

Abstract
The accuracy of using 2D anteroposterior (AP) pelvic radiographically determined cup coverage for patients with developmental dysplasia of the hip (DDH) after total hip arthroplasty (THA) to assess the cup coverage in retrospective clinical studies remains unclear. Cementless THA was performed on 20 DDH patients (20 hips). During surgery but after acetabular reconstruction, bone wax was pressed onto the uncovered surface of the acetabular cup. A surface model of the bone wax was generated by 3D scanning. The percentage of the acetabular cup covered in vivo by intact host acetabular bone was calculated by Geomagic Studio software. Acetabular cup coverage was also determined from a postoperative supine anteroposterior pelvic radiograph. The height of the hip center (distance from the center of the femoral head perpendicular to the inter-teardrop line) was also determined from radiographs. The radiographically determined cup coverage was a mean 6.93% (SD 2.47) lower than the in vivo determined cup coverage for 20 DDH patients (P<0.001). However, both methods yielded highly correlated cup coverage measurements (Pearson r=0.761, P<0.001). The size of the acetabular cup (P=0.001) but not the position of the hip center (high vs normal), was significantly associated with the difference between the radiographically determined and in vivo cup coverage. The 2D radiographically determined cup coverage conservatively reflects in vivo cup coverage and remains an important index (taking 7% underestimation errs and effect of greater underestimation of larger cup size into account) for assessing the stability of the cup and monitoring for adequate ingrowth of bone.
1. Introduction
Developmental dysplasia of the hip (DDH) is a leading cause of hip arthritis in young adults. Total hip arthroplasty (THA) is considered to be the standard of care when end-stage osteoarthritis (OA) results in significant pain and loss of function.1 During a THA, the placement of a standard-sized prosthetic acetabular cup in a dysplastic acetabulum may leave part of the cup uncovered by host bone because of the shallow and oval-shaped acetabulum. Lack of support from the host bone increases the stress at the bone-cup interface, which in turn increases the probability of mechanical failure.2 Thus, insufficient cup coverage is considered an adverse factor that leads to cup loosening.3–6
The purpose of measuring cup coverage in retrospective clinic studies is to find a value of cup coverage provided by the host bone stock of the acetabulum for durable fixation with acetabular cup during acetabular reconstruction for patients with developmental dysplasia of the hip (DDH). According to this value, joint surgeons could have scientific evidence and confidence to decide if structural bone graft or augment is required when insufficient cup coverage happens during acetabular reconstruction.2 Measuring the cup coverage on anteroposterior (AP) pelvic radiographs after surgery and in follow-up time is the simplest way and commonly used by previous retrospective clinic researches.7–12 Based on this metric, previous studies recommended at least 70% cup coverage by host bone for adequate stability during the period of host bone integration with the cup.5, 9, 13 Even greater (80%) coverage has been recommended for durable fixation with a cementless prosthesis.14 In addition, to determine cup coverage surgeons would use both the AP and the lateral pelvic radiographs taken at least 6 weeks after THA so that good quality radiographs are taken.
However, the radiograph-based measurement provides limited 2D information and could not reflect the real 3D cup coverage. The accuracy of using radiographically determined cup coverage remains unclear. Wang et al measured 3D cup coverage in a simulated DDH THA using a foam pelvic model and a motion capture system.6 Xu et al recently developed a 2D mapping technique to assess the 3D cup coverage.15 Although 3D cup coverage were measured by these studies to validate the accuracy of 2D radiograph-based measurement, these measurements were based on simulated computer models, and had difficulty representing the in vivo periacetabular bony defect of DDH hips and the in vivo cup coverage of THA, thus had limitation to validate the accuracy of 2D radiograph-based cup coverage.
To validate if the 2D radiographically determined cup coverage for patients with DDH after THA is an accurate index used to assess the real cup coverage by previous retrospective clinic studies, bone wax was used intraoperatively to create a model of the uncovered acetabular cup for each DDH patient. In vivo cup coverage was measured with a new technique involving 3D scanning and computer assisted curve surface modeling. We investigated the difference between radiographically determined and in vivo determined cup coverage and the impact of factors including height of hip center and acetabular cup size.
