

Abstract
BACKGROUND:
Erosion is a widespread phenomenon with higher predilection in primary dentition.
AIM:
The aim of the present study is to assess the remineralising effect of Er,Cr:YSGG laser application combined with CPP-ACPF after erosive demineralisation by Coca-Cola in primary teeth.
METHODS:
Fifty teeth (n = 10) were divided into; Group I: Artificial saliva, (Saliva natural, Medac, UK), Group II: CPP-ACPF (MI Paste Plus, GC Corp, USA), Group III: Er,Cr:YSGG (Waterlase iPlus, USA), Group IV: CPP-ACPF + Er,Cr:YSGG, Group V: Er,Cr:YSGG + CPP-ACPF. Teeth were immersed in Coca-Cola for 10 min, 5 times/day for 5 days. DIAGNOdent (DD) measurements were taken before and after the experiment.
RESULTS:
There was a significant increase in DD readings after erosive-treatment cycles in all test groups. The highest reading was in samples immersed in artificial saliva, and the lowest was in those subjected to combined CPP-ACPF and Er,Cr:YSGG laser application, regardless of the sequence used. There was no significant difference between samples immersed in artificial saliva, and after CPP-ACPF application. Similarly, there was no significant difference between samples treated by combined treatment of CPP-ACPF and Er,Cr:YSGG application. However, there was a significant difference between samples immersed in artificial saliva or treated with CPP-ACPF application and those subjected to combined treatment CPP-ACPF along with Er,Cr:YSGG.
CONCLUSION:
Combining Er,Cr:YSGG laser and CPP-ACPF paste significantly increased enamel remineralisation, regardless of the sequence implemented. Saliva naturally and CPP-ACPF application had a comparable effect on remineralisation.
Keywords: Erosion; Primary teeth; DIAGNOdent; CPP-ACPF; Er,Cr:YSGG
Introduction
The two most common dental diseases are caries followed by erosion. There is strong evidence that the presence of dental erosion is widespread. Dental erosion is a surface phenomenon, defined as progressive, irreversible loss of tooth minerals caused by acid that are not produced by bacteria [1]. Primary teeth are more susceptible to erosion than permanent teeth [2]. Kazoullis et al. stated that the prevalence of erosion in the primary dentition is triple the prevalence in permanent dentition [3]. This can be explained by the thinner enamel, lower mineralisation, the inferior degree of crystalline arrangement and higher permeability of primary teeth. Hence, the erosive process appears shortly and more aggressively than in permanent teeth [2].
Epidemiological studies for dental erosion in children have reported a wide range of prevalence stretching between 0.6% to 95% [4], [5]. Such variation in epidemiological studies can be explained by the different evaluation standards used (examiner calibration and scoring systems) and the variation in population examined (sample size, age, gender and geographic location) [6]. The prevalence of erosion in primary dentition increases proportionally with children’s age. Huang et al., tracked erosion in the same group of children (2-4 years) annually. 7% had erosion detected for the first time at 3 years, while 28% at 4 years [7].
Common sites for erosion in primary teeth are the occlusal surface of molars and the palatal surfaces of maxillary incisors. A typical early sign of erosion appears as the smooth glazed surface. As the lesion progresses flattening of convexities, cupping of cusps and grooving of incisal edge occurs [2]. A meta-analysis by Li et al. concluded that erosion is strongly associated with carbonated soft drinks [8]. Moreover, advanced erosion (reaching dentin/pulp) was significantly correlated to the frequency of carbonated soft drinks consumption before bedtime and/or during the night [5].
Dental hard tissue is made up of hydroxyapatite crystals with the pure chemical formula; Ca10(PO4)6(OH)2. However, in reality, enamel is composed of a highly substituted hydroxyapatite-better described as a “calcium deficient” and “carbonated”-because some calcium ions can be substituted by sodium and some phosphate ions can be replaced by carbonates. Hence, making the tooth susceptible to dissolution. On the other hand, some hydroxyl groups can be replaced by fluoride ions to form fluoro-hydroxyapatite, Ca10(PO4)6(F)2, which has decreased susceptibility to dissolution, when compared to hydroxyapatite [2].
Demineralisation cannot be detected visually until it has progressed 200-300 μm into enamel, appearing chalky usually referred to as white spot lesions (WSL). Hence, diagnosis of early erosion may be overlooked, as it is accompanied by a few signs and fewer if any symptoms [9]. Various techniques have been utilised to evaluate dental erosion. Scanning electron microscope (SEM), atomic force microscopy and confocal laser scanning microscopy are examples of the qualitative assessment for surface topography. Generally, the problem with qualitative assessments is that the interpretation of the findings is subjective depending on the investigator evaluation. To get objective and measurable data, quantitative analyses should be implemented when possible. The most frequently adopted quantitative techniques include surface hardness and profilometry, as well as iodide permeability and chemical analysis of dissolved minerals. In addition to transverse microradiography, which is considered the gold standard for the quantification of enamel erosion. These techniques require sample preparation; therefore they are mainly used for in-vitro studies [2]. Both quantitative light-induced fluorescence (QLF) and ultrasonic measurement of enamel thickness are non-destructive and can be used in vivo [2], [10]. However, QLF correlated poorly with lesion depth, and ultrasonic measurement could not reliably detect early erosive lesion < 0.3 mm deep [10]. Moreover, the precise repositioning of the specimen for comparative readings is difficult. Also, the presence of organic pellicle may affect the accuracy of the reading [2].
Laser Fluorescence (LF), as in DIAGNOdent (DD), is the most recent technology for early diagnosis of demineralisation. It is a quantitative, non-invasive, chair side diagnostic tool that can be used both in vivo and in vitro. It can effectively monitor demineralisation, as well as, remineralisation for primary and permanent teeth [9], [11], [12]. Accordingly, DD provides a good means for patient education and motivation for treatment progress. It was explained that demineralisation stimulates more fluorescence [13]. There was a strong positive correlation between DD readings smooth-surface caries lesions in primary teeth and demineralisation depth measured by polarised light microscopy (r = 0.78) [14]. Mendes and Nicolau interpreted the best cut off reading to detect smooth surface demineralisation in primary teeth are at the value of 5. With this value; sensitivity, specificity, and accuracy were 0.78, 1, and 0.89, respectively [13].
