

Abstract
Background
An intraocular lens (IOL) is a synthetic lens that is surgically implanted within the eye following removal of the crystalline lens, during cataract surgery. While all modern IOLs attenuate the transmission of ultra‐violet (UV) light, some IOLs, called blue‐blocking or blue‐light filtering IOLs, also reduce short‐wavelength visible light transmission. The rationale for blue‐light filtering IOLs derives primarily from cell culture and animal studies, which suggest that short‐wavelength visible light can induce retinal photoxicity. Blue‐light filtering IOLs have been suggested to impart retinal protection and potentially prevent the development and progression of age‐related macular degeneration (AMD). We sought to investigate the evidence relating to these suggested benefits of blue‐light filtering IOLs, and to consider any potential adverse effects.
Objectives
To assess the effects of blue‐light filtering IOLs compared with non‐blue‐light filtering IOLs, with respect to providing protection to macular health and function.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (which contains the Cochrane Eyes and Vision Trials Register) (2017, Issue 9); Ovid MEDLINE; Ovid Embase; LILACS; the ISRCTN registry; ClinicalTrials.gov and the ICTRP. The date of the search was 25 October 2017.
Selection criteria
We included randomised controlled trials (RCTs), involving adult participants undergoing cataract extraction, where a blue‐light filtering IOL was compared with an equivalent non‐blue‐light filtering IOL.
Data collection and analysis
The prespecified primary outcome was the change in distance best‐corrected visual acuity (BCVA), as a continuous outcome, between baseline and 12 months of follow‐up. Prespecified secondary outcomes included postoperative contrast sensitivity, colour discrimination, macular pigment optical density (MPOD), proportion of eyes with a pathological finding at the macula (including, but not limited to the development or progression of AMD, or both), daytime alertness, reaction time and patient satisfaction. We evaluated findings related to ocular and systemic adverse effects.
Two review authors independently screened abstracts and full‐text articles, extracted data from eligible RCTs and judged the risk of bias using the Cochrane tool. We reached a consensus on any disagreements by discussion. Where appropriate, we pooled data relating to outcomes and used random‐effects or fixed‐effect models for the meta‐analyses. We summarised the overall certainty of the evidence using GRADE.
Main results
We included 51 RCTs from 17 different countries, although most studies either did not report relevant outcomes, or provided data in a format that could not be extracted. Together, the included studies considered the outcomes of IOL implantation in over 5000 eyes. The number of participants ranged from 13 to 300, and the follow‐up period ranged from one month to five years. Only two of the studies had a trial registry record and no studies referred to a published protocol. We did not judge any of the studies to have a low risk of bias in all seven domains. We judged approximately two‐thirds of the studies to have a high risk of bias in domains relating to ‘blinding of participants and personnel' (performance bias) and ‘blinding of outcome assessment' (detection bias).
We found with moderate certainty, that distance BCVA with a blue‐light filtering IOL, at six to 18 months postoperatively, and measured in logMAR, was not clearly different to distance BCVA with a non‐blue‐light filtering IOL (mean difference (MD) ‐0.01 logMAR, 95% confidence interval (CI) ‐0.03 to 0.02, P = 0.48; 2 studies, 131 eyes).
There was very low‐certainty evidence relating to any potential inter‐intervention difference for the proportion of eyes that developed late‐stage AMD at three years of follow‐up, or any stage of AMD at one year of follow‐up, as data derived from one trial and two trials respectively, and there were no events in either IOL intervention group, for either outcome. There was very low‐certainty evidence for the outcome for the proportion of participants who lost 15 or more letters of distance BCVA at six months of follow‐up; two trials that considered a total of 63 eyes reported no events, in either IOL intervention group.
There were no relevant, combinable data available for outcomes relating to the effect on contrast sensitivity at six months, the proportion of eyes with a measurable loss of colour discrimination from baseline at six months, or the proportion of participants with adverse events with a probable causal link with the study interventions after six months.
