

Abstract
Access to hospice care is widely provided in Western countries, but the supply of such service is still in its initiative stage in China. As relatives are often involved in end-of-life decision making in China, a better understanding of their cognitions toward hospice care would help policy makers and physicians to overcome the barriers of providing such service. Thus, we conducted the study to assess the level of knowledge and attitudes among Chinese outpatients and family members regarding hospice care.
A cross-sectional study was conducted in Peking University Third Hospital and Peking University Shougang Hospital. Trained interviewers recruited outpatients or family members in two hospitals as a convenience sample to complete an anonymous face-to-face survey on demographic information, knowledge, and attitudes regarding hospice care.
A total of 550 respondents completed this survey. Only 107 (19.5%) reported that they had known or heard of hospice care, with a mean knowledge score of 2.8 (standard deviation = 1.6). Of the respondents, 69.5% answered “strongly agree” or “agree” regarding the importance of providing hospice care in China. Participants who had known of hospice care were more likely to have favorite attitudes toward it.
The awareness rate of hospice care is low in the study, which may lead to poor attitude and low enrollment rate. Considering the increasing evidence to support the improved outcomes of patients and family members associated with hospice care, the public education on its scope of services, benefits, and limitations is needed in China.
Keywords: China, hospice care, knowledge and attitudes, public education
1. Introduction
The world has experienced an inevitable demographic structure transition due to the patterns of low fertility rate and high life expectancy.[1] China is a typical example and currently has the largest number of elderly population in the world, which will continue to do so in the next decades.[2] Aging is associated with a variety of diseases, including cancer, cardiovascular diseases, and neurodegenerative diseases.[3] For example, approximately 4.3 million patients are diagnosed with cancer and more than 2.8 million cancer deaths will occur every year in China.[4] Thus, it is important to pay attention to improving quality of life with these people, especially for terminally ill individuals.
Access to hospice care has been a trend in recent years as a specialty to provide interdisciplinary care for terminally ill patients. Many studies have showed that patients who received hospice care were associated with improved outcomes, such as pain control, psychosocial and spiritual needs, and family satisfactory.[5–7] To date, access to hospice care is widely provided in Western countries, but the supply of such service is still limited in mainland China.[8,9] Other than the lack of policy and financial support from the government, the traditional Chinese notion that death and dying are taboo subjects is one of major obstructions in the development of hospice care.[10,11] In general, the hospital is considered as a place to provide curative treatments and save lives, which results in many healthcare providers and family members of patients seeing death as a medical treatment failure rather than the last part of life course.[12] Besides, family members are often involved in end-of-life decision making in China, and most of them would choose painful treatments rather than hospice care for terminally ill patients.[9] They believe that hospice care is giving up hope and no treatment. However, hospice care and curative treatments can be used together.[13]
Previous studies reported that knowledge of hospice care is a critical element of end-of-life decisions.[14,15] Several individual characteristics, such as gender and experience of the death of a close one, also affect preferences on hospice utilization.[16,17] Since the hospice care is still in its initiative stage in China, a better understanding of cognitions of general public toward hospice care would help policy makers and physicians to overcome the barriers of providing end-of-life care services. Therefore, our study aimed to assess the level of knowledge and attitudes among Chinese outpatients and family members regarding hospice care in two hospitals.
2. Methods
2.1. Study design
This cross-sectional study was conducted in July 2017 in two tertiary hospitals in Beijing. One is Peking University Third Hospital (hospital T) with 1500 beds, which has not started the hospice care program. The other is Peking University Shougang Hospital (hospital S) with 1000 beds, establishing hospice care center in April 2017. Almost all the specializations of the two hospitals are represented in Beijing, from internal medicine to geriatrics, cardiology, and oncology. The survey was conducted at waiting area of departments of cardiology, geriatrics, oncology, gastroenterology, and respiratory in two hospitals. Outpatients or family members were asked by trained interviewers whether they would like to participate in the survey. Then those willing to participate took part in an anonymous face-to-face survey as a sample using convenience sampling. The study was approved by the Ethics Committee of Peking University Third Hospital. Verbally informed consent was obtained from each respondent at recruitment. Confidentiality of respondents was assured.