Conventional strategies for preventing dental erosion involve restricting contact with the acidic intake. However, the success of such methods heavily relies on patient co-operation [1]. While fluoride is an effective anti-erosive agent, researches have geared towards finding a topical compound with synergistic benefits for remineralisation therapy. As a result, current recommendations for management of demineralised lesions include the use of casein containing products. MI paste plus is composed of casein phosphopeptide (CPP) that stabilises calcium and phosphate in a soluble form; known as amorphous calcium phosphate (ACP), with the addition of sodium fluoride (900 ppm) which approximates that of adult toothpaste. Calcium, phosphate and fluoride are essential remineralising components, which form highly insoluble complexes with tooth structure [9]. CPP-ACPF showed the best remineralisation potential after erosion by Coca-Cola on primary teeth when compared to CPP-ACP, fluoridated toothpaste and artificial saliva [15]. Moreover, CPP-ACPF resulted in favourable surface changes in primary teeth [11].
Ana et al., review confirmed the significant synergism of laser irradiation combined with topical remineralising agents in increasing enamel resistance to erosion [16]. A review by Ramalho et al. stated that Er,Cr:YSGG (2.78 µm) and Er:YAG (2.94 µm) lasers are most popular in dentistry. The advantage of Er,Cr:YSGG over Er:YAG was explained due to its higher absorption by hydroxyapatite, which is the main component in enamel. Because of higher absorption in water contents of enamel, Er:YAG laser causes more micro-explosions that result in an undesirable ablation [17]. Hence, Er,Cr:YSGG laser is considered to be more effective in caries prevention with lower ablation efficacy and deeper penetration [18].
In the light of the above mentioned information, the aim of the present in-vitro study was to assess the remineralizing effect of Er,Cr:YSGG laser application combined with CPP-ACPF after erosive demineralization by Coca-Cola in primary teeth.
Materials and Methods
Hundred sound primary teeth (exfoliated/extracted for orthodontic reasons) were collected from hospitals/private practices. Initially, teeth were cleaned with wet gauze to remove blood/debris. Disinfection was carried out through immersion in 5% sodium hypochlorite for 1 hour [19]. Following the guidelines for infection control, teeth being disinfected were kept in a container with a secure lid to prevent leaking and labelled with the biohazard symbol (Figure 1) [20].
Figure 1.

Disinfection of extracted teeth
Afterwards, teeth were rinsed in distilled water and air dried for 3 seconds [21]. Then, conventional visual inspection was performed under illumination and magnification lens with a blunt probe. Teeth with cracks/restoration/hypoplasia/hypomineralization were discarded [22]. Next, extracted teeth were stored collectively in a well-sealed container, frozen at -20°C until their use (1 month). A wet cotton roll was placed in each container, without contacting the teeth (Figure 2) [21]. For proper handling, extracted teeth should be maintained in a hydrated surrounding [20]. Before starting the experiment, Teeth were defrosted to room temperature over 24 hours [21].
Figure 2.
Storage of extracted teeth
DIAGNOdent readings
After defrosting, each tooth was air dried for 3 seconds [21]. Following the manufacturer’s instructions, Probe type B (for smooth surfaces) of DIAGNOdent (KaVo, Biberach, Germany) was calibrated against its ceramic reference (Figure 3).
Figure 3.

Calibration of the probe
Then, the probe was placed in light contact perpendicular to the tooth surface. The probe tip slowly scanned all four surfaces (buccal, mesial, lingual and distal) with a uniform motion for 5 sec on each surface, to ensure covering the entire area. The tip was tilted along its vertical axis to collect fluorescence from all directions to record the highest value [9]. The mean of the highest reading for each surface was recorded and used as a reference baseline for each tooth. The device was recalibrated after every 10th reading. A single, trained examiner (DE) was responsible for recording the DD values. Only teeth with readings ≤ 5 were considered intact and were included in this study (Figure 4) [13]. Hence, a total final sample size of 50 was established. Afterwards, teeth were placed in artificial saliva at an incubator at 37°C. Measurements were repeated at the end of the experiment.
Figure 4.

Baseline reading
Sample Grouping
Teeth were randomly divided into 5 groups (n = 10) using a permuted block randomisation technique and were placed in coded containers. A double-blind investigation was fulfilled since coding was strictly maintained during DD measurements and statistical evaluation. Groups were assigned to 5 different treatment modalities as follows: Group I: Artificial saliva, (Saliva natural, Medac, UK) Group II: CPP-ACPF (MI Paste Plus, GC Corp, USA), Group III: Er,Cr:YSGG (Waterlase iPlus, USA), Group IV: CPP-ACPF + Er,Cr:YSGG, and Group V: Er,Cr:YSGG + CPP-ACPF.
Erosive cycles
After grouping, teeth were immersed in 20 ml of refrigerated freshly opened Coca-Cola drink for 10 min. Then, specimens were rinsed thoroughly by distilled water, air dried with an air syringe for 3 seconds and replaced in artificial saliva at room temperature. This erosive challenge was performed 5 times/day with 3 hours interval (9 am, 12 pm, 3 pm, 6 pm and 9 pm). Those timing imitated 3 meals and in-between snacks and were repeated for 5 consecutive days. Moreover, the enamel of primary teeth becomes more susceptible to erosion at a high frequency of acid exposure (4 times/day) [2]. Coca-Cola and artificial saliva were refreshed for each cycle [19].
MI-Paste Plus application
CPP-ACPF paste was applied to teeth in groups II, IV and V. As recommended by the manufacturer, a sufficient amount of paste was smeared evenly on all tooth surfaces using a brush and left undisturbed for 5 minutes (Figure 5). Afterwards, teeth were rinsed in distilled water and replaced in artificial saliva [9]. As recommended, the paste was applied twice per day; before the first erosive challenge and after the last one.
Figure 5.

