

Abstract
Background
Antipsychotic (neuroleptic) medication is used extensively to treat people with chronic mental illnesses. Its use, however, is associated with adverse effects, including movement disorders such as tardive dyskinesia (TD) ‐ a problem often seen as repetitive involuntary movements around the mouth and face. This review, one in a series examining the treatment of TD, covers miscellaneous treatments not covered elsewhere.
Objectives
To determine whether drugs, hormone‐, dietary‐, or herb‐supplements not covered in other Cochrane reviews on TD treatments, surgical interventions, electroconvulsive therapy, and mind‐body therapies were effective and safe for people with antipsychotic‐induced TD.
Search methods
We searched the Cochrane Schizophrenia Group’s Study‐Based Register of Trials including trial registers (16 July 2015 and 26 April 2017), inspected references of all identified studies for further trials and contacted authors of trials for additional information.
Selection criteria
We included reports if they were randomised controlled trials (RCTs) dealing with people with antipsychotic‐induced TD and schizophrenia or other chronic mental illnesses who remained on their antipsychotic medication and had been randomly allocated to the interventions listed above versus placebo, no intervention, or any other intervention.
Data collection and analysis
We independently extracted data from these trials and we estimated risk ratios (RR) or mean differences (MD), with 95% confidence intervals (CIs). We assumed that people who left early had no improvement. We assessed risk of bias and created 'Summary of findings' tables using GRADE.
Main results
We included 31 RCTs of 24 interventions with 1278 participants; 22 of these trials were newly included in this 2017 update. Five trials are awaiting classification and seven trials are ongoing. All participants were adults with chronic psychiatric disorders, mostly schizophrenia, and antipsychotic‐induced TD. Studies were primarily of short (three to six6 weeks) duration with small samples size (10 to 157 participants), and most (61%) were published more than 20 years ago. The overall risk of bias in these studies was unclear, mainly due to poor reporting of allocation concealment, generation of the sequence, and blinding.
Nineteen of the 31 included studies reported on the primary outcome 'No clinically important improvement in TD symptoms'. Two studies found moderate‐quality evidence of a benefit of the intervention compared with placebo: valbenazine (RR 0.63, 95% CI 0.46 to 0.86, 1 RCT, n = 92) and extract of Ginkgo biloba (RR 0.88, 95% CI 0.81 to 0.96, 1 RCT, n = 157), respectively. However, due to small sample sizes we cannot be certain of these effects.
We consider the results for the remaining interventions to be inconclusive: Low‐ to very low‐quality evidence of a benefit was found for buspirone (RR 0.53, 95% CI 0.33 to 0.84, 1 RCT, n = 42), dihydrogenated ergot alkaloids (RR 0.45, 95% CI 0.21 to 0.97, 1 RCT, n = 28), hypnosis or relaxation, (RR 0.45, 95% CI 0.21 to 0.94, 1 study, n = 15), pemoline (RR 0.48, 95% CI 0.29 to 0.77, 1 RCT, n = 46), promethazine (RR 0.24, 95% CI 0.11 to 0.55, 1 RCT, n = 34), insulin (RR 0.52, 95% CI 0.29 to 0.96, 1 RCT, n = 20), branched chain amino acids (RR 0.79, 95% CI 0.63 to 1.00, 1 RCT, n = 52), and isocarboxazid (RR 0.24, 95% CI 0.08 to 0.71, 1 RCT, n = 20). There was low‐ to very low‐certainty evidence of no difference between intervention and placebo or no treatment for the following interventions: melatonin (RR 0.89, 95% CI 0.71 to 1.12, 2 RCTs, n = 32), lithium (RR 1.59, 95% CI 0.79 to 3.23, 1 RCT, n = 11), ritanserin (RR 1.00, 95% CI 0.70 to 1.43, 1 RCT, n = 10), selegiline (RR 1.37, 95% CI 0.96 to 1.94, 1 RCT, n = 33), oestrogen (RR 1.18, 95% CI 0.76 to 1.83, 1 RCT, n = 12), and gamma‐linolenic acid (RR 1.00, 95% CI 0.69 to 1.45, 1 RCT, n = 16).
None of the included studies reported on the other primary outcome, 'no clinically significant extrapyramidal adverse effects'.
Authors' conclusions
This review has found that the use of valbenazine or extract of Ginkgo biloba may be effective in relieving the symptoms of tardive dyskinesia. However, since only one RCT has investigated each one of these compounds, we are awaiting results from ongoing trials to confirm these results. Results for the remaining interventions covered in this review must be considered inconclusive and these compounds probably should only be used within the context of a well‐designed evaluative study.
Plain language summary
Miscellaneous treatments for antipsychotic‐induced tardive dyskinesia
What is the aim of this review?
The aim of this Cochrane Review was to find out if drugs, supplements, surgical interventions, electroconvulsive therapy, or mind‐body therapies not covered in other Cochrane reviews of tardive dyskinesia can improve tardive dyskinesia. We collected and analysed all relevant randomised controlled trials to answer this question.
Key messages
The drug valbenazine and extract of the herb Ginkgo biloba probably improves symptoms of tardive dyskinesia. But we still need more high‐quality studies to confirm these findings that were taken from only one study per intervention.
What was studied in the review?
Antipsychotic drugs are used to treat chronic mental illnesses such as schizophrenia by controlling, for instance, abnormal perceptions (hallucinations), disordered thinking and fixed false beliefs (delusions). Tardive dyskinesia is a disfiguring and disabling disorder of abnormal, repetitive and involuntary movements, and it is often caused by antipsychotic drugs. More than 20% of people who rely on antipsychotic drugs to control their mental illness have developed tardive dyskinesia. Many different interventions have been studied for easing the symptoms of tardive dyskinesia. Several Cochrane reviews have summarised the effects of the many treatments used to manage these involuntary movements. This review focusses on 'miscellaneous', a group of other non‐connected, interventions not covered in the other Cochrane reviews on tardive dyskinesia.
What are the main results of the review?
We found 31 studies that reported on 24 different interventions to improve tardive dyskinesia in 1278 people who take antipsychotic medication for their chronic mental illnesses. Unfortunately most studies followed up on participants for a short time (most were three to six weeks) and included few participants (the average number of participants was 41 per study).
• Valbenazine probably reduces symptoms of tardive dyskinesia to a clinically important extent compared with placebo (moderate‐certainty evidence). However, this evidence is based on only one study in the USA with 92 participants; we are awaiting results from recently completed and ongoing trials to confirm these results.
• Extract of Ginkgo biloba probably reduces symptoms of tardive dyskinesia to a clinically important extent compared with placebo (moderate‐certainty evidence). However, this evidence is based on only one study in China with 157 participants; we are awaiting results from recently completed and ongoing trials to confirm these results.
• Evidence for the remaining interventions was of low‐ to very low‐certainty evidence and we consider the results for these other interventions to be inconclusive.
How up‐to‐date is this review?
We searched for studies that had been published up to 26 April 2017.
Summary of findings
Background
Description of the condition
Since the 1950's antipsychotic (neuroleptic) medication has been extensively used to treat people with chronic mental illnesses such as schizophrenia. These drugs can effectively control symptoms such as abnormal perceptions (hallucinations), disordered thinking and fixed false beliefs (delusions). In addition, maintenance therapy with neuroleptics is associated with a reduced risk of relapse (Schooler 1993).
Antipsychotic medication, however, has also been associated with a wide range of adverse effects, including movement disorders. The appearance of these movement disorders can contribute to poor compliance with antipsychotic treatment (Barnes 1993), and hence relapse.
Tardive dyskinesia (TD) is one such movement disorder and is characterised by abnormal, repetitive and involuntary movements (APA 1992). The clinical features include tongue protrusion, side‐to‐side or rotatory movement of the jaw, lip smacking, puckering and pursing, and rapid eye blinking (Casey 1994). In some people rapid movements of the arms, legs, and trunk may also occur. TD is a chronic condition of insidious onset, the severity of which spontaneously fluctuates (APA 1992). Studies on the natural history of TD have reported widely variable remission rates (1% to 62%) depending on patient age, psychiatric diagnosis, course of the psychiatric disorder, and duration of therapy (Bergen 1989; Fernandez 2001; Glazer 1990).
Although the most frequent cause of TD is the use of antipsychotic medication, it is clinically striking that dose reduction can lead to a temporary exacerbation in symptoms. Conversely, increasing the dose is often associated with a temporary remission (Cavallaro 1993; Smith 1980). The exact mechanisms of the pathophysiology of TD are unknown. Antipsychotic drugs block certain chemical receptor sites in the brain ‐ one of these is specific for dopamine (Casey 1994). One hypothesis explaining the cause of antipsychotic‐induced TD is that chronic blockade of dopamine receptors in specific cells of the brain (neurones from the nigrostriatum) causes an overgrowth of these receptors (Casey 1994). There is also a suggestion that the chronic use of antipsychotics may also cause an abnormal production of highly active atoms and chemical groups (cytotoxic free radicals), which may damage specific cells in the brain. This, in turn, could be responsible for the appearance of TD (Cadet 1989; Sachdev 2000).
TD occurs in more than 20% of those using antipsychotic medication continually for longer than three months (Glazer 2000; Kane 1982; Tarsy 2011). Every year 4% to 5% of adults and 25% to 30% of elderly persons who continually use these drugs begin to show signs of TD (APA 1992; Correll 2004). Advancing age is a risk factor for both TD's prevalence and severity, with those who are < 60 years of age being three times more likely to spontaneously remit (Jeste 2000; Smith 1980).
The prevalence of TD is often thought to be decreasing based on the use of atypical antipsychotics in place of typical antipsychotics (Cloud 2014). A systematic review found that the incidence of TD associated with atypical antipsychotics (2% to 4%) was significantly lower than that for typical antipsychotics (5% to 8%) (Correll 2008). Despite this, the widespread use of atypical antipsychotics in clinical settings, increased off‐label use, and an ageing population may still result in an overall increase in the number of cases of TD (Cloud 2014; Glazer 2000; Maher 2012). The problem will be considerably greater for people in countries where use of newer drugs is less prevalent (Ballesteros 2000; Martins 2011).
Description of the intervention
Various types of interventions have been evaluated as potential treatments for TD. There is now a series of Cochrane reviews relevant to the care of people with TD (Table 10).This review summarises any trial‐based evidence for the effects of any other treatments that were not summarised in any of the other reviews evaluating interventions for TD. Please see Included studies,6. Interventions for the 24 interventions included in this review.
1. Other relevant reviews.
| Review | Citation |
| Anticholinergics | Bergman 2018a |
| Benzodiazepines | Bergman 2018 |
| Calcium‐channel blockers | Essali 2011 |
| Cholinergics | Tammenmaa 2002 |
| GABAergic compounds | Alabed 2011 |
| Neuroleptic medications (including dose reduction and cessation) | Soares‐Weiser 2006 |
| Non‐neuroleptic compounds that impact on the dopamine and noradrenaline systems (catecholaminergics) | El‐Sayeh 2006 |
| Vitamin E | Soares‐Weiser 2011 |
| This review, Miscellaneous treatments |
How the intervention might work
Use of treatments such as botulin, endorphin, oestrogen, essential fatty acid, EX11582A, ganglioside, lithium, naloxone, periactin, phenylalanine, piracetam, stepholidine, and tryptophan is based on their possible beneficial effects in other movement disorders. Also, interventions using neurosurgery or electroconvulsive therapy have been used for managing the distressing signs and symptoms of TD.
Why it is important to do this review
Several atypical antipsychotic drugs have been produced in the last decades that claim to cause less or no TD (Lieberman 1996). These claims may or may not be true, and certainly evidence does point to the fact that thoughtful use of older generation drugs is not associated with any more problems of TD than with newer treatments (Chouinard 2008). However, in a global context, it is likely that the less expensive and more familiar drugs ‐ such as chlorpromazine or haloperidol ‐ will continue to be the mainstay of treatment of people with schizophrenia (WHO Essential List 2010). Use of drugs such as these is associated with emergence of TD and, therefore, this condition will remain a problem for years to come.
TD can result in considerable social and physical disability (Barnes 1993) and symptoms are often irreversible (Bergen 1989; Fernandez 2001; Glazer 1990). Additionally, TD is frequently associated with lower quality of life (Ascher‐Svanum 2008) and a greater mortality rate (Chong 2009). Given the high incidence and prevalence of TD among people taking antipsychotic medication, the need for prevention or treatment is clear. Unfortunately, there has been sparse evidence to guide clinicians (NICE 2014; Taylor 2009). Although many treatments have been tested, no one intervention has been shown clearly to be effective. Cessation or reduction of the dose of antipsychotic medication would be the ideal management for TD. In clinical practice this is not always possible, not least because in many individuals such a reduction would lead to relapse. This review focuses on whether the addition of different types of miscellaneous medications to those already receiving antipsychotic medication is likely to help TD.
This review is one in a series of nine Cochrane reviews (see Table 10) evaluating treatments for antipsychotic‐induced TD, and is an update of a Cochrane review first published in 2000 (McGrath 2000).
Objectives
1. To determine the effects of any of the following drugs or supplements for antipsychotic‐induced TD in people with schizophrenia or other chronic mental illnesses: botulin toxin, branched‐chain amino acids, buspirone, ceruletide, cyproheptadine, dihydrogenated ergot alkaloids, dimethylaminoethanol, eicosapentaenoic acid, endorphin, oestrogen, essential fatty acid, EX 11‐582A, gamma‐linolenic acid, ganglioside GM1, Ginkgo biloba, insulin, isocarboxazid, levetiracetam, lithium, melatonin, methylphenidate, naloxone, naltrexone, papaverine, pemoline, periactin, phenylalanine, piracetam, procyclidine, promethazine, ritanserin, selegiline, stepholidine and tryptophan, VMAT‐2 inhibitors.
2. To determine the effects of surgical interventions or electroconvulsive therapy (ECT) for antipsychotic‐induced TD in people with schizophrenia or other chronic mental illnesses.
3. To determine the effects of body therapies such as yoga, hypnosis, or relaxation for antipsychotic‐induced TD in people with schizophrenia or other chronic mental illnesses.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials. Where a trial was described as 'double‐blind', but it was only implied that the study was randomised, we included these trials in a sensitivity analysis. If there was no substantive difference within primary outcomes (see Types of outcome measures) when these 'implied randomisation' studies were added, then we included these in the final analysis. If there was a substantive difference, we only used clearly randomised trials and described the results of the sensitivity analysis in the text. We excluded quasi‐randomised studies, such as those allocating by using alternate days of the week.
Types of participants
We included people with schizophrenia and other types of schizophrenia‐like psychosis (e.g. schizophreniform and schizoaffective disorders), irrespective of the diagnostic criteria used, who: i. required the use of antipsychotics for more than three months; ii. developed TD (diagnosed by any criteria) during antipsychotic treatment; and iii. for whom the dose of antipsychotic medication had been stable for one month or more before the trial (the same applies for those free of antipsychotics). There is no clear evidence that the schizophrenia‐like psychoses are caused by fundamentally different disease processes or require different treatment approaches (Carpenter 1994).
Types of interventions
1. Compounds
Including drugs, hormone‐, dietary‐, or herb‐supplements such as botulin toxin, buspirone, ceruletide, dihydrogenated ergot alkaloids, dimethylaminoethanol, endorphin, oestrogen, essential and omega fatty acids, EX 11‐582A, Ginkgo biloba, ganglioside GM1, insulin, levetiracetam, lithium, melatonin, methylphenidate, naloxone, naltrexone, pemoline, periactin, phenylalanine, piracetam, stepholidine, tryptophan, VMAT‐2 inhibitors. Any doses, frequencies or means of administration were acceptable.
2. Surgical intervention of any sort
3. Electroconvulsive therapy (ECT)
4. Mind‐body therapies, such as relaxation techniques or hypnotherapy
Compared with:
1. Placebo, no treatment or standard care; or
2. Any other intervention for the treatment of tardive dyskinesia
Types of outcome measures
We have defined clinical efficacy as an improvement in the symptoms of TD of more than 50%, on any scale. We grouped outcomes into short term (less than six weeks), medium term (between six weeks and six months) and long term (more than six months).
Primary outcomes
1. Tardive dyskinesia
No clinically important improvement in the symptoms of individuals, defined as more than 50% improvement on any TD scale ‐ any time period.
2. Adverse effects
No clinically important extrapyramidal adverse effects ‐ any time period.
Secondary outcomes
1. Tardive dyskinesia (TD)
1.1 Any improvement in the symptoms of individuals on any TD scale, as opposed to no improvement. 1.2 Deterioration in the symptoms of individuals, defined as any deleterious change on any TD scale. 1.3 Average change in severity of TD during the trial period. 1.4 Average difference in severity of TD at the end of the trial.
2. General mental state changes
2.1 Deterioration in general psychiatric symptoms (such as delusions and hallucinations) defined as any deleterious change on any scale. 2.2 Average difference in severity of psychiatric symptoms at the end of the trial.
3. Acceptability of treatment
3.1 Acceptability of the intervention to the participant group as measured by numbers of people leaving the study early.
4. Adverse effects
4.1 Use of any anti‐parkinsonism drugs. 4.2 Average score/change in extrapyramidal adverse effects. 4.3 Acute dystonia.
5. Other adverse effects, general and specific
6. Hospital and service utilisation outcomes
6.1 Hospital admission. 6.2 Average change in number of days in hospital. 6.3 Improvement in hospital status (for example: change from formal to informal admission status, use of seclusion, level of observation).
7. Economic outcomes
7.1 Average change in total cost of medical and mental health care. 7.2 Total indirect and direct costs.
8. Social confidence, social inclusion, social networks, or personalised quality of life measures
8.1. Clinically important change in social confidence, social inclusion, social networks, or personalised quality of life measures. 8.2 Average score/change in social confidence, social inclusion, social networks, or personalised quality of life measures.
9. Behaviour
9.1 Clinically important agitation. 9.2 Use of adjunctive medication for sedation. 9.3 Aggression to self or others.
10. Cognitive state
10.1 Clinically important change. 10.2 Any change, general and specific.
'Summary of findings' tables
We used the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach to interpret findings (Schünemann 2011) and used GRADEpro GDT to export data from this review to create 'Summary of findings' tables. These tables provide outcome‐specific information concerning the overall quality of evidence from each included study in the comparison, the magnitude of effects of interventions examined and the sum of available data on all outcomes rated as important to patient care and decision making. We selected the following main outcomes for inclusion in the 'Summary of findings' tables.
1. Tardive dyskinesia 1.1 No clinically important improvement 1.2 Deterioration of symptoms
2. Adverse effects 2.1 Clinically important extrapyramidal adverse effects 2.2 Any adverse effect
3. Acceptability of treatment 3.1 Leaving the study early
4. Social confidence, social inclusion, social networks, or personalised quality of life measures* 4.1 Clinically important change in social confidence, social inclusion, social networks, or personalised quality of life measures for either recipients of care or caregivers.
* Outcome designated important to patients. We wished to add perspectives from people’s personal experience with TD to the research agenda. A consultation with service users was planned where the previously published version of another review in the tardive dyskinesia series (Soares‐Weiser 2011; Table 10) and a lay overview of that review gave the foundation for the discussions. The session was planned to provide time to reflect on current research on TD and consider gaps in knowledge. The report is published in the Health Technology Assessment (HTA) report for the UK National Institute of Health Research (Bergman 2017). We have added one figure from the report showing service user expression of frustration concerning this neglected area of research (Figure 1). Informed by the results of the consultation, for this review, we updated outcomes for the 'Summary of findings' tables.
1.

Message from one of the participants of the Public and patient involvement consultation of service user perspectives on tardive dyskinesia research.
Prioritising interventions for 'Summary of findings' tables
Twenty‐four different interventions were included in this review (see Table 11), and many of the studies were very small (< 60 participants) pilot studies testing out new interventions to treat TD. Due to the vast number of included interventions and to the small sample size and experimental nature of many of the studies, as a post hoc change to methods, we decided to prioritise interventions and create 'Summary of findings' tables only for those comparisons that: 1) included more than 60 participants, or 2) included more than one trial, or 3) was selected as an intervention of special interest for the UK National Health Service in the prioritisation process for the recently published HTA report (Bergman 2017).
2. Overview of study characteristics.
| Study | N and setting | Condition | Sex and age | Intervention and duration | Comparison | Outcomes |
| Bucci 1971 | 20 outpatients in the USA | schizophrenia + TD | F+M 45‐62 years | Isocarboxazid + AP 40 weeks | Procyclidine + AP | TD symptoms, AEs |
| Cai 1988 | 57 participants, setting not reported | TD | F+M 28‐59 years | L‐stepholidine + AP 8 weeks | Placebo + AP | TD symptoms, AEs, mental state |
| Castro 2011 | 13 in‐ and outpatients in Venezuela | various psychiatric conditions + TD | F+M 46‐75 years | Melatonin + AP 12 weeks | Placebo + AP | TD symptoms, AEs, mental state |
| Emsley 2006 | 84 in‐ and outpatients in South Africa | schizophrenia or schizoaffective disorder + TD | F+M m = 42 years | Omega‐3 fatty acid + AP 12 weeks | Placebo + AP | TD symptoms, AEs, mental state |
| Gardos 1979 | 22 inpatients in the USA | schizophrenia, dementia + TD | F+M 32‐84 years | Papaverine + AP 6 weeks | TAU + AP | TD symptoms |
| Glazer 1985 | 12 outpatients in the USA | various psychiatric conditions + TD | F 50‐65 years | Oestrogen + AP 3 weeks | Placebo + AP | TD symptoms, AEs |
| Glover 1982 | 15 outpatients in the USA | schizophrenia + TD or EPS | F+M m = 34.9 years | Hypnosis or relaxation + AP 8 sessions | TAU + AP | TD symptoms |
| Goff 1993 | 33 outpatients in the USA | TD | F+M m = 49 years | Selengiline + AP 6 weeks | Placebo + AP | TD symptoms |
| Hajioff 1983 | 20 inpatients in the UK | various psychiatric conditions + TD | F+M 60‐92 years | Ergoloid mesylates + AP 6 weeks | Placebo + AP | TD symptoms |
| Kojima 1992 | 85 in‐ and outpatients in Japan | schizophrenia + TD | F+M 31‐75 years | Ceruletide + AP 6 weeks | Placebo + AP | TD symptoms, AEs |
| Koshino 1979 | 42 inpatients in Japan | various psychiatric conditions + TD | F+M m = 56 years | Cyproheptadine + AP 4 weeks | Placebo + AP | TD symptoms, AEs |
| Koshino 1983 | 28 inpatients in Japan | schizophrenia + TD | F+M m = 59 years | Ergoloid mesylates + AP 6 weeks | Placebo + AP | TD symptoms, AEs, mental state |
| Libov 2007 | 40 inpatients in Israel | schizophrenia or schizoaffective disorder + TD | F+M 26‐69 years | Piracetam + AP 4 weeks | Placebo + AP | TD symptoms, AEs, global state |
| Mackay 1980 | 11 inpatients in the UK | various psychiatric conditions + TD | NR 56‐70 years | Lithium + AP 5 weeks | Placebo + AP | TD symptoms, AEs |
| Matsunaga 1988 | 37 inpatients in Japan | various psychiatric conditions + TD | F+M m = 59 years | Ceruletide + AP 4 weeks | Placebo + AP | TD symptoms, AEs |
| Meco 1989 | 10 inpatients in Italy | schizophrenia + TD | F+M 33‐72 years | Ritanserin + AP 4 weeks | Placebo + AP | TD symptoms, AEs, mental state |
| Mosnik 1997 | 18 in‐ and outpatients in the USA | schizophrenia + TD | M 28‐65 years | Phenylalanine + AP 1 day | Placebo + AP | Leaving the study early |
| Mouret 1991 | 20 inpatients in Morocco | schizophrenia + TD | F+M 20‐67 years | Insulin + AP 12 weeks | Placebo + AP | TD symptoms |
| O'Brien 2014 | 88 in‐ and outpatients in the USA | various psychiatric conditions + TD | NR 18‐85 years | NBI‐98854 (VMAT2 inhibitor valbenazine) + AP 6 weeks | Placebo + AP | TD symptoms, AEs |
| Rastogi 1982 | 40 inpatients in the UK | various psychiatric conditions + TD | F+M m = 70 years | Ergoloid mesylates + AP 6 weeks | Placebo + AP | TD symptoms |
| Richardson 2003 | 52 in‐ and outpatients in the USA | various psychiatric conditions + TD | M m = 45 years | Branched‐chain amino acids + AP 3 weeks | Placebo + AP | TD symptoms |
| Shamir 2000 | 19 inpatients in Israel | schizophrenia + TD | F+M 62‐91 years | Melatonin + AP 4 weeks | Placebo + AP | TD symptoms, AEs |
| Shamir 2001 | 22 inpatients in Israel | schizophrenia + TD | F+M 28‐82 years | Melatonin + AP 6 weeks | Placebo + AP | AEs |
| Shi 2009 | 76 inpatients in China | TD | F+M m = 56 years | Melatonin + AP 12 weeks | TAU + AP | Cognitive function |
| UCB Pharma 2005 | 69 inpatients in Belgium and Bulgaria | TD | F+M 18‐80 years | Levetiracetam + AP 8 weeks | Placebo + AP | TD symptoms, AEs |
| Wolkin 1986 | 16 in‐ and outpatients in the USA | schizophrenia + TD | M m = 54 years | Evening primrose oil + AP 6 weeks | Placebo + AP | TD symptoms, mental state |
| Woods 2008 | 50 outpatients in the USA | various psychiatric conditions + TD | F+M m = 47 years | Levetiracetam + AP 12 weeks | Placebo + AP | TD symptoms, mental state |
| Yang 1999 | 34 inpatients in China | schizophrenia + TD | F+M m = 50 years | Promethazine + AP 12 weeks | Placebo + AP | TD symptoms, AEs, mental state, global state |
| Zeng 1995 | 42 inpatients in China | schizophrenia + TD | F+M m = 32.5 years | Buspirone + AP 6 weeks | Placebo + AP | TD symptoms |
| Zeng 1996 | 46 inpatients in China | schizophrenia + TD | F+M m = 33 years | Pemoline + AP 6 weeks | Placebo + AP | TD symptoms |
| Zhang 2011 | 157 inpatients in China | schizophrenia + TD | M m = 45 years | Ginkgo biloba + AP 12 weeks | Placebo + AP | TD symptoms, mental state, cognitive function |
AE = adverse effects, AP = antipsychotics, EPS = extrapyramidal symptoms, F = female, M = male, m = mean, N = number, TAU = treatment as usual, TD = tardive dyskinesia
Search methods for identification of studies
Electronic searches
The 2017 review update was carried out in parallel with updating eight other TD reviews, see Table 10 for details. The search covered all nine TD reviews.
Cochrane Schizophrenia Group's Study‐Based Register of Trials
On 16 July 2015 and 26 April 2017, the information specialist searched the register using the following search strategy:
*Tardive Dyskinesia* in Health Care Condition Field of STUDY
In such a study‐based register, searching the major concept retrieves all the synonyms and relevant studies because all the studies have already been organised based on their interventions and linked to the relevant topics (Shokraneh 2017).
This register is compiled by systematic searches of major resources (AMED, BIOSIS, CINAHL, ClinicalTrials.Gov, Embase, MEDLINE, PsycINFO, PubMed, WHO ICTRP) and their monthly updates, ProQuest Dissertations and Theses A&I and its quarterly update, Chinese databases (CBM, CNKI, and Wanfang) and their annual updates, handsearches, grey literature, and conference proceedings (see Group's Module). There is no language, date, document type, or publication status limitations for inclusion of records into the register.
For previous searches, please see Appendix 1
Searching other resources
1. Reference searching
We inspected references of all identified studies for further relevant studies.
2. Personal contact
We contacted the first author of each included study for information regarding unpublished trials.
Data collection and analysis
For previous data collection and analysis please see Appendix 2
Selection of studies
For the 2017 update, Rosie Asher (RA and Antonio Grande (AG) (see Acknowledgements) inspected all abstracts of studies identified as above and selected potentially relevant reports. We resolved disagreement by discussion, or where there was still doubt, we acquired the full‐text article for further inspection. We acquired the full‐text articles of relevant reports/abstracts meeting initial criteria for re‐assessment and carefully inspected for a final decision on inclusion (see Criteria for considering studies for this review). RA and AG were not blinded to the names of the authors, institutions or journal of publication. Where difficulties or disputes arose, we asked review author Hanna Bergman (HB) for help and where it was impossible to decide, or if adequate information was not available to make a decision, we added these studies to those awaiting classification and contacted the authors of the papers for clarification.
Data extraction and management
1. Extraction
For the 2017 update, RA and HB independently extracted data from all included studies. Jun Xia (JX) and Sai Zhao (SZ) (see Acknowledgements) extracted data from studies in Chinese. For any problems, review author Karla Soares‐Weiser (KSW) helped clarify issues and we documented these final decisions. We extracted data presented only in graphs and figures whenever possible, but included only if two review authors independently had the same result. We attempted to contact authors through an open‐ended request in order to obtain missing information or for clarification whenever necessary. If studies were multi‐centre, where possible, we extracted data relevant to each component centre separately.
2. Management
2.1 Forms
For the 2017 update we extracted data online in Covidence. Extracted data are available here with a link to the original source PDF for each item.
2.2 Scale‐derived data
We included continuous data from rating scales only if: a) the psychometric properties of the measuring instrument have been described in a peer‐reviewed journal (Marshall 2000); and b) the measuring instrument has not been written or modified by one of the trialists for that particular trial. Ideally, the measuring instrument should either be i. a self‐report or ii. completed by an independent rater or relative (not the therapist). We realise that this is not often reported clearly, we noted in Description of studies if this was the case or not.
2.3 Endpoint versus change data
There are advantages of both endpoint and change data. Change data can remove a component of between‐person variability from the analysis. On the other hand, calculation of change needs two assessments (baseline and endpoint), which can be difficult in unstable and difficult to measure conditions such as schizophrenia. We decided primarily to use endpoint data, and only use change data if the former were not available. We combined endpoint and change data in the analysis as we preferred to use mean differences (MD) rather than standardised mean differences (SMD) throughout (Higgins 2011).
2.4 Skewed data
Continuous data on clinical and social outcomes are often not normally distributed. To avoid the pitfall of applying parametric tests to non‐parametric data, we applied the following standards to relevant data before inclusion.
Please note, we planned to enter data from studies of at least 200 participants in the analysis, because skewed data pose less of a problem in large studies. We entered all relevant change data as when continuous data are presented on a scale that includes a possibility of negative values (such as change data), it is difficult to tell whether data are skewed or not.
For endpoint data from studies < 200 participants:
(a) when a scale starts from the finite number zero, we subtracted the lowest possible value from the mean, and divided this by the standard deviation (SD). If this value was lower than 1, it strongly suggests a skew and we excluded these data. If this ratio was higher than one but below 2, there is suggestion of skew. We entered these data and tested whether their inclusion or exclusion changed the results substantially. Finally, if the ratio was larger than 2 we included these data, because skew is less likely (Altman 1996; Higgins 2011).
(b) if a scale starts from a positive value (such as the Positive and Negative Syndrome Scale (PANSS), (Kay 1986), which can have values from 30 to 210), we modified the calculation described above to take the scale starting point into account. In these cases skew is present if 2 SD > (S‐S min), where S is the mean score and 'S min' is the minimum score.
2.5 Common measure
Where relevant, to facilitate comparison between trials, we converted variables that can be reported in different metrics, such as days in hospital (mean days per year, per week or per month) to a common metric (e.g. mean days per month).
2.6 Conversion of continuous to binary
Where possible, we converted continuous outcome measures to dichotomous data. This can be done by identifying cut‐off points on rating scales and dividing participants accordingly into 'clinically improved' or 'not clinically improved'. It is generally assumed that if there is a 50% reduction in a scale‐derived score such as the Brief Psychiatric Rating Scale (BPRS, Overall 1962) or the Positive and Negative Syndrome Scale (PANSS, Kay 1986), this can be considered as a clinically significant response (Leucht 2005a; Leucht 2005b). If data based on these thresholds were not available, we used the primary cut‐off presented by the original authors.
2.7 Direction of graphs
Where possible, we entered data in such a way that the area to the left of the line of no effect indicated a favourable outcome for the active intervention. Where keeping to this made it impossible to avoid outcome titles with clumsy double‐negatives (e.g. 'Not un‐improved'), we presented data where the left of the line indicates an unfavourable outcome and noted this in the relevant graphs.
Assessment of risk of bias in included studies
RA and HB independently assessed risk of bias within the included studies by using criteria described in the Cochrane Handbook for Systematic Reviews of Interventions to assess trial quality (Higgins 2011). This set of criteria is based on evidence of associations between overestimate of effect and high risk of bias of the article such as sequence generation, allocation concealment, blinding, incomplete outcome data and selective reporting.
If the raters disagreed, we made the final rating by consensus, with the involvement of another member of the review group. Where inadequate details of randomisation and other characteristics of trials were provided, we contacted authors of the studies contacted in order to obtain further information. If non‐concurrence occurred, we reported this.
We noted the level of risk of bias in the text of the review and in Figure 2, Figure 3 and Table 8.
2.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
3.

'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Summary of findings 8. POLYPEPTIDE ‐ CERULETIDE versus PLACEBO for antipsychotic‐induced tardive dyskinesia.
| CERULETIDE versus PLACEBO for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: female and male 55‐59 year old (mean) patients with various psychiatric conditions and antipsychotic‐induced tardive dyskinesia Settings: in‐ and outpatients in Japan Intervention: ceruletide (0.8 microgram/kg/week) versus placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | CERULETIDE | |||||
| Tardive dyskinesia: No clinically important improvement ‐ not reported | This outcome was not reported. | |||||
|
Tardive dyskinesia: Deterioration of symptoms follow‐up: 4‐8 weeks |
20 per 1000 | 19 per 1000 (3 to 133) | RR 0.97 (0.14 to 6.80) | 103 (2 RCTs) | ⊕⊕⊝⊝ low1,2 | |
|
Adverse effects ‐ any adverse effect follow‐up: 4‐8 weeks |
233 per 1000 | 308 per 1000 (173 to 551) | RR 1.32 (0.74 to 2.36) | 122 (2 RCTs) | ⊕⊕⊝⊝ low1,2 | |
|
Acceptability of treatment (measured by participants leaving the study early) follow‐up: 8 weeks |
214 per 1000 | 234 per 1000 (105 to 514) | RR 1.09 (0.49 to 2.40) | 85 (1 RCT) | ⊕⊝⊝⊝ very low1,2,3 | |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | This outcome was not reported. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RCT: randomised controlled trial; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for risk of bias: unclear methods of randomisation, blinding not assessed, and potential introduction of detection bias due to subjective nature of outcome assessments. 2 Downgraded one step for imprecision: the two included studies included only 132 participants and the 95% CI around the effect estimate indicated both appreciable benefit for ceruletide and no effect.
3 Downgraded one step for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability.
Measures of treatment effect
1. Binary data
For binary outcomes we calculated a standard estimation of the risk ratio (RR) and its 95% confidence interval (CI). It has been shown that RR is more intuitive (Boissel 1999) than odds ratios as odds ratios tend to be interpreted as RR by clinicians (Deeks 2000).
2. Continuous data
For continuous outcomes we estimated mean difference (MD) between groups. We preferred not to calculate effect size measures (standardised mean difference (SMD)). However, if scales of very considerable similarity were used, we presumed there was a small difference in measurement, and calculated effect size and transformed the effect back to the units of one or more of the specific instruments.
Unit of analysis issues
1. Cluster trials
Studies increasingly employ 'cluster randomisation' (such as randomisation by clinician or practice) but analysis and pooling of clustered data poses problems. Firstly, authors often fail to account for intra‐class correlation in clustered studies, leading to a 'unit of analysis' error (Divine 1992) whereby P values are spuriously low, confidence intervals unduly narrow and statistical significance overestimated. This causes type I errors (Bland 1997; Gulliford 1999).
Had cluster trials been included and clustering had not been accounted for in primary studies, we would have presented such data in a table, with a (*) symbol to indicate the presence of a probable unit of analysis error. In subsequent versions of this review, if cluster‐randomised trials are included, we will seek to contact first authors of studies to obtain intra‐class correlation coefficients ICCs) for their clustered data and adjust for this by using accepted methods (Gulliford 1999). Where clustering has been incorporated into the analysis of primary studies, we will present these data as if from a non‐cluster randomised study, but adjust for the clustering effect.
We have sought statistical advice and have been advised that the binary data as presented in a report should be divided by a 'design effect'. This is calculated using the mean number of participants per cluster (m) and the ICC [Design effect=1+(m‐1)*ICC] (Donner 2002). If the ICC is not reported it will be assumed to be 0.1 (Ukoumunne 1999).
If cluster studies have been appropriately analysed taking into account ICCs and relevant data documented in the report, synthesis with other studies would be possible using the generic inverse variance technique.
2. Cross‐over trials
A major concern of cross‐over trials is the carry‐over effect. It occurs if an effect (e.g. pharmacological, physiological or psychological) of the treatment in the first phase is carried over to the second phase. As a consequence, on entry to the second phase the participants can differ systematically from their initial state despite a wash‐out phase. For the same reason cross‐over trials are not appropriate if the condition of interest is unstable (Elbourne 2002). As both effects are very likely in severe mental illness, we only used data of the first phase of cross‐over studies.
3. Studies with multiple treatment groups
Where a study involved more than two treatment arms, if relevant, we presented the additional treatment arms in comparisons. If data were binary we simply added and combined within the two‐by‐two table. If data were continuous, we combined data following the formula in section 7.7.3.8 (Combining groups) of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We did not use data where the additional treatment arms were not relevant.
Dealing with missing data
1. Overall loss of credibility
At some degree of loss of follow‐up, data must lose credibility (Xia 2009). We chose that, for any particular outcome, should more than 50% of data be unaccounted for, we would not reproduce these data or use them within analyses. If, however, more than 50% of those in one arm of a study were lost, but the total loss was less than 50%, we addressed this within the 'Summary of findings' table/s by down‐rating quality. We also downgraded quality within the 'Summary of findings' table/s should loss be 25% to 50% in total.
2. Binary
In the case where attrition for a binary outcome was between 0% and 50% and where these data were not clearly described, we presented data on a 'once‐randomised‐always‐analyse' basis (an intention‐to‐treat (ITT) analysis). We assumed all those leaving the study early to have no improvement. We undertook a sensitivity analysis to test how prone the primary outcomes were to change by comparing data only from people who completed the study to that point to the ITT analysis using the above assumptions.
3. Continuous
3.1 Attrition
We reported and used data where attrition for a continuous outcome was between 0% and 50%, and data only from people who completed the study to that point were reported.
3.2 Standard deviations
If standard deviations (SDs) were not reported, we first tried to obtain the missing values from the authors. If not available, where there were missing measures of variance for continuous data, but an exact standard error (SE) and confidence intervals available for group means, and either the P value or t value available for differences in mean, we calculated them according to the rules described in the Cochrane Handbook for Systematic reviews of Interventions (Higgins 2011). When only the SE is reported, SDs are calculated by the formula SD=SE * square root (n). Chapters 7.7.3 and 16.1.3 of the Cochrane Handbook for Systematic reviews of Interventions (Higgins 2011) present detailed formulae for estimating SDs from P values, t or F values, confidence intervals, ranges or other statistics. If these formulae did not apply, we calculated the SDs according to a validated imputation method which is based on the SDs of the other included studies (Furukawa 2006). Although some of these imputation strategies can introduce error, the alternative would be to exclude a given study’s outcome and thus to lose information. We nevertheless examined the validity of the imputations in a sensitivity analysis excluding imputed values.
3.3 Assumptions about participants who left the trials early or were lost to follow‐up
Various methods are available to account for participants who left the trials early or were lost to follow‐up. Some trials just present the results of study completers, others use the method of last observation carried forward (LOCF), while more recently methods such as multiple imputation or mixed‐effects models for repeated measurements (MMRM) have become more of a standard. While the latter methods seem to be somewhat better than LOCF (Leon 2006), we feel that the high percentage of participants leaving the studies early and differences in the reasons for leaving the studies early between groups is often the core problem in randomised schizophrenia trials. We therefore did not exclude studies based on the statistical approach used. However, we prefered to use the more sophisticated approaches. (e.g. MMRM or multiple‐imputation) and only presented completer analyses if some kind of ITT data were not available at all. Moreover, we addressed this issue in the item "incomplete outcome data" of the 'Risk of bias' tool.
Assessment of heterogeneity
1. Clinical heterogeneity
We considered all included studies initially, without seeing comparison data, to judge clinical heterogeneity. We simply inspected all studies for clearly outlying people or situations which we had not predicted would arise and discussed these in the text if they arose.
2. Methodological heterogeneity
We considered all included studies initially, without seeing comparison data, to judge methodological heterogeneity. We simply inspected all studies for clearly outlying methods which we had not predicted would arise and discussed these in the text if they arose.
3. Statistical heterogeneity
3.1 Visual inspection
We visually inspected graphs to investigate the possibility of statistical heterogeneity.
3.2 Employing the I2 statistic
We investigated heterogeneity between studies by considering the I2 method alongside the Chi2 P value. The I2 provides an estimate of the percentage of inconsistency thought to be due to chance (Higgins 2003). The importance of the observed value of I2 depends on i. magnitude and direction of effects and ii. strength of evidence for heterogeneity (e.g. P value from Chi2 test, or a confidence interval for I2). An I2 estimate greater than or equal to around 50% accompanied by a statistically significant Chi2 statistic, can be interpreted as evidence of substantial levels of heterogeneity (Section 9.5.2 Cochrane Handbook for Systematic Reviews of InterventionsHiggins 2011). We explored and discussed in the text potential reasons for substantial levels of heterogeneity (Subgroup analysis and investigation of heterogeneity).
Assessment of reporting biases
Reporting biases arise when the dissemination of research findings is influenced by the nature and direction of results (Egger 1997). These are described in Section 10 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We are aware that funnel plots may be useful in investigating reporting biases but are of limited power to detect small‐study effects. We did not use funnel plots for outcomes where there were 10or fewer studies, or where all studies were of similar sizes. In future versions of this review, if funnel plots are possible, we will seek statistical advice in their interpretation.
Data synthesis
We understand that there is no closed argument for preference for use of fixed‐effect or random‐effects models. The random‐effects method incorporates an assumption that the different studies are estimating different, yet related, intervention effects. This often seems to be true to us and the random‐effects model takes into account differences between studies even if there is no statistically significant heterogeneity. There is, however, a disadvantage to the random‐effects model. It puts added weight onto small studies, which often are the most biased ones. Depending on the direction of effect these studies can either inflate or deflate the effect size. We chose the fixed‐effect model for all analyses.
Subgroup analysis and investigation of heterogeneity
1. Subgroup analyses
With this wide range of miscellaneous treatments of mainly experimental interventions, we did not expect many studies or participants per intervention that would enable us to carry out subgroup analyses. We proposed to undertake this review and provide an overview of the effects of this group of miscellaneous treatments for people with schizophrenia in general. In addition, however, we tried to report data on subgroups of people in the same clinical state, stage and with similar problems.
2. Investigation of heterogeneity
We reported when inconsistency was high. First, we investigated whether data were entered correctly. Second, if data were correct, we visually inspected the graph and successively removed outlying studies to see if homogeneity is restored. For this review we decided that should this occur with data contributing to the summary finding of no more than around 10% of the total weighting, we would present data. If not, we did not pool such data and discussed issues. We know of no supporting research for this 10% cut‐off but are investigating use of prediction intervals as an alternative to this unsatisfactory state.
When unanticipated clinical or methodological heterogeneity were obvious, we simply discussed the issues. We did not undertake sensitivity analyses relating to these.
Sensitivity analysis
1. Implication of randomisation
If trials were described in some way as to imply randomisation, we planned to undertake a sensitivity analyses for the primary outcomes. We would have included these studies in the analyses and if there was no substantive difference when the implied randomised studies were added to those with better description of randomisation, then we would have used relevant data from these studies.
2. Assumptions for lost binary data
Where assumptions had to be made regarding people lost to follow‐up (see Dealing with missing data), we compared the findings of the primary outcomes when we used our assumption compared with completer data only. If there was a substantial difference, we reported and discussed these results but continued to employ our assumption.
Where assumptions have to be made regarding missing SDs data (see Dealing with missing data), we compared the findings on primary outcomes when we used our assumption compared with completer data only. We undertook a sensitivity analysis to test how prone results were to change when 'completer' data only were compared to the imputed data using the above assumption. If there was a substantial difference, we reported and discussed these results but continued to employ our assumption.
3. Risk of bias
We analysed the effects of excluding trials that we judged to be at high risk of bias across one or more of the domains of randomisation Risk of bias in included studies for the meta‐analysis of the primary outcomes. If the exclusion of trials at high risk of bias did not substantially alter the direction of effect or the precision of the effect estimates, we included data from these trials in the analysis.
4. Imputed values
Had we included cluster‐randomised trials, we planned to undertake a sensitivity analysis to assess the effects of including data from trials where we used imputed values for ICC in calculating the design effect in cluster‐randomised trials.
5. Fixed and random effects
We synthesised data using a fixed‐effect model, however, we also synthesised data for the primary outcomes using a random‐effects model to evaluate whether this altered the significance of the results.
If we found substantial differences in the direction or precision of effect estimates in any of the sensitivity analyses listed above, we did not pool data from the excluded trials with the other trials contributing to the outcome, but presented them separately.
Results
Description of studies
Please see Characteristics of included studies; Characteristics of excluded studies; Characteristics of studies awaiting classification, and Characteristics of ongoing studies.
Results of the search
The updated searches carries out in 2015 and 2017 were part of an update of nine Cochrane reviews, see Table 10.
The 2015 search retrieved 704 references for 344 studies, see Figure 4 for study flow diagram. We also screened the full texts of 10 additional records that were identified through screening reference lists of Cochrane reviews on tardive dyskinesia (TD). From these records we identified 60 new potentially relevant records for this review and screened the full texts. Agreement about which studies may have been randomised was 100%.
4.