2.2. Questionnaire
The questionnaire consisted of three major parts: demographic information, knowledge about hospice care, and attitudes toward hospice care. In the first part, we collected the respondents’ backgrounds including gender, age, educational level, medical insurance, occupation, experience of the death of a close one, chronic disease conditions, and self-rated health status. In the second part, the respondents’ were initially asked to report “whether you had known or heard of hospice care”. Then we assessed the level of knowledge among those respondents who answered “Yes” according to a subjective question and five objective questions (0–1 point per question). In the third part, respondents’ attitudes toward hospice care were assessed using five questions (5-scale per question).
A pilot test was conducted on a convenience sample of 12 outpatients at hospital T to assess the clarity and practicability of this questionnaire. Only 1 (8.3%) participant reported that he had known about hospice care. We decided that there was a brief introduction about its scope of services, benefits, and limitations before starting the third part, so that respondents who did not know about hospice care could continue to answer our questions. The questionnaire was put into use after several revisions, with about 10–13 min required for each respondent.
2.3. Statistical analysis
All analyses were performed using SPSS version 21 (IBM, Armonk, NY). Frequency distributions were used to describe and summarize each survey item. Univariate analyses were performed using chi-square statistics to examine the associations of hospitals, demographic factors, experience of the death of a close one, and self-reported health status with the outcome that whether respondents had known or heard of hospice care (Yes/No). Multivariate logistic regression was then performed according to results from our univariate analyses and previously related studies. Mann–Whitney U test was used to identify differences on participants’ attitudes between two groups that whether respondents had known or heard of hospice care. A P-value less than .05 was considered statistically significant.
3. Results
3.1. General characteristics of study participants
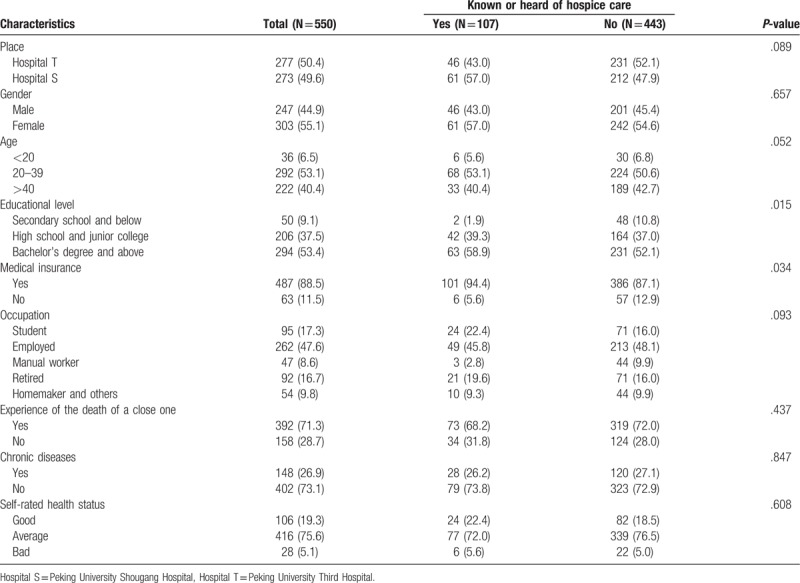
A total of 550 individuals completed the questionnaire in this survey, with a response rate of 95.2%. Two hundred and seventy-seven (50.4%) participants were recruited at hospital T and 273 (49.6%) participants were recruited at hospital S. The reason for nonparticipation was mostly because of response that potential participants did not have enough time to complete the questionnaire. Sociodemographic characteristics are presented in Table 1. More than half of the respondents were female (55.1%), and the mean age was 39 years old (standard deviation [SD] = 16). Of the respondents, 50 (9.1%) were educated to a level of secondary school or below, whereas 294 (53.4%) had a bachelor's degree or above. Most of respondents had medical insurance (88.5%), and reported experience of the death of a close one (71.3%).