MI-Paste Plus application
Er,Cr:YSGG laser irradiation
Teeth in groups III, IV and V were irradiated with Er,Cr:YSGG under the supervision of the faculty staff at Misr International University (MIU). MGG6 Sapphire tip (diameter of 600 μm-9 mm long) was placed in the hand piece according to the manufacturer instructions. Laser tip was inspected for scratches/contamination under magnification (Viqsy x30, Japan). Wavelength-specific protective eyewear was worn by the operator (OD 5+).
The device was adjusted at the following parameters: the power of 0.75 W, the energy density of 8.5 J/cm2, energy per pulse of 12.5 mJ, the pulse width of 140 μs in (H mode), and frequency of 20 Hz without air/water cooling [23]. Teeth were removed from artificial saliva, air dried for 3 sec. And immediately radiated to avoid drying and resultant corruption of results [21]. Laser tip was kept perpendicular to the tooth surface and at a standardised distance of 1 mm. This was achieved by fixing an endodontic file with a rubber stop positioned at 1 mm to ensure a constant spot size (Figure 6).
Figure 6.

Tip was kept 1mm away
The laser was applied twice a day, before the first erosive challenge and after the last one. Each tooth surface was radiated horizontally and vertically. The handpiece was moved slowly for 10 sec in each direction to promote homogenous radiation covering the whole surface. Regular inspection to laser tip was performed every 5 teeth. The scratched tip was replaced while the contaminated tip was cleaned by cotton moistened with alcohol (Figure 7) [24].
Figure 7.

Cleaning of the contaminated tip
Statistical methodology
All data collected were tabulated and statistically compared using the SPSS software (ver. 21). Data were described using minimum-maximum, mean, standard deviation, median and inter-quartile range. Percentage change (%) was calculated as: [Measurement (after) – Measurement (before)] x 100/Measurement (before). Kolmogorov-Smirnov test (KS) of normality revealed a significance in the distribution of the variables, so the non-parametric statistics was adopted. Accordingly, box and whiskers plot was performed, and Wilcoxon Signed Ranks test was executed to compare DD readings at baseline and after the different treatment regimens. Kruskal-Wallis test was carried out to check for possible overall statistical differences between readings of the 5 subgroups. Then, Post-hoc pair-wise comparisons were carried out using Dunn-Sidak test for multiple comparisons. An alpha level was set to 5% with a significance level of 95%, and a beta error was accepted up to 20% with a power of study of 80%.
Results
The minimum-maximum DD readings, mean ± standard deviation, median and interquartile range at baseline and after treatment, as well as, the percentage change is represented in Table 1. Percentage change was calculated to evaluate the change in DD readings over time for better comparison.
Table 1.
DIAGNOdent readings at baseline, after treatment and percentage change
| Groups | Test of significance p (value) | |||||
|---|---|---|---|---|---|---|
| Arificial Saliva (n = 10) | CPP- ACPF (n = 10) | Er,Cr: YSGG (n = 10) | CPP-ACPF + Er,Cr:YSGG (n = 10) | Er,Cr:YSGG + CPP-ACPF (n = 10) | ||
| Baseline | X2 (df=4)(KW) = 0.2 P = 1.00 | |||||
| Min-Max | 2-5 | 1-5 | 3-5 | 1-5 | 1-5 | |
| Mean ± SD | 3.8 ± 1.0 | 3.6 ± 1.6 | 3.9 ± 0.9 | 3.6 ± 1.2 | 3.7 ± 1.3 | |
| Median | 4 | 4 | 4 | 4 | 4 | |
| IQR | 3-5 | 3-5 | 3-5 | 3-4 | 3-5 | |
| KS | D = 0.18, p = 0.20 | D = 0.21, p = 0.20 | D = 0.25, p = 0.08 | D = 0.23, p = 0.13 | D = 0.20, p = 0.20 | |
| After treatment | X2 (df = 4)(KW) = 40.9 P = 0.00 * | |||||
| Min-Max | 13-23 | 9-15 | 8-14 | 5-8 | 3-9 | |
| Mean ± SD | 18.0 ± 3.6 | 12.6 ± 2.0 | 11.4 ± 1.8 | 6.6 ± 1.2 | 6.4 ± 1.8 | |
| Median | 17.5a, b, c | 13.0a, b, c | 11.5a, b, c, d, e | 6.5c, d, e | 6.5c, d, e | |
| IQR | 15-21 | 11-14 | 10-13 | 6-8 | 5-8 | |
| KS | D = 0.20, p = 0.20 | D = 0.28, p = 0.02* | D = 0.13, p = 0.20 | D = 0.20, p = 0.20 | D = 0.13, p = 0.20 | |
| Percentage change | X2(df = 4)(KW) = 30.0 P = 0.00 * | |||||
| Min-Max | 225-667 | 120-1200 | 100-300 | 50-400 | 50-200 | |
| Mean ± SD | 409.2 ± 176.9 | 376.0 ± 351.1 | 202.2 ± 64.8 | 110.3 ± 107.5 | 83.3 ± 43.2 | |
| Median | 330.0a, b, c | 225.0a, b, c | 212.5a, b, c, d, e | 70.8c, d, e | 70.8c, d, e | |
| IQR | 250-600 | 160-367 | 160-250 | 60-100 | 60-80 | |
| KS | D = 0.25, p = 0.07 | D = 0.31, p = 0.00* | D = 0.14, p = 0.20 | D = 0.34, p = 0.00* | D = 0.33, p = 0.00* | |
| Test of significance p (value) | Z(WSR) = 2.8 P = 0.005* | Z(WSR) = 2.8 P = 0.005* | Z(WSR) = 2.8 P = 0.005* | Z(WSR) = 2.8 P = 0.004* | Z(WSR) = 2.9 P = 0.004* | # Z(WSR) = 6.2 P = 0.00 * |
KS: Kolmogorov-Smirnov test; WSR: Wilcoxon Signed Ranks test; KW: Kruskal-Wallis test;
: Statistically significant (p < 0.05);
: Paired sample test for all samples (n = 50); Different superscript letters indicate significant pair-wise comparison.
