

Abstract
Researchers have argued there are bidirectional associations between heavy alcohol use and sexual assault; however, research in this area is inconclusive due to methodological differences, particularly in study design. The purpose of this study is to clarify the longitudinal associations between heavy alcohol use and incapacitated sexual assault among first-year college women, accounting for hypothesized autoregressive effects within each construct over their first year of college. A sample of 483 women completed regular surveys that assessed a range of health behaviors, including alcohol use and sexual behavior, during their first year of college. We used cross-lagged analyses to examine prospective associations between incapacitated sexual assault and heavy alcohol use (frequency of heavy episodic drinking and peak blood alcohol content). There were significant autoregressive effects, such that women who were engaging in heavier alcohol use as they entered college continued to be heavier alcohol users throughout their first year, and women with a history of assault at college entry were at greater risk for assault during their first year of college. There was a significant cross-lagged effect from precollege incapacitated assault to first-semester alcohol use after controlling for pre-college alcohol use. There were no significant cross-lag paths from alcohol use to subsequent incapacitated assault. Women with a history of incapacitated sexual assault engaged in heavier drinking during their transition to college, but heavy alcohol use did not predict subsequent assault risk.
Keywords: Sexual assault, College women, Alcohol use, Longitudinal study, Cross-lagged analysis
1. Introduction
Sexual assault and alcohol misuse are pressing public health concerns for young women. Systematic reviews highlight that one in five women endorse they were sexually assaulted in college (Muehlenhard, Peterson, Humphreys, & Jozkowski, 2017), with first- and second-year women demonstrating the greatest risk of assault (Humphrey & White, 2000; Krebs, Lindquist, Warner, Fisher, & Martin, 2009). Notably, the transition into college also coincides with an increase in alcohol use (Sher & Rutledge, 2007) and alcohol-involved assault, specifically incapacitated sexual assault (i.e., assault that occurs when an individual is unable to consent or object due to alcohol or drug intoxication) (Carey, Durney, Shepardson, & Carey, 2015). During their first semester alone, 8% of women experience an attempted or completed incapacitated sexual assault (i.e., unwanted oral, vaginal, or anal sex) (Carey et al., 2015). Importantly, heavy episodic drinking (HED) is associated with risk of sexual assault among college women, and this association is stronger during the first semester of college (Testa & Hoffman, 2012).
In an effort to design efficacious prevention programming, and given the long-term impact of sexual assault on physical and psychological well-being (Paras et al., 2009), researchers have attempted to identify the temporal associations between alcohol use and sexual assault. Some researchers have hypothesized that heavy alcohol use and sexual assault evidence bidirectional associations over time (Bryan et al., 2016; Ullman, 2003), although most research in this area has examined only whether heavy alcohol use is prospectively associated with sexual assault. Heavier alcohol use might contribute to increased risk over time through the normalization of unwanted sexual contact in drinking settings (Thompson & Cracco, 2008), decreased risk perception, and less reliance on active resistance strategies (e.g., Stoner et al., 2007; Testa, Vanzile-Tamsen, Livingston, & Buddie, 2006). Many researchers have found support for this prospective association among college women (Gidycz et al., 2007; McCauley, Calhoun, & Gidycz, 2010; Messman-Moore, Ward, & Brown, 2009; Mouilso, Fischer, & Calhoun, 2012); however, other researchers have found this path to be non-significant after controlling for alcohol use over time (e.g., both prior and current levels of use: Parks, Hsieh, Taggart, & Bradizza, 2014; Testa & Hoffman, 2012).
Less work has examined the temporal pathway from sexual violence to subsequent alcohol use longitudinally; however, given the prevalence of sexual assault, this pathway is critical to the design of efficacious support services. Assault may lead to subsequent increases in alcohol use as women cope with the distress and psychological sequelae of assault (e.g., self-medication hypothesis). Much of the research in this area has focused on childhood sexual abuse (CSA). Women with a history of CSA demonstrate more alcohol misuse than their peers (e.g., Langeland & Hartgers, 1998; Moncrieff & Farmer, 1998), often attributed to drinking to cope motives (Grayson & Nolen-Hoeksema, 2005); alcohol misuse, in turn, predicts revictimization risk (Messman-Moore & Long, 2002). However, longitudinal investigations are needed, because it is possible that women were already engaging in heavier drinking they merely sustain, or that dysphoric symptoms pursuant to a sexual assault actually curtail drinking (e.g., Kaysen et al., 2014). Whereas Parks et al. (2014) found that heavier alcohol use followed a sexual assault (Parks et al., 2014), other researchers have not found support for this pathway among college women (e.g., Gidycz et al., 2007; Kaysen, Neighbors, Martell, Fossos, & Larimer, 2006; Parks, Hsieh, Bradizza, & Romosz, 2008) or women generally (e.g., Testa, Livingston, & Hoffman, 2007).
