

Abstract
Background
Vitamin B12 deficiency is common, and the incidence increases with age. Most people with vitamin B12 deficiency are treated in primary care with intramuscular (IM) vitamin B12. Doctors may not be prescribing oral vitamin B12 formulations because they may be unaware of this option or have concerns regarding its effectiveness.
Objectives
To assess the effects of oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency.
Search methods
We searched CENTRAL, MEDLINE, Embase, and LILACS, as well as the WHO ICTRP and ClinicalTrials.gov. The latest search date was 17 July 2017. We applied no language restrictions. We also contacted authors of relevant trials to enquire about other published or unpublished studies and ongoing trials.
Selection criteria
Randomised controlled trials (RCTs) comparing the effect of oral versus IM vitamin B12 for vitamin B12 deficiency.
Data collection and analysis
We used standard methodological procedures expected by Cochrane. Our primary outcomes were serum vitamin B12 levels, clinical signs and symptoms of vitamin B12 deficiency, and adverse events. Secondary outcomes were health‐related quality of life, acceptability to patients, haemoglobin and mean corpuscular volume, total homocysteine and serum methylmalonic acid levels, and socioeconomic effects. We used GRADE to assess the quality of the evidence for important outcomes. We did not perform meta‐analyses due to the small number of included trials and substantial clinical heterogeneity.
Main results
Three RCTs met our inclusion criteria. The trials randomised 153 participants (74 participants to oral vitamin B12 and 79 participants to IM vitamin B12). Treatment duration and follow‐up ranged between three and four months. The mean age of participants ranged from 38.6 to 72 years. The treatment frequency and daily dose of vitamin B12 in the oral and IM groups varied among trials. Only one trial had low or unclear risk of bias across all domains and outcome measures. Two trials reported data for serum vitamin B12 levels. The overall quality of evidence for this outcome was low due to serious imprecision (low number of trials and participants). In two trials employing 1000 μg/day oral vitamin B12, there was no clinically relevant difference in vitamin B12 levels when compared with IM vitamin B12. One trial used 2000 μg/day vitamin B12 and demonstrated a mean difference of 680 pg/mL (95% confidence interval 392.7 to 967.3) in favour of oral vitamin B12. Two trials reported data on adverse events (very low‐quality evidence due to risk of performance bias, detection bias, and serious imprecision). One trial stated that no treatment‐related adverse events were seen in both the oral and IM vitamin B12 groups. One trial reported that 2 of 30 participants (6.7%) in the oral vitamin B12 group left the trial early due to adverse events. Orally taken vitamin B12 showed lower treatment‐associated costs than IM vitamin B12 in one trial (low‐quality evidence due to serious imprecision). No trial reported on clinical signs and symptoms of vitamin B12 deficiency, health‐related quality of life, or acceptability of the treatment scheme.
Authors' conclusions
Low quality evidence shows oral and IM vitamin B12 having similar effects in terms of normalising serum vitamin B12 levels, but oral treatment costs less. We found very low‐quality evidence that oral vitamin B12 appears as safe as IM vitamin B12. Further trials should conduct better randomisation and blinding procedures, recruit more participants, and provide adequate reporting. Future trials should also measure important outcomes such as the clinical signs and symptoms of vitamin B12 deficiency, health related‐quality of life, socioeconomic effects, and report adverse events adequately, preferably in a primary care setting.
Plain language summary
Oral vitamin B12 compared with intramuscular vitamin B12 for vitamin B12 deficiency
Review question
Does oral vitamin B12 have similar effects as intramuscular injections of vitamin B12 for people with vitamin B12 deficiency?
Background
Vitamin B12 (cobalamin) is necessary for basic body functions, such as the growth and development of red blood cells and the nervous system. Vitamin B12 deficiency (a lack of vitamin B12) is very common. Many factors contribute to vitamin B12 deficiency, such as age, blood disease, vegetarian diet, indigestion, use of drugs, as well as poor nutrition. Doctors are more likely to give vitamin B12 using injections into the muscle (intramuscular injection) because they may be unaware of the option to use oral vitamin B12 or uncertain about how well it works.
Study characteristics
We found three randomised controlled studies (clinical studies where people are randomly put into one of two or more treatment groups). The studies randomised 153 participants (74 participants to oral vitamin B12 and 79 participants to intramuscular vitamin B12). Treatment duration and follow‐up ranged between three and four months. The mean age of participants ranged from 39 to 72 years.
Key results
Two studies used 1000 μg/day oral vitamin B12 and showed no relevant difference to intramuscularly applied vitamin B12 with regard to vitamin B12 blood levels. One trial used 2000 μg/day vitamin B12 and showed higher vitamin B12 blood levels in favour of oral vitamin B12. Two studies reported side effects. One study stated that no treatment‐related side effects were seen in both the oral and intramuscular vitamin B12 groups. One study reported that 2 of 30 participants in the oral vitamin B12 group left the trial early due to side effects. Orally taken vitamin B12 showed lower treatment‐associated costs than intramuscular vitamin B12 in one trial. No study reported on clinical signs and symptoms of vitamin B12 deficiency (e.g. fatigue, depression, neurological complications), health‐related quality of life, or acceptability of the treatment scheme.
Quality of the evidence
The overall quality of the evidence was low or very low, mainly due to the small number of included studies and the low numbers of participants in these studies.
Summary of findings
Summary of findings for the main comparison. Oral versus intramuscular vitamin B12 for vitamin B12 deficiency.
| Oral versus intramuscular vitamin B12 for vitamin B12 deficiency | ||||||
|
Patient: people with vitamin B12 deficiency
Setting: outpatients Intervention: oral versus IM vitamin B12 | ||||||
| Outcomes | IM vitamin B12 | Oral vitamin B12 | Relative effect (95% CI) | No. of participants (trials) | Quality of the evidence (GRADE) | Comments |
|
Serum vitamin B12 levels Normal value: > 300 pg/mL (> 221 pmol/L) Follow‐up: 90 days and 4 months |
See comment | See comment | Not estimable | 153 (3) | ⊕⊕⊝⊝ lowa | 1 trial (60 participants) used 1000 μg/day oral or IM vitamin B12 (total dose 15 mg): MD was ‐11.7 pg/mL (95% CI ‐29.5 to 6.1) (Bolaman 2003). 1 trial (33 participants) used 2000 μg/day vitamin B12 (total dose 240 mg) or 1000 μg/day IM vitamin B12 (total dose 9 mg): MD was 680 pg/mL (95% CI 392.7 to 967.3) in favour of oral vitamin B12 (Kuzminski 1998). 1 trial (60 participants) (using 1000 μg/day oral or IM vitamin B12 (total dose 90 mg and 15 mg, oral and IM respectively) reported that 27/30 in the IM vitamin B12 group (90%) and 20/30 in the oral vitamin B12 group (66.7%) achieved normalisation of serum vitamin B12, defined as ≥ 200 pg/mL (Saraswathy 2012). |
| Clinical signs and symptoms | Not reported | |||||
| Adverse events Follow‐up: 90 days and 3 months | See comment | See comment | Not estimable | 120 (2) | ⊕⊝⊝⊝ very lowb |
Bolaman 2003 reported no treatment‐related adverse events in both the oral and IM vitamin B12 groups. Saraswathy 2012 reported that 2/30 participants (6.7%) in the oral vitamin B12 group left the trial early due to adverse events. |
| Health‐related quality of life | Not reported | |||||
| Acceptability | Not reported | |||||
|
Socioeconomic effects Follow‐up: 90 days |
See comment | See comment | Not estimable | 60 (1) | ⊕⊕⊝⊝ lowc | Only 1 trial reported data for this outcome (Bolaman 2003). The costs per treatment were USD 80 per person in the oral vitamin B12 group compared with USD 220 per person in the IM group. |
| CI: confidence interval; IM: intramuscular; MD: mean difference | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
aDowngraded by two levels due to serious imprecision (low numbers of trials and participants); see Appendix 12. bDowngraded by three levels due to risk of bias (performance bias, detection bias) and serious imprecision (low numbers of trials and participants); see Appendix 12. cDowngraded by two levels due to serious imprecision (low numbers of trials and participants); see Appendix 12.
Background
Description of the condition
Vitamins are a group of substances required for effective human metabolism. Under normal circumstances it is essential that they are present in a person's diet because, with few exceptions, the human body is unable to manufacture them. Vitamins often work together with enzymes, cofactors, and other substances. Vitamin B12 (cobalamin) is necessary for the development of red blood cells, growth, and nervous system maintenance. The only dietary sources of vitamin B12 are animal products, such as eggs, fish, and meats. Daily requirements are age‐related: the recommended dietary amounts for adults and infants are 1.5 µg and 0.4 µg, respectively (Anonymous 1991; FAO/WHO 1988).
Vitamin B12 is absorbed in the terminal ileum. This absorption is almost entirely dependent upon the intrinsic factor, a glycoprotein secreted by parietal cells situated in the mucosa of the stomach. Intrinsic factor binds to vitamin B12, and the complex is transported across the cell membrane bound to another glycoprotein called transcobalamin. The most common cause of vitamin B12 deficiency is autoimmune pernicious anaemia, a condition that carries an increased risk of gastric cancer. In pernicious anaemia, absorption is impaired due to intrinsic factor deficiency arising from autoimmune destruction of parietal cells. Other common causes of vitamin B12 deficiency include gastrectomy, ileal resection, pancreatic insufficiency, and malabsorption syndromes including Crohn's disease and celiac disease. Other less common causes of vitamin B12 deficiency include use of drugs such as biguanides (metformin), antacids (proton pump inhibitors and H2 receptors antagonists), aminoglycoside, antibiotics and colchicines, and rarely, malabsorption due to gastrointestinal bacterial overgrowth, congenital defects (e.g. birth transcobalamin deficiency), and infestation. Pure nutritional deficiency is rare and usually occurs only in strict vegans (Watanabe 2013). In some cases, vitamin B12 deficiency can be a risk factor for cardiovascular disease (Pawlak 2015). It is recommended that vegetarians take vitamin B12 supplements to prevent vitamin B12 deficiency (Pawlak 2013).
The prevalence of vitamin B12 deficiency varies among countries, and manifests in population groups when the vitamin B12 demand increases whilst the intake remains unchanged or is reduced, such as in infants, pregnant women, and the elderly. The incidence of vitamin B12 deficiency increases with age, probably due to the fact that elderly people are more likely to suffer from food‐cobalamin malabsorption. This malabsorption is caused primarily by gastric atrophy but also by chronic carriage of Helicobacter pylori, long‐term ingestion of metformin and proton pump inhibitors, and increased chances of having gastric surgery (Andres 2004; De Jager 2010; Lam 2013). The prevalence of vitamin B12 deficiency in the elderly varies substantially in different studies, with reported figures between 1.5% and 15% (Brito 2015; Clarke 2004; Figlin 2003; MacFarlane 2011; Pennypacker 1992; Rajan 2002; van Walraven 1999). The differences may be due to inconsistent diagnostic criteria for vitamin B12 deficiency.
As well as varying with age, prevalence also varies with gender and ethnic group: elderly men are more likely to have low vitamin B12 levels than elderly women. The prevalence of vitamin B12 deficiency is higher in Europe than in the USA (Lindenbaum 1994; Pennypacker 1992). African and Asian countries have the highest rates of vitamin B12 deficiency, for example both Kenyan and Indian schoolchildren have a rate above 70%, as well as Indian adults (Allen 2009).
Vitamin B12 is a cofactor to methylation, which facilitates DNA synthesis and haemopoiesis and maintains neurological function (Green 2013). Vitamin B12 deficiency can cause serious clinical symptoms such as megaloblastic anaemia, paralysis, dementia, fatigue, and mood disturbance. If left untreated, serious neurological and neuropsychiatric complications can occur. Vitamin B12 deficiency has also been linked with an increased risk of myocardial infarction and stroke. A recent study reported that there is a relationship between vitamin B12 deficiency and delirium in elderly patients undergoing cardiac surgery (Schroll 2015).
The diagnosis of vitamin B12 deficiency is based mainly on blood measurements of serum vitamin B12 level less than 200 pg/mL (148 pmol/L), complemented with second‐line tests including total homocysteine and methylmalonic acid levels, which are metabolic indicators of vitamin B12 deficiency. Studies have indicated that an estimated 20% of people can present with neuropsychiatric symptoms in the absence of haematological abnormalities (Quadros 2010).
Description of the intervention
Vitamin B12 was first isolated in its cyano‐form in 1948 (Rickes 1948; Smith 1948), and is now widely used for the treatment of vitamin B12 deficiency. Most vitamin B12‐deficient individuals in the UK and other countries are treated with intramuscular vitamin B12, and vitamin B12 replacement has been traditionally administered intramuscularly. Intramuscular vitamin B12 can be administered in two different forms: cyanocobalamin and hydroxocobalamin. In some countries hydroxocobalamin has completely replaced cyanocobalamin as first choice for vitamin B12 therapy because it is retained in the body longer and can be administered at intervals of up to three months (BNF 2004).
Several case control and case series studies have since suggested that oral vitamin B12 has an equal efficacy and safety as intramuscular vitamin B12 (Andres 2010; Bahadir 2015; Bolaman 2003; Castelli 2011; Kuzminski 1998). However, despite its availability in most countries and its very safe track record, vitamin B12 is rarely prescribed in the oral form. Two exceptions to this are in Canada and Sweden, where in the year 2000 oral vitamin B12 accounted for 73% of the total vitamin B12 prescribed (Nilsson 2005). Possible reasons for doctors not prescribing oral formulations may include a lack of awareness of this option or concerns regarding unpredictable absorption (Graham 2007; Lederle 1998). In the UK, oral vitamin B12 is currently not available on National Health Service (NHS) prescription in high‐dose formulations.
Adverse effects of the intervention
Intramuscular vitamin B12 can cause significant pain, especially in thin people (Elia 1998). While serious adverse reactions are rare, injections can be dangerous in anticoagulated individuals. No adverse effects of oral administration have been reported (Andres 2010).
How the intervention might work
The mechanism for the intramuscular route is most probably that vitamin B12 can be absorbed and transported by fluid diffusion. Doctors traditionally believed that the main reasons of vitamin B12 deficiency were that the patients were lacking intrinsic factor or had gastrointestinal disease or bowel resection. Gastrointestinal absorption barriers of vitamin B12 can be avoided by intramuscular injection.
The mechanism for the oral route is most probably that free vitamin B12 can be absorbed both passively (without binding to intrinsic factor) as well as actively (following binding to intrinsic factor) in the terminal ileum. Passive diffusion accounts for 1.2% of total absorption with a bioavailability unaffected in people with pernicious anaemia or gastro‐duodenal surgical resection (Berlin 1968; Berlin 1978). High doses of oral vitamin B12 (e.g. 1000 µg daily) may be able to produce adequate absorption of vitamin B12 even in the presence of intrinsic factor deficiency, and therefore may be an alternative to the intramuscular route for many people.
Why it is important to do this review
This review is an update of the Cochrane Review comparing oral with intramuscular vitamin B12 published in 2005 (Vidal‐Alaball 2005). The original review suggested that high doses of oral vitamin B12 may be as effective as intramuscular administration in obtaining short‐term haematological and neurological responses in vitamin B12‐deficient people.
Intramuscular injections are a "considerable source of work" for healthcare professionals, mainly general practitioners and community nurses (Middleton 1985). There is little difference in the cost of oral versus intramuscular therapy when the medication alone is considered. However, intramuscular administration often involves a special trip to a health facility or a home visit by a health professional to administer the injection (Houle 2014). Oral treatment could therefore save considerable health service resources.
A recent Canadian study estimated that converting people aged over 65 years on B12 replacement from the intramuscular to oral form could save CAD 13,975,883, even if no additional physician visits were billed for people receiving intramuscular therapy. A total of CAD 8,444,346 could be saved from reduced administration costs alone over five years (Houle 2014).
Objectives
To assess the effects of oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled clinical trials examining the use of oral versus intramuscular vitamin B12 to treat vitamin B12 deficiency. We regarded a two‐week treatment duration as minimum trial duration.
We excluded trials examining the role of vitamin B12 in the prevention of cardiovascular diseases, because the dose of vitamin B12 used in those trials may be different from the dose used to treat vitamin B12 deficiency, and the majority of participants included in such trials are not vitamin B12 deficient.
Types of participants
Trial participants with vitamin B12 deficiency, meeting criteria for vitamin B12 replacement therapy.
Diagnostic criteria for vitamin B12 deficiency
We used a cut‐off point of below 200 pg/mL (below 148 pmol/L) as a threshold serum level for vitamin B12 deficiency.
Excluded populations
We excluded trials with participants with:
primary folate deficiency, because the concomitant use of folate might confound the metabolic outcome measures;
end‐stage renal disease or on haemodialysis, because renal disease might confound the metabolic outcome measures.
Types of interventions
Intervention
Oral vitamin B12
Comparator
Intramuscular vitamin B12
Where a trial included multiple arms, we included any arm that met the inclusion criteria of our review.
