

Abstract
Background
Foot ulcers in people with diabetes are a prevalent and serious global health issue. Dressings form a key part of ulcer treatment, with clinicians and patients having many different types to choose from including hydrogel dressings. A clear and current overview of current evidence is required to facilitate decision‐making regarding dressing use.
Objectives
To assess the effects of hydrogel wound dressings compared with alternative dressings or none on the healing of foot ulcers in people with diabetes.
Search methods
For this first update, in April 2013, we searched the following databases the Cochrane Wounds Group Specialised Register; The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library); Ovid MEDLINE; Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations); Ovid EMBASE; and EBSCO CINAHL. There were no restrictions based on language or date of publication.
Selection criteria
Published or unpublished randomised controlled trials (RCTs) that have compared the effects on ulcer healing of hydrogel with alternative wound dressings or no dressing in the treatment of foot ulcers in people with diabetes.
Data collection and analysis
Two review authors independently performed study selection, risk of bias assessment and data extraction.
Main results
We included five studies (446 participants) in this review. Meta analysis of three studies comparing hydrogel dressings with basic wound contract dressings found significantly greater healing with hydrogel: risk ratio (RR) 1.80, 95% confidence interval (CI) 1.27 to 2.56. The three pooled studies had different follow‐up times (12 weeks, 16 weeks and 20 weeks) and also evaluated ulcers of different severities (grade 3 and 4; grade 2 and grade unspecified). One study compared a hydrogel dressing with larval therapy and found no statistically significant difference in the number of ulcers healed and another found no statistically significant difference in healing between hydrogel and platelet‐derived growth factor. There was also no statistically significant difference in number of healed ulcers between two different brands of hydrogel dressing. All included studies were small and at unclear risk of bias and there was some clinical heterogeneity with studies including different ulcer grades. No included studies compared hydrogel with other advanced wound dressings.
Authors' conclusions
There is some evidence to suggest that hydrogel dressings are more effective in healing (lower grade) diabetic foot ulcers than basic wound contact dressings however this finding is uncertain due to risk of bias in the original studies. There is currently no research evidence to suggest that hydrogel is more effective than larval therapy or platelet‐derived growth factors in healing diabetic foot ulcers, nor that one brand of hydrogel is more effective than another in ulcer healing. No RCTs comparing hydrogel dressings with other advanced dressing types were found.
Keywords: Humans; Bandages, Hydrocolloid; Wound Healing; Diabetic Foot; Diabetic Foot/drug therapy; Hydrogel, Polyethylene Glycol Dimethacrylate; Hydrogel, Polyethylene Glycol Dimethacrylate/therapeutic use; Randomized Controlled Trials as Topic
Plain language summary
Hydrogel dressings to promote diabetic foot ulcer healing
Diabetes, a condition which leads to high blood glucose concentrations, is a common condition with around 2.8 million people affected in the UK (approximately 3% of the population). Dressings are a widely used treatment when caring for foot ulcers in people with diabetes. There are many types of dressings that can be used, which also vary considerably in cost. This review (five studies involving a total of 446 people) suggests that hydrogel dressings may be more effective than basic wound contact dressings in healing foot ulcers in people with diabetes although the original research may be biased. There is insufficient research comparing hydrogel with advanced dressing types to allow conclusions to be drawn regarding relative effectiveness in terms of ulcer healing.
Summary of findings
Summary of findings for the main comparison. Hydrogel dressings compared to basic wound contact dressings for foot ulcers in people with diabetes.
| Hydrogel dressings compared to basic wound contact dressings for foot ulcers in people with diabetes | ||||||
| Patient or population: patients with foot ulcers in people with diabetes Settings: Intervention: Hydrogel dressings Comparison: basic wound contact dressings | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Basic wound contact dressings | Hydrogel dressings | |||||
| Number of ulcers healed Follow‐up: mean 16 weeks | Low risk of healing1 | RR 1.80 (1.27 to 2.56) | 198 (3 studies) | ⊕⊕⊕⊝ moderate2,3 | ||
| 340 per 1000 | 612 per 1000 (432 to 870) | |||||
| Moderate risk of healing1 | ||||||
| 530 per 1000 | 954 per 1000 (673 to 1000) | |||||
| High risk of healing1 | ||||||
| 650 per 1000 | 1000 per 1000 (825 to 1000) | |||||
| Adverse events Follow‐up: mean 16 weeks | Study population | Not estimable | 0 (3 studies) | See comment | Some adverse event data were reported, however, lack of methodological detail about reporting and type of data presented prevent further comment. | |
| See comment | See comment | |||||
| Moderate | ||||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Baseline risk of healing obtained from external source in which data from 27,630 patients with a diabetic neuropathic foot ulcer was used to develop a simple prognostic model to predict likelihood of ulcer healing (Margolis DJ, Allen‐Taylor L, Hoffstad O, Berlin JA. Diabetic neuropathic foot ulcers: predicting which ones will not heal. Am J Med. 2003;115:627‐31). It is important to note that given an outcome of ulcer healing, low risk refers to a low risk of healing and thus reflects the most severe patient populations. Conversely high risk refers to a high risk of healing. 2 Many of the risk of bias domains were unclear limiting judgements that could be made. 3 The confidence interval around the estimate of relative risk is consistent with a 27% relative increase in healing with hydrogel to a 256% relative increase in healing with hydrogel.
Summary of findings 2. Hydrogel dressings compared to Larval therapy for foot ulcers in people with diabetes.
| Hydrogel dressings compared to Larval therapy for foot ulcers in people with diabetes | ||||||
| Patient or population: patients with foot ulcers in people with diabetes Settings: Intervention: Hydrogel dressings Comparison: Larval therapy | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Larval therapy | Hydrogel dressings | |||||
| Number of ulcers healed Follow‐up: 10 days | Low risk of healing1 | RR 0.40 (0.08 to 1.99) | 140 (1 study) | ⊕⊕⊝⊝ low2,3 | ||
| 340 per 1000 | 136 per 1000 (27 to 677) | |||||
| Moderate of healing1 | ||||||
| 530 per 1000 | 212 per 1000 (42 to 1000) | |||||
| High risk of healing1 | ||||||
| 650 per 1000 | 260 per 1000 (52 to 1000) | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Baseline risk of healing obtained from external source in which data from 27,630 patients with a diabetic neuropathic foot ulcer was used to develop a simple prognostic model to predict likelihood of ulcer healing (Margolis DJ, Allen‐Taylor L, Hoffstad O, Berlin JA. Diabetic neuropathic foot ulcers: predicting which ones will not heal. Am J Med. 2003;115:627‐31). It is important to note that given an outcome of ulcer healing, low risk refers to a low risk of healing and thus reflects the most severe patient populations. Conversely high risk refers to a high risk of healing 2 All domains classed at unclear risk of bias making judgement difficult. 3 7 participants achieved the endpoint of healing in the study, this is an underpowered comparison. The confidence interval around the estimate of relative risk is consistent with a 92% relative reduction in healing with hydrogel and a 199% relative increase in healing with hydrogel.
Summary of findings 3. Hydrogel dressing compared to platelet‐derived growth factor for foot ulcers in people with diabetes.
| Hydrogel dressing compared to platelet‐derived growth factor for Foot ulcers in people with diabetes | ||||||
| Patient or population: patients with Foot ulcers in people with diabetes Settings: Intervention: Hydrogel dressing Comparison: platelet‐derived growth factor | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Platelet‐dervided growth factor | Hydrogel dressing | |||||
| Number of ulcers healed Follow‐up: 20 weeks | Low risk of healing1 | RR 0.81 (0.5 to 1.32) | 104 (1 study) | ⊕⊕⊝⊝ low2 | ||
| 340 per 1000 | 275 per 1000 (170 to 449) | |||||
| Moderate risk of healing1 | ||||||
| 530 per 1000 | 429 per 1000 (265 to 700) | |||||
| High risk of healing1 | ||||||
| 650 per 1000 | 527 per 1000 (325 to 858) | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Baseline risk of healing obtained from external source in which data from 27,630 patients with a diabetic neuropathic foot ulcer was used to develop a simple prognostic model to predict likelihood of ulcer healing (Margolis DJ, Allen‐Taylor L, Hoffstad O, Berlin JA. Diabetic neuropathic foot ulcers: predicting which ones will not heal. Am J Med. 2003;115:627‐31). It is important to note that given an outcome of ulcer healing, low risk refers to a low risk of healing and thus reflects the most severe patient populations. Conversely high risk refers to a high risk of healing 2 40 participants achieved the endpoint of healing in the study, this is an underpowered comparison. The confidence interval around the estimate of relative risk is consistent with a 39% relative reduction in healing with hydrogel and a 26% relative increase in healing with hydrogel.
Summary of findings 4. Purilon hydrogel compared to Intrasite hydrogel for foot ulcers in people with diabetes.
| Purilon hydrogel compared to Intrasite hydrogel for foot ulcers in people with diabetes | ||||||
| Patient or population: patients with foot ulcers in people with diabetes Settings: Intervention: Purilon hydrogel Comparison: Intrasite hydrogel | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Intrasite hydrogel | Purilon hydrogel | |||||
| Number of ulcers healed Follow‐up: 10 weeks | Study population | Not estimable | 0 (1 study) | See comment | 35% of ulcers healed in the Purilon group compared with 19% in the Intrasite group. The numbers used for these calculations are not presented. Limiting analyses | |
| See comment | See comment | |||||
| Moderate | ||||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
Background
Description of the condition
Diabetes, high glucose levels in the blood, is a common condition, with around 2.8 million people affected in the UK (approximately 4.3% of the population) (Diabetes UK). Global projections suggest that the worldwide prevalence of diabetes is expected to rise to 4.4% by 2030, meaning that approximately 366 million people will be affected (Wild 2004).
Success in treating diabetes has improved the life expectancy of patients. However, the increased prevalence of diabetes coupled with the extended time people live with the disease has led to a rise in the number of diabetes‐related complications, such as neuropathy and peripheral arterial disease (PAD). It is estimated that lower extremity disease is twice as common in people with diabetes compared with people without (Gregg 2004). Both neuropathy and PAD are risk factors for diabetic foot ulceration (Pecoraro 1990; Reiber 1999), which is a problem reported to affect 15% or more of the diabetic population at some time in their lives. (Reiber 1996; Singh 2005). Around 1% to 4% of people with diabetes have foot ulcers at any given time (Abbott 2002; Kumar 1994). An ulcer forms as a result of damage to the epidermis and subsequent loss of underlying tissue. Specifically, the International Consensus on the Diabetic Foot defines a foot ulcer as a wound extending through the full thickness of the skin below the level of the ankle (Apelqvist 2000a). This is irrespective of duration and the ulcer can extend to muscle, tendon and bone. The Wagner wound classification system is well established and widely used for grading diabetic foot ulcers. The system assesses ulcer depth and the presence of osteomyelitis or gangrene in the following grades: grade 0 (pre‐ or post‐ulcerative lesion), grade 1 (partial/full thickness ulcer), grade 2 (probing to tendon or capsule), grade 3 (deep with osteitis), grade 4 (partial foot gangrene) and grade 5 (whole foot gangrene) (Wagner 1981). However, newer grading systems, such as the PEDIS system (Schaper 2004) and the University of Texas Wound Classification System (Oyibo 2001) have been developed.
PAD and neuropathy can occur separately (ischaemic foot and neuropathic foot) or in combination (in the neuroischaemic foot). The over‐arching term 'diabetic neuropathy' refers to a number of neuropathic syndromes. Chronic distal sensorimotor symmetrical neuropathy (abbreviated to distal symmetrical neuropathy) is the most common, affecting around 28% of people with diabetes. It can lead to ulceration through the following route(s) (Tesfaye 1996).
Sympathetic autonomic neuropathy leads to decreased sweating causing anhidrotic (dry) skin, which is prone to cracks and fissures causing a break in the dermal barrier (Tesfaye 1996).
Motor neuropathy causes wasting of the small, intrinsic muscles of the foot by de‐enervation. As the muscles waste they cause retraction of the toes and lead to a subsequent deformity. The abnormal foot shape can promote ulcer development due to an increase in plantar pressures (Murray 1996).
Sensory neuropathy results in impaired sensation, making the patient unaware of potentially dangerous foreign bodies and injuries.
People with diabetes‐related foot ulceration are treated in a variety of settings, for example community clinics, surgeries and their own homes, by a variety of practitioners; this can make data collection challenging. A UK study estimated that 2% of community‐based diabetic patients develop new foot ulcers each year (Abbott 2002). In terms of healing, a meta‐analysis of trials in which people with neuropathic ulcers received good wound care reported that 24% of ulcers attained complete healing by 12 weeks and 31% by 20 weeks (Margolis 1999). However, the risk of ulcer recurrence post‐healing is high. Pound 2005 reported that 62% of ulcer patients (n = 231) became ulcer‐free at some stage over a 31‐month observation period. However, of the ulcer‐free group 40% went on to develop a new or recurrent ulcer after a median of 126 days. The ulcer recurrence rate over five years can be as high as 70% (Dorresteijn 2010; Van Gils 1999).
Diabetic foot ulcers can seriously impact on an individual's quality of life and as many as 85% of foot‐related amputations are preceded by ulceration (Apelqvist 2000b; Pecoraro 1990). Patients with diabetes have a 10 to 20‐fold higher risk of losing a lower limb or part of a lower limb due to non‐traumatic amputation than those without diabetes (Morris 1998; Wrobel 2001).
Diabetic foot ulcers represent a major use of health resources, incurring costs not only for dressings applied, but also staff costs (for podiatry, nurses, doctors), tests and investigations, antibiotics and specialist footwear. Currie 1998 estimated the cost of healing a foot ulcer in a patient with diabetes at around GBP 1451. Hospital admissions add further to the costs. Ten years ago the cost of diabetic foot ulceration to the UK National Health Service was believed to be about GBP 12.9 million per year (Spencer 2000) and this figure is likely to have increased significantly. The economic impact is also high in terms of the personal costs to patients and carers, for example costs associated with lost work time and productivity while the patient is non‐weight bearing or hospitalised.
Description of the intervention
Broadly, the treatment of diabetic foot ulcers includes pressure relief (or off‐loading) by resting the foot or wearing special footwear or shoe inserts (or both); the removal of dead cellular material from the surface of the wound (debridement or desloughing); infection control; and the use of wound dressings. Other general strategies in the treatment of diabetic foot ulcers include: patient education; optimisation of blood glucose control; correction (where possible) of arterial insufficiency; and surgical interventions (debridement, drainage of pus, revascularisation, amputation).
Dressings are widely used in wound care, both to protect the wound and to promote healing. Classification of a dressing normally depends on the key material used. Several attributes of an ideal wound dressing have been described (BNF 2010), including:
the ability of the dressing to absorb and contain exudate without leakage or strike‐through;
lack of particulate contaminants left in the wound by the dressing;
thermal insulation;
permeability to water and bacteria;
avoidance of wound trauma on dressing removal;
frequency with which the dressing needs to be changed;
provision of pain relief; and
comfort.
There is a vast choice of dressings available to treat chronic wounds such as diabetic foot ulcers. For ease of comparison this review has categorised dressings according to the British National Formulary 2010 (BNF 2010) which is freely available via the internet. We will use 'generic' names where possible, also providing UK trade names and manufacturers where these are available to allow cross‐referencing with the BNF. However, it is important to note that the way dressings are categorised as well as dressing names, manufacturers and distributors of dressings vary from country to country, so these are provided as a guide only. Below is a description of all categories of dressings and includes the category of dressing (hydrogel) which is the focus of this review:
Basic wound contact dressings
Low‐adherence dressings and wound contact materials: usually cotton pads which are placed directly in contact with the wound. They can be either non‐medicated (e.g. paraffin gauze dressing) or medicated (e.g. containing povidone iodine or chlorhexidine). Examples are paraffin gauze dressing, BP 1993 and Xeroform (Covidien) dressing ‐ a non‐adherent petrolatum blend with 3% bismuth tribromophenate on fine mesh gauze.
