

Abstract
Background
Mechanical ventilation is important in caring for patients with critical illness. Clinical complications, increased mortality, and high costs of health care are associated with prolonged ventilatory support or premature discontinuation of mechanical ventilation. Weaning refers to the process of gradually or abruptly withdrawing mechanical ventilation. The weaning process begins after partial or complete resolution of the underlying pathophysiology precipitating respiratory failure and ends with weaning success (successful extubation in intubated patients or permanent withdrawal of ventilatory support in tracheostomized patients).
Objectives
To evaluate the effectiveness and safety of two strategies, a T‐tube and pressure support ventilation, for weaning adult patients with respiratory failure that required invasive mechanical ventilation for at least 24 hours, measuring weaning success and other clinically important outcomes.
Search methods
We searched the following electronic databases: Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2012, Issue 6); MEDLINE (via PubMed) (1966 to June 2012); EMBASE (January 1980 to June 2012); LILACS (1986 to June 2012); CINAHL (1982 to June 2012); SciELO (from 1997 to August 2012); thesis repository of CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) (http://capesdw.capes.gov.br/capesdw/) (August 2012); and Current Controlled Trials (August 2012).
We reran the search in December 2013. We will deal with any studies of interest when we update the review.
Selection criteria
We included randomized controlled trials (RCTs) that compared a T‐tube with pressure support (PS) for the conduct of spontaneous breathing trials and as methods of gradual weaning of adult patients with respiratory failure of various aetiologies who received invasive mechanical ventilation for at least 24 hours.
Data collection and analysis
Two authors extracted data and assessed the methodological quality of the included studies. Meta‐analyses using the random‐effects model were conducted for nine outcomes. Relative risk (RR) and mean difference (MD) or standardized mean difference (SMD) were used to estimate the treatment effect, with 95% confidence intervals (CI).
Main results
We included nine RCTs with 1208 patients; 622 patients were randomized to a PS spontaneous breathing trial (SBT) and 586 to a T‐tube SBT. The studies were classified into three categories of weaning: simple, difficult, and prolonged. Four studies placed patients in two categories of weaning. Pressure support ventilation (PSV) and a T‐tube were used directly as SBTs in four studies (844 patients, 69.9% of the sample). In 186 patients (15.4%) both interventions were used along with gradual weaning from mechanical ventilation; the PS was gradually decreased, twice a day, until it was minimal and periods with a T‐tube were gradually increased to two and eight hours for patients with difficult and prolonged weaning. In two studies (14.7% of patients) the PS was lowered to 2 to 4 cm H2O and 3 to 5 cm H2O based on ventilatory parameters until the minimal PS levels were reached. PS was then compared to the trial with the T‐tube (TT).
We identified 33 different reported outcomes in the included studies; we took 14 of them into consideration and performed meta‐analyses on nine. With regard to the sequence of allocation generation, allocation concealment, selective reporting and attrition bias, no study presented a high risk of bias. We found no clear evidence of a difference between PS and TT for weaning success (RR 1.07, 95% CI 0.97 to 1.17, 9 studies, low quality of evidence), intensive care unit (ICU) mortality (RR 0.81, 95% CI 0.53 to 1.23, 5 studies, low quality of evidence), reintubation (RR 0.92, 95% CI 0.66 to 1.26, 7 studies, low quality evidence), ICU and long‐term weaning unit (LWU) length of stay (MD ‐7.08 days, 95% CI ‐16.26 to 2.1, 2 studies, low quality of evidence) and pneumonia (RR 0.67, 95% CI 0.08 to 5.85, 2 studies, low quality of evidence). PS was significantly superior to the TT for successful SBTs (RR 1.09, 95% CI 1.02 to 1.17, 4 studies, moderate quality of evidence). Four studies reported on weaning duration, however we were unable to combined the study data because of differences in how the studies presented their data. One study was at high risk of other bias and four studies were at high risk for detection bias. Three studies reported that the weaning duration was shorter with PS, and in one study the duration was shorter in patients with a TT.
Authors' conclusions
To date, we have found evidence of generally low quality from studies comparing pressure support ventilation (PSV) and with a T‐tube. The effects on weaning success, ICU mortality, reintubation, ICU and LWU length of stay, and pneumonia were imprecise. However, PSV was more effective than a T‐tube for successful spontaneous breathing trials (SBTs) among patients with simple weaning. Based on the findings of single trials, three studies presented a shorter weaning duration in the group undergoing PS SBT, however a fourth study found a shorter weaning duration with a T‐tube.
Plain language summary
Weaning from mechanical ventilation using pressure support or a T‐tube for a spontaneous breathing trial
Patients with severe lung disease, such as acute respiratory failure, may require invasive mechanical ventilation through an endotracheal tube or tracheostomy until their underlying disease is either treated or stabilized. Both early suspension of or delay in withdrawing mechanical ventilation can however lead to complications that may delay the weaning of patients from mechanical ventilation and prolong their length of stay in the intensive care unit (ICU) and hospital. Previous studies and systematic reviews suggest that a weaning protocol should be implemented in order to make daily assessments of patients who may be ready for weaning from mechanical ventilation. The ability to breathe spontaneously can be assessed with a spontaneous breathing trial using a T‐tube (T‐piece) or by reducing the applied airway pressure to provide low levels of pressure support (PS) (5 to 10 cm H2O). After removal of the endotracheal tube (extubation) the patients are monitored for 48 hours. If over this period ventilatory support does not need to be reintroduced, this is taken to indicate successful weaning. For this Cochrane systematic review we searched the medical literature databases until June 2012 and included nine studies with 1208 adult patients who had been on invasive mechanical ventilation for at least 24 hours. The trials compared pressure support (PS) and the use of a T‐tube (622 patients randomized to PS and 586 randomized to a T‐tube). There was no clear evidence to confirm that PS was superior to a T‐tube with regard to the success of weaning, need for reintubation, ICU mortality, and other factors including long‐term weaning unit (LWU) length of stay, pneumonia and a rapid shallow breathing index. Among patients who received PS, a greater number of patients had a successful spontaneous breathing trial and the airway tube was removed. For respiratory rate and tidal volume outcomes PS was superior to using a T‐tube in two trials. Three studies reported that the weaning duration was shorter during PS, and in one study in which patients submitted to a T‐tube the weaning time was shorter. Because of limitations in the design of the studies and imprecision in the effect estimates we have rated the quality of the evidence to be low. We reran the search in December 2013. We will deal with any studies of interest when we update the review.
Summary of findings
Summary of findings for the main comparison. Pressure support versus T‐tube for weaning from mechanical ventilation in adults.
| Pressure support versus T‐tube for weaning from mechanical ventilation in adults | ||||||
| Patient or population: patients on weaning from mechanical ventilation in adults. Settings: ICU or LWU length of stay. Intervention: pressure support versus T‐tube. | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Pressure support versus T‐tube | |||||
| Weaning success Follow‐up: mean 24 hours | Study population | RR 1.07 (0.97 to 1.17) | 935 (9 studies) | ⊕⊕⊝⊝ low1,2 | The physicians need to take into consideration the age, baseline disease, duration of mechanical ventilation before weaning | |
| 730 per 1000 | 781 per 1000 (708 to 855) | |||||
| Low | ||||||
| 600 per 1000 | 642 per 1000 (582 to 702) | |||||
| High | ||||||
| 950 per 1000 | 1000 per 1000 (922 to 1000) | |||||
| ICU mortality | Study population | RR 0.81 (0.53 to 1.23) | 725 (5 studies) | ⊕⊕⊝⊝ low1,2,3 | The physicians need to take into consideration the age of patients, disease severity, duration of mechanical ventilation before weaning, baseline disease (COPD), cause of respiratory failure | |
| 125 per 1000 | 101 per 1000 (66 to 154) | |||||
| Low | ||||||
| 50 per 1000 | 41 per 1000 (26 to 62) | |||||
| High | ||||||
| 200 per 1000 | 162 per 1000 (106 to 246) | |||||
| Reintubation Follow‐up: mean 48 hours | Study population | RR 0.92 (0.66 to 1.26) | 823 (7 studies) | ⊕⊕⊝⊝ low3,4 | The physicians need to take into consideration the age, time of mechanical ventilation, before weaning | |
| 159 per 1000 | 146 per 1000 (105 to 200) | |||||
| Low | ||||||
| 50 per 1000 | 46 per 1000 (33 to 63) | |||||
| High | ||||||
| 200 per 1000 | 184 per 1000 (132 to 252) | |||||
| ICU or LWU length of stay (days) | The mean ICU or LWU length of stay (days) in the intervention groups was 7.08 lower (16.26 lower to 2.1 higher) | 118 (2 studies) | ⊕⊕⊝⊝ low1,2,5,6 | The physicians need to take into consideration the age, time of mechanical ventilation, weaning process (prolonged weaning) and baseline disease | ||
| Pneumonia | Study population | RR 0.67 (0.08 to 5.85) | 118 (2 studies) | ⊕⊝⊝⊝ very low3,7,8 | The physicians need to take into consideration the time of mechanical ventilation | |
| 82 per 1000 | 55 per 1000 (7 to 480) | |||||
| Low | ||||||
| 10 per 1000 | 7 per 1000 (1 to 58) | |||||
| High | ||||||
| 200 per 1000 | 134 per 1000 (16 to 1000) | |||||
| Successful spontaneous breathing trial Follow‐up: mean 2 hours | Study population | RR 1.09 (1.02 to 1.17) | 940 (4 studies) | ⊕⊕⊕⊝ moderate9 | The physicians need to take into consideration the time of mechanical ventilation, age of patients, disease severity | |
| 732 per 1000 | 798 per 1000 (747 to 857) | |||||
| Low | ||||||
| 500 per 1000 | 545 per 1000 (510 to 585) | |||||
| High | ||||||
| 800 per 1000 | 872 per 1000 (816 to 936) | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Two studies with high and moderate risk of bias in at least two items of methodological quality. 2 Confidence intervals include the unit (1), and P > 0.05. 3 Large confidence interval. 4 Funnel plot asymmetric. 5 Inconsistency test > 50%, but with the same direction of effect. 6 Reduction of seven days in the ICU stay is considered a large effect. 7 Two studies were considered high risk of bias in at least one item of methological quality. 8 Opposite effect directions, but inconsistency test < 50%. 9 One of four studies was considered high risk of bias in one item of methological quality. Two studies were considered unclear risk of bias in at least one item of methodological quality.
Background
Description of the condition
Mechanical ventilation, while providing partial or full support to patients with respiratory failure of different aetiologies (Marini 1998), exerts important effects on global oxygen delivery and reduces the full or partial work of breathing. While enabling clinicians to support patients with respiratory failure, invasive mechanical ventilation has been shown to initiate lung injury, exacerbate pre‐existing parenchymal lung injury, and induce ultrastructural abnormalities (Marini 1998) and clinical complications. Clinical complications may include ventilator associated pneumonia (VAP) (Eggimann 2001), with a prevalence of 9 to 24 cases per 100 patients depending on the population examined (Morehead 2000); respiratory muscle weakness (Le Bourdelles 1994; Levine 2008; Powers 2002); sinusitis (van Zanten 2005) (with a higher incidence in nasotracheal than in orotracheal intubation) (Michelson 1991); barotrauma (Baeza 1975; Petersen 1983); gastrointestinal bleeding (Pingleton 1988; Schuster 1984) and critical illness polyneuropathy (CIP) (Garnacho‐Montero2005). These complications have in turn been associated with failure to wean from mechanical ventilation, prolonged duration of intubation and hospital stay (Combes 2003; Rello 1991) and increased intensive care unit (ICU) mortality (Esteban 2002; Fagon 1996).
Early recognition of weaning candidates ready for reduction and discontinuation of ventilatory support is important in order to minimize exposure to prolonged invasive ventilation (Blackwood 2010; Ely 1996; Kollef 1997; Marelich 2000), specifically unnecessary sedation doses, increased infection risk, higher costs, morbidity and mortality (Esteban 2002). On the other hand, early withdrawal of mechanical ventilation can lead to post‐extubation failure as well as respiratory muscle fatigue, hypoxaemia, hypercapnia, and the risk of complications during reintubation procedures, which are associated with increased ICU stay and mortality (Epstein 1997).
Weaning refers to the process of gradually or abruptly withdrawing mechanical ventilation. The weaning process begins after partial or complete resolution of the underlying pathophysiology that precipitated respiratory failure and ends with weaning success (successful extubation in intubated patients or permanent withdrawal of ventilatory support in tracheostomized patients) (Boles 2007). The weaning duration extends to 41% of the total time of mechanical ventilation (MV); in patients with chronic obstructive pulmonary disease (COPD) and cardiac failure, the weaning duration can reach 59% and 48% of the total time of MV, respectively (Esteban 1994). Over the past decade, scientific investigations have focused on strategies to limit the duration of invasive ventilation, including daily withdrawal of sedation (Girard 2008; Luetz 2012), assessment of physiologic criteria or 'weaning parameters', spontaneous breathing trials (SBTs) (Esteban 1997) and methods to reduce support in patients who fail a SBT (Brochard 1994; Esen 1992; Esteban 1995; MacIntyre 2001). Most weaning parameters, individually or in combination, are evaluated while the patient is receiving MV. Such evaluations assess the strength of the respiratory muscles, gas exchange, and comfort and are used to identify early candidates who are 'ready to wean' (Epstein 2000; Epstein 2001), that is, those capable of maintaining spontaneous breathing (Ely 1996; Kollef 1997; Marelich 2000).
Several studies have demonstrated that while the majority of patients (69% to 75%) satisfying 'readiness criteria' will tolerate an initial SBT, only a minority of patients require a more gradual withdrawal of invasive ventilation (Caroleo 2007; Peňuelas 2011). Patients are classified into three categories according to the difficulty and length of the weaning process: simple weaning, encompassing patients who are successfully extubated on the first SBT; difficult weaning, encompassing patients who require up to three SBTs or until seven days of MV after the first attempt to achieve weaning success; and prolonged weaning, encompassing the patients who fail three SBTs or remain on invasive ventilatory support for over seven days after the first SBT (Boles 2007; Tonnelier 2011).
Description of the intervention
The ability to breathe spontaneously can be assessed by means of a SBT (Boles 2007; MacIntyre 2012). Several studies have investigate the best technique for performing a SBT; the most common modes include: synchronized intermittent mechanical ventilation (SIMV), continuous positive airway pressure (CPAP), automatic tube compensation (ATC), pressure support ventilation (PSV) and T‐tube (T‐piece). Several reviews (Alia 2000; Butler 1999; Cook 2000; Caroleo 2007; Meade 2001), reported that SIMV is the method least preferred for weaning patients from mechanical ventilation, and the use of this method has thus reduced to 1.6% (Esteban 2008). An SBT may range from 30 minutes to two hours in duration on simple and difficult weaning with similar outcomes when compared to one another in two randomized controlled trials (Esteban 1999; Perren 2002). In prolonged weaning patients, T‐tube for long periods or gradual reduction of PS levels can be used as weaning strategies (Vitacca 2001).
How the intervention might work
Low levels of pressure support (PS) and a T‐tube can simulate the ventilatory load after extubation and can thus be used to evaluate a patient's ability to maintain spontaneous ventilation without ventilatory support; that is, they can be employed to select patients who are ready for extubation (Boles 2007; Esteban 1997; MacIntyre 2012). In a T‐tube SBT, the patient is disconnected from the ventilator and allowed to breathe spontaneously through a simple T‐piece with supplemental oxygen. For some patients the work of breathing during the test may be excessive, causing them to fail the SBT. In PSV mode, the patients remain connected to ventilatory support and the PS minimum value (5 to 10 cm H2O) is adjusted to decrease the work of breathing imposed by the endotracheal tube during a SBT (Nathan 1993).
Why it is important to do this review
The current literature asserts that an SBT must be performed prior to extubation. Some studies say that there appears to be no difference between SBTs (PSV and T‐tube) on relevant clinical outcomes (Boles 2007; Caroleo 2007; Esteban 1997). According to MacIntyre 2012, controversies exist regarding the best techniques involved in an SBT. The T‐tube technique is used more frequently for SBTs in the simple weaning group in clinical practice (76%), while the use of PSV as an SBT has increased slightly (14%) (Esteban 2008).
Weaning from MV is an important area of research as the optimal strategy for trials to wean patients from invasive MV remains to be elucidated and as solid evidence to answer this question is lacking. In this systematic review we evaluated, synthesized and compared the best evidence for using a T‐tube (T‐piece) and PSV as SBTs and on the gradual withdrawal process aimed towards releasing invasively ventilated adults from mechanical support.
Objectives
We aimed to evaluate the effectiveness and safety of two strategies, a T‐tube and pressure support ventilation (PSV), for weaning adult patients with respiratory failure that required mechanical ventilation for at least 24 hours, measuring weaning success and other clinically important outcomes.
Methods
Criteria for considering studies for this review
Types of studies
We included all randomized controlled trials (RCTs) that compared a T‐piece with PSV for the conduct of SBTs to liberate patients from invasive ventilation.
Types of participants
We included adult patients (at least 18 years of age) with respiratory failure of various aetiologies who received invasive mechanical ventilation (MV) for at least 24 hours. We included postoperative adult patients (following cardiac surgery, neurosurgery etc.) requiring invasive ventilation for at least 24 hours.
Types of interventions
We included RCTs that compared T‐piece to invasive PS weaning.
We excluded trials that extubated patients directly to non‐invasive positive pressure ventilation (NPPV) for the purpose of weaning.
Types of outcome measures
Primary outcomes
Weaning success (defined as the absence of the requirement for ventilatory support within 48 hours after extubation (translaryngeal tube) or withdrawal (tracheostomy tube) of MV, or as defined by the authors)
Secondary outcomes
We included the following secondary outcomes.
Mortality (ICU mortality and hospital mortality, or as defined by the study authors).
Time of weaning from MV or weaning duration (the time from randomization to extubation).
Proportion requiring reintubation (as defined by the authors) or reintubation.
Proportion requiring tracheostomy.
Intensive care unit (ICU) and hospital length of stay (LOS) (the time from randomization to ICU and hospital discharge, respectively).
Proportion with VAP.
Total duration of MV (days or hours).
Adverse events related to weaning.
Quality of life.
Physiologic parameters, including:
a. respiratory rate (RR),
b. tidal volume (VT),
c. rapid and shallow breathing index (RSBI or RR/VT).
Outcomes defined post hoc during the review process
Successful spontaneous breathing trial (SBT)
Search methods for identification of studies
Electronic searches
We searched the current issue of the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2012, Issue 6); MEDLINE (January 1966 to June 2012); EMBASE (January 1980 to June 2012); LILACS (1986 to June 2012); CINAHL (1982 to June 2012), SciELO (from 1997 to August 2012); the thesis repository CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) (http://capesdw.capes.gov.br/capesdw/); as well as Current Controlled Trials (www.controlled‐trials.com) for RCTs meeting our inclusion criteria. Our search terms included synonyms for ventilator weaning, spontaneous breathing trial (SBT), T‐tube (or T‐piece), pressure support and respiratory failure as the clinical condition, interventions and target population of interest.