Minimum duration of intervention
We defined minimum trial duration as two weeks, and only included trials with interventions that lasted longer than two weeks. We planned to list trials with less than two weeks duration in an Additional table but not include them in the analyses, however we did not encounter any such trials.
Types of outcome measures
We analysed the following outcomes in the review, but did not use them as a basis for including or excluding studies. Had we found relevant trials not reporting any of our primary or secondary outcomes, we would have included the trials but we would not have evaluated them in detail.
Primary outcomes
Serum vitamin B12 levels.
Clinical signs and symptoms of vitamin B12 deficiency.
Adverse events.
Secondary outcomes
Health‐related quality of life.
Acceptability.
Haemoglobin and mean corpuscular volume (MCV).
Total homocysteine and serum methylmalonic acid levels.
Socioeconomic effects.
Method and timing of outcome measurement
All outcomes required a minimum of two weeks follow‐up from baseline. We categorised the time points of outcome measurement as short term (two weeks to three months), medium term (three to nine months), and long term (more than nine months).
Serum vitamin B12 levels: measured at the end of study (mean values and whether these were normalised; normalised serum vitamin B12 was defined as > 240 pg/mL).
Clinical signs and symptoms of vitamin B12 deficiency: e.g. fatigue, macrocytosis, pancytopenia, depression, tiredness, paralysis, dementia psychosis measured at short, medium, and long term.
Adverse events: e.g. itching, exanthema, chills, fever, hot flushes, nausea, dizziness, and anaphylaxis and measured at short, medium, and long term.
Health‐related quality of life: evaluated by a validated instrument such as 36‐item Short Form Health Survey (SF‐36) and measured at short, medium, and long term.
Acceptability: acceptability to participants as defined by trial authors and measured at short, medium, and long term.
Haemoglobin and MCV: measured at short, medium, and long term.
Total homocysteine and serum methylmalonic acid levels: measured at short, medium, and long term.
Socioeconomic effects: refer to costs and measured at short, medium, and long term.
Summary of findings
We presented a 'Summary of findings' table reporting the following outcomes, listed according to priority.
Serum vitamin B12 levels.
Clinical signs and symptoms of vitamin B12 deficiency (such as depression, tiredness, paralysis, or dementia).
Adverse events.
Health‐related quality of life.
Acceptability.
Socioeconomic effects.
Search methods for identification of studies
Electronic searches
We searched the following sources between the specified dates and placed no restrictions on the language of publication.
-
Cochrane Library
Cochrane Central Register of Controlled Trials (CENTRAL) (2005 to issue 6 of 12, June 2017; search date 17 July 2017)
Database of Abstracts of Reviews of Effects (DARE) (2005 to issue 2 of 4, April 2015; search date 22 July 2015)
Health Technology Assessment Database (2005 to issue 2 of 4, April 2015; search date 22 July 2015)
NHS Economic Evaluation Database (2005 to issue 2 of 4, April 2015; search date 22 July 2015)
Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R) <1946 to present> (1 December 2014 to 17 July 2017)
Embase <1974 to 2016 November 09> (2004 Week 48 to 10 November 2016)
LILACS (Latin American and Caribbean Health Sciences Literature database) (<last update 27 October 2006>) (Inception to 10 November 2016)
ClinicalTrials.gov (clinicaltrials.gov) (search date 17 July 2017)
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (apps.who.int/trialsearch/) (search date 10 November 2016)
We continuously applied a MEDLINE (via Ovid) email alert service established by the Cochrane Metabolic and Endocrine Disorders (CMED) Group to identify newly published studies using the same search strategy as described for MEDLINE (for details on search strategies, see Appendix 1).
Searching other resources
We attempted to identify other potentially eligible trials or ancillary publications by searching the reference lists of retrieved included trials, systematic reviews, meta‐analyses, and health technology assessment reports. In addition, we contacted authors of included trials to identify any further published or unpublished trials and ongoing trials that we may have missed.
Data collection and analysis
Selection of studies
For this update, two review authors (HYW and THL) independently scanned the abstract or title, or both, of every record retrieved, to determine which studies should assessed further. We investigated the full‐text articles of all potentially relevant articles. Any discrepancies were resolved through consensus or by recourse to a third review author (YNS). If we could not resolve a disagreement, we categorised the study as a 'study awaiting classification' and contacted the study authors for clarification. We have presented an adapted PRISMA flow diagram to show the process of study selection (Figure 1) (Liberati 2009).
1.
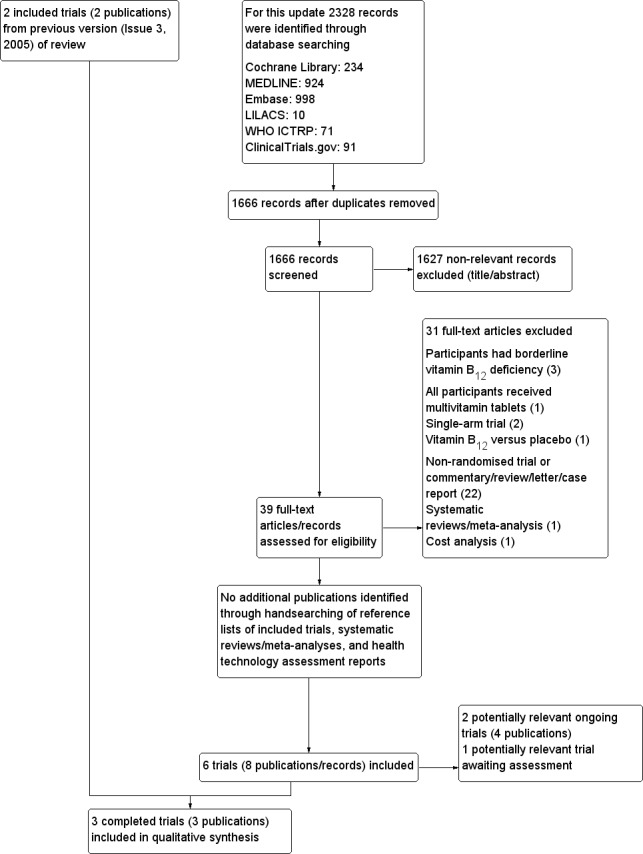
Study flow diagram.
Data extraction and management
For trials that fulfilled the inclusion criteria, two review authors (LYL and LLQ) independently extracted key participant and intervention characteristics and outcomes. We included key characteristics of the trials, such as trial design, setting, sample size, population, and how outcomes were defined or collected in the trials. In addition, we also collected data on the method of diagnosing vitamin B12 deficiency, any pre‐existing treatment and titration period.
We reported data on efficacy outcomes and adverse events using standard data extraction templates supplied by the CMED Group (for details see Characteristics of included studies; Table 2; Appendix 2; Appendix 3; Appendix 4; Appendix 5; Appendix 6; Appendix 7; Appendix 8; Appendix 9; Appendix 10). Any disagreements were resolved by discussion or, if required, by consultation with a third review author (YNS).
1. Overview of trial populations.
| Intervention(s) and comparator(s) | Description of power and sample size calculation | Screened/eligible (N) | Randomised (N) | Analysed (N) | Finishing trial (N) | Randomised finishing trial (%) | Follow‐up (extended follow‐up)a | |
|
Bolaman 2003 (parallel RCT) |
I: 1000 µg oral vitamin B12 | — | — | 26 | 26 | 26 | 100 | 90 days (none) |
| C: 1000 µg IM vitamin B12 | 34 | 34 | 34 | 100 | ||||
| Total: | 60b | 60 | 60 | 100 | ||||
|
Kuzminski 1998 (parallel RCT) |
I: 2000 µg oral vitamin B12 | — | 138 | 18 | 18 | 18 | 100 | 4 months (none) |
| C: 1000 µg IM vitamin B12 | 15 | 15 | 15 | 100 | ||||
| Total: | 33c | 33 | 33 | 100 | ||||
|
Saraswathy 2012 (parallel RCT) |
I: 1000 μg oral vitamin B12 | "Sample size was estimated to be 23 in each study arm, assuming equal response of 90% and non inferiority margin of 25% /alpha = 0.25, 1‐beta = 80%)" | — | 30 | 22 | 22 | 73 | 3 months (none) |
| C: 1000 μg IM vitamin B12 | 30 | 27 | 27 | 90 | ||||
| Total: | 60 | 49 | 49 | 82 | ||||
| Grand total | All interventions | 74 | 66 | |||||
| All comparators | 79 | 76 | ||||||
| All interventions and comparators | 153 | 142 | ||||||
— denotes not reported
C: comparator; I: intervention; IM: intramuscular; RCT: randomised controlled trial
aFollow‐up under randomised conditions until end of trial (= duration of intervention + follow‐up postintervention or identical to duration of intervention); extended follow‐up refers to follow‐up of participants once the original trial was terminated as specified in the power calculation. bOf 70 participants enrolled in the trial, 10 were excluded because of failure to appear for follow‐up after 10 days of treatment. c38 participants were randomised; after completion of the trial 5 participants were judged to have primary folate deficiency rather than vitamin B12 deficiency and were excluded from the final analysis.
We provided information about potentially relevant ongoing studies, including the trial identifier number, in the Characteristics of ongoing studies and in Appendix 5 (matrix of trial endpoints (publications and trial documents)). We attempted to find the protocol for each included study and reported primary, secondary, and other outcomes in comparison with data in publications in Appendix 5 .
We emailed all authors of the included trials to enquire whether they would be willing to answer questions regarding their trials. Appendix 11 shows the results of this survey. Thereafter, when required, we sought relevant missing information on the trial from the primary author(s) of the article.
Dealing with duplicate and companion publications
In the event of duplicate publications, companion documents, or multiple reports of a primary study, we planned to maximise the information yield by collating all available data and using the most complete data set aggregated across all known publications. We listed duplicate publications, companion documents, or multiple reports of a primary trial as secondary references under the study ID of the included or excluded trial.
Data from clinical trial registers
In cases where the data of included trials were available as study results in clinical trial registers such as ClinicalTrials.gov or similar sources, we planned to make full use of this information and used this to extract data. If there was also a full publication of the trial, we collated and critically appraised all available data. If an included trial was marked as a completed study in a clinical trial register but no additional information was available, we added this trial to the Characteristics of studies awaiting classification table.
Assessment of risk of bias in included studies
Two review authors (LYL and LLQ) independently assessed the risk of bias of each included study. Any disagreements were resolved by consensus, or by consultation with a third review author (YNS). If adequate information was not available from the publications or trial protocols, we contacted trial authors for missing data on 'Risk of bias' items. We contacted authors of included studies but not due to inadequate information on 'Risk of bias' items.
Using the Cochrane 'Risk of bias' assessment tool (Higgins 2011a; Higgins 2011b), we judged 'Risk of bias' criteria as having either low, high, or unclear risk, evaluating the individual bias items described in the Cochrane Handbook for Systematic Reviews of Interventions according to the criteria and associated categorisations contained therein (Higgins 2011a).
Random sequence generation (selection bias due to inadequate generation of a randomised sequence) ‐ assessment at trial level
For each included trial we described the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
Low risk of bias: the sequence generation was achieved using computer‐generated random numbers or a random numbers table. Drawing of lots, tossing a coin, shuffling cards or envelopes, and throwing dice are adequate if performed by an independent person not otherwise involved in the trial. We considered the use of the minimisation technique as equivalent to being random.
Unclear risk of bias: insufficient information about the sequence generation process.
High risk of bias: the sequence generation method was non‐random or quasi‐random (e.g. sequence generated by odd or even date of birth; sequence generated by some rule based on date (or day) of admission; sequence generated by some rule based on hospital or clinic record number; allocation by judgement of the clinician; allocation by preference of the participant; allocation based on the results of a laboratory test or a series of tests; allocation by availability of the intervention).
Allocation concealment (selection bias due to inadequate concealment of allocation prior to assignment) ‐ assessment at trial level
For each included trial we described the method used to conceal allocation to interventions prior to assignment and assessed whether intervention allocation could have been foreseen in advance of or during recruitment, or changed after assignment.
Low risk of bias: central allocation (including telephone, interactive voice‐recorder, web‐based, and pharmacy‐controlled randomisation); sequentially numbered drug containers of identical appearance; sequentially numbered, opaque, sealed envelopes.
Unclear risk of bias: insufficient information about the allocation concealment.
High risk of bias: using an open random allocation schedule (e.g. a list of random numbers); assignment envelopes were used without appropriate safeguards; alternation or rotation; date of birth; case record number; any other explicitly unconcealed procedure.
Blinding of participants and study personnel (performance bias due to knowledge of the allocated interventions by participants and personnel during the trial) ‐ assessment at outcome level
We evaluated the risk of detection bias separately for each outcome (Hróbjartsson 2013). We noted whether endpoints were self reported, investigator assessed, or adjudicated outcome measures (see below).
Low risk of bias: blinding of participants and key study personnel ensured, and unlikely that the blinding could have been broken; no blinding or incomplete blinding, but the review authors judge that the outcome is not likely to be influenced by lack of blinding.
Unclear risk of bias: insufficient information about the blinding of participants and study personnel; the trial did not address this outcome.
High risk of bias: no blinding or incomplete blinding, and the outcome is likely to be influenced by lack of blinding; blinding of trial participants and key personnel attempted, but likely that the blinding could have been broken, and the outcome is likely to be influenced by lack of blinding.
Blinding of outcome assessment (detection bias due to knowledge of the allocated interventions by outcome assessment) ‐ assessment at outcome level
We evaluated the risk of detection bias separately for each outcome (Hróbjartsson 2013). We noted whether endpoints were self reported, investigator assessed, or adjudicated outcome measures (see below).
Low risk of bias: blinding of outcome assessment ensured, and unlikely that the blinding could have been broken; no blinding of outcome assessment, but the review authors judge that the outcome measurement is not likely to be influenced by lack of blinding.
Unclear risk of bias: insufficient information about the blinding of outcome assessors; the trial did not address this outcome.
High risk of bias: no blinding of outcome assessment, and the outcome measurement was likely to be influenced by lack of blinding; blinding of outcome assessment, but likely that the blinding could have been broken, and the outcome measurement is likely to be influenced by lack of blinding.
Incomplete outcome data (attrition bias due to amount, nature, or handling of incomplete outcome data) ‐ assessment at outcome level
For each included trial and for each outcome, we described the completeness of data, including attrition and exclusions from the analysis. We stated whether trials reported attrition and exclusions, and the number of participants included in the analysis at each stage (compared with the number of randomised participants per intervention/comparator groups). We also noted if trials reported the reasons for attrition or exclusion and whether missing data were balanced across groups or were related to outcomes. We considered the implications of missing outcome data per outcome, such as high dropout rates (e.g. above 15%) or disparate attrition rates (e.g. difference of 10% or more between trial arms).
Low risk of bias: no missing outcome data; reasons for missing outcome data unlikely to be related to true outcome (for survival data, censoring unlikely to introduce bias); missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups; for dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically relevant impact on the intervention effect estimate; for continuous outcome data, plausible effect size (mean difference or standardised mean difference) among missing outcomes not enough to have a clinically relevant impact on observed effect size; appropriate methods, such as multiple imputation, were used to handle missing data.
Unclear risk of bias: insufficient information to assess whether missing data in combination with the method used to handle missing data were likely to induce bias; the trial did not address this outcome.
High risk of bias: reason for missing outcome data likely to be related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups; for dichotomous outcome data, the proportion of missing outcomes compared with observed event risk enough to induce clinically relevant bias in intervention effect estimate; for continuous outcome data, plausible effect size (mean difference or standardised mean difference) among missing outcomes enough to induce clinically relevant bias in observed effect size; 'as‐treated' or similar analysis done with substantial departure of the intervention received from that assigned at randomisation; potentially inappropriate application of simple imputation.
Selective reporting (reporting bias due to selective outcome reporting) ‐ assessment at trial level
We assessed outcome reporting bias by integrating the results of Appendix 5 'Matrix of trial endpoints (publications and trial documents)' (Boutron 2014; Mathieu 2009), with those of Appendix 6 'High risk of outcome reporting bias according to Outcome Reporting Bias In Trials (ORBIT) classification' (Kirkham 2010). This analysis formed the basis for the judgement of selective reporting.
Low risk of bias: the trial protocol was available, and all of the trial's prespecified (primary and secondary) outcomes that are of interest in the review have been reported in the prespecified way; the study protocol is not available, but it was clear that the published reports include all expected outcomes (ORBIT classification).
Unclear risk of bias: insufficient information about selective reporting.
High risk of bias: not all of the trial's prespecified primary outcomes have been reported; one or more primary outcomes is reported using measurements, analysis methods, or subsets of the data (e.g. subscales) that were not prespecified; one or more reported primary outcomes were not prespecified (unless clear justification for their reporting is provided, such as an unexpected adverse effect); one or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis; the trial report fails to include results for a key outcome that would be expected to have been reported for such a trial (ORBIT classification).