We were unable to draw reliable conclusions on the relative equivalence or superiority of blue‐light filtering IOLs versus non‐blue‐light filtering IOLs in relation to longer‐term effects on macular health. We were also not able to determine with any certainty whether blue‐light filtering IOLs have any significant effects on MPOD, contrast sensitivity, colour discrimination, daytime alertness, reaction time or patient satisfaction, relative to non‐blue‐light filtering IOLs.
Authors' conclusions
This systematic review shows with moderate certainty that there is no clinically meaningful difference in short‐term BCVA with the two types of IOLs. Further, based upon available data, these findings suggest that there is no clinically meaningful difference in short‐term contrast sensitivity with the two interventions, although there was a low level of certainty for this outcome due to a small number of included studies and their inherent risk of bias. Based upon current, best‐available research evidence, it is unclear whether blue‐light filtering IOLs preserve macular health or alter risks associated with the development and progression of AMD, or both. Further research is required to fully understand the effects of blue‐light filtering IOLs for providing protection to macular health and function.
Plain language summary
Artificial, blue‐light filtering lenses in the eye for protecting the macula (back of the eye) after cataract surgery
What is the aim of the review? The aim of this Cochrane Review was to find out if blue‐light filtering artifical lenses, also known as intraocular lenses (IOLs) protect the back of the eye. Cochrane Review authors collected and analysed all relevant studies to answer this question and found 51 studies.
Key messages There is little evidence of any important differences between blue‐light filtering and non‐blue‐light filtering lenses. However, studies have been too small and too short‐term to provide a reliable answer to this question.
What was studied in the review? Sometimes the lens in the eye becomes cloudy, often as people become older. Cataract surgery involves removing the cloudy lens and replacing it with an artificial one. This artificial lens is known as an 'intraocular lens' or IOL. These IOLs contain a filter to block harmful ultra‐violet (UV) light. Some lenses also have a filter to block visible blue light. In theory, high levels of blue light could damage the back of the eye that controls central vision (the macula). It has been suggested that blue‐light filtering IOLs may help to protect the macula and prevent a common cause of visual loss in older people, age‐related macular degeneration.
What are the main results of the review? Cochrane Review authors included 51 studies from 17 different countries in this review. The review showed that:
• there is probably no important difference in distance vision between blue‐light filtering artificial lenses and non‐blue‐light filtering lenses 12 months after surgery (we are moderately certain about this evidence); • there were no relevant data on contrast sensitivity (being a person's ability to differentiate an object from its background) and colour discrimination, being two measures of macular health; • none of the people taking part in these studies developed age‐related macular degeneration within the follow‐up period (we are very uncertain about this evidence); • there was no evidence on adverse outcomes that may be related to the blue‐light filtering IOLs (for example, sleep disturbance).
How up‐to‐date is this review? Cochrane Review authors searched for studies that had been published up to 25 October 2017.
Summary of findings
Summary of findings for the main comparison. Blue‐light filtering intraocular lenses (IOL) compared to non blue‐light filtering IOL for protecting macular health.