Therefore, the research evidence regarding the bidirectional associations between heavy alcohol use and sexual assault risk is far from definitive. In a sample of first-year college women, this study seeks to clarify prior findings using cross-lagged modeling to examine the associations between heavy alcohol use and incapacitated assault, and thereby inform the less-often examined pathway from assault to subsequent alcohol use.
1.1. Synthesizing the findings: Directionality of alcohol and assault risk
Discrepant findings across studies are likely due to methodological and design considerations, including differing definitions of sexual assault and methodological approaches. First, the definition of sexual assault impacts findings, such that severe sexual assault appears to be associated with subsequent increases in heavy alcohol use (e.g., Parks et al., 2014), whereas any form of unwanted touching is not (e.g., Gidycz et al., 2007; Mouilso et al., 2012; Parks et al., 2008; Testa et al., 2007). In a sample of community women, Testa et al. (2007) examined the longitudinal effect of rape versus any sexual victimization on subsequent heavy drinking. In most cases, they found that neither rape nor any sexual victimization predicted subsequent drinking after controlling for prior drinking. However, when there were differences between assault severity – for example, when predicting maximum drinks per occasion – they found that rape was a significant predictor above and beyond prior alcohol use, but any level of sexual victimization was not.
Second, a prior sexual assault robustly predicts victimization risk (e.g., Testa & Hoffman, 2012) and problematic alcohol use robustly predicts future heavy alcohol use over college (e.g., Borsari, Murphy, & Barnett, 2009; Crosnoe, Kendig, & Benner, 2018). Therefore, it is imperative to account for the robust effects of within-construct stability when examining a bidirectional hypothesis. When studies have controlled for the robust predictive effect of prior drinking history, they have typically found that sexual victimization does not prospectively predict heavy alcohol use (e.g., Messman-Moore, Coates, Gaffey, & Johnson, 2008; Mouilso et al., 2012). However, this is not the case in all studies. For example, Bryan et al. (2016) followed a community-drawn sample of sexually active women who engaged in binge drinking. They found support for a reciprocal relationship between alcohol use and sexual victimization over 1 year, such that women who experienced sexual victimization drank more at the subsequent time point, and greater drinking predicted assault risk over the follow-up period. In another study, Parks et al. (2014) followed first-year college women annually over a period of 5 years. Using HLM, they modeled alcohol use and victimization risk in separate models controlling for the other. After doing so, they did not find that alcohol prospectively predicted sexual assault risk, but they did find that an assault predicted subsequent increases in heavy drinking. Given that most research in this area is inconsistent with that of Parks et al. (2014) in finding support for the prospective pathway from problematic alcohol use to assault risk (e.g., Bryan et al., 2016; Gidycz et al., 2007; McCauley et al., 2010; Messman-Moore et al., 2008; Mouilso et al., 2012; Testa & Livingston, 2000), but not vice versa (e.g., Gidycz et al., 2007; McCauley et al., 2010; Mouilso et al., 2012; Testa & Livingston, 2000), it is critical to replicate these findings.
One additional measurement difference that influences findings is the timing and duration of assessments. First, given the evidence that women have a higher risk of experiencing assault in their first year of college (Humphrey & White, 2000), and the associations between heavy drinking and assault appear to be strongest during this first semester of college (Testa & Hoffman, 2012), it is important to examine women as they transition into college specifically. Second, associations over shorter time periods, such as a day or week (e.g., Parks et al., 2008), differ from those over year-long assessment periods (e.g., Parks et al., 2014). As alcohol use is typically conceived of as a means of coping with post-assault psychological sequelae (e.g., self-medication hypothesis), this effect might not be immediately apparent. Given that depressive symptoms are most acute following a sexual assault (Atkeson, Calhoun, Resick, & Ellis, 1982), it is possible that the association between assault and alcohol use might only emerge over time, whereas shorter durations will capture acute intoxication effects of alcohol on assault risk.
1.2. Rationale for the present study
This study presents a rigorous evaluation of the hypothesis that alcohol use and sexual assault demonstrate bidirectional associations among college women over time. It addresses a number of limitations in existing investigations in order to accomplish this, including (1) clearly operationalizing sexual assault; (2) controlling for within-construct stability (e.g., prior alcohol use to subsequent alcohol use); and (3) modeling both outcomes simultaneously. We focus specifically on assault due to incapacitation (IA) because of its higher prevalence in college settings and its stronger association with alcohol use compared to forcible assault as women begin college (e.g., Griffin & Read, 2012). We aimed to advance existing research by modeling the associations between alcohol use and assault risk in the same model using cross-lagged models, which account for autoregressive associations within each construct over time. Further, we utilized semester-long assessments to explore the associations between these constructs over the first year of college, as the first year of college appears to be a particularly critical time for heavy alcohol use and IA (Testa & Hoffman, 2012).
Hypothesis 1. Alcohol use and IA will be stable over time (as indicated by significant autoregressive pathways).
