

Abstract
Purpose:
The aim of this study was to analyze rates of perioperative complications and subsequent cervical surgeries in patients treated for cervical degenerative disc disease with anterior cervical discectomy and fusion (ACDF) and those treated with artificial cervical disc arthroplasty (ACDA) for up to 5-year follow-up.
Methods:
California’s Office of Statewide Health Planning and Development discharge database was analyzed for patients aged 18 to 65 years undergoing single-level ACDF or ACDA between 2003 and 2010. Medical comorbidities were identified with CMS-Condition Categories. Readmissions for short-term complications of the procedure were identified and rates of subsequent cervical surgeries were calculated at 90-day and 1-, 3-, and 5-year follow-up. Multivariate regression modeling was used to identify associations with complications and subsequent cervical surgeries correcting for patient and provider characteristics.
Results:
A total of 52,395 eligible cases were identified; 50,926 ACDF and 1,469 ACDA. Readmission was less common in the ACDA group (OR: 0.69, 95% CI:.48 – 1.0, p=0.048). Subsequent cervical spine surgery was more common in the ACDF group in the immediate perioperative period (within 90 days of surgery) (ACDF 3.35% vs. ACDA 2.04%, OR: 0.63, 95% CI: 0.44–0.92, p=0.015). At 1-year, 3-years, and 5-years postoperatively, rates of subsequent cervical surgeries were similar between the two cohorts.
Conclusions:
We found no protective benefit for ACDA versus ACDF for single-level disease at up to 5-year follow-up in the largest cohort of patients examined to date. Early complications were rare in both cohorts stressing the value of large cohort studies to study risk factors for rare events.
Keywords: artificial disc, cervical degenerative disc disease, reoperations, spinal fusion, total disc arthroplasty
Graphical Abstract
Introduction
Anterior cervical discectomy and fusion (ACDF) has been considered the gold-standard treatment for single-level cervical degenerative disc disease causing radiculopathy or myelopathy.[1] This procedure is associated with high union rates and patient success; however, nonunion is a common cause of reoperation after ACDF surgeries.[2] Modern ACDF techniques often involve anterior cervical instrumentation, which has been associated with post-operative dysphagia and adjacent level ossification development (ALOD).[3,4] The most vexing complication associated with cervical fusions is adjacent segment pathology (ASP) leading to reoperation.[5,6] After ACDF, adjacent segment stresses are altered and may encourage degeneration of the adjacent segments.[7] Symptomatic degeneration is a common cause for reoperation and has been studied extensively. Hilibrand reported a symptomatic adjacent segment degeneration rate of 2.9% per year after anterior cervical fusion, a rate recently supported by an analysis of a cohort of patients treated for degenerative cervical diseases with a number of different surgeries and approaches.[6,5] An implication from this consistent rate is that ASP may be part of the natural history of a degenerating cervical spine, rather than the result of ACDF and altered biomechanics.
Artificial cervical total disc arthroplasty (ACDA) is a motion-sparing procedure proposed as an alternative to ACDF.[8] These low profile devices have been associated with less dysphagia and eliminate the need for reoperation due to nonunion.[9] In addition to obviating the need for union, motion-sparing devices may limit the alteration of stresses at adjacent segments and decrease rates of reoperation due to ASP.[7,10–12] Investigational device exemption (IDE) trials have reported lower rates of reoperation following ACDA versus ACDF.[10,13] However, these results have not been consistent with non-IDE studies raising concern regarding the external validity of IDE results.[14,15] Industry-sponsored research is subject to biases, including confirmation bias, funding bias and other financial conflicts, which may be causes for lower reoperation following ACDA.[16] These concerns are supported by a recent report, offering similar rates of reoperation for patients undergoing surgeries for cervical degenerative disease regardless of anterior technique used.[6]
The purpose of this paper was to report rates of short-term perioperative complication and longer-term rates of subsequent cervical surgeries in a large administrative database of patients treated for single-level cervical degenerative disc disease with ACDF and ACDA at up to five years of follow-up. We hypothesized that perioperative complications would be higher in the ACDA group, given the learning curve associated with the introduction of a new technology. Conversely, we hypothesized that rates of reoperation would be higher in those patients treated with ACDF versus ACDA, consistent with the previously published IDE trials.