| Blue‐light filtering IOL compared to non‐blue‐light filtering IOL for protecting macular health | ||||||
| Patient or population: adults undergoing cataract surgery with IOL implantation Setting: eye hospitals Intervention: blue‐light filtering IOL Comparison: non‐blue‐light filtering IOL | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with non‐blue‐light filtering IOL | Risk with blue‐light filtering IOL | |||||
| Change in distance BCVA, between baseline and 12 months | Mean change in distance BCVA between baseline and 12 months was 0 logMAR | MD 0.01 logMAR lower (0.03 lower to 0.02 higher) | ‐ | 131 (2 RCTs) | ⊕⊕⊕⊝ Moderatea | A lower BCVA (in logMAR) indicates a higher level of visual acuity. Studies in this analysis reported data at the end of the follow‐up period rather than change from baseline. |
| Distance BCVA, considered as a dichotomous outcome (being the proportion of eyes that experienced loss of 15 or more letters from baseline BCVA), at six months | See comments | Not estimable | 63 (2 RCTs) | ⊕⊝⊝⊝ Very lowb,c | There were no eyes, in either intervention group that had a loss of 15 or more letters from baseline BCVA. | |
| Contrast sensitivity function, measured in log Contrast Sensitivity at six months | ‐ | ‐ | ‐ | ‐ | ‐ | No relevant combinable data available for this outcome |
| Colour discrimination, measured as the proportion of eyes that had a measurable loss from baseline using Farnsworth‐Munsell 100‐hue colour test score under photopic conditions at six months | ‐ | ‐ | ‐ | ‐ | ‐ | No relevant combinable data available for this outcome |
| Proportion of participants with adverse events with a probable causal link with the study interventions at six months follow‐up | ‐ | ‐ | ‐ | ‐ | ‐ | No relevant combinable data available for this outcome |
| Proportion of eyes that developed late‐stage AMD, being CNV and/or GA, at three years of follow‐up | See comments | Not estimable | 50 (1 RCT) | ⊕⊝⊝⊝ Very lowd | In the 1 trial (Kara Junior 2011) there were no eyes, in either intervention group that developed late‐stage AMD at five years of follow‐up. | |
| Proportion of eyes that developed any stage of AMD at 12 months | See comments | Not estimable | 144 (2 RCTs) | ⊕⊝⊝⊝ Very lowe | In both studies, there were no eyes, in either intervention group that developed any stage of AMD over the nominated follow‐up period. | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). AMD: age‐related macular degeneration; BCVA: best‐corrected visual acuity; CI: confidence interval; CNV: choroidal neovascularisation; GA: geographic atrophy; MD: mean difference; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High‐certainty: we are very confident that the true effect lies close to that of the estimate of the effect Moderate‐certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low‐certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low‐certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded for risk of bias (‐1). Data derive from two relatively small studies, with one (Caporossi 2009) judged to have a high risk of bias in both masking domains, and the other (Vuori 2006) having an unclear risk of bias in most domains. bDowngraded for imprecision (‐2). Schmack 2012 excluded participants with surgical or postoperative complications, including vitreous loss, capsule tears or prolonged intraocular inflammation from the analysis, and hence did not capture these outcomes (which may affect BCVA) in this study. In addition, there were no events in either study group. cDowngraded for risk of bias (‐1). Data derive from two relatively small studies (Leibovitch 2006; Schmack 2012), which both had an unclear risk of bias in at least three key domains. dDowngraded for risk of bias (‐1) and imprecision (‐2). Data derive from one small trial involving 60 participants (Kara Júnior 2006), with an unknown risk of bias in multiple domains. In this trial, there were no events in either study group. eDowngraded for risk of bias (‐2) and imprecision (‐1). Data derive from two small trials (Kara Junior 2011; Mester 2008a). The Kara Junior 2011 study has an unknown risk of bias in multiple domains, and we judged Mester 2008a as having a high risk of bias in multiple domains, including performance bias and detection bias. In both trials, there were no events in either study group.
Background
Description of the condition
The macula is the specialised region of the human retina that mediates the central 15 to 20 degrees of vision (Holz 2013). Anatomically, the macula corresponds to an area of approximately 5 mm in diameter within the posterior pole (Snell 1998) and has a distinctive yellow pigmentation resulting from the presence of the carotenoid pigments, lutein and zeaxanthin (Beatty 1999; Wald 1945). The macular pigments are thought to protect against the hazards of short‐wavelength visible light, which includes violet and blue light. Functionally, the macula enables high‐resolution spatial vision and colour perception. The maintenance of macular health is essential to normal visual function. It follows that diseases adversely affecting the macula can lead to significant vision impairment. In 2010, 2.1 million people globally were blind and 6.0 million people were visually impaired due to macular diseases (Jonas 2014).
