

Abstract
Background
Tardive dyskinesia (TD) is a disabling movement disorder associated with the prolonged use of antipsychotic medication. Several strategies have been examined in the treatment of TD. Currently, however, there is no clear evidence of the effectiveness of these drugs in TD and they have been associated with many side effects. One particular strategy would be to use pharmaceutical agents which are known to influence the catecholaminergic system at various junctures.
Objectives
1. To determine the effects of any of the following drugs for antipsychotic‐induced TD in people with schizophrenia or other chronic mental illnesses. i. Drugs which influence the noradrenergic system. ii. Dopamine receptor agonists. iii. Dopamine receptor antagonists. iv. Dopamine‐depletor drugs. v. Drugs that increase the production or release of dopamine.
2. To examine whether any improvement occurred with short periods of intervention (less than 6 weeks) and, if this did occur, whether this effect was maintained at longer periods of follow‐up.
3. To examine if there was a differential effect for the various compounds.
4. To examine whether the use of non‐antipsychotic catecholaminergic drugs are most effective in those with more recent onset TD (less than five years).
Search methods
We retrieved 712 references from searching the Cochrane Schizophrenia Group Trials Register (July 2015 and April 2017). We also inspected references of all identified studies for further trials and contacted authors of trials for additional information.
Selection criteria
We selected studies if they were randomised controlled trials focusing on people with schizophrenia or other chronic mental illnesses and antipsychotic‐induced tardive dyskinesia. We compared the use of catecholaminergic interventions versus placebo, no intervention, or any other intervention for the treatment of antipsychotic‐induced tardive dyskinesia.
Data collection and analysis
We independently extracted data from these trials and we estimated risk ratios (RRs) with 95% confidence intervals (CIs). We assumed that people who left the studies early had no improvement.
Main results
There are 10 included trials (N = 261) published between 1973 and 2010; eight are new from the 2015 and 2017 update searches. Forty‐eight studies are excluded. Participants were mostly chronically mentally ill inpatients in their 50s, and studies were primarily of short (2 to 6 weeks) duration. The overall risk of bias in these studies was unclear, mainly due to poor reporting of allocation concealment and generation of the sequence. Studies were also not clearly blinded and we are unsure if data are incomplete or selectively reported, or if other biases were operating.
One small, three‐arm trial found that both alpha‐methyldopa (N = 20; RR 0.33, 95% CI 0.14 to 0.80; low‐quality evidence) and reserpine (N = 20; RR 0.52 95% CI 0.29 to 0.96; low‐quality evidence) may lead to a clinically important improvement in tardive dyskinesia symptoms compared with placebo after 2 weeks' treatment, but found no evidence of a difference between alpha‐methyldopa and reserpine (N = 20; RR 0.60, 95% CI 0.19 to 1.86; very low quality evidence). Another small trial compared tetrabenazine and haloperidol after 18 weeks' treatment and found no evidence of a difference on clinically important improvement in tardive dyskinesia symptoms (N = 13; RR 0.93, 95% CI 0.45 to 1.95; very low quality evidence). No study reported on adverse events.
For remaining outcomes there was no evidence of a difference between any of the interventions: alpha‐methyldopa versus placebo for deterioration of tardive dyskinesia symptoms (1 RCT; N = 20; RR 0.33, 95% CI 0.02 to 7.32; very low quality evidence), celiprolol versus placebo for leaving the study early (1 RCT; N = 35; RR 5.28, 95% CI 0.27 to 102.58; very low quality evidence) and quality of life (1 RCT; N = 35; RR 0.87, 95% CI 0.68 to 1.12; very low quality evidence), alpha‐methyldopa versus reserpine for deterioration of tardive dyskinesia symptoms (1 RCT; N = 20; not estimable, no reported events; very low quality evidence), reserpine or carbidopa/levodopa versus placebo for deterioration of tardive dyskinesia symptoms (2 RCTs; N = 37; RR 1.18, 95% CI 0.35 to 3.99; very low quality evidence), oxypertine versus placebo for deterioration of mental state (1 RCT; N = 42; RR 2.20, 95% CI 0.22 to 22.45; very low quality evidence), dopaminergic drugs (amantadine, bromocriptine, tiapride, oxypertine, carbidopa/levodopa) versus placebo for leaving the study early (6 RCTs; N = 163; RR 1.29, 95% CI 0.65 to 2.54; very low quality evidence), and tetrabenazine versus haloperidol for deterioration of tardive dyskinesia symptoms (1 RCT; N = 13; RR 1.17, 95% CI 0.09 to 14.92) and leaving the study early (1 RCT; N = 13; RR 0.23, 95% CI 0.01 to 4.00).
Authors' conclusions
Although there has been a large amount of research in this area, many studies were excluded due to inherent problems in the nature of their cross‐over designs. Usually data are not reported before the cross‐over and the nature of TD and its likely response to treatments make it imprudent to use this data. The review provides little usable information for service users or providers and more well‐designed and well‐reported studies are indicated.
Plain language summary
Non‐antipsychotic catecholaminergic drugs for antipsychotic‐induced tardive dyskinesia
Review question.
To determine if catecholaminergic drugs help in the treatment of tardive dyskinesia for people with schizophrenia or similar mental health problems.
Background.
People with schizophrenia often hear voices and see things (hallucinations) and have strange beliefs (delusions). The main treatment of schizophrenia is antipsychotic drugs. However, these drugs can have debilitating side‐effects. Tardive dyskinesia is an involuntary movement that causes the face, mouth, tongue and jaw to convulse, spasm and grimace. It is caused by long‐term or high‐dose use of antipsychotic drugs, is difficult to treat and can be incurable. One suggested treatment is to use medication that affects the catecholaminergic system, which is a group of brain chemicals.
Study characteristics.
The review includes 10 small, short studies published mainly in the 1980s involving a total of 261 people.
Key results.
One small study found that after 2 weeks' treatment both alpha‐methyldopa and reserpine may lead to clinically important improvement in tardive dyskinesia symptoms compared with placebo, but the quality of evidence was low. We are uncertain about the effect of reserpine versus alpha‐methyldopa; quality of evidence was very low. Another small trial compared tetrabenazine and haloperidol after 18 weeks' treatment, but again we are uncertain about the effect as the quality of evidence was very low. The included studies did not report on any harmful effects of the drugs.
Quality of the evidence.
Evidence is weak, limited, short term, and small scale. It is not possible to recommend these drugs as a treatment for tardive dyskinesia and their use is entirely experimental. There is a need for larger and more rigorous research in the area.
This plain language summary was adapted by the review authors from a summary originally written by Ben Gray, Senior Peer Researcher, McPin Foundation (mcpin.org/).
Summary of findings
Background
Description of the condition
Since the 1950s, antipsychotic (or neuroleptic) medication has been extensively used to treat people with chronic mental illnesses, such as schizophrenia. These drugs can effectively control symptoms such as abnormal perceptions (hallucinations), disordered thinking and fixed false beliefs (delusions). In addition, maintenance therapy with antipsychotics is associated with a reduced risk of relapses (Schooler 1993). Antipsychotic medication, however, has also been associated with a wide range of adverse effects, including movement disorders. The appearance of these movement disorders can contribute to poor compliance with antipsychotic treatment and hence relapse (Barnes 1993).
Tardive dyskinesia (TD) is one such movement disorder and is characterised by abnormal, repetitive and involuntary movements (APA 1992). The clinical features include tongue protrusion, side‐to‐side or rotatory movement of the jaw, lip smacking, puckering and pursing, and rapid eye blinking (Casey 1994). In some people rapid movements of the arms, legs, and trunk may also occur. TD is a chronic condition of insidious onset, the severity of which spontaneously fluctuates (APA 1992). Studies on the natural history of tardive dyskinesia have reported widely variable remission rates (1% to 62%) depending on patient age, psychiatric diagnosis, course of the psychiatric disorder, and duration of therapy (Bergen 1989; Fernandez 2001; Glazer 1990).
Although the most frequent cause of TD is the use of antipsychotic medication, it is clinically striking that dose reduction can lead to a temporary exacerbation in symptoms. Conversely, increasing the dose is often associated with a temporary remission (Cavallaro 1993; Smith 1980). The exact mechanisms of the pathophysiology of TD are unknown. Antipsychotic drugs block certain chemical receptor sites in the brain — one of these is specific for dopamine (Casey 1994). One hypothesis explaining the cause of antipsychotic‐induced TD is that chronic blockade of dopamine receptors in specific cells of the brain (neurones from the nigrostriatum) causes an overgrowth of these receptors (Casey 1994). There is also suggestion that the chronic use of antipsychotics may also cause an abnormal production of highly active atoms and chemical groups (cytotoxic free radicals), which may damage specific cells in the brain. This, in turn, could be responsible for the appearance of TD (Cadet 1989; Sachdev 2000).
TD occurs in more than 20% of those using antipsychotic medication continually for longer than three months (Glazer 2000; Kane 1982; Tarsy 2011). Every year 4% to 5% of adults and 25% to 30% of elderly persons who continually use these drugs begin to show signs of TD (APA 1992; Correll 2004). Advancing age is a risk factor for both TD's prevalence and severity, with those who are under 60 years of age being three times more likely to spontaneously remit (Jeste 2000; Smith 1980).
The prevalence of tardive dyskinesia is often thought to be decreasing based on the use of atypical antipsychotics in place of typical antipsychotics (Cloud 2014). A systematic review found that the incidence of tardive dyskinesia associated with atypical drugs (2% to 4%) was significantly lower than that for typicals (5% to 8%) (Correll 2008). Despite this, the widespread use of atypical drugs in clinical settings, increased off‐label use, and an ageing population may still result in an overall increase in the number of cases of TD (Cloud 2014; Glazer 2000; Maher 2012). The problem will be considerably greater for people in countries where use of newer drugs is less prevalent (Ballesteros 2000; Martins 2011).
Description of the intervention
Catecholamines occur naturally in the body. They are synthesised from the amino acid tyrosine, and examples include epinephrine (adrenaline), norepinephrine and dopamine. There are several pharmaceutical compounds acting as catecholamine analogues that have been tested as treatment for tardive dyskinesia, especially during the 1980s (Jeste 1988). This review will present data on pharmaceutical compounds affecting catecholamiergic pathways in different ways.
The catecholaminergic systems involve a complex cascade of steps that can be modified by pharmaceutical compounds at various junctures. Several strategies have been examined in the treatment of TD. These include: i. increasing the presynaptic release of dopamine (e.g. amantadine); ii. increasing the production of dopamine (e.g. L‐dopa); iii. dopamine receptor antagonists (e.g. alpha‐methyl‐paratyrosine (AMTP)); iv. dopamine receptor agonists (e.g. apomorphine); v. agents that deplete dopamine (e.g. tetrabenazine); vi. agents that block the beta‐adrenergic receptors (e.g. propanolol); vii. agents that act as 'false neurotransmitters' (e.g. methyldopa) (see Types of interventions for the full list of drugs).
How the intervention might work
One of the most influential theories to explain the appearance of TD suggests that long‐term use of antipsychotic medication leads to an increase in the number of dopamine and dopamine‐related receptors. This hypothesis is usually referred to as the dopamine supersensitivity theory (Browne 1986b; Casey 1994); and hence drugs that influence the catecholaminergic (noradrenergic and dopaminergic) function in the extrapyramidal system have been used as treatments for antipsychotic‐induced TD. It was thought that these compounds could reverse dopamine supersensitivity by increasing the levels of available dopamine, thus overcoming the antipsychotic‐induced dopamine blockade (Friedhoff 1977).
Currently, however, there is no clear evidence of the effectiveness of these drugs in treating TD. Nevertheless, they have been associated with many side effects, including drowsiness, confusion, postural hypotension, depression and worsening of psychosis (Turjanski 2005). In addition, an excess of dopamine has itself been associated with movement disorders (choreoathetoid).
Why it is important to do this review
Several atypical antipsychotic drugs have been produced in the last decades that claim to cause less or no TD (Lieberman 1996). These claims may or may not be true, and certainly evidence does point to the fact that thoughtful use of older‐generation drugs is not associated with any more problems of TD than are newer treatments (Chouinard 2008). However, in a global context, it is likely that the less expensive and more familiar drugs — such as chlorpromazine or haloperidol — will continue to be the mainstay of treatment of people with schizophrenia (WHO Essential List 2010). Use of drugs such as these is associated with emergence of TD and, therefore, this condition will remain a problem for years to come.
TD can result in considerable social and physical disability (Barnes 1993); and symptoms are often irreversible (Bergen 1989; Fernandez 2001; Glazer 1990). Additionally, TD is frequently associated with lower quality of life (Ascher‐Svanum 2008); and a greater mortality rate (Chong 2009). Given the high incidence and prevalence of TD among people taking antipsychotic medication, the need for prevention or treatment is clear. Unfortunately, there has been sparse evidence to guide clinicians (NICE 2014; Taylor 2009). Although many treatments have been tested, no one intervention has been shown clearly to be effective. Cessation or reduction of the dose of antipsychotic medication would be the ideal management for TD. In clinical practice this is not always possible, not least because in many individuals such a reduction would lead to relapse. This review focuses on whether the addition of different types of catecholaminergic medications to those already receiving antipsychotic medication is likely to help TD.
This review is one in a series of Cochrane Reviews evaluating treatments for antipsychotic‐induced TD (see Table 5), and is an update of a Cochrane Review first published in 2006 (El‐Sayeh 2006).
1. Other reviews in the series.
| Interventions | Reference |
| Anticholinergic medication | Soares‐Weiser 1997 |
| Benzodiazepines | Bhoopathi 2006 |
| Calcium channel blockers | Essali 2011 |
| Cholinergic medication | Tammenmaa 2002 |
| Gamma‐aminobutyric acid agonists | Alabed 2011 |
| Miscellaneous treatments | Soares‐Weiser 2003 |
| Neuroleptic reduction and/or cessation and neuroleptics | Soares‐Weiser 2006 |
| Non‐neuroleptic catecholaminergic drugs | This review |
| Vitamin E | Soares‐Weiser 2011 |
Objectives
1. To determine the effects of any of the following drugs for antipsychotic‐induced TD in people with schizophrenia or other chronic mental illnesses. i. Drugs which influence the noradrenergic system. ii. Dopamine receptor agonists. iii. Dopamine receptor antagonists. iv. Dopamine‐depletor drugs. v. Drugs that increase the production or release of dopamine.
2. To examine whether any improvement occurred with short periods of intervention (less than 6 weeks) and, if this did occur, whether this effect was maintained at longer periods of follow‐up.
3. To examine if there was a differential effect for the various compounds.
4. To examine whether the use of non‐antipsychotic catecholaminergic drugs are most effective in those with more recent onset TD (less than five years).
Methods
Criteria for considering studies for this review
Types of studies
We included all relevant randomised controlled trials. Where a trial was described as 'double‐blind' but it was implied that the study was randomised, we included these trials in a sensitivity analysis. If there was no substantive difference within primary outcomes (see Types of outcome measures) when these 'implied randomisation' studies were added, then we included these in the final analysis. If there was a substantive difference, we only used clearly randomised trials and described the results of the sensitivity analysis in the text. We excluded quasi‐randomised studies, such as those allocating by using alternate days of the week.
Types of participants
People with schizophrenia or any other chronic mental illness, diagnosed by any criteria, irrespective of gender, age or nationality who: i. required the use of antipsychotics for more than three months; ii. developed tardive dyskinesia (diagnosed by any criteria) during antipsychotic treatment; and iii. for whom the dose of antipsychotic medication had been stable for one month or more before the trial (the same applies for those free of antipsychotics).
Types of interventions
A. Noradrenergic drugs
i. Celiprolol, clonidine, disulfiram, fusaric acid, methyldopa, pindolol, propanolol, oxprenolol or yohimbine, compared with placebo or no intervention. For the 2017 update a post hoc decision was made to also include studies evaluating the above‐mentioned noradrenergic drugs compared to any other intervention for the treatment of tardive dyskinesia.
B. Dopaminergic drugs
i. The dopamine receptor agonists (apomorphine, bromocriptine, CF25‐397, dopamine, hydergine, lisuride); ii. the dopamine receptor antagonists (AMTP, oxiperomide, metoclopramide, papaverine, tiapride); iii. the dopamine‐depleting drugs (oxypertine, reserpine, tetrabenazine); iv. drugs that increase the release (amantadine, amphetamine) or production (L‐dopa) of dopamine; all compared with placebo or no intervention. For the 2017 update a post hoc decision was made to also include studies evaluating the above mentioned dopaminergic drugs compared to any other intervention for the treatment of tardive dyskinesia.
Types of outcome measures
We have defined clinical efficacy as an improvement in the symptoms of TD of more than 50%, on any scale. We grouped outcomes into short term (less than six weeks), medium term (between six weeks and six months) and long term (more than six months).
Primary outcomes
1. Tardive dyskinesia
No clinically important improvement in the symptoms of individuals, defined as more than 50% improvement on any tardive dyskinesia scale ‒ any time period.
2. Adverse effects
No clinically significant extrapyramidal adverse effects ‒ any time period.
Secondary outcomes
1. Tardive dyskinesia (TD)
1.1 Any improvement in the symptoms of individuals on any TD scale, as opposed to no improvement. 1.2 Deterioration in the symptoms of individuals, defined as any deleterious change on any TD scale. 1.3 Average change in severity of TD during the trial period. 1.4 Average difference in severity of TD at the end of the trial.
2. General mental state changes
2.1 Deterioration in general psychiatric symptoms (such as delusions and hallucinations) defined as any deleterious change on any scale. 2.2 Average difference in severity of psychiatric symptoms at the end of the trial.
3. Acceptability of the treatment
3.1 Acceptability of the intervention to the participant group as measured by numbers of people dropping out during the trial.
4. Adverse effects
4.1 Use of any anti‐parkinsonism drugs. 4.2 Average score/change in extrapyramidal adverse effects. 4.3 Acute dystonia.
5. Other adverse effects, general and specific
6. Hospital and service utilisation outcomes
6.1 Hospital admission. 6.2 Average change in days in hospital. 6.3 Improvement in hospital status (for example: change from formal to informal admission status, use of seclusion, level of observation).
7. Economic outcomes
7.1 Average change in total cost of medical and mental health care. 7.2 Total indirect and direct costs.
8. Social confidence, social inclusion, social networks, or personalised quality of life measures
8.1. No significant change in social confidence, social inclusion, social networks, or personalised quality of life measures. 8.2 Average score/change in social confidence, social inclusion, social networks, or personalised quality of life measures.
9. Behaviour
9.1 Clinically significant agitation. 9.2 Use of adjunctive medication for sedation. 9.3 Aggression to self or others.
10. Cognitive state
10.1 No clinically important change. 10.2 No change, general and specific.
'Summary of findings' table
We used the GRADE approach to interpret findings (Schünemann 2011) and used GRADEpro to export data from this review to create 'Summary of findings' tables. These tables provide outcome‐specific information concerning the overall quality of evidence from each included study in the comparison, the magnitude of effects of interventions examined and the sum of available data on all outcomes rated as important to patient care and decision making. This summary was used to guide our conclusions. We selected the following main outcomes for inclusion in the 'Summary of findings' table.
1. Tardive dyskinesia 1.1 Improved to a clinically important extent 1.2 Deteriorated
2. Mental state 2.1 Deteriorated
3. Adverse effect 3.1 Any adverse event 3.2 Adverse effects: no clinically significant extrapyramidal adverse effects
4. Acceptability of treatment 4.1 Leaving the study early
5. Social confidence, social inclusion, social networks, or personalised quality of life measures* 5.1 No significant change in social confidence, social inclusion, social networks, or personalised quality of life measures for either recipients of care or caregivers
* Outcome designated important to patients. We wished to add perspectives from people’s personal experience with TD to the research agenda. A consultation with service users was planned where the previously published version of another review in the tardive dyskinesia series and a lay overview of that review gave the foundation for the discussions (Soares‐Weiser 2011; Table 5). The session was planned to provide time to reflect on current research on TD and consider gaps in knowledge. The report is published in the Health Technology Assessment (HTA) report for the UK National Institute of Health Research (Appendix 1, Bergman 2017). We have added one figure showing a service user's expression of frustration concerning this neglected area of research (Figure 1). Informed by the results of the consultation, for this review we updated outcomes for the 'Summary of findings' table.
1.
Message from one of the participants of the Public and patient involvement consultation of service user perspectives on tardive dyskinesia research.
Search methods for identification of studies
Electronic searches
The 2017 review update was carried out in parallel with updating eight other TD reviews; see Table 5 for details. The search covered all nine tardive dyskinesia reviews.
1. Cochrane Schizophrenia Group’s Register
We searched Cochrane Schizophrenia Group’s Study‐Based Register of Trials on 16 July 2015 and 26 April 2017 using the following string: *Tardive Dyskinesia* in Healthcare Condition Field of Study. In a study‐based register such as this, searching the major concept retrieves all the synonym keywords and relevant studies because all the studies have already been organised based on their interventions and linked to the relevant topics. The Cochrane Schizophrenia Group’s Register of Trials is compiled by systematic searches of major resources (including AMED, BIOSIS, CINAHL, Embase, MEDLINE, PsycINFO, PubMed, and registries of clinical trials) and their monthly updates, handsearches, grey literature, and conference proceedings (see Group’s Module). There is no language, date, document type, or publication status limitations for inclusion of records into the register.
3. Details of previous electronic searches
See Appendix 1.
Searching other resources
1. Reference searching
We inspected references of all identified studies for further relevant studies.
2. Personal contact
We contacted the first author of each included study for information regarding unpublished trials.
Data collection and analysis
Selection of studies
For the 2017 update, reviewers RA and AG (see Acknowledgements) inspected all abstracts of studies identified as above and identified potentially relevant reports. We resolved disagreement by discussion, or where there was still doubt, we acquired the full article for further inspection. We acquired the full articles of relevant reports/abstracts meeting initial criteria for reassessment and carefully inspected for a final decision on inclusion (see Criteria for considering studies for this review). RA and AG were not blinded to the names of the authors, institutions or journal of publication. Where difficulties or disputes arose, we asked author HB for help and where it was impossible to decide or if adequate information was not available to make a decision, we added these studies to those awaiting assessment and contacted the authors of the papers for clarification.
Data extraction and management
1. Extraction
For the 2017 update, reviewers RA and HB independently extracted data from all included studies. Again, we discussed any disagreement and documented decisions. With remaining problems KSW helped clarify issues and we documented these final decisions. We extracted data presented only in graphs and figures whenever possible, but included only if two reviewers independently had the same result. We attempted to contact authors through an open‐ended request in order to obtain missing information or for clarification whenever necessary. If studies were multi‐centre, where possible we extracted data relevant to each component centre separately.
2. Management
2.1 Forms
For the 2017 update we extracted data online in Covidence. Extracted data are available here with a link to the original source PDF for each item.
2.2 Scale‐derived data
We included continuous data from rating scales only if: a) the psychometric properties of the measuring instrument have been described in a peer‐reviewed journal (Marshall 2000); and b) the measuring instrument has not been written or modified by one of the trialists for that particular trial. Ideally the measuring instrument should either be i. a self‐report or ii. completed by an independent rater or relative (not the therapist). We realise that this is not often reported clearly; we noted in Description of studies if this was the case or not.
2.3 Endpoint versus change data
There are advantages of both endpoint and change data. Change data can remove a component of between‐person variability from the analysis. On the other hand calculation of change needs two assessments (baseline and endpoint) which can be difficult in unstable and difficult‐to‐measure conditions such as schizophrenia. We decided to primarily use endpoint data, and only use change data if the former were not available. We combined endpoint and change data in the analysis as we preferred to use mean differences (MD) rather than standardised mean differences throughout (Higgins 2011).
