

Abstract
Background
To evaluate subtle and early premature ventricular complex (PVC)–induced ventricular impairment in patients with frequent PVCs and without structural heart disease by real‐time 3‐dimensional (3D) speckle tracking echocardiography (RT3D‐STE).
Hypothesis
Patients with frequent premature ventricular complexes with normal left ventricular ejection fraction have subtle left ventricular dysfunction.
Methods
Forty patients (22 male) with a single source of frequent PVCs and 40 healthy controls (24 male) underwent assessment by conventional 2‐dimensional (2D) echocardiography and RT3D‐STE. Left ventricular ejection fraction (LVEF), and global longitudinal, circumferential, radial, and area strain (GLS, GCS, GRS, and GAS, respectively) and individual segment strain were calculated using off‐line analysis software and compared between the 2 groups.
Results
There were no significant differences in baseline clinical or 2D echocardiographic variables including LVEF between groups. However, all RT3D‐STE assessed variables, including GLS, GCS, GRS, GAS, and individual segment strain, were significantly lower (P < 0.05) in the PVC group than the control group, and showed strong correlations, most prominently GCS (r = −0.84, P = 0.020), with LV function as assessed by LVEF. 3D‐STE measurements showed good intraobserver, interobserver, and test–retest agreement.
Conclusions
In patients with frequent PVCs and normal LVEF, 3D ‐STE revealed lower global and regional strain values than in healthy controls. RT3D‐STE is a novel, feasible and reproducible method to assess cardiac function and appears suitable to detect subtle left ventricular dysfunction.
Keywords: Premature Ventricular Complexes, Echocardiography, Real‐Time 3‐Dimensional Speckle Tacking Imaging, Left Ventricular Function
1. INTRODUCTION
Premature ventricular complexes (PVCs) are commonly seen in clinical practice. In recent years, studies have shown that frequent PVCs without structural heart disease might lead to cardiac dysfunction, and even cardiomyopathy.1, 2, 3, 4 However, traditional echocardiographic methods may not effectively evaluate subtle and early forms of PVC‐induced ventricular function impairment. Real‐time 3‐dimensional (3D) speckle tracking echocardiography (STE), an advancement over conventional 2‐dimensional (2D) STE, provides a new, convenient and noninvasive method for quantitative evaluation of cardiac function by allowing to measure strain values, better capturing 3D cardiac motion and addressing the failure of 2D‐STE to track out‐of‐plane speckle motion.5, 6, 7, 8 The present study evaluated subtle and early forms of PVC‐induced ventricular impairment in patients with PVCs and without structural heart disease by 3D‐STE, which might be useful for early detection and risk stratification of cardiac function impairment.
2. METHODS
All research of this study have been approved by the ethics committee of Zhongshan Hospital, Fudan University.
2.1. Study population
The present study enrolled 40 patients (22 males; age 40 ± 17 years [range, 18–66 years]), who were admitted to our hospital from July 2013 to March 2014 for frequent PVCs (>10,000 monomorphic PVCs/24 hours of continuous Holter monitoring recording) over 3.1 ± 1.2 years. Structural and ischemic heart disease were excluded in all patients, as were hypertension, diabetes, hyperthyroidism, or other diseases that may cause damage to cardiovascular structure and function.
A total of 40 healthy controls (24 males; age 42 ± 12 years [range, 20–62 years]) were chosen during the same period. Cardiopulmonary diseases were excluded by routine physical examination, chest x‐ray, electrocardiogram (ECG), and echocardiography.
2.2. Echocardiographic examination
A GE Vivid E9 Color Doppler Ultrasound Scanner (General Electric Vingmed, Horten, Norway) was used. For 2D ultrasonography, a M5S‐D active area‐array single‐crystal phased array probe (frequency: 1.5–4.6 MHz) was used, and for 3D ultrasonography, a 4 V‐D active area array probe (phased‐array 4‐dimensional [4D] volume probe, frequency: 1.5–4.0 MHz) and GE EchoPAC off‐line analysis software workstation (version no. 110) were used.
2.3. Routine 2D echocardiography
The subjects were placed in left lateral decubitus, and then the depth, angle, and gain were adjusted in 2D mode to clearly display the endocardia. The section views in routine examination included parasternal long‐axis, parasternal short axis, and apex views. Aortic root diameter, left atrium diameter, left ventricular end‐diastolic diameter, left ventricular end‐systolic diameter, interventricular septum thickness, and left ventricular posterior thickness were measured; left ventricular end‐diastolic volume (LVEDV) and left ventricular end‐systolic volume (LVESV) were measured, and left ventricular ejection fraction (LVEF) was calculated.