See Appendix 1 (EMBASE); Appendix 2 (CINAHL); Appendix 3 (CENTRAL); Appendix 4 (MEDLINE); Appendix 5 (LILACS); Appendix 6 (SciELO); Appendix 7 (CAPES) and Appendix 8 (Current Controlled Trials) for details of the search strategies used for each database. We utilized the Cochrane highly sensitive RCT filter for MEDLINE from the Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 (Higgins 2011). We did not apply any language restrictions.
We reran the search in December 2013. We will deal with any studies of interest when we update the review.
Searching other resources
We handsearched the bibliographies of all retrieved articles and review articles to identify potentially relevant trials.
Data collection and analysis
We followed the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Three review authors (ML, FV, and BG) are physiotherapists and clinical experts in the support of adult patients admitted to the ICU. All review authors are experts in Cochrane systematic reviews.
Selection of studies
Two authors (ML and BG) independently screened citations identified by the initial search for RCTs against the predefined inclusion criteria. Two authors (FV and RA) retrieved and reviewed the full text articles to reaffirm that the inclusion criteria were met. Disagreements were resolved through discussion with a third author (SP). Only studies containing at least two arms of interest (PS and T‐tube) were considered for inclusion in the review.
Data extraction and management
Two authors (ML and RA) independently extracted the data pertaining to participant characteristics, details of the interventions applied, and outcomes for all studies meeting the inclusion criteria. We used a data extraction form developed for this systematic review. For relevant data that were missing or not clearly reported, we contacted the first authors for the required information (see data extraction form: Appendix 9).
Assessment of risk of bias in included studies
Two authors (ML and BS) assessed each included trial for study design characteristics and features of internal validity. Two authors (ML and RA) independently assessed the methodologic quality of the included studies using the following criteria (see Risk of bias in included studies).
Was the allocation sequence adequately generated?
Yes (low risk of bias): adequate sequence generation
Unclear (moderate risk of bias): not reported in the paper or determined by contacting authors
No (high risk of bias): not adequate (quasi‐randomized studies)
Was allocation adequately concealed?
Yes (low risk of bias): adequate allocation concealment
Unclear (moderate risk of bias): not reported in the paper or by determined by contacting authors
No (high risk of bias): not adequate
Free of detection bias ?
Yes (low risk of bias): outcome assessors were independent from the individuals administering or supervising the assigned treatments
Unclear (moderate risk of bias): not reported in the paper or determined by contacting authors
No (high risk of bias): outcome assessors aware about the assigned treatments
Free of attrition bias?
Yes (low risk of bias): dropouts without substantial (statistically significant) difference between the two comparison groups or a substantial dropout rate within the sample as a whole
Unclear (moderate risk of bias): not reported in the paper or determined by contacting authors
No (high risk of bias): dropouts with substantial (statistically significant) difference between the two treatment groups or a substantial dropout rate within the sample as a whole
Free of selective reporting?
Yes (low risk of bias): reports of the study free of suggestion of selective outcome reporting
Unclear (moderate risk of bias): not reported in the paper or by contacting authors
No (high risk of bias): reports of the study with suggestion of selective outcome reporting
Free of other bias?
Yes (low risk of bias): the study appears to be free of other sources of bias
Unclear (moderate risk of bias): there may be a risk of bias
No (high risk of bias): there is at least one important risk of bias
Measures of treatment effect
Dichotomous data
We summarized the dichotomous data using relative risk (RR) as a summary estimate of treatment effect, with 95% confidence interval (CI). Where feasible, we calculated and reported the number needed to treat (NNT).
Continuous data
We summarized the continuous outcomes using the mean difference (MD). For data reported using different scales, which could not be converted to a uniform scale, we planned to use the standardized mean difference (SMD).
Unit of analysis issues
The unit of analysis was based on the individual patient. We considered cross‐over RCTs only if the data from the first phase were available (Higgins 2011).
Dealing with missing data
For continuous and dichotomous data we carried out available case analysis.
Assessment of heterogeneity
Clinical heterogeneity
We used the term 'clinical heterogeneity' to describe clinical differences in the studies related to the participants studied, interventions applied, and outcomes reported. We based the decision to pool studies on the absence of important clinical heterogeneity. We judged clinical heterogeneity based on patient demographics, clinical circumstances, and the comparability of the interventions applied.
Statistical heterogeneity
We performed an evaluation of the heterogeneity of the data using Cochran's Q statistic, a Chi2 test, with a threshold P value of less than 0.10 (Fleiss 1986). The consistency of the results was assessed visually using forest plots and by the I2 statistic (Higgins 2002). The I2 statistic describes the proportion of variation in point estimates that is attributable to heterogeneity as opposed to sampling error.
Assessment of reporting biases
We planned to construct a funnel plot (trial effect versus standard error) to assess possible reporting bias if sufficient (at least five) studies were identified (Egger 1997).
Data synthesis
Qualitative information
Qualitative information relating to methods, risk of bias, description of participants, and outcome measurements was synthesized in the Characteristics of included studies and Table 2.
1. Results: characteristics of included studies.
| Results: characteristics of included studies | ||||||||||||||||||||
| Studies | Patients number | Characteristics of patients | Interventions | Risk of methodological bias | Study design | |||||||||||||||
| Total | PSV | TT | Age | Male | Fem | Score Health | MV days | % COPD | Prosthesis | Weaning Process | PSV min | SBTs time | AG? | AC? | RS? | OB? | DB? | AB? | ||
| Brochard 1994 | 109 | 31 | 35 | 58 | 74 | 35 | SAPs II 12 | 14 | 27% | TOT/TQT | DW/PW | 8 | TT2h/ PS24h |
Low | Low | Low | High | High | Low | M RCT |
| Esteban 1995 | 130 | 37 | 31 | 58 | not reported | APACHE 18,6 | 9,3 | 40 | TOT | DW | 5 | 2h | Low | Low | Low | Low | Low | Low | M RCT | |
| Esteban 1997 | 484 | 238 | 246 | 0 | 343 | 141 | SAPs II 36 | 6 (4‐12) | 20 | TOT | SW/DW | 7 | 2h | Low | Low | Low | Low | Low | Low | M RCT |
| Haberthür2002 | 90 | 30 | 30 | 57 | 58 | 32 | APACHE 20 | 6 | 10 | TOT | SW/DW | 5 | 2h | Low | Low | Low | Mod | Low | Low | CO RCT |
| Koh 2000 | 36 | 20 | 22 | 61 | 23 | 13 | APACHE 35 | 12 | 0 | TOT | SW/DW | 7.6 | TT1h/ PS30 |
Low | Low | Low | Mod | High | Low | RCT |
| Koksal 2004 | 60 | 20 | 20 | 74 | 28 | 32 | APACHE 18,5 | not rep | not rep | TOT | SW | 10 | 2h | Low | Mod | Low | Low | Low | Low | RCT |
| Matić 2004 | 260 | 150 | 110 | 0 | 170 | 90 | APACHE 19‐28 | 6,75 | 13 | TOT | DW | 8 | 2h | Mod | Low | Low | Low | Mod | Low | RCT |
| Matić 2007 | 136 | 70 | 66 | 0 | 36 | 27 | APACHE 23‐34 | 3.6‐6.3 | 100% | TOT | DW | 5 | 2h | Low | Low | Low | Low | High | Low | RCT |
| Vitacca 2001 | 52 | 26 | 26 | 72.5 | not reported | APACHE 17 | 15‐39 | 100% | TQT | PW | 8 | 8h | Low | Low | Low | Low | High | Low | M RCT | |
| Total | 1357 | 622 | 586 | 732 | 370 | |||||||||||||||
Quantitative information
For dichotomous variables, we calculated the risk ratio (RR) and pooled the estimated effects from the studies by using the Mantel‐Haenszel statistical method. For continuous variables, we calculated the MD by using the inverse variance statistical method when studies reported their results through the same variables measured with the same instruments (same measurement units). When continuous data were reported with non‐interchangeable measurement units, we planned to pool them through the SMD. We calculated their respective 95% confidence intervals (CI).
For continuous and dichotomous data, we used a random‐effects statistical model since we were expecting substantial clinical and methodological heterogeneity, which could generate substantial statistical heterogeneity.
Subgroup analysis and investigation of heterogeneity
We planned to perform subgroup analyses to assess the impact of the:
aetiology for MV (medical versus surgical studies);
duration of MV prior to randomization (less than versus more than seven days);
duration of SBTs before extubation (target durations of 30 and 120 minutes) on weaning time.
Subgroup analysis post hoc during the review process
Weaning process divided into three categories: simple, difficult and prolonged weaning
Endotracheal prosthesis (tracheostomy versus translaryngeal tube)
Conduct of the proposed subgroup analyses, defined a priori, were 'hypothesis generating'. We anticipate that all subgroup analyses will be underpowered and consequently we will view these as exploratory given their propensity to generate misleading conclusions (Oxman 1992; Yusuf 1991).
Sensitivity analysis
We planned to conduct a sensitivity analysis to access the impact of excluding studies with a high risk of bias on pooled estimates of weaning time, mortality, and the proportion requiring reintubation.
Results
Description of studies
Results of the search
See Figure 1.
1.
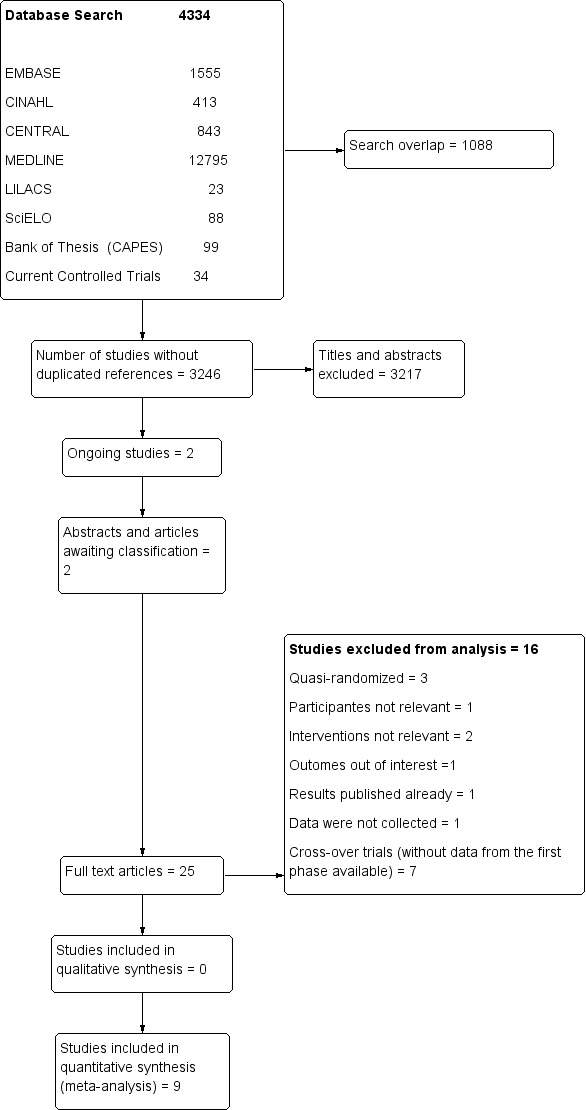
Study flow diagram. Search reran in December 2013.
We reran the search in December 2013. The search strategies retrieved 4334 titles and abstracts from the various electronic databases, the thesis repository and handsearches (Figure 1). We excluded 3217 references and 28 studies were retrieved as possibly meeting the inclusion criteria; one of them (Zhang 2009) is awaiting classification since the abstract was published in English and the full paper was written in Chinese, and two ongoing studies (Agarwal 2008; Pellegrini 2011) are registered in Current Controlled Trials. We found one study (Jubran 2013) of interest in the search that was rerun in December 2013. We will deal with this study when we update the review. We evaluated 25 full papers that were potentially eligible for the review and included nine studies. We excluded 16 studies from the analysis (see Excluded studies). The studies that were included represented international experience in conducting SBTs. The various countries included Argentina, Brazil, Croatia, France, Italy, Korea, Spain, Switzerland, Turkey and Venezuela. All the included studies were published in the English language.
Included studies
See Characteristics of included studies and Table 2 for the summary of the characteristics of the included studies.
Among the studies included, four were multicentre (Brochard 1994; Esteban 1995; Esteban 1997; Vitacca 2001), four RCTs were conducted at only one centre (Koh 2000; Koksal 2004; Matić 2004; Matić 2007), and one study was a cross‐over trial (Haberthur 2002).
The studies enrolled 1357 patients with acute respiratory failure of various aetiologies that required mechanical ventilation for more than 24 hours, and 1208 were included in this review. The number of participants in each study ranged from 36 (Koh 2000) to 484 (Esteban 1997). The mean participant age ranged from 58 to 74 years in six trials. Three studies reported these data as the median and interquartile range (IQR): Esteban 1997, 64 years (50 to 72); Matić 2004, 51 years (2 to 64.2); Matić 2007, 57 years (32 to 71) years. The gender distribution was 732 males and 370 females in seven studies, while two studies (Esteban 1995; Vitacca 2001) did not report the sex of the patients. In seven studies (Esteban 1995; Esteban 1997; Haberthur 2002; Koh 2000; Koksal 2004; Matić 2004; Matić 2007) the participants were intubated by means of a translaryngeal tube, Brochard 1994 had intubated and tracheostomized patients and, in one study (Vitacca 2001), all the patients (N = 52) were tracheostomized.
The disease severity was evaluated by the Acute Physiology and Chronic Health Evaluation score (APACHE II) (Knaus 1985) in seven studies, and the Simplified Acute Physiology score (SAPs II) (Le Gall 1993) was used for two studies (Brochard 1994; Esteban 1997).
In two studies (Matić 2007; Vitacca 2001) all the participants presented with chronic obstructive pulmonary disease (COPD), whereas in one study (Koksal 2004) the patients' underlying diagnoses were not reported. In six studies the proportion of patients with COPD ranged from 0% (Koh 2000) to 40% (Esteban 1995).
The mean duration of MV before weaning ranged from 6.3 (Haberthur 2002) to 14 days (Brochard 1994) in four trials. The median duration of MV before the trials in three studies (Esteban 1997; Matić 2004; Matić 2007) was 6.0, 6.75 and 5.0 days, respectively. The duration of MV before transfer to a long‐term weaning unit ranged from 15 to 39 days in one study (Vitacca 2001). Koksal 2004 did not report the duration of mechanical ventilation before SBT.
All studies started the process of withdrawal of ventilatory support after partial or complete improvement of the cause that led to acute respiratory failure, based on clinical and laboratory criteria. In seven studies (Brochard 1994; Esteban 1995; Esteban 1997; Haberthur 2002; Matić 2004; Matić 2007; Vitacca 2001) the patients were submitted to a T‐tube trial for two to five minutes, when respiratory parameters (respiratory rate (RR), tidal volume (VT), maximal inspiratory pressure (MIP) and rapid shallow breathing index (RSBI)) were measured. Two studies (Koh 2000; Koksal 2004) did not report the initial T‐tube trial. The criteria for discontinuation of SBT (see Table 3), weaning success and reintubation outcomes were previously defined and they were similar for all authors.
2. Intolerance criteria to spontaneous breathing trial.
| Signs to poor tolerance to spontaneous breathing trial | |||||
| Studies |
Respiratory rate (bpm) |
SaO2 |
Heart rate (beats/min) |
Systolic blood pressure (mm Hg) |
Others |
| Brochard 1994 | > 35 | PaO2 < 50 | ≤ 20% basal | > 20% basal | Agitation, diaphoresis, depressed mental status |
| Esteban 1995 | > 35 | < 90% | > 140 | > 180 | Agitation, anxiety or diaphoresis |
| Esteban 1997 | > 35 | < 90% | > 140 | > 200 | Agitation, anxiety or diaphoresis |
| Haberthur 2002 | > 35 | < 90% | > 140 | > 180 | Agitation, anxiety or diaphoresis |
| Koh 2000 | > 40 | PaO2 < 55 | ≤ 20% basal | > 20% basal | Agitation, diaphoresis, depressed mental status |
| Koksal 2004 | ≥ 35 | ≤ 90% | ≥ 140 | ≤ 90 or ≥ 180 | Agitation, diaphoresis, depressed mental status |
| Matić 2004 | > 35 | < 90% | > 140 | > 200 | Stable clinical condition |
| Matić 2007 | > 25 | < 90% | > 140 | > 200 | Restlessness |
| Vitacca 2001 | > 35 | PaO2 < 50 | > 145 | > 180 | Agitation, anxiety or diaphoresis |
The patients of the included studies were classified into three categories (simple, difficult, and prolonged weaning) according to the difficulty and length of the weaning process, as presented by Laurent Brochard at the Fifth International Concensus Conference in Intensive Care Medicine (Boles 2007). Four authors evaluated PS versus T‐tube in patients who were successfully extubated on the first SBT, simple weaning (Esteban 1997; Haberthur 2002; Koh 2000; Koksal 2004). Seven studies (Brochard 1994; Esteban 1995; Esteban 1997; Haberthur 2002; Koh 2000; Matić 2004; Matić 2007) were classified as presenting cases of patients who required up to three SBTs, or until seven days of MV after the first attempt to achieve weaning success, that is, difficult weaning. In two studies (Brochard 1994; Vitacca 2001) the patients were considered as prolonged weaning category, that is, the patients failed three spontaneous breathing trials or remained on invasive ventilatory support for more than seven days after the first SBT; in the study by Vitacca 2001 the participants were tracheostomized patients who were transferred to a weaning unit. Only the study of Esteban 1997 compared and showed the data of relevant clinical outcomes for two categories of weaning: patients with simple and difficult weaning processes.
With regard to the interventions, five studies (Esteban 1997; Koh 2000; Matić 2004; Matić 2007; Vitacca 2001) compared two interventions (PSV versus T‐tube) for conducting SBTs. Three studies (Brochard 1994; Haberthur 2002; Koksal 2004) compared three interventions, synchronized intermittent mechanical ventilation (SIMV), automatic tube compensation (ATC) and continuous positive airway pressure (CPAP), with PSV and the T‐tube. One study (Esteban 1995) compared four interventions (intermittent mandatory ventilation (IMV) and intermittent SBTs were compared with PSV and a once daily trial with a T‐tube). We took into consideration only the interventions that this review was focusing on.