2.4 Skewed data
Continuous data on clinical and social outcomes are often not normally distributed. To avoid the pitfall of applying parametric tests to non‐parametric data, we applied the following standards to relevant data before inclusion (see (a), (b) and (c) below).
Please note: we entered data from studies of at least 200 participants in the analysis, because skewed data pose less of a problem in large studies. We also entered all relevant change data as when continuous data are presented on a scale that includes a possibility of negative values (such as change data), it is difficult to tell whether data are skewed or not.
For endpoint data from studies with fewer than 200 participants:
(a) when a scale starts from the finite number zero, we subtracted the lowest possible value from the mean, and divided this by the standard deviation. If this value was lower than 1, it strongly suggests a skew and we excluded these data. If this ratio was higher than 1 but below 2, there is suggestion of skew. We entered these data and tested whether their inclusion or exclusion changed the results substantially. Finally, if the ratio was larger than 2 we included these data, because skew is less likely (Altman 1996; Higgins 2011).
(b) if a scale starts from a positive value (such as the Positive and Negative Syndrome Scale (PANSS) (Kay 1986), which can have values from 30 to 210), we modified the calculation described above to take the scale starting point into account. In these cases skew is present if 2 SD > (S − S min), where S is the mean score and 'S min' is the minimum score.
2.5 Common measure
Where relevant, to facilitate comparison between trials we converted variables that can be reported in different metrics, such as days in hospital (mean days per year, per week or per month) to a common metric (e.g. mean days per month).
2.6 Conversion of continuous to binary
Where possible, we converted continuous outcome measures to dichotomous data. This can be done by identifying cut‐off points on rating scales and dividing participants accordingly into 'clinically improved' or 'not clinically improved'. It is generally assumed that if there is a 50% reduction in a scale‐derived score such as the Brief Psychiatric Rating Scale (BPRS, Overall 1962) or the Positive and Negative Syndrome Scale (PANSS, Kay 1986), this can be considered as a clinically significant response (Leucht 2005a; Leucht 2005b). If data based on these thresholds were not available, we used the primary cut‐off presented by the original authors.
Assessment of risk of bias in included studies
Reviewers RA (see Acknowledgements) and HB independently assessed risk of bias within the included studies by using criteria described in the Cochrane Handbook for Systematic Reviews of Interventions to assess trial quality (Higgins 2011). This set of criteria is based on evidence of associations between overestimate of effect and high risk of bias of the article such as sequence generation, allocation concealment, blinding, incomplete outcome data and selective reporting.
If the raters disagreed, we made the final rating by consensus, with the involvement of another member of the review group. Where inadequate details of randomisation and other characteristics of trials were provided, we contacted authors of the studies in order to obtain further information. If non‐concurrence occurred, we reported this.
We noted the level of risk of bias in the text of the review and in Figure 2, Figure 3, Table 1 and Table 3.
2.
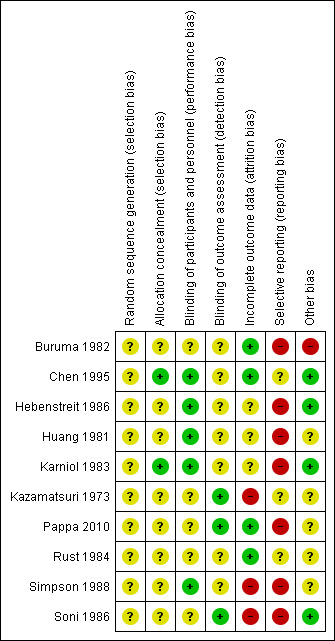
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
3.
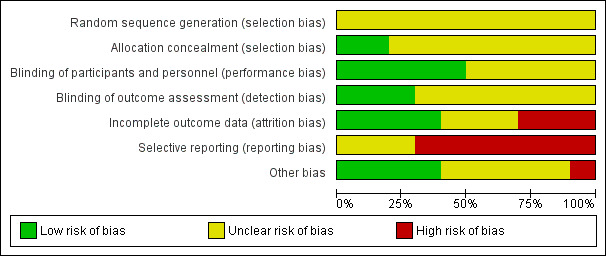
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Summary of findings for the main comparison. NORADRENERGIC DRUGS compared to PLACEBO for antipsychotic‐induced tardive dyskinesia.
| NORADRENERGIC DRUGS compared to PLACEBO for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: patients with antipsychotic‐induced tardive dyskinesia Settings: inpatients in Austria and the USA Intervention: NORADRENERGIC DRUGS (alpha‐methyldopa, celiprolol) Comparison: PLACEBO | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| PLACEBO | NORADRENERGIC DRUGS | |||||
|
Tardive dyskinesia: No clinically important improvement follow‐up: 2 weeks |
1000 per 1000 | 330 per 1000 (140 to 800) | RR 0.33 (0.14 to 0.80) | 20 (1 study) | ⊕⊕⊝⊝ low1,2 | The included study evaluated alpha‐methyldopa. |
|
Tardive dyskinesia: deterioration follow‐up: 2 weeks |
100 per 1000 | 33 per 1000 (2 to 732) | RR 0.33 (0.02 to 7.32) | 20 (1 study) | ⊕⊝⊝⊝ very low1,3 | The included study evaluated alpha‐methyldopa. |
| Adverse events ‐ not reported | See comment | See comment | Not estimable | 0 (0) | See comment | We found no studies rating this outcome. |
| Mental state ‐ not reported | See comment | See comment | Not estimable | 0 (0) | See comment | We found no studies rating this outcome. |
|
Acceptability of treatment: Leaving the study early follow‐up: 13 weeks |
0 per 1000 | 0 per 1000 (0 to 0) | RR 5.28 (0.27 to 102.58) | 35 (1 study) | ⊕⊝⊝⊝ very low1,3 | The included study evaluated celiprolol. |
|
No improvement in quality of life follow‐up: 13 weeks |
944 per 1000 | 822 per 1000 (642 to 1000) | RR 0.87 (0.68 to 1.12) | 35 (1 study) | ⊕⊝⊝⊝ very low1,3 | The included study evaluated celiprolol. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for risk of bias: unclear whether randomisation procedure and allocation concealment were carried out adequately, blinding of outcome assessors was not described. 2 Downgraded one step for imprecision: few events and small sample size. 3 Downgraded two steps for imprecision: few events, small sample size and wide CI that includes both no effect and appreciable benefit for intervention group. 4 Downgraded one level for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability.
Summary of findings 3. DOPAMINERGIC DRUGS compared to PLACEBO for antipsychotic‐induced tardive dyskinesia.
| DOPAMINERGIC DRUGS compared to PLACEBO for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: patients with antipsychotic‐induced tardive dyskinesia Settings: inpatients in the UK and the USA Intervention: DOPAMINERGIC DRUGS (carbidopa/levodopa, oxypertine, reserpine) Comparison: PLACEBO | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| PLACEBO | DOPAMINERGIC DRUGS | |||||
|
Tardive dyskinesia: No clinically important improvement follow‐up: 2 weeks |
1000 per 1000 | 520 per 1000 (290 to 960) | RR 0.52 (0.29 to 0.96) | 20 (1 study) | ⊕⊕⊝⊝ low1,2 | The included study evaluated reserpine. |
|
Tardive dyskinesia: Deterioration follow‐up: 2‐6 weeks |
167 per 1000 | 197 per 1000 (58 to 665) | RR 1.18 (0.35 to 3.99) | 37 (2 studies) | ⊕⊝⊝⊝ very low1,3 | The included studies evaluated reserpine and carbidopa/levodopa. |
| Adverse events ‐ not reported | See comment | See comment | Not estimable | 0 (0) | See comment | We found no studies rating this outcome. |
|
General mental state: Deterioration follow‐up: 24 weeks |
45 per 1000 | 100 per 1000 (10 to 1000) | RR 2.2 (0.22 to 22.45) | 42 (1 study) | ⊕⊝⊝⊝ very low3,4 | The included study evaluated oxypertine. |
|
Acceptability of treatment: Leaving the study early follow‐up: 2‐24 weeks |
111 per 1000 | 143 per 1000 (72 to 282) | RR 1.29 (0.65 to 2.54) | 163 (6 studies) | ⊕⊝⊝⊝ very low3,5,6,7 | Only two studies (59 participants) evaluating carbidopa/levodopa and oxypertine reported any events for this outcome. 4 studies evaluating amantadine, bromocriptine, and tiapride reported no events and consequently no estimates could be made for these 3 compounds. |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | See comment | See comment | Not estimable | 0 (0) | See comment | This outcome was designated to be of importance, especially to patients. We found no studies rating this outcome. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for risk of bias: unclear whether randomisation procedure and allocation concealment were carried out adequately, blinding of outcome assessors was not described. 2 Downgraded one step for imprecision: few events and small sample size. 3 Downgraded two steps for imprecision: few events, small sample size and wide CI that includes both no effect and appreciable benefit for intervention group. 4 Downgraded one step for risk of bias: unclear whether randomisation procedure and allocation concealment were carried out adequately, attrition was high (45%). 5 Downgraded one step for risk of bias: unclear whether randomisation procedure and allocation concealment were carried out adequately, attrition was high (45%) or unbalanced between groups (25% vs. 0%). 6 Downgraded one step for inconsistency: statistical heterogeneity was high (I² = 58%). 7 Downgraded one step for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability.
Measures of treatment effect
1. Binary data
For binary outcomes we calculated a standard estimation of the risk ratio (RR) and its 95% confidence interval (CI). It has been shown that RR is more intuitive than odds ratios (Boissel 1999), as odds ratios tend to be interpreted as RR by clinicians (Deeks 2000).
2. Continuous data
For continuous outcomes we estimated mean difference (MD) between groups. We preferred not to calculate effect size measures (standardised mean difference (SMD)). However, if scales of very considerable similarity were used, we presumed there is a small difference in measurement, and calculated effect size and transformed the effect back to the units of one or more of the specific instruments.
Unit of analysis issues
1. Cluster trials
Studies increasingly employ 'cluster randomisation' (such as randomisation by clinician or practice) but analysis and pooling of clustered data poses problems. Firstly, authors often fail to account for intra‐class correlation in clustered studies, leading to a 'unit of analysis' error whereby P values are spuriously low, confidence intervals unduly narrow and statistical significance overestimated (Divine 1992). This causes type I errors (Bland 1997; Gulliford 1999).
If any of the included trials had randomised participants by clusters, and where clustering is not accounted for in primary studies, we would have presented such data in a table, with a (*) symbol to indicate the presence of a probable unit of analysis error. In subsequent versions of this review we will seek to contact first authors of studies to obtain intra‐class correlation coefficients for their clustered data and to adjust for this by using accepted methods (Gulliford 1999). Where clustering has been incorporated into the analysis of primary studies, we will present these data as if from a non‐cluster randomised study, but adjust for the clustering effect.
We have sought statistical advice and have been advised that the binary data as presented in a report should be divided by a 'design effect'. This is calculated using the mean number of participants per cluster (m) and the intra‐class correlation coefficient (ICC) (Design effect = 1 + (m − 1) * ICC] (Donner 2002)). If the ICC is not reported it will be assumed to be 0.1 (Ukoumunne 1999).
If cluster studies have been appropriately analysed taking into account intra‐class correlation coefficients and relevant data documented in the report, synthesis with other studies would be possible using the generic inverse variance technique.
2. Cross‐over trials
A major concern of cross‐over trials is the carry‐over effect. It occurs if an effect (pharmacological, physiological or psychological) of the treatment in the first phase is carried over to the second phase. As a consequence on entry to the second phase the participants can differ systematically from their initial state despite a wash‐out phase. For the same reason cross‐over trials are not appropriate if the condition of interest is unstable (Elbourne 2002). As both effects are very likely in severe mental illness, we only used data of the first phase of cross‐over studies.
3. Studies with multiple treatment groups
Where a study involves more than two treatment arms, if relevant we presented the additional treatment arms in comparisons. If data were binary we simply added and combined within the two‐by‐two table. If data were continuous we combined data following the formula in section 7.7.3.8 (Combining groups) of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We did not use data where the additional treatment arms were not relevant.
Dealing with missing data
1. Overall loss of credibility
At some degree of loss to follow‐up, data must lose credibility (Xia 2009). We chose that, for any particular outcome, should more than 50% of data be unaccounted for, we would not reproduce these data or use them within analyses. If, however, more than 50% of those in one arm of a study were lost, but the total loss was less than 50%, we addressed this within the 'Summary of findings' table/s by down‐rating quality. We also downgraded quality within the 'Summary of findings' table/s should loss be 25% to 50% in total.
2. Binary
In the case where attrition for a binary outcome is between 0% and 50% and where these data are not clearly described, we presented data on a 'once‐randomised‐always‐analyse' basis (an intention‐to‐treat analysis). We assumed all those leaving the study early had no improvement. We undertook a sensitivity analysis testing how prone the primary outcomes were to change by comparing data only from people who completed the study to that point to the intention‐to‐treat analysis using the above assumptions.
3. Continuous
3.1 Attrition
We reported and used data where attrition for a continuous outcome was between 0% and 50%, and data only from people who completed the study to that point were reported.
3.2 Standard deviations
If standard deviations were not reported, we first tried to obtain the missing values from the authors. If not available, where there were missing measures of variance for continuous data, but an exact standard error and confidence intervals available for group means, and either P value or t value available for differences in mean, we calculated them according to the rules described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011): when only the standard error (SE) is reported, standard deviations (SDs) are calculated by the formula SD = SE * √(n). Chapters 7.7.3 and 16.1.3 of the Cochrane Handbook for Systematic Reviews of Interventions present detailed formulae for estimating SDs from P, t or F values, confidence intervals, ranges or other statistics (Higgins 2011). If these formulae did not apply, we calculated the SDs according to a validated imputation method which is based on the SDs of the other included studies (Furukawa 2006). Although some of these imputation strategies can introduce error, the alternative would be to exclude a given study’s outcome and thus to lose information. We nevertheless examined the validity of the imputations in a sensitivity analysis excluding imputed values.
3.3 Assumptions about participants who left the trials early or were lost to follow‐up
Various methods are available to account for participants who left the trials early or were lost to follow‐up. Some trials just present the results of study completers; others use the method of last observation carried forward (LOCF); while more recently, methods such as 'multiple imputation' or 'mixed effects' models for repeated measurements (MMRM) have become more of a standard. While the last two methods seem to be somewhat better than LOCF (Leon 2006), we feel that the high percentage of participants leaving the studies early and differences in the reasons for leaving the studies early between groups is often the core problem in randomised schizophrenia trials. We therefore did not exclude studies which used the statistical approach. However, we preferred to use the more sophisticated approaches (e.g. MMRM or 'multiple imputation') and only presented completer analyses if some kind of ITT data were not available at all. Moreover, we addressed this issue in the item 'Incomplete outcome data' of the 'Risk of bias' tool.
Assessment of heterogeneity
1. Clinical heterogeneity
We considered all included studies initially, without seeing comparison data, to judge clinical heterogeneity. We simply inspected all studies for clearly outlying people or situations which we had not predicted would arise; and discussed in the text if they arose.
2. Methodological heterogeneity
We considered all included studies initially, without seeing comparison data, to judge methodological heterogeneity. We simply inspected all studies for clearly outlying methods which we had not predicted would arise; and discussed in the text if they arose.
3. Statistical heterogeneity
3.1 Visual inspection
We visually inspected graphs to investigate the possibility of statistical heterogeneity.
3.2 Employing the I² statistic
We investigated heterogeneity between studies by considering the I² method alongside the Chi² P value. The I² provides an estimate of the percentage of inconsistency thought to be due to chance (Higgins 2003). The importance of the observed value of I² depends on i. magnitude and direction of effects and ii. strength of evidence for heterogeneity (e.g. P value from Chi² test, or a confidence interval for I²). An I² estimate greater than or equal to around 50% accompanied by a statistically significant Chi² statistic can be interpreted as evidence of substantial levels of heterogeneity (Section 9.5.2 Cochrane Handbook for Systematic Reviews of Interventions;Higgins 2011). We explored and discussed in the text potential reasons for substantial levels of heterogeneity (Subgroup analysis and investigation of heterogeneity).
Assessment of reporting biases
Reporting biases arise when the dissemination of research findings is influenced by the nature and direction of results (Egger 1997). These are described in Section 10 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We are aware that funnel plots may be useful in investigating reporting biases but are of limited power to detect small‐study effects. We did not use funnel plots for outcomes where there are 10 or fewer studies, or where all studies were of similar sizes. If funnel plots are possible in future versions of this review, we will seek statistical advice in their interpretation.
Data synthesis
We understand that there is no closed argument for fixed‐effect over random‐effects models, or vice versa. The random‐effects method incorporates an assumption that the different studies are estimating different, yet related, intervention effects. This often seems to be true to us and the random‐effects model takes into account differences between studies even if there is no statistically significant heterogeneity. There is, however, a disadvantage to the random effects model: it puts added weight onto small studies which often are the most biased ones. Depending on the direction of effect these studies can either inflate or deflate the effect size. We chose the fixed‐effect model for all analyses.
Subgroup analysis and investigation of heterogeneity
1. Subgroup analyses
1.1 Type of compound
As different non‐antipsychotic catecholaminergic compounds may have differential effects on antipsychotic‐induced tardive dyskinesia, we performed a subgroup analysis to compare the effects of different non‐antipsychotic catecholaminergic drugs. We proposed to undertake comparisons only for primary outcomes to minimise the risk of multiple comparisons.
1.2 Duration of treatment
We also anticipated a sub‐group analysis to examine whether any improvement occurred with short periods of intervention (less than six weeks); and if this did occur, whether this effect was maintained at longer periods of follow‐up.
1.3 Clinical state, stage or problem: recent onset TD
We proposed to undertake this review and provide an overview of the effects of non‐antipsychotic catecholaminergic drugs for people with schizophrenia in general. In addition, however, we tried to report data on subgroups of people in the same clinical state, stage and with similar problems. We anticipated testing the hypothesis that the use of non‐antipsychotic catecholaminergic drugs is most effective for those with more recent onset TD (less than five years). We had hoped to present data for this subgroup for the primary outcomes.
2. Investigation of heterogeneity
We reported when inconsistency was high. First we investigated whether data were entered correctly. Second, if data were correct, we visually inspected the graph and successively removed studies from the rest to see if homogeneity was restored. For this review we decided that should this occur with data contributing to the summary finding of no more than around 10% of the total weighting, we would present data. If not, we did not pool such data and discussed issues. We know of no supporting research for this 10% cut‐off but we are investigating use of prediction intervals as an alternative to this unsatisfactory state.
When unanticipated clinical or methodological heterogeneity were obvious, we simply discussed. We did not undertake sensitivity analyses relating to these.
Sensitivity analysis
1. Implication of randomisation
If trials were described in some way as to imply randomisation we undertook sensitivity analyses for the primary outcomes. We included these studies in the analyses and if there was no substantive difference when the implied randomised studies were added to those with better description of randomisation, then we used relevant data from these studies.
2. Assumptions for lost binary data
Where assumptions had to be made regarding people lost to follow‐up (see Dealing with missing data) we compared the findings of the primary outcomes when we used our assumption compared with completer data only. If there was a substantial difference, we reported and discussed these results but continued to employ our assumption.
Where assumptions have to be made regarding missing SDs data (see Dealing with missing data), we compared the findings on primary outcomes when we used our assumption with completer data only. We undertook a sensitivity analysis, testing how prone results were to change when 'completer' data only were compared to the imputed data using the above assumption. If there was a substantial difference, we reported and discussed these results but continued to employ our assumption.
3. Risk of bias
We analysed the effects of excluding trials that we judged to be at high risk of bias across one or more of the domains of randomisation (implied as randomised with no further details available), allocation concealment, blinding and outcome reporting for the meta‐analysis of the primary outcome. If the exclusion of trials at high risk of bias did not substantially alter the direction of effect or the precision of the effect estimates, we included data from these trials in the analysis.
4. Imputed values
Had cluster trials been included, we would have undertaken a sensitivity analysis to assess the effects of including data from trials where we used imputed values for ICC in calculating the design effect.
If we found substantial differences in the direction or precision of effect estimates in any of the sensitivity analyses listed above, we did not pool data from the excluded trials with the other trials contributing to the outcome, but presented them separately
5. Fixed and random effects
We synthesised data using a fixed‐effect model; however, we also synthesised data for the primary outcome using a random‐effects model to evaluate whether this altered the significance of the results.
Results
Description of studies
Please see Characteristics of included studies, Characteristics of excluded studies and Characteristics of studies awaiting classification.
Results of the search
The 2015 and 2017 update searches were part of an update search of nine Cochrane Reviews; see Table 5. The 2015 search retrieved 704 references for 344 studies; see Figure 4 for study flow diagram. After having excluded irrelevant references at title and abstract screening, we screened full texts of 71 references (58 studies). Forty‐eight studies (57 references) were excluded, and 29 of these are new excluded studies for the 2017 update. Two studies were awaiting assessment in the previous version of the review and have since been assessed in Chinese and Portuguese, found to have met inclusion criteria, and included (Chen 1995; Karniol 1983). Another six new studies were included from the 2015 search (Huang 1981; Kazamatsuri 1973; Pappa 2010; Rust 1984; Simpson 1988; Soni 1986). Ten studies are now included in this review.
4.
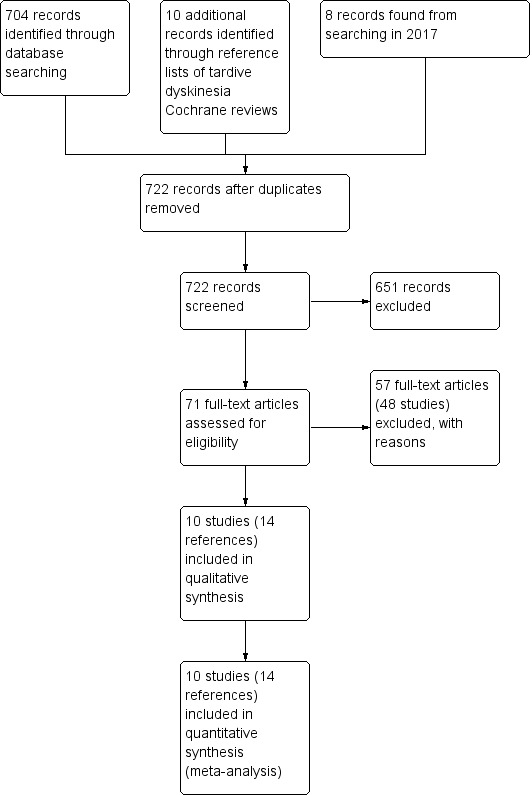
Study flow diagram for 2015 and 2017 searching
The 2017 search found eight records (five studies). The Editorial base of Cochrane Schizophrenia screened these records and no new studies were relevant to this review. They could be relevant to the other reviews in this series of TD reviews (see Table 5), and have been put into 'Studies awaiting classification' of the Soares‐Weiser 2006 miscellaneous treatments review.
Included studies
Overall the review now includes 10 studies with 261 participants published between 1973 and 2010. Eight of these studies were added at the 2017 update (Chen 1995; Huang 1981; Karniol 1983; Kazamatsuri 1973; Pappa 2010; Rust 1984; Simpson 1988; Soni 1986).
1. Methods
All studies were stated to be randomised and double blind. For further details, please see sections below on Allocation (selection bias) and Blinding (performance bias and detection bias).
2. Design
All included studies presented a parallel longitudinal design. Three of the 10 studies used a cross‐over design with two periods (Buruma 1982; Chen 1995; Pappa 2010). We had considered this possibility when embarking on the review and have used only the data from before the first cross‐over for the reasons outlined above (see Unit of analysis issues).