2.4. Real‐time 3D speckle tracking echocardiography
The subjects were placed in left lateral decubitus, breathing peacefully, and connected to the synchronous ECG recorder. The depth, angle, and gain were adjusted in 2D mode to display clearly the endocardia. The probe was placed on the cardiac apex; after A4C was displayed, fan beam angle and depth were adjusted properly; the harmonic wave and optimized mode were enabled to display the optimal apical 4‐chamber view; the probe was switched to 4D mode, and the patients were asked to hold their breath after breathing out to acquire the 15° * 60° narrow‐angled stereoscopic images in 4 successive steady sinus cardiac cycles, which generated 60° * 60° wide‐angled, pyramid‐shaped, full‐volume real‐time 3D images. All image series were loaded into the memory for off‐line data analysis.
An EchoPAC off‐line analysis software workstation (EchoPAC version 110; GE Medical Systems, Horten, Norway) was used to automatically convert the images into left ventricular Ap4C view, Ap2C, and 3 short‐axis views (namely basal, papillary muscle, and cardiac apex levels) in the three dimensional speckle tracking image (3D‐STI) analysis environment. At left ventricular end‐diastole and left ventricular end‐systole, 1 point was graphed at the center of mitral annulus and apical endocardia, respectively. The software automatically drew the tracing curves of end‐diastolic and end‐systolic endocardia and measured LVEDV and LVESV. The program then automatically calculated and generated bull's eye plots and strain rate curves of strain parameters of left ventricular segments and recorded longitudinal strain (LS), circumferential strain (CS), radial strain (RS), and area strain (AS) of the entire left ventricle and of each segment.
2.5. Repeated test
3D‐STE images of 10 subjects were randomly sampled. They were analyzed 2 times by 1 analyzer to calculate intraobserver differences and 2 times by different analyzers to calculate interobserver differences.
2.6. Statistical analysis
Statistical analysis was conducted for all the acquired data using SPSS 19.0 software (IBM, Armonk, NY); normality tests were conducted for all groups of data. All parameters had normal distributions and are expressed as mean ± standard deviation, The t test with 2 independent samples was used to compare the same variable in different groups. The Pearson method was used to analyze the correlation between global left ventricular strain and LVEF. Intraclass correlation coefficients and Bland‐Altman test were used to analyze interobserver and intraobserver differences. A value of P < 0.05 was considered statistically significant.
3. RESULTS
3.1. Patient characteristics and 2D echocardiography result analysis
In 3D‐STE analysis, 2 patients with frequent PVCs and 1 control were not included because of poorer image quality (>3 segments could not be analyzed).
The frequent PVC and control groups were comparable in terms of baseline clinical characteristics (Table 1). The patients with frequent PVCs had mean disease duration of 3.1 ± 1.2 years, PVC load of 22.8% ± 9.7%, and time limit of PVC wide QRS wave of 163 ± 3 ms, with single morphology. PVC morphology was left bundle branch block and right bundle branch block in 36 and 2 patients, respectively.
Table 1.
Baseline clinical and two‐dimensional echocardiographic characteristics of control and PVC groups
| Variable | Controls (n = 39) | PVC Group (n = 38) | P Value |
|---|---|---|---|
| Age (y) | 42 ± 12 | 40 ± 17 | 0.655 |
| Gender (M/F) | 23/16 | 22/16 | 0.402 |
| Body surface area (m2) | 1.76 ± 0.15 | 1.72 ± 0.19 | 0.719 |
| AORD (mm) | 30.55 ± 3.50 | 30.12 ± 3.72 | 0.638 |
| LAD (mm) | 33.76 ± 3.63 | 34.32 ± 4.79 | 0.591 |
| LVEDD (mm) | 46.24 ± 4.22 | 48.04 ± 4.37 | 0.100 |
| LVESD (mm) | 28.62 ± 3.12 | 28.84 ± 2.72 | 0.109 |
| IVST (mm) | 8.24 ± 0.93 | 8.40 ± 1.26 | 0.539 |
| LVPWT (mm) | 8.33 ± 0.95 | 8.08 ± 1.12 | 0.328 |
| LVEF (%) | 66.74 ± 3.85 | 65.12 ± 4.02 | 0.107 |
Abbreviations: AORD, aortic root diameter; F, female; IVST, interventricular septum thickness; LAD, left atrium diameter; LVEDD, left ventricular end diastolic diameter; LVEF, left ventricular ejection fraction; LVESD, left ventricular end systolic diameter; LVPWT, left ventricular posterior thickness; M, male; PVC, premature ventricular complex.
