; NCT03100214; NCT03109912), one study was added under ongoing studies (NCT02700243) and five studies were excluded (NCT02277860; NCT02715921; NCT02821130; NCT03117764; NCT02875366). A search of the WHO ICTRN identified three additional studies; one is listed as awaiting classification (ACTRN12617001009303) and two have been added under ongoing studies (Donadio 2017; Gupta 2017). From this update we have stated a minimum duration of the intervention as being at least two weeks. |
| 15 June 2015 | New citation required but conclusions have not changed | Two authors from the original review have stepped down at this update and a new team of authors have taken on the review. The title of the review has been changed from 'Physical training for cystic fibrosis' to 'Physical exercise training for cystic fibrosis' as the new team felt this better reflected the content of the review. Despite the inclusion of new studies and data in this update of the review, the conclusions remain the same. |
| 15 June 2015 | New search has been performed | A search of the Cystic Fibrosis and Genetic Disorders Group's Cystic Fibrosis Register identified 32 new references which were potentially eligible for inclusion in this review. Three new studies (one reference each) were included (Rovedder 2014; Santana‐Sosa 2012; Santana‐Sosa 2014). Two studies previously listed as excluded have been reassessed and moved to included studies with two new references each (although one paper referred to both studies) (Hebestreit 2010; Kriemler 2013). One study has been moved from 'Awaiting classification' to included studies with an additional two references (Hommerding 2015). One was an additional reference to an already excluded study (Kuys 2011). A total of 14 new studies (20 references) were excluded (Alarie 2012; Amelina 2006; Asher 1982; Balfour 1998; del Corral Nunez‐Flores 2011; Dwyer 2008; Gruet 2012; Lima 2014; Lowman 2012; Petrovic 2013; Rand 2012; Reix 2012; Salonini 2015; Vivodtzev 2013). One study (one reference) has been listed as 'Awaiting classification' until we are able to obtain further information (Almajan 2011). |
| 22 May 2012 | Amended | Contact details updated. |
| 7 March 2011 | New search has been performed | A total of two new references were identified in a search of the Group's CF Trials Register. One study was excluded as it compared Nintendo Wii exercise training to an existing exercise programme and hence did not meet the inclusion criteria (Kuys 2011). The other study did meet the inclusion criteria but outlined in its abstract that recruitment was ongoing and for this reason it has been listed as an ongoing study; results will be included in the review once the study has been completed (Phillips 2008a). In addition some amendments were made to the Background in order to incorporate updated guidelines and a relevant survey. |
| 19 January 2009 | Amended | The fourth primary outcome 'mortality' was moved to Secondary outcomes in line with Cochrane Collaboration guidance to limit the number of primary outcomes to three. |
| 5 January 2009 | New search has been performed | A search of the Group's Cystic Fibrosis Trials Register did not identify any references to trials which are potentially eligible for inclusion in this review. |
| 12 November 2008 | Amended | Converted to new review format. |
| 14 November 2007 | Amended | The generic inverse variance method has been used to analyse data which were previously not able to be presented in the 'Statistical Analysis'. The 'Synopsis' has been replaced by a new 'Plain Language Summary'. |
| 14 November 2007 | New search has been performed | The search identified 11 new references. Of these, two were additional references to already excluded studies (Albinni 2004; Edlund 1986). The remaining nine studies did not fulfill the inclusion criteria; four of these studies which seemed eligible from the title, have been excluded on the basis of trial design and are listed under 'Excluded studies' (Acquino 2006; Balestri 2004; Orenstein 2004; Stanghelle 1998). The study which was previously listed as 'Awaiting assessment' has been moved to the list of excluded studies after correspondence with the study authors (Hebestreit 2003). |
| 13 November 2007 | New citation required and conclusions have changed | Substantive amendment |
| 25 May 2005 | New search has been performed | A further article has been included (Klijn 2004). The full paper of the trial by Moorcroft (Moorcroft 2004) has also been included. Following publication of this paper, the details about the published abstracts of this trial, previously listed in the 'Characteristics of included studies' table, under Dodd 1998 and Moorcroft 2000 have been listed under Moorcroft 2004. We contacted authors of trials already included in the review regarding confirmation of data and requests for additional data. Their responses have been included in section detailing the search strategy. One trial has been moved from the 'Studies awaiting assessment' section to the 'Excluded studies' section of the review (Tuzin 1998). One trial has been added to the section 'Studies awaiting assessment' section (Hebestreit 2003). The authors have been contacted and have indicated that this study is in preparation for publication. |
| 31 July 2003 | Amended | The presentation of the data in MetaView has been re‐formatted. |
| 31 July 2003 | New search has been performed | The full paper of the Selvadurai trial has now been included, previously only the abstract of this trial was included in the review (Selvadurai 2002). A further two trials added to the 'Excluded studies' section of the review (Barry 2001; Kriemler 2001). |
Acknowledgements
We would like to thank Dr Judy Bradley and Dr Fidelma Moran, who have stepped down at the 2015 update, for their previous contributions to the review which are detailed below.
We would like to kindly thank Nikki Jahnke from the Cochrane Cystic Fibrosis and Genetics Disorders Group for her guidance and support during the process of writing this review.
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to the Cochrane Cystic Fibrosis and Genetic Disorders Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Data and analyses
Comparison 1. Aerobic training versus no physical training.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Change in VO2 peak during maximal exercise (ml/min per kg BW) | 3 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 At hospital discharge | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 8.53 [4.85, 12.21] |
| 1.2 At 1 month after discharge | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 4.91 [1.13, 8.69] |
| 1.3 At 3 months | 2 | 59 | Mean Difference (IV, Fixed, 95% CI) | 2.29 [‐2.71, 7.29] |
| 1.4 At 6 months | 1 | 25 | Mean Difference (IV, Fixed, 95% CI) | 18.33 [8.95, 27.71] |
| 1.5 At 6 months off training | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | 9.51 [‐1.32, 20.34] |
| 1.6 At 18 months off training | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 2.86 [‐9.70, 15.42] |
| 2 Change in FEV1(% predicted) | 4 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 At hospital discharge | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 2.03 [‐2.31, 6.37] |
| 2.2 At 1 month after discharge | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 1.53 [‐2.93, 5.99] |
| 2.3 At 3 months | 2 | 58 | Mean Difference (IV, Fixed, 95% CI) | 7.21 [2.49, 11.94] |
| 2.4 At 6 months | 1 | 25 | Mean Difference (IV, Fixed, 95% CI) | 17.17 [8.59, 25.75] |
| 2.5 At 6 months off training | 1 | 23 | Mean Difference (IV, Fixed, 95% CI) | 16.92 [6.07, 27.77] |
| 2.6 At 18 months off training | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | 12.45 [1.27, 23.63] |
| 2.7 Annual rate of change over 36 months | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | 2.01 [‐0.06, 4.08] |
| 3 Change in health‐related quality of life | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.1 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Change in mean power during WAnT (W per kg BW) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Change in strength (Newton metres) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Change in peak work capacity during maximal exercise (W per kg BW) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 Annual rate of change in peak work capacity during maximal exercise over 36 month (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8 Change in treadmill speed (km/h) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 Change in treadmill exercise time (min) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 Change in heart rate (beats per min) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 10.1 At rest at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 At maximal exercise at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 At maximal exercise ‐ annual rate of change over 36 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 Change in oxygen saturation (%) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 11.1 During maximal exercise at hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.2 During maximal exercise at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11.3 At rest at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 Annual rate of change in peak VE over 36 months (L/min) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 13 Change in FVC (% predicted) | 4 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 13.1 At hospital discharge | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 0.06 [‐2.55, 2.67] |
| 13.2 At 3 months | 2 | 58 | Mean Difference (IV, Fixed, 95% CI) | 4.89 [0.69, 9.08] |
| 13.3 At 6 months | 1 | 25 | Mean Difference (IV, Fixed, 95% CI) | 12.51 [5.90, 19.12] |
| 13.4 At 1 month after discharge | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐0.11 [‐2.64, 2.42] |
| 13.5 At 6 months off training | 1 | 23 | Mean Difference (IV, Fixed, 95% CI) | 15.09 [6.01, 24.17] |
| 13.6 At 18 months off training | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | 9.10 [‐0.94, 19.14] |
| 13.7 Annual rate of change over 36 months | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | 2.17 [0.47, 3.87] |
| 14 Change in FEF25‐75 (% predicted) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 14.1 Annual rate of change | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 Change in RV/TLC (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 15.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 Change in FEV1/FVC (% predicted) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 16.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 Change in total physical activity (counts per min) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 17.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 Change in moderate‐to‐vigorous physical activity (hours per week) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 18.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 Change in total physical activity (MJ/day) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 19.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 Change in body weight (kg) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 20.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.2 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 Change in BMI (kg/m2) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 21.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 Change in BMI z score | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 22.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23 Change in fat‐free mass (kg) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 23.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.2 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.3 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.4 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.5 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.6 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 24 Change in body fat (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 24.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 24.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 24.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 24.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 25 Annual rate of change of ideal weight for height (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 26 Change in triceps skinfold thickness (mm) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 26.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 27 Change in arm muscle circumference (cm) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 27.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 2. Anaerobic training versus no physical training.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Change in VO2 peak during maximal exercise (ml/min per kg BW) | 3 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 At hospital discharge | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 1.95 [‐1.61, 5.51] |
| 1.2 At 1 month after discharge | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐0.40 [‐4.03, 3.23] |
| 1.3 At 3 months | 2 | 41 | Mean Difference (IV, Fixed, 95% CI) | 5.54 [‐0.25, 11.34] |
| 1.4 At 6 months | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 17.7 [5.98, 29.42] |
| 1.5 At 6 months off training | 1 | 16 | Mean Difference (IV, Fixed, 95% CI) | 11.59 [‐1.02, 24.20] |
| 1.6 At 18 months off training | 1 | 15 | Mean Difference (IV, Fixed, 95% CI) | 9.26 [‐4.26, 22.78] |
| 2 Change in FEV1 (% predicted) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.4 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.5 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.6 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Change in HRQoL | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.1 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Change in HRQoL physical function (CF questionnaire) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Change in peak power during WAnT (W) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Change in mean power during WAnT (W) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 Change in mean power during WAnT (W per kg BW) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 Change in lower limb strength (Newton metres) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 Change in peak work capacity during maximal exercise (W) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 Change in peak work capacity during maximal exercise (W per kg body weight) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 10.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 Change in lactate during maximal exercise (mmol/L) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 11.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 Change in peak oxygen saturation during maximal exercise (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 12.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 Change in FVC (% predicted) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 13.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.3 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.4 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.5 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.6 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 Change in RV/TLC (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 14.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 Change in total physical activity (counts per min) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 15.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 Change in moderate to vigorous physical activity (hours per week) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 16.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 Change in physical activity (MJ/day) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 17.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 Change in weight (kg) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 18.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 Change in BMI (kg/m2) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 19.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 Change in fat‐free mass (kg) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 20.1 At hospital discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.2 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.3 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.4 At 1 month after discharge | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.5 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.6 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 Change in body fat (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 21.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.2 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.4 At 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 3. Combined aerobic and anaerobic training versus no physical training.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Change in VO2 peak during maximal exercise (ml/min per kg BW) | 2 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 1.1 At 12 weeks | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 At 3 ‐ 6 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 At 6 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.4 At 12 ‐ 18 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Change in FEV1 (% predicted) | 3 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 At 3 ‐ 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.4 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.5 At 12 ‐ 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Annual change in FEV1 (mL) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 3.1 At 12 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Change in subjective health perception (CFQ‐R) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 4.1 At 3 ‐ 6 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 At 6 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 At 12 ‐ 18 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Change in Quality of Life: CFQ‐R | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1 Physical Functioning at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Vitality at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 Emotional state at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.4 Eating disturbances at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.5 Treatment burden at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.6 Health perception at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.7 Social limitations at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.8 Body image at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.9 Role limitations at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.10 Weight problems at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.11 Respiratory symptoms at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.12 Digestion symptoms at 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Change in peak power during WAnT (W per kg body weight) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 At 3 ‐ 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.3 At 12 ‐ 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 Change in mean power during WAnT (W per kg body weight) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1 At 3 ‐ 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.3 At 12 ‐ 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 Change in muscle strength (all limbs) (1RM test) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8.1 Right upper limb at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Left upper limb at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.3 Right lower limb at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.4 Left lower limb at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 Change in muscular strength ‐ leg press (kg; 1 RM test) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 Change in Muscular Strength ‐ Chest press (kg; 1 RM test) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 10.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 Change in Muscular Strength ‐ Latpull down (kg; 1 RM test) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 11.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 Change in Muscular Strength ‐ Biceps curl (kg; RM test) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 12.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 Change in Muscular Endurance ‐ Number of push ups | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 13.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 Change in Muscular Endurance ‐ Number of sit ups | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 14.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 Change in Muscular Endurance ‐ Flexibility (cm) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 15.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 Change in Muscular Endurance ‐ hand grip strength (kg) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 16.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 Change in peak work capacity during maximal exercise (W per kg BW) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 17.1 At 3 ‐ 6 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.2 At 6 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 17.3 At 12 ‐ 18 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 Change in functional exercise capacity | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 18.1 6MWT distance (m) at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 6MWT distance (% predicted) at 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 Change in peak heart rate during 6MWT (beats/min) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 19.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 Annual change in peak heart rate (beat/min) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 20.1 Constant load bicycle ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.2 Constant load arm ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 Annual change in VE (L/min) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 21.1 Constant load bicycle ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21.2 Constant load arm ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 Change in peak ventilation (VE) during maximal exercise | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 22.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23 Annual change in lactate (mmol/l) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 23.1 Constant load bicycle ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 23.2 Constant load arm ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 24 Change in RR during 6MWT (breaths/min) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 24.1 At 3 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 25 Annual change in RR (breaths/min) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 25.1 Constant load bicycle ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 25.2 Constant load arm ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26 Annual change in RER | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 26.1 Constant load bicycle ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.2 Constant load arm ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 27 Change in oxygen saturation (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 27.1 At rest (at 3 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.2 During 6MWT (at 3 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 28 Change in Borg breathlessness score | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 28.1 At rest (at 3 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 28.2 During 6MWT (at 3 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 29 Annual change in Borg breathlessness score | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 29.1 Constant load bicycle ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 29.2 Constant load arm ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 30 Change in Borg fatigue score | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 30.1 At rest (at 3 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 30.2 During 6MWT (at 3 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 31 Annual change in Borg muscle effort | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 31.1 Constant load bicycle ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 31.2 Constant load arm ergometry (at 1 year) | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 32 Change in FVC (% predicted) | 3 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 32.1 At 12 weeks | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 32.2 At 3 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 32.3 At 3 ‐ 6 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 32.4 At 6 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 32.5 At 12 ‐ 18 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 33 Annual change in FVC (mL) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 33.1 At 1 year | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 34 Change in RV/TLC (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 34.1 At 3 ‐ 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 34.2 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 34.3 At 12 ‐ 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 35 Change in Total Energy Expenditure (k/cal) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 35.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 36 Change in the Number of Steps | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 36.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 37 Change in Physical Activity (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 37.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 38 Change in vigorous physical activity (hours per week) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 38.1 At 3 ‐ 6 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 38.2 At 6 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 38.3 At 12 ‐ 18 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 39 Change in body weight (kg) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 39.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 39.2 At 3 ‐ 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 39.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 39.4 At 12 ‐ 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 40 Change in BMI (kg/m2) | 3 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 40.1 At 12 weeks | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 40.2 At 3 ‐ 6 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 40.3 Annual change | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 40.4 At 6 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 40.5 At 12 ‐ 18 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 41 Change in sum of four skinfolds (mm) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 41.1 At 3‐6 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 41.2 At 6 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 41.3 At 12‐18 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 42 Change in body fat (%) | 2 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 42.1 At 12 weeks | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 42.2 At 3 ‐ 6 months | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 42.3 At 6 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 42.4 At 12 ‐ 18 months off training | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 43 Change in fat‐mass (kg) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 43.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 44 Change in fat‐free mass (kg) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 44.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 44.2 At 3 ‐ 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 44.3 At 6 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 44.4 At 12 ‐ 18 months off training | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 45 Change in metabolic parameters (HbA1c (%)) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 45.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 46 Change in metabolic parameters (Glucose AUC) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 46.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 47 Change in metabolic parameters (Total Insulin AUC) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 47.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 48 Change in metabolic parameters (Insulin Sensitivity Index) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 48.1 At 12 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 49 Change in Plasma Glucose (mmol/L) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 49.1 After 0 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 49.2 After 30 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 49.3 After 60 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 49.4 After 90 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 49.5 After 120 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 50 Change in Plasma Insulin (µU/mL) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 50.1 After 0 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 50.2 After 30 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 50.3 After 60 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 50.4 After 90 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 50.5 After 120 minutes | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Beaudoin 2017.
| Methods | Design: single‐centre, open‐label, parallel RCT (the record on clinicaltrials.gov states cross‐over design, but this is not evident from published paper). Inclusion criteria: participants with CF; age > 18 years; sedentary (less than 100 min/week of structured exercise assessed by physical activity questionnaire and phone interview; FEV1 > 40 % predicted; clinically stable for the last 6 weeks; IGT; CFRD without pharmacological treatment or elevated 1‐h plasma glucose concentration during an oral glucose tolerance test (indeterminate 1‐h glucose concentration of > 11.0 but 2‐h plasma glucose concentration < 7.8 mmol/L‐1). Exclusion criteria: current pulmonary exacerbation; use of oral or intravenous corticosteroids; low SaO2 during exercise; history of haemoptysis in the last 6 weeks. |
|
| Participants | 14 participants with CF. Group demographics Exercise group (n = 8): mean (range) age 31.9 (24; 41) years. Control groups (n = 6): mean (range) age 35.5 (22; 57) years. |
|
| Interventions | 12‐week combined aerobic and resistance training study. Exercise group: aerobic and resistance training exercises 3x per week for about 20 ‐ 40 minutes with a day off between the training sessions (in total 36 training sessions). Exercise intensity and volume were progressively increased. Participants recorded their training sessions in a diary. Once every 4 weeks, participants received a supervised training session and a phone call on a weekly basis.
