

Abstract
Background
Despite the progress made to decrease risk factors for cardiovascular diseases, disparities still exist. We examined how education and ethnicity interact to determine disparities in cardiovascular health (CVH) as defined by the American Heart Association.
Hypothesis
Education modifies the effect of ethnicity on CVH.
Methods
Individual CVH metrics (smoking, physical activity, body mass index, diet, total cholesterol, blood pressure, and blood glucose) were defined as ideal, intermediate, or poor. Combined scores were categorized as inadequate, average, or optimal CVH. Education was categorized as postgraduate, college, some college, and high school or less; ethnicity was categorized as white, Hispanic, black, and other. Main and interactive associations between education, ethnicity, and the measures of CVH were calculated with multinomial logistic regression.
Results
Of 9056 study participants, 74% were women, and mean age was 43 (±12) years. Over half were Hispanic, and two‐thirds had at least a college education. With postgraduate education category as the reference, participants with less than a college education were less likely to achieve ideal status for most of the individual CVH metrics, and also less likely to achieve 6 to 7 ideal metrics, and optimal CVH scores. In most of the educational categories, Hispanic participants had the highest proportion with optimal CVH scores and 6 to 7 ideal metrics, whereas black participants had the lowest proportion. However, there were no statistically significant interactions of education and ethnicity for ideal CVH measures.
Conclusions
Higher educational attainment had variable associations with achieved levels of ideal CVH across race/ethnic groups. Interventions to improve CVH should be tailored to meet the needs of target communities.
Keywords: Cardiovascular, Epidemiology, Preventive Cardiology, Socioeconomic Aspects, Ideal Cardiovascular Health Metrics, Life's Simple 7
1. INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of death globally, responsible for about one‐third of all deaths.1 In the United States, an estimated 85.6 million adults have at least 1 type of CVD, with approximately $316.6 billion spent annually in direct and indirect costs.2 Despite the progress made in the United States over the last 3 decades in decreasing the risk factors of CVD along with the morbidity and mortality associated with the established disease,3, 4, 5, 6, 7 disparities still exist.8 For example, African Americans have a higher prevalence of CVD risk factors such as hypertension and obesity compared to whites.9, 10 The disparities between race/ethnic groups have been explained in part by differences in socioeconomic factors such as education and income.11, 12, 13, 14, 15, 16
Nevertheless, few studies17, 18 have investigated the effect modifications of these socioeconomic factors on race/ethnicity in the expression of the new construct of “ideal cardiovascular health” introduced in 2010 by the American Heart Association (AHA) to monitor, assess, and promote cardiovascular health (CVH) and wellness.19 Ideal CVH is defined as “the presence of both ideal health behaviors (nonsmoking, body mass index [BMI] <25 kg/m2, physical activity at goal levels, and pursuit of a diet consistent with current guideline recommendations) and ideal health factors (untreated total cholesterol <200 mg/dL, untreated blood pressure <120/<80 mm Hg, and fasting blood glucose <100 mg/dL).” 19
Using data from the Baptist Health South Florida (BHSF) Employee Study, a cross‐sectional study of employees of a large not‐for‐profit healthcare organization, we examined how education and ethnicity interact to determine disparities in CVH. We tested the following hypotheses: 1 Education will modify the effect of ethnicity on CVH.2 Higher educational attainment is associated with improved CVH.
2. METHODS
2.1. Study population
The methodology of this study has been previously described.20, 21 Briefly, we examined data from the 2014 wellness fair and Health Risk Assessment (HRA) at BHSF, a healthcare organization with the largest employee population in South Miami, Florida. The wellness fair and HRA are a part of an incentive‐driven wellness program. To be eligible for incentives, employees must be enrolled and contribute toward a BHSF medical plan. For every criteria met (nonsmoking, BMI <25 mg/m2, blood pressure <140/90 mm Hg, total cholesterol <240 mg/dL, and blood glucose ≤140 mg/dL), a $50 reimbursement was given to each employee. For this study, 9056 employees were included in the analyses after exclusion of those without complete data on the CVH health metrics. Participation rate was estimated at 60% from over 15,000 employees who were eligible to participate in the 2014 HRA. As part of the HRA, employees were required to complete an online health questionnaire utilizing the WebMD platform. Data collected from the questionnaire included: demographic characteristics (eg, age, gender, education, and ethnicity); lifestyle habits such as diet, smoking status, physical activity levels, sleep habits, alcohol intake; self‐assessment of health status; perception of stress levels; and attitudes toward behavioral change. Afterward, employees attended a wellness fair, where trained healthcare professionals took biometric measures such as height, weight, BMI, waist circumference, blood pressure, blood glucose, and total cholesterol. Consent for the use of health data for research was obtained from study participants. The study was approved by the BHSF Institutional Review Board.