In the included studies, 622 patients underwent a PSV trial and 586 patients underwent a T‐tube trial. The PS values during the SBT ranged from five (Esteban 1995; Haberthur 2002; Matić 2007) to 10 cm H2O (Koksal 2004). The PSV and T‐tube were utilized for the SBT in 844 (69.9%) patients for four studies; in three studies (Brochard 1994; Esteban 1995; Vitacca 2001) in approximately 186 (15.4%) patients the PS value was gradually reduced until reaching minimal PS (PSmin) for SBT and periods of using a T‐tube increased twice a day until the full duration time of the SBTs. In two studies in 178 (14.7%) patients the PS was lowered to 2 to 4 cm H2O (Matić 2007) and 3 to 5 cm H2O (Koh 2000), based on ventilatory parameters, until reaching the PSmin for SBT. Koh 2000 established the PSmin using the formula: PSmin = peak inspiratory flow rate (PIFR) x total ventilatory system resistance. The duration of the SBTs (PSV and T‐tube) were the same in seven studies, two hours for six studies (Esteban 1995; Esteban 1997; Haberthur 2002; Koksal 2004; Matić 2004; Matić 2007) and eight hours in one study (Vitacca 2001). Two studies compared different durations of SBTs: Brochard 1994 compared a 24 hours PSV SBT versus two hours of a T‐tube trial; and in the trial by Koh 2000 the patients underwent an additional one‐hour T‐tube trial versus 30 min of a PSV SBT.
Six studies only evaluated clinical outcomes, while three (Haberthur 2002; Koh 2000; Koksal 2004) evaluated clinical and surrogate outcomes (physiological parameters, work of breathing (WOB) and endocrine response). However, 33 different outcomes were evaluated for all included studies, see Appendix 10. Weaning success or successful extubation was defined as the absence of support ventilation , when no mechanical ventilatory support was required 48 hours after extubation, or the withdrawal of mechanical ventilation in all included studies.
Five studies (Brochard 1994; Haberthur 2002; Koh 2000; Koksal 2004; Vitacca 2001) reported the findings as mean ± SD for continuous parameters and four studies (Esteban 1995; Esteban 1997; Matić 2004; Matić 2007) expressed their data using the median and IQR. See Appendix 11; Appendix 12; Appendix 13; Appendix 14.
Excluded studies
See Characteristics of excluded studies.
We excluded 16 studies from this review. Three studies (Colombo 2007; Emmerich 1997; Niembro 1996) compared PS and T‐tube as SBT trials, but the randomization strategy was not adequate (quasi‐randomized). Eight studies (Cabello 2010; Costa 2005; Guntzel 2007; Kuhlen 2003; Patel 1996; Rieder 2004; Santos 2008; Schifelbain 2011; Sassoon 1991) were cross‐over clinical trials that evaluated surrogate outcomes (WOB, pressure time product (PTP), energy expenditure (EE), physiological variables and others) and the results of the first moment (before cross‐over) were not available. Figueiredo 2001 conducted an RCT comparing PS and T‐tube but the examined patient populations were outside the scope of this review. The results from one excluded study (Goldwasser 1998) were considered in the results reported by another included trial (Esteban 1997). In two studies the patients were allocated to T‐tube for either 30 or 120 minutes (Esteban 1999) and PSV for 30 or 120 minutes (Perren 2002).
Risk of bias in included studies
A synthesis of the assessment of the methodological quality items described below is presented in Figure 2 and Figure 3. See Risk of bias in included studies and Table 2.
2.
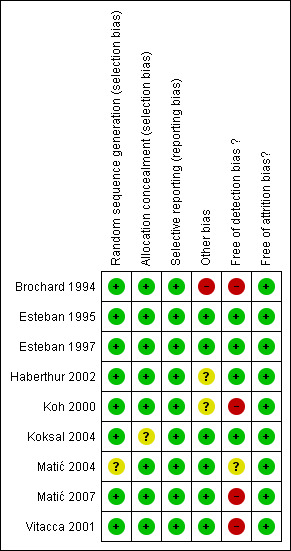
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
3.
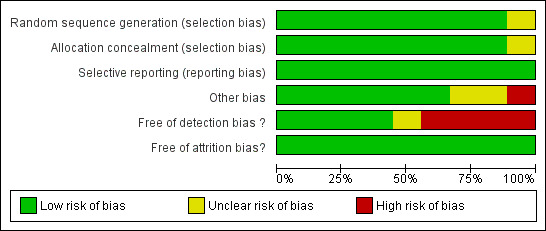
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Randomization
The generation of the allocation sequence was adequate (low risk of bias) in eight studies. Brochard 1994 reported that the randomization was stratified according to centre and the aetiology of the process responsible for difficult weaning. It was performed by means of a random number table in the studies by Esteban 1995; Esteban 1997 and Koh 2000. Two authors (Haberthur 2002; Vitacca 2001) reported, by e‐mail contact, that the patients were allocated to each one of the interventions based on a computer‐generated random list. The randomization was achieved by pulling slips of paper labelled I, II and III from a bag (20 pieces per group) in the study of Koksal 2004. One study (Matić 2007) reported that the patients were randomly assigned by means of a draw of envelopes.
The risk of bias in one trial (Matić 2004) was considered to be moderate because the authors did not describe the randomization method in the published study, nor by contact with the author.
Allocation concealment
The allocation concealment was reported to have been done by means of sealed envelopes in eight trials (Brochard 1994; Esteban 1995; Esteban 1997; Haberthur 2002; Koh 2000; Matić 2004; Matić 2007; Vitacca 2001). One author (Koksal 2004) did not report sufficient details regarding the allocation concealment. This study was considered to be at moderate risk of bias.
Blinding
Detection bias
The risk of detection bias was low in four studies (Esteban 1995; Esteban 1997; Haberthur 2002; Koksal 2004) and their authors stated by e‐mail that the outcome assessors were blinded to the interventions. Matić 2004 was considered to present a moderate risk of bias since the author did not report whether the outcomes assessor was different from the study researchers.
Three authors (Brochard 1994; Koh 2000; Vitacca 2001) reported that their studies did not have any blinding after randomization. These three studies were considered to present a high risk of detection bias. Matić 2007 stated that his study was single‐blinded, with a protocol published in Current Controlled Trials.
Incomplete outcome data
In all studies (Brochard 1994; Esteban 1995; Esteban 1997; Haberthur 2002; Koh 2000; Koksal 2004; Matić 2004; Matić 2007; Vitacca 2001) the risk of attrition bias was considered to be low. They reported a clear patient flow or intention to treat (ITT). One study (Koh 2000) explicitly reported eight withdrawals (18%), and it described the reasons for these withdrawals.
Selective reporting
All the studies were considered to have a low risk of bias based on the relevant outcomes considered to evaluate the effectiveness and safety of SBTs, with an absence of suspected selective outcome reporting (Brochard 1994; Esteban 1995; Esteban 1997; Haberthur 2002; Koh 2000; Koksal 2004; Matić 2004; Matić 2007; Vitacca 2001).
Other potential sources of bias
Brochard 1994 reported that the criteria for extubation were different in the three groups (high risk of bias). Koh 2000 described results from 42 weaning trials on 36 patients (cross‐over occurred in six patients) who were randomly assigned to an additional one‐hour period in the T‐tube trial group and immediate extubation in the PSmin group. The study design of Haberthur 2002 was a cross‐over trial. These studies were considered to present moderate risk of methodological bias.
In six studies (Esteban 1995; Esteban 1997; Koksal 2004; Matić 2004; Matić 2007; Vitacca 2001) we did not suspect any other potential sources of bias.
Effects of interventions
See: Table 1
Weaning success
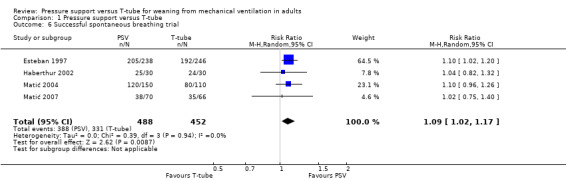
In nine studies (Brochard 1994; Esteban 1995; Esteban 1997; Haberthur 2002; Koh 2000; Koksal 2004; Matić 2004; Matić 2007; Vitacca 2001), involving 935 patients, we found that a larger but not statistically significant proportion of patients assigned to PS (357/464) were successfully extubated or withdrawn from invasive MV, or both, compared with patients assigned to T‐tube SBT (344/471) (RR 1.07, 95% CI 0.97 to 1.17, P = 0.16) in the presence of non‐significant heterogeneity (P = 0.27; I2 = 19%). The test for subgroup differences was not significant (I2 = 0%) (Analysis 1.1). We performed a subgroup analysis to evaluate the differences among the four weaning categories (simple, difficult, prolonged, and mixed weaning). In the simple weaning group, three studies (Esteban 1997; Haberthur 2002; Koksal 2004) involving 497 patients compared PS versus T‐tube in patients who tolerated the first SBTs and were extubated. We did not find any statistically significant difference in the proportion of patients extubated with success (RR 1.05, 95% CI 0.91 to 1.22, P = 0.47) in the presence of non‐significant heterogeneity (I2 = 34%). For four studies (Esteban 1995; Esteban 1997; Matić 2004; Matić 2007) on 278 patients who were considered to present difficult weaning, we did not find any significant difference between the patients who underwent PS (95/132) versus T‐tube (101/146), with low heterogeneity (I2 = 36%) (RR 1.06, 95% CI 0.87 to 1.29, P = 0. 56). We classified one study (Vitacca 2001) as presenting prolonged weaning. This trial involved 52 tracheostomized COPD patients with more than 15 days of MV. We did not find any statistical differences between PS (19/26) and T‐tube SBTs (20/26) (RR 0.95, 95% CI 0.69 to 1.30, P = 0.75). Two studies (Brochard 1994; Koh 2000) that involved 108 patients were included in the mixed weaning group because they did not report data for each weaning group. We did not find any statistically significant difference in the proportion of patients extubated with success (RR 1.33, 95% CI 1.01 to 1.76, P = 0.05), without any heterogeneity (I2 = 0%).
1.1. Analysis.
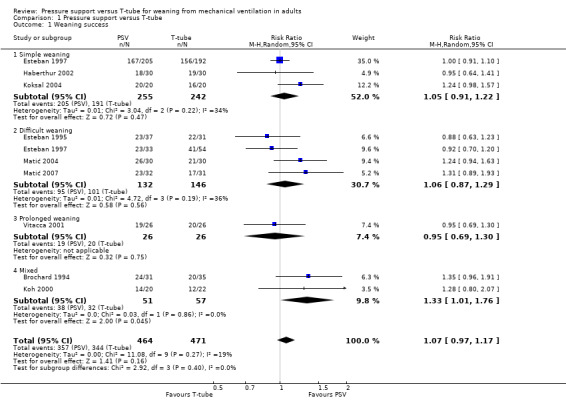
Comparison 1 Pressure support versus T‐tube, Outcome 1 Weaning success.
ICU mortality
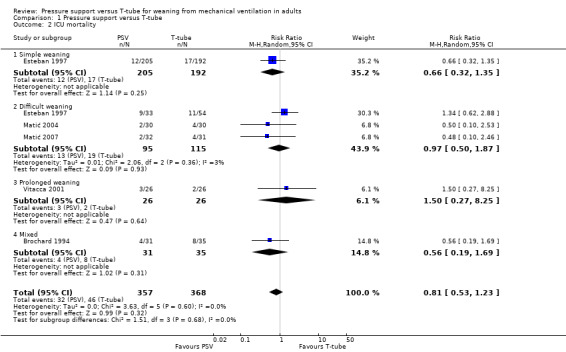
In five trials (Brochard 1994; Esteban 1997; Matić 2004; Matić 2007; Vitacca 2001) reporting on 725 patients, we found a lower but not statistically significant probability of ICU mortality favouring patients undergoing PS (32/357) versus T‐tube SBT (46/368) (RR 0.81, 95% CI 0.53 to 1.23, P = 0.32), without any heterogeneity (I2 = 0%). The test for subgroup differences was not significant (I2 = 0%).
We performed subgroup analysis to evaluate the differences among weaning groups (simple weaning, difficult weaning, prolonged, and mixed weaning). Four studies were classified into four categories of weaning; Brochard 1994 was included in the mixed subgroup analysis as the patients were classified as difficult and prolonged weaning but the data were not reported for each weaning category. Mortality was evaluated for only one study in simple weaning (Esteban 1997) for which we found a lower rate of ICU mortality in the PS group (12/205) than in the T‐tube group (17/192), but this was statistically non‐significant (RR 0.66, 95% CI 0.32 to 1.35, P = 0.25). Three studies (Esteban 1997; Matić 2004; Matić 2007) evaluated ICU mortality among 210 difficult weaning patients and the result from the meta‐analysis for mortality in the difficult weaning subgroup did not show any statistically significant difference between PS and T‐tube (RR 0.97, 95% CI 0.50 to 1.87, P = 0.93), with low heterogeneity (I2 = 3%). In the study by Vitacca 2001, among 52 tracheostomized patients with prolonged weaning three died in the group that underwent PS versus two patients with the T‐tube (26 patients in each group) (RR 1.50, 95% CI 0.27 to 8.25, P = 0.64). See Analysis 1.2.
1.2. Analysis.
Comparison 1 Pressure support versus T‐tube, Outcome 2 ICU mortality.
Time of weaning from mechanical ventilation (weaning duration)
Four studies (Brochard 1994; Esteban 1995; Matić 2004; Matić 2007) evaluated the weaning duration. Three studies (Esteban 1995; Matić 2004; Matić 2007) reported weaning duration data using medians. We did not pool these studies, thus it was not possible to quantitatively evaluate which SBT led to a shorter time for weaning from MV. Brochard 1994 made data available on the time taken to wean from MV, which favoured the PS group over the T‐tube group with a mean difference of ‐2.80 days, but the difference was not statistically significant (95% CI ‐5.84 to 0.24, P = 0.07). Matić 2004 showed better median results for the PS group (54 hours, range 47 to 88) than for the T‐tube group (94 hours, range 79 to 132) (P < 0.001 according to the Mann–Whitney test). Matić 2007 also reported the time taken for weaning as median values, with 43 hours for PS (range 35 to 49) and 63 hours for T‐tube (range 51 to 69) (P < 0.001 according to the Mann‐Whitney test) thus favouring the PS group. However, Esteban 1995 observed better results for the T‐tube group (72 hours, range 24 to 144) than for the PS group (96 hours, range 48 to 288) (P value not available). See Appendix 11.
Reintubation
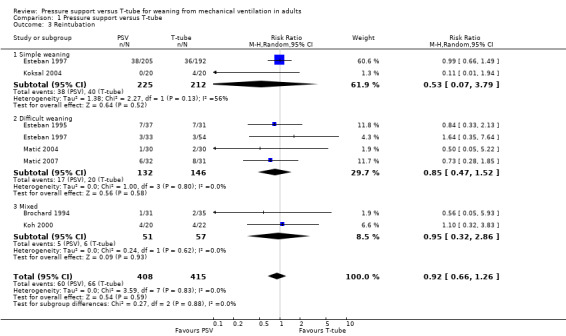
Reintubation was evaluated in seven studies (Brochard 1994; Esteban 1995; Esteban 1997; Koh 2000; Koksal 2004; Matić 2004; Matić 2007) with 823 patients. We did not find any significant difference in the proportion of patients requiring reintubation within 48 hours after extubation (RR 0.92, 95% CI 0.66 to 1.26, P = 0.59), without heterogeneity (I2 = 0%). The test for subgroup differences was not significant (I2 = 0%). See Analysis 1.3.
1.3. Analysis.
Comparison 1 Pressure support versus T‐tube, Outcome 3 Reintubation.
Although we observed that statistical heterogeneity was absent, the studies pooled for analysis on reintubation were clinically different with regard to the weaning process. We performed subgroup analysis for simple, difficult, and mixed weaning. Two studies (Esteban 1997; Koksal 2004) with 437 patients whose weaning was simple had low rates of reintubation in the PS group, which was not statistically significantly different from the T‐tube SBT group (RR 0.53, 95% CI 0.07 to 3.79, P = 0.52) in the presence of moderate heterogeneity (P = 0.13; I2 = 56%).
In four studies (Esteban 1995; Esteban 1997; Matić 2004; Matić 2007) with 278 patients the result from the meta‐analysis for the subgroup of patients who presented with difficult weaning did not show any significant difference between SBTs (PS versus T‐tube) (RR 0.85, 95% CI 0.47 to 1.52, P = 0.58), without any heterogeneity (I2 = 0). Two studies (Brochard 1994; Koh 2000) were included in a third analysis (mixed categories of weaning) because they did not report data for each weaning group. We did not find any statistically significant difference in the proportion of patients that were reintubated (RR 0.95, 95% CI 0.32 to 2.86, P = 0.93), without any heterogeneity (I2 = 0%).
ICU or long‐term weaning unit (LWU) length of stay (days)
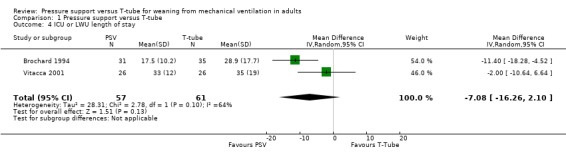
Five studies evaluated the ICU or LWU length of stay and meta‐analysis was done for two studies; the estimated effects on ICU or LWU length of stay favoured the PS group in two studies (Brochard 1994; Vitacca 2001) but without statistical significance (MD ‐7.08 days, 95% CI ‐16.26 to 2.10, P = 0.13). We observed substantial heterogeneity between the studies included in this outcome (P = 0.10; I2 = 64%). The clinical heterogeneity can be explained by at least four characteristics among the participants: mean age (58 versus 73 years), process of weaning (difficult and prolonged versus prolonged weaning), endotracheal prosthesis type (translaryngeal and tracheostomy tubes versus all tracheostomized patients), and percentage of patients with COPD (27% versus 100%). See Analysis 1.4.
1.4. Analysis.
Comparison 1 Pressure support versus T‐tube, Outcome 4 ICU or LWU length of stay.
In three trials (Esteban 1997; Matić 2004; Matić 2007) the estimated effects were reported as median values: 270 (235 to 290) and 331 (292 to 396) hours observed in the PS and T‐tube groups, respectively (P < 0.001; Mann‐Whitney test) (Matić 2004); and 210 (186 to 241) and 241 (211 to 268) hours observed in the PS and T‐tube groups, respectively (P < 0.001, Mann‐Whitney test) (Matić 2007). However, the only study which showed an estimated effect favouring the T‐tube was Esteban 1997, with median values of 12 (288 hours) and 10 (240 hours) for PS and T‐tube, respectively (P = 0.33, Mann‐Whitney test). See Appendix 12.
Pneumonia
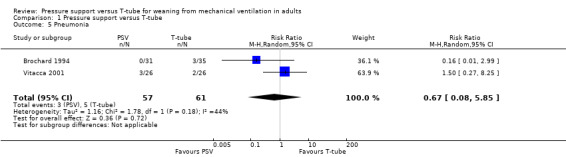
We pooled the results from two trials (Brochard 1994; Vitacca 2001) that evaluated pneumonia in 118 patients. Of these, 3/57 in the PS group and 5/61 in the T‐tube group developed pneumonia (RR 0.67, 95% CI 0.08 to 5.85, P = 0.72), with moderate statistical heterogeneity (I2 = 44%). See Analysis 1.5.