Other bias (bias due to problems not covered elsewhere) ‐ assessment at trial level
Low risk of bias: the trial appeared to be free of other sources of bias.
Unclear risk of bias: insufficient information to assess whether an important risk of bias existed; insufficient rationale or evidence that an identified problem introduced bias.
High risk of bias: had a potential source of bias related to the specific trial design used; has been claimed to have been fraudulent; had some other serious problem.
We have presented a 'Risk of bias' graph and a 'Risk of bias' summary figure.
We distinguished between self reported, investigator‐assessed, and adjudicated outcome measures.
We defined the following outcomes as self reported.
Clinical signs and symptoms of vitamin B12 deficiency, as reported by participants.
Health‐related quality of life.
Acceptability.
Adverse events, as measured by participants.
We defined the following outcomes as investigator‐assessed outcome.
Clinical signs and symptoms of vitamin B12 deficiency, as reported by study personnel.
Haemoglobin and MCV.
Total homocysteine and serum methylmalonic acid levels.
Adverse events, as measured by study personnel.
Socioeconomic effects.
Summary assessment of risk of bias
Risk of bias for a trial across outcomes: some 'Risk of bias' domains like selection bias (sequence generation and allocation sequence concealment) affect the risk of bias across all outcome measures in a trial. In case of high risk of selection bias, we planned to mark all endpoints investigated in the associated trial as high risk. Otherwise, we would not perform a summary assessment of the risk of bias across all outcomes for a trial.
Risk of bias for an outcome within a trial and across domains: we planned to assess the risk of bias for an outcome measure including all of the entries relevant to that outcome (i.e. both trial‐level entries and outcome‐specific entries). We considered low risk of bias to denote a low risk of bias for all key domains; unclear risk to denote an unclear risk of bias for one or more key domains; and high risk to denote a high risk of bias for one or more key domains.
Risk of bias for an outcome across trials and across domains: these are our main summary assessments which we would incorporate in our judgements about the quality of evidence in the 'Summary of findings table 1'. We defined outcomes as at low risk of bias when most information came from trials at low risk of bias,; unclear risk when most information came from trials at low or unclear risk of bias; and high risk when a sufficient proportion of information came from trials at high risk of bias.
Measures of treatment effect
When at least two studies were available for a comparison and a given outcome, we expressed dichotomous data as odds ratio (OR) or risk ratio (RR) with 95% confidence interval (CI). We expressed continuous data as mean difference (MD) with 95% CIs. We planned to express time‐to‐event data as hazard ratio (HR) with 95% CI, however we did not encounter this type of data.
Unit of analysis issues
We planned to take into account the level at which randomisation occurred, such as cross‐over trials, cluster‐randomised trials, and multiple observations for the same outcome.
If more than one comparison from the same trial was eligible for inclusion in the same meta‐analysis, we would either combine groups to create a single pair‐wise comparison or appropriately reduce the sample size so that the same participants did not contribute multiple times (splitting the 'shared' group into two or more groups). While the latter approach offers some solution to adjusting the precision of the comparison, it does not account for correlation arising from the same set of participants being in multiple comparisons (Higgins 2011a).
Dealing with missing data
If possible, we obtained missing data from trial authors and carefully evaluated important numerical data such as screened, randomly assigned participants as well as intention‐to‐treat, as‐treated, and per‐protocol populations. We investigated attrition rates (e.g. dropouts, losses to follow‐up, withdrawals) and critically appraised issues concerning missing data and imputation methods (e.g. last observation carried forward).
In trials where the standard deviation (SD) of the outcome was not available at follow‐up or could not be re‐created, we standardised by the average of the pooled baseline SD from those trials in which this information was reported.
Where trials did not report means and SDs for outcomes, and we could not obtain the needed information from trial authors, we imputed these values by estimating the mean and variance from the median, range, and the size of the sample (Hozo 2005).
We planned to investigate the impact of imputation on meta‐analyses by performing sensitivity analyses, and we reported per outcome which trials were included with imputed SDs. However, we eventually did not perform meta‐analysis due to significant clinical heterogeneity.
Assessment of heterogeneity
We planned to identify heterogeneity (inconsistency) by visually inspecting the forest plots and by using a standard Chi² test with a significance level of α = 0.1. In view of the low power of this test, we also planned to consider the I² statistic, which quantifies inconsistency across studies to assess the impact of heterogeneity on the meta‐analysis (Higgins 2002; Higgins 2003); an I² statistic of 75% or more indicates a considerable level of heterogeneity (Higgins 2011a).
When we found heterogeneity, we attempted to determine potential reasons for it by examining individual study and subgroup characteristics.
In the event of substantial clinical, methodological, or statistical heterogeneity, we did not report study results as meta‐analytically pooled effect estimates.
Assessment of reporting biases
Had we included 10 or more trials investigating a particular outcome, we would have used funnel plots to assess small‐study effects. Several explanations may account for funnel plot asymmetry, including true heterogeneity of effect with respect to trial size, poor methodological design (and hence bias of small trials), and publication bias, therefore we would have interpreted the results carefully (Sterne 2011).
Data synthesis
Unless good evidence showed homogeneous effects across studies, we primarily summarised data at low risk of bias using a random‐effects model (Wood 2008). We interpreted random‐effects meta‐analyses with consideration of the whole distribution of effects, ideally by presenting a prediction interval (Higgins 2009). A prediction interval specifies a predicted range for the true treatment effect in an individual study (Riley 2011). For rare events such as event rates below 1%, we used Peto's odds ratio method, provided there was no substantial imbalance between intervention and comparator group sizes, and intervention effects were not exceptionally large. In addition, we also performed statistical analyses according to the statistical guidelines presented in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a).
If in the future adequate data become available, we will use this method of analysis.
Quality of the evidence
We rated the overall quality of the evidence for each outcome according to the GRADE approach, which takes into account issues related not only to internal validity (risk of bias, inconsistency, imprecision, publication bias) but also to external validity, such as directness of results. Two review authors (HYW and THL) independently rated the quality of the evidence for each outcome. We have presented a summary of the evidence in a 'Summary of findings' table, which provides key information about the best estimate of the magnitude of the effect, in relative terms and as absolute differences, for each relevant comparison of alternative management strategies, numbers of participants and studies addressing each important outcome, and rating of overall confidence in effect estimates for each outcome.
We selected six important outcomes and created the Table 1 based on methods described in the Cochrane Handbook for Systematic Reviews of Interventions, by means of the table editor in Review Manager 5, including Appendix 12 'Checklist to aid consistency and reproducibility of GRADE assessments' to help with standardisation of the 'Summary of findings' table (Higgins 2011a; Meader 2014; RevMan 2014; Schünemann 2011). As meta‐analysis was not possible, we presented the results in a narrative format in the 'Summary of findings' table. We justified all decisions to downgrade the quality of studies using footnotes, and we made comments to aid the reader's understanding of the review where necessary.
Subgroup analysis and investigation of heterogeneity
We expected the following characteristics to introduce clinical heterogeneity, and planned to carry out the following subgroup analysis with investigation of interactions. If in the future adequate data become available, we will conduct this method of analysis.
Newly diagnosed participants.
Participants already established on intramuscular treatment.
Participants over 65 years of age.
Participants who have had stomach or small bowel resection.
Vegetarians.
Participants taking anti‐ulcer medication over long periods.
Participants with dementia.
Participants with AIDS.
Sensitivity analysis
We planned to perform sensitivity analyses to explore the influence of the following factors (when applicable) on effect sizes by restricting analysis to the following.
Published trials.
Taking into account risk of bias, as specified in the Assessment of risk of bias in included studies section.
Very long or large trials, to establish the extent to which they dominate the results.
Trials using the following filters: diagnostic criteria, imputation, language of publication, source of funding (industry versus other), or country.
We also planned to test the robustness of results by repeating the analyses using different measures of effect size (RR, OR, etc.) and different statistical models (fixed‐effect and random‐effects models). If in the future adequate data become available, we will conduct this method of analysis.
Results
Description of studies
For a detailed description of trials, see Table 2, Characteristics of included studies, Characteristics of excluded studies,Characteristics of ongoing studies, and 'Studies awaiting classification.
Results of the search
The updated search identified 2328 records, of which 39 full‐text articles and records were identified for further examination. We excluded the publications/records based on their titles or abstracts, because they did not meet the inclusion criteria or were not relevant to the question under study (see Figure 1 ). After screening the full texts of the selected publications/records, six trials met the inclusion criteria with two ongoing trials (EUCTR 2009‐014468‐20‐AT; NCT01476007), and one trial awaiting assessment (Ashok 2011). As two trials, Bolaman 2003 and Kuzminski 1998, have been included in the previous version of this review (Vidal‐Alaball 2005), a total of three trials were included in this update (Bolaman 2003; Kuzminski 1998; Saraswathy 2012). We sought additional information from the trial authors but did not receive a response.
Handsearching
Searching the bibliographies of the selected articles and other relevant publications did not identify additional trials.
Included studies
A detailed description of the characteristics of included trials is presented elsewhere (see Characteristics of included studies and Appendix 2; Appendix 3; Appendix 4). The following is a succinct overview.
Trial design
All included trials were parallel randomised controlled trials. Two trials had a superiority design (Bolaman 2003; Kuzminski 1998), and one trial was a non‐inferiority study (Saraswathy 2012). One trial was multicentre study conducted at four centres (Kuzminski 1998). Two trials had an open‐label design (Bolaman 2003; Saraswathy 2012), and one trial did not report on blinding conditions (Kuzminski 1998).
One trial was conducted between 2009 to 2010 (Saraswathy 2012). Two trials were performed more than 10 years ago: from 1993 to 1996 in Kuzminski 1998 and from 1999 to 2003 in Bolaman 2003. The treatment duration and follow‐up period ranged between three and four months (Table 2). No trial was terminated early.
Settings
The three trials were conducted in South India (Saraswathy 2012), Turkey (Bolaman 2003), and the USA (Kuzminski 1998). Recruiting and treating participants occurred in tertiary care hospitals and ambulatory care centres.
Participants
For detailed characteristics of participants, please refer to Appendix 3 and Appendix 4.
The trials randomised a total of 153 participants. Ten participants in Bolaman 2003 left the trial early, and five participants in Kuzminski 1998 were judged to have primary folate deficiency rather than cobalamin deficiency and were excluded from the final analysis. Eleven participants in Saraswathy 2012 left the study early due to adverse events (n = 2), loss to follow‐up (n = 6), lack of subjective improvement (n = 2), and "expired" (n = 1). Finally, 142 participants completed the three trials (92.8%).
Only one trial reported the ethnicity of participants (Kuzminski 1998).
No trials reported the duration of vitamin B12 deficiency.
Diagnostic criteria
Two trials included people with a serum vitamin B12 level of less than 160 pg/mL (Bolaman 2003; Kuzminski 1998); the other trial used a threshold of less than 200 pg/mL.
Inclusion and exclusion criteria
Two trials excluded people with folate deficiency (Bolaman 2003; Kuzminski 1998). One trial excluded people who were already on vitamin B12 supplements (Saraswathy 2012). The details of inclusion and exclusion criteria in individual trials are outlined in Characteristics of included studies.
Gender distribution
We could ascertain the overall gender distribution of the 153 participants: 56% were male and 44% were female.
Age distribution
The mean age of participants ranged from 38.6 to 72 years. Kuzminski 1998 investigated participants with a mean age of 72 years for the oral group and 71 years for the intramuscular (IM) group. Bolaman 2003 investigated participants with a mean age of 60 years for the oral group and 64 years for the IM group. Saraswathy 2012 investigated a younger population group with an average age of 38.6 in the oral vitamin B12 group and 44.3 in the IM vitamin B12 group.
Comorbidities
In one trial 74% of participants had conditions that could have been associated with malabsorption from the gut (including seven people with pernicious anaemia and three people with ileal resection), although it appears that people with inflammatory bowel disease and celiac disease were not included (Kuzminski 1998). One trial included 50% of participants with conditions affecting the ileum that could have been associated with malabsorption from the gut (Bolaman 2003). It appears that people with inflammatory bowel disease and celiac disease were not included. One trial did not report the comorbidities of participants (Saraswathy 2012).
Interventions
All trials compared oral vitamin B12 with IM vitamin B12 (see Appendix 2).
The total daily dosage of vitamin B12 in the oral group was 1000 μg, in Bolaman 2003 and Saraswathy 2012, or 2000 μg, in Kuzminski 1998. Bolaman 2003 used cyanocobalamin mixed with 20 mL fruit juice, while Kuzminski 1998 used vitamin B12 tablets. Saraswathy 2012 did not report details about the administration of oral vitamin B12. The type of vitamin B12 injection used in two studies was cyanocobalamin (Bolaman 2003; Kuzminski 1998), while the third study did not report this information. However, the treatment duration, frequency, and total dose of vitamin B12 varied between trials.
Bolaman 2003 used the same dose of vitamin B12 and the same frequency of treatment in both arms. The total dose of vitamin B12 in the three‐month trial was 15 mg in each group.
Kuzminski 1998 used a substantially higher daily and total dose in the oral group (2000 µg per day for four months; total dose 240 mg), while for the IM group, the total dose of vitamin B12 was merely 9 mg over 90 days.
Saraswathy 2012 used 1000 μg of vitamin B12 daily for 3 months in the oral group (total dose 90 mg) and a total dose of 15 mg vitamin B12 over 9 weeks in the IM group.
Outcomes
One trial explicitly stated a primary endpoint in the abstract (Saraswathy 2012). The total number of measured outcomes in the included trials ranged from two to nine. All trials described definitions of outcomes in the publications, if applicable (Appendix 5; Appendix 6; Appendix 7).
Trials reporting our primary outcomes
Serum vitamin B12: two trials measured the mean values of serum vitamin B12 (Bolaman 2003; Kuzminski 1998). Two trials reported the number of participants with normalisation of serum vitamin B12 deficiency (Kuzminski 1998; Saraswathy 2012), but the definitions used varied between trials.
Clinical signs and symptoms of vitamin B12 deficiency: no trials reported this outcome. Bolaman 2003 stated measuring the "improvements in signs and symptoms of anemia", however the authors did not report data for this outcome (Appendix 6).
Adverse events: two trials reported on adverse events (Bolaman 2003; Saraswathy 2012).
Trials reporting our secondary outcomes
Health‐related quality of life: no trial reported this outcome.
Acceptability: no trial reported this outcome.
Haemoglobiln and MCV: Bolaman 2003 (60 participants) reported haemoglobin levels. Two trials (93 participants) reported MCV (Bolaman 2003; Kuzminski 1998).
Total homocysteine and serum methylmalonic acid levels: one trial (33 participants) reported this outcome (Kuzminski 1998).
Socioeconomic effects: Bolaman 2003 (60 participants) reported on the tolerability of medication (assessed by a haematologist and patient interviews), and costs, which the trial authors assessed using cost of the trial drug and the injections.
Other outcomes reported in the included trials
Mini‐Mental State Examination.
Neurologic symptoms.
Serum holotranscobalamin levels.
Serum folate.
Parietal and intrinsic factor antibodies.
Serum anti‐intrinsic factor antibodies.
Funding and conflicts of interest in trials
No funding information was reported.
Excluded studies
We excluded 31 full‐text records. The most common reason for exclusion was a non‐randomised trial design, or the comparison or population in the trial did not meet intervention criteria. Reasons for exclusion of studies are detailed in Characteristics of excluded studies.
Ongoing studies
We found two ongoing randomised controlled trials. One trial with an estimated sample size of 320 was registered on ClinicalTrials.gov and was expected to be completed by the year 2017 (NCT01476007). This trial compared oral vitamin B12 with IM vitamin B12 in elderly people (65 years and above) with vitamin deficiency (defined as serum vitamin B12 less than 179 pg/mL). Another trial was registered on the European Clinical Trials Register in 2010 (EUCTR 2009‐014468‐20‐AT). This trial compared sublingual vitamin B12 supplementation with IM vitamin B12 supplementation after gastric bypass surgery. No further details were reported.
Risk of bias in included studies
For details on the risk of bias of the included studies see Characteristics of included studies.
For an overview of review authors' judgements about each 'Risk of bias' item for individual studies and across all studies see Figure 2 and Figure 3.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies (blank cells indicate that the particular outcome was not measured in some studies).
3.
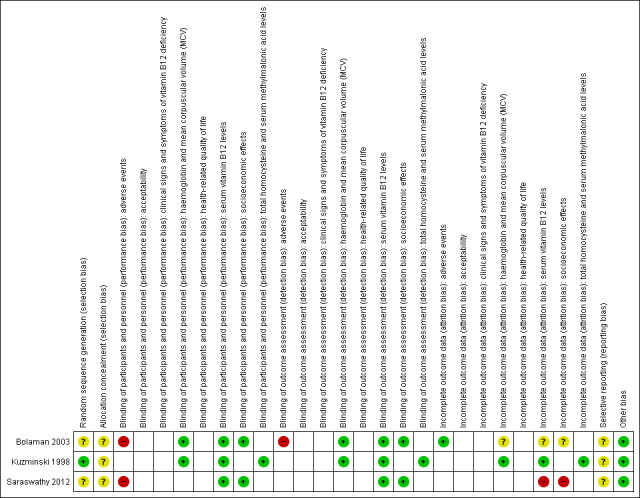
Risk of bias summary: review authors' judgements about each risk of bias item for each included study (blank cells indicate that the study did not measure that particular outcome).