2. Materials and methods
Participants and surgical procedure
A diagnosis of OA secondary to DDH was made by an expert orthopaedic surgeon using the Crowe classification.16 Inclusion criteria included: (1) primary cementless THA; (2) no history of infection; (3) a clearly distinguished region of the acetabular cup that was not covered by the host bone after acetabular reconstruction during surgery. Computer assisted preoperative planning was adopted for each patient under the guidance of the same surgeon.17 Participants who required structural bone graft or augment during acetabular reconstruction were excluded. All cases of cementless THA were performed by the same surgeon using a posterolateral approach and involving the use of the same type of acetabular cup (Pinnacle, DePuy, Warsaw, Indiana). The acetabulum was reamed to a diameter of 1 mm less than the acetabular cup size. 40° abduction and 15° anteversion angle of the cup was adopted for each patient, respectively (Figures 1A & B). The study was approved by the Institution’s Clinical Research Ethics Board and all participants provided written informed consent.
Figure 1A-E.
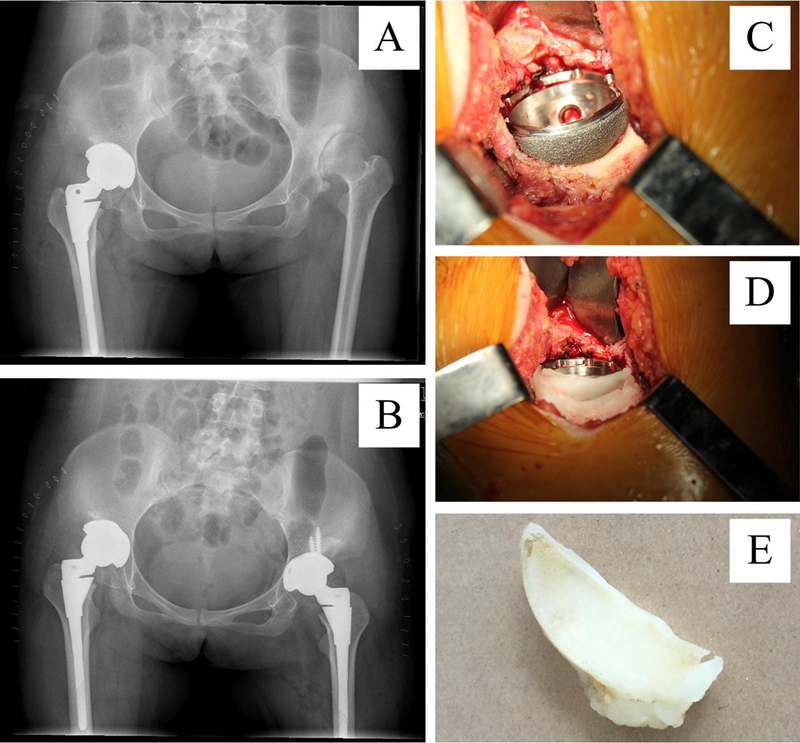
Acetabular reconstruction and methods of determining the area of uncovered acetabular cup in vivo. A preoperative (A) and postoperative (B) anteroposterior pelvic radiograph. (C). After acetabular reconstruction during surgery, the uncovered surface of cup was shown. (D). Bone wax pressed on the uncovered surface of the acetabular cup. (E). Bone wax model representing the uncovered surface was removed from the cup.
From January 1, 2014 to May 20, 2016, 20 patients (4 male, 16 female) with DDH (20 hips) were included. Among them, 6 were Crowe I, 6 were Crowe II, 3 were Crowe III, 5 were Crowe IV. The mean (standard deviation) age, height and weight of the patients at the time of THA were 54.4 (16.6) years (range 32 to 76 years), 160.4 (9.0) cm (range 145 to 177 cm) and 58.2 (11.9) kg (range 45 to 82 kg), respectively. The mean size of the acetabular cup used in acetabular reconstruction was 48.8 (3.0) mm (range 44 to 52 mm).