Study flow diagram for 2015 and 2017 searches.
Twenty‐six of these 60 new records are records for the 21 new included studies in this update (Bucci 1971; Castro 2011; Gardos 1979; Glover 1980; Goff 1993; Hajioff 1983; Koshino 1979; Koshino 1983; Meco 1989; O'Brien 2014; Rastogi 1982; Richardson 2003; Shamir 2000; Shamir 2001; Shi 2009; UCB Pharma 2005; Woods 2008; Yang 1999; Zeng 1995; Zeng 1996; Zhang 2011). Three of the records are new companion papers to two previously included studies (Libov 2007; Mosnik 1997). Twenty of the new records were excluded (11 new unique excluded studies: Chaplin 2002; Fann 1973; Goetz 2013; Huang 1981; Kabes 1985; Lieberman 1987; Lieberman 1994; Moore 1980; Shah 2012; Tamminga 1983; Vaddadi 2002), and three of which were companions to previously excluded studies (Casey 1981; Kabes 1982; Vaddadi 1989). Four of the 60 records are in awaiting classification under three of the studies (Fernandez 2016; Hauser 2016; NCT01393600 2011) and seven are ongoing studies (Garcia 1992; ISRCTN14688109 2015; NCT00621634 2008; NCT01391390 2011; NCT01688037 2012; NCT01804920 2013; NCT02291861 2014).
The 2017 search found eight records (five studies). The editorial base of Cochrane Schizophrenia screened these records and six records (four studies) have been put into awaiting classification (Fernandez 2016; Hauser 2016; Pattojoshi 2016; Xu 2012), see Characteristics of studies awaiting classification. The two remaining records are companion papers to an included study identified in the 2015 search (O'Brien 2014).
In addition, one previously excluded study could be included (Cai 1988), two studies that were in awaiting classification in the previous version of the review could be excluded (Bockenheimer 1976; Koller 1982), and one study that was in awaiting classification in the previous review was in fact a companion to the included study Libov 2007.
Included studies
This review now includes 31 studies of 24 interventions with 1278 participants, published between 1971 and 2014. See Table 11 for an overview of characteristics of the included studies.
1. Methods
All studies were stated to be randomised and most were double‐blind. For further details please see sections below on allocation and blinding.
2. Design
All included studies presented a parallel longitudinal design. Seven of the 31 studies used a cross‐over design with two periods (Gardos 1979; Libov 2007; Mackay 1980; Meco 1989; Mosnik 1997; Shamir 2000; Shamir 2001). We had considered this as likely when embarking on the review and have used only the data from before the first cross‐over for the reasons outlined above (Unit of analysis issues).
3. Duration
Most studies were of short duration (less than nine weeks) and only one had a follow‐up period longer than three months (Bucci 1971).
4. Participants
Participants, now totalling 1278 people, were mostly men in their 50s, with diagnoses of various chronic psychiatric disorders, but mainly schizophrenia. All had antipsychotic‐induced TD though only eight trials explicitly described the use of criteria for the diagnosis of TD. The number of participants ranged from 10 to 157 (median 34).
5. Setting
Most trials were conducted in hospital, seven included both in‐ and outpatients (Castro 2011; Emsley 2006; Kojima 1992; Mosnik 1997; O'Brien 2014; Richardson 2003; Wolkin 1986), and five included only outpatients (Bucci 1971; Glazer 1985; Glover 1980; Goff 1993; Woods 2008). The studies themselves were from around the world, with 10 conducted in the USA (Bucci 1971; Gardos 1979; Glazer 1985; Glover 1980; Goff 1993; Mosnik 1997; O'Brien 2014; Richardson 2003; Wolkin 1986; Woods 2008), six in China (Cai 1988; Shi 2009; Yang 1999; Zeng 1995; Zeng 1996; Zhang 2011), four in Japan (Kojima 1992; Koshino 1979; Koshino 1983; Matsunaga 1988), three in Israel (Libov 2007; Shamir 2000; Shamir 2001), three in the UK (Hajioff 1983; Mackay 1980; Rastogi 1982), and one each in Italy (Meco 1989), Venezuela (Castro 2011), South Africa (Emsley 2006), Morocco (Mouret 1991), and Belgium/Bulgaria (UCB Pharma 2005).
6. Interventions
6.1 Miscellaneous drugs
6.1.1 Alkaloids
a. Co‐dergocrine mesylate (Hydergine)
Co‐dergocrine mesylate (Hydergine; dihydrogenated ergot alkaloids) is an ergot alkaloid used to treat patients with dementia. Hajioff 1983 and Rastogi 1982 both used co‐dergocrine mesylate in a dose of 4.5 mg/day. Koshino 1983 used dihydrogenated ergot alkaloids in a dose of 6 mg/day.
b. L‐stepholidine
Stepholidine is a naturally occurring chemical compound found in the herb Stephania intermedia.Cai 1988 used L‐stepholidine in a dose of two tablets, three times per day (no exact dosage provided).
c. Papaverine
Papaverine is a vasodilating agent. Gardos 1979 used papaverine in a dose ranging from 300 mg/day to 600 mg/day.
6.1.2 Amino acids
a. Branched‐chain amino acids (BCAAs)
BCAAs are essential amino acids. Richardson 2003 used branched‐chain amino acids in a dose ranging from 56 mg/kg to 222 mg/kg body weight.
b. Phenylalanine
Phenylalanine is an essential amino acid. Mosnik 1997 used phenylalanine in a dose of 100 mg/kg body weight for one day.
6.1.3 Antidepressant
a. MAO‐B inhibitor ‐ Selegeline
Goff 1993 used selegeline, a drug that is mainly used to reduce symptoms of Parkinson's.
b. Monoamine oxidase inhibitor (MAOI) ‐ Isocarboxazid
Isocarboxazid is a MAOI) Bucci 1971 used isocarboxazid in a dose ranging from 20 mg/day to 100 mg/day.
c. SSRI ‐ Ritanserin
Ritanserin is an experimental serotonin receptor antagonist and was used in Meco 1989.
6.1.4 Antiepileptics
a. Levetiracetam
Levetiracetam is a medication used to treat epilepsy. It was used by two studies (UCB Pharma 2005; Woods 2008) in a maximum dose of 3000 mg/day.
6.1.5 Antihistamines
a. Cyproheptadine
Cyproheptadine is a first‐generation antihistamine with additional anticholinergic, antiserotonergic, and local anaesthetic properties. Koshino 1979 used cyproheptadine in a dose ranging from 12 mg/day to 24 mg/day.
6.1.6 Antipsychotics
a. Promethazine
Yang 1999 used promethazine, a drug mainly used for sedation and to treat nausea.
6.1.7 Anxiolytics
a. Buspirone
Buspirone is an anxiolytic psychotropic drug used to treat general anxiety disorder. It was used by one study (Zeng 1995) in a dose of 6 to 12 capsules per day (exact dose not provided).
6.1.8 Cognitive enhancer
a. Pemoline
Pemoline is a stimulant drug of the 4‐oxazolidinone class. It was used by Zeng 1996 in a dose of two capsules per day (exact dose not provided).
b. Piracetam
Piracetam is a cyclic derivative of GABA. Libov 2007 used piracetam in a dose of 4800 mg/day.
6.1.9 Enzyme inhibitor
a. Valbenazine (NBI‐98854)
Valbenazine is a vesicular monoamine transporter type 2 (VMAT2) inhibitor. O'Brien 2014 used NBI‐98854 in a dose ranging from 25 mg/day to 75 mg/day.
6.1.10 Fatty acid
a. Ethyl‐EPA
Ethyl‐EPA is a derivative of eicosapentaenoic acid (EPA), an omega‐3 fatty acid. Emsley 2006 used ethyl‐EPA in a dose of 2 g/day.
b. Gamma‐linolenic acid
Gamma‐linolenic acid was first isolated form the seed oil of evening primrose. It was used by one study (Wolkin 1986) in a dose of 600 mg/day.
6.1.11 Herb
a. EGb‐761
EGb‐761 is the standardised extract of Ginkgo biloba leaves that has antioxidant properties as a free radical scavenger. It was used by Zhang 2011 in a dose of 240 mg/day.
6.1.12 Hormone
a. Oestrogen
Oestrogen is the primary female sex hormone. Glazer 1985 used oestrogen in a dose of 1.25 mg/day.
b. Insulin
Insulin is a peptide hormone produced by the pancreas. Mouret 1991 used insulin in a dose of 10 units per day (exact dose not provided).
c. Melatonin
Melatonin is a naturally occurring hormone. Four studies (Castro 2011; Shamir 2000; Shamir 2001; Shi 2009) used melatonin in doses ranging from 2 mg/day to 20 mg/day.
6.1.13 Mood stabiliser
a. Lithium
Lithium is primary used for bipolar disorder. Mackay 1980 used lithium in an unspecified dose.
6.1.14 Polypeptide
a. Ceruletide
Ceruletide is a 10 amino acid oligopeptide that stimulates smooth muscle and increases digestive secretions. Kojima 1992 and Matsunaga 1988 both used ceruletide in a dose of 0.8 microgram/kg/week.
6.2 Other miscellaneous treatments
6.2.1 Hypnosis or relaxation
Glover 1980 used eight sessions of hypnosis or relaxation.
6.3 Comparison groups
In most of the studies a placebo was used as a comparison group, with few further details given. In one study the comparison group was given procyclidine (Bucci 1971), which is an anticholinergic drug (see also Bergman 2018a). Three studies (Gardos 1979; Glover 1980; Shi 2009) compared active intervention against standard treatment.
Participants remained on schizophrenia treatment antipsychotic medication during the trials.
7. Outcomes
7.1 General
Some outcomes were presented in graphs, inexact P values of differences, or a statement of significant or non‐significant difference. This made it impossible to acquire raw data for synthesis. Some continuous outcomes could not be extracted due to missing number of participants or missing means, standard deviations, or standard errors. All included studies used the last observation carried forward (LOCF) strategy for the intention‐to‐treat (ITT) analysis of dichotomous data.
7.2 Scales used to measure the TD symptoms
We have shown details of the scales that provided usable data below. We have provided reasons for exclusions of data under 'Outcomes' in the Characteristics of included studies table.
7.2.1 Abnormal Involuntary Movement Scale (AIMS)
The AIMS (Guy 1976) is a 12‐item scale consisting of a standardised examination followed by questions rating the orofacial, extremity and trunk movements, as well as three global measurements. Each of these 10 items can be scored from zero (none) to four (severe). Two additional items assess the dental status. The AIMS ranges from zero to 40, with higher scores indicating greater severity.
7.2.2 Abbreviated Dyskinesia Rating Scale ‐ Simpson Rating Scale (SRS)
This 15‐item scale measures the movements around the orofacial region, neck, trunk and extremities (Simpson 1979). Each of these items can be scored from one (absent) to six (severe). This scale ranges from 10 to 102 with higher scores indicating greater severity.
7.2.3 Rockland Tardive Dyskinesia Rating Scale‐ Rockland TD
The Rockland TD (Simpson 1970) is a 34‐item scale consisting of measurement of the movements around the orofacial region, neck, trunk and extremities. Each of these items can be scored from zero (absent) to five (severe). This scale ranges from 10 to 102, with higher scores indicating greater severity.
7.2.4 Extrapyramidal symptom rating scale (ESRS)
The ESRS was developed to assess four types of drug‐induced movement disorders (DIMD): parkinsonism, akathisia, dystonia, and TD (Chouinard 2005). The score for TD, ranging from zero to 42, is based on the sum of all seven items in the TD objective examination.
7.2.5 St. Hans Rating Scale (SHRS) for extrapyramidal syndromes
The SHRS is a multidimensional rating scale for the evaluation of antipsychotic‐induced hyperkinesia, parkinsonism, akathisia and dystonia (Gerlach 1993). Each item is rated from zero (not present) to six (present to an extreme degree). This gives a total score from zero to 48 for hyperkinesia and parkinsonism.
7.3 Scales used to measure global‐ and mental state and behaviour
7.3.1 Brief Psychiatric Rating Scale (BPRS)
The BPRS is an 18‐item scale measuring positive symptoms, general psychopathology and affective symptoms (Overall 1962). The original scale has 16 items, although a revised 18‐item scale is commonly used. Total scores can range from zero to 126. Each item is rated on a seven‐point scale, with high scores indicating more severe symptoms.
7.3.2 Wechsler Adult Intelligence Scale (WAIS
The WAIS is an IQ test designed to measure intelligence and cognitive ability in adults and older adolescents (Wechsler 1958).
7.3.3 Wechsler Memory Scale (WMS)
The WMS is a neuropsychological test designed to measure different memory functions in a person (Wechsler 1945).
7.3.4 Positive and Negative Syndrome Scale (PANSS)
The PANSS is a medical scale used for measuring symptom severity of patients with schizophrenia (Kay 1987). The patient is rated from one to seven on 30 different symptoms based on the interview as well as reports of family members or primary care hospital workers.
7.3.5 Continuous performance test (CPT)
The CPT is a neurophysiological test that measures a person's sustained and selective attention (Rosvold 1956).
7.3.6 Clinical Global Impression Scale (CGI)
The CGI assesses both severity of illness and clinical improvement by comparing conditions of the person standardised against other people with the same diagnosis (Guy 1976).
7.4 Scales used to measure adverse events
7.4.1 Treatment Emergent Symptom Scale (TESS)
The TESS is a checklist that assesses a variety of characteristics for each adverse event (Guy 1976).
Excluded studies
There are 39 excluded studies. Sixteen studies (Bjorndal 1980; Blum 1984; Bowers 1979: Casey 1981; Gardos 1978; Jus 1974; Korsgaard 1981; Moore 1980; Prange 1973; Reda 1974; Reker 1982; Simpson 1976 a; Simpson 1976 b; Villeneuve 1970; Villeneuve 1980; Volavka 1986) were not randomised and we have therefore excluded them. Eight studies (Apseloff 2000; Chaplin 2002; Emsley 2002; Goetz 2013; Lieberman 1987; Lieberman 1994; Shah 2012; Vaddadi 2002) were excluded because participants had schizophrenia or other disorders but not TD. After unfruitful attempts to contact authors for further details, we have also excluded a further 14f randomised studies which reported no usable data (Fann 1973; Fudge 1991; Gerlach 1975; Jus 1978; Kabes 1982; Kabes 1985; Koller 1982; Lindenmayer 1988; Nasrallah 1986; Peselow 1989; Tamminga 1983; Vaddadi 1989; Wonodi 2004). One study that was excluded in the previous version of this review (Huang 1981), and Bockenheimer 1976 that was previously in awaiting classification, have now been included in other intervention reviews for TD and were excluded from this review.
Awaiting classification
There are currently five studies awaiting classification.
Fernandez 2016 investigated the VMAT‐2 inhibitor deutetrabenazine (SD‐809) compared to placebo in participants with TD in the USA and three European countries. We could only identify a conference abstract with limited details for this study. We are awaiting more detailed data to add to the review.
Hauser 2016 investigated the VMAT‐2 inhibitor valbenazine (NBI‐98854) compared to placebo in participants with TD in Canada, Puerto Rico, and the USA. We could only identify two conference abstracts, a poster, and an online trial registry record with limited details for this study. We are awaiting more detailed data to add to the review.
NCT01393600 2011 investigated the VMAT‐2 inhibitor valbenazine (NBI‐98854) compared to placebo in participants with TD in the USA. This online cross‐over trial record reported outcome results for combined groups only. We are awaiting separate results for the period before cross‐over.
Pattojoshi 2016 investigated right dorsolateral prefrontal cortex‐repetitive transcranial magnetic stimulation (rTMS) versus sham rTMS in participants with TD. We could only identify a conference abstract with limited details for this study. We are awaiting more detailed data to add to the review.
Xu 2012 investigated Ginkgo biloba extract versus standard treatment in participants with TD in China. We are awaiting translation of this article in Chinese.
Ongoing studies
We identified seven ongoing studies.
Garcia 1992 investigates buspirone compared with placebo in participants with TD in the USA.
ISRCTN14688109 2015 investigates cannabidiol extract compared to vitamin E in participants with TD in Nigeria.
NCT00621634 2008 investigates omega‐3 fish oil capsules (including docosahexaenoic acid) compared to placebo in participants with TD in Canada.
NCT01391390 2011 investigates melatonin compared to placebo in participants with TD in China.
(NCT01688037 2012 investigates the VMAT‐2 inhibitor valbenazine (NBI‐98854) compared to placebo in participants with TD in the USA and Puerto Rico.
NCT01804920 2013 investigates d‐serine compared to placebo in participants with TD in Israel.
NCT02291861 2014 investigates the VMAT‐2 inhibitor deutetrabenazine (SD‐809) compared to placebo in participants with TD in the USA and five European countries.
Risk of bias in included studies
Please refer to Figure 2 and Figure 3 for graphical overviews of the risk of bias in the included studies.
Allocation
Only four studies (Shamir 2000; Shamir 2001; Yang 1999; Zhang 2011) were rated at low risk of selection bias. These studies were randomised centrally and described concealed allocation to groups. Most other studies were not explicit about how allocation was achieved or how a randomised sequence was generated other than using the word "randomized".
Blinding
Although most studies were stated to be conducted on a double‐blind basis, only five studies (Cai 1988; Goff 1993; Mackay 1980; Shamir 2000; Zhang 2011) explicitly described how blinding of the participants, personnel, and outcome assessors was performed. No study reported testing the blindness of raters, clinicians and trial participants. Many of the other studies gave no further details other than stating that they were double‐blinded.
Incomplete outcome data
Most studies reported that either all participants completed the study, or analysed outcomes for all randomised participants. Five studies (Goff 1993; Kojima 1992; Libov 2007; Matsunaga 1988; UCB Pharma 2005) were rated as having a high risk of attrition bias, due to high rate of participants who dropped out and a lack of ITT analyses.
Selective reporting
The majority of data in this review originates from published reports. Expected outcomes (impact on TD symptoms) were reported for most of the trials. Five studies reported results of all outcomes listed in the methods section fully (Glover 1980; Libov 2007; Shi 2009; Yang 1999; Zeng 1995; Zeng 1996). We rated risk of reporting bias for many of the other studies as unclear because we have had no opportunity to see protocols of these trials to compare the outcomes reported in the full‐text publications with what was measured during the conduct of the trial. Eleven studies did not fully report outcomes that were measured during the study and were rated at high risk of reporting bias. Attempts to contact authors of trials for additional data were unsuccessful.
Other potential sources of bias
All studies had small or very small sample sizes, which increases the likelihood of treatment effects going undetected. Seven of the studies used a cross‐over design (Gardos 1979; Libov 2007; Mackay 1980; Meco 1989; Mosnik 1997; Shamir 2000; Shamir 2001). One study (Glazer 1985) was rated at high risk of bias as they described unequal groups at baseline with regard to duration of TD symptoms and medication use.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7; Table 8; Table 9
Summary of findings for the main comparison. ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO for antipsychotic‐induced tardive dyskinesia.
| DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: female and male 59‐80 (mean) years old patients with antipsychotic‐induced tardive dyskinesia Settings: inpatients in Japan and the UK Intervention: dihydrogenated ergot alkaloids (co‐dergocrine mesylate) (4.5 mg/day to 6 mg/day) versus placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | DIHYDROGENATED ERGOT ALKALOIDS | |||||
| Tardive dyskinesia: No clinically important improvement follow‐up: 6 weeks | 786 per 1000 | 354 per 1000 (165 to 762) | RR 0.45 (0.21 to 0.97) | 28 (1 RCT) | ⊕⊕⊝⊝ low1,2 | |
|
Tardive dyskinesia: Deterioration of symptoms follow‐up: 6 weeks |
71 per 1000 | 24 per 1000 (1 to 539) | RR 0.33 (0.01 to 7.55) | 28 (1 RCT) | ⊕⊝⊝⊝ very low1,3 | |
|
Adverse effects ‐ any adverse effect follow‐up: 6 weeks |
214 per 1000 | 499 per 1000 (161 to 1000) | RR 2.33 (0.75 to 7.23) | 28 (1 RCT) | ⊕⊝⊝⊝ very low1,3 | |
|
Acceptability of treatment (measured by participants leaving the study early) follow‐up: 6 weeks |
42 per 1000 | 14 per 1000 (1 to 305) | RR 0.33 (0.02 to 7.32) | 48 (2 RCTs) | ⊕⊝⊝⊝ very low1,3,4 | |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | This outcome was not reported. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RCT: randomised controlled trial; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for risk of bias: randomisation procedure and allocation concealment were not adequately described. 2 Downgraded one step for imprecision: very small sample size and few events reported. 3 Downgraded two steps for imprecision: very small sample size and very few events reported with the 95% CI around the effect estimate indicating both appreciable benefit for dihydrogenated ergot alkaloids and no effect. 4 Downgraded one step for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability.
Summary of findings 2. ANTIEPILEPTIC ‐ LEVETIRACETAM versus PLACEBO for antipsychotic‐induced tardive dyskinesia.
| LEVETIRACETAM versus PLACEBO for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: female and male 47‐54 years old (mean) patients with various psychiatric conditions and antipsychotic‐induced tardive dyskinesia Settings: in‐ and outpatients in Belgium, Bulgaria, and the USA Intervention: levetiracetam (1500 mg twice per day) versus placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | LEVETIRACETAM | |||||
| Tardive dyskinesia: No clinically important improvement ‐ not reported | This outcome was not reported. | |||||
| Tardive dyskinesia: Deterioration of symptoms ‐ not reported | This outcome was not reported. | |||||
|
Adverse effects ‐ any adverse effect follow‐up: 8 weeks |
457 per 1000 | 233 per 1000 (114 to 475) | RR 0.51 (0.25 to 1.04) | 69 (1 RCT) | ⊕⊕⊝⊝ low1,2 | |
| Acceptability of treatment (measured by participants leaving the study early) follow‐up: 8‐12 weeks | 167 per 1000 | 168 per 1000 (77 to 370) | RR 1.01 (0.46 to 2.22) | 119 (2 RCTs) | ⊕⊝⊝⊝ very low1,2,3 | |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | This outcome was not reported. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RCT: randomised controlled trial; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for risk of bias: randomisation procedure, allocation concealment and blinding were not adequately described. 2 Downgraded one step for imprecision: small sample size and few events reported with the 95% CI around the effect estimate indicating both appreciable benefit for levetiracetam and no effect. 3 Downgraded one step for inconsistency: substantial heterogeneity (I2 = 73%).
Summary of findings 3. ANXIOLYTIC ‐ BUSPIRONE versus PLACEBO for antipsychotic‐induced tardive dyskinesia.
| BUSPIRONE versus PLACEBO for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: female and male 33‐year old (mean) patients with schizophrenia and antipsychotic‐induced tardive dyskinesia Setting: inpatients, China Intervention: Buspirone versus placebo. | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with placebo | Risk with buspirone | |||||
| Tardive dyskinesia: No clinically important improvement follow‐up: 6 weeks | 905 per 1,000 | 480 per 1,000 (299 to 760) | RR 0.53 (0.33 to 0.84) | 42 (1 RCT) | ⊕⊕⊝⊝ low1,2 | |
| Tardive dyskinesia: Deterioration of symptoms ‐ not reported | This outcome was not reported. | |||||
| Adverse effects ‐ not reported | This outcome was not reported. | |||||
| Acceptability of treatment (measured by participants leaving the study early) follow‐up: 6 weeks | not estimable | not estimable | RR not estimable | 42 (1 RCT) | ⊕⊝⊝⊝ very low1,3 | No events were reported. |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | This outcome was not reported. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RCT: randomised controlled trial; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded one step for risk of bias: randomisation procedure, allocation concealment and blinding were not adequately described.
2 Downgraded one step for imprecision: very small sample size and few events reported.
3 Downgraded two steps for imprecision: effect could not be estimated due to very small sample size with no events reported.
Summary of findings 4. ENZYME INHIBITOR ‐ VMAT2‐INHIBITOR (valbenazine) versus PLACEBO for antipsychotic‐induced tardive dyskinesia.
| VMAT2‐inhibitor compared to placebo for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: 18 to 85 year‐old patients with schizophrenia, schizoaffective disorder, mood disorder, or gastrointestinal disorder + antipsychotic‐induced tardive dyskinesia Settings: in‐ and outpatients in the USA Intervention: Valbenazine (NBI‐98854) (25mg to 75mg/day) versus placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | VMAT2‐inhibitor | |||||
| Tardive dyskinesia: 1. No clinically important improvement Follow‐up: 6 weeks | 826 per 1000 | 520 per 1000 (380 to 710) | RR 0.63 (0.46 to 0.86) | 92 (1 study) | ⊕⊕⊕⊝ moderate1 | |
| Adverse effects ‐ any adverse effect Follow‐up: 6 weeks | 327 per 1000 | 490 per 1000 (300 to 800) | RR 1.50 (0.92 to 2.45) | 100 (1 study) | ⊕⊕⊝⊝ low2 | |
| Leaving the study early follow‐up: 6 weeks | 98 per 1000 | 98 per 1000 (30 to 319) | RR 1.00 (0.31 to 3.25) | 102 (1 study) | ⊕⊝⊝⊝ very low2,3 | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for imprecision: small sample size and few events reported 2 Downgraded two steps for serious imprecision: small sample size and very few events reported with the 95% CI around the effect estimate indicating both appreciable benefit for valbenazine and no effect. 3 Downgraded one step for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability.
Summary of findings 5. FATTY ACID ‐ ETHYL‐EPA versus PLACEBO for antipsychotic‐induced tardive dyskinesia.
| ETHYL‐EPA versus PLACEBO for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: female and male 42 (mean) years old patients with schizophrenia or schizoaffective disorder and antipsychotic‐induced tardive dyskinesia Settings: in‐ and outpatients in South Africa Intervention: ethyl‐EPA (omega‐3 fatty acid eicosapentaenoic acid derivative) versus placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | ETHYL‐EPA | |||||
| Tardive dyskinesia: No clinically important improvement ‐ not reported | This outcome was not reported. | |||||
| Tardive dyskinesia: Deterioration of symptoms ‐ not reported | This outcome was not reported. | |||||
|
Adverse effects: EPS: parkinsonism measured by average ESRS change scores follow‐up: 12 weeks |
mean: ‐1.1 (3.3) | The mean change in ESRS: parkinsonism scale score in the ethyl‐EPA group was 0.3 points higher (1.17 lower to 1.77 higher) |
MD 0.30 (‐1.17 to 1.77) |
75 (1 RCT) |
⊕⊕⊝⊝ low1,2 | |
|
Adverse effects: EPS: dystonia measured by average ESRS change scores follow‐up: 12 weeks |
mean: 0.4 (0.5) | The mean change in ESRS: dystonia scale score in the ethyl‐EPA group was 0.35 points lower (0.58 to 0.12 lower) |
MD ‐0.35 (‐0.58 to ‐0.12) |
75 (1 RCT) |
⊕⊕⊝⊝ low1,2 | |
|
Adverse effects: EPS: akathisia measured by average ESRS change scores follow‐up: 12 weeks |
mean: ‐0.06 (0.7) | The mean change in ESRS: akathisia scale score in the ethyl‐EPA group was 0.04 points lower (0.3 lower to 0.22 higher) |
MD ‐0.04 (‐0.30 to 0.22) |
75 (1 RCT) |
⊕⊝⊝⊝ very low1,3 | |
|
Acceptability of treatment (measured by participants leaving the study early) follow‐up: 12 weeks |
548 per 1000 | 214 per 1000 (115 to 406) | RR 0. 57 (0.2 7 to 1.22) | 84 (1 RCT) | ⊕⊝⊝⊝ very low1,2,4 | |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | This outcome was not reported. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; EPS: extrapyramidal symptoms; ESRS: Extrapyramidal Symptom Rating Scale; ethyl‐EPA: ethyl‐eicosapentaenoic acid; RCT: randomised controlled trial; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for risk of bias: randomisation procedure, allocation concealment and blinding were not adequately described. 2 Downgraded one step for imprecision: small sample size. 3 Downgraded two steps for serious imprecision: small sample size with the 95% CI around the effect estimate indicating both appreciable benefit for ethyl‐EPA and no effect. 4 Downgraded one step for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability.
Summary of findings 6. HERB ‐ GINKGO BILOBA versus PLACEBO for antipsychotic‐induced tardive dyskinesia.
| GINKGO BILOBAversus PLACEBO for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: male 45.2 (mean) years old patients with schizophrenia and antipsychotic‐induced tardive dyskinesia Settings: inpatients in China Intervention:GINKGO BILOBA (EGb‐761, standardised extract of Ginkgo biloba leaves) versus PLACEBO | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | GINKGO BILOBA | |||||
| Tardive dyskinesia: No clinically important improvement follow‐up: 12 weeks | 987 per 1000 | 869 per 1000 (800 to 948) | RR 0.88 (0.81 to 0.96) | 157 (1 RCT) | ⊕⊕⊕⊝ moderate1 | |
| Tardive dyskinesia: Deterioration of symptoms ‐ not reported | This outcome was not reported. | |||||
| Adverse effects ‐ not reported | This outcome was not reported. | |||||
| Acceptability of treatment (measured by participants leaving the study early) follow‐up: 12 weeks | 51 per 1000 | 13 per 1000 (2 to 112) | RR 0.25 (0.03 to 2.22) | 157 (1 RCT) | ⊕⊝⊝⊝ very low2,3 | |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | This outcome was not reported. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RCT: randomised controlled trial; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for imprecision: small sample size and few events reported. 2 Downgraded two steps for serious imprecision: small sample size and very few events reported with the 95% CI around the effect estimate indicating both appreciable benefit for Ginkgo biloba and no effect. 3 Downgraded one step for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability.
Summary of findings 7. HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT for antipsychotic‐induced tardive dyskinesia.
| MELATONIN versus PLACEBO OR NO TREATMENT for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: female and male 28 to 91 years old patients with antipsychotic‐induced tardive dyskinesia Settings: in‐ and outpatients in Israel and Venezuela Intervention: melatonin (2‐20 mg/day) versus placebo or no treatment | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo/no treatment | MELATONIN | |||||
| Tardive dyskinesia: No clinically important improvement follow‐up: 3‐12 weeks | 1000 per 1000 | 890 per 1000 (710 to 1000) | RR 0.89 (0.71 to 1.12) | 32 (2 RCTs) | ⊕⊕⊝⊝ low1,2 | |
|
Tardive dyskinesia: Deterioration of symptoms follow‐up: 3 weeks |
200 per 1000 | 44 per 1000 (2 to 810) | RR 0.22 (0.01 to 4.05) | 19 (1 RCT) | ⊕⊕⊝⊝ low3 | |
|
Adverse effects follow‐up: 3‐12 weeks |
See comment | See comment | Not estimable | 54 (3 RCTs) | ⊕⊕⊝⊝ low3 | No events were reported. |
| Acceptability of treatment (measured by participants leaving the study early) follow‐up: 3‐12 weeks | See comment | See comment | Not estimable | 54 (3 RCTs) | ⊕⊝⊝⊝ very low3,4 | No events were reported. |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | This outcome was not reported. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RCT: randomised controlled trial; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one step for inconsistency: substantial heterogeneity (I2 = 46%). 2 Downgraded one step for imprecision: small sample size and few events reported with the 95% CI around the effect estimate indicating both appreciable benefit for melatonin and no effect. 3 Downgraded two steps for imprecision: very small sample size and no or very few events reported. 4 Downgraded one step for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability.
Summary of findings 9. HYPNOSIS or RELAXATION versus TAU for antipsychotic‐induced tardive dyskinesia.
| HYPNOSIS OR RELAXATION versus TAU for antipsychotic‐induced tardive dyskinesia | ||||||
| Patients or population: female and male 35 (mean) years old patients with schizophrenia and tardive dyskinesia, acute extrapyramidal symptoms, and/or pseudoparkinsonism Setting: outpatients in the USA Interventions: hypnosis or relaxation (8 sessions) versus TAU | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with TAU | Risk with hypnosis or relaxation | |||||
| Tardive dyskinesia: No clinically important improvement follow‐up: 8 weeks | 1,000 per 1,000 | 450 per 1,000 (210 to 940) | RR 0.45 (0.21 to 0.94) | 15 (1 RCT) | ⊕⊝⊝⊝ very low1,2 | |
| Tardive dyskinesia: Deterioration of symptoms follow‐up: 8 weeks | 200 per 1,000 | 36 per 1,000 (2 to 762) | RR 0.18 (0.01 to 3.81) | 15 (1 RCT) | ⊕⊝⊝⊝ very low1,3 | |
| Adverse effects ‐ not reported | This outcome was not reported. | |||||
| Acceptability of treatment (measured by participants leaving the study early) follow‐up: 8 weeks | 0 per 1,000 | 0 per 1,000 (0 to 0) | not estimable | 15 (1 RCT) | ⊕⊝⊝⊝ very low1,4 | No events were reported. |
| Social confidence, social inclusion, social networks, or personalised quality of life ‐ not reported | This outcome was not reported. | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RCT: randomised controlled trial; RR: Risk ratio; TAU: treatment as usual | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded two steps for risk of bias: fully randomised sequence generation and blinding was not achieved. 2 Downgraded one step for imprecision: very small sample size. 3 Downgraded two steps for imprecision: 95% CI includes benefit for both intervention arms; very small sample size with few events reported. 4 Downgraded two steps for imprecision: effect could not be estimated due to very small sample size with no events reported.
1. Comparison 1. Alkaloid ‐ Dihydrogenated ergot alkaloids (DEA) versus placebo
Three trials (Hajioff 1983; Koshino 1983; Rastogi 1982) carried out in Japan and the UK that included 88 inpatients with antipsychotic‐induced TD were included for this comparison.
1.1 TD symptoms
1.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of DEA against placebo (low‐quality evidence, 1 trial, 28 people, risk ratio (RR) 0.45, 95% confidence interval (CI) 0.21 to 0.97, Analysis 1.1).
1.1. Analysis.

Comparison 1 ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
1.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we found no benefit of DEA against placebo (1 trial, 28 people, RR 0.50, 95% CI 0.23 to 1.09, Analysis 1.2).
1.2. Analysis.

Comparison 1 ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term.
1.1.3 Deterioration of symptoms
There was no difference on deterioration of symptoms between DEA and placebo (very low‐quality evidence, 1 trial, 28 people, RR 0.33, 95% CI 0.01 to 7.55, Analysis 1.3).
1.3. Analysis.

Comparison 1 ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ medium term.
1.1.4 Average endpoint scores
TD symptoms were also measured on the continuous Simpson scale (see above). No benefit was found when DEA is compared to placebo (1 trial, 28 people, mean difference (MD) ‐2.80, 95% CI ‐12.25 to 6.65, Analysis 1.4).
1.4. Analysis.

Comparison 1 ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO, Outcome 4 Tardive dyskinesia: 3. Average endpoint scale score (Simpson scale, high=poor) ‐ medium term.
1.1.4 Average change scores
TD symptoms were also measured on the continuous Abnormal Involuntary Movement Scale (AIMS), Rockland Tardive Dyskinesia Rating Scale (RTDS), and Abbreviated Dyskinesia Scale (ADS) scales (see above). No benefit was found when pooling changes scores of these scales for DEA compared to placebo (2 trials, 59 people, standardised mean difference (SMD) ‐0.31, 95% CI ‐0.83 to 0.20, Analysis 1.5).
1.5. Analysis.

Comparison 1 ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO, Outcome 5 Tardive dyskinesia: Average scale change scores (various scales, high=poor) ‐ medium term.
1.2 Mental state
For the outcome of mental state deterioration, no benefit was found for DEA when compared to placebo (1 trial, 28 people, MD 0.50, 95% CI 0.05 to 4.90, Analysis 1.6).
1.6. Analysis.

Comparison 1 ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO, Outcome 6 Mental state: Deterioration ‐ medium term.
1.3 Adverse effects
There was no difference in the incidence of ‘any adverse effect’ between DEA and placebo (very low‐quality evidence, 1 trial, 28 people, RR 2.33 95% CI 0.75 to 7.23, Analysis 1.7).
1.7. Analysis.

Comparison 1 ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO, Outcome 7 Adverse events ‐ medium term.
1.4 Leaving the study early
Using DEA did not significantly increase the chances of a person leaving the study early (very low‐quality evidence, 2 trials, 48 people, RR 0.33, 95% CI 0.02 to 7.32, Analysis 1.8).
1.8. Analysis.

Comparison 1 ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO, Outcome 8 Leaving the study early ‐ medium term.
2. Comparison 2. Alkaloid ‐ L‐Stepholidine (SPD) versus placebo
One trial (Cai 1988) that included 57 patients with antipsychotic‐induced TD was included for this comparison.
2.1 TD symptoms
2.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of SPD against placebo (1 trial, 57 people, RR 0.54, 95% CI 0.35 to 0.82, Analysis 2.1).
2.1. Analysis.

Comparison 2 ALKALOID ‐ L‐STEPHOLIDINE (SPD) versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
2.2 Mental state
General mental state was measured using the continuous BPRS scale (see above). A benefit was found in favour of SPD when compared to placebo (1 trial, 20 people, MD ‐4.50, 95% CI ‐7.60 to ‐1.40, Analysis 2.2).
2.2. Analysis.

Comparison 2 ALKALOID ‐ L‐STEPHOLIDINE (SPD) versus PLACEBO, Outcome 2 Mental state: 1. Average endpoint scale score (BPRS, high=poor) ‐ medium term.
2.3 Adverse effects
No adverse effects were reported.
2.4 Leaving the study early
No participants left the included study early.
3. Comparison 3. Alkaloid ‐ Papaverine versus placebo
One trial (Gardos 1979) carried out in the USA that included 22 inpatients with antipsychotic‐induced TD was included for this comparison.
3.1 TD symptoms
TD symptoms were measured on the continuous AIMS scale (see above). No difference was found when papaverine was compared to placebo (1 trial, 22 people, MD 0.51, 95% CI ‐1.18 to 2.20, Analysis 3.1).
3.1. Analysis.