Allocation
We rated one trial as at low risk of bias for randomisation: Kuzminski 1998 stated that they used a statistical package for randomisation. We rated the other two trials as at unclear risk of bias: Bolaman 2003 stated that participants were randomised using the block randomisation method, but did not state how the randomisation was performed. Saraswathy 2012 did not report how the randomisation was conducted.
No trial reported adequate details of allocation concealment. Baseline characteristics were balanced between the two intervention groups for all included trials.
Blinding
Participants in two trials were not blinded, as the design was open‐label randomised controlled trial (Bolaman 2003; Saraswathy 2012). The other trial did not report sufficient information about blinding procedures (Kuzminski 1998). However, we judged the performance bias and detection bias as low risk due to the objective nature of outcome measurements other than the outcome adverse events, which was judged as high risk.
Incomplete outcome data
In Kuzminski 1998, 38 participants were randomised, but five participants (13%) were excluded from the final analysis because they were judged to have primary folate deficiency rather than vitamin B12 deficiency. As the missing data were not likely to impact the effect, we assessed attrition bias as low risk.
In Bolaman 2003, 70 participants were enrolled in the study, but 10 (14%) were excluded because of failure to appear at follow‐up. The final analysis included 26 participants in the oral group and 34 randomised to receive intramuscular treatment. The authors did not analyse data according to the intention‐to‐treat principle. We assessed the attrition bias as unclear risk.
In Saraswathy 2012, 60 participants were randomised, but 11 participants (18.3%) left the study early due to various reasons: eight participants dropped out from the oral vitamin B12 group due to adverse events (n = 2), loss to follow‐up (n = 4), and lack of subjective improvement (n = 2); three participants from the IM vitamin B12 group left the study early due to expired (n = 1) and loss to follow‐up (n = 2). The attrition rate was high, and the missing data were likely to impact the estimate of effects. We therefore assessed attrition bias as high risk.
Selective reporting
No trial reported any information about their protocols, therefore it was difficult to judge what outcomes were measured but not reported (Appendix 5). We assessed reporting bias at trial level as unclear risk. Three outcomes predefined in our protocol were not reported by any of the included trials: i) clinical signs and symptoms of vitamin B12 deficiency; ii) health‐related quality of life; and iii) acceptability. Details about which outcomes were reported by the original trials can be found in Appendix 6.
Other potential sources of bias
We did not identify other obvious bias in the three included trials and rated this domain as low risk.
Sample size calculation
Only one trial provided a sample size calculation (Saraswathy 2012). The calculation was based on the assumption that an equal response of 90% between oral and IM vitamin B12 groups and a non‐inferiority margin of 25% (alpha = 0.25, 1 ‐ beta = 0.80). The expected sample size in each group was 23.
Effects of interventions
See: Table 1
Baseline characteristics
For details of baseline characteristics, see Appendix 3 and Appendix 4. Due to the small number of included trials and substantial clinical heterogeneity, instead of pooling the data we primarily presented the extracted data in the forest plots and reported the results descriptively.
Oral vitamin B12 versus intramuscular vitamin B12
Primary outcomes
Serum vitamin B12 levels
Two trials reported serum vitamin B12 levels (Bolaman 2003; Kuzminski 1998). For a detailed description of the interventions, see Appendix 2. The overall quality of the evidence was low due to serious imprecision.
One trial used an oral or IM vitamin B12 dose of 1000 μg per day and a total dose of 15 mg within three months of treatment (Bolaman 2003). The oral treatment compared with the IM treatment showed a mean difference (MD) of ‐11.7 pg/mL (95% confidence interval (CI) ‐29.5 to 6.1; P = 0.20; 60 participants; Analysis 1.1) (Bolaman 2003). After three months, the mean serum vitamin B12 concentration in the oral vitamin B12 group was 213.8 pg/mL compared with 225.5 pg/mL in the IM group (normal value: above 300 pg/mL).
1.1. Analysis.
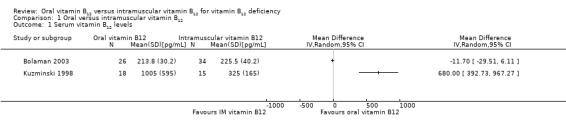
Comparison 1 Oral versus intramuscular vitamin B12, Outcome 1 Serum vitamin B12 levels.
Another trial compared an oral vitamin B12 dose of 2000 μg per day for 120 days (total dose 240 mg) with an IM vitamin B12 dose of 1000 μg per day over a period of 90 days (total dose 9 mg) (Kuzminski 1998). The oral compared with the IM treatment showed an MD of 680 pg/mL (95% CI 392.7 to 967.3; P < 0.001; 33 participants; Analysis 1.1) (Kuzminski 1998), in favour of oral vitamin B12. At four months, the mean serum vitamin B12 concentration in the oral vitamin B12 group was 1005 pg/mL (18/18 participants > 300 pg/mL) compared with 325 pg/mL (7/14 participants > 300 pg/mL) in the IM group.
When the normalisation of serum vitamin B12 was defined as greater than 200 pg/mL, differences between the oral vitamin B12 and IM vitamin B12 groups depended on the dose of vitamin B12 (Analysis 1.2)
1.2. Analysis.
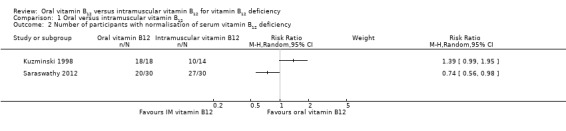
Comparison 1 Oral versus intramuscular vitamin B12, Outcome 2 Number of participants with normalisation of serum vitamin B12 deficiency.
Saraswathy 2012 reported the number of participants achieving normalisation of the serum vitamin B12 level, defined as ≥ 200 pg/mL (Saraswathy 2012). The trial employed an oral vitamin B12 dose of 1000 μg per day for three months (total dose 90 mg) and an IM vitamin B12 dose of 1000 μg (total dose of 15 mg within three months of treatment). A total of 27/30 in the IM vitamin B12 group (90%) and 20/30 in the oral vitamin B12 group (66.7%) achieved this target; although fewer participants in the oral vitamin B12 group achieved the target, the difference was statistically non‐significant (Analysis 1.2) (Saraswathy 2012). However, Kuzminski 1998 used a much higher dose of oral vitamin B12 (240 mg in total) versus a much lower dose of IM vitamin B12 (total dose 9 mg). A total of 10/14 in the IM vitamin B12 group (71.4%) and 18/18 in the oral vitamin B12 group (100%) achieved this target; although more participants in the oral vitamin B12 group achieved the target, the difference was statistically non‐significant (Analysis 1.2) (Kuzminski 1998).
Clinical signs and symptoms
No trial reported this outcome.
Adverse effects
Two trials reported this outcome (Bolaman 2003; Saraswathy 2012). The overall quality of the evidence was very low due to risk of performance and detection bias and serious imprecision.
One trial reported no adverse events in both the oral and IM vitamin B12 groups (Bolaman 2003). The other trial reported that two participants in the oral vitamin B12 group left the trial early due to adverse events (Analysis 1.3) (Saraswathy 2012).
1.3. Analysis.
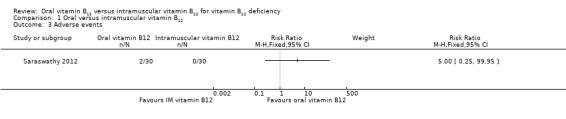
Comparison 1 Oral versus intramuscular vitamin B12, Outcome 3 Adverse events.
Secondary outcomes
Health‐related quality of life
No trial reported this outcome.
Acceptability to patients
No trial reported this outcome.
Haemoglobin and mean corpuscular volume
Only one trial reported on haemoglobin measurements (Bolaman 2003). There was no substantial difference between the oral and intramuscular supplementation of vitamin B12: MD 0.1 g/dL, 95% CI ‐0.30 to 0.50; P = 0.63; 60 participants; Analysis 1.4.
1.4. Analysis.
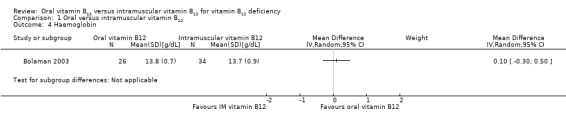
Comparison 1 Oral versus intramuscular vitamin B12, Outcome 4 Haemoglobin.
Two trials reported on MCV measurements (Bolaman 2003; Kuzminski 1998). One trial showed an MD between oral and IM vitamin B12 treatment of 0.20 fL (95% CI ‐1.84 to 2.24; P = 0.85; 60 participants; Analysis 1.5) (Bolaman 2003). The other trial reported an MD of ‐1.00 fL (95% CI ‐5.80 to 3.80; P = 0.68; 33 participants; Analysis 1.5) (Kuzminski 1998).
1.5. Analysis.
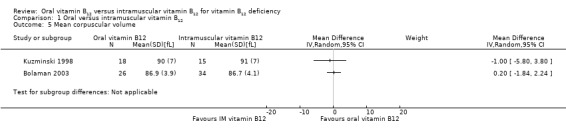
Comparison 1 Oral versus intramuscular vitamin B12, Outcome 5 Mean corpuscular volume.
Total homocysteine and serum methylmalonic acid levels
One trial reported on homocysteine measurements. The MD between oral and IM vitamin B12 treatment was ‐1.60 μmol/L (95% CI ‐4.50 to 1.30; P = 0.28; 33 participants; Analysis 1.6) (Kuzminski 1998).
1.6. Analysis.
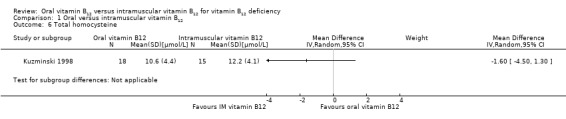
Comparison 1 Oral versus intramuscular vitamin B12, Outcome 6 Total homocysteine.
This trial also investigated serum methylmalonic acid. The MD between oral and IM vitamin B12 treatment was ‐96 nmol/L (95% CI ‐200.76 to 8.76; P = 0.07; 33 participants; Analysis 1.7).
1.7. Analysis.
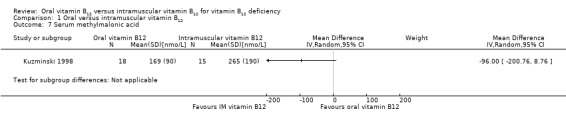
Comparison 1 Oral versus intramuscular vitamin B12, Outcome 7 Serum methylmalonic acid.
Socioeconomic effects
Only one trial reported the costs of the two administration schemes of vitamin B12 (Bolaman 2003). The quality of evidence was low due to serious imprecision. The results demonstrated that the costs per treatment were USD 80 per person in the group taking oral vitamin B12 compared to USD 220 per person in the group using IM vitamin B12 (P < 0.001). The trial authors did not report which economic analysis was performed.
Subgroup analyses
We did not perform subgroup analyses due to the small number of included trials and substantial variety among characteristics of population, interventions, and outcome measurements of the included trials. The dosage of orally taken vitamin B12 might be a potential prognostic factor influencing the treatment effect.
Sensitivity analyses
Due to substantial clinical heterogeneity and the low number of included trials, we did not pool the data and did not conduct the planned sensitivity analyses.
Assessment of reporting bias
We did not draw funnel plots due to the limited number of included trials.
Discussion
Summary of main results
Low‐quality evidence showed that both oral vitamin B12 and IM vitamin B12 can improve serum vitamin B12 levels for people with vitamin B12 deficiency. However, the dosage of oral vitamin B12 might be a clinical factor to affect this outcome. When oral vitamin B12 was used in higher dosages (2000 μg/day with a total dose of 240 mg), the serum vitamin B12 levels were much higher (on average 680 pg/mL higher) than that in the IM vitamin B12 group (1000 μg/day with a total dose of 9 mg). Similarly, the number of participants achieving normalisation of vitamin B12 levels also depended on the dose of vitamin B12 and was higher in the oral vitamin B12 group when treated with 2000 μg/day. We found no substantial differences were between the intervention groups for adverse events. There were also no substantial differences between intervention groups in haemoglobin and MCV levels, total homocysteine, and serum methylmalonic acid levels. The costs of treatment in the oral vitamin B12 group were lower than those in the IM vitamin B12 group. The overall quality of the evidence was low or very low. Two trials are still ongoing, and the full report of one trial was not published. It is likely that the estimate of the effect may change when data from these trials are included.
Most of the dietary vitamin B12 is absorbed actively via intrinsic factor, and passive diffusion accounts for about 1% of vitamin B12 absorption. Therefore, an oral dose of 1000 µg daily should be sufficient to meet the dietary daily amount recommended (Kolber 2014). This theory also explains why higher oral vitamin B12 can achieve similar effects as intramuscular vitamin B12. A previous study confirmed that oral therapy can be effective even in intrinsic factor‐lacking and gastrointestinal‐disabled people (Andres 2008; Andres 2009; Andres 2010). Some of the participants in our included trials, such as those with atrophic gastritis, also showed improvements after oral vitamin B12 therapy. However, these results must be interpreted with caution due to the small number of participants and trials.
Overall completeness and applicability of evidence
More elderly males with vitamin B12 deficiency were included in the current review. A higher prevalence of vitamin B12 deficiency amongst the elderly is documented (Stabler 2013), and vitamin B12 deficiency occurs more frequently in elderly men than in elderly women. None of the trials was conducted in a primary care setting, where most people with vitamin B12 deficiencies are treated; this makes generalisation of the results more difficult. It should be noted that one ongoing trial recruiting participants from 23 primary settings may add important information (NCT01476007). Another factor affecting generalisation is that the three included trials used strict and numerous exclusion criteria.
Secondly, for IM interventions, there are two main kinds of vitamin B12 injections: cyanocobalamin and hydroxocobalamin. Only cyanocobalamin was used in the studies included in this review. It should be noted that the bioavailability of injectable hydroxocobalamin preparations is much higher than the water solution preparations of cyanocobalamin (Boddy 1968; Glass 1961).
Thirdly, the number of outcomes reported was limited, and several important outcomes were not measured in the original trials, such as clinical signs and symptoms of vitamin B12 deficiency after the intervention. Notably, using the normalisation of serum levels of vitamin B12 and its metabolites to reflect the response to treatment is not enough. There may be no direct correlation between normalisation of serum vitamin B12 and improvement of clinical symptoms (Andres 2009; Hall 1977).
Quality of the evidence
Using GRADE, we judged the quality of the evidence in the review to be low or very low. This was mainly due to serious imprecision, inconsistency between trials, and high risk of bias for some domains of included trials. The body of evidence did not allow robust conclusions regarding the objectives of our review. We could include only three trials with small numbers of participants. Missing data (attrition rates ranged from 13.2% to 18.3%) may also have affected some effects estimates. The inconsistency between trials was associated with substantial clinical heterogeneity.
Potential biases in the review process
The incomplete correspondence with trial authors and the missing results of the two ongoing trials limit our evidence base. We failed to obtain the full text of one trial (Ashok 2011), in which 38 participants were recruited. The definitions of vitamin B12 deficiency used in this review differed from that defined in our protocol, in which we used a more strict threshold to define vitamin B12 deficiency in order to reflect common practice.
Agreements and disagreements with other studies or reviews
This is an update of a previous review (Vidal‐Alaball 2005). We included one additional trial in this update (Saraswathy 2012), but the conclusions remain unchanged. We identified no recent systematic review or health technology assessment report on oral versus IM vitamin B12 supplement for vitamin B12 deficiency.
Authors' conclusions
Implications for practice.
Questions about the use of oral or intramuscular (IM) vitamin B12 have been debated by doctors for nearly 50 years, and a conclusive answer is still lacking. Low‐quality evidence indicates that an oral dose of 1000 μg/day vitamin B12 works similarly to IM vitamin B12 in restoring serum B12 levels and acquiring haematological responses in people who are vitamin B12 deficient. An oral dose of 2000 μg/day vitamin B12 might be more effective than IM vitamin B12 .
Adverse events were rare, and low‐quality evidence indicates that oral vitamin B12 costs less than IM vitamin B12 injections. No trial reported on clinical signs and symptoms of vitamin B12 deficiency, health‐related quality of life, or acceptability of the treatment scheme.
Implications for research.
All of the trials included in our review had methodological shortcomings and an insufficient set of outcome data. Further trials should conduct better blinding procedures, recruit more participants, and provide adequate reporting. In addition, future trials should also measure important outcomes such as the clinical signs and symptoms of vitamin B12 deficiency, health‐related quality of life, and socioeconomic effects. It is also important that the protocol considers adverse effects and that these are reported as part of the trial.