3. Duration
Treatment phases of five studies were of short duration (2 to 5 weeks) (Buruma 1982; Chen 1995; Huang 1981; Karniol 1983; Pappa 2010); and treatment phases of the remaining five studies were of medium duration (6 to 24 weeks) (Hebenstreit 1986; Kazamatsuri 1973; Rust 1984; Simpson 1988; Soni 1986).
4. Participants
Participants, now totalling 261 people, were mostly men in their 50s, with diagnoses of various chronic psychiatric disorders, but mainly schizophrenia. All had antipsychotic‐induced tardive dyskinesia (TD), though only four studies reported the specific diagnostic criteria used (Hebenstreit 1986; Pappa 2010; Simpson 1988; Soni 1986). The number of participants ranged from 12 to 50 (median 21).
5. Setting
One trial was conducted with outpatients in Greece (Pappa 2010); and the rest with psychiatric inpatients in the USA (Huang 1981; Kazamatsuri 1973; Simpson 1988), Austria (Hebenstreit 1986), Brazil (Karniol 1983), China (Chen 1995), France (Rust 1984), the Netherlands (Buruma 1982), and the UK (Soni 1986).
6. Interventions
6.1 Noradrenergic drugs
6.1.1 Alpha‐methyldopa
Huang 1981 used alpha‐methyldopa in a dose ranging from 750 to 1500 mg/day. Methyldopa inhibits dopamine production and is also an adrenergic receptor agonist, and is used to treat hypertension and pregnancy‐induced hypertension.
6.1.2 Celiprolol
Hebenstreit 1986 used celiprolol in a 200 mg/day dose. Celiprolol is a cardioselective beta blocker reported to possess intrinsic sympathomimetic activity and direct vasodilator activity. Celiprolol is used as the hydrochloride in the management of hypertension and angina pectoris.
6.2 Dopaminergic drugs
6.2.1 Amantadine
Pappa 2010 used amantadine in a dose of 100 mg/day. Amantadine is a glutamate receptor antagonist and anticholinergic that increases dopamine release and blocks dopamine reuptake. It can be used both as an antiviral and antiparkinsonian drug.
6.2.2 Bromocriptine
Chen 1995 used bromocriptine one capsule twice per day (exact dose unknown). Bromocriptine is a dopamine agonist used to treat various conditions including pituitary tumours, Parkinson's disease, type 2 diabetes, and cocaine withdrawal.
6.2.3 Carbidopa/levodopa (L‐dopa)
Simpson 1988 used carbidopa/levodopa in a dose of 50/350 mg/day. Karniol 1983 used levodopa in a dose ranging from 500 mg to 2000 mg. Carbidopa is used in Parkinson's disease in combination with levodopa to make levodopa more accessible. L‐dopa is the precursor to the catecholaminergic neurotransmitters dopamine, noradrenaline and adrenaline. L‐dopa can also be manufactured and is used as a drug to treat Parkinson's disease.
6.2.4 Oxypertine
Soni 1986 used oxypertine in a dose ranging from 80 mg/day to 240 mg/day. Oxypertine is a dopamine depleter drug used in the treatment of mania, disturbed behaviour, psychosis and schizophrenia.
6.2.5 Reserpine
Huang 1981 used reserpine in a dose ranging from 0.75 to 1.5 mg/day. Reserpine is a dopamine depleter drug that has been used in the past to treat psychosis and hypertension. Today it is mainly used as a horse tranquilliser.
6.2.6 Tetrabenazine
Kazamatsuri 1973 used tetrabenazine in a dose ranging from 50 mg to 200 mg/day. Tetrabenazine is a dopamine depleter drug approved to treat symptoms of Huntington's disease chorea.
6.2.7 Tiapride
Two studies used tiapride in a dose ranging from 300 mg to 600 mg/day (Buruma 1982; Rust 1984). Tiapride is a substituted benzamide with general properties similar to those of the antipsychotic sulpiride. It is usually given as the hydrochloride in the management of behavioural disorders and to treat dyskinesias. Tiapride has been tried in the treatment of Tourette's syndrome and chorea such as Huntington's chorea.
6.3 Comparison group
In most of the studies a placebo was used as a comparison group, with no further details given. In one study the comparison group was haloperidol (Kazamatsuri 1973). Another trial compared groups with different doses of L‐dopa and placebo (Karniol 1983); and Huang 1981 included three arms: celiprolol (noradrenergic), reserpine (dopamine depleter) and placebo.
Participants remained on stable schizophrenia treatment antipsychotic medication during the trials.
7. Outcomes
7.1 General
Some outcomes were presented in graphs, inexact P values of differences, or a statement of significant or non‐significant difference. This made it impossible to acquire raw data for synthesis. Some continuous outcomes could not be extracted due to missing number of participants or missing means, standard deviations, or standard errors.
7.2 Scales used to measure TD symptoms
We have shown details of the scales that provided usable data below. We have provided reasons for exclusions of data under 'Outcomes' in the Characteristics of included studies table.
7.2.1 Abnormal Involuntary Movement Scale (AIMS)
Simpson 1988 reported using AIMS to assess TD symptoms, and Hebenstreit 1986 reported using SKAUB, the German version of AIMS. The AIMS is a 12‐item scale consisting of a standardised examination followed by questions rating the orofacial, extremity and trunk movements, as well as three global measurements (Guy 1976). Each of these 10 items can be scored from 0 (none) to 4 (severe). Two additional items assess dental status. The AIMS ranges from 0 to 40, with higher scores indicating greater severity.
7.2.2 Extrapyramidal Bilan scale (EBS)
Karniol 1983 used the EBS. The EBS is a nine‐item rating scale for use by neurologists, to measure severity of symptoms such as facial mask, tremor, rigidity, akathisia, dystonia, dyskinesia and others (Tetreault 1969). Each item can be scored from 0 to 3, such that the overall score can range from 0 (no symptoms) to a possible 27 (severe symptoms of all types).
7.2.3 Clinical assessment
Two studies reported using a frequency count of mouth movements, performed by a psychiatrist, to assess oral dyskinesia (Huang 1981; Kazamatsuri 1973).
Excluded studies
There are 48 excluded studies (57 references). Thirteen studies were not randomised and we therefore excluded them (Asher 1981; Chouza 1982; Delwaide 1980; Fahn 1983; Ferrari 1972; Gerlach 1976; Kazamatsuri 1972; Konig 1996; Leblhuber 1987; Levy 1984; Ringwald 1978; Rondot 1987; Smith 1977). Seven RCTs did not meet inclusion criteria because they recruited participants without tardive dyskinesia (Adler 1990; DiMascio 1976; Fann 1976; Gutierrez 1979; NCT00310661 2006; NCT00845000 2009; O'Suilleabhain 2003). Participants in two RCTs were not on stable antipsychotic medication before and during the study and were consequently not eligible for inclusion (Jankovic 1982; Lieberman 1989). Two RCTs evaluated selegiline, an intervention that is not relevant for this review: Goff 1993 is included in the update of the 'Miscellaneous treatments for antipsychotic‐induced tardive dyskinesia' Cochrane Review (Soares‐Weiser 2003); and Stearns 1996 also reported no usable data so was excluded from the Soares‐Weiser 2003 review as well as from this review.
Twenty‐four studies had to be excluded because data were all unusable, in 18 of these as a result of failure to report outcomes from the first phase before cross‐over. We contacted authors of six of these 18 studies but received no reply (Doongaji 1982; Hemnani 1982; Jeste 1983; Lieberman 1988; Nasrallah 1986; Tamminga 1980); and since they were all published over 25 years ago and we assumed we would be very unlikely to receive a reply with data so many years later, they were excluded. We did not identify up‐to‐date contact details of authors for 12 of 18 cross‐over studies and decided to also exclude them as they were published 20 to 45 years ago and again we assumed we would be very unlikely to receive a reply with data so many years later (Angus 1997; Auberger 1985; Bateman 1979; Braun 1989; Browne 1986a; Chien 1978; Delwaide 1979; Freeman 1980; Gardos 1979; Glover 1980; Godwin Austen 1971; Viukari 1975). No usable outcome data were reported in the six remaining studies. We contacted authors of Alpert 1983 and Diehl 1999 but received no reply. We could not identify up‐to‐date contact details for authors of Greendyke 1988, Ludatscher 1989, Reker 1982 and Silver 1995. These six studies were also excluded as they were published 15 to 30 years ago and again we assumed we would be very unlikely to receive a reply with data so many years later.
See Characteristics of excluded studies for more details on each excluded study.
Studies awaiting classification
There are currently no studies awaiting classification.
Ongoing studies
As far as we are aware, there are currently no ongoing studies.
Risk of bias in included studies
Please refer to Figure 2 and Figure 3 for graphical overviews of the risk of bias in the included studies, and Characteristics of included studies for details.
Allocation
Reporting of randomisation and allocation concealment was poor overall. No study explicitly reported the method for sequence generation other than using the word "randomized" and consequently all studies were rated at unclear risk of bias for sequence generation. Only two studies were rated at low risk of bias for allocation concealment. Chen 1995 reported the allocation of participants by an external site while Karniol 1983 used sealed opaque envelopes. The remaining studies were rated at unclear risk of bias for allocation concealment.
Blinding
Although all studies were stated to be conducted on a double‐blind basis, not all explicitly described how this was undertaken and none tested the blindness of raters, clinicians and trial participants. Chen 1995, Hebenstreit 1986, Karniol 1983, Pappa 2010 and Simpson 1988 described how the participants and personnel were blinded and were rated at low risk of performance bias. Kazamatsuri 1973, Pappa 2010, and Soni 1986 described how the raters were blinded and were rated at low risk of detection bias. The remaining studies were rated at unclear risk of performance or detection bias, or both.
Incomplete outcome data
In four studies all randomised participants completed the study and were included in analyses; these were rated at low risk of attrition bias (Buruma 1982; Chen 1995; Pappa 2010; Rust 1984). Three studies did not report fully on attrition and were at unclear risk of bias (Hebenstreit 1986; Huang 1981; Karniol 1983). Three studies had 30% or greater loss to follow‐up (Soni 1986), or unbalanced loss to follow‐up between groups (Kazamatsuri 1973; Simpson 1988), and did not report outcomes for participants lost to follow‐up. These studies were rated at high risk of attrition bias. In all cases, however, we tried to ensure that every person randomised was analysed.
Selective reporting
Data in this review originates from published reports. Expected outcomes (impact on tardive dyskinesia symptoms, adverse events) were not reported sufficiently for most of the trials. In addition, we have had no opportunity to see protocols of these trials to compare the outcomes reported in the full publications with what was planned and measured during the conduct of the trial. Three studies were rated at unclear risk of reporting bias as it was unclear whether all outcomes were fully reported (Chen 1995; Kazamatsuri 1973; Rust 1984). The remaining seven studies were at high risk of reporting bias as they failed to fully report all measured outcomes.
Other potential sources of bias
All studies had small or very small sample sizes. Three of the studies used a cross‐over design (Buruma 1982; Chen 1995; Pappa 2010); four of the studies had the drugs used in the trials provided by pharmaceutical companies (Buruma 1982; Kazamatsuri 1973; Simpson 1988; Soni 1986); and in six studies no details of funding were given (Chen 1995; Hebenstreit 1986; Huang 1981; Karniol 1983; Pappa 2010; Rust 1984).
Nevertheless, we rated four studies at low risk bias as they seemed to be free from other sources of bias and baseline characteristics were balanced between groups (Chen 1995; Hebenstreit 1986; Karniol 1983; Soni 1986). Five studies were at unclear risk of other bias as insufficient information was available to make a judgement otherwise (Huang 1981; Kazamatsuri 1973; Pappa 2010; Rust 1984; Simpson 1988). Finally, Buruma 1982 was at high risk of other bias as the placebo group contained participants more severely affected by TD at baseline.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4
Summary of findings 2. NORADRENERGIC DRUGS compared to DOPAMINERGIC DRUGS for antipsychotic‐induced tardive dyskinesia.
| NORADRENERGIC DRUGS compared to DOPAMINERGIC DRUGS for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: patients with antipsychotic‐induced tardive dyskinesia Setting: inpatients in the USA Intervention: NORADRENERGIC DRUGS (alpha‐methyldopa) Comparison: DOPAMINERGIC DRUGS (reserpine) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with DOPAMINERGIC DRUGS | Risk with NORADRENERGIC DRUGS | |||||
|
Tardive dyskinesia: No clinically important improvement follow‐up: 2 weeks |
Study population | RR 0.60 (0.19 to 1.86) | 20 (1 study) | ⊕⊝⊝⊝ very low1,2 | ||
| 500 per 1,000 | 300 per 1,000 (95 to 930) | |||||
|
Tardive dyskinesia: Deterioration follow‐up: 2 weeks |
Study population | not estimable | 20 (1 study) | ⊕⊝⊝⊝ very low1,3 | Among the 20 participants no events were reported. | |
| 0 per 1,000 | 0 per 1,000 (0 to 0) | |||||
|
Adverse events ‐ not reported |
See comment | See comment | not estimable | 0 (0) | See comment | We found no studies reporting on this outcome. |
|
Mental state ‐ not reported |
See comment | See comment | not estimable | 0 (0) | See comment | We found no studies reporting on this outcome. |
| Acceptability of treatment: Leaving the study early | See comment | See comment | not estimable | 0 (0) | See comment | We found no studies reporting on this outcome. |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | See comment | See comment | not estimable | 0 (0) | See comment | We found no studies reporting on this outcome. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded one step for risk of bias: unclear whether randomisation procedure and allocation concealment were carried out adequately. 2 Downgraded two steps for imprecision: few events, very small sample size, and wide CI that includes both appreciable benefit and appreciable harm for intervention group as well as no effect. 3 Downgraded two steps for imprecision: no events were reported, effect estimate cannot be calculated.
Summary of findings 4. DOPAMINERGIC DRUGS compared to OTHER DRUGS for antipsychotic‐induced tardive dyskinesia.
| DOPAMINERGIC DRUGS compared to OTHER DRUGS for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: patients with antipsychotic‐induced tardive dyskinesia Setting: inpatients in the USA Intervention: DOPAMINERGIC DRUGS (tetrabenazine) Comparison: OTHER DRUGS (haloperidol) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with OTHER DRUGS | Risk with DOPAMINERGIC DRUGS | |||||
|
Tardive dyskinesia: No clinically important improvement follow‐up: 18 weeks |
Study population | RR 0.93 (0.45 to 1.95) | 13 (1 study) | ⊕⊝⊝⊝ very low1,2 | ||
| 714 per 1000 | 664 per 1000 (321 to 1000) | |||||
|
Tardive dyskinesia: Deterioration follow‐up: 18 weeks |
Study population | RR 1.17 (0.09 to 14.92) | 13 (1 study) | ⊕⊝⊝⊝ very low1,2 | ||
| 143 per 1000 | 167 per 1000 (13 to 1,000) | |||||
|
Adverse events ‐ not reported |
See comment | See comment | not estimable | 0 (0) | See comment | We found no studies reporting on this outcome. |
|
Mental state ‐ not reported |
See comment | See comment | not estimable | 0 (0) | See comment | We found no studies reporting on this outcome. |
|
Acceptability of treatment: Leaving the study early follow‐up: 18 weeks |
Study population | RR 0.23 (0.01 to 4.00) | 13 (1 study) | ⊕⊝⊝⊝ very low1,2 | ||
| 286 per 1000 | 66 per 1000 (3 to 1,000) | |||||
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | See comment | See comment | not estimable | 0 (0) | See comment | We found no studies reporting on this outcome. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. | ||||||
1 Downgraded one step for risk of bias: unclear whether randomisation procedure and allocation concealment were carried out adequately. 2 Downgraded two steps for imprecision: few events, very small sample size, and wide CI that includes both appreciable benefit and appreciable harm for intervention group as well as no effect.
1. Comparison 1: noradrenergic drugs versus placebo
1.1 TD symptoms
We had chosen 'any improvement in TD symptoms of more than 50% on any TD scale – any time period' as a primary outcome. Although the data we found in trials did not fit this exactly we feel that the outcome 'not improved to a clinically important extent' fits best with what we had hoped to find.
1.1.1 Not improved to a clinically important extent
The overall results for 'clinically relevant improvement' found a significant benefit of alpha‐methyldopa over placebo after 2 weeks' treatment (low‐quality evidence, 1 trial, 20 people; RR 0.33, 95% CI 0.14 to 0.80; Analysis 1.1).
1.1. Analysis.
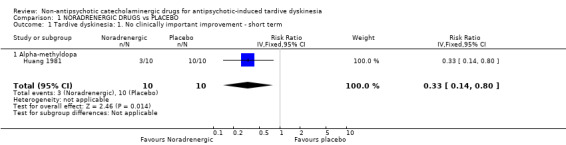
Comparison 1 NORADRENERGIC DRUGS vs PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term.
1.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms' we found no significant difference between noradrenergic drugs (alpha‐methyldopa, celiprolol) and placebo after 2 to 13 weeks' treatment (2 trials, 55 people; RR 0.91, 95% CI 0.65 to 1.27; I² = 0%, Analysis 1.2).
1.2. Analysis.
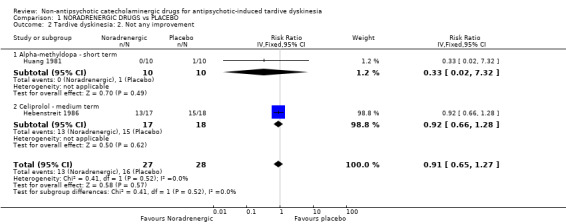
Comparison 1 NORADRENERGIC DRUGS vs PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement.
1.1.3 Deterioration of symptoms
There was no significant difference in deterioration of symptoms between people allocated to alpha‐methyldopa or placebo after 2 weeks' treatment (very low quality evidence, 1 trial, 20 people; RR 0.33, 95% CI 0.02 to 7.32; Analysis 1.3).
1.3. Analysis.
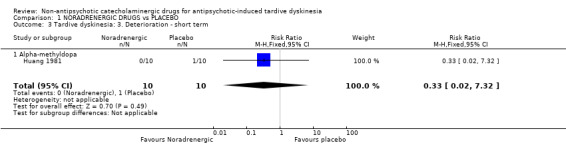
Comparison 1 NORADRENERGIC DRUGS vs PLACEBO, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ short term.
1.2 Leaving the study early
Using celiprolol did not significantly increase the chances of a person leaving the study early compared with placebo after 13 weeks' treatment (very low quality evidence, 1 trial, 35 people; RR 5.28, 95% CI 0.27 to 102.58; Analysis 1.4).
1.4. Analysis.
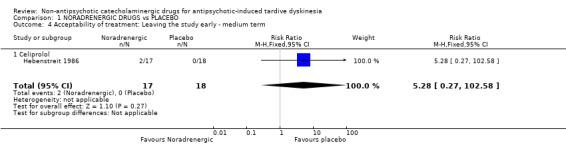
Comparison 1 NORADRENERGIC DRUGS vs PLACEBO, Outcome 4 Acceptability of treatment: Leaving the study early ‐ medium term.
1.3 Quality of life
There was no significant difference in quality of life between people allocated to celiprolol or placebo after 13 weeks' treatment (very low quality evidence, 1 trial, 35 people; RR 0.87, 95% CI 0.68 to 1.12; Analysis 1.5).
1.5. Analysis.
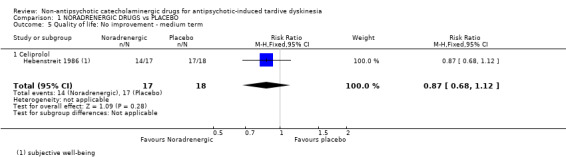
Comparison 1 NORADRENERGIC DRUGS vs PLACEBO, Outcome 5 Quality of life: No improvement ‐ medium term.
We did not identify any studies that reported on hospital and service utilisation outcomes, economic outcomes, behaviour, or cognitive state.
1.4 Subgroup analysis
1.4.1 Type of compound
There were no significant subgroup differences (I² = 0%, P = 0.52, Analysis 1.2) for alpha‐methyldopa versus placebo (RR 0.33, 95% CI 0.02 to 7.32; 20 participants, 1 study) and celiprolol versus placebo (RR 0.92, 95% CI 0.66 to 1.28; 35 participants, 1 study) on 'not any improvement in TD symptoms', the only outcome for this comparison that evaluated more than one non‐antipsychotic catecholaminergic compound.
1.4.2 Duration of follow‐up
Any effects that noradrenergic drugs may have did not clearly change in relation to duration of follow‐up compared with placebo.
1.4.3 Clinical stage: recent onset TD
It was not possible to evaluate whether those with recent onset TD responded differently to those with more established problems, since no trial reported data for groups with different durations of TD that could be extracted for separate analyses.
1.5 Heterogeneity
Data were homogeneous. We did not detect clinical, methodological or statistical heterogeneity as described in Assessment of heterogeneity.
1.6 Sensitivity analyses
1.6.1 Implication of randomisation
We aimed to include trials in a sensitivity analysis if they were described in some way as to imply randomisation. Only one study was included for the primary outcome: consequently this sensitivity analysis could not be performed.
1.6.2 Assumptions for lost binary data
The above results are based on data as presented in the original study reports, with the assumption that those who left early before the end of the trial had not improved (see Dealing with missing data). We planned to test the sensitivity of the results to this assumption, but all randomised participants were reported for the primary outcome 'no clinically important improvement in TD symptoms'. Therefore, we could not undertake this sensitivity analysis. If there had been a substantial difference, we would have reported results and discussed them but continued to employ our assumption.
1.6.3 Risk of bias
We planned to exclude trials that we judged to be at high risk of bias across one or more of the domains, but only one study was included for the primary outcome. Consequently this sensitivity analysis could not be performed.
1.6.4 Imputed values
We would have undertaken a sensitivity analysis to assess the effects of including data from cluster randomised trials where we used imputed values for ICC in calculating the design effect. No cluster randomised trials were included.
1.6.5 Fixed and random effects
We also synthesised data using a random effects model. This did not alter the effect estimates or CIs (analysis not shown).
2. Comparison 2: noradrenergic drugs versus dopaminergic drugs
2.1 TD symptoms
2.1.1 Not improved to a clinically important extent
The overall results for 'clinically relevant improvement' found no significant benefit of alpha‐methyldopa over reserpine after 2 weeks' treatment (1 trial, 20 people; RR 0.60, 95% CI 0.19 to 1.86; Analysis 2.1).
2.1. Analysis.
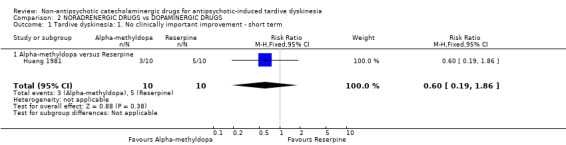
Comparison 2 NORADRENERGIC DRUGS vs DOPAMINERGIC DRUGS, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term.
2.1.2 Not any improvement
We could not estimate the effect of alpha‐methyldopa compared with reserpine on any improvement in TD symptoms as no events were reported (1 trial, 20 participants, Analysis 2.2).
2.2. Analysis.
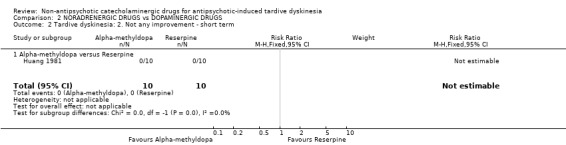
Comparison 2 NORADRENERGIC DRUGS vs DOPAMINERGIC DRUGS, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ short term.
2.1.3 Deterioration of symptoms
We could not estimate the effect of alpha‐methyldopa compared with reserpine on deterioration of TD symptoms as no events were reported (1 trial, 20 participants, Analysis 2.3).