Control group: no information was reported in the original publication. Detailed information on control intervention is available on clinicaltrials.gov. |
|
| Outcomes | Included in this study were: pulmonary function (FVC, FEV1); metabolic parameters (HbA1c, plasma glucose area under the curve, insulin sensitivity index, plasma insulin area under the curve (0 ‐ 120 min); exercise capacity measured by a cycle cardiopulmonary exercise test (VO2 peak and VE at VO2 peak); muscle strength (leg press, chest press, latpull down, biceps curl) and endurance (push‐up, sit‐up, flexibility, handgrip strength); body composition (bodyweight, BMI, body fat and fat‐free mass); HRQoL and objectively measured physical activity (steps per days; energy expenditure) and assessed by questionnaire. Further, inflammatory markers were measured in this study (e.g., IL‐1; IL‐6; IL‐8; YKL‐40 and CRP‐hs) but inflammatory biomarkers are not outcomes relevant for this review. |
|
| Notes |
Study registration: The study was registered as cross‐over trial (Clinicaltrials.gov NCT02127957) but results were reported as parallel‐design study. The authors confirmed that they had to stop the study due to recruitment problems. The authors presented only results from the first study phase (12 weeks). Information provided on clinicaltrials.gov "Intervention Model: Crossover Assignment" "Following the visit #6, patients in the control group will be invited to participate in a second study phase to participate in supervised exercise program. This participation will involve an additional 12 weeks of follow‐up, which included the same visit as Group 1 with exercises. In this case, to simplify participation and reduce the volume of blood collected, the final visit (#5) of the project will also be the first visit of exercises phase. This part of study, involves 2 supervised training sessions and 8 follow up phone call. The exercises program will be performed three times per week for about one hour." |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly assigned open‐label study with two parallel arms. Randomisation was conducted in blocks by gender with a ratio of 2:2. No details given for generation of sequence. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear whether outcome assessors blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | At screening,1 participant could not be randomized due to an adverse event during cardiopulmonary exercise testing. There were 3 dropouts post‐randomisation (18%).
The study was registered as crossover study but results for the second study part were not presented. |
| Selective reporting (reporting bias) | High risk | Heart rate and SaO2 were measured during cardiopulmonary exercise testing, but results were not reported. The second study phase was not reported in the original publication. |
| Other bias | High risk |
Sample size Information on sample size and recruitment goals differ between the information provided under Clinicaltrials.gov and the final publication. This study aimed to recruit 24 participants (12 exercise group, 12 control group), see Clinicaltrials.gov, NCT02127957. The recruitment goal was not achieved (N = 18 were recruited but only 17 randomised ), but no information was provided in the final paper. According to the power calculation provided in the original publication, 18 participants (9 per group) were required for the analysis. Finally, 14 participants completed the study so the study is likely to be underpowered. Statistical analyses The authors reported pre‐post within‐group changes and no between‐group differences as would be appropriate for a RCT. We received raw data from the authors and calculated between‐group differences for plasma glucose and plasma insulin values during the oral glucose tolerance test. Our results differ compared to the results reported in the original publication. The initial power analysis, aiming to demonstrate a difference of 1.5 mmol/L in plasma glucose levels 120 minutes after ingestion of the glucose solution after exercise training required a study sample of 18 participants (9 per group). Finally, only 14 participants completed the study that reduces the statistical power to observe a difference between the interventions in the study. Control intervention In the original publication, no information was provided on the control intervention. We noticed discrepancies between the registered (clinicaltrials.gov) and published trial design (cross‐over versus parallel‐group design). |
Cerny 1989.
| Methods | Design: single‐centre, parallel RCT during hospital admission for acute exacerbation. Inclusion criteria: participants with CF who were admitted to the hospital for treatment of an acute exacerbation. Those who were able to perform a pulmonary function test and provided written informed consent (assumed patient or parental depending on age) were included. Exclusion criteria: not described. |
|
| Participants | 17 participants with CF.
Group demographics Exercise group (n = 9): mean (SD) age 15.4 (4.9) years. Bronchial hygiene group (n = 8): mean (SD) age 15.9 (4.9) years. |
|
| Interventions | Short‐term aerobic study.
Group 1: 2 cycle ergometer sessions and 1 bronchial hygiene session per day during admission: mean (SD) 13 (3) days. Group 2: 3 bronchial hygiene sessions per day during admission: mean (SD) 13 days (2.6 days). |
|
| Outcomes | Included in this study were: pulmonary function (FVC, ERV, IC, FEV1, FEF25‐75,RV, FRC, TLC, Raw, SGAW, SaO2, and PFS); exercise performance during cycle ergometry with load increased by 0.3 W/kg every 2 minutes until participant could continue no longer (SaO2, peak load, EMG activity, peak HR, peak VE to peak load ratio, peak HR to peak load ratio); cough (15 min post treatment session); sputum (wet and dry weight, volume). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as randomised but no details of the method. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear whether outcome assessors blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There were no dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes detailed in methods were reported in results. Data reported for all time points. |
| Other bias | Unclear risk | Stated the inclusion criteria but not the exclusion criteria. Pulmonary function values FEV1 and FEF25‐75 were significantly lower in the control compared to the training group at admission. Clearly described statistical analysis methods. |
Douglas 2015.
| Methods | Design: single‐centre RCT (INSPIRE‐CF) in the UK; duration 24 months. Powered to show changes in primary outcome measure of FEV1 z score after 24 months (66 participants needed). Inclusion criteria: not described in abstract. Exclusion criteria: not described in abstract. |
|
| Participants | Recruited 71 participants with CF; age 6 to 15.5 years; mean (SD) FEV1 89 (16) % predicted. Group demographics Intervention group (n = 37). Control group (n = 34). 67 children completed the study. |
|
| Interventions | Intervention group: standard specialist care including weekly exercise training. Control group: standard specialist care without weekly exercise training. |
|
| Outcomes | Included in this study were: average and individual exercise training attendance rates (%); reason for non‐attendance to the exercise training programme. At baseline,12 and 24 months the following outcomes were measured: multiple‐breath washout (lung clearance index); spirometry (FEV1, FVC, FEV1/FVC (measured in litres and converted to z scores)); growth parameters (height; weight; BMI (measured in cm²; kg; and converted to z scores); cardiopulmonary exercise test (Bruce protocol): at peak and anaerobic threshold (VO2 peak; work rate (power); VE/VCO2; RER; HRmax; SaO2; 10m modified shuttle walk test (25‐level version) (distance in meters; level achieved); HRmax; SaO2; Cystic Fibrosis Questionnaire (CFQ UK version). At 6 months only spirometry and the 10 m modified shuttle walk test were repeated. |
|
| Notes | INSPIRE‐CF is an 24‐month exercise training study that investigates the effects of an individually tailored and supervised exercise training programme on lung function, exercise capacity and HRQoL for children with CF. This abstract evaluates the participation in the intervention group in the first year of the study (study has been completed, but not yet published in full). Study was powered to show changes after 24 months in primary outcome measure of FEV1 z score; Required 66 participants. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Described as randomised but no details of the method. Randomised by minimisation to one of the two groups (after baseline testing) by an independent blinded medical statistician using the SiMin software package (Wade 2006). |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Not possible to blind participants to intervention. Investigators confirmed that lung function (spirometry and multiple inert gas washout tests), and cycle ergometer cardiopulmonary exercise tests were performed by clinicians who were not made aware of the randomised grouping of the children. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigators confirmed blinded outcome assessment. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4 participants dropped out: 1 from the control group at 6 months (social concerns); 3 from the intervention group at 12 months (1 due to moving to a new area and changing hospitals; 2 because they no longer wished to exercise). |
| Selective reporting (reporting bias) | Unclear risk | This is an abstract so unable to assess if all outcome used in methods were reported in results. Unable to assess if data were reported for all time points. |
| Other bias | Unclear risk | None identified based on limited information available. |
Hebestreit 2010.
| Methods | Design: multicentre parallel RCT; duration 24 months (6‐month intervention and long‐term, open follow‐up period). Inclusion criteria: participants with CF; age > 12 years; FEV1> 35 % predicted; ability to perform physical activities. Exclusion criteria: non CF‐related chronic diseases and CF‐related conditions posing an increased risk to the participant when exercising. These were specifically oesophageal varicosis, pulmonary bullae, a < 80% drop in arterial oxygen saturation with exercise and signs of pulmonary hypertension on electrocardiogram and/or echocardiogram. |
|
| Participants | 38 participants with CF. Group demographics Exercise group (n = 23): mean (SD) age 19.5 (6.4) years. Control group (n = 15): mean (SD) age 19.4 (5.3) years. |
|
| Interventions | Long‐term partially supervised conditioning programme. Group 1 (intervention): exercise intervention with endurance‐type and strengthening exercises. Participants agreed to increase their vigorous physical activities by a minimum of 3x 60 min per week in the first 6 months of the study. An individual exercise plan was devised for participants; activity counselling was stopped after the first 6 months and participants were encouraged to maintain or further increase their physical activity level. Group 2 (control): participants told to keep their activity level constant during the first 12 months of the study. During the second year (period from 12 ‐ 24 months) they were free to change their activity behaviour. |
|
| Outcomes | Included in this study were: VO2 peak; peak workload; Wingate Anaerobic Test (PP, MP); FVC; FEV1; RV/TLC; vigorous physical activity; skinfold thickness; body fat; fat‐free mass and HRQoL. Outcomes were measured at baseline and after 3, 6, 12, 18 and 24 months. |
|
| Notes | This study is a full text article of the Hebestreit 2003 abstract. The author provided additional raw data for this review were not reported in detail in the original paper (e.g. data for RV/TLC, bodyweight, BMI, body fat and fat‐free mass). The control group in this study is also used in the Kriemler study (Kriemler 2013). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | 40 folded paper tickets were put into a bag with a 3:2 ratio, i.e. 24 tickets for the intervention group and 16 for the control group. Participants drew a ticket at random and the drawn ticket was then destroyed. Principal investigator was aware of the number of lots in the bag. |
| Allocation concealment (selection bias) | High risk | Participants drew a folded paper ticket from an opaque bag with closed eyes. In case that all lots have been drawn out by 1 study group, allocation concealment would no longer exist. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessors were not blinded with respect to the participants' group allocation for VO2 peak and skinfold measurements. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 5 participants dropped out during the first 12 months of the study: 3 gave no reason, 1 joined another study and 1 moved away. At 18 and 24 months, dropout rate was 13% and 26% respectively. Dropouts were balanced between groups. Reasons for drop out were not recorded. Intention‐to‐treat was not performed. |
| Selective reporting (reporting bias) | Unclear risk | Anaerobic capacity (PP, MP) was only reported for 18 ‐ 24 months follow up (non‐significant) and results for HRQoL are only presented for the scale 'physical functioning'. No effects were observed for all other HRQoL scales. |
| Other bias | Unclear risk | Financial support (max 200 Euro) was offered for intervention group participants to foster the realisation of the exercise training plan. |
Hommerding 2015.
| Methods | Design: Single‐centre parallel RCT; 3‐month duration Inclusion criteria: participants with CF aged 7 ‐ 20 years; stable disease, no signs of exacerbation of respiratory symptoms in last 15 days. Exclusion criteria: cognitive impairment, non CF‐related bone and muscle abnormalities, heart disease with haemodynamic instability. |
|
| Participants | 34 participants with CF (20 boys, 14 girls). Group demographics Exercise group (n = 17): mean (SD) age 13.4 (2.8) years. Control group (n = 17): mean (SD) age 12.7 (3.3) years. |
|
| Interventions | Aerobic exercise program based on verbal and written guidelines. Exercise group: participants took part in a 3‐month aerobic exercise training program based on verbal and written guidelines. The program included exercises such as jogging, swimming, walking, ball games and stretching exercises. Participants were told to practice the exercises at least twice a week for at least 20 min. No recommendations were provided regarding exercise intensity. Participants received telephone calls every 2 weeks and instructions were provided by one of the authors. Control group: Participants were instructed about aerobic exercises once at baseline according to the CF center routine. |
|
| Outcomes | Included in this study were: VO2 peak; FVC; FEV1; FEV1/FVC; FEF25‐75; HRQoL; self‐reported physical activity; body weight; BMI z score; triceps skinfold thickness; arm muscle circumference; SaO2 at rest and peak exercise, treadmill time; treadmill speed; peak HR; Borg breathlessness and fatigue. | |
| Notes | The sample size was estimated based on a mean (SD) change of 18.1 (13.8) points in the physical score of the HRQoL questionnaire. The estimated sample size was 15 participants in each group (95% power at a 5% level of significance). 2 more participants were included in each group to account for potential dropouts. Another study from the same group using the same aerobic exercise program was published recently (Schindel 2015). The responsible author of this publication confirmed that the vast majority of included participants were the same as in the Hommerding study (Hommerding 2015). There were only marginal differences in lung function (FEV1, FVC and FEF25‐75) compared to the Hommerding study for which reasons we decided not to include lung function data in this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were allocated to the intervention or control group in blocks of 6. A computer‐based program was used for randomisation. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear whether outcome assessors blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No drop outs were reported during the study. |
| Selective reporting (reporting bias) | Unclear risk | Blood pressure was measured prior to and after cardiopulmonary exercise testing but not reported. HR at rest and SaO2 at peak exercise were measured but results were not reported at baseline. |
| Other bias | Unclear risk | No validity criteria for maximal performance during cardiopulmonary exercise testing were reported in the methods. The mean (SD) peak heart rate reached during the exercise test was 157.1 (38.5) beats per min in the training group and 167.7 (20.8) beats per min in the control group, indicative of a submaximal effort. This likely underestimates the true VO2 peak of the study participants. |
Klijn 2004.
| Methods | Design: Single‐centre, parallel RCT, 3‐month duration. Inclusion criteria: Participants with CF aged 9 ‐ 18 years; a stable clinical condition (i.e., no need for oral or IV antibiotic treatment in the 3 months prior to testing); the absence of musculoskeletal disorders; and an FEV1 > 30 % predicted. Exclusion criteria: not specified. |
|
| Participants | 20 participants with CF (stable disease) completed the study.
Group demographics Group 1 (training) (n = 11): mean (SD) age 13.6 (1.3) years. Group 2 (control) (n = 9): mean (SD) age 14.2 (2.1) years. 3 participants dropped out; 1 withdrew from the training group for practical reasons (training group) and 2 from the control group as they did not complete assessments due to pulmonary exacerbations. |
|
| Interventions | Long‐term anaerobic study (12 weeks). Group 1: anaerobic exercise (2 days per week for 30 ‐ 45 min). Group 2: normal daily activities. |
|
| Outcomes | Included in this study were: BMI; FEV1; FVC; FEF25‐75; RV/TLC; Wingate Anerobic Test (PP, MP); VO2 peak; peak working capacity; VCO2; VE; RER; lactate; habitual activity estimation scale; HRQoL; fat‐free mass. Outcomes measured again at 12 weeks follow up. |
|
| Notes | To achieve a difference in PP per kg body weight of 10% with an SD of 0.8 W/kg and a statistical power of 80%, it was calculated that 8 participants had to be included in each study group. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as randomised, but no details of the method. |
| Allocation concealment (selection bias) | Low risk | Allocation concealed in opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. The primary researcher was blinded but their role in the study is unclear. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | The primary researcher was blinded, but it is unclear whether this researcher was responsible for outcome assessment. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Clear description and details about dropouts.