Absorbent dressings: applied directly to the wound or used as secondary absorbent layers in the management of heavily exuding wounds. Examples include Primapore (Smith & Nephew), Mepore (Mölnlycke) and absorbent cotton gauze (BP 1988).
Advanced wound dressings
Hydrogel sheet and amorphous dressings: consist of a cross‐linked insoluable polymers (i.e. starch or carboxymethylcellulose) and up to 96% water. These dressings are designed to absorb wound exudate or rehydrate a wound depending on the wound moisture levels. They are supplied in either flat sheets, an amorphous hydrogel or as beads. Examples are: ActiformCool (Activa) and Aquaflo (Covidien).
Films ‐ permeable film and membrane dressings: permeable to water vapour and oxygen but not to water or microorganisms. Examples are Tegaderm (3M) and Opsite (Smith & Nephew).
Soft polymer dressings: dressings composed of a soft silicone polymer held in a non‐adherent layer. They are moderately absorbent. Examples are: Mepitel (Mölnlycke) and Urgotul (Urgo).
Hydrocolloid dressings: are occlusive dressings usually composed of a hydrocolloid matrix bonded onto a vapour‐permeable film or foam backing. When in contact with the wound surface this matrix forms a gel to provide a moist environment. Examples are: Granuflex (ConvaTec) and NU DERM (Systagenix). Fibrous alternatives have been developed which resemble alginates and are not occlusive but which are more absorbant than standard hydrocolloid dressings: Aquacel (ConvaTec).
Foam dressings: normally contain hydrophilic polyurethane foam and are designed to absorb wound exudate and maintain a moist wound surface. There are various versions and some foam dressings that include additional absorbent materials, such as viscose and acrylate fibres or particles of superabsorbent polyacrylate, or which are silicone‐coated for non‐traumatic removal. Examples are: Allevyn (Smith & Nephew), Biatain (Coloplast) and Tegaderm (3M).
Alginate dressings: highly absorbent and come in the form of calcium alginate or calcium sodium alginate and can be combined with collagen. The alginate forms a gel when in contact with the wound surface which can be lifted off with dressing removal or rinsed away with sterile saline. Bonding to a secondary viscose pad increases absorbency. Examples are: Curasorb (Covidien), SeaSorb (Coloplast) and Sorbsan (Unomedical).
Capillary‐action dressings: consist of an absorbent core of hydrophilic fibres held between two low‐adherent contact layers. Examples are: Advadraw (Advancis) and Vacutx (Protex).
Odour‐absorbent dressings: dressings that contain charcoal and are used to absorb wound odour. Often these types of wound dressings are used in conjunction with a secondary dressing to improve absorbency. Example: CarboFLEX (ConvaTec).
Antimicrobial dressings
Honey‐impregnated dressings: contain medical‐grade honey which is proposed to have antimicrobial and anti‐inflammatory properties and can be used for acute or chronic wounds. Examples are: Medihoney (Medihoney) and Activon Tulle (Advancis).
Iodine‐impregnated dressings: release free iodine when exposed to wound exudate, which is thought to act as a wound antiseptic. An example is Iodozyme (Insense).
Silver‐impregnated dressings: used to treat infected wounds as silver ions are thought to have antimicrobial properties. Silver versions of most dressing types are available (e.g. silver foam, silver hydrocolloid etc). Examples are: Acticoat (Smith & Nephew) and Urgosorb Silver (Urgo).
Other antimicrobial dressings: these dressings are composed of a gauze or low‐adherent dressing impregnated with an ointment thought to have antimicrobial properties. Examples are: chlorhexidine gauze dressing (Smith & Nephew) and Cutimed Sorbact (BSN Medical).
Specialist dressings
Protease‐modulating matrix dressings: alter the activity of proteolytic enzymes in chronic wounds. Examples are: Promogran (Systagenix) and Sorbion (H & R).
The diversity of dressings available to clinicians (including variation within each type listed above) makes evidence‐based decision‐making difficult when deciding the best treatment regimen for the patient. In a UK survey undertaken to determine treatments used for debriding diabetic foot ulcers, a diversity of treatments was reported (Smith 2003). It is possible that a similar scenario is true for dressing choice. A survey of Diabetes Specialist Nurses found that low/non‐adherent dressings, hydrocolloids and alginate dressings were the most popular for all wound types, despite a paucity of evidence for either of these dressing types (Fiskin 1996). However, several new dressing types have been made available and heavily promoted in recent years. Some dressings now have an 'active' ingredient such as silver that are promoted as dressing treatment options to reduce infection and thus possibly also promote healing in this way. With increasingly sophisticated technology being applied to wound care, practitioners need to know how effective these often expensive dressings are compared with more traditional dressings.
How the intervention might work
Animal experiments conducted over 40 years ago suggest that acute wounds heal more quickly when their surface is kept moist, rather than left to dry and scab (Winter 1963). A moist environment is thought to provide optimal conditions for the cells involved in the healing process as well as allowing autolytic debridement, which is thought to be an important part of the healing pathway (Cardinal 2009). The desire to maintain a moist wound environment is a key driver for the use of wound dressings. Different wound dressings vary in their level of absorbency so that a very wet wound can be treated with an absorbent dressing (such as a foam dressing) to draw excess moisture away from the wound to avoid skin damage, whilst a drier wound can be treated with a more occlusive dressing to maintain a moist environment. Hydrogels are insoluble polymers that bind together a relatively large volume of water. This water can then be donated to wounds to maintain a moist environment. Additionally as the hydrogel polymer matrix is not fully hydrated, it can also absorb some wound exudate with the aim of optimising the moist level of the wound. When hydrogel material is formed into a fixed structure via cross‐linking of the polymers it is considered a hydrogel sheet dressing.
Why it is important to do this review
Diabetic foot ulcers are a prevalent and serious global issue. Treatment with dressings forms a key part of the treatment pathway when caring for diabetic foot ulcers and there are many types of dressings that can be used, which also vary considerably in cost. Guidelines for the treatment of diabetic ulcer (e.g. Steed 2006) maintain that clinical judgement should be used to select a moist wound dressing.
However, previous reviews of the evidence for wound dressings as treatments for diabetic foot ulcers have not found evidence to support a specific dressing choice. Ten trials were eligible for inclusion in a UK Health Technology Assessment review of wound dressings published in 2000 (O'Meara 2000). The review included nine trials that investigated a dressing or topical treatment for healing diabetic foot ulcers. The review did not find any evidence to suggest that one dressing type was more or less effective in terms of treating diabetic foot ulcers. The methodological quality of trials was poor and all were small. Only one comparison was repeated in more than one trial. A further systematic review conducted some years ago reported similar findings (Mason 1999). A more recent systematic review on the effectiveness of interventions to enhance the healing of chronic ulcers of the foot (Hinchliffe 2008) (search date December 2006) included only eight trials (randomised and non‐randomised) did not identify any evidence that one dressing type was superior to another in terms of promoting ulcer healing. A Cochrane Review of silver‐based wound dressings and topical agents for treating diabetic foot ulcers (Bergin 2006; search date 2010) did not find any studies that met its inclusion criteria. Finally, a review of antimicrobial treatments for diabetic foot ulcers (Nelson 2006) included dressings and found that existing evidence was too weak to recommend any antimicrobial product.
This review is part of a suite of Cochrane Reviews investigating the use of dressings in the treatment of foot ulcers in people with diabetes. Each review will focus on a particular dressing type which in this review is the hydrogel dressing. These reviews will be summarised in an overview of reviews (Higgins 2009) which will draw together all existing Cochrane Review evidence regarding the use of dressings to treat foot ulcers in people with diabetes. Whilst other existing review evidence may also be included in this overview, following Cochrane guidance, this will only occur in the absence of a relevant Cochrane intervention review (Higgins 2009).
Objectives
To assess the effects of hydrogel wound dressings compared with alternative dressings or none on the healing of foot ulcers in people with diabetes.
Methods
Criteria for considering studies for this review
Types of studies
Published or unpublished randomised controlled trials (RCTs) that evaluated the effects of any type of hydrogel wound dressing in the treatment of diabetic foot ulcers, irrespective of publication status or language.
Types of participants
Trials recruiting people with type I or type II diabetes, with an open foot ulcer. Since study‐specific classifications of ulcer diagnosis were likely to be too restrictive, we accepted study authors' definitions of what was classed a diabetic foot ulcer. There was no restriction in relation to the aetiology of the ulcer; trials recruiting people with ulcers of neuropathic, ischaemic or neuroischaemic causes were all eligible for inclusion.
We included participants of any age. We excluded trials which included patients with a number of different wound aetiologies in addition to diabetic foot ulcers (e.g. pressure ulcers, mixed arterial/venous arterial) unless the results for the subgroup of patients with a diabetic foot ulcer were reported separately or available from authors on contact.
Types of interventions
The primary intervention was the hydrogel wound dressing (BNF 2010). We included any RCT in which the presence or absence of a hydrogel dressing was the only systematic difference between treatment groups. We anticipated that likely comparisons would include hydrogel dressings compared with either a different hydrogel dressing or other dressing types and/or other interventions (which could be non‐dressing treatments, i.e. topical applications).
Types of outcome measures
Primary outcomes
Time to ulcer healing.
Number of ulcers completely healed within a specific time period (we assumed that the period of time in which healing occurred was the duration of the trial unless otherwise stated).
Secondary outcomes
Health‐related quality of life (measured using a standardised generic questionnaire such as EQ‐5D, SF‐36, SF‐12 or SF‐6 or disease‐specific questionnaire). We did not include ad‐hoc measures of quality of life which are likely not to be validated and would not be common to multiple trials.
Number and level of amputations.
Adverse events, including pain (measured using survey/questionnaire/data capture process or visual analogue scale).
Cost (including measurements of resource use such as number of dressing changes and nurse time).
Ulcer recurrence.
Change in ulcer area expressed as absolute changes (e.g. surface area changes in cm2 since baseline) or relative changes (e.g. percentage change in area relative to baseline).
Search methods for identification of studies
For the search methods used in the original version of this review see Appendix 1
Electronic searches
For this first update we searched the following databases in April 2013:
The Cochrane Wounds Group Specialised Register (searched 11 April 2013);
The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2013, Issue 3); Ovid MEDLINE (1950 to March Week 4 2013);
Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations, April 10, 2013);
Ovid EMBASE (1980 to 2011 April 05);
EBSCO CINAHL (1982 to 4 April 2013).
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) using the following exploded MeSH headings and keywords:
#1 MeSH descriptor Occlusive Dressings explode all trees #2 MeSH descriptor Biological Dressings explode all trees #3 MeSH descriptor Alginates explode all trees #4 MeSH descriptor Hydrogels explode all trees #5 MeSH descriptor Silver explode all trees #6 MeSH descriptor Honey explode all trees #7 (dressing* or alginate* or hydrogel* or "foam" or "bead" or "film" or "films" or tulle or gauze or non‐adherent or "non adherent" or silver or honey or matrix):ti,ab,kw #8 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7) #9 MeSH descriptor Foot Ulcer explode all trees #10 MeSH descriptor Diabetic Foot explode all trees #11 diabet* NEAR/3 ulcer*:ti,ab,kw #12 diabet* NEAR/3 (foot or feet):ti,ab,kw #13 diabet* NEAR/3 wound*:ti,ab,kw #14 (#9 OR #10 OR #11 OR #12 OR #13) #15 (#8 AND #14)
We adapted this strategy to search Ovid MEDLINE, Ovid EMBASE and EBSCO CINAHL. We combined the Ovid MEDLINE search with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐ and precision‐maximising version (2008 revision) (Lefebvre 2011). We combined the EMBASE and CINAHL searches with the trial filters developed by the Scottish Intercollegiate Guidelines Network (SIGN 2009). There were no restrictions on the basis of date or language of publication.
Searching other resources
In the original version of this review we attempted to contact researchers to obtain any unpublished data when needed. We also searched the reference lists of the included studies and previous systematic reviews. We contacted appropriate manufacturers (Smith & Nephew, Convatec Ltd, Mölnlycke Health Care, 3M Healthcare, Coloplast Ltd) for details of any unpublished studies.
Data collection and analysis
Selection of studies
Two review authors independently assessed the titles and abstracts of retrieved studies for relevance. After this initial assessment, we obtained all studies felt to be potentially relevant in full. Two review authors then independently checked the full papers for eligibility, with disagreements resolved by discussion and, where required, the input of a third review author. We recorded all reasons for exclusion.
Data extraction and management
We extracted and summarised details of the eligible studies using a data extraction sheet. Two review authors extracted data independently and resolved disagreements by discussion. Where data were missing from reports we attempted to contact the study authors to obtain the missing information. We included studies published in duplicate once but maximally extracted data. We extracted the following data:
country of origin;
type of ulcer;
unit of investigation (per patient) ‐ single ulcer or foot or patient or multiple ulcers on the same patient;
care setting;
number of participants randomised to each trial arm;
eligibility criteria and key baseline participant data;
details of the dressing/treatment regimen received by each group;
details of any co‐interventions;
primary and secondary outcome(s) (with definitions);
outcome data for primary and secondary outcomes (by group);
duration of follow up;
number of withdrawals (by group);
adverse events, including amputation; and
source of funding.
Assessment of risk of bias in included studies
Two review authors independently assessed each included study using the Cochrane Collaboration tool for assessing risk of bias (Higgins 2009). This tool addresses six specific domains, namely sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other issues (e.g. extreme baseline imbalance, issues with unit of investigation) (see Appendix 2 for details of the criteria on which the judgement was based). We assessed blinding and completeness of outcome data for each outcome separately. We completed a 'Risk of bias' table for each eligible study. We resolved disagreements about risk of bias assessment by discussion. Where a lack of reported information resulted in an unclear decision, where possible we contacted authors for clarification.
We have presented our assessment of risk of bias findings using a 'Risk of bias' summary figure, which presents all of the judgements in a cross‐tabulation of study by entry. This display of internal validity indicates the weight the reader may give the results of each study. We also aimed to present this assessment in the narrative review.
We classified trials as being at high risk of bias if they are rated 'high' for any of three key criteria (randomisation sequence, allocation concealment and blinded outcome assessment).
Measures of treatment effect
Where possible, we present the outcome results for each trial with 95% confidence intervals (CI). We report estimates for dichotomous outcomes (e.g. ulcers healed during time period) as risk ratio (RR). We used the RR rather than odds ratio (OR), since ORs (when interpreted as RR) can give an inflated impression of the effect size when event rates are high, as is the case for many trials reporting healing of chronic wounds (Deeks 2002). We planned to reported outcomes relating to continuous data (e.g. percentage change in ulcer area) as mean difference (MD) and overall effect size (with 95% CI calculated). Where a study reported time to healing data (the probability of healing over a consecutive time period) we planned to report and plot these data (where possible) using hazard ratio estimates. If studies reporting time‐to‐event data (e.g. time to healing) did not report a hazard ratio or reported these data incorrectly as a continuous variable then, where feasible, we planned to estimate this using other reported outcomes such as the numbers of events through the application of available statistical methods (Tierney 2007).
Unit of analysis issues
We recorded whether trials measured outcomes in relation to an ulcer, a foot, a participant or whether multiple ulcers on the same participant are studied. We also recorded where multiple ulcers on a participant had been (incorrectly) treated as independent in a study, rather than within‐patient analysis methods being applied. We have recorded this as part of the risk of bias assessment. Unless otherwise, where the number of wounds appeared to equal the number of participants we treated the ulcer as the unit of analysis in this review.
Dealing with missing data
Missing data are common in trial reports. Excluding participants post‐randomisation from the analysis or ignoring those participants lost to follow up can, in effect, compromise the process of randomisation and thus potentially introduce bias into the trial. In individual studies, where "proportion of ulcers healed data" were presented, we assumed that where randomised participants were not included in an analysis, their wound did not heal (that is, they will be considered in the denominator but not the numerator). Where a trial did not specify participant group numbers prior to dropout, we planned to present only complete case data. We planned to present data for time to healing, area change and for all secondary outcomes as a complete case analysis.
