

Abstract
Background
Sweet potato (Ipomoea batatas) is among the most nutritious subtropical and tropical vegetables. It is also used in traditional medicine practices for type 2 diabetes mellitus. Research in animal and human models suggests a possible role of sweet potato in glycaemic control.
Objectives
To assess the effects of sweet potato for type 2 diabetes mellitus.
Search methods
We searched several electronic databases, including The Cochrane Library (2013, Issue 1), MEDLINE, EMBASE, CINAHL, SIGLE and LILACS (all up to February 2013), combined with handsearches. No language restrictions were used.
Selection criteria
We included randomised controlled trials (RCTs) that compared sweet potato with a placebo or a comparator intervention, with or without pharmacological or non‐pharmacological interventions.
Data collection and analysis
Two authors independently selected the trials and extracted the data. We evaluated risk of bias by assessing randomisation, allocation concealment, blinding, completeness of outcome data, selective reporting and other potential sources of bias.
Main results
Three RCTs met our inclusion criteria: these investigated a total of 140 participants and ranged from six weeks to five months in duration. All three studies were performed by the same trialist. Overall, the risk of bias of these trials was unclear or high. All RCTs compared the effect of sweet potato preparations with placebo on glycaemic control in type 2 diabetes mellitus. There was a statistically significant improvement in glycosylated haemoglobin A1c (HbA1c) at three to five months with 4 g/day sweet potato preparation compared to placebo (mean difference ‐0.3% (95% confidence interval ‐0.6 to ‐0.04); P = 0.02; 122 participants; 2 trials). No serious adverse effects were reported. Diabetic complications and morbidity, death from any cause, health‐related quality of life, well‐being, functional outcomes and costs were not investigated.
Authors' conclusions
There is insufficient evidence about the use of sweet potato for type 2 diabetes mellitus. In addition to improvement in trial methodology, issues of standardization and quality control of preparations ‐ including other varieties of sweet potato ‐ need to be addressed. Further observational trials and RCTs evaluating the effects of sweet potato are needed to guide any recommendations in clinical practice.
Plain language summary
Sweet potato for type 2 diabetes mellitus
Sweet potato (Ipomoea batatas) is a plant found in the tropical and subtropical belts and is one of the most nutritious tropical and subtropical vegetables. As well as being popular in cooking in countries in Asia‐Pacific, Africa and North America, sweet potato is also used in traditional medicine for the treatment of diabetes mellitus. We decided to investigate whether there is enough evidence from medical trials to show whether sweet potato works as a treatment for diabetes. This review of randomised controlled trials found only three studies (with a total of 140 participants) that evaluated the effects of sweet potato for type 2 diabetes mellitus compared with a fake medicine (placebo). All these trials were of very low quality. Two studies with 122 participants showed improved long‐term metabolic control of blood sugar levels as measured by glycosylated haemoglobin A1c (HbA1c) which was moderately lowered by 0.3% in participants who were given 4 g sweet potato tablets a day for three to five months. The duration of treatment ranged from six weeks to five months. No study investigated diabetic complications, death from any cause, health‐related quality of life, well‐being, functional outcomes or costs. Adverse effects were mostly mild, and included abdominal distension and pain. There are many varieties of sweet potatoes and sweet potato preparations. More trials are needed to assess the quality of the various sweet potato preparations as well as to evaluate further the use of different varieties of sweet potato in the diet of diabetic people.
Summary of findings
Summary of findings for the main comparison. Ipomoea batatas (Caiapo) tablets compared to placebo for type 2 diabetes mellitus.
| Ipomoea batatas (Caiapo) tablets compared to placebo for type 2 diabetes mellitus | ||||||
| Patient or population: people with type 2 diabetes mellitus Settings: out‐patients Intervention:Ipomoea batatas (Caiapo) tablets Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Ipomoea batatas (Caiapo) tablets | |||||
| Morbidity | See comment | See comment | Not estimable | See comment | See comment | Not investigated |
| Adverse effects Follow‐up: 1.5 to 5 months | See comment | See comment | Not estimable | 140 (3) | ⊕⊝⊝⊝ very lowa | 2 out of 3 studies reported adverse eventsb |
| Health‐related quality of life | See comment | See comment | Not estimable | See comment | See comment | Not investigated |
| Well‐being | See comment | See comment | Not estimable | See comment | See comment | Not investigated |
| Functional outcomes | See comment | See comment | Not estimable | See comment | See comment | Not investigated |
| Costs | See comment | See comment | Not estimable | See comment | See comment | Not investigated |
| HbA1c [%] (final values) Follow‐up: 3 or 5 months | Final values for HbA1c across control groups ranged from 6.5 to 7.1 | Final values for Hba1c in the intervention groups were 0.3 lower (0.6 to 0.04 lower) | ‐ | 122 (2) | ⊕⊝⊝⊝ very lowc | ‐ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: we are very uncertain about the estimate | ||||||
aDowngraded by three due to high risk of bias (insufficient information on the process of randomisation, blinding, selective outcome and incomplete data reporting), small number of trials and participants and no replication of trials by other authors (same investigating team throughout) bMild gastrointestinal symptoms such as nausea, diarrhoea, constipation, gastric pain and abdominal distension
cDowngraded by three due to imprecision, high risk of attrition bias and indirectness
Background
Description of the condition
Diabetes mellitus is a metabolic disorder resulting from a defect in insulin secretion, insulin action, or both. A consequence of this is chronic hyperglycaemia (that is elevated levels of plasma glucose) with disturbances in carbohydrate, fat and protein metabolism. Long‐term complications of diabetes mellitus include retinopathy, nephropathy and neuropathy (i.e. problems with the eyes, kidneys and peripheral nerves). Diabetes mellitus also increases the risk of cardiovascular disease. For a detailed overview of diabetes mellitus, please see the 'Additional information' section in the information about the Metabolic and Endocrine Disorders Group in The Cochrane Library (see 'About', 'Cochrane Review Groups (CRGs)'). For an explanation of methodological terms, see the main glossary in The Cochrane Library.
Type 2 diabetes mellitus (T2DM) is a global public health issue (Abegunde 2007; Wild 2004). The increase in numbers of people with T2DM across the age spectrum is of concern. Given the progressive nature of the disease, and the multiple pathophysiological (disease) abnormalities associated with it, accelerated ageing is suspected. This is supported by evidence both at molecular and functional levels (Monnier 2005).
Description of the intervention
Sweet potato (Ipomoea batatas) is a member of the Convolvulaceae family; it is a dicotyledonous perennial plant found in the tropical and subtropical belts (Woolfe 1992). Most varieties are edible, and all parts of the plants ‐ shoots, leaves, vine and tubers ‐ are consumed. The large, sweet‐tasting tuberous roots, young leaves and shoots are common market vegetables. Sweet potato is rich in nutrients and ranked highest in nutritional value amongst vegetables available in the United States of America (USDA 2010). Among the important nutrients found in tubers are monosaccharides (Salvador 2000), complex carbohydrates (Sabater‐Molina 2009), dietary fibre, beta‐carotene (a source of vitamin A) (Maiani 2009), vitamin C, vitamin B6, anthocyanins (Miyazaki 2008), and minerals (Antia 2006). The leaves of sweet potato are rich in protein, fibre, fat, vitamins, and minerals (Antia 2006). Linoleic and alpha‐linolenic acids (Almazan 1998), galactolipids (Napolitano 2007), and bioactive substances (e.g. dietary antioxidants, including anthocyanins (Islam 2002), polyphenols (Thu 2004), flavonoids (Miean 2001), and caffeic acid derivatives (Islam 2003)) are also present. These compounds have been extensively investigated for their role in health promotion in many countries.
As well as being popular in the cuisines of countries in the Asia‐Pacific area, Africa and North America, sweet potato is also used in traditional medical practices for the treatment of T2DM (Duke 1981). In addition, various parts of the plants are used to treat asthma, nausea, fever, tumours, bug bites, burns, upset stomach, diarrhoea, boils, and acne. It is also used as a tonic for lactating women and during convalescence.
Adverse effects of the intervention
There have been anecdotal reports of instances of anaphylaxis after ingestion of sweet potato (Velloso 2004), however, there have been no reports of adverse effects such as hypoglycaemia (low blood sugar levels), weight gain or an increased risk of fractures. Even though there are low levels of toxins in the leaves of sweet potato ‐ phytic acid, tannic acid, and, to a lesser extent, oxalic acid ‐ these can be reduced to negligible levels with conventional blanching (Mosha 1995). Furthermore, microwave blanching also reduces trypsin and chemotrypsin inhibitors, which improves digestibility of proteins (Mosha 1999).
How the intervention might work
The blood glucose‐lowering activities of sweet potato were demonstrated in animal studies. A number of bioactive compounds were isolated from the leaves (Li 2009), and also the tubers (Kusano 2001; Sakuramata 2004). These compounds, together with dietary fibre, contribute to blood glucose‐lowering activitiy. Besides glycaemic control, sweet potato has shown anti‐sclerotic activity and inhibition of glycation in vitro (Miyazaki 2008; Park 2010), as well as antihypertensive (Egert 2009), antioxidative (Huang 2007; Islam 2009), antimutagenic (Kurata 2007), chemopreventive (Wang 2008), and cardioprotective properties (Maiani 2009). Finally, there is a suggestion that sweet potato may delay amyloid formation and prevent neuronal damage in the brain of mice (Kim 2011; Lu 2010; Wang 2010; Wu 2008; Ye 2010).
In clinical terms, the aforementioned properties of the sweet potato plant may not only contribute to glycaemic control, but may also show possible protective effects on target organs. The presence of other biologically‐active compounds may have positive impacts on health and well‐being of people with T2DM.
Why it is important to do this review
Asia is in the midst of the current T2DM epidemic (Chan 2009). The intense resource requirements of diabetic care, and high quality care of the disabled, coupled with the current epidemic of T2DM, particularly in the developing countries, are of concern. Both cross‐sectional and longitudinal studies have demonstrated that T2DM is a risk factor for both cognitive and physical functional limitations and disabilities, especially in older adults (Bruce 2005; De Rekeneire 2003; Gregg 2002; Kalyani 2010; Mogi 2004; Yen 2010). Limitations in activities of daily living and instrumental activities of daily living lead to an increased likelihood of hospitalisation, institutionalisation, and loss of economic self‐sufficiency (Abbatecola 2009). Thus, T2DM is a burden to families, the community, and social and healthcare systems.
It has been suggested that proper glycaemic control is a modifiable factor of disability, particularly with respect to those disabilities related to instrumental activities of daily living (Abbatecola 2009). Studies on animal models have demonstrated the protective effect of glycaemic control on beta‐cells (Grossman 2010).
A healthy diet consisting of low fat levels, with high levels of complex carbohydrates, appropriate portions of proteins, essential micronutrients and minerals in the therapeutic nutritional management of T2DM has been well‐established (Bantle 2008). In the past decade, the enhanced global research into botanicals as potential contributors to the management of T2DM beyond nutritional therapy has identified more than 600 plants that may be helpful (Grover 2002; Li 2004; Malviya 2010; Mukherjee 2006). However, there is currently insufficient evidence to recommend the use of an individual botanical and its products specifically in mainstream medical practice for the management of T2DM.
In addition, there are also concerns of ‘botanical’‐drug interactions with the concurrent use of oral hypoglycaemics (Genser 2008). Adverse consequences such as severe hypoglycaemia may result if these interactions are not identified and managed properly. Other important longer‐term adverse factors that may affect function include weight gain and increase in fracture risk. Should this happen, the cumulative effect of worsening impairments and increasing the risk of disabilities and dependency would aggravate the existing burden of care, and compound the escalating health and social‐care costs.
Most of the evidence implicating the influence of sweet potato on glucose‐insulin metabolism are preclinical studies and anecdotal case reports. There are still gaps in the knowledge regarding its potential use in the management of T2DM in the clinical context. Apart from the nutritional qualities of the plant, powder, tablets and food supplements containing compounds extracted from sweet potato are also available ‐ all touting its benefit in diabetes management. Better insight into this common botanical may enable clinicians to improve the management of T2DM, complementing 'lifestyle' management.
Given the potentially devastating outcomes of the disease, especially in older adults, addressing the gaps in the literature is important. To date, there has been no literature review specifically investigating the clinical effects of sweet potato in the management of T2DM.
Objectives
To assess the effects of sweet potato for type 2 diabetes mellitus.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled clinical trials.
Types of participants
We included adults over 18 years of age, of either gender, with type 2 diabetes mellitus based on the diagnostic criteria below. Individuals with normal fasting blood glucose and postprandial glucose levels were excluded. People with concomitant endocrinopathy affecting their blood glucose levels were also excluded.
Diagnostic criteria
To be consistent with changes in classification and diagnostic criteria of diabetes mellitus through the years, the diagnosis should have been established using the standard criteria valid at the time of the beginning of the trial (for example ADA 1999; ADA 2008; WHO 1998). Ideally, diagnostic criteria should have been described. If necessary, we used authors' definition of diabetes mellitus. We planned to subject diagnostic criteria to a sensitivity analysis.
Types of interventions
Intervention
Any orally administered mono‐preparation of sweet potato in any dose or form. This could be the sole intervention, or given in combination with diet, insulin, oral hypoglycaemic agents, or both.
Control
Placebo or no treatment, with or without diet, active medications, such as insulin, oral hypoglycaemic agents, or other herbal or nutritional preparations.
Co‐interventions were considered if both arms of the randomised trial received similar interventions. However, we excluded combination preparations of sweet potato with other nutritional or herbal preparations.
