

Abstract
Gordonia is a catalase-positive, aerobic, nocardioform, Gram-positive staining actinomycete that also shows weak acid-fast staining. Several Gordonia species are commonly found in the soil. The bacterium has been isolated from the saliva of domesticated/wild dogs as well. In hospitalized patients, most commonly it is found in the setting of intravascular catheter-related infections. However, recent reports show that it is being increasingly isolated from sternal wounds, skin/neoplastic specimens and from pleural effusions. Gordonia shares many common characteristics with Rhodococcus and Nocardia. Ergo, it is commonly misrecognized as Nocardia or Rhodococcus. Since this pathogen requires comprehensive morphological and biochemical testing, it is often difficult and cumbersome to isolate the species. Broad-range Polymerase Chain Reaction (PCR) and sequencing with genes like 16S rRNA or hsp65 are used to correctly identify the species. Identification is essential for choosing and narrowing the right antimicrobial agent. Herein, we report our experience with a patient who presented with sternal osteomyelitis after infection with this elusive bug.
Keywords: Gordonia bronchialis, infection, sternal osteomyelitis
“All things are hidden, obscure and debatable if the cause of the phenomena is unknown, but everything is clear if its cause be known.”
-Louis Pasteur in The Germ Theory and Its Application to Medicine and Surgery
Introduction
Gordonia is a catalase-positive, aerobic, nocardioform, Gram positive staining actinomycete that also shows weak acid-fast staining.[1] Several Gordonia species are commonly found in the soil.[2] The bacterium has been isolated from the saliva of domesticated/wild dogs as well.[3] In hospitalized patients, it is most commonly found in the setting of intravascular catheter-related infections. However, recent reports have shown that it has recently been isolated from sternal wounds,[4] skin/neoplastic specimens, and from pleural effusions.[5] Gordonia shares many common characteristics with Rhodococcus and Nocardia. Therefore, it is commonly misrecognized as Nocardia or Rhodococcus. Because Gordonia requires comprehensive morphological and biochemical testing, it is often difficult and cumbersome to isolate the species. It has an incubation period of a minimum of 4 days.[6] Broad-range polymerase chain reaction (PCR) and sequencing, with genes like 16S rRNA or hsp65, are used to correctly identify the species.[7] Here, we report a patient who presented with sternal osteomyelitis after infection with this elusive bug.
Case Description
A 74-year-old male patient with past medical history of essential hypertension, benign prostatic hyperplasia, asthma, and coronary artery disease presented with sternal chest pain. Upon examination, he was found to have wound dehiscence and sternal abscess. Patient had undergone a coronary artery bypass grafting (CABG) procedure 3 months back for his CAD. He underwent sternal debridement and removal of one sternal wire 1 month after the CABG. He endorsed minimal drainage from the sternal wound site. No associated fever, chills, nausea, vomiting, or shortness of breath were noted. Computed tomography (CT) scan of the chest showed persistent gas at the median sternotomy site with osseous destruction likely secondary to chronic osteomyelitis with abscess [Figure 1]. Post debridement, specimen was initially identified as a Corynebacterium; the patient received broad coverage with IV vancomycin and meropenem. The sternal abscess was drained by surgery and deep tissue cultures were sent for special microbiological testing.
Figure 1.
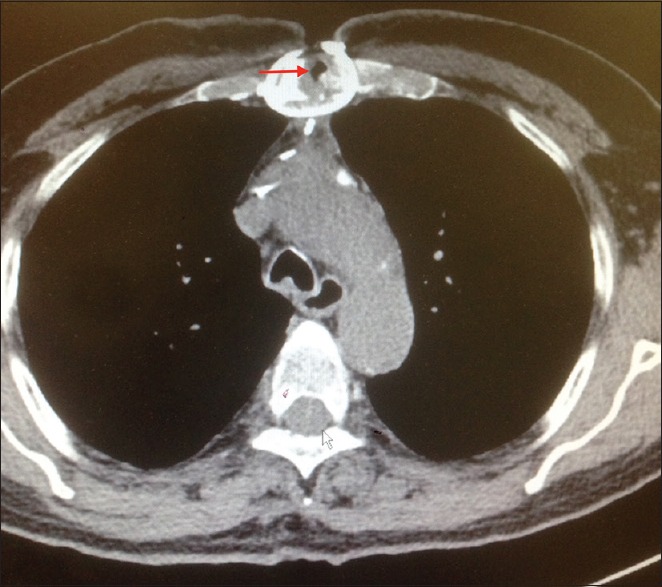
Computed tomography of the chest shows osteomyelitis of the sternum (red arrow)
Discussion
We isolated G. bronchialis from sternal deep tissue wound cultures of a patient who had undergone CABG 3 months back. G. bronchialis was the only microorganism cultured from the patient, and the patient was the only one with G. bronchialis infection in the hospital at the time. More than one specimen grew the same organism. Therefore, we can safely conclude that it was a true pathogen.