KS test of normality showed significance in DD readings after treatment with CPP-ACPF (p = 0.02) and in values of percentage change after treatment with CPP-ACPF, applied alone and in combination with Er,Cr:YSGG (p = 0.00). This indicates that DD readings are not normally distributed and there is distortion in mean values. Therefore, it was recommended to use the median as a representative value for the study sample, as well as non-parametric tests for comparisons. Accordingly, box and whiskers graph was plotted to describe data distribution (Figure 8).
Figure 8.
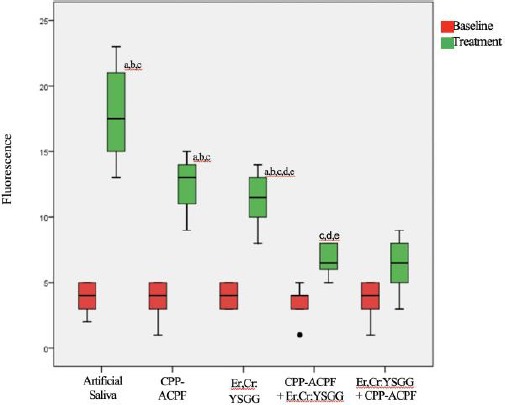
Box and whisker plot; (Different superscript letters indicate significant pair-wise comparison)
At baseline, there was no significant difference in DD readings between all test groups (p = 1.00), as sample size compromised only of teeth with readings ≤ 5. There was a significant difference in DD readings between baseline and after erosive-treatment cycles in each group (p = 0.004 and p = 0.005) and collectively (p = 0.00).
There was an increase in DD readings after erosive-treatment cycles in all test groups. The highest reading was in samples immersed in artificial saliva (Median = 17.5), and the lowest was in those subjected to combined CPP-ACPF and Er,Cr:YSGG laser application, regardless the sequence used (Median = 6.5). Similar to the percentage change values, the highest median was for samples immersed in artificial saliva (330%), while the lowest median was for samples with combined CPP-ACPF and Er,Cr:YSGG laser treatment, regardless the sequence used (70.8%).
There was a significant difference in DD readings, as well as, percentage change between groups after erosive-treatment cycles (p = 0.00). Pair-wise comparisons revealed that there was no significant difference between samples immersed in artificial saliva and after CPP-ACPF or Er,Cr:YSGG application.
Table 2.
After treatment
| Sample 1 — Sample 2 | Test Statistics | Std. Error | Std. Test Statistics | Sig. | Adj. Sig. |
|---|---|---|---|---|---|
| Er,Cr:YSGG + CPP-ACPF — CPP-ACPF + Er,Cr:YSGG | 0.300 | 6.497 | 0.046 | 0.963 | 1.000 |
| Er,Cr:YSGG + CPP-ACPF — Er,Cr:YSGG | 17.900 | 6.497 | 2.755 | 0.006 | 0.059 |
| Er,Cr:YSGG + CPP-ACPF — CPP-ACPF | 22.700 | 6.497 | 3.494 | 0.000 | 0.005 |
| Er,Cr:YSGG + CPP-ACPF — Artificial Saliva | 33.850 | 6.497 | 5.210 | 0.000 | 0.000 |
| CPP-ACPF + Er,Cr:YSGG — Er,Cr:YSGG | 17.600 | 6.497 | 2.709 | 0.007 | 0.067 |
| CPP-ACPF + Er,Cr:YSGG — CPP-ACPF | 22.400 | 6.497 | 3.448 | 0.001 | 0.006 |
| CPP-ACPF + Er,Cr:YSGG — Artificial Saliva | 33.550 | 6.497 | 5.164 | 0.000 | 0.000 |
| Er,Cr:YSGG — CPP-ACPF | 4.800 | 6.497 | 0.739 | 0.460 | 1.000 |
| Er,Cr:YSGG — Artificial Saliva | 15.950 | 6.497 | 2.455 | 0.014 | 0.141 |
| CPP-ACPF — Artificial Saliva | 11.150 | 6.497 | 1.716 | 0.086 | 0.861 |
Similarly, there was no significant difference between samples treated by Er,Cr:YSGG used alone or combined with CPP-ACPF. However, there was a significant difference between samples immersed in artificial saliva or treated with CPP-ACPF application and those subjected to combined treatment CPP-ACPF along with Er,Cr:YSGG (Figure 9).
Figure 9.
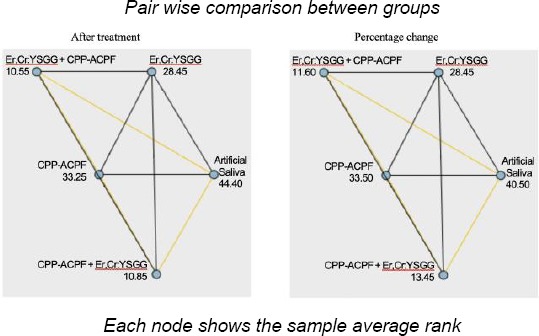
Multiple comparisons of Dunn orders
Table 3.
Percentage change
| Sample 1 — Sample 2 | Test Statistics | Std. Error | Std. Test Statistics | Sig. | Adj. Sig. |
|---|---|---|---|---|---|
| Er,Cr:YSGG + CPP-ACPF — CPP-ACPF + Er,Cr:YSGG | 1.850 | 6.512 | 0.284 | 0.776 | 1.000 |
| Er,Cr:YSGG + CPP-ACPF — Er,Cr:YSGG | 16.850 | 6.512 | 2.587 | 0.010 | 0.097 |
| Er,Cr:YSGG + CPP-ACPF — CPP-ACPF | 21.900 | 6.512 | 3.363 | 0.001 | 0.008 |
| Er,Cr:YSGG + CPP-ACPF — Artificial Saliva | 28.900 | 6.512 | 4.438 | 0.000 | 0.000 |
| CPP-ACPF + Er,Cr:YSGG — Er,Cr:YSGG | 15.000 | 6.512 | 2.303 | 0.021 | 0.213 |
| CPP-ACPF + Er,Cr:YSGG — CPP-ACPF | 20.050 | 6.512 | 3.079 | 0.002 | 0.021 |
| CPP-ACPF + Er,Cr:YSGG — Artificial Saliva | 27.050 | 6.512 | 4.154 | 0.000 | 0.000 |
| Er,Cr:YSGG — CPP-ACPF | 5.050 | 6.512 | 0.775 | 0.438 | 1.000 |
| Er,Cr:YSGG — Artificial Saliva | 12.050 | 6.512 | 1.850 | 0.064 | 0.643 |
| CPP-ACPF — Artificial Saliva | 7.000 | 6.512 | 1.075 | 0.282 | 1.000 |
Each row tests the null hypothesis that the Sample 1 and Sample 2 distributions are the same; Asymptomatic significance (2-sided tests) are displayed. The significance level is 0.05.
