

Abstract
Objective
Participation restriction, common among people with knee osteoarthritis (OA), may be influenced by positive and negative affect. We examined the risk of incident participation restriction over 84 months conferred by positive and negative affect among people with knee OA.
Methods
Participants are from the Multicenter Osteoarthritis Study and had or were at high risk of knee OA. Participation restriction and positive and negative affect were measured with the Late Life Disability Index, Instrumental Role Limitation subscale and the positive affect and depressed mood subscales of the Center for Epidemiological Studies Depression Scale, respectively. Robust Poisson regression was used to calculate risk of incident participation restriction over 84 months conferred by combinations of low and high positive and negative affect, adjusting for covariates.
Results
Of 1810 baseline participants (mean: 62.1 years, 56% female), 470 (26%) had incident participation restriction over 84 months. Participants with low positive affect had 20% greater risk of incident participation restriction than those with high positive affect; participants with high negative affect had 50% greater risk of incident participation compared to those with low negative affect. Participants with both low positive and high negative affect had 80% greater risk of incident participation restriction compared to other combinations of positive and negative affect.
Conclusion
Low positive and high negative affect, both alone and in combination, increase risk of participation restriction among adults with knee OA. Efforts aimed at preventing participation restriction in this population should consider these mood states.
Participation restriction, operationalized in the World Health Organization’s International Classification of Health, Functioning, and Disability (ICF) model as “problems an individual may experience in involvement in life situations,”(1) affects nearly 23 million people with arthritis in the United States (2). Osteoarthritis (OA), the most prevalent type of arthritis, is the leading cause of disability in older adults (3,4) and an estimated 1 in 3 adults over age 60 in the United States have radiographic knee OA(5). Participation restriction is common among people with OA, with people reporting difficulties engaging in social and community activities, working, or managing one’s home (6,7). Little is known about the mood states that influence risk of participation restriction among people with OA.
Positive and negative affect, emotions that impact coping, may be risk factors for participation restriction. The Dynamic Model of Affect posits that stressful life events, such as chronic pain, may result in altered levels of positive and negative affect (8). Positive affect is “the extent to which a person feels a zest for life,” and includes emotions such as hope, happiness, (9) and emotional vitality (10). Negative affect is the “extent to which a person is feeling upset or unpleasantly engaged rather than peaceful,” (9) and includes an array of emotions or moods such as sadness, fear, and anxiety (11). Negative affect is a different construct from depression, which consists of persistent depressive thoughts resulting in a loss of interest and inability to function (9,11). While people with high levels of negative affect may have depressed mood, people with low negative affect exhibit calmness and low levels of distress. Indeed, most people with negative affect do not develop or meet the clinical definition of depression (9,12). Previous studies show positive and negative affect are associated with coping behaviors among people with arthritis and could be important in participation outcomes (13,14). Yet, this relationship has not been explored.
Positive affect and negative affect have been found to have independent associations with important health outcomes of older adults. In several studies, high positive affect is linked to greater social participation among adults with stroke (15) and decreased risk of disability in older adults (16,17). Conversely, higher levels of negative affect have been found to be significantly associated with functional limitation, worse pain, quality of life, and disability among older adults (18,19). Among people with OA, research has focused on the relationship of positive and negative affect with pain, but not with participation restriction. Finan et al. (2013) found that negative affect was a stronger predictor of pain over time than positive affect among people with knee OA (20). While a few short-term longitudinal studies identify associations between affect and disability among older adults, no study to date has measured the long-term risk of incident participation restriction associated with positive affect or negative affect among adults with knee OA, a common chronic disease in adults over age 50 characterized by high levels of pain and functional limitations.
Additionally, there are no longitudinal studies investigating the long-term, combined impact of both positive and negative affect on participation. Indeed, individuals who exhibit both low positive affect and high negative affect may have a greater risk of poor health outcomes than those with either low positive affect or high negative affect alone. Previous research studies investigating health outcomes among people with combined positive and negative affect levels are cross-sectional, making it difficult to determine their long-term impact on health (19,21,22). These studies have also examined the impact of having both high positive affect and low negative affect (21) on health outcomes, not the combination of low positive and high negative affect.
To address these gaps in the literature, we investigated the relative risk of incident participation restriction over 84 months in adults with or at risk of knee osteoarthritis conferred by 1) low positive affect compared to high positive affect, 2) high negative affect compared to low negative affect, and 3) different combinations of positive and negative affect (high positive affect and high negative affect; low positive affect and low negative affect; low positive affect and high negative affect) compared to the combination of high positive and low negative affect. Due to the literature, we hypothesized that people with a combination of low positive and high negative affect would be at the greatest risk of incident participation restriction over time compared to people with either low positive affect or high negative affect alone, and even more than those with both high positive and low negative affect.
Materials and Methods
Data for these analyses are from the Multicenter Osteoarthritis Study (MOST), an ongoing, prospective study aimed at determining risk factors for knee osteoarthritis (OA). Adults age 50–79 at baseline were recruited to MOST from Iowa City, Iowa and Birmingham, Alabama between 2003–2005 if they had a diagnosis of radiographic knee or hip OA with knee or hip pain, or were at risk of developing OA due to obesity, knee pain, or previous knee surgery or injury (23). Participants were ineligible if they needed a walker or personal assistance to walk, had a diagnosis of rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, or reactive arthritis, had bilateral total knee replacements, had cancer in the past 3 years, or if they were currently on dialysis (24).
