

Abstract
Background
Polycystic ovary syndrome (PCOS) is characterised by infrequent or absent ovulation, and high levels of androgens and insulin (hyperinsulinaemia). Hyperinsulinaemia occurs secondary to insulin resistance and is associated with increased risk of cardiovascular disease and diabetes mellitus. Insulin‐sensitising agents such as metformin may be effective in treating PCOS‐related anovulation.
Objectives
To evaluate the effectiveness and safety of insulin‐sensitising drugs in improving reproductive and metabolic outcomes for women with PCOS undergoing ovulation induction.
Search methods
We searched the following databases from inception to January 2017: Cochrane Gynaecology and Fertility Group Specialised Register, CENTRAL, MEDLINE, Embase, PsycINFO and CINAHL. We searched registers of ongoing trials and reference lists from relevant studies.
Selection criteria
We included randomised controlled trials of insulin‐sensitising drugs compared with placebo, no treatment, or an ovulation‐induction agent for women with oligo and anovulatory PCOS.
Data collection and analysis
Two review authors independently assessed studies for eligibility and bias. Primary outcomes were live birth rate and gastrointestinal adverse effects. Secondary outcomes included other pregnancy outcomes, menstrual frequency and metabolic effects. We combined data to calculate pooled odds ratios (ORs) and 95% confidence intervals (CIs). We assessed statistical heterogeneity using the I2 statistic and reported quality of the evidence for primary outcomes using GRADE methodology.
Main results
We assessed the interventions metformin, clomiphene citrate, metformin plus clomiphene citrate, D‐chiro‐inositol, rosiglitazone and pioglitazone. We compared these with each other, placebo or no treatment. We included 48 studies (4451 women), 42 of which investigated metformin (4024 women). Evidence quality ranged from very low to moderate. Limitations were risk of bias (poor reporting of methodology and incomplete outcome data), imprecision and inconsistency.
Metformin versus placebo or no treatment
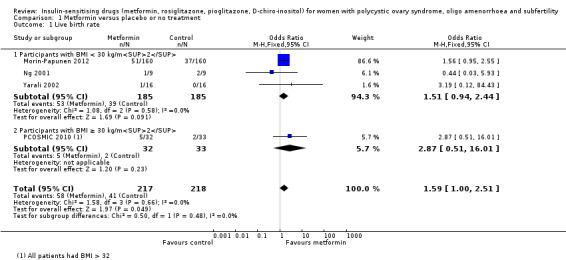
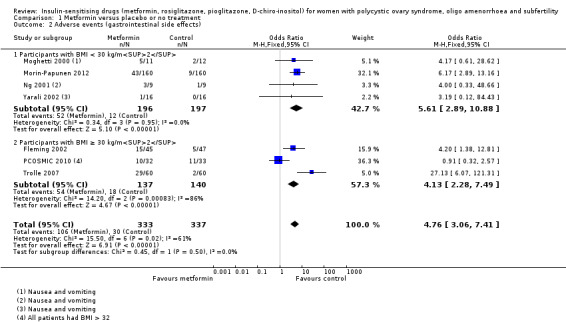
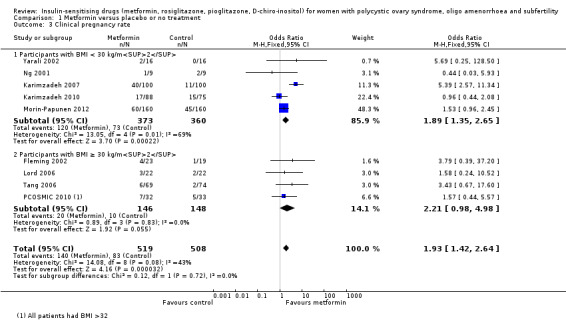
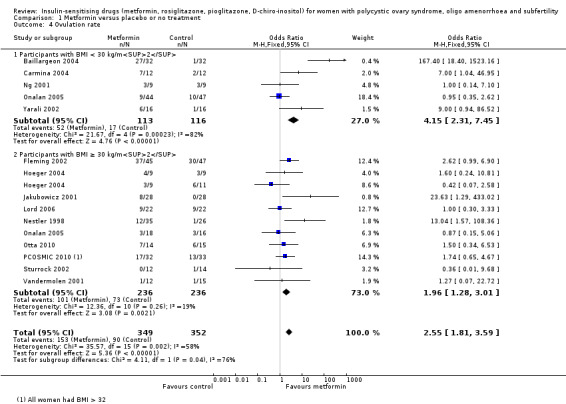
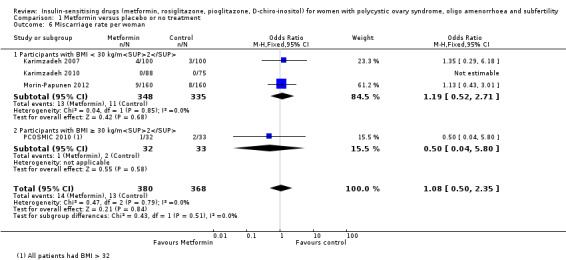
The evidence suggests that metformin may improve live birth rates compared with placebo (OR 1.59, 95% CI 1.00 to 2.51, 4 studies, 435 women, I2 = 0%, low‐quality evidence). The metformin group experienced more gastrointestinal side effects (OR 4.76, 95% CI 3.06 to 7.41, 7 studies, 670 women, I2 = 61%, moderate‐quality evidence) but had higher rates of clinical pregnancy (OR 1.93, 95% CI 1.42 to 2.64, 9 studies, 1027 women, I2 = 43%, moderate‐quality evidence), ovulation (OR 2.55, 95% CI 1.81 to 3.59, 14 studies, 701 women, I2 = 58%, moderate‐quality evidence) and menstrual frequency (OR 1.72, 95% CI 1.14 to 2.61, 7 studies, 427 women, I2 = 54%, low‐quality evidence). There was no clear evidence of a difference in miscarriage rates (OR 1.08, 95% CI 0.50 to 2.35, 4 studies, 748 women, I2 = 0%, low‐quality evidence).
Metformin plus clomiphene citrate versus clomiphene citrate alone
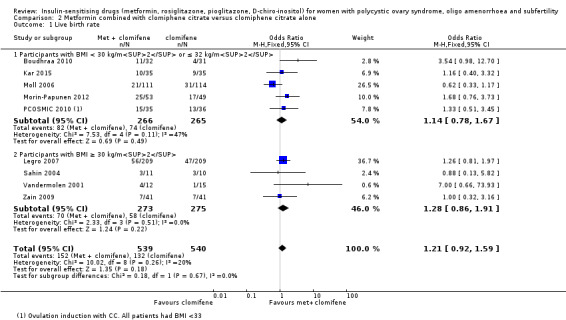
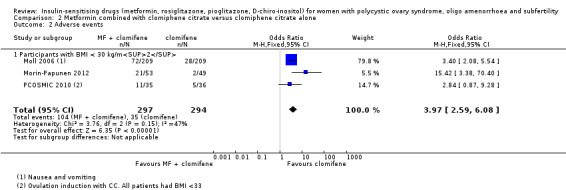
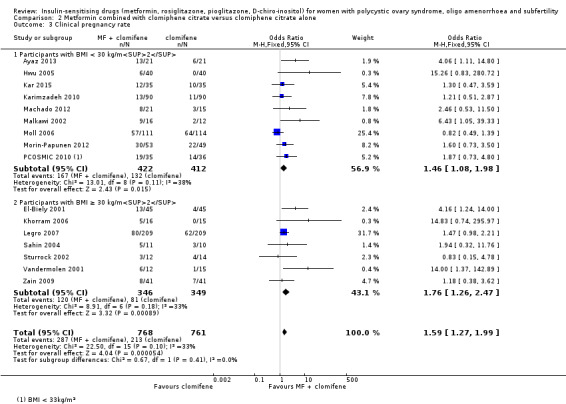
There was no conclusive evidence of a difference between the groups in live birth rates (OR 1.21, 95% CI 0.92 to 1.59, 9 studies, 1079 women, I2 = 20%, low‐quality evidence), but gastrointestinal side effects were more common with combined therapy (OR 3.97, 95% CI 2.59 to 6.08, 3 studies, 591 women, I2 = 47%, moderate‐quality evidence). However, the combined therapy group had higher rates of clinical pregnancy (OR 1.59, 95% CI 1.27 to 1.99, 16 studies, 1529 women, I2 = 33%, moderate‐quality evidence) and ovulation (OR 1.57, 95% CI 1.28 to 1.92, 21 studies, 1624 women, I2 = 64%, moderate‐quality evidence). There was a statistically significant difference in miscarriage rate per woman, with higher rates in the combined therapy group (OR 1.59, 95% CI 1.03 to 2.46, 9 studies, 1096 women, I2 = 0%, low‐quality evidence) but this is of uncertain clinical significance due to low‐quality evidence, and no clear difference between groups when we analysed miscarriage per pregnancy (OR 1.30, 95% CI 0.80 to 2.12, 8 studies; 400 pregnancies, I2 = 0%, low‐quality evidence).
Metformin versus clomiphene citrate
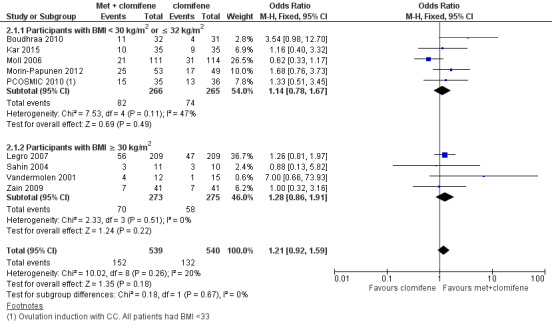
When all studies were combined, findings for live birth were inconclusive and inconsistent (OR 0.71, 95% CI 0.49 to 1.01, 5 studies, 741 women, I2 = 86%, very low‐quality evidence). In subgroup analysis by obesity status, obese women had a lower birth rate in the metformin group (OR 0.30, 95% CI 0.17 to 0.52, 2 studies, 500 women, I2 = 0%, very low‐quality evidence), while data from the non‐obese group showed a possible benefit from metformin, with high heterogeneity (OR 1.71, 95% CI 1.00 to 2.94, 3 studies, 241 women, I2 = 78%, very low‐quality evidence). Similarly, among obese women taking metformin there were lower rates of clinical pregnancy (OR 0.34, 95% CI 0.21 to 0.55, 2 studies, 500 women, I2 = 0%, very low‐quality evidence) and ovulation (OR 0.29, 95% CI 0.20 to 0.43 2 studies, 500 women, I2 = 0%, low‐quality evidence) while among non‐obese women, the metformin group had more pregnancies (OR 1.56, 95% CI 1.05 to 2.33, 5 studies, 490 women, I2 = 41%, very low‐quality evidence) and no clear difference in ovulation rates (OR 0.81, 95% CI 0.51 to 1.28, 4 studies, 312 women, low‐quality evidence, I2=0%). There was no clear evidence of a difference in miscarriage rates (overall: OR 0.92, 95% CI 0.50 to 1.67, 5 studies, 741 women, I2 = 52%, very low‐quality evidence).
D‐chiro‐inositol (2 studies), rosiglitazone (1 study) or pioglitazone (1 study) versus placebo or no treatment
We were unable to draw conclusions regarding other insulin‐sensitising drugs as no studies reported primary outcomes.
Authors' conclusions
Our updated review suggests that metformin alone may be beneficial over placebo for live birth, although the evidence quality was low. When metformin was compared with clomiphene citrate, data for live birth were inconclusive, and our findings were limited by lack of evidence. Results differed by body mass index (BMI), emphasising the importance of stratifying results by BMI. An improvement in clinical pregnancy and ovulation suggests that clomiphene citrate remains preferable to metformin for ovulation induction in obese women with PCOS.
An improved clinical pregnancy and ovulation rate with metformin and clomiphene citrate versus clomiphene citrate alone suggests that combined therapy may be useful although we do not know whether this translates into increased live births. Women taking metformin alone or with combined therapy should be advised that there is no evidence of increased miscarriages, but gastrointestinal side effects are more likely.
Plain language summary
Insulin‐sensitising drugs for women with a diagnosis of polycystic ovary syndrome and subfertility
Review question
Researchers reviewed the evidence about the effectiveness and safety of metformin and other drugs that improve the body's sensitivity to insulin, for inducing ovulation in women with polycystic ovary syndrome (PCOS). Of interest were live birth rate, adverse effects and additional reproductive and metabolic outcomes.
Background
Women with PCOS typically have infrequent or absent periods due to a lack of ovulation, which can result in infertility. Women with PCOS are also at risk of developing metabolic problems, such as diabetes, high blood pressure and high cholesterol levels. High insulin levels are thought to play a role in PCOS and are generally worse with obesity. The treatments, which increase the sensitivity to insulin that are considered in this review are metformin, rosiglitazone, pioglitazone and D‐chiro‐inositol.
Study characteristics
The search for suitable studies was completed on 12 January 2017. We have analysed a total of 48 randomised controlled trials (4451 women) in this review. The current review update includes five additional studies, which all investigated metformin in women with PCOS. The studies compared insulin‐sensitising drugs with placebo, no treatment, or the ovulation‐induction agent, clomiphene citrate.
Key results
Our updated review showed that metformin may be beneficial in improving the chances of having a live birth compared with either no treatment or placebo. It is not clear from the available evidence whether metformin or clomiphene citrate is superior for live birth rate, although pregnancy and ovulation rates are improved with clomiphene citrate, and women taking clomiphene citrate have fewer side effects. However, it is possible that a woman's body mass index may affect which treatment she should take for the greatest benefit, although further research is required to establish this. Metformin did not appear to increase the risk of miscarriage.
The limited improvement in metabolic outcomes with metformin treatment highlights the importance of weight loss and lifestyle adjustment, particularly in overweight women with PCOS.
Quality of the evidence
The quality of the evidence ranged from very low to moderate. Main limitations were risk of bias (associated with poor reporting of study methodology and incomplete outcome data), imprecision and inconsistency.
Summary of findings
Background
Description of the condition
Polycystic ovary syndrome (PCOS) is a common endocrine disorder affecting at least 5% to 15% of women of reproductive age (Balen 2014; March 2010). The disorder is heterogeneous, encompassing a broad spectrum of signs and symptoms of ovarian dysfunction. The classic presentation, as described by Stein and Leventhal (Stein 1935), with features of obesity, amenorrhoea and hirsutism is one end of the spectrum that, at the other end, includes women with normal menstrual cyclicity and yet with ultrasound evidence of a polycystic ovarian appearance (Fauser 2012). Therefore, no single diagnostic criterion (such as hyperandrogenism or PCO) is sufficient for the clinical diagnosis. The 2003 Rotterdam consensus revised diagnostic criteria for a diagnosis of PCOS are as follows, with two of the following being required: 1. oligo or anovulation, or both, that is, menstrual disturbance; 2. clinical or biochemical signs, or both, of hyperandrogenism; 3. PCO on ultrasound; 4. exclusion of other aetiologies of menstrual disturbance and hyperandrogenism (such as congenital adrenal hyperplasia, androgen‐secreting tumours, Cushing's syndrome) (ESHRE/ASRM 2004). The Rotterdam consensus also defined the diagnostic criteria for ultrasound PCO morphology as either 12 or more follicles measuring 2 mm to 9 mm in diameter or increased ovarian volume, over 10 cm3, when using a transvaginal ultrasound scan (ESHRE/ASRM 2004).
Although PCOS is the commonest cause of anovulatory infertility (Balen 2014), many women may remain undiagnosed in the community. This was indicated by a prospective birth cohort study that investigated PCOS in 728 adult women and found that 69% of women with PCOS did not have a pre‐existing diagnosis (March 2010).
The expression of PCOS symptoms is multifaceted, and the reduced conception rates associated with PCOS may be related to hyperandrogenism, obesity and insulin resistance (Balen 2014). Over the last 20 years, the body of evidence indicating that increased insulin resistance and compensatory high insulin concentrations (hyperinsulinaemia) play a key role in the pathogenesis of PCOS has grown (Balen 2014; Diamanti‐Kandarakis 2010). Insulin resistance is more common in overweight women but can also occur in slim women with the disorder (Alebic 2014; Stepto 2013).
The insulin resistance associated with PCOS can worsen both women's symptom profile and their likelihood of achieving a live birth. Women with insulin resistance have a significantly higher level of testosterone and increased prevalence of hirsutism than women with non‐insulin resistant PCOS (Legro 2006a). In addition, Robinson 1993 reported that women with PCOS who developed menstrual disturbance had lower insulin sensitivity than controls; whilst those with regular cycles had normal insulin sensitivity, similar to controls. Insulin resistant women with PCOS also have a lower ovulation rate and are more likely to develop resistance to ovulation induction with clomiphene citrate compared with women with non‐insulin resistant PCOS.
The impaired glucose tolerance results in accelerated development of type 2 diabetes mellitus compared with the background population (Celik 2014). Celik 2014 conducted a prospective study of insulin resistance in 84 women with PCOS, with a mean follow‐up period of 2.6 years. Of those with normal glucose tolerance, 11.5% converted to insulin resistance (annual incidence rate 4.5%). This compares to 2.3% in the healthy control population (n = 45), with an annual progression of 0.9%. For women with impaired glucose tolerance at the outset, 33.3% developed diabetes (annual incidence rate 10.4%). The prevalence of insulin resistance in women with PCOS is likely to be exacerbated by obesity; at least 50% of women with PCOS are obese (Balen 2014). Correspondingly, a Spanish study found a 28% prevalence of PCOS in obese women versus 5% in normal‐weight women (Alvarez‐Blasco 2006). Obesity, and particularly abdominal obesity as indicated by an increased waist to hip ratio, is correlated with reduced fecundity (Lord 2002; Pasquali 2003). A small study demonstrated increased preterm birth and low birth‐weight infants in obese versus normal‐weight women with PCOS (De Frene 2014). Weight loss has been shown to improve the endocrine profile, menstrual cyclicity and the likelihood of ovulation (Huber‐Buchholz 1999; Kiddy 1992). A meta‐analysis of six studies found that weight loss reduced testosterone and insulin resistance, although there was insufficient evidence to determine whether reproductive outcomes were improved (Moran 2011). There is therefore considerable overlap between metabolic syndrome and the metabolic disturbances that feature in PCOS. Metabolic syndrome is a cluster of risk factors that confer an increased risk for cardiovascular disease and type II diabetes (Apridonidze 2005; Ford 2004). Women with metabolic syndrome may have a higher mortality from cardiovascular disease overall, coronary heart disease and stroke compared to women without the syndrome (Ford 2004). The prevalence of metabolic syndrome among women with PCOS was estimated to be nearly two‐fold higher than in the general population (43% versus 24%) (Apridonidze 2005). The prevalence also varies amongst different ethnic groups, which is likely to be influenced by the background prevalence of insulin resistance (Hahn 2007; Soares 2007; Weerakiet 2007). Furthermore, women with PCOS and metabolic syndrome tend to have a higher body mass index (kg/m2) (BMI), waist circumference, blood pressure, fasting glucose and insulin concentration than those without (Ehrmann 2006). PCOS therefore affects reproductive outcomes and confers significant long‐term health risks to patients. PCOS also has a significant psychological impact, with associated with low self esteem, anxiety and depression (Moran 2012). With the increasing prevalence of obesity in society, the prevalence of PCOS is likely to rise. There are therefore significant financial implications for the funding of PCOS management by health care providers. A 2005 study calculated approximately USD 4.36 billion are spent on managing reproductive‐age women with PCOS, of which USD 533 million is related to infertility (Azziz 2005).
Description of the intervention
Metformin is an antihyperglycaemic biguanide drug, widely used for the treatment of type 2 diabetes mellitus. However, the exact mechanism of action through which metformin has its glucose‐lowering effect, is still being explored (Pernicova 2014). Metformin inhibits hepatic gluconeogenesis and reduces the action of glucagon, resulting in a reduction in circulating insulin and glucose. This is thought to occur via inhibition of mitochondrial complexes with downstream effects on cyclic (adenosine monophosphate) AMP and protein kinase signalling pathways. The effect on protein kinase may also modulate lipid synthesis. Metformin is known to exert its effect on several tissues affected by insulin resistance, including the liver, adipose tissue and the ovaries (Pernicova 2014).
The additional interventions considered in this review are thiazolidinediones including troglitazone, rosiglitazone and pioglitazone. Thiazolidinedione is a selective ligand of the nuclear transcription factor perioxisomes proliferator activated receptor γ. These are widely available, standard medications for the treatment of non‐insulin‐dependent diabetes mellitus (NIDDM). Whilst they lower elevated sugar levels in people with diabetes, when given to non‐diabetic people, insulin levels are lowered but blood glucose levels remain unchanged.
Troglitazone had been used as a therapy for people with diabetes and in some trials involving women with PCOS. However, rare cases of liver damage were reported during its marketed use. The liver damage was usually reversible but very rare cases of hepatic failure, leading to death or liver transplant, were reported (Graham 2003). Injury occurred after short‐ and long‐term troglitazone treatment, leading to its withdrawal from the market in March 2000 (FDA 2002).
Rosiglitazone and pioglitazone do not carry the same degree of risk of hepatotoxicity and are commonly used in clinical trials on women with PCOS. However, they are classified as pregnancy category C drugs according to the Food and Drug Administration (FDA) due to the potential risk of causing fetal growth restriction in animal experiments (Yki‐Jarvinen 2004). A high incidence of weight gain among the users further hampers their use in obese women with PCOS (Baillargeon 2004). Rosiglitazone is currently available in the USA but has been suspended from use in the European Union by the European Medicines Agency and has also been withdrawn from India, New Zealand and South Africa. Pioglitazone has been withdrawn from some countries due to an association with bladder cancer reported with long‐term use (EMA 2011).
How the intervention might work
Increased insulin resistance, hyperandrogenism and obesity have a significant impact on menstrual cyclicity and reproductive health. Metformin may therefore have beneficial effects on anovulatory infertility in PCOS, with reduced levels of circulating insulin acting on the ovaries. Within the ovary itself, metformin may also have a direct impact on cells to reduce excessive steroidogenesis and follicular growth, although the molecular mechanisms remain incompletely understood (Diamanti‐Kandarakis 2010).
As insulin resistance and resulting hyperinsulinaemia are key metabolic features in women with PCOS, their amelioration through either metformin or thiazolidinediones could improve PCOS‐associated symptoms and conception rates.
Why it is important to do this review
This is an update of a Cochrane Review first published in 2003, and previously updated in 2009 and 2012. For this third update, comparing the efficacy and safety of insulin‐sensitising drugs, such as metformin, against placebo or the commonly used clomiphene citrate, for ovulation induction in PCOS, remains clinically important and there are still unanswered questions. A focus of this review has been identifying high‐quality studies that report live birth as a primary outcome.
The first Cochrane Review on the use of insulin‐sensitising drugs for PCOS indicated that metformin was an effective treatment for anovulation in women with PCOS (Lord 2003). However, the study populations in the review had a wide range of BMI. It was therefore difficult to interpret the findings when the results were combined for analysis. Furthermore, most of the included studies had a relatively small sample size, with the highest number recruited (94 women) in the study by Fleming 2002. The first updated review (Tang 2009), included a number of large appropriately powered studies (Legro 2007; Moll 2006; Tang 2006). The current search has included studies up to January 2017. We have added five additional studies with a low risk of bias (Ayaz 2013; Begum 2014; Kar 2015; Machado 2012; Morin‐Papunen 2012). No new studies investigating thiazolidinediones were identified.
Details of abbreviations used in this review and conversion factors of biochemical results can be found in Table 4 and Table 5, respectively.
1. Abbreviations used.
| Abbreviation | Definition |
| BMI | Body mass index |
| CC | Clomiphene citrate |
| CI | Confidence interval |
| CT | Computerised tomography scan |
| DHEAS | Dehydroepiandrosterone sulphate |
| FSH | Follicle stimulating hormone |
| GTT | Glucose tolerance test |
| HbA1C | Glycosylated haemoglobin |
| HDL | High‐density lipoprotein cholesterol |
| IGFBP‐1 | Insulin growth factor binding protein 1 |
| LDL | Low‐density lipoprotein cholesterol |
| LH | Luteinising hormone |
| NIDDM | Non insulin dependent diabetes mellitus |
| PAI‐1 | Plasminogen activator inhibitor 1 |
| PCO | Polycystic ovary |
| PCOS | Polycystic ovary syndrome |
| RCT | Randomised controlled trial |
| rFSH | Recombinant follicle stimulating hormone |
| SD | Standard deviation |
| SE | Standard error of the mean |
| SHBG | Sex hormone‐binding globulin |
| VLDL | Very low density lipoprotein cholesterol |
| vs | Versus |
| MD | Mean difference |
2. Conversion factors.
| Convert from | Convert to | Conversion factor | |
| Cholesterol | mg/dL | mmol/L | 0.026 |
| Triglycerides | mg/dL | mmol/L | 0.11 |
| Insulin | pmol/L | mIU/L (= microIU/mL) | 0.1667 |
| Glucose | mg/dL | mmol/L | 0.056 |
| Progesterone | ng/mL | nmol/L | 3.18 |
| Testosterone | ng/dL | nmol/L | 0.03467 |
| Androstenedione | ng/dL | nmol/L | 0.0349 |
| Estradiol | ng/dL | pmol/L | 36.71 |
| 17‐beta oestradiol | ng/dL | pmol/L | 36.71 |
| Dehydroepiandrosterone sulphate | microg/dL | micromol/L | 0.02714 |
| Sex hormone‐binding globulin | microg/dL | nmol/L | 34.7 |
| Standard deviation | Standard error | Standard deviation | Sqrt n |
| Confidence intervals | Confidence intervals | Standard error | (upper limit ‐ lower limit)/3.92 |
Objectives
To evaluate the effectiveness and safety of insulin‐sensitising drugs in improving reproductive and metabolic outcomes for women with PCOS undergoing ovulation induction.
Methods
Criteria for considering studies for this review
Types of studies
Published and unpublished randomised controlled trials (RCTs) were eligible for inclusion. We excluded non‐randomised and quasi‐randomised studies due to the high risk of bias. Cross‐over studies were included but we only included data from the first phase in meta‐analyses.
Types of participants
We included women with oligo and anovulatory PCOS, based on the diagnostic criteria set by the Rotterdam consensus (ESHRE/ASRM 2004), undergoing ovulation induction. Women having in vitro fertilisation (IVF) or intracytoplasmic spermatic injection (ICSI) were excluded, as this is covered in a separate Cochrane Review (Tso 2014).
Types of interventions
Metformin, rosiglitazone or pioglitazone versus placebo or no therapy
Metformin, rosiglitazone or pioglitazone in conjunction with an ovulation induction agent versus the ovulation induction agent
Metformin, rosiglitazone or pioglitazone versus clomiphene citrate
Since troglitazone has been withdrawn from the market, we excluded studies involving troglitazone from the current review. The use of gonadotrophins, contraceptive pills or aromatase inhibitors, such as letrozole, for the treatment of PCOS are the subject of separate Cochrane Reviews (Bordewijk 2017; Costello 2007; Franik 2014, respectively).
Types of outcome measures
Primary outcomes
1. Live birth rate, as defined by included studies
2. Adverse events (gastrointestinal side effects)
Secondary outcomes
3. Clinical pregnancy rate, as defined by included studies (biochemical pregnancies were excluded)
4. Ovulation rate, as defined by included studies
5. Menstrual frequency, as defined by included studies
6. Miscarriage, as defined by included studies
7. Multiple pregnancy
8. Anthropometric outcomes:
a) Body mass index (BMI)
b) Waist to hip ratio
c) Blood pressure
9. Endocrine outcomes
a) Serum testosterone
b) Serum sex hormone‐binding globulin
10. Metabolic outcomes
a) Fasting blood glucose
b) Fasting insulin
c) Cholesterol
d) Triglycerides
Search methods for identification of studies
We searched for all published and unpublished RCTs without language restriction and in consultation with Cochrane Gynaecology and Fertility's (CGF) Information Specialist. The original search was conducted in 2003. The first updated search was completed on 11 September 2008, the second update was completed on 3 October 2011 and the current search was completed on 12 January 2017.
Electronic searches
We searched the CGF Specialised Register of Controlled Trials, PROCITE platform (searched 12 January 2017) (Appendix 1); the Cochrane Central Register of Controlled Trials via the Cochrane Register of Studies Online (CRSO) (searched 12 January 2017) (Appendix 2); MEDLINE Ovid (from 1946 to 12 January 2017) (Appendix 3); Embase Ovid (from 1980 to 12 January 2017) (Appendix 4); PsycINFO Ovid (from 1806 to 12 January 2017) (Appendix 5); and CINAHL EBSCO platform (from 1961 to 12 January 2017) (Appendix 6).
We combined the MEDLINE search with the Cochrane highly sensitive search strategy for identifying randomised trials, which appears in the Cochrane Handbook of Systematic Reviews of Interventions (Lefebvre 2011). The Embase, PsycINFO and CINAHL searches were combined with trial filters developed by the Scottish Intercollegiate Guidelines Network (SIGN) www.sign.ac.uk/search‐filters.html.
Other electronic sources of trials included:
-
trial registers for ongoing and registered trials‐
ClinicalTrials.gov
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP)
DARE (Database of Abstracts of Reviews of Effects) in the Cochrane Library
Web of Science (http://metodologia.lilacs.bvsalud.org/php/)
OpenGrey for unpublished literature from Europe (http://www.greynet.org/opengreyrepository.html)
LILACS database for trials in Portuguese and Spanish (http://metodologia.lilacs.bvsalud.org/php/)
PubMed and Google Scholar for recent trials not yet indexed in MEDLINE
Searching other resources
We handsearched the reference sections of all trials obtained. In liaison with the CGF Information Specialist we searched relevant journal articles and conference abstracts that are not covered in the CGF register.
Data collection and analysis
Selection of studies
The first review of this subject (Lord 2003) was undertaken by three review authors (JML, IHF and RJN), two of whom work in reproductive medicine (JML, RJN). Three review authors (TT, EY, AHB) updated the review (Tang 2009; Tang 2012). Three review authors (LCM, TT and AHB) performed the current update. We employed the search strategy described previously to obtain titles and, where possible, abstracts of studies that were potentially relevant to the review. Two review authors (LCM and TT) screened the titles and abstracts and then obtained copies of the relevant full‐text articles. Two review authors (LCM and TT) independently assessed whether the studies met the inclusion criteria, with disagreements resolved by discussion (for details of the screening and selection process see Figure 1; Figure 2).
1.
Study flow diagram since publication
2.
Study flow diagram 2017 update
Data extraction and management
Data collection process
Two review authors (LCM and TT) independently extracted data from eligible studies, and resolved any disagreements by discussion. We extracted data onto a pre‐designed form (see Data items). Further information was sought from the authors where papers contained insufficient information to make a decision about eligibility.
Data items
We have presented a summary of included trials in the table 'Characteristics of included studies'. This information includes the following:
Method of randomisation
Blinding to treatment allocation
Quality of allocation concealment
Number of women randomised
Location, duration and timing of the trial
Characteristics of women
Mean age, BMI, testosterone, fasting insulin and glucose levels
Study inclusion and exclusion criteria
Dropout rate
Interventions
Type of insulin‐sensitising drug
Co‐interventions such as clomiphene citrate or lifestyle advice
Outcomes
As stated under 'Types of outcome measures'
Assessment of risk of bias in included studies
We performed risk of bias assessment in accordance with the Cochrane 'Risk of bias' assessment tool (Higgins 2011).
We judged the following items and summarised them in the 'Risk of bias' table (Figure 3; Figure 4).
3.
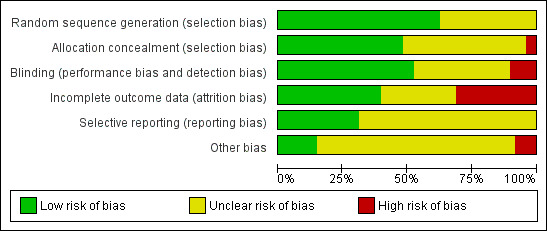
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
4.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study
-
Sequence generation
low risk (for example, computer‐generated random numbers, random number table)
high risk (systematic methods such as alternation; assignment based on case record number, date of presentation or date of birth)
unclear risk (insufficient information in the study or from the study author about the process of sequence generation)
-
Allocation concealment
low risk (for example, central randomisation, sequentially numbered, opaque, sealed envelopes)
high risk (for example, open‐label trial, assignment based on case record number, date of presentation or date of birth)
unclear risk (insufficient information in the study or from the study author about the process of allocation concealment)
-
Blinding
low risk (double‐blind study: participants, providers and assessors blinded)
high risk (unblinded)
unclear risk (insufficient information in the study or from the study author about the level of blinding)
-
Incomplete outcome data addressed
low risk (for example, no missing data, reasons for missing data were reported and were unlikely to influence the outcomes, or missing data were balanced across the groups)
high risk (for example, reasons for missing data were not addressed, missing data likely to affect the outcomes, or data analysed per protocol)
unclear risk (insufficient information in the study or from the author about the detail of incomplete outcome data)
-
Selective outcome reporting
low risk (for example, the study protocol was available, pre‐specified outcome measures were reported)
high risk (for example, the study protocol was unavailable and pre‐specified outcome measures were not reported)
unclear risk (insufficient information in the study or from the author about process of outcome reporting)
Measures of treatment effect
We used odds ratio (OR) as the measure of effect for each dichotomous outcome and the mean difference (MD) for each continuous outcome. We have presented 95% confidence intervals (CI) for all outcomes.
Unit of analysis issues
The primary unit of analysis was each woman, for example, we calculated ovulation rate as rate of women in whom ovulation was confirmed. Where studies reported 'per‐cycle' data, we contacted the study authors to request 'per‐woman' data. When these data were not available, we have not pooled the per‐cycle ovulation data but presented them in additional tables (Table 6; Table 7; Table 8; Table 9; Table 10). The exceptions to this were miscarriage and multiple pregnancy rates, which we analysed per woman, followed by a sensitivity analysis using per‐pregnancy data.
3. Metformin vs placebo: ovulation rate per cycle.
| Study ID | Metformin | Placebo | P value | ||
| Events | Cycles | Events | Cycles | ||
| BMI < 30 kg/m2 | |||||
| Baillargeon 2004 | 27 | 32 | 11 | 32 | |
| Carmina 2004 | 7 | 12 | 3 | 12 | |
| Ng 2001 | 3 | 9 | 3 | 9 | |
| Onalan 2005 | 17 | 153 | 20 | 150 | |
| Yarali 2002 | 6 | 16 | 1 | 16 | |
| BMI ≥ 30 kg/m2 | |||||
| Fleming 2002 | 37 | 45 | 30 | 47 | |
| Hoeger 2004 | 3 | 9 | 6 | 11 | |
| Hoeger 2004 | 4 | 9 | 3 | 9 | |
| Jakubowicz 2001 | 8 | 28 | 0 | 28 | |
| Lord 2006 | 9 | 22 | 9 | 22 | |
| Nestler 1998 | 12 | 35 | 1 | 26 | |
| Onalan 2005 | 5 | 63 | 5 | 51 | |
| Otta 2010 | 7 | 14 | 6 | 15 | |
| PCOSMIC 2010 | 17 | 32 | 13 | 33 | |
| Sturrock 2002 | 0 | 12 | 1 | 14 | |
| Vandermolen 2001 | 1 | 12 | 1 | 15 | |
4. Metformin + clomiphene citrate vs clomiphene citrate: ovulation rate per cycle.
| Study ID | Metformin + clomiphene citrate | Clomiphene citrate alone | P value | ||
| Events | Cycles | Events | Cycles | ||
| BMI < 30 kg/m2 | |||||
| Ayaz 2013 | 16 | 21 | 8 | 21 | |
| Ben Ayed 2009 | 10 | 16 | 6 | 16 | |
| Boudhraa 2010 | 17 | 32 | 10 | 31 | |
| El‐Biely 2001 | 35 | 45 | 29 | 45 | |
| Hwu 2005 | 17 | 40 | 5 | 40 | |
| Machado 2012 | 15 | 21 | 5 | 15 | |
| Malkawi 2002 | 11 | 16 | 3 | 12 | |
| Moll 2006 | 84 | 141 | 98 | 168 | |
| Ng 2001 | 4 | 9 | 1 | 9 | |
| PCOSMIC 2010 | 27 | 35 | 23 | 36 | |
| BMI ≥ 30 kg/m2 | |||||
| Jakubowicz 2001 | 26 | 28 | 22 | 28 | |
| Khorram 2006 | 7 | 16 | 1 | 15 | |
| Legro 2007 | 582 | 964 | 462 | 942 | |
| Nestler 1998 | 19 | 21 | 2 | 25 | |
| Sahin 2004 | 38 | 51 | 34 | 55 | |
| Siebert 2009 | 34 | 52 | 36 | 55 | |
| Sturrock 2002 | 5 | 12 | 4 | 14 | |
| Vandermolen 2001 | 9 | 12 | 4 | 15 | |
| Zain 2009 | 38 | 41 | 24 | 41 | |
5. Metformin vs clomiphene citrate: ovulation rate per cycle.
| Metformin | Clomiphene citrate | ||||
| Study ID | Events | Cycles | Events | Cycles | P value |
| BMI < 30 kg/m2 | |||||
| Palomba 2005 | 129 | 205 | 148 | 221 | |
| PCOSMIC 2010 | 23 | 35 | 23 | 36 | |
| BMI ≥ 30 kg/m2 | |||||
| Legro 2007 | 296 | 1019 | 462 | 942 | |
| Zain 2009 | 4 | 42 | 7 | 41 | |
6. D‐Chiro‐inositol vs placebo: ovulation rate per cycle.
| Inositol | Placebo | ||||
| Study ID | Events | Cycles | Events | Cycles | P value |
| BMI < 30 kg/m2 | |||||
| Gerli 2003 | 128 | 136 | 130 | 147 | |
| Nestler 1999 | 19 | 22 | 6 | 22 | |
7. Rosiglitazone vs placebo: ovulation rate per cycle.
| Rosiglitazone | Placebo | ||||
| Study ID | Events | Cycles | Events | Cycles | P value |
| BMI ≥ 30 kg/m2 | |||||
| Baillargeon 2004 | 16 | 32 | 11 | 32 | |
In order to reduce a carry‐over of treatment effect in cross‐over trials, we only used data from the first phase (such as before cross‐over) when the washout period was less than two months. The rationale is that oligo amenorrhoea is usually accepted as a menstrual cycle length over five to eight weeks. Therefore, the washout period of treatment effect on ovulation should ideally be more than eight weeks.
Dealing with missing data
We analysed the data on an intention‐to‐treat basis where possible and sought any missing data from the study authors.
When this information was not available, we performed the analysis using the original number of women randomised.
Assessment of heterogeneity
Heterogeneity reflects any type of variability among the studies in a systematic review. A consistent treatment effect among the included studies suggests there is sufficient homogeneity for pooled analysis. We used the I2 statistic (Higgins 2003) to quantify the inconsistency among the studies. We regarded an I2 statistic of over 50% as indicative of substantial heterogeneity (Deeks 2011).
Assessment of reporting biases
In view of the difficulty of detecting and correcting for publication bias and other reporting biases, we aimed to minimise the potential impact by ensuring a comprehensive search for eligible studies and by being alert for duplication of data. We planned to produce funnel plots for the primary outcome, live birth, which explore the possibility of small study effects (a tendency for estimates of the intervention effect to be more beneficial in smaller studies) (Sterne 2011).
Data synthesis
We performed statistical analyses according to the statistical guidelines for review authors developed by Cochrane and published in the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011). We used Review Manager 5 (RevMan 5) to perform all the statistical analyses (RevMan 2014).
We used odds ratio (OR), with 95% confidence interval (CI), as the measure of effect for each dichotomous outcome using the Mantel‐Haenszel method; whilst we presented continuous outcome differences between the two groups as mean difference (MD) with 95% CI. We employed a fixed‐effect model in the analysis, and have commented on significant heterogeneity where it occurred.
For clinical outcomes, we stratified comparisons by BMI, divided into obese and non‐obese groups, with an additional stratum for studies in which BMI was not reported. We defined 'obese' as BMI equal to or over 30 kg/m2.
Subgroup analysis and investigation of heterogeneity
As noted above, we subgrouped the primary analysis by BMI (obese or non‐obese), in order to assess any differences in effect within these subgroups.
We also conducted subgroup analyses by sensitivity to clomiphene citrate (sensitive or resistant), in relevant analyses (i.e. including clomiphene citrate group) where substantial heterogeneity was detected (I2 over 50%).
We also planned to explore other possible explanations where heterogeneity was substantial, by examining other clinical or methodological differences between the studies.
Sensitivity analysis
To determine that the conclusions of this review were robust, we performed sensitivity analyses after excluding studies with unclear or high risk of bias in sequence generation, allocation concealment or blinding method. We also performed a sensitivity analysis to compare the effect of reporting miscarriage and multiple pregnancy data 'per pregnancy'.