Future trials should be performed in primary care settings on participants without considering gender, ethnicity, age, and region. It is important for future research to include participants with poor absorption of oral vitamin B12, such as those with pernicious anaemia, gastrointestinal disease or resection. Considering that the diagnosis and treatment of vitamin B12 deficiency is related to the metabolism of vitamin B12, more research should be conducted focusing on the absorption, distribution, metabolism, and excretion processes of vitamin B12.
What's new
| Date | Event | Description |
|---|---|---|
| 26 October 2017 | New search has been performed | In this update we included one additional trial. |
| 26 October 2017 | New citation required but conclusions have not changed | In this update we included a total of three trials. |
Notes
We included a total of three trials in this update (one additional trial compared to the first published version in 2005).
Acknowledgements
Christopher C Butler, Rebecca Cannings‐John, Andrew Goringe, Kerry Hood, Andrew McCaddon, Ian McDowell, Alexandra Papaioannou, Johannes C van der Wouden, and Rianne Langeveld (original Cochrane Review).
The search strategies for this review update were designed and run by the CMED Group's Information Specialist, Maria‐Inti Metzendorf.
We thank Ms Sai Zhao from Systematic Review Solution Ltd for being our methodology and reporting consultant.
Appendices
Appendix 1. Search strategies
| Cochrane Library |
| 1. [mh "Vitamin B 12"] 2. ((vitamin* or vit or coenzym*) near/1 (b12 or "b 12" or b12? or "b 12?")):ti,ab 3. (cobalamin* or hydrox?cobalamin* or c?anocobalamin* or methylcobalamin* or adenosylcobalamin* or dibencozid* or cobamamid* or cobamid*):ti,ab 4. {or #1‐#3} 5. [mh "Vitamin B 12 Deficiency"] 6. ((b12 or "b 12" or b12? or "b 12?" or cobalamin* or cyanocobalamin) near/3 deficien*):ti,ab 7. #5 or #6 8. #4 and #7 [Publication Year from 2005 to 2017] |
| MEDLINE (Ovid SP) |
| 1. exp Vitamin B 12/ 2. ((vitamin* or vit or coenzym*) adj1 (b12? or "b 12?")).tw. 3. (cobalamin* or hydrox?cobalamin* or c?anocobalamin* or methylcobalamin* or adenosylcobalamin* or dibencozid* or cobamamid* or cobamid*).tw. 4. or/1‐3 5. exp Vitamin B 12 Deficiency/ 6. ((b12? or "b 12?" or cobalamin* or cyanocobalamin) adj3 deficien*).tw. 7. or/5‐6 8. 4 and 7 [9‐19: Cochrane Handbook 2008 RCT filter ‐ sensitivity max. version] 9. randomized controlled trial.pt. 10. controlled clinical trial.pt. 11. randomi?ed.ab. 12. placebo.ab. 13. drug therapy.fs. 14. randomly.ab. 15. trial.ab. 16. groups.ab. 17. or/9‐16 18. exp animals/ not humans/ 19. 17 not 18 20. 8 and 19 21. (200412?? or 2005* or 2006* or 2007* or 2008* or 2009 or 201*).dc. 22. 20 and 21 |
| Embase (Ovid SP) |
| 1. cobalamin derivative/ 2. hydroxocobalamin/ 3. methylcobalamin/ 4. cyanocobalamin/ 5. cobamamide/ 6. cobalamin/ 7. ((vitamin* or vit or coenzym*) adj1 (b12? or "b 12?")).tw. 8. (cobalamin* or hydrox?cobalamin* or c?anocobalamin* or methylcobalamin* or adenosylcobalamin* or dibencozid* or cobamamid* or cobamid*).tw. 9. or/1‐8 10. cyanocobalamin deficiency/ 11. ((b12? or "b 12?" or cobalamin* or cyanocobalamin) adj3 deficien*).tw. 12. or/10‐11 13. 9 and 12 [13Wong 2006"sound treatment studies" filter – BS version] 14. random*.tw. or clinical trial*.mp. or exp health care quality/ 15. 13 and 14 16. (200412?? or 2005* or 2006* or 2007* or 2008* or 2009 or 201*).dc. 17. 15 and 16 |
| LILACS (iAHx) |
| (MH:" Vitamin B 12" OR ((vitamin$ OR coenzym$ OR coenzim$) AND (B12 OR "B 12")) OR (cobalamin$ OR hydroxicobalamin$ OR hydroxocobalamin$ hidroxicobalamin$ OR hidroxocobalamin$ OR cyanocobalamin$ OR cianocobalamin$ OR methylcobalamin$ OR metilcobalamin$ OR adenosylcobalamin$ OR adenosilcobalamin$ OR dibencozid$ OR cobamamid$ OR cobamid$)) AND (MH: "Vitamin B 12 Deficiency" OR ((B12 OR "B 12" OR cobalamin$ OR cyanocobalamin$ OR cianocobalamin$) AND deficien$)) + Filter "Controlled Clinical Trial" |
| ClinicalTrials.gov (Expert search) |
| ( hydroxocobalamin OR hydroxicobalamin OR methylcobalamin OR cyanocobalamin OR cobamamide OR cobalamin OR dibencozid OR adenosylcobalamin OR cobamide OR "vitamin B12" OR "vitamin B 12" OR "coenzym B12" OR "coenzym B 12" ) AND ( B12 OR "B 12" OR cobalamin OR cyanocobalamin ) AND ( deficiency OR deficiencies OR deficient ) AND EXACT "Interventional" [STUDY‐TYPES] |
| ICTRP Search Portal (Standard search) |
| deficien* AND vitamin B12 OR deficien* AND vitamin B 12 OR vitamin B12 deficiency OR vitamin B 12 deficiency OR deficien* AND cobalamin* OR deficien* AND cyanocobalamin* |
Appendix 2. Description of interventions
| Trial ID | Intervention(s) (route, frequency, total dose/day) | Comparator(s) (route, frequency, total dose/day) |
| Bolaman 2003 | Oral: 1000 µg cyanocobalamin (ampoule mixed with 20 mL fruit juice) self administered once daily for 10 days; after 10 days, once a week for 4 weeks and then once a month for life | Intramuscular: 1000 µg cyanocobalamin (ampoule, injection by a nurse into the gluteus muscle) once daily for 10 days; after 10 days, once a week for 4 weeks and then once a month for life |
| Kuzminski 1998 | Oral: 2000 µg cyanocobalamin (two 1000 µg tablets) with breakfast daily for 4 months | Intramuscular: 1000 µg cyanocobalamin on days 1, 3, 7, 10, 14, 21, 30, 60, and 90 (injection by a nurse) |
| Saraswathy 2012 | Oral: 1000 μg of vitamin B12 daily for 3 months | Intramuscular: 1000 μg of vitamin B12 once daily for a week followed by once a week for 8 weeks |
Appendix 3. Baseline characteristics (I)
| Trial ID | Intervention(s) and comparator(s) | Duration of intervention (duration of follow‐up) | Description of participants | Trial period (year to year) | Country | Setting | Ethnic groups (%) | Duration of vitamin B12 deficiency (mean years (SD)) | Vitamin B12 levels (mean pg/mL (SD)) |
| Bolaman 2003 | I: oral vitamin B12 | 90 days (90 days) | People with megaloblastic anaemia due to vitamin B12 deficiency (defined as serum vitamin B12 level < 160 pg/mL) | 1999 to 2003 | Turkey | Hospital | ‐ | ‐ | 72.9 (54.8) |
| C: intramuscular vitamin B12 | 90 days (90 days) | 70.2 (59.1) | |||||||
| Kuzminski 1998 | I: oral vitamin B12 | 4 months (4 months) | People with newly diagnosed vitamin B12 deficiency (defined as serum vitamin B12 level < 160 pg/mL) | 1993 to 1996 | USA | Ambulatory care centres | White: 97 Latina: 3 |
‐ | 93 (46) |
| C: intramuscular vitamin B12 | 90 days (4 months) | 95 (92) | |||||||
| Saraswathy 2012 | I: oral vitamin B12 | 3 months (3 months) | Consecutive patients with vitamin B12 deficiency (serum vitamin B12 level < 200 pg/mL) | 2009 to 2010 | South India | A tertiary care hospital | ‐ | ‐ | 149.8 (37.6) |
| C: intramuscular vitamin B12 | 9 weeks (3 months) | 146.0 (42.1) | |||||||
| ‐ denotes not reported C: comparator; I: intervention; SD: standard deviation | |||||||||
Appendix 4. Baseline characteristics (II)
| Trial ID | Intervention(s) and comparator(s) | Sex (female %) | Age (mean years (SD) | MCV (mean fL (SD)) | Haemoglobin (mean g/dL (SD)) | Total homocysteine (mean μmol/L (SD)) | Serum methylmalonic acid (mean nmol/L (SD)) | Comedications/Cointerventions | Comorbidities |
| Bolaman 2003 | I: oral vitamin B12 | 39 | 60 (15) | 112.3 (11.4) | 8.4 (2.1) | ‐ | ‐ | 18/26 participants with upper GI endoscopy | Atrophic gastritis: 5 Chronic antral gastritis: 5 Chronic pangastritis: 3 Enterogastric reflux: 2 Alkaline reflux: 2 |
| C: intramuscular vitamin B12 | 50 | 64 (10) | 114.8 (10.9) | 8.3 (2.3) | ‐ | ‐ | 27/34 participants with upper GI endoscopy | Atrophic gastritis: 9 Chronic antral gastritis: 2 Chronic pangastritis: 4 Enterogastric reflux: 2 Alkaline reflux: 4 Erosive gastritis: 1 | |
| Kuzminski 1998 | I: oral vitamin B12 | 67 | 72 (11) | 100 (12) | ‐ | 37.2 (44.9) | 3850 (6930) | ‐ | Atrophic gastritis: 7 (3 unclear) Pernicious anaemia: 5 Inadequate dietary protein intake: 3 |
| C: intramuscular vitamin B12 | 87 | 71 (15) | 102 (11) | ‐ | 40.0 (26.2) | 3630 (7040) | ‐ | Atrophic gastritis: 7 Pernicious anaemia: 2 Inadequate dietary protein intake: 2 Prior ileal resection: 1 Prior gastric stapling: 1 | |
| Saraswathy 2012 | I: oral vitamin B12 | 36.7 | 38.6 (14.8) | 92.8 (14.3) | 11.7 (2.4) | ‐ | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 16.7 | 44.3 (9.3) | 89.4 (16.3) | 12.4 (2.7) | ‐ | ‐ | ‐ | ‐ | |
| ‐ denotes not reported C: comparator; GI: gastrointestinal tract; I: intervention; MCV: mean corpuscular volume; SD: standard deviation | |||||||||
Appendix 5. Matrix of trial endpoints (publications and trial documents)
| Trial ID | Endpoints quoted in trial document(s) (ClinicalTrials.gov, FDA/EMA document, manufacturer's website, published design paper)a | Trial results/ publications available in trial register | Endpoints quoted in publication(s)b,c | Endpoints quoted in abstract of publication(s)b,c |
| Saraswathy 2012 | Source: N/T | No full publication | Primary outcome measure: proportion of participants with serum vitamin B12 normalisation (≥ 200 pg/mL) after 60 days of treatment | |
| Secondary outcome measure: compliance: ensured by pill/ampoule count and verification of injection records | ||||
| Other outcome measure(s): ‐ | ||||
| Bolaman 2003 | Source: N/T | Primary outcome measure(s): ‐ | Primary outcome measure(s): ‐ | |
| Secondary outcome measure(s): ‐ | Secondary outcome measure(s): ‐ | |||
| Other outcome measure(s): haemoglobin level, improvements in signs and symptoms of anaemia; response to therapy (detection of reticulocytosis between days 5 and 10, and recovery of the haematologic parameters on complete blood counts and peripheral blood smears at days 10, 30, and 90 of treatment); tolerability ‐ adverse events (assessed by a haematologist at days 0, 30, and 90 using laboratory tests, e.g. serum potassium level, eosinophilia on blood smear, and patient interviews); costs (costs of the study drug and of the injections); serum vitamin B12 levels; serum autoantibodies to gastric parietal cells; cognitive function (Mini‐Mental State Examination); vibration threshold; neurologic sensory assessment (soft‐touch, pinprick examination) | Other outcome measure(s): therapeutic effectiveness (haematologic parameters on days 0, 10, 30, and 90); serum vitamin B12 (on days 0 and 90); cognitive function, vibration threshold; neurologic sensory assessment; tolerability | |||
| Kuzminski 1998 | Source: N/T | Primary outcome measure(s): ‐ | Primary outcome measure(s): ‐ | |
| Secondary outcome measure(s): ‐ | Secondary outcome measure(s): ‐ | |||
| Other outcome measure(s): serum vitamin B12 levels, serum folate levels, serum anti‐intrinsic factor antibodies, unsaturated serum cobalamin‐binding capacity, serum methylmalonic acid levels, serum homocysteine levels, serum pepsinogen I levels, neurologic symptoms, haematocrit, mean corpuscular volume | Other outcome measure(s): therapeutic effectiveness: haematologic and neurologic improvement and changes in serum levels of cobalamin (normal: 200 to 900 pg/mL), methylmalonic acid (normal: 73 to 271 nmol/L), and homocysteine (normal: 5.1 to 13.9 µmol/L) | |||
| ‐ denotes not reported
EMA: European Medicines Agency; FDA: US Food and Drug Administration; N/T: no trial document available aTrial document(s) refers to all available information from published design papers and sources other than regular publications (e.g. FDA/EMA documents, manufacturer's websites, trial registers). bPublication(s) refers to trial information published in scientific journals (primary reference, duplicate publications, companion documents or multiple reports of a primary trial). cOther outcome measures refers to all outcomes not specified as primary or secondary outcome measures. | ||||
Appendix 6. High risk of outcome reporting bias according to Outcome Reporting Bias In Trials (ORBIT) classification
| Trial ID | Outcome | High risk of bias (category A)a | High risk of bias (category D)b | High risk of bias (category E)c | High risk of bias (category G)d |
| Bolaman 2003 | Clinical signs and symptoms of vitamin B12 deficiency | No | Yes | No | No |
| Kuzminski 1998 | N/A | ||||
| Saraswathy 2012 | N/A | ||||
| N/A: not applicable aClear that outcome was measured and analysed; trial report states that outcome was analysed but only reports that result was not significant. (Classification 'A', table 2, Kirkham 2010) bClear that outcome was measured and analysed; trial report states that outcome was analysed but no results reported. (Classification 'D', table 2, Kirkham 2010) cClear that outcome was measured; clear that outcome was measured but not necessarily analysed; judgement says likely to have been analysed but not reported due to non‐significant results. (Classification 'E', table 2, Kirkham 2010) dUnclear whether the outcome was measured; not mentioned, but clinical judgement says likely to have been measured and analysed but not reported on the basis of non‐significant results. (Classification 'G', table 2, Kirkham 2010) | |||||
Appendix 7. Definition of endpoint measurementa
| Trial ID | Definition of vitamin B12 deficiency | Therapeutic efficacy | Clinical signs and symptoms of vitamin B12 deficiency | Adverse events | Health‐related quality of life | Acceptability | Socioeconomic effects |
| Bolaman 2003 | Serum vitamin B12 concentrations < 160 pg/mL, megaloblastic anaemia, mean corpuscular volume > 94 fL (IO) | Response to therapy (detection of reticulocytosis between days 5 and 10, and recovery of the haematologic parameters on complete blood counts and peripheral blood smears at days 10, 30, and 90 of treatment) (IO) | Cognitive function (Mini‐Mental State Examination) | Tolerabilty ‐ adverse events (assessed by a haematologist at days 0, 30, and 90 using laboratory tests, e.g. serum potassium level, eosinophilia on blood smear, and participant interviews) (IO) | N/I | Tolerabilty ‐ adverse events (assessed by a haematologist at days 0, 30, and 90 using laboratory tests, e.g. serum potassium level, eosinophilia on blood smear, and participant interviews) (IO) | Costs of the study drug and of the injections (IO) |
| Kuzminski 1998 | Serum vitamin B12 concentrations < 160 pg/mL (IO) | Haematologic and neurologic improvement and changes in serum levels of vitamin B12 (normal: 200 to 900 pg/mL), methylmalonic acid (normal: 73 to 271 nmol/L), and homocysteine (normal: 5.1 to 13.9 µmol/L) (IO) | "Neurologic improvement" (IO) | N/I | N/I | N/I | N/I |
| Saraswathy 2012 | Serum vitamin B12 concentrations < 200 pg/mL (IO) | Proportion of participants in each treatment arm in whom vitamin B12 levels were normalised (≥ 200 ng/mL) at 3 months after initial treatment | N/I | N/I | N/I | N/I | N/I |
| AO: adjudicated outcome measurement; IO: investigator‐assessed outcome measurement; N/I: not investigated; SO: self reported outcome measurement aIn addition to definition of endpoint measurement, description of who measured the outcome (AO: adjudicated outcome measurement; IO: investigator‐assessed outcome measurement; SO: self reported outcome measurement). | |||||||
Appendix 8. Adverse events (I)
| Trial ID | Intervention(s) and comparator(s) | Participants included in analysis (N) | Deaths (N) | Deaths (%) | Participants with adverse events (N) | Participants with adverse events (%) | Participants with severe/serious adverse events (N) | Participants with severe/serious adverse events (%) |
| Bolaman 2003 | I: oral vitamin B12 | 26a | 0 | 0 | 0 | 0 | 0 | 0 |
| C: intramuscular vitamin B12 | 34a | 0 | 0 | 0 | 0 | 0 | 0 | |
| Kuzminski 1998 | I: oral vitamin B12 | 18b | 0 | 0 | ‐ | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 15b | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
| Saraswathy 2012 | I: oral vitamin B12 | 22c | 0 | 0 | ‐ | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 27d | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
| ‐ denotes not reported C: comparator; I: intervention aTen participants in Bolaman 2003 left the trial early, and the group assignment of the 10 participants was not reported ("no treatment related adverse events were reported in either treatment group"). bFive participants in Kuzminski 1998 were judged to have deficiency of primary folate rather than of cobalamin, therefore they were excluded from the data analysis. cEight participants in this group left the trial early due to adverse events (n = 2), loss to follow‐up (n = 4), and lack of subjective improvement (n = 2). dThree participants in this group left the trial early due to expired (n = 1) and loss to follow‐up (n = 2). | ||||||||