Participation was self-reported in MOST with the Instrumental Role Limitation subscale of the Late Life Disability Index (LLDI) at 0, 30, 60, and 84 months. The LLDI has acceptable reliability, validity, and sensitivity to change (25,26). The Instrumental Role subscale assesses perceived limitations in participating in 12 activities in the home and community (e.g., taking part in recreation, social activities, visiting friends and family); participation in each activity is scored from 1–5 with total scores ranging from 12–60. Scores were transformed to a 0–100 scale for interpretability and a cut-point of <67.6/100 was used to define participation restriction (27); this cut-off score was previously validated in a population-based sample of older adults and correlates to moderate to severe limitations in activities (28). Participants meeting this definition of participation restriction at baseline were removed from the analyses. Incident participant restriction was defined as new cases of participation restriction at 30, 60, or 84 months.
The Center for Epidemiological Studies Depression Scale (CES-D) was used to assess positive and negative affect at baseline. The CES-D is a self-report measure used as a screening tool for depressive symptoms, (29) and has been validated for use in older adults. Multiple studies have confirmed the validity of a four-factor structure of the CES-D; the 20 items of the scale load onto four factors: positive mood (4 items), depressed mood (7 items), somatic symptoms (7 items), and interpersonal difficulties (2 items) (29). Consistent with previous studies, (17,30,31) we refer to the CES-D items related to positive mood and depressed mood as positive and negative affect, respectively. The four-item positive affect subscale has been used widely as a valid measure of positive affect (15,31,32). In this study, the four items had good internal consistency (Cronbach’s alpha: 0.74) across the four follow-up time points (baseline, 30, 60, 84 months) (See appendix). Each of the items is scored from 0–3 with total scores ranging from 0–12 (higher scores indicate higher positive affect). Due to the skewed distribution of the CES-D, we dichotomized scores for both negative and positive affect into low and high using the median as the cut-off, a similar approach to the one used in Freak-Poli (2015)(30). Participants’ baseline scores on the four positive affect items were dichotomized into low positive affect (score < 11) and high positive affect (score ≥ 11) using the median score of 11. The seven items measuring negative affect were summed (total scores: 0–21) and dichotomized into low negative affect (score = 0) and high negative affect (score ≥ 1) using the baseline median score of zero. The negative affect items had good internal consistency in this sample over the 7 years (Cronbach’s alpha: 0.77). Participants were also split into four groups (low positive affect and low negative affect; low positive affect and high negative affect; high positive affect and low negative affect; high positive affect and high negative affect) at baseline based on their dichotomized scores for both low/high positive affect and low/high negative affect; this allowed us to examine which combination of low and high positive and negative affect had the highest risk of incident participation restriction compared to people with high positive affect and low negative affect.
Baseline characteristics that may confound the relationship between affect and incident participation restriction were used as covariates in this study and included demographic characteristics, disease factors, and functional measures. Demographics (age, sex, race, marital status, education) were collected via self-report questionnaires. Race, marital status, and education were dichotomized into White/Caucasian vs. non-white or other, married vs. non-married, and some college or more vs. high school graduate or less, respectively. Body mass index (BMI) was calculated using participants’ height and weight in the standard equation: weight (kg)/height (m2). A Modified Charlson comorbidity index was calculated based on the participant’s self-reported comorbidities. Widespread pain (present or absent) was defined using the American College of Rheumatology definition of pain above and below the waist, pain on both sides of the body, and back pain by having participants mark their patterns of pain on a human body drawing (33). Reports of total knee replacement (TKR) were verified using radiographs and/or medical records at each time point. Radiographic knee OA was considered present if a knee had a Kellgren/Lawrence scale grade ≥ 2 as determined during radiographic testing at baseline (24). Knee pain and knee stiffness over the past 30 days was assessed using the Western Ontario and McMaster Osteoarthritis Index (WOMAC) and the highest score of both participants’ knees was used for each variable. Walking speed (seconds) was measured by assessing the time it took a participant to walk a distance of 20 meters.
Analyses
Participants in MOST who reported TKR at any time point were removed from the present analyses due to the impact that this significant surgery may have had on positive affect, negative affect, and participation. Participants who met our definition of participation restriction at baseline were also removed, as they were not eligible to develop new participation restriction during follow-up. Baseline descriptive statistics were calculated for the entire sample and for affect groups within the three analyses of positive affect, negative affect, and combinations of positive and negative affect. We also compared baseline characteristics within each analysis by performing tests of ANOVA and Chi-square tests as appropriate for continuous and categorical covariates, respectively. The relative risks of incident participation restriction over 84 months conferred by 1) low positive affect vs. high positive affect, 2) high negative affect vs. low negative affect, and 3) the combinations of negative and positive affect were calculated in separate analyses using robust Poisson regression for binary data (34), adjusting for covariates. For the analysis of combinations of negative and positive affect, we also conducted an analysis of the interaction between the dichotomized positive and negative affect variables.