A common form of macular disease is age‐related macular degeneration (AMD), which is a leading cause of blindness in developed countries (Congdon 2004; Pascolini 2012). AMD is a slowly progressive retinal degenerative condition that selectively affects the macula and, thereby, central vision. The prevalence of AMD increases dramatically with age (Owen 2003; Wong 2014). Approximately one‐third of people aged 80 years or over are likely to show clinical signs of AMD (Klein 1992), with about 6% of people having late‐stage disease by this age (Rudnicka 2012). Established risks for AMD include increasing age, genetic factors (Klein 2005; Yang 2006) and smoking (Thornton 2005). It has been hypothesised, but remains unclear, whether other factors, including long‐term exposure to environmental short‐wavelength light, contribute to AMD (Beatty 1999).
AMD is typically asymptomatic in its early stages. Clinically, a key retinal sign is the appearance of drusen, visible as amorphous yellow deposits between the retinal pigment epithelium (RPE) and Bruch’s membrane, which result from the deposition of lipoproteineous material (Bressler 1994; Sarks 1999). The presence of large drusen and hyper‐ or hypo‐pigmentary changes, or both, within the macula, confers a higher risk of progression to late‐stage AMD (Ferris 2005). Progressive disease may result in the development of geographic atrophy and/or choroidal neovascularisation (CNV); both of these forms of late‐stage AMD pose a high risk of significant vision loss.
High‐contrast visual acuity is currently the most consistently reported measure of visual function in studies of AMD, but is a relatively insensitive tool (Downie 2014a). A range of other functional measures have also been shown to be affected in AMD; these include static and flicker perimetry (Luu 2013), microperimetry (Wu 2013), colour vision (Downie 2014b) and the multifocal electroretinogram (Gin 2011).
There is currently no intervention for preventing the development of AMD, nor a cure for AMD. Although treatments, in the form of intra‐vitreal vascular endothelial growth factor inhibitors, exist for CNV, at present therapeutic treatments for early stages of AMD, or geographic atrophy, are still considered to be experimental. Given that AMD is the leading cause of irreversible vision impairment in people aged 50 years or older in developed countries (Coleman 2008), there is great interest in interventions that can be used to prevent the development of AMD or delay progression to late‐stage AMD.
Description of the intervention
Sunlight is composed of electromagnetic radiation that ranges from ultraviolet (UV) through to infrared (IR) light. UV radiation involves wavelengths in the 200 to 400 nanometre (nm) range (Youssef 2011). Visible light is in the 380 to 760 nm range; short‐wavelength visible light (400 to 500 nm) corresponds to the violet (400 to 440 nm) and blue (440 to 500 nm) colours within the visible spectrum (Mainster 2005). Modern technological devices, such as light emitting diodes (LEDs) and compact fluorescent lamps (CFLs) also emit relatively high levels of blue light.
Blue‐light filtering, also termed ‘blue‐blocking’, ophthalmic lenses are lenses that are designed to selectively attenuate the transmission of UV radiation and short‐wavelength visible light (Mainster 2006). They were first introduced into ophthalmologic practice in 1991. Two main categories of blue‐light filtering ophthalmic lens products are currently commercially available, being intraocular lenses (IOLs) and spectacle lenses; this review focusses specifically on IOLs. Spectacle lens filters have been considered elsewhere (Downie 2017; Lawrenson 2017).
An IOL is a synthetic lens that is surgically implanted within the eye following removal of the natural crystalline lens, during cataract surgery. Blue‐blocking IOLs typically contain yellow chromophores that attenuate the transmission of about half of incident short‐wavelength light, depending upon their dioptric power (Brockmann 2008; Mainster 2006). Blue‐blocking IOLs contrast with UV‐blocking IOLs, which are colourless and absorb most UV radiation and a small amount of violet light (Mainster 1986; Mainster 2006). A range of blue‐blocking IOLs are currently available on the market; examples include the OptiBlue (AMO), AF‐1 (Hoya), AcrySof Natural (Alcon) and PC 440Y Orange Series (Optech).