Comparison 3 ALKALOID ‐ PAPAVERINE versus PLACEBO, Outcome 1 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term.
4. Comparison 4. Amino acid ‐ Branched‐chain amino acids (BCAA) versus placebo
One trial (Richardson 2003) carried out in the USA that included 52 in‐ and out‐patients with antipsychotic‐induced TD was included for this comparison.
4.1 TD symptoms
4.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found no benefit of BCAA against placebo (1 trial, 52 people, RR 0.79, 95% CI 0.63 to 1.00, Analysis 4.1).
4.1. Analysis.

Comparison 4 AMINO ACID ‐ BRANCHED‐CHAIN AMINO ACID (BCAA) versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term.
4.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found no benefit of BCAA against placebo (1 trial, 52 people, RR 0.64, 95% CI 0.36 to 1.11, Analysis 4.2).
4.2. Analysis.

Comparison 4 AMINO ACID ‐ BRANCHED‐CHAIN AMINO ACID (BCAA) versus PLACEBO, Outcome 2 Tardive dyskinesia: 1. Not any improvement ‐ short term.
4.1.3 Deterioration of symptoms
There was no difference on deterioration of symptoms between BCAA and placebo (1 trial, 36 people, RR 0.29, 95% CI 0.07 to 1.19, Analysis 4.3).
4.3. Analysis.

Comparison 4 AMINO ACID ‐ BRANCHED‐CHAIN AMINO ACID (BCAA) versus PLACEBO, Outcome 3 Tardive dyskinesia: 2. Deterioration ‐ short term.
4.1.4 Average endpoint scores
TD symptoms were also measured on the continuous Simpson scale (see above). A benefit was found in favour of BCAA when compared to placebo (1 trial, 41 people, MD ‐92.90, 95% CI ‐167.57 to ‐18.23, Analysis 4.4).
4.4. Analysis.

Comparison 4 AMINO ACID ‐ BRANCHED‐CHAIN AMINO ACID (BCAA) versus PLACEBO, Outcome 4 Tardive dyskinesia: Average endpoint score (Simpson scale, high=poor) ‐ short term.
4.2 Leaving the study early
Using BCAA did not significantly increase the chances of a person leaving the study early when compared to placebo (1 trial, 52 people, RR 0.84, 95% CI 0.37 to 1.92, Analysis 4.5).
4.5. Analysis.

Comparison 4 AMINO ACID ‐ BRANCHED‐CHAIN AMINO ACID (BCAA) versus PLACEBO, Outcome 5 Leaving the study early ‐ short term.
5. Comparison 5. Amino acid ‐ Phenylalanine versus placebo
One trial (Mosnik 1997) carried out in the USA that included 18 in‐ and out‐patients with antipsychotic‐induced TD was included for this comparison.
5.1 Leaving the study early
Using phenylalanine did not significantly increase the chances of a person leaving the study early when compared to placebo (1 trial, 18 people, RR 2.45, 95% CI 0.11 to 53.25, Analysis 5.1).
5.1. Analysis.

Comparison 5 AMINO ACID ‐ PHENYLALANINE versus PLACEBO, Outcome 1 Leaving the study early ‐ short term.
6. Comparison 6. Antidepressant (MAO‐B inhibitor) ‐ Selegiline versus placebo
One trial (Goff 1993) carried out in the USA that included 33 outpatients with antipsychotic‐induced TD was included for this comparison.
6.1 TD symptoms
6.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found no benefit of selegiline against placebo (1 trial, 33 people, RR 1.37, 95% CI 0.96 to 1.94; Analysis 6.1).
6.1. Analysis.

Comparison 6 ANTIDEPRESSANT (MAO‐B inhibitor) ‐ SELEGILINE versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
6.2 Leaving the study early
Using selegiline did not significantly increase the chances of a person leaving the study early (1 trial, 33 people, RR 10.39, 95% CI 0.62 to 173.97; Analysis 6.2).
6.2. Analysis.

Comparison 6 ANTIDEPRESSANT (MAO‐B inhibitor) ‐ SELEGILINE versus PLACEBO, Outcome 2 Leaving the study early ‐ medium term.
7. Comparison 7. Antidepressant (MAOI) ‐ Isocarboxazid versus procyclidine
One trial (Bucci 1971) carried out in the USA that included 20 outpatients with antipsychotic‐induced TD was included for this comparison.
7.1 TD symptoms
7.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of isocarboxazid against procyclidine (1 trial, 20 people, RR 0.24, 95% CI 0.08 to 0.71, Analysis 7.1).
7.1. Analysis.

Comparison 7 ANTIDEPRESSANT (MAOI) ISOCARBOXAZID versus PROCYCLIDINE, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ long term.
7.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found a benefit in favour of isocarboxazid against procyclidine (1 trial, 20 people, RR 0.14, 95% CI 0.03 to 0.64, Analysis 7.2).
7.2. Analysis.

Comparison 7 ANTIDEPRESSANT (MAOI) ISOCARBOXAZID versus PROCYCLIDINE, Outcome 2 Tardive dyskinesia: 1. Not any improvement ‐ long term.
7.2 Adverse effects
There was no difference in the incidence of ‘any adverse effect’ between isocarboxazid and procyclidine (1 trial, 20 people, RR 3.00, 95% CI 0.14 to 65.90, Analysis 7.3).
7.3. Analysis.
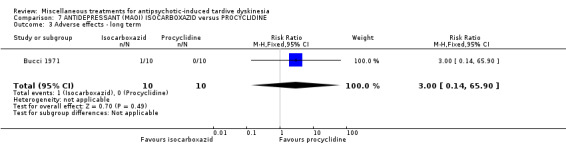
Comparison 7 ANTIDEPRESSANT (MAOI) ISOCARBOXAZID versus PROCYCLIDINE, Outcome 3 Adverse effects ‐ long term.
7.3 Leaving the study early
Using isocarboxazid did not significantly increase the chances of a person leaving the study early compared with procyclidine (1 trial, 20 people, RR 3.00, 95% CI 0.14 to 65.90, Analysis 7.4).
7.4. Analysis.

Comparison 7 ANTIDEPRESSANT (MAOI) ISOCARBOXAZID versus PROCYCLIDINE, Outcome 4 Leaving the study early ‐ long term.
8. Comparison 8. Antidepressant (SSRI) ‐ Ritanserin versus placebo
One trial (Meco 1989) carried out in Italy that included 10 inpatients with antipsychotic‐induced TD was included for this comparison.
8.1 TD symptoms
8.1.1 No clinically important improvement
For the outcome of 'any improvement in TD symptoms', we found no benefit of ritanserin against placebo (1 trial, 10 people, RR 1.00, 95% CI 0.70 to 1.43; Analysis 8.1).
8.1. Analysis.

Comparison 8 ANTIDEPRESSANT (SSRI) ‐ RITANSERIN vs PLACEBO, Outcome 1 Tardive dyskinesia: No clinically important improvement (short term).
8.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found no benefit of ritanserin against placebo (1 trial, 10 people, RR 0.28, 95% CI 0.02 to 4.66; Analysis 8.2).
8.2. Analysis.

Comparison 8 ANTIDEPRESSANT (SSRI) ‐ RITANSERIN vs PLACEBO, Outcome 2 Tardive dyskinesia: Not any improvement (short term).
8.1.3 Deterioration of symptoms
There was no difference on deterioration of TD symptoms between ritanserin and placebo (1 trial, 10 people, RR 0.47, 95% CI 0.02 to 9.26; Analysis 8.3).
8.3. Analysis.

Comparison 8 ANTIDEPRESSANT (SSRI) ‐ RITANSERIN vs PLACEBO, Outcome 3 Tardive dyskinesia: Deterioration (short term).
8.1.4 Average change scores
TD symptoms were measured on the continuous AIMS scale (see above). No difference was found when ritanserin was compared to placebo (1 trial, 10 people, MD ‐2.00, 95% CI ‐5.93 to 1.93; Analysis 8.4).
8.4. Analysis.

Comparison 8 ANTIDEPRESSANT (SSRI) ‐ RITANSERIN vs PLACEBO, Outcome 4 Tardive dyskinesia: Average change score (AIMS, high=poor) (short term).
8.2 Mental state
8.2.1 Deterioration of symptoms
There was no difference on deterioration of mental state symptoms between ritanserin and placebo (1 trial, 10 people, RR 0.47, 95% CI 0.02 to 9.26; Analysis 8.5).
8.5. Analysis.

Comparison 8 ANTIDEPRESSANT (SSRI) ‐ RITANSERIN vs PLACEBO, Outcome 5 General mental state: Deterioration (short term).
8.2.2 Average change scores
General mental state was measured using the continuous BPRS scale (see above). No benefit was found for ritanserin when compared to placebo (1 trial, 10 people, MD ‐0.80, 95% CI ‐3.10 to 1.50; Analysis 8.6).
8.6. Analysis.

Comparison 8 ANTIDEPRESSANT (SSRI) ‐ RITANSERIN vs PLACEBO, Outcome 6 General mental state: Average change score (BPRS, high=poor) (short term).
9. Comparison 9. Antiepileptic ‐ Levetiracetam versus placebo
Two trials (UCB Pharma 2005; Woods 2008) carried out in Belgium, Bulgaria, and the USA that included 119 in‐ or out‐patients with antipsychotic‐induced TD were included for this comparison.
9.1 TD symptoms
9.1.1 Average endpoint scores
TD symptoms were measured on the continuous AIMS scale (see above). A benefit was found in favour of levetiracetam compared to placebo (1 trial, 50 people, MD ‐2.18, 95% CI ‐3.65 to ‐0.71, Analysis 9.1).
9.1. Analysis.

Comparison 9 ANTIEPILEPTIC ‐ LEVETIRACETAM versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. Average endpoint score (AIMS, high=poor) ‐ medium term.
9.1.1 Average change scores
TD symptoms were also measured on the continuous St Hans rating scale (see above). There was no difference in change scores between levetiracetam and placebo (1 trial, 69 people, MD 0.13, 95% CI ‐0.73 to 0.99, Analysis 9.2).
9.2. Analysis.

Comparison 9 ANTIEPILEPTIC ‐ LEVETIRACETAM versus PLACEBO, Outcome 2 Tardive dyskinesia: 1. Average change score (hyperkinesia subscale of the SHRS , high=poor) ‐ medium term.
9.2 Leaving the study early
Using levetiracetam did not significantly increase the chances of a person leaving the study early (very low‐quality evidence, 2 trials, 119 people, RR 1.01, 95% CI 0.46 to 2.22, Analysis 9.3).
9.3. Analysis.

Comparison 9 ANTIEPILEPTIC ‐ LEVETIRACETAM versus PLACEBO, Outcome 3 Leaving the study early ‐ medium term.
9.3 Adverse effects
There was no difference in the incidence of ‘any adverse effect’ between levetiracetam and placebo (low‐quality evidence, 1 trial, 69 people, RR 0.51,95% CI 0.25 to 1.04, Analysis 9.4).
9.4. Analysis.

Comparison 9 ANTIEPILEPTIC ‐ LEVETIRACETAM versus PLACEBO, Outcome 4 Adverse effects ‐ medium term.
9.4 Mental state
We found no difference between levetiracetam and placebo for deterioration of mental state (1 trial, 50 people, RR 0.67, 95% CI 0.12 to 3.65, Analysis 9.5).
9.5. Analysis.

Comparison 9 ANTIEPILEPTIC ‐ LEVETIRACETAM versus PLACEBO, Outcome 5 Mental state: deterioration ‐ medium term.
10. Comparison 10. Antihistamine ‐ Cyproheptadine versus placebo
One trial (Koshino 1979) carried out in Japan that included 42 inpatients with schizophrenia and TD was included for this comparison.
10.1 TD symptoms
10.1.1 Not any improvement
For the outcome of 'any improvement in TD symptoms', we found no benefit of cyproheptadine against placebo (1 trial, 42 people, RR 0.54, 95% CI 0.27 to 1.08, Analysis 10.1).
10.1. Analysis.

Comparison 10 ANTIHISTAMINE ‐ CYPROHEPTADINE versus PLACEBO, Outcome 1 Tardive dyskinesia: 2. Not any improvement ‐ short term.
10.1.2 Deterioration of symptoms
There was no difference on deterioration of symptoms between cyproheptadine and placebo (1 trial, 42 people, RR 0.33, 95% CI 0.01 to 7.74, Analysis 10.2).
10.2. Analysis.

Comparison 10 ANTIHISTAMINE ‐ CYPROHEPTADINE versus PLACEBO, Outcome 2 Tardive dyskinesia: 3. Deterioration ‐ short term.
10.2 Adverse effects
There was no difference in the incidence of ‘any adverse effect’ between cyproheptadine and placebo (1 trial, 42 people, RR 0.33, 95% CI 0.04 to 2.95, Analysis 10.3).
10.3. Analysis.
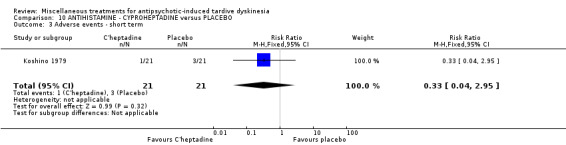
Comparison 10 ANTIHISTAMINE ‐ CYPROHEPTADINE versus PLACEBO, Outcome 3 Adverse events ‐ short term.
10.3 Leaving the study early
Using cyproheptadine did not significantly increase the chances of a person leaving the study early (1 trial, 42 people, RR 0.33, 95% CI 0.01 to 7.74, Analysis 10.4).
10.4. Analysis.

Comparison 10 ANTIHISTAMINE ‐ CYPROHEPTADINE versus PLACEBO, Outcome 4 Leaving the study early ‐ short term.
11. Comparison 11. Antipsychotic ‐ Promethazine versus placebo
One trial (Yang 1999) carried out in China that included 34 inpatients with antipsychotic‐induced TD was included for this comparison.
11.1 TD symptoms
11.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of promethazine against placebo (1 trial, 34 people, RR 0.24, 95% CI 0.11 to 0.55, Analysis 11.1).
11.1. Analysis.

Comparison 11 ANTIPSYCHOTIC ‐ PROMETHAZINE vs PLACEBO, Outcome 1 Tardive dyskinesia: No clinically important improvement (medium term).
11.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found a benefit in favour of promethazine against placebo (1 trial, 34 people, RR 0.06, 95% CI 0.01 to 0.43; Analysis 11.2).
11.2. Analysis.

Comparison 11 ANTIPSYCHOTIC ‐ PROMETHAZINE vs PLACEBO, Outcome 2 Tardive dyskinesia: Not any improvement (medium term).
11.1.3 Average endpoint scores
A benefit in favour of promethazine against placebo was also found for reduction of TD symptoms on the AIMS scale (1 trial, 34 people, MD ‐7.10, 95% CI ‐9.53 to ‐4.67; Analysis 11.3).
11.3. Analysis.

Comparison 11 ANTIPSYCHOTIC ‐ PROMETHAZINE vs PLACEBO, Outcome 3 Tardive dyskinesia: Average endpoint score (AIMS, high=poor) (medium term).
11.2 Mental state
11.2.1 Average endpoint scores
General mental state was measured using the continuous BPRS scale (see above). No benefit was found for promethazine when compared to placebo (1 trial, 34 people, MD 0.70, 95% CI ‐3.77 to 5.17; Analysis 11.4).
11.4. Analysis.

Comparison 11 ANTIPSYCHOTIC ‐ PROMETHAZINE vs PLACEBO, Outcome 4 General mental state: Average endpoint score (BPRS, high=poor) (medium term).
11.3 Adverse effects
11.3.1 Any adverse effects
No difference was found for any adverse events measured on the TESS scale (see above) between promethazine and placebo (1 trial, 34 people, MD ‐0.10, 95% CI ‐0.53 to 0.33; Analysis 11.5).
11.5. Analysis.

Comparison 11 ANTIPSYCHOTIC ‐ PROMETHAZINE vs PLACEBO, Outcome 5 Adverse effects: Any adverse effects (TESS, high=poor) (medium term).
11.3.2 Parkinsonism: average endpoint scores
No difference was found for parkinsonism adverse events measured on the RSESE scale (see above) between promethazine and placebo (1 trial, 34 people, MD ‐0.50, 95% CI ‐1.36 to 0.36; Analysis 11.6).
11.6. Analysis.

Comparison 11 ANTIPSYCHOTIC ‐ PROMETHAZINE vs PLACEBO, Outcome 6 Adverse effects: Parkinsonism ‐ Average endpoint score (RSESE) (medium term).
11.4 Global state
11.4.1 Average endpoint scores
Global state was measured using the continuous Clinical Global Impression (CGI) scale (see above). A benefit in global state was found for promethazine when compared to placebo (1 trial, 34 people, MD ‐3.00, 95% CI ‐3.78 to ‐2.22; Analysis 11.7).
11.7. Analysis.

Comparison 11 ANTIPSYCHOTIC ‐ PROMETHAZINE vs PLACEBO, Outcome 7 Global state: Average endpoint score (CGI, high=poor) (medium term).
12. Comparison 12. Anxiolytic ‐ Buspirone versus placebo
One study (Zeng 1995) carried out in China that included 42 inpatients with schizophrenia and TD was included for this comparison.
12.1 TD symptoms
We had chosen 'any improvement in TD symptoms of more than 50% on any TD scale ‐ any time period' as a primary outcome. Although the data we found in trials did not fit this exactly we feel that the outcome 'clinically relevant improvement' fits best with what we had hoped to find.
12.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of buspirone against placebo (low‐quality evidence, 1 trial, 42 people, RR 0.53, 95% CI 0.33 to 0.84, Analysis 12.1).
12.1. Analysis.

Comparison 12 ANXIOLYTIC ‐ BUSPIRONE versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
12.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we found a benefit of buspirone against placebo (1 trial, 42 people, RR 0.33, 95% CI 0.15 to 0.75, Analysis 12.2).
12.2. Analysis.

Comparison 12 ANXIOLYTIC ‐ BUSPIRONE versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term.
12.1.3 Average endpoint scores
TD symptoms were also measured on the continuous AIMS scale (see above). No difference was found when buspirone was compared to placebo (1 trial, 42 people, MD 0.00, 95% CI ‐1.45 to 1.45, Analysis 12.3).
12.3. Analysis.

Comparison 12 ANXIOLYTIC ‐ BUSPIRONE versus PLACEBO, Outcome 3 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term.
12.2 Leaving the study early
No participants left the included study early.
13. Comparison 13. Cognitive enhancer ‐ Piracetam versus placebo
One trial (Libov 2007) carried out in Israel that included 40 inpatients with antipsychotic‐induced TD was included for this comparison.
13.1 TD symptoms
13.1.1 Average endpoint scores
TD symptoms were measured on the continuous Extrapyramidal System Rating Scale (ESRS) scale (see above). No difference was found between piracetam and placebo (1 trial, 35 people, MD ‐0.70, 95% CI ‐4.30 to 2.90, Analysis 13.1).
13.1. Analysis.

Comparison 13 COGNITIVE ENHANCER ‐ PIRACETAM versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. Average endpoint score (ESRS, high=poor) ‐ short term.
13.2 Adverse effects
Symptoms of parkinsonism were also measured on the continuous ESRS scale (see above). No difference was found between piracetam and placebo (1 trial, 35 people, MD 2.50, 95% CI ‐4.73 to 9.73, Analysis 13.2).
13.2. Analysis.

Comparison 13 COGNITIVE ENHANCER ‐ PIRACETAM versus PLACEBO, Outcome 2 Parkinsonism: 1. Average endpoint score (ESRS, high=poor) ‐ short term.
13.3 Leaving the study early
Using piracetam did not significantly increase the chances of a person leaving the study early (1 trial, 40 people, RR 0.23, 95% CI 0.03 to 1.85, Analysis 13.3).
13.3. Analysis.

Comparison 13 COGNITIVE ENHANCER ‐ PIRACETAM versus PLACEBO, Outcome 3 Leaving the study early ‐ short term.
13.4 Global state
We found no difference in global state measured by the CGI (see above) between piracetam and placebo (1 trial, 35 people, MD 0.20, 95% CI ‐0.35 to 0.75, Analysis 13.4).
13.4. Analysis.

Comparison 13 COGNITIVE ENHANCER ‐ PIRACETAM versus PLACEBO, Outcome 4 Global state: Average endpoint score (CGI, high=poor) ‐ short term.
14. Comparison 14. Cognitive enhancer/stimulant ‐ Pemoline versus placebo
One trial (Zeng 1996) carried out in China that included 46 inpatients with antipsychotic‐induced TD was included for this comparison.
14.1 TD symptoms
14.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of pemoline against placebo (1 trial, 46 people, RR 0.48, 95% CI 0.29 to 0.77, Analysis 14.1).
14.1. Analysis.

Comparison 14 COGNITIVE ENHANCER/STIMULANT ‐ PEMOLINE versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
14.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found a benefit in favour of pemoline against placebo (1 trial, 46 people, RR 0.29, 95% CI 0.13 to 0.66, Analysis 14.2).
14.2. Analysis.
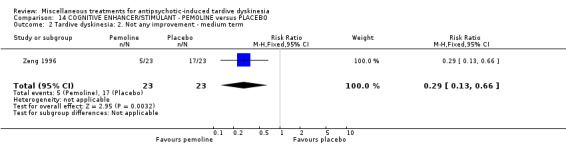
Comparison 14 COGNITIVE ENHANCER/STIMULANT ‐ PEMOLINE versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term.
14.1.3 Average endpoint scores
TD symptoms were also measured on the continuous AIMS scale (see above). A difference in favour of pemoline was found when compared to placebo (1 trial, 46 people, MD ‐3.90, 95% CI ‐5.47 to ‐2.33, Analysis 14.3).
14.3. Analysis.

Comparison 14 COGNITIVE ENHANCER/STIMULANT ‐ PEMOLINE versus PLACEBO, Outcome 3 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term.
14.2 Leaving the study early
No participants left the included study early.
15. Comparison 15. Enzyme inhibitor ‐ VMAT2 inhibitors versus placebo
15.1 TD symptoms
15.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of valbenazine (NBI‐98854) against placebo (moderate‐quality evidence, 1 trial, 92 people, RR 0.63, 95% CI 0.46 to 0.86, Analysis 15.1).
15.1. Analysis.

Comparison 15 ENZYME INHIBITOR ‐ VMAT2 INHIBITORS versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
15.1.2 Average change scores
TD symptoms were measured on the continuous AIMS scale (see above). A benefit in favour of valbenazine was found against placebo (1 trial, 89 people, MD ‐2.50, 95% CI ‐4.00 to ‐1.00; Analysis 15.2)
15.2. Analysis.

Comparison 15 ENZYME INHIBITOR ‐ VMAT2 INHIBITORS versus PLACEBO, Outcome 2 Tardive dyskinesia: 3. Average change score (AIMS, high=poor) ‐ medium term.
15.2 Adverse effects
The incidence of overall adverse events such as fatigue, headache, decreased appetite, nausea and somnolence was higher in the valbenazine group compared to placebo (low‐quality evidence, 1 trial, 100 people, RR 1.50, 95% CI 0.92 to 2.45; Analysis 15.3), but the difference was not significant.
15.3. Analysis.

Comparison 15 ENZYME INHIBITOR ‐ VMAT2 INHIBITORS versus PLACEBO, Outcome 3 Adverse events ‐ medium term.
15.3 Leaving the study early
Using VMAT2‐I did not significantly increase the chances of a person leaving the study early (very low‐quality evidence, 1 trial, 102 people, RR 1.00, 95% CI 0.31 to 3.25, Analysis 15.4).
15.4. Analysis.

Comparison 15 ENZYME INHIBITOR ‐ VMAT2 INHIBITORS versus PLACEBO, Outcome 4 Leaving the study early ‐ medium term.
16. Comparison 16. Fatty acid ‐ Ethyl‐eicosapentaenoic acid (ethyl‐EPA) versus placebo
One trial (Emsley 2006) carried out in South Africa that included 84 in‐ and out‐patients with antipsychotic‐induced TD was included for this comparison.
16.1 TD symptoms
16.1.1 Not any improvement
For the outcome of 'any improvement in TD symptoms', there was no benefit of ethyl‐EPA against placebo (1 trial, 75 people, RR 0.82, 95% CI 0.57 to 1.18, Analysis 16.1).
16.1. Analysis.

Comparison 16 FATTY ACID ‐ ETHYL EICOSAPENTAENOIC ACID versus PLACEBO, Outcome 1 Tardive dyskinesia: 2. No clinically important improvement ‐ medium term.
16.2 Mental state
There was no difference on deterioration of mental state between ethyl‐EPA and placebo (1 trial, 75 people, RR 0.49, 95% CI 0.05 to 5.14, Analysis 16.2).
16.2. Analysis.

Comparison 16 FATTY ACID ‐ ETHYL EICOSAPENTAENOIC ACID versus PLACEBO, Outcome 2 Mental state: deterioration ‐ medium term.
16.3 Adverse effects
16.3.1 Extrapyramidal symptoms: parkinsonism
Symptoms of parkinsonism were measured on the continuous ESRS scale (see above). No difference was found between ethyl‐EPA and placebo (low‐quality evidence, 1 trial, 75 people, MD 0.30, 95% CI ‐1.17 to 1.77, Analysis 16.3).
16.3. Analysis.

Comparison 16 FATTY ACID ‐ ETHYL EICOSAPENTAENOIC ACID versus PLACEBO, Outcome 3 Adverse events: Parkinsonism ‐ Average change in scale score (ESRS, low=better) ‐ medium term.
16.3.2 Extrapyramidal symptoms: dystonia
Symptoms of dystonia were measured on the continuous ESRS scale (see above). A benefit was found in favour of ethyl‐EPA when compared to placebo (low‐quality evidence, 1 trial, 75 people, MD ‐0.35, 95% CI ‐0.58 to ‐0.12, Analysis 16.4).
16.4. Analysis.

Comparison 16 FATTY ACID ‐ ETHYL EICOSAPENTAENOIC ACID versus PLACEBO, Outcome 4 Adverse events: Dystonia ‐ Average change in scale score (ESRS, low=better) ‐ medium term.
16.3.3 Extrapyramidal symptoms: akathisia
Symptoms of akathisia were measured on the continuous ESRS scale (see above). No difference was found between ethyl‐EPA and placebo (very low‐quality evidence, 1 trial, 75 people, MD ‐0.04 CI ‐0.30 to 0.22, Analysis 16.5).
16.5. Analysis.

Comparison 16 FATTY ACID ‐ ETHYL EICOSAPENTAENOIC ACID versus PLACEBO, Outcome 5 Adverse events: Akathisia ‐ Average change in scale score (ESRS, low=better) ‐ medium term.
16.4 Leaving the study early
Using ethyl‐EPA did not significantly increase the chances of a person leaving the study early (very low‐quality evidence, 1 trial, 84 people, RR 0.57, 95% CI 0.27 to 1.22, Analysis 16.6).
16.6. Analysis.

Comparison 16 FATTY ACID ‐ ETHYL EICOSAPENTAENOIC ACID versus PLACEBO, Outcome 6 Leaving the study early ‐ medium term.
17. Comparison 17. Fatty acid ‐ Gamma‐linolenic acid versus placebo
One trial (Wolkin 1986) carried out in the USA that included 16 in‐ and out‐patients with antipsychotic‐induced TD was included for this comparison.
17.1 TD symptoms
17.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement', added across all time points, found no benefit of gamma‐linolenic acid against placebo (1 trial, 16 people, RR 1.00, 95% CI 0.69 to 1.45, Analysis 17.1).
17.1. Analysis.

Comparison 17 FATTY ACID ‐ GAMMA‐LINOLENIC ACID versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
17.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found no benefit of gamma‐linolenic acid against placebo (1 trial, 16 people, RR 0.75, 95% CI 0.24 to 2.33, Analysis 17.2).
17.2. Analysis.

Comparison 17 FATTY ACID ‐ GAMMA‐LINOLENIC ACID versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term.
17.1.3 Deterioration of symptoms
There was no difference on deterioration of symptoms between gamma‐linolenic acid and placebo (1 trial, 16 people, RR 1.50, 95% CI 0.34 to 6.70, Analysis 17.3).
17.3. Analysis.

Comparison 17 FATTY ACID ‐ GAMMA‐LINOLENIC ACID versus PLACEBO, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ medium term.
17.1.4 Average change scores
TD symptoms were also measured on the continuous AIMS scale (see above). No benefit was found for gamma‐linolenic acid when compared to placebo (1 trial, 16 people, MD ‐0.20, 95% CI ‐3.10 to 2.70, Analysis 17.4).
17.4. Analysis.
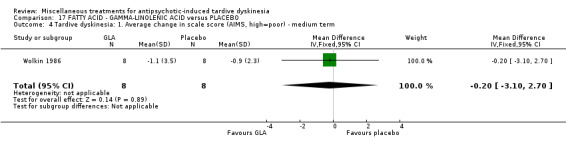
Comparison 17 FATTY ACID ‐ GAMMA‐LINOLENIC ACID versus PLACEBO, Outcome 4 Tardive dyskinesia: 1. Average change in scale score (AIMS, high=poor) ‐ medium term.
17.2 Mental state
General mental state was measured using the continuous Brief Psychiatric Rating Scale (BPRS) (see above). No benefit was found for gamma‐linolenic acid when compared to placebo (1 trial, 10 people, MD ‐6.00, 95% CI ‐15.99 to 3.99, Analysis 17.5).
17.5. Analysis.

Comparison 17 FATTY ACID ‐ GAMMA‐LINOLENIC ACID versus PLACEBO, Outcome 5 Mental state: 2. Average change in scale score (BPRS, high=poor) ‐ medium term.
17.3 Leaving the study early
No participants left the included study early.
18. Comparison 18. Herb ‐ Ginkgo biloba versus placebo
One trial (Zhang 2011) carried out in China that included 157 inpatients with antipsychotic‐induced TD was included for this comparison.
18.1 TD symptoms
18.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of G inkgo biloba when compared to placebo (moderate‐quality evidence, 1 trial, 157 people, RR 0.88, 95% CI 0.81 to 0.96, Analysis 18.1).
18.1. Analysis.

Comparison 18 HERB ‐ GINKGO BILOBA versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
18.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found a benefit of G inkgo biloba when compared to placebo (1 trial, 157 people, RR 0.51, 95% CI 0.41 to 0.65, Analysis 18.2).
18.2. Analysis.

Comparison 18 HERB ‐ GINKGO BILOBA versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term.
18.1.3 Average endpoint scores
TD symptoms were also measured on the continuous AIMS scale (see above). A benefit was found in favour of G inkgo biloba compared to placebo (1 trial, 157 people, MD ‐2.06, 95% CI ‐2.94 to ‐1.18, Analysis 18.3).
18.3. Analysis.

Comparison 18 HERB ‐ GINKGO BILOBA versus PLACEBO, Outcome 3 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term.
18.2 Leaving the study early
Using G inkgo biloba did not significantly increase the chances of a person leaving the study early (very low‐quality evidence, 1 trial, 157 people, RR 0.25, 95% CI 0.03 to 2.22, Analysis 18.4).
18.4. Analysis.

Comparison 18 HERB ‐ GINKGO BILOBA versus PLACEBO, Outcome 4 Leaving the study early ‐ medium term.
18.3 Mental state
18.3.1 Deterioration of mental state
There was no difference in deterioration of mental state between G inkgo biloba and placebo (1 trial, 157 people, RR 0.34, 95% CI 0.01 to 8.16, Analysis 18.5).
18.5. Analysis.

Comparison 18 HERB ‐ GINKGO BILOBA versus PLACEBO, Outcome 5 Mental state: deterioration ‐ medium term.
18.3.2 Average endpoint scores
Mental state was also measured using the continuous Positive and Negative Syndrome Scale (PANSS) (see above). A benefit was found in favour of G inkgo biloba when compared to placebo (1 trial, 157 people, MD ‐3.30, 95% CI ‐6.51 to ‐0.09, Analysis 18.6).
18.6. Analysis.

Comparison 18 HERB ‐ GINKGO BILOBA versus PLACEBO, Outcome 6 Mental state: 1. Average endpoint scale score (PANSS total, high=poor) ‐ medium term.
18.4 Cognitive function
Cognitive function was measured using the continuous CPT‐37 scale (see above). No difference was found between G inkgo biloba and placebo on this outcome (1 trial, 119 people, MD ‐0.02, 95% CI ‐0.10 to 0.06, Analysis 18.7).
18.7. Analysis.

Comparison 18 HERB ‐ GINKGO BILOBA versus PLACEBO, Outcome 7 Cognitive function: CPT‐37 ‐ proportion correct responses (high=better) ‐ medium term.
19. Comparison 19. Hormone ‐ Oestrogen versus placebo
One trial (Glazer 1985) carried out in the USA that included 12 outpatients with antipsychotic‐induced TD was included for this comparison.
19.1 TD symptoms
19.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found no benefit of oestrogen against placebo (1 trial, 12 people, RR 1.18, 95% CI 0.76 to 1.83, Analysis 19.1).
19.1. Analysis.

Comparison 19 HORMONE ‐ OESTROGEN versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term.
19.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found no benefit of oestrogen against placebo (1 trial, 12 people, RR 0.33, 95% CI 0.05 to 2.37, Analysis 19.2).
19.2. Analysis.

Comparison 19 HORMONE ‐ OESTROGEN versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ short term.
19.1.3 Deterioration of symptoms
There was no difference on deterioration of symptoms between oestrogen and placebo (1 trial, 10 people, RR 0.20, 95% CI 0.01 to 3.35, Analysis 19.3).
19.3. Analysis.

Comparison 19 HORMONE ‐ OESTROGEN versus PLACEBO, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ short term.
19.1.4 Average endpoint scores
TD symptoms were also measured on the continuous AIMS scale (see above). No difference was found between oestrogen and placebo (1 trial, 10 people, MD ‐1.20, 95% CI ‐4.18 to 1.78, Analysis 19.4).
19.4. Analysis.

Comparison 19 HORMONE ‐ OESTROGEN versus PLACEBO, Outcome 4 Tardive dyskinesia: 4. Average scale score (AIMS, high=poor) ‐ short term.
19.2 Adverse effects
There was no difference in the incidence of ‘any adverse effect’ between oestrogen and placebo (1 trial, 12 people, RR 0.33, 95% CI 0.02 to 6.86, Analysis 19.5).
19.5. Analysis.

Comparison 19 HORMONE ‐ OESTROGEN versus PLACEBO, Outcome 5 Adverse effects ‐ short term.
19.3 Leaving the study early
Using oestrogen did not significantly increase the chances of a person leaving the study early (1 trial, 12 people, RR 1.00, 95% CI 0.08 to 12.56, Analysis 19.6).
19.6. Analysis.

Comparison 19 HORMONE ‐ OESTROGEN versus PLACEBO, Outcome 6 Leaving the study early ‐ short term.
20. Comparison 20. Hormone ‐ Insulin versus placebo
One trial (Mouret 1991) carried out in Morocco that included 20 inpatients with antipsychotic‐induced TD was included for this comparison.
20.1 TD symptoms
20.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of insulin against placebo (1 trial, 20 people, RR 0.52, 95% CI 0.29 to 0.96, Analysis 20.1).
20.1. Analysis.

Comparison 20 HORMONE ‐ INSULIN versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
20.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found a benefit in favour of insulin against placebo (1 trial, 20 people, RR 0.06, 95% CI 0.00 to 0.90, Analysis 20.2).
20.2. Analysis.
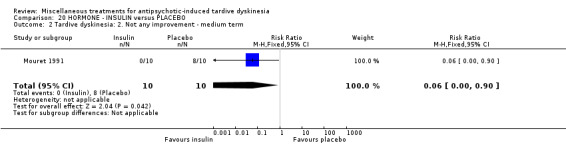
Comparison 20 HORMONE ‐ INSULIN versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term.
20.1.3 Deterioration of symptoms
There was no difference on deterioration of symptoms between insulin and placebo (1 trial, 20 people, RR 0.14, 95% CI 0.01 to 2.45, Analysis 20.3).
20.3. Analysis.

Comparison 20 HORMONE ‐ INSULIN versus PLACEBO, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ medium term.
20.1.4 Average endpoint scores
TD symptoms were also measured on the continuous AIMS scale (see above). A benefit in favour of insulin was found when compared to placebo (1 trial, 20 people, MD ‐6.20, 95% CI ‐10.53 to ‐1.87, Analysis 20.4).
20.4. Analysis.

Comparison 20 HORMONE ‐ INSULIN versus PLACEBO, Outcome 4 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term.
20.2 Leaving the study early
No participants left the included study early.
21. Comparison 21. Hormone ‐ Melatonin versus placebo or no treatment
Four trials (Castro 2011; Shamir 2000; Shamir 2001; Shi 2009) carried out in China, Israel, and Venezuela that included 132 in‐ and out‐patients with antipsychotic‐induced TD was included for this comparison.
21.1 TD symptoms
21.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement', added across all time points, found no benefit of melatonin against placebo (low‐quality evidence, 2 trials, 32 people, RR 0.89, 95% CI 0.71 to 1.12, Analysis 21.1).
21.1. Analysis.

Comparison 21 HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement.
21.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we again found no benefit of melatonin against placebo (1 trial, 19 people, RR 1.11, 95% CI 0.47 to 2.60, Analysis 21.2).
21.2. Analysis.

Comparison 21 HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ short term.
21.1.3 Deterioration of symptoms
There was no difference on deterioration of symptoms between melatonin and placebo (low‐quality evidence, 1 trial, 19 people, RR 0.22, 95% CI 0.01 to 4.05, Analysis 21.3).
21.3. Analysis.

Comparison 21 HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ short term.
21.1.4 Average endpoint scores
TD symptoms were also measured on the continuous AIMS scale (see above). No benefit was found for melatonin when compared to placebo (1 trial, 13 people, MD ‐2.38, 95% CI ‐6.58 to 1.82, Analysis 21.4).
21.4. Analysis.

Comparison 21 HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT, Outcome 4 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term.
21.2 Adverse effects
No participants reported adverse effects.
21.3 Leaving the study early
No participants left the included studies early.
21.4 Cognitive function
Cognitive function was measured using the continuous Wechsler Adult Intelligence Scale (WAIS) and Wechsler Memory Scale (WMS) scales (see above). There was a benefit in favour of melatonin when compared to placebo on the WAIS (1 trial, 76 people, MD 15.83, 95% CI 4.61 to 27.05, Analysis 13.7), however this benefit was not seen on the WMS (1 trial, 76 people, MD 3.77, 95% CI ‐8.21 to 15.75, Analysis 21.7).
21.7. Analysis.

Comparison 21 HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT, Outcome 7 Cognitive function: Average scale score ‐ medium term.
21.5 Mental state
No participants reported deterioration of mental state.
22. Comparison 22. Mood stabiliser ‐ Lithium versus placebo
One trial (Mackay 1980) carried out in the UK that included 11 inpatients with antipsychotic‐induced TD was included for this comparison.
22.1 TD symptoms
22.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found no benefit of lithium against placebo (1 trial, 11 people, RR 1.59,, 95% CI 0.79 to 3.23, Analysis 22.1).
22.1. Analysis.

Comparison 22 MOOD STABILISER ‐ LITHIUM versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term.
22.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we found no benefit of lithium against placebo (1 trial, 11 people, RR 4.29, 95% CI 0.25 to 72.90, Analysis 22.2).
22.2. Analysis.

Comparison 22 MOOD STABILISER ‐ LITHIUM versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ short term.
22.1.3 Deterioration of symptoms
There was no difference on deterioration of symptoms between lithium and placebo (1 trial, 11 people, RR 4.29, 95% CI 0.25 to 72.90, Analysis 22.3).
22.3. Analysis.

Comparison 22 MOOD STABILISER ‐ LITHIUM versus PLACEBO, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ short term.
22.1.4 Average endpoint scores
TD symptoms were also measured on the continuous AIMS scale (see above). No difference was found when lithium was compared to placebo (1 trial, 11 people, MD 0.63, 95% CI ‐5.23 to 6.49, Analysis 22.4).
22.4. Analysis.

Comparison 22 MOOD STABILISER ‐ LITHIUM versus PLACEBO, Outcome 4 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ short term.
22.2 Adverse effects
There was no difference in the incidence of ‘any adverse effect’ between lithium and placebo (1 trial, 11 people, RR 6.00, 95% CI 0.38 to 94.35, Analysis 22.5).
22.5. Analysis.

Comparison 22 MOOD STABILISER ‐ LITHIUM versus PLACEBO, Outcome 5 Adverse events ‐ short term.
22.3 Leaving the study early
Using lithium did not significantly increase the chances of a person leaving the study early (1 trial, 11 people, RR 2.57, 95% CI 0.13 to 52.12, Analysis 22.6).
22.6. Analysis.

Comparison 22 MOOD STABILISER ‐ LITHIUM versus PLACEBO, Outcome 6 Leaving the study early ‐ short term.
23. Comparison 23. Polypeptide ‐ Ceruletide versus placebo
Two trials (Kojima 1992; Matsunaga 1988) carried out in Japan that included 85 in‐ and out‐patients with schizophrenia and TD, or chronic psychosis and TD were included for this comparison.
23.1 TD symptoms
23.1.1 Not any improvement
For the outcome of 'any improvement in TD symptoms', we found no benefit of ceruletide against placebo (2 trials, 132 people, RR 0.83, 95% CI 0.65 to 1.07, Analysis 23.1).
23.1. Analysis.

Comparison 23 POLYPEPTIDE ‐ CERULETIDE versus PLACEBO, Outcome 1 Tardive dyskinesia: 1. Not any improvement.
23.1.2 Deterioration of symptoms
There was no difference on deterioration of symptoms between ceruletide and placebo (low‐quality evidence, 2 trials, 103 people, RR 0.97 CI 0.14 to 6.80, Analysis 23.2).
23.2. Analysis.