Overall quality of the body of evidence: 'Summary of findings' table
We prepared 'Summary of findings' tables using GRADEpro GDT software (GRADEpro GDT 2015). These tables evaluated the overall quality of the body of evidence for the main review outcomes (live birth, adverse events, clinical pregnancy, menstrual frequency, ovulation and miscarriage) with respect to the most clinically relevant comparisons (metformin versus placebo or no treatment, metformin with clomiphene citrate versus clomiphene citrate alone, metformin versus clomiphene citrate). Two review authors working independently evaluated the quality of the evidence using GRADE criteria (study limitations (i.e. risk of bias), consistency of effect, imprecision, indirectness and publication bias). Judgements about evidence quality (high, moderate, low or very low) were justified, documented, and incorporated into reporting of results for each outcome (Schünemann 2011; Schünemann 2013). We resolved any disagreements by consensus.
For one of our comparisons (metformin versus clomiphene citrate), there was high heterogeneity for some outcomes which was associated with BMI status, so for this comparison we decided as a post hoc measure to present the data by BMI subgroup.
Details of abbreviations used in this review and conversion factors of biochemical results can be found in Table 4 and Table 5, respectively.
Results
Description of studies
See Characteristics of included studies and Characteristics of excluded studies for full details of the trials.
Results of the search
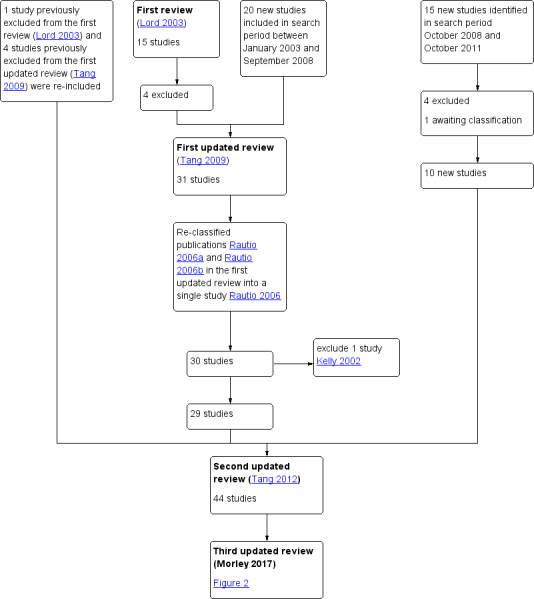
In this updated review there are 48 included studies and 35 excluded studies(Figure 2).
In the first review (Lord 2003), 24 RCTs met the initial eligibility criteria. Nine studies were excluded, leaving 15 to be included in the analysis.
In the first update of the review (Tang 2009) (search period January 2003 to September 2008), the review authors identified 37 RCTs, of which 20 were suitable for inclusion. They excluded four previously included studies (Azziz 2001; Kocak 2002; Nestler 1996; Pasquali 2000). Including the studies in the first review (Lord 2003; total amended to 11 studies), Tang 2009 included 31 studies in the analysis (Figure 1).
In the second update of the review (Tang 2012) (search period October 2008 to October 2011), the review authors identified 15 studies. They excluded four studies and one study awaited classification. Therefore, 10 new studies were identified for inclusion (Ben Ayed 2009; Boudhraa 2010; Karimzadeh 2010; Ladson 2011; Lam 2011; Otta 2010; PCOSMIC 2010; Romualdi 2010; Siebert 2009; Williams 2009) (Figure 1). After further consideration, they re‐included five previously excluded studies (Brettenthaler 2004; Carmina 2004; Khorram 2006; Pasquali 2000; Sahin 2004). Furthermore, they re‐classified two publications in the first updated review (Tang 2009) into a single study (Rautio 2006; formerly Rautio 2006a and Rautio 2006b) and removed Kelly 2002, after a protocol update removed hirsutism from secondary outcomes. Hence, Tang 2012 included a total of 44 studies in the analysis (Figure 1).
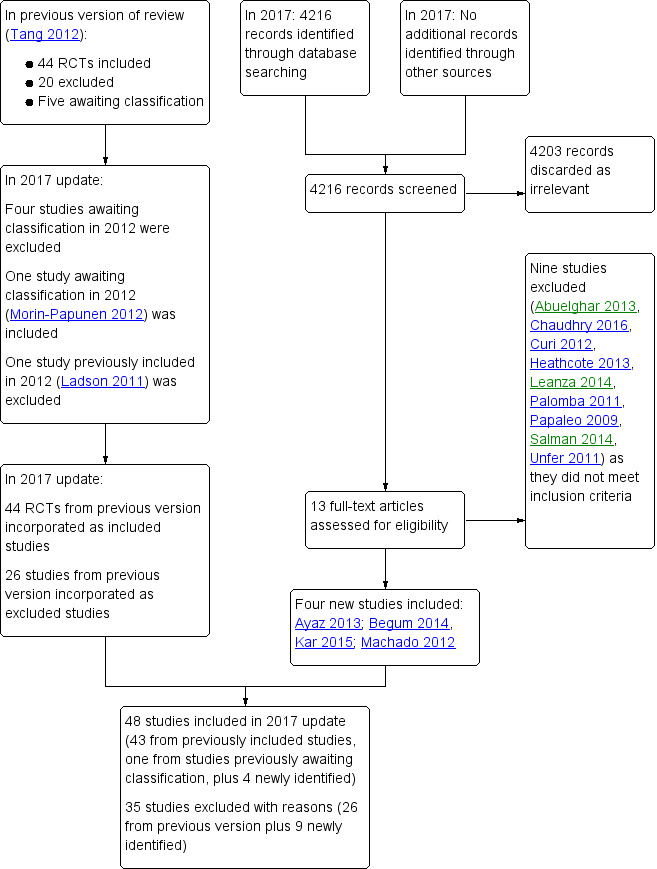
In the current review update, (third update, search period January 2011 to January 2017), we considered the full texts of 13 articles (Figure 2). Of these, we excluded nine (Abuelghar 2013; Curi 2012; Chaudhry 2016; Heathcote 2013;Leanza 2014; Palomba 2011; Papaleo 2009; Salman 2014; Unfer 2011) and included four (Ayaz 2013; Machado 2012; Kar 2015; Begum 2014). Morin‐Papunen 2012 was the study awaiting classification from the previous update, and we have now included it in this update, therefore we have included a total of five additional studies in this review.
Included studies
Study design and Setting
The newly included studies for this current update (Ayaz 2013; Begum 2014; Kar 2015; Machado 2012;Morin‐Papunen 2012) all recorded pregnancy outcomes following treatment. In these studies, metformin was investigated with, and without the addition of clomiphene citrate.
Twenty‐three of the included studies were documented as being double blind. Five studies were not double blind: Hwu 2005;Khorram 2006;Nestler 1998;Siebert 2009;Zain 2009; and the remainder were classified as unclear.
Two of the studies were cross‐over trials (Sturrock 2002; Trolle 2007). We only analysed the first phase from Sturrock 2002 as we considered the washout period to be short (four weeks). Although the study by Trolle 2007 was also a cross‐over study, there was an eight‐week washout period and no women became pregnant during the trial period. We therefore decided to include the published data of this study after the cross‐over period (second phase).
The included studies originated from a number of countries, including Argentina, Bangladesh, Brazil, Denmark, Egypt, Finland, Germany, Hong Kong, India, Iran, Italy, Malaysia, the Netherlands, New Zealand, Saudi Arabia, South Africa, Tunisia, Turkey, UK, USA and Venezuela.
Participants
The number of women in the studies ranged from 19 to 626. In total, 4451 women (4014 participants had metformin, 497 participants had other insulin‐sensitising drugs) were included in this updated review. The range of BMI in included participants was (24.3 to 39.4 kg/m2).
All the women had a diagnosis of PCOS based upon standardised criteria; two out of three of PCOS on ultrasound, oligo or anovulation, clinical or biochemical signs of hyperandrogenism (ESHRE/ASRM 2004). The age range of participants was 24.2 to 32.8 years with the range of fasting insulin concentrations between 6.3 and 54.67 mIU/L and testosterone levels of 1.3 to 4.67 nmol/L. However, several studies did not provide these data.
Most women recruited in the studies using rosiglitazone, pioglitazone or D‐chiro‐inositol (Brettenthaler 2004; Glintborg 2005; Lam 2011; Rautio 2006) were not planning a pregnancy due to the uncertainty of the safety of using these products in pregnancy.
Interventions
In total, including the first review and the last update, 42 out of 48 trials assessed the benefits of using metformin for women with PCOS. Eighteen trials compared metformin alone with placebo or no treatment (Baillargeon 2004; Carmina 2004; Fleming 2002; Hoeger 2004; Jakubowicz 2001; Karimzadeh 2007; Karimzadeh 2010; Lord 2006; Morin‐Papunen 2012; Nestler 1998; Ng 2001; Onalan 2005; Otta 2010; Pasquali 2000; PCOSMIC 2010; Tang 2006; Vandermolen 2001; Yarali 2002).
Twenty‐two studies investigated the benefits of using metformin combined with clomiphene citrate on reproductive outcomes (Ayaz 2013; Ben Ayed 2009; Boudhraa 2010; El‐Biely 2001; Hwu 2005; Jakubowicz 2001; Kar 2015; Karimzadeh 2010; Khorram 2006; Legro 2007; Machado 2012; Malkawi 2002; Moll 2006; Nestler 1998; Ng 2001; PCOSMIC 2010; Sahin 2004, Siebert 2009; Sturrock 2002; Vandermolen 2001; Williams 2009; Zain 2009). Five studies compared metformin versus clomiphene citrate (Begum 2014; Karimzadeh 2010; Legro 2007; Palomba 2005; Zain 2009).
Specific advice on lifestyle modification was included in the study protocol in ten trials (Ben Ayed 2009; Boudhraa 2010; Brettenthaler 2004; Hoeger 2004; Karimzadeh 2010; Otta 2010; Pasquali 2000; PCOSMIC 2010; Romualdi 2010; Tang 2006).
The duration of the trials ranged from 4 to 48 weeks with an average of 19.5 weeks. The median daily dose of metformin used in the trials was 1500 mg.
Outcomes
Most trials reported clinical pregnancy rate but only 11 studies reported live birth rates (Boudhraa 2010; Kar 2015; Legro 2007; Moll 2006; Morin‐Papunen 2012; Ng 2001; PCOSMIC 2010; Sahin 2004; Vandermolen 2001; Yarali 2002; Zain 2009). The four studies listed largest studies reporting live birth rate were Legro 2007; Moll 2006; Morin‐Papunen 2012; PCOSMIC 2010. Only two studies (Legro 2007; PCOSMIC 2010) identified live birth rate as a primary outcome measure. Eight studies that were suitable for meta‐analysis reported adverse events (Fleming 2002; Moghetti 2000; Moll 2006; Morin‐Papunen 2012; Ng 2001; PCOSMIC 2010; Trolle 2007; Yarali 2002).
Excluded studies
In the previous update of the review (Tang 2012), the review authors excluded a total of 22 studies. Of these, they excluded two studies due to lack of randomisation (Aroda 2009; Santonocito 2009) and four studies (Azziz 2001; Azziz 2003; Dunaif 1996; Mantzoros 1997) because troglitazone had been withdrawn from the market. Another study, Kelly 2002 was excluded because the revised protocol had removed hirsutism from the outcomes.
In this third update of the review, we excluded four of the studies previously awaiting classification due to inadequate information (Chaudhury 2008; Constantino 2009; Farzadi 2006;Refaie 2005). In the updated search (January 2011 to January 2017), we identified 13 studies for possible inclusion, of which nine were excluded (Abuelghar 2013; Chaudhry 2016; Curi 2012; Heathcote 2013; Leanza 2014; Palomba 2011; Papaleo 2009; Salman 2014; Unfer 2011). We excluded Palomba 2011 as participants were undergoing in vitro fertilisation, which does not meet the inclusion criteria for this review (Types of participants).
A summary of studies included and excluded in the different versions of this review can be found in Figure 2.
Risk of bias in included studies
See Figure 3 for risk of bias and Figure 4 for a summary of the risk of bias.
We carried out sensitivity analysis by including data only from studies with low risk of bias, determined by sequence generation, allocation concealment and blinding method. Only 18 out of 48 studies met this criterion (Baillargeon 2004; Chou 2003; Eisenhardt 2006; Fleming 2002; Glintborg 2005; Hoeger 2004; Karimzadeh 2007; Lam 2011; Legro 2007; Lord 2006; Machado 2012; Maciel 2004; Moll 2006; Morin‐Papunen 2012; Ng 2001; Pasquali 2000; PCOSMIC 2010; Tang 2006) with 15 out of the 18 studies investigating the effects of metformin. Three out of the 10 newly included studies, in the search period between October 2008 and October 2011, met this criterion (Ladson 2011; Lam 2011; PCOSMIC 2010). Two studies from the January 2011 to January 2017 update met the criteria for subgroup analysis; Machado 2012 and Morin‐Papunen 2012.
Allocation
Sequence generation
Sequence generation was unclear in 18 studies (Ayaz 2013; Begum 2014; Ben Ayed 2009; Boudhraa 2010; Brettenthaler 2004; Carmina 2004; Jakubowicz 2001; Kar 2015; Karimzadeh 2010; Malkawi 2002; Moghetti 2000; Nestler 1998; Nestler 1999; Romualdi 2010; Sahin 2004; Sturrock 2002; Williams 2009; Zain 2009).
Allocation concealment
Allocation concealment was unclear in 25 studies (Begum 2014; Ben Ayed 2009; Boudhraa 2010; Brettenthaler 2004; Carmina 2004; El‐Biely 2001; Gerli 2003; Hwu 2005; Kar 2015; Karimzadeh 2010; Khorram 2006; Malkawi 2002; Nestler 1998; Onalan 2005; Otta 2010; Palomba 2005; Rautio 2006; Sahin 2004; Siebert 2009; Sturrock 2002; Trolle 2007; Vandermolen 2001; Williams 2009; Yarali 2002; Zain 2009). We included one open label‐trial (Hwu 2005).
Blinding
The majority of the studies (38/48) were described as double‐blinded. However, the risk of bias related to the method of blinding was unclear for 18 of the 48 (Ayaz 2013; Begum 2014; Ben Ayed 2009; Boudhraa 2010; Brettenthaler 2004; Carmina 2004; El‐Biely 2001; Gerli 2003; Karimzadeh 2010; Malkawi 2002; Onalan 2005; Otta 2010; Palomba 2005; Rautio 2006; Sahin 2004;Sturrock 2002; Williams 2009; Yarali 2002). We clarified allocation concealment and blinding in the Machado 2012 study through correspondence with the study authors. We classified the risk of bias in five studies as high for this domain (Hwu 2005; Khorram 2006; Nestler 1998; Siebert 2009; Zain 2009).
Incomplete outcome data
Fifteen studies were at high risk of attrition bias due to high dropout rates, unequal dropouts between the groups, reasons of missing data not provided or use of per‐protocol analysis (Baillargeon 2004; Brettenthaler 2004; Chou 2003; Fleming 2002; Gerli 2003; Jakubowicz 2001; Kar 2015; Lam 2011; Nestler 1998; Onalan 2005; Otta 2010; Pasquali 2000; Sturrock 2002; Tang 2006; Zain 2009). Nineteen studies were at low risk of attrition bias (Ayaz 2013; Glintborg 2005; Hoeger 2004; Hwu 2005; Khorram 2006; Legro 2007; Machado 2012; Maciel 2004; Malkawi 2002; Moghetti 2000; Morin‐Papunen 2012; Nestler 1999; Palomba 2005; PCOSMIC 2010; Rautio 2006; Romualdi 2010; Siebert 2009; Trolle 2007; Yarali 2002).
Selective reporting
Low risk of selective reporting was found in fifteen studies (Eisenhardt 2006; Glintborg 2005; Hoeger 2004; Karimzadeh 2010; Lam 2011; Legro 2007; Lord 2006; Moghetti 2000; Moll 2006; Ng 2001; Pasquali 2000; PCOSMIC 2010; Romualdi 2010; Tang 2006; Trolle 2007).
Other potential sources of bias
Overall four studies appeared to be at high risk of other sources of bias (Hwu 2005; Legro 2007; Moghetti 2000; Trolle 2007) although the majority of the studies did not provide sufficient information for analysis. We have presented forest plots for the primary outcome live birth rate in Figure 5; Figure 6; Figure 7, for Analysis 1.1, Analysis 2.1 and Analysis 3.1, respectively.
5.
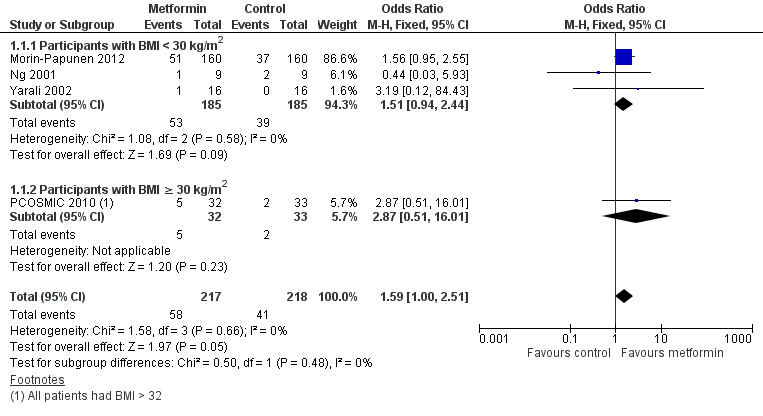
Forest plot of comparison: 1 Metformin versus placebo or no treatment, outcome: 1.1 Live birth rate
6.
Forest plot of comparison: 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, outcome: 2.1 Live birth rate
7.
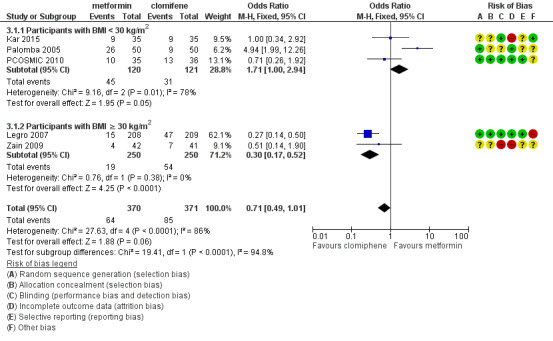
Forest plot of comparison: 3 Metformin versus clomiphene citrate, outcome: 3.1 Live birth.
1.1. Analysis.
Comparison 1 Metformin versus placebo or no treatment, Outcome 1 Live birth rate.
2.1. Analysis.
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 1 Live birth rate.
3.1. Analysis.
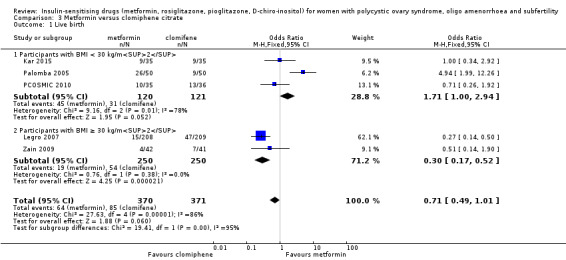
Comparison 3 Metformin versus clomiphene citrate, Outcome 1 Live birth.
Effects of interventions
See: Table 1; Table 2; Table 3
Summary of findings for the main comparison. Metformin compared to placebo or no treatment for women with polycystic ovary syndrome.
| Metformin compared to placebo or no treatment for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility | ||||||
| Patient or population: women with polycystic ovary syndrome, oligo amenorrhoea and subfertility Settings: outpatient Intervention: metformin Comparison: placebo or no treatment | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo or no treatment | Metformin | |||||
| Live birth rate per woman | 141 per 1000 | 208 per 1000 (141 to 292) | OR 1.59 (1.00 to 2.51) | 435 (4 studies) | ⊕⊕⊝⊝ lowa,b | |
| Adverse events (gastrointestinal) per woman | 106 per 1000 | 362 per 1000 (267 to 469) |
OR 4.76 (3.06 to 7.41) |
670 (7 studies) |
⊕⊕⊕⊝ moderatea,c | |
| Clinical pregnancy rate per woman | 110 per 1000 | 193 per 1000 (149 to 246) | OR 1.93 (1.42 to 2.64) | 1027 (9 studies) | ⊕⊕⊕⊝ moderatea | |
| Menstrual frequency per woman | 183 per 1000 | 278 per 1000 (203 to 368) |
OR 1.72 (1.14 to 2.61) |
427 (7 studies) |
⊕⊕⊝⊝ lowa,d | |
| Ovulation rate per woman | 200 per 1000 | 389 per 1000 (312 to 473) |
OR
2.55 (1.81 to 3.59) |
701 (14 studies) | ⊕⊕⊕⊝ moderatea | |
| Miscarriage rate per woman | 40 per 1000 | 43per 1000 (20 to 89) | OR 1.08 (0.50 to 2.35) | 748 (4 studies) | ⊕⊕⊝⊝ lowa,b | Miscarriage rate per pregnancy OR 0.58, 95% CI 0.25 to 1.34, 200 pregnancies |
| *The basis for the assumed risk is the median control group risk across studies. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different Low quality: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect Very low quality: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded one level for serious risk of bias related to failure to report methods of randomisation and/or serious risk of attrition bias in some of the studies. bDowngraded one level for serious imprecision as the event rate is low and findings are compatible with benefit in one or both groups or with no meaningful difference between the groups. cModerate inconsistency (I2 = 61%), but not downgraded, as all heterogeneity is attributable to a single small study and the direction of effect largely consistent. dDowngraded one level for serious inconsistency (I2= 54%); largest study shows no evidence of effect.
Summary of findings 2. Metformin combined with clomiphene citrate versus clomiphene citrate alone for women with polycystic ovary syndrome.
| Metformin combined with clomiphene versus clomiphene alone for women with polycystic ovary syndrome | ||||||
| Population: women with polycystic ovary syndrome Setting: outpatient Intervention: metformin combined with ovulation induction agent clomiphene Comparison: clomiphene alone | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with clomiphene alone | Risk with metformin combined with clomiphene | |||||
| Live birth rate per woman | 257 per 1000 | 295 per 1000 (241 to 355) | OR 1.21 (0.92 to 1.59) | 1079 (9 studies) | ⊕⊕⊝⊝ lowa,b | |
| Adverse events (gastrointestinal) per woman | 134 per 1000 | 381 per 1000 (286 to 485) | OR 3.97 (2.59 to 6.08) | 591 (3 studies) | ⊕⊕⊕⊝ moderatea | |
| Clinical pregnancy rate per woman | 243 per 1000 | 338per 1000 (330 to 436) | OR 1.59 (1.27 to 1.99) | 1529 (16 studies) | ⊕⊕⊕⊝ moderatea | |
| Menstrual frequency per woman | Not reported by any of the included studies | |||||
| Ovulation rate per woman | 381per 1000 | 491 per 1000 (441to 542) | OR 1.57 (1.28 to 1.92) |
1624 (21 studies) | ⊕⊕⊕⊝ moderatea,c | |
| Miscarriage rate per woman | Median rates not calculable as there were no events in the control group in 5/8 studies | OR 1.59 (1.03 to 2.46) | 1096 (9 studies) | ⊕⊕⊝⊝ lowa,b | Miscarriage rate per pregnancy OR 1.30 95% CI 0.80 to 2.12, 400 pregnancies | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the median risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded one level for serious risk of bias related to failure to describe study methods and/or serious risk of attrition bias in several of the studies. bDowngraded one level for serious imprecision as findings are compatible with benefit in one or both groups or with no meaningful difference between the group. cHigh heterogeneity (I2 = 62%), but not downgraded as direction of effect consistent and most inconsistency is due to a single small study.
Summary of findings 3. Metformin compared to clomiphene citrate for women with polycystic ovary syndrome.
| Metformin compared to clomiphene citrate for women with polycystic ovary syndrome | ||||||
| Population: women with polycystic ovary syndrome Setting: outpatient Intervention: metformin Comparison: clomiphene citrate | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with clomiphene citrate | Risk with metformin | |||||
|
Live birth rate per woman Participants with BMI < 30 kg/m2 or ≤ 32 kg/m2a |
225 per 1000 | 171 per 1000 (124 to 227) |
OR 1.71 (1.00 to 2.94) | 241 (3 studies) |
⊕⊝⊝⊝ very lowc,d |
High heterogeneity (I2 = 78%) |
|
Live birth rate per woman Participants with BMI ≥ 30 kg/m2a |
198 per 1000 | 69 per 1000 (40 to 114) |
OR 0.30 (0.17 to 0.52) |
500 (2 studies) |
⊕⊝⊝⊝ very lowc,d | 74 events |
|
Adverse events (gastrointestinal) |
Not reported by any of the included studies | |||||
| Clinical pregnancy rate per woman Participants with BMI < 30 kg/m2 or ≤ 32 kg/m2a | 320 per 1000 | 423 per 1000 (331 to 523) | OR 1.56 (1.05 to 2.33) | 490 (5 studies) | ⊕⊝⊝⊝ very lowc,d | 103 events |
| Clinical pregnancy rate per woman Participants with BMI ≥ 30 kg/m2a | 234 per 1000 | 94 per 1000 (60 to 144) | OR 0.34 (0.21 to 0.55) | 500 (2 studies) | ⊕⊝⊝⊝ very lowc,d | 98 events |
| Menstrual frequency | Not reported by any of the included studies | |||||
|
Ovulation rate per woman Participants with BMI < 30 kg/m2b |
625 per 1000 | 574 per 1000 (459 to 681) | OR 0.81 (0.51 to 1.28) | 312 (4 studies) | ⊕⊕⊝⊝ lowc | |
|
Ovulation rate per woman Participants with BMI ≥ 30 kg/m2b |
534per 1000 | 250per 1,000 (187 to 330) | OR 0.29 (0.20 to 0.43) | 500 (2 studies) | ⊕⊕⊝⊝ lowc | |
| Miscarriage rate per woman | 29 per 1000 | 26 per 1000 (15 to 47) |
OR 0.92 (0.50 to 1.67) | 741 (5 studies) | ⊕⊝⊝⊝ very lowc,e |
High heterogeneity (I2 = 52%) |
| *The risk in the intervention group (and its 95% confidence interval) is based on the median risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aData subgrouped by BMI, as pooling of BMI groups resulted in high heterogeneity (I2 > 85%) with differing directions of effect. bData subgrouped by BMI, as pooling of BMI groups resulted in high heterogeneity (I2 = 74%), though direction of effect was consistent. cEvidence downgraded two levels for very serious risk of bias, due to failure to report study methods and/or risk of attrition bias in one or more studies and because findings are based on subgroup analysis. dEvidence downgraded one level for serious imprecision: low event rate (total 74 events). eEvidence downgraded for serious inconsistency (where further downgrading feasible).
1. Metformin versus placebo or no treatment
1.1 Live birth rate
When we compared metformin to placebo, only a limited number of studies reported live birth rate (Morin‐Papunen 2012; Ng 2001; PCOSMIC 2010; Yarali 2002). When we pooled these four studies, there was marginal evidence of a difference in live birth rate favouring metformin, with a number needed to treat for an additional beneficial outcome of 13 women (OR 1.59, 95% CI 1.00 to 2.51, 4 studies, 435 women, I2 = 0%, low‐quality evidence (Analysis 1.1). However, the wide‐ranging confidence intervals and low evidence quality make the advantage offered by metformin difficult to interpret clinically.
In the subgroup analysis by obesity status the test for subgroup differences showed no evidence of a difference between the subgroups. There was no clear evidence of a difference in live birth rate in either subgroup (BMI of < 30 kg/m2: OR 1.51, 95% CI 0.94 to 2.44, 3 studies, 370 women, I2 = 0% or BMI > 30 kg/m2: OR 2.87, 95% CI 0.51 to 16.01, 1 study, 65 women, I2 = 0%) (Analysis 1.1). However, the broad confidence intervals due to reducing the number of combined studies for this analysis, render the results unclear. A sensitivity analysis, which excluded studies with unclear or high risk of bias left two studies remaining (Morin‐Papunen 2012; PCOSMIC 2010) (OR 1.64, 95% CI 1.02 to 2.63, 2 studies, 385 women, I2 = 0%). It should be noted that the women in these two studies had a BMI greater than 30 kg/m2. The large and good‐quality study by Morin‐Papunen 2012 contributed 93.8% of the weight of the result (OR 0.95, 95% CI 0.95 to 2.55, 320 women). These results therefore suggest a potential benefit in live birth rate when using metformin compared with placebo, although the number of studies were small.
1.2 Adverse events
1.2. Analysis.
Comparison 1 Metformin versus placebo or no treatment, Outcome 2 Adverse events (gastrointestinal side effects).
Women in the metformin group experienced a higher incidence of gastrointestinal side effects than the placebo group (OR 4.76, 95% CI 3.06 to 7.41, 7 studies, 670 women, I2 = 61%, moderate‐quality evidence). In the subgroup analysis by obesity status, the test for subgroup differences showed no evidence of a difference between the subgroups. Sensitivity analysis, which excluded studies with unclear or high risk of bias did not change the inference.
1.3 Clinical pregnancy rate
1.3. Analysis.
Comparison 1 Metformin versus placebo or no treatment, Outcome 3 Clinical pregnancy rate.
Nine trials reported clinical pregnancy rates (Fleming 2002; Karimzadeh 2007; Karimzadeh 2010; Lord 2006; Morin‐Papunen 2012; Ng 2001; PCOSMIC 2010; Tang 2006; Yarali 2002) (Analysis 1.3). Pregnancy rates were higher in the metformin arm (OR 1.93, 95% CI 1.42 to 2.64, 9 studies, 1027 women, I2 = 43%, moderate‐quality evidence). In subgroup analysis by obesity status the test for subgroup differences showed no evidence of a difference between the subgroups. In an attempt to improve heterogeneity we performed a sensitivity analysis, which excluded studies with unclear or high risk of bias, including the following studies (Fleming 2002; Karimzadeh 2007; Lord 2006; Machado 2012; Morin‐Papunen 2012; Ng 2001; PCOSMIC 2010; Tang 2006). However, this did not alter the inference or improve heterogeneity.
1.4 Ovulation rate
1.4. Analysis.
Comparison 1 Metformin versus placebo or no treatment, Outcome 4 Ovulation rate.
There was evidence of a benefit from metformin with respect to the ovulation rate per participant (OR 2.55, 95% CI 1.81 to 3.59, 14 studies, 701 women, I2 = 58%, moderate‐quality evidence). We have presented ovulation rate per cycle in an additional table (Table 6). Subgroup analysis by obesity status suggested a significant difference between the subgroups (test for subgroup differences: Chi² = 4.11, df = 1, P = 0.04, I² = 75.7%), with a stronger benefit from metformin in the non‐obese group (OR 4.15, 95% CI 2.31 to 7.45). However heterogeneity in this subgroup was very high (I2 = 82%) and was attributable to a single study (Baillargeon 2004); when this study was excluded from analysis there was no longer any suggestion of a difference between the subgroups (I2 = 0%). When both subgroups were pooled, heterogeneity was improved after sensitivity analysis by study quality, which included only five studies (Fleming 2002; Hoeger 2004; Lord 2006; Ng 2001; PCOSMIC 2010), with an overall I2 of 0% . However, the overall inference remained unchanged.
1.5 Menstrual frequency
1.5. Analysis.
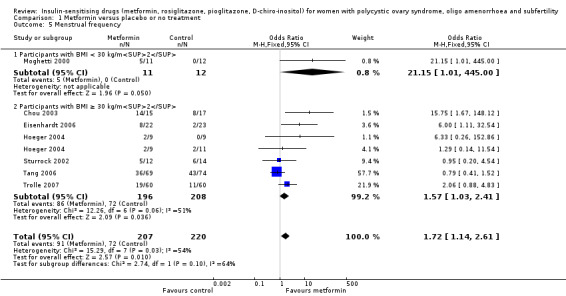
Comparison 1 Metformin versus placebo or no treatment, Outcome 5 Menstrual frequency.
There was evidence of a beneficial effect of metformin on menstrual frequency with an OR of 1.72 (95% CI 1.14 to 2.61, 7 studies, 427 women, I2 = 54%). Due to only one trial in the non‐obese group, subgroup analysis did not improve the heterogeneity. In subgroup analysis by obesity status the test for subgroup differences showed no evidence of a difference between the subgroups. Sensitivity analysis, which excluded studies with unclear or high risk of bias, included five studies (Chou 2003; Eisenhardt 2006; Fleming 2002; Hoeger 2004; Tang 2006); this did not improve heterogeneity and did not change the inference.
1.6 Miscarriage
1.6. Analysis.
Comparison 1 Metformin versus placebo or no treatment, Outcome 6 Miscarriage rate per woman.
Four studies reported on miscarriage and there was no conclusive evidence of a difference between metformin and placebo in miscarriage rate per woman (OR 1.08, 95% CI 0.50 to 2.35, 4 studies, 748 women, I2 = 0%). A sensitivity analysis using per pregnancy rates was also inconclusive (OR 0.58, 95% CI 0.25 to 1.34, 4 studies, 200 pregnancies, I2 = 0%, low‐quality evidence). A subgroup analysis by obesity status showed no evidence of a difference between the subgroups. However, only one study was available with women with BMI more than 30 kg/m2 (PCOSMIC 2010).
1.7 Multiple pregnancy
Data were not available for this outcome.
1.8 Anthropometric outcomes
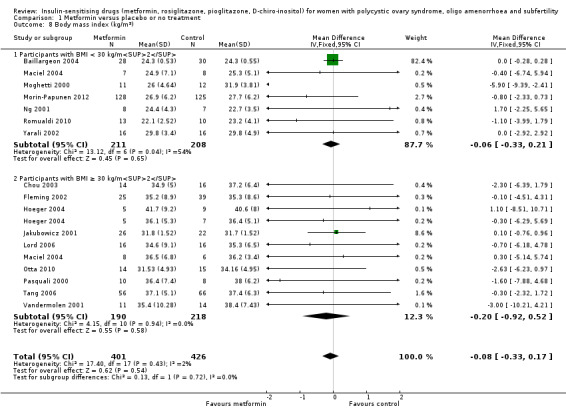
BMI
There was no clear evidence of an effect of metformin on BMI (MD ‐0.08, 95% CI ‐0.33 to 0.17, 16 studies, 827 women, I2 = 2%) (Analysis 1.8) with an average duration of treatment of 5.75 months and average dose of 1500 mg. Baillargeon 2004 provided 82% of the weight of this analysis, which found no significant evidence of a difference in BMI (MD 0.00, 95% CI ‐0.28 to 0.28). The other studies are smaller as reflected in their broader confidence intervals. Overall heterogeneity was low (I2 = 2%); but was moderately high in the non‐obese group (I2 = 54%). Sensitivity analysis by study quality (Baillargeon 2004; Chou 2003; Fleming 2002; Hoeger 2004; Lord 2006; Maciel 2004; Morin‐Papunen 2012; Ng 2001; Pasquali 2000; Tang 2006) improved heterogeneity (non‐obese group I2 = 0%; obese group I2 = 0%) but did not change the inference.
1.8. Analysis.
Comparison 1 Metformin versus placebo or no treatment, Outcome 8 Body mass index (kg/m2).
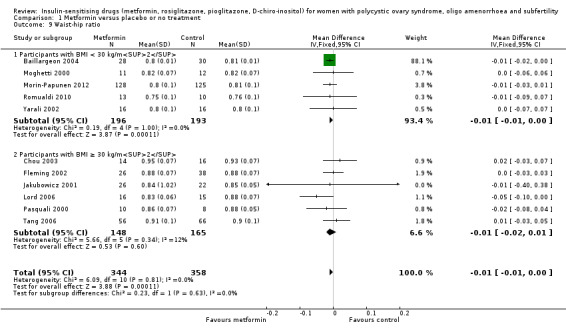
Waist to hip ratio
There was evidence of a marginal benefit from metformin on waist to hip ratio (MD ‐0.01, 95% CI ‐0.01 to 0.00, 11 studies, 702 women) (Analysis 1.9). The magnitude of heterogeneity was low in both the non‐obese and the obese subgroups (I2 = 0% and I2 = 12%, respectively). The sensitivity analysis by study quality (Baillargeon 2004; Chou 2003; Fleming 2002; Lord 2006; Morin‐Papunen 2012; Pasquali 2000; Tang 2006) demonstrated a similar inference.
1.9. Analysis.
Comparison 1 Metformin versus placebo or no treatment, Outcome 9 Waist‐hip ratio.
Blood pressure
Metformin reduced systolic blood pressure with a mean difference of ‐3.59 mm Hg (95% CI ‐5.13 to ‐2.04, 7 studies, 379 women) (Analysis 1.10) and significant heterogeneity (I2 = 57%). However, we did not observe a similar benefit in the diastolic blood pressure (MD ‐0.14, 95% CI ‐1.35 to 1.07, 6 studies, 292 women, I2 = 21% (Analysis 1.11). Furthermore, neither subgroup analysis (Analysis 1.10) nor sensitivity analysis by study quality (Baillargeon 2004; Chou 2003; Lord 2006; Maciel 2004; Tang 2006) improved heterogeneity in the systolic blood pressure analysis.
1.10. Analysis.
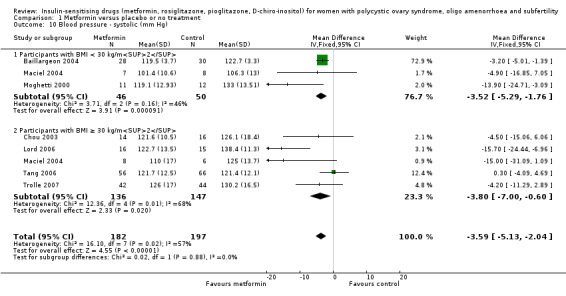
Comparison 1 Metformin versus placebo or no treatment, Outcome 10 Blood pressure ‐ systolic (mm Hg).
1.11. Analysis.
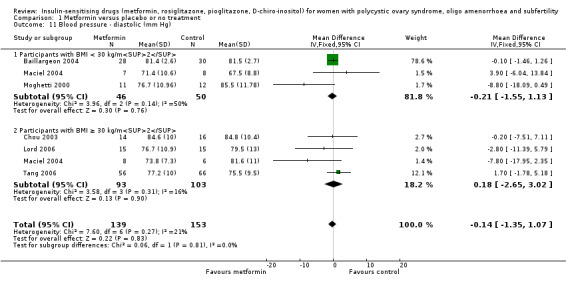
Comparison 1 Metformin versus placebo or no treatment, Outcome 11 Blood pressure ‐ diastolic (mm Hg).
1.9 Endocrine outcomes
Testosterone
There was evidence that metformin reduced serum total testosterone levels with a MD of ‐0.49 nmol/L (95% CI ‐0.59 to ‐0.39, 15 studies, 863 women, I2 = 92%) (Analysis 1.12). However, we observed high heterogeneity (I2 = 92%). In subgroup analysis by BMI, there was evidence of a difference between the subgroups (test for subgroup differences: Chi² = 15.68, df = 1, P = < 0.00001, I2 = 93.6%) with metformin having a stronger effect in the non‐obese group (MD ‐0.71 versus ‐0.29 nmol/L). Linear regression analysis did not demonstrate any correlation between the baseline mean BMI and the mean fasting insulin concentrations among all the included studies (data not shown). Furthermore, we did not observe a positive correlation between the baseline mean fasting insulin concentrations and the mean testosterone concentrations (data not shown). These data suggested that the heterogeneity may have been caused by the different background prevalence in hyperandrogenism and insulin resistance among different study populations (Wijeyaratne 2002; Wijeyaratne 2004). Furthermore, different biochemical assays used in different studies could contribute towards this heterogeneity. Sensitivity analysis by study quality did not improve the heterogeneity. However, removing the two extreme results (Baillargeon 2004; Jakubowicz 2001) improved heterogeneity (non‐obese group I2 = 49%; obese group I2 = 44%) without altering the inference.
1.12. Analysis.
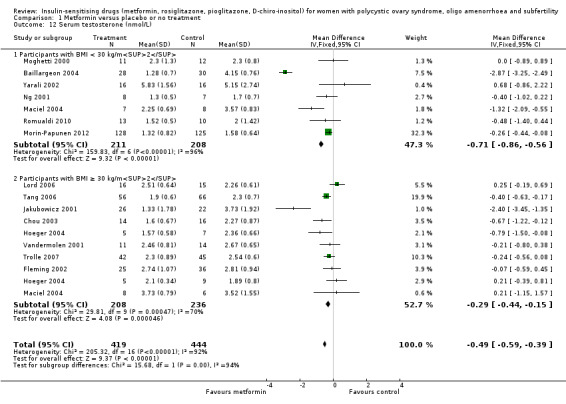
Comparison 1 Metformin versus placebo or no treatment, Outcome 12 Serum testosterone (nmol/L).