In vivo determined acetabular cup coverage
During surgery but after acetabular reconstruction, uncovered surface of the acetabular cup was shown (Figure 1C). 5.0g bone wax (Johnson and Johnson international, Warsaw, Indiana) was pressed onto the uncovered surface of the acetabular cup to create a bone wax model representing the uncovered area (Figure 1D).The bone wax model was carefully removed from the cup, cleaned by submersion in normal saline and retained at room temperature until measured (Figure 1E).To quantify the uncovered cup area, the bone wax model was 3D scanned (CRONOS 3D Scanner, Open Technologies Srl, Rezzato, Italy) as shown in Figure 2A. The point cloud data of the bone wax model were recorded using a data acquisition software (Phasen 3DMV, Open Technologies Srl, Rezzato, Italy) and exported in ASC format, as shown in Figure 2B. The point cloud data were processed in Geomagic Studio (version 12.0.0, Geomagic, North Carolina, USA) to generate a surface model of the bone wax. The uncovered cup surface was identified from the bone wax model according to the feature boundary line (Figure 2C) and then smoothed. The area of the uncovered cup surface (A1) was calculated automatically in Geomagic Studio software (Figure 2D). Acetabular cups of known sizes (44, 46, 48 and 52 mm) were also 3D scanned and data processed using the same procedure as above. The cup area representing the porous coated surface (A2) was recorded. The in vivo percentage of each acetabular cup covered by intact host acetabular bone was determined using the following equation.
Figure 2A-D.
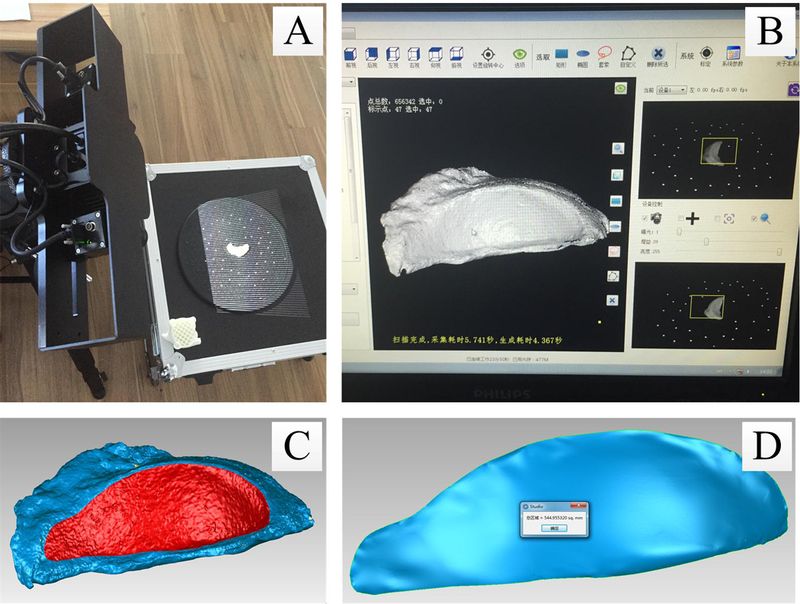
3D scan and processing of the bone wax model representing the uncovered surface of the acetabular cup. (A). 3D scanning. (B). Point cloud data processing. (C). Surface identification. (D). Area calculation.
Radiographically determined acetabular cup coverage
Supine anteroposterior pelvic radiographs were obtained one day after THA (Figure 3). The uncovered cup angle (α) was measured.9 The radiographically determined percentage of each acetabular cup covered by intact host acetabular bone was recorded using the following equation.
Figure 3.