Assessment of heterogeneity
We considered both clinical and statistical heterogeneity. Wherever appropriate, we pooled data using meta‐analysis (conducted using RevMan 5.1 (RevMan 2011)), that is where studies appeared similar in terms of level of participants, intervention type and duration and outcome type. We assessed statistical heterogeneity using the Chi² test (a significance level of P < 0.1 was considered to indicate heterogeneity) and the I² statistic (Higgins 2003). The I² statistic examines the percentage of total variation across studies due to heterogeneity rather than to chance. Values of I² over 50% indicate a high level of heterogeneity. In the absence of clinical heterogeneity and in the presence of statistical heterogeneity (I² over 50%), we used a random‐effects model. However, we did not pool studies where heterogeneity was very high (I² over 50%). Where there was no clinical or statistical heterogeneity we envisaged using a fixed‐effect model.
Data synthesis
We combined studies using a narrative overview with meta‐analyses of outcome data where appropriate (in RevMan 5.1). The decision to include studies in a meta‐analysis depended on the availability of treatment effect data and assessment of heterogeneity. For time‐to‐event data, we planned to plot log rank observed minus expected events estimates using a fixed‐effect model (a random‐effects model is not available for this analysis in RevMan 5.1). Where relevant and possible we planned to conduct sensitivity analysis to investigate the potential impact of studies at high risk of bias on pooled results.
Results
Description of studies
See Characteristics of included studies; Characteristics of excluded studies.
Results of the search
The systematic search yielded 346 abstracts which we screened for potential inclusion in the review. Of these, we obtained 103 reports in full (for 84 studies) for a more detailed assessment and five studies were eligible for inclusion in the review. No eligible studies were obtained from the five commercial companies that were contacted. We are not aware of any relevant on‐going studies (checked ISRCTN register 25 April 2013). The update search conducted in April 2013 yielded 116 citations of which two studies was obtained for further information: Turns 2012 (excluded) and Wang 2012 (awaiting assessment as requires translation from Chinese).
Included studies
We included five studies (446 participants) in this review (D'Hemecourt 1998; Jensen 1998; Markevich 2000; Vandeputte 1997; Whalley 2001): a summary is presented in Table 5. One study was single‐centred (Jensen 1998) and three were multi‐centred (D'Hemecourt 1998; Markevich 2000; Whalley 2001); the remaining study did not detail the number of centres. Two studies were undertaken in the USA (D'Hemecourt 1998; Jensen 1998); one in Belgium (Vandeputte 1997) and one study was multi‐national, taking place in Spain, UK, Lithuania and Belgium (Whalley 2001). Markevich 2000 did not detail country(ies) of conduct.
1. Summary of studies.
| First author | Group A | Group B | Group C | Duration of follow up | % healed data |
| D'Hemecourt 1998 | Good wound care and NaCMC gel; a thin layer was applied daily for morning dressing change for 20 weeks or until ulcers healed No brand information |
Good wound care (daily wet‐to‐moist saline dressing changes every 12 hours, sharp debridement of the ulcer when deemed necessary by the investigator, systemic control of infection if present, and off‐loading of pressure) No brand information |
Good wound care and becaplermin gel (100 µg/g) | 20 weeks | Yes |
| Jensen 1998 | Hydrogel dressing (Carrington Laboratories, Inc) | Gauze pad soaked in sterile saline | 16 weeks | Yes | |
| Markevich 2000 | Hydrogel (no data on brand of hydrogel) | Larvae of the green‐bottle fly Lucilia sericata (larval therapy). Absorbent dressings were used over the larvae and were changed as required. | 10 days | Yes | |
| Vandeputte 1997 | Hydrogel dressing (Elasto gel with 65% glycerol, 17.5% water and 17.5% polyacrylamide) | Dry gauze twice a day | 12 weeks | Yes | |
| Whalley 2001 | Purilon gel (Coloplast A/S) | IntraSite Gel (S&N Hlth) | 10 weeks | Yes |
All studies were undertaken in adults with diabetes, with one study including people with both type 1 or type 2 diabetes (D'Hemecourt 1998). This study also included participants with at least one ulcer of Wagner grade 3 or 4, where as Whalley 2001 included only ulcers that were Wagner grade 1 or 2 ulcers and Jensen 1998 only included Wagner grade 2 ulcers. One study only included participants with ulcers that were neuropathic (Whalley 2001). Vandeputte 1997 specified that it allowed entry to people with infected non‐neuropathic and sloughy ulcers whereas Jensen 1998 only included participants with no signs of ulcer infection, and a documented blood supply consistent will the ability to heal (no further information or measures provided). In general it seems that a wide range of ulcer types were evaluated across these studies from potentially more complex wounds (D'Hemecourt 1998; Vandeputte 1997) to potentially less complex (Jensen 1998). The duration of trial follow up ranged from 10 days (Markevich 2000) to 20 weeks (D'Hemecourt 1998), details presented in Table 5. Of the five included studies, four were two‐arm and one was three‐arm (D'Hemecourt 1998). All studies reported the number of ulcers healed. Mean time to healing was reported in Jensen 1998 and D'Hemecourt 1998 (summary estimate not provided). Adverse event reporting did not appear systematic in most studies (potentially with the exception of D'Hemecourt 1998) although this was difficult to assess, particularly for Markevich 2000 and Whalley 2001 which were reported as conference abstracts only.
Excluded studies
We excluded 79 studies from the review (an additional exclude was added from the update search). The main reasons for exclusion were: the study was not randomised (n = 9), no single, identifiable dressing type was evaluated (n = 11); another intervention, not a dressing, differed between study groups (n = 26); the dressing(s) evaluated were not hydrogel (n = 26). Another reason was recorded for seven studies.
Risk of bias in included studies
We classified studies rated 'high risk' for any of three key domains: randomisation sequence, allocation concealment and blinded outcome assessment, as being at high risk of bias (Characteristics of included studies; Figure 1; Figure 2). We rated all five studies as being at unclear risk of bias due to poor reporting.
1.
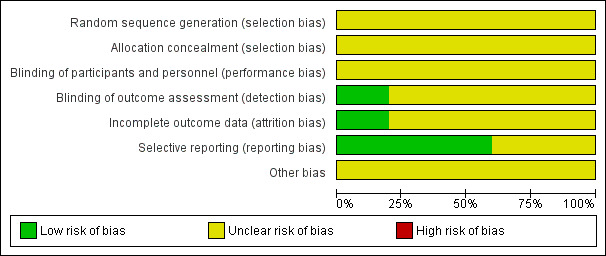
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
2.
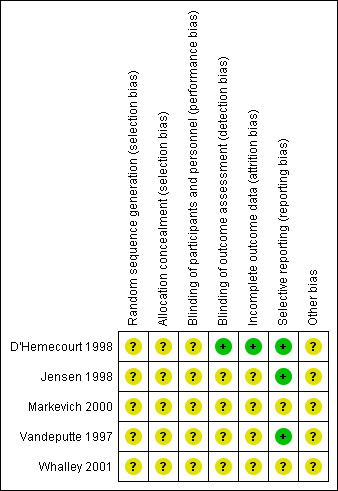
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Adequacy of randomisation process
All five studies were described as "randomised", however, none reported the method used to generate randomisation sequence and hence we judged all to be unclear for this domain.
Allocation concealment
None of the studies reported the allocation procedure such that we could assess the degree of concealment and hence we judged all trials to be unclear for this domain.
Blinding
Assessment of wound healing can be subjective and thus has the potential to be influenced if the outcome assessor is aware of the treatment allocation. In this review we focused on whether the studies had conducted blinded outcome assessment. We judged D'Hemecourt 1998 to be at low risk of bias and the other studies to be unclear for this domain.
Incomplete outcome data
Whilst D'Hemecourt 1998 reported some trial loss to follow up it stated that "analysis of efficacy was based on the intention to treat population, which included patients who were randomised to treatment, received at least one treatment and had any post‐baseline data". All numbers presented in the analysis matched the number of participants randomised it was deemed that an intention‐to‐treat (ITT) analysis had been conducted and the study was judged to be at low risk of bias for this domain. Jensen 1998 reported that five participants of 31(16%) were excluded post‐randomisation; it seems that the authors conducted an ITT analysis but this is not clear. Likewise the remaining studies did not report enough information to make a judgement about ITT analysis and so were classed as unclear.
Selective reporting
All studies reported outcomes adequately and we deemed them to be at unclear or low risk of bias. However, it is important to note that judgement for this domain may be of limited value given it was made at face value based on the reporting of outcomes in the results that were described in the methods. Study reports were not compared to study protocols, which were not actively sought.
Other potential sources of bias
One study was funded by a commercial organisation (Jensen 1998). Funding for the remaining four studies was unclear. All included studies reported no or limited baseline data thus the potential for imbalance was unclear.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4
Dressing compared with non‐dressing
Dressing compared with larval therapy
Comparison 1: hydrogel dressing compared with larval therapy (one trial; 140 participants)
Markevich 2000 was a two‐arm study with 140 participants that compared a hydrogel dressing with the application of the larvae of the green‐bottle fly Lucilia sericata (larval therapy) (Table 5).
Primary outcome: ulcer healing
Markevich 2000 had a follow‐up period of 10 days, suggesting that the primary outcome was debridement rather than complete healing (the study also measured number of wounds with granulation tissue covering 50% of the wound); explaining the low numbers of healing events in this study. There was no statistically significant difference in the number of ulcers healed in the hydrogel‐dressed group (2/70; 3%) compared with the larval therapy‐treated group (5/70; 7%): risk ratio (RR) 0.40, 95% confidence interval (CI) 0.08 to 1.99 (Analysis 1.1). The proportion of participants with more than a 50% reduction in wound area was 27% in the hydrogel‐dressed group and 51% in the larval therapy‐treated group (values and standard deviation (SD) not reported; attempts to contact author unsuccessful).
1.1. Analysis.
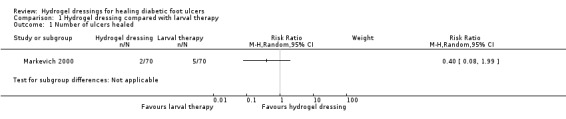
Comparison 1 Hydrogel dressing compared with larval therapy, Outcome 1 Number of ulcers healed.
Secondary outcomes: not reported
Summary: hydrogel dressing compared with larval therapy
Limited data from one small study with a very short follow up period found no difference in numbers of ulcers healed between larval therapy‐treated ulcers and hydrogel‐dressed ulcers.
Dressing compared with platelet‐derived growth factor
Comparison 2: hydrogel dressing compared with platelet‐derived growth factor (one trial; 104 participants)
D'Hemecourt 1998 was a three‐arm study (two groups relevant to this comparison) with a maximum follow up of 20 weeks. The two relevant arms contained 104 participants and compared a hydrogel dressing with a platelet‐derived growth factor (becaplermin gel, 100 µg/g). There was no statistically significant difference in the number of ulcers healed in the hydrogel‐dressed ulcers (25/70; 36%) compared with the growth‐factor‐treated ulcers (15/34; 44%): RR 0.81, 95% CI 0.50 to 1.32 (Analysis 2.1).
2.1. Analysis.
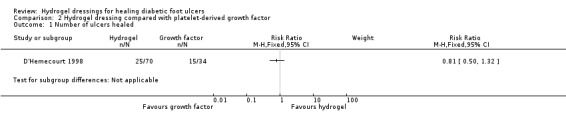
Comparison 2 Hydrogel dressing compared with platelet‐derived growth factor, Outcome 1 Number of ulcers healed.
Summary: hydrogel dressing compared with platelet‐derived growth factor
There was no statistically significant difference in healing between ulcers treated with hydrogel and platelet‐derived growth factors.
Dressing compared with dressing
Advanced wound dressing compared with basic wound contact dressing
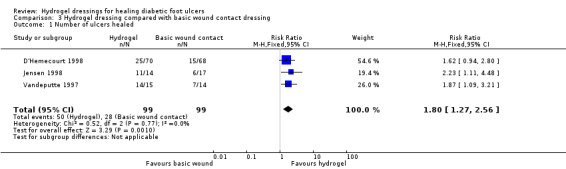
Comparison 3: hydrogel dressing compared with basic wound contact dressing (three trials; 198 participants)
Three studies (D'Hemecourt 1998; Jensen 1998; Vandeputte 1997) compared a hydrogel with a basic wound contact dressing (Table 5). D'Hemecourt 1998 was a three‐arm study, with two arms relevant to this comparison that contained 138 participants and compared a hydrogel with a wet‐to‐moist saline dressing. Jensen 1998 was a two‐arm study with 31 participants that compared a hydrogel dressing with gauze pad soaked in sterile saline. Vandeputte 1997 was a two‐arm study with 29 participants that compared a hydrogel dressing (elasto gel with 65% glycerol, 17.5% water and 17.5% polyacrylamide) with dry gauze.
Primary outcome: ulcer healing
D'Hemecourt 1998 had a maximum follow‐up of 20 weeks . There was no statistically significant difference in the number of ulcers healed in the hydrogel‐dressed group (25/70; 36%) compared with the basic wound contact dressed group (15/68; 22%): RR 1.62, 95% CI 0.94 to 2.80 (Analysis 3.1). This study undertook blinded outcome assessment. Additionally, whilst 41 (24%) of study participants were reported as withdrawn, the report confirms that the intention‐to‐treat population was the primary population for analysis.
3.1. Analysis.
Comparison 3 Hydrogel dressing compared with basic wound contact dressing, Outcome 1 Number of ulcers healed.
Jensen 1998 had a maximum follow‐up of 16 weeks. Significantly more ulcers healed in the hydrogel‐dressed group (11/14; 79%) compared with the basic wound contact dressed‐group (6/17; 35%): RR 2.23, 95% CI 1.11 to 4.48 (Analysis 3.1). Five participants were not included in the analysis with one participant lost from the hydrogel‐dressed group and four from the basic wound contact‐dressed group. As explained earlier, we have included these participants in our analysis as denominators but not numerators (i.e. assumed not to have healed). The mean time to healing was reported as 10.3 weeks in the hydrogel‐dressed group compared with 11.69 weeks in the basic wound contact‐dressed group. In general median and not mean time to healing is the best time to healing summary estimate. The use of mean vales can result in biased estimates ‐ since to calculate mean time to healing either all participants must have healed and/or assumptions need to be made about the shape of the survival curve.
Vandeputte 1997 had a follow‐up of 12 weeks. Significantly more ulcers healed in the hydrogel‐dressed group (14/15; 93%) compared with the basic wound contact‐dressed group (7/14; 50%): RR 1.87, 95% CI 1.09 to 3.21 (Analysis 3.1).
We pooled ulcer healed data from these three studies (D'Hemecourt 1998; Jensen 1998; Vandeputte 1997) with a total of 198 participants using a fixed‐effect model (Chi²: P = 0.77; I² = 0%) (Analysis 3.1). Significantly more ulcers healed in the hydrogel‐dressed groups compared with the basic wound contact‐dressed groups: RR 1.80, 95% 1.27 to 2.56. However, we stress that the baseline ulcer grade was different in these trials: D'Hemecourt 1998 (grade 3 and 4), Jensen 1998 (grade 2) and Vandeputte 1997 (not specific about grade but did include more severe ulcers), as was trial follow‐up time. These differences may partly explain the difference in overall ulcer healing that is observed in these studies (29% over 20 weeks in D'Hemecourt 1998 and 55% over 16 weeks in Jensen 1998).
Secondary outcomes:
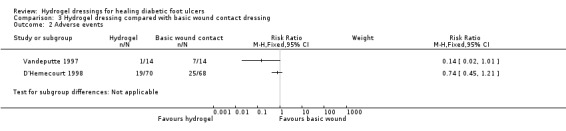
D'Hemecourt 1998: reported the number of wound‐related adverse events. There was no statistically significant difference in number of adverse events between the hydrogel‐dressed group (19/70; 27%) and the basic wound contact‐dressed group (25/68; 37%): RR 0.74, 95% CI 0.45 to 1.21 (Analysis 3.2). Neither was there a statistically significant difference in number of participants reporting pain as an adverse event between the groups (11/70; 16% in the hydrogel‐treated group compared with 10/68; 15%): RR 1.07, 95% CI 0.49 to 2.35 (Analysis 3.3).