Discussion
Both caries and erosion arise due to acidic attack on enamel — caries results from bacterial acids with a predilection for sites of plaque accumulation and fissures. In contrast, erosive lesions are caused by the acid of non-bacterial origin repeatedly ‘washing’ the enamel surface; at sites free of plaque [1].
A literature review by Taji and Seow added the incisal surface of maxillary teeth as a common site of erosion [1]. Similar to previous studies, the incisal/occlusal surface was not included in any intervention/measurement to avoid the confusion between attrition and erosion especially during the mixed dentition stage. The strong correlation between the prevalence of erosion and the frequent consumption of soft drinks at bedtime can be justified by the low salivary flow and the lack of remineralising factors such as brushing with fluoride toothpaste [5], [6].
Many studies revealed that DD has good reproducibility with a high degree of sensitivity and specificity in smooth surface lesions in primary teeth [13], [14]. Virajsilp et al., compared DD with bitewing in proximal caries diagnosis for primary teeth using the histological examination as a gold standard. The study revealed a stronger correlation between histological findings and DD reading (r = 0.85) than that with bitewing (r = 0.79). The sensitivity and specificity for DD in initial lesions were 0.75 and 0.89 respectively, compared to 0.69 and 0.55 for bitewing evaluation. Moreover, both inter- and intraexaminer reliabilities using DD were very high (0.97 and 0.99 respectively), indicating high reproducibility [25].
On the contrary, Mepparambath et al. compared the accuracy of DD to bitewing radiography in detecting proximal caries in primary teeth in-vivo. It was concluded that DD is not good at detecting initial enamel lesions in the proximal surface of primary teeth with low sensitivity (0.39). This controversy can be explained by the higher cut off limits for DD followed by Mepparambath et al. besides, DD was not compared to histological gold standard [12].
In the present study, primary teeth from children aged 6-13 years were collected from the public as well as private centres to include different genetic and socioeconomic variations. Unlike previous researches, primary teeth used in this study were not sectioned [19], [26]. Similar to Subramaniam and Pandey, primary teeth were used as a whole to avoid exerting mechanical stress on the tooth which may affect DD readings and to allow scanning of all axial surfaces for more accurate measurements [22].
Collected teeth were cleaned with wet gauze only, and rotating brush polishing was avoided in order not to interfere with DD readings [27]. Storing teeth frozen at -20°C was favoured over other commonly used mediums (formalin-thymol, chlorhexidine-sodium hypochlorite-salivary substitute-saline), as it does not significantly change the fluorescence readings [28].
A review by Western and Dicksit concluded that autoclaving, and formalin could be efficiently used for sterilisation of extracted teeth. Their use was discouraged, as autoclaving disrupts organic matrix of the tooth and formalin possess a major health hazard as a potential carcinogen [29]. The authors of the current study aimed for intermediate disinfection time, as performed by a previously [19]. This predilection was to avoid any possible change in LF readings, as well as any likely alteration in mechanical properties [28]. Besides, the authors view complete sterilisation to be only critical in the case of microbial studies, and that handling disinfected teeth with proper personal protective attire fulfils adequate infection control measures.
Thymol was also used to disinfect primary teeth in previous researches studying laser assisted remineralisation [22]. However, the authors of this study preferred the use of sodium hypochlorite due to its superior efficacy [29]. Teeth were air dried for only 3 sec before DD measurements as prolonged drying increases the fluorescence readings [21]. In this present study, the authors preferred to use a refrigerated beverage to mimic a real-life situation. The current study used artificial saliva at 37°C as a storage medium to simulate the oral environment.
For caries preventive treatment, laser irradiation is not intended to ablate the surface but only change the morphological/chemical composition of enamel instead. The authors of the current study deliberately avoided using air/water cooling with the subablative laser parameters by previous studies [23], [24]. This is explained in reviews by Ana et al., and Ramalho et al., through the strong absorption of Erbium lasers in water. Laser energy is rapidly and efficiently converted into thermal energy in water particles-either contained in enamel or existing freely at the surface – resulting in abrupt vaporisation of water droplets and the removal of hard tissue. This thermal ablation is recognised to be hydrokinetic explosive mechanism meaning that it is water-mediated rather than by direct vaporisation of hydroxyl apatite crystals itself [16], [17].
However, other studies implemented the air/water cooling parameters to avoid the excessive increase of temperature beyond the ablation threshold or causing pulpal damage [22], [26]. Previous studies measured the temperature after Er,Cr:YSGG application under the same parameters without air/water mist at the enamel surface (212 ± 23°C) and in the pulp (2.1°C) [30], [31]. While other studies reported the ablation temperature for enamel is at 600 ± 50°C and that a temperature rises above 5.5°C in the pulp is a potential for loss of vitality [18], [32]. Therefore, the parameters used in the present study permit safe temperature rise for surface changes without causing pulpal trauma.
Studies investigating the simultaneous application of fluoride and laser to enhance acid resistance on primary teeth are scarce. Subramaniam and Pandey studied the cumulative effect of Er,Cr:YSGG laser (4W) and CPP-ACP, while Molaasadollah et al., (0.5W) observed its conjunction with APF [22], [26]. In the present study, the DD readings at baseline are by Kamath et al., [11].