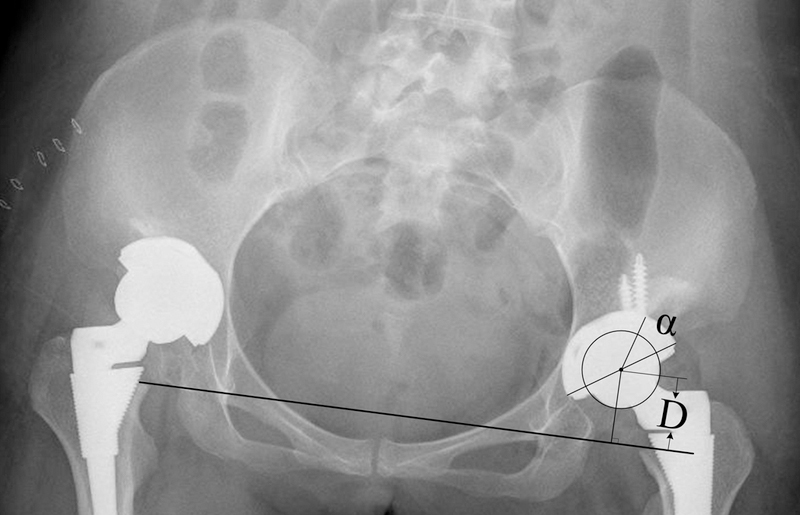
Radiographically determined cup coverage and high hip center measurement. α: The uncovered cup angle; D: The height of the hip center.
The position of the cup was defined as the vertical distance of the center of rotation in relation to the acetabular teardrop as described by Russotti and Harris.18 The height of the hip center was defined as the vertical distance along a line extending from the center of the femoral head perpendicular to the inter-teardrop line (Figure 3). A high arthroplasty hip center was defined as a center at least 35 mm above the anatomic teardrop;19 a normal hip center was defined as within 0–35 mm above the anatomic teardrop.
Statistics
A paired t-test was conducted to evaluate the mean differences between radiographically determined and in vivo determined acetabular cup coverage. An unpaired t-test was used to compare the cup coverage by difference in hip center heights. Pearson’s correlation was used to evaluate the association between radiographically determined and in vivo determined cup coverage, and between cup size and A cup coverage (in vivo determined cup coverage-radiographically determined cup coverage). All statistical analyses were performed using SPSS statistical software version 19.0 (IBM, Armonk, NY). A value of P<0.05 was considered significant.
3. Results
The mean radiographically determined cup coverage for all patients was 84.27 (3.63)%. The radiographically determined cup coverage was significantly less (P<0.001) than the in vivo determined cup coverage for the patients overall and for both the high hip center and the normal hip center groups. The mean percent difference (Δ cup coverage) between in vivo determined and radiographically determined cup coverage, 6.93 (2.47)% (range 1.94 to 12.23%), was similar for both the high and normal hip center groups (Table 1). Cup coverage by both in vivo determined and radiographically determined methods, was significantly higher (P=0.017 and 0.002, respectively) for the normal hip center group compared with the high hip center group.
Table 1.
Radiographic versus in vivo determined cup coverage.
| Radiographic cup coverage (%) |
In vivo cup coverage (%) |
Δ cup coverage (%) |
P value (P1) |
|
|---|---|---|---|---|
| All patients (n=20) | 84.27 (3.63) | 91.20 (3.50) | 6.93 (2.47) | <0.001 |
| High hip center(n=8) | 81.42 (2.62) | 88.99 (3.59) | 7.57 (1.18) | <0.001 |
| Normal hip center (n=12) | 86.17 (2.92) | 92.67 (2.67) | 6.50 (3.02) | <0.001 |
| P value (P2) | 0.002 | 0.017 | 0.357 | |
Δ cup coverage (%)=in vivo cup coverage–radiographic cup coverage; P1: Comparing radiographic and in vivo cup coverage; P2: Comparing high and normal hip center groups.
Means (standard deviations) are provided above for cup coverage.
Radiographically determined cup coverage was significantly correlated with In vivo determined cup coverage (Correlation coefficient=0.761, P<0.001, Figure 4A). Larger acetabular cup size was positively associated with larger percent difference (A cup coverage) between in vivo determined and radiographically determined cup coverage (Correlation coefficient = 0.697, P = 0.001, Figure 4B).
Figure 4A-B.