Comparison 23 POLYPEPTIDE ‐ CERULETIDE versus PLACEBO, Outcome 2 Tardive dyskinesia: 2. Deterioration.
23.2 Adverse effects
There was no difference in the incidence of ‘any adverse effect’, across all time periods, between ceruletide and placebo (low‐quality evidence, 2 trials, 122 people, RR 1.32, 95% CI 0.74 to 2.36, Analysis 23.3).
23.3. Analysis.

Comparison 23 POLYPEPTIDE ‐ CERULETIDE versus PLACEBO, Outcome 3 Adverse effects.
23.3 Leaving the study early
Using ceruletide did not significantly increase the chances of a person leaving the study early (very low‐quality evidence, 1 trial, 85 people, RR 1.09, 95% CI 0.49 to 2.40, Analysis 23.4).
23.4. Analysis.

Comparison 23 POLYPEPTIDE ‐ CERULETIDE versus PLACEBO, Outcome 4 Leaving the study early ‐ medium term.
24. Comparison 24. Hypnosis or relaxation versus treatment as usual (TAU)
One trial (Glover 1980) carried out in the USA that included 15 outpatients with antipsychotic‐induced TD was included for this comparison.
24.1 TD symptoms
24.1.1 No clinically important improvement
The overall results for 'clinically relevant improvement' found a benefit in favour of hypnosis or relaxation when compared to TAU (very low‐quality evidence, 1 trial, 15 people, RR 0.45, 95% CI 0.21 to 0.94, Analysis 24.1). There was no difference, however, when hypnosis was compared to relaxation (1 trial, 10 people, RR 0.11, 95% CI 0.01 to 1.64, analysis not shown).
24.1. Analysis.

Comparison 24 HYPNOSIS OR RELAXATION versus TREATMENT AS USUAL, Outcome 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term.
24.1.2 Not any improvement
For the outcome of 'any improvement in TD symptoms', we found no benefit of hypnosis or relaxation when compared to TAU (1 trial, 15 people, RR 0.18, 95% CI 0.01 to 3.81, Analysis 24.2).
24.2. Analysis.

Comparison 24 HYPNOSIS OR RELAXATION versus TREATMENT AS USUAL, Outcome 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term.
24.1.3 Deterioration of symptoms
There was no difference on deterioration of symptoms between hypnosis or relaxation and TAU (very low‐quality evidence, 1 trial, 15 people, RR 0.18, 95% CI 0.01 to 3.81, Analysis 24.3).
24.3. Analysis.

Comparison 24 HYPNOSIS OR RELAXATION versus TREATMENT AS USUAL, Outcome 3 Tardive dyskinesia: 3. Deterioration ‐ medium term.
24.2 Leaving the study early
No participants left the included study early.
25. Subgroup analyses
25.1 Clinical stage: Recent onset TD
It was not possible to evaluate whether those with recent onset TD responded differently to those with more established problems, since no trial reported data for groups with different durations of TD that could be extracted for separate analyses.
25.2 Duration of follow‐up
Any effects that the miscellaneous interventions described in this review may have did not clearly change in relation to duration of follow‐up.
26. Heterogeneity
For most comparisons only one study was included, consequently, for these comparisons subgroup‐ and sensitivity analyses could not be undertaken and there was no heterogeneity. For the four comparisons that included more than one study (ceruletide, levetiracetam, melatonin, and dehydrogenated ergot alkaloids), pooled data for leaving the study early for levetiracetam versus placebo were statistically heterogeneous (Analysis 9.3, I2=73%), but neither study (UCB Pharma 2005; Woods 2008, total N=119) found statistically significant results.
27. Sensitivity analyses
27.1 Implication of randomisation
We aimed to include trials in a sensitivity analysis if they were described in some way as to imply randomisation. As all studies were stated to be randomised, we did not undertake this sensitivity analysis.
27.2 Assumptions for lost binary data
We were unable to perform this sensitivity analysis because there were so few studies within each comparison in this review.
27.3 Risk of bias
We were unable to perform this sensitivity analysis because there were so few studies within each comparison in this review.
27.4 Imputed values
We would have undertaken a sensitivity analysis to assess the effects of including data from cluster‐randomised trials where we used imputed values for intra‐class correlation coefficients (ICCs) in calculating the design effect. No cluster‐randomised trials were included.
27.5 Fixed and random effects
We were unable to perform this sensitivity analysis because there were so few studies within each comparison in this review.
Discussion
Summary of main results
1. Searching
This review has identified mainly old studies published before the year 2000 (65%); only six studies were published in the past 10 years. These more recent studies assessed melatonin (Castro 2011; Shi 2009), piracetam (Libov 2007), valbenazine (NBI‐98854) (O'Brien 2014), levetiracetam (Woods 2008), and Ginkgo biloba (Zhang 2011).
2. Few data
Overall, data from 1278 people were included in this review, but few participants were included for each intervention. The number of participants per comparison ranged from 10 (experimental compound ritanserin) to 157 (Chinese herb Ginkgo biloba). It is possible that real, and important, effects have not been highlighted because of the necessarily wide confidence intervals of the findings. Many outcomes were not measured at all (see Overall completeness and applicability of evidence), including one of our pre‐stated outcome measures. We may have been overambitious in hoping for some of these outcomes in tardive dyskinesia (TD) trials but simple reporting of satisfaction with care or quality of life still does not seem too demanding and does remain of interest.
3. Alkaloid ‐ dihydrogenated ergot alkaloids (DEAs) versus placebo
3.1 TD symptoms
We found low‐quality evidence (downgraded due to risk of bias and small sample size) favouring DEAs compared with placebo for no clinically important improvement in TD symptoms after six weeks (RR 0.45, 95% CI 0.21 to 0.97, 1 study, 28 participants). Because the quality of evidence is low, we have limited confidence in the effect estimates and CIs; the true effects may be substantially different. We also found very low‐quality evidence (downgraded due to risk of bias and small sample size) of little or no difference in deterioration of TD symptoms at six‐week follow‐up (RR 0.33, 95% CI 0.01 to 7.55, 1 study, 28 participants). Because the quality of evidence is very low, we are very uncertain about the estimate.
3.2 Adverse events
More participants in the DEAs group experienced adverse events compared with placebo (50% and 21%, respectively), however, the difference was not significant (very low‐quality evidence, RR 2.33, 95% CI 0.75 to 7.23, 1 study, 28 participants). Because the quality of evidence is very low, we are very uncertain about the estimate.
3.3 Acceptability of treatment (measured through participants leaving the study early)
We found very low‐quality evidence (downgraded due to risk of bias, indirectness of measurement, and small sample size) of little to no difference in acceptability of treatment (RR 0.33, 95% CI 0.02 to 7.32, 2 studies, 48 participants). Because the quality of evidence is very low, we are very uncertain about the estimate.
The included study did not report on 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 1 for GRADE ratings.
4. Anxiolytic ‐ buspirone versus placebo
4.1 TD symptoms
We found low‐quality evidence (downgraded due to risk of bias and small sample size) favouring buspirone compared with placebo for no clinically important improvement in TD symptoms after 6 weeks (RR 0.53, 95% CI 0.33 to 0.84, 1 study, 42 participants). Because the quality of evidence is low, we have limited confidence in the effect estimates and CIs; the true effects may be substantially different.
4.2 Acceptability of treatment (measured through participants leaving the study early)
It is always unclear what leaving the study early means. It could be to do with the participant not accepting treatment for a series of reasons, or of participants finding the trial intolerable. It also could be a function of a trial design in which willing participants are still asked to leave because of some degree of protocol violation. In any event, all randomised participants completed the trial and there were no dropouts among 42 participants in one trial with a duration of six weeks.
The included study did not report on 'adverse events' or 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 3 for GRADE ratings.
5. Antiepileptic ‐ levetiracetam versus placebo
5.1 TD symptoms
No studies reported on the TD symptoms outcomes chosen for our 'Summary of findings' tables ('no clinically important improvement in TD symptoms' and 'deterioration of TD symptoms').
5.2 Adverse events
We found low‐quality evidence (downgraded due to risk of bias and small sample size) that more participants experienced adverse events with placebo (46%) compared with levetiracetam (23.5%) at eight‐week follow‐up, however, the difference was not significant (RR 0.51, 95% CI 0.25 to 1.04, 69 participants, 1 study). Because the quality of evidence is low, we have limited confidence in the effect estimates and CIs; the true effects may be substantially different.
5.3 Acceptability of treatment (measured through participants leaving the study early)
We found very low‐quality evidence (downgraded due to risk of bias, inconsistency (I2= 73%), and small sample size) that 17% of participants left the study early, and there was little to no difference between levetiracetam and placebo (RR 1.01, 95% CI 0.46 to 2.22, 119 participants, 2 studies). Because the quality of evidence is very low, we are very uncertain about the estimate.
The included studies did not report on 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 2 for GRADE ratings.
6. Enzyme inhibitor ‐ VMAT2‐inhibitors versus placebo
6.1 TD symptoms
We found moderate‐quality evidence (downgraded due to small sample size) favouring valbenazine (NBI‐98854) compared with placebo for no clinically important improvement in TD symptoms after six weeks (RR 0.63, 95% CI 0.46 to 0.86, 1 study, 92 participants). Because the quality of evidence is moderate, further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
6.2 Adverse events
More participants in the valbenazine group experienced adverse events compared with placebo (49% and 33%, respectively), however, the difference was not significant (low‐quality evidence, (RR 1.50, 95% CI 0.92 to 2.45, 1 study, 100 participants). Because the quality of evidence is low (downgraded due to small sample size and very few events reported), we have limited confidence in the effect estimates and CIs; the true effects may be substantially different.
6.3 Acceptability of treatment (measured through participants leaving the study early)
We found very low‐quality evidence (downgraded due to small sample size and very few events reported, and indirectness of measurement) that 10% of participants left the study early, and there was little to no difference between the valbenazine group and the placebo group (RR 1.00, 95% CI 0.31 to 3.25, 102 participants, 1 study). Because the quality of evidence is very low, we are very uncertain about the estimate.
The included study did not report on 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 4 for GRADE ratings.
7. Fatty acid ‐ ethyl‐EPA versus placebo
7.1 TD symptoms
No studies reported on the TD symptoms outcomes chosen for our 'Summary of findings' tables ('no clinically important improvement in TD symptoms' and 'deterioration of TD symptoms').
7.2 Adverse events
We found low‐quality evidence (downgraded due to risk of bias and small sample size) of little to no difference between ethyl‐EPA and placebo in parkinsonism extrapyramidal symptoms (EPSs) measured on the Extrapyramidal System Rating Scale (ESRS) (MD 0.30, 95% CI ‐1.17 to 1.77, 1 trial, 75 participants), and of a benefit to ethyl‐EPA compared with placebo in dystonia EPSs measured on the ESRS (MD ‐0.35, 95% CI ‐0.58 to ‐0.12) 1 trial, 75 participants). Because the quality of evidence is low, further research is likely to have an important impact on our confidence in the estimates of effect and may change the estimates. Further, we found very low‐quality evidence (downgraded due to risk of bias and small sample size with very wide CIs) of little to no difference between ethyl‐EPA and placebo in akathisia EPSs measured on the ESRS (MD ‐0.04, 95% CI ‐0.30 to 0.22, 1 trial, 75 participants). Because the quality of evidence is very low, we are very uncertain about the estimate.
7.3 Acceptability of treatment (measured through participants leaving the study early)
More participants in the placebo group left the study early than in the ethyl‐EPA group (33% and 19%, respectively), however, the difference was not significant (very low‐quality evidence, (RR 0.57, 95% CI 0.27 to 1.22, 1 study, 84 participants). Because the quality of evidence is very low, we are very uncertain about the estimate.
The included study did not report on 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 5 for GRADE ratings.
8. Herb ‐ Ginkgo biloba versus placebo
8.1 TD symptoms
We found moderate‐quality evidence (downgraded due to small sample size) favouring G inkgo biloba compared with placebo for no clinically important improvement in TD symptoms after 12 weeks (RR 0.88, 95% CI 0.81 to 0.96, 1 trial, 157 participants). Because the quality of evidence is moderate, further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
8.3 Acceptability of treatment (measured through participants leaving the study early)
More participants left the study early in the placebo group compared to the G inkgo biloba group (5% and 1.3%, respectively), however the difference was not significant (very low‐quality evidence, RR 0.25, 95% CI 0.03 to 2.22, 1 trial, 157 participants). Because the quality of evidence is very low (downgraded due to small sample size with very few events reported and indirectness of measurement), we are very uncertain about the estimate.
The included study did not report on 'adverse events' or 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 6 for GRADE ratings.
9. Hormone ‐ melatonin versus placebo
9.1 TD symptoms
We found low‐quality evidence (downgraded due to inconsistency (I2 = 46%) and small sample size) of little or no difference for no clinically important improvement in TD symptoms for melatonin compared with placebo after three to 12 weeks (RR 0.89, 95% CI 0.71 to 1.12, 2 studies, 32 participants). Again, we found low‐quality evidence (downgraded due to very small sample size) of little or no difference in deterioration of TD symptoms at three‐week follow‐up (RR 0.22, 95% CI 0.01 to 4.05, 1 study, 19 participants). Because the quality of evidence is low for these outcomes, we have limited confidence in the effect estimates and CIs; the true effects may be substantially different.
9.2 Adverse events
No events were reported for this outcome among 54 participants in three studies with a duration of three to 12 weeks.
9.3 Acceptability of treatment (measured through participants leaving the study early)
All randomised participants completed the trial and there were no dropouts among 54 participants in three studies with a duration of three to 12 weeks.
The included studies did not report on 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 7 for GRADE ratings.
10. Polypeptide ‐ ceruletide versus placebo
10.1 TD symptoms
We found low‐quality evidence (downgraded due to risk of bias and small sample size) of little or no difference in deterioration of TD symptoms at four to eight weeks follow‐up (RR 0.97, 95% CI 0.14 to 6.80, 2 studies, 103 participants). Because the quality of evidence is low, we have limited confidence in the effect estimates and CIs; the true effects may be substantially different.
10.2 Adverse events
We found low‐quality evidence (downgraded due to risk of bias and small sample size) that more participants experienced adverse events with ceruletide (31%) compared with placebo (23%) at four to eight weeks follow‐up, however, the difference was not significant (RR 1.32, 95% CI 0.74 to 2.36, 122 participants, 2 studies). Because the quality of evidence is low, we have limited confidence in the effect estimates and CIs; the true effects may be substantially different.
10.3 Acceptability of treatment (measured through participants leaving the study early)
We found very low‐quality evidence (downgraded due to risk of bias, indirectness of measurement, and small sample size) that around 20% of participants left the study early, and there was little to no difference between ceruletide and placebo (RR 1.09, 95% CI 0.49 to 2.40, 85 participants, 1 study). Because the quality of evidence is very low, we are very uncertain about the estimate.
The included studies did not report on 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 8 for GRADE ratings.
11. HYPNOSIS OR RELAXATION versus TAU
11.1 TD symptoms
We found very low‐quality evidence favouring hypnosis or relaxation compared with placebo for 'no clinically important improvement in TD symptoms' after 8 sessions (RR 0.45, 95% CI 0.21 to 0.94, 1 study, 15 participants). We also found very low quality evidence of little or no difference in deterioration of TD symptoms between hypnosis or relaxation and placebo after 8 sessions (RR 0.18, 95% CI 0.01 to 3.81, 1 study, 15 participants). Because the quality of evidence is very low (downgraded due to serious risk of bias and very small sample size), we are very uncertain about these estimates.
11.3 Acceptability of treatment (measured through participants leaving the study early)
All randomised participants completed the study and there were no dropouts among 15 participants in one study of eight sessions (exact duration was not reported).
The included study did not report on 'adverse events' and 'social confidence, social inclusion, social networks, or personalised quality of life' ‐ outcomes assessed by patients and review authors as particularly important (see Types of outcome measures). Please see Table 9 for GRADE ratings.
12. OTHER COMPARISONS
The remaining 15 comparisons (cyproheptadine, lithium, papaverine, pemoline, piracetam, promethazine, ritanserin, selegiline, isocarboxazid, oestrogen, insulin, gamma‐linolenic acid, branched‐chain amino acids, phenylalanine, and stepholidine) included less than 60 participants each (10 to 57 participants per intervention with a median of 22 participants) and were not prioritised in the selection process for the NIHR HTA systematic review (Bergman 2017). Consequently, we did not create 'Summary of findings' tables for these interventions (see Prioritising interventions for 'Summary of findings' tables, Types of outcome measures). We summarise the results from these trials narratively below. We would like to point out that due to the small sample sizes per comparison, potential treatment effects could have gone undetected.
12.1 TD symptoms
A benefit for the intervention compared with placebo was found for pemoline, promethazine, insulin, and branched‐chain amino acids, and for isocarboxazid compared with procyclidine (one trial per comparison, average number of participants: 38, follow‐up duration: three to 40 weeks (median: 12 weeks)). However, due to the small sample sizes and risk of biases for most of these trials, we are very uncertain about these results. For lithium, ritanserin, selegiline, oestrogen, and gamma‐linolenic acid compared to placebo, results showed no significant difference between groups on 'no clinically important improvement in TD symptoms' (one trial per comparison, average number of participants: 16, follow‐up duration: three to six weeks). Due to the small sample sizes, short study duration, and risk of biases for most of these trials, we are very uncertain about these results. Studies assessing cyproheptadine, papaverine, piracetam, and phenylalanine did not report on 'no clinically important improvement in TD symptoms'.
For cyproheptadine, lithium, ritanserin, oestrogen, and gamma‐linolenic acid compared to placebo, results showed no significant difference between groups on 'deterioration of TD symptoms' (one trial per comparison, average number of participants: 18, follow‐up duration: three to six weeks). Due to the small sample sizes, short study duration, and risk of biases for most of these trials, we are very uncertain about these results. Studies assessing papaverine, pemoline, piracetam, promethazine, selegiline, isocarboxazid, insulin, branched‐chain amino acids, phenylalanine, and stepholidine did not report on 'deterioration of TD symptoms'.
12.2 Adverse events
Only seven of the 15 other comparisons reported on adverse events. Studies evaluating cyproheptadine, lithium, piracetam, promethazine, and oestrogen found no significant difference between intervention and placebo (one trial per comparison, average number of participants: 28, follow‐up duration: three to 12 weeks (median: four weeks)), the study evaluating isocarboxazid versus procyclidine also found no significant difference between groups (one trial, 20 participants, follow‐up duration: 40 weeks), and the study assessing stepholidine versus placebo reported that no adverse events occurred (57 participants, follow‐up duration: eight weeks). Due to the small sample sizes, short study duration, and risk of biases for most of these trials, we are very uncertain about these results. Studies assessing papaverine, pemoline, ritanserin, selegiline, insulin, gamma‐linolenic acid, branched‐chain amino acids, and phenylalanine did not report on adverse events.
12.3 Acceptability of treatment (measured through participants leaving the study early)
Studies assessing cyproheptadine, lithium, pemoline, piracetam, promethazine, selegiline, isocarboxazid, oestrogen, insulin, gamma‐linolenic acid, branched‐chain amino acids, phenylalanine, and stepholidine reported no significant differences in participants leaving the studies early compared to placebo groups (one trial per comparison, average number of participants: 31, follow‐up duration: one day to 40 weeks (median: six weeks)). Again, due to the small sample sizes, short study duration, and risk of biases for most of these trials, we are very uncertain about these results. Studies assessing papaverine and ritanserin did not clearly report on number of randomised participants and were consequently not analysed for this outcome.
12.4 Social confidence, social inclusion, social networks, or personalised quality of life
Again, none of the other included studies assessed this group of outcomes that were prioritised by patients as particularly important (see Types of outcome measures).
Overall completeness and applicability of evidence
1. Completeness
No outcomes in this review involved large numbers of people. Many of the included studies were no more than pilot studies, and due to their small size, they cannot really be expected to fully answer any questions about the effects of this miscellaneous group of interventions for people with TD.
Some outcomes are general measures and more subtle findings are not recorded. For example, we identified few data on the outcome of ‘any adverse effect’ but none on the binary outcomes ‘use of any anti‐parkinsonism drugs’ or ‘no clinically significant extrapyramidal adverse effects ‐ any time period’‐ the latter being one of our pre‐stated primary outcomes. There were no data on the patient‐designated important outcomes of social confidence, social inclusion, social networks, or personalised quality of life for either recipients of care or caregivers, nor were there data on hospital and service utilisation outcomes, or economic outcomes.
Deutetrabenazine and valbenazine, both recently approved by the FDA for TD (Brooks 2017; FDA 2017), are VMAT‐2 inhibitors that were assessed in included study O'Brien 2014 (valbenazine), in awaiting classification studies Fernandez 2016, Hauser 2016 and NCT01393600 2011, and in ongoing studies NCT01688037 2012 and NCT02291861 2014. We look forward to including results from these new and ongoing trials in a future update of this review.
2. Applicability
Trials were a mixture of hospital‐based and outpatient, and were on people who would be recognisable in everyday care, however, mostly on men in their 50s with schizophrenia in hospital and mostly in high‐income countries. Overall, sample sizes in relevant studies were particularly small. In light of the lack of power available to examine the compounds of interest, the results should be interpreted as inconclusive rather than negative at this stage. The majority of studies had a duration of six weeks or less whilst only seven had a duration of at least 12 weeks. Whether the effects of the interventions were maintained at longer periods of follow‐up may therefore be under‐reported in short‐term studies.
Quality of the evidence
Overall, the quality of the evidence is low to very low. This means that we have limited to very little confidence in the effect estimates, and the true effect may be, or is likely to be, substantially different from the estimate of the effect. The main reasons for our low confidence in the evidence include the following.
Poor study methodology and reporting of methods resulting in downgrading evidence for risk of bias. Allocation concealment was not described, generation of the sequence was not explicit, studies were not clearly blinded, we are unsure if data are incomplete or selectively reported or if other biases were operating.
Very small sample sizes resulting in downgrading evidence for imprecision. The median sample size in this review was only 34 people. A trial of this size is unable to detect subtle, yet important differences due to an intervention with any confidence. In order to detect a 20% difference between groups, probably about 150 people are needed in each arm of the study (alpha 0.05, beta 0.8).
Wide CIs (often due to low event rates) that included appreciable benefit or harm for the intervention as well as no effect, resulting in downgrading evidence for imprecision.
Please see Additional tables, 'Summary of findings' tables 1‐9 for full details.
The small trial sizes, along with the poor reporting of trials, would be associated with an exaggeration of effect of the experimental treatment (Jűni 2001) when an effect was detected.
Potential biases in the review process
1. Missing studies
Every effort was made to identify relevant trials. However, these studies are all small and it is likely that we have failed to identify other studies of limited power. It is likely that such studies would also not be in favour of the intervention group. If they had been so, it is more likely that they would have been published in accessible literature. We do not, however, think it likely that we have failed to identify large relevant studies.
2. Missing data
We excluded 12 studies published between 1973 and 2004 that did not provide any usable data, see Excluded studies. We contacted authors and two replied to confirm no usable data are available. Authors of eight studies did not reply, and we could not find up‐to‐date contact details for authors of two studies (both over 30 years old). We find it very unlikely we would receive a reply from authors regarding research conducted so many years ago; therefore, these studies were also excluded.
3. Introducing bias
This review has now been updated several times. We have tried to be balanced in our appraisal of the evidence but could have inadvertently introduced bias. We welcome comments or criticisms. New methods and innovations now make it possible to report data where, in the past, we could not report data at all or had to report data in a different way. We believe the 'Summary of findings' tables are a valuable innovation – but problematic to those not ‘blind’ to the outcome data. It is possible to ‘cherry pick’ significant findings for presentation in this table. We have tried to decrease the chance of doing this by asking a new review author (HB) to select outcomes relevant for these tables before becoming familiar with the data.
Agreements and disagreements with other studies or reviews
This review substantially updates earlier versions. The previous version of this review contained assessments of eight interventions (ceruletide, gammalinolenic acid, insulin, lithium, oestrogen, phenylalanine, piracetam, and ethyl‐EPA) and the conclusions on those interventions has not changed with this update. In addition, we have updated this review with evidence from another 16 interventions. Bergman 2017 reports on interventions in all nine Cochrane reviews on TD in this series (see Table 10) and is in agreement with the findings and conclusions of this review.
Other systematic reviews have covered melatonin (Nelson 2003), extract of Ginkgo biloba (Zheng 2016), and any treatment for TD (Alimi 2013). We are in agreement with both Nelson 2003, that "There are inadequate data at the present time to support the use of melatonin in patients with TD", and with Zheng 2016, that Ginkgo biloba appears to be safe and effective for improving TD symptoms and that better randomised controlled trials are needed to confirm this evidence.
Alimi 2013 found that three of the interventions included in this review may help to improve TD symptoms: BCAAs, Ginkgo biloba, and piracetam. Our review included the same studies for these three interventions and also found that BCAAs and Ginkgo biloba appear to reduce TD symptoms. However, for BCAAs, we also conclude that due to the small sample size (n = 68), short follow‐up (three weeks), and risk of bias, we are very uncertain about this result, and for Ginkgo biloba, we also conclude that further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate because evidence was of moderate quality (due to small sample size, n = 157). Libov 2007, the study that evaluated piracetam, is a cross‐over study and we extracted data only from the first phase because of risk of carry‐over effect despite a wash‐out period and because TD is an unstable condition (see Implications for research, 2.1 Use of cross‐over design). This may be why our results differed from Alimi 2013 on piracetam; we found no benefit.
Authors' conclusions
Implications for practice.
1. For people with antipsychotic induced tardive dyskinesia (TD)
Most of this group of miscellaneous treatments do not look even promising for helping symptoms of TD. There is, however, some suggestion that valbenazine and extract of Ginkgo biloba may alter the course of TD for those with schizophrenia. The findings on Ginkgo biloba are in keeping with other reviews (Alimi 2013; Zheng 2016), and valbenazine has been approved by the FDA for use in TD (FDA 2017). To date, these data are still weak and should be interpreted with caution. If offered any of these treatments to offset symptoms of TD a person taking antipsychotic medication would be justified in asking for evidence, and encouraging generation of new, better evidence by volunteering to help with a well‐designed evaluative study.
2. For clinicians
Most of this miscellaneous group of treatments remain purely experimental and there is no place for their use in every day practice. This review generates a theory that valbenazine and extract of Ginkgo biloba could reduce TD symptoms to a clinically important degree. The data in this review do not justify routine use of these treatments, however, valbenazine is the only treatment included in this review that has been approved by the FDA for use in TD (FDA 2017). It would be reasonable, however, to ask people with schizophrenia to complicate their treatment plan if the use of this group of miscellaneous treatments were to generate data better than seen in this review. There is a real place for clinician‐driven research, with prescription within the context of a randomised trial and routine data collection on outcomes of relevance to people with TD and their clinicians.
3. For policy makers and managers
This is the largest in the series of Cochrane reviews on TD. We found inconclusive (low‐ to very low‐certainty evidence) evidence on most of the interventions, however, there was moderate‐certainty evidence that adding valbenazine or extract of Ginkgo biloba to treatment with antipsychotic medication probably helps with the symptoms of TD. Valbenazine is the only treatment included in this review that has been approved by the FDA for use in TD (FDA 2017). More well‐designed randomised controlled trials are needed to confirm these results. This unattractive adverse effect is caused, to a greater or lesser extent, by antipsychotic drugs. Clinicians and researchers should feel responsible enough to continue to try to help it. Those compiling guidance could encourage supportive activity and more research into this neglected area.
Implications for research.
1. General
The power of this review would have been greatly enhanced by better reporting of data. For example, only five studies (16%) made explicit how randomisation was undertaken, and only seven (23%) described allocation concealment. Many of the studies we found were performed decades ago, before CONSORT (CONsolidated Standards of Reporting Trials; CONSORT; Moher 2001). This is intended to improve reporting of randomised controlled trials, enabling readers to understand the design, conduct, analysis and interpretation, and to assess the validity of results. CONSORT emphasises that this can only be achieved through complete transparency from authors. It is only too easy to judge studies of the past by standards of today, future studies, however, should report to a much higher standard.
2. Specific
The number of disparate compounds targeted in this review is indicative of the frustration felt by researchers. Still, after decades of research, no clearly effective treatments for TD have emerged. Presumably an even greater variety of interventions never even reached the stage of warranting examination in a randomised controlled trial. As basic science increases our understanding of the neurobiological basis of involuntary movements, psychiatric researchers should remain vigilant for new candidate compounds for the treatment of TD. TD remains a large problem and worthy of research, even with use of lower doses and newer compounds. Well‐designed randomised controlled trials, involving a large number of participants over protracted periods of time, are needed if we are to see if an intervention could have a role in prevention and treatment of TD. Such studies are of importance to people with the problem (Figure 1) and have long been ignored.
2.1 Use of cross‐over design
Trialists find it difficult to identify people with both TD and schizophrenia to participate in trials (Schmidt 1991). Randomised cross‐over design is used in the hope of improving the power of the study to find outcomes of interest. This design initially asks participants to be randomised to one of the experimental interventions, and then, at a pre‐specified time, to be crossed over to the treatment that they did not at first receive. Conditions with a more stable time course than TD are better suited for cross‐over studies (Fleiss 1984). Further difficulties are the carry‐over effect. Unless cross‐over studies include a mid‐study washout period (where the person is free of treatment before starting the next arm of the study), any effect of an intervention may continue into the second half placebo arm of the trial – the 'carry‐over effect'. Also, carry‐over may involve the re‐growth or retreat of neuroreceptors. This slow re‐balancing, if started, could continue long after all traces of the intervention are gone, so physiological half‐life of the experimental treatment may not be the only variable to consider when thinking though the issues of carry‐over. TD is also an unstable condition and people with TD may not remain compliant with medication. All these factors make the arguments for not using cross‐over methodology strong, despite the initial attraction (Armitage 1991; Fleiss 1984; Pocock 1983).
2.2 Sample size calculation
The results suggest that larger sample size should be used to provide more precise estimates of effect and to help avoid false conclusions about the effects of the proposed treatment.
2.3 Length of study
One study included in this review (Bucci 1971) used the intervention for more than three months. TD, however, is a chronic condition of insidious onset, the severity of which fluctuates spontaneously (APA 1992). Even if an intervention has a swift effect, it is the long‐term outcomes that must be considered of most clinical value.
2.4 Outcomes
Scale‐derived data do have their place. Trials most commonly used the Abnormal Involuntary Movement Scale (AIMS) scale. This is a very widely used tool to measure the severity of symptoms of those who have TD. The use of this scale to measure change as a result of treatment is, however, problematic (Bergen 1984). It is therefore important that a scale is validated for measuring changes secondary to treatment in those with TD. In addition, many of the outcomes we initially desired when we started this review have not been investigated. Finally, a service user consultation also informed the addition of outcomes of special importance to patients. We have reconsidered all these outcomes in case they were too ambitious and tried to tailor them to a real‐world pragmatic trial design (see Table 12).
3. Suggestions for design of future study.
| Methods | Allocation: randomised, with sequence generation and concealment of allocation clearly described. Blindness: double, tested. Duration: 12 months beyond end of intervention at least. Raters: independent. |
| Participants | People with antipsychotic‐induced tardive dyskinesia.* Age: any. Sex: both. History: any. N = 300.** |
| Interventions | 1. Active intervention. N = 150. 2. Placebo: N = 150. |
| Outcomes | Tardive dyskinesia: any clinically important improvement in TD, any improvement, deterioration.*** Adverse effects: no clinically significant extrapyramidal adverse effects ‐ any time period***, use of any antiparkinsonism drugs, other important adverse events. Leaving the study early. Service outcomes: admitted, number of admissions, length of hospitalisation, contacts with psychiatric services. Compliance with drugs. Economic evaluations: cost‐effectiveness, cost‐benefit. General state: relapse, frequency and intensity of minor and major exacerbations. Social confidence, social inclusion, social networks, or personalised quality of life: binary measure Distress among relatives: binary measure. Burden on family: binary measure. |
| Notes | * This could be diagnosed by clinical decision. If funds were permitting all participants could be screened using operational criteria, otherwise a random sample should suffice. ** Size of study with sufficient power to highlight about a 10% difference between groups for primary outcome. *** Primary outcome. The same applies to the measure of primary outcome as for diagnosis. Not everyone may need to have operational criteria applied if clinical impression is proved to be accurate. |
What's new
| Date | Event | Description |
|---|---|---|
| 16 January 2018 | New citation required but conclusions have not changed | Results of 2017 updated search have been added to the review and have not changed the overall conclusions of the review. |
| 26 April 2017 | New search has been performed | Search was updated again, five Studies (eight References) were found and assessed. |
| 31 October 2016 | Amended | Title updated, results of 2015 update search added ‐ 22 new included studies included, outcomes list updated due to patient consultation, PRISMA study flow chart added, 'Summary of findings' tables added, text (including methods) updated, conclusions updated. |
History
Protocol first published: Issue 1, 1997 Review first published: Issue 3, 1997
| Date | Event | Description |
|---|---|---|
| 5 October 2011 | Amended | Contact details updated. |
| 13 April 2011 | Amended | Contact details updated. |
| 16 October 2009 | New search has been performed | Two new studies included, two awaiting assessment, one excluded. Reformatted. |
| 23 January 2003 | New citation required and conclusions have changed | Substantive amendment |
| 2 June 1997 | New citation required and conclusions have changed | First version of Cochrane review |
| 27 November 1996 | Amended | Protocol first published |
Acknowledgements
The authors are indebted to Geoff Davies, Kirsten Mason, Carmel Meir and Leanne Roberts for assistance with this review.
We are especially grateful to the following trialists who provided additional material; Professor Jes Gerlach, Dr Tetsuo Matsunaga, Dr Jacques Mouret, Dr Jan Sikora, Dr Krishna Viddadi and Dr Adam Wolkin. Thank you to John McGrath for protocol development, data extraction and assimilation and report writing. John authored this review from 1997‐2002.
For the 2017 update, we wish to thank Rosie Asher (RA) and Antonio Grande (AG) for screening literature and helping with data extraction, Farhad Sokraneh for carrying out the trial search and helping to find full‐text papers, Ben Gray for writing the Plain language summary, and Nicholas Henschke and Loukia Spineli for assistance with preparing the report. We also acknowledge Dawn‐Marie Walker, Ruth Sayers, Megan Lees, and Vanessa Pinfold from McPin Foundation for organising and holding the public and patient involvement consultation with TD service users that contributed to selecting outcomes for the 'Summary of findings' tables and to guide future research. Finally, we wish to thank Sai Zhao and Jun Xia for assessing and extracting data from articles in Chinese.
The Cochrane Schizophrenia Group Editorial Base in Nottingham produces and maintains standard text for use in the Methods sections of their reviews. We have used this text as the basis of what appears here and adapted it as required.
Appendices
Appendix 1. Earlier searches
1.1 The 2002 update search
The Cochrane Schizophrenia Group's Register (January 2002) was searched with the following phrase
*dyskinesia* AND (*botulin* or *endorphin* or *estrogen* or *fatty acid* or *EX ?11?582A* or *ganglioside* or *insulin* or *lithium* or *naloxone* or *periactin* or *phenylalanine* or *piracetam* or *stepholidine* or *tryptophan* or *neurosurg* or * ect*)
1.2 The search for the previous versions of this review
1.2.1 Biological Abstracts (January 1982 to May 1995) was searched using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase:
[and ((tardive near (dyskine* or diskine*) or (abnormal near movement* near disorder*) or (involuntar* near movement*))]
The resulting set of reports was handsearched for possible trials and researched, within the bibliographic package, ProCite, with the phrase [botulin or endorphin or estrogen or (fatty and acid) or EX ?11?582A or ganglioside or lithium or naloxone or periactin or phenylalanine or piracetam or stepholidine or tryptophan or neurosurg* or ect]
1.2.2 Cochrane Schizophrenia Group's Register (January 1996) was searched using the phrase:
[(dyskinesia or (#30=60) or (#30=2)) and botulin or endorphin or estrogen or (#42=297) or (fatty and acid) or EX ?11?582A or ganglioside or lithium or (#42=16) or naloxone or (#42=8) or periactin or phenylalanine or piracetam or (#42=119) or stepholidine or tryptophan or (#42=181) or neurosurg* or ect or (#42=48))]
1.2.3 EMBASE (January 1980 to May 1995) was searched using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase:
[and ((tardive dyskinesia in thesaurus ‐subheadings, prevention, drug therapy, side effect and therapy) or (neuroleptic dyskinesia in thesaurus ‐all subheadings) or (tardive or dyskines*) or (movement* or disorder*) or (abnormal or movement* or disorder*))]
The resulting set of reports was handsearched for possible trials and researched, within the bibliographic package, ProCite, with the phrase [botulin or endorphin or estrogen or (fatty and acid) or EX ?11?582A or ganglioside or lithium or naloxone or periactin or phenylalanine or piracetam or stepholidine or tryptophan or neurosurg* or ect]
1.2.4 LILACS (January 1982 to September 1996) was searched using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase:
[and ((tardive or (dyskinesia* or diskinesia*)) or (drug induced movement disorders in thesaurus))]
The resulting set of reports was handsearched for possible trials and researched, within the bibliographic package, ProCite, with the phrase [botulin or endorphin or estrogen or (fatty and acid) or EX ?11?582A or ganglioside or lithium or naloxone or periactin or phenylalanine or piracetam or stepholidine or tryptophan or neurosurg* or ect]
1.2.5 MEDLINE (January 1966 to May 1995) was searched using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase:
[and ((movement‐disorders in MeSH / explode all subheadings) or (anti‐dyskinesia‐agents in MeSH / explode all subheadings) or (dyskinesia‐drug‐induced in MeSH / explode all subheadings) and (psychosis in MeSH / explode all subheadings) or (schizophrenic disorders in MeSH / explode all subheadings) or (tardive near (dyskine* or diskine*)) or (abnormal* near movement* near disorder*) or (involuntar* near movement*))]
The resulting set of reports was handsearched for possible trials and researched, within the bibliographic package, ProCite, with the phrase [botulin or endorphin or estrogen or (fatty and acid) or EX ?11?582A or ganglioside or lithium or naloxone or periactin or phenylalanine or piracetam or stepholidine or tryptophan or neurosurg* or ect]
1.2.6 PsycLIT (January 1974 to May 1995) was searched using the Cochrane Schizophrenia Group's phrase for randomised controlled trials (see Group search strategy) combined with the phrase:
[and ((explode movement‐disorders in DE) or (explode tardive‐dyskinesia in DE) or (tardive near (dyskine* or diskine*)]
The resulting set of reports was handsearched for possible trials and researched, within the bibliographic package, ProCite, with the phrase [botulin or endorphin or estrogen or (fatty and acid) or EX ?11?582A or ganglioside or lithium or naloxone or periactin or phenylalanine or piracetam or stepholidine or tryptophan or neurosurg* or ect]
1.2.7 SCISEARCH ‐ Science Citation Index Each of the included studies was sought as a citation on the SCISEARCH database. Reports of articles that had cited these studies were inspected in order to identify further trials.
Appendix 2. Previous methods
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials. Where a trial was described as 'double‐blind', but it was only implied that the study was randomised, we included these trials in a sensitivity analysis. If there was no substantive difference within primary outcomes (seeTypes of outcome measures) when these 'implied randomisation' studies were added, then we included these in the final analysis. If there was a substantive difference, we only used clearly randomised trials and described the results of the sensitivity analysis in the text. We excluded quasi‐randomised studies, such as those allocating by using alternate days of the week.
Types of participants
We included people with schizophrenia and other types of schizophrenia‐like psychosis (e.g. schizophreniform and schizoaffective disorders), irrespective of the diagnostic criteria used, who: i. required the use of neuroleptics for more than three months; ii. developed tardive dyskinesia (diagnosed by any criteria) during neuroleptic treatment; and iii. for whom the dose of neuroleptic medication had been stable for one month or more before the trial. There is no clear evidence that the schizophrenia‐like psychoses are caused by fundamentally different disease processes or require different treatment approaches (Carpenter 1994).
Types of interventions
1. Drugs Botulin toxin, dimethylaminoethanol, endorphin, oestrogen, essential fatty acid, EX 11‐582A, ganglioside GM1, lithium, methylphenidate, naloxone, naltrexone, periactin, phenylalanine, piracetam, stepholidine, tryptophan. Any doses, frequencies or means of administration were acceptable.
2. Surgical intervention of any sort.
3. Electroconvulsive therapy (ECT).
Compared with:
1. Standard care; or
2. Placebo or no treatment.
Types of outcome measures
Where possible, outcomes were grouped into time periods ‐ short term (less than 6 weeks), medium term (between 6 weeks and 6 months) and long term (over 6 months).
Primary outcomes
1. Tardive dyskinesia 1.1 No clinically important change in tardive dyskinesia
2. Mental state 2.1 No clinically important change in general mental state 3. Adverse effects 3.1 Clinically important general adverse effects 4. Leaving the study early 4.1 For general reasons
Secondary outcomes
1. Tardive dyskinesia 1.2 Not any change in tardive dyskinesia 1.3 Average endpoint tardive dyskinesia score 1.4 Average change in tardive dyskinesia score
2. Mental state 2.1 Not any change in general mental state 2.2 Average endpoint general mental state score 2.3 Average change in general mental state score 2.4 No clinically important change in specific symptoms 2.5 Not any change in specific symptoms 2.6 Average endpoint specific symptom score 2.7 Average change in specific symptom score
3. Adverse effects 3.1 Any general adverse effects 3.2 Average endpoint general adverse effect score 3.3 Average change in general adverse effect score 3.4 Clinically important change in specific adverse effects 3.5 Any change in specific adverse effects 3.6 Average endpoint specific adverse effects 3.7 Average change in specific adverse effects
4. Leaving the study early 4.1 For specific reasons
Search methods for identification of studies
Electronic searches
1. Update of 2009 We searched the Cochrane Schizophrenia Group Trials Register (September 2009) using the phrase:
[*dyskinesia* in title, abstract and index fields or REFERENCE]
This register is compiled by systematic searches of major databases, hand searches and conference proceedings (see Group Module).
2. Previous searches for earlier versions of this review Please see (Appendix 1).
Searching other resources
1. Reference searching We also inspected the references of all studies identified in this way for more studies.
2. Personal contact We contacted the first author of each included study for information regarding unpublished trials.
Data collection and analysis
Selection of studies
Two reviewers independently inspected all study citations identified by the searches, and full reports of the studies of agreed relevance were obtained. Where disputes arose, we acquired the full report for more detailed scrutiny. These articles were then inspected, independently, by two reviewers to assess their relevance to this review. Again, where disagreement occurred attempts were made to resolve this through discussion; if doubt still remained we added these trials to the list of those awaiting assessment pending acquisition of further information.
Data extraction and management
1. Extraction We independently extracted data. Where disagreement occurred attempts were made to resolve this by discussion, where doubt still remained we sought further information from the study authors to resolve the dilemma, and added the trial to the list of those awaiting assessment.
2. Management 2.1 Data storage We extracted the data onto standard, simple forms. Where possible, data were entered into RevMan in such a way that the area to the left of the 'line of no effect' indicates a 'favourable' outcome for the treatment group. Where this was not possible, (e.g. scales that calculate higher scores=improvement) the graphs in RevMan analyses were labelled accordingly so that the direction of effects were clear.
2.2 Categorical or continuous into binary Where possible, efforts were made to convert outcome measures to binary data. This can be done by identifying cut off points on rating scales and dividing participants accordingly into "clinically improved" or "not clinically improved". It is generally assumed that if there is a 50% reduction in a scale‐derived score such as the Brief Psychiatric Rating Scale (BPRS Overall 1962) or the Positive and Negative Syndrome Scale (PANSS, Kay 1986, this could be considered a clinically significant response (Leucht 2005a, Leucht 2005). It is recognised that for many people, especially those with chronic or severe illness, a less rigorous definition of important improvement (e.g. 25% on the BPRS) would be equally valid. If individual patient data are available, we used the 50% cut‐off point for non‐chronically ill people and a 25% cut‐off point for those with chronic illness. If data based on these thresholds were not available, we used the primary cut‐off presented by the original authors.
2.3 Continuous data and their distribution Continuous data on outcomes in mental health trials are often not normally distributed. To avoid the pitfall of applying parametric tests to non‐parametric data we applied the following standards to all endpoint data derived from continuous measures. The criteria were used before inclusion: (a) standard deviations and means had to be obtainable; and, for finite scores, such as endpoint measures on rating scales, (b) the standard deviation (SD), when multiplied by 2 had to be less than the mean (as otherwise the mean was unlikely to be an appropriate measure of the centre of the distribution) (Altman 1996). If a scale starts from a positive value (such as PANSS, which can have values from 30 to 210) the calculation described above in (b) should be modified to take the scale starting point into account. In these cases skewness is present if 2SD>(S‐Smin), where S is the mean score and Smin is the minimum score.
Skewed endpoint data from studies with less the 200 participants were not shown graphically, but were added to 'Other data' tables and briefly commented on in the text. However, skewed endpoint data from larger studies (=/>200 participants) pose less of a problem and we entered the data for analysis (Higgins 2009).
For continuous mean change data (endpoint minus baseline) the situation is even more problematic. In the absence of individual patient data it is impossible to know if change data are skewed. The RevMan meta‐analyses of continuous data are based on the assumption that the data are, at least to a reasonable degree, normally distributed. We included such data, unless endpoint data were also reported from the same scale.
2.4 Final endpoint value versus change data Where both final endpoint data and change data were available for the same outcome category, only final endpoint data were presented. We acknowledge that by doing this much of the published change data may be excluded, but argue that endpoint data is more clinically relevant and that if change data were to be presented along with endpoint data, it would be given undeserved equal prominence.
3. Scale‐derived data A wide range of instruments are available to measure outcomes in mental health studies. These instruments vary in quality and many are not validated, or are even ad hoc. It is accepted generally that measuring instruments should have the properties of reliability (the extent to which a test effectively measures anything at all) and validity (the extent to which a test measures that which it is supposed to measure) (Rust 1989). Unpublished scales are known to be subject to bias in trials of treatments for schizophrenia (Marshall 2000). Therefore continuous data from rating scales were included only if the measuring instrument had been described in a peer‐reviewed journal. In addition, the following minimum standards for instruments were set: the instrument should either be (a) a self‐report or (b) completed by an independent rater or relative (not the therapist) and (c) the instrument should be a global assessment of an area of functioning.
Assessment of risk of bias in included studies
We assessed risk of bias using the tool described in the Cochrane Collaboration Handbook (Higgins 2009). This tool encourages consideration of how the sequence was generated, how allocation was concealed, the integrity of blinding at outcome, the completeness of outcome data, selective reporting and other biases. We would not have included studies where sequence generation was at high risk of bias or where allocation was clearly not concealed.
The categories are defined below:
YES ‐ low risk of bias NO ‐ high risk of bias UNCLEAR ‐ uncertain risk of bias
If disputes arose as to which category a trial has to be allocated, again, resolution was made by discussion, after working with a third reviewer.
Earlier versions of this review used a different means of categorising risk of bias (see Appendix 3).
Measures of treatment effect
1. Binary data For binary outcomes we calculated the relative risk (RR) and its 95% confidence interval (CI) based on the fixed effects model. Relative Risk is more intuitive (Boissel 1999) than odds ratios and odds ratios tend to be interpreted as RR by clinicians (Deeks 2000). This misinterpretation then leads to an overestimate of the impression of the effect. When the overall results were significant we calculated the number needed to treat (NNT) and the number‐ needed‐ to‐ harm (NNH). Where people were lost to follow up at the end of the study, we assumed that they had had a poor outcome and once they were randomised they were included in the analysis (intention‐to‐treat /ITT analysis).
2. Continuous data For continuous outcomes we estimated a weighted mean difference (WMD) between groups based on a fixed effects model.
Unit of analysis issues
1. Cluster trials Studies increasingly employ cluster randomisation (such as randomisation by clinician or practice) but analysis and pooling of clustered data poses problems. Firstly, authors often fail to account for intra class correlation in clustered studies, leading to a unit‐of‐analysis error (Divine 1992) whereby p values are spuriously low, confidence intervals unduly narrow and statistical significance overestimated. This causes Type I errors (Bland 1997, Gulliford 1999).
Where clustering had not been accounted for in primary studies, we presented the data in a table, with a (*) symbol to indicate the presence of a probable unit of analysis error. In subsequent versions of this review we will seek to contact first authors of studies to obtain intra‐class correlation co‐efficients of their clustered data and to adjust for this using accepted methods (Gulliford 1999). Where clustering has been incorporated into the analysis of primary studies, we will also present these data as if from a non‐cluster randomised study, but adjusted for the clustering effect.
We have sought statistical advice and have been advised that the binary data as presented in a report should be divided by a design effect. This is calculated using the mean number of participants per cluster (m) and the intraclass correlation co‐efficient (ICC) [Design effect=1+(m‐1)*ICC] (Donner 2002). If the ICC is not reported we assumed it to be 0.1 (Ukoumunne 1999). If cluster studies had been appropriately analysed taking into account intra‐class correlation coefficients and relevant data documented in the report, we synthesised these with other studies using the generic inverse variance technique.
2. Cross‐over design A major concern of cross‐over trials is the carry‐over effect. It occurs if an effect (e.g. pharmacological, physiological or psychological) of the treatment in the first phase is carried over to the second phase. As a consequence on entry to the second phase the participants can differ systematically from their initial state despite a wash‐out phase. For the same reason cross‐over trials are not appropriate if the condition of interest is unstable (Elbourne 2002). As both effects are very likely in schizophrenia,¬we will only use¬data¬of the first phase of cross‐over studies.
3. Studies with multiple treatment groups Where a study involved more than two treatment arms, if relevant, the additional treatment arms were presented in comparisons. Where the additional treatment arms were not relevant, these data were not reproduced.
Dealing with missing data
1. Overall loss of credibility At some degree of loss to follow‐up data must lose credibility (Xia 2007). We are forced to make a judgment where this is for the trials likely to be included in this review. Should more than 50% of data be unaccounted for by 8 weeks we did not reproduce these data or use them within analyses.
2 Intention to treat analysis We excluded data from studies where more than 50% of participants in any group were lost to follow up (this did not include the outcome of 'leaving the study early'), as such data were felt to be too prone to bias. In studies with less than 50% dropout rate, people leaving early were considered to have had the negative outcome, except for the event of death. We analysed the impact of including studies with high attrition rates (25‐50%) in a sensitivity analysis. If inclusion of data from this latter group resulted in a substantive change in the estimate of effect, we did not add their data to trials with less attrition, but presented them separately.
Assessment of heterogeneity
1. Clinical heterogeneity We preempted heterogeneity by keeping different treatment groups separate but also tried to think if there were such obvious clinical differences in studies that synthesis be inadvisable.
2. Statistical 2.1 Visual inspection We visually inspected graphs to investigate the possibility of statistical heterogeneity.
2.2 Employing the I‐squared statistic This provided an estimate of the percentage of inconsistency thought to be due to chance. I‐squared estimate greater than or equal to 50% was interpreted as evidence of high levels of heterogeneity (Higgins 2003).
Assessment of reporting biases
Reporting biases arise when the dissemination of research findings is influenced by the nature and direction of results. These are described in section 10.1 of the Cochrane Handbook (Higgins 2009). We are aware that funnel plots may be useful in investigating reporting biases but are of limited power to detect small‐study effects (Egger 1997). We did not use funnel plots for outcomes where there were ten or fewer studies, or where all studies were of similar sizes. Should funnel plots have been possible, we would have sought statistical advice in their interpretation.
Data synthesis
Where possible we used a fixed effects model for analyses. We understand that there is no closed argument for preference for use of fixed or random effects models. The random effects method incorporates an assumption that the different studies are estimating different, yet related, intervention effects. This does seem true to us, however, random effects does put added weight onto the smaller studies ‐ those trials that are most vulnerable to bias.
Subgroup analysis and investigation of heterogeneity
When heterogeneous results were found, we investigated the reasons for this. Where heterogeneous data substantially altered the results and the reasons for the heterogeneity were identified, these studies were not summated in the meta‐analysis, but presented separately and discussed in the text.
Sensitivity analysis
Apart from the investigation of heterogeneity, the effect of including studies with high attrition rates were analysed in sensitivity analyses.
Appendix 3. Assessment of quality
Trials were allocated to three quality categories, as described in the Cochrane Collaboration Handbook (Clarke 2000) by each reviewer working independently. When disputes arose as to which category a trial was allocated to, again, resolution was attempted by discussion. When this was not possible, and further information was necessary, data were not entered into the analyses and the study was allocated to the list of those awaiting assessment. Only trials in Category A or B were included in the review.
Data and analyses
Comparison 1. ALKALOID ‐ DIHYDROGENATED ERGOT ALKALOIDS versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 28 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.45 [0.21, 0.97] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term | 1 | 28 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.5 [0.23, 1.09] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ medium term | 1 | 28 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.01, 7.55] |
| 4 Tardive dyskinesia: 3. Average endpoint scale score (Simpson scale, high=poor) ‐ medium term | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | ‐2.80 [‐12.25, 6.65] |
| 5 Tardive dyskinesia: Average scale change scores (various scales, high=poor) ‐ medium term | 2 | 59 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.31 [‐0.83, 0.20] |
| 5.1 AIMS+RTDS | 1 | 40 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.31 [‐0.93, 0.32] |
| 5.2 ADS | 1 | 19 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.33 [‐1.24, 0.57] |
| 6 Mental state: Deterioration ‐ medium term | 1 | 28 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.5 [0.05, 4.90] |
| 7 Adverse events ‐ medium term | 1 | 28 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.33 [0.75, 7.23] |
| 8 Leaving the study early ‐ medium term | 2 | 48 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.02, 7.32] |
Comparison 2. ALKALOID ‐ L‐STEPHOLIDINE (SPD) versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 57 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.35, 0.82] |
| 2 Mental state: 1. Average endpoint scale score (BPRS, high=poor) ‐ medium term | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐4.5 [‐7.60, ‐1.40] |
| 3 Adverse events: any adverse events ‐ medium term | 1 | 57 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Leaving the study early ‐ medium term | 1 | 57 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
2.3. Analysis.