3.2. Analysis.
Comparison 3 Hydrogel dressing compared with basic wound contact dressing, Outcome 2 Adverse events.
3.3. Analysis.
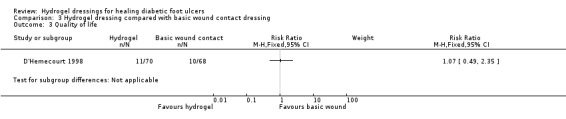
Comparison 3 Hydrogel dressing compared with basic wound contact dressing, Outcome 3 Quality of life.
Jensen 1998: there were no amputations in the hydrogel‐dressed group compared with one amputation in the basic wound contract‐dressed group. Adverse events recording was minimal with three specific adverse events being reported for the hydrogel‐dressed group compared with four for the basic wound contact‐dressed group. The average cost per day of treatment in US Dollars was USD 7.01 in the hydrogel‐dressed group and USD 12.28 in the basic wound contact‐dressed group. However, these costs were not collected or compared as part of a full economic evaluation.
Vandeputte 1997: reported the number of infection related complications in each study group. There was no statistically significant difference in number of events between the hydrogel‐dressed group (1/15; 7%) compared with the basic wound contact‐dressed group (7/14; 50%): RR 0.14, 95% 0.02 to 1.01. It is important to remember that this study did not have blinded outcome assessment and neither were the mechanisms for reporting adverse events clearly detailed.
Given the lack of methodological detail regarding the collection of adverse event data and the differences in the type of data presented, we did not pool these data.
Summary: hydrogel dressings compared with basic wound contact dressing
Data from three studies (n=198) found a statistically significant increase in the healing of diabetic foot ulcers in hydrogel‐treated ulcers compared with those treated with basic wound contact dressings. This difference is driven by two small trials of unclear risk of bias.
Advanced dressing compared with advanced dressing
Comparison 4: hydrogel dressing compared with hydrogel dressing (one trial; 74 participants)
Primary outcome: ulcer healing
Whalley 2001 recruited 74 participants and compared one type of hydrogel (Purilon) with another (Intrasite) for a maximum of 10 weeks. Data were only available from conference abstracts.
Whilst 74 participants were randomised, data were only presented for 66 of these. The study reports that 35% of ulcers achieved complete healing in the Purilon group compared with 19% in the Intrasite group. The numbers of people in each group were not reported in the abstract (attempts to contact author unsuccessful), nor was the baseline comparability of the participants by treatment group which makes the data impossible to interpret with confidence,
Secondary outcomes:
The direct cost of wound treatments to reach a 75% reduction in wound area were reported to be 32% lower for the Purilon hydrogel. However, no further details are presented and we must stress that this is a very limited analysis that should not be interpreted as an economic evaluation.
Summary: hydrogel dressing compared with hydrogel dressing
There was no evidence that more ulcers dressed with a Purilon hydrogel healed within 10 weeks compared with Intrasite‐dressed ulcers.
Summary of Findings Table
We have included a Summary of Findings table (Table 1; Table 2; Table 3; Table 4): this aims to give a concise overview and synthesis of the volume and quality of the evidence for this comparison. The Summary of Findings table confirm our conclusion that the quality of evidence is of moderate quality where hydrogel is compared with basic wound contact dressings: we note that according to the GRADE definition this still means that "Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate." We also note that the three studies in this comparison had limited details reported to inform the individual risk of bias assessments. We did not downgrade the evidence under the GRADE risk of bias for this comparison (as there were no domains assessed at high risk of bias) ‐ however, a large number were unclear and this must be acknowledged. The quality of estimates for other comparisons is considered low.
Discussion
Summary of main results
This review has identified, appraised and presented all available RCT evidence (five studies) regarding the clinical effectiveness of hydrogel wound dressings in the treatment of diabetic foot ulcers. When data from three studies (20, 16 and 12 weeks follow‐up; n = 198) were pooled there was a statistically significant increase in ulcer healing with hydrogel compared with basic wound contact dressings. All studies were at unclear risk of bias due to poor reporting of trial methods. It is important to note that included ulcers in D'Hemecourt 1998 were predominantly grade 3, where as Jensen 1998 only included grade 2 ulcers. Ulcer grade was not specified in Vandeputte 1997 but based on the inclusion criteria there was the potential for more serious ulcers to be included. The different ulcer grades may explain why study healing was lower in D'Hemecourt 1998 compared to Jensen 1998 even though D'Hemecourt 1998 had a longer follow‐up time. There is no evidence to inform clinicians as to how hydrogel compares with other advanced dressings in terms of clinical and/or cost‐effectiveness.
There was no evidence of any difference between hydrogel and larval therapy or platelet derived growth factor, nor between different brands of hydrogel in terms of ulcer healing.
Quality of the evidence
We deemed all studies to be at unclear risk of bias given the lack of methodological detail reported. Many included studies did not follow good practice conduct and reporting guidelines, e.g. CONSORT (Schulz 2010). Key areas of good practice are the robust generation of a randomisation sequence, for example, computer‐generated, robust allocation concealment, for example the use of a telephone randomisation service, and blinded outcome assessment where possible. All this information should be clearly stated in the study report as all trial authors should anticipate the inclusion of their trials in systematic reviews. In terms of analysis, where possible, data from all participants should be included, that is an intention‐to‐treat analysis is conducted. Steps should be taken during trial conduct to prevent missing data as far as is possible. Where missing data is an issue, imputation methods should be considered and clearly reported when implemented. Finally, where possible, robust economic data should be collected.
Potential biases in the review process
The review considered as much evidence as it was possible to obtain, including studies that were not published in English‐language journals. We contacted relevant pharmaceutical companies but did not receive any relevant RCT data from them. There is the potential for publication bias. It is also important to note that three studies are awaiting assessment and may be included in future reviews. However, we anticipate this is unlikely for the majority of these studies.
Agreements and disagreements with other studies or reviews
Prior to this systematic review, the most recent and relevant review regarding the healing of diabetic foot ulcers (Hinchliffe 2008) included one RCT (Jensen 1998 also included here) that compared a hydrogel dressing in the treatment of diabetic foot ulcers. No conclusions were made regarding the results of this study. However, our review included and pooled data from the same three studies (D'Hemecourt 1998; Jensen 1998; Vandeputte 1997) as another Cochrane Review (Edwards 2010), which had the primary aim of assessing the debridement of diabetic foot ulcers. Thus Edwards 2010 also suggested that hydrogel may be more effective than basic contact wound dressings in the treatment of diabetic foot ulcers. However, caution must be advised in changing clinical practice on the basis of findings informed largely by small trials of unknown risk of bias. Clinicians should also be aware of the types of ulcers that were included in each trial.
Authors' conclusions
Implications for practice.
Based on a comprehensive review of current evidence hydrogel dressings may be better than basic contact wound dressings at healing non‐complex diabetic foot ulcers. However, any potential change in practice regarding the use of hydrogels would need to be informed by clinical experience and acknowledge the uncertainty around this decision due to the quality of data used to inform these analyses. It is also important to note that this review was unable to present information on how hydrogel dressings compare with other advanced wound dressings. Thus, practitioners may elect to consider other characteristics such as cost and symptom management properties when choosing between alternatives
Implications for research.
Current evidence suggests that hydrogel may be better than basic contact wound dressings at healing diabetic foot ulcers, although there is some uncertainty around this decision. There is no available evidence regarding the effectiveness of hydrogel with other advanced dressing types, thus further research may be warranted. Given the large number of dressing options, the design of future trials should be driven by the questions of high priority to patients and other decision‐makers. It is also important for research to ensure that the outcomes that are collected in research studies are those that matter to patients, carers and health professionals. It may be that dressings should be viewed as management tools and that other treatments that address patient lifestyle issues merit the main focus in terms of future research. Where trials are conducted, good practice guidelines must be followed in their design, implementation and reporting. Further reviews are being conducted to synthesise evidence regarding the effect of other dressings on the treatment of diabetic foot ulcers. It would then be useful to conduct further evidence synthesis (overview of reviews, mixed treatment comparisons or both) to aid decision‐making regarding the choice of dressings for diabetic foot ulcers across all available options.
What's new
| Date | Event | Description |
|---|---|---|
| 25 June 2013 | New search has been performed | First update, new search, no new trials identified. |
| 25 June 2013 | New citation required but conclusions have not changed | Summary of findings table included, conclusions not changed. |
Acknowledgements
The authors would like to thank the following people who reviewed the protocol for clarity, readability and rigour: Wounds Group editors (Julie Bruce, Andrea Nelson and Gill Worthy) and peer referees (David Armstrong, Duncan Chambers and Janet Yarrow). In addition we would like to acknowledge the contribution of the copy editor Jenny Bellorini.
Appendices
Appendix 1. Search methods used in the original version of this review ‐ June 2011
Electronic searches
We searched the following databases:
the Cochrane Wounds Group Specialised Register (searched 10 June 2011);
the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2011, Issue 2);
Ovid MEDLINE (1950 to June Week 1 2011);
Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations, June 8, 2011);
Ovid EMBASE (1980 to 2011 Week 22); and
EBSCO CINAHL (1982 to 3 June 2011).
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) using the following exploded MeSH headings and keywords:
#1 MeSH descriptor Occlusive Dressings explode all trees #2 MeSH descriptor Biological Dressings explode all trees #3 MeSH descriptor Alginates explode all trees #4 MeSH descriptor Hydrogels explode all trees #5 MeSH descriptor Silver explode all trees #6 MeSH descriptor Honey explode all trees #7 (dressing* or alginate* or hydrogel* or "foam" or "bead" or "film" or "films" or tulle or gauze or non‐adherent or "non adherent" or silver or honey or matrix):ti,ab,kw #8 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7) #9 MeSH descriptor Foot Ulcer explode all trees #10 MeSH descriptor Diabetic Foot explode all trees #11 diabet* NEAR/3 ulcer*:ti,ab,kw #12 diabet* NEAR/3 (foot or feet):ti,ab,kw #13 diabet* NEAR/3 wound*:ti,ab,kw #14 (#9 OR #10 OR #11 OR #12 OR #13) #15 (#8 AND #14)
We adapted this strategy to search Ovid MEDLINE, Ovid EMBASE and EBSCO CINAHL. We combined the Ovid MEDLINE search with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐ and precision‐maximising version (2008 revision). We combined the EMBASE and CINAHL searches with the trial filters developed by the Scottish Intercollegiate Guidelines Network. There were no restrictions on the basis of date or language of publication.
Searching other resources
We attempted to contact researchers to obtain any unpublished data when needed. We also searched the reference lists of the included studies and previous systematic reviews. We contacted appropriate manufacturers (Smith & Nephew, Convatec Ltd, Mölnlycke Health Care, 3M Healthcare, Coloplast Ltd) for details of any unpublished studies. We also checked for ongoing studies in the ISRCTN register.
Appendix 2. Risk of bias criteria
1. Was the allocation sequence randomly generated?
Low risk of bias
The investigators describe a random component in the sequence generation process such as: referring to a random number table; using a computer random number generator; coin tossing; shuffling cards or envelopes; throwing dice; drawing of lots.
High risk of bias
The investigators describe a non‐random component in the sequence generation process. Usually, the description would involve some systematic, non‐random approach, for example: sequence generated by odd or even date of birth; sequence generated by some rule based on date (or day) of admission; sequence generated by some rule based on hospital or clinic record number.
Unclear
Insufficient information about the sequence generation process to permit judgement of low or high risk of bias.
2. Was the treatment allocation adequately concealed?
Low risk of bias
Participants and investigators enrolling participants could not foresee assignment because one of the following, or an equivalent method, was used to conceal allocation: central allocation (including telephone, web‐based and pharmacy‐controlled randomisation); sequentially‐numbered drug containers of identical appearance; sequentially‐numbered, opaque, sealed envelopes.
High risk of bias
Participants or investigators enrolling participants could possibly foresee assignments and thus introduce selection bias, such as allocation based on: using an open random allocation schedule (e.g. a list of random numbers); assignment envelopes were used without appropriate safeguards (e.g. if envelopes were unsealed or nonopaque or not sequentially numbered); alternation or rotation; date of birth; case record number; any other explicitly unconcealed procedure.
Unclear
Insufficient information to permit judgement of low or high risk of bias. This is usually the case if the method of concealment is not described or not described in sufficient detail to allow a definite judgement, for example if the use of assignment envelopes is described, but it remains unclear whether envelopes were sequentially numbered, opaque and sealed.
3. Blinding ‐ was knowledge of the allocated interventions adequately prevented during the study?
Low risk of bias
Any one of the following.
No blinding, but the review authors judge that the outcome and the outcome measurement are not likely to be influenced by lack of blinding.
Blinding of participants and key study personnel ensured, and unlikely that the blinding could have been broken.
Either participants or some key study personnel were not blinded, but outcome assessment was blinded and the non‐blinding of others unlikely to introduce bias.
High risk of bias
Any one of the following.
No blinding or incomplete blinding, and the outcome or outcome measurement is likely to be influenced by lack of blinding.
Blinding of key study participants and personnel attempted, but likely that the blinding could have been broken.
Either participants or some key study personnel were not blinded, and the non‐blinding of others likely to introduce bias.
Unclear
Any one of the following.
Insufficient information to permit judgement of low or high risk of bias.
The study did not address this outcome.
4. Were incomplete outcome data adequately addressed?
Low risk of bias
Any one of the following.
No missing outcome data.
Reasons for missing outcome data unlikely to be related to true outcome (for survival data, censoring unlikely to be introducing bias).
Missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups.
For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically relevant impact on the intervention effect estimate.
For continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes not enough to have a clinically relevant impact on observed effect size.
Missing data have been imputed using appropriate methods.
High risk of bias
Any one of the following.
Reason for missing outcome data likely to be related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups.
For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk enough to induce clinically relevant bias in intervention effect estimate.
For continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes enough to induce clinically relevant bias in observed effect size.
‘As‐treated’ analysis done with substantial departure of the intervention received from that assigned at randomisation.
Potentially inappropriate application of simple imputation.
Unclear
Any one of the following.
Insufficient reporting of attrition/exclusions to permit judgement of low or high risk of bias (e.g. number randomised not stated, no reasons for missing data provided).
The study did not address this outcome.
5. Are reports of the study free of suggestion of selective outcome reporting?
Low risk of bias
Any of the following.
The study protocol is available and all of the study’s pre‐specified (primary and secondary) outcomes that are of interest in the review have been reported in the pre‐specified way.
The study protocol is not available but it is clear that the published reports include all expected outcomes, including those that were pre‐specified (convincing text of this nature may be uncommon).
High risk of bias
Any one of the following.
Not all of the study’s pre‐specified primary outcomes have been reported.
One or more primary outcomes is reported using measurements, analysis methods or subsets of the data (e.g. subscales) that were not pre‐specified.
One or more reported primary outcomes were not pre‐specified (unless clear justification for their reporting is provided, such as an unexpected adverse effect).
One or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis.
The study report fails to include results for a key outcome that would be expected to have been reported for such a study.
Unclear
Insufficient information to permit judgement of low or high risk of bias. It is likely that the majority of studies will fall into this category.
6. Other sources of potential bias
Low risk of bias
The study appears to be free of other sources of bias.
High risk of bias
There is at least one important risk of bias. For example, the study:
had a potential source of bias related to the specific study design used; or
had extreme baseline imbalance; or
has been claimed to have been fraudulent; or
had some other problem.
Unclear
There may be a risk of bias, but there is either:
insufficient information to assess whether an important risk of bias exists; or
insufficient rationale or evidence that an identified problem will introduce bias.