2.3. Analysis.
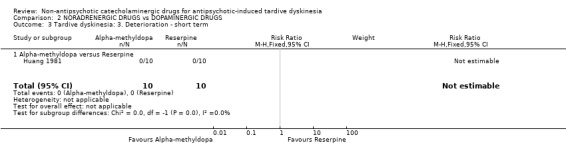
Comparison 2 NORADRENERGIC DRUGS vs DOPAMINERGIC DRUGS, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ short term.
2.2 Heterogeneity, subgroup‐ and sensitivity analyses
Only one study was included in this comparison: consequently subgroup and sensitivity analyses could not be undertaken and there was no heterogeneity.
3. Comparison 3: dopaminergic drugs versus placebo
3.1 TD symptoms
3.1.1 Not improved to a clinically important extent
The overall results for 'clinically relevant improvement' found a significant benefit of reserpine over placebo after 2 weeks' treatment (low‐quality evidence, 1 trial, 20 people; RR 0.52, 95% CI 0.29 to 0.96; Analysis 3.1).
3.1. Analysis.
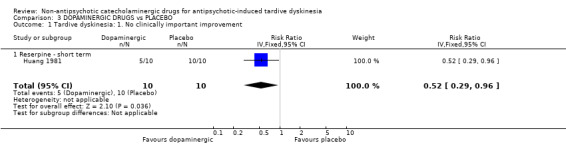
Comparison 3 DOPAMINERGIC DRUGS vs PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement.
3.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms' we found no significant difference between dopaminergic drugs (Carbidopa/levodopa, L‐dopa, reserpine) and placebo after 2 to 6 weeks' treatment (3 trials, 57 people;RR 0.60, 95% CI 0.35 to 1.03; I² = 0%, Analysis 3.2).
3.2. Analysis.
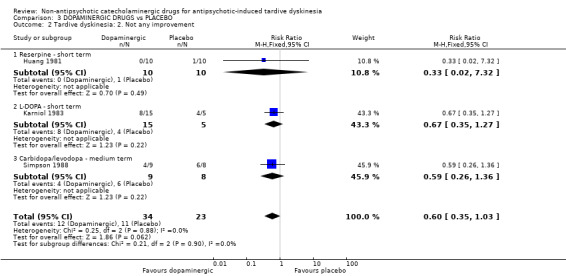
Comparison 3 DOPAMINERGIC DRUGS vs PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement.
3.1.3 Deterioration of symptoms
There was no significant difference in deterioration of symptoms between people allocated to dopaminergic drugs (carbidopa/levodopa, reserpine) or placebo after 2 to 6 weeks' treatment (very low quality evidence, 2 trials, 37 people; RR 1.18, 95% CI 0.35 to 3.99; I² = 0%, Analysis 3.3).
3.3. Analysis.
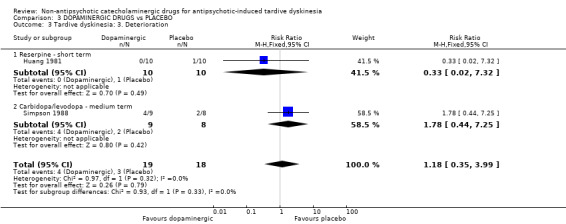
Comparison 3 DOPAMINERGIC DRUGS vs PLACEBO, Outcome 3 Tardive dyskinesia: 3. Deterioration.
3.2 Mental state
There was no significant difference between oxypertine and placebo on deterioration of mental state after 24 weeks' treatment (very low quality evidence, 1 trial, 42 people; RR 2.20, 95% CI 0.22 to 22.45; Analysis 3.4).
3.4. Analysis.
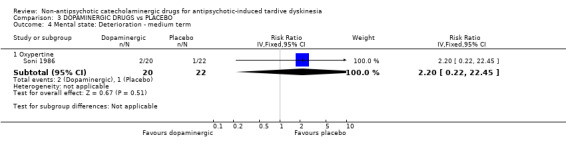
Comparison 3 DOPAMINERGIC DRUGS vs PLACEBO, Outcome 4 Mental state: Deterioration ‐ medium term.
3.3 Leaving the study early
Using dopaminergic drugs (amantadine, bromocriptine, carbidopa/levodopa, oxypertine, tiapride) did not significantly affect the chances of a person leaving the study early compared with placebo after 2 to 24 weeks' treatment (very low quality evidence, 6 trials, 163 people; RR 1.29, 95% CI 0.65 to 2.54; I² = 58%, Analysis 3.5).
3.5. Analysis.
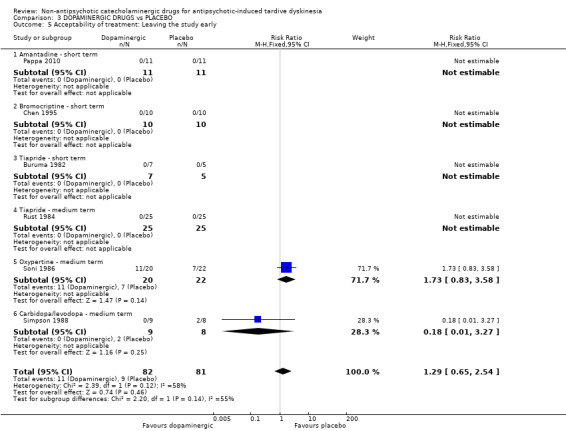
Comparison 3 DOPAMINERGIC DRUGS vs PLACEBO, Outcome 5 Acceptability of treatment: Leaving the study early.
3.4 Subgroup analysis
3.4.1 Type of compound
There were no significant subgroup differences (I² = 0%, P = 0.90, Analysis 3.2) for reserpine versus placebo (RR 0.33, 95% CI 0.02 to 7.32; 20 participants, 1 study), L‐dopa versus placebo (RR 0.67, 95% CI 0.35 to 1.27; 20 participants, 1 study), and carbidopa/levodopa versus placebo (RR 0.59, 95% CI 0.26 to 1.36; 17 participants, 1 study) on 'not any improvement in TD symptoms'. For 'deterioration of TD symptoms' there were no significant subgroup differences (I² = 0%, P = 0.32, Analysis 3.3) for reserpine versus placebo (RR 0.33, 95% CI 0.02 to 7.32; 20 participants, 1 study) and carbidopa/levodopa versus placebo (RR 1.78, 95% CI 0.44 to 7.25; 17 participants, 1 study). Finally, for 'acceptability of treatment: leaving the study early', there were subgroup differences (I² = 54.5%, P = 0.14, Analysis 3.5) for the subgroups that reported events, oxypertine versus placebo (RR 1.73, 95% CI 0.83 to 3.58; 42 participants, 1 study) and carbidopa/levodopa versus placebo (RR 0.18, 95% CI 0.01 to 3.27; 17 participants, 1 study; see '3.5 Heterogeneity' below).
3.4.2 Duration of follow‐up
Any effects that dopaminergic drugs may have did not clearly change in relation to duration of follow‐up compared with placebo.
3.4.3 Clinical stage: recent onset TD
It was not possible to evaluate whether those with recent onset TD responded differently to those with more established problems, since no trial reported data for groups with different durations of TD that could be extracted for separate analyses.
3.5 Heterogeneity
Data were mostly homogeneous. We detected statistical heterogeneity (I² = 58%, P = 0.12) as described in Assessment of heterogeneity for the outcome 'acceptability of treatment: leaving the study early'. Six studies reported on this outcome, but only two reported any events. One of these two studies reported an effect estimate favouring placebo over oxypertine after 24 weeks' treatment and the other study reported an effect estimate favouring carbidopa/levodopa over placebo after 6 weeks' treatment, but none of the studies reported statistically significant differences between groups (see Analysis 3.5 and '3.4.1 Type of compound' above).
3.6 Sensitivity analysis
3.6.1 Implication of randomisation
We aimed to include trials in a sensitivity analysis if they were described in some way as to imply randomisation. Only one study was included for the primary outcome: consequently this sensitivity analysis could not be performed.
3.6.2 Assumptions for lost binary data
The above results are based on data as presented in the original study reports, with the assumption that those who left early before the end of the trial had not improved (see Dealing with missing data). We planned to test the sensitivity of the results to this assumption, but all randomised participants were reported for the primary outcome 'no clinically important improvement in TD symptoms'. Therefore we could not undertake this sensitivity analysis. If there had been a substantial difference, we would have reported results and discussed them but continued to employ our assumption.
3.6.3 Risk of bias
We planned to exclude trials that we judged to be at high risk of bias across one or more of the domains, but only one study was included for the primary outcome. Consequently this sensitivity analysis could not be performed.
3.6.4 Imputed values
We would have undertaken a sensitivity analysis to assess the effects of including data from cluster randomised trials where we used imputed values for ICC in calculating the design effect. No cluster randomised trials were included.
3.6.5 Fixed and random effects
We also synthesised data using a random‐effects model. This did not alter the effect estimate or CIs for the primary outcome (analyses not shown).
4. Comparison 4: dopaminergic drugs versus other drugs
4.1 TD symptoms
4.1.1 Not improved to a clinically important extent
We found no significant benefit of tetrabenazine over haloperidol for 'no clinically relevant improvement after 18 weeks' treatment' (1 trial, 13 people; RR 0.93, 95% CI 0.45 to 1.95; Analysis 4.1).
4.1. Analysis.
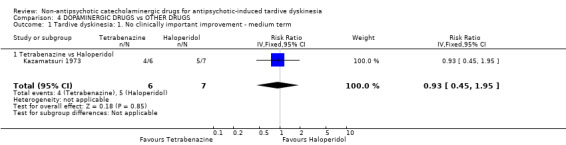
Comparison 4 DOPAMINERGIC DRUGS vs OTHER DRUGS, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
4.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we found no significant difference between tetrabenazine and haloperidol after 18 weeks' treatment (1 trial, 13 people; RR 0.39, 95% CI 0.05 to 2.83; Analysis 4.2).
4.2. Analysis.
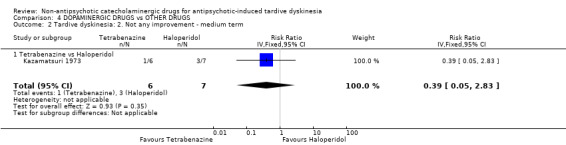
Comparison 4 DOPAMINERGIC DRUGS vs OTHER DRUGS, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term.
4.1.3 Deterioration of symptoms
There was no significant difference in deterioration of TD symptoms between people allocated to tetrabenazine or haloperidol after 18 weeks' treatment (1 trial, 13 people; RR 1.17, 95% CI 0.09 to 14.92; Analysis 4.3).
4.3. Analysis.
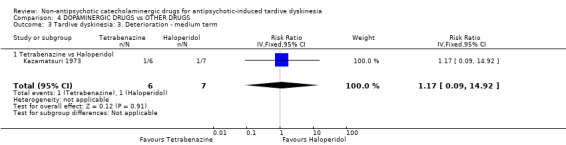
Comparison 4 DOPAMINERGIC DRUGS vs OTHER DRUGS, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ medium term.
4.2 Leaving the study early
There was no significant difference between tetrabenazine and haloperidol in the chances of a person leaving the study early after 18 weeks' treatment (1 trial, 13 people; RR 0.23, 95% CI 0.01 to 4.00; Analysis 4.4).
4.4. Analysis.
Comparison 4 DOPAMINERGIC DRUGS vs OTHER DRUGS, Outcome 4 Acceptability of treatment: Leaving the study early ‐ medium term.
4.3 Heterogeneity, and subgroup and sensitivity analyses
Only one study was included in this comparison. Consequently, subgroup and sensitivity analyses could not be undertaken; and there was no heterogeneity.
Discussion
Summary of main results
1. The search
This area of research does not seem to be active. The 2017 update has identified additional data, but most trials predate the year 2000: only one was carried out after, published in 2010. This could be because of reasons such as less concern with TD, or less emergence of the problem in research‐active communities because of more thoughtful use of antipsychotic drugs or loss of faith in non‐antipsychotic catecholaminergic drugs as a potential treatment.
2. Few data
Only a little over 250 people have been included in this review. It is possible that real, and important, effects have not been highlighted because of the necessarily wide CIs of the findings. Many outcomes were not measured at all (see Overall completeness and applicability of evidence), including one of our pre‐stated outcome measures. We may have been overambitious in hoping for some of these outcomes in TD trials but simple reporting of satisfaction with care or quality of life still does not seem too demanding and does remain of interest.
3. Comparison 1: noradrenergic drugs versus placebo
3.1 TD symptoms
Results from one study show that significantly more participants on alpha‐methyldopa than on placebo improved to a clinically important level at short term; however, our confidence in the evidence is low so further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
3.2 Acceptability of treatment
It is always unclear what leaving the study early means. It could be to do with the participant not accepting treatment for a series of reasons, or of participants finding the trial intolerable. It also could be a function of a trial design in which willing participants are still asked to leave because of some degree of protocol violation. In any event, one study reported that 2/17 participants left the celiprolol group compared with a 'not significantly different' 0/18 in the placebo group.
3.3 Social confidence, social inclusion, social networks, or personalised quality of life
This group of outcomes was selected as being of importance to patients for the 2017 review update following a service user consultation. One study reported on 'no improvement in quality of life' and found no difference between celiprolol and placebo; however, we are uncertain about the results as the evidence is of very low quality.
No studies comparing noradrenergic drugs versus placebo were identified that reported on adverse events or mental state. See Table 1 for a summary of the evidence.
4. Comparison 2: noradrenergic drugs versus dopaminergic drugs
4.1 TD symptoms
Only one small, short duration trial reported on this comparison and found no difference between alpha‐methyldopa and reserpine on 'no clinically important improvement in TD'. The size and duration of the trial were so limited that only a treatment of very great potency could have really shown up as effective.
No studies were identified that reported on adverse events, mental state, acceptability of treatment or social confidence, social inclusion, social networks, or personalised quality of life.
5. Comparison 3: dopaminergic drugs versus placebo
3.1 TD symptoms
Results from one small study show that significantly more participants on reserpine than on placebo improved to a clinically important level at short term; however, our confidence in the evidence is low so further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. We are uncertain about the results on 'not any improvement in TD' and 'deterioration of TD'; evidence was of very low quality.
3.2 Mental state
We are uncertain about the results on 'deterioration in mental state'; evidence was of very low quality.
3.3 Acceptability of treatment
We are uncertain about the results on 'acceptability of treatment', measured by the number of participants leaving the study early; evidence was of very low quality.
No studies were identified that reported on adverse events or social confidence, social inclusion, social networks, or personalised quality of life. See Table 3 for a summary of the evidence.
6. Comparison 4: dopaminergic drugs versus other drugs
3.1 TD symptoms
Only one small, short‐duration trial reported on this comparison and found no difference between tetrabenazine and haloperidol on 'no clinically important improvement in TD', on 'not any improvement in TD', or on 'deterioration of TD'. The size and duration of the trial were so limited that only a treatment of very great potency could have really shown up as effective.
3.2 Acceptability of treatment
None out of six participants left the tetrabenazine group compared with a 'not significantly different' two out of seven in the haloperidol group.
No studies were identified that reported on adverse events, mental state, or social confidence, social inclusion, social networks, or personalised quality of life.
Overall completeness and applicability of evidence
1. Completeness
Although we identified a large number of studies on the initial database search, the number of relevant studies was very small in comparison. The majority of studies selected were excluded because of inherent problems in the nature of their cross‐over design. That only eight studies were included in the final review does not give full justice to the fact that there has obviously been a reasonable amount of research in this area. This may have implications for future studies as discussed below.
No outcomes in this review involve large numbers of people, and many outcomes reported no events. None of the studies reported on adverse events. Even if these small studies only set out to show efficacy, not reporting on adverse events is unexpected as non‐antipsychotic catecholaminergic compounds are associated with several side effects (Turjanski 2005). In addition, there were very few data on the patient‐designated important outcomes of social confidence, social inclusion, social networks, or personalised quality of life; and there were no data on hospital and service utilisation outcomes, economic outcomes, behaviour or cognitive response.
2. Applicability
All but one trial were hospital‐based but were nevertheless on people who would be recognisable in everyday care. Trials were set in North and South America, Asia, and Europe. Outcomes are understandable in terms of clinical practice. However, most of the interventions in question are experimental in the treatment of tardive dyskinesia. Therefore, should any of the non‐antipsychotic catecholaminergic compounds have had important effects, findings might only have been applicable for those compounds accepted as treatment of TD.
Quality of the evidence
Overall, the quality of the evidence is low to very low. This means that we have limited to very little confidence in the effect estimates, and the true effect may be, or is likely to be, substantially different from the estimate of the effect. The main reasons for our low confidence in the evidence were as follows.
Poor study methodology and reporting of methods resulting in downgrading evidence for risk of bias. Overall the quality of reporting of these trials was poor (see Figure 3). Allocation concealment was not described; generation of the sequence was not explicit; studies were not clearly blinded and we are unsure if data are incomplete or selectively reported or if other biases were operating.
Very small sample sizes resulting in downgrading evidence for imprecision. The largest trial in this review randomised only 50 people. A trial of this size is unable to detect subtle, yet important, differences due to an intervention with any confidence. In order to detect a 20% difference between groups, probably about 150 people are needed in each arm of the study (alpha 0.05, beta 0.8).
Wide CIs (often due to low event rates) that included appreciable benefit or harm for the intervention as well as no effect, resulting in downgrading evidence for imprecision.
The small trial sizes, along with the poor reporting of trials, is associated with an exaggeration of effect of the experimental treatment where an effect is detected (Jűni 2001). This is only evident for the outcome of ‘no clinically important improvement in TD' where there is indeed an effect favouring the noradrenergic and dopaminergic drugs compared with placebo (see Table 1 and Table 3). This finding may be real — but could equally be a function of biases or of chance.
Potential biases in the review process
1. Missing studies
We made every effort to identify relevant trials. However, these studies are all small and it is likely that we have failed to identify other studies of limited power. It is likely that such studies would also not be in favour of the intervention group: if they had been so, it is more likely that they would have been published in accessible literature. We do not, however, think it likely that we have failed to identify large relevant studies.
2. Introducing bias
We have tried to be balanced in our appraisal of the evidence but could have inadvertently introduced bias. We welcome comments or criticisms. New methods and innovations now make it possible to report data where, in the past, we could not report data at all or had to report data in a different way. We think the 'Summary of findings' tables to be a valuable innovation — but problematic to those not ‘blind’ to the outcome data. It is possible to ‘cherry pick’ significant findings for presentation in this table. We have tried to decrease the chance of doing this by asking a new reviewer (HB) to select outcomes relevant for this table before becoming familiar with the data.
Agreements and disagreements with other studies or reviews
The only other relevant quantitative review we know of is the previous Cochrane Review (El‐Sayeh 2006). This update expands and improves this review but does not substantially change the conclusions.
Authors' conclusions
Implications for practice.
1. For people with antipsychotic‐induced tardive dyskinesia
These studies provide no useful information for service‐users. It is unlikely that these data will impact upon the uptake of established strategies for TD such as early detection, dose/drug modification, vitamin E and use of tetrabenazine. However, people with TD could consider these as other experimental treatments for which very little supportive data exist. Few data exist for any treatment for TD.
2. For clinicians
These treatments are purely experimental. This does not mean that they are not viable choices. If the drugs are available, these treatments could be used, but it would be advisable to study use of these treatments within a real‐world randomised trial.
3. For policy makers
There seem few implications for policy makers except that, perhaps, these compounds should only be used for TD within the context of a well‐designed randomised controlled trial.
Implications for research.
1. General
The power of this review would have been greatly enhanced by better reporting of data. For example, none of the studies made explicit how randomisation was undertaken; and few studies provide data for before the first period of cross‐over. We realise that much of the work for these trials predates CONSORT — first published in Begg 1996 — and that it is only too easy to judge studies of the past by standards of today. Future studies, however, should report to a much higher standard than what we have seen in trials eligible for this review.
2. Specific
Well‐designed randomised controlled trials, involving a large number of participants over protracted periods of time, are needed if we are to see if non‐antipsychotic catecholaminergic drugs could have a role in prevention and treatment of TD. Such studies are of importance to people with the problem, who have long been ignored (Figure 1).
2.1 Use of cross‐over design
Despite a large number of studies initially highlighted in the search, the data available for this review are very limited. The large number of studies we found, together with the disparate nature of these compounds, highlights the effort as well as the frustration that has gone into researching this topic. As previously mentioned, it is difficult to draw conclusions from a study that only includes 12 participants (Buruma 1982). It seems wasteful that so many studies were excluded because of inadequately designed cross‐over formats. Although there are certain advantages in using a cross‐over design in chronic conditions such as TD, there are also major disadvantages, one of which is the expected duration over which the drugs in question exert their actions. This cannot be considered as consisting solely of the time taken for the active drug to be removed from the bloodstream — the much longer period of time that these drugs may effect neurotransmitter or receptor function as well as structure must also be considered. It cannot be assumed that a washout period of a few weeks or less will adequately counteract these carry‐over effects. TD is also an unstable condition and people with TD may not remain compliant with medication. All these factors make the arguments for not using cross‐over methodology strong, despite the initial attraction (Armitage 1991; Fleiss 1984; Pocock 1983).
2.2 Sample size
The results suggest that larger sample size should be used to provide more precise estimates of effect and to help avoid false conclusions about the effects of the proposed treatment.
2.3 Length of study
Only one study included in this review used the intervention for more than five months (Soni 1986). TD, however, is a chronic condition of insidious onset, the severity of which fluctuates spontaneously (APA 1992). Even if the compounds under investigation have a swift effect, it is the long‐term outcomes that must be considered of most clinical value.
2.4 Outcomes
Scale‐derived data do have their place. It is important that a scale is validated for measuring changes secondary to treatment in those with TD. Many studies have not used clinically meaningful markers of outcome. They instead tend to either use obscure/modified ratings scales (such as SKAUB) (Hebenstreit 1986); or even more nebulous surrogate end‐point measures. Scale‐derived data do have their place, but it is important that a scale is validated for measuring changes secondary to treatment in those with TD. In addition, many of the outcomes we initially desired when we started this review have not been investigated. Finally, a service user consultation also informed the addition of outcomes of special importance to patients. We have reconsidered all these outcomes in case they were too ambitious and tried to tailor them to a real‐world pragmatic trial design (see Table 6). Future studies could be well served by using guidelines as described in the CONSORT statement (Moher 2001). These may help avoid some of the rectifiable flaws in the study methodologies and as a result allow more studies to be included in the final analyses.