3 participants dropped out: 1 participant from the training group withdrew for practical reasons; 2 from the control group did not complete assessments due to pulmonary exacerbations. Intention‐to‐treat analysis was not performed. |
| Selective reporting (reporting bias) | Unclear risk | Results for HRQoL are only presented for the scale 'physical functioning' which was significantly higher in the training group after the 12‐week training period. No change in this HRQoL scale was observed in the control group after 12‐weeks. No significant effects were observed for any other HRQoL scales. Data were not reported in detail. |
| Other bias | Unclear risk | Clearly stated inclusion criteria but exclusion criteria were not reported. Described statistical methods used in analysis. |
Kriemler 2013.
| Methods | Design: multi‐centre, parallel RCT with 3 arms; 24 months (6‐month intervention and long‐term, open follow‐up period). Inclusion criteria: diagnosis of CF; aged 12 years and over; a FEV1 % predicted ≥ 35%; ability to perform physical activity without harm. Exclusion criteria: non‐CF related chronic diseases and conditions posing an increased risk to the participant when exercising. |
|
| Participants | 39 participants with CF split into 3 groups. Group demographics Group 1 (aerobic training) (n = 17): mean (95% CI) age 23.8 (21.5 to 26.5) years. Group 2 (strength training) (n = 12): mean (95% CI) age 19.0 (16.0 to 22.0) years. Group 3 (control) (n = 10): mean (95% CI) age 20.3 (17.0 to 23.6) years. A separate control group from a parallel study (Hebestreit 2010) was added due to an unusual deterioration of physical health in the control group in this study (n = 15), mean (95% CI) age 19.5 (16.8 to 22.2) years. |
|
| Interventions | Long‐term exercise study. Group 1: participants consented to perform 3 aerobic training sessions per week of 30 ‐ 45 min duration for the first 6 months and received support which was stopped thereafter. Group 2: participants consented to perform 3 strength training sessions per week of 30 ‐ 45 min duration for the first 6 months and received support which was stopped thereafter. Group 3: participants in the control group were told to keep their activity level constant. Free access to a fitness centre for 1 year was offered after the first study year. |
|
| Outcomes | Included in this study were: FEV1; FVC; RV/TLC; VO2 peak; peak workload; Wingate anaerobic test (PP, MP); physical activity; body fat; fat‐free mass. | |
| Notes | This study is a full text article of the Kriemler 2001 and Hebestreit 2003 abstracts. The control group experienced a deterioration of physical health during the study. In the original paper, a second control group from a German study with similar design and methods (Hebestreit 2010) was used for comparisons. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Participants were randomly assigned by a lot that was drawn from an opaque bag with closed eyes. Investigator was aware of the number of lots in the bag. |
| Allocation concealment (selection bias) | High risk | Participants drew a lot from an opaque bag with closed eyes. In case that all lots have been drawn out by one study group, allocation concealment would no longer exist. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors were blinded for pulmonary function testing (primary outcome FEV1). Outcome assessors were not involved in supervision and delivery of the intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Clear description and details about excluded participants and drop‐outs. 3 participants were excluded at baseline due to FEV1 below 35% predicted. 8 participants dropped out at different time points (exacerbation n = 1; non‐compliance n = 2; death n = 2; unclear reasons n = 3). 2 of the participants that dropped out for unclear reasons were in the control group and one was in the aerobic training group. Dropout rate was 21%. Intention‐to‐treat analysis was not performed. |
| Selective reporting (reporting bias) | Low risk | All outcome detailed in methods were reported in results except HRQoL (secondary outcome) which was mentioned to be reported separately. In the meantime published as Hebestreit et al. BMC Pulm Med. 2014, 27;14:26. HRQoL data were pooled from two intervention studies (Hebestreit 2010; Kriemler 2013) and results were presented for baseline and 6‐month follow up. |
| Other bias | Unclear risk | Clearly stated inclusion and exclusion criteria and described statistical methods used in analysis. Due to the deterioration of physical health in the control group, the results of this study should be interpreted with caution. |
Michel 1989.
| Methods | Design: single‐centre, parallel RCT during hospital admission. Inclusion criteria: not specified. Exclusion criteria: not specified. |
|
| Participants | 9 participants with CF, not stated how many allocated to each group.
Group demographics Exercise group: mean (SD) age 25.5 (10.5) years. Non‐exercise group: mean (SD) age 21.5 (3.2) years. |
|
| Interventions | Short‐term aerobic study.
Group 1: exercise and standardised CF protocol. Group 2: standardised CF protocol. |
|
| Outcomes | Included in this study were: skin folds; mid‐arm circumference; grip strength; respiratory muscle strength; ideal body weight. Measured at 1 month post‐discharge. |
|
| Notes | Limited information as published as abstract only. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as randomised, but no details of method. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear whether outcome assessors blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No details of dropouts or whether intention‐to‐treat analysis had been used. |
| Selective reporting (reporting bias) | Unclear risk | This is an abstract so unable to assess if all outcome used in methods were reported in results. Unable to assess if data were reported for all time points. |
| Other bias | Unclear risk | Do not state inclusion or exclusion criteria, nor do they describe the methods of statistical analysis used. |
Moorcroft 2004.
| Methods | Design: single‐centre, parallel RCT; 1‐year duration. Inclusion criteria: participants with CF who were willing to participate were recruited from a population of 150 attending the adult CF centre in Manchester at the time of the study. All participants had documented CF on the basis of clinical history plus either an increased sweat chloride or abnormal genetic testing. Exclusion criteria: participation in another clinical trial; pregnancy; transplant listing, or clinical cor pulmonale. |
|
| Participants | 51 participants with CF were randomised; 42 completed the study.
Group demographics Exercise group (n = 30): mean (SD) age 23.5 (6.4) years. Control group (n = 18): 23.6 (5.5) years. 3 participants dropped out at the start of programme: 1 from training group due to failure to attend on initial assessment; and 2 in the control group were withdrawn due to ill health. A further 6 participants dropped out during the 1‐year period. |
|
| Interventions | Long‐term aerobic and anaerobic study over 1 year.
Group 1: unsupervised exercise (based on individual preferences general aerobic exercises for lower body and weight training for upper body) 3 times per week. Group 2: control (continue with usual activities). |
|
| Outcomes | Included in this study were: FEV1; FVC; whole blood lactate; RER; heart rate; Borg breathlessness and muscle effort; VE, RR peak for arm and bicycle ergometry at 55% maximal workload; BMI and weight. | |
| Notes | This study is a full text article of Dodd 1998 and Moorcroft 2000 abstracts. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised to either active or control groups in a ratio of 3:2. A stratified randomisation in blocks (block size not stated) was used to balance the groups for FEV1, sputum colonisation by Burkholderia cepacia and gender. No details of method reported. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear whether outcome assessors blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 3 participants dropped out at the start of programme: 1 from training group due to failure to attend on initial assessment; and 2 in the control group were withdrawn due to ill health. A further 6 participants dropped out during the 1‐year period. Reasons for dropout were not clearly reported. After 1 year, overall dropout rate was 18% and balanced among the groups (19% in the intervention and 15% in the control group). Intentition‐to‐treat analysis was not performed. Missing data were treated by omission and only data for those who completed study presented. |
| Selective reporting (reporting bias) | Low risk | All outcome detailed in methods were reported in results. Data reported for all time points. |
| Other bias | Low risk | Clearly stated inclusion and exclusion criteria and described method of statistical analysis used. |
Rovedder 2014.
| Methods | Design: single‐centre, parallel RCT; 3‐months home‐based exercise programme. Inclusion criteria: participants diagnosed with CF in accordance with the criteria of the consensus;aged ≥16 years; ≥ 30 days of clinical respiratory disease stability. Exclusion criteria: participants who refused to take part in the study; pregnant ladies; individuals with heart disease, orthopaedic or traumatological problems. |
|
| Participants | 41 participants with CF. Group demographics Exercise group (n = 22): mean (SD) age 23.8 (8.3) years. Control group (n = 19): mean (SD) age 25.4 (6.9) years. 2 study participants in the exercise group could not be assessed at the 3‐months follow up due to lung transplant assessment. |
|
| Interventions | 3‐month home‐based exercise programme. Group 1: participants received printed guidance for aerobic and muscle strengthening exercises and were advised to perform the programme on a daily basis. Weekly telephone contacts were performed during the 3‐month period. Group 2: control group participants received standard programme without any specific exercise instructions. |
|
| Outcomes | Included in this study were: HRQoL; FEV1; FVC; walking distance (6MWT); SaO2 at peak exercise; RR at peak exercise; peak exercise HR; dyspnoea and fatigue scores; upper and lower body muscle strength. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomly allocated in blocks of 6 to the exercise or control group. A computer programme was used to generate randomisation sequence. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. 1 researcher was blinded to the randomisation and intervention and was responsible for database entries. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2 participants in the exercise group could not be assessed at the 3‐month visit due to submission to the lung transplant programme. Intention‐to‐treat analysis was used and imputations for missing data were performed for these 2 participants. |
| Selective reporting (reporting bias) | Low risk | All outcome detailed in methods were reported in results. Data reported for all time points. |
| Other bias | Unclear risk | Clearly stated inclusion and exclusion criteria and described method of statistical analysis used. Baseline between‐group differences existed in BMI which could possibly impact on HRQoL (primary outcome). |
Santana‐Sosa 2012.
| Methods | Design: single‐centre, parallel RCT; 3‐month duration (8 weeks training, 4 weeks detraining). Inclusion criteria: potential participants included 111 children previously diagnosed using a genetic test for CF and treated at the Children’s Hospital Nino Jesus in Madrid. Males or females aged 5 to 15 years and living in the Madrid area (able to attend training sessions). Exclusion criteria: severe lung deterioration, as defined by an FEV1 < 50% predicted; unstable clinical condition (i.e. hospitalisation within the previous 3 months); Burkholderia cepacia infection; musculoskeletal disease or any other disorder impairing exercise. |
|
| Participants | 22 participants with CF. Group demographics. Training group (n = 11): mean (SEM, range) age 11 years (3 years, 5 ‐ 15 years). Control group (n = 11): mean (SEM, range) age 10.0 years (2 years, 6 ‐ 14 years). |
|
| Interventions | 8‐week intrahospital programme followed by a 4‐week detraining period. All participants received the same chest physiotherapy during the entire study period. Group 1: endurance and strengthening exercises, 3 times per week. Group 2: control. |
|
| Outcomes | Included in this study were: VO2 peak; upper and lower body strength (bench press, leg press, seated row); FEV1; FVC; PImax; SaO2 at peak exercise; body weight; BMI; fat‐free mass; body fat; HRQoL; Timed Up and Go test (TUG); Timed Up and Down Stairs test (TUDS). | |
| Notes | Additional raw data for all included outcomes provided by the authors | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants were randomly assigned to exercise or control group with a block on gender based on the randomisation sequence. No details about how randomisation sequence was generated. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Personnel involved in training not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors were blinded to participants group assignment. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Clear description of missing outcome data. 5 participants could not be assessed at different time points (1 post‐intervention and 4 after detraining) due to hospitalisations (n = 3), relocation (n = 1) and parents who declined further evaluation (n = 1). Dropout rate was unbalanced with 28% in the control group and 9% in the intervention group after the detraining period. Intention‐to‐treat analysis was used and missing outcome data (at post‐training or detraining visit) were replaced by baseline data. |
| Selective reporting (reporting bias) | Low risk | All outcomes detailed in methods were reported in results. Data reported for all time points. |
| Other bias | High risk | Some raw data were made available, but there were inconsistencies between raw data and data reported in the original publication. There were significant between‐group differences in primary (VO2 peak) and secondary (strength measures) outcome measures at baseline. |
Santana‐Sosa 2014.
| Methods | Design: single‐centre, parallel RCT; 3‐month study (8 weeks training, 4 weeks detraining). Inclusion criteria: potential participants included 95 outpatient children previously diagnosed with CF by genetic testing and treated at the Children’s Hospital Nino Jesus in Madrid. Males or females aged 6 – 17 years and living in the Madrid area (able to attend training sessions). Exclusion criteria: severe lung deterioration (FEV1 < 50% predicted); unstable clinical condition (i.e., hospitalisation within the previous 3 months); Burkholderia cepacia infection or any disorder (e.g., musculoskeletal) impairing exercise. |
|
| Participants | 20 participants with CF. Group demographics Training group (n = 10): mean (SEM) age 11.1 (1.1) years. Control group (n = 10): mean (SEM) age 10.1 (1.1) years. |
|
| Interventions | 8‐week programme followed by a 4‐week detraining period. All participants received the same standard chest physiotherapy. Group 1: whole body aerobic and weight training 3 times per week, plus two daily inspiratory muscle training sessions Group 2: control group performed inspiratory muscle training only at a low intensity. |
|
| Outcomes | Included in this study were: VO2 peak; FVC; FEV1; PImax; SaO2 at peak exercise, muscle strength; body weight; body fat; fat‐free mass; and HRQoL. | |
| Notes | Additional raw data for all included outcomes provided by the authors | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation to intervention or control group with block on gender. No details given for sequence generation. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Personnel involved in training not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors were blinded to participants group assignment. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Clear description of missing outcome data. 3 participants of the control group could not be assessed at different time points (1 for post‐intervention and detraining phase and 2 after detraining phase) due to hospitalisation for lung transplantation preparation (n = 1), infection with Burkholderia cepacia (n = 1) and refusal (n = 1). Unbalanced distribution of dropouts. Dropout rate in the control group was 30% versus none in the intervention group. Intention‐to‐treat analysis was reported, but it is not clear how missing data were handled. |
| Selective reporting (reporting bias) | Low risk | All outcome detailed in methods were reported in results. Data reported for all time points. |
| Other bias | High risk | Some raw data were made available, but there were inconsistencies between raw data and data reported in the original publication. Significant between‐group differences in primary outcomes (VO2 peak and strength measures) existed at baseline. |
Schneiderman‐Walker 2000.
| Methods | Design: single‐centre, parallel RCT, 3‐year duration. Inclusion criteria: participants with CF aged 7 ‐ 19 years with an FEV1 > 40% predicted. Exclusion criteria: not specified. |
|
| Participants | 65 participants with CF; 2 groups similar at baseline. 7 dropouts.
Group demographics Exercise group (n = 30): mean (SD) age 13.4 (3.9 years). Control group (n = 35): mean (SD) age 13.3 (3.6) years. |
|
| Interventions | Long‐term aerobic study.
Group 1: minimum of 20 min aerobic activity plus 5 min warm up and cool down 3 times per week. Group 2: maintained regular activity (control). |
|
| Outcomes | Included in this study were: FVC; FEV1; FEF25‐75; PEFR; TV; VO2 peak; VCO₂; peak exercise heart rate; peak exercise VE; VE peak/MVV; RER; blood pressure; % of ideal weight for height; compliance and sense of well‐being; feasibility of exercise; hospital stays and number of days in hospital; chest X‐ray; and Schwachman scores. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation sequence. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Pulmonary function assessors were blinded to group assignment (primary outcome measure). |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Clear description and details about 7 dropouts were recorded. Intention‐to‐treat analysis was reported to yield similar results for pulmonary function. Results were only reported for 65 participants who completed the 2‐year follow up. |
| Selective reporting (reporting bias) | Low risk | All outcome detailed in methods were reported in results. Data reported for all time points. |
| Other bias | Unclear risk | Groups similar at baseline. Stated the inclusion criteria but not the exclusion criteria. Described statistical methods used in analysis. |
Selvadurai 2002.
| Methods | Design: single‐centre, parallel RCT; hospital admission for recurrent chest infections. Inclusion criteria: children with CF, aged 8 ‐ 16 years who were admitted the the Royal Alexandria Hospital for Children for the treatment of an infectious pulmonary exacerbation. Exclusion criteria: children with known pulmonary hypertension, or who required daytime oxygen prior to the pulmonary exacerbation which led to the hospital admission. |
|
| Participants | 66 children with CF (28 males, 38 females). No dropouts.
Group demographics Aerobic training group (n = 22): mean (SD) age 13.2 (2.0) years), 9 males and 13 females. Resistance training group (n = 22): mean (SD) age 13.1 (2.1) years, 10 males and 12 females. Control group (n = 22): mean (SD) age 13.2 (2.0) years, 9 male and 1 females. |
|
| Interventions | Short‐term aerobic and anaerobic/strength training study during hospital admission (mean duration 18.7 days, range 14 ‐ 36 days).
Group 1: 30 min supervised aerobic exercise training 5 times per week. Group 2: 30 min supervised resistance training 5 times per week. Group 3: no specific training. |
|
| Outcomes | Included in this study were: VO2 peak; peak VE; VCO₂; peak HR; HRQoL; FEV1; FVC; weight; lower limb strength; and fat‐free mass. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random allocation in sets of 6. No details given for generation of sequence. |
| Allocation concealment (selection bias) | Low risk | Concealed information inside opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear whether outcome assessors blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Stated no dropouts. |
| Selective reporting (reporting bias) | Unclear risk | Did not report on all secondary outcomes detailed in methods (e.g. VE, VCO2, RQ) in results. Data reported for all time points. |
| Other bias | Low risk | Clearly stated inclusion and exclusion criteria. Described statistical methods used to analyse data. |
Turchetta 1991.
| Methods | Design: single‐centre, parallel RCT; hospital admission for routine assessment of clinical condition. Inclusion criteria: not specified. Exclusion criteria: not specified. |
|
| Participants | 12 children with CF, 8 males, mean age 12.3 years. No group demographics available. | |
| Interventions | Short‐term aerobic study.