Sex hormone‐binding globulin
There was no convincing evidence of an effect of metformin on serum sex hormone‐binding globulin levels (MD 0.49, 95% CI ‐1.82 to 2.81, 15 studies, 823 women, I2 = 62%) (Analysis 1.13). Neither the subgroup analysis nor the sensitivity analysis by study quality improved heterogeneity or changed the inference.
1.13. Analysis.
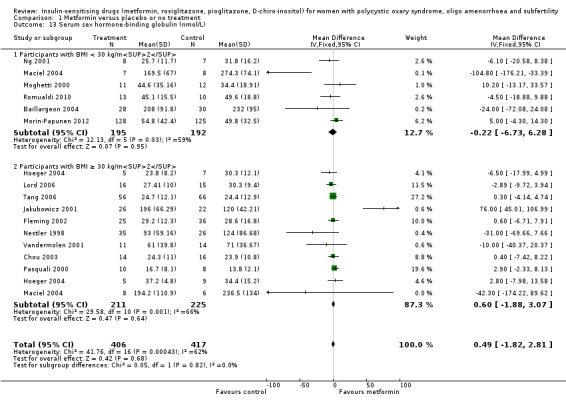
Comparison 1 Metformin versus placebo or no treatment, Outcome 13 Serum sex hormone‐binding globulin (nmol/L).
1.10 Metabolic outcomes
Glucose
There was evidence of a reduction in fasting glucose levels with metformin compared to placebo (MD ‐0.14 mmol/L, 95% CI ‐0.21 to ‐0.07, 15 studies, 849 women, I2 = 38%) (Analysis 1.14). Subgroup analysis only improved heterogeneity in the obese group (I2 = 14%) without changing the inference. Sensitivity analysis by study quality (Baillargeon 2004; Chou 2003; Fleming 2002; Hoeger 2004; Maciel 2004; Morin‐Papunen 2012; Pasquali 2000; Tang 2006) eliminated overall heterogeneity (I2 = 0%) and the results indicated no evidence of metformin on fasting glucose concentrations (MD 0 mmol/L, 95% CI ‐0.13 to 0.12).
1.14. Analysis.
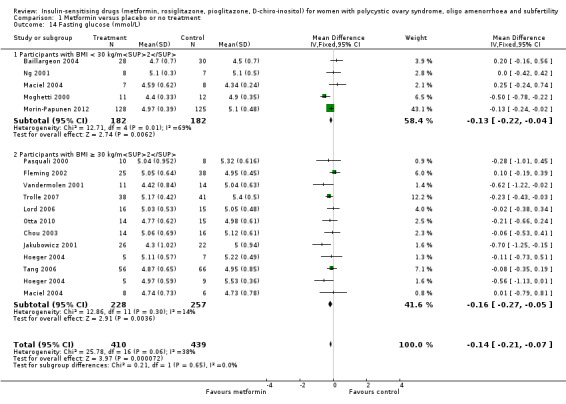
Comparison 1 Metformin versus placebo or no treatment, Outcome 14 Fasting glucose (mmol/L).
Insulin
Metformin reduced fasting insulin levels with a MD of ‐4.13 mIU/L (95% CI ‐5.67 to ‐2.58, 14 studies, 573 women) (Analysis 1.15) but with significant heterogeneity (I2 = 63%). In subgroup analysis by BMI the test for subgroup differences showed no evidence of a difference between the subgroups. Sensitivity analysis by study quality (Chou 2003; Fleming 2002; Hoeger 2004; Lord 2006; Maciel 2004; Morin‐Papunen 2012; Ng 2001; Pasquali 2000; Tang 2006) did not improve the heterogeneity. Once again, the heterogeneity was likely to be caused by variations in background prevalences of hyperandrogenism and insulin resistance among different study populations.
1.15. Analysis.
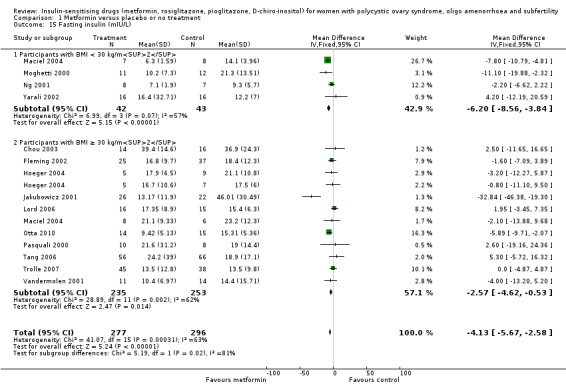
Comparison 1 Metformin versus placebo or no treatment, Outcome 15 Fasting insulin (mIU/L).
Cholesterol
When we combined 11 studies, there was no conclusive evidence of a difference in serum cholesterol with the use of metformin (MD ‐0.14 mmol/L, 95% CI ‐0.31 to 0.02, 11 studies, 562 women, I2 = 62%, Analysis 1.16). However, in subgroup analysis by BMI,the test for subgroup differences showed no conclusive evidence of a difference between the subgroups (test for subgroup differences: Chi² = 2.02, df = 1, P = 0.15, I² = 50.6%).
1.16. Analysis.
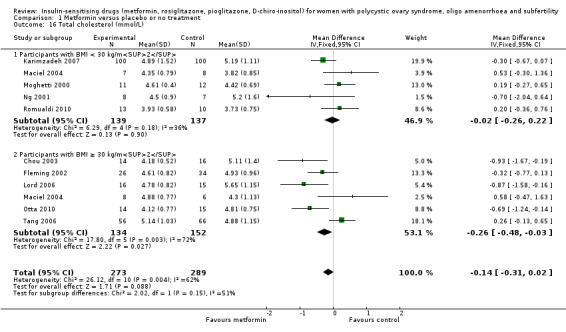
Comparison 1 Metformin versus placebo or no treatment, Outcome 16 Total cholesterol (mmol/L).
Triglycerides
In general, the current review showed that there was no conclusive evidence of a difference in serum triglycerides with the use of metformin (MD 0.14 mmol/L, 95% CI ‐0.05 to 0.32, 7 studies, 309 women, I2 = 0%) (Analysis 1.17). Neither subgroup analysis nor sensitivity analysis by study quality changed the inference, however the number of participants was low, and the results show broad confidence intervals.
1.17. Analysis.
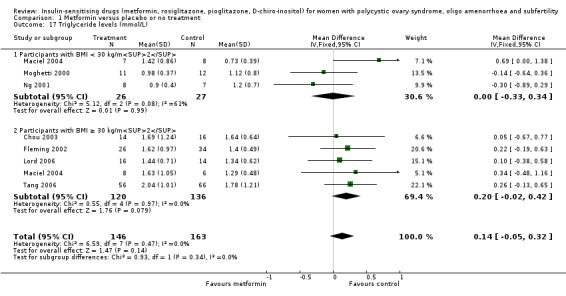
Comparison 1 Metformin versus placebo or no treatment, Outcome 17 Triglyceride levels (mmol/L).
2. Metformin with clomiphene citrate versus clomiphene citrate alone
2.1 Live birth rate
There was no conclusive evidence of a difference in live births when metformin in combination with clomiphene citrate was compared with clomiphene citrate alone (OR 1.21, 95% CI 0.92 to 1.59, 9 studies, 1079 women, I2 = 20%, low‐quality evidence).
In subgroup analysis, the test for subgroup differences showed no evidence of a difference between the subgroups: obese group (OR 1.28, 95% CI 0.86 to 1.91, 4 studies, 548 women), non‐obese group (OR 1.14, 95% CI 0.78 to 1.67, 5 studies, 531 women).
Sensitivity analysis by evidence quality (Legro 2007; Moll 2006; Morin‐Papunen 2012; PCOSMIC 2010), with 816 women, also did not change the inference nor improve heterogeneity.
2.2 Adverse events
2.2. Analysis.
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 2 Adverse events.
There was evidence of more frequent gastrointestinal side effects in the metformin group, including nausea and vomiting (OR 3.97, 95% CI 2.59 to 6.08, 3 studies, 591 women, I2 = 47%, moderate‐quality evidence) compared with the control group. All participants in this analysis were non‐obese. Sensitivity analysis by study quality did not change our findings.
2.3 Clinical pregnancy rate
2.3. Analysis.
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 3 Clinical pregnancy rate.
When combined with clomiphene citrate, there was evidence that metformin had a beneficial effect on pregnancy rate compared to clomiphene citrate alone (OR 1.59, 95% CI 1.27 to 1.99, 16 studies, 1529 women, I2 = 33%, moderate‐quality evidence).
In subgroup analysis, the test for subgroup differences showed no evidence of a difference between the subgroups: the effect on pregnancy rates was seen in both analyses: obese group (OR 1.76, 95% CI 1.26 to 2.47, 7 studies, 695 women) and non‐obese group (OR 1.46, 95% CI 1.08 to 1.98, 9 studies, 834 women). Sensitivity analysis by study quality (Legro 2007; Moll 2006; Morin‐Papunen 2012), with 745 participants, did not change the inference or improve heterogeneity.
2.4 Ovulation rate
2.4. Analysis.
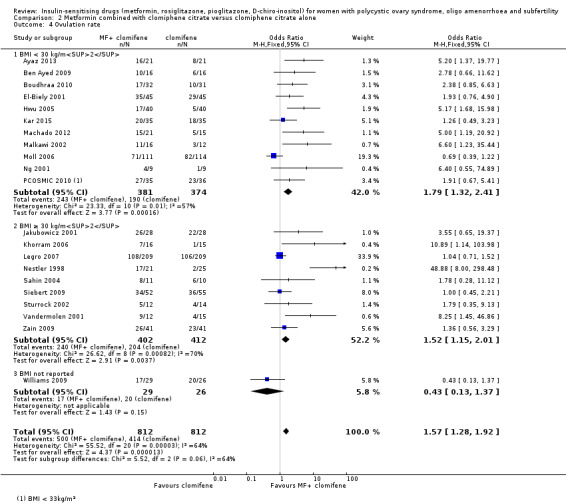
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 4 Ovulation rate.
2.5. Analysis.
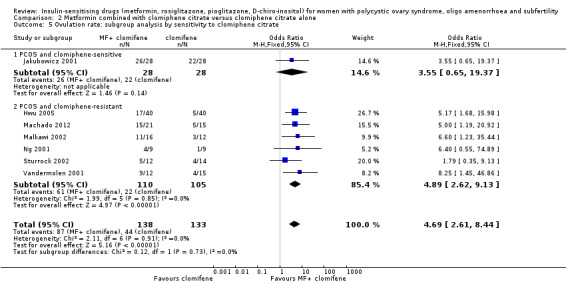
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 5 Ovulation rate: subgroup analysis by sensitivity to clomiphene citrate.
There was evidence of a beneficial effect for metformin combined with clomiphene citrate versus clomiphene citrate alone on ovulation per woman, (OR 1.57, 95% CI 1.28 to 1.92, 21 studies, 1624 women, I2 = 64%, moderate‐quality evidence). We have presented ovulation rate per cycle in an additional table (Table 7). In subgroup analysis, the test for subgroup differences showed no evidence of a difference between the subgroups. Heterogenity remained high (I2 = 70%) in the obese sub group, but the direction of effect was consistent. We conducted a subgroup analysis based on sensitivity to clomiphene citrate. Seven studies were available that had recorded clomiphene citrate‐resistance status. Six of these included women with clomiphene citrate resistance (Hwu 2005; Machado 2012; Malkawi 2002; Ng 2001; Sturrock 2002; Vandermolen 2001). This analysis showed an improvement in ovulation rate with combined therapy (OR 4.89, 95% CI 2.62 to 9.13, 6 studies, 215 women, I2 = 0%, moderate‐quality evidence). Only one small study of clomiphene citrate‐sensitive women was available, and a conclusion cannot be drawn from the result (OR 3.55, 95% CI 0.65 to 19.37, 56 women). Sensitivity analysis by study quality (Legro 2007; Moll 2006; Ng 2001; PCOSMIC 2010) did not alter our findings.
2.5 Menstrual frequency
Data were not available for this outcome.
2.6 Miscarriage rate
2.6. Analysis.
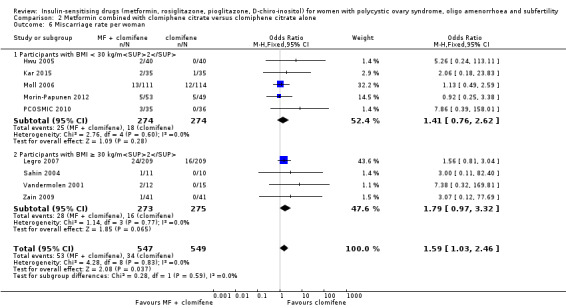
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 6 Miscarriage rate per woman.
2.7. Analysis.
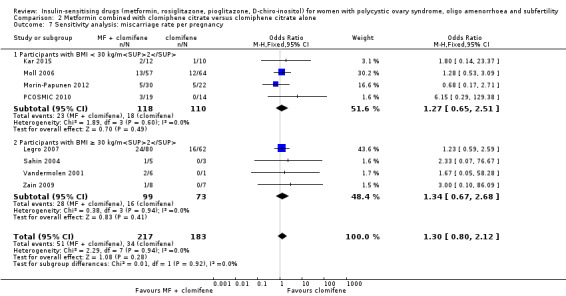
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 7 Sensitivity analysis: miscarriage rate per pregnancy.
When we pooled the data from nine studies, we detected a difference in miscarriage rate per woman (OR 1.59, 95% CI 1.03 to 2.46, 9 studies, 1096 women I2 = 0%, low‐quality evidence). This suggests that the likelihood of miscarriage may be greater with combined therapy than when clomiphene citrate is used alone. When we analysed a subgroup by BMI, the test for subgroup differences showed no evidence of a difference between the subgroups. When we performed an analysis of miscarriage rate per pregnancy, there was no clear evidence of a difference between the groups (OR 1.30, 95% CI 0.80 to 2.12, 400 pregnancies, I2 = 0%), still with no evidence of a difference between the BMI subgroups. Sensitivity analysis by study quality (Legro 2007; Moll 2006; Morin‐Papunen 2012; PCOSMIC 2010) also did not alter the inference. Any increase in miscarriage conferred by using clomiphene citrate therapy in isolation is therefore difficult to interpret and apply clinically.
2.7 Multiple pregnancy rate
2.8. Analysis.
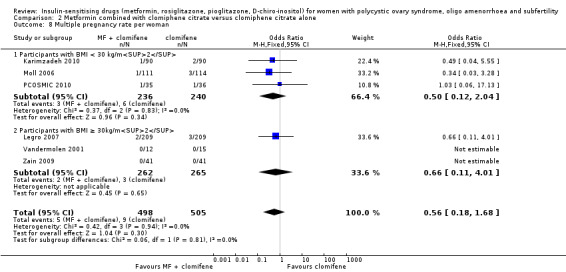
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 8 Multiple pregnancy rate per woman.
2.9. Analysis.
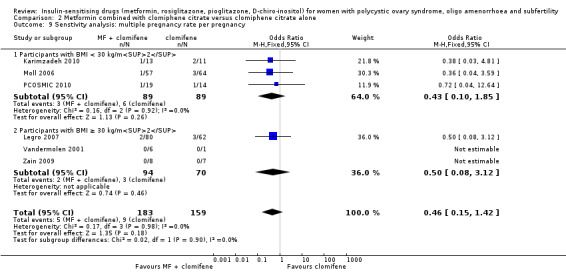
Comparison 2 Metformin combined with clomiphene citrate versus clomiphene citrate alone, Outcome 9 Senstivity analysis: multiple pregnancy rate per pregnancy.
There was no conclusive evidence of a difference between metformin combined with clomiphene citrate versus clomiphene citrate alone (OR 0.56, 95% CI 0.18 to 1.68, 6 studies, 1003 women, I2=0%). Sensitivity analysis using per pregnancy rates did not produce different findings
(OR 0.46, 95% CI 0.15 to 1.42, 6 studies, 342 pregnancies, I2 = 0%). Sensitivity analysis by study quality (Legro 2007; Moll 2006; PCOSMIC 2010) did not alter the inference either.
Other outcomes
Data were not available for anthropometric, endocrine or metabolic outcomes.
3. Metformin versus clomiphene citrate
3.1 Live birth rate
When we combined the data from five studies (Kar 2015; Legro 2007; Palomba 2005; PCOSMIC 2010; Zain 2009), there was no conclusive evidence of a difference between the groups, with high heterogeneity (OR 0.71, 95% CI 0.49 to 1.01, 5 studies, 741 women, I2 = 86%, very low‐quality evidence) (Analysis 3.1). However, in the subgroup analysis by obesity status, there was evidence of a difference between the subgroups (test for subgroup differences: Chi² = 19.41, df = 1, P < 0.0001, I2 = 94.8%). Among obese women, live births were lower in the metformin group (OR 0.30, 95% CI 0.17 to 0.52, 2 studies, 500 women); 62% of the weight of this finding was provided by a single study (Legro 2007). In the non‐obese subgroup the direction of effect favoured metformin with high heterogeneity (OR 1.71, 95% CI 1.00 to 2.94, 3 studies, 241 women, I2 = 78%, very low‐quality evidence).
3.2 Adverse events
Data were not available for this outcome.
3.3 Clinical pregnancy rate
3.2. Analysis.
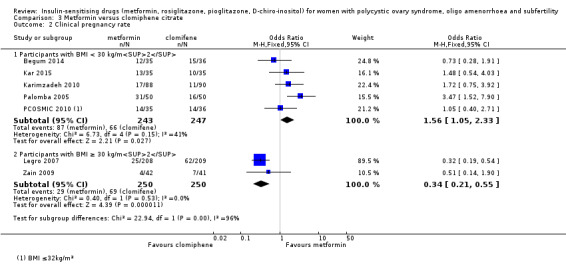
Comparison 3 Metformin versus clomiphene citrate, Outcome 2 Clinical pregnancy rate.
The overall heterogeneity was high (I2 = 86%) and the data were not appropriate to be pooled. However, subgroup analysis by obesity status showed evidence of a difference between the subgroups (test for subgroup differences: Chi² = 22.94, df = 1, P < 0.00001, I2 = 95.6%). In the non‐obese group, there was evidence of higher pregnancy rates in women who took metformin compared to those who took clomiphene citrate (OR 1.56, 95% CI 1.05 to 2.33, 5 studies, 490 women, I2 = 41%, very low‐quality evidence) whilst a different effect was observed in the obese group (OR 0.34, 95% CI 0.21 to 0.55, 2 studies, 500 women, I2 = 0%, very low‐quality evidence). Sensitivity analysis by study quality did not change the inference.
3.4 Ovulation rate
3.3. Analysis.
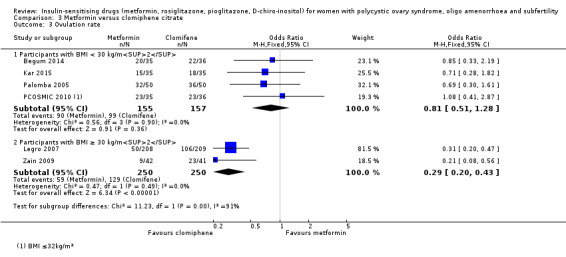
Comparison 3 Metformin versus clomiphene citrate, Outcome 3 Ovulation rate.
The overall heterogeneity was high (I2 = 74%) and the data were not appropriate to be pooled.
Subgroup analysis by obesity status again showed evidence of a difference between the subgroups (test for subgroup differences: Chi² = 11.23, df = 1, P = 0.0008, I² = 91.1%). In the obese group, combining the results from Legro 2007 and Zain 2009 found improved ovulation rates with clomiphene citrate therapy (OR 0.29, 95% CI 0.20 to 0.43, 2 studies, 500 women, 2044 cycles, I2 = 0%). In the non‐obese group, the data were inconclusive. Sensitivity analysis by study quality did not change the inference. We have presented ovulation rate per cycle in an additional table (Table 8).
3.5 Menstrual frequency
Data were not available for this outcome.
3.6 Miscarriage rate
3.4. Analysis.
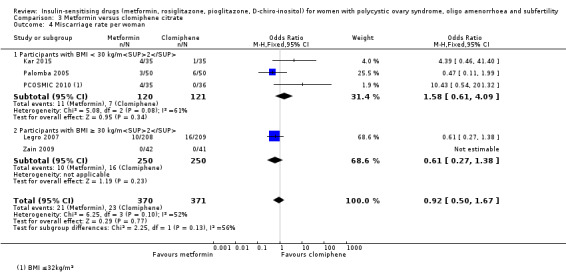
Comparison 3 Metformin versus clomiphene citrate, Outcome 4 Miscarriage rate per woman.
3.5. Analysis.
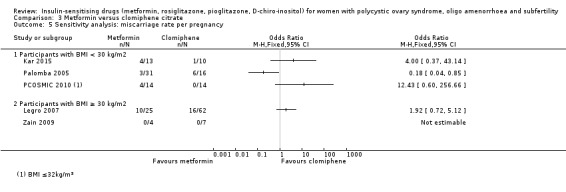
Comparison 3 Metformin versus clomiphene citrate, Outcome 5 Sensitivity analysis: miscarriage rate per pregnancy.
The data regarding miscarriage rate with either clomiphene citrate or metformin treatment were inconclusive across both BMI groups (OR 0.92, 95% CI 0.50 to 1.67, 5 studies, 741 women, I2 = 52%).
Per‐pregnancy data were unsuitable for pooling in a subgroup analysis due to high heterogeneity (I2 = 78%) and differing directions of effect, so no conclusions could be drawn. Neither subgroup analysis by obesity status nor sensitivity analysis by study quality improved the heterogeneity in the per‐pregnancy analysis.
3.7 Multiple pregnancy rate
3.6. Analysis.
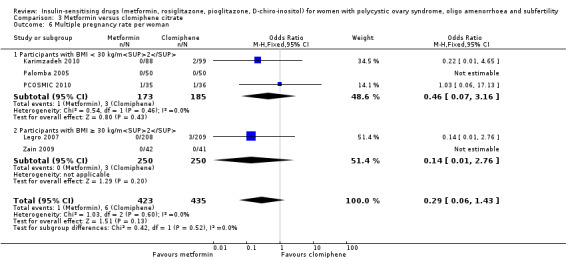
Comparison 3 Metformin versus clomiphene citrate, Outcome 6 Multiple pregnancy rate per woman.
3.7. Analysis.
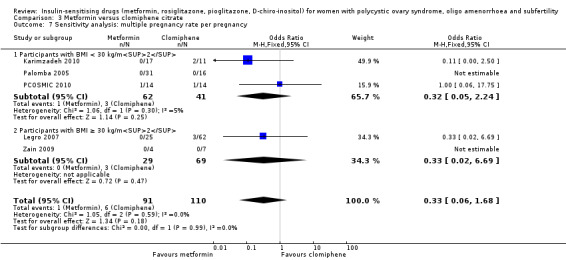
Comparison 3 Metformin versus clomiphene citrate, Outcome 7 Sensitivity analysis: multiple pregnancy rate per pregnancy.
There was no conclusive evidence of a difference between the groups (0.29, 95% CI 0.06 to 1.43, 5 studies, 858 women, I2 = 0%). In the subgroup analysis by obesity status, there was no evidence of a difference between the subgroups. Sensitivity analysis by study quality did not change the inference.
Other outcomes
Data were not available for anthropometric, endocrine or metabolic outcomes.
4 D‐chiro‐inositol versus placebo or no treatment
Although two trials were included (Gerli 2003; Nestler 1999), the number of women in the analysis remained small. Furthermore, one of the trials (Gerli 2003) reported analysable data for only one outcome of interest (ovulation rate, moderate‐quality evidence). It would be difficult to make any conclusions based on the current findings.
4.1 Live birth
Data were not available for this outcome.
4.2 Adverse events
Data were not available for this outcome.
4.3 Clinical pregnancy
Data were not available for this outcome.
4.4 Ovulation rate
4.1. Analysis.
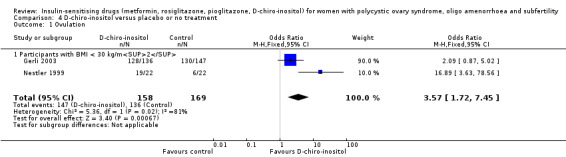
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 1 Ovulation.
The data suggested that D‐chiro‐inositol may improve ovulation rates per woman (OR 3.57, 95% CI 1.72 to 7.45; 2 studies, 327 women, I2 = 81%), however there were only two studies and the results correspondingly show very wide confidence intervals. Neither a subgroup analysis nor sensitivity analysis were possible due to the inadequate number of studies. We have presented ovulation rate per cycle in an additional table (Table 9).
Other outcomes
Data were not available for other reproductive outcomes.
1.8 Anthropometric outcomes
(Analysis 4.2; Analysis 4.3; Analysis 4.4; Analysis 4.5)
4.2. Analysis.
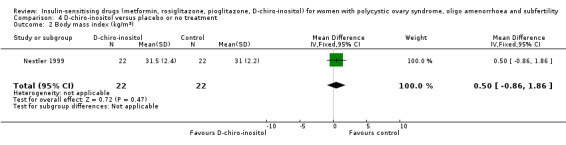
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 2 Body mass index (kg/m2).
4.3. Analysis.
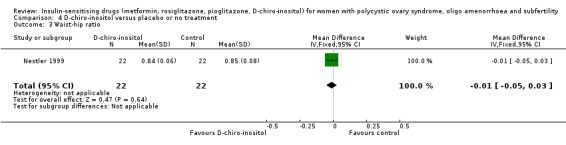
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 3 Waist‐hip ratio.
4.4. Analysis.
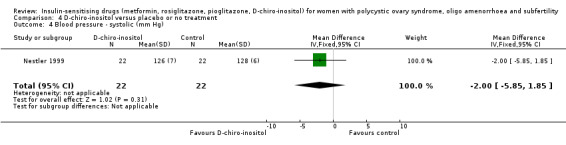
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 4 Blood pressure ‐ systolic (mm Hg).
4.5. Analysis.
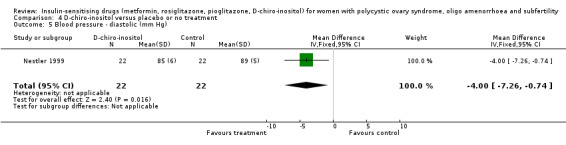
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 5 Blood pressure ‐ diastolic (mm Hg).
Only one study, with 44 women (Nestler 1999) was included in the analysis. There was no conclusive evidence that D‐chiro‐inositol had an effect on BMI, waist to hip ratio or blood pressure.
1.9, 1.10 Endocrine and metabolic outcomes
(Analysis 4.6; Analysis 4.7; Analysis 4.8; Analysis 4.9; Analysis 4.10; Analysis 4.11)
4.6. Analysis.
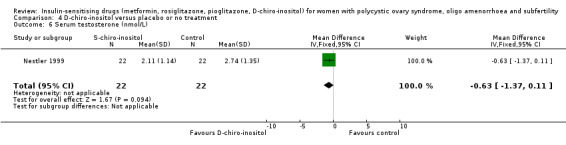
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 6 Serum testosterone (nmol/L).
4.7. Analysis.
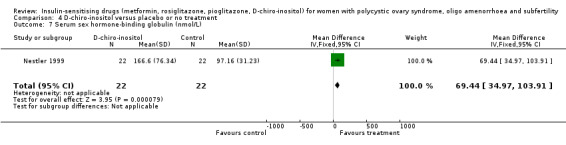
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 7 Serum sex hormone‐binding globulin (nmol/L).
4.8. Analysis.
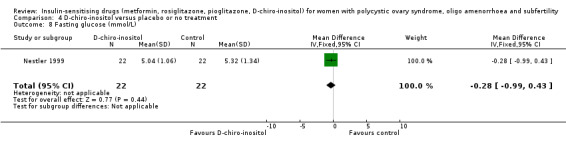
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 8 Fasting glucose (mmol/L).
4.9. Analysis.
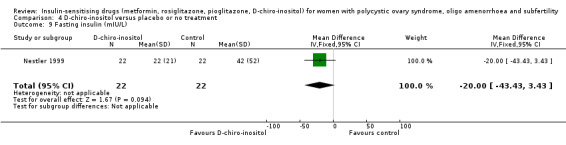
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 9 Fasting insulin (mIU/L).
4.10. Analysis.
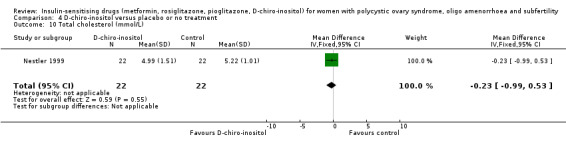
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 10 Total cholesterol (mmol/L).
4.11. Analysis.
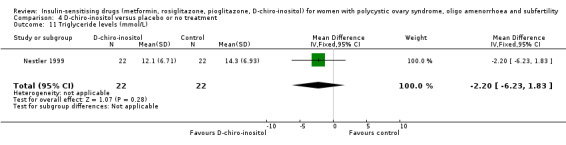
Comparison 4 D‐chiro‐inositol versus placebo or no treatment, Outcome 11 Triglyceride levels (mmol/L).
Only one study (Nestler 1999) was included in the analysis. There was no conclusive evidence that D‐chiro‐inositol had an effect on these parameters (i.e. testosterone, sex hormone‐binding globulin, fasting glucose, fasting insulin, lipids (total cholesterol, triglycerides) except for serum sex hormone‐binding globulin levels.
5 Rosiglitazone versus placebo or no treatment
Three trials were included in the current review. Due to the withdrawal of troglitazone from the market, the drug used in the trials was either rosiglitazone or pioglitazone.
Data were not available for primary outcomes, but were available for some secondary outcomes, including ovulation rate, menstrual frequency and anthropometric, endocrine and metabolic outcomes.
5.4 Ovulation rate
5.1. Analysis.
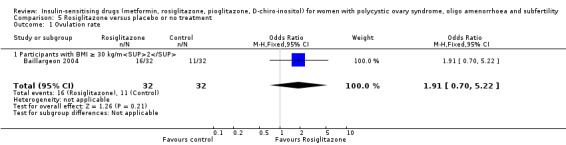
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 1 Ovulation rate.
Only the Baillargeon 2004 study of 64 women was available for this outcome (OR 1.91, 95% CI 0.70 to 5.22, 64 women, very low‐quality evidence), so no conclusions can be drawn. We have presented ovulation rate per cycle in an additional table (Table 10).
5.5 Menstrual frequency
5.2. Analysis.
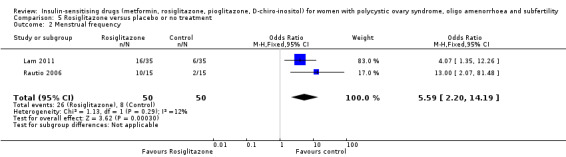
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 2 Menstrual frequency.
Evidence of an improvement in menstrual pattern with rosiglitazone was observed in two studies (OR 5.59, 95% CI 2.20 to 14.19; 2 studies, 100 women, I2 = 12%).
5.8 Anthropometric outcomes
Women who took rosiglitazone were found to have an increased BMI (MD 0.68, 95% CI 0.40 to 0.96, 3 studies, 132 women, I2 = 15%) (Analysis 5.3 ).
5.3. Analysis.
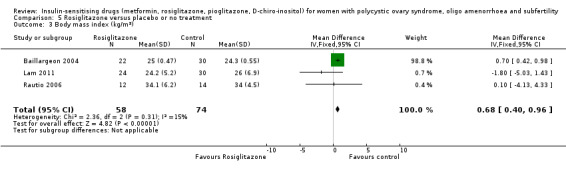
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 3 Body mass index (kg/m2).
Rosiglitazone was found to have a marginal benefit on waist to hip ratio (MD ‐0.01, 95% CI ‐0.02 to 0.00, 3 studies, 132 women, I2 = 0%, Analysis 5.4).
5.4. Analysis.
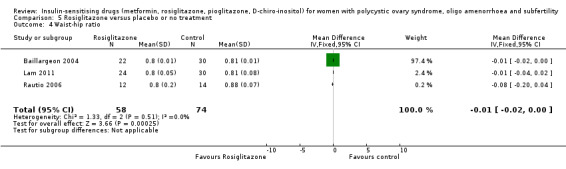
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 4 Waist‐hip ratio.
Based on one study (Baillargeon 2004), the effect on blood pressure was small (Analysis 5.5; Analysis 5.6).
5.5. Analysis.
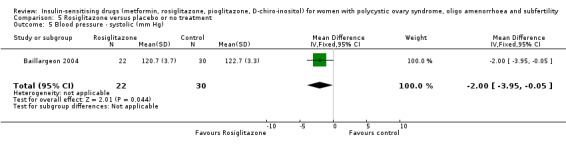
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 5 Blood pressure ‐ systolic (mm Hg).
5.6. Analysis.
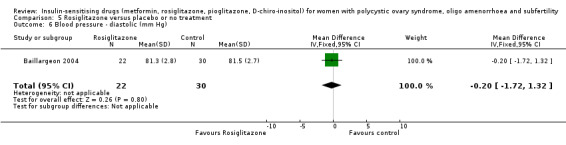
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 6 Blood pressure ‐ diastolic (mm Hg).
5.9, 5.10 Endocrine and metabolic outcomes
The effects on testosterone, sex hormone‐binding globulin, insulin, glucose, cholesterol and triglyceride were found to be minimal (Analysis 5.7; Analysis 5.8; Analysis 5.9; Analysis 5.10; Analysis 5.11; Analysis 5.12).
5.7. Analysis.
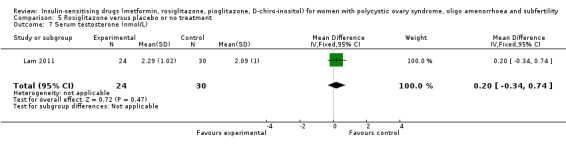
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 7 Serum testosterone (nmol/L).
5.8. Analysis.
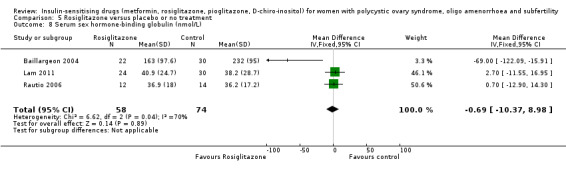
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 8 Serum sex hormone‐binding globulin (nmol/L).
5.9. Analysis.
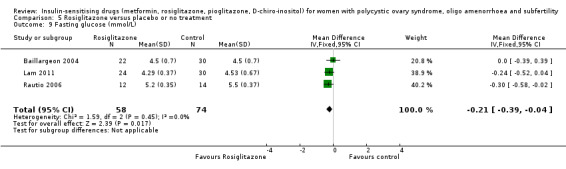
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 9 Fasting glucose (mmol/L).
5.10. Analysis.
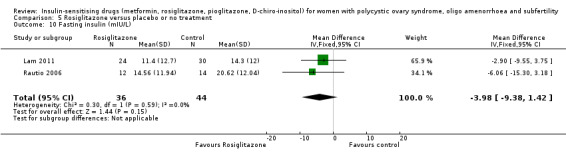
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 10 Fasting insulin (mIU/L).
5.11. Analysis.
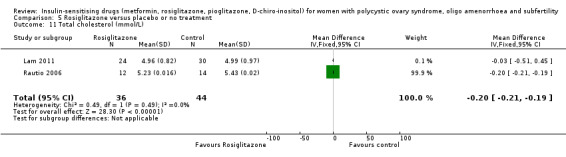
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 11 Total cholesterol (mmol/L).
5.12. Analysis.
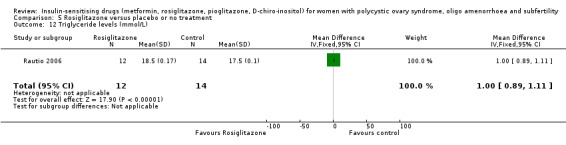
Comparison 5 Rosiglitazone versus placebo or no treatment, Outcome 12 Triglyceride levels (mmol/L).
6 Pioglitazone versus placebo or no treatment
Data were not available for primary outcomes, but were available for some secondary outcomes, including menstrual frequency and anthropometric, endocrine and metabolic outcomes. There was evidence that pioglitazone improved the menstrual pattern (OR 8.88, 95% CI 2.35 to 33.61, 2 studies, 70 women, I2 = 0%, moderate‐quality evidence) (Analysis 6.1). The studies differed in obesity status (only one study in each category), and both found an benefit in the intervention group.
6.1. Analysis.
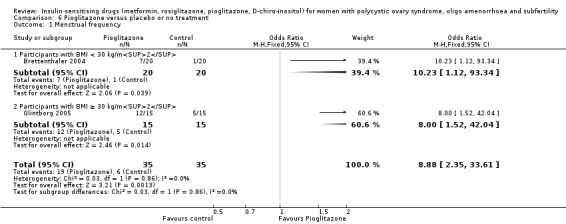
Comparison 6 Pioglitazone versus placebo or no treatment, Outcome 1 Menstrual frequency.
There was no evidence of a difference between the groups for anthropometric outcomes (BMI (Analysis 6.2); waist to hip ratio (Analysis 6.3)), endocrine outcomes (testosterone (Analysis 6.4); sex hormone‐binding globulin (Analysis 6.5)) or metabolic outcomes (fasting insulin (Analysis 6.6)).
6.2. Analysis.

Comparison 6 Pioglitazone versus placebo or no treatment, Outcome 2 Body mass index (kg/m2).
6.3. Analysis.
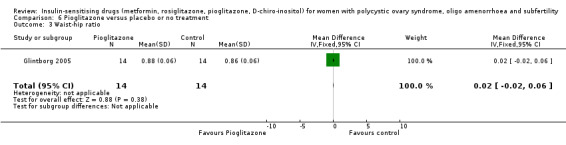
Comparison 6 Pioglitazone versus placebo or no treatment, Outcome 3 Waist‐hip ratio.
6.4. Analysis.
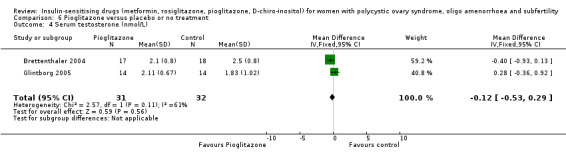
Comparison 6 Pioglitazone versus placebo or no treatment, Outcome 4 Serum testosterone (nmol/L).
6.5. Analysis.
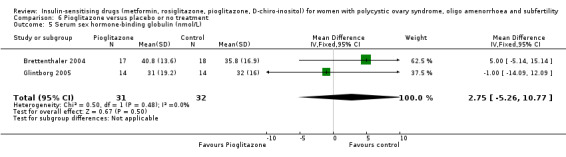
Comparison 6 Pioglitazone versus placebo or no treatment, Outcome 5 Serum sex hormone‐binding globulin (nmol/L).
6.6. Analysis.
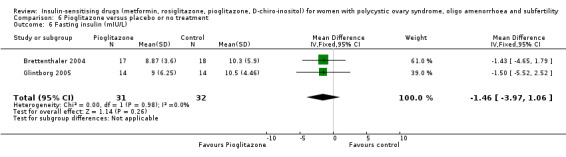
Comparison 6 Pioglitazone versus placebo or no treatment, Outcome 6 Fasting insulin (mIU/L).
Publication bias
We planned to assess publication bias using a funnel plot but no analyses of primary outcomes had sufficient included studies.
Discussion
Summary of main results
Our findings suggest that metformin is associated with a beneficial effect on ovulation and clinical pregnancy rates, regardless of BMI, when compared with placebo. The addition of newer data to this review shows a potential benefit of metformin over placebo for live birth rate. However, more high‐quality studies that report live birth as a primary outcome are required. When comparing outcomes following the use of metformin or clomiphene citrate, higher ovulation rates suggest that clomiphene citrate is beneficial over metformin, alongside a reduced side‐effect profile. However, there was no evidence to suggest that either treatment would increase the likelihood of a live birth over the other. Further data stratified by the BMI of participants are required to determine the subgroups of women who may achieve improved outcomes with metformin or clomiphene citrate treatment.
Women who are known to be resistant to clomiphene citrate therapy may benefit from improved ovulation with the addition of metformin to clomiphene citrate. However, data were not available to determine if this would improve live birth rates in this group of women. Women taking metformin should be advised that there does not appear to be an increased miscarriage risk with treatment, but the likelihood of gastrointestinal side effects is higher than with placebo or clomiphene citrate. The use of metformin needs to be placed in the context of the principal first line therapies for ovulation induction for anovulatory women with PCOS, namely the use of clomiphene citrate and the aromatase inhibitor (letrozole) (Balen 2016).