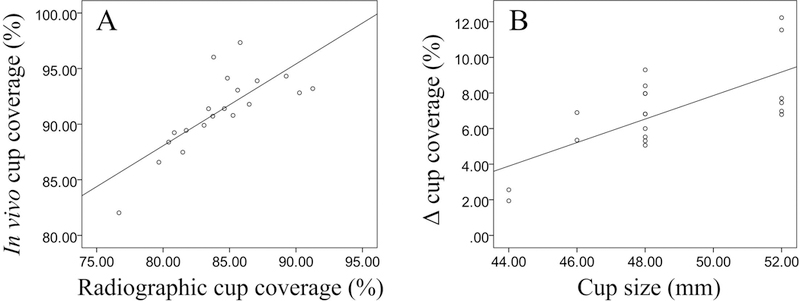
Correlation analysis. (A). Correlation (r=0.761, P<0.001) between radiographically determined and in vivo determined cup coverage. (B). Correlation (r=0.697, P=0.001) between acetabualar cup size and Δ cup coverage defined as the difference between cup coverage determined radiographically versus in vivo as follows:
Δ cup coverage (%)=in vivo cup coverage-radiographical cup coverage.
4. Discussion
Various methods have been proposed for determining cup coverage from anteroposterior (AP) pelvic radiographs. One such method involves measuring the circumference of the cup in contact with the host bone.11 Another method involves measuring the percentage of the cup area covered by host bone.6 Using radiographically determined methods, Mulroy and Harris recommended at least 70% coverage of the cup by intact native bone,9 whereas Hartofilakidis et al. recommended 80% coverage for a cementless acetabular component.14 However, these determinations were all based on the 2D information from radiographs that has an uncertain accuracy to assess the real cup coverage.
Two past studies reported that radiographically determined methods overestimate cup coverage of THA by 12.73% to 15% in DDH patients.6, 15 In contrast, in our study we found that radiographically determined cup coverage tended to underestimate the in vivo determined cup coverage by a mean 6.93 (2.47)%, and the Pearson’s correlation coefficient (0.761) between the two methods was more than previously reported (0.470) by Wang et al.6 These differences are likely attributable to differences in measurement methodology. Wang et al.6 created 6 DDH-THA foam pelvic models; the 3D cup coverage was measured using a motion capture system and imaging software. Xu et al.15 simulated acetabular cup implantation and calculated the 3D coverage using a 3D model and image mapping technique. For these two previous studies, 3D cup coverage was determined by in vitro simulation and without in vivo validation. However, our study measured the 3D cup coverage in vivo directly from a bone wax model created intra-operatively. Our results support the supposition that radiographically determined cup coverage underestimates in vivo determined cup coverage due to poor visualization of the posterior acetabulum on anteroposterior radiographs (Figure 5). In addition, the methodology of in vivo measured acetabular cup coverage in our study could be potentially used in prospective studies related to uncoverage of cups in both primary and revision hip replacement scenarios.
Figure 5A-B.
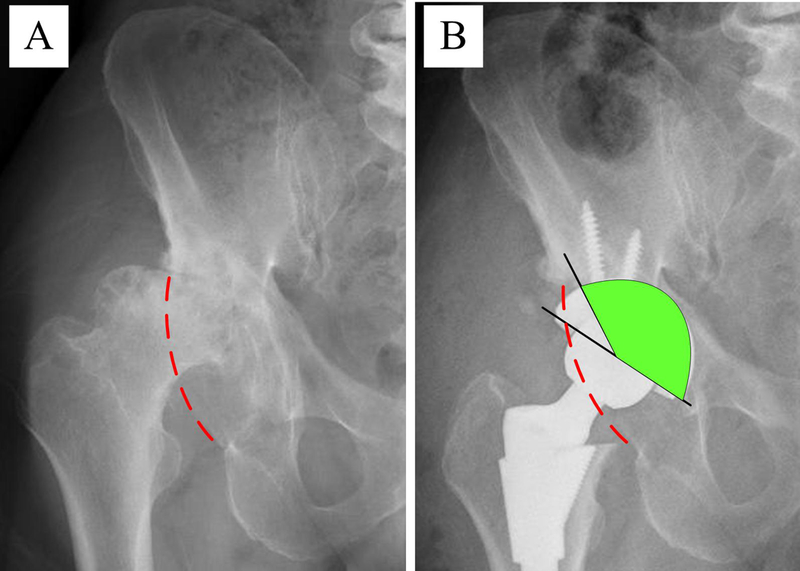
Schematic diagram illustrating why the 2D radiographically determined cup coverage tended to underestimate the in vivo determined cup coverage. Preoperative (A) and postoperative (B) anteroposterior pelvic radiographs. The red dashed line represents the edge of the posterior acetabulum; the green region represents the 2D radiographic cup coverage. In this case, the 2D radiographically determined and the in vivo determined cup coverage were 83.80% and 96.03%, respectively. The biggest single Δ cup coverage equaled 12.23%.