No significant differences in routine 2D echocardiography, including LVEF, were apparent between the frequent PVC and control groups (P > 0.05) (Table 1).
3.2. Analysis of 3D‐STI bull's eye plot and strain rate curves
In the control group, the bull's eye plot had uniform color and the strain curves were consistent. Global longitudinal strain (GLS), global circumferential strain (GCS), and global area strain (GAS) curve waveforms mainly consisted of negative single peaks. GAS was the complex of GLS and GCS, representing the percentage of endocardial surface area changes in a cardiac cycle starting from the start frame, with the maximum absolute strain value in the middle segment. Global radial strain (GRS) curve waveforms mainly consisted of positive single peaks, with the maximum absolute strain value in the middle segment and minimum value in the apical segment. (See Supporting Figures 1 and 3in the online version of this article).
In the PVC group, the bull's eye plot had uneven color and the strain curves were inconsistent, disordered, and unsmooth. In addition, their wave amplitudes were greatly lower than in the control group.
3.3. 3D‐STE result analysis
There were no significant differences in mean heart rate, LVEDV, LVESV, 3D LVEF, or other indicators between the PVC and control groups (P > 0.05). In the PVC vs control groups, GLS (−13.50% ± 3.00% vs −18.31% ± 3.12%, P = 0.001), GCS (−13.21% ± 4.52% vs −19.49% ± 2.60%, P = 0.001), GAS (−22.43% ± 5.02% vs −29.86% ± 4.81%, P = 0.001), and GRS (36.31% ± 8.81% vs 49.61% ± 10.12%, P = 0.001) were significantly lower (P < 0.05), as were LS, CS, AS, and RS values of left ventricular basal, middle, and apical segments (Table 2).
Table 2.
Three‐dimensional speckle tracking echocardiography result analysis of the control and PVC groups
| Variable | Controls (n = 39) | PVC Group (n = 38) | P Value |
|---|---|---|---|
| HR (bpm) | 71.33 ± 0.58 | 74.53 ± 9.53 | 0.571 |
| LVEDV (mL) | 88.50 ± 9.29 | 82.76 ± 13.48 | 0.267 |
| LVESV (mL) | 36.63 ± 6.68 | 33.55 ± 7.63 | 0.309 |
| 3D LVEF (%) | 64.25 ± 2.71 | 63.00 ± 2.27 | 0.194 |
| GLS (%) | −18.31 ± 3.12 | −13.50 ± 3.00 | 0.001 |
| GCS (%) | −19.49 ± 2.60 | −13.21 ± 4.52 | 0.001 |
| GAS (%) | −29.86 ± 4.81 | −22.43 ± 5.02 | 0.001 |
| GRS (%) | 49.61 ± 10.12 | 36.31 ± 8.81 | 0.001 |
| Basal segment LS (%) | −16.22 ± 2.81 | −11.63 ± 2.66 | 0.002 |
| Middle segment LS (%) | −19.87 ± 3.88 | −14.60 ± 3.54 | 0.005 |
| Apical segment LS (%) | −17.70 ± 2.90 | −13.87 ± 3.01 | 0.008 |
| Basal segment CS (%) | −17.59 ± 4.29 | −10.95 ± 2.77 | 0.000 |
| Middle segment CS (%) | −19.70 ± 2.90 | −13.94 ± 2.96 | 0.000 |
| Apical segment CS (%) | −20.53 ± 2.82 | −14.28 ± 2.84 | 0.000 |
| Basal segment AS (%) | −27.46 ± 5.31 | −17.40 ± 6.17 | 0.001 |
| Middle segment AS (%) | −34.71 ± 5.26 | −25.88 ± 6.25 | 0.002 |
| Apical segment AS (%) | −30.23 ± 5.76 | −22.25 ± 6.54 | 0.007 |
| Basal segment RS (%) | 51.45 ± 10.50 | 35.57 ± 6.14 | 0.001 |
| Middle segment RS (%) | 55.04 ± 9.85 | 36.14 ± 8.57 | 0.000 |
| Apical segment RS (%) | 46.54 ± 11.02 | 23.43 ± 9.59 | 0.000 |
Abbreviations: AS, area strain; CS, circumferential strain; GAS, global area strain; GCS, global circumferential strain; GLS, global longitudinal strain; GRS, global radial strain; HR, heart rate; LS, longitudinal strain; LV, left ventricular; LVEDV, left ventricular end‐diastolic volume; LVESV, left ventricular end‐systolic volume; PVC, premature ventricular complex; RS, radial strain.