2. Suggestions for design of future studies.
| Methods | Allocation: randomised, with sequence generation and concealment of allocation clearly described. Blindness: double, tested. Duration: 12 months beyond end of intervention at least. Raters: independent. |
| Participants | People with antipsychotic‐induced tardive dyskinesia.* Age: any. Sex: both. History: any. N = 300.** |
| Interventions | 1. Non‐antipsychotic catecholaminergic compound. N = 150. 2. Placebo: N = 150. |
| Outcomes | Tardive dyskinesia: any clinically important improvement in TD, any improvement, deterioration.*** Adverse effects: no clinically significant extrapyramidal adverse effects ‐ any time period***, use of any antiparkinsonism drugs, other important adverse events. Leaving the study early. Service outcomes: admitted, number of admissions, length of hospitalisation, contacts with psychiatric services. Compliance with drugs. Economic evaluations: cost‐effectiveness, cost‐benefit. General state: relapse, frequency and intensity of minor and major exacerbations. Social confidence, social inclusion, social networks, or personalised quality of life: binary measure Distress among relatives: binary measure. Burden on family: binary measure. |
| Notes | * This could be diagnosed by clinical decision. If funds were permitting all participants could be screened using operational criteria, otherwise a random sample should suffice. ** Size of study with sufficient power to highlight about a 10% difference between groups for primary outcome. *** Primary outcome. The same applies to the measure of primary outcome as for diagnosis. Not everyone may need to have operational criteria applied if clinical impression is proved to be accurate. |
What's new
| Date | Event | Description |
|---|---|---|
| 4 October 2017 | New citation required but conclusions have not changed | Results from latest searches do not change conclusions of this review |
| 26 April 2017 | New search has been performed | Update search run 26 April, 2017. Eight records found and assessed by editorial base Cochrane Schizophrenia, no new studies relevant to this review found. The 8 records have been added to Studies awaiting classification of Miscellaneous treatments for antipsychotic‐induced tardive dyskinesia (see also Results of the search) |
| 16 November 2016 | Amended | Title changed from 'Non‐neuroleptic catecholaminergic drugs for neuroleptic‐induced tardive dyskinesia'. Eight new trials added (Chen 1995; Huang 1981; Karniol 1983; Kazamatsuri 1973; Pappa 2010; Rust 1984; Simpson 1988; Soni 1986), analyses and text updated, outcomes' list updated due to patient consultation, 'Summary of findings' table added, conclusions not substantially changed. |
History
Protocol first published: Issue 1, 1997 Review first published: Issue 1, 2006
| Date | Event | Description |
|---|---|---|
| 16 July 2015 | Amended | Update search run July 16, 2015. 704 records found and assessed by review authors. |
| 31 January 2013 | Amended | Contact details updated. |
| 17 October 2012 | Amended | Contact details updated. |
| 18 January 2012 | Amended | Contact details updated. |
| 14 April 2010 | Amended | Contact details updated. |
| 11 November 2009 | Amended | Contact details updated. |
| 26 April 2008 | Amended | Converted to new review format. |
| 5 October 2005 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
We would like to thank Clive Adams, Gill Rizzello and Tessa Grant for their advice and technical support. Thanks also to Ben Gray for writing the Plain Language Summary, and to Farhad Sokraneh for carrying out the 2015 trial search. We would like to thank João Paulo Lyra da Silva for his contribution to the previously published version of this review. We are also grateful to Dawn‐Marie Walker, Ruth Sayers, Megan Lees, and Vanessa Pinfold from McPin Foundation for organising and holding the public‐ and patient‐involvement consultation with TD service users that contributed to selecting outcomes for the 'Summary of findings' tables and to guiding future research. Finally, we wish to thank Rosie Asher and Antonio Grande for screening literature and helping with data extraction for the 2017 update, and Nicholas Henschke, Linda Levi and Loukia Spineli for assisting with updating the report.
Appendices
Appendix 1. Previous methods
Methods
Criteria for considering studies for this review
Types of studies
We included all relevant randomised controlled trials. Where a trial was described as 'double‐blind' but it was implied that the study was randomised, we included these trials in a sensitivity analysis. If there was no substantive difference within primary outcomes (see types of outcome measures) when these 'implied randomisation' studies were added, then we included these in the final analysis. If there was a substantive difference, we only used clearly randomised trials were and described the results of the sensitivity analysis in the text. We excluded quasi‐randomised studies, such as those allocating by using alternate days of the week.
Types of participants
People with schizophrenia or any other chronic mental illnesses, diagnosed by any criteria, irrespective of gender, age or nationality who: i. required the use of neuroleptics for more than three months; ii. developed tardive dyskinesia (diagnosed by any criteria) during neuroleptic treatment; and iii. for whom the dose of neuroleptic medication had been stable for one month or more before the trial.
Types of interventions
A. Noradrenergic drugs i. Celiprolol, clonidine, disulfiram, fusaric acid, methyldopa, pindolol, propanolol, oxprenolol or yohimbine, compared with placebo or no intervention.
B. Dopaminergic drugs i. The dopamine receptor agonists (apomorphine, bromocriptine, CF25‐397, dopamine, hydergine, lisuride); ii. the dopamine receptor antagonists (AMTP, oxiperomide, metoclopramide, papaverine, tiapride); iii. the dopamine depleter drugs (oxypertine, reserpine, tetrabenazine); iv. drugs that increase the release (amantadine, amphetamine) or production (L‐dopa) of dopamine; all compared with placebo or no intervention.
Types of outcome measures
1. Tardive dyskinesia 1.1. No clinically important change in tardive dyskinesia* 1.2. Not any change in tardive dyskinesia 1.3. Average endpoint tardive dyskinesia score 1.4. Average change in tardive dyskinesia scores
2. Mental state 2.1. No clinically important change in general mental state* 2.2. Not any change in general mental state 2.3. Average endpoint general mental state score 2.4. Average change in general mental state scores 2.5. No clinically important change in specific symptoms 2.6. Not any change in specific symptoms 2.7. Average endpoint specific symptom score 2.8. Average change in specific symptom scores
3. Adverse effects 3.1. Clinically important general adverse effects* 3.2. Any general adverse effects 3.3. Average endpoint general adverse effect score 3.4. Average change in general adverse effect scores 3.5. Clinically important change in specific adverse effects 3.6. Any change in specific adverse effects 3.7. Average endpoint specific adverse effects 3.8. Average change in specific adverse effects
4. Leaving the study early 4.1. For specific reasons 4.2. For general reasons*
* Primary outcomes
When possible, outcomes were grouped into time periods ‐ short term (less than 6 weeks), medium term (between 6 weeks and 6 months) and long term (over 6 months).
Search methods for identification of studies
1. Electronic searching for the update (2005) 1.1. We identified relevant randomised trials by searching the Cochrane Schizophrenia Group's register using the phrase:
SELECT tblStudy.CRGStudyID FROM tblStudy WHERE tblStudy.CRGStudyID In (SELECT tblStudyIntervention.CRGStudyID FROM tblIntervention INNER JOIN tblStudyIntervention ON tblIntervention.InterventionID=tblStudyIntervention.InterventionID WHERE InterventionDescription Like "*amantadin*" OR InterventionDescription Like "*amphetamin*" OR InterventionDescription Like "*apomorphin*" OR InterventionDescription Like "*bromocriptin*" OR InterventionDescription Like "*celiprolol*" OR InterventionDescription Like "*clonidin*" OR InterventionDescription Like "*dopa*" OR InterventionDescription Like "*disulfiram*" OR InterventionDescription Like "*fusaric*" OR InterventionDescription Like "*hydergin*" OR InterventionDescription Like "*lisurid*" OR InterventionDescription Like "*metoclopramid*" OR InterventionDescription Like "*oxiperomid*" OR InterventionDescription Like "*oxprenolol*" OR InterventionDescription Like "*oxypertin*" OR InterventionDescription Like "*papaverin*" OR InterventionDescription Like "*pindolol*" OR InterventionDescription Like "*propranolol*" OR InterventionDescription Like "*reserpine*" OR InterventionDescription Like "*tetraben*" OR InterventionDescription Like "*tiaprid*" OR InterventionDescription Like "*yohimb*");
2. Details of previous searches:
We identified relevant randomised trials by searching several electronic databases (Biological Abstracts, the Cochrane Schizophrenia Group's Register of trials, EMBASE, LILACS, MEDLINE, PsycLIT and SCISEARCH).
2.1. Biological Abstracts We searched Biological Abstracts (January 1982 to May 1995) using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase:
[and ((tardive near (dyskinesia* or disk ine*) or (abnormal near movement* near disorder*) or (involuntary* near movement*)) and (amantadine or amphetamine or AMTP or apomorphine or bromocriptine or celiprolol or CF?25397 or clonidine or *dopa* or disulfiram or fusaric or hydergine or lisuride or methyldopa or metoclopramide or oxiperomide or oxprenolol or oxypertine or papaverine or pindolol or propanolol or reserpine or tetrabenazine or tiapride or yohimbine)]
2.2. The Cochrane Schizophrenia Group's Register (1997)
We searched The Cochrane Schizophrenia Group's register using the phrase: [(dyskinesia) and (amantadine or amphetamine or AMTP or apomorphine or bromocriptine or celiprolol or CF?25397 or clonidine or *dopa* or disulfiram or fusaric or hydergine or lisuride or methyldopa or metoclopramide or oxiperomide or oxprenolol or oxypertine or papaverine or pindolol or propanolol or reserpine or tetrabenazine or tiapride or yohimbine)]
2.3. EMBASE We searched EMBASE (January 1980 to May 1995) using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase:
[and ((tardive dyskinesia in thesaurus ‐subheadings, prevention, drug therapy, side effect and therapy) or (neuroleptic dyskinesia in thesaurus ‐all subheadings) or (tardive or dyskinesia*) or (movement* or disorder*) or (abnormal or movement* or disorder*)) and (amantadine or amphetamine or AMTP or apomorphine or bromocriptine or celiprolol or CF?25397 or clonidine or *dopa* or disulfiram or fusaric or hydergine or lisuride or methyldopa or metoclopramide or oxiperomide or oxprenolol or oxypertine or papaverine or pindolol or propanolol or reserpine or tetrabenazine or tiapride or yohimbine)]
2.4. LILACS
We searched LILACS (January 1982 to September 1996) using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase: [and ((tardive or (dyskinesia* or dyskinesia*)) or (drug induced movement disorders in thesaurus)) and (amantadine or amphetamine or AMTP or apomorphine or bromocriptine or celiprolol or CF?25397 or clonidine or *dopa* or disulfiram or fusaric or hydergine or lisuride or methyldopa or metoclopramide or oxiperomide or oxprenolol or oxypertine or papaverine or pindolol or propanolol or reserpine or tetrabenazine or tiapride or yohimbine)]
2.5. MEDLINE
We searched MEDLINE (January 1966 to May 1995) using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase: [and ((movement‐disorders in MeSH / explode all subheadings) or (anti‐dyskinesia‐agents in MeSH / explode all subheadings) or (dyskinesia‐drug‐induced in MeSH / explode all subheadings) and (psychosis in MeSH / explode all subheadings) or (schizophrenic disorders in MeSH / explode all subheadings) or (tardive near (dyskine* or diskine*)) or (abnormal* near movement* near disorder*) or (involuntar* near movement*)) and (amantadine or amphetamine or AMTP or apomorphine or bromocriptine or celiprolol or CF?25397 or clonidine or *dopa* or disulfiram or fusaric or hydergine or lisuride or methyldopa or metoclopramide or oxiperomide or oxprenolol or oxypertine or papaverine or pindolol or propanolol or reserpine or tetrabenazine or tiapride or yohimbine)]
2.6. PsycLIT
We searched PsycLIT (January 1974 to May 1995) using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase: [and ((explode movement‐disorders in DE) or (explode tardive‐dyskinesia in DE) or (tardive near (dyskine* or diskine*) or (abnormal* near movement* near disorder*) or (involuntar* near movement*)) and (amantadine or amphetamine or AMTP or apomorphine or bromocriptine or celiprolol or CF?25397 or clonidine or *dopa* or disulfiram or fusaric or hydergine or lisuride or methyldopa or metoclopramide or oxiperomide or oxprenolol or oxypertine or papaverine or pindolol or propanolol or reserpine or tetrabenazine or tiapride or yohimbine)]
3. SCISEARCH ‐ Science Citation Index
We sought each of the included studies as a citation on the SCISEARCH database. We inspected reports of articles that had cited these studies in order to identify further trials.
4. Reference searching
We inspected the references of all identified studies for more studies.
5. Personal contact
We contacted the first author of each included study for information regarding unpublished trials.
Data collection and analysis
1. Selection of trials We downloaded citations from electronic sources including details of author, institution or journal of publication. We (HGE) inspected all reports. These were then re‐inspected by (KS and JR) in order to ensure reliable selection. Any disagreement was resolved by discussion, and where there was still doubt we acquired the full article for further inspection. Once the full articles were obtained, we (HGE, KS and JR) decided whether the studies met the review criteria. Whenever we could not resolve any disagreement by discussion, we sought further information and added these trials to the list of those awaiting assessment.
2. Assessment of methodological quality The methodological quality of all included trials was assessed using the criteria described in the Cochrane Handbook (Higgins 2005) and the Jadad Scale (Jadad 1996). The former is based on the evidence of a strong relationship between allocation concealment and direction of effect (Schulz 1995). The categories are defined below:
A. Low risk of bias (adequate allocation concealment) B. Moderate risk of bias (some doubt about the results) C. High risk of bias (inadequate allocation concealment). For the purpose of the analysis in this review, trials were included if they met the Cochrane Handbook criteria A or B.
The Jadad Scale measures a wider range of factors that impact on the quality of a trial. The scale includes three items: 1. Was the study described as randomised? 2. Was the study described as double‐blind? 3. Was there a description of withdrawals and drop outs?
Each item receives one point if the answer is positive. In addition, a point can be deducted if either the randomization or the blinding/masking procedures described were inadequate. For the purpose of the analysis in this review, in addition to the criteria according to the Cochrane Handbook, a cut‐off of two points was used in the Jadad scale to check the assessment made by the Handbook criteria. However, we did not use the Jadad Scale to exclude trials in this review.
3. Data collection HGE and JR independently extracted data from selected trials, while KS separately re‐extracted information from two different samples (10%). When disputes arose we attempted resolution by discussion. When this was not possible and further information was necessary to resolve the dilemma, we did not enter data but added this outcome of the trial to the list of those awaiting assessment.
4. Data synthesis 4.1 Data types We assessed outcomes using continuous (for example changes on a behaviour scale), categorical (for example, one of three categories on a symptoms scale, such as 'little change', 'moderate change' or 'much change') or dichotomous measures (for example, either 'no important changes' or 'important changes' in a person's symptoms). Currently RevMan does not support categorical data so we could not analyse them as such.
4.2 Incomplete data With the exception of the outcome of leaving the study early, we did not include trial outcomes if more than 40% of people were not reported in the final analysis.
4.3 Dichotomous ‐ yes/no ‐ data We analysed data on an intention to treat analysis. On the condition that more than 60% of people completed the study, we counted everyone allocated to the intervention regardless of whether they completed the follow up. We assumed that those who dropped out had the negative outcome, with the exception of death. Where possible we made efforts to convert outcome measures to dichotomous data. This can be done by identifying cut off points on rating scales and dividing subjects accordingly into 'clinically improved' or 'not clinically improved'. If the authors of a study had used a predefined cut off point for determining clinical effectiveness we used the reviewers' criteria where appropriate. Otherwise we generally assumed that if there had been a 50% reduction in a scale‐derived score, this could be considered as a clinically significant response. Similarly, a rating of 'at least much improved' according to the Clinical Global Impression Scale (Guy 1970) could be considered as a clinically significant response.
We calculated the relative risk (RR) and its 95% confidence interval (CI) based on the random effects model, as it takes into account any differences between studies even if there is no statistically significant heterogeneity. It has been shown that RR is more intuitive than odds ratios (Boissel 1999), and also that odds ratios tend to be interpreted as RR by clinicians (Deeks 2000). This misinterpretation then leads to an overestimate of the impression of the effect. We inspected graphs to see if an analysis using a fixed effects model made any substantive difference in outcomes that were not statistically significantly heterogeneous. When the overall results were significant we calculated the number needed to treat (NNT) and the number‐needed‐to‐harm (NNH) as the inverse of the risk difference.
4.4 Continuous data 4.4.1 Normally distributed data: data on continuous outcomes are frequently skewed, the mean not being the centre of the distribution. The statistics for meta‐analysis are thought to be able to cope with some skew, but were formulated for parametric data. To avoid this potential pitfall we applied the following standards to all data before inclusion: (a) standard deviations and means were reported or obtained from authors and (b) for data with finite limits, such as endpoint scale data, the standard deviation (SD), when multiplied by two, was less than the mean. Otherwise the mean is unlikely to be an appropriate measure of the centre of the distribution (Altman 1996). We reported data that did not meet the first or second standard in the 'other data' tables. If a scale starts from a positive value (such as PANSS, which can have values from 30‐210) the calculation described above should be modified to take the scale starting point into account. In these cases skewness is present if 2SD>(S‐Smin), where S is the mean score and Smin is the minimum score.
For change data (endpoint minus baseline), the situation is even more problematic. In the absence of individual patient data it is impossible to know if data are skewed, though this is likely. After consulting the ALLSTAT electronic statistics mailing list, we presented change data in MetaView in order to summarise available information. In doing this, it is assumed either that data were not skewed or that the analyses could cope with the unknown degree of skewness. Without individual patient data it is impossible to test this assumption. Where both change and endpoint data were available for the same outcome category only endpoint data are presented. We acknowledge that by doing this much of the published change data were excluded, but argue that endpoint data is more clinically relevant and that if change data were to be presented along with endpoint data it would be given undeserved equal prominence. We are contacting authors of studies reporting only change data for endpoint figures. We reported non‐normally distributed data in the 'Other data types' tables.
4.4.2 Cluster trials Studies increasingly employ 'cluster randomisation' (such as randomisation by clinician or practice) but analysis and pooling of clustered data poses problems. Firstly, authors often fail to account for intra class correlation in clustered studies, leading to a 'unit of analysis' error (Divine 1992) whereby P values are spuriously low, confidence intervals unduly narrow and statistical significance overestimated. This causes type I errors (Bland 1997, Gulliford 1999).
Where clustering was not accounted for in primary studies, we presented the data in a table, with a (*) symbol to indicate the presence of a probable unit of analysis error. In subsequent versions of this review we will seek to contact first authors of studies to obtain intra‐class correlation co‐efficients of their clustered data and to adjust for this using accepted methods (Gulliford 1999). Where clustering has been incorporated into the analysis of primary studies, we will also present these data as if from a non‐cluster randomised study, but adjusted for the clustering effect.
We have sought statistical advice and have been advised that the binary data as presented in a report should be divided by a 'design effect'. This is calculated using the mean number of participants per cluster (m) and the intraclass correlation co‐efficient (ICC) [Design effect = 1+(m‐1)*ICC] (Donner 2002). If the ICC was not reported it was assumed to be 0.1 (Ukoumunne 1999).
4.4.2 Rating scales: A wide range of instruments is available to measure mental health outcomes. These instruments vary in quality and many are not valid, or even ad hoc. For outcome instruments some minimum standards have to be set. It has been shown that the use of rating scales which had not been described in a peer‐reviewed journal (Marshall 2000) is associated with bias and therefore we excluded the results of such scales. Furthermore, the instrument should either be a self report or be completed by an independent rater or relative (not the therapist), and the instrument could be considered a global assessment of an area of functioning. However, as it was expected that therapists would frequently also be the rater, we did include such data but commented on this data as 'prone to bias'.
4.4.3 Summary statistic For continuous outcomes we estimated the weighted mean difference (WMD) between groups, again based on the random effects model, as it takes into account any differences between studies even if there is no statistically significant heterogeneity. We inspected data to see if analysis using a fixed effects model made any substantive difference when the results were not statistically significantly heterogeneous. Whenever possible, we took the opportunity to make direct comparisons between trials that used the same measurement instrument to quantify specific outcomes. Where continuous data were presented from different scales rating the same effect, we presented both sets of data and the general direction of effect was inspected.
5. Heterogeneity Firstly, we considered all of the included studies within any comparison to judge clinical heterogeneity. Then we visually inspected graphs used to investigate the possibility of statistical heterogeneity and supplemented this by using, primarily, the I‐squared statistic. This provides an estimate of the percentage of variability due to heterogeneity rather than chance alone. Where the I‐squared estimate was greater than or equal to 75%, we interpreted this as indicating the presence of high levels of heterogeneity (Higgins 2003). If inconsistency was high, we did not summate the data, but presented it separately and reasons for heterogeneity were investigated.
6. Addressing publication bias We entered all data from selected trials into a funnel graph (trial effect versus trial size) in an attempt to investigate the likelihood of overt publication bias.
7. Sensitivity analyses We analysed the effect of including studies with high attrition rates in the sensitivity analysis.
8. General Where possible, we entered data in such a way that the area to the left of the line of no effect indicated a favourable outcome for the treatment groups.
Data and analyses
Comparison 1. NORADRENERGIC DRUGS vs PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 0.33 [0.14, 0.80] |
| 1.1 Alpha‐methyldopa | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 0.33 [0.14, 0.80] |
| 2 Tardive dyskinesia: 2. Not any improvement | 2 | 55 | Risk Ratio (IV, Fixed, 95% CI) | 0.91 [0.65, 1.27] |
| 2.1 Alpha‐methyldopa ‐ short term | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 0.33 [0.02, 7.32] |
| 2.2 Celiprolol ‐ medium term | 1 | 35 | Risk Ratio (IV, Fixed, 95% CI) | 0.92 [0.66, 1.28] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ short term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.02, 7.32] |
| 3.1 Alpha‐methyldopa | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.02, 7.32] |
| 4 Acceptability of treatment: Leaving the study early ‐ medium term | 1 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.28 [0.27, 102.58] |
| 4.1 Celiprolol | 1 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.28 [0.27, 102.58] |
| 5 Quality of life: No improvement ‐ medium term | 1 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.68, 1.12] |
| 5.1 Celiprolol | 1 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.68, 1.12] |
Comparison 2. NORADRENERGIC DRUGS vs DOPAMINERGIC DRUGS.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.6 [0.19, 1.86] |
| 1.1 Alpha‐methyldopa versus Reserpine | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.6 [0.19, 1.86] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ short term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2.1 Alpha‐methyldopa versus Reserpine | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ short term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3.1 Alpha‐methyldopa versus Reserpine | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 3. DOPAMINERGIC DRUGS vs PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 0.52 [0.29, 0.96] |
| 1.1 Reserpine ‐ short term | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 0.52 [0.29, 0.96] |
| 2 Tardive dyskinesia: 2. Not any improvement | 3 | 57 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.35, 1.03] |
| 2.1 Reserpine ‐ short term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.02, 7.32] |
| 2.2 L‐DOPA ‐ short term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.35, 1.27] |
| 2.3 Carbidopa/levodopa ‐ medium term | 1 | 17 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.59 [0.26, 1.36] |
| 3 Tardive dyskinesia: 3. Deterioration | 2 | 37 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.18 [0.35, 3.99] |
| 3.1 Reserpine ‐ short term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.02, 7.32] |
| 3.2 Carbidopa/levodopa ‐ medium term | 1 | 17 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.78 [0.44, 7.25] |
| 4 Mental state: Deterioration ‐ medium term | 1 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 Oxypertine | 1 | 42 | Risk Ratio (IV, Fixed, 95% CI) | 2.2 [0.22, 22.45] |
| 5 Acceptability of treatment: Leaving the study early | 6 | 163 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.65, 2.54] |
| 5.1 Amantadine ‐ short term | 1 | 22 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.2 Bromocriptine ‐ short term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.3 Tiapride ‐ short term | 1 | 12 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.4 Tiapride ‐ medium term | 1 | 50 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.5 Oxypertine ‐ medium term | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.73 [0.83, 3.58] |
| 5.6 Carbidopa/levodopa ‐ medium term | 1 | 17 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.18 [0.01, 3.27] |
Comparison 4. DOPAMINERGIC DRUGS vs OTHER DRUGS.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 13 | Risk Ratio (IV, Fixed, 95% CI) | 0.93 [0.45, 1.95] |
| 1.1 Tetrabenazine vs Haloperidol | 1 | 13 | Risk Ratio (IV, Fixed, 95% CI) | 0.93 [0.45, 1.95] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term | 1 | 13 | Risk Ratio (IV, Fixed, 95% CI) | 0.39 [0.05, 2.83] |
| 2.1 Tetrabenazine vs Haloperidol | 1 | 13 | Risk Ratio (IV, Fixed, 95% CI) | 0.39 [0.05, 2.83] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ medium term | 1 | 13 | Risk Ratio (IV, Fixed, 95% CI) | 1.17 [0.09, 14.92] |
| 3.1 Tetrabenazine vs Haloperidol | 1 | 13 | Risk Ratio (IV, Fixed, 95% CI) | 1.17 [0.09, 14.92] |
| 4 Acceptability of treatment: Leaving the study early ‐ medium term | 1 | 13 | Risk Ratio (IV, Fixed, 95% CI) | 0.23 [0.01, 4.00] |
| 4.1 Tetrabenazine vs Haloperidol | 1 | 13 | Risk Ratio (IV, Fixed, 95% CI) | 0.23 [0.01, 4.00] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Buruma 1982.
| Methods | Allocation: randomised, no further details.