Hypothesis 2. Alcohol use and IA will exhibit a bidirectional association such that (a) alcohol use indicative of intoxication [peak blood alcohol content (BAC), frequency of HED episodes] at baseline and end of first semester will predict IA in the subsequent semester, and (b) IA at baseline and during the first semester will predict heavier alcohol use (higher peak BAC, frequency of HED) in the following semester.
2. Materials and methods
2.1. Participants
Data for this study come from a longitudinal study of women's sexual behavior and sexual health over the first year in college (Fielder, Walsh, Carey, & Carey, 2013). All matriculating first-year women at a private university in the Northeast, excluding scholarship athletes, transfer students, and those under 18, were invited to participate. Scholarship athletes were excluded due to NCAA policies that prohibit them from being paid by the University while they are on athletic scholarships. Twenty-six percent of the incoming female students participated (N = 483). On average, participants were 18 years old (range: 18–25) and the majority identified as White (64%) and heterosexual (96%). Smaller proportions identified as Asian (11%), Black (10%), Hispanic (9%), and as “other” or multiple races (13%). At the initial assessment, 29% of participants were in a committed relationship. Based on demographic data from the university registrar, women who participated in the study were representative of the population of all first-year female students in terms of race and ethnicity.
2.2. Procedures
Matriculating first-year women were recruited to participate in the study via a mass mailing strategy in addition to on-campus flyers and the university Psychology Department's research pool. The mailings and flyers identified the study focus as women's health broadly and described it as an investigation of women's relationships and health behaviors over the first year of college. Potential participants were required to attend an in-person orientation once they arrived on campus. Women who consented in person then completed the baseline survey on personal computers. For the next year, they completed monthly online surveys, which were completed within the first week of each month and assessed the events of the previous month. Participants were compensated $20 at baseline and $10 for each monthly survey. The university's institutional review board approved all procedures.
2.3. Measures
2.3.1. Sexual assault
Sexual assault was assessed at three non-overlapping time points: baseline (since age 14), the end of the first semester, and the end of the second semester. We used the Sexual Experiences Survey-Revised (SES-R; Koss et al., 2007), adapted for use in college settings (Testa, Hoffman, Livingston, & Turrisi, 2010). The 20-item SES-R assesses four perpetrator tactics (i.e., verbal coercion, physical force, threats, incapacitation). For each tactic, participants reported how many times (i.e., 0, 1, 2, 3, 4+) they experienced five types of unwanted sexual contact (i.e., touching, oral sex, attempted vaginal intercourse, completed vaginal intercourse, anal penetration). The present analyses were restricted to unwanted oral sex, attempted or completed vaginal intercourse and anal penetration due to incapacitation, referred to here as IA. IA experiences were assessed with the following question stem: “When you were incapacitated (e.g., by drugs or alcohol) and unable to object or consent, has anyone ever…” Assault due to threats and/or use of force as well as verbal coercion (control variables) were also defined as unwanted oral sex, attempted or completed vaginal intercourse and anal penetration achieved by these tactics.
2.3.2. Alcohol use
Participants completed measures of alcohol use at baseline and monthly. We used two measures to assess different aspect of drinking: frequency of HED and peak BAC. Heavy episodic drinking was assessed using one question about frequency of heavy drinking in the last month [i.e., “On how many days (0-30) in the last month have you had 4 or more drinks on one occasion?”]. Peak BAC was estimated using participants' responses about the heaviest amount of alcohol consumed on one day and the amount of time over which it was consumed (Matthews & Miller, 1979). Whereas frequency of HED reflects a heavier drinking lifestyle, peak BAC reflects the presence of a high-risk event in terms of acute intoxication and potential impairment. HED has been more frequently studied in relation to sexual assault. In contrast to HED, which assesses the frequency of consuming ≥4 drinks, peak BAC provides different information because it accounts for an individual's body size as well as the time over which they consumed alcohol. BAC is a better measure of intoxication or drunkenness than HED because it takes the duration of drinking into account (Lange & Voas, 2001). Importantly, associations between lifetime attempted or completed assault and each form of alcohol use appears to differ (e.g., Testa et al., 2007), and thus we thought it important to use both measures.
2.4. Data management and analyses
A dichotomous IA variable was created from the baseline and the two end-of-semester surveys that assessed whether participants had experienced attempted or completed vaginal penetration, oral sex, or anal penetration due to incapacitation before college (since age 14) or since the last assessment (first semester IA, second semester IA). Participants had missing data if they did not complete a survey or if they did not complete the sexual assault questions. However, if a participant positively endorsed one or more of the IA outcomes, they were considered positive for IA at that time even if they did not answer all IA questions. The models controlled for the experience of attempted or completed assault due to threats or use of force and verbal coercion at each time point.