Table 1.
Characteristics of survey participants.
3.2. Knowledge about hospice care
Of the respondents, only 107 (19.5%) reported that they had known or heard of hospice care. The awareness rate among participants at hospital S was higher than that at hospital T (22.3% and 16.6%, respectively). As shown in Figure 1, those who had known or heard of hospice care answered “how did you get related information” by a multiple-choice question. 49.5% heard about hospice care from the Internet or television, whereas 39.3% heard about it through newspapers or magazines, and 19.6% from doctor introduction.
Figure 1.
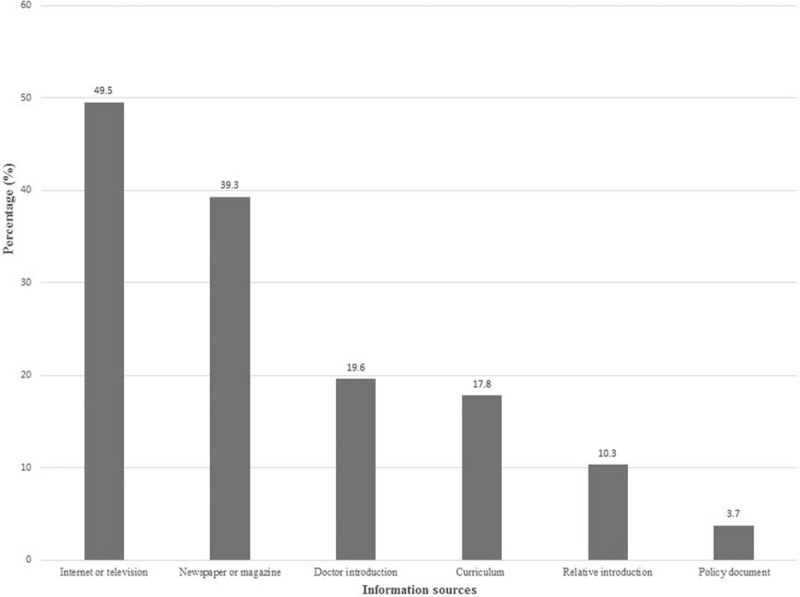
A multiple-choice question for the information sources of palliative care among 107 respondents who had known or heard of it.
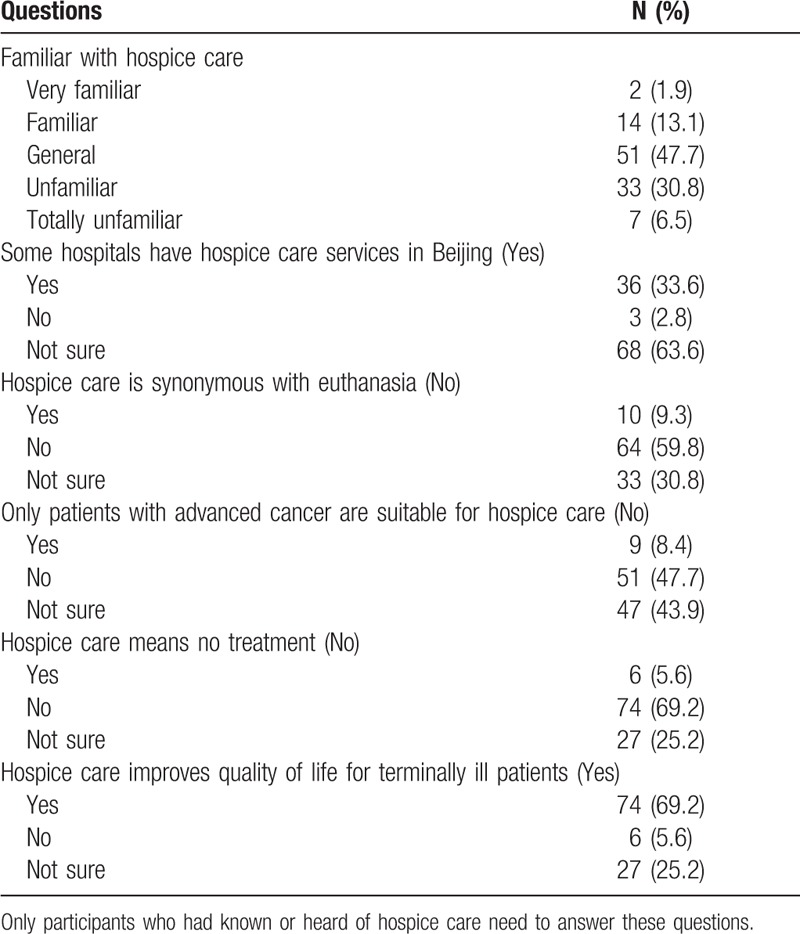
Respondents who had known or heard of hospice care were assessed the level of knowledge. Sixteen participants reported “very familiar” or “familiar” with hospice care. The average score was 2.8 (SD = 1.6) out of five. Most of