1.5. Analysis.
Comparison 1 Pressure support versus T‐tube, Outcome 5 Pneumonia.
Successful spontaneous breathing trial (SBT)
The result of the meta‐analysis pooling four studies (Esteban 1997; Haberthur 2002; Matić 2004; Matić 2007) involving 940 patients in relation to successful SBT revealed a statistically significant difference in the proportion of patients in the PS group (388/488) compared with the patients in the T‐tube group (331/452) (RR 1.09, 95% CI 1.02 to 1.17, P = 0.009; risk difference (RD) 0.07, 95% CI 0.02 to 0.12, P = 0.009). We observed that there was no statistical heterogeneity between the studies (I2 = 0%). All the patients had received a translaryngeal tube, the duration of the SBT was two hours, and the patients were considered to present simple weaning. Using these estimates, 14 patients would need to be treated with a PS SBT to have one additional successful SBT. See Analysis 1.6.
1.6. Analysis.
Comparison 1 Pressure support versus T‐tube, Outcome 6 Successful spontaneous breathing trial.
Respiratory rate (RR)
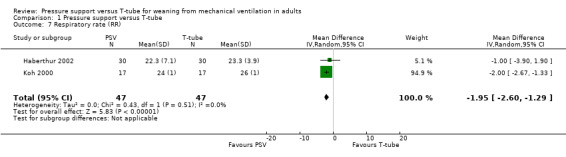
A meta‐analysis on two studies (Koh 2000; Haberthur 2002) compared the RR in 94 intubated patients. The MD ‐1.95 breaths/minute (95% CI ‐2.60 to ‐1.29, P < 0.00001) in favour of PS without any heterogeneity (I2 = 0%). See Analysis 1.7.
1.7. Analysis.
Comparison 1 Pressure support versus T‐tube, Outcome 7 Respiratory rate (RR).
Tidal volume (VT)
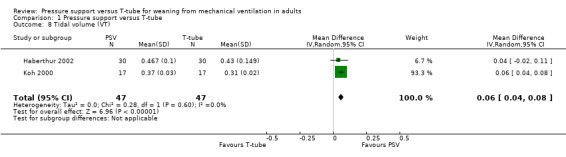
Koh 2000 and Haberthur 2002 evaluated tidal volume (VT) in 94 patients, showing a statistically significant difference in VT in the PS group. The MD was 0.06 L/min (95% CI 0.04 to 0.08, P < 0.00001) without any heterogeneity (I2 = 0%). See Analysis 1.8.
1.8. Analysis.
Comparison 1 Pressure support versus T‐tube, Outcome 8 Tidal volume (VT).
Rapid and shallow breathing index (RSBI or RR/VT)
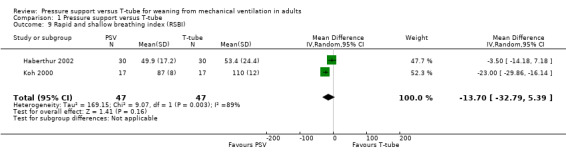
There was no statistical difference in relation to RSBI or RR/VT, with a mean difference of ‐13.70 breaths/min/L (95% CI ‐32.79 to 5.39, P = 0.16) in two studies (Haberthur 2002; Koh 2000) involving 94 patients, with significant heterogeneity (I2 = 89%). See Analysis 1.9.
1.9. Analysis.
Comparison 1 Pressure support versus T‐tube, Outcome 9 Rapid and shallow breathing index (RSBI).
Adverse events
Vitacca 2001 considered new episodes of pneumonia and arrhythmia as complications. The pneumonia outcome was assessed by two studies, and the meta‐analysis for this outcome was described in Analysis 1.5. The same author reported new episodes of arrhythmias in three patients in the PSV and T‐tube groups, and agitation was reported in seven patients assigned to PSV versus three patients in the T‐tube group. Matić 2004 reported that three patients had life‐threatening complications during the procedures in the group submitted to the T‐tube compared to one patient in the PSV group. Brochard 1994 reported ischaemic heart failure during weaning in one patient in each SBT group.
Continuous and dichotomous outcomes that were impossible to combine in a meta‐analysis
1. Proportion of patients requiring tracheostomy
Only one study (Esteban 1997) reported the number of patients who were tracheostomized among 484 intubated patients. There was a statistically non‐significant difference between PS and T‐tube (RR 0.72, 95% CI 0.39 to 1.33, P = 0.29). See Table 4 (item 2).
3. Dichotomous outcomes evaluated by one study.
| Outcomes | N | Estimated effect (RR, 95% CI, P) | Favoured group | Study |
| 1. Hospital mortality | 397 | RR 1.03, 0.65 to 1.64, P = 0.89 | T‐tube | Esteban 1997 |
| 2. Proportion of patients requiring tracheostomy | 484 | RR 0.72, 0.39 to 1.33, P = 0.29 | PS | Esteban 1997 |
2. Hospital mortality
Only one study (Esteban 1997) reported hospital mortality among patients undergoing PS (32/205) and T‐tube SBT (29/192) (RR 1.03, 95% CI 0.65 to 1.64, P = 0.89). See Table 4 (item 1).
3. Hospital length of stay (days)
Two studies (Esteban 1997; Vitacca 2001) measured the total hospital length of stay among intubated and tracheostomized COPD patients, respectively. The data were not pooled because Esteban 1997 presented the results as the median and the IQR was not available in the published study. Vitacca 2001 reported a MD of ‐1.0 day favourable to PSV compared with T‐tube but with no statistical significance (95% CI ‐17.09 to 15.09, P = 0.90). See Appendix 13.
4. Total duration of mechanical ventilation (MV) (hours)
Three studies evaluated total duration of MV, and only one study (Vitacca 2001) reported the mean duration of MV: 181 hours in the PS SBT compared with 130 hours in the T‐tube SBT, among 52 patients. There was a MD of 51 hours, but without statistical significance (95% CI ‐23.09 to 125.09, P = 0.18). Two trials (Matić 2004; Matić 2007) reported the total duration of MV in terms of medians and IQRs. Matić 2004 reported median values for PS versus T‐tube of 215 (range 187 to 259) and 262 hours (range 216 to 328), respectively, thus significantly favouring the PS group (P < 0.001, Mann‐Whitney test). Matić 2007 reported median values favouring the PS group (163, range 113 to 203) compared with the T‐tube group (187, range 143 to 328) (P < 0.001). See Appendix 14.
Quality of life
None of the studies included in this review evaluated quality of life.
Reporting bias
The reporting bias was evaluated for weaning success because this outcome pooled nine studies. We did not identify asymmetry of the funnel plot. See Figure 4.
4.
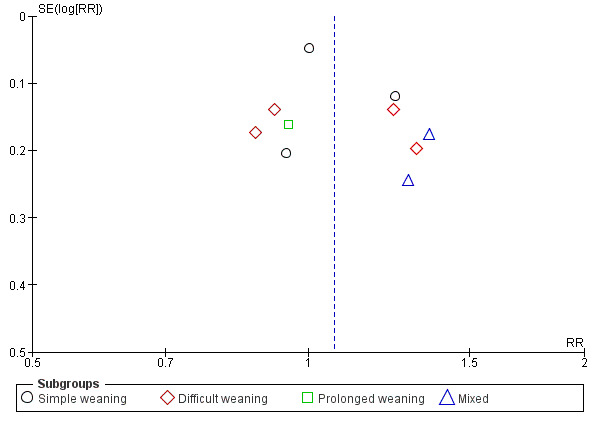
Funnel plot of comparison: 1 Pressure support versus T‐tube, outcome: 1.1 Weaning success.
Subgroup analyses
The studies included in this review could be classified in terms of endotracheal prosthesis: one study with a tracheostomy tube (Vitacca 2001), one study with both tracheostomy and a translaryngeal tube (Brochard 1994), seven studies with a translaryngeal tube (1090, 92.3% of patients) where a tracheostomy tube was an exclusion criterion in these studies. Pooling two studies (Brochard 1994; Vitacca 2001) the number of included tracheostomized patients was about 118 (9.7%); this difference in proportions between intubated and tracheostomized patients was not sufficient to perform subgroups analysis by type of tracheal prosthesis. No included study evaluated PSV versus T‐tube in surgical patients who were ventilated for at least 24 hours. The duration of the SBTs was at least two hours in eight studies; Koh 2000 evaluated weaning success and reintubation outcomes for a PS SBT for 30 minutes compared with an additional 1‐hour period of T‐tube SBT.
Clinically, the nine studies were classified into three groups of weaning: simple weaning (Esteban 1997; Haberthur 2002; Koh 2000; Koksal 2004); difficult weaning (Brochard 1994; Esteban 1995; Esteban 1997; Koh 2000; Matić 2004; Matić 2007); and patients considered to present prolonged weaning (Brochard 1994; Vitacca 2001). Esteban 1997 reported data both for simple and difficult weaning patients. Subgroup analysis based on the weaning process could be carried out for three outcomes: ICU mortality, weaning success, and reintubation. Two studies (Brochard 1994; Koh 2000) were excluded from the subgroup analysis.
Sensitivity analysis
There was a potential risk of detection bias in four studies (Brochard 1994; Koksal 2004; Matić 2007; Vitacca 2001). There were not significant changes to the estimates when the data of these studies were excluded from analysis for the following outcomes: weaning success, ICU mortality and reintubation.
In this review, data for dichotomous outcomes were analysed by ITT.
Discussion
Summary of main results
The studies included here were conducted in various parts of the world, in Europe, South America, and Asia, although all of them were published in the English language. The results of this systematic review have external validity for adult patients, mostly intubated, who were on mechanical ventilation for at least 24 hours due to acute respiratory failure of different aetiologies and classified into three categories of weaning (simple, difficult, and prolonged). Despite the fact that the included studies had not defined respiratory failure, the causes of respiratory failure or reasons for the initiation of mechanical ventilation were described for eight studies. The criteria for interruption of ventilatory support were described by all authors.
Pressure support (PS) ventilation and a T‐tube were used directly as spontaneous breathing trials (SBTs) in four studies with 844 patients (69.9% of the sample). In 186 (15.4%) included patients, both interventions were used along with a gradual weaning from mechanical ventilation; the PS was gradually decreased, twice a day, until the minimal PS was reached (PSmin) and periods with a T‐tube were gradually increased to two hours (Brochard 1994; Esteban 1995) and eight hours (Vitacca 2001) of SBTs for patients with difficult and prolonged weaning. In two studies involving 178 (14.7%) patients, the PS was lowered to 2 to 4 cm H2O (Matić 2007) and 3 to 5 cm H2O (Koh 2000), based on ventilatory parameters, until they reached the PSmin, and then the results were compared with one trial with the T‐tube.
The duration of the SBTs was 30 minutes in patients submitted to pressure support ventilation (PSV) in one study (Koh 2000), two hours in six studies, and longer (eight and 24 hours) in two studies (Brochard 1994; Vitacca 2001). Two authors (Esteban 1999; Perren 2002) reported no statistical differences between 30 minutes versus 120 minutes of SBTs on the outcomes weaning success and reintubation. The results of this review apply to at least a two hour SBT.
The nine included studies were classified according to the difficulty and length of the weaning process. Four studies presented patients who achieved simple weaning (Esteban 1997; Haberthur 2002; Koh 2000; Koksal 2004). In six studies (Brochard 1994; Esteban 1995; Esteban 1997; Koh 2000; Matić 2004; Matić 2007) the patients failed on their first attempt at a SBT or required seven days of mechanical ventilation before successful weaning. They were classified as having a difficult weaning. Two studies (Brochard 1994; Vitacca 2001) presented patients with prolonged weaning. They had failed three attempted SBTs or required more than seven days of mechanical ventilation after their first SBT to finally achieve successful weaning. Four studies had patients classified into two weaning groups, and only Esteban 1997 followed up on simple and difficult weaning patients until their discharge or death. The classification of patients into three groups of weaning was based on expert opinion during the Fifth Conference of the International Consensus Intensive in 2005, according to difficulty and duration of weaning from mechanical ventilation (Boles 2007). We classified the included studies into three categories of weaning based on information reported in the original articles and by contacting the authors. Further studies are being conducted to establish this classification and to evaluate how the outcomes of ICU mortality, reintubation, and length of stay in the ICU are affected in each category of weaning (Funk 2010; Peňuelas 2011; Sellares 2011).
Weaning success was defined as the absence of the requirement for ventilatory support within 48 hours after extubation (translaryngeal tube) or withdrawal (tracheostomy tube) of mechanical ventilation in all included studies. Nine studies assessed this outcome in 935 patients; approximately 77% of the patients who underwent PS and 73% with a T‐tube achieved weaning success, although this difference was statistically non‐significant. The weaning success was 80%, 70%, and 75% on simple, difficult, and prolonged weaning, respectively. Boles 2007 reported weaning success in 1710 (68.8%) patients (adult and paediatric) pooled in six studies, and therefore the SBTs, population, and duration of the SBT differed among the studies. In this review, the percentages of patients in simple, difficult, and prolonged weaning groups were 60%, 34%, and 6%, respectively. In the Funk 2010 trial, the percentage of patients in the weaning categories was similar to this review: 60% and 26% for simple and difficult weaning, and 35% for prolonged weaning. Our sample size for prolonged weaning was smaller (52 patients).
The ICU mortality rate was not statistically different among the patients who passed the SBTs using PS and T‐tube, independent of the weaning process. The overall mortality rate was 10.7% (78) among 725 patients. The mortality rate was 7.3% for the patients with simple weaning, 15.2% among those with difficult weaning, and 9.6% among those with prolonged weaning. The mortality rate was higher among the patients with difficult weaning. Peňuelas 2011 reported the same mortality rate between simple and difficult weaning groups (7%) and 22% for prolonged patients in the 2714 patients who were weaned. In the 257 patients of an observational study, Funk 2010 described a higher mortality rate (22%) for prolonged weaning compared to 3% for the simple group and 1% in the difficult weaning group. Our sample size for prolonged weaning was small (52 patients transferred to weaning units).
The duration of weaning from mechanical ventilation was analysed qualitatively, even though four studies (Brochard 1994; Esteban 1997; Matić 2004; Matić 2007) had already evaluated this outcome. The data of three of these studies were reported as medians and interquartile ranges. The mean and standard deviation can be estimated from the median (Hozo 2005), but we chose not to perform meta‐analysis with estimated data. Based on the qualitative analysis of these three studies (Brochard 1994; Matić 2004; Matić 2007), there was a tendency of PS to reduce the time for weaning of difficult and prolonged weaning groups (see Appendix 11). The weaning duration depends on the cause of the respiratory failure as, for example, COPD patients can spend up to 59% of their total time on mechanical ventilation in the process of withdrawal of ventilatory support (Esteban 1994). Blackwood 2010 reported that implementation of weaning protocols was related to the shorter duration of weaning, a reduction of 78% on the time spent for weaning, given the significant heterogeneity among the included studies; this systematic review did not establish the SBTs (PSV versus T‐tube) that influenced weaning duration.
In this review, the reintubation rate was higher among patients who used the T‐tube (16% versus 15% for PS) but we did not find any statistically significant difference between them. The rate of reintubation within 48 hours after extubation among 823 participants was 16.5%. Esteban 1999 and Boles 2007 reported reintubation in 13.5% (453) and 13.0% (1962) of the patients extubated after successful SBTs. From the subgroup analysis on two categories of the weaning process, the reintubation rate was higher among the patients with simple rather than difficult weaning: 18.% and 13%, respectively. Again, there was not any statistically significant difference between PSV and the T‐tube. According to MacIntyre 2012, reintubation rates of 5% to 20% seem to be reasonable as low values of reintubation can be associated with delays in the withdrawal of a mechanical ventilator and higher rates suggest early interruption of ventilatory support. The rates of reintubation with simple and difficult weaning in two observational studies (Funk 2010; Peňuelas 2011) were 19% and 5% and 10% and 10%, respectively. In this review, the reintubation rate was lower in the difficult weaning group.
The successful SBT (PSV or T‐tube) is used as a predictor of weaning success from mechanical ventilation, so this outcome was added to the systematic review. Data were available from four included studies. A statistically significantly percentage (79.5% versus 73.2%) of the patients on simple weaning who underwent two hours of PS passed the SBT and were extubated. A greater number of patients undergoing T‐tube trials failed the two hours of SBT, and these patients returned to mechanical ventilation for at least 24 hours. After pooling the data on 940 patients in a meta‐analysis, 719 (76.4%) were found to have had a successful SBT. Weaning success or successful extubation is the absence of ventilatory support (Brochard 1994; Vitacca 2001) 48 hours after extubation or the withdrawal of mechanical ventilation in all included studies. In all studies included here, the intolerance criteria or tolerance criteria for SBTs were similar: respiratory rate and pattern, gas exchange (arterial oxygen saturation), and haemodynamic stability (heart rate and systolic blood pressure) (see Table 3). Ezingeard 2006 observed that the intubated patients who failed the SBT through the T‐tube but continued the SBT with PS of 7 or 10 cm H20 were successfully extubated. Several studies showed that work of breathing is significantly higher during T‐tube trials compared with PSV trials (Cabello 2010; Koh 2000; Kuhlen 2003; Patel 1996).
The ICU and long‐term weaning unit (LWU) lengths of stay were evaluated by five authors (Brochard 1994, Esteban 1997; Matić 2004; Matić 2007; Vitacca 2001). The mean difference of 7.08 days, favourable for PSV, in our meta‐analysis of two studies (Brochard 1994; Vitacca 2001) with 118 patients did not reach a statistical significance. Three studies (Esteban 1997; Matić 2004; Matić 2007) were not pooled in a meta‐analysis because they described their results as medians and interquartile ranges (IQRs) and we decided not to perform meta‐analysis with the mean estimated by median data. The results reported by two studies (Matić 2004; Matić 2007) were favourable to PSV and Esteban 1997 reported two days reduced ICU length of stay in simple weaning patients submitted to the T‐tube. Blackwood 2010 reported a 10% reduction in ICU length of stay in studies that adopted a weaning protocol. All studies included in this review followed the criteria for the interruption of mechanical ventilation, an initial T‐tube test, and SBTs.