Blindness: unclear.
Duration: 4 weeks (2 weeks then crossed over to another 2 weeks).
Design: cross‐over.
Setting: inpatients at 2 long‐stay psychiatric hospitals, the Netherlands. Raters: blinding of raters not reported. |
|
| Participants | Diagnosis: psychiatric disease (no operational criteria) and institutionalised with antipsychotic‐induced tardive dyskinesia.
N = 12.
Sex: 4 M, 8 F.
Age: range 39 to 70 years, mean 59 years. Duration of TD: not reported. |
|
| Interventions | 1. Tiapride: dose 100 mg tid/day for 2 weeks. N = 7. 2. Placebo: N = 5. Previous treatment, including that prescribed for the TD, was continued without alterations throughout the trial. No further details on concomitant medications were reported. |
|
| Outcomes | Leaving the study early. Unable to use ‐ Adverse effects: tardive dyskinesia (doppler‐radar movement counter, videotaped dyskinesia scores, not reported pre‐cross‐over). |
|
| Notes | Sponsorship source: Delagrange provided Tiapride. Additional sponsorship details not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomly allocated to two groups"; further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Unclear, in the introduction it is stated that: "However, the results from these studies seemed to justify a double‐blind controlled cross‐over trial and objective evaluation of the effect of Tiapride on the involuntary movements"; the Methods section does not report blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "All twelve patients completed the trial". |
| Selective reporting (reporting bias) | High risk | "Besides these quantitative methods, self‐assessment analogue three‐point scales were made by the patients, and subjective analogue ratings were made on a five‐point scale by family, nurses and attendant doctors. At each recording session the patient was asked about possible side‐effects of the treatment. At each investigation motor performance speed was quantified (Schuhfried apparatus) to study possible parkinsonian effect of Tiapride ". "The results of the assessment analogue scales were inaccurate. The patients gave inconsistent answers in 3.1%, the nurses and the attendant doctors even in 37%. Further analysis of the subjective results has been discarded because of the reason outlined above and the fact that statistical analysis on three and five‐point scales does not have enough sensitivity for such a small group of patients." |
| Other bias | High risk | "the randomization has partly failed with respect to the seriousness of the dyskinesia of the patients: the second group consisted of more affected patients." |
Chen 1995.
| Methods | Allocation: "cross over randomized trial".
Blinding: double‐blind with adequate description. Duration: 4 weeks. Design: cross‐over. Setting: inpatients, China. Raters: blinding of raters not reported. |
|
| Participants | Diagnosis: Antipsychotics‐induced tardive dyskinesia. N = 20*. Sex: 12 M, 8 F. Agemean 34.86 (SD 7.82) years old. Duration of TD: mean 3.52 (SD 2.38) years. |
|
| Interventions | 1. Bromocriptine Group: at first phase of the trial, the participants received bromocriptine, 1 capsule each time, twice per day for 4 weeks. The second phase was a 2‐week washout period. At the third phase of the trial, the participants received placebo for 4 weeks. N = 10.* 2. Placebo Group: at first phase of the trial, the participants received placebo for 4 weeks. The second phase was a 2‐week washout period. At the third phase of the trial, the participants received bromocriptine, 1 capsule each time, twice per day for 4 weeks. N = 10.* All participants received stable doses of antipsychotics before and during the study. Other concomitant medication was not reported. |
|
| Outcomes | Leaving the study early. Unable to use (data from first phase before cross‐over not reported separately) ‐ Abnormal Involuntary Movement Scale (AIMS). Clinical response of TD.** Adverse events: dizziness, nausea. Study authors were contacted but no more information was received. |
|
| Notes | *sequential test method was used; when the 10th participants completed the trial, a significant difference was detected, so they terminated enrolling participants. **clinical improvement defined as the decrease rate of AIMS score ≥ 20%. Data extracted by Sai Zhao from Chinese language report. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "cross over randomized trial"; no further details reported. |
| Allocation concealment (selection bias) | Low risk | "the interventions were coded as intervention A or B by the researcher in pharmacy". |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "double blind study, the interventions were coded as intervention A or B by the researcher in pharmacy" "Participants and personnel did not know the allocation result". The 2 drugs were contained in capsules with same appearance. Blinding of participants and key study personnel ensured. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants completed the study. |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all predefined outcomes have been reported. A protocol is not available for verification. |
| Other bias | Low risk | The study seems to be free of other sources of bias. |
Hebenstreit 1986.
| Methods | Allocation: randomised, no further details.
Blindness: double (identical film‐coated tablets).
Duration: 3 months.
Design: parallel. Setting: psychiatric ward, Austria. Raters: all assessments were made by the same examiner. No reference to rater blinding was reported. |
|
| Participants | Diagnosis: symptoms of TD using AIMS. N = 35. Sex: only female. Age: range 43 to 82 years. Duration TD: not reported. | |
| Interventions | 1. Celiprolol: single dose 200 mg/day. N = 17. 2. Placebo: N = 18. All patients received additional antipsychotic medication. |
|
| Outcomes | Improvement in TD symptom using SKAUB (German version of AIMS). Quality of life. Leaving the study early. Unable to use ‐ Adverse effects: diarrhoea, hypotensive circulatory dysregulation, collapsing, cold sensation in extremities, tremor, heartburn, dizziness, sleeplessness, changes in blood pressure (systolic and diastolic) and pulse (no usable data). |
|
| Notes | No information on sponsorship. Article in German. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized"; details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double blind, identical film‐coated tablets. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information is provided. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Exclusions are reported but no information on whether they were accounted for or discounted from the analysis. |
| Selective reporting (reporting bias) | High risk | Outcome data for adverse events not fully reported. |
| Other bias | Low risk | The study seems to be free from other sources of bias. |
Huang 1981.
| Methods | Allocation: randomised. Blindness: double blind, identical‐appearing capsules. Duration: each patient was observed for 4 days in a control period before test medication was given. This was followed by a period of 2 weeks of research medication, and a post‐medication period. Design: parallel. Setting: inpatients, USA. Raters: assessments were done subjectively by the same observer at the same time (4:00pm) every day. |
|
| Participants | Diagnosis: psychosis (diagnosis details not reported); antipsychotic induced TD. Total number randomised: N = 30. Sex: not reported. Age: 40 to 65 years. Duration of TD: no information. |
|
| Interventions | 1. Alpha‐methyldopa (Aldomet)*: 750 to 1500 mg/d. N = 10. 2. Reserpine*: 0.75 to 1.5 mg/d; N = 10. 3. Placebo (lactose): N = 10. Patients were allowed to continue taking antipsychotic and anticholinergic medications throughout this study as required to control persistent psychosis. Antipsychotic and antiparkinsonism medications had been stabilized for more than 1 year and were kept strictly constant. |
|
| Outcomes | TD symptoms: improvement and deterioration. Unable to use‐ TD symptoms scale scores, using a tardive dyskinesia rating scale with no published psychometric tests. Adverse effects: sedation, hypotension and mood depression (no usable data). |
|
| Notes | Sponsorship source: not reported. *The dose of the research medication was increased during the testing period in order to obtain maximal therapeutic response. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “Thirty patients were randomly assigned to three medication groups”; no further details reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | “The study was carried out by a double‐blind controlled method. Each identical appearing capsule contained either a‐methyldopa (Aldomet) 250 mg, reserpine 0.25 mg or placebo (lactose)”. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | “The severity of... movements were assessed subjectively by the same observer (C. C. Huang) at the same time (4:00pm) every day”, but blinding details of outcome assessor were not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | All subjects seem to have completed the 2‐week study. However, attrition information has not been clearly reported. |
| Selective reporting (reporting bias) | High risk | Adverse effects data not reported. Efficacy data reported as ‘medication scores’: “The mean of daily scores recorded during the 7 days in which the highest doses were given was designated as the medication score.” Post medication scores reported for 22/30 subjects: “Post‐medication evaluations were followed in eight patients who received alpha‐methyldopa, nine patients who received placebo and in five patients who received reserpine.” |
| Other bias | Unclear risk | Baseline information available only for the premedication scores per group (groups are balanced). |
Karniol 1983.
| Methods | Allocation: "randomly" ‐ the drugs were given in sealed opaque envelope.
Blindness: double, described.
Design: parallel group.
Duration: 5 weeks. Setting: inpatients, Brazil. Rater: not described. |
|
| Participants | Diagnosis: 15 participants with schizophrenia, 2 with other associated psychosis, and 2 with effective psychosis and 1 mental retardation. N = 20. Sex: 10 M, 10 F. Age: 58.2 years. | |
| Interventions | 1. Placebo: starch pill. N = 5. 2. L‐dopa 500 mg: growing dosage per week. From the fourth week the dosage was 500 mg. N = 5. 3‐ L‐dopa 1000 mg: growing dosage per week. From the fourth week the dosage was 1000 mg. N = 5. 4‐ L‐dopa 2000 mg: growing dosage per week. From the fourth week the dosage was 2000 mg. N = 5. All participants were on antipsychotics for a period higher than 6 months, 17 participants were on antipsychotic at the study period, 9 participants were on anticholinergic and 8 had hypnotic or anticonvulsants. |
|
| Outcomes | TD symptoms: any improvement. Unable to use ‐ TD symptoms: Bordeleau scale/EBS (only medians reported). |
|
| Notes | Sponsorship source: not reported. Article in Portuguese; assessed and data extracted by Antonio Grande. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "participants were randomly assigned to each group". |
| Allocation concealment (selection bias) | Low risk | "the drugs were given in sealed opaque envelope". |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Each week a number of envelopes were given to the nurse containing a number, so only the researcher knew what was being administered. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not enough information in the study. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No mention about loss of follow‐up. |
| Selective reporting (reporting bias) | High risk | Author reported only TD score medians and there is no availability of study protocol. |
| Other bias | Low risk | The study seems to be free of other sources of bias. |
Kazamatsuri 1973.
| Methods | Allocation: "randomly".
Blindness: double.
Duration: 18 weeks.
Design: parallel. Setting: Inpatients, USA. Raters: "[.] a psychiatrist blind to the study design, was used to assess oral dyskinesia", "[.] the ward nurses, who were also blind to the study design, to assess the ward adjustment of the patients". |
|
| Participants | Diagnosis: chronic psychotic patients who manifested typical bucco‐linguo‐masticatory oral dyskinesia associated with long‐term antipsychotic medication.
N = 13.
Sex: 8 M, 5 F.
Age: mean 55.8 years, range 41 to 63 years. Duration of TD: no information available. |
|
| Interventions | 1. Haloperidol: dose 4 mg b.i.d. From week 15 dose was doubled to 16 mg/d. N = 7.
2. Tetrabenazine: dose 50 mg b.i.d. From week 15 onwards, dose was doubled to 200 mg/d. N = 6. Pre‐placebo period: initially, all antipsychotic and antiparkinsonian drugs were completely withdrawn and were replaced by placebo for the first 4 weeks. Other medications, such as antidiabetic or anticonvulsant drugs were continued unchanged. |
|
| Outcomes | TD symptoms: not improved. TD symptoms: deterioration. Leaving the study early. |
|
| Notes | Sponsorship source: supported in part by Public Health Service grant from the National institute of Mental Health. Tetrabenazine and placebo tablets were provided by Hoffman‐La Roche. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "The 13 patients were divided randomly into two groups"; further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding of participants and personnel not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "A frequency count of mouth movements, done by a psychiatrist blind to the study design, was used to assess oral dyskinesia". |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 2/7 (29%) subjects dropped out from the haloperidol group during the 18th week; no further details are provided for addressing the outcomes of these participants. No participants dropped out from the tetrabenazine group. |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all predefined outcomes have been reported. |
| Other bias | Unclear risk | Insufficient information to make a judgement. |
Pappa 2010.
| Methods | Allocation: "randomly assigned".
Blindness: double, identically appearing capsules.
Duration: 4 weeks and 4 days (2 weeks followed by 4 days wash‐out then another 2 weeks).
Design: cross‐over. Setting: outpatients, Greece. Raters: "Tardive dyskinesia was assessed by means of the Abnormal Involuntary Movements Scale (AIMS) by a blinded, experienced rater". |
|
| Participants | Diagnosis: schizophrenia and TD (DSM‐4) and stable psychiatric condition.
N = 22.
Sex: 14 M, 8 F.
Age: mean 52 years, range 32 to 68 years. Duration of TD: patients have been ill for 10 (SD 7) years and were receiving stable medical treatment. |
|
| Interventions | 1. Amantadine: dose 100 mg/d for 2 weeks (followed by 4‐day washout and 2 weeks of placebo). N = 11.
2. Placebo: 2 weeks (followed by 4‐day washout and 2 weeks of amantadine). N = 11. Patients received their usual antipsychotic treatment at the same dosage. |
|
| Outcomes | Leaving the study early. Unable to use ‐ changes in TD severity at baseline and endpoint using AIMS. Mental state: BPRS, MMSE, CGI. Adverse effects: insomnia, constipation, dizziness, headache. Study authors were contacted for additional data, no information was received. |
|
| Notes | Sponsorship source: there was no financial funding for this study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Eligible patients were randomly assigned to receive either amantadine or placebo"; further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Participants received identically appearing capsules containing either amantadine (100 mg) or placebo." "double blind", however the authors report that "Those unable to safely tolerate each succeeding dose returned to a lower dose for the remainder of the study or until they were able to tolerate a higher dose". This may have unblinded personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Tardive dyskinesia was assessed by means of the Abnormal Involuntary Movements Scale (AIMS) by a blinded, experienced rater". "All safety issues were handled by an unmasked safety officer who was not involved in data collection". |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "All 22 enrolled patients completed the study". |
| Selective reporting (reporting bias) | High risk | Many outcomes were not fully reported. TD outcomes: average scores (no SD), range and P for amantadine and placebo at baseline and end of the study have been reported. Mental state outcomes (BPRS, MMSE, CGI): average scores (no SD), range and P for amantadine and placebo reported only for end of study. |
| Other bias | Unclear risk | Insufficient information to make a judgement. |
Rust 1984.
| Methods | Allocation: "random".
Blindness: double.
Duration: 8 weeks.
Design: parallel. Setting: inpatients, France. Raters: not reported. |
|
| Participants | Diagnosis: schizophrenia (25), organic or affective psychoses, severe personality disorders + dyskinesia (mainly localized to the buccofacial region) induced by long‐term antipsychotic treatment.
N = 50.
Sex: 50 M.
Age: mean 48 years. Duration of TD: in both groups the dyskinesia had been present for an average period of 4 years. |
|
| Interventions | 1. Tiapride: dose 400 mg/d for the first 30 days followed by 600 mg/d for the next 30 days. N = 25.
2. Placebo for 8 weeks. N = 25. Throughout the course of the study the patients continued to take antipsychotics to avoid spontaneous remission or worsening of symptoms. Other associated medication such as anticholinergic drugs was not prescribed during the study. Patients had not been treated previously for their dyskinesia. |
|
| Outcomes | Leaving the study early. Unable to use ‐ TD symptoms: Skaub's scale (German version of AIMS) ‐ reduction of symptoms. |
|
| Notes | Sponsorship source: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "random allocation of either tiapride or placebo for 8 weeks"; further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind". Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double‐blind". Details not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "all patients continued in the study until the end of treatment." |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all predefined outcomes have been reported. Reduction of symptoms not fully reported. |
| Other bias | Unclear risk | Insufficient information to make a judgement. Baseline characteristic not reported per intervention group. Unclear if there were confounding variables. |
Simpson 1988.
| Methods | Allocation: "randomly assigned".
Blindness: double, identical‐appearing tablets.
Duration: 20 weeks (6 weeks observation, 4 weeks dose finding, 6 weeks' treatment, 4 weeks follow‐up).
Design: parallel. Setting: Inpatients from 2 chronic care institutions, USA. Raters: not reported. |
|
| Participants | Diagnosis: tardive dyskinesia in subjects treated with antipsychotics.
N = 17.
Sex: 8 M, 9 F.
Age: mean 46 years, range 32 to 70 years. Duration of TD: no information. |
|
| Interventions | 1. Carbidopa/levodopa: full dose: 50/350 mg/d (6 weeks of treatment, and 4 weeks of follow‐up after drug withdrawal). N = 9. 2. Placebo (6 weeks of treatment, and 4 weeks of follow‐up after drug withdrawal). N = 8. "When the appropriate dose was established in the dose finding period, patients received that dose for the next 6 weeks". Concomitant medication: no information. |
|
| Outcomes | TD symptoms: improvement and deterioration (AIMS and Simpson Abbreviated Dyskiesia Scale). Leaving the study early. Unable to use ‐ Treatment‐related side‐effects. Mental state: BPRS, SANS (F and P values only). |
|
| Notes | Sponsorship source: not reported. Medication and placebo supplied by Merck Sharp and Dohme, Rahway, NJ. (Unclear if medications were supplied free of charge). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomly assigned"; further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "active (Sinemet) or placebo tablets (supplied by Merck Sharp and Dohme, Rahway, NJ). Both groups of patients received the same number of identical‐appearing tablets." |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double‐blind". Details not reported. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | "Fifteen of the 17 patients completed the trial; there were two dropouts. A female patient experienced "seizures" and the blind was, therefore, broken; a male patient eloped from the hospital. Both patients were found to be in the placebo group." 25% dropped out from the placebo group versus 0% in the active medication group. According to the degrees of freedom in the F‐test, only completers must have been analysed. |
| Selective reporting (reporting bias) | High risk | "Because the AIMS and Simpson scale were very highly correlated, only data from the Simpson scale are presented." Also, mental state data (BPRS and SANS) unusable: reported as F and P values. Adverse Events (Treatment Emergent Side Effects Scale) outcome data not reported. |
| Other bias | Unclear risk | Insufficient information reported to make a judgement. |
Soni 1986.
| Methods | Allocation: "randomly allocated" unclear.
Blindness: double, unclear.
Duration: 24 weeks.
Design: parallel. Setting: Inpatients in a psychiatric hospital, UK. Raters: AIMS assessments were carried out by the same rater throughout the study and the rater was blind to the treatment. |
|
| Participants | Diagnosis: RDC criteria for chronic schizophrenia and associated TD.
N = 42. Sex: 25 M, 17 F. Age: mean 59 years, range 42 to 71 years. Duration of TD: TD present for at least 3 consecutive months. |
|
| Interventions | 1. Oxypertine: flexible dose 80 mg/d to 240 mg/d for 24 weeks. N = 20.
2. Placebo for 24 weeks. N = 22. "It was required that their psychiatric condition had been stable on conventional neuroleptic medication for at least 12 months before entry." Anticholinergic antiparkinsonian drugs already prescribed were maintained throughout the trial. The only other drug permitted was nitrazepam for insomnia (10 to 20 mg) but only when required. |
|
| Outcomes | Mental state: clinical relapse of psychosis. Leaving the study early. Unable to use ‐ Adverse events: AIMS, EPS (not fully reported). |
|
| Notes | Sponsorship source: Sterling Winthrop Ltd. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly allocated to either the treatment or the control group"; further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind", matched placebo. Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The AIMS assessment was carried out by the same rater throughout the study and the rater was blind to the treatment. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | "11 oxypertine and 7 placebo patients has withdrawn..." High overall rate of participants dropping out (45%): oxypertine group (55%) and placebo group (32%). |
| Selective reporting (reporting bias) | High risk | "Table 6 gives the results of only those analyses which showed a statistically significant change: non‐significant results are excluded." Global AIMS scores not reported. EPS data descriptively reported. |
| Other bias | Low risk | The study seems to have been free of other sources of bias. The 2 groups were well matched on specific baseline characteristics. |
General Acn ‐ anticholinergics Bz ‐ benzodiazepine CPE ‐ chlorpromazine equivalent
Scales AIMS ‐ Abnormal Involuntary Movement BRS ‐ Barnes & Kidger Rating GRS ‐ Gerlach Rating SEPS ‐ Smith Extrapyramidal SRS ‐ Simpson Rating Scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Adler 1990 | Allocation: randomised. Participants: people with schizophrenia and antipsychotic‐induced akathisia, not tardive dyskinesia. Interventions: metoprolol versus propranolol. |
| Alpert 1983 | Allocation: randomised. Participants: patients with tardive dyskinesia and at least 2‐year exposure to antipsychotic drugs. Intervention: carbidopa/levodopa 30/300 mg vs carbidopa/levodopa 50/500 mg vs carbidopa/levodopa 75/750 mg. A non‐randomised treatment as usual group was also included. Outcomes: not reported for the pre‐defined randomised groups. 5 subjects were randomised to 3 groups. N per group and baseline characteristics not reported. Data reported for “low dose” and “high dose” participants based on what appears to be a post hoc decision, and not for each intervention group separately. Study authors were contacted for data: no information was received and this over 30 years old study was excluded. |
| Angus 1997 | Allocation: randomised. Participants: chronically ill psychiatric inpatients with TD. Interventions: amantadine vs placebo. Outcomes: no usable data, not reported for the first phase before crossing over. No up‐to‐date contact details were found for the study authors of this 19‐year‐old study. |
| Asher 1981 | Allocation: not randomised. |
| Auberger 1985 | Allocation: double blind, cross‐over.
Participants: people with chronic tardive dyskinesia.
Interventions: tiapride versus placebo.
Outcomes: no usable data, not reported for the first phase before crossing over. No up‐to‐date contact details were found for the study authors of this over 30‐year‐old study. |
| Bateman 1979 | Allocation: randomised. Participants: people with schizophrenia and antipsychotic induced tardive dyskinesia. Intervention: placebo versus haloperidol versus metoclopramide. Outcomes: no usable data, not reported for the first phase before crossing over. No up‐to‐date contact details were found for the study authors of this over 35‐year‐old study. |
| Braun 1989 | Allocation: unclear; "double‐blind crossover".
Participants: Huntington’s disease (5), Tourette’s syndrome (2), tardive dyskinesia (2), idiopathic torsion dystonia (1).
Intervention: SKF 38393 (selective D‐l dopamine receptor agonist) versus placebo.
Outcomes: no usable data, not reported for the first phase before crossing over. We were unable to identify up‐to‐date study author contact details for this over 25‐year‐old study. |
| Browne 1986a | Allocation: randomised. Participants: adult outpatients suffering with antipsychotic‐induced tardive dyskinesia. Intervention: sodium valproate versus oxypertine versus deanol versus placebo. Outcomes: no usable data, not reported for the first phase before crossing over. We were unable to identify up‐to‐date study author contact details for this 30‐year‐old study. |
| Chien 1978 | Allocation: randomised.
Participants: people with TD.
Intervention: sodium valproate versus oxypertine versus deanol.
Outcomes: no usable data, not reported for the first phase before crossing over. We were unable to identify up‐to‐date study author contact details for this over 35 year‐old‐study. |
| Chouza 1982 | Allocation: not randomised. |
| Delwaide 1979 | Allocation: randomised.
Participants: hospitalised patients with tardive dyskinesia on a psychogeriatric ward.
Intervention: thiperazine versus tiapride versus placebo.
Outcomes: no usable data, not reported for the first phase before crossing over. The study is over 35 years old and we were unable to identify contact details for the author. |
| Delwaide 1980 | Allocation: not randomised.