Gordonia (previously known as Gordona) genus was first isolated from other aerobic actinomycetes in 1971.[8] Because awareness about Gordonia is slowly increasing, it now comprises a significant minority of aerobic actinomycetes found in humans. One study reported that of 171 aerobic actinomycete isolates sent to the National Institutes of Health from 1996 to 2003, approximately 56% were Nocardia spp., 12% Mycobacteria spp., 11% Streptomyces spp., 8% Rhodococcus spp., 6% Gordonia spp., 0.6% Tsukamurella spp., and 0.6% Corynebacterium spp.[9]
Since 1971, 29 different Gordonia species have been isolated. Though the literature is scarce, there are few published reports of ventriculitis with an underlying ventricular shunt,[10] otitis externa and bronchitis,[11] arthritis associated with a biological absorbable bone/joint screw,[12] breast abscess,[13,14] keratitis/conjunctivitis,[15] skin and soft tissue infections,[16,17] and endocarditis from underlying central venous catheter.[18,19] A Spanish hospital published a report on Gordonia induced skin abscess, due to needle injection.[20] Two cases of peritoneal dialysis-related peritonitis by Gordonia have also been reported.[21,22]
In our review of the literature, we found only 6 reported cases of G. bronchialis sternal infection in humans over the past 26 years [Table 1]. Most of the reported sternal wound infections were due to outbreak in the hospital due to intraoperative transmission from a health care worker. A cluster of 7 cases after coronary artery bypass surgery were traced back to the dog of an operating room nurse. Ciprofloxacin, ceftriaxone, and cotrimoxazole were used as therapy.[3] One patient developed wound dehiscence post sternal closure following mitral valve replacement surgery. Samples from the wound site grew G bronchialis; clindamycin and ceftazidime were given.[23] A cluster of three cases developed sternal osteomyelitis following CABG; they were treated by wound debridement and negative pressure.[24] Another case after CABG was treated with vancomycin and cefotetan.[25] Similarly ceftriaxone and ciprofloxacin were used in 2013 following CABG.[26]
Table 1.
Reported cases of sternal infection by Gordonia
| Number of cases | Age | Sex | Year | Procedure | Immunity status | Therapy | Treatment duration | Method of identification | Reference |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 64 | Female | 2016 | Mitral valve replacement | Normal | Clindamycin and ceftazidime | 8 weeks | 16 sRNA sequencing | 28 |
| 3 | 47-68 | Male/Female | 2014 | CABG | Normal | Wound debridement and negative pressure wound therapy | Unknown | NA | 25 |
| 1 | 69 | Female | 2014 | CABG | Diabetes Mellitus | Vancomycin and Cefotetan; imipenem | 8 weeks | 16sRNA sequencing | 26 |
| 1 | 76 | Female | 2013 | CABG | Normal | Ceftriaxone and ciprofloxacin; wound debridement and VAC | Unknown | 16sRNA sequencing | 27 |
| 3 (Cluster) | 56-80 | Male | 2012 | CABG | Diabetes Mellitus (2 cases), Normal (1 case) | Imipenem, moxifloxacin, linezolid and minocycline; wound debridement | 60 days (mean), 120 days respectively | 16sRNA sequencing | 4 |
| 7 (cluster) | 51-68 | Male | 1991 | CABG | Diabetes mellitus (1 case), Steroid use (1 case), Obesity (3 cases), Prostate cancer (1 case), chronic lung disease (2 cases) | Ciprofloxacin, Cotrimoxazole, Ceftriaxone and Ciprofloxacin | 74 days, 122 days, 38 days 108 days respectively. | Conventional biochemical test | 3 |
Salient points of this report
The importance of correctly identifying Gordonia infection cannot be stressed enough. The most common confounding pathogen in making the correct diagnosis, is the coryneform Gram-positive rod[10]
Currently 16S rDNA or hsp65 gene sequencing is used to identify G. bronchialis at the species level. Mass spectrometry using matrix-assisted laser desorption ionization-time of flight mass spectrometry allows rapid identification of aerobic actinomycetes from cultured colonies. However, the isolate yielded log score between <2 and ≥1.7 cannot be used to be identify at the species level
No conclusive evidence-based treatment guidelines exist for G. bronchialis infection. Minocycline and ciprofloxacin were used in one report.[27] In another case, carbapenem or fluoroquinolone in combination with an aminoglycoside was used.[27] Trimethoprim-sulfamethoxazole has been reported to have poor efficacy against Gordonia species[28]