The physiologic parameters planned for this review were evaluated by seven studies, and these parameters were measured in an initial T‐tube test between two to five minutes before the SBTs. Only two studies (Haberthur 2002; Koh 2000) evaluated RR, VT, and rapid shallow breathing index (RSBI) during SBTs; for two outcomes, RR and VT, the PS was statistically superior to the T‐tube in a meta‐analysis of two studies with 94 pooled patients. We did not find any differences between PS and T‐tube SBTs among the 94 pooled simple weaning patients with regard to RSBI. The RSBI was used as a weaning predictor test before trials of extubation (SBTs) as recommended by Boles 2007 and MacIntyre 2012. In this review, the PSV was not statistically different from T‐tube, and some studies (Cabello 2010; Gonçalves 2012; Santos 2007) reported that RSBI measured with PSV of 5 to 10 cm H2O is overestimated, that is, the value of the rapid and shallow breathing index (RSBI or RR/VT)is lower than was measured for PSV.
It was not possible to perform meta‐analyses for hospital length of stay, total duration of mechanical ventilation, proportion of patients requiring a tracheostomy, and hospital mortality outcomes. Although at least two studies evaluated the total duration of mechanical ventilation and hospital length of stay, the data from three studies were reported as the median and interquartile range but we chose not to perform meta‐analysis with estimated data. Patients in difficult weaning who submitted to PSV spent less time on mechanical ventilation (median of ‐47 hours) than patients who submitted to the T‐tube. Vitacca 2001 reported a mean of 51 hours of mechanical ventilation in tracheostomized patients on prolonged weaning and weaned by T‐tube (see Appendix 13 and Appendix 14). Only the study by Esteban 1997 assessed hospital mortality and the proportion of patients requiring tracheostomy. There was not any statistical difference between PSV and T‐tube for these outcomes (see Table 4).
Adverse effects were reported by three studies (Brochard 1994; Matić 2004; Vitacca 2001). New episodes of pneumonia and arrhythmia were diagnosed in 11.5% and 7% of patients, respectively, while 3% of the patients submitted to SBTs presented with ischaemic heart failure during weaning. Agitation needing low dose sedative was found in 19% of patients (seven in PSV versus three in T‐tube SBTs), and life‐threatening complications during the procedure were reported in 6.7% of patients (one (3.5%) in PSV versus three (10%) in T‐tube SBTs). The studies did not find any significant statistical difference between patients who underwent PS and T‐tube SBTs. Costa 2005 reported a higher frequency of arrhythmias in cardiac patients compared to patients without heart disease, regardless of SBTs (PSV versus T‐tube). The SBTs appear to be safe for weaning patients from mechanical ventilation.
Subgroup analysis was conducted in accordance with the weaning process (simple, difficult, and prolonged) for the three outcomes ICU mortality, weaning success and reintubation. Four studies compared the PSV versus T‐tube techniques in two weaning groups; only Esteban 1997 reported all of the data evaluated for each weaning group, while two studies (Brochard 1994; Koh 2000) did not present data for each weaning category and were excluded from the subgroup analysis. Haberthur 2002 evaluated and reported the data for weaning success in patients in the simple and difficult weaning groups. However, the study design was cross‐over. We thus collected the results of the first study moment, that is, prior to cross‐over.
None of the studies evaluated comfort, quality of life, or costs. The agitation during SBTs may be associated with patient discomfort.
Overall completeness and applicability of evidence
The results from this systematic review applied to adult patients with at least 24 hours of invasive mechanical ventilation. The patients were clinically and biogenically stable, their weaning was either simple or difficult, and they underwent SBTs through PS and the T‐tube. The results were favourable towards PS but were non‐statistically significant for weaning success, ICU mortality, reintubation and other factors. The RR and VT were statistically significant in favour of PS. The patients who underwent PS for 120 minutes (two hours) were extubated because they demonstrated a successful SBT.
Quality of the evidence
We defined six relevant outcomes (weaning success, ICU mortality, reintubation, ICU or LWU length of stay, pneumonia, and successful SBT) in order to assess the quality of evidence. Four outcomes (weaning success, ICU mortality, reintubation, ICU or LWU length of stay) yielded low quality evidence. Successful SBT was classified as moderate quality evidence, and pneumonia as very low quality evidence. See Table 1.
Potential biases in the review process
The protocol was published in 2006 (Ladeira 2006).
In the seven years since publication of the protocol, the original primary outcome, weaning duration, has been discarded. The binary variable weaning success is now considered the preferred outcome when evaluating the effectiveness of both PSV and T‐tube as SBTs for simple and difficult weaning. For prolonged weaning patients, the weaning duration may be better to evaluate the effectiveness of PSV and T‐tube as methods for gradual withdrawal from mechanical ventilation.
In this review, we added a successful SBT as a secondary outcome and we included subgroup analyses according to the difficulty and length of the weaning process, as presented by Laurent Brochard at the 5th International Consensus Conference in Intensive Care Medicine: weaning from mechanical ventilation (Boles 2007).
Only one study (Vitacca 2001), which included 52 tracheostomized patients, was classified as presenting prolonged weaning. The results of the present systematic review are limited in relation to this category of weaning.
The data taken to indicate success of weaning in the study by Brochard 1994 were based on failure to wean. We removed all weaning failures from the total number in each group (PS and T‐tube) and considered the difference between them to be weaning success.
Meta‐analysis was not performed for the outcomes of ICU and hospital length of stay, time of weaning from mechanical ventilation, and total duration of mechanical ventilation because the data from the included studies were presented as medians and interquartile ranges. We could have made an estimate of the mean using the values of the median values and the low and high ends of the range to perform a meta‐analysis for continuous data (Hozo 2005) but we chose not to perform meta‐analysis with estimated data.
Seven cross‐over trials, which evaluated appropriate surrogate outcomes in order to perform cross‐over, such as work of breathing, pressure‐time product, energy expenditure, RR, VT and RSBI, were excluded from this review because no data from the initial period were available in the published trials.
Agreements and disagreements with other studies or reviews
We have not found any other systematic review with meta‐analysis that compared PS versus T‐tube spontaneous breathing trials; this is therefore the first one.
The published reviews on mechanical ventilation and weaning (Boles 2007; Caroleo 2007; Luetz 2012) reported no difference between PS and T‐tube spontaneous breathing trials for several outcomes. The present systematic review showed that PS was significantly superior to T‐tube for predicting extubation in simple weaning patients (RR 1.09, 95% CI 1.02 to 1.17, P = 0.009, NNT = 14), but the weaning success was not statistically favourable to PSV.
Studies have shown that when RSBI was measured with PS in comparison with spontaneous ventilation through the T‐tube, the RSBI value was overestimated with PSV (Gonçalves 2012; Patel 2009; Santos 2007). In the present systematic review we grouped only two studies and pooled 94 patients, and PS was not statistically superior to the T‐tube.
Authors' conclusions
Implications for practice.
Pressure support and T‐tube can be used as SBTs to evaluate whether patients in the simple and difficult weaning groups are able to assume spontaneous ventilation. In prolonged weaning patients, both interventions can be used in the gradual weaning process from mechanical ventilation. The classification of patients into three weaning groups follows the criteria established at the 5th Conference of the International Consensus Intensive in 2005 (Boles 2007). Based on our assessment of each key outcome we consider the quality of evidence to be generally low. We found no clear evidence of any differences between PS and T‐tube in the three weaning groups with regards to successful weaning, reintubation, ICU mortality, pneumonia and RBSI. Pressure support of 5 to 10 cm H2O for two hours allowed 79.5% of patients in the simple weaning category to be extubated compared with 73.5% with the T‐tube (NNT = 14).
Implications for research.
Further randomized clinical trials should be conducted in order to assess whether or not PSV is safer and more effective compared to the T‐tube method for achieving relevant clinical outcomes (including weaning success, success of spontaneous breathing trials, reintubation, ICU mortality, time of weaning, ICU and hospital length of stay, total duration of mechanical ventilation, costs, adverse effects, work of breathing and the comfort of patients) among adult patients with at least 24 hours of invasive ventilatory support. Such characteristics as spontaneous breathing trial duration, participants, weaning categories (simple, difficult and prolonged) and minimal values of PS must be established and reported.
What's new
| Date | Event | Description |
|---|---|---|
| 14 December 2018 | Amended | Editorial team changed to Cochrane Emergency and Critical Care |
History
Protocol first published: Issue 2, 2006 Review first published: Issue 5, 2014
| Date | Event | Description |
|---|---|---|
| 28 September 2008 | Amended | Converted to new review format. |
Acknowledgements
We would like to thank Harald Herkner, John F Fraser, Tasnim Sinuff, Kathie Godfrey, Nete Villebro, Amy Woodruffe and Karen Burns for their help and editorial advice during the preparation of the protocol.
We would like to thank Harald Herkner (content editor), Nathan Pace (Statistical editor), Imelda M Galvin, Mauricio Ferri (peer reviewers) and Janet Wale (consumer editor) for their help and editorial advice during the preparation of this systematic review.
Special thanks to Laurent Brochard, Andrés Esteban, Christoph Haberthür, Güniz Koksal, Younsuck Koh, Michele Vitacca for their prompt reply to our additional questions.
Appendices
Appendix 1. Search strategy for EMBASE (OvidSP)
1. exp respiratory‐failure/ or (respiratory adj3 (insufficien* or failure)).mp. 2. exp artificial‐ventilation/ or positive‐end‐expiratory‐pressure/ or (Pressure support adj3 weaning).mp. or (Mechanical adj3 ventilat*).mp. or (Ventilator adj3 Weaning).mp. 9orT tube.mp. 3. (placebo.sh. or controlled study.ab. or random*.ti,ab. or trial*.ti,ab.) and human*.ec,hw,fs. 4. 1 and 2 and 3
Appendix 2. Search strategy for CINAHL (EBSCOhost)
S1. MW Respiratory Failure or TX (respiratory failure) or (respiratory insufficiency) S2. MW Ventilation Mechanical or MW Ventilator‐Weaning or MW Positive‐Pressure‐Ventilation or TX (pressure support weaning) or TX (mechanical ventilation) or TX (ventilator weaning) or TX T tube S3. TX random$ or TX clinical trial$ or TX placebo or TX controlled study or TI trial* S4. S1 and S2 and S3
Appendix 3. Search strategy for CENTRAL, The Cochrane Library
#1 MeSH descriptor Respiratory Insufficiency exp all trees #2 (respiratory near failure) #3 (#1 OR #2) #4 MeSH descriptor Respiration, Artificial exp all trees #5 MeSH descriptor Ventilator Weaning exp all trees #6 MeSH descriptor Positive‐Pressure Respiration exp all trees #7 ((pressure near support) near weaning) or (mechanical near ventilation) or (ventilator near weaning) or t tube #8 (#4 OR #5 OR #6 OR #7) #12 (#3 AND #8)
Appendix 4. Search strategy for MEDLINE (OvidSP)
1. exp Respiratory‐Insufficiency/ or (respiratory adj3 (insufficien* or failure)).mp. 2. Ventilation/ or (mechanical adj3 ventilat*).mp. or exp Ventilator‐Weaning/ or exp Positive‐Pressure‐Respiration/ or (pressure support adj3 weaning).mp. or (ventilat* adj3 weaning).mp. or T tube.mp. 3. ((randomized controlled trial or controlled clinical trial).pt. or randomized.ab. or placebo.ab. or clinical trials as topic.sh. or randomly.ab. or trial.ti.) and humans.sh. 4. 1 and 2 and 3
Appendix 5. Search strategy for LILACS (via BIREME interface)
("RESPIRATORY DEPRESSION/" or "RESPIRATORY FAILURE/" or "RESPIRATORY INSUFFICIENCY/" or "Respiratory Failure" or "Respiratory Insufficien$" or "Insuficincia respiratria" or "Escasez respiratoria" or "Depresin respiratoria" or "Depresso respiratria") and ("MECHANICAL VENTILATOR WEANING/" or "RESPIRATOR WEANING/" or "WEANING/" or "Artificial Respirat$" or "Weaning Ventilator" or "Respirator Weaning" or "Pressure support" or "T TUBE" or "Ventilao mecnica" or "Ventilacin mecnica" or "Respiracin artificial" or "Respirao artificial" or "Sustentao da presso" or "Ayuda de la presin")
Appendix 6. Search strategy for SciELO
(spontaneous breathing trial) or (weaning mechanical ventilation)
Appendix 7. Search strategy for CAPES
(desmame da ventilação mecânica)
(teste de respiração espontânea)
Appendix 8. Search strategy for Current Controlled Trials
(spontaneous breathing trial) or (spontaneous breathing trials)
(ventilator weaning)
(pressure support or pressure support ventilation)
Appendix 9. Data Extraction Form
Review: Pressure support versus T‐tube for weaning from mechanical ventilation in adults.
Review ID: CARG 124
Reviewer: Ladeira, Magdaline T.
Date: ___ / ___ / 20____.
1) Included study ( ) 2)Excluded study( ) If 2, Why? ____________________
____________________________________________________________________________________________________________________________________________
| Identification | |||||||||||||
| Study ID | |||||||||||||
| Title | |
||||||||||||
| Journal | |||||||||||||
| Authors | |
||||||||||||
| Year of publication | |||||||||||||
| Medline ID | |||||||||||||
| Volume, Issue e page | |||||||||||||
| Language | |||||||||||||
| Design study | |||||||||||||
| Participants | |||||||||||||
| Total | PS | T‐Tube | |||||||||||
| 1. N | |||||||||||||
| 2. Age | |||||||||||||
| 3. Gender (Men) (Women) |
|||||||||||||
| 4. Inclusion criteria | |
||||||||||||
| 5. Exclusion criteria | |
||||||||||||
| 6. Time of MV before trial (hours or days) | |||||||||||||
| 7. Translaryngeal or tracheotomy tube | |||||||||||||
| 8. Score Health | |||||||||||||
| 9. Similarity between groups | |||||||||||||
| 10. Notes | |||||||||||||
| Interventions | |||||||||||||
| Number of interventions | |||||||||||||
| 1. Intervention in experimental Group 1 (PS) | |||||||||||||
| Pressure support level (cmH2O) | |||||||||||||
| Duration of SBT (30, 60, 120min or other) | |||||||||||||
| FiO2 | |||||||||||||
| 2. Intervention in experimental Group 2 (T‐tube) | |||||||||||||
| T‐tube (T‐piece) | |||||||||||||
| Duration of SBT(30, 60,120min or other) | |||||||||||||
| O2 L/min | |||||||||||||
| Methods | |||||||||||||
| 1.Statistical Analysis (mean/ median) | |||||||||||||
| 2. Sample size calculation | |
||||||||||||
| 3. Intention‐to‐treat analysis | |||||||||||||
| Risk of Bias | |||||||||||||
| Bias | Authors Judgement | Support for Judgement | |||||||||||
| Adequate sequence generation? | |||||||||||||
| Allocation concealment? | |||||||||||||
| Free of selective reporting? | |||||||||||||
| Free of detection bias? | |||||||||||||
| Free of attrition bias? | |||||||||||||
| Free of other bias? | |||||||||||||
| Outcomes measured | |||||||||||||
| Weaning processes |
Simple weaning |
Difficult weaning | Prolonged weaning | ||||||||||
| Outcomes | PS | T‐tube | PS | T‐tube | PS | T‐tube | |||||||
| 1‐ Time of weaning from MV | |||||||||||||
| 2‐ ICU mortality | |||||||||||||
| 3‐ Hospital mortality | |||||||||||||
| 4‐ Weaning success (successful extubation) | |||||||||||||
| 5‐ Reintubation | |||||||||||||
| 6‐ Tracheostomy | |||||||||||||
| 7‐ ICU Length of stay | |||||||||||||
| 8‐ Hospital Length of stay | |||||||||||||
| 9‐ Pneumonia | |||||||||||||
| 10‐ Duration of mechanical ventilation | |||||||||||||
| 11‐ Adverse events | |||||||||||||
| 12‐ Quality of life | |||||||||||||
| 13‐ Successful spontaneous breathing trial | |||||||||||||
| 14‐ Respiratory Rate (RR) | |||||||||||||
| 15‐ Tidal Volume( VT) | |||||||||||||
| 16‐ Oxygenation index | |||||||||||||
| 17‐ Pi max | |||||||||||||
| 18‐ Rapid and shallow breathing index (RSBI) | |||||||||||||
Reviewer/ Co‐reviewer:_______________________________________________________
Appendix 10. Outcomes list obtained from primary studies
1. Arrhythmias
2. Blood glucose
3. CO2 arterial pressure (PaCO2)
4. Continued MV after 14 days
5. Duration of weaning (days)
6. Extubation failure
7. Failure at 21 days
8. Failure before 21 days (reintubation or early interruptions resulting from the weaning process)
9. Failure of weaning
10. Mortality in ICU
11. Hospital mortality
12. Inspired oxygen fraction (FiO2)
13. Length of ICU stay
14. Length of hospital stay
15. Life‐threatening complications during procedure
16. LWU duration
17. Minute ventilation (VE)
18. P 0.1
19. Partial arterial oxygen pressure (PaO2)
20. Plasma cortisol
21. Plasma insulin
22. Pneumonia
23. Pressure time product (PTP)
24. Proportion requiring tracheostomy
25. Rapid shallow breathing index (RSBI and RR/VT)
26. Reintubation
27. Respiratory rate (RR)
28. Successful extubation
29. Successful weaning
30. Sucessful spontaneous breathing trial
31. Tidal volume (VT)
32. Urine vanillylmandelic acid (VMA)
33. Work of breathing (WOB)
Appendix 11. Time of weaning from mechanical ventilation (MV) (duration of weaning)
| Study | PSV | T‐tube | P value |
| Brochard 1994 | 5.7d±3.7, N = 26 | 8.5d±8.3, N = 30 | < 0.05 |
| Esteban 1995 | 96h (IQ 48 ‐ 288), N = 37 | 72h (IQ 24‐ 144), N = 31 | not available |
| Matić 2004 | 54h (IQ 47 ‐ 88), N = 30 | 94h (IQ 79 ‐132), N = 30 | < 0.001 |
| Matić 2007 | 43h (IQ 35 ‐ 49), N = 32 | 63h (IQ 51 ‐ 69), N = 31 | < 0.001 |
Appendix 12. ICU length of stay
| Study | PSV | T‐tube | P value |
| Esteban 1997 | 12d (IQ not available, N = 205) | 10d (IQ not available, N = 192) | P = 0.33 |
| Matić 2004 | 270h (IQ 235‐290, N = 30) | 331h (IQ 292‐396, N = 30) | < 0.001 |
| Matić 2007 | 210h (IQ 186‐241, N = 32) | 241h (IQ 211‐268, N = 31) | < 0.001 |
Appendix 13. Hospital length of stay
| Study | PSV | T‐tube | P value |
| Esteban 1997 | 28d (IQ not available, N = 205) | 24d (IQ not available, N = 192) | P = 0.33 |
| Vitacca 2001 | 49d ± 27, N = 26 | 50d ± 32, N = 26 | not available |
Appendix 14. Total duration of mechanical ventilation (MV)
| Study | PSV | T‐Tube | P value |
| Matić 2004 | 215h (IQ 187‐ 259), N = 30 | 262h (IQ 216‐328), N = 30 | < 0.001 |
| Matić 2007 | 163h (IQ 113‐203), N = 32 | 187h (IQ 143‐222), N = 31 | < 0.001 |
| Vitacca 2001 | 181h ± 161, N = 26 | 130h ± 106, N = 26 | not available |
Data and analyses
Comparison 1. Pressure support versus T‐tube.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Weaning success | 9 | 935 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.97, 1.17] |
| 1.1 Simple weaning | 3 | 497 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.91, 1.22] |
| 1.2 Difficult weaning | 4 | 278 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.87, 1.29] |
| 1.3 Prolonged weaning | 1 | 52 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.69, 1.30] |
| 1.4 Mixed | 2 | 108 | Risk Ratio (M‐H, Random, 95% CI) | 1.33 [1.01, 1.76] |
| 2 ICU mortality | 5 | 725 | Risk Ratio (M‐H, Random, 95% CI) | 0.81 [0.53, 1.23] |
| 2.1 Simple weaning | 1 | 397 | Risk Ratio (M‐H, Random, 95% CI) | 0.66 [0.32, 1.35] |
| 2.2 Difficult weaning | 3 | 210 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.50, 1.87] |
| 2.3 Prolonged weaning | 1 | 52 | Risk Ratio (M‐H, Random, 95% CI) | 1.5 [0.27, 8.25] |
| 2.4 Mixed | 1 | 66 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.19, 1.69] |
| 3 Reintubation | 7 | 823 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.66, 1.26] |
| 3.1 Simple weaning | 2 | 437 | Risk Ratio (M‐H, Random, 95% CI) | 0.53 [0.07, 3.79] |
| 3.2 Difficult weaning | 4 | 278 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.47, 1.52] |
| 3.3 Mixed | 2 | 108 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.32, 2.86] |
| 4 ICU or LWU length of stay | 2 | 118 | Mean Difference (IV, Random, 95% CI) | ‐7.08 [‐16.26, 2.10] |
| 5 Pneumonia | 2 | 118 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.08, 5.85] |
| 6 Successful spontaneous breathing trial | 4 | 940 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [1.02, 1.17] |
| 7 Respiratory rate (RR) | 2 | 94 | Mean Difference (IV, Random, 95% CI) | ‐1.95 [‐2.60, ‐1.29] |
| 8 Tidal volume (VT) | 2 | 94 | Mean Difference (IV, Random, 95% CI) | 0.06 [0.04, 0.08] |
| 9 Rapid and shallow breathing index (RSBI) | 2 | 94 | Mean Difference (IV, Random, 95% CI) | ‐13.70 [‐32.79, 5.39] |
| 10 Time of weaning from MV (Duration of weaning) | 4 | Mean Difference (IV, Random, 95% CI) | Totals not selected |