Comparison 2 ALKALOID ‐ L‐STEPHOLIDINE (SPD) versus PLACEBO, Outcome 3 Adverse events: any adverse events ‐ medium term.
2.4. Analysis.

Comparison 2 ALKALOID ‐ L‐STEPHOLIDINE (SPD) versus PLACEBO, Outcome 4 Leaving the study early ‐ medium term.
Comparison 3. ALKALOID ‐ PAPAVERINE versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | 0.51 [‐1.18, 2.20] |
Comparison 4. AMINO ACID ‐ BRANCHED‐CHAIN AMINO ACID (BCAA) versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term | 1 | 52 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.63, 1.00] |
| 2 Tardive dyskinesia: 1. Not any improvement ‐ short term | 1 | 52 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.36, 1.11] |
| 3 Tardive dyskinesia: 2. Deterioration ‐ short term | 1 | 36 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.29 [0.07, 1.19] |
| 4 Tardive dyskinesia: Average endpoint score (Simpson scale, high=poor) ‐ short term | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | ‐92.9 [‐167.57, ‐18.23] |
| 5 Leaving the study early ‐ short term | 1 | 52 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.84 [0.37, 1.92] |
Comparison 5. AMINO ACID ‐ PHENYLALANINE versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Leaving the study early ‐ short term | 1 | 18 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.45 [0.11, 53.25] |
Comparison 6. ANTIDEPRESSANT (MAO‐B inhibitor) ‐ SELEGILINE versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.37 [0.96, 1.94] |
| 2 Leaving the study early ‐ medium term | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 10.39 [0.62, 173.97] |
Comparison 7. ANTIDEPRESSANT (MAOI) ISOCARBOXAZID versus PROCYCLIDINE.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ long term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.24 [0.08, 0.71] |
| 2 Tardive dyskinesia: 1. Not any improvement ‐ long term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.03, 0.64] |
| 3 Adverse effects ‐ long term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.14, 65.90] |
| 4 Leaving the study early ‐ long term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.14, 65.90] |
Comparison 8. ANTIDEPRESSANT (SSRI) ‐ RITANSERIN vs PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: No clinically important improvement (short term) | 1 | 10 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.70, 1.43] |
| 2 Tardive dyskinesia: Not any improvement (short term) | 1 | 10 | Risk Ratio (IV, Fixed, 95% CI) | 0.28 [0.02, 4.66] |
| 3 Tardive dyskinesia: Deterioration (short term) | 1 | 10 | Risk Ratio (IV, Fixed, 95% CI) | 0.47 [0.02, 9.26] |
| 4 Tardive dyskinesia: Average change score (AIMS, high=poor) (short term) | 1 | 10 | Mean Difference (IV, Fixed, 95% CI) | ‐2.0 [‐5.93, 1.93] |
| 5 General mental state: Deterioration (short term) | 1 | 10 | Risk Ratio (IV, Fixed, 95% CI) | 0.47 [0.02, 9.26] |
| 6 General mental state: Average change score (BPRS, high=poor) (short term) | 1 | 10 | Mean Difference (IV, Fixed, 95% CI) | ‐0.80 [‐3.10, 1.50] |
Comparison 9. ANTIEPILEPTIC ‐ LEVETIRACETAM versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. Average endpoint score (AIMS, high=poor) ‐ medium term | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | ‐2.18 [‐3.65, ‐0.71] |
| 2 Tardive dyskinesia: 1. Average change score (hyperkinesia subscale of the SHRS , high=poor) ‐ medium term | 1 | 69 | Mean Difference (IV, Fixed, 95% CI) | 0.13 [‐0.73, 0.99] |
| 3 Leaving the study early ‐ medium term | 2 | 119 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.46, 2.22] |
| 4 Adverse effects ‐ medium term | 1 | 69 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.51 [0.25, 1.04] |
| 5 Mental state: deterioration ‐ medium term | 1 | 50 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.12, 3.65] |
Comparison 10. ANTIHISTAMINE ‐ CYPROHEPTADINE versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 2. Not any improvement ‐ short term | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.27, 1.08] |
| 2 Tardive dyskinesia: 3. Deterioration ‐ short term | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.01, 7.74] |
| 3 Adverse events ‐ short term | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.04, 2.95] |
| 4 Leaving the study early ‐ short term | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.01, 7.74] |
Comparison 11. ANTIPSYCHOTIC ‐ PROMETHAZINE vs PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: No clinically important improvement (medium term) | 1 | 34 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.24 [0.11, 0.55] |
| 2 Tardive dyskinesia: Not any improvement (medium term) | 1 | 34 | Risk Ratio (IV, Fixed, 95% CI) | 0.06 [0.01, 0.43] |
| 3 Tardive dyskinesia: Average endpoint score (AIMS, high=poor) (medium term) | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐7.10 [‐9.53, ‐4.67] |
| 4 General mental state: Average endpoint score (BPRS, high=poor) (medium term) | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | 0.70 [‐3.77, 5.17] |
| 5 Adverse effects: Any adverse effects (TESS, high=poor) (medium term) | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.53, 0.33] |
| 6 Adverse effects: Parkinsonism ‐ Average endpoint score (RSESE) (medium term) | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐0.5 [‐1.36, 0.36] |
| 7 Global state: Average endpoint score (CGI, high=poor) (medium term) | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐1.00 [‐3.78, ‐2.22] |
Comparison 12. ANXIOLYTIC ‐ BUSPIRONE versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.53 [0.33, 0.84] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.15, 0.75] |
| 3 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term | 1 | 42 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐1.45, 1.45] |
| 4 Leaving the study early ‐ medium term | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
12.4. Analysis.

Comparison 12 ANXIOLYTIC ‐ BUSPIRONE versus PLACEBO, Outcome 4 Leaving the study early ‐ medium term.
Comparison 13. COGNITIVE ENHANCER ‐ PIRACETAM versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. Average endpoint score (ESRS, high=poor) ‐ short term | 1 | 35 | Mean Difference (IV, Fixed, 95% CI) | ‐0.70 [‐4.30, 2.90] |
| 2 Parkinsonism: 1. Average endpoint score (ESRS, high=poor) ‐ short term | 1 | 35 | Mean Difference (IV, Fixed, 95% CI) | 2.5 [‐4.73, 9.73] |
| 3 Leaving the study early ‐ short term | 1 | 40 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.23 [0.03, 1.85] |
| 4 Global state: Average endpoint score (CGI, high=poor) ‐ short term | 1 | 35 | Mean Difference (IV, Fixed, 95% CI) | 0.20 [‐0.35, 0.75] |
Comparison 14. COGNITIVE ENHANCER/STIMULANT ‐ PEMOLINE versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 46 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.29, 0.77] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term | 1 | 46 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.29 [0.13, 0.66] |
| 3 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term | 1 | 46 | Mean Difference (IV, Fixed, 95% CI) | ‐3.90 [‐5.47, ‐2.33] |
| 4 Leaving the study early ‐ medium term | 1 | 46 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
14.4. Analysis.

Comparison 14 COGNITIVE ENHANCER/STIMULANT ‐ PEMOLINE versus PLACEBO, Outcome 4 Leaving the study early ‐ medium term.
Comparison 15. ENZYME INHIBITOR ‐ VMAT2 INHIBITORS versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 92 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.46, 0.86] |
| 2 Tardive dyskinesia: 3. Average change score (AIMS, high=poor) ‐ medium term | 1 | 89 | Mean Difference (IV, Fixed, 95% CI) | ‐2.5 [‐2.00, ‐1.00] |
| 3 Adverse events ‐ medium term | 1 | 100 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.50 [0.92, 2.45] |
| 4 Leaving the study early ‐ medium term | 1 | 102 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.31, 3.25] |
Comparison 16. FATTY ACID ‐ ETHYL EICOSAPENTAENOIC ACID versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 2. No clinically important improvement ‐ medium term | 1 | 75 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.57, 1.18] |
| 2 Mental state: deterioration ‐ medium term | 1 | 75 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.49 [0.05, 5.14] |
| 3 Adverse events: Parkinsonism ‐ Average change in scale score (ESRS, low=better) ‐ medium term | 1 | 75 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [‐1.17, 1.77] |
| 4 Adverse events: Dystonia ‐ Average change in scale score (ESRS, low=better) ‐ medium term | 1 | 75 | Mean Difference (IV, Fixed, 95% CI) | ‐0.35 [‐0.58, ‐0.12] |
| 5 Adverse events: Akathisia ‐ Average change in scale score (ESRS, low=better) ‐ medium term | 1 | 75 | Mean Difference (IV, Fixed, 95% CI) | ‐0.04 [‐0.30, 0.22] |
| 6 Leaving the study early ‐ medium term | 1 | 84 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.27, 1.22] |
Comparison 17. FATTY ACID ‐ GAMMA‐LINOLENIC ACID versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.69, 1.45] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.24, 2.33] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ medium term | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.5 [0.34, 6.70] |
| 4 Tardive dyskinesia: 1. Average change in scale score (AIMS, high=poor) ‐ medium term | 1 | 16 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐3.10, 2.70] |
| 5 Mental state: 2. Average change in scale score (BPRS, high=poor) ‐ medium term | 1 | 10 | Mean Difference (IV, Fixed, 95% CI) | ‐6.0 [‐15.99, 3.99] |
| 6 Leaving the study early ‐ medium term | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
17.6. Analysis.

Comparison 17 FATTY ACID ‐ GAMMA‐LINOLENIC ACID versus PLACEBO, Outcome 6 Leaving the study early ‐ medium term.
Comparison 18. HERB ‐ GINKGO BILOBA versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 157 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.81, 0.96] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term | 1 | 157 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.51 [0.41, 0.65] |
| 3 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term | 1 | 157 | Mean Difference (IV, Fixed, 95% CI) | ‐2.06 [‐2.94, ‐1.18] |
| 4 Leaving the study early ‐ medium term | 1 | 157 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.25 [0.03, 2.22] |
| 5 Mental state: deterioration ‐ medium term | 1 | 157 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.01, 8.16] |
| 6 Mental state: 1. Average endpoint scale score (PANSS total, high=poor) ‐ medium term | 1 | 157 | Mean Difference (IV, Fixed, 95% CI) | ‐3.30 [‐6.51, ‐0.09] |
| 7 Cognitive function: CPT‐37 ‐ proportion correct responses (high=better) ‐ medium term | 1 | 119 | Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.10, 0.06] |
Comparison 19. HORMONE ‐ OESTROGEN versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term | 1 | 12 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.18 [0.76, 1.83] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ short term | 1 | 12 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.05, 2.37] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ short term | 1 | 10 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.2 [0.01, 3.35] |
| 4 Tardive dyskinesia: 4. Average scale score (AIMS, high=poor) ‐ short term | 1 | 10 | Mean Difference (IV, Fixed, 95% CI) | ‐1.2 [‐4.18, 1.78] |
| 5 Adverse effects ‐ short term | 1 | 12 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.02, 6.86] |
| 6 Leaving the study early ‐ short term | 1 | 12 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.08, 12.56] |
Comparison 20. HORMONE ‐ INSULIN versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.52 [0.29, 0.96] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.06 [0.00, 0.90] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ medium term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.01, 2.45] |
| 4 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐6.20 [‐10.53, ‐1.87] |
| 5 Leaving the study early ‐ medium term | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
20.5. Analysis.

Comparison 20 HORMONE ‐ INSULIN versus PLACEBO, Outcome 5 Leaving the study early ‐ medium term.
Comparison 21. HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement | 2 | 32 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.71, 1.12] |
| 1.1 Short term | 1 | 19 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.83, 1.21] |
| 1.2 Medium term | 1 | 13 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.44, 1.23] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ short term | 1 | 19 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.47, 2.60] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ short term | 1 | 19 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.22 [0.01, 4.05] |
| 4 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ medium term | 1 | 13 | Mean Difference (IV, Fixed, 95% CI) | ‐2.38 [‐6.58, 1.82] |
| 5 Adverse effects | 3 | 54 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.1 Short term | 1 | 19 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.2 Medium term | 2 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Leaving the study early | 3 | 54 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.1 Short term | 1 | 19 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 Medium term | 2 | 35 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Cognitive function: Average scale score ‐ medium term | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 WAIS | 1 | 76 | Mean Difference (IV, Fixed, 95% CI) | 15.83 [4.61, 27.05] |
| 7.2 WMS | 1 | 76 | Mean Difference (IV, Fixed, 95% CI) | 3.77 [‐8.21, 15.75] |
| 8 Mental state: deterioration ‐ medium term | 1 | 13 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
21.5. Analysis.

Comparison 21 HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT, Outcome 5 Adverse effects.
21.6. Analysis.

Comparison 21 HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT, Outcome 6 Leaving the study early.
21.8. Analysis.

Comparison 21 HORMONE ‐ MELATONIN versus PLACEBO OR NO TREATMENT, Outcome 8 Mental state: deterioration ‐ medium term.
Comparison 22. MOOD STABILISER ‐ LITHIUM versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ short term | 1 | 11 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.59 [0.79, 3.23] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ short term | 1 | 11 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.29 [0.25, 72.90] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ short term | 1 | 11 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.29 [0.25, 72.90] |
| 4 Tardive dyskinesia: 3. Average scale score (AIMS, high=poor) ‐ short term | 1 | 11 | Mean Difference (IV, Fixed, 95% CI) | 0.63 [‐5.23, 6.49] |
| 5 Adverse events ‐ short term | 1 | 11 | Risk Ratio (M‐H, Fixed, 95% CI) | 6.0 [0.38, 94.35] |
| 6 Leaving the study early ‐ short term | 1 | 11 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.57 [0.13, 52.12] |
Comparison 23. POLYPEPTIDE ‐ CERULETIDE versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. Not any improvement | 2 | 132 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.65, 1.07] |
| 1.1 Short term | 1 | 47 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.73 [0.50, 1.06] |
| 1.2 Medium term | 1 | 85 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.64, 1.27] |
| 2 Tardive dyskinesia: 2. Deterioration | 2 | 103 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.14, 6.80] |
| 2.1 Short term | 1 | 37 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.85 [0.12, 65.74] |
| 2.2 Medium term | 1 | 66 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.01, 7.90] |
| 3 Adverse effects | 2 | 122 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.74, 2.36] |
| 3.1 Short term | 1 | 37 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.79 [0.47, 30.77] |
| 3.2 Medium term | 1 | 85 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.13 [0.61, 2.07] |
| 4 Leaving the study early ‐ medium term | 1 | 85 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.09 [0.49, 2.40] |
Comparison 24. HYPNOSIS OR RELAXATION versus TREATMENT AS USUAL.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Tardive dyskinesia: 1. No clinically important improvement ‐ medium term | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.45 [0.21, 0.94] |
| 2 Tardive dyskinesia: 2. Not any improvement ‐ medium term | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.18 [0.01, 3.81] |
| 3 Tardive dyskinesia: 3. Deterioration ‐ medium term | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.18 [0.01, 3.81] |
| 4 Leaving the study early ‐ medium term | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.1 Short term | 1 | 15 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
24.4. Analysis.