How the intervention might work
While light is essential to visual perception, it is also a potential ocular hazard. Fortunately, the natural absorbance characteristics of the anterior structures of the eye limit the amount of potentially damaging UV radiation that reaches the retina. The cornea absorbs UV radiation below 300 nm (Boettner 1962) and the crystalline lens blocks most light between 300 nm and 400 nm (Boettner 1962; Norren 1974). The crystalline lens becomes progressively less transparent and more yellowed with age; the result of this physiological process is a relative reduction in the transmittance of short‐wavelength visible light to the retina (Van Norren 2007). The aged crystalline lens therefore demonstrates blue‐light filtering properties, whereas younger crystalline lenses allow more short‐wavelength visible light to be transmitted to the retina. It has been suggested that following cataract surgery, the implantation of an IOL that enables relatively greater transmittance of short‐wavelength visible light than the aged crystalline lens, could precipitate retinal dysfunction, in particular AMD; there are insufficient data currently to support this suggestion (Casparis 2012). The relative vulnerability of the younger eye to retinal damage due to the natural transmittance of blue light has also been raised.
Blue‐light filtering ophthalmic lenses are proposed to protect against potential light‐induced retinal damage, a phenomenon known as retinal phototoxicity, which may arise from short‐wavelength visible light. Laboratory studies have shown that retinal phototoxicity is commonly due to photochemical damage (Youssef 2011), which occurs when light is absorbed by a photosensitiser (a chromophore) and reactive oxygen species (ROS) are liberated (Boulton 2001). ROS can induce cytotoxic retinal damage through various processes, including lipid peroxidation, protein oxidation and mutagenesis (Boulton 2001). Although the retina has cellular defence mechanisms to combat ROS, for various reasons the efficiency of these compensatory processes typically decline with age (Margrain 2004). The highly oxygenated outer retinal layers, in particular the RPE and photoreceptors, are considered most vulnerable to photochemical damage. Under experimental conditions, short‐wavelength visible light has been shown to induce cellular damage to the RPE (Ham 1978; Ham 1984); this region of the visible spectrum has the most potential for retinal phototoxicity (Ham 1976), which forms the basis for the commonly‐adopted phrase, ‘blue light hazard’ (Boulton 2001). Although the precise intracellular chromophore(s) that mitigate the reported blue‐light sensitivity of RPE cells is not certain, the lipofuscin component A2E has been proposed to be a likely candidate. This fluorophore is found specifically in RPE cells and accumulates with age (Parish 1998); the absorbance spectrum for lipofuscin also mirrors the action spectra for blue‐light phototoxicity (Mainster 2010).
Based mostly on evidence from animal studies, it has been hypothesised that cumulative retinal damage in humans, due to phototoxicity from environmental light exposure (Mainster 1978), may contribute to the macular changes that occur in AMD. Based upon this hypothesis, blue‐light filtering ophthalmic lenses have been suggested to have a role in protecting the macula and possibly preventing the development or progression of AMD, or both (Beatty 1999; Bernstein 2010). Concerns regarding the possible disruption of circadian rhythms, to affect sleep quality and daytime alertness, by blue‐light filtering ophthalmic lenses remain controversial (Mainster 2006).
Why it is important to do this review
While the rationale for blue‐light filtering ophthalmic lenses is scientifically plausible, there is significant academic debate with regard to the merit, or otherwise, of these ophthalmic devices for protecting the macula (Lee 2012; Mainster 2011; Symes 2012). This is due, at least in part, to apparently contradictory evidence relating to their merit, and creates potential confusion for eye care practitioners seeking to provide best‐practice care.