those respondents correctly answered that hospice care does not equal no care (69.2%) and can improve the quality of life for terminally ill patients (69.2%). 47.7% were aware that hospice care can be used not only for patients with advanced cancer. However, only one third of respondents were aware that some hospitals have hospice care services in Beijing (Table 2).
Table 2.
Responses to knowledge about hospice care among the study participants (N = 107).
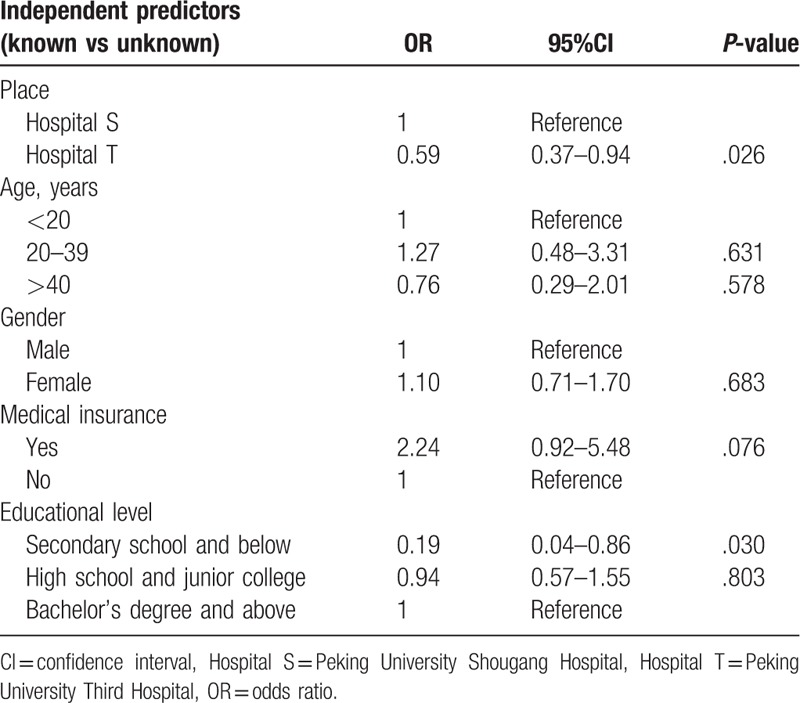
Predictors that were associated in univariate analysis with the outcome that whether respondents had known or heard of hospice care included medical insurance and educational level. According to previously related studies, we also included place, gender, and age into the multivariate logistic regression model. Those who were unknown with hospice care were more likely to be recruited in hospital T (odds ratio [OR] 0.59, 95%CI 0.37–0.94), and have a low educational background (OR 0.19, 95%CI 0.04–0.86 for secondary school and below) (Table 3).