Materials and Methods
Data Source
Data were obtained from California’s Office of Statewide Health Planning and Development (OSHPD) database, which contains codes for up to 24 diagnoses and 20 inpatient procedures per hospitalization from all licensed nonfederal hospitals in California. The OSHPD database includes patient and hospital characteristics including age, gender, race/ethnicity, insurance type, comorbidities, and hospital volume. Patients are assigned unique identifiers to allow for longitudinal tracking. These data were linked to the California State Death Statistical Master File (DSMF) for tracking of patient mortality.
Inclusion and Exclusion Criteria
The OSHPD database was queried for patients aged 18 to 65 years from 01/01/2003 to 12/31/2010. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure and diagnosis codes were used to identify patients undergoing the procedures of interest (ACDF: 81.02; ACDA: 84.62) and to eliminate patients meeting the exclusion criteria. Exclusion criteria included patients with infections, neoplasms, pathologic fractures or those undergoing revision procedures as their first procedure within the study period (Figure 1). Medical comorbidities were identified with CMS-Condition Categories. Readmissions for medical and procedure-specific complications within 90 days of the index procedure were identified by ICD-9-CM codes.
Figure 1.

Patient selection flow chart
Rates of Subsequent Cervical Surgery
Patients were identified as having subsequent cervical surgeries using diagnosis and procedure codes following the index procedure, as previously described.[17] Death within 30 days from the admission date of index hospitalization was identified using the DSMF. Multivariate logistic regression assessed the relationship between procedure and complication while controlling for known comorbidities and provider volume. Rates of subsequent cervical surgery are reported at time periods of 1, 3, and 5 years following each index procedure for additional cervical surgery procedure codes. Incidence densities (calculated as events/100 person*years) were calculated for ACDF and ACDA at each postoperative time point.
Time-to-Event Analysis: Associations with Subsequent Cervical Surgery
Time-to-event analysis assessed the protective effect of ACDA relative to ACDF against subsequent cervical surgeries. Patients were assigned into one of three categories following the index procedure – a) having a subsequent cervical operation, b) death, or c) neither by the end date of the study (12/31/2010). The covariates analyzed included both patient and hospital characteristics such as age, gender, race/ethnicity, comorbidities, insurance type, and hospital volume. Time-to-event analysis was performed examining each of these covariates for potential associations with subsequent cervical surgery.
Statistical Analysis
T-tests and Chi-squared tests were used to evaluate differences in patient demographics for continuous and categorical variables respectively. Comparisons of rates of comorbidities, complications, deaths, and subsequent cervical surgery were performed using Fisher’s exact test. Logistic regression was used to determine the effects of independent variables on the risk of readmission for short-term complications. Time-to-event analysis was conducted using a Cox proportional hazards model with the longer-term outcome of subsequent cervical surgery as the dependent variable. All analyses were performed using STATA 13 (StataCorp LP, College Station, TX).
Funding
This study was funded by a grant from the Cervical Spine Research Society.
Results
52,395 Eligible cases were identified with 50,926 ACDF and 1,469 ACDA. Demographic details are found in Table 1. Patients undergoing ACDF were slightly older (ACDF: 53.0 ±7.8, ACDA: 50.2±8.0, p<0.0001) and the distribution of insurance payers varied between groups (Workers Compensation: ACDF 17.0%, ACDA 26.7%, p<0.0001). Gender and race distributions were similar. Diabetes was more common in the ACDF group (ACDF 9.4%, ACDA 5.7%, p <0.0001). The mean total comorbidities, as defined by the Center for Medicare and Medicaid Services, was higher for ACDF versus ACDA (ACDF 0.8, ACDA 0.5, p<0.0001).