Blue‐blocking IOLs are routinely used for cataract surgery, accounting for approximately 25% of IOLs implanted worldwide (Mainster 2011). This is despite the relative paucity of epidemiological evidence to corroborate the postulated benefit of blue‐blocking lenses for macular protection; 10 of the 12 major population‐based studies that sought to determine whether there was a correlation between light exposure and AMD did not report a positive association (Mainster 2006). Similarly inconclusive are studies that have sought to determine whether cataract surgery is a risk factor for the development or progression of AMD; while some studies have reported positive associations (Klein 1998; Liu 1989), others have found no clear effects upon AMD progression (Baatz 2008; Chew 2009). Importantly, observational studies have acknowledged methodological limitations, including the potential influences of bias and confounding, which can limit the interpretation of their findings.
Whether blue‐light filtering lenses protect macular health is a major public health issue. AMD is a leading cause of blindness worldwide, and effective methods for preventing its development or progression would be expected to have immense benefits in reducing the individual and economic burden of this disease. The relevance of these potential gains is heightened in the context of global demographic shifts toward enhanced longevity. A systematic review, considering the best‐available research evidence, is essential to objectively evaluate the relative appropriateness of current practices in relation to the prescription of blue‐light filtering ophthalmic lenses. Such an evaluation considers both the relative benefits and potential harms of these devices. We consider this topic to be of significant interest to clinicians, researchers and the wider community. The undertaking of this systematic review may also identify areas of focus for future research in the field.
Objectives
To assess the effects of blue‐light filtering IOLs compared with non‐blue‐light filtering IOLs, with respect to providing protection to macular health and function.
Methods
Criteria for considering studies for this review
Types of studies
We considered randomised controlled trials (RCTs) only.
Types of participants
We included RCTs in which the participants were adults (i.e., at least 18 years of age).
Types of interventions
We included RCTs that compared a blue‐light filtering IOL with an equivalent type of non‐blue‐light filtering IOL. We did not include studies that used blue‐light filtering IOLs in combination with any other potential intervention for AMD.
Types of outcome measures
Primary outcomes
The prespecified primary outcome was the change in distance best‐corrected visual acuity (BCVA), considered as a continuous outcome, between baseline and 12 months of follow‐up. For this outcome, we accepted BCVA measures between six and 18 months of follow‐up. If studies did not report the change in distance BCVA, we utilised data reported at the end of the follow‐up period.
Secondary outcomes
We considered the following secondary outcomes:
proportion of eyes with late‐stage AMD, being neovascular AMD or geographic atrophy as defined by the study investigators, at three years of follow‐up (with an acceptable follow‐up range of between two and four years);
proportion of eyes with any stage of AMD, as defined by the study investigators, at 12 months (with an acceptable follow‐up range of between six and 18 months);
proportion of eyes with a finding of pathological structural change at the macula, detected by clinical observation, optical coherence tomography (OCT) or retinal fundus photography, at 12 months (with an acceptable follow‐up range of between six and 18 months);
effect on distance BCVA, measured in logMAR and considered as a dichotomous outcome (being the proportion of eyes that experienced a loss of 15 or more letters from baseline BCVA), at six months (with an acceptable follow‐up range of three to nine months);
effect on contrast sensitivity function, measured in log Contrast Sensitivity (%), and considered as a continuous outcome using the mid‐range of the available spatial frequencies (between six and 12 cycles per degree), under photopic conditions, as determined by various contrast acuity charts, at six months (with an acceptable follow‐up range of three to nine months);
effect on colour discrimination, measured as the proportion of eyes that had a measurable loss of colour discrimination from baseline using the Farnsworth‐Munsell 100‐hue colour test score under photopic conditions, at six months (with an acceptable follow‐up range of three to nine months);
effect on average retinal macular pigment optical density (MPOD), measured as the proportion of eyes that had a significant increase in MPOD at six months (with an acceptable follow‐up range of three to nine months);
effect on daytime alertness, considered as the proportion of participants who had reduced daytime alertness when measured using the Epworth Sleepiness Scores, at six months (with an acceptable follow‐up range of three to nine months);
effect on reaction time, as a cognitive outcome variable, considered as the proportion of participants who had reduced reaction times, at six months (with an acceptable follow‐up range of three to nine months);
proportion of people who were overall satisfied with their visual outcome at six months (with an acceptable follow‐up range of three to nine months).