Data and analyses
Comparison 1. Hydrogel dressing compared with larval therapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of ulcers healed | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only |
Comparison 2. Hydrogel dressing compared with platelet‐derived growth factor.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of ulcers healed | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 3. Hydrogel dressing compared with basic wound contact dressing.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of ulcers healed | 3 | 198 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.80 [1.27, 2.56] |
| 2 Adverse events | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3 Quality of life | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only |
Comparison 4. Trial data.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Trial data | Other data | No numeric data |
4.1. Analysis.
Comparison 4 Trial data, Outcome 1 Trial data.
| Trial data | |||||||
|---|---|---|---|---|---|---|---|
| Study | Groups | Primary outcome: ulcer healing | Secondary: health‐related quality of life | Number and level of amputations | Adverse events, including pain | Cost | Ulcer recurrence |
| D'Hemecourt 1998 | Group A (n = 70): good wound care and NaCMC gel Group B (n = 68): good wound care Group C (n = 34): good wound care and becaplermin gel (100 µg/g) |
Number of ulcers healed:
Group A: 25/70 Group B: 15/68 Group C: 15/34 Time to complete healing (days): Group A: 98* Group B: 141* Group C: 85* *It is unclear if these are mean or median times to healing. Although a life plot table presented suggests that median time to healing was not reached in any group. Explained by the very short follow‐up time of this trial ‐ 10 days. |
n/r | n/r |
Wound related:
Group A: 19/70
Group B: 25/68 Group C: 7/34 Pain reported as adverse event: Group A: 11/70 Group B: 10/68 Group C: 2/34 |
n/r | n/r |
| Jensen 1998 | Group A (n = 14): hydrogel dressing Group B (n = 17): gauze pad soaked in sterile saline | Number of ulcers healed: Group A: 11 Group B: 6 Average time to close (weeks): Group A: 10.30 Group B: 11.69 | n/r | Amputation: Group A: 0 Group B: 1 | Group A: cellulitis = 2; hospitalised for non study‐related dehydration = 1 Group B: partial amputation = 1; increased eschar formation = 2; cellulitis = 1 | Cost in US dollars/day/group including nursing time and cost of products used, it is not clear if this is per patient): Group A: $7.01 per day Group B: $12.28 per day | n/r |
| Markevich 2000 | Group A (n = 70): hydrogel (no data on brand) Group B (n = 70): larvae of the green‐bottle fly Lucilia sericata (larval therapy) |
Number of ulcers healed at 10 days:
Group A: 2/70 Group B: 5/70 Proportion of patients with granulation tissue covering over 50% of wound (numbers not supplied) Group A: 34% Group B : 60% Proportion of patients with more than a 50% reduction in wound area (numbers not supplied) Group A: 27% Group B : 51% |
n/r | n/r | n/r | n/r | n/r |
| Vandeputte 1997 | Group A (n = 15): hydrogel dressing (Elasto gel with 65% glycerol, 17.5% water and 17.5% polyacrylamide) and wounds cleansed with a dermal wound cleanser Group B (n = 14): dry gauze change twice a day and irrigated with chlorhexidine (0.05% solution) | Number of ulcers healed: Group A: 14/15 Group B: 7/14 | n/r | n/r |
Infective complications
Group A: 1/15
Group B: 7/14 Two participants in the control group died |
n/r | n/r |
| Whalley 2001 | Group A: Purilion gel Group B: IntraSite gel |
Percentage of ulcers healed at 10 weeks (numbers not presented):
Group A: 35%
Group B: 19% Change in mean wound area Group A: 2.5 cm2 (SD 3.2) to 0.6 cm2 (SD 1.1) Group B: 2.4 cm2 (SD 2.9) to 1.0 cm2 (SD 1.8) Average time to 75% reduction in wound area (days): Group A: 35 days Group B: 46 days |
Direct cost associated with wound treatment to reach 75% reduction in wound area was 32% lower for patients treated with Purilion gel | ||||
Characteristics of studies
Characteristics of included studies [ordered by study ID]
D'Hemecourt 1998.
| Methods | Multi‐centred (10 sites), 3‐arm RCT comparing good wound care with good wound care and sodium carboxymethylcellulose aqueous hydrogel (NaCMC hydrogel) and good wound care and becaplermin gel; undertaken in USA Duration of follow up: until wound healing or 20 weeks if not healed | |
| Participants | 172 patients Inclusion criteria: patients of 19 years of age or older with type 1 or type 2 diabetes mellitus. Patients with at least one full thickness (stage 3 or 4), chronic diabetic foot ulcer present for at least 8 weeks prior to the study. A target area between 1.0 and 10 cm2 was required. Transcutaneous oxygen tension (TcPO2) on the limb with the target ulcer had to be ≥ 30 mm Hg. Exclusion criteria: osteomyelitis affecting the area of the target ulcer was present. After debridement, the target ulcer area measured was < 1 cm2 or > 10 cm2. Patients having more than 3 chronic ulcers present at baseline. Patients with ulcers resulting from any cause other than diabetes or patients with cancer at the time of enrolment were excluded. Patients on concomitant medications known to affect wound healing. Women who were pregnant or nursing, or of childbearing potential and not using an acceptable method of birth control were also excluded. |
|
| Interventions | Group A (n = 70): good wound care (daily wet‐to‐moist saline dressing changes every 12 hours, sharp debridement of the ulcer when deemed necessary by the investigator, systemic control of infection if present, and off‐loading of pressure) and NaCMC hydrogel. A thin layer was applied daily for morning dressing change for 20 weeks or until ulcers healed. Group B (n = 68): good wound care Group C (n = 34): good wound care and becaplermin gel (100 µg/g). A thin layer was applied daily for morning dressing change for 20 weeks or until ulcers healed Co‐intervention: off‐loading and systemic control of infection No brand details provided for any intervention |
|
| Outcomes | Primary outcome: ulcer healing (number of ulcers healed; time to complete healing) Secondary outcomes: adverse events (wound‐related; pain reported as adverse event) Health‐related quality of life; amputation; costs and ulcer recurrence not reported | |
| Notes | Trial data: Analysis 4.1 Funding source: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned in a 2:2:1 ratio to one of three treatment groups." Comment: method of generation of random schedule not reported |
| Allocation concealment (selection bias) | Unclear risk | Comment: not stated |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "both the NaCMC gel and becaplermin gel treatment groups were conducted in double blind fashion; the group receiving good wound care alone was blinded to the investigator by a third party." Comment: insufficient information to judge if the participants were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "evaluator blinded" Comment: outcome assessors were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "...41 (24%) of study participants withdrawn from the study..." "The intention to treat population was the primary population for analysis" Comment: the presentation of data and the methods outlined suggest that an ITT analysis was done considering all randomised participants in the denominator |
| Selective reporting (reporting bias) | Low risk | Comment: based on paper only, protocol not obtained |
| Other bias | Unclear risk | Comment: some baseline differences in groups of interest for ulcer depth and duration. However, these baseline data were only presented for 24 participants so risk has been classed unclear. Funding source was not reported |
Jensen 1998.
| Methods | Single‐centre, 2‐arm RCT comparing a hydrogel dressing with a standard wet‐to‐moist saline dressing undertaken in the USA. Duration of follow up: until ulcer healing or up to 16 weeks if healing did not occur. | |
| Participants | 31 participants Inclusion criteria: no signs of infection in the ulcer or the peri‐wound tissue. Diabetic foot ulcer measuring at least 1 cm diameter, diabetic patients with foot ulcers of Wagner grade 2 defined as full thickness into subcutaneous tissue but not involving tendon, joint capsule or bone, having palpable pulse and willingness to comply to the treatment. Documented blood supply consistent with the ability to heal (no further information or measures provided), willingness to comply with protocol instructions. Exclusion criteria: not reported | |
| Interventions | Group A (n = 14): hydrogel dressing (Carrington Laboratories, Inc). An 1/8 to 1/4 inch layer of hydrogel dressing applied over the entire surface of wound Group B (n = 17): gauze pad soaked in sterile saline. The saline‐moist gauze was moistened as needed In both groups the wound was cleansed with ULTRAKLENZ wound cleanser, and the trial dressings were covered with a gauze pad, wrapped with a Kling bandage and secured with tape. Dressings were bandaged daily. Co‐intervention: all participants were initially treated with sharp debridement to remove all non‐viable tissue in and around the ulcer. All received custom made healing sandals. Instructions were given on the importance of weight distribution and offloading of the ulcer. | |
| Outcomes | Primary outcome: ulcer healing (number of ulcers healed; average time to close) Secondary outcomes: amputation; adverse events; costs Health‐related quality of life and ulcer recurrence not reported | |
| Notes | Trial data: Analysis 4.1 Funding source: Carrington Laboratories, Inc. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The patients were then randomised to receive one of the following daily protocols for the study period of up to 16 weeks." Comment: method of generation of random schedule not reported |
| Allocation concealment (selection bias) | Unclear risk | Comment: the process of randomising participants, including who did this is not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: no mention of blinding in study report |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: no mention of blinding in study report |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: in total 5 patients (of the total 31, 16%) were excluded post‐randomisation. However, it is unclear from the study report what data were included in the analysis. |
| Selective reporting (reporting bias) | Low risk | Comment: based on study report, protocol not obtained |
| Other bias | Unclear risk | Comment: funded by commercial organisation. No baseline data reported. The report states that "wound chronicity could not be adequately determined for all patients, where data were available the average ulcer duration was longer in the hydrogel group (8.9 months) than in the saline control group (3 months)". It is important to note that these data are NOT complete and so can not be used to inform the interpretation of findings. |
Markevich 2000.
| Methods | Multi‐centred, 2‐arm RCT comparing a hydrogel dressing with the use of larval therapy. The study was of 30 months duration but patient follow up was reported as 10 days. | |
| Participants | 140 patients
Inclusion and exclusion criteria not stated. Mean age reported as 53.6 +/‐ 15.4 years. Group A: 15.14 cm2 Group B: 14.9 cm2 |
|
| Interventions | Group A (n = 70): hydrogel (no data on brand of hydrogel or on frequency of dressing change) Group B (n = 70): larvae of the green‐bottle fly Lucilia sericata (larval therapy) for 72 hrs. Absorbent dressings were used over the larvae and were changed as required. |
|
| Outcomes | Primary outcome: ulcer healing (number of ulcers healed at 10 days; % patients with granulation tissue covering over 50% of wound; proportion of patients with more than a 50% reduction in wound area) Secondary outcomes: not reported | |
| Notes | Trial data: Analysis 4.1 Very short follow‐up data presented Conference abstract only Funding source: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: published abstract only ‐ method of generation of random schedule not reported. Does however state that patients were "randomly assigned" to treatment with maggots or hydrogel. |
| Allocation concealment (selection bias) | Unclear risk | Comment: published abstract only ‐ no details in the text |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: reported as double‐blind but no details in the published abstract to judge if the participants and personnel were blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: reported as double‐blind but no details in the published abstract to judge if the outcome assessors were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: published abstract only ‐ unable to assess incomplete outcome data |
| Selective reporting (reporting bias) | Unclear risk | Comment: published abstract only ‐ unable to assess selective outcome reporting |
| Other bias | Unclear risk | Comment: published abstract only. Baseline measures were reported as being balanced at baseline but only baseline mean surfaces areas were reported. |
Vandeputte 1997.
| Methods | Two‐arm RCT, comparing hydrogel dressing with dry gauze undertaken in Belgium. The maximum duration of follow up was 12 weeks (3 months). | |
| Participants | 29 participants (30 wounds) Inclusion criteria: any patient who was diabetic and had wound on his foot (neuropathic or not) was included in the trial Necrotic and infected wounds and patients who already had amputated toe were not excluded Exclusion criteria: patients receiving systemic antibiotics |
|
| Interventions | Group A (n = 15): hydrogel dressing (Elasto gel with 65% glycerol, 17.5% water and 17.5% polyacrylamide) and wounds cleansed with a dermal wound cleanser
Group B (n = 14): dry gauze change twice a day and irrigated with chlorhexidine (0.05% solution) We assumed that the dermal cleanser noted was also chlorhexidine |
|
| Outcomes | Primary outcome: ulcer healing (number of ulcers healed) Secondary outcomes: adverse events (infective complications) Health‐related quality of life; amputation; costs; and ulcer recurrence not reported | |
| Notes | Trial data: Analysis 4.1 Funding source: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were allocated to treatment groups according to a pre‐prepared randomisation listing." Comment: method of generation of random schedule not reported |
| Allocation concealment (selection bias) | Unclear risk | Comment: not stated |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "At each dressing change, the state of the ulcer and surrounding skin was assessed and the nurse also observed the ease of removal and application of dressing. The wounds were photographed every four weeks" Comment: Not clear who assessed the wounds for healing.. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Methods and Results sections report control group as n = 14. Results section states: "two patients in the control group died?" Comment: information insufficient to judge concerning patients death in control group |
| Selective reporting (reporting bias) | Low risk | Nine parameters pre‐specified in the Methods section were reported in results |
| Other bias | Unclear risk | Comment: baseline data like mean ulcer area not reported. Hence, insufficient information to assess if any important source of bias exists. Unclear if participant with more than one wound that was followed without taking this lack of independence into account in the analysis. |
Whalley 2001.