In dysplastic hips, the superolateral acetabular deficiency prevents placement of a standard cup due to inadequate coverage. Special techniques, such as a high hip center, may be necessary to address inadequate bone coverage by the acetabular component.2, 17–21 Based on our results, the vertical position of the acetabular reconstruction would not be expected to influence the difference between the 2D radiographic and 3D in vivo cup coverage. Interestingly, we found that a larger acetabular cup size was associated with a tendency for greater underestimation of the in vivo cup coverage by the radiographically determined cup coverage method. This finding further supports our supposition that the portion of cup covered by the posterior acetabulum is not accounted for by the radiographically determined cup coverage calculation due to poor visualization of this region on the radiograph.
There are a number of limitations that must be taken into account and should be addressed in future studies. First, the sample size was relatively small. Second, in our study participants who required structural bone graft or augment during acetabular reconstruction were excluded, which might weaken the sample integrity. Third, this was a cross-sectional study. Follow up of these DDH patients will be necessary to investigate the association of in vivo determined cup coverage on clinical and biomechanical outcomes.
5. Conclusion
In conclusion, our study measured 3D acetabular cup coverage in vivo for DDH patients based on a bone wax model created intra-operatively of the uncovered cup surface area. Although the 2D radiographically determined cup coverage tended to underestimate the in vivo determined cup coverage by 7%, an underestimation errs on the side of safety compared with an overestimation as suggested by previous studies. Therefore, to find a value of cup coverage provided by the host bone stock of the acetabulum for durable fixation with acetabular cup during acetabular reconstruction for patients with DDH, the 2D radiographically determined cup coverage remains an important index and the simplest way (taking 7% underestimation errs and effect of greater underestimation of larger cup size into account) for assessing the in vivo cup coverage whose measurement is impractical for each DDH patient. However, the methodology of in vivo measured acetabular cup coverage in our study could be potentially used in prospective studies related to uncoverage of cups in both primary and revision hip replacement scenarios. With the development of acetabular cup design, the value of cup coverage provided by the host bone stock of the acetabulum for durable fixation need further investigation in retrospective clinic researches for patients with DDH.
Acknowledgements
This work was supported by National Natural Science Foundation of China under Grant (81601894) and Science & Technology Foundation of Sichuan Province of China (2017HH0062) as well as the NIH/NIA 028716. The authors do not have any proprietary interests in the materials described in the article.
References
- 1.Sanchez-Sotelo J, Berry DJ, Trousdale RT, Cabanela ME. Surgical treatment of developmental dysplasia of the hip in adults: II. Arthroplasty options. The Journal of the American Academy of Orthopaedic Surgeons 2002;10:334–344. [DOI] [PubMed] [Google Scholar]
- 2.Dapuzzo MR, Sierra RJ. Acetabular considerations during total hip arthroplasty for hip dysplasia. The Orthopedic clinics of North America 2012;43:369–375. [DOI] [PubMed] [Google Scholar]
- 3.Chougle A, Hemmady MV, Hodgkinson JP. Severity of hip dysplasia and loosening of the socket in cemented total hip replacement. A long-term follow-up. J Bone Joint Surg Br 2005;87:16–20. [PubMed] [Google Scholar]
- 4.Hartofilakidis G; Karachalios T. Total hip arthroplasty for congenital hip disease. J Bone Joint Surg Am 2004;86-a:242–250. [DOI] [PubMed] [Google Scholar]