2.2. Dependent variables
The dependent variables were the 7 CVH metrics (smoking, physical activity, BMI, diet, total cholesterol, blood pressure, and blood glucose). Data on smoking, physical activity, and diet were collected from self‐reported questionnaires. Smoking was classified as current smokers, former smokers (if they quit <12 months ago), and never smokers (if they have never smoked or quit ≥12 months ago). Diet was measured from 5 items: fruits/vegetables, whole grains, protein, salt, and sugary drinks. Study participants reported daily servings consumed of each item. A healthy diet score was calculated on a scale of 0 to 10 based on the daily servings reported. For physical activity, study participants reported weekly levels as either moderate or vigorous intensity, and the duration of these activities were reported in minutes. BMI was measured by trained healthcare professionals and reported in kilograms per square meter from the calculation of measured weight and height. Self‐reported use of medication for hypertension, hypercholesterolemia, and diabetes was factored into the definition of the categories for total cholesterol, blood pressure, and blood glucose, measured using electronic devices. Nonfasting samples were taken for the measurement of total cholesterol and blood glucose (see Supporting Table 1 in the online version of this article).
Table 1.
Characteristics of study participants (N = 9056)
| Variable | Value |
|---|---|
| Age, y, mean (SD) | 43 (12) |
| Women | 6706 (74%) |
| Education | |
| Postgraduate | 1925 (21%) |
| College | 4087 (45%) |
| Some college | 2204 (24%) |
| High school or less | 840 (9%) |
| Ethnicity | |
| White | 1560 (17%) |
| Hispanic | 5188 (57%) |
| Black | 1459 (16%) |
| Other | 849 (9%) |
| Cardiovascular health metrics | |
| Smoking | |
| Ideal | 8890 (98%) |
| Intermediate | 97 (1%) |
| Poor | 69 (1%) |
| Physical activity | |
| Ideal | 6710 (74%) |
| Intermediate | 1885 (21%) |
| Poor | 461 (5%) |
| BMI | |
| Ideal | 2855 (32%) |
| Intermediate | 3178 (35%) |
| Poor | 3023 (33%) |
| Diet | |
| Ideal | 383 (4%) |
| Intermediate | 2219 (25%) |
| Poor | 6454 (71%) |
| Total cholesterol | |
| Ideal | 6234 (69%) |
| Intermediate | 2192 (24%) |
| Poor | 630 (7%) |
| Blood pressure | |
| Ideal | 3566 (39%) |
| Intermediate | 3835 (42%) |
| Poor | 1655 (18%) |
| Blood glucose | |
| Ideal | 7359 (81%) |
| Intermediate | 1297 (14%) |
| Poor | 400 (4%) |
| No. of ideal metrics | |
| 0–2 | 1083 (12%) |
| 3–5 | 6935 (77%) |
| 6–7 | 1038 (11%) |
| Cardiovascular health score | |
| Inadequate, 0–8 | 2482 (27%) |
| Average, 9–10 | 3424 (38%) |
| Optimal, 11–14 | 3150 (35%) |
Abbreviations: BMI, body mass index; SD, standard deviation.
Values are presented as number (%) unless otherwise indicated. Percents are rounded up to 1 decimal place.
Each of the 7 CVH metrics was scored as follows: ideal (2 points), intermediate (1 point), and poor (0 point) according to AHA criteria (see Supporting Table 1 in the online version of this article), with the poor category serving as the reference group in each category.19 We categorized the number of ideal metrics into 3 summary categories (0–2, 3–5, and 6–7). We also assessed a combined CVH score by summing the total scores from the 7 individual metrics. As previously described, the total CVH score ranged from 0 to 14.22 An inadequate score was 0 to 8 points, an average score was 9 to 10 points, and an optimal score was 11 to 14 points,23 with the inadequate score serving as reference. We also counted the number of ideal metrics achieved by each participant. A higher CVH score or a greater number of ideal metrics signifies better CVH.
2.3. Independent variables
Education and ethnicity were the independent variables. The data on these variables were collected from the online self‐reported health questionnaire mentioned previously. We categorized education into 4 groups as follows: postgraduate (includes professional degrees), college graduate, some college, and high school or less. Ethnicity was categorized into 4 groups as follows: Hispanic, white, black, or other (includes Asian, American Indian, Alaskan Native, Native Hawaiian, Pacific Islander, and multiethnic). Postgraduate whites were used as the reference group.
2.4. Statistical analysis
We reported the overall frequency distribution of study participants by education, ethnicity, and the CVH metrics. By strata defined by education and race/ethnic groups, we reported the proportion of participants in each of the 3 categories of ideal metrics (ie, 0–2, 3–5, and 6–7) as well as the 3 categories of total CVH score (ie, inadequate, average, and optimal).
We computed P values to examine the differences across the education/ethnicity strata using the χ2 test or Fisher exact test as appropriate. Using a multinomial logistic regression, we calculated the main and interactive associations of education and ethnicity on ideal and intermediate CVH metrics, the summary categories of the number of ideal metrics achieved 3, 4, 5, 6, 7, in addition to the CVH scores (average and optimal). This analysis was also stratified by gender and age (<40 and ≥40 years). Education and ethnicity dummy variables were created, with interaction terms representing unique cross products of each nonreferent level of both variables. Individual and global tests of significance of interaction terms on the multiplicative scale were assessed using Wald and likelihood χ2 P values, respectively. Odds ratios were adjusted for age and sex. Additive interaction was assessed by comparing the odds ratios associated with education and ethnicity strata to the summation of their respective education‐ and ethnicity‐only odds ratios. Odds ratio differences of 0 or confidence interval containing 0 were determined as meaningfully or statistically insignificant. Statistical significance was corrected using the Bonferroni approach to account for the 9 CVH outcomes in the main and interactive models as well as for ideal and intermediate categories of each outcome. Therefore, statistical significance was set as 0.0014 (0.05/36) to account for higher false‐positive rates under multiple testing. All data analyses were performed using statistical software (SAS 9.3 for Windows; SAS, Inc., Cary, NC).