Types of outcome measures
Primary outcomes
Glycaemic control (fasting blood glucose levels (FBG); two‐hour postprandial blood glucose levels; glycosylated haemoglobin A1c (HbA1c)).
Morbidity (both type 2 diabetes mellitus‐related morbidities and cardiovascular‐related co‐morbidities; all cause morbidity).
Adverse effects (e.g. hypersensitivity reaction, hypoglycaemia).
Secondary outcomes
Serum insulin, C‐peptide or insulin sensitivity (homeostasis model assessment of insulin resistance (HOMA‐IR)).
Body weight or body mass index (BMI).
Blood levels of lipids: total cholesterol, low‐density lipoprotein (LDL)‐cholesterol, high‐density lipoprotein (HDL)‐cholesterol, triglycerides.
Functional outcomes (both physical and cognitive functions).
Health‐related quality of life.
Well‐being.
Costs.
Timing of outcome measurement
Two of the outcomes, fasting blood glucose and two‐hour postprandial glucose levels, required trials with durations of at least six weeks, or more, to yield meaningful results. HbA1c trials needed to be run over three months.
Search methods for identification of studies
Electronic searches
We searched the following sources from inception to the present.
The Cochrane Library (2013, Issue 1).
MEDLINE (until February 2013).
EMBASE (until February 2013).
CINAHL (until February 2013).
LILACS (www.bireme.br/bvs/I/ibd.htm ‐ until February 2013).
Natural Medicines Comprehensive Database (until February 2013).
SIGLE (System for Information on Grey Literature in Europe ‐ until 2013).
Theses:
Proquest Dissertations and Theses database.
For detailed search strategies see Appendix 1.
We also searched databases of ongoing trials (www.clinicaltrials.gov/ and www.clinicaltrialsregister.eu/). We planned to provide information including trial identifiers about potentially‐relevant ongoing studies in the table 'Characteristics of ongoing studies' and in a 'Matrix of study endpoints (protocol/trial documents)'. We wanted to find the protocol of each included study, either in databases of ongoing trials, in publications of study designs, or both, and specify data in an appendix 'Matrix of study endpoints (protocol/trial documents)'.
No additional key words of relevance were detected during any of the electronic or other searches. Thus, the electronic search strategies were not modified. Studies published in any language were included.
We sent results of electronic searches to the editorial office of the Cochrane Metabolic and Endocrine Disorders Group for databases to which their staff did not have access.
Searching other resources
We tried to identify additional studies by searching the reference lists of included trials and (systematic) reviews, meta‐analyses and health technology assessment reports. We approached content experts and associations for further additional information, additional references, unpublished data and/or updated results of ongoing interventions. We also contacted manufacturers of powder, tablets and food supplements that contain compounds extracted from sweet potato for additional information, where necessary.
Data collection and analysis
Selection of studies
To determine which studies should be assessed further, two review authors (CPO, SCL) independently scanned the abstract, title, or both, of every record retrieved. The full text of all potentially relevant articles was investigated. We selected only three studies for inclusion in this review. Where differences in opinion existed, they were resolved by a third party (from the editorial office). Had resolution of a disagreement not been possible, the article would have been added to the 'Studies awaiting classification' section and the study authors would have been contacted for clarification. This process is summarised in the PRISMA (preferred reporting items for systematic reviews and meta‐analyses) flow‐chart (Figure 1) of study selection (Liberati 2009).
1.
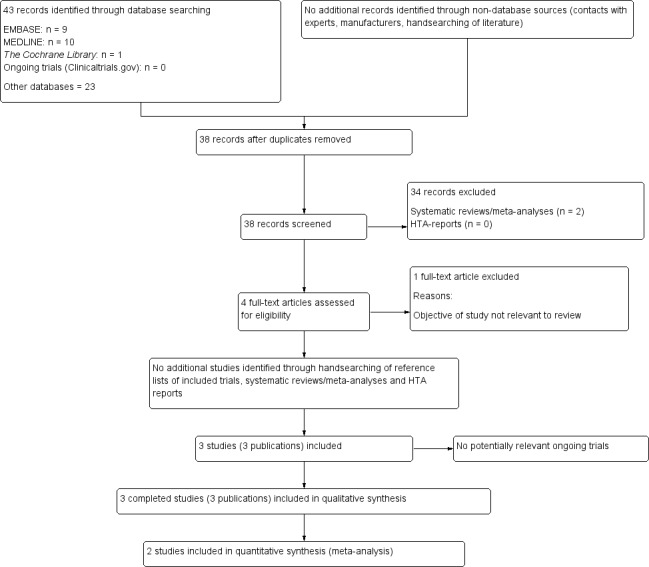
Study flow diagram
Data extraction and management
For studies that fulfilled inclusion criteria, two authors (CPO, SCL) independently extracted characteristics about the relevant population and the interventions using standard data extraction templates (for details see Characteristics of included studies; Table 2; Appendix 2; Appendix 3; Appendix 4; Appendix 5; Appendix 6; Appendix 7; Appendix 8; Appendix 9; Appendix 10; Appendix 11). Any disagreements were resolved by discussion, or, when required, by a third party (editorial office). We attempted to contact the authors for relevant details about the trials. The results of this survey are displayed in Appendix 12.
1. Overview of study populations.
| Characteristic | Intervention(s) and comparator(s) | Sample size | [N] Screened/ eligible | [N] Randomised | [N] Safety | [N] ITT | [N] Finishing study | [%] Randomised finishing study | Follow‐upa |
| Ludvik 2002 | I1: 2 g powdered white‐skinned sweet potato (Ipomoea batatas) tablet | ‐ | ‐ | 6 | 6 | ‐ | 6 | 100 | 6 weeks |
| I2: 4 g powdered white‐skinned sweet potato (Ipomoea batatas) tablet | 6 | 6 | 6 | 100 | |||||
| C: Placebo | 6 | 6 | 6 | 100 | |||||
| Total: | 18 | 18 | 18 | 100 | |||||
| Ludvik 2004 | I: 4 g of Caiopo (Ipomoea batatas) tablet | ‐ | ‐ | 30 | 30 | ‐ | 30 | 100 | 3 months |
| C: Placebo | 31 | 31 | 31 | 100 | |||||
| Total: | 61 | 61 | 61 | 100 | |||||
| Ludvik 2008 | I: 4 g of Caiopo (Ipomoea batatas) tablet | 21 | ‐ | ‐ | ‐ | ‐ | 27 | N/A | 5 months |
| C Placebo | 21 | ‐ | ‐ | 34 | N/A | ||||
| Total: | 42 | 88 | ‐ | 61 | 69.3 | ||||
| Grand total | All interventions | I1: 63 + ? I2: 6 | I1: 63 I2: 6 | ||||||
| All comparators | 71 + ? | 71 | |||||||
| All interventions and comparators | 140 + ? | 140 | |||||||
aDuration of intervention and/or follow‐up under randomised conditions until end of study
"‐" denotes not reported
"+ ?" denotes number of unreported participants who took part in the study
C: comparator; I: intervention; ITT: intention‐to‐treat; N/A: not applicable
Dealing with duplicate publications
Should there be duplicate publications and companion papers relating to a primary study, we intend to maximize the yield of information by simultaneous evaluation of all available data.The publication that reported the longest follow‐up associated with our primary or secondary outcomes will obtain priority and be marked as the primary reference for that study.
Assessment of risk of bias in included studies
Two authors (CPO, SCL) assessed each trial independently for risk of bias. Disagreements were resolved by consensus, or by consultation with a third party (editorial office).
We assessed risk of bias using The Cochrane Collaboration’s tool for assessment of risk of bias (Higgins 2011). We used the following criteria in this assessment.
Random sequence generation (selection bias).
Allocation concealment (selection bias).
Blinding (performance bias and detection bias), blinding of participants and personnel assessed separately from blinding of outcome assessment.
Incomplete outcome data (attrition bias).
Selective reporting (reporting bias).
Other bias.
We judged risk of bias criteria as being at 'low risk', 'high risk' or 'unclear risk', and evaluated individual bias items as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We presented a 'Risk of bias' graph (Figure 2) and 'Risk of bias' summary (Figure 3).
2.
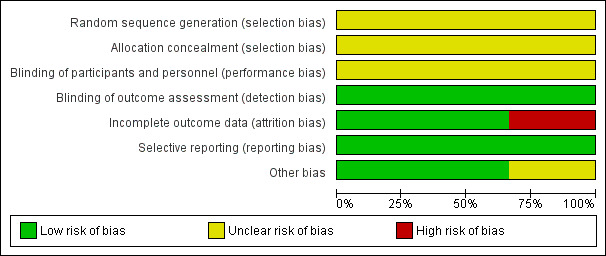
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
3.
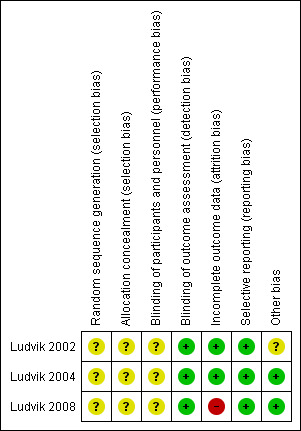
Risk of bias summary: review authors' judgements about each risk of bias item for each included study
We assessed the impact of individual bias domains on study results at endpoint and at study levels.
Measures of treatment effect
We expressed dichotomous data as odds ratios (ORs) or risk ratio (RRs) with 95% confidence intervals (CIs). We expressed continuous data as mean differences (MD) with 95% CI.
Unit of analysis issues
We took into account the level at which randomisation occurred, such as cross‐over trials, cluster‐randomised trials and multiple observations for the same outcome.
Dealing with missing data
We attempted to obtain missing data from authors. If it was feasible, we performed careful evaluation of important numerical data such as screened, randomised participants as well as intention‐to‐treat (ITT), and as‐treated and per‐protocol (PP) populations. We investigated attrition rates, for example drop‐outs, losses to follow‐up and withdrawals, and appraised issues of missing data and imputation methods critically (for example last‐observation‐carried‐forward (LOCF)).
Assessment of heterogeneity
In the event of substantial clinical, methodological, or statistical heterogeneity we did not report study results as pooled meta‐analysed effect estimates.
We planned to identify heterogeneity by visual inspection of the forest plots and by using a standard Chi2 test. As this test has a low power, a significance level was set at α = 0.1. We specifically examined heterogeneity employing the I2 statistic, which quantifies inconsistency across studies, to assess the impact of heterogeneity on the meta‐analysis (Higgins 2002; Higgins 2003); an I2 statistic of 75% or more indicates a considerable level of inconsistency (Higgins 2011).
When heterogeneity was found, we planned to determine potential reasons for it by examining individual study and subgroup characteristics.
We expected the following characteristics to introduce clinical heterogeneity.
Compliance with treatment (including medical and nutritional management).
Co‐medications (e.g. insulin, oral hypoglycaemics).
Assessment of reporting biases
If we had identified more than 10 RCTs that investigated a particular outcome, we planned to use funnel plots to assess small study bias. There are a number of explanations for asymmetry in a funnel plot (Sterne 2001), and we planned to interpret results carefully (Lau 2006).
Data synthesis
Unless there was good evidence for homogeneous effects across studies, we planned to summarise primarily low‐risk of bias data by means of a random‐effects model (Wood 2008). We wanted to interpret random‐effects meta‐analyses with due consideration of the whole distribution of effects, ideally by presenting a prediction interval (Higgins 2009). A prediction interval specifies a predicted range for the true treatment effect in an individual study (Riley 2011). Primarily, we summarised data statistically if they were available, sufficiently similar and of sufficient quality. We performed statistical analyses according to the statistical guidelines in the latest version of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Subgroup analysis and investigation of heterogeneity
We planned to carry out subgroup analyses if any one of the primary outcome parameters (see above) demonstrated statistically significant differences between intervention groups.
The following subgroup analyses were planned.
Studies with normal or below baseline nutritional status.
Effect of dosage of sweet potato extract or products.
Effect of forms of sweet potato extract or products.
Effect of duration therapy of sweet potato extract or products.
We planned to apply tests of interaction to determine subgroup effects (Altman 2003).
We anticipated the direction of the subgroup effects to be as follows (Sun 2010).
Direction of effect on glycaemic control is reversed for sweet potato extract or products, that is, sweet potato and its products have beneficial effects for those with below baseline nutritional status.
Direction of effect on glycaemic control is unchanged for the effects of dosage, forms and duration of therapy of sweet potato extract or products.
Sensitivity analysis
We planned to perform sensitivity analyses in order to explore the influence of the following factors on effect sizes.
Restricting the analysis to published studies.
Restricting the analysis by taking into account risk of bias, as specified in the section Assessment of risk of bias in included studies.
Restricting the analysis to very long or large studies to establish the extent to which they dominate the results.
Restricting the analysis to studies using the following filters: diagnostic criteria, language of publication, source of funding (industry versus other), country.
We also wanted to test the robustness of the results by repeating the analysis using different measures of effect size (RR, OR etc.) and different statistical models (fixed‐effect and random‐effects models).
Results
Description of studies
For details see Characteristics of included studies and Characteristics of excluded studies. There are no studies awaiting classification.
Results of the search
The original electronic searches identified 12 articles (Figure 1). No additional records or unpublished studies were identified through other sources. We removed four duplicates. On reading the titles and abstracts, we excluded a further four articles because they were reviews and non‐clinical studies. This search for the review update identified a total of 31 additional references, however, no new studies were identified.
We selected a total of four publications describing randomised controlled clinical trials for further assessment (Ludvik 2002; Ludvik 2003; Ludvik 2004; Ludvik 2008). Two publications were analyses from the same trial (Ludvik 2002; Ludvik 2003). One of them was published as a 'letter to the editor' (Ludvik 2002), and, therefore, provided limited information. The second publication evaluated the mechanism of sweet potato (Caiapo) (Ludvik 2003). All the trials were published in the English language.