Adverse effects
We tabulated findings relating to ocular and systemic adverse effects, as reported in the included studies.
Search methods for identification of studies
Electronic searches
The Cochrane Eyes and Vision Information Specialist conducted systematic searches in the following databases for RCTs. There were no language or publication year restrictions. The date of the search was 25 October 2017.
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 9) (which contains the Cochrane Eyes and Vision Trials Register) in the Cochrane Library (searched 25 October 2017) (Appendix 1);
MEDLINE Ovid (1946 to 25 October 2017) (Appendix 2);
Embase Ovid (1980 to 25 October 2017) (Appendix 3);
LILACS (1982 to 25 October 2017) (Appendix 4);
ISRCTN registry (www.isrctn.com/editAdvancedSearch; searched 25 October 2017) (Appendix 5);
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; searched 25 October 2017) (Appendix 6);
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp; searched 25 October 2017) (Appendix 7).
Searching other resources
We undertook additional searching using the bibliographies of included RCTs to identify other potentially relevant studies. We did not handsearch conference abstracts for this review, as Cochrane Eyes and Vision routinely conducts handsearching for RCTs from major ophthalmology meetings and incorporates these results into CENTRAL.
Data collection and analysis
Selection of studies
We adopted a two‐stage process to select studies for this review.
First, two of the review authors (LED, PRK) independently evaluated the title and abstract results from the electronic search strategies, in order to identify potentially suitable studies for inclusion in the review.
Next, we obtained full‐text copies for studies that at least one review author deemed relevant or possibly relevant to the review. Two review authors (LED, PRK) independently assessed each full‐text article and classified its suitability for inclusion in the review, according to the Criteria for considering studies for this review into one of three categories: (i) definitely include, (ii) inclusion status unclear or (iii) definitely exclude.
We resolved discrepancies in classification by discussion to reach consensus between the two review authors. For cases where we considered further information was necessary to determine the eligibility of a study for inclusion, we contacted the study authors for this information. If we did not receive a response from the study authors within four weeks of initial contact, or they did not provide the requested information, we used the information within the full‐text article to decide upon the eligibility of the study. We have provided details relating to the reason for excluding studies that underwent full‐text review in the ‘Characteristics of excluded studies’ table.
Data extraction and management
Two review authors (LED, PRK) independently extracted key study data (detailed in Appendix 8) using Covidence (Covidence). We collected details relating to the study design, participant characteristics, number of participants, outcomes, results and any other relevant information (e.g. funding sources). Wherever possible, we extracted quantitative data for outcomes. We resolved any discrepancies in data extraction by discussion to reach consensus; adjudication by the third review author was not required. After reaching consensus in Covidence, one review author (LED) exported collated data into Cochrane's Review Manager 5 (RevMan 5) software (RevMan 2014) and a second review author (LB) independently verified the data.
Assessment of risk of bias in included studies
Two review authors (LED, PRK) independently assessed the risk of bias in each of the included studies using the guidelines in Chapter 8 of the Cochrane Handbook for Systematic Review of Interventions (Higgins 2011a). We evaluated the risk of bias in the following domains:
selection bias (random sequence generation and allocation concealment);
performance bias (masking of participants and personnel);
detection bias (masking of outcome assessment);
attrition bias (incomplete outcome data);
reporting bias (selective reporting of outcomes);
other bias (funding source, other conflicts of interest).
Each review author made a judgement regarding the estimated risk of each type of bias in each included study as: (i) low risk, (ii) unclear risk (due to either lack of information or uncertainty over the potential for bias) or (iii) high risk. The review authors (LED, PRK) resolved disagreements in bias assessment by consensus.
Measures of treatment effect
We undertook the data analyses according to the methods described in Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011).