| Methods | Multi‐centred, 2‐arm RCT comparing the effectiveness of two hydrogels Purilon gel and IntraSite gel undertaken in multiple countries: Spain, UK, Lithuania and Belgium. The duration of follow up was for a minimum of 4 weeks until healing or for a maximum 10 weeks. | |
| Participants | 74 patients; (66 patients evaluated) no further data available Inclusion criteria: neuropathic foot ulcer, Wagner grade 1 or 2 Exclusion criteria: not stated |
|
| Interventions | Group A: Purilon gel (Coloplast A/S) Group B: IntraSite gel (Smith & Nephew) Co‐intervention: dressings changed every second day. All patients had appropriate off‐loading. Weekly assessment of ulcer area, peri‐ulcer skin reactions, inflammation/infection of peri‐ulcer skin and patient comfort. Biatain non‐adhesive dressing used as a secondary dressing. |
|
| Outcomes | Primary outcome: ulcer healing (% ulcers healed at 10 weeks; change in mean wound area; average time to 75% reduction in wound area) Secondary outcomes: costs (description) Amputation; adverse events; health‐related quality of life and ulcer recurrence not reported |
|
| Notes | Trial data: Analysis 4.1 Conference abstract only Funding source: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: published abstract only. Method of generation of random schedule not reported. The abstract does state that participants were 'recruited and randomised to Purilon Gel or Intrasite...' |
| Allocation concealment (selection bias) | Unclear risk | Comment: published abstract only ‐ no details in the text |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: published abstract only ‐ blinding not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: published abstract only ‐ blinding not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: reports that "66 patients were evaluated out of 74 randomised". Not clear if intention‐to‐treat analysis conducted. |
| Selective reporting (reporting bias) | Unclear risk | Comment: published abstract only ‐ unable to assess incomplete outcome data |
| Other bias | Unclear risk | Comment: published abstract only ‐ unable to assess other risk of bias |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Agas 2006 | Study did not randomise participants |
| Ahroni 1993 | The dressing groups evaluated in this study were not hydrogel dressings |
| Altman 1993 | No single, identifiable dressing type evaluated |
| Alvarez 2003 | The dressing groups evaluated in this study were not hydrogel dressings |
| Apelqvist 1990 | Relevant outcome data are not reported: study outcome was limited to change in size of necrotic material on the wound. Study authors were unable to provide the original healing outcome data. |
| Apelqvist 1996 | No single, identifiable dressing type evaluated |
| Apelqvist 2004 | No single, identifiable dressing type evaluated |
| Armstrong 2004 | No single, identifiable dressing type evaluated |
| Baker 1993 | The dressing groups evaluated in this study were not hydrogel dressings |
| Belcaro 2010 | The dressing groups evaluated in this study were not hydrogel dressings |
| Blackman 1994 | The dressing groups evaluated in this study were not hydrogel dressings |
| Bogaert 2004 | Study did not randomise participants |
| Bradshaw 1989 | Trial stopped after recruiting six participants. No data presented. Authors not contacted for healing data. |
| Caravaggi 2003 | Other intervention, not dressings, differs between trial arms |
| Chang 2000 | Study did not include diabetic foot ulcers |
| Chauhan 2003 | Other intervention, not dressings, differ between trial arms |
| Chirwa 2010 | Study did not randomise participants |
| Clever 1995 | The dressing groups evaluated in this study were not hydrogel dressings |
| Cuevas 2007 | No single, identifiable dressing type evaluated |
| Dash 2009 | Other intervention, not dressings, differ between trial arms |
| Diehm 2005 | Study did not randomise participants |
| Donaghue 1998 | The dressing groups evaluated in this study were not hydrogel dressings |
| Driver 2006 | Other intervention, not dressings, differs between trial arms |
| Edmonds 2009 | Other intervention, not dressings, differs between trial arms |
| Eginton 2003 | No single, identifiable dressing type evaluated |
| Etoz 2003 | Study did not randomise participants |
| Farac 1999 | Author contacted: study not suitable for inclusion due to data quality issues |
| Foo 2004 | The dressing groups evaluated in this study were not hydrogel dressings |
| Foster 1994 | The dressing groups evaluated in this study were not hydrogel dressings |
| Foster 1999 | Other intervention, not dressings, differs between trial arms |
| Gao 2007 | Other intervention, not dressings, differs between trial arms |
| Gentzkow 1996 | Other intervention, not dressings, differs between trial arms |
| Gottrup 2011 | The dressing groups evaluated in this study were not hydrogel dressings |
| Hanft 2002 | Other intervention, not dressings, differs between trial arms |
| Jeffcoate 2009 | The dressing groups evaluated in this study were not hydrogel dressings |
| Jeffery 2008 | Study did not randomise participants |
| Jude 2007 | The dressing groups evaluated in this study were not hydrogel dressings |
| Kordestani 2008 | The dressing groups evaluated in this study were not hydrogel dressings |
| Lalau 2002 | The dressing groups evaluated in this study were not hydrogel dressings |
| Landsman 2010 | Other intervention, not dressings, differs between trial arms |
| Lazaro‐Martinez 2007 | No single, identifiable dressing type evaluated |
| Lipkin 2003 | Other intervention, not dressings, differs between trial arms |
| Marston 2001 | Other intervention, not dressings, differs between trial arms |
| Mazzone 1993 | The dressing groups evaluated in this study were not hydrogel dressings |
| McCallon 2000 | Study did not randomise participants |
| Mody 2008 | Study did not include diabetic foot ulcers |
| Moretti 2009 | Other intervention, not dressings, differs between trial arms |
| Mueller 1989 | Other intervention, not dressings, differs between trial arms |
| Mulder 1994 | Required further data specific to diabetic foot ulcers. Unablet o obtain. |
| Munter 2006 | The dressing groups evaluated in this study were not hydrogel dressings |
| Novinscak 2010 | No homogenous dressing group evaluated |
| Ogce 2007 | The dressing groups evaluated in this study were not hydrogel dressings |
| Palao i Domenech 2008 | The dressing groups evaluated in this study were not hydrogel dressings |
| Parish 2009 | Other intervention, not dressings, differs between trial arms |
| Pham 1999 | Other intervention, not dressings, differs between trial arms |
| Piaggesi 1997 | Study did not randomise participants |
| Piaggesi 2001 | The dressing groups evaluated in this study were not hydrogel dressings |
| Reyzelman 2009 | No single, identifiable dressing type evaluated |
| Roberts 2001 | The dressing groups evaluated in this study were not hydrogel dressings |
| Robson 2005 | Other intervention, not dressings, differs between trial arms |
| Robson 2009 | Study did not include diabetic foot ulcers |
| Sabolinski 2000 | Other intervention, not dressings, differs between trial arms |
| Sabolinski 2001 | Other intervention, not dressings, differs between trial arms |
| Shaw 2010 | Other intervention, not dressings, differs between trial arms |
| Shukrimi 2008 | Other intervention, not dressings, differs between trial arms |
| Sibbald 2011 | The dressing groups evaluated in this study were not hydrogel dressings |
| Solway 2011 | Study did not randomise participants |
| Steed 1992 | Other intervention, not dressings, differs between trial arms |
| Steed 1995 | Other intervention, not dressings, differs between trial arms |
| Steed 1996 | Other intervention, not dressings, differs between trial arms |
| Subrahmanyam 1993 | The dressing groups evaluated in this study were not hydrogel dressings |
| Trial 2010 | The dressing groups evaluated in this study were not hydrogel dressings |
| Turns 2012 | Other intervention, not dressings |
| Urbaneie 1999 | No homogenous dressing group evaluated |
| Varma 2006 | No homogenous dressing group evaluated |
| Veves 2001 | Other intervention, not dressings, differs between trial arms |
| Veves 2002 | The dressing groups evaluated in this study were not hydrogel dressings |
| Woo 2010 | The dressing groups evaluated in this study were not hydrogel dressings |
| Yao 2007 | Other intervention, not dressings, differs between trial arms |
| Zimny 2003 | Other intervention, not dressings, differs between trial arms |
Characteristics of studies awaiting assessment [ordered by study ID]
Wang 2012.
| Methods | RCT? |
| Participants | People with diabetes and foot ulcers |
| Interventions | Topical bismuth subgallate/borneol (Suile) dressing compared with hydrogel |
| Outcomes | Unsure |
| Notes | Awaiting retrieval and translation |
Contributions of authors
Jo Dumville developed the review and co‐ordinated development, completed the first draft of the protocol, made an intellectual contribution, approved the final version prior to submission and is the guarantor of the review and the update. Susan O’Meara edited the review, made an intellectual contribution and approved the final version of the review and the update prior to submission. Sohan Deshpande completed the first draft of the review, made an intellectual contribution and approved the final version of the review prior to submission. Katharine Speak made an intellectual contribution to the review, advised on the review and approved the final version prior to submission.
Contributions of editorial base:
Nicky Cullum: edited the protocol and review; advised on methodology, interpretation and content. Approved the final review prior to submission. Sally Bell‐Syer: co‐ordinated the editorial process. Advised on methodology, interpretation and content. Edited and copy edited the review and the update. Ruth Foxlee: designed the search strategy and edited the search methods section.
Sources of support
Internal sources
Department of Health Sciences, University of York, UK.
External sources
NIHR Programme Grants for Applied Research, UK.
NIHR/Department of Health (England), Cochrane Wounds Group, UK.
Declarations of interest
Susan O'Meara and Jo Dumville receive funding from the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research programme. This review presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research programme (RP‐PG‐0407‐10428). The views expressed in this presentation are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Sohan Deshpande and Katherine Speak: none declared.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
D'Hemecourt 1998 {published data only}
- D'Hemecourt PA, Smiell JM, Karim MR. Sodium carboxymethyl cellulose aqueous‐based gel vs becaplermin gel in patients with nonhealing lower extremity diabetic ulcers. Wounds 1998;10(3):69‐75. [Google Scholar]
Jensen 1998 {published data only}
- Jensen JL, Seeley J, Brian Gillin. A controlled, randomized comparison of two moist wound healing protocols: Carrasyn hydrogel wound dressing and wet‐to‐moist saline gauze. Advances in Wound Care 1998;11(7 Suppl 1):1‐4. [PubMed] [Google Scholar]
Markevich 2000 {published data only}
- Markevich YO, McLeod‐Roberts J, Mousley M, Melloy E. Maggot therapy for diabetic neuropathic foot wounds. Diabetologia: Proceedings of the 36th Annual Meeting of the European Association for the Study of Diabetes 2000;43(Suppl 1):A 15. [Google Scholar]
Vandeputte 1997 {published data only}
- Vandeputte J, Gryson L. Diabetic foot infection controlled by immuno‐modulating hydrogel containing 65% glycerine. Presentation of a clinical trial. 6th European Conference on Advances in Wound Management. Amsterdam, 1997:50‐3.
Whalley 2001 {published data only}
- Capillas R, Whalley A, Boulton AMJ, Dargis V, Harding K, Acker K. Performance characteristics and safety of hydrogels using a non‐adhesive foam dressing as secondary dressing in the treatment of diabetic foot ulcers. 12th Conference of the European Wound Management Association; 23‐25 May, 2002; Granada, Spain. Granada, Spain, 2002.
- Gottrup F, Hahn TW, Thomsen JK. Cost‐effectiveness of hydrogel treatment in diabetic foot ulcers. 12th Conference of the European Wound Management Association; 23‐25 May, 2002; Granada, Spain. 2002.
- Whalley A, Boulton AJM, Harding K, Acker K, Capillas R. Performance characteristics and safety of Purilon gel versus Intrasite using Biatain non‐adhesive dressing as secondary dressing in the treatment of diabetic foot ulcers. 11th european tissue repair society annual conference; 2001 5‐8 September; Cardiff, Wales. Cardiff, Wales, 2001.
References to studies excluded from this review
Agas 2006 {published data only}
- Agas CM, Bui TD, Driver VR, Gordon IL. Effect of window casts on healing rates of diabetic foot ulcers. Journal of Wound Care 2006;15(2):80‐3. [DOI] [PubMed] [Google Scholar]
Ahroni 1993 {published data only}
- Ahroni JH, Boyko EJ, Pecoraro RE. Diabetic foot ulcer healing: extrinsic vs intrinsic factors. Wounds 1993;5(5):245‐55. [Google Scholar]
Altman 1993 {published data only}
- Altman MI, Mulder GD. Multi‐centre evaluation of Nu‐Gel wound dressing in full‐thickness chronic wounds of the lower extremities. 3rd European Conference on Advances in Wound Management. Harrogate, UK, 1993,19‐22 October.
Alvarez 2003 {published data only}
- Alvarez OM, Roger RS, Booker JG, Patel M. Effect of non contact normothermic wound therapy on the healing of neuropathic (diabetic) foot ulcers: an interim analysis of 20 patients. Journal of Foot and Ankle Surgery 2003;42(1):30‐5. [DOI] [PubMed] [Google Scholar]
Apelqvist 1990 {published data only}
- Apelqvist J, Larsson J, Stenstrom A. Topical treatment of necrotic foot ulcers in diabetic patients:a comparative trial of DuoDerm and MeZinc. British Journal of Dermatology 1990;123:787‐92. [DOI] [PubMed] [Google Scholar]
Apelqvist 1996 {published data only}
- Apelqvist J, Ragnarson‐Tennvall G. Cavity foot ulcers in diabetic patients: a comparative study of cadexomer iodine ointment and standard treatment. An economic analysis alongside a clinical trial. Acta Dermato‐Venereologica 1996;76(3):321‐5. [DOI] [PubMed] [Google Scholar]
Apelqvist 2004 {published data only}
- Apelqvist J, Piaggesi A. Enamel matrix protein in diabetic foot ulcers: a controlled multicentre study. 2nd World Union of Wound Healing Societies Meeting. Paris, 2004, 8‐13.
Armstrong 2004 {published data only}
- Armstrong DG, Lavery LA, Frykberg RG, Andros G, Attinger CE, Boulton AJM. VAC therapy appears to heal complex DFU. 2nd World Union of Wound Healing Societies Meeting; 8‐13 July, 2004; Paris. 2004.
Baker 1993 {unpublished data only}
- Baker NR, Creevy J. A randomised comparative pilot study to evaluate Allevyn hydrocellular dressings and Sorbsan calcium‐alginate dressings in the treatment of diabetic foot ulcers. Unpublished 1993.
Belcaro 2010 {published data only}
- Belcaro G, Cesarone MR, Errichi BM, Ricci A, Dugall M, Pellegrini L, et al. Venous and diabetic ulcerations: management with topical multivalent silver oxide ointment. Panminerva Medica 2010;52(2 (Suppl 1)):37‐42. [PubMed] [Google Scholar]
Blackman 1994 {published data only}
- Blackman JD, Senseng D, Quinn L, Mazzone T. Clinical evaluation of a semipermeable polymeric membrane dressing for the treatment of chronic diabetic foot ulcers. Diabetic Care 1994;17(4):322‐5. [DOI] [PubMed] [Google Scholar]
Bogaert 2004 {published data only}
- Bogaert T, Meert S, Derre B, Goethals E. Topical autologous platelet gel enhances healing of chronic diabetic ulcer: Preliminary report. 22nd World Union of Wound Healing Societies Meeting; 8‐13 July, 2004; Paris. 2004.
Bradshaw 1989 {published data only}
- Bradshaw T, Gem J, Boulton A. The use of Kaltostat in the treatment of ulceration in the diabetic foot. Chiropodist 1989;44(9):204‐7. [Google Scholar]
Caravaggi 2003 {published data only}
- Caravaggi C, Giglio R, Pritelli C, Sommaria M, Dalla Noce S, Faglia E, et al. HYAFF 11‐based autologous dermal and epidermal grafts in the treatment of noninfected diabetic plantar and dorsal foot ulcers: a prospective, multicenter, controlled, randomized clinical trial. Diabetes Care 2006;10:2853‐9. [DOI] [PubMed] [Google Scholar]
Chang 2000 {published data only}
- Chang DW, Sanchez LA, Veith FJ, Wain RA, Okhi T, Suggs WD. Can a tissue‐engineered skin graft improve healing of lower extremity foot wounds after revascularization?. Annals of Vascular Surgery 2000;14:44‐9. [DOI] [PubMed] [Google Scholar]
Chauhan 2003 {published data only}
- Chauhan VS, Rasheed MA, Pandley SS, Shukla VK. Nonhealing wounds ‐ a therapeutic dilemma. International Journal of Lower Extremity Wounds 2003;2(1):40‐5. [DOI] [PubMed] [Google Scholar]
Chirwa 2010 {published and unpublished data}
- Chirwa Z, Bhengu T, Litiane K. The cost effectiveness of using calcium alginate silver matrix in the treatment of wounds. European Wound Management Association Journal 2010;10(2):257, Abstract P299. [Google Scholar]
Clever 1995 {published data only}
- Clever HU, Dreyer M. Comparing two wound dressings for the treatment of neuropathic diabetic foot ulcers. 5th European Conference on Advances in Wound Management; Harrogate, UK. 1995:201‐3.
Cuevas 2007 {published data only}
- Cuevas FR, Velázquez Méndez AA, Andrade IC. Zinc hyaluronate effects on ulcers in diabetic patients [Efecto delhialuronato de zinc sobre las úlceras en pacientes con diabetes]. Gerokomos 2007;18(2):91‐105. [Google Scholar]
Dash 2009 {published data only}
- Dash NR, Dash SN, Routray P, Mohapatra S, Mohapatra PC. Targeting nonhealing ulcers of lower extremity in human through autologous bone marrow‐derived mesenchymal stem cells. Rejuvenation Research 2009;12(5):359‐66. [DOI] [PubMed] [Google Scholar]
Diehm 2005 {published data only}
- Diehm C, Lawall H. Evaluation of Tielle hydro polymer dressings in the management of chronic exuding wounds in primary care. International Wound Journal 2005;2(1):26‐35. [DOI] [PMC free article] [PubMed] [Google Scholar]
Donaghue 1998 {published data only}
- Donaghue VM, Chrzan JS, Rosenblum BI, Giurini JM, Habershaw GM, Veves A. Evaluation of a collagen‐alginate wound dressing in the management of diabetic foot ulcers. Advances in Wound Care 1998;11(3):114‐9. [PubMed] [Google Scholar]
Driver 2006 {published data only}
- Driver VR, Hanft J, Fylling CP, Beriou JM, Autologel Diabetic Foot Ulcer Study Group. A prospective, randomized, controlled trial of autologous platelet‐rich plasma gel for the treatment of diabetic foot ulcers. Ostomy/Wound Management 2006;52(6):68‐70, 72, 74. [PubMed] [Google Scholar]
Edmonds 2009 {published data only}
- Edmonds M. Apligraf in the treatment of neuropathic diabetic foot ulcers. International Journal of Lower Extremity Wounds 2009;8(1):11‐8. [DOI] [PubMed] [Google Scholar]
Eginton 2003 {published data only}
- Eginton MT, Brown KR, Seabrook GR, Towne JB, Cambria RA. A prospective randomized evaluation of negative‐pressure wound dressings for diabetic foot wounds. Annals of Vascular Surgery 2003;17(6):645‐9. [DOI] [PubMed] [Google Scholar]
Etoz 2003 {published data only}
- Etoz A, Ozgenel Y, Ozcan M. The use of negative pressure wound therapy on diabetic foot ulcers: a preliminary controlled trial. Wounds: A Compendium of Clinical Research and Practice 2004;16(8):264‐9. [Google Scholar]
Farac 1999 {published data only}
- Farac KP, Grief R, Sessler DI. Radiant heat bandage speeds healing of diabetic‐neuropathic foot ulcers. 31st Annual Wound, Ostomy and Continence Conference; June 1999; Minneapolis, MN. 1999.