3. RESULTS
Table 1 shows the characteristics of study participants. Of the 9056 participants, 74% were women and the overall mean age was 43 (±12) years. A large proportion of participants had at least a college education (66%) compared to <10% who had a high school education or less. The majority of participants identified as Hispanic, whereas an almost equal proportion identified as white or black. For the metrics of smoking, physical activity, total cholesterol, and blood glucose, more than two‐thirds of participants met the criteria for the ideal category. Approximately one‐third of participants fell into each category of BMI. For diet, the majority of participants fell into the poor category, and about 1 in 5 participants fell into the poor category of blood pressure. Only 1 in 10 participants achieved 6 to 7 ideal metrics, and over one‐third had optimal CVH scores.
Table 2 shows the distribution of the CVH metrics by ethnicity within educational categories. For the metric of smoking, over 90% of participants met the ideal criteria regardless of education or ethnicity. Over two‐thirds of participants in most of the educational and ethnic categories met the ideal for physical activity. However, participants with a high school or less education had a slightly higher proportion that fell into the poor category for physical activity. The distribution of the BMI categories was even across the substrata. Participants who identified as black had the highest proportion in the poor BMI category. For the dietary metric, white participants with a postgraduate education had the largest proportion with ideal diet, and white participants with a high school or less education had the largest proportion with a poor diet. Although over half of participants in all the strata achieved ideal status for total cholesterol, white participants had the smallest proportion in the ideal category except in the education stratum for high school or less. Hispanic participants had the largest proportion with blood pressure in the ideal category, whereas participants who identified as black had the largest proportion with blood pressure in the poor category, especially those with a high school or less education (approximately 50%). For blood glucose, the proportion of participants in the ideal category was over 75%, except for the high school or less substrata. As illustrated in the Figure, most of the study participants achieved 3 to 5 ideal metrics, and only 1% of black participants with a high school or less education achieved 6 to 7 ideal metrics. In most of the educational categories, Hispanic participants had the highest proportion of optimal CVH scores or 6 to 7 ideal metrics, whereas black participants had the lowest proportion.
Table 2.
Distribution of cardiovascular health metrics by ethnicity within educational categories
| Postgraduate | College | Some College | High School or Less | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| White | Hispanic | Black | Other | P Value | White | Hispanic | Black | Other | P Value | White | Hispanic | Black | Other | P Value | White | Hispanic | Black | Other | P Value | |
| Sample size | 427 | 1085 | 203 | 210 | 754 | 2304 | 570 | 459 | 304 | 1363 | 409 | 128 | 75 | 436 | 277 | 52 | ||||
| Smoking | ||||||||||||||||||||
| Ideal | 98% | 99% | 100% | 99.5% | 0.5591 | 97% | 99% | 99% | 98% | 0.0066 | 95% | 98% | 99% | 95% | 0.0329 | 93% | 97% | 98% | 100% | 0.4281 |
| Intermediate | 1% | 0.4% | 0% | 0.5% | 2% | 1% | 0.4% | 1% | 3% | 1% | 1% | 3% | 4% | 1% | 1% | 0% | ||||
| Poor | 1% | 1% | 0% | 0% | 2% | 0.4% | 0.5% | 0.4% | 2% | 1% | 1% | 2% | 3% | 2% | 1% | 0% | ||||
| Physical activity | ||||||||||||||||||||