Group 1: 20 min running or treadmill per day for 2 weeks. Group 2: normal hospital treatment. |
|
| Outcomes | Included in this study were: FEV1 and FVC. | |
| Notes | This study has only been reported in a single abstract and therefore the information is limited. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as randomised, but no details given for sequence generation. |
| Allocation concealment (selection bias) | Unclear risk | Not discussed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not possible to blind participants to intervention. Unclear whether personnel blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear whether outcome assessors blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No details of dropouts or whether intention‐to‐treat analysis had been used. |
| Selective reporting (reporting bias) | Unclear risk | This is an abstract so unable to assess if all outcome used in methods were reported in results. Data were reported for all time points. |
| Other bias | Unclear risk | Do not state inclusion or exclusion criteria, nor do they describe the methods of statistical analysis used. |
BMI: body mass index CF: cystic fibrosis CFRD: cystic fibrosis‐related diabetes FEF25‐75: forced expiratory flow 25‐75% FEV1: forced expiratory volume at one second FRC: functional residual capacity FVC: forced vital capacity HRQoL: health‐related quality of life IGT: impaired glucose tolerance MP: mean power MVV: maximal voluntary ventilation PFS: progression‐free survival PImax: maximum inspiratory mouth pressure PP: peak power Raw: airways resistance RCT: randomised controlled trial RER: respiratory exchange ratio RR: respiratory rate RV: residual volume SaO2: oxygen saturation SD: standard deviation SEM: standard error of the mean SGAW: specific airways conductance TLC: total lung capacity VE: minute ventilation VO2 peak: peak oxygen consumption VCO2: carbon dioxide production VO2: oxygen uptake W: watt WAnT: Wingate Anaerobic Test 6MWT: six‐minute walk test
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Alarie 2012 | This study compared the acute cardiovascular response in participants playing different active video games. No control group included. |
| Albinni 2004 | This study was designed with the exercise group as the control group, therefore we could not compare data with baseline, no physical exercise training as per our protocol. |
| Amelina 2006 | IMT training and not physical exercise training as per our protocol. |
| Andreasson 1987 | Not a randomised controlled study. |
| Aquino 2006 | This study was designed with the aim of comparing the effectiveness of a single treatment sessions of exercise and PEP on sputum clearance. Participants in this study did not undertake a programme of physical training. |
| Asher 1982 | IMT training and not physical exercise training as per our protocol. |
| Balestri 2004 | This study was designed with the aim of comparing the effectiveness of a single treatment session of exercise and PEP on sputum clearance. Participants in this study did not undertake a programme of physical training. |
| Balfour 1998 | Not a physical exercise training study, comparison of different tests for assessing exercise capacity. |
| Barry 2001 | Not a randomised controlled study. |
| Bieli 2017 | Study of respiratory muscle endurance training, not a physical exercise training study. |
| Bilton 1992 | This study was designed with the aim of comparing the effectiveness of a single treatment session of exercise or physiotherapy or exercise and physiotherapy on sputum clearance and lung function. Participants in this study did not undertake a programme of physical training. |
| Bongers 2015 | Study evaluating the clinical usefulness of the steep ramp test and not a physical training study. |
| Calik‐Kutukcu 2016 | No control group with no physical training. |
| Chang 2015 | Study of methods for evaluating muscle function and not a physical training study. |
| Chatham 1997 | This study involved respiratory muscle training exclusively. This intervention does not constitute physical training as defined within our protocol. |
| de Jong 1994 | Not a randomised controlled study. |
| del Corral Nunez‐Flores 2011 | No control group with no physical training. |
| Dwyer 2008 | Study duration insufficient, |
| Dwyer 2017 | Study duration insufficient, |
| Edlund 1986 | Not a randomised controlled study. |
| Falk 1988 | This study was designed with the aim of comparing the effectiveness of a single treatment session of exercise or positive expiratory pressure on lung function. Participants in this study did not undertake a programme of physical training. |
| Giacomodonato 2015 | Study of respiratory muscle endurance training and not a physical training study. |
| Gruet 2012 | No control group with no physical training. |
| Haynes 2016 | Evaluation of the incremental step test not a study of physical training. |
| Heijerman 1992 | Not a randomised controlled study. |
| Irons 2012 | Not a physical exercise training study, examines effect of a singing program compared to no singing. |
| Kriemler 2016 | Study duration insufficient, only 3 single day interventions on non‐consecutive days of a week. |
| Kuys 2011 | Compares Nintendo Wii exercise training to an existing exercise programme, no control group with no physical training. |
| Lannefors 1992 | This study was designed with the aim of comparing the effectiveness of a single treatment session of exercise and FET or positive expiratory pressure and FET or postural drainage, thoracic expansion exercises and FET on mucous clearance. Participants in this study did not undertake programme of physical training. |
| Lima 2014 | No physical exercise training study, study looks at effect of non‐invasive ventilation on exercise capacity and lung function. |
| Lowman 2012 | No control group with no physical training. |
| NCT02277860 | Not a randomised controlled study, single arm trial of physical exercise, |
| NCT02715921 | Not a randomised controlled study, single arm trial of physical exercise, |
| NCT02821130 | A study of CFTR potentiator therapy and effects on exercise capacity. |
| NCT02875366 | A study of CFTR potentiator therapy and effects on exercise capacity. |
| NCT03117764 | Not a randomised controlled study, study of the effect of antibiotics on muscular strength and not physical training. |
| Orenstein 1981 | Not a randomised controlled study. |
| Orenstein 2004 | Compares aerobic training to upper‐body strength training, no control group with no physical training. |
| Ozaydin 2010 | IMT training and not physical exercise training as per our protocol. |
| Patterson 2004 | Study to evaluate the efficacy of the test of incremental respiratory endurance, not a physical training study. |
| Petrovic 2013 | Not a randomised controlled study. |
| Rand 2012 | Not a physical exercise training study. This study was designed to develop an incremental field exercise test for children with CF. |
| Reix 2012 | Acute study comparing exercise with expiratory breathing manoeuvres to breathing techniques for airway clearance. |
| Salh 1989 | Not a randomised controlled study. |
| Salonini 2015 | A comparison of two exercise interventions (Xbox Kinect versus stationary cycle). No control group with no physical training. |
| Shaw 2016 | No control group with no physical training. |
| Stanghelle 1998 | Not a randomised controlled study. |
| Tuzin 1998 | Not a randomised controlled study. |
| Vallier 2016 | Study to evaluate modified shuttle test and not a study of physical training. |
| Vivodtzev 2013 | This study evaluated neuromuscular electrical stimulation prior to endurance training in people with CF. No control group with no physical training. |
| Wheatley 2015 | Intervention only given on 3 single days, comparison of physical training and albuterol for airway clearance. |
CF: cystic fibrosis FET: forced expiration technique IMT: inspiratory muscle training PEP: positive expiratory pressure
Characteristics of studies awaiting assessment [ordered by study ID]
ACTRN12617001009303.
| Methods | RCT. Parallel design. Duration: 12 weeks. |
| Participants | Target sample size: 150. Inclusion criteria: confirmed diagnosis of CF, hospital inpatient admission (including hospital in the home) for IV antibiotic therapy for a respiratory cause, informed consent, access to the Internet via computer or mobile device. Exclusion criteria: presence of severe co‐morbidity limiting mobilisation or physical activity participation, previous lung transplantation, pregnancy. Age minimum: 12 Years Age maximum: 24 Years Gender: Both males and females |
| Interventions |
Intervention group: use of the ActivOnline program, via the Internet, as well as usual care. ActivOnline was developed in accordance of the principles of motivational interviewing and has been used to promote physical activity participation in older adults with chronic respiratory disease. Those allocated to the ActivOnline group will be provided with a unique logon and password to access the ActivOnline program and will be asked to record their daily physical activity and exercise using the secure portal. When logging onto ActivOnline they will be prompted to set goals, will record their PA or exercise using a pedometer or other device of their choice and will regularly enter data about that will be displayed graphically so they can see their progress. Control group: usual care. Usual care provides details for an online resource regarding physical activity participation and physical activity targets for children and young adults (www.nhs.uk/Livewell/fitness/Pages/physical‐activity‐guidelines‐for‐young‐people.aspx) as well as activity and exercise guidance, as indicated, as part of their routine clinical care on hospital discharge. |
| Outcomes |
Primary outcome Change in physical activity participation objectively measured via accelerometry Secondary outcomes Change in exercise capacity as measured by the MST Change in health related quality of life as assessed by the CFQ‐R Change in HADS Change in lung function as measured by FEV1 Change in physical activity participation objectively measured via accelerometry Change in physical activity participation self reported by the HAES Change in the CES‐D scale Change in the PSQI Number of hospital inpatient days by medical record review Time to first hospital admission, by medical record review |
| Notes | Supported by UK CF Trust. Email confirmation from lead investigator (17 August 2017) that trial has been completed and they are currently analysing data. We hope to obtain data for the CF participants once the trial has been published. |
Almajan 2011.
| Methods | Parallel design RCT. 6‐month intervention. |
| Participants | 38 participants with CF aged 7 ‐ 13 years. No group demographics available. Inclusion criteria: not specified. Exclusion criteria: not specified. |
| Interventions | Group 1 (n = 19): classical physiotherapy plus sport activities 3 times per week. Group 2 (n = 19): classical physiotherapy alone. |
| Outcomes | Eligible for inclusion are: FEV1; FVC; FEF25‐75; number of hospitalisations; participation at school; and activities of daily living. |
| Notes | No information were available in the abstract about types of exercises, intensity, frequency and duration of exercise training. |
Housinger 2015.
| Methods | Design: Modified RCT; motivational incentive‐based walking program for patients hospitalised with pulmonary exacerbation. Series of 2‐week intervals with 1‐week wash‐out periods were created and randomized as either treatment or control. |
| Participants | 29 participants with CF (11 males; 18 females). Group demographics: Intervention group (n = 18) Control group (n = 11) Inclusion criteria: not specified. Exclusion criteria: not specified. |
| Interventions |
Intervention group (n = 18): incentive‐based walking program plus standard care including daily (Monday to Friday) physical therapy. Control group (n = 11): standard care including daily (Monday to Friday) physical therapy. |
| Outcomes | Included in this study were: 6MWT distance; vital signs; Bruininks‐Oseretsky Test of Motor Proficiency; strengths assessment score and HRQoL (CFQ‐R). Data were collected within 72 hours of hospital admission and within 48 hours of hospital discharge. |
| Notes |
Johnston 2004.
| Methods | Design: parallel RCT; 6‐week exercise programme followed by a 16‐week home‐based programme. |
| Participants | 89 participants aged 7 ‐ 11 years old and with different lung conditions: asthma (n = 60), CF (n = 12), a history of chronic neonatal lung disease (n = 17). Group demographics are not available. No information on dropouts. Inclusion criteria: not specified. Exclusion criteria: not specified. |
| Interventions | 6‐week exercise programme with weekly exercise sessions followed by a home‐based programme using behaviour change strategies to promote aerobic exercise. Participants were evaluated at baseline, 7 weeks and 24 weeks. Intervention group: n = 45. Control group: n = 44. |
| Outcomes | Included in this study were: aerobic fitness (exercise test not specified); vigorous physical activity; self perception of athletic competence and physical appearance. |
| Notes | We plan to contact the authors to obtain the CF‐specific data. |
Lorenc 2015.
| Methods | Design: parallel RCT; single centre comparative effectiveness trial at the Royal Brompton Hospital, London, UK. Phase 2 study. |
| Participants | 72 participants with CF aged over 6 years from the Royal Brompton Hospital, London. Group demographics are not available. Inclusion criteria: not specified. Exclusion criteria: not specified. |
| Interventions | Phase 2 study. Group 1: 8x one‐on‐one Tai Chi sessions then given a DVD and a handout to use at home for 9 months and encouraged to practice up to 5 times per week. Group 2: no treatment (standard care) for the first 3 months (this is the control), then 8x online Tai Chi sessions (e.g. via Skype) and given a DVD and a handout to use at home for 6 months and again encouraged to practice up to 5 times per week. The programme was evaluated at baseline and after 3, 6 and 9 months. |
| Outcomes | Included in this study were: HRQoL; mindfulness, sleep (not specified); medical data (not specified) and respiratory function (not specified); participants' experience; Tai Chi feasibility; perceived health impact and study participation. |
| Notes | We plan to contact the authors to obtain more information on study design and results. |
Mandrusiak 2011.
| Methods | Design: parallel RCT, 10 ‐ 14 day inpatient period at a tertiary hospital followed by a 8 ‐ 12 week home‐based program. Blinded assessor. |
| Participants | 31 participants with CF aged 8.5 to 17.6 years and with a mean FEV1 of 66.74 %. Group demographics Group 1: exercise program (n = 15). Group 2: standard physiotherapy exercise (n = 16). Inclusion criteria: not specified. Exclusion criteria: not specified. |
| Interventions |
Group 1 (n = 15): a novel exercise program including a portable exercise package (FitKit™ ‐ exercise in a bag including instruction cards, exercise equipment and daily exercise log). Group 2 (n = 16): standard physiotherapy exercise practice. |
| Outcomes | Performance on study measures (scoped within the framework of the International Classification of Functioning, Disability and Health model) ‐ details not reported. Assessment at 3 time points:
|
| Notes | No data available currently, but will be added when study published in full. |
NCT00609050.
| Methods | Design: cross‐over RCT; single blind (outcome assessor); 6 months duration; single‐centre study at Children's Hospital of Pittsburgh, USA. |
| Participants | Enrolment goal: 38 participants with CF. Inclusion criteria: CF diagnosis; males and females; age 10 ‐ 18 years; reliable pulmonary function test; living at home; able to read; able to ride a stationary bike; able to walk and/pr run on a treadmill. Exclusion criteria: enrolled in another intervention study; participation in structured aerobic exercise for 30 continuous minutes 3 times per week; sibling enrolled in study. |
| Interventions |
Intervention group: home‐based exercise programme at least 3 times per week for 6 months with telephone reinforcement. After the first 6 months, participants receive instructions to maintain their self‐regulated exercise activity for another 6 months without receiving telephone calls. Control group: standard recommendations for exercise activity during the first 6 months. Thereafter, the control group will cross over to the self‐regulated exercise without telephone reinforcement. |
| Outcomes | Included in this study were: VO2 peak; peak workload; VO2 150 (VO2 at a heart rate of 150 bpm per minute during an exercise test); FEV1; sustained phonation time; HRQoL (CF questionnaire and well‐being scale) and exercise experiences of children and parents assessed with interviews. |
| Notes | A 6‐month program of self‐regulated, home‐based exercise programme with telephone reinforcement on cardiorespiratory fitness, pulmonary function and HRQoL of children with CF, compared to controls. A secondary aim is to exploring the exercise experiences of the children and parents. The principal investigator confirmed that the trial is completed and data are currently being analyzed. |
NCT00792194.
| Methods | Design: parallel RCT; open‐label; duration 24 months; partially‐supervised; single‐centre study at University Hospital, Strasbourg, France. |
| Participants | Enrolment goal: 50 participants with CF. Inclusion criteria: males and females aged 15 ‐ 65 years with CF diagnosed by clinical history and positive genetic or sweat testing; signed informed consent (or by parents for paediatric participants); participant covered by social security; participant has no indication of cardiac issues; stable disease (FEV1 > 1000 mL); in the case of insulin‐dependent diabetes, it must be stable; participant had been informed of the results of the medical examination; women of childbearing age confirmed not to be pregnant by urine test. Exclusion criteria: participant with unstable diabetes or known cardiac issues; participant on transplant list. |
| Interventions |
Intervention group: partially‐supervised exercise training programme with the aim of exercising 3x per week over 24 months; exercise intensity controlled with heart rate monitors and supported by exercise coaches. Control group: normal daily activities and physiotherapy regimen. |
| Outcomes | Included in this study were: VO2 peak; HRQoL (CFQ‐14+ and SF 36). |
| Notes | The principal investigator of this study responded on our request and confirmed that the study has been closed prematurely due to local organisational and recruitment problems. No publication is planned for this study. |
NCT02552043.
| Methods | Design: parallel RCT; duration 6 weeks; open‐label; single‐centre study at Universidad Autonoma de Madrid, Spain. |
| Participants | Enrolment goal: 41 participants with CF. Inclusion criteria: males and females aged 7‐18 years diagnosed with CF; clinically stable with no exacerbations of the disease in the previous 6 weeks to the inclusion date. Exclusion criteria: clinical evidence of cardiovascular, neuromuscular or osteo‐articular co‐morbidities that limit the participation in exercise programmes; lung transplant candidates and participants that followed any kind of rehabilitation programme 12 months before the study. |
| Interventions |
Intervention group: 30 ‐ 60 min exercise using a Nintendo Wii platform with the game EA SPORTS ACTIVE 2, 5 days/week for 6 weeks. The exercise activities are loaded into each participant's console during the clinical interview and the exercises adjusted according to their age: <12 years and >13 years. The program consists of 6 different workouts (1st and 2nd weeks: legs exercises; 3rd week: upper limb exercises; 4th week: thorax exercises; 5th and 6th weeks: cardio exercises) with gradually increasing intensities reaching the maximum load at the end of the training. Control group: routine clinical management. |
| Outcomes | Included in this study were: exercise capacity (6MWT; modified shuttle walk test); muscular strength (horizontal jump test, medicine ball throw, handgrip strength); HRQoL using 3 versions of the CFQ‐R (CFQ‐R 6‐11, CFQ‐R 14+, CFQ‐R Parents). |
| Notes | The aim of this study is to evaluate the efficacy of a long‐term domiciliary exercise program using the Wii video game platform as a training modality in people with CF. |
NCT03100214.
| Methods | Design: parallel RCT; outcome assessor (exercise supervisor) blinded; single‐centre study at Hospital de Clínicas de Porto Alegre, Brazil. |
| Participants | Estimated enrolment: 68 participants with CF. Inclusion criteria: males and females age 16 ‐ 50 years, diagnosed with CF according to consensus criteria and regularly followed up in the Hospital de Clinicas de Porto Alegre Programme for Adolescents and Adults with CF; admitted to hospital (for at least 24 hours) due to exacerbation of lung disease. Exclusion criteria: participants with cardiac, orthopedic or trauma complications that make it impossible to perform the proposed exercises; pregnancy; participants with haemodynamic instability, massive haemoptysis, pneumothorax, and continuous use of non‐invasive ventilation. |
| Interventions |
Intervention group: aerobic and anaerobic exercise 5 times a week during the hospitalisation period, with sessions lasting about an hour, programme beginning within 48 hours of admission. Control group: physiotherapeutic follow‐up (including respiratory physiotherapy, inhalation therapy and techniques for removal of secretions) performed by the physiotherapist of the programme for adults with CF during the hospitalisation period. |
| Outcomes | Included in this study were: primary outcome: 6MWT distance; secondary outcomes: FEV1; HRQoL (CFQ‐R); C‐reactive protein; interleukin‐6; interleukin‐8 and tumor necrosis factor. |
| Notes | This study study aims to evaluate the effects of an early rehabilitation programme based on aerobic training and muscle strength training in adolescent and adult participants with CF hospitalised at Hospital de Clinicas de Porto Alegre for exacerbation of lung disease. |
NCT03109912.