Table 1.
Demographic Data.
| ACDF N=50,926 |
ACDA N=1,469 |
p-value | |
|---|---|---|---|
| Age | 53.0 (±7.8, 24–65) | 50.2 (±8.0, 21–65) | <0.0001 |
| Gender | |||
| Male | 24,759 (48.6%) | 693 (47.2%) | 0.28 |
| Female | 26,167 (51.4%) | 776 (52.8%) | |
| Race | |||
| Caucasian | 41,017 (80.5%) | 1,204 (82.0%) | 0.13 |
| African American | 3,353 (6.6% | 74 (5.0%) | |
| Asian | 2,217 (4.4%) | 59 (4.0%) | |
| Native American | 186 (0.4%) | 8 (0.6%) | |
| Other | 4,153 (8.2%) | 124 (8.4%) | |
| Payer | |||
| Private | 32,088 (63.0%) | 824 (56.1%) | <0.0001 |
| Medicare | 3,760 (7.4%) | 87 (5.9%) | |
| MediCal | 3,546 (7.0%) | 54 (3.7%) | |
| Worker’s Compensation | 8,679 (17.0%) | 392 (26.7%) | |
| Other | 2,853 (5.6%) | 112 (7.6%) |
Short-term perioperative complication rates and multivariate regression analysis results are reported in Table 2. For complications with few events, regression did not return meaningful results. Cox regression results are shown in Table 3 for the longer-term outcome of subsequent cervical surgeries and complications. This was the main outcome of interest given that this was hypothesized to be possibly attributable to the choice of index surgery, fusion or arthroplasty.
Table 2.
Short-term perioperative complication rates and multivariate regression results for ACDA/ACDF association.
| Complication | ACDF N = 50,926 |
ACDA N = 1,469 |
Odds Ratio | p-value |
|---|---|---|---|---|
| Readmission | 1991 (3.91%) | 31 (2.11%) | 0.69 (0.48 – 1.0) | 0.048 |
| Death | 93 (0.18%) | 0 (0%) | NA | 0.185 |
| Acute Myocardial Infarction | 7 (0.01%) | 1 (0.07%) | NA | NA |
| Pneumonia | 77 (0.15%) | 3 (0.2%) | NA | NA |
| Pulmonary Embolism | 55 (0.11%) | 1 (0.07%) | NA | NA |
| Device Related Mechanical Complication | 205 (0.4%) | 9 (0.61%) | 1.94 (0.99 – 3.82) | 0.054 |
| Wound Infection | 140 (0.27%) | 2 (0.14%) | 0.69 (0.17 – 2.79) | 0.597 |
| Esophageal Injury | 2 (0%) | 1 (0.07%) | NA | NA |
| Vertebral Artery Injury | 24 (0.05%) | 4 (0.27%) | 7.76 (2.56 – 23.52) | 0.0003 |
| Dural Tear | 4 (0.01%) | 1 (0.07%) | NA | NA |
| Subsequent Cervical Surgery (within 90 days) | 1707 (3.35%) | 30 (2.04%) | 0.63 (0.44 – 0.92) | 0.015 |
Table 3.
Cox proportional hazard model results for longer-term rates of subsequent cervical surgery .