Autoregressive cross-lagged modeling was performed in Mplus version 6.0 (Muthén & Muthén, 1998–2010) to examine the associations between IA and alcohol use (Model 1: heavy episodic drinking frequency; Model 2: peak BAC). Prior to conducting the analyses, skewed variables (i.e., HED) were log transformed and peak BAC values were multiplied by 10. Equality constraints were imposed on factor loadings and model paths to increase parsimony when such constraints did not lead to a significant decrease in model fit. In addition to the factor loadings on both fall and spring HED and BAC, the following equality constraints were imposed: autoregressive pathways for IA and cross-lag pathways from alcohol use (HED, peak BAC) to IA.
3. Results
3.1. Missing data
Of the 483 women assessed at baseline, 440 (91%) completed the assessment at the end of the first semester, and 413 (86%) at the end of the second semester. Completers did not differ from first- and second-semester non-completers, respectively, in terms of age [t(481) = 0.58; t(481) = −0.35], peak BAC [t(478) = −0.50; t(478) = 0.34] or HED frequency at baseline [t(481) = −1.08; t(481) = 0.80], or likelihood of experiencing IA at baseline [χ2(483) = 1.31; χ2(483) = 3.48] or in the first semester [χ2(483) = 0.93].
3.2. Prevalence
Nearly one-fifth of women (19%) reported precollege IA, 9% reported IA in the first semester, and 6% reported IA in the second semester. On average, women reported peak BAC levels of 0.08 during the month before starting college, and peak BAC levels ranging from 0.08 to 0.11 over the year. One-half of women reported HED in the month prior to college; 70% of women reported at least one instance of HED in the first semester and 73% endorsed an instance of HED in the second semester.
3.3. Incapacitated assault and alcohol use
The model fit was good for the peak BAC model, χ2(67, N = 452) = 194.65, p < .05, CFI = 0.96, TLI = 0.95, RMSEA = 0.04, 95% CI [0.03, 0.05], and the HED model, χ2(67, N = 452) = 154.07, p < .05, CFI = 0.96, TLI = 0.95, RMSEA = 0.03, 95% CI [0.02, 0.04]. As hypothesized, autoregressive paths were significant, such that IA, peak BAC, and HED predicted future respective levels of these variables (Figs. 1, 2). After accounting for the stability within constructs, precollege IA prospectively predicted both HED (β = 0.17, p < .05) and peak BAC (β = 0.18, p < .05) during the first semester. No other cross-lagged paths were significant.
Fig. 1.
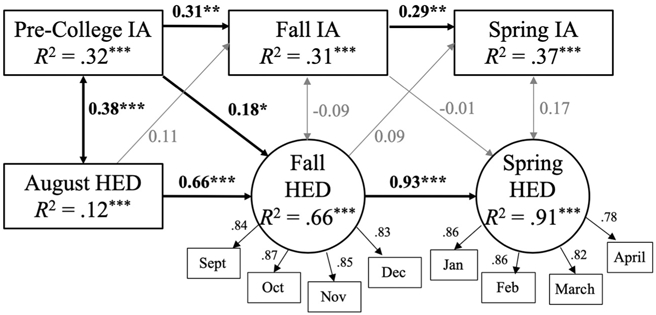
Cross lagged model of incapacitated assault (IA) and HED over women's first year in college. Models fitted using a WLSMV estimator in Mplus. Monthly HED measures are the log of the number of episodes reported. Standardized coefficients are presented. Control variables (not pictured) include White/non-White race, sorority membership, and other forms of sexual victimization.
Fig. 2.
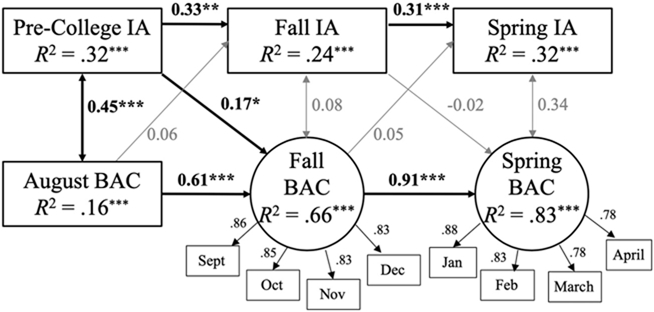
Cross lagged model of incapacitated assault (IA) and peak BAC over women's first year in college. Models fitted using a WLSMV estimator in Mplus. Standardized coefficients are presented. Monthly BAC measures are 10*BAC. Control variables (not pictured) include White/non-White race, sorority membership, and other forms of sexual victimization.
Regarding covariates, compared to non-White participants, White participants reported more precollege HED (β = 0.17, p < .001) and higher baseline peak BAC levels (β = 0.18, p < .001) and were more likely to report precollege IA (β = 0.22, p < .01). Compared to women who did not, women who joined sororities reported more precollege HED (β = 0.31, p < .001) and higher baseline peak BAC levels (β = 0.23, p < .001) but were not more likely to report precollege IA (β = 0.10, p = .19). Women with a precollege history of forcible assault reported lower levels of heavy alcohol use during the first semester (HED: β = −0.11, p < .01; peak BAC: β = −0.08, p < .05).