Table 3.
Multivariate logistic regression analysis of independent predictors of the known or heard of hospice care in this survey (N = 550).
3.3. Attitudes regarding hospice care
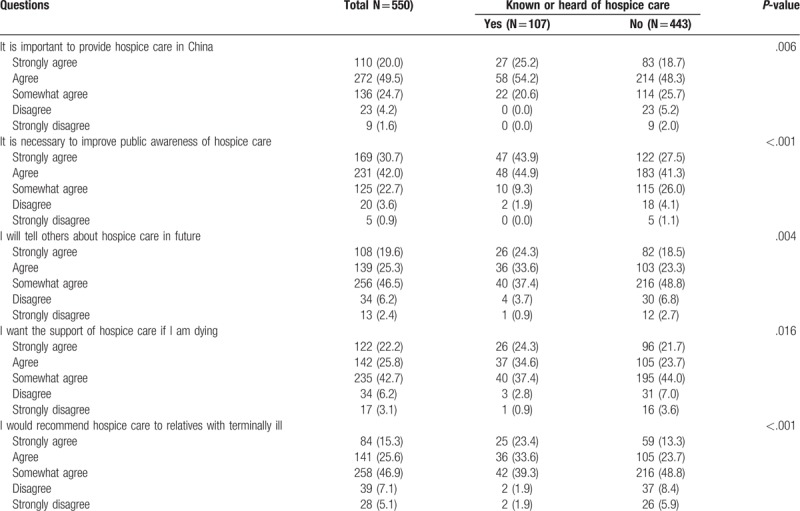
Of the respondents, 69.5% answered “strongly agree” or “agree” regarding the importance of providing hospice care in China. However, less than half of respondents answered “strongly agree” or “agree” regarding their likelihood of choosing hospice care when they were dying (48.0%), and of recommending it for relatives with advanced diseases (40.9%). As shown in Table 4, respondents who had known or heard of hospice care were more likely to have positive attitudes about these questions (all P < .05). However, no statistically significant differences were found on participants’ attitudes between two groups that whether respondents had experience of the death of a close one.
Table 4.
Responses to attitudes about hospice care among the participants (N = 550).
4. Discussion
Our study showed that only 19.5% of respondents had known or heard of hospice care. The average score of knowledge among respondents who had known or heard of it was 2.8 out of five. In a study conducted in the United States,[18] the awareness rate of hospice care was 86% among general public, which was significantly higher than that in our study. Studies reported that the lack of a good understanding of hospice services among patients and relatives when they were recommended was associated with poor attitudes and low enrollment rate.[15,19] Our results provide further evidence that misperception of hospice care may help to explain the low utilization rate among general public in China.
In the 2015 Quality of Death Index, mainland China was ranked 71 out of 80 countries or regions, behind Taiwan, Japan, South Korea, and Hong Kong, and was reported to be “facing difficulties from slow adoption of hospice program”. Considering the rapidly aging population, the needs for hospice care are increasing in China. However, there is a big imbalance between the provider and the potential need for services. About 2400 patients receive palliative and hospice care annually, which accounts for only 1% of patients who need such services in China.[20] One of the major barriers is that governmental policies lag far behind developed countries and regions to guide both healthcare providers and general public in the knowledge of end-of-life care.[8,11] Since courses in hospice care has begun to introduce in medical universities, the public education on its scope of services, benefits, and limitations should be also carried out more widely and effectively.