| Hazard Ratio (95% Confidence Interval) | p-value | |
|---|---|---|
| Index Procedure | ||
| ACDF | Reference | |
| ACDA | 0.86 (0.60 – 1.23) | 0.402 |
| Age | 1.01 (1.00 – 1.02)* | 0.016 |
| Payer | ||
| Private Insurance | Reference | |
| Medicare | 1.19 (0.99 – 1.42) | 0.064 |
| MediCal | 0.94 (0.76 – 1.15) | 0.526 |
| Worker’s Compensation | 0.78 (0.68 – 0.89)* | 0.0004 |
| Gender | ||
| Male | Reference | |
| Female | 0.68 (0.67 – 0.75)* | <0.0001 |
| Race | ||
| Caucasian | Reference | |
| African American | 1.27 (1.06 – 1.52)* | 0.011 |
| Asian | 0.97 (0.76 – 1.23) | 0.800 |
| Native American | 1.24 (0.59 – 2.61) | 0.569 |
| Other | 0.96 (0.77 – 1.20) | 0.718 |
p<0.05
Short-term readmission was more common in the ACDF group and a protective association of ACDA was found (OR: 0.69, 95% CI:.48 – 1.0, p=0.048). This result should be interpreted with caution, as the 95% confidence interval includes, but does not cross, 1.0. Vertebral artery injuries were rare but more common in the ACDA group (ACDF: 24 (0.05%), ACDA: 4 (0.27%); p=0.0003). Device-related mechanical complications were more common in the ACDA group, though no relationship was found when controlling for comorbid conditions. Similarly, wound infections were more common in the ACDF group, though no relationship between the index surgery choice and infection was found in multivariate modeling correcting for patient comorbidities. Short-term subsequent cervical spine procedures were less common in the ACDA group at 2.04% compared to the ACDF group 3.35% (OR: 0.63, 95% CI: 0.44–0.92, p=0.015).
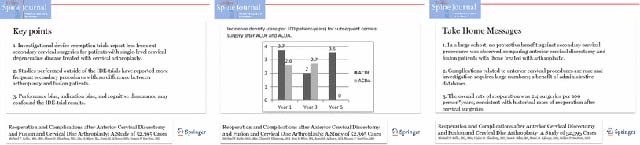
The longer-term outcome of subsequent cervical surgery was not different comparing ACDA to ACDF (HR: 0.86, 95% CI: 0.60–1.23, p=0.402) Reoperation was more likely in older patients (Age HR: 1.01, 95% CI: 1.00–1.02, p=0.016) and in African American patients (HR: 1.27, 95% CI: 1.06–1.52, p=0.011). Worker’s compensation patients were less likely to undergo subsequent surgery (HR: 0.78, 95% CI: 0.68–0.89, p=0.0004) (Table 3). At 1-year, 3-years, and 5-years postoperatively, rates of subsequent cervical surgeries were similar between the two cohorts. Rates appear similar, though comparison at 5-years is not possible due to the small number of patients in the ACDA group available for follow-up at this point. The incidence densities per 100 person years are found in Figure 2. The overall rate of subsequent surgeries, combining both ACDF and ACDA, was 2.7 patients per 100 patient-years. Hospital volume was not associated with complication or reoperation.
Figure 2.

Incidence density (case per 100 patient-years) for subsequent cervical surgery after ACDF and ACDA.
Discussion
ACDA was introduced in 2003 as a motion-sparing technology aimed at decreasing reoperation due to nonunion and adjacent segment pathology. IDE studies have suggested that ACDA may be effective in achieving this goal, with fewer subsequent surgeries performed in patients treated with ACDA versus ACDF.[10,18,19,11] However, these results have not been consistent across the literature, which raises concern for bias arising from the industry-sponsored investigations and the generalizability of the results from these studies.[6,20,14] Furthermore, the introduction of new technologies is necessarily associated with a learning curve and, as such, perioperative complications may be more common as the technology is adopted. The purpose of this study was to investigate short-term perioperative complication rates and longer-term rates of subsequent cervical surgeries following ACDA and ACDF in a large, administrative database.
We found that perioperative complications were uncommon and similar between both groups (Table 2). This is likely because of the many similarities between ACDF and ACDA, in terms of approach, decompression, and interbody device placement. Vertebral artery injury was more common in the ACDA group; though it must be emphasized that the overall rate of vertebral artery injury was low. At 5-years follow-up, reoperation rates were similar between groups, with incidence densities approaching previously published rates of reoperation and symptomatic adjacent degeneration.[5,6] No protective effect for ACDA against subsequent cervical spine surgeries was observed at up to 5 years follow-up, while Worker’s Compensation (HR: 0.78) and female (HR: 0.68) patients were less likely and African Americans (HR: 1.27) were more likely to undergo future surgeries.
