

Abstract
Objective:
The aim of the study was to describe the effects of TX-001HR (17β-estradiol [E2] and natural progesterone [P4] in a single oral capsule) on menopause-specific quality of life in women with moderate to severe vasomotor symptoms (VMS).
Methods:
The REPLENISH study (NCT01942668) was a phase 3, randomized, double-blind, placebo-controlled, multicenter trial which evaluated four E2/P4 doses in postmenopausal women with VMS and a uterus. Women with moderate to severe hot flushes (≥7/d or ≥50/wk) were included in a VMS substudy. Participants self-administered the Menopause-Specific Quality of Life (MENQOL) questionnaire. Baseline changes in MENQOL overall and domains were determined as well as correlations between changes in MENQOL scores and VMS frequency or severity.
Results:
In the VMS substudy, women treated with E2/P4 had significantly greater improvements from baseline in their MENQOL overall score at week 12, and months 6 and 12, compared with placebo (all, P < 0.05, except the lowest E2/P4 dose at months 6 and 12). Improvements from baseline for the MENQOL vasomotor domain score were significantly greater with TX-001HR doses versus placebo at all time points (all, P < 0.01). Changes in MENQOL vasomotor scores moderately correlated with changes in VMS frequency (r = 0.56, P < 0.0001) and severity (r = 0.55, P < 0.0001).
Conclusion:
In the REPLENISH trial, women with moderate to severe VMS treated with most E2/P4 doses reported significant improvements in quality of life from baseline to 12 weeks compared with placebo, which were maintained up to 12 months. TX-001HR, if approved, may provide the first oral hormone therapy formulation in a single capsule containing E2 and P4 for the treatment of VMS in postmenopausal women with a uterus.
Keywords: Estradiol, Hot flushes, Menopause, Progesterone, Vasomotor symptoms
Vasomotor symptoms (VMS) are widely considered bothersome to postmenopausal women,1-3 with a negative impact on quality of life,1,4 sleep,1,5 and work productivity.4,6 Despite the benefits of hormone therapy (HT) for relief of VMS,7 many women stopped taking US Food and Drug Administration (FDA)-approved HT formulations8 after publication of the Women's Health Initiative (WHI) trial results and, as a result, many women take compounded “natural” products, falsely believing they are safer.9,10 Since then, use of unapproved, compounded HT formulations has skyrocketed,9-12 reaching 39 million prescriptions.13 Efficacy and safety of compounded HT, which may not provide sufficient endometrial protection, has, however, not been rigorously tested.14-18
Although micronized progesterone (P4), which is chemically identical to endogenous hormones, may be safer than the synthetic progestogens typically included in approved HT formulations, according to recent data on risk of breast cancer19,20 and venous thromboembolism,21 no FDA-approved formulation combines natural 17β-estradiol (E2) and P4 in a single capsule. The combination of E2 and P4 in a single capsule has been historically challenging because of the differences in their structure and solubility.22 Recently, an investigational combination of E2 and P4 (sometimes referred to as bioidentical) in a single, oral, softgel capsule (TX-001HR; TherapeuticsMD, Boca Raton, FL) was evaluated in the REPLENISH trial for the treatment of moderate to severe VMS in postmenopausal women with a uterus. The REPLENISH trial found that women taking TX-001HR versus placebo had statistically significant and clinically meaningful decreases in moderate to severe VMS frequency from baseline to week 12 (all, P ≤ 0.002) with significant improvement in VMS severity from baseline to week 12 with the three highest doses.23 No endometrial hyperplasia or cancer was found with any of the doses.23
With more than half (60%) of women in midlife seeking medical care or advice at least once for menopausal symptoms, as reported in one survey,24 a need for effective treatments that relieve VMS is apparent. Although the direct effect of treatment on VMS frequency and severity is important, evaluating effects of treatment should also include its impact on quality of life measures. A more complete understanding of treatment effects could allow healthcare providers to better counsel their patients regarding treatment options. The objective of this analysis was to determine the effects of TX-001HR on quality of life when used for the treatment of moderate to severe VMS in the REPLENISH trial, using the Menopause-Specific Quality of Life (MENQOL) questionnaire.
METHODS
Study design and participants
The REPLENISH trial (NCT01942668) was a phase 3, prospective, randomized, double-blind, placebo-controlled, multicenter trial evaluating four doses of E2/P4 combined in a single, oral, softgel capsule formulation (TX-001HR) for the treatment of moderate to severe VMS in postmenopausal women . Enrollment began in August 2013 and the last participant completed the trial in October 2016. The study was designed, conducted, and monitored in accordance with ethical guidelines of Good Clinical Practice and the Declaration of Helsinki, and all participants gave written informed consent.