Participants: people with dementia and TD. Intervention: all participants were started on placebo and then switched to bromocriptine. |
| Diehl 1999 | Allocation: randomised. Participants: tardive oro‐facial dyskinesia. Intervention: pergolid 0,15 mg/d vs placebo. Outcomes: results not reported for the studied outcomes (irrespective of cross‐over period). Study authors were contacted for data. No information was received and this over 15‐year‐old study was excluded. |
| DiMascio 1976 | Allocation: randomised. Participants: people with schizophrenia and extrapyramidal side effects, no TD measure at baseline, not stable dose of antipsychotics. Interventions: amantadine hydrochloride versus Benztropine mesylate. |
| Doongaji 1982 | Allocation: randomised. Participants: diagnosis of TD. Interventions: metoclopramide vs placebo. Outcomes: no usable data, not reported for the first phase before crossing over. Study authors were contacted but no information was received. Consequently, this over 30‐year‐old study was excluded. |
| Fahn 1983 | Allocation: not randomised. |
| Fann 1976 | Allocation: randomised.
Participants: no TD symptoms at baseline. Intervention: amantadine vs trihexyphenidyl. |
| Ferrari 1972 | Allocation: not randomised. |
| Freeman 1980 | Allocation: randomisation implied.
Participants: people with schizophrenia and tardive dyskinesia.
Intervention: oxypertine versus placebo.
Outcomes: no usable data, not reported for the first phase before crossing over. No up‐to‐date contact details were found for the study authors of this over 35 years old study. |
| Gardos 1979 | Allocation: randomised. Participants: adult inpatients. Intervention: papaverine versus placebo. Outcomes: no usable data, not reported for the first phase before crossing over. No up‐to‐date contact details were found for the study authors of this over 35‐year‐old study. |
| Gerlach 1976 | Allocation: not randomised, controlled clinical trial. |
| Glover 1980 | Allocation: randomised. Participants: adult patients with significant antipsychotic‐induced tardive dyskinesia. Intervention: amantadine versus placebo. Outcomes: no usable data, not reported for the first phase before crossing over. No up‐to‐date contact details were found for the study authors of this over 35 year‐old‐study. |
| Godwin Austen 1971 | Allocation: randomised.
Participants: people with moderate to severe dementia and antipsychotic induced tardive dyskinesia. Intervention: diazepam vs tetrabenazine. Outcomes: no usable data, not reported for the first phase before crossing over. Study is over 40 years old, we were unable to identify contact details for the authors. |
| Goff 1993 | Allocation: randomised. Participants: antipsychotic‐induced tardive dyskinesia according to DSM‐III‐R (SCID), Schooler and Kane criteria. Interventions: selegiline vs placebo. Included in Miscellaneous review. |
| Greendyke 1988 | Allocation: randomised. Participants: psychiatric inpatients with TD. Interventions: pindolol versus placebo. Outcomes: no usable data reported in this brief report. No up‐to‐date contact details were found for the study authors of this over 25‐year‐old study. |
| Gutierrez 1979 | Allocation: randomised. Participants: people with schizophrenia and extrapyramidal symptoms, not tardive dyskinesia. Intervention: L‐dopa versus placebo. |
| Hemnani 1982 | Allocation: randomised. Participants: people with a TD diagnosis. Interventions: metoclopramide 10 mg vs metoclopramide 20 mg vs metoclopramide 40 mg vs placebo. Outcomes: no usable data, not reported for the first phase before crossing over. Study authors were contacted but no information was received. Consequently, this over 30‐year‐old study was excluded. |
| Jankovic 1982 | Allocation: randomised. Participants: various hyperkinetic movement disorders; dose of antipsychotic medication was not stable: "All medications were either discontinued 1 week before the study or continued at the same dosage throughout the study" |
| Jeste 1983 | Allocation: randomised. Participants: schizophrenia patients (Research Diagnostic Criteria; antipsychotic therapy; good physical condition). 5/11 were diagnosed as having TD. 1 TD patient also had tardive Tourette's syndrome. Interventions: apomorphine vs bromocriptine vs placebo. Outcomes: no usable data, not reported for the first phase before crossing over. Study authors were contacted but no information was received. Consequently, this over 30‐year‐old study was excluded. |
| Kazamatsuri 1972 | Allocation: not randomised. |
| Konig 1996 | Allocation: not randomised, controlled clinical trial. Participants: no TD ratings at baseline. Interventions: amantadine vs biperiden. |
| Leblhuber 1987 | Allocation: not randomised. |
| Levy 1984 | Allocation: not randomised. |
| Lieberman 1988 | Allocation: randomised.
Participants: TD according to the criteria of Schooler and Kane, schizophrenia, schizoaffective disorder, major affective disorder and attention deficit disorder. Intervention: physostigmine vs bromocriptine vs benztropine vs haloperidol for 1 day, then crossed over. Outcomes: no usable data, not reported for the first phase before crossing over. Author was contacted but no information was received and this over 25 year‐old‐study was excluded. |
| Lieberman 1989 | Allocation: randomised.
Participants: psychiatric patients with persistent TD,N = 18, participants not on stable dose for a month at study entry. Intervention: bromocriptive vs placebo. |
| Ludatscher 1989 | Allocation: randomised.
Participants: chronic schizophrenics who had symptoms of severe persistent TD and who had been treated with antipsychotics. Intervention: L‐dopa 500 mg + carbidopa 50 mg/d + low dose antipsychotics vs placebo + anticholinergic medication + low dose antipsychotic. Outcomes: no outcome data could be used. The study is over 25 years old and we were unable to identify contact details for the author. |
| Nasrallah 1986 | Allocation: randomised, cross‐over design.
Participants: psychiatric patients with persistent TD (Schooler and Kane criteria). N = 25. Interventions: alpha‐methyl‐p‐tyrosine (AMPT) vs L‐dihydroxyphenylalanine vs choline chloride vs valproic acid vs hydroxytryptophan. Outcomes: no usable data, not reported for the first phase before crossing over. Authors were contacted and no reply was received. Consequently, this 30‐year‐old study was excluded. |
| NCT00310661 2006 | Allocation: randomised. Participants: people with Parkinson's disease, not tardive dyskinesia. |
| NCT00845000 2009 | Allocation: randomised. Participants: people with Parkinson's disease, not tardive dyskinesia. |
| O'Suilleabhain 2003 | Allocation: randomised. Participants: people with Huntington's disease, not tardive dyskinesia. |
| Reker 1982 | Allocation: unclear. Participants: "psychiatric patients with tardive dyskinesia". Interventions: naloxone versus placebo. Outcomes: no usable data. |
| Ringwald 1978 | Allocation: not randomised. |
| Rondot 1987 | Allocation: not randomised, double blind. Participants: people with schizophrenia. Interventions: progabide for 6 weeks followed by placebo, no parallel arm. |
| Silver 1995 | Allocation: randomised. Participants: people with schizophrenia with and without TD. Interventions: biperiden vs amantadine. Outcomes: unable to use data. No up‐to‐date contact details were found for the study authors of this over 20‐year‐old study. |
| Smith 1977 | Allocation: not randomised. |
| Stearns 1996 | Allocation: randomised. Participants: schizophrenia patients. Interventions: selegiline versus placebo. Outcomes: no usable data, not reported for the first phase before crossing over. We contacted study authors that replied, but no further data were available. |
| Tamminga 1980 | Allocation: randomised. Participants: antipsychotic‐free schizophrenia patients with TD. Interventions: CF 25‐397 vs bromocriptine vs placebo. Outcomes: no usable data, not reported for the first phase before crossing over. Study authors were contacted but no information was received. Consequently, this over 35‐year‐old study was excluded. |
| Viukari 1975 | Allocation: randomised. Participants: psychogeriatric patients treated with antipsychotics with severe dyskinesia for at least a year. Interventions: methyldopa versus placebo. Outcomes: no usable data, not reported for the first phase before crossing over. Study is over 40 years old, we were unable to identify contact details for the authors. |
GVG ‐ Gamma‐vynil GABA; GAG ‐ Gamma‐acetylenic GABA; THIP ‐ TetrahydroisoxazolopyridinolSCD ‐ Saccadic distractibility; Sz ‐ Schizophrenia; TD ‐ Tardive dyskinesia
Differences between protocol and review
The protocol as published with this review has evolved over time. The revisions of protocol are in line with the development of RevMan and in keeping with Cochrane guidance. We think the revisions have greatly improved and enhanced this review. We do not think, however, that it has materially affected our conduct of the review or interpretation of the results.
In the 2017 review update, the biggest changes to affect the review methods were to:
broaden the inclusion criteria, and add the comparison 'Non‐antipsychotic catecholaminergic drug vs other drug';
change the title from 'Non‐neuroleptic catecholaminergic drugs for neuroleptic‐induced tardive dyskinesia' to 'Non‐antipsychotic catecholaminergic drugs for antipsychotic‐induced tardive dyskinesia';
update list of outcomes following consultation with consumers; and
add 'Summary of findings' tables.
Previous methods are reproduced in Appendix 1.
Contributions of authors
Hany El‐Sayeh ‐ protocol updating, searching, trial selection, data extraction and assimilation (original version).
John Rathbone ‐ selected studies, data extraction, data assimilation (original version).
Karla Soares‐Weiser ‐ protocol writing, searching, trial selection, data extraction and assimilation (original version).
Hanna Bergman ‐ 2017 update: trial selection, data extraction and assimilation, 'Summary of findings' tables, report writing (2017 update).
Sources of support
Internal sources
CAPES ‐ Ministry of Education, Brazil.
Universidade Federal de Sao Paulo, Brazil.
Academic Unit of Psychiatry, Leeds., UK.
-
Enhance Reviews Ltd., UK.
Logistics support for Hanna Bergman for the 2016 update.
External sources
-
NIHR HTA Project Grant, reference number: 14/27/02, UK.
Salary support for Hanna Bergman. Support for patient involvement consultation. Support for traceable data database.
Declarations of interest
None known.
KSW is the Deputy Editor‐in‐Chief for Cochrane and Cochrane Innovations. When the NHIR HTA programme grant relevant to this review update was awarded, KSW was the Managing Director of Enhance Reviews Ltd.
HB worked for Enhance Reviews Ltd. during preparation of this review and was paid for her contribution to this review. Enhance Reviews Ltd. was a private company that performs systematic reviews of literature. HB works for Cochrane Response, an evidence consultancy that takes commissions from healthcare guideline developers and policy makers.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Buruma 1982 {published data only}
- Buruma OJS, Roos RAC, Bruyn GW. Tiapride in the treatment of tardive dyskinesia. Acta Neurologica Scandinavica 1982;65(1):38‐44. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Roos RAC, Buruma OJS, Bruyn GW, Kemp B, vd Velde EA, Zelvelder WG. Tiapride in Huntington's chorea and tardive dyskinesia. A double‐blind, placebo controlled crossover clinical trial [Tiaprid bij chorea van Huntington en tardieve dyskinesie. Een dubbelblind, placebo‐gecontroleerd cross‐overonderzoek]. Tijdschrift voor Geneesmiddelenonderzoek 1982;7(2):1234‐9. [Google Scholar]
Chen 1995 {published data only}
- Chen J, Zhong X, Cao Z. A double‐blind auto‐control study on the effect of bromocriptine on tardive dyskinesia. Chinese Journal of Pharmaco Epiolemiology 1995;4(4):203‐5. [MEDI95S5] [Google Scholar]
Hebenstreit 1986 {published data only}
- Hebenstreit GF, Hoffmann H, Hoffmann W, Pittner H. Beta blockade with celiprolol in tardive dyskinesia patients treated with neuroleptics [Betablockade mit Celiprolol bei Neuroleptikabehandelten Patienten mit Tardiver Dyskinesie]. Wiener Klinische Wochenschrift 1986;98(12):388‐92. [MEDLINE: ] [PubMed] [Google Scholar]
Huang 1981 {published data only}
- Huang CC, Wang RIH, Hasegawa A, Alverno L. Evaluation of reserpine and alpha‐methyldopa in the treatment of tardive dyskinesia. Psychopharmacology Bulletin 1980;16:41‐3. [PubMed] [Google Scholar]
- Huang CC, Wang RIH, Hasegawa A, Alverno L. Reserpine and alpha‐methyldopa in the treatment of tardive dyskinesia. Psychopharmacology 1981;73:359‐62. [DOI] [PubMed] [Google Scholar]
Karniol 1983 {published data only}
- Karniol G, Giampietro AC, Moura DSP, Vilela WA, Oliveira MA, Zuardi AW. A double‐blind study of the effect of L‐dopa in psychotic patients with tardive dyskinesia [Estudo duplo‐cego sobre a ação de L‐dopa em pacientes psicóticos com discinesia tardia]. Acta Psiquiatrica y Psicologica de America Latina 1983;29:261‐6. [PubMed] [Google Scholar]
Kazamatsuri 1973 {published data only}
- Kazamatsuri H, Chien CP, Cole JO. Long‐term treatment of tardive dyskinesia with haloperidol and tetrabenazine. American Journal of Psychiatry 1973;130(4):479‐83. [DOI] [PubMed] [Google Scholar]
Pappa 2010 {published data only}
- Pappa S, Tsouli S, Apostolou G, Mavreas V, Konitsiotis S. Effects of amantadine on tardive dyskinesia: a randomized, double‐blind, placebo‐controlled study. Clinical Neuropharmacology 2010;33(6):271‐5. [DOI] [PubMed] [Google Scholar]
- Pappa S, Tsouli S, Apostolou G, Mavreas V, Konitsiotis S. Efficacy of amantadine in the treatment of tardive dyskinesia: a randomized, double‐blind, placebo‐controlled study. 9th World Congress of Biological Psychiatry; 28 June‐2 July 2009; Paris, France. 2009:171.
- Pappa S, Tzouli S, Mavreas V, Konitsiotis S. Efficacy of an NMDA receptor antagonist in the treatment of tardive dyskinesia: A randomized, double‐blind, placebo‐controlled study. Schizophrenia Research 2012;136:S358. [Google Scholar]
Rust 1984 {published data only}
- Rust M. Tiapride treatment of tardive dyskinesia due to long‐term neuroleptic treatment. Semaine des Hopitaux 1984;60(30):2195‐6. [Google Scholar]
Simpson 1988 {published data only}
- Simpson GM, Yadalam KG, Stephanos MJ. Double‐blind carbidopa‐levodopa and placebo study in tardive dyskinesia. Journal of Clinical Psychopharmacology 1988;8(Suppl 4):S49‐51. [PubMed] [Google Scholar]
Soni 1986 {published data only}
- Soni SD, Freeman HL, Bamrah JS, Sampath G. Oxypertine in tardive dyskinesia: a long‐term controlled study. Acta Psychiatrica Scandinavica 1986;74(5):446‐50. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Adler 1990 {published data only}
- Adler LA, Angrist B, Rotrosen J. Metoprolol versus propranolol. Biological Psychiatry 1990;27(6):673‐5. [MEDLINE: ; PMID 1969753] [DOI] [PubMed] [Google Scholar]
Alpert 1983 {published data only}
- Alpert M, Friedhoff AJ, Diamond F. Use of dopamine receptor agonists to reduce dopamine receptor number as treatment for tardive dyskinesia. Advances in Neurology 1983;37:253‐8. [PubMed] [Google Scholar]
Angus 1997 {published data only}
- Angus S, Sugars J, Boltezar R, Koskewich S, Schneider NM. A controlled trial of amantadine hydrochloride and neuroleptics in the treatment of tardive dyskinesia. Journal of Clinical Psychopharmacology 1997;17(2):88‐91. [DOI] [PubMed] [Google Scholar]
Asher 1981 {published data only}
- Asher S, Aminoff MJ. Tetrabenazine and movement disorders. Neurology 1981;31(8):1051‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Auberger 1985 {published data only}
- Auberger S, Greil W, Ruther E. Tiapride in the treatment of tardive dyskinesia. A double‐blind study. Pharmacopsychiatry 1985;18(1):61‐2. [MEDLINE: ; PMID 6124989]6124989 [Google Scholar]
- Greil W, Auberger S, Haag H, Ruther E. Tiapride: effects on tardive dyskinesia and on prolactin plasma concentrations. Neuropsychobiology 1985;14(1):17‐22. [DOI] [PubMed] [Google Scholar]
Bateman 1979 {published data only}
- Bateman DN, Dutta DK, McClelland HA, Rawlins MD. Metoclopramide and haloperidol in tardive dyskinesia. British Journal of Psychiatry 1979;135:505‐8. [DOI] [PubMed] [Google Scholar]
- Bateman DN, Dutta DK, McClelland HA, Rawlins MD. The effect of metoclopramide and haloperidol on tardive dyskinesia. British Journal of Pharmacology 1979;66(3):475‐6. [PMC free article] [PubMed] [Google Scholar]
Braun 1989 {published data only}
- Braun A, Mouradian MM, Mohr E, Fabbrini G, Chase TN. Selective D‐1 dopamine receptor agonist effects in hyperkinetic extrapyramidal disorders. Journal of Neurology, Neurosurgery, and Psychiatry 1989;52(5):631‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Browne 1986a {published data only}
- Browne J, Silver H, Martin R, Hart R, Mergener M, Williams P. The use of clonidine in the treatment of neuroleptic induced tardive dyskinesia. Journal of Clinical Psychopharmacology 1986;6(2):88‐92. [PubMed] [Google Scholar]
Chien 1978 {published data only}
- Chien CP, Jung K, Ross‐Townsend A. Efficacies of agents related to GABA, dopamine, and acetylcholine in the treatment of tardive dyskinesia. Psychopharmacology Bulletin 1978;14(2):20‐2. [MEDLINE: ] [PubMed] [Google Scholar]
Chouza 1982 {published data only}
- Chouza C, Romero S, Lorenzo J, Camano JL, Fontana AP, Alterwain P, et al. Clinical trial of tiapride in patients with dyskinesia. Semaine des Hopitaux 1982;58:725‐33. [PubMed] [Google Scholar]
Delwaide 1979 {published data only}
- Delwaide PJ, Desseilles M. Controlled therapeutic study of spontaneous bucco‐linguo‐facial dyskinesias (author's translation) [Etude therapeutique controlee des dyskinesies bucco‐linguo‐faciales spontanees]. Semaine des Hopitaux 1979;55(35‐6):1585‐9. [MEDLINE: ] [PubMed] [Google Scholar]
Delwaide 1980 {published data only}
- Delwaide P, Hurlet A. Bromocriptine and Buccolinguofacial Dyskinesias in Patients With Senile Dementia. Archives of Neurology 1980;37(7):441‐3. [DOI] [PubMed] [Google Scholar]
Diehl 1999 {published data only}
- Diehl A, Braus DF, Buchel C, Krumm B, Medori, R, Gattaz WF. Tardive dyskinesia: pergolid, a possible therapeutic option [Tardive Dyskinesien: Pergolid als mögliche therapeutische Option]. Psychiatrische Praxis 2003;30:333‐7. [DOI] [PubMed] [Google Scholar]
- Diehl A, Dittmann RW, Gattaz W, Rubin M, Hundemer HP. Low dose pergolide in the treatment of tardive dyskinesia (td): a double blind, placebo controlled randomised cross over trial. 11th World Congress of Psychiatry; 1999 Aug 6‐11; Hamburg, Germany. 1999:243.
- Diehl A, Hundemer HP, Rubin M, Dittmann RW, Gattaz W. Low‐dose pergolide in the treatment of tardive dyskinesia (TD): a double‐blind, placebo‐controlled randomized cross‐over trial. Journal of the European College of Neuropsychopharmacology. 1999:S359. [MEDLINE: ]
DiMascio 1976 {published data only}
- DiMascio A, Bernardo DL, Greenblatt DJ, Marder JE. A controlled trial of amantadine in drug‐induced extrapyramidal disorders. Archives of General Psychiatry 1976;33(5):599‐602. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- DiMascio A, Bernardo DL, Greenblatt DJ, Marder JE. A controlled trial of amantadine in drug‐induced extrapyramidal disorders. Psychopharmacology Bulletin 1977;13(3):31‐3. [PubMed] [Google Scholar]
Doongaji 1982 {published data only}
- Doongaji DR, Jeste DV, Jape NM. Effects of intravenous metoclopramide in 81 patients with tardive dyskinesia. Journal of Clinical Psychopharmacology 1982;2(6):376‐9. [PubMed] [Google Scholar]
Fahn 1983 {published data only}
- Fahn S. Long term treatment of tardive dyskinesia with presynaptically acting dopamine‐depleting agents. In: Fahn S, Calne DB, Shoalson I editor(s). Advances in Neurology: Experimental Therapeutics of Movement Disorders. New York: Raven Press, 1983:267‐76. [PubMed] [Google Scholar]
Fann 1976 {published data only}
- Fann WE, Lake CR. Amantadine versus trihexyphenidyl in the treatment of neuroleptic‐induced parkinsonism. American Journal of Psychiatry 1976;133(8):940‐3. [DOI] [PubMed] [Google Scholar]
Ferrari 1972 {published data only}
- Ferrari P, Robotti E, Nardini M. Experimental design of a pilot study on amantadine in the extrapyramidal syndrome induced by neuroleptic drugs [Disegno sperimentale di uno studio pilota sull'amantadina nella sindrome extrapiramidale da farmaci neurolettici]. Bollettino Chimico Farmaceutico 1972;111(10):610‐5. [MEDLINE: ] [PubMed] [Google Scholar]
Freeman 1980 {published data only}
- Freeman HL, Soni SD, Carpenter L. A controlled trial of oxypertine in tardive dyskinesia. International Pharmacopsychiatry 1980;15(5):281‐91. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Gardos 1979 {published data only}
- Gardos G, Granacher RP, Cole JO, Sniffin C. The effects of papaverine in tardive dyskinesia. Progress in Neuro‐Psychopharmacology and Biological Psychiatry 1979;3(5‐6):543‐50. [DOI] [PubMed] [Google Scholar]
Gerlach 1976 {published data only}
- Gerlach J. The relationship betwen parkisonism and tardive dyskinesia. American Journal of Psychiatry 1977;134(7):781‐4. [DOI] [PubMed] [Google Scholar]
- Gerlach J, Thorsen K. The movement pattern of oral tardive dyskinesia in relation to anticholinergic and antidopaminergic treatment. Internal Pharmacopsychiatry 1976;11(1):1‐7. [DOI] [PubMed] [Google Scholar]
Glover 1980 {published data only}
- Glover O. Alternative treatment modalities for drug induced psychomotor dysfunctions. PhD dissertation submitted to the Wright Institute 1980:150.