4. Discussion
In this longitudinal analysis, we used cross-lagged modeling to inform the hypothesis that heavy alcohol use and sexual assault evidence bidirectional associations. Consistent with our hypotheses, and existing research (e.g., Parks et al., 2014), women who were engaging in heavier alcohol use as they entered college continued to be heavier alcohol users across their first year, and women with a history of IA were more likely to experience subsequent IA.
This study represents the first attempt to simultaneously model these related outcomes, a unique possibility afforded by cross-lagged models. After accounting for the significant stability effects, IA was associated with subsequent alcohol use, such that women with a history of IA at baseline engaged in heavier drinking during the first semester. However, heavy alcohol use was not prospectively associated with subsequent IA risk. This pattern of findings highlights the importance of modeling the robust stability of heavy alcohol use over time and are most consistent with the findings of Parks et al. (2014) that examined attempted or completed assault using HLM. These studies present a coherent picture of alcohol as a concurrent, but not prospective, risk factor for IA.
Following a sexual assault, some college women engage in alcohol use for particular motives, such as to cope with negative emotions (Messman-Moore, Ward, Zerubavel, Chandley, & Barton, 2015), to enhance positive emotions (Kaysen et al., 2014), or in order to conform to social pressures to drink (i.e., conformity motives; Stappenbeck, Bedard-Gilligan, Lee, & Kaysen, 2013). Given that the transition to college is a time of social and personal change for many students, these motives for use might explain our observation that women with a history of precollege IA engage in heavier drinking as they transition into college. Because we did not measure drinking motives, we cannot address this hypothesis with data from the current study; thus, further research on specific motive-driven drinking and IA is needed.
Importantly, our findings show that the cross-lagged effect from IA to alcohol use was significant only as women transitioned into college over their first semester. Therefore, as women with a history of IA enter college, they transition into heavier drinking and reach greater levels of intoxication (peak BAC) relative to their non-victimized peers. These findings are concerning given that heavy drinking is strongly associated with assault risk in the same time period (e.g., Parks et al., 2008) and that heavy drinking is most strongly associated with women's assault risk during their first semester in college (Testa & Hoffman, 2012). Further, given that heavy drinking has widespread and long-lasting effects, our results suggest that women with a history of IA would likely benefit from receiving a targeted intervention regarding alcohol use and risk reduction at college entry (or earlier). These programs might draw upon existing work in this area (e.g., Gilmore, Lewis, & George, 2015).
Our finding that alcohol use did not prospectively predict increased assault risk corroborated the results of Parks et al. (2014) but differed from the results of other studies (e.g., Bryan et al., 2016; McCauley et al., 2010; Messman-Moore et al., 2009; Mouilso et al., 2012). There are several potential methodological explanations for discrepancies across studies, including the current study's (1) focus on women's transition to college, and (2) assessment of incapacitated assault.
First, this study focused on women's transition into and across their first year of college, which is a period associated with increased risk for incapacitated sexual assault (Carey et al., 2015) and increases in alcohol use (Sher & Rutledge, 2007). Further, there is a strong concurrent association between alcohol use and assault in the first semester of college (Testa & Hoffman, 2012). Therefore, these findings might differ from studies of college women in general (e.g., McCauley et al., 2010; Messman-Moore et al., 2009) or community women who binge drink (e.g., Bryan et al., 2016), as these women engage in different patterns of alcohol use and use alcohol in different settings. These different settings for alcohol use may differentially expose first-year women to perpetrators (e.g., Testa & Cleveland, 2017). Moreover, perhaps women's marked risk for assault during the first semester, and the robust autoregressive association in assault risk over the first year, account for so much of the variance in assault risk that alcohol use does not predict assault in the second semester. Finally, perhaps women engaging in high-risk drinking (i.e., samples limited to binge-drinking women [Bryan et al., 2016] or monthly binge drinkers [McCauley et al., 2010]) are more likely to incur increased assault risk over time in a way that women who drink less are not. As this study included first-year women regardless of their alcohol use, future research should continue to investigate these associations in samples of women who both are and are not heavy drinkers.
Second, this study focused only on women who experienced attempted or completed sexual assault due to incapacitation. Because alcohol is more likely to be involved in such assaults, this pattern of results might differ from other forms of assault. For example, other researchers who have found support for the alcohol-to-assault pathway among college women (Mouilso et al., 2012) and community women (Bryan et al., 2016) have defined sexual assault as any form of unwanted touching. Given the elevated prevalence of unwanted touching in bar and party settings (e.g., Graham, Bernards, Abbey, Dumas & Wells, 2017), it is possible that alcohol use prospectively predicts future unwanted touching, but not more severe forms of assault, via social exposure. Therefore, our findings may differ from some prior work that included unwanted touching because of how sexual assault is defined.