Appendix 9. Adverse events (II)
| Trial ID | Intervention(s) and comparator(s) | Participants included in analysis (N) | Participants discontinuing study due to adverse events (N) | Participants discontinuing study due to adverse events (%) | Participants hospitalised (N) | Participants hospitalised (%) | Participants with outpatient treatment (N) | Participants with outpatient treatment (%) |
| Bolaman 2003 | I: oral vitamin B12 | 26a | 0 | 0 | ‐ | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 34a | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
| Kuzminski 1998 | I: oral vitamin B12 | 18b | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 15b | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | |
| Saraswathy 2012 | I: oral vitamin B12 | 22c | 2 | 6.7 | ‐ | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 27d | 0 | 0 | ‐ | ‐ | ‐ | ‐ | |
| ‐ denotes not reported C: comparator; I: intervention aTen participants in Bolaman 2003 left the trial early, and the group assignment of the 10 participants was not reported. bFive participants in Kuzminski 1998 were judged to have deficiency of primary folate rather than of cobalamin, therefore they were excluded from the data analysis. cEight participants in this group left the trial early due to adverse events (n = 2), loss to follow‐up (n = 4), and lack of subjective improvement (n = 2). dThree participants in this group left the trial early due to expired (n = 1) and loss to follow‐up (n = 2). | ||||||||
Appendix 10. Adverse events (III)
| Trial ID | Intervention(s) and comparator(s) | Participants included in analysis (N) | Participants with specific adverse events (description) | Participants with specific adverse events (N) | Participants with specific adverse events (%) |
| Bolaman 2003 | I: oral vitamin B12 | 26a | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 34a | ‐ | ‐ | ‐ | |
| Kuzminski 1998 | I: oral vitamin B12 | 18b | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 15b | ‐ | ‐ | ‐ | |
| Saraswathy 2012 | I: oral vitamin B12 | 22c | ‐ | ‐ | ‐ |
| C: intramuscular vitamin B12 | 27d | ‐ | ‐ | ‐ | |
| ‐ denotes not reported C: comparator; I: intervention aTen participants in Bolaman 2003 left the trial early, and the group assignment of the 10 participants was not reported. bFive participants in Kuzminski 1998 were judged to have deficiency of primary folate rather than of cobalamin, therefore they were excluded from the data analysis. cEight participants in this group left the trial early due to adverse events (n = 2), loss to follow‐up (n = 4), and lack of subjective improvement (n = 2). dThree participants in this group left the trial early due to expired (n = 1) and loss to follow‐up (n = 2). | |||||
Appendix 11. Survey of study investigators providing information on included trials
| Trial ID | Date trial author contacted | Date trial author replied | Date trial author asked for additional information (short summary) | Date trial author provided data (short summary) |
| Bolaman 2003 | 18 March 2016 | No reply | N/A | N/A |
| Kuzminski 1998 | 18 March 2016 | No reply | N/A | N/A |
| Saraswathy 2012 | 23 December 2016 | No reply | N/A | N/A |
| N/A: not applicable | ||||
Appendix 12. Checklist to aid consistency and reproducibility of GRADE assessments
| Serum vitamin B12 level | Clinical signs and symptoms of vitamin B12 deficiency | Adverse events | Health‐related quality of life | Acceptability | Socioeconomic effects | ||
| Trial limitations (risk of bias)a | Was random sequence generation used (i.e. no potential for selection bias)? | Yes | N/R | Unclear | N/R | N/R | Unclear |
| Was allocation concealment used (i.e. no potential for selection bias)? | Unclear | Unclear | Unclear | ||||
| Was there blinding of participants and personnel (i.e. no potential for performance bias) or outcome not likely to be influenced by lack of blinding? | Yes | No (↓) | Yes | ||||
| Was there blinding of outcome assessment (i.e. no potential for detection bias) or was outcome measurement not likely to be influenced by lack of blinding? | Yes | No (↓) | Yes | ||||
| Was an objective outcome used? | Yes | No (↓) | Yes | ||||
| Were more than 80% of participants enrolled in trials included in the analysis (i.e. no potential reporting bias)?e | Yes | Yes | Yes | ||||
| Were data reported consistently for the outcome of interest (i.e. no potential selective reporting)? | Yes | Unclear | Unclear | ||||
| No other biases reported (i.e. no potential for other bias)? | N/A | Yes | Yes | ||||
| Did the trials end as scheduled (i.e. not stopped early)? | Yes | Yes | Yes | ||||
| Inconsistencyb | Point estimates did not vary widely? | N/A | N/A | N/A | |||
| To what extent did confidence intervals overlap (substantial: all confidence intervals overlap at least one of the included studies point estimate; some: confidence intervals overlap but not all overlap at least one point estimate; no: at least one outlier: where the confidence intervals of some of the studies do not overlap with those of most included studies)? | N/A | N/A | N/A | ||||
| Was the direction of effect consistent? | N/A | N/A | N/A | ||||
| What was the magnitude of statistical heterogeneity (as measured by I²): low (I² < 40%), moderate (I² 40% to 60%), high (I² > 60%)? | N/A | N/A | N/A | ||||
| Was the test for heterogeneity statistically significant (P < 0.1)? | N/A | N/A | N/A | ||||
| Indirectnessa | Were the populations in the included studies applicable to the decision context? | Yes | Yes | Yes | |||
| Were the interventions in the included studies applicable to the decision context? | Highly applicable | Highly applicable | Highly applicable | ||||
| Was the included outcome not a surrogate outcome? | Yes | Yes | Yes | ||||
| Was the outcome time frame sufficient? | Sufficient | Sufficient | Sufficient | ||||
| Were the conclusions based on direct comparisons? | Yes | Yes | Yes | ||||
| Imprecisionc | Was the confidence interval for the pooled estimate not consistent with benefit and harm? | N/A | N/A | N/A | |||
| What is the magnitude of the median sample size (high: 300 participants, intermediate: 100 to 300 participants, low: < 100 participants)?e | Low (↓) | Low (↓) | Low (↓) | ||||
| What was the magnitude of the number of included studies (large: > 10 studies, moderate: 5 to 10 studies, small: < 5 studies)?e | Small (↓) | Small (↓) | Small (↓) | ||||
| Was the outcome a common event (e.g. occurs more than 1/100)? | N/A | Yes | N/A | ||||
| Publication biasd | Was a comprehensive search conducted? | Yes | Yes | Yes | |||
| Was grey literature searched? | Yes | Yes | Yes | ||||
| Were no restrictions applied to study selection on the basis of language? | Yes | Yes | Yes | ||||
| There was no industry influence on studies included in the review? | Unclear | Unclear | Unclear | ||||
| There was no evidence of funnel plot asymmetry? | N/A | N/A | N/A | ||||
| There was no discrepancy in findings between published and unpublished trials? | N/A | N/A | N/A | ||||
| (↓): key item for possible downgrading the quality of the evidence (GRADE) as shown in the footnotes of the 'Summary of findings' table(s); N/A: not applicable; N/R: not reported aQuestions on risk of bias are answered in relation to the majority of the aggregated evidence in the meta‐analysis rather than to individual trials. bQuestions on inconsistency are primarily based on visual assessment of forest plots and the statistical quantification of heterogeneity based on I². cWhen judging the width of the confidence interval, it is recommended that a clinical decision threshold be used to assess whether the imprecision is clinically meaningful. dQuestions address comprehensiveness of the search strategy, industry influence, funnel plot asymmetry, and discrepancies between published and unpublished trials. eDepends on the context of the systematic review area. | |||||||
Data and analyses
Comparison 1. Oral versus intramuscular vitamin B12.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Serum vitamin B12 levels | 2 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Number of participants with normalisation of serum vitamin B12 deficiency | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 3 Adverse events | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4 Haemoglobin | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5 Mean corpuscular volume | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6 Total homocysteine | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 7 Serum methylmalonic acid | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bolaman 2003.
| Methods | Parallel randomised controlled clinical trial; randomisation ratio 1:1; open label; observation period 90 days | |
| Participants |
Inclusion criteria: people with megaloblastic anaemia due to vitamin B12 deficiency
Exclusion criteria:
Diagnostic criteria: people with megaloblastic anaemia due to vitamin B12 deficiency |
|
| Interventions |
Number of study centres: 1 Treatment before study: unknown |
|
| Outcomes | Composite outcome measures reported: no | |
| Study details |
Run‐in period: none Study terminated early: no |
|
| Publication details |
Language of publication: English Commercial funding/non‐commercial funding/other funding: unknown Publication status: peer‐reviewed journal |
|
| Stated aim for study | Quote from publication: "This study assessed the effects and cost of PO versus IM vitamin B12 treatment in patients with megaloblastic anaemia duo to vitamin B12" | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk |
Quote from publication: "using the block randomizations method" Comment: no details provided |
| Allocation concealment (selection bias) | Unclear risk | Comment: no details provided |
| Blinding of participants and personnel (performance bias) adverse events | High risk |
Quote from publication: "open‐label study" Comment: outcome measure likely to be influenced by lack of blinding |
| Blinding of participants and personnel (performance bias) haemoglobin and mean corpuscular volume (MCV) | Low risk | Quote from publication: "open‐label" Comment: outcome measure unlikely to be influenced by lack of blinding |
| Blinding of participants and personnel (performance bias) serum vitamin B12 levels | Low risk | Quote from publication: "open‐label" Comment: outcome measure unlikely to be influenced by lack of blinding |
| Blinding of participants and personnel (performance bias) socioeconomic effects | Low risk |
Quote from publication: "open‐label study" Comment: outcome measure unlikely to be influenced by lack of blinding |
| Blinding of outcome assessment (detection bias) adverse events | High risk |
Quote from publication: "open‐label study" Comment: outcome measure likely to be influenced by lack of blinding |
| Blinding of outcome assessment (detection bias) haemoglobin and mean corpuscular volume (MCV) | Low risk |
Quote from publication: "open‐label study" Comment: outcome measure unlikely to be influenced by lack of blinding |
| Blinding of outcome assessment (detection bias) serum vitamin B12 levels | Low risk |
Quote from publication: "open‐label study" Comment: outcome measure unlikely to be influenced by lack of blinding |
| Blinding of outcome assessment (detection bias) socioeconomic effects | Low risk |
Quote from publication: "open‐label study" Comment: outcome measure unlikely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) adverse events | Low risk |
Quote from publication: "No treatment‐related adverse events were reported in either treatment group" Comment: no adverse events were reported |
| Incomplete outcome data (attrition bias) haemoglobin and mean corpuscular volume (MCV) | Unclear risk | Comment: 10 of 70 participants left the study because they did not appear for follow‐up after 10 days of treatment |
| Incomplete outcome data (attrition bias) serum vitamin B12 levels | Unclear risk | Comment: 10 of 70 participants left the study because they did not appear for follow‐up after 10 days of treatment |
| Incomplete outcome data (attrition bias) socioeconomic effects | Unclear risk | Comment: 10 of 70 participants left the study because they did not appear for follow‐up after 10 days of treatment |
| Selective reporting (reporting bias) | Unclear risk | Comment: primary endpoint "improvements in signs and symptoms of anaemia" neither defined nor results reported, no protocol available |
| Other bias | Low risk | Comment: none detected |
Kuzminski 1998.
| Methods | Parallel randomised controlled clinical trial; randomisation ratio 1:1; observation period 4 months | |
| Participants |
Inclusion criteria:
Exclusion criteria:
Diagnostic criteria: people with newly diagnosed vitamin B12 deficiency (defined as serum vitamin B12 concentrations less than 160 pg/mL) |
|
| Interventions |
Number of study centres: 4 centres Treatment before study: unknown |
|
| Outcomes | Composite outcome measures reported: no | |
| Study details |
Run‐in period: none Study terminated early: no |
|
| Publication details |
Language of publication: English Commercial funding/non‐commercial funding/other funding: unknown Publication status: peer‐reviewed journal |
|
| Stated aim for study | Quote from publication: "However, oral treatment with the vitamin has never been the subject of a controlled study. Therefore, we conducted a randomised, controlled trial of oral versus parenteral cyanocobalamin therapy in patients with vitamin B12 deficiency" | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote from publication: "... patients were randomized (Statistical Analysis System; SAS Institute, Cary, NC) ..." Comment: computer randomisation |
| Allocation concealment (selection bias) | Unclear risk | Comment: not reported |
| Blinding of participants and personnel (performance bias) haemoglobin and mean corpuscular volume (MCV) | Low risk | Comment: not reported, outcome measure unlikely to be affected by blinding conditions |
| Blinding of participants and personnel (performance bias) serum vitamin B12 levels | Low risk | Comment: not reported, outcome measure unlikely to be affected by blinding conditions |
| Blinding of participants and personnel (performance bias) total homocysteine and serum methylmalonic acid levels | Low risk | Comment: not reported, outcome measure unlikely to be affected by blinding conditions |
| Blinding of outcome assessment (detection bias) haemoglobin and mean corpuscular volume (MCV) | Low risk | Comment: not reported, outcome measure unlikely to be affected by blinding conditions |
| Blinding of outcome assessment (detection bias) serum vitamin B12 levels | Low risk | Comment: not reported, outcome measure unlikely to be affected by blinding conditions |
| Blinding of outcome assessment (detection bias) total homocysteine and serum methylmalonic acid levels | Low risk | Comment: not reported, outcome measure unlikely to be affected by blinding conditions |
| Incomplete outcome data (attrition bias) haemoglobin and mean corpuscular volume (MCV) | Low risk | Comment: outcomes measured for 33 participants (5 participants turned out to have low folate levels and were excluded post hoc). The missing data are not likely to impact the effect. |
| Incomplete outcome data (attrition bias) serum vitamin B12 levels | Low risk | Comment: outcomes measured for 33 participants (5 participants turned out to have low folate levels and were excluded post hoc). The missing data are not likely to impact the effect. |
| Incomplete outcome data (attrition bias) total homocysteine and serum methylmalonic acid levels | Low risk | Comment: outcomes measured for 33 participants (5 participants turned out to have low folate levels and were excluded post hoc). The missing data are not likely to impact the effect. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol available |
| Other bias | Low risk | Comment: none detected |
Saraswathy 2012.