Details of the trial, including inclusion and exclusion criteria, are reported elsewhere.23 Briefly, participants were healthy postmenopausal women (40-65 y, ≤34 kg/m2) with a uterus who were seeking treatment for VMS. Women were eligible for the VMS substudy if they experienced a minimum of 7 moderate to severe VMS (hot flushes) daily or 50 per week before enrollment. Women eligible for the VMS substudy were randomly assigned 1:1:1:1:1 to daily oral E2/P4 (mg/mg) at doses of 1/100, 0.5/100, 0.5/50, or 0.25/50, or to matching placebo, whereas women not eligible for the VMS substudy were randomized 1:1:1:1 to the active E2/P4 doses only (no placebo) for 12 months (to assess endometrial and overall safety, as reported elsewhere23). Women were randomized to treatment at each site using a reproducible, computer-generated block randomization schedule. Because the different doses were two different sizes, a double-blind, double-dummy design was used to maintain blinding; all women took two capsules (one large and one small capsule; one of which was a placebo capsule) with food at bedtime. Participants were instructed to use a dosing diary to record all treatment doses taken and missed; the diary was used to determine study compliance (defined as ≥80% of study drug taken).
Each participant was instructed to complete a daily VMS diary by recording the number and severity of their VMS through week 12. The severity of hot flushes was defined as mild (sensation of heat without sweating), moderate (sensation of heat with sweating, able to continue activity), or severe (sensation of heat with sweating, causing cessation of activity). Baseline number and severity of VMS per week for each participant were determined before randomization; women with frequent moderate to severe VMS (≥7/d or 50/wk) were enrolled in the VMS substudy. On-treatment weekly severity score was defined as the [(number of mild hot flushes for 7 d) × 1 + (number of moderate hot flushes for 7 d) × 2 + (number of severe hot flushes for 7 d) × 3]/(total number of mild, moderate, and severe hot flushes over 7 d).
The four coprimary efficacy endpoints were mean changes in frequency and severity of moderate to severe VMS with E2/P4 doses versus placebo from baseline to weeks 4 and 12 in the VMS substudy and the primary safety endpoint was the incidence of endometrial hyperplasia with E2/P4 at 12 months. A secondary efficacy endpoint was to evaluate the effects of TX-001HR on quality of life when used for the treatment of moderate to severe VMS.
Quality of life assessment
To determine associations between VMS treatment and quality of life, women self-administered the validated MENQOL questionnaire25 at baseline, week 12, and months 6 and 12. The MENQOL questionnaire consists of 29 items (symptoms) which, if experienced over the previous 1-month period, were rated on a 7-point Likert scale ranging from 0 = “not at all bothered” to 6 = “extremely bothered.” Items were grouped into four domains: vasomotor (3 items), psychosocial (7 items), physical (16 items), and sexual (3 items). Scores in each domain were converted to an analysis score with a range of 1 (no symptoms) to 8 (extremely bothered).
Statistical analysis
The modified intent-to-treat (MITT) population included all randomized participants who took at least one dose (two capsules with blinding) of the study medication. The MITT-VMS population was the primary efficacy population and included all women randomized to the VMS substudy who took at least one dose (two capsules) of study medication, had ≥5 days of VMS diary data at baseline, and had ≥4 days of VMS diary data for one on-treatment week. Sample size determined for the VMS population was 150 women per treatment group who provided at least 90% power to test the primary VMS hypotheses of the 12-week VMS substudy while allowing a 20% discontinuation rate, as previously reported.
MENQOL outcomes were assessed in both MITT and MITT-VMS populations. Changes from baseline in the overall MENQOL score and each of the four domains were analyzed in the MITT-VMS population using analysis of covariance with treatment group and region as factors, and baseline score as covariate for the MITT-VMS and MITT populations separately. Handling of missing MENQOL data was performed as follows: if ≥50% of the items were answered for each domain function score (ie, ≥8 of 16 questions were answered for physical domain, ≥4 of 7 for psychosocial domain, and ≥2 of 3 for vasomotor domain and sexual domain), then a domain score was calculated based on the mean of the non-missing responses; if ≥50% of the items were missing, no score was calculated and will be considered missing. Missing data were not imputed.