Comparison 24 HYPNOSIS OR RELAXATION versus TREATMENT AS USUAL, Outcome 4 Leaving the study early ‐ medium term.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bucci 1971.
| Methods | Allocation: random, further details not reported. Blindness: not reported. Duration: 40 weeks. Design: parallel. Setting: outpatients, USA (probably). |
|
| Participants | Diagnosis: chronic schizophrenia treated with phenothiazine for several years and demonstrating obvious dyskinetic manifestations. N = 20 Sex: 16 female and 4 male Age: range 45‐62 years History: at least two years of TD. |
|
| Interventions | 1. Procyclidine (Anticholinergic), 5 mg twice a day + chlorpromazine, 100 mg three times a day N = 10.
2. Isocarboxazid (MAOI), 10 mg twice a day + chlorpromazine, 100 mg three times a day N = 10. Continuous phenothiazine‐antiparkisonian treatment for at least 2 years. . Other concomitant medication was not reported. |
|
| Outcomes | TD symptoms (clinical evaluation, scale not reported) Leaving the study early Adverse events Unable to use ‐ Mental state (data not reported for both groups) |
|
| Notes | Sponsorship source: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “The patients were divided at random into groups of 10 each”, no further details reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding of participants and personnel not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Blinding of outcome assessment not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | “One male patient on chlorpromazine and isocarboxazid was discontinued after 6 weeks as he became increasingly tense, apprehensive and sleepless” |
| Selective reporting (reporting bias) | High risk | Adverse effects reported only as those related to treatment. Mental state data not reported for group 2. Unclear if all outcomes have been reported, a protocol is not available for verification. |
| Other bias | Unclear risk | Insufficient information to make a judgement |
Cai 1988.
| Methods | Allocation: not reported.
Blinding: double‐blind.
Duration: 8 weeks. Design: parallel Setting: not reported. |
|
| Participants | Diagnosis: antipsychotic‐induced TD; N = 57 Sex: 33 male and 24 female 24 Age: mean 39.5 (SD 10.3) years old, range 28‐59 History: Duration of TD on average 2.4 (SD 1.8) years. Patients assigned to the treatment group were stable to AP dose from 0.7 to 27 years, whereas patients assigned to the control group were stable to AP dose from 1 to 10 years before start of study. |
|
| Interventions | 1. L‐stepholidine (SPD) Group: Management: L‐stepholidine was prescribed two tablets each time, three times per day for 8 weeks. N = 42 2. Placebo Group: The placebo with similar appearance to L‐stepholidine was prescribed two tablets each time, three times per day for 8 weeks. N = 15 All participants received stable AP and concomitant anticholinergic drug. Other concomitant medication is not reported. |
|
| Outcomes | Clinical improvement on TD symptoms: no definition.
Clinical improvement on psychosis symptoms: no definition.
Mental state: BPRS
Adverse event: any adverse events ‐‐Unable to use TESS, (the author did not report the data) Blood routine examination, urine routine test and liver function test, electrocardiography. (the author only stated results of these tests were normal but did not report the data) |
|
| Notes | Twenty cases from the SPD group received blood routine examination, urine routine test and liver function test; five cases received electrocardiography. Ten cases in each group received BPRS and TESS measurements. We attempted to contact the study author for information on randomisation, but were informed he had retired. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "...randomized, parallel‐group..." no further details. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "double blind" "The placebo with similar appearance", Blinding of participants and key study personnel ensured. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "double blind" "The placebo with similar appearance", Blinding of participants and key study personnel ensured. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants completed the trial. |
| Selective reporting (reporting bias) | High risk | The author did not report the outcome: TESS, Blood routine examination, urine routine test and liver function test, electrocardiography |
| Other bias | Unclear risk | No further details reported |
Castro 2011.
| Methods | Allocation: randomised. Blindness: "double blind". Duration: 12 weeks. Design: parallel. Setting: inpatients and outpatients, Venezuela | |
| Participants | Diagnosis: Psychiatric patients meeting DSM‐IV‐TR diagnostic criteria for the diagnosis of antipsychotic‐induced TD. N = 13. Sex: 4 female and 9 male Age: mean (SD) 59.9 (2.7) years; range 46‐75 years. History: Duration of TD not reported. Most of the patients have been receiving the same antipsychotic treatment for at least 3 years up to 10 years. Antipsychotics received were levomepromazine (9 patients), haloperidol (4), clozapine (2), aripiprazole (2), olanzapine (1), quetiapine (1) and risperidone (1). |
|
| Interventions | 1. Melatonin: 20 mg/day. N = 7. Duration: 12 weeks. 2. Placebo: N = 6. Duration: 12 weeks. All individuals who participated faithfully complied with antipsychotic treatment and maintained it throughout the study. Other concomitant medication: The treatment with anticholinergics was maintained for ethical reasons. In each of the groups two patients received biperidine. Other treatments applied were, in the melatonin group, valproic acid (1 patient), carbamazepine (1 patient), alprazolam (1 patient), indapamide (1 patient); in the placebo group: carbamazepine (2 patients), chlorimipramine (2 patients) and lithium carbonate (1 patient). During the study there were no dosage adjustments. |
|
| Outcomes | Tardive dyskinesia: Brief Psychiatric Rating Scale (BPRS) Tardive dyskinesia: symptoms: AIMS Adverse events: other observed effects. Leaving the study early |
|
| Notes | This study was supported by the Instituto Venezolano de Investigaciones Científicas (IVIC), Venezuela | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "The individuals selected were divided randomly into two groups", no further details. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "A group of 6 patients received placebo capsules, identical in appearance". |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double blind". Blinding of outcome assessors not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants completed the trial. |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all pre‐defined outcomes were reported. A protocol is not available for verification. |
| Other bias | Low risk | The study seems to be free of other sources of bias. |
Emsley 2006.
| Methods | Allocation: randomised. Blindness: double‐blind. Duration: 12 weeks. Design: parallel. Setting: inpatients and outpatients, South Africa. | |
| Participants | Diagnosis: schizophrenia, schizoaffective disorder with TD (DSM‐IV). N = 84. Sex: 51 male and 26 female Age: mean 42 years. History: Duration of TD more than 5 years. Patients were stabilised for at least 6 months prior to trial. | |
| Interventions | 1. Ethyl‐eicosapentaenoic acid (omega‐3 fatty acid eicosapentaenoic acid derivative): dose 2 g/day + antipsychotics. N = 42.
2. Placebo + antipsychotics. N = 42. Patients who were stabilised on other psychotropic medications (anxiolytic, hypnotic, antidepressant, mood stabilising) before entry to the trial were allowed to continue on these medications; anticholinergic medication for treatment‐emergent extrapyramidal symptoms (EPS); anxiolytic or hypnotic medication for treatment emergent insomnia or acute anxiety; any medication for physical conditions that was taken prior to the commencement of the trial could be continued; medication for other conditions that arose during the course of the trial, at the investigator's discretion. Other omega‐3 fatty acid preparations, additional antipsychotics or antidepressants were not permitted. |
|
| Outcomes | Extrapyramidal symptoms: ESRS Mental state deterioration Leaving the study early. Unable to use ‐ Mental state: PANSS (no usable data). Global state: CGI (no usable data) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "...randomized, parallel‐group..." no further details. |
| Allocation concealment (selection bias) | Unclear risk | No details. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "...double‐blind..." "Subjects were randomly assigned to receive either an encapsulated ethyl‐EPA supplement 2 g/day... or an identical capsule containing placebo (medicinal liquid paraffin BP 2 g/day)... Trial supplies were packed by an independent contract clinical trials supplies company (DHP), who prepared the placebo and active packs for the entire trial and assigned the randomization numbers to the packs. The randomization code was broken after completion of the trial". |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessors for efficacy outcomes (TD symptoms and Mental State) not reported. Adverse events blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Overall drop‐out rate: 35%. 7/84 (8%) participants dropped out before the first post‐randomisation visit. 7/84 (8%) participants were not included in the analysis. "Data from... 77 patients were included in the final analysis". "The number of subjects who discontinued medication prematurely in the ethyl‐EPA group was 8 (19%) (consent withdrawal n=4; non‐compliance n=3; protocol violation n=1), and in the placebo group 14 (33%) (consent withdrawal n=9; non‐compliance n=3; adverse events n=2 (congestive cardiac failure; nose‐bleed) (Chisquare=2.2, df=1, p=0.1)." It seems that these participants were included in the analysis. |
| Selective reporting (reporting bias) | High risk | Data for some outcomes stated in the protocol have not been reported (e.g. remission, CGI severity) |
| Other bias | Unclear risk | "The demographic characteristics and baseline PANSS scores in the two treatment groups were similar, but baseline ESRS dystonia subscale and TD CGI scores differed significantly". Unclear if the differences (confounding variables) may be biased |
Gardos 1979.
| Methods | Allocation: "randomised" unclear.
Blindness: single‐blind.
Duration: 12 weeks. (6 weeks then crossed over to another 6 weeks. Washout period unknown)
Design: cross‐over. Setting: inpatients, USA |
|
| Participants | Diagnosis: psychogeriatric (23) and schizophrenic (18) patients with obvious TD.
N = 41
Sex: 28 female and 13 male.
Age: mean 64 years, range 32‐84 years. History: Duration of TD not reported. |
|
| Interventions | 1. Papaverine: dose 150 mg/day twice a day for the first week and 300 mg twice a day for the subsequent 5 weeks. N = 21.
2. No treatment: 6 weeks (followed by 6 weeks of papaverine). N = 20. Concomitant medication: antipsychotics, antidepressants, anxiolytics, or no medication. No changes were made in psychotropic drug administration during the study. |
|
| Outcomes | TD symptoms: AIMS (only reported for Boston sample) Unable to use (not reported for first treatment phase before cross‐over) Leaving the study early Adverse effects: Parkinsonism |
|
| Notes | Sponsorship source: Supported in part by a grant from the Drug Abuse and Mental Health Administration of HEW. * Authors state that the two samples differed greatly in the incidence and severity of tardive dyskinesia prior to the study. The differences were to a large extent due to the differences in the two populations: Boston patients were older with longer duration of disability and hospitalizations and showed more extensive dyskinesia. In view of the major differences in the populations, data from the two groups were analysed separately. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "random order", further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "single‐blind". As the participants were randomised to receive papaverine or not, neither the participants nor the study personnel could have been blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "A single blind design was used with blind raters and a 6‐weeks no drug control condition." |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Although not clearly reported, it seems that 1/23 participants in the Boston sample and 0/18 participants in the Kentucky sample were withdrawn from the study. |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all predefined outcomes have been reported. Also, the reason for not assessing TD symptoms using AIMS in the Kentucky sample is not reported. |
| Other bias | Unclear risk | The two samples were very different in their baseline characteristics. However, this was controlled by reporting data separately. Unclear if there might have been other confounding variables to affect bias. |
Glazer 1985.
| Methods | Allocation: randomised. Blindness: double‐blind. Duration: 3 weeks. Design: parallel. Setting: Outpatients, Connecticut Mental Health Center, USA | |
| Participants | Diagnosis: psychiatric disorder (no operational criteria) and Schooler&. Kane's criteria for TD N = 12. Sex: 12 females. Age: 50‐65 years, mean 57 years. History: Duration of TD on average 32.3 months (range 6‐60 months). Patients maintained their antipsychotic medication | |
| Interventions | 1. Oestrogen: 1.25 mg/day. N = 6.*
2. Placebo. N = 6. Nine of the 10 patients were on medications other than antipsychotics; 7 were on psychiatric medication. Further details not provided. |
|
| Outcomes | Tardive dyskinesia: AIMS improved/not improved, deterioration in symptoms, AIMS scale scores .
Adverse events: other observed effects.
Leaving the study early. Unable to use ‐ Adverse events: Parkinson scores (no data). Mental state: BPRS (no data). |
|
| Notes | Sponsorship source: Supported by HD 13587 and Ayerst Pharmaceuticals | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized". Details not reported |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind". Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | TD related and mental state outcomes: "double‐blind". "All ratings were administered without knowledge of the study status of the individual subject. Patients were videotaped during the research nurse's rating on visits 1 and 4. These tapes were subsequently rated by a senior psychiatric resident who administered the AIMS and counted the frequency of abnormal movements of the most severely affected anatomical region as determined by the study psychiatrist during the baseline assessment". Details of blinding not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "Twelve patients were admitted to the study, and 10 completed the 3‐week trial. One patient in the placebo group was hospitalized for congestive heart failure. One patient in the oestrogen group required psychiatric hospitalization after taking an overdose of medications; she had been depressed at the onset of the trial and became worse at the third visit during a period of severe marital discord." Balance between groups, reasons reported. |
| Selective reporting (reporting bias) | High risk | TD symptoms data not reported as mean (SD) but rather as mean only (table 1). Data for Mental state (BPRS) not reported. Adverse effects reported only as adverse events leading to study discontinuation. |
| Other bias | High risk | "Although our study involved randomization and double‐blind drug procedures to prevent bias, the small sample size resulted in some imbalances between groups at the first visit. Thus, the conjugated oestrogen group had less exposure to antipsychotic medication and a shorter duration of TD. They also had higher mean baseline AIMS scores than did the placebo group, thereby leaving more possibility for improvement in scores. The small sample size does not allow statistical analysis to adjust for these differences. Although we found a positive but non‐significant association between duration of TD and decrease in AIMS score between visits 1 and 4, we doubt that TD duration is a confounding factor, since the direction of this association is the opposite of what we would have expected". |
Glover 1980.
| Methods | Allocation: randomised. Blindness: not mentioned. Duration: 8 sessions. Design: parallel. Setting: Outpatients, USA | |
| Participants | Diagnosis: Diagnosis of chronic schizophrenia; diagnoses of either acute extra pyramidal symptoms, TD, and/or pseudoparkinsonism. N = 15. Sex: 12 females and 3 males. Age: mean 34.9 years. History: Duration of TD not reported. Not reported whether patients were stabilised prior to study. | |
| Interventions | 1. Hypnosis: 8 sessions. N = 5.
2. Relaxation. 8 sessions. N = 5. 3. Treatment as usual (control group). 8 sessions. N = 5. Psychotropic medication continued. |
|
| Outcomes | Leaving the study early: number of dropouts | |
| Notes | Sponsorship source: Sponsorship source not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | "There was a total of fifteen subjects randomly selected". "I made the assumption that the order in which patients approached the clinic was not related in any way to their susceptibility or effectiveness of subsequent treatments. Based on these assumptions I assigned the first patient who came into the study to group 1, the second patient '"as assigned to group 2, and the third patient was assigned to Group 3; after every three assignments I started the assignments with group 1 again and continued until each treatment modality had a total of five" |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As participants in group 1 received hypnosis, those in group 2 received relaxation training, and those in group 3, TAU without any other treatment, blinding could not be achieved |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessors not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There were no refusals, or dropouts among the referrals. |
| Selective reporting (reporting bias) | Low risk | It seems that all outcomes have been reported. However data are not usable. |
| Other bias | Unclear risk | "(Tables 1, 2 and 3). Using a non‐parametric test for testing differences on demographic data between treatment groups yielded no significant difference among these groups (Table 7). With respect to the regimen of medication for each patient (Tables 4, 5, 6), there was close similarity in each group. The majority of patients in each group received either haloperidol or trifluoperazine; therefore any alternative treatment differences could not be influenced by medication. However, due to the formula which is used by physicians in dispensing medication, it was not possible to use a statistical procedure for testing the equality of the three groups in this study. The sample size, sex and marital status variables was so small to preclude a statistical test on these two variables." |
Goff 1993.
| Methods | Allocation: "randomly assigned" unclear.
Blindness: double, (identical capsules).
Duration: 6 weeks.
Design: parallel. Setting: outpatients, USA Raters: "AIMS were videotaped and scored by a second rater unaware of the temporal sequence of examinations" |
|
| Participants | Diagnosis: antipsychotic‐induced TD according to DSM‐III‐R, Schooler and Kane criteria with a score of at least 3 (moderate) on a single item or 2 (mild) on at least two items of the AIMS and have a history of at least 6 months of exposure to a antipsychotic prior to onset of dyskinetic movements.
N = 33
Sex: 13 female and 20 male.
Age: mean 48.8 (SD 9.8) years Duration TD: not reported. |
|
| Interventions | 1. Selengiline (L‐Deprenyl): dose 5 mg (one capsule daily for the first week, then one twice daily thereafter) for 6 weeks. N = 17.
2. Placebo for 6 weeks. N = 16 Doses of antipsychotics and anticholinergic agents were stable for at least 4 months before the trial. Patients receiving depot antipsychotic were included only if injections were administered on a biweekly schedule. |
|
| Outcomes | TD symptoms: not significant clinically improved (defined as an improvement of more than 50%) Leaving the study early Unable to use: Adverse effects: severity of parkinsonian symptoms and akathisia using SAS, Mental state: BPRS for positive, negative and depressive symptoms, Global assessment scale, Average change in severity of TD using AIMS |
|
| Notes | Sponsorship source: Supported by PHS grant | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomly assigned", further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "identical capsules containing either selegiline 5 mg or placebo." "double‐blind" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Examinations with the AIMS were videotaped and scored by a second rater unaware of the temporal sequence of examinations." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | "Five subjects, all receiving selegiline, dropped out prior to the completion of week 1 and so were not included in analysis of outcome." 29% drop out in the active medications group, not ITT. |
| Selective reporting (reporting bias) | High risk | Data not reported for mental state (BPRS total and sub scales), severity of parkinsonian symptoms (SAS) |
| Other bias | Low risk | The study seems to be free of other sources of bias. |
Hajioff 1983.
| Methods | Allocation: "randomly assigned", no further details.
Blindness: double‐blind
Duration: 14 weeks (2 week run‐in, 6 week treatment, 6 week no‐treatment follow‐up)
Design: parallel Setting: Inpatients, UK (probably) |
|
| Participants | Diagnosis: schizophrenia (9), dementia (3 with paranoid features, 3 without), depression (3), pre‐senile dementia (1). and epileptic psychosis (1).
N = 20.
Sex: 10 female and 5 male.
Age: mean 65.4 (males)‐79.5 (females) years, range 60‐92 years History: Duration of TD not reported. Seventeen patients were each receiving one antipsychotic drug, thioridazine (5), promazine (5), chlorpromazine (3), haloperidol (2), trifluoperazine (1) and chlomethiazole (1). Their dosage regimen had remained constant for at least 6 months. Two patients with chronic schizophrenia and one with depression were not taking any antipsychotic drugs for the same period. |
|
| Interventions | 1. 4.5 mg co‐dergocrine mesylate once daily for 6 weeks. N = 10.
2. Placebo once daily for 6 weeks. N = 10. Only two patients had never received anti‐Parkinsonian drugs, the remainder receiving therapy for various periods of time (3 months to 8 years). Two other patients were receiving anti‐Parkinsonian drugs at a constant dose during the study period. Details of medications, not reported. |
|
| Outcomes | The abbreviated dyskinesia scale of the Rockland Research Institute (ADS). Death. Leaving study early. |
|
| Notes | Sponsorship source not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly assigned", no further details. |
| Allocation concealment (selection bias) | Unclear risk | Details on allocation concealment were not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double blind", no further details. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Details on blinding of outcome assessment were not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | One participant from the placebo group died in the second week of the study (run‐in phase) and was not part of the final analyses. |
| Selective reporting (reporting bias) | Unclear risk | No details. |
| Other bias | Unclear risk | No details. |
Kojima 1992.
| Methods | Allocation: randomised, not described. Blindness: double, not described. Duration: 8 weeks. Design: parallel. Setting: Inpatients and outpatients, Japan | |
| Participants | Diagnosis: schizophrenia (DSM‐III‐R). N = 85. Sex: 34 female and 32 male. Age: 31‐75 years, mean 55.2 years. History: antipsychotic‐induced TD (mean duration 5 years). | |
| Interventions | 1. Ceruletine IM: dose 0.8 mcg/kg/week for 3 weeks. N = 43.
2. Placebo. N = 42. Previous background medication and treatment held constant throughout trial. |
|
| Outcomes | Tardive dyskinesia: AIMS improved/not improved, deterioration in symptoms. Adverse events: other observed effects. Leaving the study early. | |
| Notes | Data presented for 33 matched pairs only. Sponsorship source: Sponsorship source not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "...patients were randomized into matched pairs on the basis of age and sex, and of the severity and duration of TD symptoms." Details not reported |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐ blind", further details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double‐ blind", further details not reported. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | "Of the 85 patients who entered the study, eight were excluded from data analysis because of protocol violations (e.g., an insufficient severity of TD symptoms during the baseline period or missing observations)." One patient was discontinued due to adverse event (table 2). Actually, 19 participants were excluded from the analysis (66/85 participants, 33 in each group, were analysed. "Analyses were performed on the 33 pairs (i.e., 33 patients in the ceruletide group vs. 33 patients in the placebo group). p. 131, 1st paragraph. |
| Selective reporting (reporting bias) | High risk | Judgement Comment: "Of the 85 patients who entered the study, eight were excluded from data analysis because of protocol violations (e.g., an insufficient severity of TD symptoms during the baseline period or missing observations)." "Analyses were performed on the 33 pairs (i.e. 33 patients in the ceruletine group versus 33 patients in the placebo group)" |
| Other bias | Unclear risk | Insufficient information. Baseline information reported for participants included in the analyses but not for the participants who were not entered to the analysis due to "protocol violations" |
Koshino 1979.
| Methods | Allocation: "randomly allocated", Details not reported. Blindness: "double‐blind," Details not reported Duration: 4 weeks Design: Parallel Setting: Inpatients in 4 psychiatric hospitals in Japan |
|
| Participants | Diagnosis: Schizophrenia (n = 35), others (n = 7), drug‐induced TD N = 42 Sex: Male 13, Female 29 Age: 56.1 (SD: 8.69) History: Duration of TD not reported. |
|
| Interventions | 1. Cyproheptadine (12 mg/day to 24 mg/day Flexible, 4 week). N = 21
2. Placebo. N = 21 Concomitant medication not reported. |
|
| Outcomes | Tardive dyskinesia: Assessment scale developed by the researchers Leaving the study early. Adverse effects |
|
| Notes | Sponsorship source: Cyproheptadine and placebo tablets supplied by Merck‐Banyu Co.Ltd Assessed and data extracted by Yusuke Ogawa. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly allocated", Details not reported. |
| Allocation concealment (selection bias) | Low risk | Randomization was conducted by the third person (outside of the research group). Allocation codes were stored until the end of the study |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind," Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double‐blind," Details not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Forty‐two patients were admitted to the study, and 41 completed the 4‐week trial. One patient in the placebo group dropped out due to side effects. Reason reported. |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all pre‐defined outcomes were reported. A protocol is not available. |
| Other bias | Unclear risk | Insufficient information to make a judgement. |
Koshino 1983.
| Methods | Allocation: "randomly allocated", Details not reported. Blindness: "double‐blind," Details not reported Duration: 6 weeks Design: Parallel Setting: Inpatients in a psychiatric hospital in Japan |
|
| Participants | Diagnosis: antipsychotic‐induced TD, Schizophrenia N = 28 Sex: Male 16, Female 12 Age: 59.3 (SD: 8.29) History: Duration of TD not reported. |
|
| Interventions | 1. Dihydrogenated Ergot Alkaloids (6 mg/day, 6 week). N = 14
2. Placebo. N = 14 Concomitant medication not reported. |
|
| Outcomes | Tardive dyskinesia: Not clinically improved Tardive dyskinesia: Not any improved Tardive dyskinesia: Simpson scale Tardive dyskinesia: Deterioration Mental state: Not any change in general mental state Adverse effects general Leaving the study general Leaving the study Due to side effect |
|
| Notes | Sponsorship source: Dihydrogenated Ergot Alkaloids and placebo tablets supplied by Sandoz Assessed and data extracted by Yusuke Ogawa. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly allocated", Details not reported. |
| Allocation concealment (selection bias) | Low risk | Randomization was conducted by the third person (outside of the research group). Allocation codes were stored until the end of the study |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind," Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double‐blind," Details not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Twenty‐eight patients were admitted to the study, and all of them completed the 4‐week trial. |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all pre‐defined outcomes were reported. A protocol is not available. |
| Other bias | Unclear risk | Insufficient information to make a judgement. |
Libov 2007.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 9 weeks. Design: cross‐over, 4 weeks treatment one week wash out. Setting: Inpatients, Be'er Sheva Mental Health Center, Israel. | |
| Participants | Diagnosis: schizophrenia, schizoaffective disorder (DSM‐IV). N = 40. Sex: 27 male, 23 female. Age: 26‐69 years; mean 44.9 (SD 12.4) years. History: Duration of TD at least 1 year. Patients were stabilised at least one month prior to entry. Antipsychotic medication was not altered. | |
| Interventions | 1. Piracetam: dose 4800 mg/day + conventional antipsychotics. N = 21
2. Placebo. N = 19 Twenty‐four patients received various mood stabilisers (lithium, carbamazepine, or valproate) in combination with antipsychotic agents |
|
| Outcomes | Tardive dyskinesia: Extrapyramidal System Rating Scale (ESRS). TD symptoms: not any improvement Adverse events: other observed effects. Leaving the study early. |
|
| Notes | Sponsorship source: Supported by a Clinical Trials Grant from the Stanley Medical Research Institute, Bethesda, Md. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "subjects were randomized to receive either piracetam or placebo." Details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Both patients and raters were blinded to group allocation." further details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "raters were blinded to group allocation" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | "Of the 40 randomly assigned patients, 5 subjects (4 taking placebo and 1 taking piracetam) did not comply with the treatment regimen following the first 2 weeks of the study and were not included in the statistical analysis. Therefore, 35 patients completed phase I, and, of these, 4 patients (2 receiving placebo and 2 receiving piracetam) did not agree to continue to phase II, resulting in 31 patients completing both phases of the crossover protocol. The main reason for patient dropout was the large size and number of the capsules that they were required to take." In the first phase there was a 12.5% dropout while in the completed cross‐over trial 22.5% dropout. Patients who dropped out were not included in the analysis |
| Selective reporting (reporting bias) | Low risk | Outcomes defined in the Protocol have been reported. NCT00190008 |
| Other bias | Low risk | The study seems to be free of other sources of bias. |
Mackay 1980.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 5 weeks treatment per arm separated by 6 week washout. Design: cross‐over. Setting: Chronic inpatients, UK | |
| Participants | Diagnosis: schizophrenia (7), bipolar affective illness (3), depressive psychosis (1) (no diagnostic criteria). N = 11. Sex: not described. Age: 56‐70 years, median 59 years. History: antipsychotic‐induced TD for at least one year and not pre‐dating antipsychotic treatment; treatment with antipsychotics for a period of at least 2 years. | |
| Interventions | 1. Lithium: dose not specified. N = 6.
2. Placebo. N = 5. Previous background medication and treatment continued throughout trial, patients were receiving a variety of antipsychotic and anxiolytic drugs: 4 patients received no antipsychotic medication. |
|
| Outcomes | Tardive dyskinesia: improved/not improved, deterioration in symptoms, Rockland TD scale score.
Adverse events: other observed effects ‐ parkinsonian and drowsiness.
Leaving the study early. Unable to use ‐ Tardive dyskinesia: SAS (no data). Mental state: BPRS (no data). Behavioiur: NOSIE (no data). |
|
| Notes | Sponsorship source: Sponsorship source not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "A random Li (Camcolit QDS)/placebo cross‐over design", further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Raters, nurses and patients were blind to treatment. Two non‐blind 'coordinators'... adjusted the oral dose of Li carbonate to aim at a serum concentration between 0.8 and 1.3 mM. Adjustment of U dosage was mirrored by a similar change for the 'placebo twin'" "At completion of the study, the patients, a psychiatrist and nursing staff involved in ratings were asked to guess the nature of the treatment block. There was a choice of 3 alternative answers: inactive tablets, active drug or uncertain. "Analysis of the guesses made by staff and patients as to the sequence of treatments showed that correct guesses occurred randomly. Thus, despite inevitable cues from side‐effects, it seemed that the double‐blind nature of the study was preserved". |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Raters, nurses and patients were blind to treatment." "At completion of the study, the patients, a psychiatrist and nursing staff involved in ratings were asked to guess the nature of the treatment block. There was a choice of 3 alternative answers: inactive tablets, active drug or uncertain. "Analysis of the guesses made by staff and patients as to the sequence of treatments showed that correct guesses occurred randomly. Thus, despite inevitable cues from side‐effects, it seemed that the double‐blind nature of the study was preserved". |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1/11 participants (in the lithium first group) did not complete the study. Reason not reported. |
| Selective reporting (reporting bias) | High risk | Mental State and behaviour outcome data not reported. TD symptoms scale scores data not reported. |
| Other bias | Unclear risk | "Patients were divided, as far as possible into matched for age, sex, severity of TD, duration of psychiatric illness and duration of neuroleptic treatment. Matching for sex was exact and the maximum discrepancies between members for any pair for other variables were as follows: age ± 4 years, total Rockland TD scores ±17, duration of illness ±11years, duration of neuroleptic treatment ±5 years" Unclear of a discrepancy of ±17 on the total Rockland TD scores is significant. |
Matsunaga 1988.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 4 weeks. Design: parallel group. Setting: inpatient, Japan | |
| Participants | Diagnosis: chronic psychotic inpatients with TD N = 47 Sex: 22 female and 15 male Age: 59 (SD 8.8) years History: antipsychotic‐induced TD from 7 months to 20 years. Patients stabilised at least 3 weeks prior to entry. | |
| Interventions | 1. Ceruletide: 0.8 mcg/kg/week. N = 19.
2. Placebo. N = 18. Background medication and treatment continued throughout trial. |
|
| Outcomes | Tardive dyskinesia: AIMS improved/ not improved, deterioration in symptom. Adverse events: other observed effects. Leaving study early. | |
| Notes | Sponsorship source: Shionogi & Co., Ltd., Japan supplied Ceruletide | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "The patients were assigned at random". Details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind" Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double blind" Details not reported. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | "Of the original 47 patients, one patient dropped out of the study because of fever of unknown origin. Nine patients in whom assessment of TD symptoms was unreliable either due to the erratic variation in symptomatology or to the emotional or situational effect unrelated to the drug treatment, were excluded from the final analyses before opening of the key code. Thus, 37 patients were available for analysis, 19 receiving Ceruletide and 18 receiving placebo". Data not reported for 21% of the participants. |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to make a judgement. A protocol is not available to verify all outcomes defined prior to study. |
| Other bias | Low risk | The study seems to be free of other sources of bias. |
Meco 1989.
| Methods | Allocation: randomised.
Blindness: double‐blind.
Design: cross‐over. Setting: inpatients, Italy. Duration: 30 days (then crossed over to another 30 days). |
|
| Participants | Diagnosis: Chronic schizophrenia (DSM‐III‐R criteria) and suffering from antipsychotic‐induced TD previously untreated with other drugs. N = 10. Age: mean 57 years, range 33‐72 years. Sex: 5 Male and 5 Female History: Duration of TD ranging from 0.5 to 3 years; Eight patients received anticholinergic drugs before TD; Duration of antipsychotic therapy ranging from 4 to 15 years. | |
| Interventions | No washout period was reported before trial entry. 1. Ritanserin: dose 10 mg three times a day for 30 days. N = 4. 2. Placebo for 30 days. N = 6. Concomitant medication: The patients continued receiving their basic treatment for the psychosis (i.e. haloperidol, lorazepam, haloperidol decanoate, chlorpromazine, clotiapine, thioridazine) |
|
| Outcomes | TD symptoms (AIMS): not clinically improved, not improved, deteriorated Mental state: BPRS |
|
| Notes | Sponsorship source: Sponsorship source not reported Results are presented for each phase |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Six patients, chosen at random (patients 1‐6; group A), first received the placebo and then ritanserin; the other four patients (patients 7 ‐10; group B) received treatment in the reverse order" Further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind" Details not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double‐blind" Details not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participant flow through the study is not clearly reported. However, full data for all participants have been reported for all visits including post intervention. |
| Selective reporting (reporting bias) | Unclear risk | All outcomes seem to have been reported. However, a protocol is not available for verification. |
| Other bias | Low risk | The study seems to have been free of other sources of bias. |
Mosnik 1997.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 2 days (1 day/single dose crossed over to another day/single dose) Design: cross‐over. Setting: Inpatients and outpatients, USA. | |
| Participants | Diagnosis: schizophrenia (DSM‐III‐R). N = 18. Sex: 18 male. Age: 28‐65 years, mean 44 (SD 11.8) years. History: currently receiving antipsychotics, clinically significant TD. Duration of TD nor reported. Patient stabilisation prior to study entry not reported. | |
| Interventions | 1. Phenylalanine: 100 mg/kg body weight (day 1) followed by placebo (day 2). N = 10.
2. Placebo: (day 1) followed by phenylalanine 100mg/kg body weight (day 2). N = 8. Background medication and treatment continued throughout trial. |
|
| Outcomes | Leaving the study early. Unable to use ‐ Tardive dyskinesia: AIMS endpoint score (not reported for placebo group or not reported for the first treatment phase before crossing over to the next treatment) Cognitive ability: Rey Auditory Verbal Learning Test (AVLT) (not reported for the first treatment phase before crossing over to the next treatment) Mental state: SANS & SAPS (modified version of scales used). Cognitive ability: Edinburgh Inventory test (no data) |
|
| Notes | Sponsorship source: Supported in part by a VA Merit Review grant to one of the authors by The National Institute of Mental Health Grants to a second author, and a NARSAD Young Investigator Award to a third author. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomized..." Details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Drinks were prepared by an assistant and administered by the first author in a double blind manner". "The fine white L‐phenylalanine powder could not be tasted or detected visually when mixed with the bright orange colored powder." Thus, patients may have been blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "TD ratings were performed double‐blind". No further details are reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "One subject in the group who received phenylalanine on the first day, left the hospital against medical advice after completing only 1 day of the study; however, his data were included in the analyses" |
| Selective reporting (reporting bias) | Unclear risk | Not all data are fully reported. Some data are reported partially. No protocol are available |
| Other bias | Low risk | The study seems to be free of other sources of data |
Mouret 1991.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 12 weeks. Design: parallel. Setting: inpatients, Morocco | |
| Participants | Diagnosis: schizophrenia (DSM‐III). N = 20. Sex: 7 female and 13 male Age: 20‐67 years, mean 38.3 years. History: chronic with antipsychotic‐induced TD. Duration of TD from 1 to 9 years. The antipsychotic therapy was maintained at the same dose but it is not clear the duration of stabilisation prior to study entry. | |
| Interventions | 1. Insulin, 'standard' type: 10 units/day for 15 days administered at 10:00am; weekly for 5 weeks thereafter. N = 10.
2. Placebo. N = 10. Background medication and treatment continued throughout trial. Anticholinergics were withdrawn at least 2 weeks prior to the beginning of the study |
|
| Outcomes | Tardive dyskinesia: AIMS improved/not improved, deterioration in symptoms, AIMS scale scores. Leaving the study early. | |
| Notes | Sponsorship source: Standard Insulin or placebo supplied by Novo Industry. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "They were randomly assigned..." Details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Judgement Comment: Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "...double‐blind... " "The patients and the rater were blind to treatment conditions" Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "...double‐blind... " "The patients and the rater were blind to treatment conditions". Details not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Attrition information has not been reported. However, as end of trial data had been individually reported for all randomised participants, it is assumed that all participants completed the trial |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to make a judgement. A protocol is not available to verify all outcomes defined prior to study. |
| Other bias | Unclear risk | "At day 0, all 20 patients had severe orofacial dyskinesia and the two groups of patients did not differ in scores, age, duration of disease. Neuroleptic treatment was however significantly (p=0.037) longer in the placebo group than in the insulin group". Unclear if this could have influenced bias. |
O'Brien 2014.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 6 weeks. Design: parallel. Setting: inpatients/outpatients, USA | |
| Participants | Diagnosis: schizophrenia or schizoaffective disorder, mood disorder,or gastrointestinal disorder + antipsychotic‐induced TD
N = 78.
Sex: not reported
Age: 18‐85 years History: Duration of TD at least 3 months prior to study. Patient stabilisation was minimum of 30 days before study start. Participants who were not using antipsychotic medication had stable psychiatric status. |
|
| Interventions | 1. NBI‐98854 (VMAT2 inhibitor): dose 25mg/d‐75mg/d for 6 weeks. N = 39.
2. Placebo for 6 weeks. N = 49. Concomitant medication not reported. |
|
| Outcomes | Tardive dyskinesia: AIMS. CGI‐TD and a patient‐reported scale were also reported for TD symptoms but not included in the review.
Adverse events. Leaving the study early |
|
| Notes | Sponsorship source: Neurocrine Biosciences | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated block randomisation. |
| Allocation concealment (selection bias) | Low risk | Central interactive web response system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | ""double‐blind, "blinded physician investigator," Personnel blinded, details not reported for participants but we judge that participants were likely to be blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Movement Disorder Neurologists as blinded central AIMS raters" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "Early discontinuation rates were comparable (5 subjects each, placebo and active)." Active 13% and placebo 10% dropouts. Reasons were reported. |
| Selective reporting (reporting bias) | Unclear risk | Results for some scales to assess safety were not fully reported. |
| Other bias | Low risk | Appears to be free from other sources of bias. |
Rastogi 1982.
| Methods | Allocation: "randomly allocated"
Blindness: double‐blind, unclear.
Duration:12 weeks (6 weeks intervention and 6 weeks post intervention follow‐up).
Design: parallel Setting: Inpatients, UK |
|
| Participants | Diagnosis: Schizophrenia (29), dementia (5), depressive psychosis (3), oligophrenia (2), bipolar affective psychosis (1). Presence of persistent involuntary movements predominantly in the orofacial region and unrelated to drug‐induced Parkinsonian movements.
N = 40.
Sex: 22 female and 18 male.
Age: mean 69.9 years. History: Duration of TD at least 1 year.. |
|
| Interventions | 1. Co‐dergocrine (hydergine): dose 4.5 mg/day for 6 weeks. N = 19.
2. Placebo for 6 weeks. N = 21 Background antipsychotic and antiparkinsonian medication was held constant throughout the study. |
|
| Outcomes | TD symptoms: AIMS combined with abbreviated Rockland Tardive Dyskinesia Rating Scale | |
| Notes | Sponsorship source: Sponsorship source not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomly allocated to two groups" Further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "[...], one of which received co‐dergocrine, 4.5 mg tablets once daily for 6 weeks, and the other received an identical placebo tablet for the same period. The 2 raters, ward staff and patients were blind to the treatment procedure." |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Details not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Attrition information not reported. |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all outcomes have been reported. |
| Other bias | Unclear risk | Baseline characteristics, except for age, sex, and TD scores, not reported per intervention group. |
Richardson 2003.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 3 weeks. Design: parallel. Setting: Inpatients and outpatients, USA | |
| Participants | Diagnosis: Psychiatric patients with long histories of antipsychotic treatment
N = 68.
Sex: 68 male
Age: mean 44.6(SD 9.9). History: Duration of TD: "presumably long‐standing tardive dyskinesia". Patients stable for 2 weeks prior to entry. Patients who began the trial with stable doses of medication but who had changes in antipsychotic antiparkinson, antidepressant, or anticonvulsant drug doses during the trial were dropped from the study. |
|
| Interventions | 1. Branched‐chain amino acids: low dose 56 mg/kg of body weight for 3 weeks. N = not reported
2. Branched‐chain amino acids: medium dose 167 mg/kg of body weight for 3 weeks. N = not reported 3. Branched‐chain amino acids: high dose 222 mg/kg of body weight for 3 weeks. N = 25 4. Placebo for 3 weeks. N = 27 Only results from the high dose and placebo groups were reported. Concomitant medication not reported |
|
| Outcomes | Tardive dyskinesia: Simpson Abbreviated Dyskinesia Scale: improvement, deterioration, scale scores. Leaving the study early. | |