The current study concluded that combining Er,Cr:YSGG irradiation with CPP-ACPF application significantly increased enamel remineralisation of primary teeth - regardless the sequence of application used.- when compared to either CPP-ACPF or artificial saliva used alone. It is difficult to compare the results of the present study because none of the previously mentioned investigations used DD as a method of evaluation. However, the results of this present study are in agreement with previous studies. It was concluded that combining Er,Cr:YSGG and APF-regardless the sequence of application used – significantly reduced the amount calcium ion lost significantly increased calcium fluoride retained after demineralisation, when compared to APF used alone. These researches used untreated enamel surface as the control group, unlike the current study, in which artificial saliva was adopted to simulate oral condition [33], [34].
Comparing with previous studies evaluating Er,Cr:YSGG assisted fluoride treatment on acid resistance in primary teeth, the findings of this study is in accordance to Subramaniam and Pandey-despite the different laser parameters used-who concluded that repeated Er,Cr:YSGG irradiation followed by CPP-ACP application significantly increased surface hardness of primary enamel more than CPP-ACP applied alone [22]. However, the findings of this study oppose to Molaasadollah et al., in which irradiation by Er,Cr:YSGG laser followed by the APF application was comparable to applying APF alone in reducing the area of WSL in primary teeth measured under a stereomicroscope. This disagreement can be attributed to the different laser parameters/material used, a single application of surface treatment, a different method of assessment [26].
The results of this study showed that the application of CPP-ACPF were comparable to immersion in artificial saliva, this is in accordance to previous studies [35], [37]. Gade justified this finding to be due to the short duration of the investigation (7 days), the absence of biofilm that enhances the adherence of CPP-ACPF and the lack of frequent demineralization that activates the CPP-ACPF [35]. However, other studies found no statistical difference under pH cycling for 30 days and after incubation with Streptococcus mutans for biofilm formation [36], [37].
The authors of the current study further suggest that the insignificant difference between artificial saliva and CPP-ACPF may attributed to the presence of xylitol in the composition of Saliva natura. This explanation is supported by Chunmuang et al., who explained that xylitol is able to form complexes with calcium ions, which results in its strong remineralizing potential [38]. The authors of this study preferred using the commercially available salivary substitute (Saliva natura) over a laboratory prepared artificial saliva due to the lack of calcium and phosphate in its composition when compared to previous studies [9], [11], [36]. The authors of the present study suggest that the insignificant difference between the Er,Cr:YSGG and all the other groups can be overcomed by increasing the sample size.
CO2 laser has higher absorption coefficient by hydroxyapatite crystals than Er,Cr:YSGG [16]. Anaraki et al., and Kaur et al. compared acid resistance of both lasers. CO2 laser had significantly higher surface hardness than Er,Cr:YSGG and showed significantly the least calcium ions released after demineralization. However, SEM analysis of enamel surface radiated with CO2 laser appeared rough and cracked, which might act as retentive areas for plaque. In contrast to Er,Cr:YSGG group which revealed a smooth and glossy surface devoid of any cracks, making enamel impervious to acidic dissolution [39], [40].
More in-vivo/in-vitro studies with larger sample size need to be carried out to specify Er,Cr:YSGG parameters giving the best results under various methods of assessment and to identify the sequence/method of the combined fluoride application i.e. laser should be applied before, after or through fluoride treatment. Long term studies are needed to assess the efficiency of single verses multiple application of surface treatment. Further investigations are essential to compare the effectiveness of Er,Cr:YSGG and CO2 laser to preventing demineralisation.
Based on the findings of this study and within its limitations, the current study concluded the following:
1) Combining Er,Cr:YSGG laser and CPP-ACPF paste significantly increased enamel remineralisation
2) Er,Cr:YSGG laser irradiation either before or after CPP-ACPF application did not affect remineralisation.
3) Saliva naturally and CPP-ACPF application had a comparable effect on remineralisation.
4) The effect of Er,Cr:YSGG laser application on remineralisation was similar to all other treatment options.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Taji S, Seow WK. A literature review of dental erosion in children. Aust Dent J. 2010;c55(4):358–67. doi: 10.1111/j.1834-7819.2010.01255.x. [DOI] [PubMed] [Google Scholar]
- 2.Lussi A. Dental erosion:from diagnosis to therapy. Karger. 2006 https://doi.org/10.1159/isbn.978-3-318-01331-3 PMCid:PMC2063555. [Google Scholar]
- 3.Kazoullis S, Seow WK, Holcombe T, Newman B, Ford D. Common dental conditions associated with dental erosion in school children in Australia. Pediatr Dent. 2007;29(1):33–9. PMid:18041510. [PubMed] [Google Scholar]
- 4.Moimaz SA, Araújo PC, Chiba FY, Garbín CA, Saliba NA. Prevalence of deciduous tooth erosion in childhood. Int J Dent Hyg. 2013;11(3):226–30. doi: 10.1111/idh.12020. https://doi.org/10.1111/idh.12020 PMid:23506560. [DOI] [PubMed] [Google Scholar]