| Ideal | 76% | 76% | 68% | 72% | 0.0819 | 74% | 78% | 71% | 70% | <0.0001 | 65% | 75% | 73% | 75% | 0.0151 | 63% | 71% | 65% | 79% | 0.1053 |
| Intermediate | 21% | 19% | 26% | 24% | 21% | 17% | 23% | 27% | 29% | 19% | 22% | 20% | 28% | 22% | 29% | 13% | ||||
| Poor | 3% | 5% | 6% | 4% | 5% | 5% | 5% | 3% | 6% | 6% | 5% | 5% | 9% | 8% | 6% | 8% | ||||
| BMI | ||||||||||||||||||||
| Ideal | 38% | 34% | 26% | 49% | <0.0001 | 40% | 36% | 25% | 44% | <0.0001 | 29% | 25% | 14% | 23% | <0.0001 | 29% | 23% | 11% | 29% | <0.0001 |
| Intermediate | 34% | 38% | 35% | 33% | 33% | 35% | 36% | 36% | 31% | 36% | 29% | 38% | 28% | 37% | 36% | 46% | ||||
| Poor | 27% | 28% | 39% | 18% | 27% | 29% | 39% | 20% | 40% | 38% | 57% | 39% | 43% | 40% | 53% | 25% | ||||
| Diet | ||||||||||||||||||||
| Ideal | 8% | 5% | 3% | 4% | <0.0001 | 7% | 4% | 2% | 3% | <0.0001 | 5% | 3% | 2% | 5% | 0.2769 | 3% | 3% | 2% | 4% | 0.1251 |
| Intermediate | 36% | 27% | 26% | 21% | 30% | 25% | 24% | 24% | 22% | 22% | 19% | 24% | 11% | 18% | 22% | 29% | ||||
| Poor | 56% | 68% | 71% | 74% | 63% | 71% | 73% | 73% | 73% | 75% | 79% | 71% | 87% | 79% | 76% | 67% | ||||
| Total cholesterol | ||||||||||||||||||||
| Ideal | 53% | 72% | 70% | 64% | <0.0001 | 61% | 74% | 74% | 67% | <0.0001 | 55% | 75% | 75% | 70% | <0.0001 | 60% | 63% | 65% | 56% | 0.6431 |
| Intermediate | 37% | 22% | 22% | 28% | 31% | 20% | 21% | 26% | 33% | 21% | 21% | 23% | 32% | 28% | 29% | 33% | ||||
| Poor | 9% | 5% | 8% | 8% | 8% | 6% | 6% | 7% | 12% | 7% | 5% | 8% | 8% | 10% | 7% | 12% | ||||
| Blood pressure | ||||||||||||||||||||
| Ideal | 32% | 47% | 31% | 38% | <0.0001 | 37% | 50% | 37% | 35% | <0.0001 | 30% | 39% | 28% | 25% | <0.0001 | 21% | 33% | 17% | 21% | <0.0001 |
| Intermediate | 46% | 42% | 38% | 44% | 45% | 40% | 41% | 45% | 43% | 44% | 43% | 49% | 49% | 42% | 36% | 50% | ||||
| Poor | 22% | 12% | 31% | 18% | 18% | 11% | 23% | 20% | 26% | 17% | 29% | 26% | 29% | 25% | 47% | 29% | ||||
| Blood glucose | ||||||||||||||||||||
| Ideal | 76% | 84% | 81% | 82% | 0.0001 | 76% | 86% | 83% | 80% | <0.0001 | 76% | 83% | 78% | 79% | 0.0158 | 63% | 80% | 65% | 67% | <0.0001 |
| Intermediate | 20% | 13% | 11% | 13% | 19% | 12% | 14% | 16% | 19% | 12% | 15% | 13% | 32% | 12% | 24% | 23% | ||||
| Poor | 4% | 3% | 8% | 5% | 5% | 2% | 3% | 4% | 6% | 5% | 6% | 8% | 5% | 8% | 11% | 10% | ||||
Percents are rounded up to 1 decimal place.
Figure 1.
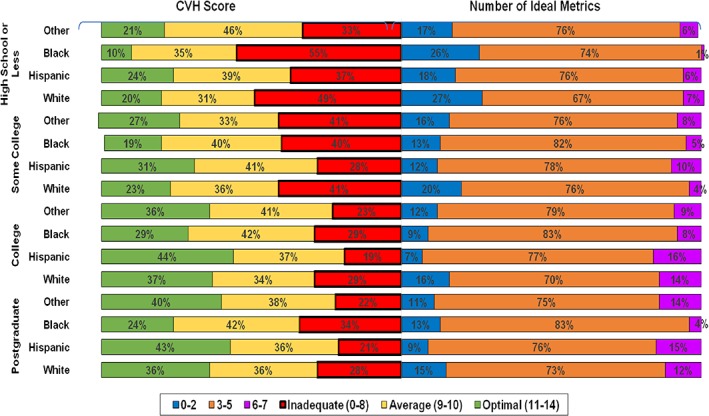
Distribution of the cardiovascular health score and the number of ideal metrics by education and ethnicity
The main and interactive associations of education and ethnicity on achieving ideal CVH metrics (Table 3) and of intermediate CVH metrics (see Supporting Table 2 in the online version of this article) are illustrated. With the postgraduate education category serving as reference, participants with college, some college, and high school education or less were less likely to achieve ideal status for most of the individual CVH metrics, and also less likely to achieve 6 to 7 ideal metrics, and optimal CVH scores. However, some of the associations were not statistically significant. Compared to white participants, Hispanic and black participants were less likely to meet the ideal criteria for BMI in contrast to participants who identified as other. Black participants were more likely to meet the criteria for ideal total cholesterol but less likely to meet the criteria for ideal blood pressure, 6 to 7 ideal metrics, and optimal scores. Although the associations varied across gender and age groups (<40 and ≥40 years), the majority were not statistically significant (see Supporting Tables 3–6 in the online version of this article).
Table 3.