- 5.Hartofilakidis G; Stamos K, Karachalios T. Treatment of high dislocation of the hip in adults with total hip arthroplasty. Operative technique and long-term clinical results. J Bone Joint Surg Am 1998;80:510–517. [DOI] [PubMed] [Google Scholar]
- 6.Wang L, Thoreson AR, Trousdale RT, Morrey BF, Dai K, An KN. Two-dimensional and three-dimensional cup coverage in total hip arthroplasty with developmental dysplasia of the hip. Journal of biomechanics 2013;46:1746–1751. [DOI] [PubMed] [Google Scholar]
- 7.Anwar MM, Sugano N, Masuhara K, Kadowaki T, Takaoka K, Ono K. Total hip arthroplasty in the neglected congenital dislocation of the hip. A five- to 14-year follow-up study. Clin Orthop Relat Res 1993:127–134. [PubMed] [Google Scholar]
- 8.Dewal H, Chen F, Su E, Di Cesare PE. Use of structural bone graft with cementless acetabular cups in total hip arthroplasty. The Journal of arthroplasty 2003;18:23–28. [DOI] [PubMed] [Google Scholar]
- 9.Mulroy RD Jr., Harris WH. Failure of acetabular autogenous grafts in total hip arthroplasty. Increasing incidence: a follow-up note. J Bone Joint Surg Am 1990;72:1536–1540. [PubMed] [Google Scholar]
- 10.Sarmiento A, Ebramzadeh E, Gogan WJ, McKellop HA. Cup containment and orientation in cemented total hip arthroplasties. J Bone Joint Surg Br 1990;72:996–1002. [DOI] [PubMed] [Google Scholar]
- 11.Silber DA, Engh CA. Cementless total hip arthroplasty with femoral head bone grafting for hip dysplasia. The Journal of arthroplasty 1990;5:231–240. [DOI] [PubMed] [Google Scholar]
- 12.Sugano N, Nishii T, Nakata K, Masuhara K, Takaoka K. Polyethylene sockets and alumina ceramic heads in cemented total hip arthroplasty. A ten-year study. J Bone Joint Surg Br 1995;77:548–556. [PubMed] [Google Scholar]
- 13.Anderson MJ, Harris WH. Total hip arthroplasty with insertion of the acetabular component without cement in hips with total congenital dislocation or marked congenital dysplasia. J Bone Joint Surg Am 1999;81:347–354. [DOI] [PubMed] [Google Scholar]
- 14.Hartofilakidis G Georgiades G Babis GC, Yiannakopoulos CK. Evaluation of two surgical techniques for acetabular reconstruction in total hip replacement for congenital hip disease: results after a minimum ten-year follow-up. J Bone Joint Surg Br 2008;90:724–730. [DOI] [PubMed] [Google Scholar]
- 15.Xu J, Xu C, Mao Y, Zhang J, Li H, Zhu Z. Posterosuperior Placement of a Standard-Sized Cup at the True Acetabulum in Acetabular Reconstruction of Developmental Dysplasia of the Hip With High Dislocation. The Journal of arthroplasty 2016;31:1233–1239. [DOI] [PubMed] [Google Scholar]
- 16.Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am 1979;61:15–23. [PubMed] [Google Scholar]
- 17.Nie Y, Pei F, Shen B, Kang P, Li Z. Implication of acetabular width on the anteroposterior pelvic radiograph of patients with developmental dysplasia of the hip. The Journal of arthroplasty 2015;30:489–494. [DOI] [PubMed] [Google Scholar]
- 18.Russotti GM, Harris WH. Proximal placement of the acetabular component in total hip arthroplasty. A long-term follow-up study. J Bone Joint Surg Am 1991;73:587–592. [PubMed] [Google Scholar]
- 19.Antoniades J, Pellegrini VD Jr. Cross-sectional anatomy of the ilium: implications for acetabular component placement in total hip arthroplasty. Clin Orthop Relat Res 2012;470:3537–3541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chen M, Luo Z-L, Wu K-R, Zhang X-Q, Ling X-D, Shang X-F. Cementless Total Hip Arthroplasty With a High Hip Center for Hartofilakidis Type B Developmental Dysplasia of the Hip: Results of Midterm Follow-Up. The Journal of arthroplasty 2016;31:1027–1034. [DOI] [PubMed] [Google Scholar]
- 21.Restrepo C, Grisafi F, Rothman RH. Total hip arthroplasty in patients with developmental dysplasia of the hip. Semin Arthroplasty 2005;16:80–85. [Google Scholar]