| Methods | Design: parallel RCT ("Do More, B'More, Live Fit"), duration 6 months; single‐centre study at Johns Hopkins University, Baltimore, US. |
| Participants | Enrollment goal: 60 participants with CF. Inclusion criteria: males and females aged 12 ‐ 21 years old with CF and cared for at Johns Hopkins; participants must have a smartphone and/or computer with universal serial bus (USB) to set‐up FitBit Flex. Exclusion criteria: FEV1 < 40% predicted; individuals already participating in vigorous physical activity (as assessed by the study team) in year‐round organised sports and/or aerobic exercise for longer than 30 minutes more than 5x per weeks may or may not be included in this study at the discretion of the principal investigator and study team. |
| Interventions |
Intervention group: at baseline assessment participants given individualised exercise prescriptions with the aim of achieving 30‐minutes of an endurance‐style exercise (team sports, walking, jump roping, stair climbing or more complex Tabata‐style workouts) 5 times/week for 6 months. At 4‐6 weeks and 8‐10 weeks post‐enrolment, participants attend a follow‐up 30‐minute session which will vary based on initial assessment and previous exercise prescription success, but will include strength training for major muscles groups and/or flexibility exercises with yoga as well as reinforcement of previously learned techniques with additional individualised recommendations. Participants will also receive motivational messages starting 14 days after enrolment via preferred contact method (SMS, telephone call and/or email) every 3‐4 days over the 6‐month study period. Participants also given access to "Do More, B'More, Live Fit" web page which includes spotlighted exercises, instructional exercise photos and videos; also invited to join the "Do More, B'More, Live Fit" Activity Group via the FitBit Dashboard and to friend the study team members and other exercise‐intervention participants in order to take part in FitBit step‐goal challenges. Control group: at baseline assessment, the FitBit daily step goal is set at the manufacturer standard 10,000 steps. At routine clinic visits, baseline and follow‐up assessments (3 and 6 month clinic visits) participants given generic, non‐personalised encouragement and recommendations (if requested by the participant) for physical activity. At the 3‐ and 6‐month visits, exercise is reinforced with generic encouragement, export FitBit data and review any missing data concerning for equipment failure or user error. |
| Outcomes | Included in this study were: Primary outcomes: LCI (LCI 2.5 and LCI 5.0); daily activity via FitBit step count and daily step count (mean, median and highest daily) recorded through participant FitBit flex. Secondary outcomes: FEV1 % predicted; self‐reported physical activity (Habitual Activity estimation Scale); HRQoL (CFQ‐R); exercise capacity (modified shuttle walk test); acceptability and feasibility of the programme using semi‐structured interviews. |
| Notes | This study evaluates the "Do More, B'More, Live Fit", a 6‐month fitness programme designed to optimise exercise habits of participants with CF through structured exercises with personalised coaching, exercise equipment including the FitBit Flex, online support and motivational messages delivered electronically. The intervention incorporates fitness preferences and encompasses endurance, strength and flexibility exercises while adjusting to physical fitness needs. The hypothesis is that intervention participants will have increased and sustained engagement and better health outcomes compared to control group participants. |
Oliveira 2010.
| Methods | Design: parallel, prospective controlled clinical study; single‐centre study; not clear from the abstract whether participants were randomly allocated to different interventions. |
| Participants | 20 participants with CF, mean age 13.21 years. Intervention group: n = 10. Control group: n = 10. Inclusion criteria: not specified Exclusion criteria: not specified. |
| Interventions |
Group 1: physical training at a private clinic and physiotherapy clinic. Group 2: no physical training. |
| Outcomes | Included in this study were: lung function (not specified), 3‐minute step test, maximum exertion test (not specified), collection of blood samples and a quality of life questionnaire. |
| Notes | Unclear whether this is a RCT. We contacted one author of the abstract, but have not received a reply to date. No information available in the abstract about types of exercises, intensity, frequency and duration of exercise training. |
Phillips 2008.
| Methods | Design: parallel RCT. |
| Participants | 35 participants aged 8 ‐ 21 years with an FEV1 < 60%, who were admitted for a ≥ 10 day hospitalisation for a CF exacerbation. 29 participants, mean (SD) age 15 (3.5) years, completed the study; 4 dropouts were recorded. Inclusion criteria: not specified. Exclusion criteria: not specified. |
| Interventions | Training for PT management of a CF exacerbation during an inpatient hospital stay. Group 1: standardized moderate‐to‐high intensity resistance and aerobic training consisting of 1 hour of resistance training and flexibility training 3 days per week and 20 ‐ 30 min of aerobic and balance training 2 days per week. Group 2: current standard of care which included 20 ‐ 30 min of variable intensity aerobic training 5 days per week. |
| Outcomes | MST and multiple measures of peripheral muscle performance at admission and discharge. Adverse effects. |
| Notes | Study completed in 2008. |
CF: cystic fibrosis CFQ‐R: cystic fibrosis questionnaire ‐ revised FEF25‐75: mid forced expiratory flow FEV1: forced expiratory volume FVC: forced vital capacity HRQoL: health‐related quality of life MST: modified shuttle test PT: physical therapy RCT: randomised controlled trial SD: standard deviation VO2 max: maximum oxygen consumption 6MWT: 6‐minute walk test
Characteristics of ongoing studies [ordered by study ID]
Donadio 2017.
| Trial name or title | Effect of exercise orientations in the posture and plantar pressure distribution in children and adolescents with cystic fibrosis. |
| Methods | RCT (open‐label). Design: parallel (2 arms). Duration: 3 months. |
| Participants | Target sample size: 34 Inclusion criteria: diagnosis of CF, clinically stable disease and regular follow‐up at the CF outpatient clinic. Exclusion criteria: children and adolescents with comprehension deficits and/or who present arms/legs problems that would make it impossible to perform the tests. Age minimum: 6 years. Age maximum: 20 years. |
| Interventions |
Intervention group (n = 17): participants will receive a written manual with orientations regarding physical activity, including weekly frequency. The manual contains physical activities and stretching orientations and participants are advised to perform their favourite exercise modality with a minimal frequency of 3 times per week, during 40 minutes. The manual also contains a calendar where the participant will mark the days when activities were performed. Control group (n = 17): participants will keep with their regular routine care orientations. |
| Outcomes |
Primary outcome General posture improvement: measured by the number of degrees obtained for kyphosis, lordosis, head position and chest size, using a specific software. Secondary outcomes Change in balance (measured using a baropodometer). Lung function using spirometry (FEV1). |
| Starting date | Date of first enrolment; 01 November 2013. Recruitment completed. |
| Contact information | Márcio Vinícius Fagundes Donadio (mdonadio@pucrs.br) ‐ União Brasileira de Educação e Assistência ‐ Porto Alegre, RS, Brazil |
| Notes |
Gupta 2017.
| Trial name or title | Effects of exercise intervention program on bone mineral accretion in children and adolescents with cystic fibrosis. |
| Methods | RCT (stratified block randomization, allocation concealed using sequentially numbered, sealed, opaque envelopes, open label). Design: parallel. Single centre. Duration: 1 year. |
| Participants | Total sample size: 30. Inclusion criteria: children with confirmed diagnosis of CF (sweat chloride ≥ 60 mEq/l on 2 or more occasions in a child with clinical features suggestive of CF), stable medical condition (not required IV antibiotics for last 1 month prior to enrolment), FEV1 ≥ 20%. Exclusion criteria: children unwilling to participate in the study; presence of any prior diagnosed musculoskeletal disorder such as rheumatoid arthritis, muscular dystrophy, chronic renal failure. Age minimum: 6 years. Age maximum: 18 years. Gender: both. |
| Interventions | Intervention group: exercise program ‐ resistance exercise and plyometric jumping exercise, 1x daily, 3x a week for 1 year. Control group: no exercise program, continue with regular physical activity for 1 year. |
| Outcomes |
Primary outcome Mean bone mineral density at 1 year. Secondary outcomes Lung function (FEV1 and FVC) at baseline, 3 months, 6 months, 9 months and at the end of 1 year. Exercise capacity at baseline and at the end of 1 year. CFQ‐R at baseline and at the end of year. |
| Starting date | Date of first enrolment: 08 September 2012. |
| Contact information | Sumita Gupta (Physiotherapist) All India Institute of Medical Sciences, Department of Pediatrics, AIIMS, Ansari Nagar,New Delhi, DELHI 110029, India. Email sumitabisoi@gmail.com Professor SK Kabra Department of Pediatrics, AIIMS, Ansari Nagar,New Delhi, DELHI 110029, India. Email: skkabra@hotmail.com |
| Notes |
Hebestreit 2016.
| Trial name or title | Effects of a Partially Supervised Conditioning Program in CF (ACTIVATE‐CF, NCT01744561) |
| Methods | Design: parallel RCT; duration 12 months; international, multicentre study. |
| Participants | A total of 292 participants will be recruited. Inclusion criteria: males and females aged 12 years and older with a confirmed diagnosis of CF; FEV1 ≥ 35% predicted and access to Internet. Exclusion criteria: participation in another clinical trial up to 4 weeks prior to the first baseline visit; pregnancy or breast feeding; inability to exercise; more than 4 hours of reported strenuous physical activities per week currently or up to 3 months prior to baseline measurements and not already planned within the coming 6 months; unstable condition precluding exercise (major haemoptysis or pneumothorax within the last 3 months, acute exacerbation and IV antibiotics during the last 4 weeks, planned surgery, listed for lung transplantation, major musculoskeletal injuries such as fractures or sprains during the last 2 months, others according to the impression of the doctor); cardiac arrhythmias with exercise; requiring additional oxygen with exercise; recent diagnosis of diabetes 3 months prior to screening or at screening; recent changes in medication 1 month or less prior to screening (systemic steroids, ibuprofen, inhaled antibiotics, mannitol, DNAse, hypertonic saline); at least one G551D mutation and not on ivacaftor (VX770) yet but planned start or planned stop of ivacaftor during the trial and colonization with Burkholderia cenocepacia. |
| Interventions |
Intervention group: addition of 3 hours of intense physical activities per week to baseline activities. Weekly exercise should include at least 30 min of strength building activities and at least 2 hours of aerobic activities. Exercise bouts lasting 20 min or longer will be counted with respect to total weekly training time. Participants are given exercise counselling to boost motivation towards an active lifestyle, strategies include face‐to‐face information, motivational interviewing, clear goal settings, a written "activity contract" with specific information on which activities are scheduled for which day and for how long, a pedometer, a web‐based activity diary (www.activate‐cf.org) providing feedback on missing time in intense activities to reach the weekly goal, and repeated counselling via telephone contacts and during clinic visits. A full manual describing the intervention and all intervention materials including the website are available in four languages: Dutch, English, French, and German. Control group: the control group is requested to their keep activity level constant. |
| Outcomes |
Primary outcome: FEV1 % predicted (change from baseline to 6 months) Secondary outcomes: VO2 peak (% predicted change from baseline to 6 months and baseline to 12 months); maximal aerobic power (% predicted change from baseline to 6 months and baseline to 12 months); steps per day (change from baseline to 6 months and baseline to 12 months); exercise steps per day (change from baseline to 6 months and baseline to 12 months); self‐reported physical activity (baseline to 6 months and baseline to 12 months); FEV1 (% predicted, change from 6 months to 12 months and baseline to 12 months); FVC (% predicted, change from baseline to 6 months and baseline to 12 months); residual volume in % of total lung capacity (change from baseline to 6 months and baseline to 12 months); time to first exacerbation (baseline to 6 months and baseline to 12 months); number of upper respiratory tract infections from diary (baseline to 6 months and baseline to 12 months); days on additional oral or IV antibiotics from questionnaire (baseline to 6 months and baseline to 12 months); body mass index (baseline to 6 months and baseline to 12 months); muscle mass (baseline to 6 estimated from skinfold thickness (baseline to 6 months and baseline to 12 months); body fat estimated from skinfold thickness (baseline to 6 months and baseline to 12 months); HRQoL (CFQ‐R, baseline to 6 months and baseline to 12 months); depression, anxiety and stress scores from Depression Anxiety Stress Scales (baseline to 6 months and baseline to 12 months); plasma glucose concentrations 1 and 2 hours after a standardised glucose load (standardised oral glucose tolerance test only for participants without CF‐related diabetes mellitus (baseline to 9 months); adverse events possibly or likely related to exercise (causality as judged by investigator, baseline to 6 months and baseline to 12 months); severe adverse events and serious adverse events (baseline to 6 months and baseline to 12 months). Other outcome measures: compliance with the exercise goal based on questionnaire and diary (baseline to 6 months and baseline to 12 months); lung clearance index based on nitrogen multiple breath washout, in selected centres only (baseline to 6 months and baseline to 12 months); time spent in moderate‐and‐vigorous physical activity based on accelerometry, in selected centres only (baseline to 6 months and baseline to 12 months); bone mineral density and body composition based on dual energy x‐ray absorptiometry, in selected centres only (baseline to 6 months and baseline to 12 months); mucociliary clearance with exercise based on nuclear medicine scans, US centres only (baseline to 6 months). |
| Starting date | July 2014 |
| Contact information | Prof. Dr. Helge U Hebestreit Telephone: +49 931 201 22 728 E‐mail: hebstreit@uni‐wuerzburg.de |
| Notes | ACTIVATE‐CF is an international, multicentre, randomised controlled trial to assess the effects of additional intense physical activity on a variety of outcomes. A combination of several strategies is used to boost motivation towards an active lifestyle. The primary objective of this study is to evaluate the effects of a 12‐months partially supervised exercise intervention along with regular motivation on FEV1 in a large international group of people with CF. |
NCT02700243.
| Trial name or title | Increase Tolerance for Exercise and Raise Activity Through Connectedness Trial (INTERACT) |
| Methods | Design: parallel RCT, single‐centre study at Boston Children’s Hospital, USA. |
| Participants | Enrolment goal: 80 participants with CF. Inclusion criteria: males and females aged 18 years and older with a confirmed diagnosis of CF; able to complete at least level 1 of the baseline exercise fitness test; participants must not have required IV antibiotics for a CF exacerbation within 30 days of starting the study. Exclusion criteria: pregnancy at enrolment; a history of CF exacerbation requiring IV antibiotics with the last month; use of a fitness tracker or similar product with 6 months of enrolment. |
| Interventions |
Intervention group: given a Fitbit and followed for 1 year, completing surveys and exercise tests. Control group: usual care for 1 year, then offered a Fitbit in the 2nd year. Followed to assess use of Fitbit and health outcomes. |
| Outcomes | Included in this study were: Primary outcome: submaximal exercise capacity (graded exercise test: 2 years at enrolment, 6 months, 12 months, 24 months) Secondary outcomes: Fitbit activity data (2 years); self‐reported physical activity (Habitual Activity Estimation Scale, 2 years); FEV1 relative change (% predicted, 2 years); FEV1 from before study (baseline, to each data collection time point, and from one data collection time point to the next); FVC relative change (% predicted, 2 years); FVC from before study (baseline, to each data collection time point, and from one data collection time point to the next); FEF25‐75 relative change (% predicted, 2 years; FEF25‐75 from before study (baseline, to each data collection time point, and from one data collection time point to the next); incidence of exacerbations requiring IV antibiotics (2 years); body mass index (2 years); HRQoL (CFQ‐R, 2 years); overall qualitative assessment of participant’s satisfaction with the Fitbit (2 years; 6‐month time point); overall qualitative assessment of participant's potential barriers to Fitbit use (2 years, 6‐month time point); qualitative data obtained by open‐ended interview; depression (PHQ9, 2 years: enrolment, 6 months, 12 months, 18 months, 24 months); anxiety (GAD‐7, 2 years: enrolment, 6 months, 12 months, 18 months, 24 months). |
| Starting date | March 14, 2016 |
| Contact information | Ahmet Uluer, Director, Adult Cystic Fibrosis Program, Boston Children's Hospital. |
| Notes | The aim of this study is to evaluate whether the use of a Fitbit device and an exercise prescription is associated with increased daily activity and in turn increased exercise tolerance in young adult patients with cystic fibrosis (CF). The investigators hypothesize that use of the Fitbit and an exercise prescription will be associated with increased exercise tolerance compared to standard counselling and an exercise prescription alone. |
CES‐D scale: Centre for Epidemiological Studies ‐ Depression scale CF: cystic fibrosis CFQ‐R: Cystic Fibrosis Questionnaire‐Revised FEV1: forced expiratory volume in 1 second FVC: forced vital capacity HADS: Hospital Anxiety and Depression Scale HAES: Habitual Activity Estimation Scale IV: intravenous MST: modified shuttle test PSQI: Pittsburgh Sleep Quality Index RCT: randomised controlled trial
Differences between protocol and review
Post hoc changes for the 2017 update
Summary of findings tables have been added in line with Cochrane guidance.
It was stipulated that the duration of each included study duration should be at least two weeks, which is the typical length of (drug) treatment for pulmonary exacerbations where people with CF may also take part in in‐hospital exercise training. Moreover, from an exercise physiology perspective, less than two weeks of structured exercise are unlikely to elicit meaningful changes in the chosen outcomes measures.
We added the lung clearance index (LCI) derived from multiple‐breath washout to secondary outcomes "4. Additional indices of pulmonary function and respiratory muscle strength". The LCI is a relatively new and much examined pulmonary function outcome measure and included in many clinical studies including exercise training interventions.
We also added the diffusing capacity for carbon monoxide (DLCO) and the diffusing capacity for nitric oxide (DLNO) to secondary outcomes "4. Additional indices of pulmonary function and respiratory muscle strength". Non‐invasive measurement of the pulmonary diffusing capacity can provide novel physiological insights into the exercise training effects on pulmonary function beyond the much examined FEV1, derived from spirometry.
Post hoc changes for the 2015 update
The title of the review has been changed from 'Physical training for cystic fibrosis' to 'Physical exercise training for cystic fibrosis' as the new team felt this better reflected the content of the review.