For those who had known or heard of hospice care in our study, many respondents heard about it from Internet or television (49.5%). Recently, television series based on medicine are popular in China. It is worth considering to involve plots of hospice services for patients with advanced diseases into series, contributing the improvement of awareness of hospice care among general public. The multivariate logistic regression on the independent predictors of known of hospice care showed that respondents recruited at hospital S were more likely to known or heard about it than those recruited at hospital T. Hospital S established a hospice care center in April 2017. The introduction of hospice services is one of video news, continuously showing in the outpatient hall. Interestingly, no respondent who recruited at hospital S reported that he had known about hospice care from the video news.
After a brief introduction of hospice care by trained interviewers, most expressed favorable opinions about it. About 72.7% agreed that it is important to improve the public awareness of hospice care. In addition, about half of respondents had a desire to access to hospice care when they were dying. This result is inconsistent with a previous finding in Hong Kong, where 87.6% of participants would prefer to receive hospice services.[21] Perhaps, based on limited information from interviewers, participants cannot comprehensively understand the benefits and limitations of hospice care at once and then to express the need for it. In our study, although some participants had a favorable opinion about access to hospice care by themselves, they were reluctant to recommend it to relatives with terminally ill, mostly due to traditional Chinese notion of filial piety. The results that respondents who had known or heard of hospice care were more likely to have positive attitudes about it, which provides evidence that knowledge about hospice services may contribute to change the opinion regarding hospice care ethics and utilization rate among general public. We found that there were no statistically significant differences on participants’ attitudes toward hospice care between two groups that whether respondents had experience of the death of a close one. This finding is not in accordance with other studies.[17,22] It is partly because of the lack of knowledge regarding surrogate decisions for end-of-life care among participants, which results in no association between experience of the death of a close one and favorite attitudes about hospice care.
This study had some limitations. First, the questionnaire was designed by our authors; the internal validity may be affected. Second, the convenience sampling method was used in our study to recruit participants with a small simple size, which may be not representative of the retire population and then lead to result bias. Studies with large sample sizes by random sampling are needed to confirm our findings. Third, the study was conducted in Beijing, and respondents were more educated than people in the rest of China. Since those who had a higher educational level were more likely to know about hospice care, the awareness rate of hospice care in mainland China may be lower than that in our study. Fourth, many participants were less than 40 years and they may be not interested in the hospice services, which leads to low awareness rate. Those respondents’ answers may not really express their attitudes toward hospice services, because they cannot have a good understanding of its scope of services, benefits, and limitations at once after a brief introduction by interviewers.
5. Conclusions
Despite these limitations, the study contributes important information about the level of knowledge and attitudes regarding hospice care among Chinese outpatients and family members. Considering the increasing evidence to support the improved outcomes associated with hospice care and the low awareness rate of it in China, future studies should focus on public education of end-of-life care. Such interventions may have positive effects on the opinions and access to hospice care among general public.
Author contributions
Conceptualization: Hua Zhang.
Data curation: Hongling Chu.
Formal analysis: Hua Zhang.
Investigation: Kaiwen Ni, Yining Gong, Furong Li, Xi Cao, Tong Li, Abulikemu Mairipaiti.
Methodology: Hua Zhang, Hongling Chu, Nan Li.
Project administration: Yiming Zhao.
Supervision: Yiming Zhao, Nan Li.
Writing – original draft: Kaiwen Ni.
Writing – review & editing: Kaiwen Ni, Yining Gong.
Footnotes
Abbreviations: Hospital S = Peking University Shougang Hospital, Hospital T = Peking University Third Hospital, OR = odds ratio, SD = standard deviation.
KN and YG contributed equally to this study.
Ethical approval (IRB00006761-M2018095) for this study was approved by the Ethics Committee of Peking University Third Hospital. Verbally informed consent was obtained from each respondent at recruitment.
Data and protocol of this study are available on request by emailing the corresponding author.
This study was funded by the National Natural Science Foundation of China (No. 81701067).
The authors have no conflicts of interest to disclose.