Reproductive outcomes
When compared with placebo, the results suggest a possible benefit from using metformin treatment in improving live birth rates (Analysis 1.1). One high‐quality study included in this updated review contributed the majority of the weight to this finding (Morin‐Papunen 2012). However, the wide‐ranging confidence intervals and lower‐quality evidence when the Morin‐Papunen 2012 results were combined with other included studies, makes the advantage offered by metformin difficult to interpret clinically. However, clinical pregnancy rates were higher with the use of metformin for ovulation induction (Analysis 1.3). Menstrual frequency also appeared to be improved with metformin versus placebo (Analysis 1.5). This resulted in a benefit in ovulation rate, which persisted following a subgroup analysis by BMI (Analysis 1.4).
There was no conclusive evidence that adding metformin in combination with clomiphene citrate, increased live birth compared to clomiphene citrate monotherapy (Analysis 2.1). However, clinical pregnancy and ovulation rates were improved with combination treatment in both BMI groups (Analysis 2.3; Analysis 2.4). We attempted to analyse data depending on whether women were known to be sensitive or resistant to clomiphene citrate. Unfortunately, these data were only available for ovulation rate (Analysis 2.5). The test for subgroup differences showed no evidence of a difference between the subgroups.
When metformin was compared to clomiphene citrate, findings were complicated by a difference based on the obesity status of the participants. Here, women in the non‐obese group were more likely to achieve a live birth rate with metformin, whilst the obese women appeared to benefit from clomiphene citrate therapy. This pattern was also evident for clinical pregnancy and ovulation rate, although these analyses were hampered by a paucity of data (Analysis 3.2; Analysis 3.3).
Miscarriage was not commonly reported as an outcome in the studies included in this review. When analysing the available data, the use of metformin monotherapy did not appear to increase the rate of miscarriage (Analysis 1.6). The comparison between metformin and clomiphene citrate found no conclusive evidence of a difference in the likelihood of miscarriage between the two treatments (Analysis 3.4). There was evidence to suggest an increase in miscarriage when clomiphene citrate was combined with metformin rather than used in isolation , although this effect did not persist after subgroup analysis per pregnancy, by BMI or study quality (Analysis 2.6; Analysis 2.7). Any increase in miscarriage conferred by using combined clomiphene citrate therapy is therefore difficult to interpret and apply clinically.
For the outcome multiple pregnancy, there was no available data regarding metformin versus placebo. The results were inconclusive for combination therapy versus clomiphene citrate monotherapy, and for the comparison between metformin and clomiphene citrate (Analysis 2.8; Analysis 3.6).
Adverse effects
There was evidence that use of metformin was associated with higher rates of gastrointestinal disturbance than placebo, and that adding in metformin therapy increased rates of gastrointestinal side effects compared with clomiphene citrate alone (Analysis 1.2; Analysis 2.2). Data on adverse effects comparing metformin versus clomiphene citrate were not available.
Metabolic and anthropometric outcomes
Data on the effect of metformin on anthropometric outcomes were only available for the comparison between metformin and placebo. There was no conclusive evidence that metformin resulted in reduction in BMI, although there was an effect on waist to hip ratio (Analysis 1.8; Analysis 1.9). Similarly, there was an effect on systolic blood pressure, but the evidence was not conclusive for diastolic blood pressure (Analysis 1.10; Analysis 1.11) or cholesterol (Analysis 1.16).
With regards to endocrine outcomes, we observed a treatment effect on serum testosterone concentration, although this was seen only in the non‐obese women (Analysis 1.12). We also found an effect on reducing fasting insulin levels in both BMI groups (Analysis 1.15). There was no conclusive evidence of an effect of metformin on serum lipid profiles (Analysis 1.17).
It is therefore unclear whether these metabolic and endocrine effects would be of any clinical benefit to women with PCOS. The data on these outcomes also tended to be associated with high heterogeneity.
The role of metformin in reducing the risk of developing metabolic syndrome in women with PCOS remains unclear. Given the significant negative impact of obesity on pregnancy outcomes (Cedergren 2004; Legro 2007) and longer‐term cardiovascular health, anovulatory obese women with PCOS should still be advised to undergo lifestyle changes before any fertility treatment (ESHRE/ASRM 2008).
Limitations
See Quality of the evidence and Potential biases in the review process.
Overall completeness and applicability of evidence
This review includes a large number of women, all meeting the Rotterdam diagnostic criteria for PCOS (ESHRE/ASRM 2004). However, we still observed significant heterogeneity in many of the analyses. This was particularly evident in the biochemical outcomes, even after adjustment for BMI, dosage of metformin and duration of treatment. Heterogeneity remained unchanged after sensitivity analysis by study quality. However, the prevalence and magnitude of insulin resistance are influenced by ethnicity (Wijeyaratne 2002; Wijeyaratne 2004), therefore, combining trials from different study populations would introduce heterogeneity despite all meeting the diagnostic criteria of PCOS. Another factor is the range of biochemical assays used in different studies, which may introduce some heterogeneity
The efficacy of metformin in PCOS was first described by Velazquez 1997. A number of small, and often short‐duration, observational studies followed, which showed variable outcomes. Indeed, in a systematic review by Costello 2003 nine out of the 12 published studies on the effects of metformin alone on the menstrual cycle in women with PCOS had a sample size of fewer than 30 women. The first Cochrane Review by Lord 2003 included nearly 1000 women from 15 RCTs. However, most of the studies had relatively small sample sizes with the largest one containing 94 women (Fleming 2002). In this third updated review, we included 48 RCTs (4451 women) with the two largest studies of high quality being by Morin‐Papunen 2012 and Legro 2007, with sample sizes of 320 and 626 women, respectively.
Reproductive outcomes
The primary outcome of this updated review is the effect of metformin for ovulation induction on live birth rate. When compared to placebo, there was a potential benefit in live birth when using metformin, with a number needed to treat for an additional beneficial outcome of 13. This is supported by the corresponding increase in clinical pregnancy rate, ovulation rate and menstrual frequency with treatment. These results were seen in both obese and non‐obese BMI groupings. As such, BMI does not appear to be a discriminatory factor in predicting ovulation success with metformin treatment compared with placebo, although the moderate degree of heterogeneity observed in the data should be noted. The heterogeneity between the non‐obese and the obese groups could be explained by the limited effect of metformin on reducing serum insulin concentrations in the obese group compared with the non‐obese group of women with PCOS (Analysis 1.4). Furthermore, obese women with PCOS have a higher insulin resistance (higher serum insulin concentrations) than non‐obese women with PCOS (Tang 2006).
The suggestion of an improvement in live births with metformin differs from the previous review, due to the inclusion of the new, high‐quality study, Morin‐Papunen 2012. However, there are still only four studies reporting live birth available for analysis, and the overall quality of the evidence is low. Given the wide‐ranging confidence intervals and evidence quality, the advantage offered by metformin remains difficult to interpret clinically. Therefore more high‐quality studies are required investigating the use of metformin, with live birth rate as the primary outcome.
Clomiphene citrate is traditionally employed as the first line ovulation induction therapy for anovulatory women with PCOS. However, there was a paucity of data comparing the efficacy and safety of metformin against clomiphene citrate therapy. When we combined the five available studies, we regarded the data as very low quality and with high heterogeneity. The results here differed by BMI, whereby clomiphene citrate appeared to increase live births in the obese group, with a large weighting attributed to the study by Legro 2007. In the non‐obese group however, metformin was superior, although this analysis included only small studies of low quality. As such, more high‐quality studies with a larger number of participants are required to assess metformin versus clomiphene citrate for live birth rate.
The beneficial effect of combination treatment with metformin and clomiphene citrate versus clomiphene citrate alone on live birth rate was not supported by the current evidence. Combination therapy appeared to improve clinical pregnancy rate and ovulation per woman. In our subgroup analysis, women who previously developed clomiphene citrate resistance had a larger effect with combined therapy than women who were clomiphene citrate sensitive or of undefined status. In addition, heterogeneity was low in the analysis of ovulation rates in the clomiphene citrate resistant group (I2 = 0%). Therefore, clomiphene citrate resistance can be a useful discriminatory factor to predict the response to the combined therapy. Future studies of the effect of metformin and clomiphene citrate on live birth rate should therefore be presenting the clomiphene citrate sensitivity of participants. In a subgroup analysis by BMI, the level of heterogeneity was very high in both groups. In addition, the number of women needed to treat to achieve ovulation in both the non‐obese and obese groups was high, 7.7 and 10 respectively. This compares to a number of women needed to treat of 3 in women with known clomiphene citrate resistance. Given that, in clinical practice, women would often receive only six cycles of clomiphene citrate treatment, the benefit afforded by metformin co‐therapy may be limited.
A large proportion of the women included in this review fall into the high‐BMI grouping. Given that the aim is for a pregnancy in these women, and that metformin does not have a conclusive effect on BMI, it is worth considering the impact of obesity on their reproductive outcomes. Cedergren 2004 conducted a prospective population‐based study on over 3000 morbidly obese mothers (BMI > 40 kg/m2) and demonstrated higher incidences of adverse pregnancy outcomes compared with a group of normal weight, including pre‐eclampsia, stillbirth, large‐for‐gestational‐age babies, fetal distress and early neonatal death. This emphasises the importance of weight loss in any obese women aiming for a pregnancy, alongside any additional treatment for ovulation induction. Lifestyle modification should therefore form an integral part of managing obese PCOS women suffering from anovulatory infertility (Tang 2006).
In this review, there was no convincing evidence of an effect on miscarriage or multiple pregnancy rates attributable to metformin. However, women should be counselled on the increased side‐effect profile with metformin, which may hamper clinical compliance, and the longer duration of treatment required with metformin.
Metabolic and anthropometric outcomes
There is yet to be any long‐term data on the use of metformin for women with PCOS in reducing the risk of developing diabetes or metabolic syndrome. Our analyses found no evidence of an effect of metformin on reducing BMI or improving lipid profiles. There was however, a reduction in cholesterol compared to placebo and reduced waist to hip ratio in the non‐obese group. There was also reduction in fasting glucose and fasting insulin levels when compared to placebo. However, the clinical relevance of these differences for the long‐term prevention of diabetes remains unclear. We saw an effect on systolic blood pressure but the magnitude of effect (MD ‐3.59 mm Hg) is unlikely to be clinically significant.
Metformin had a beneficial effect on serum testosterone, with a greater mean difference in the non‐obese group. However, meta‐regression did not support any effect of the daily dose or the duration of metformin treatment on the magnitude of the reduction in testosterone levels. High insulin levels stimulate an increase in androgen production from the ovaries and therefore an inadequate reduction of insulin concentrations induced by metformin in obese women with PCOS may be a reason why the reduction of testosterone was less marked in the obese group. The effect of metformin on serum testosterone could therefore benefit women with hirsutism. However, a Cochrane Review (Costello 2007) indicated that limited data were available comparing the effects of metformin with combined oral contraceptives for hirsutism. Given the increased efficacy of combined oral contraceptives at reducing serum testosterone (MD 0.54, 95% CI 0.22 to 0.86) and the free androgen index (MD 3.69, 95% CI 2.56 to 4.83) in their review, metformin is unlikely to become a first‐line therapy for hirsutism.
In respect to the use of rosiglitazone and pioglitazone in women with PCOS, our analysis, with a limited number of trials, showed that these drugs improve ovulation rate without evidence of an effect on biochemical parameters. Given that these drugs are classified as category C (FDA 2002) and hence most recruited women were not planning a pregnancy, it would be difficult to assess pregnancy outcomes. Furthermore, a high incidence of weight gain (Analysis 5.3) among the users further hampers their use in obese women with PCOS (Baillargeon 2004). There is also concern about links between rosiglitazone and increased risk of myocardial infarction (Lago 2007).
Quality of the evidence
Overall, we graded only 18 out of the 48 included studies as having low risk of bias related to sequence generation, allocation concealment and blinding. The main limitation of the comparisons in this review is therefore the risk of bias and imprecision within the included studies, as discussed in Table 1; Table 2; Table 3 and Figure 3 and Figure 4. However, sensitivity analysis on the studies with adequate sequence generation, allocation concealment and blinding method did not alter the clinical findings, except on fasting serum glucose concentrations. We classified the overall quality of evidence for metformin versus placebo as low for live birth rate and ovulation rate, and moderate for clinical pregnancy and miscarriage rate (Table 1). This was due to a moderate risk of bias, marginal effect size and statistical imprecision. The evidence for D‐chiro‐inositol, rosiglitazone and pioglitazone was of moderate quality. The overall quality of evidence for metformin versus clomiphene citrate and for metformin plus clomiphene citrate versus clomiphene citrate alone was moderate.
Potential biases in the review process
We conducted a thorough search, used sound methodology and are not aware of any biases in the review process.
Agreements and disagreements with other studies or reviews
Reproductive outcomes
A 2015 systematic review investigating the efficacy of metformin in women with anovulatory infertility for the improvement of reproductive outcomes (Abu Hashim 2016). For metformin versus placebo, only a previous version of this Cochrane Review was identified. The authors reviewed two meta‐analyses comparing metformin with clomiphene citrate for ovulation induction (Palomba 2009 and Siebert 2012). In accordance with our findings, they found improved ovulation rates with clomiphene citrate rather than metformin. There was no conclusive benefit of either treatment on clinical pregnancy or live birth rate, with wide confidence intervals noted. They therefore conclude that clomiphene citrate remains the "gold standard first‐line pharmacological treatment for ovulation induction in anovulatory infertile women with PCOS". An analysis of four studies that compared metformin with clomiphene citrate in non‐obese women found no significant difference in reproductive outcomes (Misso 2013). The conclusions drawn by Abu Hashim 2016 echo the ESHRE consensus, which documented that the first line treatment for anovulatory infertility is clomiphene citrate, whilst obese women should be advised to undergo lifestyle modifications (ESHRE/ASRM 2008).
When evaluating the Palomba 2009 and Siebert 2012 meta‐analyses, Abu Hashim 2016 found no evidence of an improvement in live birth when metformin was used in combination with clomiphene citrate. Our review also found no conclusive evidence of a difference in live birth rate, although clinical pregnancy and ovulation were improved with co‐therapy. Given the increased side‐effect profile with metformin, as found in our review, Abu Hashim 2016 do not recommend adding in metformin to clomiphene citrate therapy. However, their results are not stratified by BMI.
Metabolic and anthropometric outcomes
Our review found mixed evidence of an effect of metformin on metabolic outcomes, which is of unclear clinical significance for the prevention of diabetes in the long term. These findings are supported by Diabetes Prevention Program Research group study of over 3000 obese women (mean BMI 34 kg/m2) with an average follow‐up period of 2.8 years (Knowler 2002). They reported that both metformin and lifestyle‐intervention groups (7.8 and 4.8 cases per 100 person years respectively) had a lower incidence of diabetes compared with placebo (11 per 100 person years). However, the lifestyle‐intervention group achieved a significantly better weight reduction compared with the metformin (58% versus 31%). Furthermore, the initial modest weight loss in the metformin group was not sustainable after three years of follow‐up. In contrast, in the lifestyle group an average of 4% weight loss was still maintained after four years. Likewise, the Finnish Diabetes Prevention Study demonstrated that weight loss improved insulin sensitivity, waist circumference and serum triglyceride levels compared with controls in 150 obese women with impaired glucose tolerance (Uusitupa 2000). A 2007 meta‐analysis also concluded that the lifestyle interventions are more effective than metformin in obese women (Gillies 2007).
Authors' conclusions
Implications for practice.
Our updated review suggests that metformin alone may have a beneficial effect over placebo for live birth, although the evidence quality was low. When metformin was compared with clomiphene citrate, data for live birth were inconclusive, and our findings were limited by a lack of evidence. Results differed by BMI, emphasising the need for future studies to stratify results by BMI. An improvement in clinical pregnancy and ovulation rates suggests that clomiphene citrate remains preferable to metformin for ovulation induction in obese women with polycystic ovary syndrome (PCOS).
An improved rate of clinical pregnancy and ovulation rate with metformin and clomiphene citrate versus clomiphene citrate alone suggests that combined therapy may have a useful role although we do not know if this translates into an increased live birth rate. Women taking metformin alone or with combined therapy should be advised that there is no evidence of an increased miscarriage risk, but gastrointestinal side effects are more likely.
Implications for research.
Possible future strategies for insulin‐sensitising drugs include glucagon‐like peptide 1 (GLP‐1) analogues, which have been studied recently in women with PCOS (Jensterle 2014). These agents include exenatide and liraglutide and are currently only licensed for the treatment of type 2 diabetes mellitus. Future updates of this review may include comparative studies between metformin and these newer agents. The development of mitochondrial inhibitors may present an additional new therapeutic strategy for managing PCOS (Colca 2013; Zhang 2012).
Future studies of metformin should include live birth rate as the primary outcome. Studies should subdivide data on reproductive outcomes by resistance to clomiphene citrate and body mass index (BMI) (accounting for women having bariatric surgery). The magnitude of insulin resistance is also influenced by ethnicity (Wijeyaratne 2002; Wijeyaratne 2004). Trials should therefore perform subgroup analyses according to the ethnic origin of participants. These subgroups may reduce the heterogeneity in meta‐analyses. It may be prudent to investigate the efficacy of early intervention in young women or adolescents, or both, with a diagnosis of PCOS. Further data in this area may improve patient selection when determining the appropriate therapeutic strategy. Studies should also focus on the long‐term impact of lifestyle changes and the use of insulin‐sensitising drugs to modulate the risk of developing metabolic syndrome.
Good‐quality studies of adequate power are required to investigate the efficacy and safety of any new insulin‐sensitising agents. Although there is no current evidence that metformin is teratogenic (Cassina 2014), if it is used widely to treat anovulation then it is possible that rare effects may be unmasked. Metformin therapy therefore needs to be kept under continuing surveillance and adverse outcomes reported.
What's new
| Date | Event | Description |
|---|---|---|
| 16 February 2018 | Review declared as stable | Evidence is now settled and further evidence is unlikely to change the conclusions of the review. |
History
Protocol first published: Issue 2, 2001 Review first published: Issue 3, 2003
| Date | Event | Description |
|---|---|---|
| 15 September 2017 | New search has been performed | Five new studies added (Ayaz 2013; Begum 2014; Kar 2015; Machado 2012; Morin‐Papunen 2012). Six studies reclassified as excluded (Chaudhry 2016; Chaudhury 2008; Constantino 2009; Farzadi 2006; Ladson 2011; Refaie 2005). The review now includes 48 studies. |
| 15 September 2017 | New citation required and conclusions have changed | The Inclusion and exclusion of studies at this update has led to a modification in the conclusions of this review. |
| 19 April 2012 | New citation required but conclusions have not changed | New studies added but no change to conclusions |
| 2 October 2011 | New search has been performed | New studies added: Ben Ayed 2009; Boudhraa 2010; Brettenthaler 2004; Carmina 2004; Karimzadeh 2010; Khorram 2006; Ladson 2011; Lam 2011; Otta 2010; Pasquali 2000; Romualdi 2010; Sahin 2004; Siebert 2009; Williams 2009 Re‐classified publications Rautio 2006a; Rautio 2006b into a single study Rautio 2006 Protocol changes: removed secondary outcomes of hirsutism, waist circumference and HDL cholesterol; Removed Kelly 2002, Re‐classification of risk of bias in included studies according to the CRG recommendations |
| 6 December 2010 | New search has been performed | New Studies added: PCOSMIC 2010 |
| 1 March 2010 | Amended | Error in abstract corrected |
| 12 June 2008 | New citation required and conclusions have changed | Converted to new review format. Twenty‐one new RCTs were added to the review: Baillargeon 2004, Chou 2003, Eisenhardt 2006, Gerli 2003, Glintborg 2005, Hoeger 2004 and b, Karimzadeh 2007, Legro 2007, Lord 2006, Maciel 2004 and b, Moll 2006Onalan 2005 and b, Palomba 2005, Rautio 2006, Rautio 2006b, Tang 2006, Trolle 2007 and Zain 2009. Some changes to the methodology were made in accordance with Revman 5 and one new comparison was added (Metformin versus Clomifene). Studies using troglitazone were removed as this drug has been removed from the market because of safety concerns. |
| 7 December 2006 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
The authors wish to thank Cochrane Pregnancy and Childbirth for their assistance with developing this systematic review. We also thank Dr Machado and Professor Morin‐Papunen for answering email queries regarding their studies.
We would also like to thank the corresponding authors of the following trials who took time to respond to our requests for further data, some of whom took the trouble to perform repeat analyses for us:
Chou 2003; Fleming 2002; Glintborg 2005; Hoeger 2004; Hwu 2005; Jakubowicz 2001; Ladson 2011; Legro 2007; Lord 2006; Malkawi 2002; Moghetti 2000; Morin‐Papunen 2012; Nestler 1997; Nestler 1999; Ng 2001; Rautio 2006; Sturrock 2002; Trolle 2007; Vandermolen 2001; Yarali 2002.
We would also like to thank the Cochrane Menstrual Disorders and Subfertility Review Group in Auckland (now Cochrane Gynaecology and Fertility), and in particular their Managing Editor (to 2011) Jane Clarke, for all their help and support. We are also grateful to Rafael Perera of the UK Cochrane Centre for statistical advice.
The authors of the 2017 update wish to thank Dr Jonathan Lord for his contributions to all previous versions of this review.
Appendices
Appendix 1. Cochrane Gynaecology and Fertility specialised register search strategy
From inception to 12 January 2017
PROCITE platform
Keywords CONTAINS "polycystic ovary syndrome" or "PCOS" or "ovarian failure" or "polycystic ovary morphology" or "hyperandrogenemia" or "hyperandrogenism" or "hyperinsulinaemia" or "hyperandrogenicity" or Title CONTAINS "polycystic ovary syndrome" or "PCOS" or "ovarian failure" or "polycystic ovary morphology" or "hyperandrogenemia" or "hyperandrogenism" or "hyperinsulinaemia" or "hyperandrogenicity"
AND
Keywords CONTAINS "metformin" or "rosiglitazone" or "pioglitazone" or "troglitazone" or "Hypoglycemic Agents" or "plasminogen activator" or "thiazolidinedione" or "thiazolidinediones" or "Inositol" or "d‐chiro‐inositol" or "d‐chiro‐inositol‐containing inositol phosphoglycan mediator" or "Myo‐inositol" or Title CONTAINS "metformin" or "rosiglitazone" or "pioglitazone" or "troglitazone" or "Hypoglycemic Agents" or "plasminogen activator" or "thiazolidinedione" or "thiazolidinediones" or "Inositol" or "d‐chiro‐inositol" or "d‐chiro‐inositol‐containing inositol phosphoglycan mediator" or "Myo‐inositol"
(448 hits)
Appendix 2. Cochrane Central Register of Studies Online (CRSO) search strategy
Searched 12 January 2017
Web platform
#1 MESH DESCRIPTOR Polycystic Ovary Syndrome EXPLODE ALL TREES 882
#2 PCOS:TI,AB,KY 1285
#3 (polycystic ovar*):TI,AB,KY 1703
#4 PCOD:TI,AB,KY 24
#5 #1 OR #2 OR #3 OR #4 1862
#6 MESH DESCRIPTOR Metformin EXPLODE ALL TREES 1777
#7 metformin:TI,AB,KY 4409
#8 (dimethylbiguanidium or dimethylguanylguanidine or glucophage or glucovance):TI,AB,KY 38
#9 MESH DESCRIPTOR Hypoglycemic Agents EXPLODE ALL TREES 12901
#10 MESH DESCRIPTOR Thiazolidinediones EXPLODE ALL TREES 1166
#11 Thiazolidinediones:TI,AB,KY 1287
#12 glitazone:TI,AB,KY 86
#13 Rosiglitazone:TI,AB,KY 767
#14 (Pioglitazone or Troglitazone):TI,AB,KY 1403
#15 MESH DESCRIPTOR Inositol EXPLODE ALL TREES 298
#16 D‐chiro‐Inositol:TI,AB,KY 29
#17 chiro‐Inositol:TI,AB,KY 30
#18 myoinositol:TI,AB,KY 41
#19 inositol:TI,AB,KY 439
#20 MESH DESCRIPTOR Biguanides EXPLODE ALL TREES 3465
#21 Biguanides:TI,AB,KY 237
#22 MESH DESCRIPTOR Plasminogen Activator Inhibitor 1 EXPLODE ALL TREES 517
#23 (Plasminogen Activator Inhibitor‐1):TI,AB,KY 979
#24 MESH DESCRIPTOR Hyperandrogenism EXPLODE ALL TREES WITH QUALIFIERS DT 65
#25 MESH DESCRIPTOR Hyperinsulinism EXPLODE ALL TREES WITH QUALIFIERS DT 392
#26 #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 19047
#27 #5 AND #26 779
Appendix 3. MEDLINE search strategy
From 1946 to 12 January 2017
OVID platform
1 Polycystic Ovary Syndrome/ (13316) 2 PCOS.ti,ab,sh. (9205) 3 polycystic ovar$.ti,ab,sh. (17095) 4 PCOD.ti,ab,sh. (291) 5 (stein‐leventhal or leventhal).tw. (765) 6 (ovar$ adj (scelerocystic or polycystic or degeneration)).tw. (89) 7 or/1‐6 (17641) 8 Metformin/ (11192) 9 metformin.ti,ab,sh. (17508) 10 (dimethylbiguanidium or dimethylguanylguanidine or glucophage or glucovance).tw. (128) 11 exp Hypoglycemic Agents/ (241886) 12 Thiazolidinediones/ (12017) 13 glitazone$.tw. (717) 14 Rosiglitazone.tw. (5810) 15 Pioglitazone.tw. (4986) 16 Troglitazone.tw. (2338) 17 exp Inositol/ (25263) 18 D‐chiro‐Inositol.tw. (203) 19 chiro‐Inositol.tw. (336) 20 mesoinositol.tw. (37) 21 myoinositol.tw. (1261) 22 inositol.tw. (39226) 23 exp Biguanides/ (23990) 24 Biguanides.tw. (1124) 25 Plasminogen Activator Inhibitor 1/ (9074) 26 Plasminogen Activator Inhibitor‐1.tw. (8087) 27 Hyperandrogenism/dt [Drug Therapy] (265) 28 Hyperinsulinism/dt [Drug Therapy] (561) 29 or/8‐28 (322597) 30 7 and 29 (3505) 31 randomized controlled trial.pt. (508190) 32 controlled clinical trial.pt. (98209) 33 randomized.ab. (438707) 34 placebo.tw. (210044) 35 clinical trials as topic.sh. (197851) 36 randomly.ab. (298926) 37 trial.ti. (201903) 38 (crossover or cross‐over or cross over).tw. (79969) 39 or/31‐38 (1250853) 40 exp animals/ not humans.sh. (4853750) 41 39 not 40 (1154033) 42 30 and 41 (820)
Appendix 4. Embase search strategy
From 1980 to 12 January 2017
OVID platform
1 exp ovary polycystic disease/ (21998) 2 PCOS.tw. (12495) 3 polycystic ovar$.tw. (18101) 4 PCOD.tw. (354) 5 (stein‐leventhal or leventhal).tw. (598) 6 (ovar$ adj (scelerocystic or polycystic or degeneration)).tw. (84) 7 or/1‐6 (25142) 8 Metformin/ (47713) 9 metformin.tw. (23994) 10 (dimethylbiguanidium or dimethylguanylguanidine or glucophage or glucovance).tw. (1682) 11 exp antidiabetic agent/ (431456) 12 exp 2,4 thiazolidinedione derivative/ (12655) 13 Thiazolidinedione$.tw. (6887) 14 glitazone$.tw. (1092) 15 Rosiglitazone.tw. (7114) 16 Troglitazone.tw. (2495) 17 exp INOSITOL/ (12456) 18 D‐chiro‐Inositol.tw. (223) 19 chiro‐Inositol.tw. (389) 20 mesoinositol.tw. (13) 21 myoinositol.tw. (1510) 22 inositol.tw. (36587) 23 Biguanides.tw. (1311) 24 Plasminogen Activator Inhibitor‐1.tw. (8788) 25 exp hyperinsulinism/dt [Drug Therapy] (1474) 26 or/8‐25 (481745) 27 7 and 26 (7679) 28 Clinical Trial/ (1019530) 29 Randomized Controlled Trial/ (472724) 30 exp randomization/ (84526) 31 Single Blind Procedure/ (28735) 32 Double Blind Procedure/ (138900) 33 Crossover Procedure/ (54650) 34 Placebo/ (326024) 35 Randomi?ed controlled trial$.tw. (153072) 36 Rct.tw. (23004) 37 random allocation.tw. (1649) 38 randomly allocated.tw. (26969) 39 allocated randomly.tw. (2221) 40 (allocated adj2 random).tw. (847) 41 Single blind$.tw. (18934) 42 Double blind$.tw. (174826) 43 ((treble or triple) adj blind$).tw. (672) 44 placebo$.tw. (250674) 45 prospective study/ (394570) 46 or/28‐45 (1815100) 47 case study/ (94777) 48 case report.tw. (327043) 49 abstract report/ or letter/ (994732) 50 or/47‐49 (1407253) 51 46 not 50 (1763646) 52 27 and 51 (2001)
Appendix 5. PsycINFO search strategy
From 1806 to 12 January 2017
OVID platform
1 exp Endocrine Sexual Disorders/ (1081) 2 PCOS.tw. (217) 3 polycystic ovar$.tw. (340) 4 PCOD.tw. (5) 5 (stein‐leventhal or leventhal).tw. (274) 6 (ovar$ adj (scelerocystic or polycystic or degeneration)).tw. (0) 7 or/1‐6 (1576) 8 metformin.tw. (333) 9 (dimethylbiguanidium or dimethylguanylguanidine or glucophage or glucovance).tw. (1) 10 Hypoglycemic Agent$.tw. (66) 11 Thiazolidinedione$.tw. (72) 12 glitazone$.tw. (2) 13 Rosiglitazone.tw. (147) 14 Pioglitazone.tw. (146) 15 Troglitazone.tw. (8) 16 Inositol.tw. (1353) 17 D‐chiro‐Inositol.tw. (0) 18 chiro‐Inositol.tw. (3) 19 mesoinositol.tw. (0) 20 myoinositol.tw. (124) 21 Biguanides.tw. (5) 22 Plasminogen Activator Inhibitor 1.tw. (117) 23 or/8‐22 (2241) 24 7 and 23 (15)
Appendix 6. CINAHL search strategy
From 1961 to 12 January 2017
EBSCO platform
| # | Query | Results |
| S33 | S20 AND S32 | 153 |
| S32 | S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 | 1,104,354 |
| S31 | TX allocat* random* | 5,937 |
| S30 | (MH "Quantitative Studies") | 15,220 |
| S29 | (MH "Placebos") | 9,962 |
| S28 | TX placebo* | 42,956 |
| S27 | TX random* allocat* | 5,937 |
| S26 | (MH "Random Assignment") | 42,231 |
| S25 | TX randomi* control* trial* | 117,132 |
| S24 | TX ( (singl* n1 blind*) or (singl* n1 mask*) ) or TX ( (doubl* n1 blind*) or (doubl* n1 mask*) ) or TX ( (tripl* n1 blind*) or (tripl* n1 mask*) ) or TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) | 870,250 |
| S23 | TX clinic* n1 trial* | 197,808 |
| S22 | PT Clinical trial | 79,975 |
| S21 | (MH "Clinical Trials+") | 208,633 |
| S20 | S4 AND S19 | 417 |
| S19 | S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 | 23,283 |
| S18 | TX Plasminogen Activator Inhibitor | 1,020 |
| S17 | TX Biguanides | 219 |
| S16 | TX myoinositol | 71 |
| S15 | TX mesoinositol | 0 |
| S14 | TX chiro‐Inositol | 29 |
| S13 | TX D‐chiro‐Inositol | 26 |
| S12 | TX Inositol | 690 |
| S11 | (MM "Inositol+") | 225 |
| S10 | TX (glitazone or Rosiglitazone or Pioglitazone or Troglitazone) | 2,401 |
| S9 | (MM "Thiazolidinediones") OR (MH "Rosiglitazone") OR (MH "Pioglitazone") OR (MH "Troglitazone") | 2,074 |
| S8 | TX (dimethylbiguanidium or dimethylguanylguanidine or glucophage or glucovance) | 42 |
| S7 | TX Metformin | 5,078 |
| S6 | (MM "Metformin") | 1,960 |
| S5 | (MM "Hypoglycemic Agents+") | 18,757 |
| S4 | S1 OR S2 OR S3 | 3,296 |
| S3 | TX polycystic ovar* | 2,379 |
| S2 | TX PCOS or TX PCOD | 1,793 |
| S1 | (MM "Polycystic Ovary Syndrome") | 1,426 |
Data and analyses
Comparison 1. Metformin versus placebo or no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Live birth rate | 4 | 435 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.59 [1.00, 2.51] |
| 1.1 Participants with BMI < 30 kg/m2 | 3 | 370 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.51 [0.94, 2.44] |
| 1.2 Participants with BMI ≥ 30 kg/m2 | 1 | 65 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.87 [0.51, 16.01] |
| 2 Adverse events (gastrointestinal side effects) | 7 | 670 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.76 [3.06, 7.41] |
| 2.1 Participants with BMI < 30 kg/m2 | 4 | 393 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.61 [2.89, 10.88] |
| 2.2 Participants with BMI ≥ 30 kg/m2 | 3 | 277 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.13 [2.28, 7.49] |
| 3 Clinical pregnancy rate | 9 | 1027 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.93 [1.42, 2.64] |
| 3.1 Participants with BMI < 30 kg/m2 | 5 | 733 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.89 [1.35, 2.65] |
| 3.2 Participants with BMI ≥ 30 kg/m2 | 4 | 294 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.21 [0.98, 4.98] |
| 4 Ovulation rate | 14 | 701 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.55 [1.81, 3.59] |
| 4.1 Participants with BMI < 30 kg/m2 | 5 | 229 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.15 [2.31, 7.45] |
| 4.2 Participants with BMI ≥ 30 kg/m2 | 10 | 472 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.96 [1.28, 3.01] |
| 5 Menstrual frequency | 7 | 427 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.72 [1.14, 2.61] |
| 5.1 Participants with BMI < 30 kg/m2 | 1 | 23 | Odds Ratio (M‐H, Fixed, 95% CI) | 21.15 [1.01, 445.00] |
| 5.2 Participants with BMI ≥ 30 kg/m2 | 6 | 404 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.57 [1.03, 2.41] |
| 6 Miscarriage rate per woman | 4 | 748 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.50, 2.35] |
| 6.1 Participants with BMI < 30 kg/m2 | 3 | 683 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.19 [0.52, 2.71] |
| 6.2 Participants with BMI ≥ 30 kg/m2 | 1 | 65 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.5 [0.04, 5.80] |
| 7 Sensitivity analysis: miscarriage rate per pregnancy | 4 | 200 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.58 [0.25, 1.34] |
| 7.1 Participants with BMI < 30 kg/m2 | 3 | 188 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.26, 1.53] |
| 7.2 Participants with BMI ≥ 30 kg/m2 | 1 | 12 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.25 [0.02, 4.00] |
| 8 Body mass index (kg/m2) | 16 | 827 | Mean Difference (IV, Fixed, 95% CI) | ‐0.08 [‐0.33, 0.17] |
| 8.1 Participants with BMI < 30 kg/m2 | 7 | 419 | Mean Difference (IV, Fixed, 95% CI) | ‐0.06 [‐0.33, 0.21] |
| 8.2 Participants with BMI ≥ 30 kg/m2 | 10 | 408 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐0.92, 0.52] |
| 9 Waist‐hip ratio | 11 | 702 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.01, ‐0.00] |
| 9.1 Participants with BMI < 30 kg/m2 | 5 | 389 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.01, ‐0.00] |
| 9.2 Participants with BMI ≥ 30 kg/m2 | 6 | 313 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.02, 0.01] |
| 10 Blood pressure ‐ systolic (mm Hg) | 7 | 379 | Mean Difference (IV, Fixed, 95% CI) | ‐3.59 [‐5.13, ‐2.04] |
| 10.1 Participants with BMI < 30 kg/m2 | 3 | 96 | Mean Difference (IV, Fixed, 95% CI) | ‐3.52 [‐5.29, ‐1.76] |
| 10.2 Participants with BMI ≥ 30 kg/m2 | 5 | 283 | Mean Difference (IV, Fixed, 95% CI) | ‐3.80 [‐5.00, ‐0.60] |
| 11 Blood pressure ‐ diastolic (mm Hg) | 6 | 292 | Mean Difference (IV, Fixed, 95% CI) | ‐0.14 [‐1.35, 1.07] |
| 11.1 Participants with BMI < 30 kg/m2 | 3 | 96 | Mean Difference (IV, Fixed, 95% CI) | ‐0.21 [‐1.55, 1.13] |
| 11.2 Participants with BMI ≥ 30 kg/m2 | 4 | 196 | Mean Difference (IV, Fixed, 95% CI) | 0.18 [‐2.65, 3.02] |
| 12 Serum testosterone (nmol/L) | 15 | 863 | Mean Difference (IV, Fixed, 95% CI) | ‐0.49 [‐0.59, ‐0.39] |
| 12.1 Participants with BMI < 30 kg/m2 | 7 | 419 | Mean Difference (IV, Fixed, 95% CI) | ‐0.71 [‐0.86, ‐0.56] |
| 12.2 Participants with BMI ≥ 30 kg/m2 | 9 | 444 | Mean Difference (IV, Fixed, 95% CI) | ‐0.29 [‐0.44, ‐0.15] |
| 13 Serum sex hormone‐binding globulin (nmol/L) | 15 | 823 | Mean Difference (IV, Fixed, 95% CI) | 0.49 [‐1.82, 2.81] |
| 13.1 Participants with BMI < 30 kg/m2 | 6 | 387 | Mean Difference (IV, Fixed, 95% CI) | ‐0.22 [‐6.73, 6.28] |
| 13.2 Participants with BMI ≥ 30 kg/m2 | 10 | 436 | Mean Difference (IV, Fixed, 95% CI) | 0.60 [‐1.88, 3.07] |
| 14 Fasting glucose (mmol/L) | 15 | 849 | Mean Difference (IV, Fixed, 95% CI) | ‐0.14 [‐0.21, ‐0.07] |
| 14.1 Participants with BMI < 30 kg/m2 | 5 | 364 | Mean Difference (IV, Fixed, 95% CI) | ‐0.13 [‐0.22, ‐0.04] |
| 14.2 Participants with BMI ≥ 30 kg/m2 | 11 | 485 | Mean Difference (IV, Fixed, 95% CI) | ‐0.16 [‐0.27, ‐0.05] |
| 15 Fasting insulin (mIU/L) | 14 | 573 | Mean Difference (IV, Fixed, 95% CI) | ‐4.13 [‐5.67, ‐2.58] |
| 15.1 Participants with BMI < 30 kg/m2 | 4 | 85 | Mean Difference (IV, Fixed, 95% CI) | ‐6.20 [‐8.56, ‐3.84] |
| 15.2 Participants with BMI ≥ 30 kg/m2 | 11 | 488 | Mean Difference (IV, Fixed, 95% CI) | ‐2.57 [‐4.62, ‐0.53] |
| 16 Total cholesterol (mmol/L) | 10 | 562 | Mean Difference (IV, Fixed, 95% CI) | ‐0.14 [‐0.31, 0.02] |
| 16.1 Participants with BMI < 30 kg/m2 | 5 | 276 | Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.26, 0.22] |
| 16.2 Participants with BMI ≥ 30 kg/m2 | 6 | 286 | Mean Difference (IV, Fixed, 95% CI) | ‐0.26 [‐0.48, ‐0.03] |
| 17 Triglyceride levels (mmol/L) | 7 | 309 | Mean Difference (IV, Fixed, 95% CI) | 0.14 [‐0.05, 0.32] |
| 17.1 Participants with BMI < 30 kg/m2 | 3 | 53 | Mean Difference (IV, Fixed, 95% CI) | 0.00 [‐0.33, 0.34] |
| 17.2 Participants with BMI ≥ 30 kg/m2 | 5 | 256 | Mean Difference (IV, Fixed, 95% CI) | 0.20 [‐0.02, 0.42] |
1.7. Analysis.
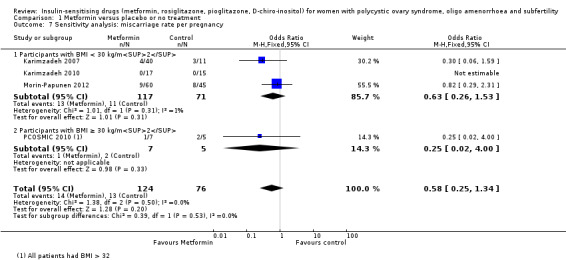
Comparison 1 Metformin versus placebo or no treatment, Outcome 7 Sensitivity analysis: miscarriage rate per pregnancy.