Foo 2004 {published data only}
- Foo LSS, Chua BSY, Chia GT, Tan SB, Howe TS. Vacuum assisted closure vs moist gauze dressing in post‐operative diabetic foot wounds: early results from a randomised controlled trial. 2nd World Union of Wound Healing Societies Meeting; 8‐13 July, 2004; Paris. July, Paris, 2004.
Foster 1994 {published data only}
- Foster AVM, Greenhill MT, Edmonds ME. Comparing two dressings in the treatment of diabetic foot ulcers. Journal of Wound Care 1994;3(5):224‐8. [DOI] [PubMed] [Google Scholar]
Foster 1999 {published data only}
- Foster A, Bates M, Doxford M, Edmonds ME. Treatment of indolent neuropathic ulceration of the diabetic foot with Hyaff. The Diabetic Foot 1999;2(2):72. [Google Scholar]
Gao 2007 {published data only}
- Gao L, Xu GX, Zhou HB. Efficacy evaluation of diabetic foot ulceration treated with iodophors dressings therapy. Journal of Clinical Nursing 2007;6(4):21‐2. [Google Scholar]
Gentzkow 1996 {published data only}
- Gentzkow GD, Iwasaki SD, Hershon KS, Mengel M, Prendergast JJ, Ricotta JJ, et al. Use of Dermagraft, a cultured human dermis, to treat diabetic foot ulcers. Diabetes Care 1996;19(4):350‐4. [DOI] [PubMed] [Google Scholar]
Gottrup 2011 {published data only}
- Gottrup F, Gibson M, Karlsmark T, Bishoff‐Mikkelsen M, Nisbet L, Cullen B. Collagen/ORC/silver treatment of diabetic foot ulcers; a randomised controlled trial. Wound Repair and Regeneration 2011;19(2):A24. [DOI] [PubMed] [Google Scholar]
- Gottrup F, Karlsmark T, Cullen B, Gibson M, Nisbet L. Comparative clinical study to determine the effects of collagen/orc+silver therapy on wound healing of diabetic foot ulcers. EWMA Journal 2010;10(2):83 Abstract 126. [Google Scholar]
Hanft 2002 {published data only}
- Hanft JR, Surprenant MS. Healing of chronic foot ulcers in diabetic patients treated with a human fibroblast‐derived dermis. Journal of Foot and Ankle Surgery 2002;41(5):291. [DOI] [PubMed] [Google Scholar]
Jeffcoate 2009 {published data only}
- Jeffcoate WJ, Price PE, Phillips CJ, Game FL, Mudge E, Davies S, et al. Randomised controlled trial of the use of three dressing preparations in the management of chronic ulceration of the foot in diabetes. Health Technology Assessment 2009;13(54):1‐110. [DOI] [PubMed] [Google Scholar]
Jeffery 2008 {published data only}
- Jeffery S. A honey‐based dressing for diabetic foot ulcers: a controlled study. The Diabetic Foot Journal 2008;11(2):87‐91. [Google Scholar]
Jude 2007 {published data only}
- Jude EB, Apelqvist, Spraul M, Martini J. Prospective randomized controlled study of Hydrofiber dressing containing ionic silver or calcium alginate dressings in non‐ischaemic diabetic foot ulcers. Diabetic Medicine 2007;24:280‐8. [DOI] [PubMed] [Google Scholar]
Kordestani 2008 {published data only}
- Kordestani S, Shahrezaee M, Tahmasebi MN, Hajimahmodi H, Ghasemali DH, Abyaneh MS. A randomised controlled trial on the effectiveness of an advanced wound dressing used in Iran. Journal of Wound Care 2008;17(7):323‐7. [DOI] [PubMed] [Google Scholar]
Lalau 2002 {published data only}
- Lalau JD, Bresson R, Charpentier P, Coliche V, Erlher S, Ha Van G, et al. Efficacy and tolerance of calcium alginate versus Vaseline gauze dressings in the treatment of diabetic foot lesions. Diabetes & Metabolism 2002;28(3):223‐9. [PubMed] [Google Scholar]
Landsman 2010 {published data only}
- Landsman A, Agnew P, Parish L, Joseph R, Galiano RD. Diabetic foot ulcers treated with Becaplermin and TheraGauze, a moisture‐controlling smart dressing: a randomized, multicenter, prospective analysis. Journal of the American Podiatric Medical Association 2010;100(3):155‐60. [DOI] [PubMed] [Google Scholar]
Lazaro‐Martinez 2007 {published data only}
- Lázaro‐Martíneza JL, García‐Moralesa E, Aragón‐Sánchezc FJ. Randomized comparative trial of a collagen/oxidized regenerated cellulose dressing in the treatment of neuropathic diabetic foot ulcers. 18th Conference of the European Wound Management Association. Universidad, Complutense, Spain, 2008:Poster 371.
- Lázaro‐Martíneza JL, García‐Moralesa E, Beneit‐Montesinosa JV, Martínez‐de‐Jesúsb FR, Aragón‐Sánchezc FJ. Randomized comparative trial of a collagen/oxidized regenerated cellulose dressing in the treatment of neuropathic diabetic foot ulcers [Estudio aleatorizado y comparativo de unapósito de colágeno y celulosa oxidadaregenerada en el tratamiento de úlcerasneuropáticas de pie diabético]. Cirugia Espanola 2007;82(1):27‐31. [DOI] [PubMed] [Google Scholar]
Lipkin 2003 {published data only}
- Lipkin S, Chaikof E, Isseroff Z, Silverstein P. Effectiveness of bilayered cellular matrix in healing of neuropathic diabetic foot ulcers: results of a multicenter pilot trial. Wounds: A Compendium of Clinical Research and Practice 2003;15(7):230‐6. [Google Scholar]
Marston 2001 {published data only}
- Marston W, Foushee K, Farber M. Prospective randomized study of a cryopreserved, human fibroblast‐derived dermis in the treatment of chronic plantar foot ulcers associated with diabetes mellitus. 14th Annual Symposium on Advances in Wound Care and Medical Research Forum on Wound Repair; 30 April‐3 May, 2001. Las Vegas, Nevada, 2001.
Mazzone 1993 {published data only}
- Mazzone T, Blackman JD. [Evaluation of a new loaded foam membrane on the healing rate of diabetic foot ulcers]. 1st Joint Meeting of the Wound Healing Society and the European Tissue Repair Society; Amsterdam, The Netherlands. 1993.
McCallon 2000 {published data only}
- McCallon SK, Knight CA, Valiulus JP, Cunningham MW, McCulloch, Farinas LP. Vacuum‐Assisted Closure versus saline moistened gauze in the healing of postoperative diabetic foot wounds. Ostomy/Wound Management 2000;46(8):28‐34. [PubMed] [Google Scholar]
Mody 2008 {published data only}
- Mody GN, Nirmal IA, Duraisamy S, Perakath B. A blinded, prospective, randomized controlled trial of topical negative pressure wound closure in India. Ostomy/Wound Management 2008;54(12):36‐46. [PubMed] [Google Scholar]
Moretti 2009 {published data only}
- Moretti B, Notarnicola A, Maggio G, Moretti L, Pascone M, Tafuri S, et al. The management of neuropathic ulcers of the foot in diabetes by shock wave therapy. BMC Musculoskeletal Disorders 2009; Vol. 10, issue 54. [DOI: 10.1186/1471-2474-10-54] [DOI] [PMC free article] [PubMed]
Mueller 1989 {published data only}
- Mueller MJ, Diamond JE, Sinacore DR, Delitto A, Blair VP, Drury DA, et al. Total contact casting in treatment of diabetic plantar ulcers. Diabetes Care 1989;12(6):184‐8. [DOI] [PubMed] [Google Scholar]
Mulder 1994 {published data only}
- Mulder GD, Jensen JL, Seeley JE, Peak Andrews K. A controlled randomized study of an amorphous hydrogel to expedite closure of diabetic ulcers. 4th European Tissue Repair Society Meeting; 25–28 August 1994; Oxford, England. 1994.
Munter 2006 {published data only}
- Munter KC, Beele H, Russell L, Basse E, Grochenig E, Crespi A, et al. CONTOP study: improved healing of delayed healing ulcers with sustained silver‐releasing foam dressing versus other silver dressings. 16th Conference of the European Wound Management Association; 16‐18 May 2006. Prague, Czech Republic, 2006.
- Munter KC, Beele H, Russell L, Basse PB, Groechenig E, Crespi A, et al. The CONTOP study: a large‐scale,comparative, randomized study in patients treated with a sustained silver‐releasing foam dressing. SAWC; 30 April‐3 May 2006. San Antonio,Texas, 2006.
- Munter KC, Beele H, Russell L, Crespi A, Grocenig E, Basse P, et al. Effect of a sustained silver‐releasing dressing on ulcers with delayed healing: The CONTOP study. Journal of Wound Care 2006;15(5):199‐205. [DOI] [PubMed] [Google Scholar]
- Russell L, Nebbioso G, Munter KC, Beele H, Basse PB/Dienst H. The Contop Study: a hydro‐activated silver containing foam dressing versus standard care. 2nd World Union of Wound Healing Societies Meeting; 8–13 July 2004; Paris. Paris, 2004.
- Scalise A, Forma O, Happe M, Hahn TW. The Contop study: real life experiences from an international study comparing a silver containing hydro‐activated foam dressing with standard wound care. 13th Conference of the European Wound Management Association; 22‐23 May 2003; Pisa, Italy. 2003.
Novinscak 2010 {published data only}
- Novinscak T, Zvorc M, Trojko S, Jozinovic E, Filipovic M, Grudic R. Comparison of cost‐benefit of the three methods of diabetic ulcer treatment: dry, moist and negative pressure. Acta Medica Croatica 2010;64(Suppl 1):113‐5. [Google Scholar]
Ogce 2007 {published data only}
- Ogce F, Dramali A. The treatment of diabetic foot ulcers. Sendrom 2007;19(12):79‐81. [Google Scholar]
Palao i Domenech 2008 {published data only}
- Palao i Domenech R, Romanelli M, Tsiftsis DD, Slonkova V, Jortikka A, Johannesen N, et al. Effect of an ibuprofen‐releasing foam dressing on wound pain: a real‐life RCT. Journal of Wound Care 2008;17(8):344‐8. [DOI] [PubMed] [Google Scholar]
Parish 2009 {published data only}
- Parish L, Routh H, Parish J. Diabetic foot ulcers: a randomized multicenter study comparing a moisture‐controlling dressing with a topical growth factor. Journal of the American Academy of Dermatology 2009;60(Suppl 3):AB202. [Google Scholar]
Pham 1999 {published data only}
- Pham HT, Rosenblum BI, Lyons TE, Giurini JM, Chrzan JS, Habershaw GM, et al. Evaluation of a human skin equivalent for the treatment of diabetic foot ulcers in a prospective, randomized, clinical trial. Wounds: A Compendium of Clinical Research and Practice 1999;11(4):76‐86. [Google Scholar]
Piaggesi 1997 {published data only}
- Piaggesi A. A thin hydrocolloid occlusive dressing in diabetic foot ulcerations. Journal of Wound Care 1997;6(3):10. [Google Scholar]
Piaggesi 2001 {published data only}
- Piaggesi A, Baccetti F, Rizzo L, Romanelli, Navalesi R, Benzi L. Sodium carboxyl‐methyl‐cellulose dressings in the management of deep ulcerations of diabetic foot. Diabetic Medicine 2001;18:320‐4. [DOI] [PubMed] [Google Scholar]
Reyzelman 2009 {published data only}
- Reyzelman A, Crews RT, Moore JC, Moore L, Mukker JS, Offutt S, et al. Clinical effectiveness of an acellular dermal regenerative tissue matrix compared to standard wound management in healing diabetic foot ulcers: a prospective, randomised, multicentre study. International Wound Journal 2009;6(3):196‐208. [DOI] [PMC free article] [PubMed] [Google Scholar]
Roberts 2001 {published data only}
- Roberts GH, Hammad LH, Haggan G, Baker N, Sandeman D, Mani R, et al. Hydrocellular against non‐adherent dressings to treat diabetic foot ulcers ‐ a randomised controlled study. 11th ETRS Annual Conference. 2001.
Robson 2005 {published data only}
- Robson MC, Payne WG, Garner WL, Biundo J, Giacalone VF, Cooper DM, et al. Integrating the results of phase IV (post marketing) clinical trial with four previous trials reinforces the position that Regranex (Becaplermin) gel 0.01% is an effective adjunct to the treatment of diabetic foot ulcers. Journal of Applied Research 2005;5(1):35‐45. [Google Scholar]
Robson 2009 {published data only}
- Robson V, Dodd S, Thomas S. Standardized antibacterial honey (Medihoney) with standard therapy in wound care: randomized clinical trial. Journal of Advanced Nursing 2009;65(3):565‐75. [DOI] [PubMed] [Google Scholar]
Sabolinski 2000 {published data only}
- Sabolinski M, Giovino K, Graftskin Diabetic Foot Ulcer Study Group. Risk factors associated with the healing of diabetic foot ulcers. Wound Healing Society Educational Symposium. Toronto, Canada, 2000, 4‐6 June.
- Sabolinski M, Toole T, Giovino K, Apligraft Diabetic Foot Ulcer Study Group. Apligraf (Graftskin) bilayered living skin construct in the treatment of diabetic foot ulcers. First World Wound Healing Congress. Melbourne, Australia, 2000, 10‐13 September.
- Sabolinski ML, Veves A. Graftskin (Apligraf) in neuropathic diabetic foot ulcers. Wounds: A Compendium of Clinical Research and Practice 2000;12(5 (Suppl A)):33A‐6A. [Google Scholar]
- Sabolinski ML, Veves A. Graftskin bilayered living skin construct in the treatment of diabetic foot ulcers. 13th Annual Symposium on Advanced Wound Care and 10th Annual Medical Research Forum on Wound Repair. Dallas, USA, 1‐4 April 2000.
- Veves A, Falango V, Armstrong DG, Sabolinski ML. Graftskin (Apligraf) a human skin equivalent, promotes wound healing in diabetic foot ulcers in a prospective, randomized, multicenter clinical trial. Tenth Annual Meeting of the European Tissue Repair Society. Brussels, Belgium, 24–27 May 2000.
Sabolinski 2001 {published data only}
- Sabolinski M, Falanga V. The healing of diabetic plantar foot ulcers of greater than two‐month duration with Graftskin in a randomized prospective study. Eleventh Annual Meeting and Educational Symposium Wound Healing Society. Albuquerque, New Mexico, 2001, 16‐18 May.
Shaw 2010 {published data only}
- Shaw J, Hughes CM, Lagan KM, Stevenson MR, Irwin CR, Bell PM. The effect of topical phenytoin on healing in diabetic foot ulcers: a randomised controlled trial. Diabetologia 2010;53(Suppl 1):S463. [DOI] [PubMed] [Google Scholar]
Shukrimi 2008 {published data only}
- Shukrimi A, Sulaiman AR, Halim AY, Azril A. A comparative study between honey and povidone iodine as dressing solution for Wagner type II diabetic foot ulcers. Medical Journal of Malaysia 2008;63(1):44‐6. [PubMed] [Google Scholar]
Sibbald 2011 {published data only}
- Sibbald RG, Coutts P, Woo KY. Reduction of bacterial burden and pain in chronic wounds using a new polyhexamethylene biguanide antimicrobial foam dressing‐clinical trial results. Advances in Skin and Wound Care 2011;24(2):78‐84. [DOI] [PubMed] [Google Scholar]
Solway 2011 {published data only}
- Solway DR, Clark WA, Levinson DJ. A parallel open‐label trial to evaluate microbial cellulose wound dressing in the treatment of diabetic foot ulcers. International Wound Journal 2011;8(1):69‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Steed 1992 {published data only}
- Holloway GA, Steed DL, DeMarco MJ, Matsumoto T, Moosa HH, Webster MW, et al. A randomized controlled multicenter dose response trial of activated platelet supernatant topical CT‐102 in chronic nonhealing diabetic wounds. Wounds: A Compendium of Clinical Research and Practice 1993;5(4):198‐206. [Google Scholar]
- Steed DL. Growth factors in managing diabetic foot ulcers. 5th Annual Symposium on Advanced Wound Care. New Orleans, Louisiana, 23‐25 April, 1992.