Two trials recruited patients from offices of general practitioners from Austria, Germany and Switzerland (Ludvik 2004; Ludvik 2008). The other trial did not provide information about the setting of the study (Ludvik 2002).
Included studies
Altogether, we included three trials in this review (Ludvik 2002; Ludvik 2004; Ludvik 2008). The details of these trials are summarised in Characteristics of included studies. Participants were recruited from outpatient clinics in Switzerland (Ludvik 2004), Austria and Germany (Ludvik 2008). The third trial did not provide information about the centre of study (Ludvik 2002). All these trials used similar sweet potato tablets, of different dosages, and placebo controls. The duration of treatment ranged from six weeks to five months.
Baseline characteristics
Ludvik 2002 included only male participants, while Ludvik 2008 had a female‐to‐male ratio of 1:1 that was roughly balanced between the sweet potato (Caiapo) tablets group and the control group. Ludvik 2004 had a female‐to‐male ratio of 3:5. There was no information about the duration of diabetes in two trials (Ludvik 2002; Ludvik 2004). In the third trial, the duration of T2DM was 3.5 years (standard deviation (SD) 4.2) and 4.2 years (SD 2.9) for the intervention and control groups, respectively (Ludvik 2008). These publications did not report any relevant baseline data on co‐morbidities. A total of 69 patients with T2DM were on dietary control only in the intervention groups and 71 patients in the control groups, respectively.
Participants
A total of 140 participants with T2DM participated in the three trials, ranging from 18 to 61 patients per trial (Ludvik 2002; Ludvik 2004; Ludvik 2008). Most participants were of white complexion. The mean ages were all over 55 years. One trial recruited only male participants (Ludvik 2002), while the other two trials had female‐to‐male ratios of about 1:1 (Ludvik 2004; Ludvik 2008).
Diagnosis
All trial participants had T2DM. Criteria for diagnosis in all three trials were based on the authors’ definitions. With the small number of trials and relatively small sample sizes, sensitivity analysis on diagnostic criteria was not possible.
Treatment before study
All the participants were on diet control prior to the studies. Five patients in one study were on antidiabetic medications in addition to diet control (Ludvik 2004). These drugs included metformin and glibenclamide. There was a washout period of two weeks following withdrawal of the medications. In the trial of Ludvik 2008, medications that affected the blood glucose level (such as corticosteroids, high‐dose diuretics or beta‐blockers) were stopped during the two weeks prior to screening and for the duration of the entire study. Screening for participants took place one month prior to the start of the studies, and was followed by a washout period of four weeks after withdrawal of hypoglycaemic drugs.
Interventions
Sweet potato (Caiapo) tablets were used as the intervention in all the trials. These tablets came from the same manufacturer and were made from powdered white‐skinned sweet potato (Ipomoea batatas). One trial used two different dosages of Caiapo tablets (2 g and 4 g) (Ludvik 2002). The other two trials used a 4 g dose of Caiapo tablets (Ludvik 2004; Ludvik 2008). In all three trials, the control interventions were placebos. However, no information was provided about the content of the placebos.
Outcomes
All included trials reported glycaemic control. The parameters included fasting blood glucose and glycosylated haemoglobin A1c (HbA1c). Only one trial reported two‐hour postprandial blood glucose (Ludvik 2004). The other outcomes that were reported included lipid levels (total cholesterol, LDL‐cholesterol, HDL‐cholesterol and triglycerides), body weight, BMI and adverse events. Two of the trials reported details of adverse events (Appendix 9; Appendix 10; Appendix 11). These mild adverse events, i.e. upset stomach, abdominal distention, stomach‐ache, and nausea were observed in both the intervention and control groups. No serious adverse events were observed in the intervention groups. One trial observed no adverse events in either the control or intervention groups (Ludvik 2002). All outcomes measured were reported at the end of treatment. Only one trial reported follow‐up data at two months (Ludvik 2004). None of the trials reported outcomes on diabetic complications and morbidity, functional outcomes, health‐related quality of life, well‐being or costs.
Excluded studies
Only one RCT was excluded (Ludvik 2003). Although Ludvik 2003 was an analysis from the same study as Ludvik 2002, its objective was to evaluate the mechanism by which Ipomoea batatas worked, therefore, it was not relevant to the objective of this review. Furthermore, it did not contain relevant outcome data. There are no ongoing studies or studies awaiting classification.
Risk of bias in included studies
We detected a predominantly unclear risk of bias in the domains of selection and performance bias within and across studies (see Figure 2 and Figure 3). All the trials were of parallel‐group design, but there was limited information on design and methodology.
Allocation
None of the trials reported adequately on randomisation and allocation concealment.
Blinding
Although all trials were described as having been double‐blinded, none reported on the double‐blinding procedure.
Incomplete outcome data
In two trials, all participants completed the study, and no treatment withdrawals were reported (Ludvik 2002; Ludvik 2004). One trial reported participants lost to follow‐up with justifications (Ludvik 2008). However, there was no detail about the number of participants missing from each of the treatment and control groups. None of the three trials provided explicit reporting of intention‐to‐treat analyses or missing data.
Selective reporting
No selective reporting bias was detected (see Appendix 5; Appendix 7).
Other potential sources of bias
No other potential sources of bias were detected.
Effects of interventions
See: Table 1
Comparisons
Similar sweet potato (Caiapo) tablets were used in all the three trials. The comparisons were as follows.
Sweet potato (Caiapo) tablets 2 g or 4 g daily versus placebo (Ludvik 2002).
Sweet potato (Caiapo) tablets 4 g daily versus placebo (Ludvik 2004; Ludvik 2008).
The three trials reported outcomes that included fasting blood glucose, glycosylated haemoglobin A1c (HbA1c), total cholesterol, triglycerides and adverse effects. Ludvik 2002 and Ludvik 2008 reported on BMI, and Ludvik 2004 on body weight.
Primary outcomes
Glycaemic control
Compared with placebo, sweet potato (Caiapo) preparations of 2 g/day showed no statistically significant effect on the reduction of fasting blood glucose when used for two months or less (Analysis 1.1). However, when the dosage was increased to 4 g/day, there were statistically significant reductions in both the short (six weeks to two months) and longer terms (three to five months) (Analysis 1.1). Data for fasting blood glucose of less than three months are not reported as a pooled estimate, as there was a high level of heterogeneity for this outcome (I2 = 88%). Data from three to five months showed a mean difference in fasting blood glucose between groups of ‐0.68 mmol/L in favour of the sweet potato intervention (95% CI ‐0.84 to ‐0.52; P value < 0.00001; 122 participants; two trials; Analysis 1.1).
1.1. Analysis.
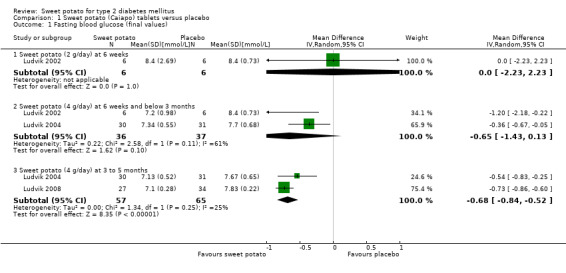
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 1 Fasting blood glucose (final values).
Data for two‐hour postprandial blood glucose were only available from one publication (Ludvik 2004). There were no statistically significant reductions in two‐hour postprandial blood glucose levels with 4 g/day sweet potato tablets compared with placebo at two or three months (Analysis 1.2).
1.2. Analysis.
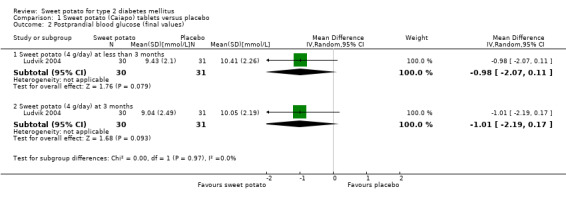
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 2 Postprandial blood glucose (final values).
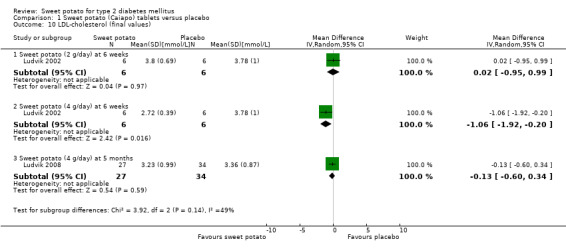
When compared with placebo, the sweet potato treatment showed statistically significant reductions in HbA1c levels (Analysis 1.3). The mean difference for HbA1c was ‐0.3% (95% CI ‐0.57 to ‐0.04; P value 0.02; 122 participants; two trials; Analysis 1.3) in favour of the sweet potato intervention.
1.3. Analysis.
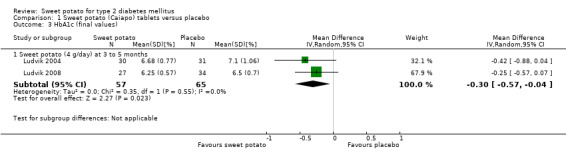
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 3 HbA1c (final values).
Morbidity
No publication presented data on T2DM‐related or cardiovascular‐related morbidities.
Adverse events
Details of adverse events are described in Appendix 9; Appendix 10; Appendix 11.
Only two out of the three studies reported adverse events (Ludvik 2004; Ludvik 2008). Adverse events were present for both intervention and control groups, and were not specific to the sweet potato intervention groups. In view of the poor quality of the reported data, quantitative analysis was not possible. Most of these reported events were mild gastrointestinal symptoms such as nausea, gastric pain, diarrhoea, constipation and abdominal distension. We were not able to contact the authors for further details (Appendix 12).
No serious adverse events such as severe hypoglycaemia were reported. There was also no explicit reporting of drop‐outs due to adverse events.
Secondary outcomes
Serum insulin, C‐peptide or insulin sensitivity (homeostasis model assessment of insulin resistance (HOMA‐IR))
Two trials provided data on fasting insulin level (Ludvik 2004; Ludvik 2008). The sample size in Ludvik 2002 was inadequate for estimation of any relevant changes. Data disclosed in Ludvik 2008 showed no statistically significant change in the fasting insulin level in the sweet potato treatment group (Analysis 1.4). Furthermore, Ludvik 2008 provided data on the measurement of beta‐cell function and insulin sensitivity; after five months of sweet potato tablets, there was a statistically significant improvement in insulin sensitivity but not in beta‐cell function (Appendix 13).
1.4. Analysis.
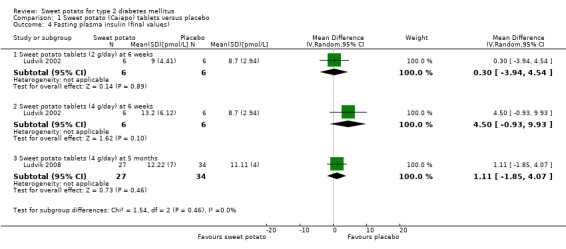
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 4 Fasting plasma insulin (final values).
Body weight or body mass index
Only one trial provided data on body weight with no BMI data (Ludvik 2004). There was no statistically significant change between the sweet potato intervention and the placebo (Analysis 1.5). Two trials reported data on BMI (Ludvik 2002; Ludvik 2008). Similarly, no statistically significant change in BMI was found in either of these trials of short‐term (Ludvik 2002) and longer term (Ludvik 2008), treatment (Analysis 1.6).
1.5. Analysis.
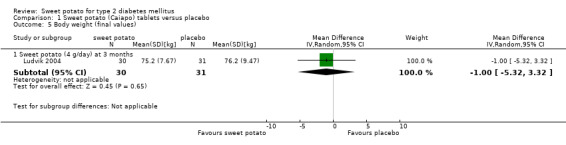
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 5 Body weight (final values).
1.6. Analysis.
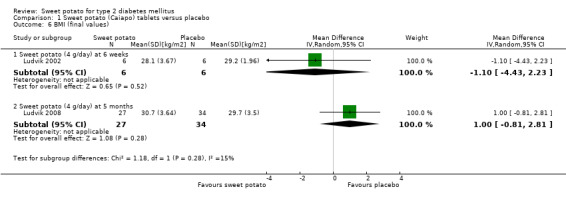
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 6 BMI (final values).
Lipids (total cholesterol, LDL‐cholesterol, HDL‐cholesterol, triglycerides)
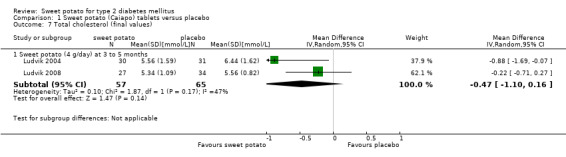
All three trials provided data on total cholesterol and triglycerides. Both Ludvik 2002 and Ludvik 2008 provided data on HDL‐ and LDL‐cholesterol. Compared with participants on placebos, those on 4 g/day sweet potato tablets demonstrated no statistically significant changes in either total cholesterol or triglyceride levels at three to five months (Analysis 1.7; Analysis 1.8).
1.7. Analysis.
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 7 Total cholesterol (final values).
1.8. Analysis.
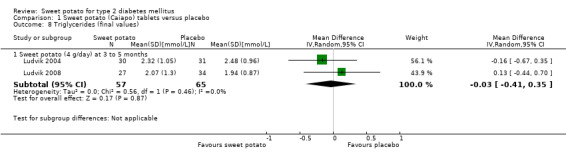
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 8 Triglycerides (final values).