The relationship between changes in the frequency and severity of moderate to severe VMS and changes in MENQOL domain and overall scores from baseline to week 12 were examined using Pearson correlations in the MITT-VMS population, regardless of treatment. Analyses were performed with Statistical Analysis System 9.2 (SAS Institute Inc, Cary, NC) and results were statistically significant at P < 0.05.
RESULTS
Disposition and demographics
A total of 1,845 women were randomized into the trial, and 1,833 were included in the MITT population; 1,273 completed 52 weeks of treatment (Fig. 1). Of the 726 included in the MITT-VMS population, 647 (89%) completed the 12-week efficacy VMS substudy and 517 (71%) completed the 52-week study. The most common reasons for discontinuation at 52 weeks were adverse events (8.5%), lost to follow-up (6.7%), consent withdrawal (6.7%), protocol deviation (3.7%), lack of efficacy (2.6%), other (0.3%), and investigator or sponsor decision (0.1%).
FIG. 1.
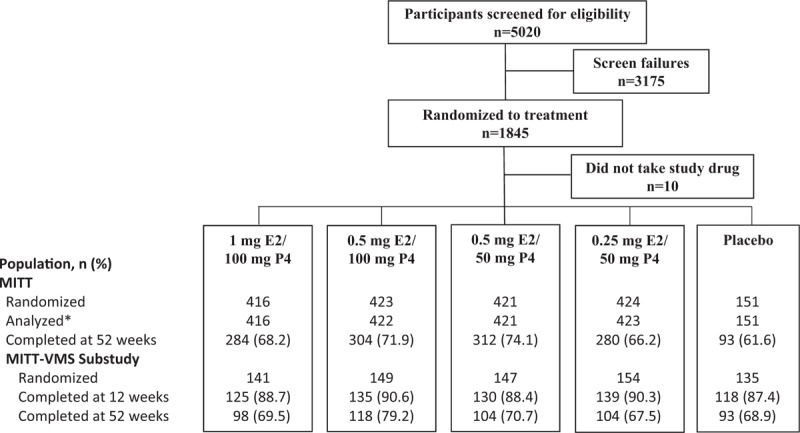
Patient disposition in the MITT-VMS population. ∗Two women were screened and randomized at two separate sites, for analysis purposes, the first randomization number and treatment for each woman was utilized. E2, 17β-estradiol; MITT, modified intent-to-treat; P4, progesterone; VMS, vasomotor symptoms.
Women in the VMS substudy had a mean age of 55 years (range, 40-65 y) and mean BMI of 27 kg/m2; 67% were white and 31% were African American (Table 1). Mean time since menopause onset was 5.9 years. Moderate to severe VMS at baseline occurred with a mean frequency of 72.1 to 77.0 per week, and with a mean weekly severity baseline score of 2.50 to 2.54. Mean MENQOL overall scores ranged from 4.3 to 4.7 and mean vasomotor domain scores ranged from 6.9 to 7.2 at baseline.
TABLE 1.
Demographics and baseline characteristics in the modified intent-to-treat vasomotor symptom (MITT-VMS) population
| Estradiol/Progesterone | |||||
| Characteristic | 1 mg/100 mg | 0.5 mg/100 mg | 0.5 mg/50 mg | 0.25 mg/50 mg | Placebo |
| N | 141 | 149 | 147 | 154 | 135 |
| Age, y | 54.7 ± 4.8 | 54.9 ± 4.5 | 54.8 ± 4.6 | 54.5 ± 3. 8 | 54.3 ± 4.3 |
| Race, n (%) | |||||
| White | 95 (67.4) | 99 (66.4) | 99 (67.3) | 102 (66.2) | 91 (67.4) |
| African American | 45 (31.9) | 48 (32.2) | 43 (29.3) | 48 (31.2) | 41 (30.4) |
| Othera | 1 (0.7) | 2 (1.3) | 5 (3.4) | 4 (2.6) | 3 (2.2) |
| BMI, kg/m2 | 26.5 ± 3.9 | 27.1 ± 4.3 | 26.6 ± 3.9 | 26.4 ± 4.0 | 26.6 ± 3.8 |
| Time since menopause, y | 6.1 ± 5.5 | 6.5 ± 5.4 | 6.0 ± 4.8 | 5.2 ± 4.8 | 5.7 ± 4.9 |
| Bilateral oophorectomy, n (%) | 3 (2.1) | 3 (2.0) | 1 (0.7) | 1 (0.6) | 0 |
| Moderate–severe VMS | |||||
| Weekly frequency | 74.4 ± 35.3 | 72.1 ± 27.8 | 75.9 ± 28.0 | 77.0 ± 30.4 | 72.4 ± 23.3 |
| Weekly severity | 2.54 ± 0.32 | 2.51 ± 0.25 | 2.50 ± 0.23 | 2.51 ± 0.26 | 2.52 ± 0.25 |
| MENQOL scores | |||||
| Overall | 4.5 ± 1.2 | 4.3 ± 1.3 | 4.7 ± 1.4 | 4.5 ± 1.3 | 4.6 ± 1.3 |
| Vasomotor | 7.1 ± 0.9 | 6.9 ± 1.1 | 7.1 ± 1.0 | 7.1 ± 1.0 | 7.2 ± 1.0 |
| Psychosocial | 3.4 ± 1.7 | 3.2 ± 1.7 | 3.6 ± 1.9 | 3.4 ± 1.8 | 3.6 ± 1.9 |
| Physical | 3.7 ± 1.6 | 3.6 ± 1.5 | 4.0 ± 1.7 | 3.7 ± 1.5 | 3.8 ± 1.6 |
| Sexual | 3.7 ± 2.4 | 3.6 ± 2.4 | 3.9 ± 2.5 | 3.9 ± 2.4 | 4.0 ± 2.4 |
Data expressed as mean ± SD unless stated otherwise.