- 5.Al-Majed I, Maguire A, Murray JJ. Risk factors for dental erosion in 5-6 year old and 12-14 year old boys in Saudi Arabia. Community Dent Oral Epidemiol. 2002;30(1):38–46. doi: 10.1034/j.1600-0528.2002.300106.x. https://doi.org/10.1034/j.1600-0528.2002.300106.x PMid:11918574. [DOI] [PubMed] [Google Scholar]
- 6.Habib M, Hottel TL, Hong L. Prevalence and risk factors of dental erosion in American children. J Clin Pediatr Dent. 2013;38(2):143–8. doi: 10.17796/jcpd.38.2.4300111x4321l313. https://doi.org/10.17796/jcpd.38.2.4300111x4321l313 PMid:24683778. [DOI] [PubMed] [Google Scholar]
- 7.Huang LL, Leishman S, Newman B, Seow WK. Association of erosion with timing of detection and selected risk factors in primary dentition:a longitudinal study. Int J Paediatr Dent. 2015;25(3):165–73. doi: 10.1111/ipd.12109. https://doi.org/10.1111/ipd.12109 PMid:24766533. [DOI] [PubMed] [Google Scholar]
- 8.Li H, Zou Y, Ding G. Dietary factors associated with dental erosion:a meta-analysis. PLoS One. 2012;7(8):e42626. doi: 10.1371/journal.pone.0042626. https://doi.org/10.1371/journal.pone.0042626 PMid:22952601 PMCid:PMC3432030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jayarajan J, Janardhanam P, Jayakumar P, Deepika Efficacy of CPP-ACP and CPP-ACPF on enamel remineralization - An in vitro study using scanning electron microscope and DIAGNOdent®. Indian J Dent Res. 2011;22(1):77–82. doi: 10.4103/0970-9290.80001. https://doi.org/10.4103/0970-9290.80001 PMid:21525682. [DOI] [PubMed] [Google Scholar]
- 10.Louwerse C, Kjaeldgaard M, Huysmans MC. The reproducibility of ultrasonic enamel thickness measurements:an in vitro study. J Dent. 2004;32(1):83–9. doi: 10.1016/j.jdent.2003.08.007. https://doi.org/10.1016/j.jdent.2003.08.007 PMid:14659722. [DOI] [PubMed] [Google Scholar]
- 11.Kamath P, Nayak R, Kamath SU, Pai D. A comparative evaluation of the remineralization potential of three commercially available remineralizing agents on white spot lesions in primary teeth:An in vitro study. J Indian Soc Pedod Prev Dent. 2017;35(3):229–37. doi: 10.4103/JISPPD.JISPPD_242_16. https://doi.org/10.4103/JISPPD.JISPPD_242_16 PMid:28762349. [DOI] [PubMed] [Google Scholar]
- 12.Mepparambath R, S Bhat S, K Hegde S, Anjana G, Sunil M, Mathew S. Comparison of proximal caries detection in primary teeth between laser fluorescence and bitewing radiography:An in vivo study. Int J Clin Pediatr Dent. 2014;7(3):163–7. doi: 10.5005/jp-journals-10005-1257. https://doi.org/10.5005/jp-journals-10005-1257 PMid:25709294 PMCid:PMC4335105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mendes FM, Nicolau J. Utilization of laser fluorescence to monitor caries lesions development in primary teeth. J Dent Child (Chic) 2004;71(2):139–42. [PubMed] [Google Scholar]
- 14.Mendes FM, Siqueira WL, Mazzitelli JF, Pinheiro SL, Bengtson AL. Performance of DIAGNOdent for detection and quantification of smooth-surface caries in primary teeth. J Dent. 2005;33(1):79–84. doi: 10.1016/j.jdent.2004.10.010. https://doi.org/10.1016/j.jdent.2004.10.010 PMid:15652172. [DOI] [PubMed] [Google Scholar]
- 15.Rallan M, Chaudhary S, Goswami M, Sinha A, Arora R, Kishor A. Effect of various remineralising agents on human eroded enamel of primary teeth. Eur Arch Paediatr Dent. 2013;14(5):313–8. doi: 10.1007/s40368-013-0085-9. https://doi.org/10.1007/s40368-013-0085-9 PMid:24068490. [DOI] [PubMed] [Google Scholar]
- 16.Ana PA, Bachmann L, Zezell DM. Lasers effects on enamel for caries prevention. Laser Phys. 2006;16(5):865–75. https://doi.org/10.1134/S1054660X06050197. [Google Scholar]
- 17.Ramalho KM, Hsu CY, De Freitas PM, Aranha AC, Esteves-Oliveira M, Rocha RG, de Paula Eduardo C. Erbium lasers for the prevention of enamel and dentin demineralization:A literature review. Photomed Laser Surg. 2015;33(6):301–19. doi: 10.1089/pho.2014.3874. https://doi.org/10.1089/pho.2014.3874 PMid:26067939. [DOI] [PubMed] [Google Scholar]
- 18.Perhavec T, Diaci J. Comparison of heat deposition of Er:YAG and Er,Cr:YSGG lasers in hard dental tissues. J Laser Health Acad. 2009;2:1–6. [Google Scholar]
- 19.Agrawal N, Shashikiran ND, Singla S, Ravi KS, Kulkarni VK. Atomic force microscopic comparison of remineralization with casein-phosphopeptide amorphous calcium phosphate paste, acidulated phosphate fluoride gel and iron supplement in primary and permanent teeth:An in-vitro study. Contemp Clin Dent. 2014;5(1):75–80. doi: 10.4103/0976-237X.128672. https://doi.org/10.4103/0976-237X.128672 PMid:24808700 PMCid:PMC4012123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kohn WG, Harte JA, Malvitz DM, Collins AS, Cleveland JL, Eklund KJ. Guidelines for infection control in dental health care settings-2003. J Am Dent Assoc. 2004;135(1):33–47. doi: 10.14219/jada.archive.2004.0019. https://doi.org/10.14219/jada.archive.2004.0019 PMid:14959873. [DOI] [PubMed] [Google Scholar]
- 21.De Benedetto MS, Morais CC, Novaes TF, De Almeida Rodrigues J, Braga MM, Mendes FM. Comparing the reliability of a new fluorescence camera with conventional laser fluorescence devices in detecting caries lesions in occlusal and smooth surfaces of primary teeth. Lasers Med Sci. 2011;26(2):157–62. doi: 10.1007/s10103-010-0757-1. https://doi.org/10.1007/s10103-010-0757-1 PMid:20157753. [DOI] [PubMed] [Google Scholar]