| Notes | Sponsorship source: Supported by NIMH grant MH‐44153, institutional support from the New York State Office of Mental Health, and a grant and product support from Scientific Hospital Supplies International, Ltd. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomly assigned" Details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind," Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Movement frequencies were counted from the videotapes by the first author, who was blind to the patients’ treatment status and the chronological order of the videotapes." |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participants treated with low and medium dose were not entered to the analysis. ITT was conducted for 41 participants who were treated with high‐dose aminoacid or placebo. |
| Selective reporting (reporting bias) | High risk | Outcome data not reported for low‐ and medium‐dose treatment. Patient recruitment of these two groups was stopped after interim analysis. Full details of interim analysis results not reported. |
| Other bias | Unclear risk | The authors state that there were no differences between participants treated with high dose and placebo. However, details of the two other groups randomised to the trial have not been reported. |
Shamir 2000.
| Methods | Allocation: randomised. Blindness: double‐blind. Duration: 3 weeks. Design: cross‐over (2 week washout) Setting: Inpatients, Israel | |
| Participants | Diagnosis: Chronic schizophrenia (DSM‐IV criteria)
N = 19.
Sex: 13 female and 6 male
Age: range 62‐91 years, mean 73 years (SD 9.9). History: Duration of TD for a minimum of 5 years. Patient stabilisation duration was unclear but "all patients continued to receive antipsychotic treatment during the trial and treatment was unchanged throughout the study". |
|
| Interventions | 1. Melatonin: dose 2 mg/day for 4 weeks. N = 9 2. Placebo for 4 weeks. N = 10 Concomitant medication not reported. |
|
| Outcomes | Tardive dyskinesia: AIMS improved/not improved, deterioration in symptoms, AIMS scale scores.
Leaving the study early. Adverse effects |
|
| Notes | Sponsorship source: Melatonin (Circadin) and placebo tablets supplied by Neurim Pharmaceuticals, Tel Aviv, Israel. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "randomly assigned". Although details of randomisation have not been reported. As allocation was done by the hospital pharmacy, it is assumed that random sequence generation was not biased. |
| Allocation concealment (selection bias) | Low risk | "Both patients and physicians were blinded to the group allocation and all medications were dispensed by the center's pharmacy and added to the patients' regular treatment regimens". |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "The patients were randomly assigned to receive placebo or melatonin 2mg/day, supplied in identical tablet form by Neurim Pharmaceuticals...Both patients and physicians were blinded to the group allocation and all medications were dispensed by the center's pharmacy and added to the patients' regular treatment regimens". |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | TD symptoms' outcomes: "The patients were randomly assigned to receive placebo or melatonin 2mg/day, supplied in identical tablet form by Neurim Pharmaceuticals...Both patients and physicians were blinded to the group allocation and all medications were dispensed by the center's pharmacy and added to the patients' regular treatment regimens". "The same investigator... rated the individual patients throughout the trial." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "All 19 patients completed the 10‐week study." |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all outcomes previously stated were reported. A protocol is not available for verification. Also, although stated that "Prior to separating the data into the 2 treatment groups, the data were examined according to order...No carryover effects were demonstrated and baseline values did not differ significantly", data not reported per period. |
| Other bias | Unclear risk | Insufficient information to make a judgement. |
Shamir 2001.
| Methods | Allocation: randomised. Blindness: double‐blind. Duration: 16 weeks. Design: cross‐over (4 week washout) Setting: inpatient (probably), Israel | |
| Participants | Diagnosis: Schizophrenia (Structured Clinical Interview for DSM‐IV); antipsychotic‐induced TD (DSM‐IV criteria)
N = 24 (2 were discharged after randomisation, but before initiation of treatment, and were not included).
Sex: 6 female and 6 male
Age: range 28‐82 years, mean 64.2 years (SD 14.3). History: Duration of TD not reported. Patient stabilisation duration unclear but "the antipsychotic medication regimens remained unchanged throughout the study". |
|
| Interventions | 1. Melatonin: dose 10 mg/day for 6 weeks. N = 12 2. Placebo for 6 weeks. N = 10 Concomitant medications: "anticholinergics 12 patients; benzodiazepines, 5 patients; antidepressants, 4 patients; and mood stabilizers, 5 patients. The regimens of these additional medications also remained unchanged throughout the study" |
|
| Outcomes | Leaving the study early. Adverse effects Unable to use ‐ Tardive dyskinesia: AIMS improved/not improved, deterioration in symptoms, AIMS scale scores (not reported separately for the first treatment phase before cross‐over to the next treatment). |
|
| Notes | Sponsorship source: Sponsorship source not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "randomized," Although details of randomisation have not been reported, as allocation was done by the hospital pharmacy, it is assumed that random sequence generation was not biased. |
| Allocation concealment (selection bias) | Low risk | "Medication and placebo were dispensed by the hospital’s pharmacy and added to the patients’ ongoing treatment regimen." |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "using sealed envelopes."...tablets identical in appearance..."...unblinding code following database lock..." |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details are provided. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "Two female patients were discharged from the hospital before initiation of the study and are not included in the analysis." Participants were randomised; 2/24(8%) were withdrawn before first dose of medication. It seems that the two withdrawn participants were originally randomised to the placebo group. |
| Selective reporting (reporting bias) | Unclear risk | Unclear if all outcomes previously stated were reported. A protocol is not available for verification. |
| Other bias | Unclear risk | Insufficent information to make a judgement. |
Shi 2009.
| Methods | Allocation: “randomly assigned”
Blinding: not reported.
Duration: 12 weeks. Design: parallel Setting: inpatient (probably) China |
|
| Participants | Diagnose: Antipsychotic‐induced TD. N = 76 Sex: male 26, female 50. Age: mean 56.1 (SD 9.12) years old History: Duration of TD not reported. Patient were stabilised before entry to trial but the duration is not reported. |
|
| Interventions | 1. Melatonin Group: dose: 9 mg melatonin, oral taken before sleep for 12 weeks. N = 39 2. Control Group: no medication control group for 12 weeks. N = 37 Concomitant medication not reported. |
|
| Outcomes | Cognitive function: Wechsler Adult Intelligence Scale (WAIS)
Cognitive function: Wechsler Memory Scale (WMS)
Cognitive function: Vocabulary fluency scale (VFS)
Adverse events: Treatment Emergent Symptom Scale (TESS) ‐‐Unable to use (These outcomes were not predefined by this review and data were translated) WAIS subscale‐score (verbal scale, verbal IQ, performance scale, performance IQ, and full scale IQ). VFT subscale‐score: animal, fruits, making words. RBANS, subscale‐score. The author did not report the total score and other subscales scores excluding the subscale‐semantic fluency; because a significant difference was only observed on the latter subscale. |
|
| Notes | Funding source: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “ randomly assigned…” The author did not state the method of randomisation |
| Allocation concealment (selection bias) | Unclear risk | No information about allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | It’s not possible that the participants and personnel could be blinded. As the control group did not receive intervention in addition to antipsychotics. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information about blinding outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants completed the study |
| Selective reporting (reporting bias) | Low risk | The authors reported all measured outcomes. |
| Other bias | Unclear risk | Insufficent information to make a judgement. |
UCB Pharma 2005.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 8 weeks. Design: parallel. Setting: inpatient (probably), Belgium and Bulgaria. | |
| Participants | Diagnosis: antipsychotic‐induced TD N = 70. Sex: 35 female and 35 male Age: 18‐80 years, mean 53.92 (SD 10.83) years. History: Duration of TD at least one month. Patient stabilised for at least 1 month prior to entry. | |
| Interventions | 1. Levetiracetam: dose: 1500 mg twice a day (stable dose) for 8 weeks. N = 34.
2. Placebo for 8 weeks. N = 36. Concomitant medication not reported. |
|
| Outcomes | Tardive dyskinesia: mean change of symptoms (hyperkinesia subscale of the St Hans rating scale).
Leaving the study early. Adverse events |
|
| Notes | Sponsorship source: Sponsored by UCB Pharma | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "...randomized ..." Clinical Study Summary (CSS). Details not reported |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | " ...double blind..." Clinical Study Summary (CSS). Details not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | " ...double blind..." Clinical Study Summary (CSS). Details not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | "All data are presented on the intent‐to‐Treat population (all randomized subjects who took at least one dose of study medication). ". Clinical Study Summary (CSS) The authors actually performed modified ITT. |
| Selective reporting (reporting bias) | High risk | Outcome data for 2/3 secondary outcomes (antipsychotic‐induced akathisia and other extrapyramidal symptoms, effect on the primary psychiatric disorder) not reported. Only summary data from Sponsor is available. |
| Other bias | Unclear risk | Insufficient information to make a judgement. |
Wolkin 1986.
| Methods | Allocation: randomised, not described. Blindness: double‐blind, not described. Duration: 6 weeks. Design: parallel. Setting: Inpatients and outpatients, USA. | |
| Participants | Diagnosis: schizophrenia* (no operational criteria). N = 16. Sex: male. Age: mean 54 (SD 9) years. History: Duration of TD at least 1 year. Individual antipsychotic regimens (including no antipsychotic drugs in three patients) were kept constant from at least 1 month before the study through termination. Chronic with antipsychotic‐induced TD. | |
| Interventions | 1. Gamma‐Linolenic acid supplementation (oil of evening primrose) 600 mg/day for 6 weeks. N = 8.
2. Placebo for 6 weeks. N = 8. Background medication and treatment continued throughout trial. 1 patient was on lithium carbonate. Other concomitant medications not reported. |
|
| Outcomes | Tardive dyskinesia: AIMS improved/not improved, deterioration in symptoms, AIMS scale scores. Mental state: BPRS scale scores. Leaving the study early**. | |
| Notes | Sponsorship source: Supported in part by Efamol, Ltd., and by the VA * one participant might have been bipolar. ** assume loss is 0 as all AIMS scores available after 6 weeks. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Subjects were assigned on a random, double‐blind basis" Details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment details not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double‐blind". Details not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double‐blind". Details not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Although attrition details have not been reported, as end of trial data are reported individually for all randomised participants, it is assumed that all participants completed the trial. |
| Selective reporting (reporting bias) | Unclear risk | Indufficent information to make a judgement. As a protocol is not available, it is not possible to verify if all outcomes defined prior to study have been reported. (e.g. adverse events have not been reported) . |
| Other bias | Low risk | The study seems to be free of other sources of bias. |
Woods 2008.
| Methods | Allocation: "assigned at random", not described. Blindness: double‐blind, not described. Duration: 12 weeks. Design: parallel Setting: outpatients, USA | |
| Participants | Diagnosis: schizophrenia/schizoaffective disorder (45), affective disorder (4), other psychiatric diagnosis (1) (DSM‐IV); and TD (Glazer‐Morgenstem criteria, i.e., total AIMS score ≥3, with at least 1 body area rated ≥2).
N = 50.
Sex: 21 female and 29 male.
Age: mean 47.4 (SD 9.6) years. History: Duration of TD in the levetiracetam group is 7.5 ± 8.4 years, whereas in the placebo group is 9.0±7.3 years. "sufficiently stable psychiatrically that their CMHC clinician indicated that changes in prescribed antipsychotic medication drug or dosage were not anticipated in the next 3 months". "Changes in the prescribed concomitant antipsychotic medications or their doses during the randomised phase occurred in 3 levetiracetam patients (12%) versus 5 placebo patients (20%)..." |
|
| Interventions | 1. Levetiracetam: maximum dose 1500 mg* twice a day for 12 weeks. N = 25 2. Placebo for 12 weeks. N = 25 * side effects permitting and assuming lack of complete response, the dose was recommended to be escalated weekly by 500 mg/day to the maximum dose of 3000 mg/day, given in 2 divided doses. Concomitant medication: baseline anticholinergics (52%, levetiracetam group; 48% placebo group). Changes occurred in 2 placebo patients and none of the active patients. |
|
| Outcomes | Tardive dyskinesia: AIMS
Leaving the study early. Adverse effects. Unable to use () ‐ Mental State: Positive and Negative Syndrome Scale (PANSS); Young Mania Scale (YMRS); Montgomery‐Asberg Depression Rating Scale (MADRS); Hamilton Rating Scale for Anxiety (HAM‐A) |
|
| Notes | Sponsorship source: Supported by a grant from UCB Pharma. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Eligible patients who gave written informed consent were assigned at random", further details not reported. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "double blind phase" no further details. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "double blind phase" no further details. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Completion rates (64% [N = 16] for the levetiracetam group and 80% [N = 20] for the placebo group, P = 0.345), reasons for discontinuation did not differ significantly between treatment groups. Data were reported for all participants randomized to the two groups (mixed‐effects model). |
| Selective reporting (reporting bias) | High risk | Primary outcome, total AIMS scores reported. However the authors stated that: "In addition to the principal analyses of the AIMS total score, we also investigated the relative rates at which subjects achieved remission, defined a priori as no longer meeting the Glazer‐Morgenstern TD entry criteria. " Remission data only reported as "...Group differences did not achieve statistical significance." Also, although not stated in the Protocol, the publication reported that: "At each study visit, patients were weighed and underwent an AIMS examination and symptom ratings using the Positive and Negative Syndrome Scale (PANSS); Young Mania Rating Scale (YMRS), Montgomery Asberg Depression Rating Scale (MADRS), and the Hamilton Rating Scale for Anxiety (HAM‐A) administered via a structured interview guide. Adverse events were rated using the Systematic Assessment for Treatment Emergent Events, general inquiry method. Complete blood counts were obtained at baseline and at 6, 12". Only baseline data for these outcomes have been reported. |
| Other bias | Low risk | "...none of the interactions with baseline were statistically significant...Further analyses revealed that the small age difference at baseline did not confound the levetiracetam treatment effect, nor did the small baseline differences in years of education, antipsychotic chlorpromazine equivalent dose, antipsychotic type at baseline (only atypical vs. any conventional), or gender." |
Yang 1999.
| Methods | Allocation: "randomly assigned”.
Blinding: double‐blind, outcome assessor was blinded. Design: parallel. Setting: inpatients, China. Duration: 12 weeks. |
|
| Participants | Diagnosis: Antipsychotics‐induced TD (Research Diagnosis Criteria for TD, RD‐TD) N = 36 (2 participants left the study early due to discharge) Sex: male 18 , female 16 Age: mean 50.2 years old, SD 13.4 years old. History: mean˜ 8.9 years (SD˜ 7.3years) TD; mean˜ 17.7years (SD˜ 9.22 years) schizophrenia. |
|
| Interventions | 1. Promethazine Group: (n = 18) Management: 50 mg promethazine was administrated by IM, twice per day for 2 weeks following with a 2‐week period of IV drip (50 mg promethazine dissolved in 500 mL normal saline, once per day). This 4‐week treatment regimen was conducted three circles in 12 weeks. 2. Placebo Group: (n = 16) Management: The same treatment regimen as promethazine. The placebo drug was 2 mL normal saline with same appearance as promethazine. All participants received antipsychotics as usual but were not allowed to use clozapine, anticholinergic drug, vitamin E or calcium channel blocker. |
|
| Outcomes | TD symptoms: improvement, AIMS Global state: CGI Mental state: BPRS Extrapyramidal side effects: RSESE (rating scale for extrapyramidal side effects) Adverse events: TESS (Treatment Emergent Symptom Scale) | |
| Notes | *defined by the 4‐level clinical response standard, recovery, obvious improvement, improvement, no clinical response. Funding source: not reported. Paper in Chinese, assessed and data extracted by Sai Zhao. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | ”randomly assigned”, no further details. Although the author did not state the method of randomisation, we have rated selection bias as low: because central allocation was used, it is very likely that an adequate randomisation sequence was generated. |
| Allocation concealment (selection bias) | Low risk | Central allocation, pharmacy‐controlled randomisation. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind", no details of blinding of participants and personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | ”The outcome assessor was blinded” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants competed the study. |
| Selective reporting (reporting bias) | Low risk | The author reported all measured outcomes. |
| Other bias | Low risk | None obvious. |
Zeng 1995.
| Methods | Allocation: "randomly assigned…"
Blinding: double‐blind study. Details are provided
Duration: 6 weeks Design: parallel Setting: inpatients |
|
| Participants | Diagnose: Antipsychotics‐induced TD Total: N = 42 Sex: male 28, female 14 Age: mean˜32.5 years old, SD˜10.3years old. Length of illness (schizophrenia): mean˜ 7.5 years, SD ˜3.4 years History: Duration of TD on average 5.4 ± 4.2 years in active group, whereas 5.7 ± 4.5 years in control group. |
|
| Interventions | 1. Buspirone Group: (n = 21) Management: The initial dosage, one capsule each day, was titrated to 6‐12 capsules each day within 10 days. 2. Placebo Group: (n = 21) Management: The initial dosage, one capsule each day, was titrated to 6‐12 capsules each day within 10 days. All participants received stable AP and concomitant anticholinergic drug. |
|
| Outcomes | Clinical response*
Tardive dyskinesia: AIMS (Abnormal Involuntary Movement Scale) Adverse events: dizziness, headache, nausea, vomiting ‐‐Unable to use Blood routine examination, urine routine test and liver function test, electrocardiography, electroencephalogram (the author only stated results of these tests were normal but did not report the data) |
|
| Notes | Funding source: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly assigned…" The author did not state the method of randomisation. |
| Allocation concealment (selection bias) | Unclear risk | The author did not state the method of allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "double blind study , the interventions were coded as intervention A or B by the researcher in pharmacy ". "Participants and personnel did not know the allocation result. The two drugs were contained in capsules with same appearance" Blinding of participants and key study personnel ensured. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants competed the study. |
| Selective reporting (reporting bias) | Low risk | The author reported all measured outcomes. |
| Other bias | Low risk | None obvious. |
Zeng 1996.
| Methods | Allocation: "randomly assigned…."
Blinding: "double blind". Details are provided.
Duration: 6 weeks. Design: parallel Setting: inpatients |
|
| Participants | Diagnosis: Antipsychotic induced TD. N = 46 Sex: male 30, female 16. Age: mean ˜33 years old, SD˜10 years old. History: Duration of TD on average 2.2 years (SD˜1.7 years). Patients stabilised prior to study for 5 ± 4 years. |
|
| Interventions | 1. Pemoline Group: (n = 23) Management: two capsules per day for six days per week, oral taken before breakfast. 2. Placebo Group: (n = 23) Management: two capsules per day for six days per week, oral taken before breakfast. All participants received stable AP and concomitant anticholinergic drug. |
|
| Outcomes | Clinical response*
Tardive dyskinesia: AIMS (Abnormal Involuntary Movement Scale)
Adverse events: dizziness and headache; nausea and anorexia ‐‐Unable to use Blood routine examination, urine routine test and liver function test, electrocardiography, electroencephalogram (the author only stated results of these tests were normal but did not report the data) |
|
| Notes | Funding source: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly assigned". The author did not state the method of randomisation. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind study), the interventions were coded as intervention I or II by the researcher in pharmacy. “Participants and personnel did not know the allocation result. The two drugs were contained in capsules with same appearance.” Blinding of participants and key study personnel ensured. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants competed the study. |
| Selective reporting (reporting bias) | Low risk | The author reported all measured outcomes. |
| Other bias | Low risk | None obvious. |
Zhang 2011.
| Methods | Allocation: "randomized", described. Blindness: double‐blind, described. Duration: 12 weeks. Design: parallel Setting: inpatients, China | |
| Participants | Diagnosis: DSM‐IV diagnosis of schizophrenia; diagnosis of TD based on the Schooler‐Kane criteria.
N = 157.
Sex: 157 male.
Age: mean 45.2 (SD 6.7) years. History: Duration of TD at least 1 year. "A stable dose of antipsychotics for at least 4 weeks prior to trial entry". |
|
| Interventions | 1. EGb‐761 (standardised extract of Ginkgo biloba leaves that has antioxidant properties as a free radical scavenger): dose 80 mg, three times a day for 12 weeks. N = 78 2. Placebo for 12 weeks. N = 79 Patient regular antipsychotic medication. Antipsychotics and all other medications remained fixed throughout the double‐blind period (i.e. clozapine, risperidone, aripiprazole, olanzapine, quetiapine, chlorpromazine, haloperidol, sulpiride). Their chlorpromazine‐equivalent doses were 429.3 mg/day and 440.2 mg/day in the EGb‐761 and placebo groups, respectively. Anticholinergics were allowed during the trial. Twenty‐seven patients (12 in the EGb‐761 group and 15 in the placebo group) were treated with anticholinergics for a long time prior to entering the study; however, anticholinergic treatment was stable during the clinical trial. No new use of anticholinergic drugs was allowed. |
|
| Outcomes | Tardive dyskinesia: AIMS improved/not improved, deterioration in symptoms, AIMS scale scores.
Mental state: PANSS; Cognitive performance Continuous Performance Test‐37 (CBT‐37) Leaving the study early. |
|
| Notes | Sponsorship source: Supported by the National Basic Research Program of China and the National Natural Science Foundation of China. Statistical analysis was funded by Glaxo Smith Kline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Patients had an equal probability of being assigned to the 2 groups. An independent third party placed them in either the active or placebo group according to a computer‐generated randomization list compiled through simple randomization" |
| Allocation concealment (selection bias) | Low risk | "To ensure the concealment of allocation, this third party used a protected computer database for the randomization list." |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "After the run‐in period, patients were randomly assigned to receive either capsulized EGb‐761... or an identically capsulized placebo in a double‐blind manner". "All of the study personnel and participants were blinded to the treatment assignment for the duration of the double‐blind period, except 1 study staff member in the pharmacy, who remained unblinded to provide the placebo and EGb‐761 treatments" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All efficacy outcomes: "Each subject was assessed by the same investigator, who was blind to treatment status". Cognitive tests: computer assessments. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "intention‐to‐treat analysis for the 2 groups of randomly assigned patients, with last‐observation‐carried‐forward imputation." |
| Selective reporting (reporting bias) | High risk | Side effects and Adverse Events data not reported. "Systemic side effects were evaluated by means of routine physical and neurologic examinations and laboratory tests and reviewed by applying the UKU Side Effect Rating Scale. These systemic side effects were all mild and brief. For none of the subjects were the routine blood cell count, chemistry, urinalysis, or electrocardiogram parameters significantly affected by the experimental treatment (data not shown)". Also, Change in Simpson‐Angus Rating Scales for EPS not reported. |
| Other bias | Low risk | The study seems to be free from other sources of bias. |
AIMS ‐ Abnormal Involuntary Movement Scale AVLT ‐ Rey Auditory and Verbal Learning Test BPRS ‐ Brief Psychiatric Rating Scale CGI ‐ Clinical Global Impression DSM ‐ Diagnostic and Statistical Manual of Mental Disorders EPS ‐ extrapyramidal symptoms ESRS ‐ Extrapyramidal System Rating Scale IM ‐ intramuscular ITT ‐ intention‐to‐treat IV ‐ intravenous MAOI ‐ monoamine oxidase inhibitor mcg ‐ microgram NOSIE ‐ Nurses Observation Scale for Inpatient Evaluation PANSS ‐ Positive and Negative Syndrome Scale Rockland TD ‐ Rockland Tardive Dyskinesia Rating Scale SANS ‐ Scale for the Assessment of Negative Symptoms SAPS ‐ Scale for the Assessment of Positive Symptoms SAS ‐ Simpson Angus Scale SD ‐ Standard deviation TAU ‐ treatment as usual TD ‐ tardive dyskinesiaTESS ‐ Treatment Emergent Symptoms Scale VMAT ‐ vesicular monoamine transporter 2
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Apseloff 2000 | Allocation: randomised. Participants: healthy, non‐smoking males, not TD. |
| Bjorndal 1980 | Allocation: not randomised. |
| Blum 1984 | Allocation: not randomised. |
| Bockenheimer 1976 | Allocation: randomised Participants: TD Intervention: Deanol vs placebo, not relevant for this review, included in Cholinergics review |
| Bowers 1979 | Allocation: not randomised. |
| Casey 1981 | Allocation: not randomised. |
| Chaplin 2002 | Allocation: randomised. Participants: schizophrenia (40), schizoaffective disorder (11), bipolar disorder (5); not TD at baseline. |
| Emsley 2002 | Allocation: randomised. Participants: people with schizophrenia, but not specifically TD. |
| Fann 1973 | Allocation: randomised. Participants: TD. Interventions: Methylphenidate vs placebo. Outcomes: No outcome data have been provided for the first phase before cross‐over. Author was contacted but no information was received and this over 40 years old study was excluded. |
| Fudge 1991 | Allocation: randomised. Participants: schizophrenia (DSM‐III‐R) and TD. Interventions: Electromyographic biofeedback vs noncontingent "false" feedback (placebo). Outcomes: No useable data were extractable. Study author was contacted but no information was received and this 25 years old study was excluded. |
| Gardos 1978 | Allocation: not randomised. |
| Gerlach 1975 | Allocation: randomised. Participants: Psychiatric inpatients with a BLM syndrome induced by antipsychotic treatment; psychiatric‐neurological condition stable and pharmacological treatment unchanged for at least 2 months. Interventions: Lithium vs placebo. Outcomes: All data unusable. Unable to extract from the fist phase of cross‐over. We were unable to find up‐to‐date contact details for the study authors of this over 40 years old study; it was excluded. |
| Goetz 2013 | Allocation: unclear if randomised. Participants: people with Parkinson's disease and not TD symptoms at baseline |
| Huang 1981 | Allocation: randomised Participants: TD Intervention: Alpha‐methyldopa vs. reserpine vs. placebo, not relevant for this review, included in the Non‐antipsychotics review. |
| Jus 1974 | Not randomised, controlled clinical trial. Benztropine vs diazepam vs diphenylhydantoin vs DL tryptophan. No placebo control. |
| Jus 1978 | Allocation: randomised. Participants: people with TD. N = 29. Interventions: deanol versus lithium carbonate versus placebo. Outcomes: AIMS, TD symptom rating scale, CGI, BPRS, NOSIE, vital signs, lab values. Trial used cross‐over design. Impossible to extract data from segment before cross‐over. One of authors contacted to confirm lack of additional data. |
| Kabes 1982 | Allocation: randomised
Population: antipsychotic‐induced extrapyramidal side effects: (i) akathisia, (ii) tremor, (iii) muscle rigidity and (iv) dyskinesia. Interventions: Piracetam versus placebo administered IV in 1‐hour intervals. Outcomes: not useable, measured 30 mins after intervention. |
| Kabes 1985 | Allocation: randomised
Population: patients suffering from TD and receiving antipsychotic treatment. Interventions: Piracetam 2.4 g/d vs Piracetam 4.8 g/d vs Piracetam 10 g/d vs placebo for 4 weeks. Outcomes: no usable data. We were unable to find up‐to‐date contact details for the study authors of this over 30 years old study; it was excluded. |
| Koller 1982 | Allocation: randomised. Participants: Various dyskinesias and movement disorders, including TD. Interventions: Oestrogen vs. placebo Outcomes: No usable data since they are reported in figures with no variability measures. No reply from author. Study is over 30 years old and was excluded. |
| Korsgaard 1981 | Allocation: not randomised. |
| Lieberman 1987 | Allocation: randomised Population: not TD |
| Lieberman 1994 | Allocation: randomised Participants: not TD, participants classified as TD or not TD only during measuring outcomes after intervention |
| Lindenmayer 1988 | Allocation: randomised. Participants: DSM‐III diagnoses were predominantly schizophrenia (N = 16) and included four cases of major affective disorder. All participants had TD for at least 1 year. Interventions: Nalaxone 20g vs Nalaxone 40 g vs placebo. Outcomes: No outcome data have been provided for the first period before cross‐over. Author was contacted but no information was received and this over 25 years old study was excluded. |
| Moore 1980 | Allocation: not randomised. |
| Nasrallah 1986 | Allocation: randomised. Participants: Psychiatric patients; Schooler and Kane criteria for persistent TD. Interventions: AMPT vs L‐DOPA vs Cholone chloride vs Valproic acid vs Hydroxytryptophan. Outcomes: No outcome data has been provided for the first period before cross‐over. Author was contacted but no information was received and this 30 years old study was excluded. |
| Peselow 1989 | Allocation: randomised. Participants: people with chronic schizophrenia with multiple hospitalisations and averaged 5.5 years of TD. Interventions: Monosialotetrahexosylganglioside (GM1) versus placebo. Outcomes: All data unusable. Authors were contacted and confirmed data were inaccessible. |
| Prange 1973 | Allocation: not randomised. |
| Reda 1974 | Allocation: not randomised. |
| Reker 1982 | Allocation: not randomised. |
| Shah 2012 | Allocation: randomised. Participants: Parkinson's disease, not TD. |
| Simpson 1976 a | Allocation: not randomised. |
| Simpson 1976 b | Allocation: not randomised. |
| Tamminga 1983 | Allocation: randomised. Participants: chronic schizophrenia patients with symptoms of TD. Interventions: Muscimol vs placebo. Outcomes: No useable data were extractable. Study author was contacted but no information was received and this over 30 years old study was excluded. |
| Vaddadi 1989 | Allocation: randomised
Population: psychiatric patients (DSM‐II criteria) with established movement disorders who had been exposed to antipsychotics over a long period of time; TD (Schooler and Kane criteria). Interventions: Efamol (essential fatty acid) + Vitamin E vs liquid paraffin + vitamin E. Outcomes: No outcome data have been provided for the first period before cross‐over. Study author was contacted but no information was received and this over 25 years old study was excluded. |
| Vaddadi 2002 | Allocation: randomised Population: Huntington's disease, not TD |
| Villeneuve 1970 | Allocation: not randomised. |
| Villeneuve 1980 | Allocation: not randomised. |
| Volavka 1986 | Allocation: not randomised. |
| Wonodi 2004 | Allocation: randomised
Population: schizophrenia patients; treated by antipsychotics; TD (Schooler and Kane). Interventions: Naltrexone vs placebo and Naltrexone + clonazepam vs placebo + clonazepam. Outcomes: No outcome data have been provided for the first phase before cross‐over. Study author was contacted but no information was received and this over 10 years old study was excluded. |
AIMS: Abnormal involuntary Movement Scale CGI ‐ Clinical Global Impression DSM ‐ Diagnostic and Statistical Manual of Mental Disorders TD = tardive dyskinesia IV = intravenous
Characteristics of studies awaiting assessment [ordered by study ID]
Fernandez 2016.
| Methods | Allocation: randomised. Blindness: double‐blind Duration: 12 weeks Design: parallel. Setting: USA, Czech Republic, Poland, Slovakia |
| Participants | Diagnosis: History of using a dopamine receptor antagonist for at least 3 months; clinical diagnosis of tardive dyskinesia and has had symptoms for at least 3 months prior to screening; participants with underlying psychiatric diagnosis are stable and have no change in psychoactive medications N = 117 Sex: male and female Age:18 to 75 years old |
| Interventions | 1. SD‐809 (deutetrabenazine) tablets taken twice daily for 12 weeks, includes a dose titration period and maintenance period. N = 58 2. Placebo tablets taken twice daily for 12 weeks. N = 59 |
| Outcomes | Change in AIMS score from baseline to week 12. Quality of life; Treatment success based on Patient Global Impression of Change (PGIC) questionnaire; Percentage reduction in AIMS score; Proportion of responders based on AIMS change from baseline |
| Notes | Other study ID: SD‐809‐C‐18 Sponsor: Auspex Pharmaceuticals, Inc. From 2017 update search, conference abstract with limited details, awaiting more detailed data. |
Hauser 2016.
| Methods | Allocation: randomised. Blindness: double‐blind Duration: 6 weeks + 42 weeks extension Design: parallel Setting: USA, Canada, Puerto Rico |
| Participants | Diagnosis: schizophrenia, schizoaffective disorder, or mood disorder (for at least 3 months prior to screening); a clinical diagnosis of antipsychotic‐induced TD for at least 3 months prior to screening; if using maintenance medication(s), be on stable doses; negative drug screen for amphetamines, barbiturates, benzodiazepines, phencyclidine, cocaine, opiates, or cannabinoids N = 240 Sex: male and female Age: 18 to 85 years old |
| Interventions | 1. NBI‐98854 administered orally as one 40 mg capsule and one placebo capsule for 6 weeks. At the end of week 6, participants will enter a double‐blind NBI‐98854 treatment period and continue with their current dose N = 80 2. Participants randomised to the NBI‐98854 80 mg dose will receive NBI‐98854 40 mg for the first week (administered orally as one 40 mg capsule and one placebo capsule), followed by NBI‐98854 80 mg administered orally as two 40 mg capsules for 5 weeks. At the end of week 6, participants will enter a double‐blind NBI‐98854 treatment period and continue with their current dose. N = 80 3. Placebo administered orally as two placebo capsules 6 weeks. At the end of Week 6, participants will enter a double‐blind NBI‐98854 treatment period and be randomised to either a 40 mg or 80 mg dose. N = 80 |
| Outcomes | Severity of TD symptoms assessed by AIMS, change from baseline Clinical Global Impression of Change ‐ TD (CGI‐TD); Tardive Dyskinesia Impact Scale (TDIS); Patient Global Impression of Change (PGIC); Percentage of participants classified as responders based on AIMS dyskinesia total score % change from baseline; Percentage of participants classified as responders based on CGI‐TD |
| Notes | Study ID: NCT02274558
Sponsor: Neurocrine Biosciences From 2017 update search, conference abstracts, poster, and online trial registration record with limited details, awaiting more detailed data. |
NCT01393600 2011.
| Methods | Allocation: randomised Blindness: double‐blind Duration: 1 month Design: cross‐over Setting: USA |
| Participants | Diagnosis: schizophrenia or schizoaffective disorder and a clinical diagnosis of antipsychotic‐induced TD (DSM‐IV) for at least 3 months prior to screening; stable dose of antipsychotic medication for a minimum of 30 days before study start; participants not using antipsychotic medication must have stable psychiatric status; the doses of concurrent medications and the conditions being treated be stable for a minimum of 30 days before study start and be expected to remain stable during the study. N = 37 Sex: male and female Age: 18 to 65 years old |
| Interventions | 1. 12.5 mg NBI‐98854 once daily dose for days 1‐14 and placebo once daily dose for days 15‐28 (participants will be randomly assigned to receive one of these treatment sequences) 2. Placebo once daily dose for days 1‐14 and 50 mg NBI‐98854 once daily dose for days 15 mg to 28 mg or 50 mg NBI‐98854 once‐daily dose for days 1‐14 and placebo once‐daily dose for days 15‐28 (participants will be randomly assigned to receive one of these treatment sequences) |
| Outcomes | Treatment efficacy (AIMS) Efficacy of 12.5 mg or 50 mg doses of NBI‐98854 administered once daily for the treatment of TD symptoms using CGI‐TD and PGIC questionnaire Safety and tolerability for adverse events |
| Notes | Other study ID: NBI‐98854‐1101
Sponsor: Neurocrine Biosciences Online trial registration record, results are provided for combined groups in this cross‐over study, awaiting separate data. |
Pattojoshi 2016.
| Methods | Randomised, double‐blind, sham‐controlled study, 22 months duration. |
| Participants | Diagnosis: psychosis with TD (Schooler and Kane criteria). |
| Interventions | 10 right dorsolateral prefrontal cortex‐repetitive transcranial magnetic stimulation (rTMS) sessions versus 10 sham rTMS sessions, total n = 30. |
| Outcomes | AIMS, MMSE, CPRS. |
| Notes | From 2017 update search, conference abstract with limited details, awaiting more detailed data. |
Xu 2012.
| Methods | Randomised controlled trial, 12 weeks duration. |
| Participants | Diagnosis: schizophrenia (CHMD‐3) with tardive dyskinesia. |
| Interventions | Ginkgo biloba extract (n = 42) versus standard treatment (n = 40). |
| Outcomes | AIMS, TESS. |
| Notes | From 2017 update search, article in Chinese, awaiting translation. |
AIMS ‐ Abnormal involuntary Movement Scale CGI ‐ Clinical Global Impression CHMD‐3 ‐ Chinese Classification of Mental Disorders Version 3 CPRS ‐ Comprehensive Psychopathological Scale DSM IV ‐ Diagnostic and Statistical Manual of Mental Disorders MMSE ‐ Mini Mental State Examination PGIC ‐ Patient Global Impression of Change rTMS ‐ right dorsolateral prefrontal cortex‐repetitive transcranial magnetic stimulation TD ‐ tardive dyskinesia TESS ‐ Treatment Emergent Symptom Scale
Characteristics of ongoing studies [ordered by study ID]
Garcia 1992.
| Trial name or title | Double‐blind placebo controlled study using buspirone in the treatment of tardive dyskinesia |
| Methods | Allocation: randomised. Blindness: double‐blind. Duration: 12 weeks. Design: cross‐over. Setting: USA. |
| Participants | Diagnosis: TD patients, criteria not reported. N = 20. Sex: not reported. Age: not reported |
| Interventions | 1. Buspirone: Not reported, increasing dose. N = 20. 2. Placebo. N = 20. |
| Outcomes | AIMS score |
| Starting date | |
| Contact information | |
| Notes | Abstract of a study protocol, there are no data to be extracted. |
ISRCTN14688109 2015.
| Trial name or title | Investigation of the potential beneficial effects of cannabidiol in the treatment of tardive dyskinesia |
| Methods | Allocation: randomised Blindness: double‐blind (no further details) Duration: 1 year Design: parallel Setting: Nigeria |
| Participants | Diagnosis: ICD‐10 diagnosis of a psychotic disorder, verified with the MINI‐PLUS questionnaire; clinical diagnosis of TD confirmed with the AIMS; currently receiving treatment for a psychotic disorder and be on either the atypical or conventional antipsychotics. N = 56 Sex: male and female Age: at least 18 years old |
| Interventions | 1. High cannabidiol extract Nabidiolex® (CBD) (300 mg) administered orally in capsules twice a day for six weeks as an adjunctive treatment alongside their usual antipsychotic medication. N = 28 2. Vitamin E (400 IU) administered daily for six weeks as an adjunctive treatment alongside their usual antipsychotic medication N = 28 |
| Outcomes | Primary: Improvement in symptoms of TD measured using the Abnormal Involuntary Movement Scale (AIMS). Secondary: Side effects of CBD; improvement in psychotic symptoms. |
| Starting date | December 2015 |
| Contact information | Dr Jaiyeola Kajero, +234 08037140976, jaiyeolakajero@yahoo.com, Nigeria |
| Notes | Sponsor: South Africa Research Chair in PTSD, Stellenbosch University |
NCT00621634 2008.
| Trial name or title | Efficacy of docosahexaenoic acid on tardive dyskinesia |
| Methods | Allocation: randomised. Blindness: double‐blind (Participant, Investigator, Outcomes Assessor). Duration: 12 weeks. Design: parallel. Setting: Canada |
| Participants | Diagnosis: chronic schizophrenia; under long‐term antipsychotic drug treatment, stable for at least 3 months before study entry; presence of TD following Schooler‐Kane research criteria (mild intensity (2/4 points) in at least two body segments, or moderate intensity (3/4 points) for at least one body segment). N = 40 Sex: male and female Age: 30‐75 years |
| Interventions | 1. Omega‐3 fish oil capsules (including docosahexaenoic acid): Fish oil capsules of 1000 mg each, including DHA 460 mg‐540 mg/capsule; dose: 6 capsules per day; N = 20. 2. Placebo: Corn/Soybean placebo 1000 mg capsules; dose: 6 capsules per day; N = 20. |
| Outcomes | Primary: Clinical rating scales (AIMS, St.Hans) Secondary: Quantitative motor testing (kinematic parameters); Monitoring of psychopathology (Neuro‐Psychiatric Inventory, Positive and Negative Syndrome Scale, Calgary Depression Scale for Schizophrenia); Erythrocyte membrane phospholipid profile (gas chromatography) |
| Starting date | February 2008 |
| Contact information | Pierre J. Blanchet, MD, PhD, (514) 890‐8123, Pierre.J.Blanchet@umontreal.ca |
| Notes | Sponsor: Université de Montréal, National Alliance for Research on Schizophrenia and Depression Study IDs: NCT00621634; HD06.067 |
NCT01391390 2011.
| Trial name or title | Melatonin treatment for tardive dyskinesia in schizophrenia. |
| Methods | Allocation: randomised Blindness: double‐blind (Subject, Investigator) Duration: 12 weeks Design: parallel Setting: China |
| Participants | Diagnosis: diagnosis of both schizophrenia and TD; duration of TD symptoms longer than 1 year; on stable doses of antipsychotic drug for at least 6 months. N = 120 Sex: male and female Age: 18 to 70 years old |
| Interventions | 1. Melatonin (other Name: APRD00742)10mg/day, 12‐week treatment. N = 60. 2. Placebo 10mg/day, 12‐week treatment. N = 60 |
| Outcomes | Primary: AIMS at 12 weeks Secondary: the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS); the Positive and Negative Syndrome Scale (PANSS); the Simpson‐Angus Scale for extrapyramidal side effects (SAS) |
| Starting date | September 2008 |
| Contact information | Lian Y Cao, MD, Beijing Hui‐Long‐Guan Hospital |
| Notes | Sponsor: Beijing HuiLongGuan Hospital, Stanley Medical Research Institute Other study ID: BJ‐7072035 |
NCT01688037 2012.
| Trial name or title | NBI‐98854 for the for the treatment of tardive dyskinesia in subjects with schizophrenia or schizoaffective disorder (KINECT study) |
| Methods | Allocation: randomised Blindness: double‐blind (Subject, Caregiver, Investigator, Outcomes Assessor) Duration: 6 weeks Design: parallel Setting: USA, Puerto Rico |
| Participants | Diagnosis: Clinical diagnosis of schizophrenia or schizoaffective disorder and a clinical diagnosis of antipsychotic‐induced TD for at least 3 months prior to screening;receiving a stable dose of antipsychotic medication for a minimum of 30 days before study start; participants not using antipsychotic medication must have stable psychiatric status;the doses of concurrent medications and the conditions being treated be stable for a minimum of 30 days before study start and be expected to remain stable during the study. N = 109 Sex: male and female Age: 18 to 65 years old |
| Interventions | 1. NBI‐98854 50 mg administered as two 25 mg capsules by mouth, taken every morning for 6 weeks. N = NR 2. NBI‐98854 100 mg and 50 mg. NBI‐98854 100 mg administered as two 50 mg capsules taken every morning between for 2 weeks. After 2 weeks, NBI‐98854 50 mg administered by two 25 mg capsules by mouth, taken every morning for remaining 4 weeks. N = NR 3. Placebo capsule containing no active substance, manufactured to mimic NBI‐98854 25 mg and 50 mg capsules. N = NR |
| Outcomes | Primary: Severity of TD symptoms assessed by AIMS Secondary: CGI‐TD; Number of participants with adverse events following dosing with NBI‐98854; Evaluation of plasma concentrations of NBI‐98854 and metabolites following repeated daily doses (50 mg and 100 mg) of NBI‐98854 |
| Starting date | September 2012 |
| Contact information | Principal Investigator: Chris O'Brien, MD |
| Notes | Other study ID: NBI‐98854‐1201 Sponsor: Neurocrine Biosciences |
NCT01804920 2013.
| Trial name or title | D‐Serine treatment for tardive dyskinesia |
| Methods | Allocation: randomised Blindness: double‐blind (Subject, Investigator, Outcomes Assessor) Duration: 8 weeks Design: parallel Setting: Israel |
| Participants | Diagnosis: Diagnosis of schizophrenia/schizoaffective disorder according to DSM‐IV criteria; history of at least 3 months antipsychotic drugs treatment and present stable dose antipsychotic treatment for at last 4 weeks; fulfilment of Schooler‐Kane TD research criteria on a first evaluation performed 2‐12 weeks prior to study entrance and on a subsequent evaluation performed prior to allocation to experimental treatment. N = 60 Sex: male and female Age: 18 to 70 years old |
| Interventions | 1. D‐Serine (amino acid) 4 g/dN for 8 weeks. N = 30 2. Placebo adjuvant treatment for 8 weeks. N = 30 |
| Outcomes | Primary: Change in AIMS total score |
| Starting date | January 2013 |
| Contact information | Contact: Uriel Heresco‐Levy, MD, +972‐2‐5316906, urielh@ekmd.huji.ac.il |
| Notes | Other Study ID Numbers: 1600 |
NCT02291861 2014.
| Trial name or title | Addressing involuntary movements in tardive dyskinesia (AIM‐TD) |
| Methods | Allocation: randomised. Blindness: double‐blind (Subject, Investigator, Outcomes Assessor). Duration: 12 weeks Design: parallel. Setting: USA, Czech Republic, Germany, Hungary, Poland, Slovakia |
| Participants | Diagnosis: History of using a dopamine receptor antagonist for at least 3 months; clinical diagnosis of TD and has had symptoms for at least 3 months prior to screening, participants with underlying psychiatric diagnosis are stable and have no change in psychoactive medications. N = 288 Sex: male and female Age: 18 to 80 years old |