BMI, body mass index; SD, standard deviation; MENQOL, Menopause-Specific Quality of Life questionnaire; VMS, vasomotor symptoms.
aOther includes: other (n = 10), American Indian or Alaska Native (n = 2), Native Hawaiian or Pacific Islander (n = 2), and unknown (n = 1).
MENQOL overall and domain scores
For the overall MENQOL score, women in the MITT-VMS population treated with all doses of E2/P4 had significantly greater mean improvements from baseline than with placebo at 12 weeks (all, P < 0.05; Fig. 2A). At months 6 and 12, overall MENQOL scores significantly improved for the three highest E2/P4 groups versus placebo. Differences in the least squares (LS) mean change from baseline in the overall score between E2/P4 doses and placebo ranged from −0.32 to −0.58 at week 12 and from −0.30 to −0.73 at month 12. Similar results were observed in the MITT population, with significant differences in the MENQOL overall score between the E2/P4 and placebo groups at week 12 (differences in LS mean change: −0.42 to −0.62; all P < 0.001) and at month 12 (−0.37 to −0.62; all P < 0.01).
FIG. 2.
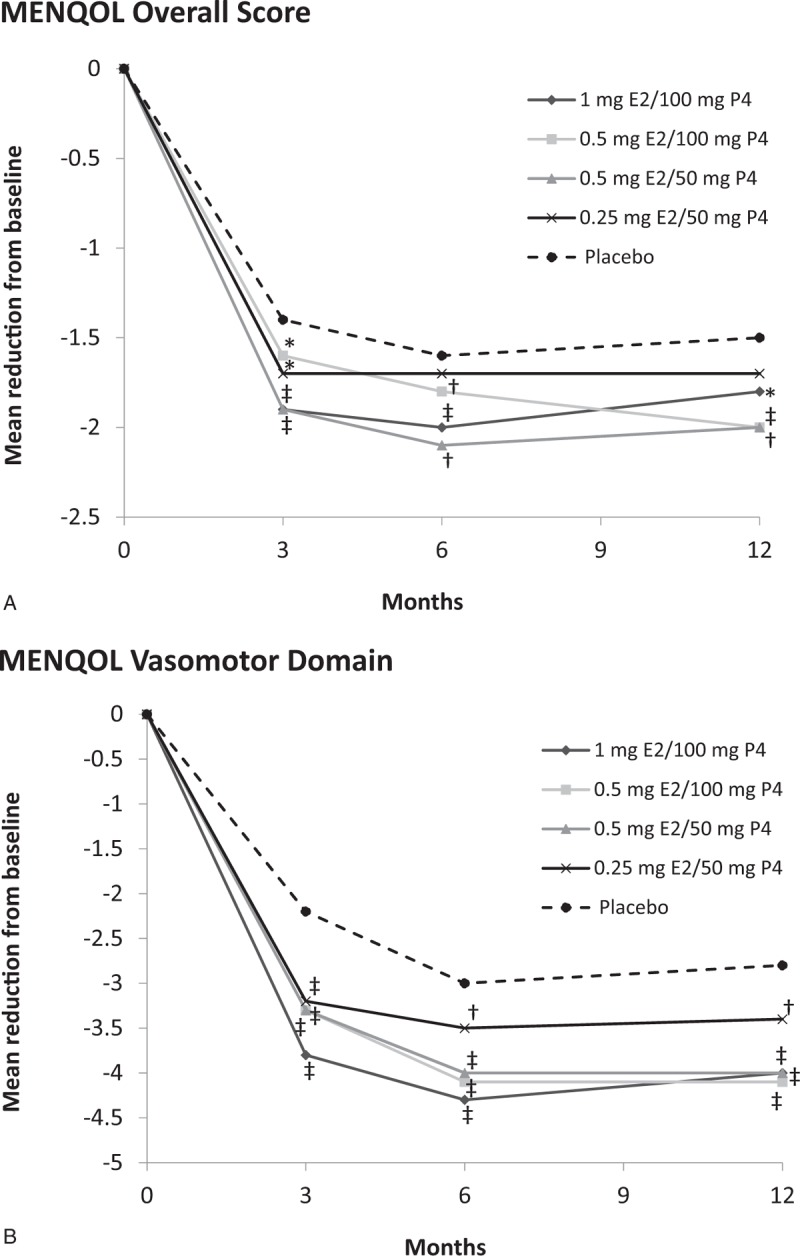
Change in (A) overall MENQOL and (B) MENQOL vasomotor domain scores over 12 months with E2/P4 groups versus placebo in the MITT-VMS population. ∗P < 0.05; †P < 0.01; ‡P < 0.001 versus placebo. E2, 17β-estradiol; MENQOL, Menopause-Specific Quality of Life Questionnaire; MITT, modified intent-to-treat; P4, progesterone; VMS, vasomotor symptoms.
Mean improvements from baseline in the MENQOL vasomotor domain score were significantly greater in all E2/P4 groups versus placebo group at all time points (all, P < 0.01) in the MITT-VMS population (Fig. 2B). Differences in the LS mean change from baseline in the vasomotor domain between E2/P4 doses and placebo ranged from −1.04 to −1.65 at week 12 and from −0.72 to −1.46 at month 12. Similarly, significant differences in the MENQOL vasomotor domain for the MITT population were observed between all active treatment groups and placebo at week 12 (differences in LS mean change: −1.25 to −1.92; all P < 0.001) and at month 12 (−1.08 to −1.65; P < 0.001).