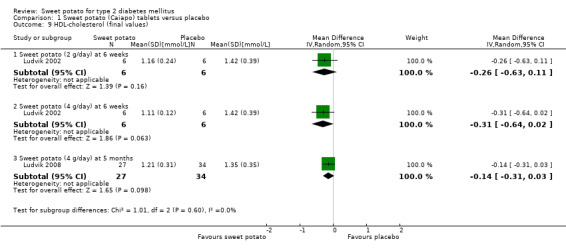
There were also no statistically significant changes between the sweet potato tablets intervention and placebo groups for both LDL‐ and HDL‐cholesterol levels (Analysis 1.9; Analysis 1.10).
1.9. Analysis.
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 9 HDL‐cholesterol (final values).
1.10. Analysis.
Comparison 1 Sweet potato (Caiapo) tablets versus placebo, Outcome 10 LDL‐cholesterol (final values).
Death from any cause, functional outcomes, health‐related quality of life, well‐being and costs
None of the publications assessed death from any cause, functional outcomes, health‐related quality of life, well being or costs.
Timing of outcome measurements
One study reported outcomes at a one month interval between measurements of endpoints (Ludvik 2004). The other two studies reported outcomes measured at the end of study (Ludvik 2002; Ludvik 2008).
Subgroup analysis
We did not perform subgroup analyses due to the small number of included studies.
Sensitivity analyses
We did not perform sensitivity analyses due to the small number of included studies.
Publication and small study bias
Drawing of funnel plots was not possible due to the small number of included studies.
Discussion
The aim of this review was to assess the effects of sweet potato (Ipomoea batatas) for type 2 diabetes mellitus (T2DM).
Summary of main results
We included three trials with 140 participants who had T2DM. The findings are presented in the Table 1. The mean duration of treatment was 3.2 months. The trials included in this review measured surrogate outcomes and evaluated adverse events (Appendix 5; Appendix 6; Appendix 7; Appendix 8; Appendix 9; Appendix 10; Appendix 11). Compared with placebo, the sweet potato tablets did not show any significant improvement in blood glucose control in terms of normalisation, or a reduction in fasting blood glucose with a low dose of 2 g/day for six weeks. However, there was a statistically significant improvement in fasting blood glucose and glycosylated haemoglobin A1c (HbA1c) with an increased dose of 4 g/day of sweet potato tablets (Analysis 1.1; Analysis 1.3). There was no documentation of serious adverse events or adverse events due to participants dropping‐out of the trials. There were suggestions of improved insulin sensitivity (Appendix 13). There were also no statistically significant changes in body weight, body mass index or lipid profiles.
However, one needs to exercise caution when interpreting these findings. Generally, the effect estimates were small. In addition to the low methodological quality of the publications, there were no data provided on diabetic complications and morbidity, functional outcomes, health‐related quality of life, well‐being, death from any cause or costs.
Overall completeness and applicability of evidence
All three trials selected for this review were conducted by the same author and used similar proprietary sweet potato (Caiapo) preparations in the interventions. No details of the type of placebos used were reported. Furthermore, the time points for assessment of the effects of intervention for the three trials differed. These time points ranged from six weeks (Ludvik 2002), to five months (Ludvik 2004; Ludvik 2008). No data on outcomes were available beyond five months. There were also no relevant data for identical time points that could be extracted from these publications. Therefore, at present there are insufficient data to assess adequately the benefit: risk ratio of sweet potato for T2DM.
Quality of the evidence
All three trials had an unclear risk of bias in at least two domains (selection and performance biases). There was insufficient information about randomisation and blinding methods. Most of the pre‐specified outcomes were objectively measured and were reported. The main limitations were the lack of information on the implementation of the randomisation and blinding processes. Furthermore, the small sample size and number of events in each trial were affected by greater sampling variation, which is reflected in the large confidence intervals of the effect estimates.
Potential biases in the review process
There are several limitations with this systematic review: firstly, the small number of trials published. Furthermore, all these trials showed findings of beneficial effects of the specific sweet potato preparation on glucose metabolism. Apart from possible publication bias, other biases may have occurred during the selection of participants, administration of treatment, and assessment of outcomes. Therefore, inadequate reporting of the processes of randomisation and blinding may be associated with exaggerated effects of the interventions. Moreover, less methodologically‐rigorous trials tend to show significantly larger intervention effects than more rigorous trials (Egger 2003; Kjaergard 2001; Moher 1998; Schulz 1995).
Secondly, the small sample size of the trials, which leads to diminished power of the results, may explain the small differences in effect estimate between the interventions and placebo. In other words, due to the size of these trials, the analyses may not establish with confidence that the two interventions have equivalent effects (Piaggio 2001; Pocock 1991). Thirdly, all the trials reported end‐of‐treatment values that ranged from six weeks to five months, and long‐term responses beyond this period are not known. Fourthly, there were insufficient data about adverse events from two trials (Ludvik 2004; Ludvik 2008). As a result, the incidence of adverse events cannot be differentiated clearly between the sweet potato intervention and placebo. Fifthly, similar sweet potato preparations were used in the intervention arms and the efficacy of other sweet potato nutraceuticals is not known. Finally, although none of the trials provided information on ethnicity of the participants, the recruitment of participants was limited to the European population. Thus, the validity and applicability of the results to other ethnic groups or populations is not known.
Agreements and disagreements with other studies or reviews
Previous reviews focused on experimental studies of animal models and the use of sweet potato in promoting health in humans. There has been no systematic review of the effects of sweet potato on T2DM. This review included three available RCTs. The relatively small sample and effect estimates unfortunately do not provide sufficient evidence for any reliable conclusion of the potential benefits or harmful effects of sweet potato for T2DM.
Authors' conclusions
Implications for practice.
There is insufficient evidence about the use of sweet potato for type 2 diabetes mellitus (T2DM).
Implications for research.
Although there is reasonable evidence from animal models and clinical trials, including randomised controlled trials (RCTs), for suggesting that the sweet potato nutraceuticals may help in the management of T2DM, there are methodological issues: only one type of tablet derived from the tuber of a specific variety of sweet potato was tested in these RCTs. The results of the trials were from a predominantly European population and of relatively short duration (five months or less). Furthermore, these trials had a low power due to small sample sizes. RCTs with sample sizes that provide adequate power, of longer duration and in different T2DM populations would be useful to assess the efficacy of this nutraceutical further. The methods for detecting and monitoring, as well as the clarity of reporting of adverse effects also need to be scrutinised.
There are many other varieties of sweet potato. In addition to the tuber, other parts of the plants may be useful in glycaemic control. However, the complex issues surrounding differences and contaminants from growing, harvesting and processing the plant, as well as climatic variations may affect the characterisation as well as the production of reliable and consistently effective products (WHO 2007). In turn, this may undermine the therapeutic usefulness of products derived from this plant in glycaemic control in mainstream medicine. In addition to teasing out these issues, cost‐benefit evaluation may also be useful.
Research into the effects of sweet potato on long‐term complications of T2DM in humans is still unavailable. The presence of confounders, variations in the diet, as well as the difficulty in recording dietary intake over a long period make it difficult to interpret these complications when present.
The contribution of the highly nutritious sweet potato plant to the health of the healthy population is well‐recognised. However, the effects of sweet potato in the diet of people with T2DM need to be evaluated, particularly in parts of the world where it is common to use many varieties of this vegetable. For reliable conclusions, observational trials and RCTs of short‐, intermediate‐ and long‐term use need to be large and of rigorous quality.
Feedback
New feedback, 9 October 2013
Summary
The authors of this review treated the SD in the Ludvik 2004 article as SEM and converted them accordingly to do the meta‐analysis and did the opposite to the Ludvik 2008 article in one analysis. Because the SD in the 2004 article was so small in comparison with the Ludvik 2002 and Ludvik 2008 articles, I agree with the authors that the SD in the 2004 article was most likely SEM, but I could not find conclusive evidence that these numbers were SEM rather than SD. In the 2002 (p.239, right lines 18‐19) and 2008 (p.588, right line 11) articles, it was stated that all data were presented as mean ± SEM but the methods section and the legend of the relevant tables in the 2004 article explicitly stated that all data were presented as mean ± SD (p.437, statistics section and legends of both tables). Should the authors treat them as SD even though the authors said they were SEM? On the other hand, the numbers in the 2008 article were labeled as SEM but entered into the review as SD in some analyses (p.28, analysis 1.1) but not in others.
All three included articles compared the effect of Ipomoea batatas (Caiapo) by comparing the biochemical measures at the end of the trial. This review seemed to agree with this reasoning and synthesized the data accordingly. One could argue that this comparison was reasonable because randomization would balance the biochemical measures in each group, so there was no difference between the groups at the beginning of the trial. There are two reasons this was a suboptimal analysis of the data. First, equal biochemical measures between the groups was always achieved by randomization, especially in small groups. This was best illustrated in the 2002 article when Ludvik et al stated “this pilot study shows beneficial effects of high‐dose caiapo on plasma glucose and total as well as LDL‐cholesterol levels in patients with type 2 diabetes.” Inspection of the table 1 in the 2002 article showed the effect of high dose Caiapo treatment on total cholesterol was greatly inflated by the different baseline levels (6.05 vs. 4.97) in these two groups. The actual difference between low and high dose of Caiapo was close (0.37 vs. 0.52) and neither would have been statistically significant. Second, perhaps more importantly in general, treating related samples as independent samples wastes information and increases the variation of the measurements. This is a well described experimental design that should be analyzed with repeated measures tests in elementary statistics, yet many clinical trials do not seem to be aware of this method. Measuring the change in each individual before and after treatment greatly reduces the variance due to interpersonal variation. This effect will almost always increase the power of the trial. To see the magnitude of this effect, one can see table 3 of the article by Akilen[1] as an example (this second paragraph is trying to make a point similar to part of the comment I sent regarding CD007170 but with more detail).
References:
1. Akilen R., Tsiami A., Devendra D., and Robinson N. Treatment glycated haemoglobin and blood pressure‐lowering effect of cinnamon in multi‐ethnic type 2 diabetic patients in the UK: a randomized, placebo‐controlled, double‐blind clinical trial. Diabetic Medicine 2010;27:1159–67.
Reply
In all the three articles, the authors specifically mentioned that the results were presented as SEM in the respective methodology sections. These results were converted to SD accordingly using the equation: SD= SEM x √n. In Ludvik 2004 and Ludvik 2008, the results were presented in mg/dL. To standardise the results across the three studies, we converted all the results to SI units (mmol/L).
On the second paragraph: power calculation was lacking in Ludvik 2002 and could not justify the small number of only six participants per group. In addition to other issues of methodological quality, there were flaws in the statistics used. Although repeated measures were used in this study, this small number does not satisfy the criteria of using parametric statistical tests. We did not include the changes in lipid levels of this study in our analysis as changes over six weeks are not clinically meaningful. Similarly, in Akilen 2010, power calculation was lacking, in addition to other issues of methodological quality and external validity of the study.
Our additional comments: Type 2 diabetes mellitus is pandemic in many countries, particularly, in Asia. The advancement in the research of type 2 diabetes mellitus has enhanced the understanding of the complex progressive multi‐pathophysiological nature of this disease that accelerates the aging process. For successful management, we need to consider issues beyond controlling glycaemia such as modifying cardiovascular risk factors as well as other risk factors for disability. Besides pharmacological management, non pharmacological means such as lifestyle modifications such like medical nutritional therapy, exercise and stop of smoking are also important. The increasing prevalence of patients in the younger age spectrum presents additional challenges. In view of the life‐long affliction of the disease, the need for long‐term complex treatments and the vulnerability of this population to irreversible disability that will escalate the burden of already pressured healthcare systems, the efficacies, benefits and safety of any new intervention for this disease need to be carefully scrutinised based on quality evidence.
Contributors
Jih‐I Yeh. Department of Family Medicine, Buddhist Tzu‐Chi General Hospital and Tzu‐Chi University, Hualien, Taiwan. Email: jihiyeh@gms.tcu.edu.tw.
For the authors: Cheow Peng.