- 22.Subramaniam P, Pandey A. Effect of erbium, chromium:yttrium, scandium, gallium, garnet laser and casein phosphopeptide-amorphous calcium phosphate on surface micro-hardness of primary tooth enamel. Eur J Dent. 2014;8(3):402–6. doi: 10.4103/1305-7456.137656. https://doi.org/10.4103/1305-7456.137656 PMid:25202223 PMCid:PMC4144141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ana PA, Tabchoury CP, Cury JA, Zezell DM. Effect of Er,Cr:YSGG laser and professional fluoride application on enamel demineralization and on fluoride retention. Caries Res. 2012;46(5):441–51. doi: 10.1159/000333603. https://doi.org/10.1159/000333603 PMid:22739669. [DOI] [PubMed] [Google Scholar]
- 24.De Freitas PM, Rapozo-Hilo M, Eduardo Cde P, Featherstone JD. In vitro evaluation of erbium, chromium:yttrium-scandium-gallium-garnet laser-treated enamel demineralization. Lasers Med Sci. 2010;25(2):165–70. doi: 10.1007/s10103-008-0597-4. https://doi.org/10.1007/s10103-008-0597-4 PMid:18787759. [DOI] [PubMed] [Google Scholar]
- 25.Virajsilp V, Thearmontree A, Aryatawong S, Paiboonwarachat D. Comparison of proximal caries detection in primary teeth between laser fluorescence and bitewing radiography. Pediatr Dent. 2005;27(6):493–9. PMid:16532891. [PubMed] [Google Scholar]
- 26.Molaasadollah F, Asnaashari M, Mashhadi Abbas F, Jafary M. In vitro comparison of fluoride gel alone and in combination with Er,Cr:YSGG laser on reducing white spot lesions in primary teeth. J Lasers Med Sci. 2017;8(4):160–5. doi: 10.15171/jlms.2017.29. https://doi.org/10.15171/jlms.2017.29 PMid:29071020 PMCid:PMC5642162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lussi A, Reich E. The influence of toothpastes and prophylaxis pastes on fluorescence measurements for caries detection in vitro. Eur J Oral Sci. 2005;113(2):141–4. doi: 10.1111/j.1600-0722.2004.00195.x. https://doi.org/10.1111/j.1600-0722.2004.00195.x PMid:15819820. [DOI] [PubMed] [Google Scholar]
- 28.Kaul R, Kaul V, Farooq R, Wazir ND, Khateeb SU, Malik AH, Masoodi AA. Cut off values of laser fluorescence for different storage methods at different time intervals in comparison to frozen condition:A 1 year in vitro study. J Conserv Dent. 2014;17(2):124–8. doi: 10.4103/0972-0707.128043. https://doi.org/10.4103/0972-0707.128043 PMid:24778506 PMCid:PMC4001266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Western JS, Dicksit DD. A systematic review of randomized controlled trials on sterilization methods of extracted teeth. J Conserv Dent. 2016;19(4):343–6. doi: 10.4103/0972-0707.186457. https://doi.org/10.4103/0972-0707.186457 PMid:27563183 PMCid:PMC4979281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ana PA, Blay A, Miyakawa W, Zezell DM. Thermal analysis of teeth irradiated with Er,Cr:YSGG at low fluences. Laser Phys Lett. 2007;4(11):827–34. https://doi.org/10.1002/lapl.200710060. [Google Scholar]
- 31.Ana PA, Velloso WF, Jr, Zezell DM. Three-dimensional finite element thermal analysis of dental tissues irradiated with Er,Cr:YSGG laser. Rev Sci Instrum. 2008;79(9):093910. doi: 10.1063/1.2953526. https://doi.org/10.1063/1.2953526 PMid:19044431. [DOI] [PubMed] [Google Scholar]
- 32.Zach L, Cohen G. Pulp response to externally applied heat. 1965; 19:515–30. doi: 10.1016/0030-4220(65)90015-0. [DOI] [PubMed] [Google Scholar]
- 33.Moslemi M, Fekrazad R, Tadayon N, Ghorbani M, Torabzadeh H, Shadkar MM. Effects of Er,Cr:YSGG laser irradiation and fluoride treatment on acid resistance of the enamel. Pediatr Dent. 2009;31(5):409–13. PMid:19947136. [PubMed] [Google Scholar]
- 34.Zezell DM, Ana PA, Benetti C, Goulart VP, Bachmann L, Tabchoury CPM, Cury JA. Compositional and crystallographic changes on enamel when irradiated by Nd:YAG or Er,Cr:YSGG lasers and its resistance to demineralization when associated with fluoride. In: Rechmann P, Fried D, editors. Lasers in Dentistry. 16th ed. Proc SPIE; 2010. pp. 1–12. https://doi.org/10.1117/12.842967. [Google Scholar]
- 35.Gade V. Comparative evaluation of remineralization efficacy of GC tooth mousse plus and enafix on artificially demineralized enamel surface:An in vitro study. Indian J Oral Health Res. 2016;2(2):67–71. https://doi.org/10.4103/2393-8692.196097. [Google Scholar]
- 36.Oliveira GM, Ritter AV, Heymann HO, Swift E, Jr, Donovan T, Brock G, Wright T. Remineralization effect of CPP-ACP and fluoride for white spot lesions in vitro. J Dent. 2014;42(12):1592–602. doi: 10.1016/j.jdent.2014.09.004. https://doi.org/10.1016/j.jdent.2014.09.004 PMid:25260438 PMCid:PMC5551488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Oliveira PR, Coutinho TC, Portela MB, Paula VC, Tostes MA. Influence of biofilm formation on the mechanical properties of enamel after treatment with CPP-ACP crème. Braz Oral Res. 2017;31:e84. doi: 10.1590/1807-3107BOR-2017.vol31.0084. https://doi.org/10.1590/1807-3107bor-2017.vol31.0084 PMid:29185603. [DOI] [PubMed] [Google Scholar]
- 38.Chunmuang S, Jitpukdeebodintra S, Chuenarrom C, Benjakul P. Effect of xylitol and fluoride on enamel erosion in vitro. J Oral Sci. 2007;49(4):293–7. doi: 10.2334/josnusd.49.293. https://doi.org/10.2334/josnusd.49.293 PMid:18195513. [DOI] [PubMed] [Google Scholar]
- 39.Anaraki SN, Serajzadeh M, Fekrazad R. Effects of laser-assisted fluoride therapy with a CO2 laser and Er,Cr:YSGG laser on enamel demineralization. 2012;34(4):92–6. [PubMed] [Google Scholar]
- 40.Kaur T, Tripathi T, Rai P, Kanase A. SEM evaluation of enamel surface changes and enamel microhardness around orthodontic brackets after application of CO2 laser, Er,Cr:YSGG laser and fluoride varnish:An in-vivo study. J Clin Diagn Res. 2017;11(9):59–63. doi: 10.7860/JCDR/2017/30292.10603. https://doi.org/10.7860/JCDR/2017/30292.10603. [DOI] [PMC free article] [PubMed] [Google Scholar]