3.4. 3D‐STE result analysis for patients with PVC load <20% and ≥20%
Comparison of LVEDV, LVESV, LVEF, GLS, GCS, GAS, and GRS between 21 (55%) patients with PVC load <20% (15.08% ± 4.82%) and 17 (46%) patients with PVC load ≥20% (32.69% ± 5.95%) revealed that patients with higher PVC load (≥20%) had numerically larger end‐diastolic volume (EDV) and end‐systolic volume (ESV), but lower LVEF and strain values than those with lower PVC load (<20%); however, the differences did not achieve statistical significance.
3.5. Correlation and repeatability tests of global left ventricular strains and LVEF
Global left ventricular strain (GLVS) and LVEF were well correlated between the frequent PVC and control groups. GLS, GCS, and GAS were negatively correlated with LVEF (r values: −0.78, −0.84, and −0.82, respectively; P < 0.05). GRS was positively correlated with LVEF (r value: 0.79, P < 0.05). GCS and LVEF had the best correlation. Intraobserver and interobserver stain values showed a consistent trend with good repeatability.
4. DISCUSSION
Although PVCs used to be considered as mostly benign, long‐term frequent PVCs may lead to cardiomegaly, cardiac hypofunction, and even PVC‐induced cardiomyopathy in some patients,9, 10, 11 via pathogenic mechanisms possibly involving ventricular systole dyssynchrony during PVCs, shortened coupling intervals, and postextrasystolic potentiation.12, 13, 14, 15, 16 PVC‐induced cardiomyopathy was first classified as an indication of ventricular tachycardia catheter ablation by European Heart Rhythm Association/Heart Rhythm Society Expert Consensus on Catheter Ablation of Ventricular Arrhythmias in 2009.17 However, no definite criteria have been established to guide clinical diagnosis of PVC‐induced cardiomyopathy, which continues to be done by exclusion or retrospectively. It also remains controversial whether interventions are required for patients with frequent PVCs who are asymptomatic or have normal LVEF.
The present study, which used the latest 3D‐STE technology to evaluate impairment of cardiac function by measuring myocardial mechanics parameters such as strain values in patients with frequent PVCs and without accompanying structural heart diseases, revealed that compared to healthy controls, even patients with no abnormal indicators by conventional echocardiography had various degrees of cardiac function impairment manifested as reduced global and regional strain values, uneven overall color of bull's eye plots, disordered strain and less smooth curves, and significantly reduced wave amplitudes.
Several previous studies concluded that premature beat load was negatively correlated with cardiac function, suggesting that premature beat load was 1 of the risk factors for development of PVC‐induced cardiomyopathy.18, 19, 20 The present study compared patients with different PVC loads using 20% as a cutoff, and found that those with higher PVC loads had numerically but not significantly larger EDV and ESV values but lower LVEF and strain values. One could posit that disease duration might be 1 of the influential factors (average disease duration was 3 years in the present study) in addition to premature beat load, and that extending the follow‐up period might increase the difference. Both the possible influence of premature beat load on cardiac function and the cutoff warrant further clinical studies. Consistent with the results of the study by Luis et al,21 the present study documented good correlation between GLVS and LVEF, being strongest for GCS. The good intergroup and intragroup repeatability in strain values measured using 3D‐STI also is consistent with previous studies.22
Based on the present study, clinical intervention including regular 24‐hour Holter monitoring and closer follow‐up appear warranted for patients with frequent PVCs (even when <10,000/24 hours) and without accompanying structural heart diseases. However, interpretation of the findings of the present study is limited by several factors. The study had a limited sample size, which also precluded the definition of predictors of PVC‐induced cardiomyopathy and of strain value cutoffs to determine need for intervention including drug treatment or radiofrequency ablation. Longer‐term follow‐up also is warranted to verify the results of the present study and to assess cardiac function recovery of patients with frequent PVCs undergoing clinical intervention. In terms of technique‐based limitations,5, 23 because 3D‐STI technology requires high‐quality images, the acquisition and analysis of apex images sometimes is affected by the close proximity of the ultrasonic probe. Although it is a reference indicator of 3D‐STE strain parameters, no gold standard thus far has been defined to evaluate left ventricular function in 3 dimensions. Currently, 3D‐STE strain values and other parameters vary with different ultrasonic machines and software workstations used for analysis, which would affect experimental results comparisons. A larger study sample is warranted to determine the clinical reference values of indicators.