The fourth primary outcome 'mortality' was moved to secondary outcomes in line with Cochrane guidance to limit the number of primary outcomes to three. For this update, primary and secondary outcome measures were changed as follows:
Primary outcomes
We limited the primary outcome measures to:
Exercise capacity by peak oxygen uptake (VO2 peak)
Pulmonary function by forced expiratory volume in one second (FEV1)
Health‐related quality of life (HRQoL).
In CF, VO2 peak and FEV1 are strong predictors of mortality, objectively measurable and are often used as primary outcomes in studies of physical exercise training. The outcome measure HRQoL is important participant‐reported outcome measure and is related to physical fitness in people with CF. None of the other primary outcomes from previous reviews has been shown to be of predictive value in CF and they should be considered explorative endpoints. All previous primary outcomes for pulmonary function are now integrated under the secondary outcome number 4 "Additional indices of pulmonary function and respiratory muscle strength" and exercise capacity variables including effort, oxygenation and fatigue are integrated into the secondary outcome number 3 " Additional indices of exercise capacity".
Secondary outcomes We removed the secondary outcomes "Symptom scores", "Compliance with other treatment, such as chest physiotherapy, nutritional regimens" and "Cost evaluation". These outcomes are of unclear relevance, difficult to measure reliably and are rarely reported in physical training studies. We added the secondary outcome "Physical activity" because it is an important outcome in exercise training studies. The outcome "Measures of bone mineral density and diabetic control" was separated into "Bone health" and "Diabetic control" because these outcomes are unrelated and should be studied and reported separately. The outcome "Weight" was removed as a separate outcome and is now integrated within the outcome "Body composition" which comprises all measures of nutrition including body weight, body fat and fat‐free mass. The secondary outcome "Number of acute exacerbations, intravenous antibiotic courses and time off work or school" was separated as "Acute exacerbations (a) number of exacerbations; (b) time to first exacerbation" and "Antibiotic use (including oral, intravenous or inhaled antibiotics)".
Contributions of authors
The title for the protocol was conceived by the Cochrane Cystic Fibrosis and Genetic Disorders Group.
Both Judy Bradley and Fidelma Moran designed and assisted in writing the protocol and produced the earlier versions of the full review. For updates from 2015, Thomas Radtke and Susi Kriemler were responsible for acquisition of data, analysis and interpretation of data, drafting and critical revision of the manuscript. Sarah Nolan provided statistical support for the 2015 update. All authors provided intellectual input, critically reviewed the manuscript and approved the final version of this updated review.
Thomas Radtke acts as guarantor for this review.
Sources of support
Internal sources
No sources of support supplied
External sources
-
National Institute for Health Research, UK.
This systematic review was supported by the National Institute for Health Research, via Cochrane infrastructure funding to the Cochrane Cystic Fibrosis and Genetic Disorders Group.
Declarations of interest
HH has received financial compensation for travel and accomodation or free meeting participation (or both) at the European Cystic Fibrosis Society conference and the North American Cystic Fibrosis Conference for chairing or presenting at sessions focusing on exercise in cystic fibrosis. For writing an educational booklet on exercise in cystic fibrosis, HH has received money from Novartis. HH is also the lead investigator on one of the studies included in the review (Hebestreit 2010). As he is the lead investigator of the international multicentre trial ACTIVATE‐CF (Hebestreit 2016), his institution has received grants from the Mukoviszidose e.V. and a Vertex Innovation Award.
TR belongs to the core study team of the ACTIVATE‐CF trial (Hebestreit 2016). TR has also received financial compensation for chairing and presenting at exercise sessions at the European Cystic Fibrosis Society conference. He has also received financial support (travel, accomodation) from Vifor Pharma Switzerland to participate at the European Cystic Fibrosis Society and European Respiratory Society conference.
SK is the lead investigator on one of the studies included in the review (Kriemler 2013) and also belongs to the core study team of the ACTIVATE‐CF trial (Hebestreit 2016)
SJN declares no known potential conflicts of interest.
Edited (no change to conclusions)
References
References to studies included in this review
Beaudoin 2017 {published data only}
- Beaudoin N, Bouvet GF, Coriati A, Rabasa‐Lhoret R, Berthiaume Y. Combined exercise training improves glycemic control in adults with cystic fibrosis. Medicine and Science in Sports and Exercise 2016:Supplemental digital content. [CFGD Register: CO62c; CRS: 5500135000001618] [DOI] [PubMed] [Google Scholar]
- Beaudoin N, Bouvet GF, Coriati A, Rabasa‐Lhoret R, Berthiaume Y. Combined exercise training improves glycemic control in adults with cystic fibrosis. Medicine and Science in Sports and Exercise 2017;49(2):231‐7. [CENTRAL: 1199954; CFGD Register: CO62b; CRS: 5500135000001617; PUBMED: 27669451] [DOI] [PubMed] [Google Scholar]
- Beaudoin N, Bouvet GF, Rabasa‐Lhoret R, Berthiaume Y. Effects of a partially supervised combined exercise program on glycemic control in cystic fibrosis: pilot study. Pediatric Pulmonology 2015;50 Suppl 41:367. [Abstract no: 466; CENTRAL: 1092169; CFGD Register: CO62a; CRS: 5500135000001365; EMBASE: 72081745] [Google Scholar]
Cerny 1989 {published data only}
- Cerny FJ. Relative effects of bronchial drainage and exercise for in‐hospital care of patients with cystic fibrosis. Physical Therapy 1989;69(8):633‐9. [CFGD Register: PE13] [DOI] [PubMed] [Google Scholar]
Douglas 2015 {published data only}
- Douglas H, Ledger S, Main E, Sarria Jaramillo L, Rayner P, Goldman A, et al. INSPIRE‐CF: An interim review of participation of children with cystic fibrosis randomised to a weekly supervised exercise intervention. Journal of Cystic Fibrosis 2015;14 Suppl 1:S97. [Abstract no: 152; CENTRAL: 1081484; CFGD Register: PE218a; CRS: 5500135000000025; EMBASE: 71951805] [Google Scholar]
- Ledger SJ, Douglas H, Sarria Jaramillo L, Rayner P, Aurora P, Main E. INSPIRE‐CF: levels of participation of children with cystic fibrosis randomised to a 24‐month weekly supervised exercise intervention. Journal of Cystic Fibrosis 2016;15 Suppl 1:S44. [Abstract no: ePS04.5; CFGD Register: PE218b; CRS: 5500135000001550; EMBASE: 614323554] [Google Scholar]
- Ledger SJ, Wade A, Douglas H, Sarria Jaramillo L, Rayner P, Goldman A, et al. Interim results for INSPIRE‐CF: A 24‐month randomised trial evaluating effects of a weekly exercise intervention for children with cystic fibrosis. Journal of Cystic Fibrosis : Official Journal of the European Cystic Fibrosis Society 2016;15 Suppl 1:S88. [Abstract no: 144; CENTRAL: 1171475; CFGD Register: PE218c; CRS: 5500135000001590; EMBASE: 614323655] [Google Scholar]
Hebestreit 2010 {published data only}
- Hebestreit A, Kriemler S, Kieser S, Junge S, Heilmann M, Ballmann M, et al. Effects of different conditioning programmes on aerobic capacity in CF [abstract]. Pediatric Pulmonology 2003;36(Suppl 25):329. [CFGD Register: PE145a] [Google Scholar]
- Hebestreit H, Kieser S, Junge S, Ballmann M, Hebestreit A, Schindler C, et al. Long‐term effects of a partially supervised conditioning programme in cystic fibrosis. European Respiratory Journal 2010;35(3):578‐83. [CFGD Register: PE145b] [DOI] [PubMed] [Google Scholar]
- Hebestreit H, Schmid K, Kieser S, Junge S, Ballmann M, Roth K, et al. Quality of life is associated with physical activity and fitness in cystic fibrosis. BMC Pulmonary Medicine 2014;14:26. [CFGD Register: PE145c//PE120c] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hommerding 2015 {published data only}
- Hommerding PX, Baptista RR, Makarewicz GT, Schindel CS, Donadio MVF, Pinto LA, et al. Effects of an educational intervention of physical activity for children and adolescents with cystic fibrosis: a randomized controlled study. Respiratory Care 2015;60(1):81‐7. [CFGD Register: PE194b] [DOI] [PubMed] [Google Scholar]
- Marostica PJ, Hommerding P, Makarewicz G, Baptista R, Donadio MV. Efficacy of an educational intervention of physical activity for children and adolescents with cystic fibrosis [abstract]. Journal of Cystic Fibrosis 2012;11 Suppl 1:S36, Abstract no: WS16.6. [CFGD Register: PE194a] [DOI] [PubMed] [Google Scholar]
- Schindel CS, Hommerding PX, Melo DAS, Baptista RR, Marostica PJC, Donadio MVF. Physical exercise recommendations improve postural changes found in children and adolescents with cystic fibrosis: a randomized controlled trial. Journal of Pediatrics 2015;166(3):710‐6. [CFGD Register: PE194c] [DOI] [PubMed] [Google Scholar]
Klijn 2004 {published data only}
- Klijn PH, Oudshoorn A, Ent CK, ann der Net J, Helders PJ. Effects of anaerobic training in children with cystic fibrosis: a randomised controlled study. Chest 2004;125(4):1299‐305. [CFGD Register: PE147] [DOI] [PubMed] [Google Scholar]
Kriemler 2013 {published data only}
- Hebestreit H, Schmid K, Kieser S, Junge S, Ballmann M, Roth K, et al. Quality of life is associated with physical activity and fitness in cystic fibrosis. BMC Pulmonary Medicine 2014;14:26. [CFGD Register: PE145c//PE120c] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kriemler S, Hebestreit A, Kieser S, Bachmann M, Hebestreit H. Six months of training improves lung function and aerobic performance in CF [abstract]. Abstracts of the 24th European Cystic Fibrosis Conference 6‐9 June 2001; Vienna. 2001:P62. [CFGD Register: PE120a]
- Kriemler S, Kieser S, Junge S, Ballmann M, Hebestreit A, Schindler C, et al. Effect of supervised training on FEV1 in cystic fibrosis: A randomised controlled trial. Journal of Cystic Fibrosis 2013;12(6):714‐20. [CFGD Register: PE120b] [DOI] [PubMed] [Google Scholar]
Michel 1989 {published data only}
- Michel SH, Darbee JC, Pequignot E. Exercise, body composition and strength in cystic fibrosis [abstract]. Pediatric Pulmonology 1989;Suppl 4:116. [CFGD Register: PE40] [Google Scholar]
Moorcroft 2004 {published data only}
- Dodd ME, Moorcroft AJ, Webb AK. Improved fitness and decreased symptoms of muscle fatigue for upper and lower body following an individualised unsupervised home exercise training programme in adults with cystic fibrosis [abstract]. Pediatric Pulmonology 1998;Suppl 17:347. [CFGD Register: PE97a] [Google Scholar]
- Moorcroft AJ, Dodd ME, Morris J, Webb AK. Individualised unsupervised exercise training in adults with cystic fibrosis: a 1 year randomised controlled trial. Thorax 2004;59(12):1074‐80. [CFGD Register: PE97c] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moorcroft AJ, Dodd ME, Webb AK. Individualised home exercise training in CF ‐ a one‐year trial [abstract]. Proceedings of the XIIIth International Cystic Fibrosis Congress; 2000 June 4‐8; Stockholm, Sweden. 2000:153. [CFGD Register: PE97b]
Rovedder 2014 {published data only}
- Rovedder PM, Flores J, Ziegler B, Casarotto F, Jaques P, Baretto SS, et al. Exercise programme in patients with cystic fibrosis: A randomized controlled trial. Respiratory Medicine 2014;108(8):1134‐40. [CFGD Register: PE214] [DOI] [PubMed] [Google Scholar]
Santana‐Sosa 2012 {published data only}
- Santana‐Sosa E, Groeneveld IF, Gonzalez‐Saiz L, Lopez‐Mojares LM, Villa‐Asensi JR, Barrio Gonzalez MI, et al. Intrahospital weight and aerobic training in children with cystic fibrosis: a randomized controlled trial. Medicine and Science in Sports and Exercise 2012;44(1):2‐11. [CFGD Register: PE191] [DOI] [PubMed] [Google Scholar]
Santana‐Sosa 2014 {published data only}
- Santana‐Sosa E, Gonzalez‐Saiz L, Groeneveld IF, Villa‐Asensi JR, Barrio Gomez de Aguero MI, Fleck SJ, et al. Benefits of combining inspiratory muscle with 'whole muscle' training in children with cystic fibrosis: a randomised controlled trial. British Journal of Sports Medicine 2014;48(20):1513‐7. [CENTRAL: 874806; CFGD Register: PE201; CRS: 5500125000000097; PUBMED: 23681502] [DOI] [PubMed] [Google Scholar]
Schneiderman‐Walker 2000 {published data only}
- Papaioannou M. A randomized controlled trial of a 3‐year home exercise program in cystic fibrosis. Pediatric Physical Therapy 2001;13(2):94‐5. [CENTRAL: 1343880; CFGD Register: PE58c; CRS: 5500135000001603; PUBMED: 17053664] [PubMed] [Google Scholar]
- Reisman JJ, Schneiderman‐Walker J, Corey M, Wilkes D, Pedder L, Levison H, et al. The role of an organized exercise program in cystic fibrosis ‐ A three year study [abstract]. Pediatric Pulmonology 1995;Suppl 12:261. [CENTRAL: 291537; CFGD Register: PE58a; CRS: 5500100000001555] [Google Scholar]
- Schneiderman‐Walker J, Pollock SL, Corey M, Wilkes DD, Canny G, Pedder L, et al. A randomised controlled trial of a 3‐year home exercise program in cystic fibrosis. Journal of Pediatrics 2000;136(3):304‐10. [CFGD Register: PE58b] [DOI] [PubMed] [Google Scholar]
Selvadurai 2002 {published data only}
- Selvadurai HC, Blimkie CJ, Meyers N, MellisCM, Cooper PJ, Asperen PP. Randomized controlled study of in‐hospital exercise training programs in children with cystic fibrosis. Pediatric Pulmonology 2002;33(3):194‐200. [CFGD Register: PE107b] [DOI] [PubMed] [Google Scholar]
- Selvadurai HC, Asperen PP, Cooper PJ, Mellis CM, Blimkie CJ. A randomised controlled study of in‐hospital exercise training programs in children with cystic fibrosis (CF) [abstract]. Pediatric Pulmonology 1999;Suppl 19:287‐8. [CFGD Register: PE107a] [DOI] [PubMed] [Google Scholar]
Turchetta 1991 {published data only}
- Turchetta A, Bella S, Calzolari A, Castro M, Ciuffetti C, Drago F, et al. Effect of controlled physical activity on lung function test of cystic fibrosis children [abstract]. Proceedings of the 17th European Cystic Fibrosis Conference; 1991 June 18‐21; Copenhagen. 1991:134. [CFGD Register: PE45]
References to studies excluded from this review
Alarie 2012 {published data only}
- Alarie N, Chan R, Thomas L, Marasco J, Amelie P, Nan W, et al. Cardiorespiratory responses to Nintendo Wii in children with cystic fibrosis: a pilot study [abstract]. Pediatric Pulmonology 2012;47(S35):367, Abstract no: 399. [CFGD Register: PE196] [Google Scholar]
Albinni 2004 {published data only}
- Albinni S, Rath R, Renner S, Eichler I. Additional inspiratory muscle training intensifies the beneficial effects of cycle ergometer training in patients with cystic fibrosis [abstract]. Journal of Cystic Fibrosis 2004;3(Suppl 1):S63. [Google Scholar]
- Eichler I, Renner S, Albinni S, Nachbaur E, Rath R. Inspiratory muscle training adds beneficial effects to cycle ergometer training in patients with cystic fibrosis [abstract]. Pediatric Pulmonology 2005;40(Suppl 28):320. [Google Scholar]
Amelina 2006 {published data only}
- Amelina E, Cherniak A, Chikina S, Krasovsky S, Appaeva A. Inspiratory muscle training (IMT) in cystic fibrosis adults [abstract]. Proceedings of European Respiratory Society Annual Congress; 2006 Sep 2‐6; Munich, Germany. 2006. [Abstract no: P4112; CFGD Register: PE177a]