| Methods | Parallel randomised controlled clinical trial; randomisation ratio 1:1; non‐inferiority design; observation period 3 months | |
| Participants |
Inclusion criteria:
Exclusion criteria:
Diagnostic criteria: people with newly diagnosed vitamin B12 deficiency (defined as serum vitamin B12 concentrations less than 200 pg/mL) |
|
| Interventions |
Number of study centres: 1 Treatment before study: unknown Titration period: not applicable |
|
| Outcomes | Composite outcome measures reported: no | |
| Study details |
Run‐in period: none Study terminated before regular end: no |
|
| Publication details |
Language of publication: English Commercial funding/non‐commercial funding/other funding: unknown Publication status: peer‐reviewed journal; conference abstract providing sufficient information |
|
| Stated aim for study | Quote from publication: "To compare the efficacy of oral versus intramuscular vitamin B12 supplementation for the treatment of vitamin B12 deficiency" | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk |
Quote from publication: "... randomised and allocated in a concealed manner ..." Comment: the method of randomisation is not reported |
| Allocation concealment (selection bias) | Unclear risk |
Quote from publication: "... randomised and allocated in a concealed manner ..." Comment: the allocation was concealed, but no details were provided. |
| Blinding of participants and personnel (performance bias) adverse events | High risk |
Quote from publication: "Randomized open label trial ..." Comment: not reported, outcome measure likely to be influenced by lack of blinding |
| Blinding of participants and personnel (performance bias) serum vitamin B12 levels | Low risk |
Quote from publication: "Randomized open label trial ..." Comment: not reported, outcome measure unlikely to be affected by lack of blinding |
| Blinding of participants and personnel (performance bias) socioeconomic effects | Low risk |
Quote from publication: "Randomized open label trial ..." Comment: not reported, outcome measure unlikely to be affected by lack of blinding |
| Blinding of outcome assessment (detection bias) serum vitamin B12 levels | Low risk | Comment: not reported, outcome measure unlikely to be affected by blinding conditions |
| Blinding of outcome assessment (detection bias) socioeconomic effects | Low risk | Comment: not reported, outcome measure unlikely to be affected by blinding conditions |
| Incomplete outcome data (attrition bias) serum vitamin B12 levels | High risk | Comment: 8 participants in the intervention group (oral vitamin B12) left the trial early due to adverse events (n = 2), loss to follow‐up (n = 4), and lack of subjective improvement (n = 2). 3 participants in the control group (intramuscular vitamin B12) left the trial early due to expired (n = 1) and loss to follow‐up (n = 2). The attrition rate is high (18.3%), and the missing data are likely to have an impact on the estimate of effect. |
| Incomplete outcome data (attrition bias) socioeconomic effects | High risk | Comment: 8 participants in the intervention group (oral vitamin B12) left the trial early due to adverse events (n = 2), loss to follow‐up (n = 4), and lack of subjective improvement (n = 2). 3 participants in the control group (intramuscular vitamin B12) left the trial early due to expired (n = 1) and loss to follow‐up (n = 2). The attrition rate is high (18.3%), and the missing data are likely to have an impact on the estimate of effect. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol |
| Other bias | Low risk | Comment: none detected |
Note: blank cells indicate that the particular outcome was not measured in trial. IM: intramuscular; MCV: mean corpuscular volume; PO: peroral; SD: standard deviation
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aguilar 2004 | Commentary |
| Andres 2005a | Review |
| Andres 2005b | Letter |
| Andres 2011 | Letter |
| Andres 2012 | Review |
| Bharath 2015 | Case report |
| Bharatwaj 2012 | Review |
| Butler 2006 | Systematic review |
| Castelli 2010 | Participants without vitamin B12 deficiency but low vitamin B12 levels only (overall mean: 273 pg/mL (SD 55.2), i.e. borderline result) |
| Emans 2013 | Letter |
| EUCTR 2013‐004835‐60 | Non‐randomised trial |
| Geisel 2005 | Non‐randomised trial |
| Haffner 2016 | Review of the evidence |
| Houle 2014 | Cost analysis |
| ISRCTN22063938 | Oral vitamin B12 versus placebo |
| Kim 2011 | Non‐randomised single‐arm trial |
| Kolber 2014 | Non‐randomised trial |
| Kripke 2006 | Non‐randomised trial |
| Leidenmuhler 2013 | All participants received a multivitamin mineral supplementation on a daily basis. |
| Leon 2013 | Commentary |
| Lin 2012 | Commentary |
| Lonn 2006 | Letter |
| Masucci 2013 | Review |
| Metaxas 2013 | Review |
| Metaxas 2017 | Eligible participants had a vitamin B12 level < 200 pmol/L (i.e. borderline result), mean vitamin B12 levels at inclusion were 158 pmol/L ± 27 pmol/L and 164 pmol/L ± 20 pmol/L for the oral and intramuscular group, respectively. |
| NCT00699478 | Non‐randomised single‐arm trial |
| Pacholok 2013 | Commentary |
| Radziwill 2014 | Commentary |
| Schijns 2016 | Mean vitamin B12 levels at inclusion were 170 pmol/L ± 22 pmol/L (i.e. borderline result), also conference abstract only. |
| Schloss 2015 | Case report |
| Stabler 2015 | Review |
SD: standard deviation
Characteristics of studies awaiting assessment [ordered by study ID]
Ashok 2011.
| Methods | Randomised, parallel‐group trial; total sample size N = 38 |
| Participants |
Diagnosis: all participants with documented vitamin B12 deficiency (serum vitamin B12 level < 200 pg/mL) Age: 18 to 80 years old Exclusion criteria:
|
| Interventions |
Group 1: oral vitamin B12 1000 mcg once daily for 3 months Group 2: intramuscular injections of vitamin B12 once daily for a week, followed by once a week for 8 weeks, followed by once‐a‐month injection for 1 month (total duration 3 months) |
| Outcomes |
Primary outcome: serum vitamin B12 levels (3 months after initiation of therapy) Secondary outcomes: change in haemoglobin, mean corpuscular volume, serum homocysteine, clinical symptoms (3 months) |
| Notes | Awaiting full text Contact information: Arun RS, assistant professor, Christian Medical College, Vellore; drarunrs@gmail.com Ashok Chacko, professor and head, Christian Medical College, Vellore; chacko.ashok@gmail.com Trial was registered retrospectively; trial is completed. |
Characteristics of ongoing studies [ordered by study ID]
EUCTR 2009‐014468‐20‐AT.
| Trial name or title | Acronym: not stated |
| Methods |
Type of study: not stated Allocation: not stated Intervention model: not stated Masking: not stated Primary purpose: not stated |
| Participants |
Condition: vitamin B12 deficiency undergoing gastric bypass surgery Enrolment: not stated Inclusion criteria: not stated Exclusion criteria: not stated |
| Interventions |
Intervention(s): sublingual vitamin B12 Comparator(s): intramuscular vitamin B12 |
| Outcomes |
Primary outcome(s): not stated Secondary outcome(s): not stated Other outcome(s): not stated |
| Starting date |
Study start date: 22 March 2010 Study completion date: not stated |
| Contact information | Responsible party/principal investigator: Medizinische Universität Wien, Univ.Klinik für Chirurgie, Abt.für Allgemeinchirurgie |
| Study identifier | EudraCT number: EUCTR2009‐014468‐20‐AT |
| Official title | A prospective comparison of vitamin B12 supplementation after gastric bypass surgery (sublingual vs intramuscular) |
| Stated purpose of study | Not stated |
| Notes |
NCT01476007.
| Trial name or title | Acronym: Project OB12 |
| Methods |
Type of study: non‐inferiority clinical trial Allocation: randomisation Intervention model: parallel assignment Masking: open label Primary purpose: treatment |
| Participants |
Condition: vitamin B12 deficiency, defined as serum vitamin B12 < 179 pg/mL Enrolment: estimated 320 Inclusion criteria:
Exclusion criteria:
|
| Interventions |
Intervention(s): oral vitamin B12 Comparator(s): intramuscular vitamin B12 |
| Outcomes |
Primary outcome(s):
Secondary outcome(s): not stated Other outcome(s): none |
| Starting date |
Study start date: July 2014; ongoing but not recruiting participants Study completion date: December 2017 |
| Contact information |
Responsible party/principal investigator: Esperanza Escortell, Epidemiology, phone 34 91 3352569, email eescortell@salud.madrid.org Rosario Riesgo, Epidemiology, phone 34 91 6956672, email rriesgo@salud.madrid.org |
| Study identifier | ClinicalTrials.gov: NCT01476007 EudraCT number: 2010‐024129‐20 |
| Official title | Oral/intramuscular B12 to treat cobalamin deficiency |
| Stated purpose of study | To determine the effectiveness of oral versus intramuscular vitamin B12 by restore vitamin B12 parameter in blood at 8, 26, and 52 weeks in ≥ 65 aged patients with vitamin B12 deficiency |
| Notes | NCT number: NCT01476007 |
Differences between protocol and review
The review authors' team changed for this update: Christopher C Butler, Rebecca Cannings‐John, Andrew Goringe, Kerry Hood, Andrew McCaddon, Ian McDowell, Alexandra Papaioannou, Johannes C van der Wouden, and Rianne Langeveld are no longer review authors.
Since the last publication of this review (Issue 3, 2005), multiple changes such as new methods and other standards were introduced, leading to a complete renewal of this Cochrane Review. We have revised the search strategies for this review update. The following sections have also been changed.
We used a cut‐off point below 200 pg/mL (below 148 pmol/L) as a threshold serum level for vitamin B12 deficiency to better differentiate vitamin B12 deficiency from borderline deficiency.
Types of outcomes: we added the section 'Method and timing of outcome measurement' to define each outcome and group the timing of outcome measurement.
Types of outcomes: we added a 'Summary of findings' table.
We updated the 'Assessment of risk of bias of included studies' section to provide further details about our judgements.
We revised the 'Data extraction and management' section by specifying data items we planned to extract; adding two sections: 'Unit of analysis issues' and ' Dealing with missing data'; and other minor amendments.
Contributions of authors
All review authors read and approved the final review draft.
Hai Yan Wang (HYW): trial selection, data analysis, data interpretation, quality of evidence assessment, and review writing.
Linyi Li (LYL): data extraction and 'Risk of bias' assessment.
Ling Ling Qin (LLQ): data extraction and 'Risk of bias' assessment.
Yanan Song (YNS): trial selection, 'Risk of bias' assessment, data analysis, data interpretation, and review update.
Josep Vidal‐Alaball (JVA): protocol draft, search strategy development, acquiring trial reports, trial selection, data extraction, data analysis, data interpretation, review draft, and future review updates.
Tong Hua Liu (THL): trial selection, data analysis, quality of evidence assessment, and data interpretation.
Sources of support
Internal sources
Department of General Practice, Wales College of Medicine, Cardiff University, UK.
National Public Health Service for Wales, Wales, UK.
Department of General Practice and Elderly Care Medicine, VU University Medical Center, Amsterdam, Netherlands.
External sources
No sources of support supplied
Declarations of interest
HYW: none known
LYL: none known.
LLQ: none known.
YNS: none known.
JVA: none known.
THL: none known.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Bolaman 2003 {published data only}
- Bolaman Z, Kadikoylu G, Yukselen V, Yavasoglu I, Barutca S, Senturk T. Oral versus intramuscular cobalamin treatment in megaloblastic anemia: a single‐center, prospective, randomized, open‐label study. Clinical Therapeutics 2003;25(12):3124‐34. [DOI] [PubMed] [Google Scholar]
Kuzminski 1998 {published data only}
- Kuzminski AM, Giacco EJ, Allen RH, Stabler SP, Lindenbaum J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood 1998;92(4):1191‐8. [PubMed] [Google Scholar]
Saraswathy 2012 {published data only}
- Saraswathy AR, Dutta A, Simon EG, Chacko A. Randomized open label trial comparing efficacy of oral versus intramuscular vitamin B12 supplementation for treatment of vitamin B12 deficiency. Gastroenterology 2012;142(5 Suppl 1):S216. [Google Scholar]
References to studies excluded from this review
Aguilar 2004 {published data only}
- Aguilar Franco C. Subcutaneous administration of vitamin B12. Atencion Primaria 2004;34:509 (author reply 509). [DOI] [PMC free article] [PubMed] [Google Scholar]
Andres 2005a {published data only}
- Andres E, Affenberger S, Vinzio S, Noel E, Kaltenbach G, Schlienger JL. Cobalamin deficiencies in adults: update of etiologies, clinical manifestations and treatment. Revue de Medecine Interne 2005;26:938‐46. [DOI] [PubMed] [Google Scholar]
Andres 2005b {published data only}
- Andres E, Noel E, Kaltenbach G. Usefulness of oral vitamin B12 therapy in vitamin B12 deficiency related to food‐cobalamin malabsorption: Short and long‐term outcome [1]. European Journal of Internal Medicine 2005;16:218. [DOI] [PubMed] [Google Scholar]
Andres 2011 {published data only}
- Andres E, Mecili M. Oral vitamin B12 therapy. Annals of Surgical Oncology 2011;18 Suppl 3:S196‐8 (author reply S199). [DOI] [PubMed] [Google Scholar]
Andres 2012 {published data only}
- Andres E. Oral cobalamin therapy: It may be perhaps time to propose international recommendations?. Presse Medicale 2012;41:895‐8. [DOI] [PubMed] [Google Scholar]
Bharath 2015 {published data only}
- Bharath V, Hsia CC. Vitamin B12 deficiency presenting as pancytopenia with ring sideroblasts. Blood 2015;126:2255. [DOI] [PubMed] [Google Scholar]
Bharatwaj 2012 {published data only}
- Bharatwaj RS. The problem of cyanocobalamin defeciency in a developing country set‐up and the possible solutions. Journal of Clinical and Diagnostic Research 2012;6:921‐2. [Google Scholar]
Butler 2006 {published data only}
- Butler CC, Vidal‐Alaball J, Cannings‐John R, McCaddon A, Hood K, Papaioannou A, et al. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency: a systematic review of randomized controlled trials. Family Practice 2006;23:279‐85. [DOI] [PubMed] [Google Scholar]
Castelli 2010 {published data only}
- Castelli MC, Friedman K, Sherry J, Brazzillo K, Genoble L, Bhargava P, et al. Comparing the efficacy and tolerability of a new daily oral vitamin B12 formulation and intermittent intramuscular vitamin B12 in normalizing low cobalamin levels: a randomized, open‐label, parallel‐group study. Clinical Therapeutics 2011;33:358‐71. [DOI] [PubMed] [Google Scholar]
- Castelli MC, Wong D, Friedman K, Bhargava P, Riley GM. Normalization of vitamin B12 (B12) levels achieved following 1000 mcg oral Eligen B12 therapy: a clinical study comparing the efficacy and safety of oral B12 therapy versus intramuscular (IM) therapy. FASEB Journal 2010;24:lb325. [Google Scholar]
Emans 2013 {published data only}
- Emans ME, Gaillard CAJM, Pfister R, Tanck MW, Boekholdt SM, Wareham NJ, et al. Response to letter by Balta et al. International Journal of Cardiology 2013;169:89‐94. [DOI] [PubMed] [Google Scholar]
EUCTR 2013‐004835‐60 {published and unpublished data}
- Vitamin deficiencies and supplementation in morbidly obese. https://www.clinicaltrialsregister.eu/ctr‐search/trial/2013‐004835‐60/NL (accessed 6 December 2017).
Geisel 2005 {published data only}
- Geisel J, Schorr H, Bodis M, Isber S, Hubner U, Knapp JP, et al. The vegetarian lifestyle and DNA methylation. Clinical Chemistry & Laboratory Medicine 2005;43:1164‐9. [DOI] [PubMed] [Google Scholar]
Haffner 2016 {published data only}
- Haffner J. Oral treatment of vitamin B12 deficiency. Tidsskrift for Den Norske Laegeforening 2016;136:108. [DOI] [PubMed] [Google Scholar]
Houle 2014 {published data only}
- Houle SK, Kolber MR, Chuck AW. Should vitamin B12 tablets be included in more Canadian drug formularies? An economic model of the cost‐saving potential from increased utilisation of oral versus intramuscular vitamin B12 maintenance therapy for Alberta seniors (Provisional abstract). BMJ Open 2014; Vol. 4, issue 5:e004501. [DOI] [PMC free article] [PubMed]
ISRCTN22063938 {published and unpublished data}
- Cobalamin deficiency in primary care: a placebo‐controlled, double‐blind, randomized trial. http://www.isrctn.com/ISRCTN22063938 (accessed 6 December 2017).
Kim 2011 {published data only}
- Kim HI, Hyung WJ, Song KJ, Choi SH, Kim CB, Noh SH. Oral vitamin B12 replacement: an effective treatment for vitamin B12 deficiency after total gastrectomy in gastric cancer patients. Annals of Surgical Oncology 2011;18:3711‐7. [DOI] [PubMed] [Google Scholar]
Kolber 2014 {published data only}
- Kolber MR, Houle SK. Oral vitamin B12: a cost‐effective alternative. Canadian Family Physician 2014;60:111‐2. [PMC free article] [PubMed] [Google Scholar]
Kripke 2006 {published data only}
- Kripke C. Is oral vitamin B12 as effective as intramuscular injection?. American Family Physician 2006;73:65. [PubMed] [Google Scholar]
Leidenmuhler 2013 {published data only}
- Shakeri‐Leidenmuhler S, Poglitsch M, Kefurt R, Felberbauer FX, Bohdjalian A, Langer FB, et al. Vitamin B12 substitution after gastric bypass surgery: sublingual or intramuscular?. European Surgery ‐ Acta Chirurgica Austriaca 2013;45(2 Suppl):S4 (O33). [Google Scholar]
Leon 2013 {published data only}
- Leon CA, Georges P, Zaeeter W. Vitamin B12 deficiency. New England Journal of Medicine 2013;368:2041. [DOI] [PubMed] [Google Scholar]
Lin 2012 {published data only}
- Lin J, Kelsberg G, Safranek S. Clinical inquiry: Is high‐dose oral B12 a safe and effective alternative to a B12 injection?. Journal of Family Practice 2012;61:162‐3. [PubMed] [Google Scholar]
Lonn 2006 {published data only}
- Lonn E. Dr. Lonn replies. New England Journal of Medicine 2006;355:209‐10. [Google Scholar]
Masucci 2013 {published data only}
- Masucci L, Goeree R. Vitamin B12 intramuscular injections versus oral supplements: a budget impact analysis. Ontario Health Technology Assessment Series 2013;13:1‐24. [PMC free article] [PubMed] [Google Scholar]
Metaxas 2013 {published data only}
- Metaxas C, Schmutz A, Walter P, Hersberger KE. Oral versus parenteral route of application: the patient's preference. International Journal of Clinical Pharmacy 2013;35(6):1295‐6. [Google Scholar]
Metaxas 2017 {published data only}
- Metaxas C, Mathis D, Jeger C, Hersberger KE, Arnet I, Walter P. Early biomarker response and patient preferences to oral and intramuscular vitamin B12 substitution in primary care: a randomised parallel‐group trial. Swiss Medical Weekly 2017;147:w14421. [DOI] [PubMed] [Google Scholar]
NCT00699478 {published and unpublished data}
- Oral vitamin B12 administration for vitamin B12 deficiency after total gastrectomy. https://clinicaltrials.gov/ct2/show/NCT00699478 (accessed 6 December 2017).
