

Abstract
Recently, traction‐assisted endoscopic submucosal dissection (ESD) using a clip and thread was reported as useful for treating lesions in the esophagus, stomach, and colorectum in terms of shortening the duration of the procedures and reducing the risk of intraoperative perforation. However, no traction method using the thread and clip for duodenal ESD as described in this article has been reported to date. We report a case in which traction‐assisted ESD using dental floss and a clip was successfully performed on a huge superficial nonampullary duodenal epithelial tumor accompanied by severe fibrosis caused by preoperative biopsies. A 65‐year‐old woman had a 55‐mm flat‐elevated tumor in the second part of the duodenum. Severe fibrosis of the submucosal layer was expected due to repeated biopsies at the same site by the patient’s previous endoscopist. We selected ESD for this lesion, and the initial incision was started from the side proximal to the lesion, but it was difficult to insert the scope under the submucosal layer directly beneath the biopsy scar. Therefore, traction with an endoclip and dental floss was performed to lift the lesion. Excellent traction allowed safe resection of the fibrotic part under accurate visual observation. Finally, the lesion was resected en bloc without adverse events. Traction‐assisted ESD using dental floss and a clip is likely to be an effective adjunctive technique for quick, safe, and successful resection of lesions in the duodenum on which it is difficult to perform ordinary ESD and that have a high probability of intraoperative perforation and massive bleeding.
Keywords: dental floss, duodenal endoscopic submucosal dissection, severe fibrosis, superficial nonampullary duodenal epithelial tumor, traction‐assisted endoscopic submucosal dissection
Introduction
Endoscopic submucosal dissection (ESD) for superficial nonampullary duodenal epithelial tumors (SNADETs) is technically challenging1 because of the high risks of perforation and bleeding. In particular, ESD of a SNADET that cannot be easily lifted by local injection due to pronounced fibrosis associated with preoperative biopsy sampling is very difficult. Recently, traction‐assisted ESD using a clip and thread was reported as useful for treating lesions in the esophagus,2 stomach,3 and colorectum4 in terms of shortening the duration of the procedures and reducing the risk of intraoperative perforation. However, no traction method using thread and clip for duodenal ESD as described in this article has been reported to date. We report a case in which traction‐assisted ESD using dental floss and a clip was successfully performed on a huge SNADET accompanied by severe fibrosis caused by preoperative biopsies.
Case Report
A 65‐year‐old woman was referred to our hospital for evaluation of a huge duodenal tumor. On esophagogastroduodenoscopic examination, she had a 55‐mm flat‐elevated tumor distal to the major papilla in the second part of the duodenum (Fig. 1a). Severe fibrosis of the submucosal layer was expected due to repeated biopsies at the same site by the patient’s previous endoscopist. The histological diagnosis by biopsy was well‐differentiated adenocarcinoma. The depth of the lesion was diagnosed by endoscopic ultrasonography (UM‐2R system; Olympus, Tokyo, Japan), and submucosal invasion was not suspected. As no lymph node or distant metastasis was observed on abdominal computed tomography, it was diagnosed as early duodenal cancer. Therefore, we selected ESD for en bloc resection of this huge lesion.
Figure 1.
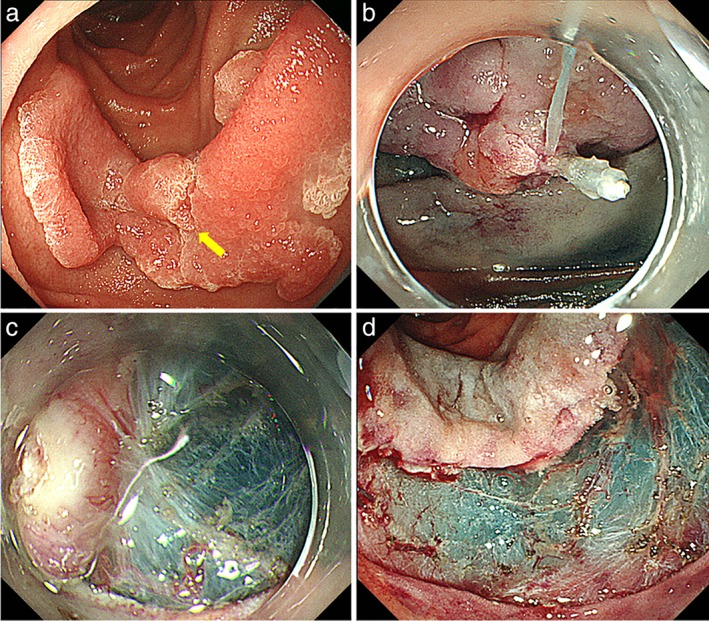
Endoscopic views. (a) A 55‐mm flat‐elevated tumor is located in the second part of the duodenum. Yellow arrow, a preoperative biopsy scar. (b) Traction technique using a clip and dental floss to lift the lesion. (c) Severe submucosal fibrosis associated with preoperative biopsy sampling. (d) Mucosal defect after endoscopic submucosal dissection.