- Cherniak A, Amelina E, Krasovsky S, Nekludova G, Chikina S. The effect of high intensity inspiratory muscle training in adults with cystic fibrosis (CF). European Respiratory Journal 2007;30(Suppl 51):767s. [Abstract no: E4514; CENTRAL: 645383; CFGD Register: PE177b; CRS: 5500050000000531] [Google Scholar]
Andreasson 1987 {published data only}
- Andreasson B, Jonson B, Kornfalt R, Nordmark E, Sandstrom S. Long‐term effects of physical exercise on working capacity and pulmonary function in cystic fibrosis. Acta Paediatrica Scandinavica 1987;76(1):70‐5. [DOI] [PubMed] [Google Scholar]
Aquino 2006 {published data only}
- Aquino A, Balestri E, Dall Ara S, Lami I, Gobb F, Ambroni M, Miano A. Efficacy of physical exercise playing a video game for mucus clearance in patients with CF [abstract]. Jounal of Cystic Fibrosis 2006;5(Suppl):S83. [Google Scholar]
Asher 1982 {published data only}
- Asher M, Pardy R, Coates A, Thomas E, Macklem PT. The effects of inspiratory muscle training in patients with cystic fibrosis [abstract]. Australian and New Zealand Journal of Medicine 1983;13:204. [CFGD Register: PE127a] [DOI] [PubMed] [Google Scholar]
- Asher MI, Pardy RL, Coates AL, Thomas E, Macklem PT. The effects of inspiratory muscle training in patients with cystic fibrosis. American Review of Respiratory Disease 1982;126(5):855‐9. [CFGD Register: PE127b] [DOI] [PubMed] [Google Scholar]
Balestri 2004 {published data only}
- Balestri E, Ambroni M, dall'Ara S, Miano A. Efficacy of physical exercise for mucus clearance in patients with cystic fibrosis (CF) [abstract]. Pediatric Pulmonology 2004;38(S27):316. [Google Scholar]
Balfour 1998 {published data only}
- Balfour Lynn IM, Prasad SA, Laverty A, Whitehead BF, Dinwiddie R. A step in the right direction: assessing exercise tolerance in cystic fibrosis. Pediatric Pulmonology 1998;25(4):278‐84. [CENTRAL: 462732; CFGD Register: PE69b; CRS: 5500100000002462] [DOI] [PubMed] [Google Scholar]
- Balfour‐Lynn IM, Prasad SA, Laverty A, Whitehead BF, Dinwiddie R. Step‐test vs 6‐minute walk: Assessing exercise tolerance in children with cystic fibrosis [abstract]. Pediatric pulmonology 1996;Suppl 13:305. [CFGD Register: PE69a] [Google Scholar]
Barry 2001 {published data only}
- Barry S, Dodd J, Jensma M, Gallagher C. Benefits of high intensity strength training in adults with cystic fibrosis [abstract]. American Journal of Respiratory and Critical Care Medicine 2001;163(5 Suppl):A968. [CFGD Register: PE133b] [Google Scholar]
- Barry S, Dodd J, Jensma M, Gallagher C. High intensity strength training improves fitness levels in adults with cystic fibrosis [abstract]. American Journal of Respiratory and Critical Care Medicine 2002;165(8 Suppl):A507. [CFGD Register: PE133a] [Google Scholar]
Bieli 2017 {published data only}
- Bieli C, Selina S, Demet I, Andreas J, Alexander M. Respiratory muscle endurance training in cystic fibrosis. European Respiratory Journal 2014;44(Suppl 58):P1972. [CFGD Register: PE237b; CRS: 5500135000001917; EMBASE: 71851116] [Google Scholar]
- Bieli C, Summermatter S, Boutellier U, Moeller A. Respiratory muscle training improves respiratory muscle endurance but not exercise tolerance in children with cystic fibrosis. Pediatric Pulmonology 2017;52(3):331‐6. [CENTRAL: 1262285; CFGD Register: PE237a; CRS: 5500135000001736; EMBASE: 614244451; PUBMED: 28114723] [DOI] [PubMed] [Google Scholar]
Bilton 1992 {published data only}
- Bilton D, Dodd M, Webb AK. The benefits of exercise combined with physiotherapy in cystic fibrosis [abstract]. Pediatric Pulmonology 1990;9(Suppl 5):238. [CFGD Register: PE41a] [Google Scholar]
- Bilton D, Dodd ME, Abbot JV, Webb AK. The benefits of exercise combined with physiotherapy in the treatment of adults with cystic fibrosis. Respiratory Medicine 1992;86(6):507‐11. [CFGD Register: PE41b] [DOI] [PubMed] [Google Scholar]
Bongers 2015 {published data only}
- Bongers BC, Werkman MS, Arets HG, Takken T, Hulzebos HJ. A possible alternative exercise test for youths with cystic fibrosis: the steep ramp test. Medicine and Science in Sports and Exercise 2015;47(3):485‐92. [CENTRAL: 1096730; CFGD Register: PE232; CRS: 5500135000001620; PUBMED: 25010405] [DOI] [PubMed] [Google Scholar]
Calik‐Kutukcu 2016 {published data only}
- Calik‐Kutukcu E, Saglam M, Vardar‐Yagli N, Cakmak A, Inal‐Ince D, Bozdemir‐Ozel C, et al. Listening to motivational music while walking elicits more positive affective response in patients with cystic fibrosis. Complementary Therapies in Clinical Practice 2016;23:52‐8. [CENTRAL: 1199953; CFGD Register: PE234; CRS: 5500135000001601; PUBMED: 27157959] [DOI] [PubMed] [Google Scholar]
Chang 2015 {published data only}
- Chang K, Cotton J, Gashgarian S, Sheppard E, Slack D, Stephenson A, et al. Vaildation of clinical assessment tools for leg muscle strength and power in adults with cystic fibrosis. Pediatric Pulmonology 2015;50 Suppl 41:368. [Abstract no: 469; CENTRAL: 1092168; CFGD Register: PE223; CRS: 5500135000001364] [Google Scholar]
Chatham 1997 {published data only}
- Chatham K, Ionescu A, Davis C, Baldwin J, Enright S, Shale DJ. Through range computer generated inspiratory muscle training in cystic fibrosis [abstract]. Pediatric Pulmonology 1997;23(Suppl 14):299. [CFGD Register: PE90] [Google Scholar]
de Jong 1994 {published data only}
- Jong W, Grevink RG, Roorda RJ, Kaptein AA, Schans CP. Effect of a home exercise training program in patients with cystic fibrosis. Chest 1994;105(2):463‐8. [DOI] [PubMed] [Google Scholar]
del Corral Nunez‐Flores 2011 {published data only}
- Corral Nunez‐Flores T, Percegona J, Seborga M, Trujillo N, Hernandez L, Rejas A, et al. Exercise physiologic response during three different video games in cystic fibrosis [abstract]. Journal of Cystic Fibrosis 2011;10 Suppl 1:S64, Abstract no: 253. [CFGD Register: PE190a] [Google Scholar]
- Corral Nunez‐Flores T, Percegona J, Seborga M, Trujillo N, Hernandez L, Rejas A, et al. Exercise physiologic response during three different video games in cystic fibrosis [abstract]. Pediatric Pulmonology 2011;46(S34):353, Abstract no: 389. [CFGD Register: PE190b] [Google Scholar]
- Corral T, Percegona J, Seborga M, Rabinovich RA, Vilaro J. Physiological response during activity programs using Wii‐based video games in patients with cystic fibrosis. Journal of Cystic Fibrosis 2014;13(6):706‐711. [CFGD Register: PE190c] [DOI] [PubMed] [Google Scholar]
- Corral T, Percegona J, Seborga M, Trujillo N, Hernandez L, Rejas A, et al. Exercise physiologic response during three different video games in cystic fibrosis patients. European Respiratory Journal 2011;38(55):878s, Abstract no: P4802. [CENTRAL: 1081933; CFGD Register: PE190d; CRS: 5500050000000474; EMBASE: 72122296] [Google Scholar]
Dwyer 2008 {published data only}
- Dwyer T, Alison J, McKeough Z, Daviskas E, Bye P. Exercise aids airway clearance by increasing respiratory flow rates and decreasing mucus viscoelasticity in CF [abstract]. Pediatric Pulmonology 2008;43 Suppl 31:386, Abstract no: 513. [CFGD Register: PE188] [Google Scholar]
Dwyer 2017 {published data only}
- Dwyer TJ, Zainuldin R, Daviskas E, Bye PT, Alison JA. Effects of treadmill exercise versus Flutter(R) on respiratory flow and sputum properties in adults with cystic fibrosis: a randomised, controlled, cross‐over trial. BMC Pulmonary Medicine 2017;17(1):14. [CFGD Register: PE239; CRS: 5500135000001880; PUBMED: 28077104] [DOI] [PMC free article] [PubMed] [Google Scholar]
Edlund 1986 {published data only}
- Adams TD, Edland LL, French RW, Herbst JJ, Ruttenberg HD, Ruhling RO. Effects of a swimming program on children with cystic fibrosis [abstract]. International Journal of Sports Medicine 1984;5:156. [CFGD Register: PE154a] [DOI] [PubMed] [Google Scholar]
- Edlund LD, French RW, Herbst JJ, Ruttenburg HD, Ruhling RO, Adams TD. Effects of a swimming program on children with cystic fibrosis. American Journal of Diseases of Children 1986;140(1):80‐3. [CFGD Register: PE154b] [DOI] [PubMed] [Google Scholar]
Falk 1988 {published data only}
- Falk M, Kelstrup M, Andersen JB, Pedersen SS, Rossing I, Dirksen H. PEP treatment or physical exercise ‐ Effects on secretions expectorated and indices of central and peripheral airway function. A controlled study [abstract]. Excerpta Medica, Asia Pacific Congress Series 1988;74:35. [CFGD Register: PE36] [Google Scholar]
Giacomodonato 2015 {published data only}
- Giacomodonato B, Graziano L, Curzi M, Perelli T, Sanctis S, Varchetta M, et al. Respiratory muscle endurance training with normocapnic hyperpnea in patients with cystic fibrosis. A randomized controlled study. Journal of Cystic Fibrosis : Official Journal of the European Cystic Fibrosis Society 2015;14 Suppl 1:S41. [Abstract no: WS21.10; CENTRAL: 1077187; CFGD Register: PE217; CRS: 5500135000000016] [Google Scholar]
Gruet 2012 {published data only}
- Gruet M, Mely L, Brisswalter J, Vallier J‐M. Neuromuscular electrical stimulation in cystic fibrosis [abstract]. Journal of Cystic Fibrosis 2012;11 Suppl 1:S109, Abstract no: 208. [CFGD Register: PE195] [Google Scholar]
Haynes 2016 {published data only}
- Haynes F, Maddison L, Millward S, Hughes T, Dewar J. Evaluation of the incremental step test with adult CF patients. Journal of Cystic Fibrosis : Official Journal of the European Cystic Fibrosis Society 2016;15 Suppl:S88. [Abstract no: 146; CENTRAL: 1171474; CFGD Register: PE233; CRS: 5500135000001589] [Google Scholar]
Heijerman 1992 {published data only}
- Heijerman HGM, Bakker W, Sterk PJ, Dijkman JH. Long‐term effects of exercise training and hyperlimentation in adult cystic fibrosis patients with severe pulmonary dysfunction. International Journal of Rehabilitation Research 1992;15(3):252‐7. [DOI] [PubMed] [Google Scholar]
Irons 2012 {published data only}
- Irons JY, Kenny D, Chang AB. Let's sing out!: The effect of singing on quality of life and lung function of children and adolescents with cystic fibrosis. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ID=83944 (accessed 10 September 2009). [CFGD Register: PE185a]
- Irons JY, Kenny DT, McElrea M, Chang AB. Singing therapy for young people with cystic fibrosis : a randomized controlled pilot study. Music and Medicine 2012;4(3):136‐45. [CENTRAL: 861294; CFGD Register: PE185b; CRS: 5500100000007892] [Google Scholar]
Kriemler 2016 {published data only}
- Kriemler S, Radtke T, Christen G, Kerstan‐Huber M, Hebestreit H. Short‐term effect of different physical exercises and physiotherapy combinations on sputum expectoration, oxygen saturation, and lung function in young patients with cystic fibrosis. Lung 2016;194(4):659‐64. [CFGD Register: PE219b; CRS: 5500135000001602; PUBMED: 27147223] [DOI] [PubMed] [Google Scholar]
- Radtke T, Christen G, Kerstan Huber M, Hebestreit H, Kriemler S. Short‐term effect of different physical exercise‐physiotherapy combinations on sputum production, oxygen saturation and lung function in young patients with cystic fibrosis. Journal of Cystic Fibrosis 2015;14 Suppl 1:S27. [Abstract no: WS14.2; CENTRAL: 1081483; CFGD Register: PE219a; CRS: 5500135000000019; EMBASE: 71951559] [Google Scholar]
Kuys 2011 {published data only}
- Hall K, Peasey M, Wood M, Cobb R, Bell S, Kuys S. The effects of nintendo‐wii exercise training in adults with cystic fibrosis. Physiotherapy (United Kingdom) 2011;97 Suppl 1:eS648. [CENTRAL: 1089274; CFGD Register: PE184c; CRS: 5500050000000475; EMBASE: 71883056] [Google Scholar]
- Hall K, Peasey M, Wood M, Cobb R, Bell SC, Kuys S. The effects of Nintendo Wii exercise training in adults with cystic fibrosis [abstract]. Journal of Cystic Fibrosis 2010;9(Suppl 1):A275. [CFGD Register: PE184a] [Google Scholar]
- Hall K, Peasey M, Wood M, Cobb R, Bell SC, Kuys S. The effects of nintendo‐wii® exercise training in adults with cystic fibrosis. Respirology (Carlton, Vic.) 2011;16(Suppl 1):P56. [Abstract no: TP 077; CFGD Register: PE184d; CRS: 5500135000001908] [Google Scholar]
- Kuys SS, Hall K, Peasey M, Wood M, Cobb R//Bell SC. Gaming console exercise and cycle or treadmill exercise provide similar cardiovascular demand in adults with cystic fibrosis: a randomised cross‐over trial. Journal of Physiotherapy 2011;57(1):35‐40. [CFGD Register: PE184b] [DOI] [PubMed] [Google Scholar]
Lannefors 1992 {published data only}
- Lannefors L, Wollmer P. Mucus clearance in cystic fibrosis (CF) ‐ a comparison between postural drainage, PEP‐mask and physical exercise [abstract]. Proceedings of the 11th International Cystic Fibrosis Congress. 1992:AHP31. [CFGD Register: PE46a] [PubMed]
- Lannefors L, Wollmerr P. Mucus clearance with three chest physiotherapy regimes in CF: a comparison between postural drainage, PEP and physical exercise. European Respiratory Journal 1992;5(6):748‐53. [CFGD Register: PE46b] [PubMed] [Google Scholar]
Lima 2014 {published data only}
- Lima C, Andrade AD, Rattes C, Campos S, Brandao D, Aliverti A, et al. Effect of noninvasive ventilation on functional exercise capacity, lung function and compartmental chest wall volume in children with cystic fibrosis. European Respiratory Journal 2013;42:1075s. [Abstract no: P5065; CENTRAL: 1099891; CFGD Register: PE216b; CRS: 5500050000000267; EMBASE: 71843506] [Google Scholar]
- Lima CA, Andrade ADFD, Campos SL, Brandao DC, Fregonezi, Mourato IP, et al. Effects of noninvasive ventilation on treadmill 6‐min walking distance and regional chest wall volumes in cystic fibrosis: randomized controlled trial. Respiratory Medicine 2014;108(10):1460‐8. [CFGD Register: PE216a] [DOI] [PubMed] [Google Scholar]
Lowman 2012 {published data only}
- Lowman JD, Britton LJ, Lee LS, Phillips AL, Hoover WC. Comprehensive exercise training during hospitalization for an acute CF exacerbation : a randomized controlled trial [abstract]. Journal of Cystic Fibrosis 2012;11 Suppl 1:S23, Abstract no: WS10.5. [CFGD Register: PE192] [Google Scholar]
NCT02277860 {published data only}
- NCT02277860. Gaming console home‐based exercise for adults with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT02277860 (first received 27 October 2014).
NCT02715921 {published data only}
- NCT02715921. Impact of telerehabilitation training on pediatric cystic fibrosis patients: an exploratory study. clinicaltrials.gov/ct2/show/NCT02715921 (first received 12 January 2016).
NCT02821130 {published data only}
- NCT02821130. Orkambi exercise study (Orkambi) [Effects of Orkambi on exertional dyspnea, exercise performance, and ventilatory responses in adults with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT02821130 (first received 06 June 2016).
NCT02875366 {published data only}
- NCT02875366. A study of the effects of lumacaftor/ivacaftor on exercise tolerance in subjects with cystic fibrosis, homozygous for the F508del‐CFTR mutation [A phase 4, randomized, double‐blind, placebo‐controlled, parallel‐design study of the effect of lumacaftor/ivacaftor combination therapy on exercise tolerance in subjects aged 12 years and older with cystic fibrosis, homozygous for the F508del‐CFTR mutation]. clinicaltrials.gov/ct2/show/NCT02875366 (first received 15 August 2016).
NCT03117764 {published data only}
- NCT03117764. Evaluation of the impact of intravenous antibiotics on muscular strength in patients with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03117764 (first received 31 March 2017).