Pacholok 2013 {published data only}
- Pacholok SM. Vitamin B12 deficiency: serious consequences. Pharmacy Times 2013;80(2):1. [Google Scholar]
Radziwill 2014 {published data only}
- Radziwill R. Can a vitamin B12 deficiency in PPI intake be offset by an increased intake of oral B12?. Medizinische Monatsschrift fur Pharmazeuten 2014;37:299. [PubMed] [Google Scholar]
Schijns 2016 {published data only}
- Schijns W, Meer van der L, Deden L, Janssen IMC, Berends FJ, Aarts EO. Efficacy of oral versus intramuscular vitamin B12 supplementation following Roux‐en‐Y gastric bypass. Obesity Facts 2016; Vol. 9, issue Suppl 1:PO3.104.
Schloss 2015 {published data only}
- Schloss J M, Colosimo M, Airey C, Vitetta L. Chemotherapy‐induced peripheral neuropathy (CIPN) and vitamin B12 deficiency. Supportive Care in Cancer 2015;23:1843‐50. [DOI] [PubMed] [Google Scholar]
Stabler 2015 {published data only}
- Stabler SP. Anemias due to essential nutrient deficiencies. World Review of Nutrition & Dietetics 2015;111:164‐8. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Ashok 2011 {published data only}
- Chacko A. Is vitamin B12 tablets as effective as vitamin B12 injections for the treatment of vitamin B12 deficiency?. Christian Medical College, Vellore India 2011.
References to ongoing studies
EUCTR 2009‐014468‐20‐AT {published and unpublished data}
- A prospective comparison of vitamin B12 supplementation after gastric bypass surgery (sublingual vs. intramuscular). https://www.clinicaltrialsregister.eu/ctr‐search/trial/2009‐014468‐20/AT (accessed 6 December 2017).
NCT01476007 {published data only}
- Gerencia de Atención Primaria Madrid. Oral/intramuscular B12 to treat cobalamin deficiency. Instituto de Salud Carlos III 2015.
- Sanz‐Cuesta T, González‐Escobar P, Riesgo‐Fuertes R, Garrido‐Elustondo S, Cura‐González I, Martín‐Fernández J, et al. Oral versus intramuscular administration of vitamin B12 for the treatment of patients with vitamin B12 deficiency: a pragmatic, randomised, multi‐centre, non‐inferiority clinical trial undertaken in the primary healthcare setting (Project OB12). BMC Public Health 2012;12:394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Área de Investigación. Oral versus intramuscular cobalamin to treat cobalamin deficiency: noninferiority randomised controlled trial, pragmatic and multi‐center in the primary healthcare setting (OB12 project). Consorcio de Apoyo a la Investigación Biomédica en red (CAIBER) 2011.
Additional references
Allen 2009
- Allen L. How common is vitamin B‐12 deficiency?. American Journal of Clinical Nutrition 2009;89:693‐6. [DOI] [PubMed] [Google Scholar]
Andres 2004
- Andres E, Loukili NH, Noel E, Kaltenbach G, Ben Abdelgheni M, Perrin AE, et al. Vitamin B12 (cobalamin) deficiency in elderly patients. Canadian Medical Association Journal 2004;171(3):251‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Andres 2008
- Andres E, Vogel T, Federici L, Zimmer J, Kaltenbach G. Update on oral cyanocobalamin (vitamin B12) treatment in elderly patients. Drugs and Aging 2008;25(11):927‐32. [DOI] [PubMed] [Google Scholar]
Andres 2009
- Andres E, Serraj K, Mecili M, Ciobanu E, Vogel T, Weitten T. Update of oral vitamin B12. Annales d Endocrinologie 2009;70(6):455‐61. [DOI] [PubMed] [Google Scholar]
Andres 2010
- Andres E, Fothergill H, Mecili M. Efficacy of oral cobalamin (vitamin B12) therapy. Expert Opinion on Pharmacotherapy 2010;11(2):249‐56. [DOI] [PubMed] [Google Scholar]
Anonymous 1991
- Dietary reference values for food energy and nutrients for the United Kingdom. Report of the panel on dietary reference values of the committee on medical aspects of food policy. Report on Health and Social Subjects 1991; Vol. 41:1‐210. [PubMed]
Bahadir 2015
- Bahadir A, Reis PG, Erduran E. Oral vitamin B12 treatment is effective for children with nutritional vitamin B12 deficiency. Journal of Paediatrics and Child Health 2014;50(9):721‐5. [DOI] [PubMed] [Google Scholar]
Berlin 1968
- Berlin H, Berlin R, Brante G. Oral treatment of pernicious anemia with high doses of vitamin B12 without intrinsic factor. Acta Medica Scandinavica 1968;184(4):247‐58. [DOI] [PubMed] [Google Scholar]
Berlin 1978
- Berlin R, Berlin H, Brante G, Pilbrant A. Vitamin B12 body stores during oral and parenteral treatment of pernicious anaemia. Acta Medica Scandinavica 1978;204(1‐2):81‐4. [DOI] [PubMed] [Google Scholar]
BNF 2004
- British Medical Association, Royal Pharmaceutical Society of Great Britain. British National Formulary. 3rd Edition. Vol. 48, London: British Medical Association, 2004:456‐7. [Google Scholar]
Boddy 1968
- Boddy K, King P, Mervyn L, Macleod A, Adams JF. Retention of cyanocobalamin, hydroxocobalamin, and coenzyme B 12 after parenteral administration. Lancet 1968;292(7570):710‐2. [DOI] [PubMed] [Google Scholar]
Boutron 2014
- Boutron I, Altman DG, Hopewell S, Vera‐Badillo F, Tannock I, Ravaud P. Impact of spin in the abstracts of articles reporting results of randomized controlled trials in the field of cancer: the SPIIN randomized controlled trial. Journal of Clinical Oncology 2014;32:4120‐6. [DOI] [PubMed] [Google Scholar]
Brito 2015
- Brito A, Mujica‐Coopman MF, López de Romaña D, Cori H, Allen LH. Folate and vitamin B12 status in Latin America and the Caribbean: an update. Food and Nutrition Bulletin 2015;36(Suppl 2):S109‐18. [DOI: 10.1177/0379572115585772] [DOI] [PubMed] [Google Scholar]
Castelli 2011
- Castelli MC, Friedman K, Sherry J, Brazzillo K, Genoble L, Bhargava P, et al. Comparing the efficacy and tolerability of a new daily oral vitamin B12 formulation and intermittent intramuscular vitamin B12 in normalizing low cobalamin levels: a randomized, open‐label, parallel‐group study. Clinical Therapeutics 2011;33(3):358‐71. [DOI] [PubMed] [Google Scholar]
Clarke 2004
- Clarke R, Grimley Evans J, Schneede J, Nexo E, Bates C, Fletcher A, et al. Vitamin B12 and folate deficiency in later life. Age and Ageing 2004;33:34‐41. [DOI] [PubMed] [Google Scholar]
De Jager 2010
- Jager J, Kooy A, Lehert P, Wulffelé MG, Kolk J, Bets D, et al. Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B‐12 deficiency: randomised placebo controlled trial. BMJ 2010;340:c2181. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elia 1998
- Elia M. Oral or parenteral therapy for B12 deficiency. Lancet 1998;352(9142):1721‐2. [DOI] [PubMed] [Google Scholar]
FAO/WHO 1988
- Report of a Joint FAO/WHO Expert Consultation. Requirements of vitamin A, iron, folate and vitamin B12. Report of a Joint FAO/WHO Expert Consultation. FAO Food and Nutrition Series. Vol. 23, Rome: Food and Agriculture Organization of the United Nations; World Health Organization, 1988. [Google Scholar]
Figlin 2003
- Figlin E, Chetrit A, Shahar A, Shpilberg O, Zivelin A, Rosenberg N, et al. High prevalences of vitamin B12 and folic acid deficiency in elderly subjects in Israel. British Journal of Haematology 2003;123:696‐701. [DOI] [PubMed] [Google Scholar]
Glass 1961
- Glass GB, Skeggs HR, Lee DH, Jones EL, Hardy WW. Hydroxocobalamin. I. Blood levels and urinary excretion of vitamin B12 in man after a single parenteral dose of aqueous hydroxocobalamin, aqueous cyanocobalamin and cyanocobalamin zinc‐tannate complex. Blood 1961;18:511‐21. [PubMed] [Google Scholar]
Graham 2007
- Graham ID, Jette N, Tetroe J, Robinson N, Milne S, Mitchell SL. Oral cobalamin remains medicine's best kept secret. Archives of Gerontology and Geriatrics 2007;44(1):49‐59. [DOI] [PubMed] [Google Scholar]
Green 2013
- Green. Physiology, dietary sources, and requirements. Encyclopedia of Human Nutrition 2013;4:351‐6. [Google Scholar]
Hall 1977
- Hall CA. The carriers of native vitamin B12 in normal human serum. Clinical Science and Molecular Medicine 1977;53:453‐7. [DOI] [PubMed] [Google Scholar]
Higgins 2002
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21(11):1539‐58. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analysis. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2009
- Higgins JPT, Thompson SG, Spiegelhalter DJ. A re‐evaluation of random‐effects meta‐analysis. Journal of the Royal Statistical Society: Series A (Statistics in Society) 2009;172(1):137‐59. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011a
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011b
- Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hozo 2005
- Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Medical Research Methodology 2005;5:13. [DOI: 10.1186/1471-2288-5-13] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hróbjartsson 2013
- Hróbjartsson A, Thomsen AS, Emanuelsson F, Tendal B, Hilden J, Boutron I, et al. Observer bias in randomized clinical trials with measurement scale outcomes: a systematic review of trials with both blinded and nonblinded assessors. Canadian Medical Association Journal 2013;185(4):E201‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kirkham 2010
- Kirkham JJ, Dwan KM, Altman DG, Gamble C, Dodd S, Smyth R, et al. The impact of outcome reporting bias in randomised controlled trials on a cohort of systematic reviews. BMJ 2010;340:c365. [DOI: 10.1136/bmj.c365] [DOI] [PubMed] [Google Scholar]
Lam 2013
- Lam JR, Schneider JL, Zhao W, Corley DA. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA 2013;310:2435‐42. [DOI] [PubMed] [Google Scholar]
Lederle 1998
- Lederle FA. Oral cobalamin for pernicious anemia: back from the verge of extinction. Journal of the American Geriatrics Society 1998;46:1125‐7. [DOI] [PubMed] [Google Scholar]
Liberati 2009
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic and meta‐analyses of studies that evaluate interventions: explanation and elaboration. PLoS Medicine 2009;6(7):1‐28. [DOI: 10.1371/journal.pmed.1000100] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lindenbaum 1994
- Lindenbaum J, Rosenberg IH, Wilson PW, Stabler SP, Allen RH. Prevalence of cobalamin deficiency in the Framingham elderly population. American Journal of Clinical Nutrition 1994;60(1):2‐11. [DOI] [PubMed] [Google Scholar]
MacFarlane 2011
- MacFarlane AJ, Greene‐Finestone LS, Shi Y. Vitamin B‐12 and homocysteine status in a folate‐replete population. American Journal of Clinical Nutrition 2011;94(4):1079‐87. [DOI] [PubMed] [Google Scholar]
Mathieu 2009
- Mathieu S, Boutron I, Moher D, Altman DG, Ravaud P. Comparison of registered and published primary outcomes in randomized controlled trials. JAMA 2009;302:977‐84. [DOI] [PubMed] [Google Scholar]
Meader 2014
- Meader N, King K, Llewellyn A, Norman G, Brown J, Rodgers M, et al. A checklist designed to aid consistency and reproducibility of GRADE assessments: development and pilot validation. Systematic Reviews 2014;3:82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Middleton 1985
- Middleton J, Wells W. Vitamin B12 injections: considerable source of work for the district nurse. BMJ 1985;290(6477):1254‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nilsson 2005
- Nilsson M, Norberg B, Hultdin J, Sandstrom H, Westman G, Lokk J. Medical intelligence in Sweden. Vitamin B12: oral compared with parenteral?. Postgraduate Medical Journal 2005;81:191‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pawlak 2013
- Pawlak R, Parrott SJ, Raj S, Cullum‐Dugan D, Lucus D. How prevalent is vitamin B12 deficiency among vegetarians?. Nutrition Reviews 2013;71(2):110‐7. [DOI] [PubMed] [Google Scholar]
Pawlak 2015
- Pawlak R. Is vitamin B12 deficiency a risk factor for cardiovascular disease in vegetarians?. American Journal of Preventive Medicine 2015;48(6):e11‐26. [DOI] [PubMed] [Google Scholar]
Pennypacker 1992
- Pennypacker LC, Allen RH, Kelly JP, Matthews LM, Grigsby J, Kaye K. High prevalence of cobalamin deficiency in elderly outpatients. Journal of the American Geriatrics Society 1992;40:1197‐204. [PubMed] [Google Scholar]
Quadros 2010
- Quadros E. Advances in the understanding of cobalamin assimilation and metabolism. British Journal of Haematology 2010;148:195‐204. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rajan 2002
- Rajan S, Wallace JI, Beresford SA, Brodkin KI, Allen RA, Stabler SP. Screening for cobalamin deficiency in geriatric outpatients: prevalence and influence of synthetic cobalamin intake. Journal of the American Geriatrics Society 2002;50(4):624‐30. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rickes 1948
- Rickes EL, Brink NG, Koniuszy FR, Wood TR, Folkers K. Crystalline vitamin B12. Science 1948;107:396. [DOI] [PubMed] [Google Scholar]
Riley 2011
- Riley RD, Higgins JP, Deeks JJ. Interpretation of random effects meta‐analyses. BMJ 2011;342:d549. [DOI] [PubMed] [Google Scholar]
Schroll 2015
- Schroll JB, Bero L. Regulatory agencies hold the key to improving Cochrane Reviews of drugs [editorial]. Cochrane Database of Systematic Reviews 2015; Vol. 4. [DOI: 10.1002/14651858.ED000098] [DOI] [PMC free article] [PubMed]
Schünemann 2011
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and ‘Summary of findings' tables. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Smith 1948
- Smith EL. Purification of anti‐pernicious anaemia factor from liver. Nature 1948;161:638. [DOI] [PubMed] [Google Scholar]
Stabler 2013
- Stabler SP. Clinical practice. Vitamin B12 deficiency. New England Journal of Medicine 2013;368(2):149‐60. [DOI] [PubMed] [Google Scholar]
Sterne 2011
- Sterne JA, Sutton AJ, Ioannidis JP, Terrin N, Jones DR, Lau J, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta‐analyses of randomised controlled trials. BMJ 2011;343:d4002. [DOI] [PubMed] [Google Scholar]
van Walraven 1999
- Walraven C, Naylor CD. Use of vitamin B12 injections among elderly patients by primary care practitioners in Ontario. Canadian Medical Association Journal 1999;161:146‐9. [PMC free article] [PubMed] [Google Scholar]
Watanabe 2013
- Watanabe F, Yabuta Y, Tanioka Y. Biologically active vitamin B12 compounds in foods for preventing deficiency among vegetarians and elderly. Journal of Agricultural and Food Chemistry 2013;61(28):6769‐75. [DOI] [PubMed] [Google Scholar]
Wong 2006
- Wong SSL, Wilczynski NL, Haynes RB. Developing optimal search strategies for detecting clinically sound treatment studies in EMBASE. Journal of the Medical Library Association 2006;94(1):41‐7. [PMC free article] [PubMed] [Google Scholar]
Wood 2008
- Wood L, Egger M, Gluud LL, Schulz KF, Juni P, Altman DG, et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta‐epidemiological study. BMJ 2008;336(7644):601‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Vidal‐Alaball 2005
- Vidal‐Alaball J, Butler CC, Cannings‐John R, Goringe A, Hood K, McCaddon A, et al. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database of Systematic Reviews 2005, Issue 3. [DOI: 10.1002/14651858.CD004655.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]