Comparison 2. Metformin combined with clomiphene citrate versus clomiphene citrate alone.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Live birth rate | 9 | 1079 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.21 [0.92, 1.59] |
| 1.1 Participants with BMI < 30 kg/m2 or ≤ 32 kg/m2 | 5 | 531 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.78, 1.67] |
| 1.2 Participants with BMI ≥ 30 kg/m2 | 4 | 548 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.28 [0.86, 1.91] |
| 2 Adverse events | 3 | 591 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.97 [2.59, 6.08] |
| 2.1 Participants with BMI < 30 kg/m2 | 3 | 591 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.97 [2.59, 6.08] |
| 3 Clinical pregnancy rate | 16 | 1529 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.59 [1.27, 1.99] |
| 3.1 Participants with BMI < 30 kg/m2 | 9 | 834 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.46 [1.08, 1.98] |
| 3.2 Participants with BMI ≥ 30 kg/m2 | 7 | 695 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.76 [1.26, 2.47] |
| 4 Ovulation rate | 21 | 1624 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.57 [1.28, 1.92] |
| 4.1 BMI < 30 kg/m2 | 11 | 755 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.79 [1.32, 2.41] |
| 4.2 BMI ≥ 30 kg/m2 | 9 | 814 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.52 [1.15, 2.01] |
| 4.3 BMI not reported | 1 | 55 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.43 [0.13, 1.37] |
| 5 Ovulation rate: subgroup analysis by sensitivity to clomiphene citrate | 7 | 271 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.69 [2.61, 8.44] |
| 5.1 PCOS and clomiphene‐sensitive | 1 | 56 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.55 [0.65, 19.37] |
| 5.2 PCOS and clomiphene‐resistant | 6 | 215 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.89 [2.62, 9.13] |
| 6 Miscarriage rate per woman | 9 | 1096 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.59 [1.03, 2.46] |
| 6.1 Participants with BMI < 30 kg/m2 | 5 | 548 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.41 [0.76, 2.62] |
| 6.2 Participants with BMI ≥ 30 kg/m2 | 4 | 548 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.79 [0.97, 3.32] |
| 7 Sensitivity analysis: miscarriage rate per pregnancy | 8 | 400 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.30 [0.80, 2.12] |
| 7.1 Participants with BMI < 30 kg/m2 | 4 | 228 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.27 [0.65, 2.51] |
| 7.2 Participants with BMI ≥ 30 kg/m2 | 4 | 172 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.34 [0.67, 2.68] |
| 8 Multiple pregnancy rate per woman | 6 | 1003 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.56 [0.18, 1.68] |
| 8.1 Participants with BMI < 30 kg/m2 | 3 | 476 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.12, 2.04] |
| 8.2 Participants with BMI ≥ 30kg/m2 | 3 | 527 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.11, 4.01] |
| 9 Senstivity analysis: multiple pregnancy rate per pregnancy | 6 | 342 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.46 [0.15, 1.42] |
| 9.1 Participants with BMI < 30 kg/m2 | 3 | 178 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.43 [0.10, 1.85] |
| 9.2 Participants with BMI ≥ 30 kg/m2 | 3 | 164 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.08, 3.12] |
Comparison 3. Metformin versus clomiphene citrate.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Live birth | 5 | 741 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.49, 1.01] |
| 1.1 Participants with BMI < 30 kg/m2 | 3 | 241 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.71 [1.00, 2.94] |
| 1.2 Participants with BMI ≥ 30 kg/m2 | 2 | 500 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.30 [0.17, 0.52] |
| 2 Clinical pregnancy rate | 7 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Participants with BMI < 30 kg/m2 | 5 | 490 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.56 [1.05, 2.33] |
| 2.2 Participants with BMI ≥ 30 kg/m2 | 2 | 500 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.21, 0.55] |
| 3 Ovulation rate | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Participants with BMI < 30 kg/m2 | 4 | 312 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.51, 1.28] |
| 3.2 Participants with BMI ≥ 30 kg/m2 | 2 | 500 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.29 [0.20, 0.43] |
| 4 Miscarriage rate per woman | 5 | 741 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.50, 1.67] |
| 4.1 Participants with BMI < 30 kg/m2 | 3 | 241 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.58 [0.61, 4.09] |
| 4.2 Participants with BMI ≥ 30 kg/m2 | 2 | 500 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.27, 1.38] |
| 5 Sensitivity analysis: miscarriage rate per pregnancy | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5.1 Participants with BMI < 30 kg/m2 | 3 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Participants with BMI ≥ 30 kg/m2 | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Multiple pregnancy rate per woman | 5 | 858 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.29 [0.06, 1.43] |
| 6.1 Participants with BMI < 30 kg/m2 | 3 | 358 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.46 [0.07, 3.16] |
| 6.2 Participants with BMI ≥ 30 kg/m2 | 2 | 500 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.01, 2.76] |
| 7 Sensitivity analysis: multiple pregnancy rate per pregnancy | 5 | 201 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.06, 1.68] |
| 7.1 Participants with BMI < 30 kg/m2 | 3 | 103 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.32 [0.05, 2.24] |
| 7.2 Participants with BMI ≥ 30 kg/m2 | 2 | 98 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.02, 6.69] |
Comparison 4. D‐chiro‐inositol versus placebo or no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Ovulation | 2 | 327 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.57 [1.72, 7.45] |
| 1.1 Participants with BMI < 30 kg/m2 | 2 | 327 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.57 [1.72, 7.45] |
| 2 Body mass index (kg/m2) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 0.5 [‐0.86, 1.86] |
| 3 Waist‐hip ratio | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.05, 0.03] |
| 4 Blood pressure ‐ systolic (mm Hg) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐2.0 [‐5.85, 1.85] |
| 5 Blood pressure ‐ diastolic (mm Hg) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐4.0 [‐7.26, ‐0.74] |
| 6 Serum testosterone (nmol/L) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐0.63 [‐1.37, 0.11] |
| 7 Serum sex hormone‐binding globulin (nmol/L) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 69.44 [34.97, 103.91] |
| 8 Fasting glucose (mmol/L) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐0.28 [‐0.99, 0.43] |
| 9 Fasting insulin (mIU/L) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐20.0 [‐43.43, 3.43] |
| 10 Total cholesterol (mmol/L) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐0.23 [‐0.99, 0.53] |
| 11 Triglyceride levels (mmol/L) | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | ‐2.20 [‐6.23, 1.83] |
Comparison 5. Rosiglitazone versus placebo or no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Ovulation rate | 1 | 64 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.91 [0.70, 5.22] |
| 1.1 Participants with BMI ≥ 30 kg/m2 | 1 | 64 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.91 [0.70, 5.22] |
| 2 Menstrual frequency | 2 | 100 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.59 [2.20, 14.19] |
| 3 Body mass index (kg/m2) | 3 | 132 | Mean Difference (IV, Fixed, 95% CI) | 0.68 [0.40, 0.96] |
| 4 Waist‐hip ratio | 3 | 132 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.02, ‐0.00] |
| 5 Blood pressure ‐ systolic (mm Hg) | 1 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐2.0 [‐3.95, ‐0.05] |
| 6 Blood pressure ‐ diastolic (mm Hg) | 1 | 52 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.72, 1.32] |
| 7 Serum testosterone (nmol/L) | 1 | 54 | Mean Difference (IV, Fixed, 95% CI) | 0.20 [‐0.34, 0.74] |
| 8 Serum sex hormone‐binding globulin (nmol/L) | 3 | 132 | Mean Difference (IV, Fixed, 95% CI) | ‐0.69 [‐10.37, 8.98] |
| 9 Fasting glucose (mmol/L) | 3 | 132 | Mean Difference (IV, Fixed, 95% CI) | ‐0.21 [‐0.39, ‐0.04] |
| 10 Fasting insulin (mIU/L) | 2 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐3.98 [‐9.38, 1.42] |
| 11 Total cholesterol (mmol/L) | 2 | 80 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐0.21, ‐0.19] |
| 12 Triglyceride levels (mmol/L) | 1 | 26 | Mean Difference (IV, Fixed, 95% CI) | 1.0 [0.89, 1.11] |
Comparison 6. Pioglitazone versus placebo or no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Menstrual frequency | 2 | 70 | Odds Ratio (M‐H, Fixed, 95% CI) | 8.88 [2.35, 33.61] |
| 1.1 Participants with BMI < 30 kg/m2 | 1 | 40 | Odds Ratio (M‐H, Fixed, 95% CI) | 10.23 [1.12, 93.34] |
| 1.2 Participants with BMI ≥ 30 kg/m2 | 1 | 30 | Odds Ratio (M‐H, Fixed, 95% CI) | 8.0 [1.52, 42.04] |
| 2 Body mass index (kg/m2) | 2 | 63 | Mean Difference (IV, Fixed, 95% CI) | 0.91 [‐1.88, 3.70] |
| 3 Waist‐hip ratio | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.02, 0.06] |
| 4 Serum testosterone (nmol/L) | 2 | 63 | Mean Difference (IV, Fixed, 95% CI) | ‐0.12 [‐0.53, 0.29] |
| 5 Serum sex hormone‐binding globulin (nmol/L) | 2 | 63 | Mean Difference (IV, Fixed, 95% CI) | 2.75 [‐5.26, 10.77] |
| 6 Fasting insulin (mIU/L) | 2 | 63 | Mean Difference (IV, Fixed, 95% CI) | ‐1.46 [‐3.97, 1.06] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ayaz 2013.
| Methods | RCT Setting: Saudi Arabia Method of randomisation: unclear Blinding: double Number randomised: 42 |
|
| Participants | Summary: metformin and CC versus CC alone Inclusion criteria: PCOS (Rotterdam criteria) Exclusion criteria: other endocrine disorders, male factor infertility, recent PID, tubal infertility Baseline characteristics of each group: metformin and CC versus CC alone Mean age (SD) 32 (3.5), 31.3 (2.9) BMI > 25 14 (56.7)), 15 (71.4) Mean thyroid stimulating hormone mIU/L (SD) 4.6 (1.3), 3.9 (1.7) Free thyroxin nmol/L (SD) 4.81 (1.6), 5.2 (1.8) Mean total testosterone: mmol/L (SD) 2.60 (0.78), 2.74 (0.65) Sex hormone‐binding globulin: nmol/L (SD) 21.7 (3.7), 18.9 (4.3) Dropouts: none |
|
| Interventions | Main intervention: metformin 500 mg 3/d Duration: 6 months until 8 weeks of a confirmed pregnancy Co‐interventions: CC 50 mg from day 2 until day 6 of cycle |
|
| Outcomes | Ovulation: follicle tracking on transvaginal US Others: menstrual pattern, pregnancy rate, multiple pregnancy rate |
|
| Notes | Endocrine and metabolic outcomes not recorded | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes used |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No women were lost to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Unclear |
Baillargeon 2004.
| Methods | RCT Setting: Venezuela Method of randomisation: fixed block of 8 randomisation which was performed by the investigational pharmacist. Blinding: double Number randomised: 128 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: PCOS (oligomenorrhoea < 8 periods/year, hyperandrogenism total testosterone > 2.43 nmol/L Normal prolactin and TFT, fasting insulin < 15 μIU/mL and fasting glucose to insulin ration > 4.5 Normal OGTT Hormonal contraceptives were not used before the trial. Exclusion criteria: late onset adrenal hyperplasia, hypertension. Previous insulin‐sensitiser users Baseline characteristics of each group:
Dropouts: 4 (12.5%) in the metformin arm, 10 (31.3%) in the rosiglitazone group and 2 (6.3%) in the placebo group |
|
| Interventions | Main intervention: metformin 850 mg, rosiglitazone 4 mg or placebo tablets twice daily Duration: 6 months Co‐interventions: none |
|
| Outcomes | Ovulation: weekly progesterone measurement with a level > 4 ng/mL was considered to be ovulation Anthropometric: weight, BMI, WHR, BP Hormones: testosterone, SHBG, free testosterone, DHEAS Metabolic markers: fasting glucose, AUC glucose and fasting glucose:insulin ratio Others: menstrual pattern |
|
| Notes | This study randomised 128 women into 4 groups (metformin alone, rosiglitazone alone, combined metformin and rosiglitazone, placebo alone). We included the combined group in our analysis. We analysed the metformin and rosiglitazone groups separately and compared the results from these 2 groups with the same group of women who took placebo. Women were predominantly white European emigrants to Venezulea Delays in the delivery of the drug rosiglitazone to the research centre resulted in higher dropout rates in this group after randomisation. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Fixed block of 8 randomisation which was performed by the investigational pharmacist |
| Allocation concealment (selection bias) | Low risk | Trial drugs packed in coded boxes allocated by the research nurse. Trial drugs were similar in appearance |
| Blinding (performance bias and detection bias) All outcomes | Low risk | "Double blinded" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropouts: 4 (12.5%) in the metformin arm, 10 (31.3%) in the rosiglitazone group and 2 (6.3%) in the placebo group. Details not provided |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Unclear |
Begum 2014.
| Methods | RCT Setting: Bangladesh (Infertility Department of women and children's hospital) Method of randomisation: envelopes used, but no other information Blinding: unclear Number randomised: 71 |
|
| Participants | Summary: PCOS meeting the Rotterdam criteria for diagnosis Inclusion criteria: subfertile women between 20‐35 years with a diagnosis of PCOS according to Rotterdam criteria Exclusion criteria: Age > 35 years, hypo‐ or hyperthyroidism, hyperprolactinaemia, diabetes mellitus and male factor infertility Baseline characteristics of each group:
Dropouts: none stated |
|
| Interventions | Main intervention: Group 1: metformin 1500 mg/d. Group 2: CC 100 mg/d for 5 d Duration: 6 months Co‐interventions: none |
|
| Outcomes | Ovulation rate Pregnancy rate |
|
| Notes | We have contacted study authors for further information regarding methodology | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of generating random sequence for distribution in envelopes is not stated. |
| Allocation concealment (selection bias) | High risk | Allocation to each group revealed in envelopes but not stated if opaque and sealed. Due to high risk of allocation concealment bias, Begum 2014 is excluded from subgroup analysis by study quality. |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | No information given |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | None stated |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | None stated |
Ben Ayed 2009.
| Methods | RCT Setting: Tunisia Method of randomisation: not stated Blinding: not stated Number randomised: 32 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: Rotterdam criteria Exclusion criteria: late onset adrenal hyperplasia, Cushing's Syndrome, abnormal TFT, hyperprolactinaemia, androgen‐secreting tumour Baseline characteristics of each group:
|
|
| Interventions | Main intervention: metformin 1700 mg/d or placebo Duration: unclear Co‐interventions: CC 100 mg from day 3 to day 7 of the cycle. Lifestyle advice on the obese subjects |
|
| Outcomes | Ovulation: USS follicular tracking with follicular size > 16 mm | |
| Notes | Inadequate information in the protocol to assess the quality of the trial No reply from study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Inadequate information |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Inadequate information |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Boudhraa 2010.
| Methods | RCT Setting: Tunisia Method of randomisation: not stated* Blinding: unblinded Number randomised: 63 |
|
| Participants | Summary: PCOS non‐obese Inclusion criteria: unclear. ? diagnostic criteria of PCOS used Exclusion criteria: male factor infertility, tubal disease Baseline characteristics of each group:
Dropouts: none |
|
| Interventions | Main intervention: metformin 850 mg Duration: not stated Co‐interventions: recommendations on healthy diet. 5 d 100 mg CC treatment |
|
| Outcomes | Ovulation: method to confirm ovulation not stated Live birth |
|
| Notes | Study protocol is too brief. Inadequate information to assess the quality of the study. No reply from study author* | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Inadequate information |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Inadequate information |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Brettenthaler 2004.
| Methods | RCT Setting: Switzertland Method of randomisation: unclear* Blinding: double Number randomised: 40 |
|
| Participants | Summary: PCOS non‐obese Inclusion criteria: menstrual dysfunction (oligo‐ or amenorrhoea), hirsutism with Ferriman‐Gallwey score > 7 or serum total testosterone > 2.5 nmol/L and SHBG < 50 nmol/L Exclusion criteria: adrenal disease, thyroid dysfunction, diabetes, hyperprolactinaemia Pregnancy or desire for pregnancy, basal FSH > 20 IU/L Medication known to affect reproductive or metabolic functions Previous hysterectomy History of liver disease or alcohol abuse Abnormal liver function tests. Baseline characteristics of each group:
Dropouts: 3 in the treatment group and 2 in the placebo group. The details were not given (lost in follow‐up and protocol violation) |
|
| Interventions | Main intervention: pioglitazone 30 mg or placebo tablet once daily Duration: 3 months Co‐interventions: recommendations on healthy diet and physical activity for weight maintenance 4 weeks prior to the study |
|
| Outcomes | Ovulation: progesterone > 9 nmol/L Anthropometric: BMI, WHR Hormones: testosterone, SHBG, DHEAS Metabolic markers: insulin, glucose, AUC insulin, AUC glucose, cholesterol, triglyceride Others: hirsutism |
|
| Notes | Participants in this study were very heterogeneous (65% European, 30% Turkish and 5% Asian) No serious side effects or abnormal liver function tests were reported. Nevertheless, women who took pioglitazone experienced more side effects compared with those who took placebo; mild peripheral oedema (18% vs 0%), mastopathy (11.7% vs 5%), sleeping disorders (23% vs 5%), headache (23% vs 5%) and stomach arch (23% vs %%) *No reply from the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Inadequate information |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Identical trial and placebo tablets. Inadequate information to assess the methodology |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Missing data not reported |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Participants in this study were very heterogeneous (65% European, 30% Turkish and 5% Asian). Inadequate information to assess. No reply from study author |
Carmina 2004.
| Methods | RCT Setting: USA Method of randomisation: random table Blinding: not stated Number randomised: 24 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: chronic anovulation with serum progesterone < 2 ng/mL on day 22 of cycle, in 2 consecutive cycles Normal TFT No clinical and biochemical features of hyperandrogenism Exclusion criteria: Baseline characteristics of each group:
Dropouts: none |
|
| Interventions | Main intervention: metformin 500 mg 3/d, placebo Duration: 3 months Co‐interventions: |
|
| Outcomes | Ovulation: method to confirm ovulation not stated | |
| Notes | This study evaluated the efficacy of metformin in women with anovulation who do not have evidence of hyperandrogenism; although > 79% of included women had USS evidence of PCO; hence, met the Rotterdam diagnostic criteria of PCOS. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Inadequate information |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Limited information to assess |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Only 79% of the subjects were PCOS |
Chou 2003.
| Methods | RCT Setting: Brazil Method of randomisation: participants were randomised by a 3rd party by using a table with random numbers (odd number assigned for the metformin group, even number assigned for the placebo group)* Blinding: double Number randomised: 32 |
|
| Participants | Summary: obese PCOS Inclusion criteria: oligomenorrhoea (< 6 menstrual cycles), clinical or biochemical hyperandrogenism BMI > 30 Non‐smoker. Participants had not used any medication 3 months before the start of the trial Exclusion criteria: renal or liver disease. CAH (serum 17‐hydroxyprogesterone > 12 ng/dL 1 h after 0.25 mg ACTH intramuscular injection) Baseline characteristics of each group:
Dropouts: 1 in each arm (protocol violation) |
|
| Interventions | Main intervention: metformin 500 mg or placebo tablet 3/d Duration: 3 months Co‐interventions: |
|
| Outcomes | Anthropometric: BMI, WHR, BP* Hormones: testosterone, SHBG* Metabolic markers: insulin, glucose, cholesterol, LDL, HDL and triglyceride* Others: menstrual pattern |
|
| Notes | This study was designed to evaluate the benefit of using metformin in obese women (BMI > 30) with PCOS. 3 participants in each arm were found to have glucose intolerance according to WHO criteria The results of the women who dropped out from the study were excluded from the analysis. *Information kindly provided by the study author that was not in the original paper |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomised by a 3rd party by using a table with random numbers. Odd number assigned for the metformin group, even number assigned for the placebo group |
| Allocation concealment (selection bias) | Low risk | Trial drugs were similar in appearance. Randomisation carried out by a 3rd party who kept the code until the end of the study. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | The results of the women who dropped out from the study were excluded from the analysis. Details of the excluded women were not given |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Eisenhardt 2006.
| Methods | RCT Setting: Germany Method of randomisation: computer‐generated random numbers with randomisation in block of 6. The code was sealed by a 3rd party until the end of the study period. Blinding: double Number randomised: 45 |
|
| Participants | Summary: obese PCOS Inclusion criteria: oligomenorrhoea (cycle length > 35days or < 9 periods/year) or amenorrhoea (cycle length > 12 weeks), PCO on USS (Rotterdam consensus 2003), clinical or biochemical hyperandrogenism (testosterone > 2.1 nmol/L or androstenedione > 10.1 nmol/L) Age between 21‐36 years Exclusion criteria: hyperprolactinaemia, diabetes, thyroid disease, CAH, Cushings's syndrome Medications that influence hormonal profiles or anti‐obesity drugs ≤ 6 months before the start of the study Baseline characteristics of each group:*
Dropouts: 1 in the metformin arm, 3 in the placebo arm. Details were not given. Furthermore, 1 in the metformin group and 2 in the placebo became pregnant and were also excluded from the analysis. |
|
| Interventions | Main intervention: metformin 500 mg or placebo tablet 3/d Duration: 12 weeks Co‐interventions: none |
|
| Outcomes | Anthropometric: BMI, weight* Hormones: testosterone, androstenedione, SHBG, oestradiol, DHEAS, LH, FSH* Metabolic markers: glucose, insulin, AUC glucose, AUC insulin* Others: hirsutism, menstrual pattern* |
|
| Notes | The objective of this study was to evaluate the effects of metformin in women with PCOS according to the status of insulin resistance. Insulin resistance was defined as fasting glucose to insulin ratio < 4.5. 32 out of 45 women (71.1%) were classified as insulin‐resistant PCOS. Insulin‐resistant PCOS women responded better than non insulin‐resistant PCOS women in terms of improvement in menstrual cyclicity. The results were presented in median and range. Hence, we could not include these data in the meta‐analysis. We are currently still waiting for a reply from the study author for the converted results in a format of mean and standard deviation. *still awaiting for a reply from the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers with randomisation in block of 6 |
| Allocation concealment (selection bias) | Low risk | The code was sealed by a 3rd party until the end of the study period. Trial drugs were provided by a pharmaceutical company not involved in study design and data analysis |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropouts: 1 in the metformin arm, 2 in the placebo arm. Details not given |
| Selective reporting (reporting bias) | Low risk | All primary outcome measures (menstrual frequency and metabolic parameters) reported |
| Other bias | Unclear risk | Inadequate information |
El‐Biely 2001.
| Methods | RCT Setting: Egypt Method of randomisation: computer‐based, blocked (block size not stated) Blinding: not stated; presumed to be unblinded Number randomised: 90 |
|
| Participants | Summary: PCOS, obese Inclusion criteria: PCOS (oligomenorrhoea, US findings of ≥ 10 ovarian cysts measuring 2‐8 mm around a dense stroma), hyperinsulinaemia (fasting insulin > 30 mIU/L) BMI > 28 kg/m2 WHR > 0.85 Normal semen analysis No tubal disease Exclusion criteria: diabetes mellitus, thyroid dysfunction, raised prolactin Baseline characteristics of each group:
Dropouts: only as a result of pregnancy (13 from metformin group, 4 from no metformin) |
|
| Interventions | Main intervention: 1 of: metformin 500 mg 3/d, no treatment Duration: 6 months Co‐interventions: CC 50 mg on days 5‐9, increased each cycle if not ovulated by 50 mg up to a maximum of 150 mg hCG 10,000 IU given to trigger ovulation |
|
| Outcomes | Ovulation: by serum progesterone (> 15.9 nmol/L) 9 d after hCG Metabolic markers: fasting insulin Others: pregnancy Number of mature follicles Diameter of largest follicle Premature ovulation rate Ovarian hyperstimulation syndrome (not defined) |
|
| Notes | The inclusion criteria did not include previous response to CC. Overall, 65% of those receiving CC and placebo ovulated (compared to 85% of those receiving CC and metformin). This trial reported a significantly higher mean number of mature follicles in the metformin group (3.1 versus 1.9, P < 0.0001), but a significantly lower rate of ovarian hyperstimulation syndrome (4 versus 31, P < 0.001). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer randomised |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Only as a result of pregnancy (13 from metformin group, 4 from no metformin) |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | The inclusion criteria did not include previous response to CC. Overall, 65% of those receiving CC and placebo ovulated (compared to 85% of those receiving CC and metformin). |
Fleming 2002.
| Methods | RCT Setting: UK Method of randomisation: computer‐generated randomisation by pharmacy in blocks of 4 Blinding: double‐blind Number randomised: 94 |
|
| Participants | Summary: obese PCOS Inclusion criteria: PCOS (oligomenorrhoea < 8 cycles/year, exclusion of other endocrinopathy, US finding of PCO) Age < 35 years Exclusion criteria: diabetes mellitus, adrenal hyperplasia, thyroid dysfunction, hyperprolactinaemia, medication likely to influence hormonal profiles Baseline characteristics of each group:
Dropouts: 30 (32%), with 22 in the treatment arm and 8 in the placebo, mainly due to gastrointestinal side effects in metformin group. Overall, 58% of the metformin arm completing the trial and 83% of the placebo arm. Included in ITT analysis |
|
| Interventions | Main intervention: 1 of metformin 850 mg 2/d, placebo Duration: 12‐16 weeks Co‐interventions: 1st week of treatment at 850 mg 1/d |
|
| Outcomes | Ovulation: by twice‐weekly serum oestradiol. Where oestradiol > 300 pmol/L, LH and progesterone (> 8 nmol/L in ≥ 2 successive samples defined ovulation*) were determined Anthropometric: BMI, WHR Reproductive hormones: total testosterone, free testosterone, androstenedione, estradiol, SHBG, FSH, LH Metabolic markers: fasting glucose, fasting insulin, AUC insulin during GTT, leptin, inhibin‐B, cholesterol (HDL, LDL, VLDL), triglycerides Others: ovarian US, pregnancy, adverse effects |
|
| Notes | Diagnostic criteria different to other trials ‐ using US not hyperandrogaenemia (although 90% did have raised androgens, and mean entry‐FAI 10 with 5% CI 8.6). Subgroup analysis showed that those who ovulated in response to metformin had significantly lower androgens. High rate of background ovulation (64% on placebo ovulated at some stage) *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation by pharmacy in blocks of 4 |
| Allocation concealment (selection bias) | Low risk | Remote allocation. Identical metformin and placebo tablets. Randomisation code kept in the pharmacy department until the end of the trial |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropouts: 30 (32%), with 22 in the treatment arm and 8 in the placebo, mainly due to gastrointestinal side effects in metformin group. Overall, 58% of the metformin arm completed the trial and 83% of the placebo arm. |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Gerli 2003.
| Methods | RCT Setting: Italy Method of randomisation: computer‐generated random number table* Blinding: double Number randomised: 283 |
|
| Participants | Summary: obese PCOS Inclusion criteria: PCO on USS, oligomenorrhoea (cycle length > 40 d or < 8 cycles/year) or amenorrhoea, clinical and biochemical hyperandrogenism Age < 35 years Exclusion criteria: CAH, thyroid dysfunction, hyperprolactinaemia Baseline characteristics of each group:
Dropouts: significantly more women withdrew in the treatment group (n = 15) compared with the placebo group (n = 5). Reasons not given |
|
| Interventions | Main intervention: inositol 100 mg or placebo tablet twice daily Duration: 16 weeks Co‐interventions: none |
|
| Outcomes | Ovulation: progesterone > 6 nmol/L Anthropometric: BMI, WHR* Hormones: Metabolic markers: insulin, glucose, AUC insulin, leptin, VLDL, LDL, HDL, triglyceride* Others: menstrual pattern, pregnancy* |
|
| Notes | This is the largest study published so far on the effects of inositol on ovarian function and metabolic factors in women with PCOS. Women were recruited from gynaecology, endocrine and infertility outpatient clinics in the study centre. Nearly half of the participants presented with history of infertility. However, only 42 women declared a wish to conceive before the start of the trial. Therefore, it would be difficult to interpret the pregnancy rate accurately. *No further information from the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random number table |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropouts: significantly more women withdrew in the treatment group (n = 15) compared with the placebo group (n = 5). Reasons not given |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Glintborg 2005.
| Methods | RCT Setting: Denmark Method of randomisation: computer‐generated numbers. Randomisation was conducted in the local pharmacist. The code was kept in the pharmacist department until the end of the trial* Blinding: double* Number randomised: 30 |
|
| Participants | Summary: obese PCOS Inclusion criteria: oligomenorrhoea (cycle length > 35 days), free testosterone > 0.035 nmol/L or clinical evidence of hirsutism Fasting insulin level > 50 pmol/L and/or BMI > 30 Participants stopped oral contraceptives for at least 3 months before the trial Normal TFT and prolactin levels Exclusion criteria: diabetes, hypertension, renal dysfunction, heart disease or abnormal liver function tests Baseline characteristics of each group:
Dropouts: 2 in total. 1 in the placebo group due to pregnancy. Another subject in the treatment group experienced side effects from pioglitazone (ankle oedema, anxiety, dizziness). No serious side effects were reported in this study and all women had normal liver function tests at the end of the trial. |
|
| Interventions | Main intervention: pioglitazone 30 mg or placebo once daily Duration: 16 weeks Co‐interventions: |
|
| Outcomes | Anthropometric: BMI, WHR, waist circumference Hormones: testosterone, SHBG, free testosterone Metabolic markers: fasting insulin Others: menstrual pattern, hirsutism |
|
| Notes | The main objective of this study was to investigate the effect of pioglitazone on growth hormone levels in women with PCOS. The secondary endpoint measures included changes in anthropometric and hormonal parameters. The participants were recruited from the local endocrine and infertility clinics. All the women were instructed to use barrier contraception combined with spermatocidal cream provided by the department throughout the trial period due to the potential risks in pregnancy. No serious side effects were reported. All participants had normal liver functions at the end of the trial period. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated numbers. Randomisation was conducted by the local pharmacist |
| Allocation concealment (selection bias) | Low risk | The code was kept in the pharmacist department until the end of the trial |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts: 2 in total, 1 in each group |
| Selective reporting (reporting bias) | Low risk | All primary measures reported |
| Other bias | Low risk | Primary objective investigated the effect of pioglitazone on growth hormone levels in women with PCOS. All women were instructed to use contraception |
Hoeger 2004.
| Methods | RCT Setting: USA Method of randomisation: computer‐generated random number, randomisation conducted by the pharmacy department* Blinding: double Number randomised: 38 |
|
| Participants | Metformin vs placebo
Summary: PCOS, obese Inclusion criteria: PCOS (oligomenorrhoea with < 6 menses/year and evidence of hyperandrogenism), BMI > 25, normal TSH, prolactin and FSH concentrations No hormonal treatment within 2 months before the trial commenced. Exclusion criteria: adrenal disease Baseline characteristics of each group:
Dropouts: 3 (33.3%) in the metformin arm and 2 (22.2%)in the placebo arm at 24 months of the trial Lifestyle advice + metformin vs lifestyle advice alone Summary: PCOS, obese Inclusion criteria: PCOS (oligomenorrhoea with < 6 menses/year and evidence of hyperandrogenism), BMI > 25, normal TSH, prolactin and FSH concentrations No hormonal treatment within 2 months before the trial commenced Exclusion criteria: adrenal disease Baseline characteristics of each group:
Dropouts: 4 (44.4%) in the metformin/lifestyle arm and 2 (18.2%)in the placebo/lifestyle arm at 24 months of the trial |
|
| Interventions | Main intervention: metformin 850 mg 2/d or placebo Duration: 24 months Co‐interventions: lifestyle modification programme to reduce calorie intake by 500‐1000 kcal/d. All women were provided with an individual, healthy, balanced meal plan. The lifestyle team consisted of a dietitian and exercise physiology. No lifestyle modification for the non‐obese group |
|
| Outcomes | Anthropometric: weight, BMI, hirsutism Hormones: total testosterone, SHBG, FAI, AUC glucose, AUC insulin, fasting glucose, fasting insulin* Metabolic markers: Others: menstrual pattern* |
|
| Notes | This trial was designed to investigate the combined effects of metformin and intensive lifestyle modification in overweight women with PCOS. The women were recruited through a direct advertisement, referral from physician and reproductive endocrinology outpatient clinic in the same study centre. The women were randomised into 4 groups (metformin alone, placebo alone, combined lifestyle changes and metformin, and lifestyle changes alone). We decided to separate the analysis into 2 groups; metformin versus placebo and combined lifestyle and metformin versus lifestyle We also decided to analyse the results for those who completed the trial at 24 weeks as there were too many dropouts at the end of the trial period at 48 weeks. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random number |
| Allocation concealment (selection bias) | Low risk | Randomisation conducted by the pharmacy department |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double. Drug and placebo packaged and labelled according to participant number by the pharmacy |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts: 3 (33.3%) in the metformin arm and 2 (22.2%)in the placebo arm at 24 months of the trial. Further 4 (44.4%) in the metformin/lifestyle arm and 2 (18.2%) in the placebo/lifestyle arm at 24 months of the trial. Baseline characteristics between the subjects completed and the drop outs were similar |
| Selective reporting (reporting bias) | Low risk | Study protocol available. Pre‐specified outcome measures (ovulation and testosterone levels) were reported |
| Other bias | Low risk | |
Hwu 2005.
| Methods | RCT Setting: Taiwan Method of randomisation: computer‐generated random numbers, block of 2 randomisation process* Blinding: no* Number randomised: 80 |
|
| Participants | Summary: CC‐resistant PCOS
Inclusion criteria: oligomenorrhoea (< 6 menses/year), clinical or biochemical hyperandrogenism (total testosterone > 2.42 nmol/L), PCO on USS (≥ 12 follicles 2‐9 mm in diameter per ovary) CC resistance was defined as no follicular development after 2 cycles up to 150 mg CC treatment for 5 d Exclusion criteria: not mentioned Baseline characteristics of each group:
Dropouts: none |
|
| Interventions | Main intervention: metformin 500 mg 3/d versus no treatment. Metformin was commenced on day 1 after induced menstruation followed by a 5‐d course of CC 150 mg treatment from day 13 of the cycle. When there was evidence of follicles > 12 mm in diameter 3 days after the last dose of CC, metformin was continued until the dominant follicles reached 20 mm. Intramuscular hCG 5000 IU was then administrated and the participants were instructed to have intercourse in the following 2 days Duration: 1 cycle Co‐interventions: CC 150 mg, hCG 5000 IU (Pregnyl; Organon, Holland) |
|
| Outcomes | Ovulation: confirmed by USS and serum progesterone > 5 ng/mL on day 7 after hCG injection Anthropometric: Hormones: Metabolic markers: Others: pregnancy and miscarriage rates |
|
| Notes | This study was to evaluate the effect of a short course of metformin as a co‐therapy in ovulation induction with CC 150 mg in women with PCOS who developed CC resistance in the previous treatment cycles. Compared with the other included studies, CC treatment was commenced at day 13 of the menstrual cycle rather than at early follicular phase. Intramuscular hCG (5000 IU) was used to trigger ovulation when a dominant follicle reached a diameter of 20 mm. The sequence of allocation was not concealed and this study was unblinded. Therefore, bias cannot be excluded. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers, block of 2 randomisation process* |
| Allocation concealment (selection bias) | High risk | The sequence of allocation was not concealed and this study was unblinded. |
| Blinding (performance bias and detection bias) All outcomes | High risk | Not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | High risk | Using hCG injection triggering ovulation rather than natural ovulation |
Jakubowicz 2001.
| Methods | RCT Setting: Venezuela (63% white, 31% Hispanic, 4% Arabic, 2% South American Indian) Method of randomisation: sequentially numbered, identical containers of identical drugs* Blinding: double‐blind Number randomised: 48 |
|
| Participants | Summary: obese PCOS, CC‐sensitive Inclusion criteria: PCOS (oligomenorrhoea ≤ 8 cycles/year, elevated free testosterone, exclusion of other endocrinopathy, ultrasonographic finding of PCO), ovulation with CC 150 mg (demonstrated by serum progesterone > 12.7 pmol/L and US) Exclusion criteria: adrenal hyperplasia, thyroid dysfunction, hyperprolactinaemia, diabetes mellitus, failure to ovulate with CC as described above, medication that could affect insulin sensitivity* Baseline characteristics of each group:
Dropouts: after randomisation, 8 (14%), 2 in metformin arm and 6 in placebo. Not included in analysis |
|
| Interventions | Main intervention: 1 of metformin 500 mg 3/d, placebo Duration: 4‐5 weeks prior to CC, then for a further 19 d after commencing CC Co‐interventions: CC 150 mg for 5 d |
|
| Outcomes | Ovulation: by serum progesterone > 12.7 pmol/L and US. Ovulation checked on 2 occasions on day 23: once after metformin/placebo cycle and once after subsequent metformin/placebo with CC. Anthropometric: BMI, WHR Reproductive hormones: total testosterone, free testosterone, androstenedione, DHEAS, 17‐beta estradiol, SHBG Metabolic markers: fasting glucose, fasting insulin, AUC insulin and glucose during GTT Others: glycodelin, IGFBP‐1, endometrial thickness, endometrial vascular penetration, resistance index of uterine spiral arteries |
|
| Notes | Women that were given metformin and ovulated received an extra week's course of treatment when compared with the placebo group. High dropout rate between recruitment and randomisation (24%) as only those who ovulated with CC prior to randomisation were included. The primary outcome measures are not relevant to this review, but the other parameters reported are. It is assumed that the units quoted for testosterone are mmol/dL and not mmol/L. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered, identical containers of identical drugs |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropouts: after randomisation, 8 (14%), 2 in metformin arm and 6 in placebo. Not included in analysis. Missing data not reported. High dropout rate between recruitment and randomisation (24%) as only those who ovulated with CC prior to randomisation were included. |
| Selective reporting (reporting bias) | Unclear risk | The primary outcome measures are not relevant to this review, but the other parameters such as ovulation reported are. |
| Other bias | Low risk | Women that were given metformin and ovulated received an extra week's course of treatment when compared with the placebo group. |
Kar 2015.
| Methods | RCT Setting: India (private hospital) Method of randomisation: envelopes prepared by a nurse "naive to this study" Blinding: double‐blind Number randomised: 105 |
|
| Participants | Summary: Asian Indian women with "treatment naive" PCOS
Inclusion criteria: history of infertility and oligomenorrhoea, meeting the Rotterdam criteria for PCOS. Normal male factor, at least 1 patent tube by hysterosalpingography, treatment naive Exclusion criteria: any major systemic illness Baseline characteristics of each group: no significant difference in age (years), duration of infertility (years), BMI, Ferriman‐Galloway score, waist circumference, hip circumference. No significant difference in biochemical parameters, such as FSH, LH, TSH, prolactin, insulin, fasting blood glucose, insulin resistance and metabolic syndrome Dropouts: 24 (81 women completed the study) |
|
| Interventions | Main intervention: 3 equal groups. Group 1: CC 50‐150 mg/d. Group 2: metformin 1700 mg/d. Group 3: CC plus metformin, doses as above) Duration: 6 months, or until pregnant, or until resistant to CC Co‐interventions: not applicable |
|
| Outcomes | Primary: live birth rate Secondary: ovulation rate, pregnancy rate, early pregnancy loss rate |
|
| Notes | We have contacted the study authors for further information regarding methodology | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of generating random sequence for distribution in envelopes not stated |
| Allocation concealment (selection bias) | Unclear risk | Allocation revealed in envelopes but not clear if opaque or sealed |
| Blinding (performance bias and detection bias) All outcomes | Low risk | A member of staff separate to the investigators supplied the envelopes containing the allocation. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 22.9% dropout rate, without reasons given Data analysis not performed as ITT |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Low risk | None noted |
Karimzadeh 2007.
| Methods | RCT Setting: Iran Method of randomisation: computer‐generated sequences that was sealed in envelopes Blinding: double Number randomised: 200 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: Rotterdam criteria 2003 Exclusion criteria: hyperprolactinaemia, CSH, thyroid disease, Cushings syndrome, androgen‐secreting tumour Baseline characteristics of each group:
Dropouts: not mentioned |
|
| Interventions | Main intervention: metformin 500 mg 3/d, placebo Duration: 3 months Co‐interventions: nil |
|
| Outcomes | Ovulation: progesterone > 10 ng/mL Metabolic markers: cholesterol, triglycerides Others: pregnancy |
|
| Notes | Women were recruited from a single centre. The primary objective of this study was to investigate the effect of metformin on lipid profile. The duration of the trial was relatively short. Therefore, it was difficult to ascertain the reliability on both of the ovulation rates and the improvement in menstrual patterns. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated sequences that were sealed in envelopes |
| Allocation concealment (selection bias) | Low risk | Sequences sealed in envelopes and code kept in the pharmacy department |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not stated |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information to assess other bias. Sample size calculation not mentioned. Unspecified recruitment period |
Karimzadeh 2010.