Multinomial logistic regression for ideal status for each cardiovascular health metrics: Main and interactive associations by education and ethnicity
| Smoking | Physical Activity | BMI | Diet | Total Cholesterol | Blood Pressure | Blood Glucose | 6–7 Ideal Metrics | Optimal Score | |
|---|---|---|---|---|---|---|---|---|---|
| Education | |||||||||
| Postgraduatea | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) |
| College | 0.70 (0.34‐1.47) | 1.03 (0.79‐1.34) | 0.87 (0.75‐1.00) | 0.83 (0.64‐1.06) | 0.95 (0.76‐1.19) | 0.88 (0.73‐1.05) | 1.07 (0.79‐1.43) | 0.90 (0.71‐1.14) | 0.86 (0.74‐1.00) |
| Some college | 0.48 (0.22‐1.02) | 0.81 (0.61‐1.07) | 0.46 (0.39‐0.53)b | 0.58 (0.42‐0.78)b | 0.93 (0.72‐1.19) | 0.59 (0.48‐0.71)b | 0.67 (0.49‐0.90)b | 0.45 (0.34‐0.59)b | 0.48 (0.40‐0.56)b |
| High school or less | 0.34 (0.14‐0.81)b | 0.60 (0.42‐0.85) b | 0.47 (0.38‐0.59)b | 0.48 (0.30‐0.77)b | 0.85 (0.62‐1.16) | 0.49 (0.38‐0.63)b | 0.50 (0.36‐0.71)b | 0.29 (0.19‐0.44)b | 0.37 (0.29‐0.47)b |
| Ethnicity | |||||||||
| White | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) |
| Hispanic | 1.91 (1.09‐3.37) | 0.89 (0.67‐1.17) | 0.78 (0.67‐0.90)b | 0.61 (0.47‐0.79)b | 1.23 (0.99‐1.54) | 1.26 (1.05‐1.52) | 1.12 (0.84‐1.49) | 1.26 (0.99‐1.61) | 1.11 (0.94‐1.29) |
| Black | 2.57 (1.14‐5.75) | 0.89 (0.63‐1.24) | 0.35 (0.29‐0.42)b | 0.36 (0.24‐0.53)b | 1.65 (1.23‐2.21)b | 0.39 (0.31‐0.48)b | 0.72 (0.52‐1.01) | 0.43 (0.30‐0.61)b | 0.44 (0.36‐0.54)b |
| Otherc | 2.20 (0.82‐5.87) | 1.17 (0.76‐1.81) | 1.42 (1.14‐1.77)b | 0.47 (0.31‐0.72)b | 1.14 (0.83‐1.57) | 0.64 (0.49‐0.83)b | 0.72 (0.49‐1.07) | 0.82 (0.57‐1.18) | 0.95 (0.76‐1.20) |
| Education and ethnicity | |||||||||
| Postgraduate white | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) | 1.0 (Ref) |
| Postgraduate Hispanic | 0.91 (0.23‐3.55) | 0.61 (0.33‐1.13) | 0.75 (0.56‐1.00) | 0.55 (0.35‐0.87) | 1.67 (1.07‐2.59) | 1.57 (1.10‐2.25) | 1.18 (0.64‐2.16) | 1.10 (0.69‐1.76) | 0.98 (0.72‐1.33) |
| Postgraduate black | — | 0.45 (0.20‐1.00) | 0.40 (0.26‐0.61)b | 0.29 (0.12‐0.70) | 1.37 (0.74‐2.55) | 0.40 (0.25‐0.65)b | 0.45 (0.22‐0.93) | 0.29 (0.12‐0.68) | 0.37 (0.23‐0.59)b |
| Postgraduate other | — | 0.77 (0.31‐1.89) | 1.72 (1.10‐2.69) | 0.42 (0.19‐0.89) | 1.07 (0.58‐1.99) | 0.85 (0.51‐1.42) | 0.63 (0.29‐1.39) | 0.98 (0.49‐1.96) | 0.96 (0.61‐1.51) |
| College white | 0.42 (0.12‐1.51) | 0.70 (0.36‐1.35) | 0.87 (0.65‐1.18) | 0.80 (0.51‐1.26) | 1.18 (0.76‐1.82) | 1.00 (0.69‐1.44) | 0.74 (0.41‐1.33) | 0.78 (0.48‐1.26) | 0.77 (0.56‐1.06) |
| College Hispanic | 1.27 (0.34‐4.79) | 0.67 (0.37‐1.21) | 0.66 (0.51‐0.86) | 0.47 (0.31‐0.71)b | 1.29 (0.87‐1.92) | 1.26 (0.91‐1.76) | 1.20 (0.68‐2.09) | 1.10 (0.71‐1.71) | 0.86 (0.65‐1.14) |
| College black | 1.09 (0.22‐5.49) | 0.55 (0.28‐1.07) | 0.34 (0.24‐0.47)b | 0.25 (0.13‐0.47)b | 1.60 (0.97‐2.64) | 0.42 (0.29‐0.62)b | 0.87 (0.44‐1.69) | 0.48 (0.27‐0.84) | 0.39 (0.28‐0.56)b |
| College other | 1.48 (0.24‐8.97) | 0.97 (0.44‐2.08) | 1.32 (0.93‐1.88) | 0.28 (0.14‐0.54)b | 1.38 (0.82‐2.30) | 0.60 (0.40‐0.89) | 0.70 (0.36‐1.37) | 0.54 (0.30‐0.96) | 0.77 (0.53‐1.10) |
| Some college white | 0.44 (0.10‐1.86) | 0.48 (0.23‐1.01) | 0.49 (0.34‐0.71)b | 0.44 (0.24‐0.84) | 0.92 (0.55‐1.53) | 0.85 (0.55‐1.31) | 0.79 (0.40‐1.59) | 0.30 (0.15‐0.63)b | 0.43 (0.29‐0.64)b |
| Some college Hispanic | 0.76 (0.21‐2.80) | 0.49 (0.27‐0.90) | 0.39 (0.29‐0.51)b | 0.30 (0.19‐0.49)b | 1.29 (0.86‐1.94) | 0.80 (0.57‐1.13) | 0.63 (0.37‐1.08) | 0.38 (0.16‐0.91)b | 0.50 (0.37‐0.67)b |
| Some college black | 0.81 (0.16‐4.08) | 0.61 (0.30‐1.77) | 0.14 (0.10‐0.21)b | 0.23 (0.11‐0.47)b | 2.18 (1.22‐3.91) | 0.27 (0.18‐0.41)b | 0.46 (0.25‐0.87) | 0.21 (0.11‐0.40)b | 0.20 (0.14‐0.29)b |
| Some college other | 0.24 (0.05‐1.22) | 0.63 (0.23‐1.71) | 0.37 (0.22‐0.62)b | 0.48 (0.19‐1.17) | 1.28 (0.60‐2.72) | 0.38 (0.20‐0.69) | 0.43 (0.19‐0.98) | 0.51 (0.32‐0.81) | 0.32 (0.19‐0.54)b |