1.10. Analysis.
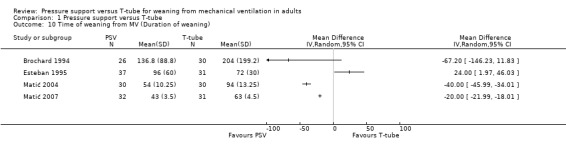
Comparison 1 Pressure support versus T‐tube, Outcome 10 Time of weaning from MV (Duration of weaning).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Brochard 1994.
| Methods | Multicentre RCT Setting: Three medical‐surgical intensive care units in France, Spain and Italy Sample size: not reported |
|
| Participants | ‐ 109 intubated and tracheostomized patients ventilated for more than 24 hours who failed at any time before or at the end of the 2h of T‐tube trial (difficult weaning) ‐ Mean age: 59.1 years ‐ Mechanical ventilation time: mean of 14 days ‐ Mean SAPS (simplified acute physiologic score): 12 ‐ Female: 35 ‐ No statistical difference existed among the groups regarding their characteristics |
|
| Interventions | 1‐ T‐ piece, several periods of disconnection from MV during the day (n=35) 3‐ Pressure support ventilation of 8cmH2O and PEEP of 4cmH2O (n=31) 2‐ SIMV (synchronized intermittent mandatory ventilation) (n=43) |
|
| Outcomes | 1‐ Success of weaning 2‐ Failure at 21 days 3‐ Failure before 21 days (reintubation or early interruptions resulting from the weaning process) 4‐ ICU mortality 5‐ Total length of stay in ICU 6‐ Weaning duration 7‐ Reintubation |
|
| Notes | ‐ Group 3 was not included in this review ‐ T‐Tube: Incremental durations of T‐piece periods were recommended two times per day. When the duration of disconnection had reached 2h with adequate gas exchange, tracheal extubation was decided ‐ PSV: Pressure support level at the beginning of the weaning procedure was 18.1±3.8 cmH20, two times per day the level of pressure support was decreased by 2 or 4 cmH20 until the pressure support of 8 cmH20 or less during 24‐h period, tracheal extubation was performed Success of weaning was considered when the patients had no need for ventilatory assistance for at least 48h after tracheal extubation or after permanent disconnection from the MV in patients with tracheostomies |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The randomization was stratified according to the centre and to etiology of the process responsible for difficult weaning |
| Allocation concealment (selection bias) | Low risk | The authors did use closed‐envelope technique |
| Selective reporting (reporting bias) | Low risk | Outcomes were clinically relevant to evaluate the effectiveness and safety of weaning strategies |
| Other bias | High risk | The authors reported: Criteria for extubation were different in three groups |
| Free of detection bias ? | High risk | The authors reported the absence of blinding after randomization in methodological bias during discussion |
| Free of attrition bias? | Low risk | The patient flow was clear and the authors performed ITT analysis for failures |
Esteban 1995.
| Methods | Multicentre RCT Setting: medical‐surgical intensive care units of 14 teaching hospitals in Spain Sample size: 31 patients were needed in each group to detect at a power of 80 % a difference in weaning time between groups of two days (alpha error: 0.05) |
|
| Participants | ‐ 130 intubated patients receiving mechanical ventilation for more than 24 hs, with signals of poor tolerance during in initial trial of spontaneous breathing (difficult weaning) ‐ Mean age: 58 years ‐ Mechanical ventilation time: mean of 9.3 days ‐ Mean APACHE II: 19.5 ‐ The groups were similar with respect to the patients' characteristics, the indications for mechanical ventilation, and respiratory function; but there was significant difference only in the duration of ventilatory support before weaning was begun (mean days = PS: 10.8, T‐tube: 8.4) |
|
| Interventions | 1‐ Intermittent mandatory ventilation (IMV) (n=29) 2‐ Pressure support ventilation of 5 cmH2O (n=37) 3‐ Intermittent trials of spontaneous breathing through either a T‐tube (n=27) or a continuous positive airways pressure (CPAP) ≤ 5cmH20 (n=6) (n=33) 4‐ Once‐daily trial of spontaneous breathing through a T‐tube circuit for up 2 hours alternating with assist‐control ventilation if signs of intolerance developed (n=31) |
|
| Outcomes | 1‐ Weaning duration (days) 2‐ Successful weaning 3‐ Reintubation 4‐ Continued MV after 14 days |
|
| Notes | ‐ Patients who had signs of poor tolerance at any time during trial of spontaneous breathing through a T‐tube were defined as having difficult weaning ‐ The groups 1 and 3 were not considered for analysis in this review ‐ Extubation criteria for PSV and T‐tube: Patients who tolerated the SBT for two hours with no apparent ill effects were extubated ‐ The level of pressure support was reduced by 2 to 4 cmH2O at least twice a day until 5 cmH2O ‐ Successful weaning was considered if extubation was achieved within the 14‐day period and reintubation was not required within 48 hours of extubation ‐ The outcome duration of weaning was reported as median in 'Additional tables' |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients were stratified according to centre and randomly assigned with the use of a random‐number table |
| Allocation concealment (selection bias) | Low risk | The patients were assigned to the groups in a blinded fashion with the use of opaque, sealed numbered envelopes |
| Selective reporting (reporting bias) | Low risk | Outcomes were clinically relevant to evaluate the effectiveness and safety of weaning strategies |
| Other bias | Low risk | Not suspected |
| Free of detection bias ? | Low risk | Outcome assessors were distinct from study researchers or blinded to the assignments (data reported by author) |
| Free of attrition bias? | Low risk | The patients flow was clear and there was a balanced number of withdrawals between comparison groups |
Esteban 1997.
| Methods | Multicentre RCT Setting: 27 medical‐surgical intensive care units in tertiary care hospital (two in Argentina, one in Brazil, 23 in Spain and one in Venezuela) Sample size: Estimated sample size was 220 patients in each comparison group to detect a 20% difference |
|
| Participants | ‐ 484 patients had endotracheal tube received mechanical ventilation for more than 48 hours before the spontaneous breathing trial ‐ Male: 343; female: 141 ‐ Median age: 64 (51‐72) years ‐ Median SAPS II: 36 (29‐ 47) ‐ Median time of MV: 6 (4 ‐ 12) days There was no significant difference between comparison groups at baseline |
|
| Interventions | 1‐ T‐tube circuit (n=246) 2‐ Pressure support ventilation of 7 cmH2O and PEEP ≤ 5 cmH20 (n=238) |
|
| Outcomes | 1‐ ICU mortality 2‐ Hospital mortality 2‐ Successful weaning or extubation 3‐ Reintubation 4‐ Proportion requiring tracheostomy 5‐ Length of ICU stay 6‐ Length of hospital stay 7‐ Successful spontaneous breathing trial |
|
| Notes | ‐ 28 patients were excluded from the analysis because of missing data, before randomization ‐ PSV and T‐Tube: The extubation was performed after the 2 hours trial of spontaneous breathing ‐ The outcomes were measured in two groups: 1‐ patients who fulfilled 2 hours trial and 2‐ patients who had signs of poor tolerance in the 2 hours trial ‐ The length of ICU and hospital stay were reported as medians in 'Additional tables' |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients were randomly assigned using a random‐number table by permuted blocks according to the study centre |
| Allocation concealment (selection bias) | Low risk | The patients were allocated to the two groups in a blinded fashion with the use of opaque, sealed, numbered envelopes, which were opened only when a patient fulfilled all of the inclusion criteria |
| Selective reporting (reporting bias) | Low risk | Outcomes were clinically relevant to evaluate the effectiveness and safety of both weaning strategies |
| Other bias | Low risk | None suspected |
| Free of detection bias ? | Low risk | The first author reported by email: assessors were distinct from study researchers or blinded to the assignments |
| Free of attrition bias? | Low risk | The patients flow was clear and there was no withdrawal after randomization |
Haberthur 2002.
| Methods | Cross‐over controlled trial Setting: Medical intensive care unit of the university hospital of Basel, Switzerland Sample size: 38 patients were needed in each group to detect, at a power of 80%, a difference in extubation outcome of 30%, with a two‐tailed alpha error of 0.05 |
|
| Participants | ‐ 90 patients with improved or resolved the underlying cause of acute respiratory failure receiving ventilatory support for more than 24 h ‐ Mean age: 57 years ‐ Male: 58; Female: 32 ‐ Mechanical ventilation time: mean of 6.3 days ‐ Mean APACHE II score: 20 ‐ There was no significant difference between comparison groups at baseline |
|
| Interventions | 1‐ T‐tube (n=30) 2‐ Pressure support of 5 cmH2O and PEEP of 5 cmH2O (n=30) 3‐ Automatic tube compensation, PEEP of 5 cmH2O (n= 30) |
|
| Outcomes | 1‐ Successful spontaneous breathing trial 2‐ Successful extubation 3‐ Extubation failure 4‐ Respiratory rate (RR) 5‐ Tidal volume (VT) 6‐ Rapid shallow breathing index (RR/VT) 7‐ Minute ventilation (VE) 8‐ Inspired oxygen fraction (FiO2) 9‐ Partial arterial oxygen pressure (PaO2) 10‐ CO2 pressure arterial (PaCO2) |
|
| Notes | Group 3 was not considered for analysis in this review Part I of the study: In patients who tolerated the 2h breathing trial well, the extubation was performed. ( we used the outcomes of part 1 these study) Part II of the study: In patients who did not tolerate the spontaneous breathing trial, another or other two modes were tried thereafter in random order Successful extubation was considered if there was no need for ventilatory assistance and/or reintubation within 48h following extubation We excluded the outcomes 7, 8, 9 and 10 the review |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Before the start of the study all (future) patients were allocated to one out of the three “ventilator modes” based on a computer‐generated random list |
| Allocation concealment (selection bias) | Low risk | Patients were randomly assigned in a blinded fashion using opaque, sealed envelopes to undergo a trial of spontaneous breathing |
| Selective reporting (reporting bias) | Low risk | Outcomes were clinically relevant. There was neither explicit nor implicit preference from authors to one or another method that could force then to elect specific outcomes |
| Other bias | Unclear risk | The study design can to be one potential risk of bias (cross‐over) |
| Free of detection bias ? | Low risk | Outcome data were assessed from the medical records by another person, not involved in the study (i.e. Rolf Bingisser). Data reported by author |
| Free of attrition bias? | Low risk | The patient flow was clear and there were no reported dropouts |
Koh 2000.
| Methods | Randomized controlled trial Setting: Medical intensive care unit between May 1997 and March 1998, Seoul, Korea Sample size: authors did not estimate sample size |
|
| Participants | ‐ 36 intubated patients who had received mechanical ventilation for more than 3 days were included in the study ‐ Mean age: 61 years ‐ Male: 23; Female: 13 ‐ Mean mechanical ventilation time: ± 288h (± 12 days) ‐ Mean APACHE II score (wean): 35 ‐ There was no significant difference between comparison groups at baseline |
|
| Interventions | 1‐ T‐tube (additional 1 hour period of T‐piece trial) (n= 22) 2‐ Pressure support ventilation of ±7.6 cm H2O for 30 minutes (n=20) |
|
| Outcomes | 1‐ Success of extubation 2‐ Reintubation 3‐ Tidal volume (VT) 4‐ Respiratory rate (RR) 5‐ Minute ventilation (VE) 6‐ Rapid shallow breathing index (RSBI and RR/VT) 7‐ Work of breathing (WOB) 8‐ P 0.1 9‐ Pressure‐time product (PTP) |
|
| Notes | 42 weaning trials in 36 patients were randomly assigned in additional 1‐hour period of T‐piece trial group and immediate extubation at PSmin level group Data collection was performed at 30min after reaching PSmin, and the end of the 1‐hour period of T‐piece trial The PSmin was calculated from the following formula: PSmin= peak inspiratory flow rate(PIFR) x total ventilatory system resistance The oesophageal catheter with a balloon at the distal end was positioned in the oesophagus. They used the CP 100 pulmonary monitor, Bicore Weaning success was defined as spontaneous breathing for more than 48h after extubation The P 0.1 and VE were excluded for analysis in the review |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | We had used list of random numbers on printed paper (data reported by author) |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered (data reported by author) |
| Selective reporting (reporting bias) | Low risk | Outcomes were clinically relevant. There was neither explicit nor implicit preference from authors to one or another method that could force them to elect specific outcomes |
| Other bias | Unclear risk | They measured 42 weaning trials in 36 patients randomly assigned in additional 1‐hour period of T‐piece trial group and immediate extubation at PSmin level group (cross‐over occurred in six patients) |
| Free of detection bias ? | High risk | The outcome assessors were not blinded |
| Free of attrition bias? | Low risk | The authors described the flow of patients, and reported the reasons for 18 patients (18%) being excluded from study after entry into protocol |
Koksal 2004.
| Methods | Randomized controlled trial Setting: Istambul University Cerrahpasa Medical Faculty, Istambul, Turkey Sample size: not estimated by the authors |
|
| Participants | ‐ 60 patients mechanically ventilated for more than 48 hours ‐ Patients with endocrine or immune system disease, patients with malignant disorders, patients who were on sympathomimetic agents or steroids were excluded from the study ‐ Mean age: 74 years ‐ Male: 28; Female: 32 ‐ Mechanical ventilation time: not reported ‐ Mean APACHE II score: 18.5 ‐ There were no differences between the groups in age, weight, gender and APACHE II |
|
| Interventions | 1‐ T‐piece (4L/min) (n=20) 2‐ Pressure support ventilation 10 cmH2O and PEEP of 5 cmH2O (n=20) 3‐ CPAP of 5 cmH2O (n=20) |
|
| Outcomes | 1‐ Successful extubation 2‐ Reintubation 3‐ Plasma insulin 4‐ Plasma cortisol 5‐ Blood glucose 6‐ Urine VMA |
|
| Notes | The durations of interventions (TT, PSV and CPAP) were 2 hours The intervention 3 was not considered for analysis in this review Weaning was considered unsuccessful if reintubation was required within 48 hours and these patients were excluded from the analysis for the laboratory variables (outcomes 3 to 6) We excluded the outcomes 3 to 6 from the review |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomization was achieved by pulling slips of paper labelled I, II, III from a bag (20 pieces per group) (data reported by first author) |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Low risk | Two outcomes were clinically relevant (extubation success and reintubation) and there was neither explicit nor implicit preference from authors to one or another method that could force then to elect specific outcomes |
| Other bias | Low risk | None suspected |
| Free of detection bias ? | Low risk | Two persons who collected and analysed the data for the study did not know which group the patient belonged to (double blind) ( data reported by author) |
| Free of attrition bias? | Low risk | There was no withdrawal of data considered for this review (successful extubation and reintubation) |
Matić 2004.
| Methods | Randomized controlled trial Setting: medical‐surgical intensive care unit (ICU) at Dr Josip Benčević Hospital in Slavonski Brod, Croatia Sample size: 60 patients would be necessary to detect 10% difference between PSV and T‐tube (power of 80%) and a weaning rate of 30% for PSV |
|
| Participants | ‐ 260 eligible adult patients with orotracheal tube requiring MV for more than 48 hours (simple and difficult weaning) ‐ Age range: 26.1 ‐ 64.2 years ‐ Male: 170; Female: 90 ‐ Mechanical ventilation time: median of 6.75 days ‐ APACHE II median: 25(19‐28.25) ‐ There was no significant difference between comparison groups at baseline |
|
| Interventions | 1‐ T‐tube (n=110) 2 ‐ Pressure support ventilation of 8 cmH20 and PEEP ≤ 5cmH20 (n=150) |
|
| Outcomes | 1‐Time to weaning from MV 2‐ ICU mortality 3‐ Successful extubation 4‐ Reintubation 5‐ Failure of extubation 6‐ Lenght of ICU stay 7‐Total time of MV 8‐ Life‐threatening complications during procedure 9‐ Successful spontaneous breathing trial (first moment of study) |
|
| Notes | T‐Tube and PSV: The extubation was performed after the 2‐hour trial of spontaneous breathing went well Patient with difficult initial weaning was defined as patients with any signs of poor procedure tolerance were observed during the 2‐h trial, the same procedure of weaning was repeated after 24h, or when the patients clinical condition permitted it. These patients were followed until ICU discharge or death Successful weaning was considered if reintubation was not required within 48h of extubation The outcomes 1, 6 and 7 were reported as medians in 'Additional tables' |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Low risk | The patients were allocated to the two groups in a blinded fashion by using closed‐envelope technique |
| Selective reporting (reporting bias) | Low risk | Outcomes were correctly selected to evaluate the effectiveness and safety of both weaning strategies |
| Other bias | Low risk | None suspected |
| Free of detection bias ? | Unclear risk | It is not clear if outcome assessors were distinct from study researchers or blinded to the assignments |
| Free of attrition bias? | Low risk | The authors made available the flow of patients and there was no withdrawal reported by the authors |
Matić 2007.