In the MITT-VMS or MITT populations, no consistent statistically significant differences were noted between the E2/P4 groups and placebo for the physical, psychosocial, or sexual domains, except for improvements in the sexual domain observed with the two highest E2/P4 doses versus placebo at month 12 in the MITT population. In the MITT population, differences in LS mean change between E2/P4 doses and placebo for the sexual domain were −0.44 (P = 0.029) for 1 mg E2/100 mg P4 and −0.45 (P = 0.026) for 0.5 mg E2/100 mg P4 at 12 months. These differences between E2/P4 and placebo for the sexual domain in the MITT-VMS population were −0.21 (P = 0.421) for 1 mg E2/100 mg P4 and −0.49 (P = 0.044) for 0.5 mg E2/100 mg P4 at 12 months.
Relationship between MENQOL scores and VMS frequency and severity
Correlations between changes in MENQOL overall and domain scores and changes in moderate to severe VMS frequency and severity from baseline to week 12 were statistically significant (Table 2). The largest correlations were observed between changes in the MENQOL vasomotor domain score and changes in moderate to severe VMS frequency (r = 0.562) and severity (r = 0.554), followed by a moderate correlation between the overall MENQOL score with VMS frequency (r = 0.397) and severity (r = 0.406). Correlations between VMS frequency and severity with the MENQOL physical, psychosocial, and sexual domains were not only smaller but also statistically significant (Table 2).
TABLE 2.
Pearson correlations (r) between changes in MENQOL overall and domain scores and changes in moderate to severe vasomotor symptoms (VMS) frequency and severity
| Change in VMS frequency | Change in VMS severity | |||
| Change in MENQOL | r | P | r | P |
| Overall score | 0.397 | <0.0001 | 0.406 | <0.0001 |
| Vasomotor domain | 0.562 | <0.0001 | 0.554 | <0.0001 |
| Physical domain | 0.260 | <0.0001 | 0.257 | <0.0001 |
| Psychosocial domain | 0.183 | <0.0001 | 0.212 | <0.0001 |
| Sexual domain | 0.159 | <0.0001 | 0.142 | 0.0004 |
MENQOL, menopause-specific quality of life questionnaire.
For all variables, change is from baseline to week 12.