5. CONCLUSION
Patients with frequent premature ventricular complexes with normal LVEF have lower global and regional strain values than healthy controls. As a novel, feasible, and reproducible method to quantitatively assess left ventricular function, 3D‐STE could be used to assess subtle left ventricular dysfunction in patients with PVCs.
Conflicts of interest
The authors declare no potential conflicts of interest.
Acknowledgement
Thanks are due to Prof. Ge Junbo and Prof. Shu Xianhong for assistance with the experiments and to Prof. Pan Cuizhen for valuable discussion.
Supporting information
Figure S1. Global longitudinal strain rate curves and Bull's eye plot of the control (left) and PVC (right) groups. Global circumferential strain rate curves and Bull's eye plot of the control (left) and PVC (right) groups.
{kind=link}
Figure S2. Global area strain rate curves and Bull's eye plot of the controls (left) and PVC (right) groups. Global radial strain rate curves and Bull's eye plot of the control (left) and PVC (right) groups.
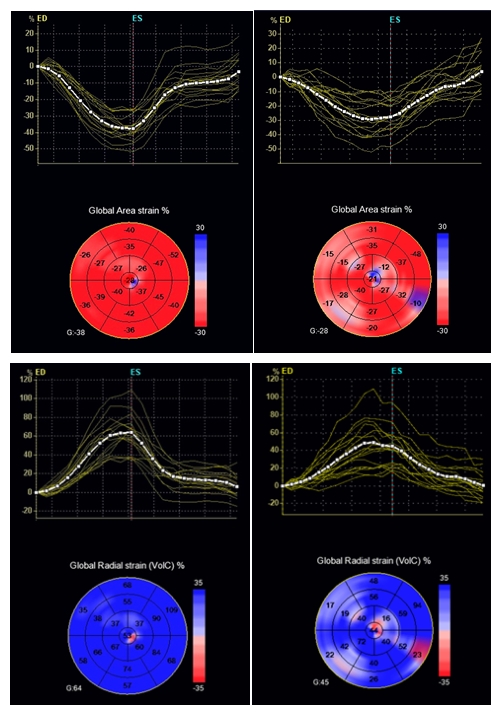{kind=link}
Ling Y, Wan Q, Chen Q and Zhu W. Assessment of subtle cardiac dysfunction in patients with frequent premature ventricular complexes by real‐time three‐dimensional speckle tracking echocardiography. Clin Cardiol. 2017;40:554–558. 10.1002/clc.22697
REFERENCES
- 1. Chugh SS, Shen WK, Luria DM, et al. First evidence of premature ventricular complex‐induced cardiomyopathy: a potentially reversible cause of heart failure. J Cardiovasc Electrophysiol. 2000;11:328–329. [DOI] [PubMed] [Google Scholar]
- 2. Kanei Y, Friedman M, Ogawa N, et al. Frequent premature ventricular complexes originating from the right ventricular outflow tract are associated with left ventricular dysfunction. Ann Noninvasive Electrocardiol. 2008;13:81–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Niwano S, Wakisaka Y, Niwano H, et al. Prognostic significance of frequent premature ventricular contractions originating from the ventricular outflow tract in patients with normal left ventricular function. Heart. 2009;95:1230–1237. [DOI] [PubMed] [Google Scholar]
- 4. Saurav A, Smer A, Abuzaid A, et al. Premature ventricular contraction‐induced cardiomyopathy. Clin Cardiol. 2015;38:251–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Urbano‐Moral JA, Patel AR, Maron MS, et al. Three‐dimensional speckle‐tracking echocardiography: methodological aspects and clinical potential. Echocardiography. 2012;29:997–1010. [DOI] [PubMed] [Google Scholar]
- 6. Blessberger H, Binder T. Two dimensional speckle tracking echocardiography: clinical applications. Heart. 2010;96:2032–2040. [DOI] [PubMed] [Google Scholar]
- 7. Szymczyk E, Lipiec P, Michalski B, et al. 2D and 3D speckle tracking echocardiography: clinical application [in Polish]. Kardiol Pol. 2013;71:77–83. [PubMed] [Google Scholar]
- 8. D'Ascenzi F, Solari M, Mazzolai M, et al. Two‐dimensional and three‐dimensional left ventricular deformation analysis: a study in competitive athletes. Int J Cardiovasc Imaging. 2016;32:1697–1705. [DOI] [PubMed] [Google Scholar]
- 9. Yarlagadda RK, Iwai S, Stein KM, et al. Reversal of cardiomyopathy in patients with repetitive monomorphic ventricular ectopy originating from the right ventricular outflow tract. Circulation. 2005;112:1092–1097. [DOI] [PubMed] [Google Scholar]
- 10. Huizar J F, Kaszala K, Potfay J, et al. Left ventricular systolic dysfunction induced by ventricular ectopy: a novel model for premature ventricular contraction‐induced cardiomyopathy. Circ Arrhythm Electrophysiol. 2011;4:543–549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Alqarawi WA, Ramirez FD, Nery PB, et al. Identifying and managing premature ventricular contraction‐induced cardiomyopathy: what, why, and how? Can J Cardiol. 2017;33:287–290. [DOI] [PubMed] [Google Scholar]
