

Abstract
Patient: Female, 38
Final Diagnosis: Talar extrusion
Symptoms: Acute right ankle posttraumatic injury
Medication: —
Clinical Procedure: Tibiocalcaneal arthrodesis placement
Specialty: Radiology
Objective:
Rare disease
Background:
Extrusion of the talus is a very rare sequela of high energy trauma. There is limited information on these cases, given the rarity, with no consensus on treatment. Our case report demonstrates the radiographic and computed tomography (CT) findings in this injury.
Case Report:
We report the case of a 38-year-old female patient who was involved in a high energy trauma secondary to a motor vehicle accident. Lower extremity CT revealed talar extrusion with posteriorly displaced residual small fracture fragments and large pockets of emphysema in its expected location. Orthopedic management consisted of open reduction, debridement, and external fixation of the ankle, with an internal fixation placed afterwards.
Conclusions:
Talar extrusion is a very rare entity with few cases reported in the literature. Prompt identification of extrusion of the talus is key given that treatment is time sensitive and surgical management is needed.
MeSH Keywords: Ankle Injuries, Foot Injuries, Orthopedic Fixation Devices, Talus
Background
Complete talar extrusion can result from high energy trauma to the distal lower extremity. It is a dislocation of the talus from the tibiotalar, subtalar, and talonavicular joints, which tends to have associated fractures (commonly malleoli, talar body, or neck). It is known as a pan-talar dislocation and luxatio tali totalis, and almost all cases are open injuries. The mechanism of injury is tibiotalar plantar flexion combined with excessive supination or pronation. The current literature on total talar dislocation is limited, with most cases describing an anterior-lateral ankle wound with the talus extruded laterally [1].
Open extrusion of the talus is well-known, but very rare, with several case reports describing the injury in the literature. The true incidence is unknown, but is estimated to be approximately 0.06% of all dislocations and 2% of all talar injuries [2,3]. There are multiple accepted therapeutic options, dependent on time elapsed from injury and vascular supply, including immediate reimplantation of the talus, reconstruction with talar replacement, or tibiocalcaneal arthrodesis [4]. In this case report, we discuss a case of an open injury with near total talar extrusion.
Case Report
A 38-year-old Hispanic female patient with no significant past medical history, presented with multiple body trauma due to a motor vehicle accident. She reported an episode of loss of consciousness after the crash, and indicated feeling pain throughout her body, more pronounced in the lower back and right ankle.
Physical evaluation revealed an alert, stable patient, without neurological deficits. Multiple abrasions and hematomas across the chest and abdomen were seen. She had point tenderness in the lower back. Her right ankle was swollen with limited range of motion and a contaminated open wound at the anterolateral aspect of the ankle which measured approximately 8 cm longitudinally. Surrounding ecchymosis and blood products were noted. No neurovascular deficit was appreciated. The wound was cleansed with saline solution and the patient was given broad-spectrum antibiotics. Overlying gauzes as well as a posterior cast were placed.
Multiple radiologic studies were performed, which revealed fractures of the right 2nd to 5th ribs, clear lungs, no intracranial abnormalities, and subcutaneous swelling throughout the left upper abdomen and right chest. She also suffered an L3 vertebral body compression fracture without spinal canal narrowing. Right lower extremity radiographs revealed right ankle traumatic dislocation and absence of the talus, consistent with talar extrusion (Figures 1, 2). Due to the necessity of emergent orthopedic care, the patient was promptly transferred to the primary trauma center of the island, where she was promptly evaluated by the orthopedic team.
Figure 1.
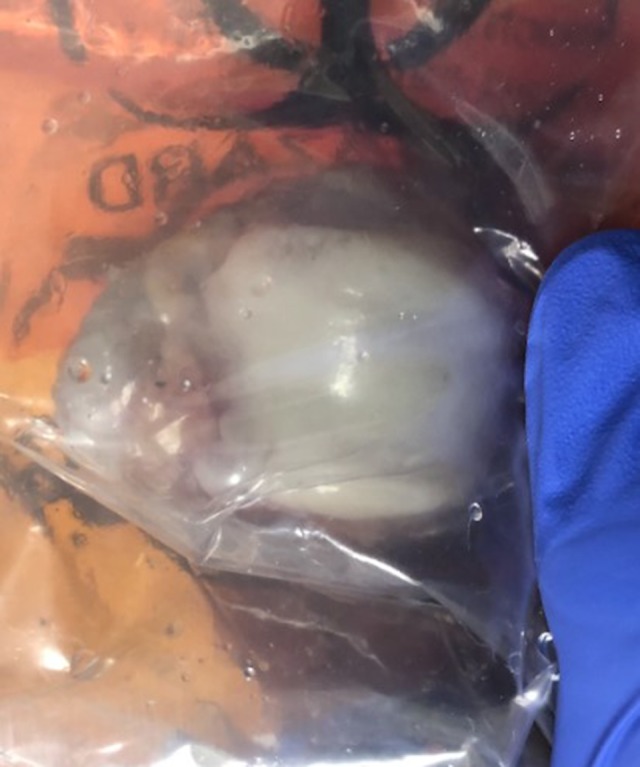
The extruded talus in this case, seen within a plastic bag.
Figure 2.