Several IDE studies, performed as randomized, controlled trials, have examined complications and reoperation after ACDF and ACDA. As ACDA was approved in 2007 in the U.S., mid-term follow-up of study participants are now available. Five-year results from one IDE trial reported a reoperation rate of 2.9% in the ACDA group versus 11.3% for the ACDF in the management of single-level disease.[12] These results were consistent with the early, 2-year follow-up data. In this cohort, the rates of subsequent surgery at the adjacent levels were similar between groups, while reoperation at the level of the index procedure was more common in the ACDF group due to pseudarthrosis. An IDE investigating 2-level ACDF versus 2-level ACDA reported 15.2% of ACDF patients required at least one subsequent surgery, as opposed to 4.0% of ACDA patients.[21] While implant designs vary, the concept of motion preservation and fusion avoidance is consistent. In contrast to the prior IDE studies, Phillips et al reported similar reoperation rates (ACDF 5.4%, ACDA 5.2%) at two-year follow-up with a different implant design.[22]
Selection bias and cognitive dissonance are limitations of IDE trial results. Singh et al noted that, in an effort to increase enrollment, patients that should have been treated with two-level surgeries may have been enrolled in the one-level trials.[14] Also, they questioned whether the thresholds for reoperation were the same in the ACDF and ACDA arms of trials. A review of patients treated with one-level ACDF surgeries found an early (i.e., within two years) reoperation rate of 2.1% and a 3.5 year reoperation rate of 7.6%, which compares more favorably with rates reported for ACDA in the IDE trials. Generalizability of IDE reoperation rates is questioned again by Gornet et al.[15] This single-surgeon review of 189 ACDA patients reported a reoperation rate of 9.0% at a minimum of one-year follow-up. This rate is certainly higher than IDE rates and it may be a rate less affected by the biases associated with participation in an IDE. Finally, Lee et al found an annual reoperation rate of 2.1% for patients undergoing cervical spine surgery, with no apparent protective effect attributed to ACDA.[6] This rate compares favorably with the frequently cited work of Hilibrand et al, who found an annual rate of adjacent segment pathologies of 2.9%.[5]
A number of recent systematic reviews and meta-analyses of published data have pooled results in an effort to clarify any differences between ACDF and ACDA.[23,24,11,25,26] Those that have included only data from prospective, randomized trials have found lower rates of adjacent segment disease, as defined by symptomatic adjacent degeneration, and lower rates of subsequent cervical procedures with ACDA. These meta-analyses are limited by the biases associated with the publications they include, which include various methods of defining adjacent segment degeneration and disease, publication bias, and unclear indications for reoperation versus continued nonoperative care of symptomatic adjacent segment degeneration. Furthermore, the majority of randomized trials are industry sponsored.[18] Our results in a cohort of patients may be more generalizable than IDE data and found no protective effect for ACDA on reoperation rates. Our findings are more consistent with the systematic review and meta-analysis by Shriver et al, who found a 2.6% rate of adjacent segment disease in ACDA trials followed longer than 24 months.[26] Not surprisingly, the rate climbed with longer follow-up. The rate of adjacent segment degeneration reported in their cohort was 16.6%, which may suggest that conclusions regarding the protective benefit of ACDA require longer than mid-term follow-up.