5. Limitations
We acknowledge several limitations of this study. First, the study design does not allow us to disentangle problematic alcohol use and IA at baseline. These behaviors predate enrollment in college, with 1 in 4 high school students reporting being drunk in the past month (Patrick & Schulenberg, 2014), and nearly 1 in 5 high school students reporting unwanted sexual activity in the past year (Williams et al., 2014). Thus, beginning the assessments at the start of college limits the prospective nature of our findings. This limitation also highlights the importance of prevention of sexual assault and alcohol misuse during the high school years. Second, the analyses focused only on assault since age 14. We did not assess CSA. Given that CSA is consistently associated with subsequent victimization as well as alcohol-related problems (Messman-Moore & Long, 2002), future research focused on IA should consider the role of CSA specifically.
Third, our operationalization of IA included both attempted and completed sexual assault due to incapacitation. Including both forms (a) acknowledges the serious potential impact of both types of assault, and (b) affords more statistical power (i.e., given the relatively low base rate of assault during a single semester). Given that the research literature is replete with differing operationalizations of assault, it is important for investigators to define terms clearly and carefully choose the definition that is most relevant to their research question.
Finally, to focus concretely on the impact of the experience of incapacitated assault, we controlled for sexual assault due to force, threats, or verbal coercion. However, the SES did not allow for the measurement of whether these tactics were used in the same or different assaults. Therefore, future work might also assess number of assault episodes by type.
6. Conclusions
The current findings have at least two practice implications. First, there is a need for interventions that will break the victimization-revictimization link for women with a history of IA at college entry. Because heavy episodic drinking is part of a cluster of risk behaviors (including engaging in hookups and selecting heavy drinking environments) that mediate the victimization-revictimization path (Testa, Hoffman, & Livingston, 2010), it is important to incorporate education about alcohol use, including training in protective behavioral strategies and drink refusal skills, into sexual assault prevention programming. Empowerment programs, bystander intervention training, and other sexual assault interventions are also needed. Second, compared to the proliferating field of prevention programs, there has been relatively little attention paid to the development of post-assault interventions. There is a need to support women post-assault and to address their use of alcohol, both to prevent revictimization and to facilitate recovery from assault (Campbell, Dworkin, & Cabral, 2009). These interventions might be particularly useful during points of transition, such as the beginning of college.
HIGHLIGHTS.
Sexual assault prior to college is a robust predictor of sexual assault during college.
Sexual assault prior to college is associated with increases in heavy drinking as women transition into college.
Heavy alcohol use was not associated with subsequent assault risk over time.
Acknowledgments
We gratefully acknowledge the study participants for their contributions. This work was supported by the National Institutes of Health [grant numbers R21-AA018257; K01-MH099956; 5P30-MH052776; T32-MH078788].
References
- Atkeson BM, Calhoun KS, Resick PA, & Ellis EM (1982). Victims of rape: Repeated assessment of depressive symptoms. Journal of Consulting and Clinical Psychology, 50, 96–102. 10.1037/0022-006X.50.1.96. [DOI] [PubMed] [Google Scholar]
- Borsari B, Murphy JG, & Barnett NP (2009). Predictors of alcohol use during the first year of college: Implications for prevention. Addictive Behaviors, 32, 2062–2086. 10.1016/j.addbeh.2007.01.017.Predictors. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryan AEB, Norris J, Abdallah DA, Stappenbeck CA, Morrison DM, Davis KC, … Zawacki T (2016). Longitudinal change in women's sexual victimization experiences as a function of alcohol consumption and sexual victimization history: A latent transition analysis. Psychology of Violence, 6, 271–279. 10.1037/a0039411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell R, Dworkin E, & Cabral G (2009). An ecological model of the impact of sexual assault on women's mental health. Trauma, Violence, & Abuse, 10, 225–246. 10.1177/1524838009334456. [DOI] [PubMed] [Google Scholar]