With the advent of 16S rRNA gene sequencing and matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS), Gordonia isolation is becoming more common. In the past, G. bronchialis infection has been underdiagnosed due to laboratory and technical limitations
This case report adds to the accumulating evidence for identifying and treating this rare Gram-positive bacterium and urges physicians to be mindful of its idiosyncrasy to cause sternal infections.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Arenskötter M, Bröker D, Steinbüchel A. Biology of the metabolically diverse genus Gordonia. Appl Environ Microbiol. 2004;70:3195–204. doi: 10.1128/AEM.70.6.3195-3204.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shen FT, Goodfellow M, Jones AL, Chen YP, Arun AB, Lai WA, et al. Gordonia soli sp. nov., a novel actinomycete isolated from soil. Int J Syst Evol Microbiol. 2006;56:2597–601. doi: 10.1099/ijs.0.64492-0. [DOI] [PubMed] [Google Scholar]
- 3.Richet HM, Craven PC, Brown JM, Lasker BA, Cox CD, McNeil MM, et al. A cluster of Rhodococcus (Gordona) bronchialis sternal-wound infections after coronary-artery bypass surgery. N Engl J Med. 1991;324:104–9. doi: 10.1056/NEJM199101103240206. [DOI] [PubMed] [Google Scholar]
- 4.Wright SN, Gerry JS, Busowski MT, Klochko AY, McNulty SG, Brown SA, et al. Gordonia bronchialis sternal wound infection in 3 patients following open heart surgery: Intraoperative transmission from a healthcare worker. Infect Control Hosp Epidemiol. 2012;33:1238–41. doi: 10.1086/668441. [DOI] [PubMed] [Google Scholar]
- 5.Johnson JA, Onderdonk AB, Cosimi LA, Yawetz S, Lasker BA, Bolcen SJ, et al. Gordonia bronchialis bacteremia and pleural infection: Case report and review of the literature. J Clin Microbiol. 2011;49:1662–6. doi: 10.1128/JCM.02121-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Drancourt M, Pelletier J, Cherif AA, Raoult D. Gordona terrae central nervous system infection in an immunocompetent patient. J Clin Microbiol. 1997;35:379–82. doi: 10.1128/jcm.35.2.379-382.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gil-Sande E, Brun-Otero M, Campo-Cerecedo F, Esteban E, Aguilar L, García-de-Lomas J. Etiological misidentification by routine biochemical tests of bacteremia caused by Gordonia terrae infection in the course of an episode of acute cholecystitis. J Clin Microbiol. 2006;44:2645–7. doi: 10.1128/JCM.00444-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tsukamura M. Proposal of a new genus, Gordona, for slightly acid-fast organisms occurring in sputa of patients with pulmonary disease and in soil. J Gen Microbiol. 1971;68:15–26. doi: 10.1099/00221287-68-1-15. [DOI] [PubMed] [Google Scholar]
- 9.Poonwan N, Mekha N, Yazawa K, Thunyaharn S, Yamanaka A, Mikami Y. Characterization of clinical isolates of pathogenic Nocardia strains and related actinomycetes in Thailand from 1996 to 2003. Mycopathologia. 2005;159:361–8. doi: 10.1007/s11046-005-1045-7. [DOI] [PubMed] [Google Scholar]
- 10.Blaschke AJ, Bender J, Byington CL, Korgenski K, Daly J, Petti CA, et al. Gordonia species: Emerging pathogens in pediatric patients that are identified by 16S ribosomal RNA gene sequencing. Clin Infect Dis. 2007;45:483–6. doi: 10.1086/520018. [DOI] [PubMed] [Google Scholar]
- 11.Iida S, Taniguchi H, Kageyama A, Yazawa K, Chibana H, Murata S, et al. Gordonia otitidis sp. nov., isolated from a patient with external otitis. Int J Syst Evol Microbiol. 2005;55:1871–6. doi: 10.1099/ijs.0.63282-0. [DOI] [PubMed] [Google Scholar]
- 12.Jannat-Khah DP, Halsey ES, Lasker BA, Steigerwalt AG, Hinrikson HP, Brown JM. Gordonia araii infection associated with an orthopedic device and review of the literature on medical device-associated Gordonia infections. J Clin Microbiol. 2009;47:499–502. doi: 10.1128/JCM.01504-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Werno AM, Anderson TP, Chambers ST, Laird HM, Murdoch DR. Recurrent breast abscess caused by Gordonia bronchialis in an immunocompetent patient. J Clin Microbiol. 2005;43:3009–10. doi: 10.1128/JCM.43.6.3009-3010.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zardawi IM, Jones F, Clark DA, Holland J. Gordonia terrae-induced suppurative granulomatous mastitis following nipple piercing. Pathology. 2004;36:275–8. doi: 10.1080/00313020410001692639. [DOI] [PubMed] [Google Scholar]