- 12. Adams JC, Srivathsan K, Shen WK. Advances in management of premature ventricular contractions. J Interv Card Electrophysiol. 2012;35:137–149. [DOI] [PubMed] [Google Scholar]
- 13. Spragg DD, Kass DA. Pathobiology of left ventricular dyssynchrony and resynchronization. Prog Cardiovasc Dis. 2006;49:26–41. [DOI] [PubMed] [Google Scholar]
- 14. Spragg DD, Akar FG, Helm RH, et al. Abnormal conduction and repolarization in late‐activated myocardium of dyssynchronously contracting hearts. Cardiovasc Res. 2005;67:77–86. [DOI] [PubMed] [Google Scholar]
- 15. Selby DE, Palmer BM, LeWinter MM, et al. Tachycardia‐induced diastolic dysfunction and resting tone in myocardium from patients with a normal ejection fraction. J Am Coll Cardiol. 2011;58:147–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Potfay J, Kaszala K, Tan AY, et al. Abnormal left ventricular mechanics of ventricular ectopic beats: insights into origin and coupling interval in premature ventricular contraction‐induced cardiomyopathy. Circ Arrhythm Electrophysiol. 2015;8:1194–1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Aliot EM, Stevenson WG, Almendral‐Garrote JM, et al. EHRA/HRS expert consensus on catheter ablation of ventricular arrhythmias: developed in a partnership with the European Heart Rhythm Association (EHRA), a Registered Branch of the European Society of Cardiology (ESC), and the Heart Rhythm Society (HRS); in collaboration with the American College of Cardiology (ACC) and the American Heart Association (AHA). Heart Rhythm. 2009;6:886–933. [DOI] [PubMed] [Google Scholar]
- 18. Baman TS, Lange DC, Ilg KJ, et al. Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm. 2010;7:865–869. [DOI] [PubMed] [Google Scholar]
- 19. Hasdemir C, Kartal Y, Simsek E, et al. Time course of recovery of left ventricular systolic dysfunction in patients with premature ventricular contraction‐induced cardiomyopathy. Pacing Clin Electrophysiol. 2013;36:612–617. [DOI] [PubMed] [Google Scholar]
- 20. Tan AY, Hu YL, Potfay J, et al. Impact of ventricular ectopic burden in a premature ventricular contraction‐induced cardiomyopathy animal model. Heart Rhythm. 2016;13:755–761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Luis SA, Yamada A, Khandheria BK, et al. Use of three‐dimensional speckle‐tracking echocardiography for quantitative assessment of global left ventricular function: a comparative study to three‐dimensional echocardiography. J Am Soc Echocardiogr. 2014;27:285–291. [DOI] [PubMed] [Google Scholar]
- 22. Bhave NM, Lang RM. Evaluation of left ventricular structure and function by three‐dimensional echocardiography. Curr Opin Crit Care. 2013;19:387–396. [DOI] [PubMed] [Google Scholar]
- 23. Gayat E, Ahmad H, Weinert L, et al. Reproducibility and inter‐vendor variability of left ventricular deformation measurements by three‐dimensional speckle‐tracking echocardiography. J Am Soc Echocardiogr. 2011;24:878–885. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Global longitudinal strain rate curves and Bull's eye plot of the control (left) and PVC (right) groups. Global circumferential strain rate curves and Bull's eye plot of the control (left) and PVC (right) groups.
Figure S2. Global area strain rate curves and Bull's eye plot of the controls (left) and PVC (right) groups. Global radial strain rate curves and Bull's eye plot of the control (left) and PVC (right) groups.