| Methods | RCT Setting: Iran Method of randomisation: not stated Blinding: not stated Number randomised: 343 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: Rotterdam criteria 2003. Age between 19 and 35, BMI 25‐29, primary infertility, normal prolactin levels, TFT, liver and renal functions Exclusion criteria: male factor infertility Baseline characteristics of each group:
Dropouts: none |
|
| Interventions | Main intervention: metformin 500 mg 3/d, no placebo Duration: 3‐6 months Co‐interventions: CC 100 mg day 3‐7; lifestyle group were advised to increase daily exercise for 30 min along with high carbohydrate diet |
|
| Outcomes | Ovulation: USS follicular tracking | |
| Notes | This study compared the effect of CC, metformin, combined CC and metformin, and lifestyle modification on subfertile women with PCOS. Very little information can be extracted from the study protocol. A large sample size without any dropouts Some of the women may have been included in the previous trial Karimzadeh 2007. No reply from study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Inadequate information |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Inadequate information |
| Selective reporting (reporting bias) | Low risk | Not all the primary outcome measures (endocrine parameters, lipid profile) data available |
| Other bias | Low risk | A large sample size without any dropouts Some of the women may have been included in the previous trial Karimzadeh 2007. No reply from study author |
Khorram 2006.
| Methods | RCT Setting: USA Method of randomisation: picking a card out of a box Blinding: none Number randomised: 31 |
|
| Participants | Summary: obese PCOS Inclusion criteria: oligomenorrhoea (< 8 cycles/year), PCO on USS, clinical (acne, hirsutism, alopecia) or biochemical hyperandrogenism (elevated testosterone level) BMI > 29 Exclusion criteria: pregnancy, hepatic or renal disease, heart disease, alcoholism, pulmonary disorder, abnormal TFT, hyperprolactinaemia, CAH or androgen‐secreting tumour Baseline characteristics of each group:
Dropouts: none |
|
| Interventions | Main intervention: metformin 500 mg 3/d. Placebo was not used Duration: 2 weeks from the start of the menstrual cycle. 1 trial cycle only Co‐interventions: CC 100 mg for 5 d from day 5 of the cycle |
|
| Outcomes | Ovulation: method to detect ovulation was not stated Hormones: free testosterone, testosterone, SHBG Metabolic markers: insulin, glucose |
|
| Notes | This study was designed to evaluate the effect of a shot course of metformin treatment on the outcomes of CC ovulation induction therapy. All participants were Hispanic except 1 African American in the CC‐only group and 1 white woman in the combined group. None of the participants had taken CC before. The trial was unblinded. The method of randomisation and concealment were inadequate. Therefore, potential bias may have been introduced. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Picking a card out of a box |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Insufficient information |
Lam 2011.
| Methods | RCT Setting: Hong Kong Method of randomisation: computer‐generated random number, block of 10 Blinding: double Number randomised: 70 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: Rotterdam criteria Exclusion criteria: CAH, Cushing's syndrome, endometrial hyperplasia, diabetes, cardiovascular, hepatic or renal disease Baseline characteristics of each group:
Dropouts: 11 in metformin, 5 in placebo |
|
| Interventions | Main intervention: rosiglitazone 4 mg or placebo Duration: 6 months Co‐interventions: |
|
| Outcomes | Menstrual cycle frequency Metabolic parameters: lipid profiles, testosterone, SHBG, glucose and insulin |
|
| Notes | This study investigated the effect of using rosiglitazone on Chinese women with PCOS. It is unclear whether the subjects were infertile. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random number |
| Allocation concealment (selection bias) | Low risk | Trial drug and placebo similar appearance, and packaged according to the trial number. The code kept in the local pharmaceutical company and concealed from the research team until the end of the trial. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | High risk | A much higher dropout rate in the rosiglitazone group than the placebo group. Missing data not reported |
| Selective reporting (reporting bias) | Low risk | A clear, detailed study protocol and all primary outcome measures reported |
| Other bias | Unclear risk | Inadequate information |
Legro 2007.
| Methods | RCT Setting: USA Method of randomisation: a large multi‐centre, randomised, placebo‐controlled study. (see Legro 2006b for detail) Blinding: double Number randomised: 626 |
|
| Participants | Summary: obese PCOS Inclusion criteria: oligomenorrhoea (< 8 periods/year), biochemical hyperandrogenism (elevated testosterone level documented within the previous year on the basis of local laboratory results) Women should have at least 1 proven patent fallopian tube. Normal uterine cavity. Normal semen analysis (sperm concentration > 20 million/mL) Exclusion criteria: hyperprolactinaemia, CSH, thyroid disease, Cushings's syndrome, androgen‐secreting tumour Baseline characteristics of each group: Mean age (SD) 28.3 (4.0), 27.9 (4.0), 28.1 (4) Mean BMI (SD) 34.2 (8.4), 36.0 (8.9), 35.6 (8.5) Mean fasting insulin mIU/L (SD) 22.4 (30), 22.6 (20.7), 24 (28.4) Mean total testosterone mmol/L (SD) 2.21 (0.98), 2.13 (1.1), 2.13 (0.87) Dropouts: 49 (23.7%) in the metformin and CC group, 55 (26.3%) in the placebo and CC group, 72 (34.6%) in the metformin group. The differences were not significant. |
|
| Interventions | Main intervention: 2 extended‐release metformin 500 mg or 2 placebo tablets twice daily Duration: up to 6 cycles or 30 weeks Co‐interventions: CC 50 mg or second matching placebo tablet was commenced concurrently from day 3‐7 of the cycle. When women had no or poor response, the dose was increased by 50 mg or 1 additional placebo tablet with the maximum dose of 150 mg or 3 placebo tablets |
|
| Outcomes | Ovulation: progesterone > 5 ng/mL Anthropometric: BMI, WHR Hormones: testosterone, SHBG Metabolic markers: insulin, proinsulin, glucose Others: pregnancy, live birth, miscarriage, side effects, serious adverse events in pregnancy |
|
| Notes | This is the largest RCT published so far on the effects of metformin on women with PCOS. A total of 626 infertile women with PCOS were randomised into 3 groups (metformin and placebo, metformin and CC, CC and placebo). The sample size calculation was based on the live birth rates. The secondary outcomes included the rate of pregnancy loss, singleton birth and ovulation. Based on the initial sample size calculation, 678 was needed to detect a 15% absolute difference in live birth rates with a power of 80% and a type I error of 0.05. Due to limitations in the supplying metformin and the matching placebo tablets, the number of required women was reduced to 626. This was approved after the assessment by the data safety and monitoring board. Because the observed live birth rate was lower than projected, the number of recruited participants (626) was sufficient to detect a 15% difference with the same magnitude of power and type I error. The backgrounds of the participants were relatively heterogeneous. Two‐thirds of the participants were white and about one‐third was Hispanic or Latino origin. Only 40% of the women had no previous exposure to metformin or CC. Ovulation was confirmed when 2 consecutive measurements of progesterone levels > 5 ng/mL in 1‐2 weeks apart. US monitoring of ovarian response was not included in the study protocol. Ovulation triggering with hCG and intrauterine insemination were not employed in this study. Metformin combined with CC did not achieve a better live birth rate compared with CC therapy. The metformin group was found to have a significantly inferior pregnancy and live‐birth rate compared with the combined therapy (metformin and CC) and the CC groups. This study also demonstrated that BMI poses a significant negative impact on live births. In this most recent update, ITT analysis was used to determine ovulation rate per woman. This was calculated from the first 3 treatment cycles, taking into account the number of women who became pregnant. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated; participants were randomised by means of an interactive voice system and stratified based on study site and previous exposure to study drugs |
| Allocation concealment (selection bias) | Low risk | Each participant received a medication package on a monthly basis that consisted of a bottle M (metformin or placebo) and a bottle C (CC or placebo). Data co‐ordinating centre at the clinical research institute Legro 2006b |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts: 49 (23.7%) in the metformin and CC group, 55 (26.3%) in the placebo and CC group, 72 (34.6%) in the metformin group. A much higher dropout rate at the metformin‐only group. The differences were not significant. Characteristics of the subjects who dropped out were not given. |
| Selective reporting (reporting bias) | Low risk | All primary and secondary outcome measures reported |
| Other bias | High risk | The original sample size was 678 to detect a 15% absolute difference in live birth rates. However, due to drug supply logistics, the sample size later reduced to 626 after the data safety and monitoring board review. |
Lord 2006.
| Methods | RCT Setting: UK Method of randomisation: randomisation was conducted centrally by computer at the hospital pharmacy department using a block with sequential numbers. The code was kept sealed until the trial was completed.* Blinding: double Number randomised: 44 |
|
| Participants | Summary: obese PCOS Inclusion criteria: oligomenorrhoea (< 6 periods/year), biochemical hyperandrogenism (FAI > 5.0) Age between 18‐40 years Exclusion criteria: diabetes, thyroid disease, hyperprolactinaemia, CAH, the use of ovulation‐induction agents or drugs that could affect insulin metabolism within 2 months before the start of the trial Baseline characteristics of each group:
Dropouts: 3 women in the metformin group and 1 in the placebo were excluded after they were assigned to the group (did not meet the inclusion criteria). Furthermore, 3 (2 due to pregnancy and 1 lost to follow‐up) in the metformin arm and 5 (3 due to pregnancy and 2 lost to follow‐up) in the placebo arm did not complete the study. Overall, 6 (27.2%) in the metformin group and 6 (27.2%) in the placebo group withdrew from the study after they had been randomised. |
|
| Interventions | Main intervention: metformin 500 mg or placebo tablet 3/d Duration: 12 weeks Co‐interventions: general advice on diet and exercise |
|
| Outcomes | Ovulation: progesterone > 30 nmol/L Anthropometric: the distributions of subcutaneous and visceral fat were measured by areal planimetry (CT scan), weight, BMI, waist circumference, WHR, BP Hormones: testosterone, SHBG, DHEAS Metabolic markers: insulin, glucose, LDL, HDL, triglyceride Others: menstrual pattern, pregnancy |
|
| Notes | This study was to ascertain the effects of metformin on metabolic parameters, visceral and subcutaneous fat distributions in women with PCOS. The fat distribution was measured with areal planimetry (CT scan). There were no significant changes in any of the measures of fat distribution between the metformin and the placebo groups. Although, metformin significantly reduced serum cholesterol concentrations, treatment effects on androgens, insulin, triglycerides, ovulation and pregnancy were not observed. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was conducted centrally by computer at the hospital pharmacy department using a block with sequential numbers. |
| Allocation concealment (selection bias) | Low risk | The code was kept sealed until the trial was completed. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Overall, 6 (27.2%) in the metformin group and 6 (27.2%) in the placebo group withdrew from the study after they had been randomised. Details of dropouts were not provided |
| Selective reporting (reporting bias) | Low risk | All outcome measures reported |
| Other bias | Unclear risk | Inadequate information |
Machado 2012.
| Methods | RCT Setting: Brazil Method of randomisation: numbered, sealed, opaque envelopes Number randomised: 36 |
|
| Participants | Summary: CC‐resistant PCOS Inclusion criteria: oligomenorrhoea or amenorrhoea, Rotterdam criteria for PCOS, lack of response to previous ovulation induction with CC Exclusion criteria: male factor and tubal infertility, endocrinology and chronic health conditions, the use of hormonal treatments within 60 days of the trial commencing Baseline characteristics of each group: placebo, metformin
Dropouts*: 67 women were initially included in the study. 21 women did not respond to CC alone and 13 became pregnant. 36 women were then randomised to receive metformin or placebo. All 36 women completed the study, with no women dropping out |
|
| Interventions | Main intervention: metformin 850 mg 2/d or placebo tablet 2/d Duration: 60 days Co‐interventions: CC 100 mg day 5‐9 with concurrent use of metformin or placebo |
|
| Outcomes | Ovulation: visible follicular growth on USS with subsequent formation of the corpus luteum. Free fluid in the POD and change of endometrial thickness also. Plasma progesterone > 3000 pg/mL on day 21 Anthropometric: BMI, WHR Metabolic markers: insulin, glucose, glucose‐insulin ratio, LFTs, creatinine Others: pregnancy rate |
|
| Notes | This study aimed to evaluate the efficacy of metformin with CC on ovulation in women previously resistant to CC alone. We did not perform a subgroup analysis by BMI in our analysis due to the small number of women in the study. *Additional information was provided by the study author on request. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Numbered envelopes used |
| Allocation concealment (selection bias) | Low risk | Sealed, opaque envelopes used |
| Blinding (performance bias and detection bias) All outcomes | Low risk | The author has confirmed in private correspondence that women and healthcare providers were blinded for the duration of the study. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data were available for all 36 women who participated in the study. |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Low risk | No other potential bias detected |
Maciel 2004.
| Methods | RCT Setting: Brazil Method of randomisation: computer‐generated random numbers Blinding: double Number randomised: 30 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: amenorrhoea or oligomenorrhoea (< 6 periods/year), clinical or biochemical hyperandrogenism. USS evident of PCO was not part of the diagnostic criteria. Age between 17‐32 years Exclusion criteria: other causes of amenorrhoea. Use of lipid‐lowering drugs, antidiabetic medications or hormonal contraception within 3 months of the recruitment; Cushing's syndrome, CAH, androgen‐secreting tumours, diabetes, renal or hepatic disease Baseline characteristics of each group:
Dropouts: details of the dropouts were not available Summary: obese PCOS Inclusion criteria: amenorrhoea or oligomenorrhoea (< 6 periods/year), clinical or biochemical hyperandrogenism. USS evident of PCO was not part of the diagnostic criteria. Age between 17‐32 years Exclusion criteria: other causes of amenorrhoea. Use of lipid‐lowering drugs, antidiabetic medications or hormonal contraception within 3 months of the recruitment; Cushing’s syndrome, CAH, androgen‐secreting tumours, diabetes, renal or hepatic disease. Baseline characteristics of each group: Mean age (SD) 20.5 (5.4), 21.1 (1.7) Mean BMI (SD) 37.2 (4.8), 35.8 (3.7) Mean fasting insulin mIU/L (SD) 22.6 (11.6) 20.9 (4.6) Mean total testosterone nmol/L (SD) 4.1 (0.8), 3.5 (2.4)) Dropouts: details of the dropouts were not available |
|
| Interventions | Main intervention: metformin 500 mg or placebo tablet 3/d Duration: 6 months Co‐interventions: none |
|
| Outcomes | Anthropometric: BMI, BP Hormones: testosterone, SHBG, free testosterone, androstenedione Metabolic markers: insulin, glucose, AUC insulin, AUC glucose, LDL, HDL and triglyceride Others: menstrual pattern, hirsutism |
|
| Notes | The primary objective of this study was to compare the clinical, hormonal and biochemical effects of metformin therapy in the obese PCOS group (BMI > 30) with the non‐obese group (BMI < 30). We entered the results of the obese group separately in the analysis. The results indicated that non‐obese participants responded better than obese participants with PCOS to metformin 1.5 g/d. Non‐obese women experienced an improvement in menstrual cyclicity, decrease in serum androgen levels and fasting insulin concentrations; whilst, obese women showed a significant reduction of free testosterone levels. Caution is needed to interpret the results as 5 of the original 34 enrolled participants did not complete the trial and these findings were not included in the analysis. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers |
| Allocation concealment (selection bias) | Low risk | Participants received a sealed envelope that contained the study number. An independent clinician recorded side effects and clinical measurements |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 5 participants were not evaluated because of pregnancy. Details were not given |
| Selective reporting (reporting bias) | Unclear risk | All pre‐specified outcome measures (androgens and metabolic parameters) |
| Other bias | Unclear risk | Although USS evidence of PCO was not employed as part of the diagnostic criteria for PCOS, the diagnostic criteria used in this study would have met the Rotterdam criteria. |
Malkawi 2002.
| Methods | RCT Setting: Jordan Method of randomisation: centralised randomisation process with women receiving a sequential number* Blinding: double‐blind* Number randomised: 28 |
|
| Participants | Summary: non‐obese PCOS, CC resistance Inclusion criteria: US findings of polycystic ovaries together with 3 of: oligomenorrhoea < 6 cycles in preceding year, Ferriman‐Gallwey score > 7, hyperandrogaenemia (free testosterone, androstenedione, DHEAS), elevated LH or LH:FSH > 2 CC resistance defined as failure to ovulate with 150 mg day 5‐9 for 3 months. Normal uterine cavity and patent tubes on hysterosalpingography. Normal semen analysis Exclusion criteria: raised prolactin, adrenal hyperplasia, thyroid dysfunction, Cushing's syndrome. Baseline characteristics of each group:
Dropouts: nil |
|
| Interventions | Main intervention: 1 of metformin 850 mg 2/d, placebo Duration: 6 months Co‐interventions: CC 50 mg day 5‐9 in the first cycle, increasing by 50 mg up to 200 mg in each subsequent cycle until ovulation achieved |
|
| Outcomes | Ovulation: serum progesterone on day 21 and 28 > 15.9 nmol/L Others: pregnancy |
|
| Notes | Units of testosterone assumed to be ng/mL *Information kindly provided by the study author that was not in the original paper |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Centralised randomisation process with women receiving a sequential number |
| Allocation concealment (selection bias) | Unclear risk | Centralised randomisation process with women receiving a sequential number |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Moghetti 2000.
| Methods | RCT Setting: Italy Method of randomisation: sequentially numbered, identical containers of identical drugs* Blinding: double‐blind Number randomised: 23 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: PCOS (oligomenorrhoea ≤ 6 cycles/year or anovulation confirmed with luteal‐phase progesterone, hyperandrogaenemia (either raised serum androgens, or clinical hyperandrogaenemia*). Exclusion of other endocrinopathy Exclusion criteria: adrenal hyperplasia, Cushing's syndrome, thyroid dysfunction, hyperprolactinaemia, androgen‐secreting tumour, concomitant disease, taking any medication. Baseline characteristics of each group:
Dropouts: nil* |
|
| Interventions | Main intervention: 1 of metformin 500 mg 3/d, placebo Duration: 26 weeks Co‐interventions: no modification in usual eating habits |
|
| Outcomes | Anthropometric: BMI, WHR, Reproductive hormones: free testosterone, androstenedione, DHEAS, SHBG, FSH, LH Metabolic markers: fasting glucose, fasting insulin, 120‐min insulin and glucose levels after GTT, insulin sensitivity, HDL, LDL, triglycerides, systolic BP, diastolic BP Others: menstrual pattern, 17‐alpha‐hydroxyprogesterone response to buserelin |
|
| Notes | Placebo group had significantly higher BMI (P < 0.05) at baseline and higher fasting insulin (non‐significant), but similar insulin sensitivity. Metformin group had higher androgens (non‐significant) Mild side effects in 5 in metformin group and 2 in placebo group It is assumed that the figures quoted in the publication are for standard errors. *Information kindly provided by the study author that was not in the original paper |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered, identical containers of identical drugs |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Low risk | All primary outcome measures reported (menstrual frequency and metabolic parameters) |
| Other bias | High risk | Placebo group had a significantly higher BMI than the metformin group. It was assumed that the figures quoted in the publication are for standard errors. |
Moll 2006.
| Methods | Multicentre RCT Setting: the Netherlands Method of randomisation: computer‐generated blocks of 4 Blinding: double‐blind Number randomised: 225 |
|
| Participants | Summary: non‐obese women with PCOS Inclusion criteria: PCOS (according to Rotterdam consensus), normal FSH concentrations Exclusion criteria: age > 40 years, abnormal liver function tests or creatinine levels > 95 umol/L, history of heart disease, history of male factor infertility with total motile sperm count < 10 x 106 Baseline characteristics of each group:
Dropouts: no significant difference in the dropout rates, 28 (25%) in the metformin arm, 21 (18%) in the placebo arm |
|
| Interventions | Main intervention: metformin 2000 mg/d (increased from 500 mg to 2000 mg over a period of 7 days in order to limit the side effects) or placebo Duration: all women received metformin or placebo for 1 month before starting CC treatment (a maximum of 6 cycles for those who ovulated with CC) Co‐interventions: CC 50 mg from day 3 (spontaneous menstruation) or day 5 (progestogen induced menstruation) for a period of 5 days. If ovulation did not occur with this dose, CC was increased with steps of 50 mg with a maximum of 150 mg/d in the next cycles |
|
| Outcomes | Ovulation: progesterone > 14 nmol/L in the second half of menstrual cycle, biphasic basal body temperature curve, follicular diameter > 16 mm on transvaginal USS or pregnancy Anthropometric: Hormones: Metabolic markers: Others: pregnancy, miscarriage and CC resistance |
|
| Notes | A large, multicentre RCT. The sample size calculation was based on the ovulation rate. In total, 228 women were initially screened and 3 were subsequently excluded. 111 women were randomised to receive metformin and CC; whilst 114 received placebo and CC. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated blocks of 4 |
| Allocation concealment (selection bias) | Low risk | Randomisation was carried out in the co‐ordinating centre (Amsterdam) and the list was kept until inclusion was completed |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double blind. Each centre received blinded, numbered container |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropouts: no significant difference in the dropout rates, 28 (25%) in the metformin arm, 21 (18%) in the placebo arm. Details of the dropout participants not mentioned; although number of dropouts in each group were similar |
| Selective reporting (reporting bias) | Low risk | Primary outcome (ovulation) and secondary outcome (pregnancy, miscarriage rates) measures reported |
| Other bias | Unclear risk | Inadequate information |
Morin‐Papunen 2012.
| Methods | Multicentre RCT (parallel‐group study) Setting: Finland Method of randomisation: randomisation codes remained concealed. Metformin and placebo identically packaged and consecutively numbered Blinding: double Number randomised: 320 |
|
| Participants | Summary: metformin and pregnancy outcomes in PCOS Inclusion criteria: anovulatory infertility for at least 6 months and 3 months since the last infertility treatment. Age range 18‐39 years Exclusion criteria: type 1 diabetes mellitus, liver, cardiac or renal disease, hormone medication, alcohol use, regular smoking Baseline characteristics of each group: Metformin, placebo
Dropouts: 61 women were lost to follow‐up or discontinued but their data were included in the ITT analysis |
|
| Interventions | Main intervention: metformin 500 mg 1/d for 1 week, then increased weekly by 1 extra tablet/d to 1.5 g in non‐obese and 2 g/d in obese women versus placebo Duration: 3‐9 months Co‐interventions: if pregnancy has not occurred by 3 months, ovulation induction was started with CC. If unsuccessful after 4‐6 cycles, gonadotrophins or aromatase inhibitors were used |
|
| Outcomes | Anthropometric: WHR, waist (cm), hirsutism score, BMI, ovarian volume Others: pregnancy rate, miscarriage rate, pregnancy complications, live birth rate |
|
| Notes | This study was to ascertain the effects of metformin on pregnancy and live birth rates. Endocrine/metabolic outcomes not measured. Additional information sought from the study authors | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Performed by hospital pharmacy with 1:1 allocation in random blocks of 10 using computer‐generated lists |
| Allocation concealment (selection bias) | Low risk | Randomisation codes remained blinded until database lock had taken place |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Metformin and placebo identically packaged and consecutively numbered |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 61 women were lost to follow‐up or discontinued but their data were included in the ITT analysis |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Unclear |
Nestler 1998.
| Methods | Multicentre RCT Setting: USA (3 participants), Venezuela (54 participants), Italy (4 participants)* Method of randomisation: centralised randomisation process*. Blinding: single‐blind, participants blinded Number randomised: 61 |
|
| Participants | Summary: PCOS, obese Inclusion criteria: PCOS (oligomenorrhoea < 6 cycles/year, hyperandrogaenemia (elevated free testosterone), exclusion of other endocrinopathy, US finding of PCO), BMI >28 Exclusion criteria: diabetes mellitus, adrenal hyperplasia, thyroid dysfunction, hyperprolactinaemia, taking any medication for previous 2 months Baseline characteristics of each group:
Dropouts: none |
|
| Interventions | Main intervention: 1 of metformin 500 mg 3/d, placebo Duration: 34 d, then those who did not ovulate continued for a further 19 d Co‐interventions: those that did not ovulate after 34 days had CC 50 mg for 5 d and continued metformin/placebo for a total of 53 d |
|
| Outcomes | Ovulation: by serum progesterone (≥ 25.6 nmol/L) measured on days 14, 28, 35 (and 44 & 53 in those that went on to receive CC) Anthropometric: BMI, WHR Reproductive hormones: total testosterone, free testosterone, androstenedione, DHEAS, SHBG, 17‐beta estradiol Metabolic markers: fasting glucose, fasting insulin, AUC of insulin and glucose during GTT |
|
| Notes | 89% of participants were recruited in Venezuela Most of the outcome measures were only reported for those that failed to ovulate during the metformin vs placebo phase of the trial. These have not been included in the analysis as a further analysis to include all participants was not possible. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Centralised randomisation process |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | High risk | Single‐blinded (participant only) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | No dropouts. Most of the outcome measures were only reported for those that failed to ovulate during the metformin vs placebo phase of the trial. |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Nestler 1999.
| Methods | Multicentre RCT Setting: Venezuela (white 73%, Hispanic 16%, Afro‐Hispanic 4.5%, Arabic 4.5%, Asian 2%) Method of randomisation: drug and placebo packaged at same time and labelled according to participant number. Randomisation in blocks of 4 Blinding: double‐blind Number randomised: 44 |
|
| Participants | Summary: PCOS, obese Inclusion criteria: PCOS (oligomenorrhoea ≤ 8 cycles/year, hyperandrogaenemia (elevated free testosterone)* or hirsutism (physician reported ‐ subjective)*, exclusion of other endocrinopathy), BMI > 28 Exclusion criteria: diabetes mellitus, thyroid dysfunction, hyperprolactinaemia, taking any medication for previous 2 months. Baseline characteristics of each group:
Dropouts: none |
|
| Interventions | Main intervention: 1 of D‐chiro inositol 1200 mg 1/d, placebo Duration: 6 weeks; those who ovulated continued for a further 2 weeks Co‐interventions: no change in usual eating habits, physical activity or lifestyle |
|
| Outcomes | Ovulation: by serum progesterone (≥ 25 nmol/L) weekly Anthropometric: BMI, WHR Reproductive hormones: total testosterone, free testosterone, androstenedione, DHEAS, SHBG, 17‐beta estradiol Metabolic markers: fasting glucose, fasting insulin, AUC of insulin and glucose during GTT, systolic BP, diastolic BP, HDL, LDL, triglycerides Others: LH response to leuprolide, 17‐alpha‐hydroxyprogesterone response to leuprolide |
|
| Notes | All women had US features of PCO, but this was not an inclusion criteria None of the participants had diabetes mellitus, but 10 (23%) had impaired glucose tolerance (6 in treatment arm, 4 in placebo arm) *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation in blocks of 4 |
| Allocation concealment (selection bias) | Low risk | Drug and placebo packaged at same time and labelled according to participant number |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Insufficient information |
Ng 2001.
| Methods | RCT Setting: Hong Kong (Chinese women) Method of randomisation: computer‐generated list in sealed envelopes Blinding: double‐blind Number randomised: 20 |
|
| Participants | Summary: non‐obese PCOS, CC resistance Inclusion criteria: PCOS (irregular cycles of ≤ 21 days or ≥ 35 days and cycle‐to‐cycle variation of > 4 days*, anovulation with mid‐luteal progesterone < 16 nmol/L whilst taking CC 100 mg for 5 d over 3 cycles, exclusion of other endocrinopathy (raised prolactin, thyroid disorder*), US findings of PCO, age < 40, day 2 FSH < 10, bilateral patent tubes demonstrated by laparoscopy, normal semen parameters Exclusion criteria: taking any sex hormones in previous 3 months, smokers, renal impairment. Baseline characteristics of each group*:
Dropouts: 5 (25%), 3 in placebo arm, 2 in metformin. Analysis on ITT |
|
| Interventions | Main intervention: 1 of metformin 500 mg 3/d, placebo Duration: 3 months. Those who did not ovulate continued for a further cycle Co‐interventions: CC 100 mg for 5 d was given after 3 months if there was no ovulation |
|
| Outcomes | Ovulation: by serum progesterone (> 16 nmol/L) weekly Anthropometric: BMI Reproductive hormones: total testosterone, androstenedione, DHEA, SHBG, FSH, LH Metabolic markers: fasting glucose, fasting insulin, 120‐min glucose levels after GTT, fasting leptin, HDL, LDL, triglycerides Other: live birth |
|
| Notes | The BMI was lower than in other trials In spite of the fact that anovulation and CC resistance was an inclusion criteria, 7 out of 9 women taking placebo ovulated (3 with placebo alone, and 4 out of the 6 remaining in the trial who had CC and placebo) *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated list |
| Allocation concealment (selection bias) | Low risk | In sealed envelopes. Double, identical appearance and packed by the hospital pharmacy. Code kept in the pharmacy department until the end of the trial |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropouts: 5 (25%), 3 in placebo arm, 2 in metformin. Analysis on ITT. Details not provided |
| Selective reporting (reporting bias) | Low risk | All primary outcome measures reported |
| Other bias | Unclear risk | In spite of the fact that anovulation and CC resistance was an inclusion criteria, 7 out of 9 women taking placebo ovulated (3 with placebo alone, and 4 out of the 6 remaining in the trial who had CC and placebo) |
Onalan 2005.
| Methods | RCT Setting: Turkey Method of randomisation: computer‐generated randomisation in blocks of 4 Blinding: double* Number randomised: 139 were randomised into 6 main groups according to the fasting glucose/insulin ratio (with a level < 4.5 classified as hyperinsulinaemia) and BMI (< 25, 25‐29.9 and > 30) |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: oligomenorrhoea (< 6 periods/year), clinical hyperandrogenism (Ferrriman‐Gallwey score > 7) and/or biochemical hyperandrogenism (free testosterone > 4 ng/dL) Exclusion criteria: other causes of hyperandrogenism, Cushing's syndrome, CAH, hyperprolactinaemia, thyroid dysfunction Baseline characteristics of each group:
Summary: obese PCOS Inclusion criteria: oligomenorrhoea (< 6 periods/year), clinical hyperandrogenism (Ferrriman‐Gallwey score > 7) and/or biochemical hyperandrogenism (free testosterone >4 ng/dL) Exclusion criteria: other causes of hyperandrogenism, Cushing's syndrome, CAH, hyperprolactinaemia, thyroid dysfunction Baseline characteristics of each group:
Dropouts: 15 in total, mainly due to gastro‐intestinal side effects. Further 8 women were excluded in the analysis because of pregnancy* Dropouts: 15 in total, mainly due to gastro‐intestinal side effects* |
|
| Interventions | Main intervention: metformin 850 mg or placebo tablet twice daily Duration: 6 months Co‐interventions: none |
|
| Outcomes | Ovulation: progesterone > 5 ng/mL Anthropometric: BMI, weight, WHR* Hormones: testosterone, free testosterone, androstenedione, DHEAS, cortisol* Metabolic markers: glucose, insulin, LDL, HDL, triglyceride* Others: hirsutism* |
|
| Notes | The objective of this study was to investigate the effects of hyperinsulinaemia (fasting glucose/insulin ratio < 4.5mg/10‐4 U and obesity (BMI > 30) on the responses to metformin treatment in women with PCOS. There were 6 subgroups, normoinsulinaemic lean (BMI < 25), overweight (BMI 25‐29.9) and obese (BMI >30); hyperinsulinaemic lean (BMI < 25), overweight (BMI 25‐29.9) and obese (BMI > 30) The results of the non‐obese subgroups were entered separately from the obese subgroup in the meta‐analysis We have written to the study author regarding the details of randomisation and concealment. Additionally, we also asked the study author to provide further information of the anthropometric, hormonal and metabolic results at the end of the trial period. *No reply from study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated blocks of 4 randomisation |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropouts: 15 in total (11%), mainly due to gastro‐intestinal side effects. Missing outcomes not addressed. Imbalance in missing data between the intervention and placebo groups. |
| Selective reporting (reporting bias) | Unclear risk | Primary outcome measures not stated. Inadequate study protocol reporting |
| Other bias | Unclear risk | Inadequate information to assess |
Otta 2010.
| Methods | RCT Setting: Argentina Method of randomisation: computer‐generated Blinding: double Number randomised: 30 |
|
| Participants | Summary: obese PCOS Inclusion criteria: oligomenorrhoea (cycle length > 35 days), biochemical hyperandrogenism (level not defined) Exclusion criteria: other causes of hyperandrogenism, Cushing's syndrome, CAH, hyperprolactinaemia, thyroid dysfunction, abnormal renal, liver functions, diabetes, infection Baseline characteristics of each group:
Dropouts: 1 in metformin, poor compliance |
|
| Interventions | Main intervention: metformin 750 mg or placebo tablet twice daily Duration: 4 months Co‐interventions: lifestyle modification (high carbohydrate diet and increase exercise with a minimum of 40 min walk/d) |
|
| Outcomes | Ovulation: method of detecting ovulation not stated Anthropometric: BMI, weight, WHR Metabolic markers |
|
| Notes | This study investigated the effects of combined metformin and lifestyle changes on endocrine and metabolic parameters in women with PCOS Methodology and study protocol were too brief. Unable to determine the quality of the trial Only 5 out of 30 subjects were trying to conceive. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Missing data not reported. 1 in metformin group and excluded from analysis |
| Selective reporting (reporting bias) | Unclear risk | Primary outcome measures were unclear |
| Other bias | Low risk | Methodology and study protocol were too brief. Unable to determine the quality of the trial Only 5 out of 30 subjects were trying to conceive. |
Palomba 2005.
| Methods | RCT Setting: Italy Method of randomisation: computer‐generated random allocation sequence in double block Blinding: double Number randomised: 100 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: National Institutes of Health criteria, age 20‐34 years, BMI < 30 kg/m2, tubal patency confirmed by hysterosalpingogram, normal semen analysis Exclusion criteria: metabolic disorders, hepatic or renal dysfunction, thyroid disease, hyperprolactinaemia, Cushing's syndrome, CAH, hormonal drugs, pelvic diseases, previous pelvic surgery Baseline characteristics of each group:
Dropouts: 5 in the metformin group and 3 in the metformin + CC group |
|
| Interventions | Main intervention: metformin 850 mg or matched placebo tablets twice daily Duration: 6 months Co‐interventions: CC 150 mg or matched placebo tablets, day 3‐7 of the cycle and timed intercourse |
|
| Outcomes | Ovulation: USS follicular tracking Pregnancy, ovulation |
|
| Notes | This study was designed to compare the effectiveness of metformin and CC treatment as a first‐line therapy in non‐obese anovulatory women with PCOS. The primary end point measure was the pregnancy rate. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random allocation sequence in double block |
| Allocation concealment (selection bias) | Unclear risk | Allocation sequence concealed until the interventions were assigned |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts: 5 in the metformin group and 3 in the metformin + CC group |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Insufficient information |
Pasquali 2000.
| Methods | RCT Setting: Italy Method of randomisation: block of 4. Drug and placebo packaged and labelled according to participant number Blinding: double‐blind Number randomised: 20 |
|
| Participants | Summary: obese PCOS Inclusion criteria: oligomenorrhoea (< 4 cycles in past 6 months), hyperandroenaemia, USS of PCO, BMI > 25, WHR > 0.8 Exclusion criteria: diabetes mellitus, adrenal hyperplasia, thyroid dysfunction, hyperprolactinaemia, cardiovascular, renal or liver dysfunction Baseline characteristics:
Dropouts: 2 from metformin arm due to pregnancy. Not included in analysis |
|
| Interventions | Main intervention: metformin 850 mg 2/d or placebo Duration: 6 months Co‐interventions: standardised hypercaloric diet 1 month prior to treatment and continued throughout the trial |
|
| Outcomes | Anthropometric parameters Reproductive hormones and metabolic markers |
|
| Notes | The trial was designed to investigate the combined effects of diet and metformin on fat distribution in women with PCOS. The study also included a control group who were matched for age, weight and WHR but with regular menstrual cycles. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block of 4, random table |
| Allocation concealment (selection bias) | Low risk | Drug and placebo packaged and labelled according to participant number |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Missing data not reported |
| Selective reporting (reporting bias) | Low risk | A clear protocol published with all primary outcome measured reported |
| Other bias | Unclear risk | Inadequate information |
PCOSMIC 2010.
| Methods | Multicentre RCT Setting: New Zealand Randomisation: double‐blind Number randomised: 171 |
|
| Participants | Inclusion criteria: women with PCOS according to Rotterdam consensus criteria Exclusion criteria: couples had undergone previous fertility treatment involving > 5 months treatment with CC or metformin; tubal factor (at least 1 tube blocked); severe male factor (< 15 mil/mL); important medical disorders |
|
| Interventions | Women with BMI > 32 kg/m2 were randomised to receive either metformin 500 mg 3/d (increasing dose over 2 weeks) or matching placebo Women with BMI ≤ 32 kg/m2 were randomised to receive either metformin 500 mg 3/d, CC 50 mg from day 2‐6 (increasing up to 150 mg over 3 months if no evidence of ovulation) or metformin 500 mg 3/d combined with CC 50 mg day 2‐6 (increasing up to 150 mg over 3 months if no evidence of ovulation) Participants received up to 2 packages of 3 months' treatments. All study drugs were stopped once the participant was pregnant |
|
| Outcomes | Primary outcomes were clinical pregnancy (intrauterine gestation sac) and live birth Secondary outcomes were ovulation, miscarriage, ectopic pregnancy or multiple pregnancy |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computerised block randomisation (blocks of 10) |
| Allocation concealment (selection bias) | Low risk | "allocation concealment was strictly maintained by a telephone call from the recruiting nurse to pharmacy, ...dispensing pre‐prepared drugs in a true third party randomisation" |
| Blinding (performance bias and detection bias) All outcomes | Low risk | "Blinding of all parties was maintained in all cases ...until the end of the course of treatment or in the event of pregnancy, until after the pregnancy" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ITT analysis planned and protocol breach and losses to follow‐up were reported in figure 3 |
| Selective reporting (reporting bias) | Low risk | Protocol published and all outcomes reported |
| Other bias | Unclear risk | Inadequate information |
Rautio 2006.
| Methods | RCT Setting: Finland Method of randomisation: computer‐generated random numbers (block of 5). Randomisation was conducted within the department.* Blinding: double* Number randomised: 30 |
|
| Participants | Summary: obese PCOS Inclusion criteria: PCOS was defined according to the Rotterdam consensus 2003. PCO on USS. Oligomenorrhoea or amenorrhoea, clinical (Ferriman‐Gallwey score > 7) or biochemical (testosterone > 2.7 nmol/L) hyperandrogenism, BMI>25 Exclusion criteria: diabetes, abnormal liver function tests, smokers, history of alcohol abuse, hormonal drugs or drugs known to affect lipid metabolism Baseline characteristics of each group:
Dropouts: 3 (20%) in the rosiglitazone group (2 due to pregnancy); 1 (6.6%) in the placebo group (personal reasons) |
|
| Interventions | Main intervention: rosiglitazone 4 mg for 2 weeks followed by 4 mg twice daily for 4 months or placebo Duration: 4 months Co‐interventions: none |
|
| Outcomes | Anthropometric: BMI, WHR* Hormones: testosterone, SHBG, androstenedione, DHEAS Metabolic markers: insulin, glucose, AUC insulin, AUC glucose*, fasting C‐peptide, insulin resistance measured by euglycaemic hyperinsulinaemic clamp test Others: hirsutism, menstrual pattern |
|
| Notes | The objective of this study was to assess the effects of rosiglitazone in obese women with PCOS. All the participants were recruited from a single endocrine clinic. All the participants were advised to use some form of non‐hormonal contraception during the study as rosiglitazone is a category C drug. Rosiglitazone improves menstrual cyclicity, insulin resistance and hyperandrogenism. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers (block of 5) |
| Allocation concealment (selection bias) | Unclear risk | Randomisation was conducted within the department. Unclear concealment, carried out by the departmental staff |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts: 3 (20%) in the rosiglitazone group (2 due to pregnancy); 1 (6.6%) in the placebo group (personal reasons) |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Romualdi 2010.
| Methods | RCT Setting: Italy Method of randomisation: block of 10 sealed envelopes containing randomisation codes assigning 5 women to metformin and 5 to placebo group Blinding: double Number randomised: 28 |
|
| Participants | Summary: non‐obese PCOS Inclusion criteria: Rotterdam consensus 2003, normal weight Exclusion criteria: abnormal TFT, LFT Baseline characteristics of each group:
Dropouts: 2 in metformin due to poor compliance; 3 in placebo group (lost to follow‐up) |
|
| Interventions | Main intervention: metformin 500 mg or placebo tablets twice daily Duration: 6 months Co‐interventions: lifestyle modification |
|
| Outcomes | Ovulation: Anthropometric: BMI, WHR Hormones: testosterone, SHBG Metabolic markers: lipid profiles |
|
| Notes | A small RCT investigated the effect of metformin on ovarian US appearance and steroidogenic function in normal‐weight normoinsulinaemic women with PCOS. Only the metabolic data was included in our analysis. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Low risk | Blocks of 10 sealed opaque envelopes containing randomisation codes |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind, placebo‐controlled |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts: 2 in metformin due to poor compliance; 3 in placebo group (lost to follow‐up) |
| Selective reporting (reporting bias) | Low risk | None identified |
| Other bias | Unclear risk | Inadequate information |
Sahin 2004.