What's new
| Date | Event | Description |
|---|---|---|
| 12 December 2013 | Feedback has been incorporated | New feedback incorporated |
History
Protocol first published: Issue 5, 2011 Review first published: Issue 2, 2012
| Date | Event | Description |
|---|---|---|
| 20 February 2013 | New search has been performed | New search: no additional studies could be included |
| 20 February 2013 | New citation required but conclusions have not changed | No additional studies could be included |
Appendices
Appendix 1. Search strategies
| Search terms and databases |
| Unless otherwise stated, search terms are free text terms '$': stands for any character; '?': substitutes one or no character; adj: adjacent (i.e. number of words within range of search term); exp: exploded MeSH; MeSH: medical subject heading (MEDLINE medical index term); pt: publication type; sh: MeSH; tw: text word. |
| The Cochrane Library |
| #1 MeSH descriptor Diabetes mellitus, type 2 explode all trees #2 MeSH descriptor Insulin resistance explode all trees #3 ( (impaired in All Text and glucose in All Text and toleranc* in All Text) or (glucose in All Text and intoleranc* in All Text) or (insulin* in All Text and resistanc* in All Text)) #4 (obes* in All Text near/6 diabet* in All Text) #5 (MODY in All Text or NIDDM in All Text or TDM2 in All Text) #6 ( (non in All Text and insulin* in All Text and depend* in All Text) or (noninsulin* in All Text and depend* in All Text) or (non in All Text and insulindepend* in All Text) or noninsulindepend* in All Text) #7 (typ* in All Text and (2 in All Text near/6 diabet* in All Text) ) #8 (typ* in All Text and (II in All Text near/6 diabet* in All Text) ) #9 (non in All Text and (keto* in All Text near/6 diabet* in All Text) ) #10 (nonketo* in All Text near/6 diabet* in All Text) #11 (adult* in All Text near/6 diabet* in All Text) #12 (matur* in All Text near/6 diabet* in All Text) #13 (late in All Text near/6 diabet* in All Text) #14 (slow in All Text near/6 diabet* in All Text) #15 (stabl* in All Text near/6 diabet* in All Text) #16 (insulin* in All Text and (defic* in All Text near/6 diabet* in All Text) ) #17 (plurimetabolic in All Text and syndrom* in All Text) #18 (pluri in All Text and metabolic in All Text and syndrom* in All Text) #19 (#1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10) #20 (#11 or #12 or #13 or #14 or #15 or #16 or #17 or #18) #21 (#19 or #20) #22 MeSH descriptor Diabetes insipidus explode all trees #23 (diabet* in All Text and insipidus in All Text) #24 (#22 or #23) #25 (#21 and not #24) #26 MeSH descriptor Ipomoea batatas explode all trees #27 MeSH descriptor Convolvulaceae explode all trees #28 Convolvulaceae in All Text #29 ( (sweet in All Text and potato in All Text) #30 (ipomoea in All Text and batatas in All Text) #31 (#26 or #27 or #28 or #29 or #30) #32 (#25 and #31) |
| MEDLINE |
| 1. ipomoea batatas.mp. 2. sweet potato.mp. 3. Convolvulaceae.mp. 4. or/1‐3 5. exp Diabetes Mellitus, Type 2/ 6. exp Insulin Resistance/ 7. exp Glucose Intolerance/ 8. (impaired glucos$ toleranc$ or glucos$ intoleranc$ or insulin resistan$).tw,ot. 9. (obes$ adj3 diabet$).tw,ot. 10. (MODY or NIDDM or T2DM).tw,ot. 11. (non insulin$ depend$ or noninsulin$ depend$ or noninsulin?depend$ or noninsulin?depend$).tw,ot. 12. ((typ? 2 or typ? II or typ?2 or typ?II) adj3 diabet$).tw,ot. 13. ((keto?resist$ or non?keto$) adj6 diabet$).tw,ot. 14. (((late or adult$ or matur$ or slow or stabl$) adj3 onset) and diabet$).tw,ot. 15. or/5‐14 16. exp Diabetes Insipidus/ 17. diabet$ insipidus.tw,ot. 18. 16 or 17 19. 15 not 17 20. 4 and 19 21. randomized controlled trial.pt. 22. controlled clinical trial.pt. 23. randomi?ed.ab. 24. placebo.ab. 25. drug therapy.fs. 26. randomly.ab. 27. trial.ab. 28. groups.ab. 29. or/21‐28 30. Meta‐analysis.pt. 31. exp Technology Assessment, Biomedical/ 32. exp Meta‐analysis/ 33. exp Meta‐analysis as topic/ 34. hta.tw,ot. 35. (health technology adj6 assessment$).tw,ot. 36. (meta analy$ or metaanaly$ or meta?analy$).tw,ot. 37. ((review$ or search$) adj10 (literature$ or medical database$ or medline or pubmed or embase or cochrane or cinahl or psycinfo or psyclit or healthstar or biosis or current content$ or systemat$)).tw,ot. 38. or/30‐37 39. (comment or editorial or historical‐article).pt. 40. 38 not 39 41. 29 or 40 42. 20 and 41 43. (animals not (animals and humans)).sh. 44. 42 not 43 |
| EMBASE |
| 1. exp Ipomoea batatas extract/ or exp Ipomoea batatas/ 2. sweet potato.tw,ot. 3. Convolvulaceae.tw,ot. 4. or/1‐3 5. exp Diabetes Mellitus, Type 2/ 6. exp Insulin Resistance/ 7. (MODY or NIDDM or T2D or T2DM).tw,ot. 8. ((typ? 2 or typ? II or typ?II or typ?2) adj3 diabet*).tw,ot. 9. (obes* adj3 diabet*).tw,ot. 10. (non insulin* depend* or non insulin?depend* or noninsulin* depend* or noninsulin?depend*).tw,ot. 11. ((keto?resist* or non?keto*) adj3 diabet*).tw,ot. 12. ((adult* or matur* or late or slow or stabl*) adj3 diabet*).tw,ot. 13. (insulin* defic* adj3 relativ*).tw,ot. 14. insulin* resistanc*.tw,ot. 15. or/5‐14 16. exp Diabetes Insipidus/ 17. diabet* insipidus.tw,ot. 18. 16 or 17 19. 15 not 18 20. 4 and 19 21. exp Randomized Controlled Trial/ 22. exp Controlled Clinical Trial/ 23. exp Clinical Trial/ 24. exp Comparative Study/ 25. exp Drug comparison/ 26. exp Randomization/ 27. exp Crossover procedure/ 28. exp Double blind procedure/ 29. exp Single blind procedure/ 30. exp Placebo/ 31. exp Prospective Study/ 32. ((clinical or control$ or comparativ$ or placebo$ or prospectiv$ or randomi?ed) adj3 (trial$ or stud$)).ab,ti. 33. (random$ adj6 (allocat$ or assign$ or basis or order$)).ab,ti. 34. ((singl$ or doubl$ or trebl$ or tripl$) adj6 (blind$ or mask$)).ab,ti. 35. (cross over or crossover).ab,ti. 36. or/21‐35 37. exp meta analysis/ 38. (metaanaly$ or meta analy$ or meta?analy$).ab,ti,ot. 39. ((review$ or search$) adj10 (literature$ or medical database$ or medline or pubmed or embase or cochrane or cinahl or psycinfo or psyclit or healthstar or biosis or current content$ or systematic$)).ab,ti,ot. 40. exp Literature/ 41. exp Biomedical Technology Assessment/ 42. hta.tw,ot. 43. (health technology adj6 assessment$).tw,ot. 44. or/37‐43 45. (comment or editorial or historical‐article).pt. 46. 44 not 45 47. 36 or 46 48. 20 and 47 49. limit 48 to human |
| 'My NCBI' alert service |
| ("ipomoea batatas"[MeSH Terms] OR ("ipomoea"[All Fields] AND "batatas"[All Fields]) OR "ipomoea batatas"[All Fields] OR ("sweet"[All Fields] AND "potato"[All Fields]) OR "sweet potato"[All Fields]) AND ("diabetes mellitus"[MeSH Terms] OR ("diabetes"[All Fields] AND "mellitus"[All Fields]) OR "diabetes mellitus"[All Fields] OR "diabetes"[All Fields] OR "diabetes insipidus"[MeSH Terms] OR ("diabetes"[All Fields] AND "insipidus"[All Fields]) OR "diabetes insipidus"[All Fields]) |
| CINAHL |
| 1. MM "sweet potato" 2. MM "ipomoea batatas" 3. MM "Convolvulaceae" 4. #1 or #2 or #3 5. MM "insulin resistance" 6. MM "Diabetes Mellitus, Non‐Insulin‐Dependent" 7. TX Diabetes Complications 8. TX MODY or NIDDM or T2DM 9. TX non insulin* depend* or noninsulin* depend* or noninsulin?depend* or non insulin?depend 10. TX diabet* N3 (typ* 2 or typ* II) 11. TX diabet* N6 (keto*resist* or non*keto* 12. TI (onset N3 (late or adult* or matur* or slow or stabl*)) and TI diabet* 13. AB (onset N3 (late or adult* or matur* or slow or stabl*)) and AB diabet* 14. TI (insulin* defic* or relativ*) 15. AB (insulin* defic* or relativ*) 16. TI (insulin* resistanc*) 17. AB (insulin* resistanc*) 18. #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 19. MM "Diabetes Insipidus" 20. TX diabet* insipidus 21. # 19 or #20 22. #18 NOT #21 23. #4 and #22 24. TX Meta‐analysis 25. TX Technology Assessment, Biomedical 26. #24 or #25 27. TX comment or editorial or historical‐article 28. #26 NOT #27 29. AB randomized controlled trial 30. AB controlled clinical trial 31. AB cross over OR crossover 32. TX random* OR blind* OR placebo* OR group* 33. TX animal* NOT (animal* AND human*) 34. #29 or #30 or #31 or #32 35. #34 NOT #33 36. #28 or #35 37. #23 and #36 |
| LILACS |
| 1. (sweet potato or ipomoea batatas or Convolvulaceae) [Subject descriptor] and 2. (Diabetes mellitus or insulin resistance) [Palavras] and 3. (random$ or placebo$ or trial or group$) [Palavras] Natural medicines comprehensive database 1. sweet potato, diabetes 2. ipomoea batatas, diabetes 3. Convolvulaceae, diabetes |
| OpenGrey |
| 1. (sweet potato or ipomoea batatas or Convolvulaceae) [Abstract] and 2. (Diabetes mellitus or insulin resistance) [Abstract] and 3. (random or placebo or trial or group) [Abstract] |
| Natural Medicines Comprehensive Databas |
| 1. sweet potato, diabetes 2. ipomoea batatas, diabetes 3. Convolvulaceae, diabetes |
| Proquest Dissertations and Theses database |
| 1. ("sweet potato") OR (“sweet potato”) OR ("convolvulaceae") Citation and document text 2. ("typ* 2") OR ("typ* II") OR ("late") OR ("maturity") OR ("n???insulin") AND ("diabet*") Citation and document text 3. (NIDDM*) OR (MODY*) OR (TIIDM) OR (T2DM) Citation and document text 4. ((("typ* 2") OR ("typ* II") OR ("late") OR ("maturity") OR ("n???insulin") AND ("diabet*")) OR ((NIDDM*) OR (MODY*) OR (TIIDM) OR (T2DM))) AND ((("sweet potato") OR (“sweet potato”) OR ("convolvulaceae"))) Citation and document text |
Appendix 2. Description of interventions
| Characteristic | Intervention(s) [route, frequency, total dose/day] | Comparator(s) [route, frequency, total dose/day] |
| Ludvik 2002 | I1: sweet potato (Caiapo) tablets: oral; 2 g 3 times/day | C: placebo; oral; 3 times/day |
| I2: sweet potato (Caiapo) tablets: oral; 4 g 3 times/day | ||
| Ludvik 2004 | I: sweet potato (Caiapo) tablets: oral; once daily; 4 g/day | C: placebo; oral; 3 times/day |
| Ludvik 2008 | I: sweet potato (Caiapo) tablets: oral; once daily; 4 g/day | C: placebo; oral; 3 times/day |
|
Footnotes C: comparator; I: intervention | ||
Appendix 3. Baseline characteristics (I)
| Characteristic | Intervention(s) and comparator(s) [dosage per day] | Duration of intervention (duration of follow‐up) | Participating population | Study period [year to year] | Country | Setting | Duration of diabetes [mean years (SD)] |
| Ludvik 2002 | I1: sweet potato (Caiapo) tablets 2 g | 6 weeks (6 weeks) | Male participants with T2DM on diet | ‐ | Austria | ‐ | ‐ |
| I2: sweet potato (Caiapo) tablets 4 g | 6 weeks (6 weeks) | ||||||
| C: placebo | 6 weeks (6 weeks) | ||||||
| Ludvik 2004 | I: sweet potato (Caiapo) tablets 4 g | 3 months (3 months) | People with T2DM on diet | ‐ | Switzerland | Outpatients (offices of general practitioners) | ‐ |
| C: placebo | 3 months (3 months) | ||||||
| Ludvik 2008 | I: sweet potato (Caiapo) tablets 4 g | 5 months (5 months) | People with T2DM | ‐ | Austria and Germany | Outpatients clinics | 3.5 (4.2) |
| C: placebo | 5 months (5 months) | 4.2 (2.9) | |||||
|
Footnotes "‐" denotes not reported C: comparator; I: intervention; SD: standard deviation; T2DM: type 2 diabetes mellitus | |||||||
Appendix 4. Baseline characteristics (II)
| Characteristic | Intervention(s) and comparator(s) | Sex [female %] | Age [mean years (SD)] | HbA1c [%] | BMI [mean kg/m2 (SD)] | Co‐medications/ co‐interventions | Co‐morbidities |
| Ludvik 2002 | I1: sweet potato (Caiapo) tablets 2 g | 0 | ‐ | 7.3 (1.0) | 25.5 (2.0) | ‐ | ‐ |
| I2: sweet potato (Caiapo) tablets 4 g | 0 | ‐ | 7.1 (0.7) | 28.6 (3.2) | |||
| C: placebo | 0 | ‐ | 7.0 (0.7) | 28.9 (2.2) | |||
| All: | 0 | 58 (8) | 27.7 (11.5) | ||||
| Ludvik 2004 | I: sweet potato (Caiapo) tablets 4 g | 50 | 55.2 (2.1) | 7.2 (0.8) | 28.2 (2.2) | ‐ | ‐ |
| C: placebo | 38.7 | 55.6 (1.5) | 7.0 (1) | 27.6 (1.7) | |||
| All: | 44.3 | 55.2 (16.4) | |||||
| Ludvik 2008 | I: sweet potato (Caiapo) tablets 4 g | 48.1 | 57.2 (9.35) | 6.5 (0.6) | 31.1 (3.7) | ‐ | ‐ |
| C: placebo | 47.1 | 61.1 (8.7) | 6.3 (0.6) | 29.9 (3.5) | |||
| All: | 47.5 | 59.4 (10.2) | |||||
| Footnotes "‐" denotes not reported C: comparator; I: intervention; SD: standard deviation | |||||||