| High School or less white | 0.28 (0.05‐1.69) | 0.27 (0.10‐0.72) | 0.50 (0.27‐0.92) | 0.20 (0.05‐0.56) | 1.62 (0.62‐4.12) | 0.58 (0.27‐1.23) | 0.75 (0.24‐2.34) | 0.40 (0.13‐1.20) | 0.34 (0.17‐0.66) |
| High School or less Hispanic | 0.41 (0.11‐1.61) | 0.36 (0.19‐0.71) | 0.39 (0.28‐0.55) | 0.29 (0.15‐0.54)b | 1.03 (0.63‐1.65) | 0.76 (0.51‐1.13) | 0.48 (0.26‐0.87)b | 0.39 (0.22‐0.71) | 0.41 (0.29‐0.59)b |
| High School or less black | 0.68 (0.14‐3.41) | 0.46 (0.21‐0.97) | 0.14 (0.09‐0.22)b | 0.16 (0.06‐0.42)b | 1.88 (1.03‐3.42) | 0.18 (0.12‐0.29)b | 0.31 (0.17‐0.58)b | 0.03 (0.01‐0.14)b | 0.11 (0.07‐0.18)b |
| High School or less other | — | 0.41 (0.13‐1.32) | 0.83 (0.37‐1.82) | 0.39 (0.09‐1.68) | 0.88 (0.34‐2.31) | 0.47 (0.19‐1.15) | 0.40 (0.14‐1.15) | 0.45 (0.11‐1.85) | 0.49 (0.21‐1.13) |
Abbreviations: BMI, body mass index; CI, confidence interval.
Values are presented as odds ratio (95% CI). Odds ratios were adjusted for age, sex, ethnicity, and education as appropriate. The “—” symbol indicates extremely small odds ratios. P values for interaction were not statistically significant.
Postgraduate includes professional degrees.
Statistically significant (P < 0.0014).
Includes Asian, American Indian, Alaskan Native, Native Hawaiian, Pacific Islander, and multiethnic.
None of the education and ethnicity interaction terms were statistically significant. The likelihood ratio test of global interaction and Wald tests for individual interaction terms were not statistically significant when comparing participants who achieved ideal or intermediate levels of overall CVH to those who were in poor CVH. Similarly, the additive effect of education on ethnicity was not meaningfully or statistically significant.
4. DISCUSSION
4.1. Summary of results
Using a large sample of employment‐based health records, we explored the interactive associations of education and ethnicity on CVH. Despite suggestions that educational attainment modifies risk of CVD among ethnic groups,17 we did not observe such a modification either on the multiplicative or additive scale in our study. We found that increasing levels of education were not always associated with improved CVH. In particular, black participants at the highest and lowest education levels experienced some of the poorest CVH indices. Additionally, higher educational attainment was associated with improved CVH outcomes among Hispanics more than any other racial/ethnic group.
4.2. Comparison to previous studies and interpretation of results
Our results are comparable to a National Health and Nutrition Examination Survey (NHANES) of more than 5000 multiethnic women, which found that black and Mexican American women displayed higher CVD risk factors compared to white women.12 The study revealed that black women with less than 9 years of education reported less leisure time physical activity, and greater BMI and systolic blood pressures than other women. Even among black women with more than 12 years of education, high prevalence of being overweight and hypertensive persisted beyond the age of 40 years.24 This may in part explain our observation that some of the lowest odds of meeting ideal CVH metrics occurred among black participants at the extremes of the educational spectrum. In contrast, Hispanics in our study were at least as healthy as whites with a postgraduate education when several indices of CVH were considered. The incongruence between CVH among Hispanics in the NHANES study and ours may be related to healthy migrant effects and differing CVD risk profiles among Hispanics originally from different parts of Latin America.25 In addition, our study population consisted of individuals who were employed in a healthcare system, and there may be a healthy‐worker bias.