Results
Of the 3,026 participants enrolled in the MOST study at baseline, 1,810 participants met eligibility criteria for this study (Figure 1). The mean age was 62 years and 56% were female (Table 1). The sample was majority white, married, with 75% reporting higher than a high school education. Forty-five percent of the sample had radiographic knee osteoarthritis at baseline and 6.9% screened positive for depressive symptoms using the CES-D cutoff score of 16 or higher (CES-D mean score: 6.1) (35). Compared to the baseline MOST participants, this sample had greater baseline LLDI scores and lower depressive symptoms but did not differ greatly on other demographic and clinical characteristics. As with other studies using the CES-D to measure positive and negative affect,(18,31) we found a small to moderate, negative correlation between the positive and negative affect scales (r= −0.4). Forty-two percent (n=754) of the sample had low positive affect at baseline, whereas 58% (n=1056) had high positive affect. Thirty-five percent (n=632) of the sample had high negative affect at baseline, whereas 65% (n=1178) had low negative affect. Finally, 23% (n=413) of participants had both low positive affect and high negative affect at baseline, whereas 46% (n=836) of participants had both high positive and low negative affect. There were 342 (19%) participants with both low positive and low negative affect, and 220 (12%) participants with both high positive and high negative affect.
Figure 1.
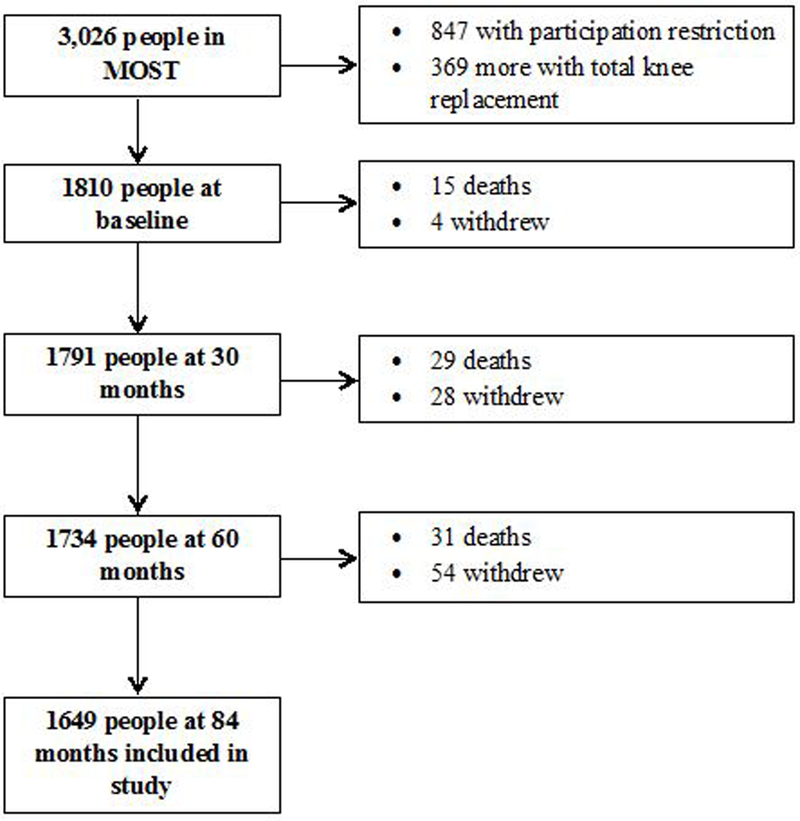
Participant flowchart
Table 1.
Baseline characteristics (N=1,810)
| Whole Sample N=1810 |
Positive Affect | Negative Affect | Combined Groups | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Low PA n=754 (41.7%) |
High PA n=1056 (58.3%) |
High NA n=632 (34.9 %) |
Low NA n=1178 (65.1%) |
Low PA/ High NA n=413 (22.8%) |
High PA/ High NA n=220 (12.1%) |
Low PA/ Low NA n=342 (18.9%) |
High PA/ Low NA n=836 (46.2%) |
||
| Female, n (%) | 1017 (56.2) | 449 (59.6) | 568 (53.8) | 422 (66.8) | 595 (50.5) | 285 (69.2) | 137 (62.3) | 164 (48.0) | 431 (51.6) |
| Age, m ± std | 62.1 ± 8.0 | 62.4 ± 8.1 | 61.9 ± 7.9 | 61.1 ± 8.0 | 62.7 ± 8.0 | 60.9 ± 8.0 | 61.4 ± 7.9 | 64.3 ± 7.8 | 62.0 ± 7.9 |
| Race | |||||||||
| White, n (%) | 1577 (87.1) | 632 (83.8) | 945 (89.5) | 530 (83.9) | 1047 (88.9) | 347 (84.2) | 183 (83.2) | 285 (83.3) | 762 (91.2) |
| Black or other, n (%) | 233 (12.9) |
122 (16.2) |
111 (10.5) |
102 (16.1) |
131 (11.1) |
65 (15.8) |
37 (16.8) |
57 (16.7) |
74 (8.8) |
| Married, n (%) | 1383 (76.4) | 553 (73.3) | 830 (78.6) | 419 (66.3) | 964 (81.8) | 276 (67.0) | 143 (65.0) | 277 (81.0) | 687 (82.2) |
| Education | |||||||||
| Some college or more, n (%) | 1362 (75.3) | 546 (72.4) | 816 (77.3) | 461 (73.0) | 901 (76.5) | 299 (72.4) | 162 (73.6) | 247 (72.2) | 654 (78.2) |
| Site | |||||||||
| Birmingham, AL, n (%) | 840 (46.4) | 381 (50.5) | 459 (43.5) | 335 (53.0) | 505 (42.9) | 218 (52.9) | 117 (53.2) | 163 (47.7) | 342 (40.9) |
| Iowa City, IA, n (%) | 970 (53.6) | 373 (49.5) | 597 (56.5) | 297 (47.0) | 673 (57.1) | 194 (47.1) | 103 (46.8) | 179 (52.3) | 494 (59.1) |
| Body mass index, m ± std | 29.8 ± 5.3 | 29.8 ± 5.1 | 29.7 ± 5.4 | 30.0 ± 5.5 | 29.6 ± 5.1 | 30.0 ± 5.3 | 30.1 ± 5.7 | 29.7 ± 4.8 | 29.6 ± 5.3 |
| Comorbidity index, m ± std | 0.4 ± 0.8 | 0.4 ± 0.8 | 0.4 ± 0.8 | 0.4 ± 0.9 | 0.4 ± 0.7 | 0.4 ± 0.9 | 0.5 ± 0.8 | 0.4 ± 0.8 | 0.4 ± 0.7 |
| Knee OA, n (%) | 825 (45.6) | 345 (45.8) | 480 (45.5) | 276 (43.7) | 549 (46.6) | 180 (43.7) | 96 (43.6) | 165 (48.3) | 384 (46.0) |
| Knee pain, m ± std | 3.3 ± 3.4 | 3.6 ± 3.6 | 3.1 ± 3.2 | 3.9 ± 3.7 | 3.0 ± 3.1 | 4.0 ± 3.8 | 3.7 ± 3.6 | 3.2 ± 3.3 | 2.9 ± 3.1 |