DISCUSSION
In this analysis of the REPLENISH trial, women with moderate to severe VMS who took TX-001HR, an oral capsule combining biosimilar E2 and P4, experienced statistically significant improvements in menopause-related quality of life as measured by MENQOL for up to 12 months. In addition, changes in VMS frequency and severity moderately correlated with changes with the MENQOL vasomotor score, supporting the hypothesis that reducing VMS frequency in postmenopausal women can lead to improvement in their quality of life. With respect to postmenopausal women with vasomotor symptoms, measuring the effects of treatment on quality of life provides valuable information to the prescribing clinician.
HT has been shown to greatly improve quality of life in postmenopausal women with bothersome symptoms.26 Not surprisingly, women with no bothersome symptoms at baseline have no significant improvement in their quality of life with treatment,26 as observed in the Women’ Health Initiative.27,28 Also important for treatment evaluation is the use of appropriate validated menopause-specific tools, such as the MENQOL questionnaire, as opposed to more generic instruments, such as the Medical Outcomes Study 36-item Short-Form Survey (SF-36).26 Although, the SF-36 has been used to evaluate QOL in older populations with chronic disease, it does not address specific menopausal-related outcomes. For the REPLENISH trial here, quality of life outcomes in women with VMS were assessed using the validated menopause-specific MENQOL questionnaire.
A clinically important difference (CID) is the change in a treatment outcome that an individual patient would identify as important and beneficial.29 Some groups have suggested that a change of 1.0 for each of the MENQOL domains is an appropriate threshold for CID.30,31 In this study, the 1.0 CID threshold for the MENQOL vasomotor domain was reached for all women who took TX-001HR from baseline to 12 months as shown by the differences in LS mean change >1.0 observed between TX-001HR and placebo. Therefore, VMS improvements could be considered clinically important and beneficial in women who took the three highest doses of TX-001HR for the treatment of moderate to severe VMS. In addition, women randomized to the two highest TX-001HR doses reported significant improvements in their MENQOL sexual domain after 12 months of treatment.
Although MENQOL is a validated questionnaire25 for the assessment of postmenopausal women's symptoms and is an effective, widely used instrument, some of its weaknesses include its limited focus (symptoms-based), lack of psychometric assessments, and lack of validation across various cultures and populations.32 Despite these limitations, MENQOL remains an appropriate instrument for measuring changes in quality of life that is reliable, valid, practical to administer, easy to score, and specific to postmenopausal women. Other limitations of this study include a study population that was composed of US women only, and a high discontinuation rate (∼30%) at 1 year, which could limit conclusions generated from the longer-term data.
Finally, use of unapproved compounded HT has become the most prevalent form of HT used in the United States by prescription volume, exposing women to risks of inadequately studied and nonstandardized hormone preparations.13 The challenge with these unregulated, compounded “bioidentical” hormones is the lack of safety and efficacy data. For women who prefer to use natural hormones and for clinicians who prefer to prescribe them, the new formulation of E2/P4 in TX-001HR, if approved, may provide a well-studied and FDA-approved option, in contrast with compounded hormone formulations. TX-001HR also combines E2 and P4 in a single oral capsule, which may be more convenient, potentially increasing adherence, which may, in turn, influence effectiveness and, by preventing use of estrogen without progesterone, endometrial safety.33,34
CONCLUSIONS
Data from the REPLENISH trial showed that treatment of moderate to severe VMS with TX-001HR, an oral, continuous-combined dose of E2/P4, significantly improved menopause-related quality of life. In conjunction with previously reported data demonstrating clinically meaningful and statistically significant reductions in moderate to severe VMS with E2/P4, and without increasing the incidence of endometrial hyperplasia,23 these data show that TX-001HR, if approved, may provide the first new oral HT formulation for the treatment of moderate to severe VMS in postmenopausal women with a uterus.
Footnotes
Data Presentation: Presented at The North American Menopause Society annual meeting, October 11-14, 2017, Philadelphia, PA.
Trial Registration: https://clinicaltrials.gov/ct2/show/NCT01942668.
Funding/support: The study was sponsored by TherapeuticsMD (Boca Raton, FL). Writing assistance was provided by Dominique J. Verlaan, PhD and Laura J. Ninger, ELS of Precise Publications, LLC (Bedminster, NJ).