| Methods | RCT Setting: Turkey Method of randomisation: not stated* Blinding: not stated* Number randomised: 21 |
|
| Participants | Summary: obese PCOS Inclusion criteria: PCO on USS (≥ 10 cysts 2‐10 mm), oligomenorrhoea (cycle length > 35 d) or amenorrhoea (no menstrual period > 6 months), clinical or biochemical hyperandrogenism (testosterone > 2.7 nmol/L); participants received no medication known to affect pituitary‐ovarian function or carbohydrate metabolism for at least 12 weeks before the study Exclusion criteria: androgen‐secreting tumour, Cushing’s syndrome, thyroid dysfunctions, CAH, hyperprolactinaemia and diabetes Baseline characteristics of each group:
Dropouts: none |
|
| Interventions | Main intervention: metformin 850 mg twice daily. Placebo was not used. Duration: metformin alone or no treatment for 3 months followed by combining CC ovulation‐induction therapy for further 6 cycles or until pregnancy occurred. Co‐interventions: CC 100 mg daily for 5 d from day 5 of the cycle. Ovulation was triggered by administration of 10,000 IU hCG (Pregnyl, Organon, Holland) |
|
| Outcomes | Ovulation: progesterone > 5.0 ng/mL Anthropometric: BMI Hormones: testosterone, free testosterone, androstenedione, SHBG, DHEAS, estradiol, prolactin Metabolic markers: insulin, glucose, AUC insulin, AUC glucose Others: pregnancy, live birth, miscarriage |
|
| Notes | Women were recruited from a single infertility unit. All participants presented with primary infertility. Tubal disease and male‐factor infertility were excluded. Of the women, 90% presented with oligomenorrhoea and 10% amenorrhoea. In addition, half of the participants had Ferriman‐Gallwey score > 8. Since placebo was not used in the study, bias may exist in the trial period. We are still waiting for a reply from the study author regarding the method of randomisation and concealment. Furthermore, all the anthropometric, hormonal and metabolic data were presented in a format of median and range, which we cannot enter in the meta‐analysis. Hence, we asked the study author to provide the results in mean and standard deviation. Ovulation rates after the initial 3 months metformin treatment alone were not given. The response to CC treatment was monitored by serial USS. When there were < 4 follicles with diameter > 15 mm with a leading follicle of > 18 mm in diameter, 10,000 IU hCG was administrated intramuscularly. Pregnancy was defined by US evidence of a gestational sac and the presence of fetal heart activity. In this most recent update, we have calculated ovulation rate per woman. In the paper, values are given as number of participants and percentage ovulation/cycle. These data have been used to infer the ovulation rate per person. *No reply from the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Inadequate information |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to assess |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Insufficient information to assess |
Siebert 2009.
| Methods | RCT Setting: South Africa Method of randomisation: computer‐generated random numbers Blinding: unblinded Number randomised: 107 |
|
| Participants | Summary: obese PCOS Inclusion criteria: PCOS (according to Rotterdam consensus 2003), confirmed tubal patency Exclusion criteria: male factor subfertility Baseline characteristics of each group:
Dropouts: no significant different in the dropout rates, 10 in metformin + CC group and 7 in CC‐only group |
|
| Interventions | Main intervention: metformin 850 mg twice daily Duration: 6 weeks before and throughout ovulation induction with CC Co‐interventions: CC 50‐150 mg day 4‐8 for 4 cycles + lifestyle modification |
|
| Outcomes | Ovulation: day 21 progesterone level (level not stated) | |
| Notes | A single‐centre RCT investigated the benefit of using metformin in CC ovulation induction treatment. ITT was used in our analysis. Participant lost to follow‐up classified as non‐responder; whilst pregnant participants did not attend follow‐up visit (one in each arm) were classified as responder | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts: no significant difference in the dropout rates, 10 in metformin + CC group and 7 in CC‐only group |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Sturrock 2002.
| Methods | Cross‐over RCT Setting: UK Method of randomisation: performed by pharmacy* Blinding: double‐blind Number randomised: 19 |
|
| Participants | Summary: obese PCOS, CC resistance Inclusion criteria: oligomenorrhoea cycle > 40 d for 6 months, anovulation demonstrated by day 20‐22 progesterone ≤ 10 nmol/L, lack of response to CC 100 mg for 5 d with US showing endometrial thickness ≤ 5 mm and no ovarian follicle ≥ 14 mm. Age 18‐40 years Exclusion criteria: raised prolactin, adrenal hyperplasia, thyroid dysfunction, medication known to affect insulin action* Baseline characteristics of each group*:
Dropouts: 4 (40%) from metformin arm and 4 (44%) from placebo arm*. Not included in analysis |
|
| Interventions | Main intervention: 1 of metformin 500 mg 3/d, placebo Duration: 6 months Co‐interventions: 1st week of treatment at 500 mg 1/d, 2nd at 500 mg 2/d and 3rd at 500 mg 3/d. Those that did not ovulate after 3 months had CC 50 mg days 2‐6, increased to 100 mg for a total of 3 cycles |
|
| Outcomes | Ovulation: by monthly serum progesterone (> 10 nmol/L) and presence of follicle ≥ 14 mm on ovarian US* Anthropometric: weight, BMI, WHR Reproductive hormones: total testosterone, FAI, SHBG Metabolic markers: fasting glucose, fasting insulin, insulin resistance, beta‐cell function, systolic BP, diastolic BP Others: pregnancy, menstrual cycle, Ferriman‐Gallwey score |
|
| Notes | This was designed as a cross‐over trial, with 6 months in the treatment/placebo arm followed by a 1‐month washout and then a 3‐month cross‐over. In this review, we only considered the first phase. The inclusion criteria were simply for CC‐resistant anovulation and not specifically PCOS. However only 2 women did not have US criteria of PCOS, and 75% had a raised FAI* In this review, only those participants who had a raised FAI were included in the analysis* *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Performed by pharmacy |
| Allocation concealment (selection bias) | Unclear risk | Performed by pharmacy |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropouts: 4 (40%) from metformin arm and 4 (44%) from placebo arm*. Not included in analysis |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Tang 2006.
| Methods | Multicentre RCT Setting: UK Method of randomisation: randomisation was performed by the research pharmacy department centrally. Using a random table, a block of 4 randomisation technique was employed in the study. Medications were supplied centrally from the research pharmacy department. The code was kept in the pharmacy department until the end of the trial period. Blinding: double Number randomised: 143 |
|
| Participants | Summary: obese PCOS Inclusion criteria: PCO on USS (> 10 cysts 2‐8 mm in diameter), oligomenorrhoea (cycle length > 35 d) or amenorrhoea (no period in 6 months) Age between 18‐39 years BMI > 30 Normal semen analysis and the participant should have at least 1 proven patent fallopian tube Exclusion criteria: concurrent hormone therapy within previous 6 weeks, metabolic or chronic disease, renal or liver disease, diabetes, CAH, androgen‐secreting tumour Baseline characteristics of each group:
Dropouts: 11 (15.9%) in the metformin arm, 6 (8.1%). The difference was not significant. |
|
| Interventions | Main intervention: metformin 850 mg or placebo tablet once twice daily Duration: 6 months Co‐interventions: lifestyle modification (combination of diet and exercise) aiming to reduce 500 kcal/d |
|
| Outcomes | Anthropometric: BMI, weight, WHR, BP Hormones: total testosterone, SHBG Metabolic markers: insulin, glucose, total cholesterol, triglyceride Others: menstrual pattern, pregnancy |
|
| Notes | A large multicentre randomised placebo controlled study was conducted to investigate the combined effects of the lifestyle modification and the use of metformin in obese women with PCOS (BMI > 30). A total of 8 centres in UK took part in the recruitment. All the participants were recruited from the infertility clinics. The ethnic origin of the participants was not recorded. Both the metformin and the placebo groups experienced improvement in weight loss and in menstrual pattern. However, the differences between the 2 groups were not significant. Participants in the metformin arm showed a greater reduction in total testosterone levels compared with women in the placebo arm. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The randomisation was performed by the research pharmacy department centrally. Using a random table, a block of 4 randomisation technique was employed in the study |
| Allocation concealment (selection bias) | Low risk | Medications were supplied centrally from the research pharmacy department. The code was kept in the pharmacy department until the end of the trial period |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropouts: 11 (15.9%) in the metformin arm, 6 (8.1%). The difference was not significant. Details of the dropout participants were not mentioned |
| Selective reporting (reporting bias) | Low risk | Primary outcome measure (menstrual frequency) and secondary outcome measures (metabolic parameters) were reported |
| Other bias | Unclear risk | Inadequate information |
Trolle 2007.
| Methods | Cross‐over RCT Setting: Denmark Method of randomisation: random number table Blinding: double Number randomised: 60 |
|
| Participants | Summary: obese PCOS Inclusion criteria: Rotterdam criteria, age between 18‐45 years Exclusion criteria: elevated serum gonadotrophins levels, hyperprolactinaemia, diabetes, abnormal thyroid, renal or liver functions, pregnancy, a wish for fertility treatment Baseline characteristics of each group:
Dropouts: 2 in each group |
|
| Interventions | Main intervention: metformin 850 mg or placebo twice daily Duration: 6 months Co‐interventions: no |
|
| Outcomes | Anthropometric: weight, systolic BP* Hormones: testosterone* Metabolic markers: insulin, glucose, HDL* |
|
| Notes | This was a single‐centre randomised, double blinded, placebo controlled cross‐over study to assess the effects of metformin on menstrual frequency and metabolic parameters. Women were randomised to receive either metformin or placebo tablets for 6 months. After a 3‐month wash‐out period, the women received the alternate treatment. Women who wished for fertility treatment were excluded. *Information that was not in the original article kindly provided by the study author. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number table |
| Allocation concealment (selection bias) | Unclear risk | The randomisation code stored in a closed envelope until the end of recruitment. Identical trial drug and placebo tablet |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2 dropouts in each group. Similar dropout rates. Baseline characteristics were comparable between the dropout and the completed groups |
| Selective reporting (reporting bias) | Low risk | A clear study protocol. Power calculation reported. Primary outcome (menstrual frequency) reported |
| Other bias | High risk | Initial power calculation indicated minimum of 50 participants in the trial. However, due to an increased dropout rate, the number of recruitment subsequently increased to 60. |
Vandermolen 2001.
| Methods | Multicentre RCT Setting: USA Method of randomisation: computer generation in blocks of 6 Blinding: double‐blind Number randomised: 27 |
|
| Participants | Summary: obese PCOS, CC resistance Inclusion criteria: PCOS (oligomenorrhoea < 6 cycles/year, anovulation with CC 150 mg for 5 d confirmed by progesterone < 4 ng/mL or amenorrhoea by day 35, hyperandrogaenemia (elevated androstenedione, free testosterone or total testosterone)* or hirsutism, exclusion of other endocrinopathy, US findings of PCO; age 18‐35; normal semen analysis; tubal patency if previous pelvic surgery or infection Exclusion criteria: diabetes mellitus, adrenal hyperplasia, thyroid dysfunction, hyperprolactinaemia, abnormal renal or liver function, medication known to affect insulin action* Baseline characteristics of each group:
Dropouts: 1 from each arm (7%); 1 in the placebo arm ovulated in response to CC but was excluded owing to non‐compliance. Not included in analysis |
|
| Interventions | Main intervention: 1 of metformin 500 mg 3/d, placebo Duration: 7 weeks initially, then those who did not ovulate continued for a further 6 cycles Co‐interventions: those that did not ovulate after 7 weeks had CC 50 mg for 5 d. If ovulation did not occur the dose was increased to 100 mg then 150 mg for a total of 6 cycles No change in usual eating habits, physical activity or lifestyle |
|
| Outcomes | Ovulation: serum progesterone ≥ 12.7 nmol/L on days 10, 20, 30 and 40 (and days 21 and 28 of subsequent cycles if received CC) Anthropometric: weight, BMI Reproductive Hormones: total testosterone, free testosterone, androstenedione, DHEAS, SHBG, estradiol, FSH, LH, 17‐alpha hydroxyprogesterone Metabolic markers: fasting glucose, fasting insulin, AUC of insulin and glucose during GTT Others: live birth, pregnancy |
|
| Notes | Although obesity was not an inclusion criteria, the mean BMI was high in this study although similar in both arms. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generation in blocks of 6 |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropouts: 1 from each arm (7%); 1 in the placebo arm ovulated in response to CC but was excluded owing to non‐compliance. Not included in analysis. Details not provided |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Williams 2009.
| Methods | RCT Setting: USA Method of randomisation: not stated Blinding: double‐blind Number randomised: 55 |
|
| Participants | Summary: PCOS Inclusion criteria: not stated. Unknown BMI and age Exclusion criteria: unknown Baseline characteristics of each group: not stated Dropouts: not stated 26 women underwent 99 blinded treatment cycles whilst 29 women underwent 88 blinded treatment cycles |
|
| Interventions | Main intervention: metformin 500 mg or placebo 3/d Duration: 6 cycles Co‐interventions: CC (dose unclear) |
|
| Outcomes | Ovulation Pregnancy |
|
| Notes | A conference abstract presented in 57th Annual Meeting of The Pacific Coast Reproductive Society 2009. No reply from study author regarding the detail of the study |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Inadequate information |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Inadequate information |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Yarali 2002.
| Methods | RCT Setting: Turkey Method of randomisation: computer‐generated numbers. Centralised randomisation process* Blinding: double‐blind Number randomised: 32 |
|
| Participants | Summary: non‐obese PCOS, CC resistance Inclusion criteria: PCOS (oligomenorrhoea < 6 cycles/year, anovulation confirmed with progesterone < 5 ng/mL, testosterone > 2.4 nmol/L, exclusion of other endocrinopathy, US findings of PCO, CC resistance to 250 mg for 5 d for up to 6 months, normal semen analysis, normal HSG or laparoscopy within 6 months Exclusion criteria: diabetes mellitus, adrenal hyperplasia, Cushing's syndrome, thyroid dysfunction, hyperprolactinaemia, medication known to alter insulin action, previous gonadotrophin treatment, infertility other than that caused by PCOS, previous pelvic surgery Baseline characteristics of each group:
Dropouts: 2 (6%) from the metformin/placebo part of the trial owing to pregnancy. They were excluded from analysis |
|
| Interventions | Main intervention: 1 of metformin 850 mg 2/d, placebo Duration: 6 weeks initially, then those who did not ovulate continued for1 cycle Co‐interventions: those that did not ovulate after 6 weeks had recombinant FSH in a low‐dose, step‐up protocol No change in usual eating habits |
|
| Outcomes | Ovulation: serum progesterone > 15.9 nmol/L weekly Anthropometric: BMI, WHR Reproductive hormones: total testosterone, free testosterone, androstenedione, DHEAS, estradiol, FSH, LH, 17‐alpha hydroxyprogesterone Metabolic markers: fasting insulin, AUC insulin and glucose during GTT, insulin sensitivity, leptin, Others: live birth, adverse events, pregnancy, duration of rFSH stimulation, total dose of FSH, oestradiol on day of hCG, monofollicular development cycle cancellation rate |
|
| Notes | Free testosterone was significantly higher in the metformin group. Fasting insulin was non‐significantly higher with a wide SD compared with placebo. *Information not in the original paper kindly provided by the study author |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated numbers. Centralised randomisation process* |
| Allocation concealment (selection bias) | Unclear risk | Inadequate information |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Inadequate information |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts: 2 (6%) from the metformin/placebo part of the trial owing to pregnancy. They were excluded from analysis |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Insufficient information |
Zain 2009.
| Methods | RCT Setting: Malaysia Method of randomisation: picking a card out of a box Blinding: no Number randomised: 124 |
|
| Participants | Summary: obese PCOS Inclusion criteria: newly diagnosed with PCOS (Rotterdam criteria), age < 40 years Exclusion criteria: diabetes, hepatic or renal dysfunction, heart disease, abnormal semen analysis (WHO criteria) Baseline characteristics of each group:
Dropouts: 4 (9.5%) in the metformin group, 2 (4.9%) in the CC group and 3 (7.3%) in the combined metformin and CC group |
|
| Interventions | Main intervention: metformin 1500 mg/d Duration: 6 months Co‐interventions: CC 50 mg from day 2‐6 of the cycle. If women did not respond to the treatment, the dose increased by 50 mg to a maximum dose of 200 mg All the women were offered dietary advice. |
|
| Outcomes | Ovulation: USS follicular tracking Hormones: testosterone Others: live birth, pregnancy, miscarriage |
|
| Notes | This study was designed to compare the live birth rates in women who received CC, metformin and combined CC and metformin treatments. Placebo tablets were not used in this unblinded RCT. Therefore, potential bias may be introduced. Most women were Malay (about 90%) Analysis was based on analysis per protocol, not ITT |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Picking a card out of a box |
| Allocation concealment (selection bias) | Unclear risk | Picking a card out of a box |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropouts: 4 (9.5%) in the metformin group, 2 (4.9%) in the CC group and 3 (7.3%) in the combined metformin and CC group. Analysis was based on analysis per protocol, not ITT |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information in the study |
| Other bias | Unclear risk | Inadequate information |
Baseline characteristics given in order of main intervention (drug, placebo).
Where the trial protocol included a statement such as, "all patients had ultrasound features of PCOS" then this has been included as an inclusion criteria (unless the authors specifically state that it was not in which case it is recorded under notes).
Abbreviations Table 4:
ACTH: AUC: area under the curve BMI: body mass index BP: blood pressure CAH: CC: clomiphene citrate CI: confidence interval CT: computerised tomography scan DHEAS: dehydroepiandrosterone sulphate FAI: free androgen index FSH: follicle stimulating hormone GTT: glucose tolerance test HbA1C: glycosylated haemoglobin HDL: high density lipoprotein cholesterol IGFBP‐1: insulin growth factor binding protein 1 ITT: intention‐to‐treat LDL: low density lipoprotein cholesterol LFT: LH: luteinising hormone OGTT: RCT: randomised controlled trial rFSH: recombinant follicle stimulating hormone PCOS: polycystic ovary syndrome PID: SD: standard deviation SE: standard error of the mean SHBG: sex hormone‐binding globulin TFT: thyroid function test TSH: US(S): ultrasound (scan) VLDL: very low density lipoprotein cholesterol WHO: World Health Organization WHR: waist:hip ratio
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abuelghar 2013 | Human chorionic gonadotrophin hormone was used an an ovulation trigger, which may have added additional heterogeneity to the results. Reasons for losses to follow up not given. Not intention to treat analysis |
| Aroda 2009 | The aim of the study was to evaluate the effects of pioglitazone on insulin action and ovarian androgen production in women with PCOS. This was a randomised, placebo‐controlled trial but the details of randomisation were not provided. Furthermore, the recruited participants did not have history of subfertility |
| Azziz 2001 | Randomised, double‐blind study comparing troglitazone (150 mg, 300 mg, 600 mg daily) with placebo. Randomisation method was unclear and no reply from the study author. Troglitazone has been withdrawn from the market due to risk of hepatic damage |
| Azziz 2003 | Randomised, double‐blind study comparing troglitazone (150 mg, 300 mg, 600 mg daily) with placebo. Randomisation method was unclear and no reply from the study author. Troglitazone has been withdrawn from the market due to risk of hepatic damage. |
| Chaudhry 2016 | This study compared 2 insulin‐sensitising agents, which does not meet the inclusion criteria for this review |
| Chaudhury 2008 | This study compared the efficacy of metformin with folic acid |
| Constantino 2009 | This study compared the efficacy of metformin with folic acid |
| Crave 1995 | Randomised, double‐blind trial comparing metformin 850 mg 2/d with placebo Participants were women with hirsutism and obesity but not necessarily anovulation. 67% had regular menses. 63% had polycystic ovaries on US. The results indicated that weight loss induced by a hypocalorific diet led to improvements in insulin and androgen levels, but that metformin gave no additional benefit over diet |
| Curi 2012 | The aim of this study was to ascertain the effects of metformin on ovarian function. The outcomes of this review, such as ovulation rate, pregnancy or live birth rate were not measured as contraception was advised during the study |
| De Leo 1999 | Randomised trial in women with CC‐resistant PCOS having 75 IU FSH for ovulation induction, comparing pre‐treatment with metformin 500 mg 3/d with no metformin pre‐treatment. The aims and outcome measures were different from the other included trials (main outcome measures were number of FSH ampoules, days of treatment and markers of ovarian hyperstimulation). The trial reported treatment cycles rather than participants, and combined the results of each group in a cross‐over type analysis. Therefore the data were not suitable for inclusion in this meta‐analysis |
| Dunaif 1996 | Randomised double blind trial in women with PCOS comparing troglitazone 200mg and troglitazone 400mg daily. This trial only randomised for dose of troglitazone, and did not have a placebo or no treatment arm |
| Elter 2002 | Randomised trial in non‐obese women with PCOS comparing metformin and the combined oral contraceptive (ethinyl estradiol/cyproterone acetate) with the combined contraceptive alone. This trial did not compare metformin with placebo, no treatment or an ovulation‐induction agent |
| Farzadi 2006 | In this study, the efficacy of metformin was compared with vitamin B, and we were unable to contact the study author |
| Heathcote 2013 | No record of this publication |
| Hou 2000 | Non‐English‐language trial in women with CC resistant PCOS, comparing metformin with the Chinese herbal formula tiangui fang. The paper makes no mention of randomisation and has therefore been classified as a controlled clinical trial. Ovulation was assessed by menstrual cyclicity and basal body temperature change but not by a biochemical method. This trial did not have a placebo or no‐treatment arm, and the only significant result reported was a reduction in testosterone and BMI in the tiangui fang arm compared with baseline |
| Ibanez 2002 | Randomised trial in lean, young women with anovulation, hyperinsulinaemia, and hyperandrogaenemia. It had 3 arms: metformin only, flutamide only and metformin and flutamide together. This trial was not included because it had no placebo arm, and the anti‐androgen flutamide is not an ovulation‐induction agent |
| Kazerooni 2009 | This study evaluated the effect of short‐course pretreatment with metformin on hyperandrogenism, insulin resistance, cervical scores and pregnancy rates in women with CC‐resistant PCOS Apart from receiving CC treatment, all participants received 10,000 U of hCG injection to stimulate ovulation followed by timed intercourse. Hence, all women received 2 ovulation‐induction agents per cycle of treatment. Therefore, it would not be appropriate to combine these subjects in the current review as all the included trial participants only received 1 type of ovulation‐induction agent with or without metformin |
| Kelly 2002 | This study was published in 2002. The objective was to ascertain the effect of metformin on hirsutism in women with PCOS. This outcome measure has been removed in the update review |
| Kocak 2002 | Quasi‐randomised trial comparing combined CC and metformin with CC on ovulation in CC‐resistant women with PCOS. Inadequate randomisation and sequence generation (sequential by order of admission). Admission determined by day of menses. Allocation performed by nurse blinded to the study. Odd numbers allocated metformin, even numbers allocated placebo |
| Ladson 2011 | In this RCT women were advised to avoid pregnancy, so the outcomes of interest in the review were not investigated |
| Leanza 2014 | Patients in this study underwent intrauterine insemination and assisted reproduction is an exclusion criteria for this review. Aspects of the methodology are missing from the article |
| Mantzoros 1997 | Randomised, double‐blind study in women with PCOS comparing troglitazone 200 mg and troglitazone 400 mg daily. This trial only randomised for dose of troglitazone, and did not have a placebo or no‐treatment arm |
| Morin‐Papunen 2000 | Randomised trial in obese women with PCOS comparing metformin 500 mg 2/d and 1 g 2/d with combined oral contraceptive (ethinyl estradiol/cyproterone acetate). This trial was not blinded and did not compare metformin with placebo, no treatment or an ovulation‐induction agent |
| Morin‐Papunen 2010 | Conference abstract. Not enough information to separate the data for analysis. Data from a published paper by the same author is included in the 3rd update of this review |
| Nestler 1996 | This study investigated whether hyperinsulinaemia stimulates ovarian cytochrome P450c17α activity in women with PCOS. Some of the participants were not infertile |
| Nestler 1997 | Partially randomised trial in lean women with PCOS comparing metformin 500 mg 3/d with placebo. The method of randomisation was initially by pulling pieces out of a hat, but then continued as an observational study. The trial was initially single‐blind, with the patient blinded The published data included both randomised and non‐randomised participants, and an analysis to include only the randomised participants was not possible |
| Palomba 2011 | Participants in this study underwent assisted conception using IVF |
| Papaleo 2009 | This study investigated the effect of insulin sensitisers on oocyte quality in IVF cycles, and therefore does not meet the inclusion criteria for this review |
| Ramzy 2003 | An open‐labelled, randomised trial comparing metformin 500 mg 3/d with placebo 6 weeks prior to CC treatment. In addition, randomisation was performed using alternate numbers. These factors introduced significant bias. |
| Refaie 2005 | Attempts to contact study author for more information unsuccessful |
| Rouzi 2006 | Randomised trial comparing CC and metformin with CC 1.5 g and rosiglitazone 4 mg in CC‐resistant women with PCOS. This trial did not compare metformin/CC with CC/placebo |
| Salman 2014 | This was a conference abstract only, with not enough detail to warrant inclusion. Literature search found no subsequent publication |
| Santonocito 2009 | The objective of this study was to compare CC with metformin on ovulation rates. However, all participants also received 2000 U of hCG injection once follicular diameter > 15 mm on USS |
| Shobokshi 2003 | The objective of this study was to compare the effects of combined rosiglitazone and CC with CC monotherapy. Since placebo was not employed in the trial, both the clinician and participants were not blinded. Therefore, bias may exist in this study. It was unclear whether the study was randomised. We are currently still waiting for a response from the study author |
| Unfer 2011 | This study investigated the effect of insulin sensitisers on oocyte quality in IVF cycles, and therefore does not meet the inclusion criteria for this review |
CC: clomiphene citrate; FSH: follicle‐stimulating hormone; IVF: in vitro fertilisation; PCOS: polycystic ovary syndrome; RCT: randomised controlled trial; US(S): ultrasound (scan)
Differences between protocol and review
Changes in 2009 update
In the 2009 update of this review, the title was changed from 'Insulin‐sensitising drugs (metformin, rosiglitazone, pioglitazone, D‐chiro‐inositol) for polycystic ovary syndrome' to 'Insulin‐sensitising drugs (metformin, rosiglitazone, pioglitazone, D‐chiro‐inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility'.
The outcome measures were restructured. One new comparison was added (metformin versus clomiphene citrate).
Studies using troglitazone were excluded.
Changes in 2017 update
Unit of analysis
We added a note to the Methods section to clarify that miscarriage and multiple pregnancy data were analysed 'per woman' and added a sensitivity analysis to check the effect of analysing these outcomes 'per pregnancy'. In addition we restricted analysis of ovulation rates to per‐woman data and reported per‐cycle data in an additional table.
'Summary of findings' table
We added more detail in the Methods section to state which comparisons and outcomes would be included in the 'Summary of findings' table. We decided to include only the three most important clinical comparisons. For one comparison (metformin versus clomiphene citrate), there was high heterogeneity for some outcomes which was associated with BMI status, so for this comparison we decided as a post hoc measure to present the data by BMI subgroup.
Contributions of authors
LCM: literature search, assessment of trials, data collection, revising and preparing the review (2017 version) TT: checking the literature search, secondary assessment of trials and data analysis in the updated review (May 2008 to January 2017). Preparation of the previous reviews (2009 and 2012 versions) EY: checking the literature search and secondary assessment of trials (2009, 2012 and 2017 versions) RN: read, commented on and approved the draft review (2009, 2012 and 2017 versions) AB: secondary assessment of trials and quality analysis. Revising and finalising the review (2009, 2012 and 2017 versions)
Sources of support
Internal sources
Peninsula Medical School, UK.
University of Adelaide, Australia.
Leeds Centre of Reproductive Medicine, Leeds, UK.
External sources
No sources of support supplied
Declarations of interest
LCM: none known TT: received consultancy fee from Finox Biotech for advisory board meeting in 2016; Finox do not manufacture insulin sensitisers. EY: received travel costs and meeting expenses to attend Ferring advisory board in 2017; Ferring do not manufacture insulin sensitisers. RN: received consultancy fee from Ferring for advisory board meeting; Ferring do not manufacture insulin sensitisers. AB: NHS Consultant in Reproductive Medicine and clinical lead for the Leeds Centre for Reproductive Medicine, which performs all fertility treatments funded by the NHS; partner in Genesis LLP, the private arm on the Leeds Centre for Reproductive Medicine, which performs all self‐funded fertility treatments using identical protocols to the NHS; Chair, Clinical Board, IVI, UK; Chair, British Fertility Society; Chair, NHS England IVF Pricing Development Expert Advisory Group; Chair, World Health Organization Expert Working Group on Global Infertility Guidelines, Management of PCOS; consultant for ad hoc advisory boards for Ferring Pharmaceuticals, Astra Zeneca, Merck Serono, IBSA, Clear Blue, Gideon Richter, Uteron Pharma & former member of ethics committee for OvaScience. Merck manufacture some products containing metformin.
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Ayaz 2013 {published data only}
- Ayaz A, Alwan Y, Farooq MU. Efficacy of combined metformin‐clomiphene citrate in comparison with clomiphene citrate alone in infertile women with polycystic ovarian syndrome (PCOS). Journal of Medicine and Life 2013;6:199‐201. [PMC free article] [PubMed] [Google Scholar]
- Ayaz A, Alwan Y, Farooq MU. Metformin‐clomiphene citrate vs. clomiphene citrate alone: polycystic ovarian syndrome. Journal of Human Reproductive Sciences 2013;6:15‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Baillargeon 2004 {published data only}
- Baillargeon JP, Jakubowicz DJ, Iuorno MJ, Jakubowicz S, Nestler JE. Effects of metformin and rosiglitazone, alone and in combination, in nonobese women with polycystic ovary syndrome and normal indices of insulin sensitivity. Fertility and Sterility 2004;82:893‐902. [DOI] [PubMed] [Google Scholar]
Begum 2014 {published data only}
- Begum H, Chowdhury TA, Begum F, Begum SN, Kabir N, Haque MDA. Effect of metformin and clomiphene citrate in improving fertility in subfertility women with polycystic ovary syndrome: a randomised controlled trial. Bangladesh Journal of Obstetrics and Gynaecology 2014;29:15‐20. [Google Scholar]
Ben Ayed 2009 {published data only}
- Ben Ayed B, Dammak Dit Mlik S, Ben Arab H, Trabelssi H, Chahtour H, Mathlouthi N. Metformin effects on clomifene‐induced ovulation in the polycystic ovary syndrome. Tunisie Medicale 2009;87(1):43‐8. [PubMed] [Google Scholar]
Boudhraa 2010 {published data only}
- Boudhrâa K, Jellouli MA, Amri M, Farhat M, Torkhani F, Gara MF. Indication of metformin in the management of hormonal dysfunction secondary to polycystic ovarian syndrome: prospective comparative study of 63 cases. [La metformine dans la prise en charge de l'infertilite du SOPK hors FIV etude prospective comparative a propos de 63 cas]. Tunisie Medicale 2010;88(5):335‐40. [PubMed] [Google Scholar]
Brettenthaler 2004 {published data only}
- Aigner E, Bachofner N, Klein K, Geyter C, Hohla F, Patsch W, et al. Retinol‐binding protein 4 in polycystic ovary syndrome‐‐association with steroid hormones and response to pioglitazone treatment. Journal of Clinical Endocrinology and Metabolism 2009;94(4):1229‐35. [DOI] [PubMed] [Google Scholar]
- Brettenthaler N, Geyter C, Huber PR, Keller U. Effect of the insulin sensitizer pioglitazone on insulin resistance, hyperandrogenism, and ovulatory dysfunction in women with polycystic ovary syndrome. Journal of Clinical Epidemiology 2004;89:3835‐40. [DOI] [PubMed] [Google Scholar]
Carmina 2004 {published data only}
- Carmina E, Lobo RA. Does metformin induce ovulation in normoandrogenic anovulatory women?. American Journal of Obstetrics and Gynecology 2004;191:1580‐4. [DOI] [PubMed] [Google Scholar]
Chou 2003 {published data only}
- Chou KH, Eye Corleta H, Capp E, Spritzer PM. Clinical, metabolic and endocrine parameters in response to metformin in obese women with polycystic ovary syndrome: a randomized, double‐blind and placebo‐controlled trial. Hormone and Metabolic Research 2003;35:86‐91. [DOI] [PubMed] [Google Scholar]
Eisenhardt 2006 {published data only}
- Eisenhardt S, Schwarzmann N, Henschel V, Germeyer A, Wolff M, Hamann A, et al. Early effects of metformin in women with polycystic ovary syndrome: a prospective randomized, double‐blind, placebo‐controlled trial. Journal of Clinical Endocrinology and Metabolism 2006;91:946‐52. [DOI] [PubMed] [Google Scholar]
El‐Biely 2001 {published data only}
- El‐Biely MM, Habba M. The use of metformin to augment the induction of ovulation in obese infertile patients with polycystic ovary syndrome. Middle East Fertility Society Journal 2001;6(1):43‐9. [Google Scholar]
Fleming 2002 {published data only}
- Fleming R, Hopkinson ZE, Wallace AM, Greer IA, Sattar N. Ovarian function and metabolic factors in women with oligomenorrhea treated with metformin in a randomized double blind placebo‐controlled trial. Journal of Clinical Endocrinology and Metabolism 2002;87(2):569‐74. [DOI] [PubMed] [Google Scholar]
- Fleming R, Hopkinson ZE, Wallace E, Greer IA, Sattar N. Metformin treatment improves ovulation frequency in women with oligomenorrhoea: a randomized, double blind placebo trial. Human Fertility 2000; Vol. 3, issue 4:389‐90.