| Knee stiffness, m ± std | 1.9 ± 1.7 | 2.1 ± 1.7 | 1.9 ± 1.6 | 2.3 ± 1.8 | 1.8 ± 1.6 | 2.3 ± 1.8 | 2.2 ± 1.8 | 1.8 ± 1.7 | 1.8 ± 1.6 |
| 20-m walk, (secs) m ± std | 16.2 ± 2.8 | 16.4 ± 3.0 | 16.1 ± 2.6 | 16.5 ± 3.2 | 16.1 ± 2.5 | 16.6 ± 3.4 | 16.4 ± 2.8 | 16.2 ± 2.4 | 16.0 ± 2.6 |
| Widespread pain, n (%) | 777 (43.4) | 351 (47.4) | 426 (40.5) | 322 (51.6) | 455 (39.0) | 216 (53.2) | 106 (48.6) | 135 (40.4) | 320 (38.4) |
| LLDI,* m ± std | 85.0 ± 11.5 | 83.0 ± 11.2 | 86.5 ± 11.5 | 82.2 ± 11.2 | 86.5 ± 11.4 | 81.5 ± 10.8 | 83.7 ± 11.7 | 84.8 ± 11.3 | 87.2 ± 11.4 |
| Depressive symptoms, n (%) | 124 (6.9) | 121 (16.1) | 3 (0.3) | 119 (18.8) | 5 (0.4) | 116 (28.2) | 3 (1.4) | 5 (1.5) | 0 (0) |
Late Life Disability Index, Instrumental Role subscale
Baseline descriptive statistics for participants with high or low positive and negative affect, and by combinations of the two types of affect can be found in Table 1. Depressive symptoms were present in 16.1% of people with low positive affect, 18.8% of people with high negative affect, and 28.2% of people with both low positive and high negative affect (Table 1). With the exceptions of age and education in the analysis of positive affect, we found significant differences by sex, race, marital status, education, and site (Alabama vs. Iowa) across the three analyses. Additionally, participants with low positive affect or high negative affect had significantly higher knee pain, greater knee stiffness, slower 20-meter walk time, and greater report of widespread pain compared to individuals with high positive affect and low negative affect, respectively. Significant differences in knee pain, knee stiffness, widespread pain, and 20-meter walk time were found between the four combinations of positive and negative affect from analysis 3 as well. Twenty-six percent of the sample (n=470) had incident participation restriction over 7 years.
Participants reporting low positive affect at baseline (n=754) had 1.2 times the risk [95% CI: 1.0, 1.4] of incident participation restriction over 84 months as compared to participants with high positive affect, after adjusting for sex, age, race, education, marital status, site, BMI, comorbidity, knee OA, widespread pain, knee pain, knee stiffness, 20-meter walk time, and negative affect (See table 2). In the analysis of negative affect, participants who reported high negative affect at baseline (n=632) had 1.5 times the risk [95% CI: 1.3, 1.7] of incident participation restriction, as compared to those with low negative affect, after adjusting for sex, age, race, education, marital status, site, BMI, comorbidity, knee OA, widespread pain, knee pain, knee stiffness, 20-meter walk time, and positive affect. Finally, participants who reported low positive affect combined with high negative affect (n=413) had an adjusted 1.8 times the risk [95% CI: 1.4, 2.1] of incident participation restriction over 84 months as compared to participants with high positive affect and low negative affect (Table 2). Additionally, when compared to the high positive affect combined with low negative affect group, the high positive affect with high negative affect group had an adjusted 1.4 times the risk [95%CI: 1.1, 1.8] of incident participation restriction. The low positive affect/low negative affect group did not have a statistically significant increased risk of incident participation restriction after adjusting for covariates [RR: 1.2; 95% CI: 0.9, 1.5]. The interaction term for positive and negative affect was positive, but not statistically significant in this model [estimate = 0.04, p=.81]. Although the interaction term was insignificant, we chose to keep it in the final model as it impacted the RRs of the other covariates.