- Carey KB, Durney SE, Shepardson RL, & Carey MP (2015). Incapacitated and forcible rape of college women: Prevalence across the first year. The Journal of Adolescent Health, 56, 678–680. 10.1016/j.jadohealth.2015.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crosnoe R, Kendig S, & Benner A (2018). College-going and trajectories of drinking from adolescence into adulthood. Journal of Health and Social Behavior, 58, 252–269. 10.1177/0022146517693050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fielder RL, Walsh JL, Carey KB, & Carey MP (2013). Predictors of sexual hookups: A theory-based, prospective study of first-year college women. Archives of Sexual Behavior, 42, 1425–1441. 10.1007/s10508-013-0106-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gidycz CA, Loh C, Lobo T, Rich C, Lynn SJ, & Pashdog J (2007). Reciprocal relationships among alcohol use, risk perception, and sexual victimization: A prospective analysis. Journal of American College Health, 56, 5–14. 10.3200/JACH.56.1.5-14. [DOI] [PubMed] [Google Scholar]
- Gilmore AK, Lewis MA, & George WH (2015). A randomized controlled trial targeting alcohol use and sexual assault risk among college women at high risk for victimization. Behaviour Research and Therapy, 74, 38–49. 10.1016/j.brat.2015.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham K, Bernards S, Abbey A, Dumas TM, & Wells S (2017). When women do not want it: Young female bargoers’ experiences with and responses to sexual harassment in social drinking contexts. Violence Against Women, 23(12), 1419–1441. 10.1177/1077801216661037. [DOI] [PubMed] [Google Scholar]
- Grayson CE, & Nolen-Hoeksema S (2005). Motives to drink as mediators between childhood sexual assault and alcohol problems in adult women. Journal of Traumatic Stress, 18, 137–145. 10.1002/jts.20021. [DOI] [PubMed] [Google Scholar]
- Griffin MJ, & Read JP (2012). Prospective effects of method of coercion in sexual victimization across the first college year. Journal of Interpersonal Violence, 27, 2503–2524. 10.1177/0886260511433518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Humphrey JA, & White JW (2000). Women's vulnerability to sexual assault from adolescence to young adulthood. The Journal of Adolescent Health, 27, 419–424. 10.1016/S1054-139X(00)00168-3. [DOI] [PubMed] [Google Scholar]
- Kaysen DL, Atkins DC, Simpson TL, Stappenbeck CA, Blayney JA, Lee CM, & Larimer ME (2014). Proximal relationships between PTSD symptoms and drinking among female college students: Results from a daily monitoring study. Psychology of Addictive Behaviors, 28, 62–73. 10.1037/a0033588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaysen DL, Neighbors C, Martell J, Fossos N, & Larimer ME (2006). Incapacitated rape and alcohol use: A prospective analysis. Addictive Behaviors, 31, 1820–1832. 10.1016/j.addbeh.2005.12.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koss MP, Abbey A, Campbell R, Cook S, Norris J, Testa C, … White J (2007). Revising the SES: A collaborative process to improve assessment of sexual aggression and victimization. Psychology of Women Quarterly, 31, 357–370. 10.1111/j.1471-6402.2007.00385.x. [DOI] [Google Scholar]
- Krebs CP, Lindquist CH, Warner TD, Fisher BS, & Martin SL (2009). College women's experiences with physically forced, alcohol- or other drug-enabled, and drug-facilitated sexual assault before and since entering college. Journal of American College Health, 57, 639–647. 10.3200/JACH.57.6.639-649. [DOI] [PubMed] [Google Scholar]
- Lange JE, & Voas RB (2001). Defining binge drinking quantities through resulting blood alcohol concentrations. Psychology of Addictive Behaviors, 15, 310–316. [DOI] [PubMed] [Google Scholar]
- Langeland W, & Hartgers C (1998). Child sexual and physical abuse and alcoholism: A review. Journal of Studies on Alcohol, 59, 336–348. [DOI] [PubMed] [Google Scholar]
- Matthews DB, & Miller WR (1979). Estimating blood alcohol concentration: Two computer programs and their applications in therapy and research. Addictive Behaviors, 4, 55–60. [DOI] [PubMed] [Google Scholar]
- McCauley JL, Calhoun KS, & Gidycz CA (2010). Binge drinking and rape: A prospective examination of college women with a history of previous sexual victimization. Journal of Interpersonal Violence, 25, 1655–1668. 10.1177/0886260509354580. [DOI] [PubMed] [Google Scholar]
- Messman-Moore T, & Long PJ (2002). Alcohol and substance use disorders as predictors of child to adult sexual revicitmization in a sample of community women. Violence and Victims, 17, 319–340. 10.1891/vivi.17.3.319.33662. [DOI] [PubMed] [Google Scholar]
- Messman-Moore T, Ward RM, & Brown AL (2009). Substance use and PTSD symptoms impact the likelihood of rape and revictimization in college women. Journal of Interpersonal Violence, 24, 499–521. 10.1177/0886260508317199. [DOI] [PubMed] [Google Scholar]
- Messman-Moore T, Ward RM, Zerubavel N, Chandley RB, & Barton SN (2015). Emotion dysregulation and drinking to cope as predictors and consequences of alcohol-involved sexual assault: Examination of short-term and long-term risk. Journal of Interpersonal Violence, 30, 601–621. 10.1177/0886260514535259. [DOI] [PubMed] [Google Scholar]
- Messman-Moore TL, Coates AA, Gaffey KJ, & Johnson CF (2008). Sexuality, substance use, and susceptibility to victimization: Risk for rape and sexual coercion in a prospective study of college women. Journal of Interpersonal Violence, 23, 1730–1746. 10.1177/0886260508314336. [DOI] [PubMed] [Google Scholar]