| Interventions | 1. SD‐809 12 mg tablets dose titrated for 4 weeks to target randomised dose. The dose is maintained for an additional 8 weeks. N = 72 2. SD‐809 24 mg tablets dose titrated for 4 weeks to target randomised dose. The dose is maintained for an additional 8 weeks. N = 72 3. SD‐809 36 mg tablets dose titrated for 4 weeks to target randomised dose. The dose is maintained for an additional 8 weeks. N = 72 4. Placebo tablets taken twice daily for 12 weeks. N = 72 |
| Outcomes | Primary: Change in AIMS score from Baseline to Week 12 Secondary:Quality of Life; treatment success based on Patient Global Impression of Change (PGIC) questionnaire; percentage reduction in AIMS score; proportion of responders based on AIMS score change from baseline. |
| Starting date | October 2014 |
| Contact information | Teva US Medical Information (+1‐800‐896‐5855) |
| Notes | Auspex Pharmaceuticals, Inc. Other Study ID Numbers: SD‐809‐C‐23 |
AIMS ‐ Abnormal Involuntary Movement Scale CGI ‐ Clinical Global Impression DHA ‐ docosahexaenoic acid DSM ‐ Diagnostic and Statistical Manual of Mental Disorders ICD ‐ International Classification of Diseases PGIC ‐ Patient Global Impression of Change TD = tardive dyskinesia
Differences between protocol and review
The protocol as published with this review has evolved over time. The revisions of protocol are in line with the development of RevMan and in keeping with Cochrane guidance. We think the revisions have greatly improved and enhanced this review. We do not think, however, that it has materially affected our conduct of the review or interpretation of the results.
There was a substantial update to the protocol in the 2016 review update with main changes being to:
change the title from 'Miscellaneous treatments for neuroleptic‐induced tardive dyskinesia';
broaden the inclusion criteria by adding the comparison: 'Any intervention compared with any other intervention for the treatment of tardive dyskinesia';
rename and update list of important outcomes following consultation with consumers;
prioritise comparisons for 'Summary of findings' tables: 'Summary of findings' tables were created only for those comparisons that: 1) included more than 60 participants, or 2) included more than one trial;
we analysed outcomes using risk ratios (see Methods) ‐ rather than odds ratios.
The previous methods are reproduced in Appendix 1; Appendix 2, and Appendix 3.
Contributions of authors
Karla Soares‐Weiser (KSW) ‐ protocol development, searching, study selection, data extraction and assimilation, report writing ‐ all versions.
John Rathbone (JR ‐ helped update review in 2009
Hanna Bergman (HB) ‐ updated review in 2017
Sources of support
Internal sources
CAPES ‐ Ministry of Education, Brazil, Brazil.
Universidade Federal de Sao Paulo, Brazil, Brazil.
Cochrane Schizophrenia Group, UK.
-
Enhance Reviews Ltd., UK.
Logistics support for Hanna Bergman for the 2016 update.
External sources
-
NIHR HTA Project Grant, reference number: 14/27/02, UK.
Salary support for Hanna Bergman. Support for patient involvement consultation.
Declarations of interest
KSW is the Deputy Editor‐in‐Chief for Cochrane and Cochrane Innovations. When the NHIR HTA programme grant relevant to this review update was awarded, KSW was the Managing Director of Enhance Reviews Ltd.
JR ‐ none known.
HB worked for Enhance Reviews Ltd. during preparation of this review and was paid for her contribution to this review. Enhance Reviews Ltd. is a private company that performs systematic reviews of literature. HB works for Cochrane Response, an evidence consultancy linked to Cochrane that take commissions from healthcare guideline developers and policy makers.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Bucci 1971 {published data only}
- Bucci L. The dyskinesias: a new approach. Diseases of the Nervous System 1971;32(5):324‐7. [PubMed] [Google Scholar]
Cai 1988 {published data only}
- Cai N. A controlled study on the treatment of tardive dyskinesia using 1‐stepholidine. Chinese Journal of Neurology and Psychiatry 1988;21(5):281‐3. [PubMed] [Google Scholar]
Castro 2011 {published data only}
- Castro F, Carrizo E, Prieto de Rincon D, Rincon CA, Asian T, Medina‐Leendertz S, et al. Effectiveness of melatonin in tardive dyskinesia. Investigación Clínica 2011;52(3):252‐60. [PubMed] [Google Scholar]
Emsley 2006 {published data only}
- Elmsley R, Oosthuizen PP. Double‐blind, randomized, parallel‐group comparison of ethyl‐eicosapentaenoic acid (ethyl‐EP A) versus placebo as add‐on medication in 84 patients with established tardive dyskinesia. Stanley Foundation Research Programs 2002.
- Emsley R. A double‐blind, randomised, parallel‐group comparison of ethyl‐eicosapentaenoic acid (ethyl‐epa) versus placebo as add‐on medication in patients with established tardive dyskinesia. https://clinicaltrials.gov/ct2/show/NCT00114595 2005.
- Emsley R. Ethyl eicosapentanoic acid for tardive dyskinesia. Stanley Foundation Research Programs 2009.
- Emsley R, Niehaus DJH, Koen L, Oosthuizen PP, Turner HJ, Carey P, et al. The effects of eicosapentaenoic acid in tardive dyskinesia: a randomized, placebo‐controlled trial. Schizophrenia Research 2006;84(1):112‐20. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Emsley R, Niehaus DJH, Oosthuizen PP, Koen L, Ascott‐Evans B, Chiliza B, et al. Safety of the omega‐3 fatty acid, eicosapentaenoic acid (EPA) in psychiatric patients: results from a randomized, placebo‐controlled trial. Psychiatry Research 2008;161(3):284‐91. [DOI] [PubMed] [Google Scholar]
Gardos 1979 {published data only}
- Gardos G, Granacher RP, Cole JO, Sniffin C. The effects of papaverine in tardive dyskinesia. Progress in Neuro‐Psychopharmacology & Biological Psychiatry 1979;3(5‐6):543‐50. [DOI] [PubMed] [Google Scholar]
Glazer 1985 {published and unpublished data}
- Glazer WM, Naftolin F, Morgenstern H, Barnea ER, MacLusky NJ, Brenner LM. Estrogen replacement and tardive dyskinesia. Psychoneuroendocrinology 1985;10(3):345‐50. [DOI] [PubMed] [Google Scholar]
Glover 1980 {published data only}
- Glover O. Alternative treatment modalities for drug induced psychomotor dysfunctions. PhD dissertation submitted to the Wright Institute 1980:150.
Goff 1993 {published data only}
- Goff DC, Renshaw PF, Sarid‐Segal O, Dreyfuss DA, Amico ET, Ciraulo DA. A placebo‐controlled trial of selegiline (L‐deprenyl) in the treatment of tardive dyskinesia. Biological Psychiatry 1993;33(10):700‐6. [DOI] [PubMed] [Google Scholar]
Hajioff 1983 {published data only}
- Hajioff J, Wallace M. Effect of Co‐dergocrine mesylate on tardive dyskinesia. A preliminary report. Psychopharmacology 1983;79(1):1‐3. [DOI] [PubMed] [Google Scholar]
Kojima 1992 {published data only}
- Kojima T, Yamauchi T, Miyasaka M, Isaki K, Nakane Y, Takahashi R, et al. Treatment of tardive dyskinesia with ceruletide: a double‐blind placebo‐controlled study. Saishin‐Igaku 1989;44(10):2177‐88. [DOI] [PubMed] [Google Scholar]
- Kojima T, Yamauchi T, Miyasaka M, Koshino Y, Nakane Y, Takahashi R, et al. Treatment of tardive dyskinesia with ceruletide: a double‐blind, placebo‐controlled study. Psychiatry Research 1992;43(2):129‐36. [DOI] [PubMed] [Google Scholar]
Koshino 1979 {published data only}
- Koshino Y, Kurata K, Hosokawa K, Yamaguchi N. Double‐blind trial of cyproheptadine on neuroleptic induced tardive dyskinesia. Clinical Psychiatry [Seishin Igaku] 1979;21(4):421‐6. [Google Scholar]
Koshino 1983 {published data only}
- Koshino Y, Hiramatsu H, Isaki K, Yamaguchi N. A double‐blind clinical trial of dihydrogenated ergot alkaloids in antipsychotic‐induced tardive dyskinesia. Clinical Psychiatry [Seishin Igaku] 1983;25(6):627‐35. [Google Scholar]
Libov 2007 {published data only}
- Anon. Piracetam reduces TD symptomstardive dyskinesia. Brown University Psychopharmacology Update 2007;18(11):3‐4. [Google Scholar]
- Lerner V. Piracetam for tardive dyskinesia. Stanley Foundation Research Programs 2009.
- Libov I, Miodownik C, Bersudsky Y, Dwolatzky T, Lerner V. Efficacy of piracetam in the treatment of tardive dyskinesia in schizophrenic patients: a randomized, double‐blind, placebo‐controlled crossover study. Journal of Clinical Psychiatry 2007;68(7):1031‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- NCT00190008. Therapeutic use of piracetam for treatment of patients suffering from tardive dyskinesia ‐ a double blind, placebo‐controlled crossover study. http://www.clinicaltrials.gov. 2005.
Mackay 1980 {published data only}
- Mackay AVP, Sheppard GP, Saha BK, Motley B, Johnson L, Marsden CD. Failure of lithium treatment in established tardive dyskinesia. Psychological Medicine 1980;10(3):583‐7. [DOI] [PubMed] [Google Scholar]
Matsunaga 1988 {published and unpublished data}
- Matsunaga T, Ohyama S, Takehara S, Kabashima K, Moriyama S, Tsuzuki J, et al. The effect of ceruletide on tardive dyskinesia: a double‐blind placebo‐controlled study. Progress in Neuro‐Psychopharmacology and Biological Psychiatry 1988;12(4):533‐9. [DOI] [PubMed] [Google Scholar]
Meco 1989 {published data only}
- Meco G, Bedini L, Bonifati V, Sonsini U. Ritanserin in tardive dyskinesia: A double‐blind crossover study versus placebo. Current Therapeutics Research 1989;46(5):884‐94. [Google Scholar]
Mosnik 1997 {published data only}
- Mosnik DM. Phenylalanine loading effects on tardive dyskinesia severity in schizophrenics. Master of Science dissertation submitted to the Finch University of Health Sciences, USA. 1994.
- Mosnik DM, Spring B, Rogers K, Baruah S. Tardive dyskinesia exacerbated after ingestion of phenylalanine by schizophrenic patients. Neuropsychopharmacology 1997;16(2):136‐46. [DOI] [PubMed] [Google Scholar]
- Mosnik DM, Spring B, Rogers K, Baruah S, Waziri R. Phenylalanine loading effects on tardive dyskinesia severity in schizophrenics. Schizophrenia Research 1995;15(1, 2):208. [Google Scholar]
Mouret 1991 {published and unpublished data}
- Mouret J, Khomais M, Lemoine P, Sebert P. Low doses of insulin as a treatment of tardive dyskinesia: conjuncture or conjecture?. European Neurology 1991;31(4):199‐203. [DOI] [PubMed] [Google Scholar]
O'Brien 2014 {published data only}
- Factor S, Hauser R, Mandri D, Castro‐Gayol J, Jimenez R, Siegert S, et al. A Phase 2 Study of valbenazine (NBI‐98854) for treatment of tardive dyskinesia: KINECT 2. Neurology 2016;86(16 SUPPL. 1):S27.007. [Google Scholar]
- NCT01733121. Nbi‐98854 dose titration study for the treatment of tardive dyskinesia. http://ClinicalTrials.gov/show/NCT01733121 (accessed on 6 October 2017) 2012.
- O'Brien CF, Jimenez R, Hauser RA, Factor SA, Burke J, Mandri D, et al. NBI‐98854, A selective monoamine transport inhibitor for the treatment of tardive dyskinesia: A randomized, double‐blind, placebo‐controlled study. Movement Disorders 2015;30(12):1681‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Brien CF, Jimenez R, Hauser RA, Factor SA, Mandri DF, Castro‐Gyol JC. Kinect 2: NBI‐98854 treatment of moderate to severe tardive dyskinesia. 18th International Congress of Parkinson's Disease and Movement Disorders, Stockholm, Sweden June 8‐12 2014;29:S305‐S306. [Google Scholar]
Rastogi 1982 {published data only}
- Rastogi SC, Blowers AJ, Gibson AC. Co‐dergocrine (hydergine) in the treatment of tardive dyskinesia. Psychological Medicine 1982;12(2):427‐9. [DOI] [PubMed] [Google Scholar]
Richardson 2003 {published data only}
- Richardson MA, Bevans ML, Read LL, Chao HM, Clelland JD, Suckow RF, et al. Efficacy of the branched‐chain amino acids in the treatment of tardive dyskinesia in men. American Journal of Psychiatry 2003;160(6):1117‐24. [DOI] [PubMed] [Google Scholar]
Shamir 2000 {published data only}
- Shamir E, Barak Y, Plopsky I, Zisapel N, Elizur A, Weizman A. Is melatonin treatment effective for tardive dyskinesia?. Journal of Clinical Psychiatry 2000;61(8):556‐8. [DOI] [PubMed] [Google Scholar]
Shamir 2001 {published data only}
- Shamir EZ, Barak F, Shalman I, Landon N, Zisapel N, Elizur A, et al. Melatonin treatment for tardive dyskinesia: a double‐blind, placebo‐controlled, cross‐over study. Annual Meeting of the American Psychiatric Association; 2001 May 5‐10; LA, USA. 2001.
- Shamir EZ, Barak F, Shalman I, Landon N, Zisapel N, Elizur A, et al. Melatonin treatment for tardive dyskinesia: a double‐blind, placebo‐controlled, cross‐over study. Archives of General Psychiatry 2001;58:1049‐52. [DOI] [PubMed] [Google Scholar]
Shi 2009 {published data only}
- Shi X, Zhu F, Zhang X, Zjang J, Zhang X, Wei L, et al. Melatonin in treatment of schizophrenia with tardive dyskinesia: A comparison study of cognitive function. Linchuang Jingshen Yixue Zazhi 2009;19(6):391‐3. [Google Scholar]
UCB Pharma 2005 {published data only}
- NCT00175955. An 8‐week exploratory, double‐blind, placebo controlled, randomized trial ‐ evaluation of the efficacy and safety of levetiracetam up to 3000 mg/day (250‐500 mg oral tablets in bid administration) on neuroleptic‐induced tardive dyskinesia in subjects with stable axis I psychiatric disorder, aged from at least 18 years to 80 years. https://clinicaltrials.gov/ct2/show/NCT00175955 2005.
Wolkin 1986 {published data only}
- Wolkin A, Jordan B, Peselow E, Rubinstein M, Rotrosen J. Essential fatty acid supplementation in tardive dyskinesia. American Journal of Psychiatry 1986;143(7):912‐4. [DOI] [PubMed] [Google Scholar]
Woods 2008 {published data only}
- NCT00291213. Levetiracetam treatment of tardive dyskinesia. www.Clinical Trials.gov (https://clinicaltrials.gov/ct2/show/NCT00291213) 2006.
- Woods SW, Saksa JR, Baker CB, Cohen SJ, Tek C. Effects of levetiracetam on tardive dyskinesia: A randomized, double‐blind, placebo‐controlled study. Journal of Clinical Psychiatry 2008;69(4):546‐54. [DOI] [PubMed] [Google Scholar]
Yang 1999 {published data only}
- Yang X, Meng F, Cui Y, Yang P, Liu R, Ma L, et al. Promethazine treatment of tardive dyskinesia: a double blind placebo controlled study. Chinese Mental Health Journal 1999;13:365‐7. [Google Scholar]
Zeng 1995 {published data only}
- Zeng Z‐X. Treatment of tardive dyskinesia with buspirone. Medical Journal of Chinese Civil Administration 1995;7:202‐3. [Google Scholar]
Zeng 1996 {published data only}
- Zeng ZX. Pemoline in the treatment of tardive dyskinesia. Chinese Journal of New Drugs and Clinical Remedies 1996;15:240‐1. [Google Scholar]
Zhang 2011 {published data only}
- NCT00672373. Extract of ginkgo biloba and tardive dyskinesia. www.ClinicalTrials.gov (https://clinicaltrials.gov/ct2/show/NCT00672373?term=NCT00672373&rank=1) 2008.
- Zhang F, Bigos K, Weinberger D. Genome‐wide analysis of antipsychotic drug response in schizophrenia. Proceedings of the 50th Annual Meeting of the American College of Neuropsychopharmacology; 2011 Dec 4‐8; Waikoloa, Hawaii. 2011; Vol. 50:135.
- Zhang WF, Tan YL, Zhang XY, Chan RC, Wu HR, Zhou DF. Extract of Ginkgo biloba treatment for tardive dyskinesia in schizophrenia: a randomized, double‐blind, placebo‐controlled trial. Journal of Clinical Psychiatry 2011;72(5):615‐21. [DOI: 10.4088/JCP.09m05125yel] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Apseloff 2000 {published data only}
- Apseloff G, Mullet D, Wilner KD, Anziano RJ, Tensfeldt TG, Pelletier SM, et al. The effects of ziprasidone on steady‐state lithium levels and renal clearance of lithium. British Journal of Clinical Pharmacology 2000;49(S1):61‐4S. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bjorndal 1980 {published data only}
- Bjorndal N, Casey DE, Gerlach J. Enkephalin, morphine, and naxoxone in tardive dyskinesia. Psychopharmacology 1980;69:133‐6. [DOI] [PubMed] [Google Scholar]
Blum 1984 {published data only}
- Blum I, Munitz H, Shalev A, Roberts E. Naloxone may be beneficial in the treatment of tardive dyskinesia. Clinical Neuropharmacology 1984;7(3):265‐7. [PubMed] [Google Scholar]
- Blum I, Nisipeanu PF, Roberts E. Naloxone in tardive dyskinesia. Psychopharmacology Berlin 1987;93(4):538. [DOI] [PubMed] [Google Scholar]
Bockenheimer 1976 {published data only}
- Bockenheimer S, Lucius G. Deanol in tardive dyskinesia: a double‐blind study [Zur Therapie mit Dimethylaminoathanol (Deanol) bei neuroleptikainduzierten extrapyramidalen Hyperkinesen]. Archiv für Psychiatrie und Nervenkrankheiten 1976;222(1):69‐75. [DOI] [PubMed] [Google Scholar]
Bowers 1979 {published data only}
- Bowers MB Jr, Moore D, Tarsy D. Tardive dyskinesia: a clinical test of the supersensitivity hypothesis. Psychopharmacology Berlin 1979;61(2):137‐1. [DOI] [PubMed] [Google Scholar]
Casey 1981 {published data only}
- Blum I, Nisipeanu PF, Roberts E, Casey DE, Korsgaard S, Gerlach J. Des‐tyr‐gamma‐endorphin in tardive dyskinesia. Proceedings of the 3rd World Congress of Biological Psychiatry 1981 Jun 28‐Jul 3; Stockholm, Sweden;93:538. [Google Scholar]
- Casey DE, Korsgaard S, Gerlach J. Des‐tyr‐gamma‐endorphin in tardive dyskinesia. Proceedings of the World Congress of Biological Psychiatry; 1981 June 28‐ July 3rd; Stockholm, Sweden. 1981.
- Casey DE, Korsgaard S, Gerlach J, Jorgensen A, Simmelsgaard H. Effect of des‐tyrosine‐gamma ‐endorphin in tardive dyskinesia. Archives of General Psychiatry 1981;38(2):158‐60. [DOI] [PubMed] [Google Scholar]
Chaplin 2002 {published data only}
- Chaplin R, Kent A. Informing patients about tardive dyskinesia: controlled trial of patient education. British Journal of Psychiatry 1998;172:78‐81. [DOI] [PubMed] [Google Scholar]
- Chaplin R, Timehin C. Informing patients about tardive dyskinesia: Four‐year follow up of a trial of patient education. Australian and New Zealand Journal of Psychiatry 2002;36(1):99‐103. [DOI: ] [DOI] [PubMed] [Google Scholar]
- Chaplin R, Zipursky RB. An educational session on tardive dyskinesia increased patients' knowledge at 6 months without affecting compliance or clinical stability. Evidence‐Based Medicine 1998;3:153. [Google Scholar]
Emsley 2002 {published data only}
- Emsley R, Myburgh C, Oosthuizen P, Rensburg SJ. Randomized, placebo‐controlled study of ethyl‐eicosapentaenoic acid as supplemental treatment in schizophrenia. American Journal of Psychiatry 2002;159(9):1596‐8. [DOI] [PubMed] [Google Scholar]
Fann 1973 {published data only}
- Fann WE, Davis JM, Wilson IC. Methylphenidate in tardive dyskinesia. American Journal of Psychiatry 1973;130(8):922‐4. [DOI] [PubMed] [Google Scholar]
Fudge 1991 {published data only}
- Fudge RC, Thailer SA, Alpert M, Intrator J, Sison CE. The effects of electromyographic feedback training on suppression of the oral‐lingual movements associated with tardive dyskinesia. Biofeedback and Self‐Regulation 1991;16(2):117‐29. [DOI] [PubMed] [Google Scholar]
Gardos 1978 {published data only}
- Gardos G, Cole JO. Pilot study of cyproheptadine (Periactin) in tardive dyskinesia. Psychopharmacolgy Bulletin 1978;14(2):18‐20. [PubMed] [Google Scholar]
Gerlach 1975 {published data only}
- Gerlach J, Thorsen K, Munkvad I. Effect of lithium on neuroleptic‐induced tardive dyskinesia compared with placebo in a double‐blind cross‐over trial. Pharmakopsychiatrie, Neuro‐Psychopharmakologie 1975;8(2):51‐6. [DOI: 10.1055/s-0028-1094443] [DOI] [PubMed] [Google Scholar]
Goetz 2013 {published data only}
- Goetz C, Stebbins G, Chung K, Hauser R, Miyasaki J, Nicholas A, et al. No PD dyskinesia scale protects against placebo responses: A comparison of multiple scales. Neurology 2013;80(7):Supplement P04.187. [Google Scholar]
- Goetz CG, Stebbins GT, Chung KA, Hauser RA, Miyasaki JM, Nicholas AP, et al. No PD dyskinesia scale protects against placebo responses: A comparison of seven scales. Movement disorders 2013;28:S115‐6. [DOI] [PubMed] [Google Scholar]
Huang 1981 {published data only}
- Huang CC, Wang RIH, Hasegawa A, Alverno L. Evaluation of reserpine and alpha‐methyldopa in the treatment of tardive dyskinesia. Psychopharmacology Bulletin 1980;16:41‐3. [PubMed] [Google Scholar]
- Huang CC, Wang RIH, Hasegawa A, Alverno L. Reserpine and alpha‐methyldopa in the treatment of tardive dyskinesia. Psychopharmacology 1981;73:359‐62. [DOI] [PubMed] [Google Scholar]
Jus 1974 {published data only}
- Jus K, Jus A, Gautier J, Villeneuve A, Pires P, Pineau R, et al. Studies on the action of certain pharmacological agents on tardive dykinesia and on the rabbit syndrome. International Journal of Clinical Pharmacology 1974;9(2):138‐45. [PubMed] [Google Scholar]
Jus 1978 {published data only}
- Jus A, Villeneuve A, Gautier J, Jus C, Villeneuve P, Pires P, et al. Deanol, lithium and placebo in the treatment of tardive dyskinesia: A double‐blind crossover study. Neuropsychobiology 1978;4:140‐9. [DOI] [PubMed] [Google Scholar]
Kabes 1982 {published data only}
- Kabes J, Sikora J Pisvejc J Skoudia V. Piracetam action in neuroleptic induced extrapyramidal side‐effects. Proceedings of the 12th CINP congress; Supplement to Progress in Neuropsychopharmacology. Pergamon Press, 1980.
- Kabes J, Sikora J, Pisvejc J, Hanzlicek L, Skondia V. Effect of piracetam on extrapyramidal side effects induced by neuroleptic drugs. International Pharmacopsychiatry 1982;17(3):185‐92. [PubMed] [Google Scholar]
- Kabes J, Sikora J, Pisvejc J, Skoudia V. Piracetam action in neuroleptic induced extrapyramidal side‐effects. Proceedings of the 12th Collegium Internationale Neuro‐Psychopharmacologicum Congress; 1980 Jun 22‐26; Goteborg, Sweden. 1980.
- Kabes J, Sikora J, Stary O, Piisvejc J, Hanzlicek L. Piracetam effectivity in tardive dyskinesia. A double‐blind placebo‐controlled cross‐over trial. Ceskoslovenska Psychiatrie 1983;79(5):339‐45. [PubMed] [Google Scholar]
- Sikora J, Kabes J, Pisvejc J. Management of neuroleptic side‐effects with piracetam. Ceskoslovenska Psychiatrie 1981;77(2):137‐42. [PubMed] [Google Scholar]
Kabes 1985 {published data only}
- Kabes J, Sikora J, Stary O, Pisvejc J. Dose‐dependent effect of piracetam in tardive‐dyskinesia ‐ double‐blind placebo controlled trial. Activitas Nervosa Superior 1985;27(1):64‐6. [Google Scholar]
Koller 1982 {published data only}
- Koller WC, Barr A, Biary N. Estrogen treatment of dyskinetic disorders. Neurology 1982;32(5):547‐9. [DOI] [PubMed] [Google Scholar]
Korsgaard 1981 {published data only}
- Korsgaard S, Casey DE, Damgaard‐Pedersen NE, Jorgensen A, Gerlach J. Vasopressin in anergic schizophrenia: a cross‐over study with lysine‐8‐vasopressin and placebo. Psychopharmacology 1981;74(4):379‐82. [DOI] [PubMed] [Google Scholar]
Lieberman 1987 {published data only}
- Lieberman JA, Kane JM, Sarantakos S, Gadaleta D, Woerner M, Alvir J, et al. Prediction of relapse in schizophrenia. Archives of General Psychiatry 1987;44:597‐603. [DOI] [PubMed] [Google Scholar]
Lieberman 1994 {published data only}
- Lieberman JA, Alvir J, Geisler S, Ramos Lorenzi J, Woerner M, Novacenko H, et al. Methylphenidate response, psychopathology and tardive dyskinesia as predictors of relapse in schizophrenia. Neuropyschopharmacology 1994;11:107‐18. [DOI] [PubMed] [Google Scholar]
Lindenmayer 1988 {published data only}
- Lindenmayer JP, Gardner E, Goldberg E, Opler LA, Kay SR, Praag HM, et al. High‐dose naloxone in tardive dyskinesia. Psychiatry Research 1988;26(1):19‐28. [DOI] [PubMed] [Google Scholar]
Moore 1980 {published data only}
- Moore DC, Bowers MB. Identification of a subgroup of tardive dyskinesia patients by pharmacologic probes. American Journal of Psychiatry 1980;137(10):1202‐5. [DOI] [PubMed] [Google Scholar]
Nasrallah 1986 {published data only}
- Nasrallah HA, Dunner FJ, McCalley Whitters M, Smith RE. Pharmacologic probes of neurotransmitter systems in tardive dyskinesia: implications for clinical management. Journal of Clinical Psychiatry 1986;47(2):56‐9. [PubMed] [Google Scholar]
Peselow 1989 {published data only}
- Peselow ED, Irons S, Rotrosen J, Alonso MT, Dorsey F. GM1 ganglioside as a potential treatment in tardive dyskinesia. Psychopharmacology Bulletin 1989;25(2):277‐80. [PubMed] [Google Scholar]
- Sommer BR, Cohen BM, Satlin A, Cole JO, Jandorf L, Dorsey F. Changes in tardive dyskinesia symptoms in elderly patients treated with ganglioside GM1 or placebo. Journal of Geriatric Psychiatry and Neurology 1994;7:234‐7. [DOI] [PubMed] [Google Scholar]
Prange 1973 {published data only}
- Prange A, Wilson JC, Morris CE, Hall CD. Preliminary experience with tryptophan and lithium in the treatment of tardive dyskinesia. Psychopharmacology Bulletin 1973;9:36‐7. [Google Scholar]
Reda 1974 {published data only}
- Reda FA, Escobar JJ, Scanlon JM. Lithium carbonate in the treatment of tardive dyskinesia. American Journal of Psychiatry 1975;132:560‐2. [DOI] [PubMed] [Google Scholar]
- Reda FA, Scanlon JM, Kem K, Escobar JJ. Treatment of tardive dyskinesia with lithium carbonate. New England Journal of Medicine 1974;291:850. [PubMed] [Google Scholar]
Reker 1982 {published data only}
- Reker D, Anderson B, Yackulic C, Cooper TB, Banay‐Schwartz M, Leon C, et al. Naloxone, tardive dyskinesia, and endogenous beta‐endorphin. Psychiatry Research 1982;7(3):321‐4. [DOI] [PubMed] [Google Scholar]
- Volavka J, Anderson B, Koz G. Naloxone and naltrexone in mental illness and tardive dyskinesia. Annals of New York Academy of Sciences 1982;398:97‐102. [DOI] [PubMed] [Google Scholar]
Shah 2012 {published data only}
- Shah BB, Connolly B, Mestre TA, Prashanth LK, Miyasaki JM, Steeves T, et al. Famotidine for the treatment of levodopa‐induced dyskinesia: An ongoing "N‐of‐1'' Study. 26th Annual Symposium on Etiology, Pathogenesis and Treatment of Movement Disorders. 2012.
Simpson 1976 a {published data only}
- Simpson GM, Branchey MH, Lee JH, Voitashevsky A, Zoubok B. Lithium in tardive dyskinesia. Pharmakopsychiatrie neuro‐psychopharmakologie 1976;9(2):76‐80. [DOI] [PubMed] [Google Scholar]
Simpson 1976 b {published data only}
- Simpson GM, Zoubok B, Lee JH. An early clinical and toxicity trial of EX 11‐582A in chronic schizophrenia. Current Therapeutic Research 1976;19(1):87‐98. [PubMed] [Google Scholar]
Tamminga 1983 {published data only}
- Nguyen JA, Thaker GK, Tamminga CA. Gamma‐aminobutyric‐acid (GABA) pathways in tardive dyskinesia. Psychiatric Annals 1989;19(6):302‐9. [Google Scholar]
- Tamminga CA, Thaker GK, Ferraro TN, Hare TA. GABA agonist treatment improves tardive dyskinesia. Lancet 1983;2:97‐8. [DOI] [PubMed] [Google Scholar]
- Tamminga CA, Thaker GK, Goldberg ST. Tardive dyskinesia: GABA agonist treatment. In: Usdin E, Carlsson A, Dahlstrom A, Engel J editor(s). Catecholamines: Neuropharmacology and Central Nervous System ‐ Therapeutic Aspects. New York: Alan R Liss, 1994. [Google Scholar]
Vaddadi 1989 {published data only}
- Vaddadi KS, Courtney P, Gilleard CJ, Manku M. A double blind trial of essential fatty acid supplementation in patients with tardive dyskinesia. Psychiatry Research 1989;27(3):313‐23. [DOI] [PubMed] [Google Scholar]
- Vaddadi KS, Gileard CJ. Essential fatty acids, tardive dyskinesia, and schizophrenia. Pathophysiology and Roles in Clinical Medicine. Wiley‐Liss, 1990:333‐43. [Google Scholar]
Vaddadi 2002 {published data only}
- Vaddadi KS, Soosai E, Chiu E, Dingjan P. A randomised, placebo‐controlled, double blind study of treatment of Huntington's disease with unsaturated fatty acids. Neuroreport 2002;13(1):29‐33. [DOI] [PubMed] [Google Scholar]
Villeneuve 1970 {published data only}
Villeneuve 1980 {published data only}
- Villeneuve A, Cazejust T, Cote M. Estrogens in tardive dyskinesia in male psychiatric patients. Neuropsychobiology 1980;6(3):145‐51. [DOI] [PubMed] [Google Scholar]
Volavka 1986 {published data only}
- Volavka J, O'Donnell J, Muragali R, Anderson BG, Gaztanaga P, Boggiano W, et al. Lithium and lecithin in tardive dyskinesia: an update. Psychiatry Research 1986;19(2):101‐4. [DOI] [PubMed] [Google Scholar]
Wonodi 2004 {published data only}
- Wonodi I, Adami H, Sherr J, Avila M, Hong LE, Thaker GK. Naltrexone treatment of tardive dyskinesia in patients with schizophrenia. Journal of Clinical Psychopharmacology 2004;24(4):441‐5. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Fernandez 2016 {published data only}
- EUCTR‐003135‐19‐PL. A randomized, double‐blind, placebo‐controlled, fixed‐dose study of sd‐809 (deutetrabenazine) for the treatment of moderate to severe tardive dyskinesia ‐ addressing involuntary movements in tardive dyskinesia (aim‐td) study. http://apps.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2014‐003135‐19‐PL 2014.
- Fernandez HH, Factor SA, Hauser RA, Jimenez‐Shahed J, Ondo W, LeDoux MS, et al. A randomized, double‐blind, placebo‐controlled trial of deutetrabenazine for the treatment of tardive dyskinesia (ARM‐TD). Movement Disorders 2016;31:S294. [Google Scholar]
- NCT02195700. A randomized, double‐blind, placebo‐controlled study of SD‐809 (Deutetrabenazine) for the treatment of moderate to severe tardive dyskinesia. www.Clinicaltrials.gov 2014.
Hauser 2016 {published data only}
- Factor SA, Hauser RA, Siegert S, Liang GS, O'Brien CF. KINECT 3: A randomized, double‐blind, placebo‐controlled phase 3 trial of valbenazine (NBI‐98854) for tardive dyskinesia. Movement Disorders 2016;31:S692. [Google Scholar]
- Grigoriadis D, Comella C, Remington G, Jimenez R, Burke J, Christopher O. Efficacy of Valbenazine (NBI‐98854) in in subjects with tardive dyskinesia: results of a long‐term extension study (KINECT 3 Extension). Neuropsychopharmacology 2016;41:S213‐4. [Google Scholar]
- Hauser R, Factor S, Marder S, Knesevich MA, Ramirez PM, Jimenez R, et al. KINECT 3: A randomized, double‐blind, placebo‐controlled phase 3 trial of valbenazine (NBI‐98854) for tardivedyskinesia. Neurology. 68th American Academy of Neurology Annual Meeting, 2016; Vol. 86 (16 SUPPL. 1).
- NCT02274558. A phase 3 study of NBI‐98854 for the treatment of tardive dyskinesia. https://clinicaltrials.gov/ct2/show/NCT02274558 (accessed on 6 October 2017) 2014.
NCT01393600 2011 {published data only}
- NCT01393600. Nbi‐98854 for the treatment of tardive dyskinesia in subjects with schizophrenia or schizoaffective disorder. www.Clinicaltrials.gov 2011.
Pattojoshi 2016 {published data only}
- Pattojoshi A, Khan AH, Lavania S. Effect of right DLPFC‐repetitive transcranial magnetic stimulation (rTMS) on tardive dyskinesia in patients with psychosis. Movement Disorders 2016;31:S691‐2. [Google Scholar]
Xu 2012 {published data only}
- Xu X. A randomized controlled study of Ginkgo biloba extract on tardive dyskinesia [银杏叶提取物治疗迟发性运动障碍的随机对照研究]. Journal of Chinese Physician 2012;14(6):843‐845. [Google Scholar]
References to ongoing studies
Garcia 1992 {published data only}
- Garcia G, Crismon ML. Double‐blind placebo controlled study using buspirone in the treatment of tardive dyskinesia. ASHP Midyear Clinical Meeting 1992;27:P‐91. [Google Scholar]
ISRCTN14688109 2015 {published data only}
- ISRCTN14688109. Investigation of the potential beneficial effects of cannabidiol in the treatment of tardive dyskinesia. http://www.isrctn.com 2015.
NCT00621634 2008 {published data only}
- NCT00621634. Efficacy of docosahexaenoic acid on tardive dyskinesia. www.Clinicaltrials.gov 2008.
NCT01391390 2011 {published data only}
- NCT01391390. Melatonin treatment for tardive dyskinesia in schizophrenia. www.Clinicaltrials.gov 2011.
NCT01688037 2012 {published data only}
- NCT01688037. NBI‐98854 for the treatment of tardive dyskinesia in subjects with schizophrenia or schizoaffective disorder (KINECT study). www.Clinicaltrials.gov 2012.
NCT01804920 2013 {published data only}
- NCT01804920. D‐Serine treatment for tardive dyskinesia. www.Clinicaltrials.gov 2013.
NCT02291861 2014 {published data only}
- NCT02291861. Addressing involuntary movements in tardive dyskinesia. www.ClinicalTrials.gov 2014.
Additional references
Alabed 2011
- Alabed S, Latifeh Y, Mohammad HA, Rifai A. Gamma‐aminobutyric acid agonists for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2011, Issue 4. [DOI: 10.1002/14651858.CD000203.pub3] [DOI] [PubMed] [Google Scholar]
Alimi 2013
- Alimi M, Gaillard P, Camus V, El‐Hage W. Treatment of tardive dyskinesia: A systematic review (1997‐2011). European Journal of Psychiatry 2013;27(3):160‐73. [Google Scholar]
Altman 1996
- Altman DG, Bland JM. Detecting skewness from summary information. BMJ 1996;313(7066):1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
APA 1992
- American Psychiatric Association. Tardive dyskinesia: a task force report of the American Psychiatric Association. American Psychiatric Association. Washington DC: American Psychiatric Association, 1992. [Google Scholar]
Armitage 1991
- Armitage P. Should we cross off the crossover?. Journal of Clinical Pharmacology 1991;32:1‐2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ascher‐Svanum 2008
- Ascher‐Svanum H, Zhu B, Faries D, Peng X, Kinon BJ, Tohen M. Tardive dyskinesia and the 3‐year course of schizophrenia: results from a large, prospective, naturalistic study. Journal of Clinical Psychiatry 2008;69:1580‐8. [DOI] [PubMed] [Google Scholar]
Ballesteros 2000
- Ballesteros J, Gonzalez‐Pinto A, Bulbena A. Tardive dyskinesia associated with higher mortality in psychiatric patients: results of a meta‐analysis of seven independent studies. Journal of Clinical Psychopharmacology 2000;20(2):188‐94. [DOI] [PubMed] [Google Scholar]
Barnes 1993
- Barnes TRE, Edwards JG. The side‐effects of antipsychotic drugs. I. CNS and neuromuscular effects. In: Barnes TRE editor(s). Antipsychotic Drugs and their Side‐effects. London: Academic Press. Harcourt Brace & Company, 1993. [Google Scholar]
Bergen 1984
- Bergen JA, Griffiths DA, Rey JM, Beumont PJV. Tardive dyskinesia: fluctuating patient or fluctuating rater. British Journal of Psychiatry 1984;144:498‐502. [DOI] [PubMed] [Google Scholar]
Bergen 1989
- Bergen JA, Eyland EA, Campbell JA. The course of tardive dyskinesia in patients on long‐term neuroleptics. British Journal of Psychiatry 1989;154:523‐8. [DOI] [PubMed] [Google Scholar]
Bergman 2017
- Bergman H, Walker DM, Nikolakopoulou A, Soares‐Weiser K, Adams CE. Systematic review of interventions for treating or preventing antipsychotic‐induced tardive dyskinesia. Health Technology Assessment 2017 Aug;21(43):1‐218. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bergman 2018
- Bergman H, Bhoopathi PS, Soares‐Weiser K. Benzodiazepines for antipsychotic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2018, Issue 1. [DOI: 10.1002/14651858.CD000205.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bergman 2018a
- Bergman H, Soares‐Weiser K. Anticholinergic medication for antipsychotic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2018, Issue 1. [DOI: 10.1002/14651858.CD000204.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bland 1997
- Bland JM. Statistics notes. Trials randomised in clusters. BMJ 1997;315:600. [DOI] [PMC free article] [PubMed] [Google Scholar]
Boissel 1999
- Boissel JP, Cucherat M, Li W, Chatellier G, Gueyffier F, Buyse M, et al. The problem of therapeutic efficacy indices. 3. Comparison of the indices and their use [Apercu sur la problematique des indices d'efficacite therapeutique, 3: comparaison des indices et utilisation. Groupe d'Etude des Indices D'efficacite]. Therapie 1999;54(4):405‐11. [PUBMED: 10667106] [PubMed] [Google Scholar]
Brooks 2017
- Brooks M. FDA OKs Deutetrabenazine (Austedo) for Tardive Dyskinesia. www.Medscape.com, available from: https://www.medscape.com/viewarticle/885051 (accessed on 13 Oct 2017) 2017.
Cadet 1989
- Cadet JL, Lohr JB. Possible involvement of free radical in neuroleptic‐induced movement disorders. Annals of the New York Academy of Sciences 1989;570:176‐85. [DOI] [PubMed] [Google Scholar]
Carpenter 1994
- Carpenter WT Jr, Buchanan RW. Schizophrenia. New England Journal of Medicine 1994;330:681‐90. [DOI] [PubMed] [Google Scholar]
Casey 1994
- Casey DE. Tardive dyskinesia: pathophysiology. In: Bloom FE, Kupfer DJ editor(s). Psychopharmacology. The Fourth Generation of Progress. New York: Raven Press, 1994. [Google Scholar]
Cavallaro 1993
- Cavallaro R, Regazzetti MG, Mundo E, Brancato V, Smeraldi E. Tardive dyskinesia outcomes: clinical and pharmacologic correlates of remission and persistence. Neuropsychopharmacology 1993;8(3):233‐9. [DOI] [PubMed] [Google Scholar]
Chong 2009
- Chong SA, Tay JA, Subramaniam M, Pek E, Machin D. Mortality rates among patients with schizophrenia and tardive dyskinesia. Journal of Clinical Psychopharmacology 2009;29(1):5‐8. [DOI] [PubMed] [Google Scholar]
Chouinard 2005
- Chouinard G, Margolese H. Manual for the Extrapyramidal Symptom Rating Scale (ESRS). Schizophrenia Research 2005;76:247‐65. [DOI] [PubMed] [Google Scholar]
Chouinard 2008
- Chouinard G, Chouinard VA. Atypical antipsychotics: CATIE study, drug‐induced movement disorder and resulting iatrogenic psychiatric‐like symptoms, supersensitivity rebound psychosis and withdrawal discontinuation syndromes. Psychotherapy and Psychosomatics 2008;77(2):69‐77. [DOI] [PubMed] [Google Scholar]
Clarke 2000
- Clarke M, Oxman AD. Cochrane Collaboration Handbook. The Cochrane Library [database on disk and CDROM]. The Cochrane Collaboration. Oxford: Update Software, 2000, issue 1.
Cloud 2014
- Cloud LJ, Zutshi D, Factor SA. Tardive dyskinesia: therapeutic options for an increasingly common disorde. Neurotherapeutics 2014;11(1):166‐76. [DOI] [PMC free article] [PubMed] [Google Scholar]
Correll 2004
- Correll CU, Leucht S, Kane JM. Lower risk for tardive dyskinesia associated with second‐generation antipsychotics: a systematic review of 1‐year studies. American Journal of Psychiatry 2004;161(3):414‐25. [DOI] [PubMed] [Google Scholar]
Correll 2008
- Correll CU, Schenka EM. Tardive dyskinesia and new antipsychotics. Current Opinion in Psychiatry 2008;21:151‐6. [DOI] [PubMed] [Google Scholar]
Deeks 2000
- Deeks J. Issues in the selection for meta‐analyses of binary data. Proceedings of the 8th International Cochrane Colloquium; 2000 Oct 25‐28; Cape Town. Cape Town: The Cochrane Collaboration, 2000.
Divine 1992
- Divine GW, Brown JT, Frazer LM. The unit of analysis error in studies about physicians' patient care behavior. Journal of General Internal Medicine 1992;7:623‐9. [DOI] [PubMed] [Google Scholar]
Donner 2002
- Donner A, Klar N. Issues in the meta‐analysis of cluster randomized trials. Statistics in Medicine 2002;21:2971‐80. [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315:629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
El‐Sayeh 2006
- El‐Sayeh HGG, Lyra da Silva JP, Rathbone J, Soares‐Weiser K. Non‐neuroleptic catecholaminergic drugs for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2006, Issue 1. [DOI: 10.1002/14651858.CD000458.pub2] [DOI] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne D, Altman DG, Higgins JPT, Curtina F, Worthingtond HV, Vaile A. Meta‐analyses involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [DOI] [PubMed] [Google Scholar]
Essali 2011
- Essali A, Deirawan H, Soares‐Weiser K, Adams CE. Calcium channel blockers for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2011, Issue 11. [DOI: 10.1002/14651858.CD000206.pub3] [DOI] [PubMed] [Google Scholar]
FDA 2017
- US Food, Drug Administration. FDA approves first drug to treat tardive dyskinesia. www.fda.gov, available from: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm552418.htm (accessed on 13 Oct 2017) 2017.
Fernandez 2001
- Fernandez HH, Krupp B, Friedman JH. The course of tardive dyskinesia and parkinsonism in psychiatric inpatients: 14‐year follow‐up. Neurology 2001;56:805‐7. [DOI] [PubMed] [Google Scholar]
Fleiss 1984
- Fleiss JL. The crossover study. The Design and Analysis of Clinical Experiments. Chichester: John Wiley & Sons, 1984. [Google Scholar]
Furukawa 2006
- Furukawa TA, Barbui C, Cipriani A, Brambilla P, Watanabe N. Imputing missing standard deviations in meta‐analyses can provide accurate results. Journal of Clinical Epidemiology 2006;59(7):7‐10. [DOI] [PubMed] [Google Scholar]
Gerlach 1993
- Gerlach J, Korsgaard S, Clemmesen P, Lauersen AML, Magelund G, Noring U, et al. The St. Hans Rating Scale for extrapyramidal syndromes: reliability and validity. Acta Psychiatrica Scandinavica 1993;87(4):244‐52. [DOI] [PubMed] [Google Scholar]
Glazer 1990
- Glazer WM, Morgenstern H, Schooler N, Berkman CS, Moore DC. Predictors of improvement in tardive dyskinesia following discontinuation of neuroleptic medication. British Journal of Psychiatry 1990;157:585‐92. [DOI] [PubMed] [Google Scholar]
Glazer 2000
- Glazer WM. Review of incidence studies of tardive dyskinesia associated with typical antipsychotics. Journal of Clinical Psychiatry 2000;61(suppl 4):15‐20. [PubMed] [Google Scholar]
Gulliford 1999
- Gulliford MC. Components of variance and intraclass correlations for the design of community‐based surveys and intervention studies: data from the Health Survey for England 1994. American Journal of Epidemiology 1999;149:876‐83. [DOI] [PubMed] [Google Scholar]
Guy 1976
- Guy W. ECDEU. Assessment Manual for Psychopharmacology, Revised. Washington DC: US Department of Health, Education and Welfare, 1976. [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2009
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.2 [updated September 2009] The Cochrane Collaboration, 2009. www.cochrane‐handbook.org 2009.
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.2 [updated September 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org..
Jeste 2000
- Jeste DV. Tardive dyskinesia in older patients. Journal of Clinical Psychiatry 2000;61(suppl 4):27‐32. [PubMed] [Google Scholar]
Jűni 2001
- Jűni P, Altman DG, Egger M. Systematic reviews in health care: assessing the quality of controlled clinical trials. BMJ 2001;323(7303):42‐6. [PUBMED: 11440947] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kane 1982
- Kane JM, Smith JM. Tardive dyskinesia: prevalence and risk factors, 1959 to 1979. Archives of General Psychiatry 1982;39:473‐81. [DOI] [PubMed] [Google Scholar]
Kay 1986
- Kay SR, Opler LA, Fiszbein A. Positive and Negative Syndrome Scale (PANSS) manual. North Tonawanda (NY): Multi‐Health Systems, 1986. [Google Scholar]
Kay 1987
- Kay S, Fiszbeln A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophrenia Bulletin 1987;13(2):261‐76. [DOI] [PubMed] [Google Scholar]
Leon 2006
- Leon AC, Mallinckrodt CH, Chuang‐Stein C, Archibald DG, Archer GE, Chartier K. Attrition in randomized controlled clinical trials: methodological issues in psychopharmacology. Biological Psychiatry 2006;59(11):1001‐5. [PUBMED: 16905632] [DOI] [PubMed] [Google Scholar]
Leucht 2005a
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. Clinical implications of Brief Psychiatric Rating Scale Scores. British Journal of Psychiatry 2005;187:366‐71. [DOI] [PubMed] [Google Scholar]
Leucht 2005b
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. What does the PANSS mean?. Schizophrenia Research 2005;79(2‐3):231‐8. [DOI] [PubMed] [Google Scholar]
Lieberman 1996
- Lieberman JA, Fleishhacker W. Introduction. British Journal of Psychiatry 1996;168(Supplement 29):7‐8. [Google Scholar]
Maher 2012
- Maher AR, Theodore G. Summary of the comparative effectiveness review on off‐label use of atypical antipsychotics. Journal of Managed Care Pharmacy 2012;18(5 Suppl B):S1‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Marshall 2000
- Marshall M, Lockwood A, Bradley C, Adams C, Joy C, Fenton M. Unpublished rating scales: a major source of bias in randomised controlled trials of treatments for schizophrenia. British Journal of Psychiatry 2000;176:249‐52. [DOI] [PubMed] [Google Scholar]
Martins 2011
- Martins ES, Rosso A, Coutinho E, Adams C, Huf G. Prevalence of tardive dyskinesia and all‐cause mortality amongst patients in a large psychiatric institute in Rio de Janeiro. Revista de Psiquiatria Clínica 2011;38:44. [Google Scholar]
Moher 2001
- Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel‐group randomised trials. Lancet 2001;357(9263):1191‐4. [PubMed] [Google Scholar]
Nelson 2003
- Nelson LA, McGuire JM, Hausafus SN. Melatonin for the treatment of tardive dyskinesia. Annals of Pharmacotherapy 2003;37(7):1128‐31. [DOI] [PubMed] [Google Scholar]
NICE 2014
- NICE. Psychosis and schizophrenia in adults: treatment and management. NICE clinical guideline 178 (guidance.nice.org.uk/cg178) 2014.
Overall 1962
- Overall JE, Gorham DR. The Brief Psychiatric Rating Scale. Psychological Reports 1962;10:799‐812. [Google Scholar]
Pocock 1983
- Pocock SJ. Crossover trials. Clinical trials. A Practical Approach. Chichester: John Wiley & Sons, 1983. [Google Scholar]
Rosvold 1956
- Rosvold HE, Mirsky AF, Sarason I, Bransome ED Jr, Beck LH. A continuous performance test of brain damage. Journal of Consulting Psychology 1956;20(5):343. [DOI] [PubMed] [Google Scholar]
Rust 1989
- Rust J, Golombok S. Modern Psychometrics. London: Routledge, 1989. [Google Scholar]
Sachdev 2000
- Sachdev P. The current status of tardive dyskinesia. Australian and New Zealand Journal of Psychiatry 2000;34(3):335‐69. [DOI] [PubMed] [Google Scholar]
Schmidt 1991
- Schmidt M, Meister P, Baumann P. Treatment of tardive dyskinesias with vitamin E. European Psychiatry 1991;6:201‐7. [Google Scholar]
Schooler 1993
- Schooler NR, Keith SJ. Clinical research for the treatment of schizophrenia. Psychopharmacology Bulletin 1993;29:431‐46. [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Shokraneh 2017
- Shokraneh F, Adams CE. Study‐based registers of randomized controlled trials: Starting a systematic review with data extraction or meta‐analysis. BioImpacts 2017;7(4):209‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
Simpson 1979
- Simpson GM, Lee JH, Soubok B, Gardos G. A rating scale for tardive dyskinesia. Psychopharmacology 1979;64:171‐9. [DOI] [PubMed] [Google Scholar]
Smith 1980
- Smith JM, Balessarini RJ. Changes in prevalence, severity and recovery in tardive dyskinesia with age. Archives of General Psychiatry 1980;37:1368‐73. [DOI] [PubMed] [Google Scholar]
Soares‐Weiser 2006
- Soares‐Weiser K, Rathbone J. Neuroleptic reduction and/or cessation and neuroleptics as specific treatments for tardive dyskinesia. Cochrane Database of Systematic Reviews 2006, Issue 1. [DOI: 10.1002/14651858.CD000459.pub2] [DOI] [PubMed] [Google Scholar]
Soares‐Weiser 2011
- Soares‐Weiser K, Maayan N, McGrath J. Vitamin E for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2011, Issue 2. [DOI: 10.1002/14651858.CD000209.pub2] [DOI] [PubMed] [Google Scholar]
Tammenmaa 2002
- Tammenmaa IA, McGrath JJ, Salias E, Soares‐Weiser K. Cholinergic medication for neuroleptic induced‐tardive dyskinesia. Cochrane Database of Systematic Reviews 2002, Issue 3. [DOI: 10.1002/14651858.CD000207] [DOI] [PubMed] [Google Scholar]
Tarsy 2011
- Tarsy D, Lungu C, Baldessarini RJ. Epidemiology of tardive dyskinesia before and during the era of modern antipsychotic drugs. Handbook of Clinical Neurology 2011;100:601‐16. [DOI] [PubMed] [Google Scholar]
Taylor 2009
- Taylor D, Paton C, Kapur S. The Maudsley Prescribing Guidelines (10th Edition). London: Informa Healthcare, 2009. [Google Scholar]
Ukoumunne 1999
- Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ. Methods for evaluating area‐wide and organistation‐based intervention in health and health care: a systematic review. Health Technology Assessment 1999;3(5):1‐75. [PubMed] [Google Scholar]
Wechsler 1945
- Wechsler D. Wechsler Memory Scale. San Antonio, TX: Psychological Corporation, 1945. [Google Scholar]
Wechsler 1958
- Wechsler D. The Measurement and Appraisal of Adult Intelligence (4th ed.). The Measurement and Appraisal of Adult Intelligence. 4th Edition. Baltimore, MD, US: Williams & Wilkins Co, 1958. [Google Scholar]
Xia 2007
- Xia J, Adams CE, Bhagat N, Bhagat V, Bhoopathi P, El‐Sayeh H, et al. The Leeds Outcomes Stakeholders Survey (LOSS) Study. Proceddings of the15th Cochrane Colloquium; 2007 Oct 23‐27; Sao Paulo. 2007.
Xia 2009
- Xia J, Adams CE, Bhagat N, Bhagat V, Bhoopathi P, El‐Sayeh H, et al. Loss to outcomes stakeholder survey: the LOSS study. Psychiatric Bulletin 2009;33(7):254‐7. [Google Scholar]
Zheng 2016
- Zheng W, Xiang YQ, Ng CH, Ungvari GS, Chiu HF, Xiang YT. Extract of Ginkgo biloba for tardive dyskinesia: Meta‐analysis of randomized controlled trials. Pharmacopsychiatry 2016;49(3):107‐11. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
McGrath 2000
- McGrath J, Soares‐Weiser K. Miscellaneous treatments for tardive dyskinesia. Cochrane Database of Systematic Reviews 2000, Issue 2. [DOI: 10.1002/14651858.CD000208; PUBMED: 10796325] [DOI] [PubMed] [Google Scholar]
Soares‐Weiser 2003
- Soares‐Weiser KV, Irving CB, Rathbone J. Miscellaneous treatments for neuroleptic‐induced tardive dyskinesia. Cochrane Database of Systematic Reviews 2003, Issue 2. [DOI: 10.1002/14651858.CD000208; PUBMED: 12804390] [DOI] [PubMed] [Google Scholar]