Despite nonsignificant interaction terms between individual racial/ethnic and educational strata, we demonstrated several differences in the distribution of ideal CVH components in our sample. For instance, postgraduate whites were the healthiest subgroup, except for their blood cholesterol readings, which were typically better among persons from other racial/ethnic groups. The odds of achieving an ideal BMI was lowest among whites with at best a high school education. Hispanics with at least a complete college education were more likely to report better blood cholesterol, glucose, and pressure than white postgraduates or others. It is not exactly clear why we did not observe significant interactions between education and ethnicity. The fact that our study participants were employees of a healthcare system with access to health information, with most being physically active and refraining from cigarette smoking, may have played a role in attenuating inherent risk differences among subgroups. It is also possible that the current study was underpowered to identify the number of interactions tested. Taken together, the results of the current study suggests that different risk factors drive CVD among racial/ethnic groups, and higher educational attainment alone may not always improve CVH.
4.3. Study strengths and limitations
Our findings are limited by selection bias, with 60% participation among those eligible. Because majority of our study participants were highly educated Hispanic women, our results may not be generalizable. Furthermore, the cross‐sectional study design does not lend itself to the more robust temporal analysis of the potentially modifying effect of education on race/ethnicity in the expression of cardiovascular health or disease. Notwithstanding, this study presents a number of methodological strengths. First, it involves the use of a large sample, thereby minimizing extreme and uncharacteristic findings. Second, blood cholesterol, pressure, and glucose were measured by trained personnel as opposed to recall, which has been frequently adopted in the past among study participants.
5. CONCLUSION
Our findings highlight the complicated interplay of the roles of education and ethnicity on CVH. Different drivers of cardiovascular risk operate among racial/ethnic groups, and higher educational attainment appears to have varying degrees of associations noted for achievement of ideal levels of overall CVH and its components. Therefore, for CVH interventions and policies to be successful, they must be tailored to address the specific challenges of target communities.
Conflicts of interest
The authors declare no potential conflicts of interest.
Supporting information
Table S1.–Proportion of study participants in each category of the cardiovascular health metrics.
Table S2.–Multinomial Logistic Regression Odds Ratios (95% CI) for intermediate status for each of the CVH Metrics: Main and Interactive associations of education and ethnicity
Table S3.–Multinomial Logistic Regression Odds Ratios (95% CI) for Ideal Status for Each CVH Metrics: Main and Interactive Associations by Education and Ethnicity for Men, n = 2,350
Table S4.–Multinomial Logistic Regression Odds Ratios (95% CI) for Ideal Status for Each CVH Metrics: Main and Interactive Associations by Education and Ethnicity for Women, n = 6,706
Table S5.–Multinomial Logistic Regression Odds Ratios (95% CI) for Ideal Status for Each CVH Metrics: Main and Interactive Associations by Education and Ethnicity for < 40, n = 3,980
Table S6.–Multinomial Logistic Regression Odds Ratios (95% CI) for Ideal Status for Each CVH Metrics: Main and Interactive Associations by Education and Ethnicity for ≥ 40, n = 5,076
Ogunmoroti O., Utuama O. A., Michos E. D., Valero‐Elizondo J., Okunrintemi V., Taleb Z. B., Bahelah R., Das S., Rouseff M., Parris D., Agatston A., Feldman T., Veledar E., Maziak W., and Nasir K. Does education modify the effect of ethnicity in the expression of ideal cardiovascular health? The Baptist Health South Florida Employee Study. Clin Cardiol. 2017;40:1000–1007. 10.1002/clc.22757
REFERENCES
- 1. World Health Organization . Cardiovascular diseases. http://www.who.int/mediacentre/factsheets/fs317/en/. Published 2016. Updated May 2017. Accessed August 18, 2016.