- 15.Kempf VAJ, Schmalzing M, Yassin AF, Schaal KP, Baumeister D, Arenskötter M, et al. Gordonia polyisoprenivorans septicemia in a bone marrow transplant patient. Eur J Clin Microbiol Infect Dis. 2004;23:226–8. doi: 10.1007/s10096-003-1087-z. [DOI] [PubMed] [Google Scholar]
- 16.Bakker XR, Spauwen PH, Dolmans WM. Mycetoma of the hand caused by Gordona terrae: A case report. J Hand Surg Br. 2004;29:188–90. doi: 10.1016/j.jhsb.2003.09.011. [DOI] [PubMed] [Google Scholar]
- 17.Lai CC, Wang CY, Liu CY, Tan CK, Lin SH, Liao CH, et al. Infections caused by Gordonia species at a medical center in Taiwan, 1997 to 2008. Clin Microbiol Infect. 2010;16:1448–53. doi: 10.1111/j.1469-0691.2009.03085.x. [DOI] [PubMed] [Google Scholar]
- 18.Lesens O, Hansmann Y, Riegel P, Heller R, Benaissa-Djellouli M, Martinot M, et al. Bacteremia and endocarditis caused by a Gordonia species in a patient with a central venous catheter. Emerg Infect Dis. 2000;6:382–5. doi: 10.3201/eid0604.000410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Verma P, Brown JM, Nunez VH, Morey RE, Steigerwalt AG, Pellegrini GJ, et al. Native valve endocarditis due to Gordonia polyisoprenivorans: Case report and review of literature of bloodstream infections caused by Gordonia species. J Clin Microbiol. 2006;44:1905–8. doi: 10.1128/JCM.44.5.1905-1908.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bartolomé-Ávarez J, Sáez-Nieto JA, Escudero-Jiménez A, Barba-Rodríguez N, Galán-Ros J, Carrasco G, et al. Cutaneous abscess due to Gordonia bronchialis: Case report and literature review. Rev Esp Quimioter. 2016;29:170–3. [PubMed] [Google Scholar]
- 21.Lam JY, Wu AK, Leung WS, Cheung I, Tsang CC, Chen JH, et al. Gordonia species as emerging causes of continuous-ambulatory-peritoneal-dialysis-related peritonitis identified by 16S rRNA and secA1 gene sequencing and matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) J Clin Microbiol. 2015;53:671–6. doi: 10.1128/JCM.02971-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ma TK, Chow KM, Kwan BC, Lee KP, Leung CB, Li PK, et al. Peritoneal-dialysis related peritonitis caused by Gordonia species: Report of four cases and literature review. Nephrology. 2014;19:379–83. doi: 10.1111/nep.12233. [DOI] [PubMed] [Google Scholar]
- 23.Rodriguez-Lozano J, Pérez-Llantada E, Agüero J, Rodríguez-Fernández A, Ruiz de Alegria C, Martinez-Martinez L, et al. Sternal wound infection caused by Gordonia bronchialis: Identification by MALDI-TOF MS. JMM Case Rep. 2016;3:e005067. doi: 10.1099/jmmcr.0.005067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nguyen DB, Gupta N, Aboud-Daoud A, KleKamp BG, Rhone C, Winston T, et al. A polymicrobial outbreak of surgical site infections following cardiac surgery at a community hospital in Florida, 2011-2012. Am J Infect Control. 2014;42:432–5. doi: 10.1016/j.ajic.2013.11.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chang JH, Ji M, Hong HL, Choi SH, Kim YS, Chung CH, et al. Sternal osteomyelitis caused by Gordonia bronchialis after open-heart surgery. Infect Chemother. 2014;46:110–4. doi: 10.3947/ic.2014.46.2.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Vasquez MA, Marne C, Villuendas MC, Arazo P. Subacute sternal osteomyelitis caused by Gordonia bronchialis after open-heart surgery. Enferm Infecc Microbiol Clin. 2013;31:559–60. doi: 10.1016/j.eimc.2013.02.012. [DOI] [PubMed] [Google Scholar]
- 27.Johnson JA, Onderdonk AB, Cosimi LA, Yawetz S, Lasker BA, Bolcen SJ, et al. Gordonia bronchialis bacteremia and pleural infection: Case report and review of the literature. J Clin Microbiol. 2011;49:1662–6. doi: 10.1128/JCM.02121-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Moser BD, Pellegrini GJ, Lasker BA, Brown JM. Pattern of antimicrobial susceptibility obtained from blood isolates of a rare but emerging human pathogen, Gordonia polyisoprenivorans. Antimicrob Agents Chemother. 2012;56:4991–3. doi: 10.1128/AAC.01251-12. [DOI] [PMC free article] [PubMed] [Google Scholar]