Gerli 2003 {published data only}
- Gerli S, Mignosa M, Renzo GC. Effects of inositol on ovarian function and metabolic factors in women with PCOS: a randomized double blind placebo‐controlled trial. European Review for Medical and Pharmacological Sciences 2003;7:151‐9. [Original article] [PubMed] [Google Scholar]
- Gerli S, Papaleo E, Ferrari A, Renzo GC. Randomized, double blind placebo‐controlled trial: effects of myo‐inositol on ovarian function and metabolic factors in women with PCOS. European Review for Medical and Pharmacological Sciences 2007;11(5):347‐54. [PubMed] [Google Scholar]
Glintborg 2005 {published data only}
- Glintborg D, Frystyk J, Hojlund K, Andersen KK, Henriksen JE, Hermann A, et al. Total and high molecular weight (HMW) adiponectin levels and measures of glucose and lipid metabolism following pioglitazone treatment in a randomized placebo‐controlled study in polycystic ovary syndrome. Clinical Endocrinology (Oxford) 2008;68(2):165‐74. [DOI] [PubMed] [Google Scholar]
- Glintborg D, Hermann AP, Andersen M, Hagen C, Beck‐Nielsen H, Veldhuis JD, et al. Effect of pioglitazone on glucose metabolism and luteinizing hormone secretion in women with polycystic ovary syndrome. Fertility and Sterility 2006;86:385‐97. [DOI] [PubMed] [Google Scholar]
- Glintborg D, Hojlund K, Andersen M, Henriksen JE, Beck‐Nielsen H, Handberg A. Soluble CD36 and risk markers of insulin resistance and atherosclerosis are elevated in polycystic ovary syndrome and significantly reduced during pioglitazone treatment. Diabetes Care 2008;31:328‐34. [DOI] [PubMed] [Google Scholar]
- Glintborg D, Stoving RK, Hagen C, Hermann AP, Frystyk J, Veldhuis JD, et al. Pioglitazone treatment increases spontaneous growth hormone (GH) secretion and stimulated GH levels in polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 2005;90:5605‐12. [original article] [DOI] [PubMed] [Google Scholar]
Hoeger 2004 {published data only}
- Hoeger KM, Kochman L, Wixom N, Craig K, Miller RK, Guzick DS. A randomized, 48‐week, placebo‐controlled trial of intensive lifestyle modification and/or metformin therapy in overweight women with polycystic ovary syndrome: a pilot study. Fertility and Sterility 2004;82:421‐9. [DOI] [PubMed] [Google Scholar]
Hwu 2005 {published data only}
- Hwu YM, Lin SY, Huang WY, Lin MH, Lee RK. Ultra‐short metformin pretreatment for clomiphene citrate‐resistant polycystic ovary syndrome. International Journal of Gynaecology and Obstetrics 2005;90:39‐43. [DOI] [PubMed] [Google Scholar]
Jakubowicz 2001 {published data only}
- Jakubowicz DJ, Seppala M, Jakubowicz S, Rodriguez‐Armas O, Rivas‐Santiago A, Koistinen H, et al. Insulin reduction with metformin increases luteal phase serum glycodelin and insulin‐like growth factor‐binding protein 1 concentrations and enhances uterine vascularity and blood flow in the polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 2001;86(3):1126‐33. [DOI] [PubMed] [Google Scholar]
Kar 2015 {published data only}
- Kar S. Metabolic risks of the lean PCOS woman. Fertility and Sterility ASRM abstracts 2013;100(S359):P‐730. [Google Scholar]
- Kar S, Sanchita S. Clomiphene citrate, metformin or a combination of both as the first line ovulation induction drug for Asian Indian women with polycystic ovarian syndrome: a randomized controlled trial. Journal of Human Reproductive Science 2015;8:197‐201. [DOI] [PMC free article] [PubMed] [Google Scholar]
Karimzadeh 2007 {published data only}
- Karimzadeh M, Tayebi N, Eftekhar M, Sakhavat L, Taheripanah R, Zare F. The effect of administration of metformin on lipid profile changes and insulin resistance in patients with polycystic ovary syndrome. Middle East Fertility Society Journal 2007;12(3):174‐8. [Google Scholar]
Karimzadeh 2010 {published data only}
- Karimzadeh MA, Javedani M. An assessment of lifestyle modification versus medical treatment with clomiphene citrate, metformin, and clomiphene citrate‐metformin in patients with polycystic ovary syndrome. Fertility and Sterility 2010;94(1):216‐20. [DOI] [PubMed] [Google Scholar]
Khorram 2006 {published data only}
- Khorram O, Helliwell JP, Katz S, Bonpane CM, Jaramillo L Khorram O, et al. Two weeks of metformin improves clomiphene citrate‐induced ovulation and metabolic profiles in women with polycystic ovary syndrome. Fertility and Sterility 2006;85:1448‐51. [DOI] [PubMed] [Google Scholar]
Lam 2011 {published data only}
- Lam PM, Tam WH, Ma RC, Cheung LP, Tsui MH, Tong PC, et al. The reproductive and metabolic effect of rosiglitazone on Chinese women with polycystic ovarian syndrome ‐ a double‐blind randomized placebo‐controlled study. Fertility and Sterility 2011;96(2):445‐51. [DOI] [PubMed] [Google Scholar]
Legro 2007 {published data only}
- Cataldo N, Barnhart H, Legro R, Myers E, Schlaff W, Carr B, et al. Extended‐release metformin does not reduce the clomiphene citrate dose required to induce ovulation in polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 2008;93(8):3147‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Legro RS, Barnhart HX, Schlaff WD, Carr BR, Diamond MP, Carson SA, et al. Clomiphene, metformin, or both for infertility in the polycystic ovary syndrome. New England Journal of Medicine 2007;356:551‐66. [original article] [DOI] [PubMed] [Google Scholar]
Lord 2006 {published data only}
- Lord J, Thomas R, Fox B, Acharya U, Wilkin T. The effect of metformin on fat distribution and the metabolic syndrome in women with polycystic ovary syndrome‐‐a randomised, double‐blind, placebo‐controlled trial. British Journal of Obstetrics and Gynaecology 2006;113:817‐24. [DOI] [PubMed] [Google Scholar]
Machado 2012 {published data only}
- Machado RC, Machado NA, Geber S. Evaluation of the use of metformin for ovulation in patients with PCOS resistant to isolated use of clomiphene citrate. Brazilian Journal Assisted Reproduction 2012;16(1):27‐31. [Google Scholar]
Maciel 2004 {published data only}
- Maciel GA, Soares Jr JM, Alves da Motta EL, Abi Haidar M, Lima GR, Baracat EC, et al. Nonobese women with polycystic ovary syndrome respond better than obese women to treatment with metformin. Fertility and Sterility 2004;81:355‐60. [DOI] [PubMed] [Google Scholar]
Malkawi 2002 {published data only}
- Malkawi HY, Qublan HS. The effect of metformin plus clomiphene citrate on ovulation and pregnancy rates in clomiphene‐resistant women with polycystic ovary syndrome. Saudi Medical Journal 2002;23(6):663‐6. [MEDLINE: ] [PubMed] [Google Scholar]
Moghetti 2000 {published data only}
- Moghetti P, Castello R, Negri C, Tosi F, Perrone F, Caputo M, et al. Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycystic ovary syndrome: a randomized, double‐blind, placebo‐controlled 6‐month trial, followed by open, long‐term clinical evaluation. Journal of Clinical Endocrinology and Metabolism 2000;85(1):139‐46. [DOI] [PubMed] [Google Scholar]
Moll 2006 {published data only}
- Moll E, Bossuyt PM, Korevaar JC, Lambalk CB, Veen F. Effect of clomifene citrate plus metformin and clomifene citrate plus placebo on induction of ovulation in women with newly diagnosed polycystic ovary syndrome: randomised double blind clinical trial. BMJ 2006;332:1485. [original article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moll E, Korevaar JC, Bossuyt PM, Veen F. Does adding metformin to clomifene citrate lead to higher pregnancy rates in a subset of women with polycystic ovary syndrome?. Human Reproduction 2008;23(8):1830‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moll E, Wely M, Lambalk CB, Bossuyt PM, Veen F. Health‐related quality of life in women with newly diagnosed polycystic ovary syndrome randomized between clomifene citrate plus metformin or clomifene citrate plus placebo. Human Reproduction 2012;27:3273‐8. [DOI] [PubMed] [Google Scholar]
Morin‐Papunen 2012 {published data only}
- Morin‐Papunen L, Rantala AS, Unkila‐Kallio L, Tiitinen A, Hippeläinen M, Perheentupa A, et al. Metformin improves pregnancy and live‐birth rates in women with polycystic ovary syndrome (PCOS): a multicenter, double‐blind, placebo‐controlled randomized trial. Journal of Clinical Endocrinology and Metabolism 2012;97:1492‐1500. [DOI] [PubMed] [Google Scholar]
Nestler 1998 {published data only}
- Nestler JE, Jakubowicz DJ, Evans WS, Pasquali R. Effects of metformin on spontaneous and clomiphene‐induced ovulation in the polycystic ovary syndrome. New England Journal of Medicine 1998;338(26):1876‐80. [DOI] [PubMed] [Google Scholar]
Nestler 1999 {published data only}
- Nestler JE, Jakubowicz DJ, Reamer P, Gunn RD, Allan G. Ovulatory and metabolic effects of D‐chiro‐inositol in the polycystic ovary syndrome. New England Journal of Medicine 1999;340(17):1314‐20. [DOI] [PubMed] [Google Scholar]
Ng 2001 {published data only}
- Ng EHY, Wat NMS, Ho PC. Effects of metformin on ovulation rate, hormonal and metabolic profiles in women with clomiphene‐resistant polycystic ovaries: a randomized, double‐blinded placebo‐controlled trial. Human Reproduction 2001;16(8):1625‐31. [DOI] [PubMed] [Google Scholar]
Onalan 2005 {published data only}
- Onalan G, Goktolga U, Ceyhan T, Bagis T, Onalan R, Pabuccu R. Predictive value of glucose‐insulin ratio in PCOS and profile of women who will benefit from metformin therapy: obese, lean, hyper or normoinsulinemic?. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2005;123:204‐11. [DOI] [PubMed] [Google Scholar]
Otta 2010 {published data only}
- Otta CF, Wior M, Iraci GS, Kaplan R, Torres D, Gaido MI, et al. Clinical, metabolic, and endocrine parameters in response to metformin and lifestyle intervention in women with polycystic ovary syndrome: a randomized, double‐blind, and placebo control trial. Gynecological Endocrinology 2010;26(3):173‐8. [DOI] [PubMed] [Google Scholar]
Palomba 2005 {published data only}
- Palomba S, Orio F Jr, Falbo A, Manguso F, Russo T, Cascella T, et al. Prospective parallel randomized, double‐blind, double‐dummy controlled clinical trial comparing clomiphene citrate and metformin as the first‐line treatment for ovulation induction in nonobese anovulatory women with polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 2005;90(7):4068‐74. [original article] [DOI] [PubMed] [Google Scholar]
- Palomba S, Orio F Jr, Falbo A, Russo T, Tolino A, Zullo F. Effects of metformin and clomiphene citrate on ovarian vascularity in patients with polycystic ovary syndrome. Fertility and Sterility 2006;86:1694‐701. [DOI] [PubMed] [Google Scholar]
Pasquali 2000 {published data only}
- Casimirri F, Biscotti M, Gambineri A, Calzoni F, Eliana B, Pasquali R. Metformin improves insulin, body fat distribution, and androgens in obese women with and without the polycystic ovary syndrome. International Journal of Obesity 1997;21 Suppl 2:61. [Google Scholar]
- Pasquali R, Gambineri A, Biscotti D, Vicennati V, Gagliardi L, Colitta D, et al. Effect of long‐term treatment with metformin added to hypocaloric diet on body composition, fat distribution, and androgen and insulin levels in abdominally obese women with and without the polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 2000;85(8):2767‐74. [DOI] [PubMed] [Google Scholar]
PCOSMIC 2010 {published data only}
- Johnson NP, Bontekoe S, Stewart AW. Analysis of factors predicting success of metformin and clomiphene treatment for women with infertility owing to PCOS‐related ovulation dysfunction in a randomised controlled trial. Australian & New Zealand Journal of Obstetrics & Gynaecology 2011;51:252‐6. [DOI] [PubMed] [Google Scholar]
- Johnson NP, Stewart AW, Falkiner J, Farquhar CM, Milsom S, Singh V‐P, et al. on behalf of REACT‐NZ (REproduction And Collaborative Trials in New Zealand), a multi‐centre fertility trials group. PCOSMIC: a multi‐centre randomized trial in women with Polycystic Ovary Syndrome evaluating Metformin for Infertility with Clomiphene. Human Reproduction 2010;25(7):1675‐83. [MEDLINE: 10.1093/humrep/deq100] [DOI] [PubMed] [Google Scholar]
Rautio 2006 {published data only}
- Rautio K, Tapanainen JS, Ruokonen A, Morin‐Papunen LC. Endocrine and metabolic effects of rosiglitazone in overweight women with PCOS: a randomized placebo‐controlled study. Human Reproduction 2006;21:1400‐7. [DOI] [PubMed] [Google Scholar]
- Rautio K, Tapanainen JS, Ruokonen A, Morin‐Papunen LC. Rosiglitazone treatment alleviates inflammation and improves liver function in overweight women with polycystic ovary syndrome: a randomized placebo‐controlled study. Fertility and Sterility 2007;87(1):202‐6. [DOI] [PubMed] [Google Scholar]
Romualdi 2010 {published data only}
- Romualdi D, Giuliani M, Cristello F, Fulghesu AM, Selvaggi L, Lanzone A, et al. Metformin effects on ovarian ultrasound appearance and steroidogenic function in normal‐weight normoinsulinemic women with polycystic ovary syndrome: a randomized double‐blind placebo‐controlled clinical trial. Fertility and Sterility 2010;93(7):2303‐10. [DOI] [PubMed] [Google Scholar]
Sahin 2004 {published data only}
- Sahin Y, Yirmibes U, Kelestimur F, Aygen E. The effects of metformin on insulin resistance, clomiphene‐induced ovulation and pregnancy rates in women with polycystic ovary syndrome. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2004;113:214‐20. [DOI] [PubMed] [Google Scholar]
Siebert 2009 {published data only}
- Siebert T, Kruger T, Lombard C. Evaluating the equivalence of clomiphene citrate with and without metformin in ovulation induction in PCOS patients. Journal of Assisted Reproduction and Genetics 2009;26(4):165‐71. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sturrock 2002 {published data only}
- Sturrock NDC, Lannon B, Fay TN. Metformin does not enhance ovulation induction in clomiphene resistant polycystic ovary syndrome in clinical practice. British Journal of Clinical Pharmacology 2002;53(5):469‐73. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tang 2006 {published data only}
- Tang T, Glanville J, Hayden CJ, White D, Barth JH, Balen AH. Combined lifestyle modification and metformin in obese patients with polycystic ovary syndrome. A randomized, placebo‐controlled, double‐blind multicentre study. Human Reproduction 2006;21:80‐9. [DOI] [PubMed] [Google Scholar]
Trolle 2007 {published data only}
- Trolle B, Flyvbjerg A, Kesmodel U, Lauszus FF. Efficacy of metformin in obese and non‐obese women with polycystic ovary syndrome: a randomized, double‐blinded, placebo‐controlled cross‐over trial. Human Reproduction 2007;22(11):2967‐73. [original article] [DOI] [PubMed] [Google Scholar]
- Trolle B, Flyvbjerg A, Kesmodel U, Lauszus FF. Efficacy of metformin in obese and non‐obese women with polycystic ovary syndrome: a randomized, double‐blinded, placebo‐controlled cross‐over trial. Obstetrics and Gynecological Survey 2008;63(2):96‐8. [DOI] [PubMed] [Google Scholar]
Vandermolen 2001 {published data only}
- Vandermolen DT, Ratts VS, Evans WS, Stovall DW, Kauma SW, Nestler JE. Metformin increases the ovulatory rate and pregnancy rate from clomiphene citrate in patients with polycystic ovary syndrome who are resistant to clomiphene citrate alone. Fertility and Sterility 2001;75:310‐5. [DOI] [PubMed] [Google Scholar]
Williams 2009 {published data only}
- Williams SC, Pastore LM, Shelly WB, Bailey AP, Baras DC, Bateman BG. A randomized, placebo‐controlled study of the influence of instant‐release metformin on response to clomiphene citrate and time to conception in polycystic ovary syndrome. Fertility and Sterility 2009;92 Suppl(3):105. [Google Scholar]
Yarali 2002 {published data only}
- Yarali H, Yildiz BO, Demirol A, Zeyneloglu HB, Yigit N, Bukulmez O, et al. Co‐administration of metformin during rFSH treatment in patients with clomiphene citrate‐resistant polycystic ovarian syndrome: a prospective randomized trial. Human Reproduction 2002;17(2):289‐94. [DOI] [PubMed] [Google Scholar]
- Yarali H, Yyldyz B, Demirol A, Zeyneloglu H, Yigit N, Bukulmez O. Co‐administration of metformin during recombinant follicle stimulating hormone (recombinant FSH) treatment using the low‐dose step protocol in patients with clomiphene citrate resistant polycystic ovary syndrome (PCOS): a prospective randomized trial. Fertility and Sterility 2001;76 Suppl(3):36. [Google Scholar]
Zain 2009 {published data only}
- Zain MM, Jamaluddin R, Ibrahim A, Norman RJ. Comparison of clomiphene citrate, metformin, or the combination of both for first‐line ovulation induction, achievement of pregnancy, and live birth in Asian women with polycystic ovary syndrome: a randomized controlled trial. Fertility and Sterility 2009;91(2):514‐21. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Abuelghar 2013 {published data only}
- Abuelghar WM, Elkady OS, Khamees AA. Clomiphene citrate alone, in combination with metformin or in combination with pioglitazone as first line therapy in induction of ovulation in infertile women with polycystic ovary syndrome, a randomised controlled trial. Middle East Fertility Society Journal 2013;18:135‐41. [Google Scholar]
Aroda 2009 {published data only}
- Aroda V, Ciaraldi T, Burke P, Mudaliar S, Clopton P, Phillips S, et al. Metabolic and hormonal changes induced by pioglitazone in polycystic ovary syndrome: a randomized, placebo‐controlled clinical trial. Journal of Clinical Endocrinology and Metabolism 2009;94(2):469‐76. [DOI] [PMC free article] [PubMed] [Google Scholar]
Azziz 2001 {published data only}
- Azziz R, Ehrmann D, Legro RS, Whitcomb RW, Hanley R, Fereshetian AG, et al. Troglitazone improves ovulation and hirsutism in the polycystic ovary syndrome: a multicenter, double blind, placebo‐controlled trial. Journal of Clinical Endocrinology and Metabolism 2001;86(4):1626‐32. [original article] [DOI] [PubMed] [Google Scholar]
- Guyatt G, Weaver B, Cronin L, Dooley JA, Azziz R. Health‐related quality of life in women with polycystic ovary syndrome, a self‐administered questionnaire, was validated. Journal of Clinical Epidemiology 2004;57:1279‐87. [DOI] [PubMed] [Google Scholar]
- Legro RS, Azziz R, Ehrmann D, Fereshetian AG, O'Keefe M, Ghazzi MN. Minimal response of circulating lipids in women with polycystic ovary syndrome to improvement in insulin sensitivity with troglitazone. Journal of Clinical Endocrinology and Metabolism 2003;88:5137‐44. [DOI] [PubMed] [Google Scholar]
Azziz 2003 {published data only}
- Azziz R, Ehrmann DA, Legro RS, Fereshetian AG, O'Keefe M, Ghazzi MN. Troglitazone decreases adrenal androgen levels in women with polycystic ovary syndrome. Fertility and Sterility 2003;79:932‐7. [DOI] [PubMed] [Google Scholar]
Chaudhry 2016 {published data only}
- Chaudhry I, Nisa SU, Nia SU. Comparison between pioglitazone and metformin in terms of efficacy in patients with polycystic ovarian syndrome. Pakistan Journal of Medical and Health Sciences 2016;10:574‐7. [Google Scholar]
Chaudhury 2008 {published data only}
- Chaudhury K, Chaudhury S, Chowdhury S. Does metformin augment the ovulation inducing effects of clomiphene in non‐obese women with polycystic ovary syndrome?. Journal of the Indian Medical Association 2008;106(10):643‐8. [PubMed] [Google Scholar]
Constantino 2009 {published data only}
- Costantino D, Minozzi G, Minozzi F, Guaraldi C. Metabolic and hormonal effects of myo‐inositol in women with polycystic ovary syndrome: a double‐blind trial. European Review for Medical and Pharmacological Sciences 2009;13(2):105‐10. [PubMed] [Google Scholar]
Crave 1995 {published data only}
- Crave JC, Fimbel S, Lejeune H, Cugnardey N, Dechaud H, Pugeat M. Effects of diet and metformin administration on sex hormone‐binding globulin, androgens, and insulin in hirsute and obese women. Journal of Clinical Endocrinology and Metabolism 1995;80(7):2057‐62. [DOI] [PubMed] [Google Scholar]
Curi 2012 {published data only}
- Curi DD, Fonseca AM, Marcondes JA, Almeida JA, Bagnoli VR, Soares JM Jr, et al. Metformin versus lifestyle changes in treating women with polycystic ovary syndrome. Gynecological Endocrinology 2010;28:182‐5. [DOI] [PubMed] [Google Scholar]
De Leo 1999 {published data only}
- Leo V, Marca A, Ditto A, Morgante G, Cianci A. Effects of metformin on gonadotropin‐induced ovulation in women with polycystic ovary syndrome. Fertility and Sterility 1999;72(2):282‐5. [DOI] [PubMed] [Google Scholar]
Dunaif 1996 {published data only}
- Dunaif A, Scott D, Finegood D, Quintana B, Whitcomb R. The insulin‐sensitizing agent troglitazone improves metabolic and reproductive abnormalities in the polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 1996;81(9):3299‐306. [DOI] [PubMed] [Google Scholar]
Elter 2002 {published data only}
- Elter K, Imir G, Durmusoglu F. Clinical, endocrine and metabolic effects of metformin added to ethinyl estradiol‐cyproterone acetate in non‐obese women with polycystic ovarian syndrome: a randomized controlled study. Human Reproduction 2002;17(7):1729‐37. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Farzadi 2006 {published data only}
- Farzadi L, Salman S. Metformin‐therapy effects in 50 clomiphene citrate resistant PCOS patients. Journal of Medical Science 2006;6:765‐71. [Google Scholar]
Heathcote 2013 {published data only}
- Heathcote G, Forbes K, Lee A, Gregor M, Luscombe G, Boothroyd C. Live birth rate after metformin and clomiphene vs clomiphene alone in polycystic ovary syndrome (PCOS): a randomized, double‐blind, placebo‐controlled trial. Draft paper supplied by authors.
Hou 2000 {published data only}
- Hou J, Yu J, Wei M. Study on treatment of hyperandrogenism and hyperinsulinism in polycystic ovary syndrome with Chinese herbal formula "tiangui fang". Zhongguo Zhong Xi Yi Jie He Za Zhi 2000;20(8):589‐92. [PubMed] [Google Scholar]
Ibanez 2002 {published data only}
- Ibanez L, Valls C, Ferrer A, Ong K, Dunger D, De‐Zegher F. Additive effects of insulin‐sensitizing and anti‐androgen treatment in young, nonobese women with hyperinsulinism, hyperandrogenism, dyslipidemia, and anovulation. Journal of Clinical Endocrinology and Metabolism 2002;87(6):2870‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Kazerooni 2009 {published data only}
- Kazerooni T, Ghaffarpasand F, Kazerooni Y, Kazerooni M, Setoodeh S. Short‐term metformin treatment for clomiphene citrate‐resistant women with polycystic ovary syndrome. International Journal of Gynaecology and Obstetrics 2009;107(1):50‐3. [DOI] [PubMed] [Google Scholar]
Kelly 2002 {published data only}
- Kelly CJ, Gordon D. The effect of metformin on hirsutism in polycystic ovary syndrome. European Journal of Endocrinology 2002;147(2):217‐21. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Kocak 2002 {published data only}
- Kocak M, Caliskan E, Simsir C, Haberal A. Metformin therapy improves ovulatory rates, cervical scores, and pregnancy rates in clomiphene citrate‐resistant women with polycystic ovary syndrome. Fertility and Sterility 2002;77(1):101‐6. [DOI] [PubMed] [Google Scholar]
Ladson 2011 {published data only}
- Ladson G, Dodson WC, Sweet SD, Archibong AE, Kunselman AR, Demers LM, et al. The effects of metformin with lifestyle therapy in polycystic ovary syndrome: a randomized double‐blind study. Fertility and Sterility 2011;95(3):1059‐66. [DOI] [PMC free article] [PubMed] [Google Scholar]
Leanza 2014 {published data only}
- Leanza V, Coco L, Grasso F, Leanza G, Zarbo G, Palumbo M. Ovulation induction with clomiphene citrate and metformin in women with polycystic ovary syndrome. Minerva Ginecologica 2014;66(3):299‐301. [PubMed] [Google Scholar]
Mantzoros 1997 {published data only}
- Mantzoros CS, Dunaif A, Flier JS. Leptin concentrations in the polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 1997;82(6):1687‐91. [DOI] [PubMed] [Google Scholar]
Morin‐Papunen 2000 {published data only}
- Morin‐Papunen LC, Vauhkonen I, Koivunen RM, Ruokonen A, Martikainen HK, Tapanainen JS. Endocrine and metabolic effects of metformin versus ethinyl estradiol‐cyproterone acetate in obese women with polycystic ovary syndrome: a randomized study. Journal of Clinical Endocrinology and Metabolism 2000;85(9):3161‐8. [DOI: 10.1210/jcem.85.9.6792] [DOI] [PubMed] [Google Scholar]
Morin‐Papunen 2010 {published data only}
- Morin‐Papunen L, Rantala A, Unkila‐Kallio L, Tiitinen A, Hippelainen M, Tinkanen H, et al. Metformin improves pregnancy and live birth rates in women with polycystic ovary syndrome ‐ a multicentre placebo‐controlled randomised trial. 26th Annual Meeting of the European Society of Human Reproduction and Embryology, ESHRE Rome Italy 2010;25:i67‐8. [Google Scholar]
Nestler 1996 {published data only}
- Nestler JE, Jakubowicz DJ. Decreases in ovarian cytochrome P450c17 alpha activity and serum free testosterone after reduction of insulin secretion in polycystic ovary syndrome. New England Journal of Medicine 1996;335(9):617‐23. [DOI] [PubMed] [Google Scholar]
Nestler 1997 {published data only}
- Nestler JE, Jakubowicz DJ. Lean women with polycystic ovary syndrome respond to insulin reduction with decreases in ovarian P450c17 alpha activity and serum androgens. Journal of Clinical Endocrinology and Metabolism 1997;82(12):4075‐9. [DOI] [PubMed] [Google Scholar]
Palomba 2011 {published data only}
- Palomba S, Falbo A, Cello A, Cappiello F, Tolino A, Zullo F. Does metformin affect the ovarian response to gonadotropins for in vitro fertilization treatment in patients with polycystic ovary syndrome and reduced ovarian reserve? A randomized controlled trial. Fertility and Sterility 2011;96:1128‐33. [DOI] [PubMed] [Google Scholar]
Papaleo 2009 {published data only}
- Papaleo E, Unfer V, Baillargeon JP, Fusi F, Occhi F, Santis L. Myo‐inositol may improve oocyte quality in intracytoplasmic sperm injection cycles. A prospective, controlled, randomized trial. Fertility and Sterility 2009;91:1750‐4. [DOI] [PubMed] [Google Scholar]
Ramzy 2003 {published data only}
- Ramzy A, El‐Kateb S, Al‐Inany H, Aboulmaaty Z, Badie M. The use of metformin in overweight and lean infertile patients with polycystic ovarian syndrome: a randomised controlled trial. Middle East Fertility Society Journal 2003;8:143‐9. [Google Scholar]
Refaie 2005 {published data only}
- Refaie A, Ibrahim G, Oash S. Characteristics of polycystic ovary syndrome with and without insulin resistance and the role of insulin sensitizing drug (metformin) in its management. Middle East Fertility Society Jounal 2005;10:142‐9. [Google Scholar]
Rouzi 2006 {published data only}
- Rouzi AA, Ardawi MS. A randomized controlled trial of the efficacy of rosiglitazone and clomiphene citrate versus metformin and clomiphene citrate in women with clomiphene citrate‐resistant polycystic ovary syndrome. Fertility and Sterility 2006;85:428‐35. [DOI] [PubMed] [Google Scholar]
Salman 2014 {published data only}
- Salman SA, Farghaly TA, Attallah DA, Abdel‐Hafeez HA, Shaaban OM. Insulin sensitizing agent (metformin) improves clinical pregnancy rate in clomiphene citrate resistant polycystic ovarian syndrome patients with acanthosis nigricans. Fertility and Sterility 2014;102(Supplement 3):e139. [Google Scholar]
Santonocito 2009 {published data only}
- Santonocito V, Rapisarda V, Abruzzo SRM, Pollicino R, Coco L, Zarbo G. Comparison between clomiphene citrate and metformin for induction of ovulatory cycles in infertile nonobese women with polycystic ovary syndrome. Giornale Italiano di Ostetricia e Ginecologia 2009;31(11‐12):455‐60. [Google Scholar]
Shobokshi 2003 {published data only}
- Shobokshi A, Shaarawy M. Correction of insulin resistance and hyperandrogenism in polycystic ovary syndrome by combined rosiglitazone and clomiphene citrate therapy. Journal of the Society for Gynecologic Investigation 2003;10:99‐104. [DOI] [PubMed] [Google Scholar]
Unfer 2011 {published data only}
- Unfer V, Carlomagno G, Rizzo P, Raffone E, Roseff S. Myo‐inositol rather than D‐chiro‐inositol is able to improve oocyte quality in intracytoplasmic sperm injection cycles. A prospective, controlled, randomized trial. European Review for Medical and Pharmacological Sciences 2011;15:452‐7. [PubMed] [Google Scholar]
Additional references
Abu Hashim 2016
- Abu Hashim H. Twenty years of ovulation induction with metformin for PCOS; what is the best available evidence?. Reproductive BioMedicine Online 2016;32:44‐53. [DOI] [PubMed] [Google Scholar]
Alebic 2014
- Alebić MS, Bulum T, Stojanović N, Duvnjak L. Definition of insulin resistance using the homeostasis model assessment (HOMA‐IR) in IVF patients diagnosed with polycystic ovary syndrome (PCOS) according to the Rotterdam criteria. Endocrine 2014;47:625‐30. [DOI] [PubMed] [Google Scholar]
Alvarez‐Blasco 2006
- Alvarez‐Blasco F, Botella‐Carretero JI, San Millán JL, Escobar‐Morreale HF. Prevalence and characteristics of the polycystic ovary syndrome in overweight and obese women. Archives of Internal Medicine 2006;166:2081‐6. [DOI] [PubMed] [Google Scholar]
Apridonidze 2005
- Apridonidze T, Essah PA, Iuorno MJ, Nestler JE. Prevalence and characteristics of the metabolic syndrome in women with polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 2005;90:1929‐35. [DOI] [PubMed] [Google Scholar]
Azziz 2005
- Azziz R, Marin C, Hoq L, Badamgarav E, Song P. Health care‐related economic burden of the polycystic ovary syndrome during the reproductive life span. Journal of Clinical Endocrinology and Metabolism 2005;90:4650‐8. [DOI] [PubMed] [Google Scholar]
Balen 2014
- Balen AH. Infertility in Practice. 4th Edition. Boca Raton: CRC Press, 2014. [13:978‐1‐84184‐5] [Google Scholar]
Balen 2016
- Balen AH, Morley LC, Misso M, Franks S, Legro RS, Wijeyaratne CN, et al. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Human Reproduction Update 2016;22:687‐708. [DOI: 10.1093/humupd/dmw025] [DOI] [PubMed] [Google Scholar]
Bordewijk 2017
- Bordewijk EM, Nahuis M, Costello MF, Veen F, Tso LO, Mol BWJ, et al. Metformin during ovulation induction with gonadotrophins followed by timed intercourse or intrauterine insemination for subfertility associated with polycystic ovary syndrome. Cochrane Database of Systematic Reviews 2017, Issue 1. [DOI: 10.1002/14651858.CD009090.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cassina 2014
- Cassina M, Donà M, Gianantonio E, Litta P, Clementi M. First‐trimester exposure to metformin and risk of birth defects: a systematic review and meta‐analysis. Human Reproduction Update 2014;20:656‐69. [DOI] [PubMed] [Google Scholar]
Cedergren 2004
- Cedergren MI. Maternal morbid obesity and the risk of adverse pregnancy outcome. Obstetrics and Gynecology 2004;103:219‐24. [DOI] [PubMed] [Google Scholar]
Celik 2014
- Celik C, Tasdemir N, Abali R, Bastu E, Yilmaz M. Progression to impaired glucose tolerance or type 2 diabetes mellitus in polycystic ovary syndrome: a controlled follow‐up study. Fertility and Sterility 2014;101:1123‐8. [DOI] [PubMed] [Google Scholar]
Colca 2013
- Colca JR, McDonald WG, Cavey GS, Cole SL, Holewa DD, Brightwell‐Conrad AS, et al. Identification of a mitochondrial target of thiazolidinedione insulin sensitizers (mTOT)‐‐relationship to newly identified mitochondrial pyruvate carrier proteins. PLoS One 2013;8:Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
Costello 2003
- Costello MF, Eden JA. A systematic review of the reproductive system effects of metformin in patients with polycystic ovary syndrome. Fertility and Sterility 2003;79:1‐13. [DOI] [PubMed] [Google Scholar]
Costello 2007
- Costello M, Shrestha B, Eden J, Sjoblom P, Johnson N. Insulin‐sensitising drugs versus the combined oral contraceptive pill for hirsutism, acne and risk of diabetes, cardiovascular disease, and endometrial cancer in polycystic ovary syndrome. Cochrane Database of Systematic Reviews 2007, Issue 1. [DOI: 10.1002/14651858.CD005552.pub2; PUBMED: 17253562] [DOI] [PubMed] [Google Scholar]
De Frene 2014
- Frène V, Vansteelandt S, T'Sjoen G, Gerris J, Somers S, Vercruysse L, et al. A retrospective study of the pregnancy, delivery and neonatal outcome in overweight versus normal weight women with polycystic ovary syndrome. Human Reproduction 2014;29:2333‐8. [DOI] [PubMed] [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JPT, Altman DG (editors). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Diamanti‐Kandarakis 2010
- Diamanti‐Kandarakis E, Christakou CD, Kandarakis E, Economou F. Metformin: an old medication of new fashion: evolving new molecular mechanisms and clinical implications in polycystic ovary syndrome. European Journal of Endocrinology 2010;162:193‐212. [DOI] [PubMed] [Google Scholar]
Ehrmann 2006
- Ehrmann DA, Liljenquist DR, Kasza K, Azziz R, Legro RS, Ghazzi MN. Prevalence and predictors of the metabolic syndrome in women with polycystic ovary syndrome. Journal of Clinical Endocrinology and Metabolism 2006;91:48‐53. [DOI] [PubMed] [Google Scholar]
EMA 2011
- European Medicines Agency. European Medicines Agency clarifies opinion on pioglitazone and the risk of bladder cancer. www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2011/10/news_detail_001368.jsp&mid=WC0b01ac058004d5c1&jsenabled=true Accessed 2011.
ESHRE/ASRM 2004
- The Rotterdam ESHRE/ASRM‐sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long‐term health risks related to polycystic ovary syndrome (PCOS). Human Reproduction 2004;19(1):41. [DOI] [PubMed] [Google Scholar]
ESHRE/ASRM 2008
- The Thessaloniki ESHRE/ASRM‐sponsored PCOS consensus workshop group. Consensus on infertility treatment related to polycystic ovary syndrome. Human Reproduction 2008;23:462‐77. [DOI] [PubMed] [Google Scholar]
Fauser 2012
- Fauser BC, Tarlatzis BC, Rebar RW, Legro RS, Balen AH, Lobo R, et al. Consensus on women's health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM‐sponsored 3rd PCOS Consensus Workshop Group. Fertility and Sterility 2012;97:28‐38. [PUBMED: 22153789] [DOI] [PubMed] [Google Scholar]
FDA 2002
- FDA (Federal Drug Administration). www.fda.gov Accessed 14 January 2003.
Ford 2004
- Ford ES. The metabolic syndrome and mortality from cardiovascular disease and all‐causes: findings from the National Health and Nutrition Examination Survey II Mortality Study. Atherosclerosis 2004;173:309‐14. [DOI] [PubMed] [Google Scholar]
Franik 2014
- Franik S, Kremer JAN, Nelen W, Farquhar C. Aromatase inhibitors for subfertile women with polycystic ovary syndrome. Cochrane Database of Systematic Reviews 2014, Issue 2. [DOI: 10.1002/14651858.CD010287.pub2] [DOI] [PubMed] [Google Scholar]
Gillies 2007
- Gillies CL, Abrams KR, Lambert PC, Cooper NJ, Sutton AJ, Hsu RT, et al. Pharmacological and lifestyle interventions to prevent or delay type 2 diabetes in people with impaired glucose tolerance: systematic review and meta‐analysis. BMJ 2007;334:299. [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Hamilton (ON): McMaster University (developed by Evidence Prime), Accessed 2015‐2017.
Graham 2003
- Graham DJ, Green L, Senior JR, Nourjah P. Troglitazone‐induced liver failure: a case study. The American Journal of Medicine 2003;114:299‐306. [DOI] [PubMed] [Google Scholar]
Hahn 2007
- Hahn S, Tan S, Sack S, Kimmig R, Quadbeck B, Mann K, et al. Prevalence of the metabolic syndrome in German women with polycystic ovary syndrome. Experimental and Clinical Endocrinology & Diabetes 2007;115:130‐5. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Huber‐Buchholz 1999
- Huber‐Buchholz MM, Carey DG, Norman RJ. Restoration of reproductive potential by lifestyle modification in obese polycystic ovary syndrome: role of insulin sensitivity and luteinizing hormone. Journal of Clinical Endocrinology and Metabolism 1999;84:1470‐4. [DOI] [PubMed] [Google Scholar]
Jensterle 2014
- Jensterle M, Kocjan T, Pfeifer M, Janez A. Short‐term intervention with liraglutide improved eating behaviour in obese women with polycystic ovary syndrome. Endocrine Research 2014;40:133‐8. [DOI] [PubMed] [Google Scholar]
Kiddy 1992
- Kiddy DS, Hamilton‐Fairley D, Bush A, Short F, Anyaoku V, Reed MJ, et al. Improvement in endocrine and ovarian function during dietary treatment of obese women with polycystic ovary syndrome. Clinical Endocrinology (Oxford) 1992;36:105‐11. [DOI] [PubMed] [Google Scholar]
Knowler 2002
- Knowler WC, Barrett‐Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. New England Journal of Medicine 2002;346:393‐403. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lago 2007
- Lago RM, Singh PP, Nesto RW. Congestive heart failure and cardiovascular death in patients with prediabetes and type 2 diabetes given thiazolidinediones: a meta‐analysis of randomised clinical trials. Lancet 2007;370(9593):1129‐36. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Legro 2006a
- Legro RS. Type 2 diabetes and polycystic ovary syndrome. Fertility and Sterility 2006;86 Suppl 1:16‐7. [DOI] [PubMed] [Google Scholar]
Legro 2006b
- Legro RS, Myers ER, Barnhart HX, Carson SA, Diamond MP, Carr BR, et al. and Reproductive Medicine Network. The Pregnancy in Polycystic Ovary Syndrome Study: baseline characteristics of the randomized cohort including racial effects. Fertility and Sterility 2006;86(4):914‐33. [DOI] [PubMed] [Google Scholar]
Lord 2002
- Lord J, Wilkin T. Polycystic ovary syndrome and fat distribution: the central issue?. Hum Fertil (Camb) 2002;5:67‐71. [DOI] [PubMed] [Google Scholar]
March 2010
- March WA, Moore VM, Willson KJ, Phillips DI, Norman RJ, Davies MJ. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Human Reproduction 2010;25:544‐51. [DOI] [PubMed] [Google Scholar]
Misso 2013
- Misso ML, Costello MF, Garrubba M, Wong J, Hart R, Rombauts L, et al. Metformin versus clomiphene citrate for infertility in non‐obese women with polycystic ovary syndrome: a systematic review and meta‐analysis. Human Reproduction Update 2013;19:2‐11. [DOI] [PubMed] [Google Scholar]
Moran 2011
- Moran LJ, Hutchison SK, Norman RJ, Teede HJ. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database of Systematic Reviews 2011, Issue 7. [DOI: 10.1002/14651858.CD007506.pub3] [DOI] [PubMed] [Google Scholar]
Moran 2012
- Moran LJ, Deeks AA, Gibson‐Helm ME, Teede HJ. Psychological parameters in the reproductive phenotypes of polycystic ovary syndrome. Human Reproduction 2012;27:2082‐8. [DOI] [PubMed] [Google Scholar]
Palomba 2009
- Palomba S, Pasquali R, Orio Jr F, Nestler JE. Clomiphene citrate, metformin or both as first‐step approach in treating anovulatory infertility in patients with polycystic ovary syndrome (PCOS): a systematic review of head‐to‐head randomized controlled studies and meta‐analysis. Clinical Endocrinology 2009;70:311‐21. [DOI] [PubMed] [Google Scholar]
Pasquali 2003
- Pasquali R, Pelusi C, Genghini S, Cacciari M, Gambineri A. Obesity and reproductive disorders in women. Human Reproduction Update 2003;9:359‐72. [DOI] [PubMed] [Google Scholar]
Pernicova 2014
- Pernicova I, Korbonits M. Metformin‐‐mode of action and clinical implications for diabetes and cancer. Nature Reviews. Endocrinology 2014;10:143‐56. [DOI: 10.1038/nrendo.2013.256] [DOI] [PubMed] [Google Scholar]
Rautio 2006a
- Rautio K, Tapanainen JS, Ruokonen A, Morin‐Papunen LC. Endocrine and metabolic effects of rosiglitazone in overweight women with PCOS: a randomized placebo‐controlled study. Human Reproduction 2006;21:1400‐7. [DOI] [PubMed] [Google Scholar]
Rautio 2006b
- Rautio K, Tapanainen JS, Ruokonen A, Morin‐Papunen LC. Rosiglitazone treatment alleviates inflammation and improves liver function in overweight women with polycystic ovary syndrome: a randomized placebo‐controlled study. Fertility and Sterility 2007;87(1):202‐6. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Robinson 1993
- Robinson S, Kiddy D, Gelding SV, Willis D, Niththyananthan R, Bush A, et al. The relationship of insulin insensitivity to menstrual pattern in women with hyperandrogenism and polycystic ovaries. Clinical Endocrinology (Oxford) 1993;39:351‐5. [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and ‘Summary of findings' tables. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from guidelinedevelopment.org/handbook.
Siebert 2012
- Siebert, TI, Viola MI, Steyn DW, Kruger TF. Is metformin indicated as primary ovulation induction agent in women with PCOS? A systematic review and meta‐analysis. Gynecologic and Obstetric Investigation 2012;73:304‐13. [DOI] [PubMed] [Google Scholar]
Soares 2007
- Soares EM, Azevedo GD, Gadelha RG, Lemos TM, Maranhao TM. Prevalence of the metabolic syndrome and its components in Brazilian women with polycystic ovary syndrome. Fertility and Sterility 2007;88(5):1389‐95. [DOI] [PubMed] [Google Scholar]
Stein 1935
- Stein. Amenorrhea associated with bilateral polycystic ovaries. American Journal of Obstetrics and Gynecology 1935;29:181‐91. [Google Scholar]
Stepto 2013
- Stepto NK, Cassar S, Joham AE, Hutchison SK, Harrison CL, Goldstein RF, et al. Women with polycystic ovary syndrome have intrinsic insulin resistance on euglycaemic‐hyperinsulaemic clamp. Human Reproduction 2013;28:544‐51. [DOI] [PubMed] [Google Scholar]
Sterne 2011
- Sterne JAC, Egger M, Moher D (editors). Chapter 10: Addressing reporting biases. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Intervention. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Tso 2014
- Tso L, Costello MF, Albuquerque LE, Andriolo RB, Macedo CR. Metformin treatment before and during IVF or ICSI in women with polycystic ovary syndrome. Cochrane Database of Systematic Reviews 2014, Issue 11. [DOI: 10.1002/14651858.CD006105.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Uusitupa 2000
- Uusitupa M, Louheranta A, Lindstrom J, Valle T, Sundvall J, Eriksson J, et al. The Finnish Diabetes Prevention Study. British Journal of Nutrition 2000;83 Suppl 1:137‐42. [DOI] [PubMed] [Google Scholar]
Velazquez 1997
- Velazquez E, Acosta A, Mendoza SG. Menstrual cyclicity after metformin therapy in polycystic ovary syndrome. Obstetrics and Gynecology 1997;90:392‐5. [DOI] [PubMed] [Google Scholar]
Weerakiet 2007
- Weerakiet S, Bunnag P, Phakdeekitcharoen B, Wansumrith S, Chanprasertyothin S, Jultanmas R, et al. Prevalence of the metabolic syndrome in Asian women with polycystic ovary syndrome: using the International Diabetes Federation criteria. Gynecological Endocrinology 2007;23:153‐60. [DOI] [PubMed] [Google Scholar]
Wijeyaratne 2002
- Wijeyaratne CN, Balen AH, Barth JH, Belchetz PE. Clinical manifestations and insulin resistance (IR) in polycystic ovary syndrome (PCOS) among South Asians and Caucasians: is there a difference?. Clinical Endocrinology (Oxford) 2002;57:343‐50. [DOI] [PubMed] [Google Scholar]
Wijeyaratne 2004
- Wijeyaratne CN, Nirantharakumar K, Balen AH, Barth JH, Sheriff R, Belchetz PE. Plasma homocysteine in polycystic ovary syndrome: does it correlate with insulin resistance and ethnicity?. Clinical Endocrinology (Oxford) 2004;60:560‐7. [DOI] [PubMed] [Google Scholar]
Yki‐Jarvinen 2004
- Yki‐Jarvinen H. Thiazolidinediones. New England Journal of Medicine 2004;351:1106‐18. [DOI] [PubMed] [Google Scholar]
Zhang 2012
- Zhang Y, Ye J. Mitochondrial inhibitor as a new class of insulin sensitizer. Acta Pharmacologica Sinica 2012;2:341‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Lord 2003
- Lord JM, Flight IH, Norman RJ. Insulin‐sensitising drugs (metformin, troglitazone, rosiglitazone, pioglitazone, D‐chiro‐inositol) for polycystic ovary syndrome. Cochrane Database of Systematic Reviews 2003, Issue 3. [DOI: 10.1002/14651858.CD003053] [DOI] [PubMed] [Google Scholar]
Tang 2009
- Tang T, Lord JM, Norman RJ, Yasmin E, Balen AH. Insulin‐sensitising drugs (metformin, rosiglitazone, pioglitazone, D‐chiro‐inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD003053.pub4; PUBMED: 20091537] [DOI] [PubMed] [Google Scholar]
Tang 2012
- Tang T, Lord JM, Norman RJ, Yasmin E, Balen AH. Insulin‐sensitising drugs (metformin, rosiglitazone, pioglitazone, D‐chiro‐inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD003053.pub5] [DOI] [PubMed] [Google Scholar]