Orenstein 1981 {published data only}
- Orenstein DM, Franklin BA, Doershuk CF, Hellerstein HK, Germann KJ, Horowitz JG, et al. Exercise conditioning and cardiopulmonary fitness in CF. The effects of a three‐month supervised running program. Chest 1981;80(4):392‐8. [CFGD Register: PE92] [DOI] [PubMed] [Google Scholar]
Orenstein 2004 {published data only}
- Orenstein DM, Hovell MF, Mulvihill M, Keating KK, Hofstetter CR, Kelsey S, et al. Strength vs aerobic training in children with cystic fibrosis: a randomised controlled trial. Chest 2004;126(4):1204‐14. [CFGD Register: PE165] [DOI] [PubMed] [Google Scholar]
Ozaydin 2010 {published data only}
- Ozaydin Z, Savci S, Saglam M, Arikan H, Inal‐Ince D, Vardar‐Yagli N, et al. Effects of inspiratory muscle training on functional capacity and muscle strength in patients with mild cystic fibrosis. European Respiratory Society Annual Congress; 2010 Sep 18‐22; Barcelona, Spain. 2010. [Abstract no: 5134; CENTRAL: 777297; CFGD Register: PE235; CRS: 5500050000000532]
Patterson 2004 {published data only}
- Patterson JE, Bradley JM. Inspiratory muscle training in adult patients with cystic fibrosis: a randomised controlled trial to evaluate the efficacy of the test of incremental respiratory endurance (TIRE). Thorax 2004;59(Suppl II):ii13. [Abstract no: S36; CENTRAL: 518434; CFGD Register: PE236; CRS: 5500050000000533] [Google Scholar]
Petrovic 2013 {published data only}
- Petrovic M, Kaluza I, Pohl W. Effects of individualised aerobic exercise training in adults with cystic fibrosis: A 4 year controlled trial [abstract]. Journal of Cystic Fibrosis 2013;12 Suppl 1:S28, Abstract no: WS14.4. [CENTRAL: 875002; CFGD Register: PE204; CRS: 5500100000011658] [Google Scholar]
Rand 2012 {published data only}
- Rand S, Hill L, Prasad SA, Main E. Development of an incremental field exercise test for children with cystic fibrosis [abstract]. Journal of Cystic Fibrosis 2012;11 Suppl 1:S36, Abstract no: WS16.7. [CFGD Register: PE193] [Google Scholar]
Reix 2012 {published data only}
- Reix P, Aubert F, Kassai B, Bige V, Bellon G. Better satisfaction of cystic fibrosis paediatric patients with autogenic drainage associated to exercise compared to conventional chest physiotherapy [abstract]. Journal of Cystic Fibrosis 2009;8 suppl 2:S73, Abstract no: 293. [CFGD Register: PE183a] [Google Scholar]
- Reix P, Aubert F, Werck‐Gallois MC, Toutain A, Mazzocchi C, Moreux N, et al. Exercise with incorporated expiratory manoeuvres was as effective as breathing techniques for airway clearance in children with cystic fibrosis: a randomised crossover trial. Journal of Physiotherapy 2012;58(4):241‐7. [CENTRAL: 841658; CFGD Register: PE183b; CRS: 5500125000000095; PUBMED: 23177226] [DOI] [PubMed] [Google Scholar]
Salh 1989 {published data only}
- Salh W, Bilton D, Dodd M, Webb AK. Effect of exercise and physiotherapy in aiding sputum expectoration in adults with cystic fibrosis. Thorax 1989;44(12):1006‐8. [CFGD Register: PE63] [DOI] [PMC free article] [PubMed] [Google Scholar]
Salonini 2015 {published data only}
- Salonini E, Gambazza S, Meneghelli I, Tridello G, Sanguanini M, Cazzarolli C, et al. Active video game playing in children and adolescents with cystic fibrosis: Exercise or just fun?. Respiratory Care 2015;60(8):1172‐9. [CENTRAL: 1161387; CFGD Register: PE207b; CRS: 5500050000000473; EMBASE: 2015465751] [DOI] [PubMed] [Google Scholar]
- Salonini E, Gambazza S, Tridello G, Sanguanini M, Cazzarolli C. Kinect active video game in cystic fibrosis: Exercise or fun? [abstract]. Journal of Cystic Fibrosis 2013;12 Suppl 1:S108, Abstract no: 233. [CENTRAL: 875196; CFGD Register: PE207; CRS: 5500100000011679] [Google Scholar]
Shaw 2016 {published data only}
- Shaw I, Kinsey JE, Richards R, Shaw BS. Individualized supervised resistance training during nebulization in adults with cystic fibrosis. Pakistan Journal of Medical Sciences 2016;32(5):1152‐7. [CENTRAL: 1343881; CFGD Register: PE242; CRS: 5500135000001737; PUBMED: 27882012] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stanghelle 1998 {published data only}
- Stanghelle JK, Hjeltnes N, Bangstad HJ, Michalsen H. Effect of daily short bouts of trampoline exercise during 8 weeks on the pulmonary function and the maximal oxygen uptake of children with cystic fibrosis. International Journal of Sports Medicine 1988;9 Suppl 1:32‐6. [CENTRAL: 568629; CFGD Register: PE155; CRS: 5500100000002860; PUBMED: 3360541] [DOI] [PubMed] [Google Scholar]
Tuzin 1998 {published data only}
- Tuzin BJ, Mulvihill MM, Kilbourn KM, Bertran DA, Buono M, Hovell MF, et al. Increasing physical activity of children with cystic fibrosis: A home based family intervention. Pediatric Exercise Science 1998;10(1):57‐68. [Google Scholar]
Vallier 2016 {published data only}
- Vallier JM, Rouissi M, Mely L, Gruet M. Physiological Responses of the Modified Shuttle Test in Adults With Cystic Fibrosis. Journal of Cardiopulmonary Rehabilitation and Prevention 2016;36(4):288‐92. [CENTRAL: 1343882; CFGD Register: PE241; CRS: 5500135000001903; PUBMED: 27182761] [DOI] [PubMed] [Google Scholar]
Vivodtzev 2013 {published data only}
- Vivodtzev I, Decorte N, Wuyam B, Gonnet N, Durieu I, Levy P, et al. Benefits of neuromuscular electrical stimulation prior to endurance training in patients with cystic fibrosis and severe pulmonary dysfunction. Chest 2013;143(2):485‐93. [CENTRAL: 906021; CFGD Register: PE201a; CRS: 5500050000000005; EMBASE: 22911373; PUBMED: 22911373] [DOI] [PubMed] [Google Scholar]
- Vivodtzev I, Decorte N, Wuyam B, Gonnet N, Durieu I, Levy P, et al. Online supplement to "Benefits of neuromuscular electrical stimulation prior to endurance training in patients with cystic fibrosis and severe pulmonary dysfunction" [online]. Chest 2013;143(2):485‐93 online. [CENTRAL: 980643; CFGD Register: PE201b; CRS: 5500125000000610] [DOI] [PubMed] [Google Scholar]
Wheatley 2015 {published data only}
- Wheatley CM, Baker SE, Morgan MA, Martinez MG, Liu B, Rowe SM, et al. Moderate intensity exercise mediates comparable increases in exhaled chloride as albuterol in individuals with cystic fibrosis. Respiratory Medicine 2015;109(8):1001‐11. [CENTRAL: 1107333; CFGD Register: PE225b; CRS: 5500050000000335; EMBASE: 2015118578] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wheatley CM, Baker SE, Morgan MA, Martinez MG, Morgan WJ, Wong EC, et al. Effects of exercise intensity compared to albuterol in individuals with cystic fibrosis. Respiratory Medicine 2015;109(4):463‐74. [CENTRAL: 1110247; CFGD Register: PE225a; CRS: 5500135000001490; PUBMED: 25749641] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
ACTRN12617001009303 {published data only}
- ACTRN12617001009303. Action: PACT. Be Active. Online. A trial to promote physical activity in young people with cystic fibrosis.. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12617001009303 (first received 06 July 2017).
Almajan 2011 {published data only}
- Almajan‐Guta B, Avram C, Almajan‐Guta V, Rusu A, Ciuca I, Cluci O, et al. High motivation for playing sports in cystic fibrosis ‐ what we play is life [abstract]. Journal of Cystic Fibrosis 2011;10 Suppl 1:S64, Abstract no: 254. [CFGD Register: PE189] [Google Scholar]
Housinger 2015 {published data only}
- Housinger E, Sullivan M, Ruiz FE. Effects of an interdisciplinary motivational incentive‐based walking program in pediatric pulmonary patients during hospitalization. Pediatric Pulmonology 2015;50 Suppl 41:369. [Abstract no: 471; CENTRAL: 1092214; CFGD Register: PE222; CRS: 5500135000001403; EMBASE: 72081750] [Google Scholar]
Johnston 2004 {published data only}
- Johnston K, Jenkins, Roberts C, Stick S. Improved attitude to exercise in overweight children with lung conditions after an exercise intervention. Respirology (Carlton, Vic.) 2004;9(2 Suppl):A60. [CENTRAL: 475664; CFGD Register: PE231; CRS: 5500050000000476] [Google Scholar]
Lorenc 2015 {published data only}
- Carr SB, Ronan P, Robinson N, Agent P, Mian A, Madge S. A randomised controlled trial of Tai Chi in cystic fibrosis. Pediatric Pulmonology 2016;51:376. [Abstract no: 480; CENTRAL: 1212611; CFGD Register: PE243c; CRS: 5500135000001919; EMBASE: 612358588] [Google Scholar]
- Lorenc A, Ronan P, Mian A, Madge S, Carr SB, Agent P, et al. Cystic fibrosis‐Children and adults Tai Chi study (CF CATS2): Can Tai Chi improve symptoms and quality of life for people with cystic fibrosis? Second phase study protocol. Chinese Journal of Integrative Medicine. China, 2015 May 26 [Epub ahead of print]. [CENTRAL: 1343883; CFGD Register: PE243a; CRS: 5500135000001904; PUBMED: 26015075] [DOI] [PubMed]
- Madge S, Ronan P, Robinson N, Agent P, Mian A, Carr SB. Assessing the benefits of tai chi in people with CF and the feasibility of delivering Tai Chi over the internet (Skype®). Pediatric Pulmonology 2016;51 Suppl 45:370. [Abstract no: 465; CENTRAL: 1343884; CFGD Register: PE243b; CRS: 5500135000001922] [Google Scholar]
Mandrusiak 2011 {published data only}
- Mandrusiak A, MacDonald J, Paratz J, Wilson C, Watter P. A novel exercise program for young people with cystic fibrosis: Moving physiotherapy forward through targeted design. Physiotherapy (United Kingdom) 2011;97:eS1550. [CENTRAL: 1076180; CFGD Register: PE229; CRS: 5500050000000415; EMBASE: 71884245; Poster no.: SI‐PO‐210‐22‐Thu] [Google Scholar]
NCT00609050 {published data only}
- NCT00609050. Exercise training study for patients with cystic fibrosis [Self‐regulated exercise in CF: a randomized trial]. clinicaltrials.gov/ct2/show/NCT00609050 (first received 31 January 2008).
NCT00792194 {published data only}
- NCT00792194. Improvement of aerobic capacity in cystic fibrosis patients with a one‐year home training period. clinicaltrials.gov/ct2/show/NCT00792194 (first received 14 November 2008).
NCT02552043 {published data only}
- NCT02552043. Video game exercise effectiveness of a domiciliary pulmonary rehabilitation program in cystic fibrosis patients. clinicaltrials.gov/ct2/show/NCT02552043 (first received 15 September 2015).
NCT03100214 {published data only}
- NCT03100214. Effects of an early rehabilitation program during hospitalization in patients with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03100214 (first received 31 January 2017).
NCT03109912 {published data only}
- NCT03109912. Do More, B'More, Live Fit [Do More, B'More, Live Fit: an outpatient fitness‐training pilot program designed to optimize the habit of exercise in adolescents and young adults with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT03109912 (first received 22 February 2017).
Oliveira 2010 {published data only}
- Oliveira ACN, Jesus TA, Mesquita‐ Ferrari RA, Oliveira JC, Oliveira LVF, Sampaio LM. Aerobic training and quality of life in cystic fibrosis. European Respiratory Journal 2010;36 Suppl 54:P2651. [CFGD Register: PE245; CRS: 5500135000001906] [Google Scholar]
Phillips 2008 {published data only}
- Phillips AL, Lee L, Britton LJ, Hoover W, Lowman JD. Efficacy of a standardised exercise protocol in inpatient care of patients with cystic fibrosis [abstract]. Pediatric Pulmonology 2008;43(Suppl 31):385, Abstract 510. [CFGD Register: PE182] [Google Scholar]
References to ongoing studies
Donadio 2017 {published data only}
- Donadio M. Effect of exercise orientations in the posture and plantar pressure distribution in children and adolescents with cystic fibrosis. apps.who.int/trialsearch/Trial2.aspx?TrialID=RBR‐3r4h5s (first received 09 July 2014).
Gupta 2017 {published data only}
Hebestreit 2016 {published data only}
- Hebestreit H. How to counsel patients regarding exercise and habitual physical activity?. Journal of Cystic Fibrosis 2016;51 Suppl 45:188. [Abstract no: S20.4; CFGD Register: PE244a; CRS: 5500135000001920] [Google Scholar]
- NCT01744561. Effects of a partially supervised conditioning program in CF (ACTIVATE‐CF) [Effects of a partially supervised conditioning program in CF: an international multi‐centre, randomized controlled trial]. clinicaltrials.gov/show/NCT01744561 (first received 05 December 2012). [CENTRAL: 1343886; CFGD Register: PE244b; CRS: 5500135000001724]
NCT02700243 {published data only}
- NCT02700243. Increase tolerance for exercise and raise activity through connectedness trial (INTERACT) [Pilot RCT study using a Fitbit device to improve exercise tolerance in 80 patients with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT02700243 (first received 21 February 2016).
Additional references
ACSM 2010
- American College of Sports Medicine. ACSM's guidelines for exercise testing prescription. 8th Edition. Philadelphia: Lippincott Williams and Williams, 2010. [Google Scholar]
Casaburi 1992
- Casaburi R. Principles of exercise training. Chest 1992;101(Suppl 5):263S‐7S. [PubMed] [Google Scholar]
Cerny 2013
- Cerny F. Exercise and cystic fibrosis (CF) 2.0. Pediatric Exercise Science 2013;25(4):616‐23. [DOI] [PubMed] [Google Scholar]
CF Foundation 2009
- Cystic Fibrosis Foundation. Patient Registry: Annual Data Report. Patient Registry: Annual Data Report. [Bethesda, Maryland], 2002. [Google Scholar]
CF Trust 2010
- Cystic Fibrosis Trust. Living with Cystic Fibrosis: Annual Review. Cystic Fibrosis Trust, 2010. [Google Scholar]
Dwyer 2011
- Dwyer TJ, Alison JA, McKeough ZJ, Daviskas E, Bye PT. Effects of exercise on respiratory flow and sputum properties in patients with cystic fibrosis. Chest 2011;139(4):870‐7. [DOI] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne DR, Altman DG, Higgins JP, Curtin F, Worthington HV, Vail A. Meta‐analyses involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [DOI] [PubMed] [Google Scholar]
Ellis 2010
- Ellis, PD. The Essential Guide to Effect Sizes: An Introduction to Statistical Power, Meta‐Analysis and the Interpretation of Research Results. United Kingdom: Cambridge University Press, 2010. [Google Scholar]
Farrell 2008
- Farrell PM. The prevalence of cystic fibrosis in the European Union. Journal of Cystic Fibrosis 2008;7(5):450‐3. [DOI] [PubMed] [Google Scholar]
Galassetti 2013
- Galassetti P, Riddell MC. Exercise and type 1 diabetes (T1DM). Comprehensive Physiology 2013;3(3):1309‐36. [DOI] [PubMed] [Google Scholar]
Hebestreit 2001
- Hebestreit A, Kersting U, Basler B, Jeschke R, Hebestreit H. Exercise inhibits epithelial sodium channels in patients with cystic fibrosis. American Journal of Respiratory and Critical Care Medicine 2001;164(3):443‐6. [DOI] [PubMed] [Google Scholar]
Hebestreit 2014
- Hebestreit H, Schmid K, Kieser S, Junge S, Ballmann M, Roth K, et al. Quality of life is associated with physical activity and fitness in cystic fibrosis. BMC Pulmonary Medicine 2014;14:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hopewell 2009
- Hopewell S, Loudon K, Clarke MJ, Oxman AD, Dickersin K. Publication bias in clinical trials due to statistical significance or direction of trial results. Cochrane Database of Systematic Reviews 2009, Issue 1. [DOI: 10.1002/14651858.MR000006.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Houston 2013
- Houston BW, Mills N, Solis‐Moya A. Inspiratory muscle training for cystic fibrosis. Cochrane Database of Systematic Reviews 2013, Issue 11. [DOI: 10.1002/14651858.CD006112.pub3] [DOI] [PubMed] [Google Scholar]
Nixon 1992
- Nixon PA, Orenstein DM, Kelsey SF, Doerschuk CF. The prognostic value of exercise testing in patients with cystic fibrosis. New England Journal of Medicine 1992;327(25):1785‐8. [DOI] [PubMed] [Google Scholar]
O'Neill 1987
- O'Neill PA, Dodds M, Phillips B, Poole J, Webb AK. Regular exercise and reduction of breathlessness in patients with cystic fibrosis. British Journal of Diseases of the Chest 1987;81(1):62‐9. [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Ruf 2010
- Ruf K, Winkler B, Hebestreit A, Gruber W, Hebestreit H. Risks associated with exercise testing and sports participation in cystic fibrosis. Journal of Cystic Fibrosis 2010;9(5):339‐45. [DOI] [PubMed] [Google Scholar]
Schneiderman 2014
- Schneiderman JE, Wilkes DL, Atenafu EG, Nguyen T, Wells GD, Alarie N, et al. Longitudinal relationship between physical activity and lung health in patients with cystic fibrosis. European Respiratory Journal 2014;43(3):817‐23. [DOI] [PubMed] [Google Scholar]
Shephard 1994
- Shephard RJ. Aerobic Fitness and Health. Leeds, England: Human Kinetic Publishers, 1994. [Google Scholar]
Tejero García 2011
- Tejero García S, Giráldez Sánchez MA, Cejudo P, Quintana Gallego E, Dapena J, García Jiménez R, et al. Bone health, daily physical activity, and exercise tolerance in patients with cystic fibrosis. Chest 2011;140(2):475‐81. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Bradley 2002
- Bradley JM, Moran F. Physical training for cystic fibrosis. Cochrane Database of Systematic Reviews 2002, Issue 2. [DOI: 10.1002/14651858.CD002768] [DOI] [PubMed] [Google Scholar]
Bradley 2008
- Bradley JM, Moran F. Physical training for cystic fibrosis. Cochrane Database of Systematic Reviews 2008, Issue 1. [DOI: 10.1002/14651858.CD002768.pub2] [DOI] [PubMed] [Google Scholar]
Radtke 2015a
- Radtke T, Nolan SJ, Hebestreit H, Kriemler S. Physical exercise training for cystic fibrosis. Cochrane Database of Systematic Reviews 2015, Issue 6. [DOI: 10.1002/14651858.CD002768.pub3] [DOI] [PubMed] [Google Scholar]