Financial disclosure/conflicts of interest: JAS has served (within the past year, or current) as a consultant/advisor to AbbVie, Allergan, AMAG, Amgen, Ascend Therapeutics, Azure Biotech, Bayer Healthcare, CEEK Enterprises, Covance, Millendo Therapeutics, Mitsubishi Tanage, ObsEva SA, Radius Health, Sanofi SA, Sebela, Sermonix, Shionogi, Symbiotec Pharmalab, TherapeuticsMD, and Valeant; and has received (within the past year, or current) grant/research support from AbbVie, Agile Therapeutics, Allergan, Bayer Healthcare, New England Research Institute, ObsEva SA, Palatin Technologies, Symbio Research, and TherapeuticsMD; and has also served (within the past year, or current) on the speaker's bureaus of Duchesnay, Novo Nordisk, Shionogi, and Valeant; and is a stockholder (direct purchase) in Sermonix Pharmaceuticals. AMK (in the past or current year) served as a consultant to or on the advisory boards of AMAG Pharmaceuticals, Bayer Healthcare, Mithra, and Shionogi Inc; and has received research support (to University of FL) from Allergan, Bayer Healthcare, and TherapeuticsMD. RK has received research support or consulting fees from AbbVie Inc, Actavis, Bayer Healthcare, Endoceutics, Palatin Technologies, Shionogi Inc, Teva, TherapeuticsMD, and Trimel. SG, BB, and SM are current full-time employees of TherapeuticsMD with stock/stock options. BB is also a board member of TherapeuticsMD.
REFERENCES
- 1.Blumel JE, Chedraui P, Baron G, et al. A large multinational study of vasomotor symptom prevalence, duration, and impact on quality of life in middle-aged women. Menopause 2011; 18:778–785. [DOI] [PubMed] [Google Scholar]
- 2.Hunter MS, Gentry-Maharaj A, Ryan A, et al. Prevalence, frequency and problem rating of hot flushes persist in older postmenopausal women: impact of age, body mass index, hysterectomy, hormone therapy use, lifestyle and mood in a cross-sectional cohort study of 10,418 British women aged 54-65. BJOG 2012; 119:40–50. [DOI] [PubMed] [Google Scholar]
- 3.Duffy OK, Iversen L, Hannaford P. The impact and management of symptoms experienced at midlife: a community-based study of women in northeast Scotland. BJOG 2012; 119:554–564. [DOI] [PubMed] [Google Scholar]
- 4.Whiteley J, Wagner JS, Bushmakin A, Kopenhafer L, Dibonaventura M, Racketa J. Impact of the severity of vasomotor symptoms on health status, resource use, and productivity. Menopause 2013; 20:518–524. [DOI] [PubMed] [Google Scholar]
- 5.Blumel JE, Cano A, Mezones-Holguin E, et al. A multinational study of sleep disorders during female mid-life. Maturitas 2012; 72:359–366. [DOI] [PubMed] [Google Scholar]
- 6.Kleinman NL, Rohrbacker NJ, Bushmakin AG, Whiteley J, Lynch WD, Shah SN. Direct and indirect costs of women diagnosed with menopause symptoms. J Occup Environ Med 2013; 55:465–470. [DOI] [PubMed] [Google Scholar]
- 7.Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA 2002; 288:321–333. [DOI] [PubMed] [Google Scholar]
- 8.Steinkellner AR, Denison SE, Eldridge SL, Lenzi LL, Chen W, Bowlin SJ. A decade of postmenopausal hormone therapy prescribing in the United States: long-term effects of the Women's Health Initiative. Menopause 2012; 19:616–621. [DOI] [PubMed] [Google Scholar]
- 9.Gass ML, Stuenkel CA, Utian WH, et al. Use of compounded hormone therapy in the United States: report of The North American Menopause Society Survey. Menopause 2015; 22:1276–1284. [DOI] [PubMed] [Google Scholar]
- 10.Fishman JR, Flatt MA, Settersten RA., Jr Bioidentical hormones, menopausal women, and the lure of the “natural” in U.S. anti-aging medicine. Soc Sci Med 2015; 132:79–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Committee on Gynecologic Practice and the American Society for Reproductive Medicine Practice Committee Committee Opinion No. 532: Compounded bioidentical menopausal hormone therapy. Obstet Gynecol 2012; 120:411–415. [DOI] [PubMed] [Google Scholar]
- 12.Manson JE, Kaunitz AM. Menopause management—getting clinical care back on track. N Engl J Med 2016; 374:803–806. [DOI] [PubMed] [Google Scholar]