Table 2.
Study 2: Risk ratio (RR) of incident participation restriction over 84 months (N=1810)
| Subjects n (%) |
Crude RR [95%CI] |
Multivariable Adjusted RR† [95%CI] |
|
|---|---|---|---|
| Positive Affect (Analysis 1) | |||
| Low | 754 (41.7) | 1.5** | 1.2* |
| [1.3, 1.8] | [1.0, 1.4] | ||
| High | 1056 (58.3) | (ref) | (ref) |
| Negative Affect (Analysis 2) | |||
| High | 632 (34.9) | 1.8** | 1.5** |
| [1.5, 2.1] | [1.3, 1.7] | ||
| Low | 1178 (65.1) | (ref) | (ref) |
| Combination (Analysis 3) | |||
| Low PA*High NA | 413 (22.8) | 1.0 [0.7, 1.3] | 1.0 [0.8, 1.4] |
| Low PA/High NA | 2.1** | 1.8** | |
| 342 (18.9) | [1.7, 2.5] | [1.4, 2.1] | |
| Low PA/Low NA | 220 (12.1) | 1.3* [1.0, 1.7] | 1.2 [0.9, 1.5] |
| High PA/High NA | 1.7** | 1.4** | |
| 836 (46.2) | [1.3, 2.1] | [1.1, 1.8] | |
| High PA/Low NA | (ref) | (ref) |
PA: positive affect; NA: negative affect
p<.05
p<.01
All models adjusted for: sex, age, education, race, marital status, site, comorbidity, BMI, knee OA, 20-meter walk time, widespread pain, knee pain, knee stiffness; negative affect was adjusted for in model for analysis 1 and positive affect adjusted for in analysis 2
Discussion
To our knowledge, this is the first study to measure the long-term effects of positive and negative affect on risk of incident participation restriction among adults with or at risk of knee osteoarthritis. We found a statistically significant, increased risk of participation restriction over 84 months among people who reported low positive affect at baseline compared to high positive affect, people with high negative affect compared to low negative affect, and among people with low positive and high negative affect combined. The finding of a positive, insignificant interaction between positive affect and negative affect indicates that the two have an independent, yet approximately additive effect on participation restriction.
This study’s results extend the current literature on positive affect in the context of participation behavior in several ways. First, while previous longitudinal studies have found a small but significant increased risk of disability conferred by low positive affect, these studies have been conducted over shorter time periods, varying from three months to two years of follow-up (15–17). Second, this study’s finding of an increased long-term risk of participation restriction conferred by low positive affect is the first to be conducted in a population of people with knee OA, a chronic disease that is highly prevalent among middle age and older adults. Third, previous studies have measured the relationship between positive affect and disability but not incident participation restriction, a more comprehensive construct than functional disability (1).
Whereas the majority of studies on negative affect in people with knee OA have investigated its relationship with pain, (20) our findings provide empirical evidence of its long-term, negative impact on participation outcomes in knee OA, a common condition among adults over 50. Additionally, we found negative affect to significantly impact incident participation restriction even after controlling for knee pain in our analyses. Our results concur with studies of the relationship between negative affect and disability in other disease conditions, such as back pain and lung cancer (18,36). Seebach et al. (2012) found that high negative affect six weeks after spine surgery among people with chronic pain was predictive of higher pain interference and disability at 3 months (36). Significant associations between high negative affect and role limitations have also been identified in older adults with lung cancer (18). These three studies’ findings suggest that negative affect may have a general negative impact on participation across health conditions, however more studies are needed to support this claim.
Previous research studies measuring the combined impact of both low positive affect and high negative affect on health outcomes among adults with arthritis have found similar results to this study, yet have been cross-sectional and have not examined incident participation restriction (19,21). For example, Cruz-Almeida et al. (2013) found that older adults with knee osteoarthritis who had high optimism (positive affect) and low negative affect had the lowest levels of functional disability, as compared to older adults with other affect group combinations. One study found that older adults with chronic conditions (arthritis, cardiovascular disease, COPD, or diabetes) who exhibited both high positive affect and low negative affect were more likely to have better self-rated health, fewer symptoms, and better function (19). Satisfaction with participation was also related to positive and negative affect in a small cross-sectional study of people with traumatic brain injury (22). Our study contributes to the field by investigating the long-term impact of having different combinations of high and low positive and negative affect on incident participation restriction.
As knee osteoarthritis is a disabling disease with no known cure and increasing prevalence, identifying specific subgroups of people who are at greater risk for limitations over time has important clinical value. Health professionals who want to decrease long-term participation restriction should consider screening patients with knee OA for low positive affect and high negative affect. Previous research studies have identified strategies for improving affect states that might be effective for this population, such as positive psychology interventions (37–40), which are low cost and can be self-administered. In a randomized controlled trial, Taylor et al. (2016) found that participants who engaged in “positive activity” exercises (e.g., positive mental imagery, performing acts of kindness or expressing gratitude) saw greater improvements in positive affect and greater decreases in negative affect than the waitlist group (41). Previous studies have also identified mindfulness and meditation as impacting positive and negative affect (42,43). More evidence of the benefits of these interventions on positive and negative affect in relation to participation outcomes is needed.