- 2. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics‐2016 update: a report from the American Heart Association. Circulation. 2016;133:e38–e360. [DOI] [PubMed] [Google Scholar]
- 3. Beaglehole R. International trends in coronary heart disease mortality morbidity and risk factors. Epidemiol Rev. 1990;12:1–15. [DOI] [PubMed] [Google Scholar]
- 4. Burt VL, Cutler JA, Higgins M, et al. Trends in the prevalence, awareness, treatment, and control of hypertension in the adult US population data from the health examination surveys, 1960 to 1991. Hypertension. 1995;26:60–69. [DOI] [PubMed] [Google Scholar]
- 5. Gregg, EW , Cheng YJ, Cadwell BL, et al. Secular trends in cardiovascular disease risk factors according to body mass index in US adults. JAMA. 2005;293:1868–1874. [DOI] [PubMed] [Google Scholar]
- 6. Center for Disease Control and Prevention . Tobacco use—United States, 1900‐1999. MMWR Morb Mortal Wkly Rep. 1999;48:986–993. [PubMed] [Google Scholar]
- 7. Johnson CL, Rifkind BM, Sempos CT, et al. Declining serum total cholesterol levels among US adults: the National Health and Nutrition Examination Surveys. JAMA. 1993;269:3002–3008. [PubMed] [Google Scholar]
- 8. Kanjilal S, Gregg EW, Cheng YJ, et al. Socioeconomic status and trends in disparities in 4 major risk factors for cardiovascular disease among US adults, 1971‐2002. Arch Intern Med. 2006;166:2348–2355. [DOI] [PubMed] [Google Scholar]
- 9. Kramer H, Han C, Post W, et al. Racial/ethnic differences in hypertension and hypertension treatment and control in the multi‐ethnic study of atherosclerosis (MESA). Am J Hypertens. 2004;17:963–970. [DOI] [PubMed] [Google Scholar]
- 10. Ogden CL, Carroll MD, Fryar CD, et al. Prevalence of obesity among adults and youth: United States, 2011‐2014. NCHS Data Brief. 2015;219:1–8. [PubMed] [Google Scholar]
- 11. Kaplan GA, Keil JE. Socioeconomic factors and cardiovascular disease: a review of the literature. Circulation. 1993;88:1973–1998. [DOI] [PubMed] [Google Scholar]
- 12. Winkleby MA, Kraemer HC, Ahn DK, et al. Ethnic and socioeconomic differences in cardiovascular disease risk factors: findings for women from the Third National Health and Nutrition Examination Survey, 1988‐1994. JAMA. 1998;280:356–362. [DOI] [PubMed] [Google Scholar]
- 13. Boykin S, Diez‐Roux AV, Carnethon M, et al. Racial/ethnic heterogeneity in the socioeconomic patterning of CVD risk factors: in the United States: the multi‐ethnic study of atherosclerosis. J Health Care Poor Underserved. 2011;22:111–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kimbro RT, Bzostek S, Goldman N, et al. Race, ethnicity, and the education gradient in health. Health Aff (Millwood). 2008;27:361–372. [DOI] [PubMed] [Google Scholar]
- 15. Kawachi I, Daniels N, Robinson DE. Health disparities by race and class: why both matter. Health Aff (Millwood). 2005;24:343–352. [DOI] [PubMed] [Google Scholar]
- 16. Farmer MM, Ferraro KF. Are racial disparities in health conditional on socioeconomic status? Soc Sci Med. 2005;60:191–204. [DOI] [PubMed] [Google Scholar]
- 17. Bostean G, Roberts CK, Crespi CM, et al. Cardiovascular health: associations with race‐ethnicity, nativity, and education in a diverse, population‐based sample of Californians. Ann Epidemiol. 2013;23:388–394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Jankovic S, Stojisavljević D, Janković J, et al. Association of socioeconomic status measured by education, and cardiovascular health: a population‐based cross‐sectional study. BMJ Open. 2014;4:e005222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Lloyd‐Jones DM, Hong Y, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association's strategic Impact Goal through 2020 and beyond. Circulation. 2010;121:586–613. [DOI] [PubMed] [Google Scholar]
- 20. Ogunmoroti O, Younus A, Rouseff M, et al. Assessment of American Heart Association's ideal cardiovascular health metrics among employees of a large healthcare organization: The Baptist Health South Florida Employee Study. Clin Cardiol. 2015;38:422–429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Ogunmoroti O, Utuama O, Spatz ES, et al. Trends in ideal cardiovascular health metrics among employees of a large healthcare organization (from the Baptist Health South Florida Employee Study). Am J Cardiol. 2016;117:787–793. [DOI] [PubMed] [Google Scholar]
- 22. Lloyd‐Jones DM. Improving the cardiovascular health of the US population. JAMA. 2012;307:1314–1316. [DOI] [PubMed] [Google Scholar]
- 23. Unger E, Diez‐Roux AV, Lloyd‐Jones DM, et al. Association of neighborhood characteristics with cardiovascular health in the Multi‐Ethnic Study of Atherosclerosis. Circ Cardiovasc Qual Outcomes. 2014;7:524–531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Rosenberg L, Palmer JR, Adams‐Campbell LL, et al. Obesity and hypertension among college‐educated black women in the United States. J Hum Hypertens. 1999;13:237–241. [DOI] [PubMed] [Google Scholar]
- 25. Schoenthaler AM, Cardiovascular health in Hispanics/Latinos: a reexamination of the Hispanic paradox. J Clin Hypertens (Greenwich). 2017;19:114–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1.–Proportion of study participants in each category of the cardiovascular health metrics.
Table S2.–Multinomial Logistic Regression Odds Ratios (95% CI) for intermediate status for each of the CVH Metrics: Main and Interactive associations of education and ethnicity
Table S3.–Multinomial Logistic Regression Odds Ratios (95% CI) for Ideal Status for Each CVH Metrics: Main and Interactive Associations by Education and Ethnicity for Men, n = 2,350
Table S4.–Multinomial Logistic Regression Odds Ratios (95% CI) for Ideal Status for Each CVH Metrics: Main and Interactive Associations by Education and Ethnicity for Women, n = 6,706
Table S5.–Multinomial Logistic Regression Odds Ratios (95% CI) for Ideal Status for Each CVH Metrics: Main and Interactive Associations by Education and Ethnicity for < 40, n = 3,980
Table S6.–Multinomial Logistic Regression Odds Ratios (95% CI) for Ideal Status for Each CVH Metrics: Main and Interactive Associations by Education and Ethnicity for ≥ 40, n = 5,076