- Moncrieff J, & Farmer R (1998). Sexual abuse and the subsequent development of alcohol problems. Alcohol and Alcoholism, 33, 592–601. [DOI] [PubMed] [Google Scholar]
- Mouilso ER, Fischer S, & Calhoun KS (2012). A prospective study of sexual assault and alcohol use among first-year college women. Violence and Victims, 27, 78–94. 10.1891/0886-6708.27-1.78. [DOI] [PubMed] [Google Scholar]
- Muehlenhard CL, Peterson ZD, Humphreys TP, & Jozkowski KN (2017). Evaluating the one-in-five statistic: Women's risk of sexual assault while in college. Journal of Sex Research, 54, 549–576. 10.1080/00224499.2017.1295014. [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (1998–2010). Mplus User's Guide (6th ed). California: Muthén & Muthén. [Google Scholar]
- Paras ML, Mohammad HM, Chen LP, Goranson EN, Sattler AL, Colbenson KM, … Zirakzadeh A (2009). Sexual abuse and lifetime diagnosis of somatic disorders: A systematic review and meta-analysis. JAMA, 302, 551–561. 10.1001/jama.2009.1091. [DOI] [PubMed] [Google Scholar]
- Parks KA, Hsieh YP, Bradizza CM, & Romosz AM (2008). Factors influencing the temporal relationship between alcohol consumption and experiences with aggression among college women. Psychology of Addictive Behaviors, 22, 210–218. 10.1037/0893-164X.22.2.210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parks KA, Hsieh YP, Taggart C, & Bradizza CM (2014). A longitudinal analysis of drinking and victimization in college women: Is there a reciprocal relationship? Psychology of Addictive Behaviors, 28, 943–951. 10.1037/a0036283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patrick ME, & Schulenberg JE (2014). Prevalence and predictors of adolescent alcohol use and binge drinking in the United States. Alcohol Research: Current Reviews, 35, 193–200. [PMC free article] [PubMed] [Google Scholar]
- Sher KJ, & Rutledge PC (2007). Heavy drinking across the transition to college: Predicting first-semester heavy drinking from precollege variables. Addictive Behaviors, 32, 819–835. 10.1016/j.addbeh.2006.06.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stappenbeck CA, Bedard-Gilligan M, Lee CM, & Kaysen D (2013). Drinking motives for self and others predict alcohol use and consequences among college women: The moderating effects of PTSD. Addictive Behaviors, 38, 1831–1839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stoner SA, Norris J, George WH, Davis KC, Masters NT, & Hessler DM (2007). Effects of alcohol intoxication and victimization history on women's sexual assault resistance intentions of secondary cognitive appraisals. Psychology of Women Quarterly, 31, 344–356. [Google Scholar]
- Testa M, & Cleveland MJ (2017). Does alcohol contribute to college men’s sexual assault perpetration? Between-and within-person effects over five semesters. Journal of Studies on Alcohol and Drugs, 78(1), 5–13. 10.15288/jsad.2017.78.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, & Hoffman JH (2012). Naturally occurring changes in women's drinking from high school to college and implications for sexual victimization. Journal of Studies on Alcohol and Drugs, 73, 26–33. 10.15288/jsad.2012.73.26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, Hoffman JH, & Livingston JA (2010). Alcohol and sexual risk behaviors as mediators of the sexual victimization-revictimization relationship. Journal of Consulting and Clinical Psychology, 78, 249–259. 10.1037/a0018914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, Hoffman JH, Livingston JA, & Turrisi R (2010). Preventing college women's sexual victimization through parent based intervention: A randomized controlled trial. Prevention Science, 11, 308–318. 10.1007/s11121-010-0168-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, & Livingston JA (2000). Alcohol and sexual aggression: Reciprocal relationships over time in a sample of high-risk women. Journal of Interpersonal Violence, 15, 413–427. 10.1177/088626000015004005. [DOI] [Google Scholar]
- Testa M, Livingston JA, & Hoffman JH (2007). Does sexual victimization predict subsequent alcohol consumption? A prospective study among a community sample of women. Addictive Behaviors, 32, 2926–2939. 10.1016/j.addbeh.2007.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, Vanzile-Tamsen C, Livingston JA, & Buddie AM (2006). The role of women's alcohol consumption in managing sexual intimacy and sexual safety motives. Journal of Studies on Alcohol, 67, 665–674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson EH, & Cracco EJ (2008). Sexual aggression in bars: What college men can normalize. The Journal of Men’s Studies, 16, 82–96. 10.3149/jms.1601.82. [DOI] [Google Scholar]
- Ullman SE (2003). A critical review of field studies on the link of alcohol and adult sexual assault in women. Aggression and Violent Behavior, 8, 471–486. 10.1016/S1359-1789(03)00032-6. [DOI] [Google Scholar]
- Williams CM, Cook-Craig PG, Bush HM, Clear ER, Lewis AM, Garcia LS, … Fisher BS (2014). Victimization and perpetration of unwanted sexual activities among high school students: Frequency and correlates. Violence Against Women, 20, 1239–1257. 10.1177/1077801214551575. [DOI] [PubMed] [Google Scholar]