This study is not without limitations. First, due to the nature of longitudinal studies, attrition occurred over time and may have created bias in the findings. Second, the study population lacked geographic variability and racial diversity; hence the findings may not be generalizable to other populations. Third, as the measurements of positive and negative affect were from subscales of the CES-D, we were unable to adjust for depressive symptoms. A CES-D score of 16 or more is considered a positive screen for depressive symptoms; therefore, as some people who had low positive affect or high negative affect may also have had depressive symptoms, we would have removed the effect of these subjects from the analyses by controlling for depressive symptoms. However, the presence of depressive symptoms was less than 30% in the three analyses (16% for low positive affect, 18% for high negative affect, and 28% for the combined low positive and high negative affect group). As depression is associated with positive affect and negative affect, (19) future studies should investigate whether it interacts with or mediates the relationship between affect and participation that this study found. Fourth, the positive and negative affect scores demonstrated ceiling and floor effects, respectively, in our study population. While the CES-D is a validated measure of positive and negative affect and similar median cut-points have been used in a previous study measuring incident disease (18), the CES-D may not capture the full range of positive and negative affect as with other measures, e.g., Positive and Negative Affect Schedule (PANAS), and may have influenced our results. Additional studies of more robust measures of positive and negative affect are warranted in examining the role of affect with incident participation restriction. Finally, while the MOST cohort has rich demographic and clinical evaluations of all participants, there are potential behavioral confounders and effect modifiers for positive and negative affect that were not measured in the present study. Factors such as self-efficacy and active and passive coping strategies may be important to assess in future studies when examining the roles of positive and negative affect on participation.
In conclusion, we found significant, increased risk of incident participation restriction over 84 months among adults with or at risk of knee osteoarthritis conferred by the individual effects of low positive affect and high negative affect, as well as combinations of high/low positive and negative affect. Individuals who reported both low positive affect and high negative affect at baseline had higher risk of incident participation restriction over time than either low positive affect or high negative affect alone, and compared to any combination of high/low positive and negative affect. This study extends the current literature by providing novel insight into the role of positive affect and negative affect in long-term participation outcomes, whereas cross-sectional study design, short follow-up periods, or populations other than people with knee OA have limited the previous literature in this area. Our findings have important clinical relevance for the treatment of knee OA among adults over 50 as it identified people with mood states who are more at risk for participation restriction over time.
Supplementary Material
Significance and Innovation.
This is the first study to investigate the long-term risk of incident participation restriction conferred by low positive affect and high negative affect among a large cohort of people with or at risk of developing knee osteoarthritis.
The finding that adults with or at risk of knee osteoarthritis with both low positive affect and high negative affect had nearly twice the risk of incident participation restriction over seven years compared to adults with other combinations of positive and negative affect contributes new evidence to the field that mood states may impact health outcomes among people with arthritis and knee pain.
This study’s findings emphasize that interventions aimed at preventing participation restriction among people with or at risk of knee osteoarthritis may need to address low positive affect and high negative affect.
Acknowledgement
This manuscript has been reviewed by MOST study investigators for its scientific content and data interpretation.
Contributor Information
Molly W. Vaughan, Boston University Sargent College of Health and Rehabilitation Sciences, Boston, MA, mvaughan@bu.edu.
Michael P. LaValley, Department of Biostatistics, Boston University School of Public Health, Boston, MA, mlava@bu.edu.
David T. Felson, Clinical Epidemiology Research & Training Unit, Clinical Translational Science Award Training Program, Boston University CTSI, Boston University School of Medicine, Boston, MA, dfelson@bu.edu.
Gael I. Orsmond, Department of Occupational Therapy, Rehabilitation Sciences Program, Boston University Sargent College of Health and Rehabilitation Sciences, Boston, MA, gorsmond@bu.edu.
Jingbo Niu, Department of Medicine - Nephrology, Baylor College of Medicine, Houston, TX, Jingbo.niu@bcm.edu.
Cora E. Lewis, Division of Preventive Medicine, University of Alabama at Birmingham School of Medicine, Birmingham, AL, bethlew@uab.edu.
Neil A. Segal, Department of Rehabilitation Medicine, University of Kansas Medical Center, Kansas City, KS, nsegal@kumc.edu.
Michael C. Nevitt, Department of Epidemiology & Biostatistics, University of California San Francisco School of Medicine, San Francisco, CA, Michael.nevitt@ucsf.edu.
Julie J. Keysor, Department of Physical Therapy and Athletic Training, Boston University Sargent College of Health and Rehabilitation Sciences, Boston, MA, jkeysor@bu.edu.