Appendix 5. Matrix of study endpoints (publications)
| Characteristic | Endpoint reported in publication | Endpoint not reported in publication | Time of measurementa | |
| Ludvik 2002 | Review's primary outcomes | |||
| Gycaemic control | x | 0, 1.5 months | ||
| Morbidity | x | |||
| Adverse effects | x | 0, 1.5 months | ||
| Review's secondary outcomes | ||||
| Serum insulin, C‐peptide or insulin sensitivity | x | |||
| Body weight or BMI | x | 0, 1.5 months | ||
| Lipids (total, LDL‐ and HDL‐cholesterol; triglycerides) | x | 0, 1.5 months | ||
| Health‐related quality of life | x | |||
| Well‐being | x | |||
| Physical and cognitive function | x | |||
| Costs | x | |||
| Other than review's primary/secondary outcomes reported in publication (classification: P/S/O)b | ||||
| Blood pressure (S): 0, 1.5 mo | ||||
| Subgroups reported in publication | ||||
| ‐ | ||||
| Ludvik 2004 | Review's primary outcomes | |||
| Gycaemic control | x | 0, 2, 3 mo | ||
| Morbidity | x | |||
| Adverse effects | x | 0, 2, 3 mo | ||
| Review's secondary outcomes | ||||
| Serum insulin, C‐peptide or insulin sensitivity | x | |||
| Body weight or BMI | x | 0, 2, 3 mo | ||
| Lipids (total, LDL‐ and HDL‐cholesterol; triglycerides) | x | 0, 2, 3 mo | ||
| Health‐related quality of life | x | |||
| Well‐being | x | |||
| Physical and cognitive function | x | |||
| Costs | x | |||
| Outcomes other than review's primary/secondary outcomes reported in publication (classification: P/S/O)b | ||||
| Blood pressure: 0, 2, 3 months | ||||
| Subgroups reported in publication | ||||
| ‐ | ||||
| Ludvik 2008 | Review's primary outcomes | |||
| Gycaemic control | x | 0, 5 months | ||
| Morbidity | x | |||
| Adverse effects | x | 0, 5 months | ||
| Review's secondary outcomes | ||||
| Serum insulin, C‐peptide or insulin sensitivity | x | 0, 5 months | ||
| Body weight or BMI | x | |||
| Lipids (total, LDL‐ and HDL‐cholesterol; triglycerides) | x | 0, 5 months | ||
| Health‐related quality of life | x | |||
| Well‐being | x | |||
| Physical and cognitive function | x | |||
| Costs | x | |||
| Other than review's primary/secondary outcomes reported in publication (classification: P/S/O)b | ||||
| Adiponectin, fibrinogen: 0, 5 months | ||||
| Subgroups reported in publication | ||||
|
Footnotes aUnderlined data denote times of measurement for primary and secondary review outcomes, if measured and reported in the results section of the publication (other times represent planned but not reported points in time) b(P) Primary or (S) secondary endpoint(s) refer to verbatim statements in the publication, (O) other endpoints relate to outcomes which were not specified as 'primary' or 'secondary' outcomes in the publication BMI: body mass index; HDL: high‐density lipoprotein; LDL: low‐density lipoprotein; N/A: not applicable | ||||
Appendix 6. Matrix of study endpoints (protocol/trial documents)
|
Characteristic/ Study ID (trial identifier) |
Endpoint | Time of measurement |
| Ludvik 2002 | Glycaemic control (P) | 0, 1.5 months |
| Serum insulin, C‐peptide or insulin sensitivity (S) | 0, 1.5 months | |
| Serum cholesterol (S) | 0, 1.5 months | |
| Weight (S) | 0, 1.5 months | |
| Adverse events (O) | 0, 1.5 months | |
| Ludvik 2004 | Glycaemic control (P) | 0, 2, 3 months |
| Serum cholesterol and triglyceride (S) | 0, 2, 3 months | |
| Adverse events (O) | 0, 2, 3 months | |
| Ludvik 2008 | Glycaemic control (P) | 0, 5 months |
| Serum cholesterol and triglyceride (S) | 0, 5 months | |
| Adverse events (O) | 0, 5 months | |
|
Footnotes aEndpoint in bold/italic = review's primary/secondary outcome b(P) Primary or (S) secondary endpoint(s) refer to verbatim statements in the publication, (O) other endpoints relate to outcomes that were not specified as 'primary' or 'secondary' outcomes in the report | ||
Appendix 7. Definition of endpoint measurement (I)
| Characteristic | Glycaemic control | Morbidity | Severe / serious adverse events | Insulin sensitivity | Health‐related quality of life | Well‐being | Physical function | Cognitive function |
| Ludvik 2002 | Change in fasting blood glucose and HbA1c | ‐ | ND | ND | ‐ | ‐ | ‐ | ‐ |
| Ludvik 2004 | Change in fasting blood glucose and HbA1c | ‐ | ND | ND | ‐ | ‐ | ‐ | ‐ |
| Ludvik 2008 | Changes in HbA1c | ‐ | ND | Oral glucose insulin sensitivity (OGIS), as glucose clearance from oral glucose tolerance test | ‐ | ‐ | ‐ | ‐ |
|
Footnotes "‐" denotes not reported HbA1c: glycosylated haemoglobin A1c; ND: not defined | ||||||||
Appendix 8. Definition of endpoint measurement (II)
|
Characteristic Study ID |
Mild hypoglycaemia | Moderate hypoglycaemia | Severe hypoglycaemia | Nocturnal hypoglycaemia |
| Ludvik 2002 | ND | ND | ND | ND |
| Ludvik 2004 | ND | ND | ND | ND |
| Ludvik 2008 | ND | ND | ND | ND |
|
Footnotes ND: not defined | ||||
Appendix 9. Adverse events (I)
| Characteristic | Intervention(s) and comparator(s) | Deaths [N] | Deaths [%] | All adverse events [N] | All adverse events [%] | Severe/serious adverse events [N] | Severe/serious adverse events [%] |
| Ludvik 2002 | I1: sweet potato (Caiapo) tablets 2 g | 0 | 0 | "No adverse events have been reported by the patients" | ‐ | ‐ | ‐ |
| I2: sweet potato (Caiapo) tablets 4 g | 0 | 0 | |||||
| C: placebo | 0 | 0 | |||||
| Ludvik 2004 | I: sweet potato (Caiapo) tablets 4 g | 0 | 0 | 16/30 | 53.3 | ‐ | ‐ |
| C: placebo | 0 | 0 | 14/31 | 45.2 | ‐ | ‐ | |
| Ludvik 2008 | I: sweet potato (Caiapo) tablets 4 g | 0 | 0 | ‐ | ‐ | ‐ | ‐ |
| C: placebo | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
|
Footnotes "‐" denotes not reported C: comparator; I: intervention | |||||||
Appendix 10. Adverse events (II)
| Characteristic | Intervention(s) and comparator(s) | Left study due to adverse events [N] | Left study due to adverse events [%] | Hospitalisation [N] | Hospitalisation [%] | Out‐patient treatment [N] | Out‐patient treatment [%] |
| Ludvik 2002 | I1: sweet potato (Caiapo) tablets 2 g | 0 | 0 | ‐ | ‐ | ‐ | ‐ |
| I2: sweet potato (Caiapo) tablets 4 g | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
| C: placebo | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
| Ludvik 2004 | I: sweet potato (Caiapo) tablets (4 g per day) | 0 | 0 | ‐ | ‐ | ‐ | ‐ |
| C: placebo | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
| Ludvik 2008 | I: sweet potato (Caiapo) tablets (4 g per day) | 0 | 0 | ‐ | ‐ | ‐ | ‐ |
| C: placebo | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
|
Footnotes "‐" denotes not reported C: comparator; I: intervention | |||||||
Appendix 11. Adverse events (III)
| Characteristic | Intervention(s) and comparator(s) | Specific adverse events [description] | Specific adverse events [N] | Specific adverse events [%] |
| Ludvik 2002 | I1: sweet potato (Caiapo) tablets 2 g | ‐ | ‐ | ‐ |
| I2: sweet potato (Caiapo) tablets 4 g | ‐ | ‐ | ‐ | |
| C: placebo | ‐ | ‐ | ‐ | |
| Ludvik 2004 | I: sweet potato (Caiapo) tablets 4 g | ‐ | ‐ | ‐ |
| C: placebo | ‐ | ‐ | ‐ | |
| Ludvik 2008 | I: sweet potato (Caiapo) tablets 4 g | ‐ | ‐ | ‐ |
| C: placebo | ‐ | ‐ | ‐ | |
|
Footnotes "‐" denotes not reported C: comparator; I: intervention | ||||
Appendix 12. Survey of authors providing information on trials
| Characteristic | Study author contacted | Study author replied | Study author asked for additional information | Study author provided data |
| Ludvik 2002 | Y | N | N/A | N/A |
| Ludvik 2004 | Y | N | N/A | N/A |
| Ludvik 2008 | Y | N | N/A | N/A |
|
Footnotes N: no; N/A: not applicable; Y: yes | ||||
Appendix 13. Beta‐cell function and insulin sensitivity
| Parameter | Mean change (SE) | Between‐group difference (SE) | P value | Comments | |
| Sweet potato (Caiapo) tablet | Placebo | ||||
| Glucose AUC (g/dL) in 180 min | ‐4.17 (1.04) | 0.68 (0.83) | ‐4.85 (1.33) | 0.0001 | Significant reduction in the Caiapo intervention group |
| Insulin AUC (mU/mL) in 180 min | ‐3.16 (1.04) | ‐0.99 (0.79) | ‐2.16 (1.31) | 0.013 | Significant reduction in the Caiapo intervention group |
| OGIS (ml/m2/min) | 28 (12) | 6 (7) | 22 (14) | 0.034 | Significant increase in insulin sensitivity in the Caiapo intervention group |
| Insulinogenic index (uUINS/mgGLUC) | 32 (23) | ‐15 (12) | 47 (25) | 0.081 | No significant increase in insulin delivery to prevailing glucose level |
| Disposition index (common units) | 127 (68) | ‐54 (39) | 180 (79) | 0.026 | Significant increase in disposition index |
|
Footnotes: From Ludvik 2008 AUC: area under curve; GLUC: glucose; INS: insulin; min: minute(s); OGIS: oral glucose insulin sensitivity; SE: standard error | |||||
Data and analyses
Comparison 1. Sweet potato (Caiapo) tablets versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Fasting blood glucose (final values) | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Sweet potato (2 g/day) at 6 weeks | 1 | 12 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐2.23, 2.23] |
| 1.2 Sweet potato (4 g/day) at 6 weeks and below 3 months | 2 | 73 | Mean Difference (IV, Random, 95% CI) | ‐0.65 [‐1.43, 0.13] |
| 1.3 Sweet potato (4 g/day) at 3 to 5 months | 2 | 122 | Mean Difference (IV, Random, 95% CI) | ‐0.68 [‐0.84, ‐0.52] |
| 2 Postprandial blood glucose (final values) | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Sweet potato (4 g/day) at less than 3 months | 1 | 61 | Mean Difference (IV, Random, 95% CI) | ‐0.98 [‐2.07, 0.11] |
| 2.2 Sweet potato (4 g/day) at 3 months | 1 | 61 | Mean Difference (IV, Random, 95% CI) | ‐1.01 [‐2.19, 0.17] |
| 3 HbA1c (final values) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 Sweet potato (4 g/day) at 3 to 5 months | 2 | 122 | Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐0.57, ‐0.04] |
| 4 Fasting plasma insulin (final values) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 Sweet potato tablets (2 g/day) at 6 weeks | 1 | 12 | Mean Difference (IV, Random, 95% CI) | 0.30 [‐3.94, 4.54] |
| 4.2 Sweet potato tablets (4 g/day) at 6 weeks | 1 | 12 | Mean Difference (IV, Random, 95% CI) | 4.5 [‐0.93, 9.93] |
| 4.3 Sweet potato tablets (4 g/day) at 5 months | 1 | 61 | Mean Difference (IV, Random, 95% CI) | 1.11 [‐1.85, 4.07] |
| 5 Body weight (final values) | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 Sweet potato (4 g/day) at 3 months | 1 | 61 | Mean Difference (IV, Random, 95% CI) | ‐1.0 [‐5.32, 3.32] |
| 6 BMI (final values) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6.1 Sweet potato (4 g/day) at 6 weeks | 1 | 12 | Mean Difference (IV, Random, 95% CI) | ‐1.10 [‐4.43, 2.23] |
| 6.2 Sweet potato (4 g/day) at 5 months | 1 | 61 | Mean Difference (IV, Random, 95% CI) | 1.0 [‐0.81, 2.81] |
| 7 Total cholesterol (final values) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 7.1 Sweet potato (4 g/day) at 3 to 5 months | 2 | 122 | Mean Difference (IV, Random, 95% CI) | ‐0.47 [‐1.10, 0.16] |
| 8 Triglycerides (final values) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 8.1 Sweet potato (4 g/day) at 3 to 5 months | 2 | 122 | Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.41, 0.35] |
| 9 HDL‐cholesterol (final values) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 9.1 Sweet potato (2 g/day) at 6 weeks | 1 | 12 | Mean Difference (IV, Random, 95% CI) | ‐0.26 [‐0.63, 0.11] |
| 9.2 Sweet potato (4 g/day) at 6 weeks | 1 | 12 | Mean Difference (IV, Random, 95% CI) | ‐0.31 [‐0.64, 0.02] |
| 9.3 Sweet potato (4 g/day) at 5 months | 1 | 61 | Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.31, 0.03] |
| 10 LDL‐cholesterol (final values) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 10.1 Sweet potato (2 g/day) at 6 weeks | 1 | 12 | Mean Difference (IV, Random, 95% CI) | 0.02 [‐0.95, 0.99] |
| 10.2 Sweet potato (4 g/day) at 6 weeks | 1 | 12 | Mean Difference (IV, Random, 95% CI) | ‐1.06 [‐1.92, ‐0.20] |
| 10.3 Sweet potato (4 g/day) at 5 months | 1 | 61 | Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.60, 0.34] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ludvik 2002.