Administrative database studies have significant limitations, as large numbers are studied at the expense of data granularity. We have used a previously published algorithm to identify patients undergoing ACDF and ACDA for cervical degenerative disease, though miscoding may have caused inclusion of inappropriate patients and exclusion of appropriate patients. Similarly, undercoding of complications is likely common, particularly dysphagia. Dysphagia is common in the early postoperative period after anterior cervical surgery and we likely underestimate the true rate of dysphagia and overestimate the risk associated with ACDF. Medical tourism could have been common with early ACDA, prior to widespread adoption, and these ACDA patients may have been lost to follow-up, thus underestimating the rate of reoperation in this cohort. Similarly, while all inpatient hospitalizations within California should be recorded, it is possible that patients in both cohorts were lost to followup via miscoding or may have moved from the state. The intent is to study all patients over a minimum of five years, though we may underestimate reoperations in both cohorts due to these potential sources of loss to followup. In the absence of clinical records, we do not know if revision surgeries were indicated, but not performed, thus overestimating the success of either procedure. Some patients may have had exclusion criteria for ACDA, such as facet arthrosis or significant disc height loss, and been treated with ACDF. Such a spondylotic neck may be more likely to undergo adjacent degeneration, thus biasing our analysis away from the null. While other methods of statistical analysis are available, such as propensity matching, logistic regression is an appropriate method in series such as these, with a large number of events and a small number of significant confounding variables. Despite these limitations, our calculated incidence density of reoperation is similar to Lee et al and is similar to the rate of symptomatic adjacent disease proposed by Hilibrand, lending external validity to our findings.[5,6]
Conclusion
In conclusion, we have found no protective benefit to ACDA relative to ACDF for single-level disease in the largest cohort of patients examined to date using a time-to-event regression model. The rate of subsequent cervical spine surgery after ACDF and ACDA was 2.4 per 100 patient years, similar to previous rates of adjacent segment degeneration and reoperation.[5,6] Early complications were rare in both cohorts stressing the value of large cohort studies to study risk factors for rare events.
Supplementary Material
Conflicts of Interest and Source of Funding
Michael P. Kelly has received support from the Washington University Institute of Clinical and Translational Sciences grant UL1TR000448 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH) and has received grants from AO North America (AONA) Spine, Orthopaedic Research and Education Foundation (OREF), Cervical Spine Research Society (CSRS), Barnes Jewish Foundation, and Fox Family Foundation. Nelson F. SooHoo has previously been supported by CSRS. For the remaining authors, no conflicts of interest or sources of funding were declared. The devices that are the subject of this manuscript are FDA-approved for this indication. The Committee for the Protection of Human Subjects (CPHS) has reviewed and approved this project (Project Number: 12-08-0514). This approval is issued under the California Health and Human Services Agency’s Federalwide Assurance #00000681. This study received direct support from the CSRS.
References
- 1.Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC (2007) Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. The Journal of bone and joint surgery American volume 89 (6):1360–1378 [DOI] [PubMed] [Google Scholar]