References
- 1.World Health Organization. International classification of functioning, disability, and health In: Geneva: World Health Organization; 2001; 2001. [Google Scholar]
- 2.Barbour KE, Helmick CG, Theis KA, Murphy LB, Hootman JM, Brady TJ, Cheng YJ. Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation-United States, 2010–2012. MMWR 2013;62(44):869–873. [PMC free article] [PubMed] [Google Scholar]
- 3.Guccione AA, Felson DT, Anderson JJ, et al. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am J Public Health 1994;84(3):351–358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zhang Y, Jordan JM. Epidemiology of Osteoarthritis. Clin Geriatr Med 2010;26(3):355–369. doi: 10.1016/j.cger.2010.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dillon CF, Rasch EK, Gu Q, Hirsch R. Prevalence of knee osteoarthritis in the United States: arthritis data from the Third National Health and Nutrition Examination Survey 1991–94. J Rheumatol 2006;33(11):2271–2279. [PubMed] [Google Scholar]
- 6.Carr AJ. Beyond disability: measuring the social and personal consequences of osteoarthritis. Osteoarthritis Cartilage 1999;7(2):230–238. doi: 10.1053/joca.1998.0154. [DOI] [PubMed] [Google Scholar]
- 7.Machado GP, Gignac MA, Badley EM. Participation restrictions among older adults with osteoarthritis: a mediated model of physical symptoms, activity limitations, and depression. Arthritis Rheum 2008;59(1):129–135. [DOI] [PubMed] [Google Scholar]
- 8.Zautra AJ, Affleck GG, Tennen H, Reich JW, Davis MC. Dynamic Approaches to Emotions and Stress in Everyday Life: Bolger and Zuckerman Reloaded with Positive as Well as Negative Affects. J Pers 2005;73(6):1511–1538. doi: 10.1111/j.0022-3506.2005.00357.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Clark LA, Watson D. Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. J Abnorm Psychol 1991;100(3):316–336. doi: 10.1037/0021-843X.100.3.316. [DOI] [PubMed] [Google Scholar]
- 10.Fredman L, Hawkes WG, Black S, Bertrand RM, Magaziner J. Elderly Patients with Hip Fracture with Positive Affect Have Better Functional Recovery over 2 Years. J Am Geriatr Soc 2006;54(7):1074–1081. doi: 10.1111/j.1532-5415.2006.00786.x. [DOI] [PubMed] [Google Scholar]
- 11.Corcoran J, Brown E, Davis M, Pineda M, Kadolph J, Bell H. Depression in Older Adults: A Meta-Synthesis. J Gerontol Soc Work 2013;56(6):509–534. doi: 10.1080/01634372.2013.811144. [DOI] [PubMed] [Google Scholar]
- 12.Huyser BA, Parker JC. NEGATIVE AFFECT AND PAIN IN ARTHRITIS. Rheum Dis Clin N Am 1999;25(1):105–121. doi: 10.1016/S0889-857X(05)70057-0. [DOI] [PubMed] [Google Scholar]
- 13.Zautra AJ, Johnson LM, Davis MC. Positive Affect as a Source of Resilience for Women in Chronic Pain. J Consult Clin Psychol 2005;73(2):212–220. doi: 10.1037/0022-006X.73.2.212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zautra AJ, Burleson MH, Smith CA, et al. Arthritis and perceptions of quality of life: An examination of positive and negative affect in rheumatoid arthritis patients. Health Psychol 1995;14(5):399–408. doi: 10.1037/0278-6133.14.5.399. [DOI] [PubMed] [Google Scholar]
- 15.Berges I-M, Seale GS, Ostir GV. The role of positive affect on social participation following stroke. Disabil Rehabil Int Multidiscip J 2012;34(25):2119–2123. doi: 10.3109/09638288.2012.673684. [DOI] [PubMed] [Google Scholar]
- 16.Hirosaki M, Ishimoto Y, Kasahara Y, et al. Positive affect as a predictor of lower risk of functional decline in community-dwelling elderly in Japan. Geriatr Gerontol Int 2013;13(4):1051–1058. doi: 10.1111/ggi.12008. [DOI] [PubMed] [Google Scholar]
- 17.Fisher MN, Snih SA, Ostir GV, Goodwin JS. Positive affect and disability among older Mexican Americans with arthritis. Arthritis Care Res 2004;51(1):34–39. doi: 10.1002/art.20079. [DOI] [PubMed] [Google Scholar]
- 18.Hirsch JK, Floyd AR, Duberstein PR. Perceived health in lung cancer patients: the role of positive and negative affect. Qual Life Res 2011;21(2):187–194. doi: 10.1007/s11136-011-9933-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jie HuGruber KJ. Positive and Negative Affect and Health Functioning Indicators among Older Adults with Chronic Illnesses. Issues Ment Health Nurs 2008;29(8):895–911. doi: 10.1080/01612840802182938. [DOI] [PubMed] [Google Scholar]
- 20.Finan PH, Quartana PJ, Smith MT. Positive and Negative Affect Dimensions in Chronic Knee Osteoarthritis: Effects on Clinical and Laboratory Pain. Psychosom Med 2013;75(5):463–470. doi: 10.1097/PSY.0b013e31828ef1d6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cruz-Almeida Y, King CD, Goodin BR, et al. Psychological Profiles and Pain Characteristics of Older Adults With Knee Osteoarthritis. Arthritis Care Res 2013;65(11):1786–1794. doi: 10.1002/acr.22070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Juengst SB, Arenth PM, Raina KD, McCue M, Skidmore ER. Affective state and community integration after traumatic brain injury. Am J Phys Med Rehabil Assoc Acad Physiatr 2014;93(12):1086–1094. doi: 10.1097/PHM.0000000000000163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Segal NA, Nevitt MC, Gross KD, et al. The Multicenter Osteoarthritis Study: Opportunities for Rehabilitation Research. PM&R 2013;5(8):647–654. doi: 10.1016/j.pmrj.2013.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Felson DT, Niu J, Guermazi A, et al. Correlation of the development of knee pain with enlarging bone marrow lesions on magnetic resonance imaging. Arthritis Rheum 2007;56(9):2986–2992. doi: 10.1002/art.22851. [DOI] [PubMed] [Google Scholar]