Right ankle radiograph (lateral view). Patient status post plaster splint placement. Absence of most of the talus is noted, with osseous fragments suggested posterior to the expected location of the talus. Soft tissue emphysema and soft tissue defect at the lateral malleolar region is seen, which involves the articular surface indicative of an open fracture dislocation lesion.
A pre-operative lower extremity computed tomography (CT) scan with multiplanar reconstruction was then performed that revealed talar extrusion with posteriorly displaced residual small fracture fragments and large pockets of emphysema in its expected location (Figures 3, 4). Additionally, loss of the normal ankle mortise and dissociation of the talofibular and tibiotalar joints was seen, as well as a linear minimally displaced chip fracture of the anterosuperior aspect of the calcaneus. The orthopedic team proceeded with surgical debridement and irrigation with broad-spectrum antibiotics, under general anesthesia. The talus was not preserved. A tibiocalcaneal external fixator was placed for stability, and the wound was closed. The external fixator was removed after 7 days, and the ankle was internally fixated with a tibiocalcaneal arthrodesis (Figure 5). No postoperative complications occurred. The extremity was rested; follow-up ankle radiographs showed an intramedullary rod at the level of the distal tibial shaft extending caudally beyond the tibia, interlocking with a perpendicular oriented orthopedic screw through the posterior aspect of the calcaneus. After 5 more days, the patient was discharged home to be followed in outpatient clinics. The patient was instructed to rest the extremity and begin non-weight bearing exercises as tolerated.
Figure 3.

Sagittal computed tomography image. Examination reveals extrusion of most of the right talus bone, with visualization of only the posterior fracture fragments which are dislocated posterosuperiorly (orange arrow) abutting the posterior malleolus. Emphysematous changes noted at ankle joint and surrounding soft tissues, with gas bubbles extending superiorly through the intramuscular fractures and subcutaneous tissues correlating with the presence of soft tissue laceration. Posterior cast is present.
Figure 4.

The 3-dimensional computed tomography reconstruction is shown. Image shows clear absence of osseous structures in the expected location of the talus.
Figure 5.