| Methods | Randomized controlled trial Setting: Multidisciplinary intensive care unit (ICU) at Dr Josip Benčević General Hospital in Slavonski Brod between April 2004 and April 2006 Sample size: 136 patients to have 70% power to detecting difference in proportion of patients experiencing 2‐hour failure (significance level, 5%) |
|
| Participants | ‐ 136 patients with COPD requiring MV longer than 24 hours were included in the trial ‐ Age range: 32‐71 years (median= 58) ‐ Mechanical ventilation time: median 5 days (3.6‐6.3) ‐ APACHE II score range 23‐34 (median 30) ‐ The two groups of patients did not significantly differ in age, sex distribution, APACHE II score, median ventilation time before spontaneous breathing trial |
|
| Interventions | 1‐ T‐tube circuit (n=66) 2 ‐ Pressure support ventilation of 5 cmH20 (n=70) |
|
| Outcomes | 1‐ Duration of weaning 2‐ Total MV duration 3‐ Time spent in ICU 4‐ ICU mortality rate 5‐ Successful extubation 6‐ Weaning failure 7‐ Reintubation 8‐ Successful spontaneous breathing trial |
|
| Notes | If one or more signs of poor procedure tolerance were observed during the 2‐hour trial, the patient was considered difficult‐to‐wean and returned to the MV The clinical characteristics of patients who failed 2h of SBTs were reported The 2h spontaneous breathing trial was performed with either T‐tube or PSV For patients who were weaned by means of PSV, initial positive pressure support was 18 cmH20. This support was then lowered by 2‐4 cm H20 and patients were extubated at pressure support of 5 cm H2O The outcomes 1 to 7 were assessed for patients with 2h trial failure (difficult‐to‐wean) The outcomes 1, 2 and 3 were reported as medians in 'Additional tables' Weaning failure was considered when the patient needed continuing MV support for > 7 days after weaning assessment or when death occurred before the ICU discharge |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The patients were randomly assigned to one of the two methods by drawing envelopes; a third party not involved in the study was asked to choose one of the envelopes |
| Allocation concealment (selection bias) | Low risk | They used two closed, non‐transparent, identical looking envelopes |
| Selective reporting (reporting bias) | Low risk | Although the outcomes were not reported in the protocol published in current controlled trials, they evaluated clinically relevant outcomes |
| Other bias | Low risk | None suspected |
| Free of detection bias ? | High risk | The authors had described that the study was simple blinded in protocol published in current controlled trials, showing that data assessors were aware of allocation groups |
| Free of attrition bias? | Low risk | The patients flow was clear and there was no reported dropout |
Vitacca 2001.
| Methods | Multicentre RCT Setting: The long‐term weaning units (LWUs) of the three hospitals: Gussago, Padova, and Casatenovo, Italy |
|
| Participants | 52 tracheostomized patients with COPD mechanically ventilated for at least 15 days that T‐piece trial failure (difficult‐to‐wean) ‐ Mean age: 72.5 years ‐ Gender of participants: did not report ‐ Mechanical ventilation time: > 15 days (range 15‐ 39) ‐ Mean APACHE II: 17 |
|
| Interventions | 1‐ T‐tube with supplemental oxygen for 8 h (n=26) 2‐ PSV of 8 cmH2O for 8 h (n=26) |
|
| Outcomes | 1‐ Weaning success rate 2‐ Time of weaning 3‐ LWU and hospital length of stay 4‐ Total MV duration 5‐ Failure of weaning 6‐ Mortality 7‐ Complications: pneumonia, arrhythmias and agitation |
|
| Notes | PSV group: the pressure support was decreased by 2 cmH2O twice a day until 8 cmH2O for 8 hours T‐tube: patients were disconnected from the ventilator and tried to breathe spontaneously twice a day, with duration from 30 min to 8h (30, 60 min, 2, 4, 8 h) Weaning success rate was considered when the patients able to tolerate at least a further 48 consecutive hours of spontaneous breathing through T‐tube Weaning failure (5) was considered when the patient died or who still needed MV after at least 30 consecutive days of weaning protocol |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The patients were randomly assigned to either the PSV or T‐Tube using a random list generated by a computer with a central allocation with 3 different blocks of 20 subjects (data reported by first author) |
| Allocation concealment (selection bias) | Low risk | The final random list was sealed envelopes (data reported by first author) |
| Selective reporting (reporting bias) | Low risk | Clinically relevant outcomes |
| Other bias | Low risk | None suspected |
| Free of detection bias ? | High risk | The outcome assessors were not blinded |
| Free of attrition bias? | Low risk | The patient flow was clear and failure was considered when the patient died or MV for more 30 days |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Cabello 2010 | Cross‐over randomized controlled trials and the initial results (before cross‐over) were not available for following outcomes RR, VT and RSBI |
| Colombo 2007 | Quasi‐randomized study compared PSV versus T‐tube as spontaneous breathing trials |
| Costa 2005 | Cross‐over randomized controlled trial and the initial results (before cross‐over) were not available for following outcomes RR and VT |
| Emmerich 1997 | Quasi‐randomized study compared T‐tube versus PSV versus SIMV as spontaneous breathing trials |
| Esteban 1999 | Randomized controlled trial testing for trial of spontaneous breathing with T‐tube circuit for up to 30 min versus up to 120 min Suitable for other review |
| Figueiredo 2001 | Participants did not meet criteria RCT compared PSV versus T‐tube as spontaneous breathing trial in postoperative adult patients following cardiac surgery with less than 12 hours of mechanical ventilation |
| Goldwasser 1998 | RCT compared PSV versus T‐tube as spontaneous breathing trials in COPD patients. The patients in this study were included in Esteban 1997 study |
| Guntzel 2007 | Cross‐over randomized controlled trial and the initial results (before cross‐over) were not available for following outcomes RR, VT and RSBI |
| Kuhlen 2003 | Cross‐over randomized controlled trial evaluated outcomes out of interest for this review (WOB) and the initial results (before cross‐over) were not available for following outcomes: VT and RSBI |
| Niembro 1996 | Quasi‐randomized study compared T‐tube versus PSV as spontaneous breathing trials |
| Patel 1996 | Cross‐over randomized controlled trial evaluated outcomes out of interest for this review (WOB) and the initial results (before cross‐over) were not available for following outcomes: RR, VT and RSBI |
| Perren 2002 | Randomized controlled trial testing PSV with 7 cmH20 target durations of 30 min versus up to 120 min Suitable for other review |
| Rieder 2004 | Cross‐over randomized controlled trial, the initial results (before cross‐over) were not available for following outcomes: RR, VT and RSBI |
| Santos 2008 | Cross‐over randomized controlled trial evaluated outcomes out of interest for this review (energy expenditure) and the initial results (before cross‐over) were not available for following outcomes: RR, VT and RSBI |
| Sassoon 1991 | Cross‐over randomized controlled trial evaluated outcomes not of interest for this review (WOB and PTP) and the initial results (before cross‐over) were not available for following outcomes: RR, VT and RSBI |
| Schifelbain 2011 | Cross‐over randomized con trolled trial evaluated cardiorespiratory changes (using doppler echocardiogram and electrocardiogram (ECG) in critical patients during PSV versus T‐tube spontaneous breathing trials The outcomes not of interest for this review |
Characteristics of studies awaiting assessment [ordered by study ID]
Jubran 2013.
| Methods | Randomized trial. |
| Participants | 316 patients with tracheotomy (prolonged weaning) |
| Interventions | Pressure support ventilation versus tracheostomy collar |
| Outcomes | Weaning duration, length of hospital stay, deaths during study, hospital at 6 and 12 months |
| Notes | The data were taken from original article. |
Zhang 2009.
| Methods | Clinical trial |
| Participants | 208 patients with oral intubation |
| Interventions | Pressure support ventilation versus T‐piece spontaneous breathing trials |
| Outcomes | Threshold value of rapid‐shallow‐breathing index(RSBI). Weaning successful? |
| Notes | The data were taken from English abstract |
Characteristics of ongoing studies [ordered by study ID]
Agarwal 2008.
| Trial name or title | Pressure support reduction versus spontaneous breathing trials in weaning from ventilation |
| Methods | RCT |
| Participants | Adult patients ventilated for more than 24 hours |
| Interventions | Pressure support ventilation versus spontaneous breathing trials |
| Outcomes | Primary: rate of weaning failure 48 hours from extubation. Secondary: PAV, reintubation, mortality |
| Starting date | April 2008 |
| Contact information | ashutosh@indiachest.org, riteshpgi@gmail.com |
| Notes |
Pellegrini 2011.
| Trial name or title | Comparison between spontaneous breathing trials through pressure support ventilation or "T" tube in the weaning of mechanical ventilation in patients with chronic obstructive pulmonary disease: A randomized Controlled Trial |
| Methods | RCT |
| Participants | COPD patients submitted to mechanical ventilation for at least 48 hours |
| Interventions | T‐tube versus pressure support spontaneous breathing trials |
| Outcomes | Primary: days spent on mechanical ventilation. Secondary: duration of ICU stay, mortality, extubation success |
| Starting date | January 2012 |
| Contact information | gutopell@yahoo.com.br |
| Notes |
Differences between protocol and review
The following differences will be found between the protocol (Ladeira 2006) and the review.
Objectives
We modified the objectives. We aimed to evaluate the effectiveness and safety of pressure support ventilation (PSV) compared to T‐tube, on weaning of adult patients from mechanical ventilation, on weaning success and other clinically important outcomes.
Participants
We also included tracheostomized patients in the systematic review, after discussion with Harald Herkner.
Outcomes
We modified the original primary outcome. We consider weaning success as the primary outcome. The weaning success outcome is more suitable to evaluate the effectiveness of PSV and T‐tube as spontaneous breathing trials for weaning from mechanical ventilation. Pressure support ventilation and T‐tube were used as spontaneous breathing trials in 1022 patients (84.6% of the sample). In 186 (15.4%) patients, both interventions were used along with a gradual weaning from mechanical ventilation.
The outcome successful extubation does not apply to tracheostomized patients, this outcome was changed to weaning success. Successful extubation and weaning success was defined as absence of requirement of ventilatory support within 48 hours after extubation (translaryngeal tube) or withdrawal of mechanical ventilation (tracheostomy tube), in all the included studies.
We added the outcome successful spontaneous breathing trial during the review process. The spontaneous breathing trial (SBT) predicts weaning success or successful extubation.
We excluded two physiologic parameters in this review: oxygenation index (PaO2/ FiO2) and maximum spontaneous inspiratory effort (MIP). They are not relevant to the evaluation of the effectiveness and safety of SBTs.
Search strategies
We modified the search strategies in January 2009. The searches were rerun across the databases by the Cochrane Anaesthesia Review Group.
We added two databases, SCIELO and CAPES (bank of thesis), in electronic searches.
Risk of bias
The approach to evaluate the risk of bias of studies included in this systematic review was modified according to the updated Handbook (Higgins 2011).
Unit of analysis issues
We added analysis for cross‐over trials in the unit of analysis issues, this analysis was not planned in the protocol.
Subgroup analysis
We excluded from subgroup analysis the positive end expiratory pressure (PEEP) levels used during weaning from mechanical ventilation. This subgroup analysis is not relevant to the weaning process and was likely due to an error during the protocol process, which included the intention to evaluate pressure support levels used during weaning rather than PEEP levels.
We included two subgroup analyses that were not planned in the protocol. When the analysis of clinical heterogeneity was performed, we observed that the studies had patients classified in three different categories of weaning: simple weaning, difficult weaning and prolonged weaning. This classification of studies, based on the three categories, was possible for three relevant outcomes (weaning success, reintubation and ICU mortality).
With the inclusion of tracheostomized patients, we added the subgroup analysis for the type of endotracheal prosthesis (tracheostomy versus translaryngeal tube).
Contributions of authors
Conceiving the review: Magdaline Ladeira (ML)
Co‐ordinating the review: ML
Undertaking manual searches: ML
Screening search results: ML, Brenda Gomes (BG)
Organizing retrieval of papers: ML, BG and Flávia Vital (FV)
Screening retrieved papers against inclusion criteria: ML, BG
Appraising quality of papers: ML and RA
Abstracting data from papers: ML and Régis Andiolo (RA)
Writing to authors of papers for additional information: ML and Stella Pecin (SP)
Providing additional data about papers: ML and FV
Obtaining and screening data on unpublished studies: ML and FV
Data management for the review: ML
Entering data into Review Manager (RevMan 5.1): ML
RevMan statistical data: ML and RA
Other statistical analysis not using RevMan: RA
Double entry of data: (data entered by person one: ML; data entered by person two: RA)
Interpretation of data: ML, BS and Álvaro N Atallah (AA)
Statistical analysis: ML and FV
Writing the review: ML, RA and AA
Securing funding for the review: ML
Guarantor for the review (one author): ML
Persons responsible for reading and checking review before submission: ML, FV, RA, BG, AA and SP
Sources of support
Internal sources
Department of Internal and Therapeutic Medicine, Universidade Federal de São Paulo, Brazil.
Brazilian Cochrane Centre, Brazil.
External sources
No sources of support supplied
Declarations of interest
None known
Edited (no change to conclusions)
References
References to studies included in this review
Brochard 1994 {published data only}
- Brochard L, Rauss A, Benito S, Conti G, Mancebo J, Rekik N, et al. Comparison of three methods of gradual withdrawal from ventilatory support during weaning from mechanical ventilation. American Journal of Respiratory and Critical Care Medicine 1994;150:896‐903. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Esteban 1995 {published data only}
- Esteban A, Frutos F, Tobin MJ, Alía I, Solsona JF, Valverdú I, et al. A comparison of four methods of weaning patients from mechanical ventilation. New England Journal of Medicine 1995;332(6):345‐50. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Esteban 1997 {published data only}
- Esteban A, Alia I, Gordo F, Fernandez R, Solsona JF, Vallverdu I, et al. Extubation outcome after spontaneous breathing trials with t‐tube or pressure support ventilation. American Journal of Respiratory and Critical Care Medicine 1999;159:512‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Haberthur 2002 {published data only}
- Haberthür C, Mols G, Elsasser S, Bingisser R, Stocker R, Guttmann J. Extubation after breathing trials with automatic tube compensation, T‐tube, or pressure support ventilation. Acta Anaesthesiologica Scandinavica 2002;46(8):973‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Koh 2000 {published data only}
- Koh Y, Hong SB, Lim CM, Lee SD, Kim WS, Kim DS, Kim WD. Effect of an additional 1‐hour T‐piece trial on weaning outcome at minimal pressure support. Journal of Critical Care 2000;15(2):41‐5. [PUBMED: 10877363] [DOI] [PubMed] [Google Scholar]
Koksal 2004 {published data only}
- Koksal GM, Sayilgan C, Sen O, Oz H. The effects of different weaning modes on the endocrine stress response. Critical Care 2004;8(1):31‐4. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Matić 2004 {published data only}
- Matić I, Majerić‐Kogler V. Comparison of pressure support and t‐tube weaning from mechanical ventilation: Randomized prospective study. Croatian Medical Journal 2004;45(2):162‐6. [MEDLINE: ] [PubMed] [Google Scholar]
Matić 2007 {published data only}
- Matić I, Davorin D, Majerić‐Kogler V, Jurjević M, Mirković I, Vucinić NM. Chronic obstructive pulmonary disease and weaning of difficult‐to‐wean patients from mechanical ventilation: Randomized prospective study. Croatian Medical Journal 2007;48(1):51‐8. [PUBMED: 17309139] [PMC free article] [PubMed] [Google Scholar]
Vitacca 2001 {published data only}
- Vitacca M, Vianello A, Colombo D, Clini E, Porta R, Bianchi L, et al. Comparison of two methods for weaning patients with chronic obstructive pulmonary disease requiring mechanical ventilation for more than 15 days. American Journal of Respiratory and Critical Care Medicine 2001;164(2):225‐30. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Cabello 2010 {published data only}
- Cabello B, Thille A, Roche‐Campo F, Brochard L, Gómez F, Mancebo J. Physiological comparison of three spontaneous breathing trials in difficult‐to‐wean patients. Intensive Care Medicine 2010;36:1171‐9. [DOI: ] [DOI] [PubMed] [Google Scholar]
Colombo 2007 {published data only}
- Colombo T, Boldrini AF, Juliano S, Juliano M, Houly J, Gebara O, et al. Implementation, assessment and comparison of the T‐tube and pressure‐ support weaning protocols applied to the intensive care unit patients who had received mechanical ventilation for more than 48 hours [Implementação, avaliação e comparação dos protocolos de desmame com tubo‐T e pressão suporte associada à pressão expiratória final positiva em pacientes submetidos à ventilação mecânica por mais de 48 horas em unidade de terapia intensiva]. Revista Brasileira de Terapia Intensiva 2007;19(1):31‐7. [PubMed] [Google Scholar]
Costa 2005 {published data only}
- Costa A, Rieder M, Vieira S. Weaning from mechanical ventilation by using pressure support or T‐tube ventilation. Comparison between patients with and without heart disease. [Desmame da ventilação mecânica utilizando pressão de suporte ou tubo T. Comparação entre pacientes cardiopatas e não cardiopatas]. Arquivos Brasileiros de Cardiologia 2005;85(1):On Line. [DOI: 10.1590/S0066-782X2005001400007] [DOI] [PubMed] [Google Scholar]
Emmerich 1997 {published data only}
- Emmerich J, Vicêncio S, Siqueira H, Simäo A, Bernhoeft C, Souza W. A comparison among three methods of weaning ventilatory support: T‐piece versus S‐IMV versus PSV [Estudo comparativo entre três modalidades de desmame do suporte ventilatório: tradicional (tubo em "T") versus S‐IML versus PSV]. Revista Brasileira de Terapia Intensiva 1997;9(4):167‐74. [Google Scholar]
Esteban 1999 {published data only}
- Esteban A, Alía I, Tobin MJ, Gil A, Gordo F, Vallverdú I, et al. Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Spanish Lung Failure Collaborative Group. American Journal of Respiratory and Critical Care Medicine 1999;159(2):512‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Figueiredo 2001 {unpublished data only}
- Figueiredo LC. Comparison of two weaning methods in uncomplicated coronary artery bypass grafting post‐operative patients [Comparação entre dois métodos de retirada do suporte ventilatório em pacientes no pós‐operatório de cirurgia cardíaca (MD Thesis)]. Biblioteca Central da Unicamp 2001.