- 25.Jette AM, Haley SM, Coster WJ, et al. Late Life Function and Disability Instrument I. Development and Evaluation of the Disability Component. J Gerontol A Biol Sci Med Sci 2002;57(4):M209–M216. doi: 10.1093/gerona/57.4.M209. [DOI] [PubMed] [Google Scholar]
- 26.Beauchamp MK, Schmidt CT, Pedersen MM, Bean JF, Jette AM. Psychometric properties of the Late-Life Function and Disability Instrument: a systematic review. BMC Geriatr 2014;14:12. doi: 10.1186/1471-2318-14-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Maxwell JL, Keysor JJ, Niu J, et al. Participation Following Knee Replacement: The MOST Cohort Study. Phys Ther 2013;93(11):1467–1474. doi: 10.2522/ptj.20130109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Jette AM, Haley SM, Kooyoomjian JT. Late-Life FDI Manual Boston University, Roybal Center for Enhancement of Late-Life Function; 2002. [Google Scholar]
- 29.Ros L, Latorre J, Aguilar M, Serrano J, Navarro B, Ricarte J. Factor Structure and Psychometric Properties of the Center for Epidemiologic Studies Depression Scale (CES-D) in Older Populations With and Without Cognitive Impairment. Int J Aging Hum Dev 2011;72(2):83–110. doi: 10.2190/AG.72.2.a. [DOI] [PubMed] [Google Scholar]
- 30.Freak-Poli R, Mirza SS, Franco OH, Ikram MA, Hofman A, Tiemeier H. Positive affect is not associated with incidence of cardiovascular disease: A population-based study of older persons. Prev Med 2015;74:14–20. doi: 10.1016/j.ypmed.2015.01.032. [DOI] [PubMed] [Google Scholar]
- 31.Ostir GV, Markides KS, Black SA. Emotional well-being predicts subsequent functional independence and survival. J Am Geriatr Soc 2000;48(5):473–478. [DOI] [PubMed] [Google Scholar]
- 32.Brummett BH, Boyle SH, Kuhn CM, Siegler IC, Williams RB. Positive Affect is Associated with Cardiovascular Reactivity, Norepinephrine Level, and Morning Rise in Salivary Cortisol. Psychophysiology 2009;46(4):862–869. doi: 10.1111/j.1469-8986.2009.00829.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.White DK, Keysor JJ, Neogi T, et al. When it hurts, a positive attitude may help: association of positive affect with daily walking in knee osteoarthritis. Results from a multicenter longitudinal cohort study. Arthritis Care Res 2012;64(9):1312–1319. doi: 10.1002/acr.21694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Chen W, Shi J, Qian L, Azen SP. Comparison of robustness to outliers between robust poisson models and log-binomial models when estimating relative risks for common binary outcomes: a simulation study. BMC Med Res Methodol 2014;14:82. doi: 10.1186/1471-2288-14-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lewinsohn PM, Seeley JR, Roberts RE, Allen NB. Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol Aging 1997;12(2):277–287. doi: 10.1037/0882-7974.12.2.277. [DOI] [PubMed] [Google Scholar]
- 36.Seebach CL, Kirkhart M, Lating JM, et al. Examining the role of positive and negative affect in recovery from spine surgery. PAIN 2012;153(3):518–525. doi: 10.1016/j.pain.2011.10.012. [DOI] [PubMed] [Google Scholar]
- 37.Cohn MA, Pietrucha ME, Saslow LR, Hult JR, Moskowitz JT. An online positive affect skills intervention reduces depression in adults with type 2 diabetes. J Posit Psychol 2014;9(6):523–534. doi: 10.1080/17439760.2014.920410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Blackwell SE, Holmes EA. Brightening the Day With Flashes of Positive Mental Imagery: A Case Study of an Individual With Depression. J Clin Psychol February 2017:n/a-n/a. doi: 10.1002/jclp.22455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Müller R, Gertz KJ, Molton IR, et al. Effects of a Tailored Positive Psychology Intervention on Well-Being and Pain in Individuals With Chronic Pain and a Physical Disability: A Feasibility Trial. Clin J Pain 2016;32(1):32–44. doi: 10.1097/AJP.0000000000000225. [DOI] [PubMed] [Google Scholar]
- 40.Sin NL, Lyubomirsky S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J Clin Psychol 2009;65(5):467–487. doi: 10.1002/jclp.20593. [DOI] [PubMed] [Google Scholar]
- 41.Taylor CT, Lyubomirsky S, Stein MB. Upregulating the positive affect system in anxiety and depression: Outcomes of a positive activity intervention. Depress Anxiety December 2016:n/a-n/a. doi: 10.1002/da.22593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Menezes CB, Bizarro L. Effects of a brief meditation training on negative affect, trait anxiety and concentrated attention. Paidéia 2015;25(62):393–401. doi: 10.1590/1982-43272562201513. [DOI] [Google Scholar]
- 43.Davis MC, Zautra AJ. An online mindfulness intervention targeting socioemotional regulation in fibromyalgia: Results of a randomized controlled trial. Ann Behav Med 2013;46(3):273–284. doi: 10.1007/s12160-013-9513-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.