Godwin Austen 1971 {published data only}
- Godwin Austen RB, Clarke T. Persistant phenothiazine dyskinesia treated with tetrabenazine. British Medical Journal 1971;4:25‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Goff 1993 {published data only}
- Goff DC, Renshaw PF, Sarid‐Segal O, Dreyfuss DA, Amico ET, Ciraulo DA. A placebo‐controlled trial of selegiline (L‐deprenyl) in the treatment of tardive dyskinesia. Biological Psychiatry 1993;33(10):700‐6. [DOI] [PubMed] [Google Scholar]
Greendyke 1988 {published data only}
- Greendyke RM, Webster JC, Kim J, Kim H. Lack of efficacy of pindolol in tardive dyskinesia. American Journal of Psychiatry 1988;145(10):1318‐9. [DOI] [PubMed] [Google Scholar]
Gutierrez 1979 {published data only}
- Gutierrez M, Alpert M, Guimon J, Friedhoff AJ, Veramendi V. Controlled study on the possibilities of L‐dopa in the residual extrapyramidal syndrome caused by neuroleptics [Un estudio controlado sobre las posibilidades de la L‐dopa en el sindrome extrapiramidal residual producido por los neurolepticos]. Actas Luso Espanolas de Neurologia Psiquiatria y Ciencias Afines 1979;7(3):181‐8. [MEDLINE: ] [PubMed] [Google Scholar]
Hemnani 1982 {published data only}
- Hemnani TJ, Dashputra PG, Sarda RN. Metoclopramide in tardive dyskinesia. Indian Journal of Pharmacology 1982;14(4):309‐12. [PMC free article] [PubMed] [Google Scholar]
- Hemnani TJ, Dashputra PG, Sarda RN. Metoclopramide in tardive dyskinesia. Indian Journal of Psychiatry 1983;25(2):134‐7. [PMC free article] [PubMed] [Google Scholar]
Jankovic 1982 {published data only}
- Jankovic J. Treatment of hyperkinetic movement disorders with tetrabenazine: a double‐blind crossover study. Annals of Neurology 1982;11(1):41‐7. [DOI] [PubMed] [Google Scholar]
Jeste 1983 {published data only}
- Jeste DV, Cutler NR, Kaufman CA, Karoum F. Low‐dose apomorphine and bromocriptine in neuroleptic‐induced movement disorders. Biological Psychiatry 1983;18(9):1085‐91. [PubMed] [Google Scholar]
Kazamatsuri 1972 {published data only}
- Kazamatsuri H, Chien C, Cole JO. Treatment of tardive dyskinesia. I. Clinical efficacy of a dopamine‐depleting agent, tetrabenazine. Archives of General Psychiatry 1972;27(1):95‐9. [DOI] [PubMed] [Google Scholar]
Konig 1996 {published data only}
- Konig P, Chwatal K, Havelec L, Riedl F, Schubert H, Schultes H. Amantadine versus biperiden ‐ a double‐blind study of treatment efficacy in neuroleptic extrapyramidal movement disorders. Neuropsychobiology 1996;33(2):80‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Leblhuber 1987 {published data only}
- Leblhuber F. Treatment of permanent tardive dyskinesia with tiapride, a selective D2‐receptor blocking agent. Clinical Neuropharmacology 1987;10(5):458‐61. [DOI] [PubMed] [Google Scholar]
Levy 1984 {published data only}
- Levy MI, Davis BM, Mohs RC, Kendler KS, Mathe AA, Trigos G, et al. Apomorphine and schizophrenia. Treatment, CSF, and neuroendocrine responses. Archives of General Psychiatry 1984;41(5):520‐4. [DOI] [PubMed] [Google Scholar]
Lieberman 1988 {published data only}
- Lieberman J, Pollack S, Lesser M, Kane J. Pharmacologic characterization of tardive dyskinesia. Journal of Clinical Psychopharmacology 1988;8(4):254‐60. [PubMed] [Google Scholar]
Lieberman 1989 {published data only}
- Lieberman JA, Alvir J, Mukherjee S, Kane JM. Treatment of tardive dyskinesia with bromocriptine. A test of the receptor modification strategy. Archives of General Psychiatry 1989;46(10):908‐13. [DOI] [PubMed] [Google Scholar]
- Perovich RM, Lieberman JA, Fleischhacker WW, Alvir J. The behavioral toxicity of bromocriptine in patients with psychiatric illness. Journal of Clinical Psychopharmacology 1989;9(6):417‐22. [PubMed] [Google Scholar]
Ludatscher 1989 {published data only}
- Ludatscher JI. Stable remission of tardive dyskinesia by L‐dopa. Journal of Clinical Psychopharmacology 1989;9(1):39‐41. [PubMed] [Google Scholar]
Nasrallah 1986 {published data only}
- Nasrallah HA, Dunner FJ, McCalley‐Whitters M, Smith RE. Pharmacologic probes of neurotransmitter systems in tardive dyskinesia: Implications for clinical management. Journal of Clinical Psychiatry 1986;47(2):56‐9. [PubMed] [Google Scholar]
NCT00310661 2006 {published data only}
- NCT00310661. A dual‐centre, double‐blind, randomized, placebo‐controlled, parallel‐group study to determine the effects of various adjunctive doses of sarizotan in the treatment of patients with neuroleptic‐induced tardive dyskinesia. www.ClinicalTrials.gov (accessed on 29 May 2016).
NCT00845000 2009 {published data only}
- NCT00845000. Acute effects of SCH 420814 on dyskinesia and Parkinsonism in levodopa treated patients. www.ClinicalTrials.gov (accessed on 29 May 2016).
O'Suilleabhain 2003 {published data only}
- O'Suilleabhain P, Dewey RB. A randomized trial of amantadine in Huntington disease. Archives of Neurology 2003;60(7):996‐8. [DOI] [PubMed] [Google Scholar]
Reker 1982 {published data only}
- Reker D, Anderson B, Yackulic C. Naloxone, tardive dyskinesia, and endogenous beta‐endorphin. Psychiatry Research 1982;7(3):321‐4. [DOI] [PubMed] [Google Scholar]
Ringwald 1978 {published data only}
- Ringwald E. Dopamine‐receptor stimulators and neuroleptic‐induced dyskinesia (author's transl). Pharmakopsychiatrie und Neuropsychopharmakologie 1978;11:294‐8. [DOI] [PubMed] [Google Scholar]
Rondot 1987 {published data only}
- Rondot P, Bathien N. Movement disorders in patients with coexistent neuroleptic‐induced tremor and tardive dyskinesia: EMG and pharmacological study. Advances in Neurology 1987;45:361‐6. [MEDLINE: ; PMID 2881446] [PubMed] [Google Scholar]
Silver 1995 {published data only}
- Silver H, Geraisy N, Schwartz M. No difference in the effect of biperiden and amantadine on Parkisonian‐ and tardive dyskinesia‐type involuntary movements: a double‐blind crossover, placebo‐controlled study in medicated chronic schizophrenic patients. Journal of Clinical Psychiatry 1995;56(4):167‐70. [PubMed] [Google Scholar]
- Silver H, Geraisy N, Schwartz M. No difference in the effect of biperiden and amantadine on parkinsonian‐ and tardive dyskinesia‐type involuntary movements: A double‐ blind crossover, PLACEBO‐controlled study in medicated chronic schizophrenic patients. Journal of Clinical Psychiatry 1995;56(9):435. [PubMed] [Google Scholar]
Smith 1977 {published data only}
- Smith RC, Tamminga CA, Haraszti J, Pandey GN, Davis JM. Effects of dopamine agonists in tardive dyskinesia. American Journal of Psychiatry 1977;134(7):763‐8. [DOI] [PubMed] [Google Scholar]
Stearns 1996 {published data only}
- Stearns AI, Sambunaris A, Elkashef AM, Issa F, Egan MF, Wyatt RJ. Selegiline for negative symptoms and tardive dyskinesia. Proceedings of the 149th Annual Meeting of the American Psychiatric Association; 1996 May 4‐9; New York, USA. American Psychiatric Association, 1996.
Tamminga 1980 {published data only}
- Tamminga CA, Chase TN. Bromocriptine and CF 25‐397 in the treatment of tardive dyskinesia. Archives of Neurology 1980;37(4):204‐5. [DOI] [PubMed] [Google Scholar]
Viukari 1975 {published data only}
- Viukari M, Linnoila M. Effect of methyldopa on tardive dyskinesia in psychogeriatric patients. Current Therapeutic Research, Clinical and Experimental 1975;18(3):417‐24. [PubMed] [Google Scholar]
Additional references
Alabed 2011
- Alabed S, Latifeh Y, Mohammad HA, Rifai A. Gamma‐aminobutyric acid agonists for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2011, Issue 4. [DOI: 10.1002/14651858.CD000203.pub3] [DOI] [PubMed] [Google Scholar]
Altman 1996
- Altman DG, Bland JM. Detecting skewness from summary information. BMJ 1996;313(7066):1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
APA 1992
- Tardive dyskinesia: a task force report of the American Psychiatric Association. American Psychiatric Association. Washington DC, 1992.
Armitage 1991
- Armitage P. Should we cross off the crossover?. Journal of Clinical Pharmacology 1991;32:1‐2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ascher‐Svanum 2008
- Ascher‐Svanum H, Zhu B, Faries D, Peng X, Kinon BJ, Tohen M. Tardive dyskinesia and the 3‐year course of schizophrenia: results from a large, prospective, naturalistic study. Journal of Clinical Psychiatry 2008;69(10):1580‐8. [DOI] [PubMed] [Google Scholar]
Ballesteros 2000
- Ballesteros J, Gonzalez‐Pinto A, Bulbena A. Tardive dyskinesia associated with higher mortality in psychiatric patients: results of a meta‐analysis of seven independent studies. Journal of Clinical Psychopharmacology 2000;20(2):188‐94. [DOI] [PubMed] [Google Scholar]
Barnes 1993
- Barnes TRE, Edwards JG. The side‐effects of antipsychotic drugs. I. CNS and neuromuscular effects. In: Barnes TRE editor(s). Antipsychotic drugs and their side‐effects. London: Academic Press. Harcourt Brace & Company, Publishers, 1993. [Google Scholar]
Begg 1996
- Begg C, Cho M, Eastwood S, Horton R, Moher D, Olkin I, et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA 1996;276(8):637‐9. [PUBMED: 8773637] [DOI] [PubMed] [Google Scholar]
Bergen 1989
- Bergen JA, Eyland EA, Campbell JA. The course of tardive dyskinesia in patients on long‐term neuroleptics. British Journal of Psychiatry 1989;154:523‐8. [DOI] [PubMed] [Google Scholar]
Bergman 2017
- Bergman H, Walker DM, Nikolakopoulou A, Soares‐Weiser K, Adams CE. Systematic review of interventions for treating or preventing antipsychotic‐induced tardive dyskinesia. Health Technol Assess 2017 Aug;21(43):1‐218. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bhoopathi 2006
- Bhoopathi PS, Soares‐Weiser K. Benzodiazepines for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2006, Issue 3. [DOI: 10.1002/14651858.CD000205.pub2] [DOI] [PubMed] [Google Scholar]
Bland 1997
- Bland JM. Statistics notes. Trials randomised in clusters. BMJ 1997;315:600. [DOI] [PMC free article] [PubMed] [Google Scholar]
Boissel 1999
- Boissel JP, Cucherat M, Li W, Chatellier G, Gueyffier F, Buyse M, et al. The problem of therapeutic efficacy indices. 3. Comparison of the indices and their use [Apercu sur la problematique des indices d'efficacite therapeutique, 3: comparaison des indices et utilisation. Groupe d'Etude des Indices D'efficacite]. Therapie 1999;54(4):405‐11. [PUBMED: 10667106] [PubMed] [Google Scholar]
Browne 1986b
- Browne J, Silver H, Martin R, Hart R, Mergener M, Willians P. The use of clonidine in the treatment of neuroleptic‐induced tardive dyskinesia. Journal of Clinical Psychopharmacology 1986;6(2):88‐92. [PubMed] [Google Scholar]
Cadet 1989
- Cadet JL, Lohr JB. Possible involvement of free radical in neuroleptic‐induced movement disorders. Annals of the New York Academy of Sciences 1989;570:176‐185. [DOI] [PubMed] [Google Scholar]
Casey 1994
- Casey DE. Tardive dyskinesia: pathophysiology. In: Bloom FE, Kupfer DJ editor(s). Psychopharmacology. The Fourth Generation of Progress. New York: Raven Press, 1994. [Google Scholar]
Cavallaro 1993
- Cavallaro R, Regazzetti MG, Mundo E, Brancato V, Smeraldi E. Tardive Dyskinesia Outcomes: Clinical and Pharmacologic Correlates of Remission and persistence. Neuropsychopharmacology 1993;8(3):233‐9. [DOI] [PubMed] [Google Scholar]
Chong 2009
- Chong SA, Tay JA, Subramaniam M, Pek E, Machin D. Mortality rates among patients with schizophrenia and tardive dyskinesia. Journal of Clinical Psychopharmacology 2009;29:5‐8. [DOI] [PubMed] [Google Scholar]
Chouinard 2008
- Chouinard G, Chouinard VA. Atypical antipsychotics: CATIE study, drug‐induced movement disorder and resulting iatrogenic psychiatric‐like symptoms, supersensitivity rebound psychosis and withdrawal discontinuation syndromes. Psychotherapy and Psychosomatics 2008;77(2):69‐77. [DOI] [PubMed] [Google Scholar]
Cloud 2014
- Cloud LJ, Zutshi D, Factor SA. Tardive Dyskinesia: Therapeutic Options for an Increasingly Common Disorder. Neurotherapeutics 2014;11:166‐176. [DOI] [PMC free article] [PubMed] [Google Scholar]
Correll 2004
- Correll CU, Leucht S, Kane JM. Lower risk for tardive dyskinesia associated with second‐generation antipsychotics: a systematic review of 1‐year studies. American Journal of Psychiatry 2004;161(3):414‐25. [DOI] [PubMed] [Google Scholar]
Correll 2008
- Correll CU, Schenka EM. Tardive dyskinesia and new antipsychotics. Current Opinion in Psychiatry 2008;21:151‐6. [DOI] [PubMed] [Google Scholar]
Deeks 2000
- Deeks J. Issues in the selection for meta‐analyses of binary data. Proceedings of the 8th International Cochrane Colloquium; 2000 Oct 25‐28; Cape Town. Cape Town: The Cochrane Collaboration, 2000.
Divine 1992
- Divine GW, Brown JT, Frazier LM. The unit of analysis error in studies about physicians' patient care behavior. Journal of General Internal Medicine 1992;7(6):623‐9. [DOI] [PubMed] [Google Scholar]
Donner 2002
- Donner A, Klar N. Issues in the meta‐analysis of cluster randomized trials. Statistics in Medicine 2002;21(19):2971‐80. [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315:629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne D, Altman DG, Higgins JPT, Curtina F, Worthingtond HV, Vaile A. Meta‐analyses involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [DOI] [PubMed] [Google Scholar]
Essali 2011
- Essali A, Deirawan H, Soares‐Weiser K, Adams CE. Calcium channel blockers for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2011, Issue 11. [DOI: 10.1002/14651858.CD000206.pub3] [DOI] [PubMed] [Google Scholar]
Fernandez 2001
- Fernandez HH, Krupp B, Friedman JH. The course of tardive dyskinesia and parkinsonism in psychiatric inpatients: 14‐year follow‐up. Neurology 2001;56:805‐7. [DOI] [PubMed] [Google Scholar]
Fleiss 1984
- Fleiss JL. The crossover study. The Design and Analysis of Clinical Experiments. Chichester: John Wiley & Sons, 1984. [Google Scholar]
Friedhoff 1977
- Friedhoff AJ. Receptor sensitivity modification (RSM): a new paradigm for the potential treatment of some hormonal and transmitter disturbances. Comprehensive Psychiatry 1977;18(4):309‐17. [DOI] [PubMed] [Google Scholar]
Furukawa 2006
- Furukawa TA, Barbui C, Cipriani A, Brambilla P, Watanabe N. Imputing missing standard deviations in meta‐analyses can provide accurate results. Journal of Clinical Epidemiology 2006;59(7):7‐10. [DOI] [PubMed] [Google Scholar]
Glazer 1990
- Glazer WM, Morgenstern H, Schooler N, Berkman CS, Moore DC. Predictors of improvement in tardive dyskinesia following discontinuation of neuroleptic medication. British Journal of Psychiatry 1990;157(4):585‐92. [DOI] [PubMed] [Google Scholar]
Glazer 2000
- Glazer WM. Review of incidence studies of tardive dyskinesia associated with typical antipsychotics. Journal of Clinical Psychiatry 2000;61(suppl 4):15‐20. [PubMed] [Google Scholar]
Gulliford 1999
- Gulliford MC. Components of variance and intraclass correlations for the design of community‐based surveys and intervention studies: data from the Health Survey for England 1994. American Journal of Epidemiology 1999;149:876‐83. [DOI] [PubMed] [Google Scholar]
Guy 1970
- Guy W, Bonato RR, eds. Clinical Global Impressions. Manual for the ECDEU Assessment Battery 2. Rev ed. National Institute of Mental Health, 1970. [Google Scholar]
Guy 1976
- Guy W. ECDEU Assessment Manual for Psychopharmacology. Revised Edition. Washington, DC: Department of Health, Education and Welfare, 1976. [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org..
Jadad 1996
- Jadad A, Moore A, Carroll D, Jenkinson C, Reynolds DJM, Gavanagh DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17(1):1‐12. [DOI] [PubMed] [Google Scholar]
Jeste 1988
- Jeste DV, Lohr JB, Clark K, Wyatt RJ. Pharmacological treatments of tardive dyskinesia in the 1980s. Journal of Clinical Psychopharmacology 1988;8(4):49S. [PubMed] [Google Scholar]
Jeste 2000
- Jeste DV. Tardive dyskinesia in older patients. Journal of Clinical Psychiatry 2000;61(suppl 4):27‐32. [PubMed] [Google Scholar]
Jűni 2001
- Jűni P, Altman DG, Egger M. Systematic reviews in health care: assessing the quality of controlled clinical trials. BMJ (Clinical research ed.) 2001;323(7303):42‐6. [PUBMED: 11440947] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kane 1982
- Kane JM, Smith JM. Tardive dyskinesia: prevalence and risk factors, 1959 to 1979. Archives of General Psychiatry 1982;39(4):473‐81. [DOI] [PubMed] [Google Scholar]
Kay 1986
- Kay SR, Opler LA, Fiszbein A. Positive and Negative Syndrome Scale (PANSS) Manual. North Tonawanda, NY: Multi‐Health Systems, 1986. [Google Scholar]
Leon 2006
- Leon AC, Mallinckrodt CH, Chuang‐Stein C, Archibald DG, Archer GE, Chartier K. Attrition in randomized controlled clinical trials: methodological issues in psychopharmacology. Biological Psychiatry 2006;59(11):1001‐5. [PUBMED: 16905632] [DOI] [PubMed] [Google Scholar]
Leucht 2005a
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel RR. What does the PANSS mean?. Schizophrenia Research 2005;79(2‐3):231‐8. [PUBMED: 15982856] [DOI] [PubMed] [Google Scholar]
Leucht 2005b
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. Clinical implications of brief psychiatric rating scale scores. British Journal of Psychiatry 2005;187:366‐71. [PUBMED: 16199797] [DOI] [PubMed] [Google Scholar]
Lieberman 1996
- Lieberman JA, Fleishhacker W. Introduction. British Journal of Psychiatry 1996;168(Supplement 29):7‐8. [Google Scholar]
Maher 2012
- Maher AR, Theodore G. Summary of the comparative effectiveness review on off‐label use of atypical antipsychotics. Journal of Managed Care Pharmacy 2012;18(5 Suppl B):S1‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Marshall 2000
- Marshall M, Lockwood A, Bradley C, Adams C, Joy C, Fenton M. Unpublished rating scales: a major source of bias in randomised controlled trials of treatments for schizophrenia. British Journal of Psychiatry 2000;176:249‐52. [DOI] [PubMed] [Google Scholar]
Martins 2011
- Martins ES, Rosso A, Coutinho E, Adams C, Huf G. Prevalence of tardive dyskinesia and all‐cause mortality amongst patients in a large psychiatirc institute in Rio de Janeiro. Revista de Psiquiatria Clínica 2011;38:44. [Google Scholar]
Moher 2001
- Moher D, Schulz KF, Altman D. The CONSORT Statement: Revised Recommendations for Improving the Quality of Reports of Parallel‐Group Randomised Trials. Journal of the American Medical Association 2001;285(15):1987‐91. [DOI] [PubMed] [Google Scholar]
NICE 2014
- NICE. Psychosis and schizophrenia in adults: treatment and management. NICE clinical guideline 178 (guidance.nice.org.uk/cg178) 2014.
Overall 1962
- Overall JE, Gorham DR. The brief psychiatric rating scale. Psychological Reports 1962;10:799‐812. [Google Scholar]
Pocock 1983
- Pocock SJ. Crossover trials. Clinical trials. A practical approach. Chichester: John Wiley & Sons, 1983. [Google Scholar]
Sachdev 2000
- Sachdev P. The Current Status of Tardive Dyskinesia. Australian and New Zealand Journal of Psychiatry 2000;34(3):335‐69. [DOI] [PubMed] [Google Scholar]
Schooler 1993
- Schooler NR, Keith SJ. Clinical research for the treatment of schizophrenia. Psychopharmacology Bulletin 1993;29:431‐46. [PubMed] [Google Scholar]
Schulz 1995
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias: dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273(5):408‐12. [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Smith 1980
- Smith JM, Balessarini RJ. Changes in prevalence, severity and recovery in tardive dyskinesia with age. Archives of General Psychiatry 1980;37:1368‐73. [DOI] [PubMed] [Google Scholar]
Soares‐Weiser 1997
- Soares‐Weiser K, Mobsy C, Holliday E. Anticholinergic medication for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 1997, Issue 2. [DOI: 10.1002/14651858.CD000204] [DOI] [PubMed] [Google Scholar]
Soares‐Weiser 2003
- Soares‐Weiser K, Joy C. Miscellaneous treatments for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2003, Issue 2. [DOI: 10.1002/14651858.CD000208] [DOI] [PubMed] [Google Scholar]
Soares‐Weiser 2006
- Soares‐Weiser K, Rathbone J. Neuroleptic reduction and/or cessation and neuroleptics as specific treatments for tardive dyskinesia. Cochrane Database of Systematic Reviews 2006, Issue 1. [DOI: 10.1002/14651858.CD000459.pub2] [DOI] [PubMed] [Google Scholar]
Soares‐Weiser 2011
- Soares‐Weiser K, Maayan N, McGrath J. Vitamin E for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2011, Issue 2. [DOI: 10.1002/14651858.CD000209.pub2] [DOI] [PubMed] [Google Scholar]
Tammenmaa 2002
- Tammenmaa I, McGrath J, Sailas E, Soares‐Weiser K. Cholinergic medication for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2002, Issue 3. [DOI: 10.1002/14651858.CD000207] [DOI] [PubMed] [Google Scholar]
Tarsy 2011
- Tarsy D, Lungu C, Baldessarini RJ. Epidemiology of tardive dyskinesia before and during the era of modern antipsychotic drugs. Handbook of Clinical Neurology / Edited by P.J. Vinken and G.W. Bruyn 2011;100:601‐16. [DOI] [PubMed] [Google Scholar]
Taylor 2009
- Taylor D, Paton C, Kapur S. The Maudsley Prescribing Guidelines (10th Edition). London: Informa Healthcare, 2009. [Google Scholar]
Tetreault 1969
- Tetreault L, Bordeleau JM, Albert JM, Rajotte P. Comparative study of fluphenazine ethanate, fluphenazine bichlorhydrate and placebos in chronic schizophrenics [Etude comparative de l'enanthate de fluphenazine, du bichlorhydrate de fluphenazine et du placebo chez le schizophrene chronique]. Canadian Psychiatric Association Journal 1969;14(2):191‐8. [DOI] [PubMed] [Google Scholar]
Turjanski 2005
- Turjanski N, Lloyd GG. Psychiatric side‐effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11(1):58‐70. [Google Scholar]
Ukoumunne 1999
- Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ. Methods for evaluating area‐wide and organistation‐based intervention in health and health care: a systematic review. Health Technology Assessment 1999;3(5):1‐75. [PubMed] [Google Scholar]
Xia 2009
- Xia J, Adams CE, Bhagat N, Bhagat V, Bhoopathi P, El‐Sayeh H, et al. Loss to outcomes stakeholder survey: the LOSS study. Psychiatric Bulletin 2009;33(7):254‐7. [Google Scholar]
References to other published versions of this review
El‐Sayeh 2006
- El‐Sayeh HG, Lyra da Silva JP, Rathbone J, Soares‐Weiser K. Non‐neuroleptic catecholaminergic drugs for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2006, Issue 1. [DOI: 10.1002/14651858.CD000458.pub2] [DOI] [PubMed] [Google Scholar]