- 13.Pinkerton J, Santoro N. Compounded bioidentical hormone therapy: identifying use trends and knowledge gaps among US women. Menopause 2015; 22:926–936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pinkerton JV, Pickar JH. Update on medical and regulatory issues pertaining to compounded and FDA-approved drugs, including hormone therapy. Menopause 2016; 23:215–223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Eden JA, Hacker NF, Fortune M. Three cases of endometrial cancer associated with “bioidentical” hormone replacement therapy. Med J Aust 2007; 187:244–245. [DOI] [PubMed] [Google Scholar]
- 16.Davis R, Batur P, Thacker HL. Risks and effectiveness of compounded bioidentical hormone therapy: a case series. J Womens Health (Larchmt) 2014; 23:642–648. [DOI] [PubMed] [Google Scholar]
- 17.Dezman VL, Gersak MZ, Gersak K. Two case of atypical endometrial hyperplasia associated with “bioidentical” hormone replacement therapy: IGCS-0084 Uterine Cancer, including Sarcoma. Int J Gynecol Cancer 2015; 25 Suppl. 1:71. [DOI] [PubMed] [Google Scholar]
- 18.Stuenkel C, Manson J. Compounded bioidentical hormone therapy: does the regulatory double standard harm women? JAMA Intern Med 2017; 177:1719-1720. [DOI] [PubMed] [Google Scholar]
- 19.Cordina-Duverger E, Truong T, Anger A, et al. Risk of breast cancer by type of menopausal hormone therapy: a case-control study among post-menopausal women in France. PLoS One 2013; 8:e78016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat 2008; 107:103–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol 2010; 30:340–345. [DOI] [PubMed] [Google Scholar]
- 22.Pickar JH, Bon C, Amadio JM, Mirkin S, Bernick B. Pharmacokinetics of the first combination 17beta-estradiol/progesterone capsule in clinical development for menopausal hormone therapy. Menopause 2015; 22:1308–1316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lobo RA, Archer DF, Kagan R, et al. A 17beta-estradiol-progesterone oral capsule for vasomotor symptoms in postmenopausal women: a randomized controlled trial. Obstet Gynecol 2018; 132:161–170. [DOI] [PubMed] [Google Scholar]
- 24.Williams RE, Kalilani L, DiBenedetti DB, Zhou X, Fehnel SE, Clark RV. Healthcare seeking and treatment for menopausal symptoms in the United States. Maturitas 2007; 58:348–358. [DOI] [PubMed] [Google Scholar]
- 25.Hilditch JR, Lewis J, Peter A, et al. A menopause-specific quality of life questionnaire: development and psychometric properties. Maturitas 1996; 24:161–175. [DOI] [PubMed] [Google Scholar]
- 26.Utian WH, Woods NF. Impact of hormone therapy on quality of life after menopause. Menopause 2013; 20:1098–1105. [DOI] [PubMed] [Google Scholar]
- 27.Hays J, Ockene JK, Brunner RL, et al. Effects of estrogen plus progestin on health-related quality of life. N Engl J Med 2003; 348:1839–1854. [DOI] [PubMed] [Google Scholar]
- 28.Brunner RL, Gass M, Aragaki A, et al. Effects of conjugated equine estrogen on health-related quality of life in postmenopausal women with hysterectomy: results from the Women's Health Initiative Randomized Clinical Trial. Arch Intern Med 2005; 165:1976–1986. [DOI] [PubMed] [Google Scholar]
- 29.Guyatt G, Walter S, Norman G. Measuring change over time: assessing the usefulness of evaluative instruments. J Chronic Dis 1987; 40:171–178. [DOI] [PubMed] [Google Scholar]
- 30.Juniper EF, Guyatt GH, Willan A, Griffith LE. Determining a minimal important change in a disease-specific Quality of Life Questionnaire. J Clin Epidemiol 1994; 47:81–87. [DOI] [PubMed] [Google Scholar]
- 31.Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials 1989; 10:407–415. [DOI] [PubMed] [Google Scholar]
- 32.Utian WH, Janata JW, Kingsberg SA, Schluchter M, Hamilton JC. The Utian Quality of Life (UQOL) Scale: development and validation of an instrument to quantify quality of life through and beyond menopause. Menopause 2002; 9:402–410. [DOI] [PubMed] [Google Scholar]
- 33.Sutton SS, Hardin JW, Bramley TJ, D'Souza AO, Bennett CL. Single- versus multiple-tablet HIV regimens: adherence and hospitalization risks. Am J Manag Care 2016; 22:242–248. [PubMed] [Google Scholar]
- 34.Coca A, Agabiti-Rosei E, Cifkova R, Manolis AJ, Redon J, Mancia G. The polypill in cardiovascular prevention: evidence, limitations and perspective—position paper of the European Society of Hypertension. J Hypertens 2017; 35:1546–1553. [DOI] [PubMed] [Google Scholar]