- Steed DL, Goslen JB, Holloway GA, Malone JM, Bunt TJ, Webster MW. Randomized prospective double‐blind trial in healing chronic diabetic foot ulcers. Diabetic Care 1992;15(11):1598‐604. [DOI] [PubMed] [Google Scholar]
Steed 1995 {published data only}
- Steed DL, Ricotta JJ, Prendergast JJ, Kaplan RJ, Webstar MW, McGill JB. Promotion and acceleration of diabetic ulcer healing by arginine‐glycine‐aspartic acid (RGD) peptide matrix. RGD Study Group. Diabetes Care 18;1:39‐46. [DOI] [PubMed] [Google Scholar]
Steed 1996 {published data only}
- Steed DL, Edington HD, Webster MW. Recurrence rate of diabetic neurotrophic foot ulcers healed using topical application of growth factors released from platelets. Wound Repair and Regeneration 1996;4(2):230‐3. [DOI] [PubMed] [Google Scholar]
Subrahmanyam 1993 {published data only}
- Subrahmanyam M. Honey as a surgical dressing for burns and ulcers. Indian Journal of Surgery 1993;55(9):468‐73. [Google Scholar]
Trial 2010 {published data only}
- Teot L, Trial C, Lavigne JP. Results of RCT on the antimicrobial effectiveness of a new silver alginate wound dressing. European Wound Management Association Journal 2008;8(Suppl 2):54 Abstract no. 69. [Google Scholar]
- Trial C, Darbas H, Lavigne J‐P, Sotto A, Simoneau G, Tillet Y, et al. Assessment of the antimicrobial effectiveness of a new silver alginate wound dressing: a RCT. Journal of Wound Care 2010;19(1):20‐6. [DOI] [PubMed] [Google Scholar]
Turns 2012 {published data only}
- Turns M. Evaluation of NOSF in neuropathic diabetic. Wounds UK 2012;8(1):100‐106. [Google Scholar]
Urbaneie 1999 {published data only}
- Urbaneie‐Rovan V. Efficacy and cost of different dressings. Practical Diabetes International 1999;16(2):S3. [Google Scholar]
Varma 2006 {published data only}
- Varma AK, Bal A, Kumar H, Kesav R, Nair S. Efficacy of polyurethane foam dressing in debrided diabetic lower limb wounds. Wounds: A Compendium of Clinical Research and Practice 2006;18(10):300‐6. [Google Scholar]
Veves 2001 {published data only}
- Veves A, Falanga V, Armstrong DG, Sabolinski ML. Graftskin, a human skin equivalent, is effective in the management of neuropathic diabetic foot ulcers. Diabetes Care 2001;24(2):290‐5. [DOI] [PubMed] [Google Scholar]
Veves 2002 {published data only}
- Sheehan P, Jones P, Caselli A, Giurini JM, Veves A. Percent change in wound area of diabetic foot ulcers over a 4‐week period is a robust predictor of complete healing in a 12‐week prospective trial. Diabetes Care 2003;26(6):1879‐82. [DOI] [PubMed] [Google Scholar]
- Veves A. Promogran clinical trial. The Diabetic Foot 2001;4(4):S4‐S5. [Google Scholar]
- Veves A. Wound care device expert meeting. Summary report. Promogran ‐ clinical trial data. The Diabetic Foot 2001;4(3):S8‐S10. [Google Scholar]
- Veves A, Sheehan P, Pham HT. A randomized controlled trial of Promogran (a collagen / oxidised regenerated cellulose dressing) vs standard treatment in the management of diabetic foot ulcers. Archives of Surgery 2002;137:822‐7. [DOI] [PubMed] [Google Scholar]
Woo 2010 {published data only}
- Woo K, Sibbald G, Coutts P. Reduction of infection and pain in chronic wounds using a new antimicrobial foam dressing. European Wound Management Association Journal 2010;10(2):59 Abstract 78. [Google Scholar]
Yao 2007 {published data only}
- Yao XZ, Chen W. Effectiveness of feet soaking with Chinese herbs combined with changing dressings in the treatment of diabetic foot ulceration. Journal of Nursing Science 2007;22(5):42‐3. [Google Scholar]
Zimny 2003 {published data only}
- Zimny S, Schatz H, Pfohl U. The effects of applied felted foam on wound healing and healing times in the therapy of neuropathic diabetic foot ulcers. Diabetic Medicine 2003;20(8):622‐5. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Wang 2012 {published data only}
- Wang F, Yuan N, Wang Y, Wang C, Wang A, Yu T, Liu G, Xu Z, Ran X. Clinical study on topical bismuth subgallate/borneol (Suile) dressing for treatment of diabetic foot ulcers]. [Chinese] . Zhongguo xiu fu chong jian wai ke za zhi [Chinese journal of reparative and reconstructive surgery] 2012;26(8):955‐960. [PubMed] [Google Scholar]
Additional references
Abbott 2002
- Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, et al. The North West Diabetes Foot Care Study: incidence of and risk factors for, new diabetic foot ulceration in a community‐based patient cohort. Diabetic Medicine 2002;19:377‐84. [DOI] [PubMed] [Google Scholar]
Apelqvist 2000a
- Apelqvist J, Bakker K, Houtum WH, Nabuurs‐Franssen MH, Schaper NC. International consensus and practical guidelines on the management and the prevention of the diabetic foot. International Working Group on the Diabetic Foot. Diabetes Metabolism Research and Review 2000;16(Suppl 1):S84‐92. [DOI] [PubMed] [Google Scholar]
Apelqvist 2000b
- Apelqvist J, Larsson J. What is the most effective way to reduce incidence of amputation in the diabetic foot?. Diabetes Metabolism Research and Reviews 2000;16(Suppl 1):S75‐83. [DOI] [PubMed] [Google Scholar]
Bergin 2006
- Bergin SM, Wraight P. Silver based wound dressings and topical agents for treating diabetic foot ulcers. Cochrane Database of Systematic Reviews 2006, Issue 1. [DOI: 10.1002/14651858.CD005082.pub2] [DOI] [PubMed] [Google Scholar]
BNF 2010
- British Medical Association and Royal Pharmaceutical Society of Great Britain. British National Formulary Appendix 8: Wound management products and elastic hosiery. http://www.bnf.org.uk/bnf/bnf/current Sept 2010;60.
Cardinal 2009
- Cardinal M, Eisenbud DE, Armstrong DG, Zelen C, Driver V, Attinger C, et al. Serial surgical debridement: a retrospective study on clinical outcomes in chronic lower extremity wounds. Wound Repair and Regeneration 2009;17(3):306‐11. [DOI] [PubMed] [Google Scholar]
Currie 1998
- Currie CJ, Morgan CL, Peters JR. The epidemiology and cost of inpatient care for peripheral vascular disease, infection, neuropathy, and ulceration in diabetes. Diabetes Care 1998;21(1):42‐8. [DOI] [PubMed] [Google Scholar]
Deeks 2002
- Deeks JJ. Issues in the selection of a summary statistic for meta‐analysis of clinical trials with binary outcomes. Statistics in Medicine 2002;21:1575‐600. [DOI] [PubMed] [Google Scholar]
Diabetes UK [Computer program]
- www.diabetes.org.uk. Key diabetes statistics and reports. www.diabetes.org.uk, accessed July 2011.
Dorresteijn 2010
- Dorresteijn JAN, Kriegsman DMW, Valk GD. Complex interventions for preventing diabetic foot ulceration. Cochrane Database of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/14651858.CD007610.pub2] [DOI] [PubMed] [Google Scholar]
Edwards 2010
- Edwards J, Stapley S. Debridement of diabetic foot ulcers. Cochrane Database of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/14651858.CD003556] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fiskin 1996
- Fiskin R, Digby M. Which dressing for diabetic foot ulcers?. Practical Diabetes International 1996;13(4):107‐9. [Google Scholar]
Gregg 2004
- Gregg EW, Sorlie P, Paulose‐Ram R, Gu Q, Eberhardt MS, Wolz M, et al. Prevalence of lower‐extremity disease in the U.S. adult population >40 years of age with and without diabetes. Diabetes Care 2004;27(7):1591‐7. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2009
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.2 [updated September 2009]. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
Hinchliffe 2008
- Hinchliffe R, Valk GD, Apelqvist J, Armstrong DG, Bakker K, Game FL, et al. A systematic review of the effectiveness of interventions to enhance the healing of chronic ulcers of the foot in diabetes. Diabetes Metabolism Research Review 2008;24(Suppl 1):S119‐44. [DOI] [PubMed] [Google Scholar]
Kumar 1994
- Kumar S, Ashe HA, Parnell LN, Fernando DJ, Tsigos C, Young RJ, et al. The prevalence of foot ulceration and its correlates in type 2 diabetic patients: a population‐based study. Diabetic Medicine 1994;11:480‐4. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J, on behalf of the Cochrane Information Retrieval Methods Group. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Margolis 1999
- Margolis D, Kantor J, Berlin J. Healing of diabetic neuropathic foot ulcers receiving standard treatment. A meta‐analysis. Diabetes Care 1999;22:692‐5. [DOI] [PubMed] [Google Scholar]
Mason 1999
- Mason J, O'Keeffe C, Hutchinson A, McIntosh A, Young R, Booth A. A systematic review of foot ulcer in patients with type 2 diabetes mellitus. II: treatment. Diabetes Medicine 1999;16(11):889‐909. [DOI] [PubMed] [Google Scholar]
Morris 1998
- Morris AD, McAlpine R, Steinke D, Boyle DI, Ebrahim AR, Vasudev N, et al. Diabetes and lower limb amputations in the community. A retrospective cohort study. DARTS/MEMO Collaboration. Diabetes Audit and Research in Tayside Scotland/Medicines Monitoring Unit. Diabetes Care 1998;21:738‐43. [DOI] [PubMed] [Google Scholar]
Murray 1996
- Murray HJ, Young MJ, Hollis S, Boulton AJ. The association between callus formation, high pressures and neuropathy in diabetic foot ulceration. Diabetic Medicine 1996;13:979‐82. [DOI] [PubMed] [Google Scholar]
Nelson 2006
- Nelson EA, O'Meara S, Golder S, Dalton J, Craig D, Iglesias C, DASIDU Steering Group. Systematic review of antimicrobial treatments for diabetic foot ulcers. Diabetes Medicine 2006;23(4):348‐59. [DOI] [PubMed] [Google Scholar]
O'Meara 2000
- Meara S, Cullum N, Majid M, Sheldon T. Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration. Health Technology Assessment 2000;4(21):1‐237. [PubMed] [Google Scholar]
Oyibo 2001
- Oyibo SO, Jude EB, Tarawneh I, Nguyen HC, Harkless LB, Boulton AJ. A comparison of two diabetic foot ulcer classification systems: the Wagner and the University of Texas wound classification systems. Diabetes Care 2001;24(1):84‐8. [DOI] [PubMed] [Google Scholar]
Pecoraro 1990
- Pecoraro RE, Reiber GE, Burgess EM. Pathways to diabetic limb amputation: basis for prevention. Diabetes Care 1990;13:513‐21. [DOI] [PubMed] [Google Scholar]
Pound 2005
- Pound N, Chipchase S, Treece K, Game F, Jeffcoate W. Ulcer‐free survival following management of foot ulcers in diabetes. Diabetic Medicine 2005;22(10):1306‐9. [DOI] [PubMed] [Google Scholar]
Reiber 1996
- Reiber G. The epidemiology of diabetic foot problems. Diabetic Medicine 1996;13S:S6‐11. [PubMed] [Google Scholar]
Reiber 1999
- Reiber GE, Vileikyte L, Boyko EJ, Aguila M, Smith DG, Lavery LA, et al. Causal pathways for incident lower extremity ulcers in patients with diabetes from two settings. Diabetes Care 1999;22:157‐62. [DOI] [PubMed] [Google Scholar]
RevMan 2011 [Computer program]
- The Nordic Cochrane Centre. Review Manager (RevMan). Version 5.1.. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration 2011.
Schaper 2004
- Schaper NC. Diabetic foot ulcer classification system for research purposes: a progress report on criteria for including patients in research studies. Diabetes Metabolism and Research Review 2004;20(S1):S90‐5. [DOI] [PubMed] [Google Scholar]
Schulz 2010
- Schulz KF, Altman DG, Moher D, CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Medicine 2010;7(3):e1000251. [DOI] [PMC free article] [PubMed] [Google Scholar]
SIGN 2009
- Scottish Intercollegiate Guidelines Network (SIGN). Search filters. http://www.sign.ac.uk/methodology/filters.html#random (accessed 14 July 2009).
Singh 2005
- Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA 2005;293:217‐28. [DOI] [PubMed] [Google Scholar]
Smith 2003
- Smith J. A national survey of podiatry practice in the treatment of diabetic foot ulcers. Unpublished.
Spencer 2000
- Spencer S. Pressure relieving interventions for preventing and treating diabetic foot ulcers. Cochrane Database of Systematic Reviews 2000, Issue 3. [DOI: 10.1002/14651858.CD002302] [DOI] [PubMed] [Google Scholar]
Steed 2006
- Steed DL, Attinger C, Colaizzi T, Crossland M, Franz M, Harkless L, et al. Guidelines for the treatment of diabetic ulcers. Wound Repair and Regeneration 2006;14(6):680‐92. [DOI] [PubMed] [Google Scholar]
Tesfaye 1996
- Tesfaye S, Stephens L, Stephenson J, Fuller J, Platter ME, Ionescu‐Tirgoviste C, et al. The prevalence of diabetic neuropathy and its relationship to glycaemic control and potential risk factors: The EURODIAB IDDM complications study. Diabetalogia 1996;39:1377‐84. [DOI] [PubMed] [Google Scholar]
Tierney 2007
- Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time‐to‐event data into meta‐analysis. Trials 2007;7(8):16. [DOI] [PMC free article] [PubMed] [Google Scholar]
Van Gils 1999
- Gils C, Wheeler LA, Mellsrom M, Brinton EA, Mason S, Wheeler CG. Amputation prevention by vascular surgery and podiatry collaboration in high risk diabetic and non‐diabetic patients ‐ the operation desert foot experience. Diabetes Care 1999;22(5):678‐83. [DOI] [PubMed] [Google Scholar]
Wagner 1981
- Wagner FW. The dysvascular foot: a system of diagnosis and treatment. Foot and Ankle 1981;2:64‐122. [DOI] [PubMed] [Google Scholar]
Wild 2004
- Wild S. Global prevalence of diabetes estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27(5):1047‐53. [DOI] [PubMed] [Google Scholar]
Winter 1963
- Winter GD, Scales JT. Effect of air drying and dressings on the surface of a wound. Nature 1963;197:91. [DOI] [PubMed] [Google Scholar]
Wrobel 2001
- Wrobel JS, Mayfield JA, Reiber GE. Geographic variation of lower limb extremity major amputation in individuals with and without diabetes in the Medicare population. Diabetes Care 2001;24:860‐4. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Gottrup 2002, 23‐25 May
- Gottrup F, Hahn TW, Thomsen JK. Cost‐effectiveness of hydrogel treatment in diabetic foot ulcers. 12th Conference of the European Wound Management Association. Granada, Spain, 2002, 23‐25 May.