References
- [1].Beard JR, Officer A, de Carvalho IA, et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet 2016;387:2145–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Fang EF, Scheibye-Knudsen M, Jahn HJ, et al. A research agenda for aging in China in the 21st century. Ageing Res Rev 2015;24:197–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Brunet A, Berger SL. Epigenetics of aging and aging-related disease. J Gerontol A Biol Sci Med Sci 2014;69Suppl 1:S17–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin 2016;66:115–32. [DOI] [PubMed] [Google Scholar]
- [5].Miller SC, Mor V, Wu N, et al. Does receipt of hospice care in nursing homes improve the management of pain at the end of life? J Am Geriatr Soc 2002;50:507–15. [DOI] [PubMed] [Google Scholar]
- [6].Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end-of-life care at the last place of care. JAMA 2004;291:88–93. [DOI] [PubMed] [Google Scholar]
- [7].Zimmermann C, Swami N, Krzyzanowska M, et al. Early palliative care for patients with advanced cancer: a cluster-randomised controlled trial. Lancet 2014;383:1721–30. [DOI] [PubMed] [Google Scholar]
- [8].Hu K, Feng D. Barriers in palliative care in China. Lancet 2016;387:1272. [DOI] [PubMed] [Google Scholar]
- [9].Huang QS. A review on problems of China's hospice care and analysis of possible solutions. Chin Med J (Engl) 2015;128:279–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Kang L, Liu XH, Zhang J, et al. Attitudes toward advance directives among patients and their family members in China. J Am Med Dir Assoc 2017;18:808.e7–11. [DOI] [PubMed] [Google Scholar]
- [11].Yin Z, Li J, Ma K, et al. Development of palliative care in China: a tale of three cities. Oncologist 2017;22:1362–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Waldrop DP, Meeker MA. Communication and advanced care planning in palliative and end-of-life care. Nurs Outlook 2012;60:365–9. [DOI] [PubMed] [Google Scholar]
- [13].Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 2010;363:733–42. [DOI] [PubMed] [Google Scholar]
- [14].Cagle JG, Kovacs PJ. Informal caregivers of cancer patients: perceptions about preparedness and support during hospice care. J Gerontol Soc Work 2011;54:92–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Johnson KS, Kuchibhatla M, Tulsky JA. What explains racial differences in the use of advance directives and attitudes toward hospice care? J Am Geriatr Soc 2008;56:1953–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Bookwala J, Coppola KM, Fagerlin A, et al. Gender differences in older adults’ preferences for life-sustaining medical treatments and end-of-life values. Death Stud 2001;25:127–49. [DOI] [PubMed] [Google Scholar]
- [17].Higginson IJ, Sen-Gupta GJ. Place of care in advanced cancer: a qualitative systematic literature review of patient preferences. J Palliat Med 2000;3:287–300. [DOI] [PubMed] [Google Scholar]
- [18].Cagle JG, Van Dussen DJ, Culler KL, et al. Knowledge about hospice: exploring misconceptions, attitudes, and preferences for care. Am J Hosp Palliat Care 2016;33:27–33. [DOI] [PubMed] [Google Scholar]
- [19].Casarett D, Crowley R, Stevenson C, et al. Making difficult decisions about hospice enrollment: what do patients and families want to know? J Am Geriatr Soc 2005;53:249–54. [DOI] [PubMed] [Google Scholar]
- [20].Li J, Davis MP, Gamier P. Palliative medicine: barriers and developments in mainland China. Curr Oncol Rep 2011;13:290–4. [DOI] [PubMed] [Google Scholar]
- [21].Chung RY, Wong EL, Kiang N, et al. Knowledge, attitudes, and preferences of advance decisions, end-of-life care, and place of care and death in Hong Kong. A population-based telephone survey of 1067 adults. J Am Med Dir Assoc 2017;18:367.e19–27. [DOI] [PubMed] [Google Scholar]
- [22].Webb NM, Tucker D. Young adults’ opinions about hospice and home death. J Palliat Med 2009;12:337–42. [DOI] [PubMed] [Google Scholar]