Goldwasser 1998 {published and unpublished data}
- Goldwasser R. Study on the effectiveness of two different tolerance tests on weaning from mechanical ventilation, for predicting the success of extubation in patients with chronic obstructive pulmonary disease [Estudo da eficácia de dois diferentes testes de tolerância de interrupção da ventilação mecânica para predizer o êxito da extubação em pacientes portadores de Doença Pumonar Obstrutiva Crônica]. Universidade Federal do Rio de Janeiro. Rio de Janeiro, 1998:88p.
Guntzel 2007 {published data only}
- Gűntzel A, Moraes R, Chiappa Z, Ferlin E, Vieira S. The effect of T‐tube and Pressure Support on Cardiorespiratory Variables and Heart Rate Variability during Weaning from Mechanical Ventilation [O efeito do tuboT e da pressão de suporte sobre variáveis cardiorespiratórias e variabilidade da frequência cardíaca durante o desmame da ventilação mecânica]. The effect of T‐tube and pressure support on cardiorespiratory variables and heart rate variability during weaning from mechanical ventilation (thesis). Porto Alegre: Porto Alegre University, 2007:1‐84. [Google Scholar]
Kuhlen 2003 {published data only}
- Kuhlen R, Max M, Dembinski R, Terbeck S, Jürgens E, Rossaint R. Breathing pattern and workload during automatic tube compensation, pressure support and T‐piece trials in weaning patients [2003]. European Journal Anaesthesiology 2003;20(1):10‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Niembro 1996 {published data only}
- Niembro R, Liendo A, Fisher R, Lopez J, Granillo J, Gonzáles J, et al. Comparison of T piece vs pressure support ventilation during weaning from mechanical ventilation [Pieza T vs ventilación con presión de soporte como método de retiro de la asistencia mecánica ventilatoria]. Revista de la Associación Mexicana de Medicina Critica y Terapia Intensiva 1996;10(6):254‐8. [LILACS ID: 187834] [Google Scholar]
Patel 1996 {published data only}
- Patel R, Petrini M, Norman J. Work of breathing and pressure‐time product on pressure support ventilation, continuous positive airway pressure, and T‐piece. Respiratory Care 1996;41(11):1013‐9. [Google Scholar]
Perren 2002 {published data only}
- Perren A, Domenighetti G, Mauri S, Genini F, Vizzardi N. Protocol‐directed weaning from mechanical ventilation: clinical outcome in patients randomized for a 30‐min or 120‐min trial with pressure support ventilation. Intensive Care Medicine 2002;28(8):1058‐63. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Rieder 2004 {published data only}
- Rieder M, Costa A, Vieira S. Positive expiratory pressure as a method for mechanical ventilation weaning: a comparison between the pressure support and T‐tube methods [O uso da pressão expiratória positiva final durante o desmame da ventilação mecânica: uma comparação com os métodos de pressão de suporte e Tubo T]. CAPES thesis data 2004.
Santos 2008 {published data only}
- Santos L, Hoff F, Kaufmann M, Condessa R, Vieira S. Energy expenditure in weaning from mechanical ventilation [Avaliação do gasto energético durante o desmame da ventilação mecânica os modos pressão suporte e Tubo T]. Universidade Federal do Rio Grande do Sul. Porto Alegre, 2008:89p.
Sassoon 1991 {published data only}
- Sassoon C, Light R, Lodia R, Sieck G, Mahutte K. Pressure‐time product during continuous positive airway pressure, pressure support ventilation, and T‐piece during weaning from mechanical ventilation. American Review of Respiratory Disease 1991;143:469‐75. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Schifelbain 2011 {published data only}
- Schifelbain LM, Vieira SR, Brauner JS, Pacheco DM, Naujorks AA. Echocardiographic evaluation during weaning from mechanical ventilation [Alterações cardio‐respiratórias em pacientes em desmame da ventilação mecânica: avaliação por ecocardiograma]. Clinics 2011;66(1):107‐11. [LILACS ID: 578605; PUBMED: 21437445] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
Jubran 2013 {published data only}
- Jubran A, Grant BJ, Duffner LA, Collins EG, Lanuza DM, Hoffman LA, Tobin MJ. Effect of pressure support vs unassisted breathing through a tracheostomy collar on weaning duration in patients requiring prolonged mechanical ventilation: a randomized trial. JAMA 2013;309(7):671‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zhang 2009 {published data only}
- Zhang B, Qin YZ. A clinical study of rapid‐shallow‐breathing index in spontaneous breathing trial with pressure support ventilation and T‐piece. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2009;21(7):397‐401. [JAMA: 2013.159.] [PubMed] [Google Scholar]
References to ongoing studies
Agarwal 2008 {published data only}
- Aggarwal A. Pressure support reduction versus spontaneous breathing trials in weaning from ventilation. www.controlled‐trials.com/mrct.
Pellegrini 2011 {published data only}
- Pellegrini J. Comparison between spontaneous breathing trials through pressure‐support ventilation or "T" tube in the weaning of mechanical ventilation in patients with chronic obstructive pulmonary disease: a randomized controlled trial. www.controlled‐trials.com 2011.
Additional references
Alia 2000
- Alia I, Esteban A. Weaning from mechanical ventilation. Critical Care 2000;4:72‐80. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Baeza 1975
- Baeza OR, Wagner RB, Lowery BD. Pulmonary hyperinflation. A form of barotrauma during mechanical ventilation. The Journal of Thoracic and Cardiovascular Surgery 1975;70(5):790‐805. [MEDLINE: ] [PubMed] [Google Scholar]
Blackwood 2010
- Blackwood B, Alderdice F, Burns K, Cardwell C, Lavery G, O'Halloran P. Protocolized versus non‐protocolized weaning for reducing the duration of mechanical ventilation in critically ill adult patients. Cochrane Database of Systematic Reviews 2010, Issue 5. [DOI: 10.1002/14651858.CD006904.pub2] [DOI] [PubMed] [Google Scholar]
Boles 2007
- Boles J, Bion J, Connors A, Herridge M, Marsh B, et al. Weaning from mechanical ventilation. European Respiratory Journal 2007;29:1033‐56. [DOI] [PubMed] [Google Scholar]
Butler 1999
- Butler R, Keenan SP, Inman KJ, Sibbald WJ, Block G. Is there a preferred technique for weaning the difficult‐to‐wean patient: a systematic review of the literature. Critical Care Medicine 1999;27(11):2331‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Caroleo 2007
- Caroleo S, Agnello F, Abdallah K, Santangelo E, Amantea B. Weaning from mechanical ventilation: an open issue. Minerva Anestesiologica 2007;73(7‐8):417‐27. [PUBMED: 17637588] [PubMed] [Google Scholar]
Combes 2003
- Combes A, Figliolini C, Trouillet JL, Kassis N, Dombret MC, Wolff M, et al. Factors predicting ventilator‐associated pneumonia recurrence. Critical Care Medicine 2003;31:1102‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Cook 2000
- Cook D, Meade M, Guyatt G, Griffith G, Booker L. Criteria for weaning from mechanical ventilation. Agency for Healthcare Research and Quality 2000;371(23):1‐4. [MEDLINE: ] [PMC free article] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey‐Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphic test. BMJ 1997;315:629‐34. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Eggimann 2001
- Eggimann P, Pittet D. Infection control in the ICU. Chest 2001;120(6):2059‐93. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ely 1996
- Ely EW, Baker AM, Dunagan DP, Burke HL, Smith AC, Kelly PT, et al. Effect of the duration of mechanical ventilation on identifying patients capable of breathing spontaneously. New England Journal of Medicine 1996;335:1864‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Epstein 1997
- Epstein SK, Ciubotaru RL, Wong JB. Effect of failed extubation on the outcome of mechanical ventilation. Chest 1997;112(1):186‐92. [PUBMED: 9228375] [DOI] [PubMed] [Google Scholar]
Epstein 2000
- Epstein SK. Weaning parameters. Respiratory Care Clinics of North America 2000;6:253‐301. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Epstein 2001
- Epstein SK. Controversies in weaning from mechanical ventilation. Journal of Intensive Care Medicine 2001;16:270‐86. [Google Scholar]
Esen 1992
- Esen F, Denkel T, Telci L, Kesecioglu J, Tutuncu AS, et al. Comparison of pressure support ventilation and intermittent mandatory ventilation during weaning in patients with acute respiratory failure. Advances in Experimental Medicine and Biology 1992;317:371‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Esteban 1994
- Esteban A, Alía I, Ibañez J, Benito S, Tobin M. Modes of Mechanical Ventilation and Weaning. Chest 1994;106:1188‐93. [DOI: ; CHEST 106.4.1188] [DOI] [PubMed] [Google Scholar]
Esteban 2002
- Esteban A, Anzueto A, Frutos F, AlÍa I, Brochard L, Stewart TE, et al. Mechanical Ventilation International Study Group. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28‐day international study. JAMA 2002;287(3):345‐55. [PUBMED: 11790214] [DOI] [PubMed] [Google Scholar]
Esteban 2008
- Esteban A, Ferguson N, Meade M, Frutos‐Vivar F, Apezteguia C, et al. Evolution of mechanical ventilation in response to clinical research. American Journal of Respiratory and Critical Care Medicine 2008;177:170‐7. [DOI] [PubMed] [Google Scholar]
Ezingeard 2006
- Ezingeard E, Diconne E, Guyomarcêh S, Venet C, Page D, Gery P, et al. Weaning from mechanical ventilation with pressure support in patients failing a T‐tube trial of spontaneous breathing. Intensive Care Medicine 2006;32(1):165‐9. [PUBMED: 16283162] [DOI] [PubMed] [Google Scholar]
Fagon 1996
- Fagon JY, Chastre J, Vuagnat A, Trouillet JL, Novara A, Gibert C. Nosocomial pneumonia and mortality among patients in intensive care units. JAMA 1996;275(11):866‐9. [MEDLINE: ] [PubMed] [Google Scholar]
Fleiss 1986
- Fleiss JL. Analysis of data from multiclinic trials. Controlled Clinical Trials 1986;7(4):267‐75. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Funk 2010
- Funk GC, Anders S, Breyer MK, Burghuber OC, Edelmann G, Heindl W, et al. Incidence and outcome of weaning from mechanical ventilation according to new categories. European Respiratory Journal 2010;35(1):88‐94. [PUBMED: 19541716] [DOI] [PubMed] [Google Scholar]
Garnacho‐Montero2005
- Garnacho‐Montero J, Amaya‐Villar R, García‐Garmendia JL, Madrazo‐Osuna J, Ortiz‐Leyba C. Effect of critical illness polyneuropathy on the withdrawal from mechanical ventilation and the length of stay in septic patients. Critical Care Medicine 2005;33(2):349‐54. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Girard 2008
- Girard TD, Kress JP, Fuchs BD, Thomason JW, Schweickert WD, Pun BT, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet 2008;371(9607):126‐34. [DOI: 10.1016/S0140-6736(08)60105-1; PUBMED: 18191684] [DOI] [PubMed] [Google Scholar]
Gonçalves 2012
- Gonçalves E, Silva E, Basile A, Auxiliadora M, Nicolini E, Gastaldi A. Low pressure support changes the rapid shallow breathing index (RSBI) in critically ill patients on mechanical ventilation. Revista Brasileira de Fisioterapia 2012; Vol. 16, issue 5:368‐74. [DOI: 10.1590/S1413-35552012005000037] [DOI] [PubMed]
Higgins 2002
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21:1539‐58. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Cochrane Database of Systematic Reviews 2011.
Hozo 2005
- Hozo S, Djulbegovic B, HozoI I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Medical Research Methodology 2005;5:13. [DOI: 10.1186/1471-2288-5-13] [DOI] [PMC free article] [PubMed] [Google Scholar]
Knaus 1985
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Critical Care Medicine 1985;13(10):818‐29. [PUBMED: 3928249] [PubMed] [Google Scholar]
Kollef 1997
- Kollef MH, Shapiro SD, Silver P, John RE, Prentice D, Sauer S, et al. A randomized, controlled trial of protocol‐directed versus physician‐directed weaning from mechanical ventilation. Critical Care Medicine 1997;25:567‐74. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Le Bourdelles 1994
- Bourdelles G, Viires N, Boczkowski J, Seta N, Pavlovic D, Aubier M. Effects of mechanical ventilation on diaphragmatic contractile properties in rats. American Journal of Respiratory and Critical Care Medicine 1994;49:1539‐44. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Le Gall 1993
- Gall JR. A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA 1993;270:2957‐63. [DOI] [PubMed] [Google Scholar]
Levine 2008
- Levine S, Nguyen T, Taylor N, Friscia ME, Budak MT, Rothenberg P, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. New England Journal of Medicine 2008;27(13):1327‐35. [PUBMED: PMID: 18367735] [DOI] [PubMed] [Google Scholar]
Luetz 2012
- Luetz A, Goldmann A, Weber‐Carstens S, Spies C. Weaning from mechanical ventilation and sedation. Current Opinion Anaesthesiology 2012;25(2):164‐9. [DOI] [PubMed] [Google Scholar]
MacIntyre 2001
- MacIntyre NR, Cook DJ, Ely EW Jr, Epstein SK, Fink JB, Heffner JE, et al. Evidence‐based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest 2001;120(6 Suppl):375S‐95S. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
MacIntyre 2012
- MacIntyre NR. Evidence‐based assessments in the ventilator discontinuation process. Respiratory Care 2012;57(10):1611‐8. [PUBMED: 23013898] [DOI] [PubMed] [Google Scholar]
Marelich 2000
- Marelich GP, Murin S, Battistella F, Inciardi J, Vierra T, Roby M. Protocol weaning of mechanical ventilation in medical and surgical patients by respiratory care practitioners and nurses. Effect on weaning time and incidence of ventilator associated pneumonia. Chest 2000;118:459‐65. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marini 1998
- Marini JJ, Slutsky AS. Physiological basis of ventilatory support. Vol. 118, New York: Marcel Dekker Inc, 1998. [Google Scholar]
Meade 2001
- Meade M, Guyatt G, Sinuff T, Griffith L, Hand L, Toprani G, et al. Trials comparing alternative weaning modes and discontinuation assessments. Chest 2001;120:425S‐37S. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Michelson 1991
- Michelson A, Kamp HD, Schuster B. Sinusitis in long‐term intubated, intensive care patients: nasal versus oral intubation. Der Anaesthesist 1991;40(2):100‐4. [MEDLINE: ] [PubMed] [Google Scholar]
Morehead 2000
- Morehead RS, Pinto SJ. Ventilator‐associated pneumonia. Archives of Internal Medicine 2000;160:1926‐36. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Nathan 1993
- Nathan SD, Ishaaya AM, Koerner SK, Belman MJ. Prediction of minimal pressure support during weaning from mechanical ventilation. Chest 1993;103(4):1215‐9. [PUBMED: 8131468] [DOI] [PubMed] [Google Scholar]
Oxman 1992
- Oxman AD, Guyatt GH. A consumer's guide to subgroup analyses. Annals of Internal Medicine 1992;116:78‐84. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Patel 2009
- Patel K, Ganatra K, Bates J, Young M. Variation in the rapid shallow breathing index associated with common measurement techniques and conditions. Respiratory Care 2009;54(11):1462‐6. [PubMed] [Google Scholar]
Petersen 1983
- Petersen GW, Baier H. Incidence of pulmonary barotrauma in a medical ICU. Critical Care Medicine 1983;11(2):67‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Peňuelas 2011
- Penuelas O, Frutos‐Vivar F, Fernández C, Anzueto A, Epstein SK, Apezteguia C, et al. Characteristics and outcomes of ventilated patients according to time to liberation from mechanical ventilation. American Journal of Respiratory and Critical Care Medicine 2011;184:430‐7. [DOI: 10.1164/rccm.201011-1887OC.; MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Pingleton 1988
- Pingleton SK. Complications of acute respiratory failure. American Review of Respiratory Disease 1988;137:1463‐93. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Powers 2002
- Powers SK, Shanely RA, Coombes JS, Koesterer TJ, McKenzie M, Gammeren D, et al. Mechanical ventilation results in progressive contractile dysfunction in the diaphragm. Journal of Applied Physiology 2002;92:1851‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Rello 1991
- Rello J, Quintana E, Ausina V, Castella J, Luquin M, Net A, et al. Incidence, etiology, and outcome of nosocomial pneumonia in mechanically ventilated patients. Chest 1991;100:439‐44. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Santos 2007
- Santos L, Borges M, Figueirêdo L, Guedes C, Vian B, Kappaz K, Araújo S. Comparison among Three Methods to Measure the Rapid Shallow Breathing Index in Patients Submitted to Weaning from Mechanical Ventilation [Comparação entre Três Métodos de Obtenção do Índicede Respiração Rápida e Superficial em Pacientes Submetidos ao Desmame da Ventilação Mecânica]. Revista Brasileira de Terapia Intensiva 2007;19(3):331‐6. [PubMed] [Google Scholar]
Schuster 1984
- Schuster DP, Rowley H, Feinstein S, McGue MK, Zuckerman GR. Prospective evaluation of the risk of upper gastrointestinal bleeding after admission to a medical intensive care unit. The American Journal of Medicine 1984;76(4):623‐30. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Sellares 2011
- Sellares J, Ferrer M, Cano E, Loureiro H, Valencia M, Torres A. Predictors of prolonged weaning and survival during ventilator weaning in a respiratory ICU. Intensive Care Medicine 2011;37(5):775‐84. [PUBMED: 21373820.] [DOI] [PubMed] [Google Scholar]
Tonnelier 2011
- Tonnelier A, Tonnelier JM, Nowak E, Gut‐Gobert C, Prat G, Renault A, et al. Clinical relevance of classification according to weaning difficulty. Respiratory Care 2011;56(5):583‐90. [PUBMED: PMID: 21276313 ] [DOI] [PubMed] [Google Scholar]
van Zanten 2005
- Zanten AR, Dixon JM, Nipshagen MD, Bree R, Girbes AR, Polderman KH. Hospital‐acquired sinusitis is a common cause of fever of unknown origin in orotracheally intubated critically ill patients. Critical Care 2005;9(5):583‐90. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Yusuf 1991
- Yusuf S, Wittes J, Probstfield J, Tyroler HA. Analysis and interpretation of treatment effects in subgroups of patients in randomized clinical trials. JAMA 1991;266:93‐8. [MEDLINE: ] [PubMed] [Google Scholar]
References to other published versions of this review
Ladeira 2006
- Ladeira MT, Burns KEA, Atallah ÁN, Vital FMR, Andriolo RB, Soares B. Pressure support versus T tube for weaning from mechanical ventilation in adults. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD006056] [DOI] [PMC free article] [PubMed] [Google Scholar]