Lateral right ankle radiograph revealing an intramedullary rod with a proximal and a distal interlocking screw fusing the tibia with the calcaneus. Perpendicular oriented orthopedic screws through the posterior aspect of the calcaneus interlocking the previous described rod. Comminuted fracture of the medial malleolus and comminuted fracture of the distal calcaneal region. Widening of the scaphoid calcaneal joint space. A skin staples about the foot and distal leg medially.
Four months after discharge, the patient began to tolerate weight bearing ambulation, with assistance of a walker. The patient was followed up in outpatient clinics every 2 weeks by the orthopedic services and back pain clinics. By approximately 5 months, the patient had adequate mobility of the joint and tolerated ambulation without assistance, with mild pain, which has since improved. Unfortunately, due to her lumbar fracture, the patient continued to have moderate back pain, and will be followed up with a lumbar magnetic resonance (MR) imaging study to assess for further treatment options.
Discussion
The talus is the only bone in the foot without muscular attachment, making it vulnerable to extrusion, a compound triarticular dislocation, involving the tibiotalar, talonavicular, and subtalar joints. Talar bone avulsion secondary to a traumatic event is a very rare event, furthermore, there is limited research and case reports on this subject, particularly of total extrusion. This case demonstrated an open dislocation of the talus with near total talar extrusion with residual small posteriorly displaced bone fragments. Open injuries, like the one in this case, account for slightly over half of the cases.
In cases of high impact trauma, it is important to fully evaluate the patient, since these fractures tend to not occur in isolation. Of note, it has been reported that talar fractures are associated with calcaneal and spine fractures due to high-energy impact loads [1], both of which were seen in this case.
The most common complications of this type of injury are infection and avascular necrosis. The rate of infection is linked to whether the injury is open or closed, with open injuries demonstrating an increased risk. Risk of avascular necrosis, like elsewhere in the body, depends on the amount of compromise of the blood supply. The talus is covered nearly completely by cartilage, limiting vascular supply. Its vascularity stems from 3 main sources. The artery of the tarsal canal and the deltoid branches of the posterior tibial artery provide blood to the talar body, with the artery of the tarsal canal providing the main bulk of the blood supply. The talar head, on the other hand, receives its blood supply from the peroneal and anterior tibial arteries, through the artery of the sinus tarsi. Additional blood supply to the talar head is also achieved through branches of the dorsalis pedis. Distal branches from these vessels eventually form a network of intraosseous anastomoses, which are complete in a sixth of the population. Susceptibility of avascular necrosis is thus dependent on the nature of these anastomosis and associated tissue damage. In cases such as the one presented here, with an open talar extrusion, and complete dissociation of almost the entirety of the talar bone, blood supply was nearly unequivocally compromised, leading to avascular necrosis. Multiple studies agree there is a very poor prognosis if total talar dislocation is involved [1,2].
There is no consensus about appropriate treatment for an extruded talus [5]. Broad-spectrum antibiotic therapy is recommended. Although immediate closed or open reduction of the talus is ideal to preserve function, it is not always feasible. In cases where the talus is preserved, radiologic follow-up is recommended to evaluate for possible development of avascular necrosis, which is best assessed with MR imaging, and the patient should be counseled about chronic changes, such as post-traumatic arthritis. If avascular necrosis develops, it can be treated in many cases conservatively, with weight bearing restrictions, with talectomy with or without arthrodesis as a secondary option. In this case, the talus was not preserved. Open reduction, debridement, and external fixation of the ankle as hindfoot was performed, followed by placement of an internal fixation.
Conclusions
Talar extrusion is a very rare entity sequela of high impact trauma, with few cases reported in the literature. Evaluation with multiple modalities, including plain radiographs and CT gives further insight into the injury and associated insult to adjacent structures. Prompt identification of extrusion of the talus is key given that treatment is time sensitive and surgical management is needed. Treatment consists of wound irrigation, debridement, and temporary stabilization, with talar preservation or tibiocalcaneal fusion.
Acknowledgments
Many thanks to the technical assistants and nurses that assisted in the conduction of the radiologic studies discussed. Also, we wish to use this opportunity to acknowledge the efforts and dedication of the orthopedic team and trauma residents involved with the patient care.
References:
- 1.Melenevsky Y, Mackey R, Brad Abrahams R, Thompson N. Talar fractures and dislocations: A radiologist’s guide to timely diagnosis and classifications. Radiographics. 2015;35:756–79. doi: 10.1148/rg.2015140156. [DOI] [PubMed] [Google Scholar]
- 2.Van Opstal N, Vandeputte G. Traumatic talar extrusion: Case reports and literature review. Acta Orthopaedica Belgica. 2009;75:699–704. [PubMed] [Google Scholar]
- 3.Kumar Y, Reddy S, Kumar Golla D, Ganesh N. Closed talar dislocation without associated fracture a very rare injury, a case report. J Orthop Case Rep. 2014;4(2):10–12. doi: 10.13107/jocr.2250-0685.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Vaienti L, Maggi F, Gazzola R, Lanzani E. Therapeutic management of complicated talar extrusion: literature review and case report. J Orthop Traumat. 2011;12(1):61–64. doi: 10.1007/s10195-011-0129-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lee HS, Chung HW, Suh JS. Total extrusion without soft tissue attachments. Clin Orthop Surg. 2014;6(2):236–41. doi: 10.4055/cios.2014.6.2.236. [DOI] [PMC free article] [PubMed] [Google Scholar]