| Methods | Parallel RCT Randomisation ratio: 1:1 Superiority design |
|
| Participants |
Inclusion criteria: clinically stable T2DM on diet only Exclusion criteria: no information Diagnostic criteria: authors' criteria |
|
| Interventions |
Number of study centres: no information Treatment before study: diabetic diet Titration period: nil Experimental intervention groups:
Participants in each group received 4 tablets 3 times daily after meals for a period of 6 weeks. A total of 2 g and 4 g/day were ingested by participants in each group, respectively Control intervention: Placebo tablets. No information on the contents of these tablets All patients were on diet regimen during the study |
|
| Outcomes |
Outcomes reported in abstract of publication: Primary outcome(s): (as stated in the publication) change in fasting blood glucose Seondary outcome(s): (as stated in the publication) change in plasma insulin level, serum cholesterol and weight Additional outcome(s): incidence of adverse events |
|
| Study details |
Run‐in period: no information Was s tudy terminated early (for benefit/because of adverse events): no |
|
| Publication details |
Language of publication: English Commercial funding: grant from manufacturer Publication status: peer review journal |
|
| Stated aim of study | Quote from publication: "To assess the effect of caiapo on glucose metabolism, its tolerability and mode of action in male Caucasian type 2 diabetic patients". | |
| Notes | Letter to editor. Pilot study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote from publication: "randomised to receive placebo or 2 (low dose) or 4 g (high dose) caiapo" Comment: there was no description of generation of the random sequence; furthermore, reports of 2 other trials by the same principal investigators that used a similar intervention also provided no information about sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Comment: there was no information provided about the method of allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote from publication: "double‐blind" Comment: there was no other information available concerning blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comment: fasting blood glucose was specifically accessed at each visit for each participant |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: all participants completed the study, no treatment withdrawals or major adverse events reported |
| Selective reporting (reporting bias) | Low risk | Comment: primary outcomes were stated |
| Other bias | Unclear risk | Comment: there was no information about the sample size calculation or exclusion criteria; there was also insufficient information to assess other important risks of bias |
Ludvik 2004.
| Methods | Parallel RCT Randomisation ratio: 1:1 Superiority design |
|
| Participants |
Inclusion criteria: clinically stable T2DM on diet only Exclusion criteria: renal, hepatic, cardiovascular, hematological, respiratory, autoimmune, neurological diseases or other endocrine dysfunction that could interfere with the study Diagnostic criteria: authors' criteria |
|
| Interventions |
Number of study centres: no information Treatment before study: oral hypoglycaemic agents withdrawn 2 weeks before trial Titration period: nil Intervention group: 4 g of Caiopo (Ipomoea batatas) once daily Control intervention: Placebo tablets; no information provided regarding the content of these tablets All participants were on diet regimen during the study |
|
| Outcomes |
Outcomes reported in abstract of publication: Primary outcome(s): (as stated in the publication) change in fasting blood glucose and 2‐hour postprandial blood glucose; change in HbA1c Seondary outcome(s): (as stated in the publication) change in cholesterol and triglyceride levels Additional outcome(s): incidence of adverse events |
|
| Study details |
Run‐in period: 5 participants on antidiabetic medication (metformin and/or glibenclamide) had their medications withdrawn 2 weeks before the start of the study Was s tudy terminated early (for benefit/because of adverse events): no |
|
| Publication details |
Language of publication: English Commercial funding: grant from manufacturer Non‐commercial funding: nil Publication status: peer review journal |
|
| Stated aim of study | Quote from publication: "... assessment of the efficacy and tolerability of Caiapo (4 g/day) compared with placebo when administered for 12 consecutive weeks for type 2 diabetic patients ..." | |
| Notes | Original research journal article | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote from publication: "randomly divided into two groups" Comment: the process of randomisation was not specified |
| Allocation concealment (selection bias) | Unclear risk | Comment: there was no information about the adequacy of allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote from publication: "double‐blind" Comment: there was no other information available about blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comment: fasting blood glucose and HbA1c were specifically measured |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: all participants completed the study, no treatment withdrawals or major adverse events reported |
| Selective reporting (reporting bias) | Low risk | Comment: primary outcome measures were stated |
| Other bias | Low risk | Comment: none detected |
Ludvik 2008.
| Methods | Parallel RCT Randomisation ratio: 1:1 Superiority design |
|
| Participants |
Inclusion criteria: clinically stable T2DM on diet only Exclusion criteria: no information Diagnostic criteria: authors' criteria |
|
| Interventions |
Number of study centres: multiple centres (no information on exact number) Treatment before study: no hypoglycaemic drugs 4 weeks prior to baseline visit Titration period: nil Intervention group: 4 g of Caiopo (Ipomoea batatas) once daily Control intervention: Placebo tablets; no information provided about the content of these tablets All participants were on diet regimen during the study |
|
| Outcomes |
Outcomes reported in abstract of publication: Primary outcome(s): (as stated in the publication) change in fasting blood glucose and 2‐hour postprandial blood glucose; change in HbA1c Seondary outcome(s): (as stated in the publication) change in cholesterol and triglyceride levels Additional outcome(s): incidence of adverse events |
|
| Study details |
Run‐in period: medications that affect blood glucose levels such as corticosteroids, high‐dose diuretics or beta‐blockers were stopped during the 2 weeks prior to screening and for the duration of the study; screening for participants took place 1 month prior to start of study; hypoglycaemic drugs were withdrawn 4 weeks before the start of the study Was s tudy terminated early (for benefit/because of adverse events): no |
|
| Publication details |
Language of publication: English Commercial other funding: grant from manufacturer Non‐commercial funding: nil Publication status: peer review journal |
|
| Stated aim of study | Quote from publication: "To further evaluate the mode of action of Caiapo on insulin sensitivity over an extended period of time as well as the effects on fibrinogen and other markers of low‐grade inflammation". | |
| Notes | Original research journal article | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote from publication: "randomised" Comment: there was no information provided about the process used to generate the random sequence |
| Allocation concealment (selection bias) | Unclear risk | Comment: there was no information provided about the adequacy of allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote from publication: "double‐blind" Comment: there was no other information available about blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comment: the primary and secondary outcomes were measured objectively |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote from publication: "27/88 patients dropped out (due to pregnancy (1) and non‐compliance to follow‐up visits)" Comment: there was no information about the number of participants who dropped out of the intervention and the control groups |
| Selective reporting (reporting bias) | Low risk | Comment: important primary and secondary outcomes were adequately reported |
| Other bias | Low risk | Comment: none detected |
RCT: randomised controlled trial; T2DM: type 2 diabetes mellitus
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ludvik 2003 | The objective was evaluation of the mechanism of action of Ipomoea batatas and not the effects of the intervention on T2DM. This paper did not contain relevant outcome data for assessment |
T2DM: type 2 diabetes mellitus
Differences between protocol and review
The Cohen's kappa test for study selection, subgroup analysis and sensitivity analysis was not performed. We reported on outcomes of beta‐cell function and insulin sensitivity.
Contributions of authors
Cheow Peng Ooi (CPO): drafting, editing and submitting the review, designing search strategies and search for trials, selection of trials for inclusion/exclusion, extraction of data, entry of data; data analyses and data interpretations.
Seng Cheong Loke (SCL): independent input on trials selection,data analysis and data interpretations; input in drafting and general advice on the review.
Sources of support
Internal sources
Institute of Gerontology, Universiti Putra Malaysia, Malaysia.
External sources
No sources of support supplied
Declarations of interest
Cheow Peng Ooi: none known.
Seng Cheong Loke: none known.
Edited (no change to conclusions), comment added to review
References
References to studies included in this review
Ludvik 2002 {published data only}
- Ludvik BH, Mahdjoobian K, Waldhaeusl W, Hofer A, Prager R, Kautzky‐Willer A, et al. The effect of Ipomoea batatas (Caiapo) on glucose metabolism and serum cholesterol in patients with type 2 diabetes: a randomized study. Diabetes Care 2002;25(1):239‐40. [DOI] [PubMed] [Google Scholar]
Ludvik 2004 {published data only}
- Ludvik B, Neuffer B, Pacini G. Efficacy of Ipomoea batatas (Caiapo) on diabetes control in type 2 diabetic subjects treated with diet. Diabetes Care 2004;27(2):436‐40. [DOI] [PubMed] [Google Scholar]
Ludvik 2008 {published data only}
- Ludvik B, Hanefeld M, Pacini G. Improved metabolic control by Ipomoea batatas (Caiapo) is associated with increased adiponectin and decreased fibrinogen levels in type 2 diabetic subjects. Diabetes Obesity and Metabolism 2008;10(7):586‐92. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Ludvik 2003 {published data only}
- Ludvik B, Waldhausl W, Prager R, Kautzky‐Willer A, Pacini G. Mode of action of ipomoea batatas (Caiapo) in type 2 diabetic patients. Metabolism 2003;52(7):875‐80. [DOI] [PubMed] [Google Scholar]
Additional references
Abbatecola 2009
- Abbatecola AM, Paolisso G. Diabetes care targets in older persons. Diabetes Research and Clinical Practice 2009;86 Suppl 1:S35‐40. [DOI] [PubMed] [Google Scholar]
Abegunde 2007
- Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and costs of chronic diseases in low‐income and middle‐income countries. The Lancet 2007;370(9603):1929‐38. [DOI] [PubMed] [Google Scholar]
ADA 1999
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 1999;22(Suppl 1):S5‐19. [DOI] [PubMed] [Google Scholar]
ADA 2008
- American Diabetes Association. Standards of medical care in diabetes ‐ 2008. Diabetes Care 2008;31(Suppl 1):S12‐54. [DOI] [PubMed] [Google Scholar]
Almazan 1998
- Almazan AM, Adeyeye SO. Fat and fatty acid concentrations in some green vegetables. Journal of Food Composition and Analysis 1998;11(4):375‐80. [Google Scholar]
Altman 2003
- Altman DG, Bland JM. Interaction revisited: the difference between two estimates. BMJ (Clinical research ed.) 2003;326(7382):219. [DOI] [PMC free article] [PubMed] [Google Scholar]
Antia 2006
- Antia BS, Akpan EJ, Okon PA, Umoren IU. Nutritive and anti‐nutritive evaluation of sweet potatoes (Ipomoea batatas) leaves. Pakistan Journal of Nutrition 2006;5(2):166‐8. [Google Scholar]
Bantle 2008
- Bantle JP, Wylie‐Rosett J, Albright AL, Apovian CM, Clark NG, Franz MJ, et al. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care 2008;31(Suppl 1):S61‐78. [DOI] [PubMed] [Google Scholar]
Bruce 2005
- Bruce DG, Davis WA, Davis TM. Longitudinal predictors of reduced mobility and physical disability in patients with type 2 diabetes: the Fremantle Diabetes Study. Diabetes Care 2005;28(10):2441‐7. [DOI] [PubMed] [Google Scholar]
Chan 2009
- Chan JC, Malik V, Jia W, Kadowaki T, Yajnik CS, Yoon KH, et al. Diabetes in Asia: epidemiology, risk factors, and pathophysiology. JAMA 2009;301.(20):2129‐40. [DOI] [PubMed] [Google Scholar]
De Rekeneire 2003
- Rekeneire N, Resnick HE, Schwartz AV, Shorr RI, Kuller LH, Simonsick EM, et al. Diabetes is associated with subclinical functional limitation in non‐disabled older individuals: the Health, Aging, and Body Composition study. Diabetes Care 2003;26(12):3257‐63. [DOI] [PubMed] [Google Scholar]
Duke 1981
- Duke JA, Wain KK. Medicinal plants of the world. Computer index with more than 85,000 entries. Longman Group UK Limited, 1981. [Google Scholar]
Egert 2009