- 2.Shriver MF, Lewis DJ, Kshettry VR, Rosenbaum BP, Benzel EC, Mroz TE (2015) Pseudoarthrosis rates in anterior cervical discectomy and fusion: a meta-analysis. The spine journal : official journal of the North American Spine Society 15 (9):2016–2027. doi: 10.1016/j.spinee.2015.05.010 [DOI] [PubMed] [Google Scholar]
- 3.Garrido BJ, Wilhite J, Nakano M, Crawford C, Baldus C, Riew KD, Sasso RC (2011) Adjacent-level cervical ossification after Bryan cervical disc arthroplasty compared with anterior cervical discectomy and fusion. The Journal of bone and joint surgery American volume 93 (13):1185–1189. doi: 10.2106/JBJS.J.00029 [DOI] [PubMed] [Google Scholar]
- 4.Rosenthal BD, Nair R, Hsu WK, Patel AA, Savage JW (2016) Dysphagia and Dysphonia Assessment Tools After Anterior Cervical Spine Surgery. Clinical spine surgery. doi: 10.1097/BSD.0000000000000373 [DOI] [PubMed] [Google Scholar]
- 5.Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH (1999) Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. The Journal of bone and joint surgery American volume 81 (4):519–528 [DOI] [PubMed] [Google Scholar]
- 6.Lee JC, Lee SH, Peters C, Riew KD (2014) Risk-factor analysis of adjacent-segment pathology requiring surgery following anterior, posterior, fusion, and nonfusion cervical spine operations: survivorship analysis of 1358 patients. The Journal of bone and joint surgery American volume 96 (21):1761–1767. doi: 10.2106/JBJS.M.01482 [DOI] [PubMed] [Google Scholar]
- 7.Anderson PA, Sasso RC, Hipp J, Norvell DC, Raich A, Hashimoto R (2012) Kinematics of the cervical adjacent segments after disc arthroplasty compared with anterior discectomy and fusion: a systematic review and meta-analysis. Spine 37 (22 Suppl):S85–95. doi: 10.1097/BRS.0b013e31826d6628 [DOI] [PubMed] [Google Scholar]
- 8.Kelly MP, Mok JM, Frisch RF, Tay BK (2011) Adjacent segment motion after anterior cervical discectomy and fusion versus Prodisc-c cervical total disk arthroplasty: analysis from a randomized, controlled trial. Spine 36 (15):1171–1179. doi: 10.1097/BRS.0b013e3181ec5c7d [DOI] [PubMed] [Google Scholar]
- 9.Skeppholm M, Olerud C (2013) Comparison of dysphagia between cervical artificial disc replacement and fusion: data from a randomized controlled study with two years of follow-up. Spine 38 (24):E1507–1510. doi: 10.1097/BRS.0b013e3182a516ef [DOI] [PubMed] [Google Scholar]
- 10.Delamarter RB, Zigler J (2013) Five-year reoperation rates, cervical total disc replacement versus fusion, results of a prospective randomized clinical trial. Spine 38 (9):711–717. doi: 10.1097/BRS.0b013e3182797592 [DOI] [PubMed] [Google Scholar]
- 11.Zhong ZM, Zhu SY, Zhuang JS, Wu Q, Chen JT (2016) Reoperation After Cervical Disc Arthroplasty Versus Anterior Cervical Discectomy and Fusion: A Meta-analysis. Clinical orthopaedics and related research. doi: 10.1007/s11999-016-4707-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zigler JE, Delamarter R, Murrey D, Spivak J, Janssen M (2013) ProDisc-C and anterior cervical discectomy and fusion as surgical treatment for single-level cervical symptomatic degenerative disc disease: five-year results of a Food and Drug Administration study. Spine 38 (3):203–209. doi: 10.1097/BRS.0b013e318278eb38 [DOI] [PubMed] [Google Scholar]
- 13.Janssen ME, Zigler JE, Spivak JM, Delamarter RB, Darden BV 2nd, Kopjar B (2015) ProDisc-C Total Disc Replacement Versus Anterior Cervical Discectomy and Fusion for Single-Level Symptomatic Cervical Disc Disease: Seven-Year Follow-up of the Prospective Randomized U.S. Food and Drug Administration Investigational Device Exemption Study. The Journal of bone and joint surgery American volume 97 (21):1738–1747. doi: 10.2106/JBJS.N.01186 [DOI] [PubMed] [Google Scholar]
- 14.Singh K, Phillips FM, Park DK, Pelton MA, An HS, Goldberg EJ (2012) Factors affecting reoperations after anterior cervical discectomy and fusion within and outside of a Federal Drug Administration investigational device exemption cervical disc replacement trial. The spine journal : official journal of the North American Spine Society 12 (5):372–378. doi: 10.1016/j.spinee.2012.02.005 [DOI] [PubMed] [Google Scholar]