The ESD procedure was performed under general anesthesia in the operating room using an upper gastrointestinal endoscope (GIF260J; Olympus) with a transparent attachment cap. The procedure was performed using a high‐frequency generator unit (VIO300D; Erbe Elektromedizin, Tübingen, Germany) with carbon dioxide insufflation. Subsequent to the local injection of sodium hyaluronate solution, a mucosal incision and submucosal dissections were performed using a Dual knife (KD650Q; Olympus). The initial incision was started from the side proximal to the lesion, but it was difficult to insert the scope under the submucosal layer directly beneath the biopsy scar. Therefore, traction with an endoclip (HX‐610‐135; Olympus Medical Systems Corp.) and dental floss was performed to lift the lesion (Fig. 1b). Severe submucosal fibrosis was found (Fig. 1c). Excellent traction allowed safe resection of the fibrotic part under accurate visual observation. The procedure time was 1 h, and the patient did not develop any adverse events such as intraoperative perforation and massive bleeding. The mucosal defect extended over about half of the circumference of the duodenum (Fig. 1d, Video Clip S1, Supporting information). The mucosal defect was completely closed using an endoloop and two 9‐mm over‐the‐scope clips (Ovesco Endoscopy GmbH, Tübingen, Germany) to prevent delayed perforation.5 The patient did not develop any adverse events and was discharged on day 3 after ESD. Histopathological examination demonstrated that the lesion was a well‐differentiated intramucosal cancer with no lymphovascular invasion and negative margins.
Discussion
In the present case, we showed the case of successful traction‐assisted ESD using dental floss and a clip for a huge SNADET in which severe fibrosis of the submucosal layer was expected due to repeated biopsies. Traction‐assisted ESD methods include thread and clip traction,4, 6 S‐O clip,6 ring‐shaped thread traction,7 clip‐flap method,8 and clip‐and‐snare method.9 For ESD of lesions in the esophagus, stomach, and colorectum, the most appropriate method is selected by considering several factors, such as the space within the hollow organ where the lesion is located and the need for removing the scope while applying traction. Regarding duodenal ESD, traction application using an S‐O clip6 and ring‐shaped thread7 has been reported. However, the traction force cannot be controlled in these traction methods, and these devices are anchored to the duodenal mucosa on the opposite wall. Therefore, they have limitations; for example, removal of the specimen and these devices after ESD is complicated. In this context, the traction method using dental floss is inexpensive and technically simple, and the traction force can be controlled.
However, in duodenal ESD, the traction method using dental floss and a clip is expected to have limitations. Characteristically, the duodenum is a highly curved organ. Thus, it is more difficult to directly apply traction force to a SNADET located at a bend, such as the superior and inferior duodenal angles, compared to those located in the esophagus and stomach, and there is a possibility of failure to achieve sufficient traction along the intended direction. Even in the case of failure to achieve sufficient traction, the traction method using dental floss and a clip has an advantage. The traction procedure can be reperformed by cutting the dental floss or removing the clip from the specimen. Therefore, we believe it is beneficial to actively use the traction method using dental floss and a clip for cases of duodenal ESD in which it is difficult to insert the scope under the submucosal layer due to poor scope maneuverability, severe fibrosis, or any other reason. The traction method is likely to be an effective adjunctive technique for quick, safe, and successful resection of lesions in the duodenum on which it is very difficult to perform ESD and which have a potentially high probability of intraoperative perforation and bleeding. We continue to further accumulate data on duodenal ESD cases using this traction method and will report its effectiveness in the future.
Supporting information
Video Clip S1 Successful traction‐assisted endoscopic submucosal dissection using dental floss and a clip for a huge nonampullary duodenal epithelial tumor with severe fibrosis.
Declaration of conflict of interest: None of the authors has any competing interests to declare.
References
- 1. Yahagi N, Kato M, Ochiai Y et al Outcomes of endoscopic resection for superficial duodenal epithelial neoplasia. Gastrointest. Endosc. 2018. in press; 88: 676–82. [DOI] [PubMed] [Google Scholar]
- 2. Koike Y, Hirasawa D, Fujita N et al Usefulness of the thread‐traction method in esophageal endoscopic submucosal dissection: randomized controlled trial. Dig. Endosc. 2015; 27: 303–9. [DOI] [PubMed] [Google Scholar]
- 3. Yoshida M, Takizawa K, Suzuki S et al Conventional versus traction‐assisted endoscopic submucosal dissection for gastric neoplasms: a multicenter, randomized controlled trial (with video). Gastrointest. Endosc. 2018; 87: 1231–40. [DOI] [PubMed] [Google Scholar]
- 4. Yamasaki Y, Takeuchi Y, Uedo N et al Efficacy of traction‐assisted colorectal endoscopic submucosal dissection using a clip‐and‐thread technique: a prospective randomized study. Dig. Endosc. 2018; 30: 467–76. [DOI] [PubMed] [Google Scholar]
- 5. Tashima T, Ohata K, Sakai E et al Efficacy of an over‐the‐scope clip for preventing adverse events after duodenal endoscopic submucosal dissection: a prospective interventional study. Endoscopy. 2018; 50: 487–96. [DOI] [PubMed] [Google Scholar]
- 6. Hashimoto R, Hirasawa D. Duodenal endoscopic submucosal dissection with traction method using the S‐O clip. Dig. Endosc. 2017; 29: 635. [DOI] [PubMed] [Google Scholar]
- 7. Goda Y, Mori H, Kobara H, Masaki T. Efficacy of sufficient operation view by ring‐shaped thread counter traction for safer duodenal ESD. Minim. Invasive Ther. Allied Technol. 2018: 1–6. [DOI] [PubMed] [Google Scholar]
- 8. Yamamoto K, Hayashi S, Saiki H et al Endoscopic submucosal dissection for large superficial colorectal tumors using the "clip‐flap method". Endoscopy. 2015; 47: 262–5. [DOI] [PubMed] [Google Scholar]
- 9. Yamada S, Doyama H, Ota R et al Impact of the clip and snare method using the prelooping technique for colorectal endoscopic submucosal dissection. Endoscopy. 2016; 48: 281–5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video Clip S1 Successful traction‐assisted endoscopic submucosal dissection using dental floss and a clip for a huge nonampullary duodenal epithelial tumor with severe fibrosis.