- Egert S, Bosy‐Westphal A, Seiberl J, Kurbitz C, Settler U, Plachta‐Danielzik S, et al. Quercetin reduces systolic blood pressure and plasma oxidised low‐density lipoprotein concentrations in overweight subjects with a high‐cardiovascular disease risk phenotype: a double‐blinded, placebo‐controlled cross‐over study. British Journal of Nutrition 2009;102(7):1065‐74. [DOI] [PubMed] [Google Scholar]
Egger 2003
- Egger M, Juni P, Bartlett C, Holenstein F, Sterne J. How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study. Health Technology Assessment 2003;7(1):1–76. [PubMed] [Google Scholar]
Genser 2008
- Genser D. Food and drug interaction: consequences for the nutrition/health status. Annals of Nutrition and Metabolism 2008;52(Suppl 1):29‐32. [DOI] [PubMed] [Google Scholar]
Gregg 2002
- Gregg EW, Mangione CM, Cauley JA, Thompson TJ, Schwartz AV, Ensrud KE, et al. Diabetes and incidence of functional disability in older women. Diabetes Care 2002;25(1):61‐7. [DOI] [PubMed] [Google Scholar]
Grossman 2010
- Grossman EJ, Lee DD, Tao J, Wilson RA, Park SY, Bell GI, et al. Glycemic control promotes pancreatic beta‐cell regeneration in streptozotocin‐induced diabetic mice. PloS One 2010;5(1):e8749. [DOI] [PMC free article] [PubMed] [Google Scholar]
Grover 2002
- Grover JK, Yadav S, Vats V. Medicinal plants of India with anti‐diabetic potential. Journal of Ethnopharmacology 2002;81(1):81‐100. [DOI] [PubMed] [Google Scholar]
Higgins 2002
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21:1539‐58. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analysis. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2009
- Higgins JPT, Thompson SG, Spiegelhalter DJ. A re‐evaluation of random‐effects meta‐analysis. Journal of the Royal Statistical Society: Series A (Statistics in Society) 2009;172(1):137‐59. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Huang 2007
- Huang Z, Wang B, Eaves DH, Shikany JM, Pace RD. Phenolic compound profile of selected vegetables frequently consumed by African Americans in the southeast United States. Food Chemistry 2007;103(4):1395‐402. [Google Scholar]
Islam 2002
- Islam MS, Yoshimoto M, Terahara N, Yamakawa O. Anthocyanin compositions in sweet potato (Ipomoea batatas L.) leaves. Bioscience, Biotechnology, and Biochemistry 2002;66(11):2483‐6. [DOI] [PubMed] [Google Scholar]
Islam 2003
- Islam MS, Yoshimoto M, Yamakawa O. Distribution and physiological functions of caffeoylquinic acid derivatives in leaves of sweet potato genotypes. Journal of Food Science 2003;68(1):111‐6. [Google Scholar]
Islam 2009
- Islam I, Shaikh AU, Shahidul IM. Antioxidative and antimutagenic potentials of phytochemicals from Ipomoea batatas (L.) lam. International Journal of Cancer Research 2009;5(3):83‐94. [Google Scholar]
Kalyani 2010
- Kalyani RR, Saudek CD, Brancati FL, Selvin E. Association of diabetes, co‐morbidities, and A1C with functional disability in older adults: results from the National Health and Nutrition Examination Survey (NHANES), 1999‐2006. Diabetes Care 2010;33(5):1055‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2011
- Kim JK, Choi SJ, Cho HY, Kim YJ, Lim ST, Kim CJ, et al. Ipomoea batatas attenuates amyloid beta peptide‐induced neurotoxicity in ICR mice. Journal of Medicinal Food 2011;14:1‐6. [DOI] [PubMed] [Google Scholar]
Kjaergard 2001
- Kjaergard LL, Villumsen J, Gluud C. Reported methodological quality and discrepancies between large and small randomised trials in meta‐analyses. Annals of Internal Medicine 2001;135:982–9. [DOI] [PubMed] [Google Scholar]
Kurata 2007
- Kurata R, Adachi M, Yamakawa O, Yoshimoto M. Growth suppression of human cancer cells by polyphenolics from sweet potato (Ipomoea batatas L.) leaves. Journal of Agricultural and Food Chemistry 2007;55(1):185‐90. [DOI] [PubMed] [Google Scholar]
Kusano 2001
- Kusano S, Abe H, Tamura H. Isolation of antidiabetic components from white‐skinned sweet potato (Ipomoea batatas L.). Bioscience, Biotechnology, and Biochemistry 2001;65(1):109‐14. [DOI] [PubMed] [Google Scholar]
Lau 2006
- Lau J, Ioannidis JPA, Terrin N, Schmid CH, Olkin I. The case of the misleading funnel plot. BMJ 2006;333:597‐600. [DOI] [PMC free article] [PubMed] [Google Scholar]
Li 2004
- Li WL, Zheng HC, Bukuru J, Kimpe N. Natural medicines used in the traditional Chinese medical system for therapy of diabetes mellitus. Journal of Ethnopharmacology 2004;92(1):1‐21. [DOI] [PubMed] [Google Scholar]
Li 2009
- Li F, Li Q, Gao D, Peng Y. The optimal extraction parameters and anti‐diabetic activity of flavonoids from Ipomoea batatas leaf. African Journal of Traditional, Complementary, and Alternative Medicines : AJTCAM / African Networks on Ethnomedicines 2009;6(2):195‐202. [DOI] [PMC free article] [PubMed] [Google Scholar]
Liberati 2009
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic and meta‐analyses of studies that evaluate interventions: explanation and elaboration. PLoS Medicine 1999;6(7):1‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lu 2010
- Lu J, Wu DM, Zheng YL, Hu B, Zhang ZF. Purple sweet potato color alleviates D‐galactose‐induced brain aging in old mice by promoting survival of neurons via PI3K pathway and inhibiting cytochrome C‐mediated apoptosis. Brain Pathology (Zurich, Switzerland) 2010;20(3):598‐612. [DOI] [PMC free article] [PubMed] [Google Scholar]
Maiani 2009
- Maiani G, Caston MJ, Catasta G, Toti E, Cambrodon IG, Bysted A, et al. Carotenoids: actual knowledge on food sources, intakes, stability and bioavailability and their protective role in humans. Molecular Nutrition & Food Research 2009;53 Suppl 2:S194‐218. [DOI] [PubMed] [Google Scholar]
Malviya 2010
- Malviya N, Jain S, Malviya S. Antidiabetic potential of medicinal plants. Acta Poloniae Pharmaceutica 2010;67(2):113‐8. [PubMed] [Google Scholar]
Miean 2001
- Miean KH, Mohamed S. Flavonoid (myricetin, quercetin, kaempferol, luteolin, and apigenin) content of edible tropical plants. Journal of Agricultural and Food Chemistry 2001;49(6):3106‐12. [DOI] [PubMed] [Google Scholar]
Miyazaki 2008
- Miyazaki K, Makino K, Iwadate E, Deguchi Y, Ishikawa F. Anthocyanins from purple sweet potato Ipomoea batatas cultivar Ayamurasaki suppress the development of atherosclerotic lesions and both enhancements of oxidative stress and soluble vascular cell adhesion molecule‐1 in apolipoprotein E‐deficient mice. Journal of Agricultural and Food Chemistry 2008;56(23):11485‐92. [DOI] [PubMed] [Google Scholar]
Mogi 2004
- Mogi N, Umegaki H, Hattori A, Maeda N, Miura H, Kuzuya M, et al. Cognitive function in Japanese elderly with type 2 diabetes mellitus. Journal of Diabetes and Its Complications 2004;18(1):42‐6. [DOI] [PubMed] [Google Scholar]
Moher 1998
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta‐analyses?. Lancet 1998;352:609–13. [DOI] [PubMed] [Google Scholar]
Monnier 2005
- Monnier VM, Mustata GT, Biemel KL, Reihl O, Lederer MO, Zhenyu D, et al. Cross‐linking of the extracellular matrix by the Maillard reaction in aging and diabetes: an update on "a puzzle nearing resolution". Annals of the New York Academy of Sciences 2005;1043(Jun):533‐44. [DOI] [PubMed] [Google Scholar]
Mosha 1995
- Mosha TC, Gaga HE, Pace RD, Laswai HS, Mtebe K. Effect of blanching on the content of anti‐nutritional factors in selected vegetables. Plant Foods for Human Nutrition 1995;47(4):361‐7. [DOI] [PubMed] [Google Scholar]
Mosha 1999
- Mosha TC, Gaga HE. Nutritive value and effect of blanching on the trypsin and chymotrypsin inhibitor activities of selected leafy vegetables. Plant Foods for Human Nutrition 1999;54(3):271‐83. [DOI] [PubMed] [Google Scholar]
Mukherjee 2006
- Mukherjee PK, Maiti K, Mukherjee KK, Houghton PJ. Leads from Indian medicinal plants with hypoglycemic potentials. Journal of Ethnopharmacology 2006;106.(1):1‐28. [DOI] [PubMed] [Google Scholar]
Napolitano 2007
- Napolitano A, Carbone V, Saggese P, Takagaki K, Pizza C. Novel galactolipids from the leaves of Ipomoea batatas L.: characterization by liquid chromatography coupled with electrospray ionization‐quadrupole time‐of‐flight tandem mass spectrometry. Journal of Agricultural and Food Chemistry 2007;55(25):10289‐97. [DOI] [PubMed] [Google Scholar]
Park 2010
- Park KH, Kim JR, Lee JS, Lee H, Cho KH. Ethanol and water extract of purple sweet potato exhibits anti‐atherosclerotic activity and inhibits protein glycation. Journal of Medicinal Food 2010;13(1):91‐8. [DOI] [PubMed] [Google Scholar]
Piaggio 2001
- Piaggio G, Pinol AP. Use of the equivalence approach in reproductive health clinical trials. Statistical Medicine 2001;20(23):3571–7. [DOI] [PubMed] [Google Scholar]
Pocock 1991
- Pocock SJ. Clinical trials. A practical approach. Vol. 2, Chichester, UK: John Wiley & Sons, 1991. [Google Scholar]
Riley 2011
- Riley RD, Higgins JP, Deeks JJ. Interpretation of random effects meta‐analyses. BMJ 2011;342:d549. [DOI] [PubMed] [Google Scholar]
Sabater‐Molina 2009
- Sabater‐Molina M, Larque E, Torrella F, Zamora S. Dietary fructo‐oligosaccharides and potential benefits on health. Journal of Physiology and Biochemistry 2009;65(3):315‐28. [DOI] [PubMed] [Google Scholar]
Sakuramata 2004
- Sakuramata Y, Oe H, Kusano S, Aki O. Effects of combination of Caiapo with other plant‐derived substance on anti‐diabetic efficacy in KK‐Ay mice. BioFactors (Oxford, England) 2004;22(1‐4):149‐52. [DOI] [PubMed] [Google Scholar]
Salvador 2000
- Salvador LD, Suganuma T, Kitahara K, Tanoue H, Ichiki M. Monosaccharide composition of sweet potato fiber and cell wall polysaccharides from sweet potato, cassava, and potato analyzed by the high‐performance anion exchange chromatography with pulsed amperometric detection method. Journal of Agricultural and Food Chemistry 2000;48(8):3448‐54. [PUBMED: 10956132] [DOI] [PubMed] [Google Scholar]
Schulz 1995
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias: dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273:408‐12. [DOI] [PubMed] [Google Scholar]
Sterne 2001
- Sterne JAC, Egger M, Davey Smith G. Investigating and dealing with publication and other biases. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic Reviews in Health Care; Meta‐analysis in Context. London: BMJ Publishing Group, 2001:189‐208. [Google Scholar]
Sun 2010
- Sun X, Briel M, Walter SD, Guyatt GH. Is a subgroup effect believable? Updating criteria to evaluate the credibility of subgroup analyses. BMJ 2010;340:850‐4. [DOI] [PubMed] [Google Scholar]
Thu 2004
- Thu NN, Sakurai C, Uto H, Chuyen N, Lien DT, Yamamoto S, et al. The polyphenol content and antioxidant activities of the main edible vegetables in northern Vietnam. Journal of Nutritional Science and Vitaminology 2004;50(3):203‐10. [DOI] [PubMed] [Google Scholar]
USDA 2010
- USDA National Nutrient Database for Standard Reference 2010, Release 23. U.S. Department of Agriculture, Agricultural Research Service; Nutrient Data Laboratory Home Page, http://www.ars.usda.gov/ba/bhnrc/ndl (accessed 20 February 2013).
Velloso 2004
- Velloso A, Baeza M, Tornero P, Herrero T, Fernandez M, Rubio M, et al. Anaphylaxis caused by Ipomoea batatas. Journal of Allergy and Clinical Immunology 2004;113(2):S242. [Google Scholar]
Wang 2008
- Wang LS, Stoner GD. Anthocyanins and their role in cancer prevention. Cancer Letters 2008;269(2):281‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wang 2010
- Wang YJ, Zheng YL, Lu J, Chen GQ, Wang XH, Feng J, et al. Purple sweet potato colour suppresses lipopolysaccharide‐induced acute inflammatory response in mouse brain. Neurochemistry International 2010;56(3):424‐30. [PUBMED: 19941923] [DOI] [PubMed] [Google Scholar]
WHO 1998
- Alberti KM, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part I: diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation. Diabetic Medicine 1998;15:539‐53. [DOI] [PubMed] [Google Scholar]
WHO 2007
- WHO guidelines for assessing quality of herbal medicines with reference to contaminants and residues. World Health Organization, Geneva 2007.
Wild 2004
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27(5):1047‐53. [DOI] [PubMed] [Google Scholar]
Wood 2008
- Wood L, Egger M, Gluud LL, Schulz KF, Juni P, Altman DG, et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta‐epidemiological study. BMJ 2008;336(7644):601‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Woolfe 1992
- Woolfe JA. Sweet potato: an untapped food resource. Cambridge University Press, United Kingdom, 1992. [Google Scholar]
Wu 2008
- Wu DM, Lu J, Zheng YL, Zhou Z, Shan Q, Ma DF. Purple sweet potato colour repairs d‐galactose‐induced spatial learning and memory impairment by regulating the expression of synaptic proteins. Neurobiology of Learning and Memory 2008;90(1):19‐27. [DOI] [PubMed] [Google Scholar]
Ye 2010
- Ye J, Meng X, Yan C, Wang C. Effect of purple sweet potato anthocyanins on beta‐amyloid‐mediated PC‐12 cells death by inhibition of oxidative stress. Neurochemical Research 2010;35(3):357‐65. [DOI] [PubMed] [Google Scholar]
Yen 2010
- Yen CH, Yeh CJ, Wang CC, Liao WC, Chen SC, Chen CC, et al. Determinants of cognitive impairment over time among the elderly in Taiwan: results of the national longitudinal study. Archives of Gerontology and Geriatrics 2010;50 Suppl 1:S53‐7. [DOI] [PubMed] [Google Scholar]