- 15.Gornet MF, Schranck FW, Copay AG, Kopjar B (2016) The Effect of Workers’ Compensation Status on Outcomes of Cervical Disc Arthroplasty: A Prospective, Comparative, Observational Study. The Journal of bone and joint surgery American volume 98 (2):93–99. doi: 10.2106/JBJS.O.00324 [DOI] [PubMed] [Google Scholar]
- 16.Narain AS, Hijji FY, Yom KH, Kudaravalli KT, Singh K (2017) Cervical disc arthroplasty: do conflicts of interest influence the outcome of clinical studies? The spine journal : official journal of the North American Spine Society 17 (7):1026–1032. doi: 10.1016/j.spinee.2017.03.018 [DOI] [PubMed] [Google Scholar]
- 17.Mehrotra A, Sloss EM, Hussey PS, Adams JL, Lovejoy S, SooHoo NF (2013) Evaluation of a center of excellence program for spine surgery. Medical care 51 (8):748–757. doi: 10.1097/MLR.0b013e31829b091d [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jee YM, Bak JS, Weinlander E, Anderson PA (2016) Comparing Nonrandomized Observational Studies With Randomized Controlled Trials in Cervical Disc Arthroplasty: A Meta-analysis. Spine 41 (5):419–428. doi: 10.1097/BRS.0000000000001377 [DOI] [PubMed] [Google Scholar]
- 19.Riew KD, Schenk-Kisser JM, Skelly AC (2012) Adjacent segment disease and C-ADR: promises fulfilled? Evidence-based spine-care journal 3 (S1):39–46. doi: 10.1055/s-0031-1298607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Phillips FM, Geisler FH, Gilder KM, Reah C, Howell KM, McAfee PC (2015) Long-term Outcomes of the US FDA IDE Prospective, Randomized Controlled Clinical Trial Comparing PCM Cervical Disc Arthroplasty With Anterior Cervical Discectomy and Fusion. Spine 40 (10):674–683. doi: 10.1097/BRS.0000000000000869 [DOI] [PubMed] [Google Scholar]
- 21.Jackson RJ, Davis RJ, Hoffman GA, Bae HW, Hisey MS, Kim KD, Gaede SE, Nunley PD (2016) Subsequent surgery rates after cervical total disc replacement using a Mobi-C Cervical Disc Prosthesis versus anterior cervical discectomy and fusion: a prospective randomized clinical trial with 5-year follow-up. Journal of neurosurgery Spine:1–12. doi: 10.3171/2015.8.SPINE15219 [DOI] [PubMed] [Google Scholar]
- 22.Phillips FM, Lee JY, Geisler FH, Cappuccino A, Chaput CD, DeVine JG, Reah C, Gilder KM, Howell KM, McAfee PC (2013) A prospective, randomized, controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. 2-year results from the US FDA IDE clinical trial. Spine 38 (15):E907–918. doi: 10.1097/BRS.0b013e318296232f [DOI] [PubMed] [Google Scholar]
- 23.Luo J, Gong M, Huang S, Yu T, Zou X (2015) Incidence of adjacent segment degeneration in cervical disc arthroplasty versus anterior cervical decompression and fusion meta-analysis of prospective studies. Archives of orthopaedic and trauma surgery 135 (2):155–160. doi: 10.1007/s00402-014-2125-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Verma K, Gandhi SD, Maltenfort M, Albert TJ, Hilibrand AS, Vaccaro AR, Radcliff KE (2013) Rate of adjacent segment disease in cervical disc arthroplasty versus single-level fusion: meta-analysis of prospective studies. Spine 38 (26):2253–2257. doi: 10.1097/BRS.0000000000000052 [DOI] [PubMed] [Google Scholar]
- 25.Zhu Y, Zhang B, Liu H, Wu Y, Zhu Q (2016) Cervical Disc Arthroplasty Versus Anterior Cervical Discectomy and Fusion for Incidence of Symptomatic Adjacent Segment Disease: A Meta-Analysis of Prospective Randomized Controlled Trials. Spine. doi: 10.1097/BRS.0000000000001537 [DOI] [PubMed] [Google Scholar]
- 26.Shriver MF, Lubelski D, Sharma AM, Steinmetz MP, Benzel EC, Mroz TE (2016) Adjacent segment degeneration and disease following cervical arthroplasty: a systematic review and meta-analysis. The spine journal : official journal of the North American Spine Society 16 (2):168–181. doi: 10.1016/j.spinee.2015.10.032 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.