For continuous outcomes, we extracted information on the change in means of the outcome measures for the intervention and comparator groups at the specified follow‐up periods and standard deviations of change. Where no change scores were reported, we extracted information on means and standard deviation of the outcome for the intervention and comparator groups at the specified follow‐up periods. We have expressed treatment effects as mean difference (MD) with 95% confidence intervals (CIs) between the intervention and comparator groups.
For dichotomous outcomes (including progression to late‐stage AMD and development of early stages of AMD), we compared the proportion of eyes reaching defined categories of AMD (i.e., any AMD or late‐stage AMD) between the intervention and control groups at the nominated time points. We have presented treatment effects as risk ratios (RRs) with 95% CIs.
Unit of analysis issues
For the purpose of this review, the unit of analysis was the enrolled study eye of the participant. Where the study collected data on more than one eye per participant, we followed guidelines for clustering or paired‐eye design described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011b).
Some trials randomised one or both eyes to the intervention or comparator. When participants were randomly allocated to treatment but only one eye per person was included in the trial, then there was no unit of analysis issue. When participants were randomly allocated to treatment and both eyes per person were included, and the average value of both eyes was reported, then there was no unit of analysis issue. When participants were randomly allocated to treatment but both eyes were included and reported separately, we indicated in our protocol that we would analyse this as 'clustered data' (i.e., adjusted for within‐person correlation). In our protocol we had also stated that if the study was a within‐person study (i.e., one eye was randomly allocated to the intervention and the other eye received the comparator intervention), then we would analyse this as 'paired data'.
There were some studies that had data relevant to the review outcomes where both eyes were included in the study (i.e., a paired‐eye trial), but the data were reported as independent observations (Bhattacharjee 2006; Mester 2008a; Schmack 2012). For these trials, we attempted to contact the study authors via email to obtain information to perform a matched analysis, but either did not receive a response within four weeks of our request, or received an automated alert that the email address no longer existed. In two studies, more than one eye from an individual participant was included in the analysis but details of the intra‐class correlation coefficient for within‐person clustering were not provided (Kennis 2004; Marshall 2005). For each of these studies, we attempted to contact the study authors via email to obtain the necessary information, but either did not receive a response within four weeks of our request, or received an automated alert that the email address no longer existed.
Dealing with missing data
For any studies where we identified missing outcome data (e.g., omitted standard deviations, standard errors), we attempted to contact the study authors (see Characteristics of included studies for further details). If we did not receive a response from them within four weeks, or if they were unable to provide this further information, we used the information that was available within the publication.
We had specified in our protocol that if an intention‐to‐treat (ITT) analysis was provided, we would use these data in our analyses. As none of the included studies reported undertaking an ITT analysis, we analysed the data reported by the study authors.
Assessment of heterogeneity
We assessed studies for heterogeneity using the recommendations outlined in Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011).
We assessed for clinical and methodological heterogeneity between studies by examining differences in trial design, participant characteristics at baseline (e.g., age, gender, eligibility criteria, etc.) and risk of bias. We quantified statistical heterogeneity between studies using the I2 statistic (Higgins 2003). We interpreted an I2 statistic of 60% or more to be at risk of moderate heterogeneity (Ng 2014). In identifying and measuring heterogeneity, we also examined the magnitude and direction of effects of individual studies as well as the strength of evidence for heterogeneity (using a P value < 0.10, from the Chi2 test) as an indication of significant heterogeneity.
Assessment of reporting biases
We had intended to assess the risk of reporting bias (due to selective reporting of outcomes) by comparing the outcomes defined in the trial protocol with those in the publication(s). However, none of the included trials had published protocols or methodological papers. There were two trials that had been prospectively registered in a clinical trials registry; for these studies, we compared study outcomes in the publication with the trial registry entry.
As we included fewer than 10 studies in any of the meta‐analyses, we were not able to assess for the potential effect of publication bias.
Data synthesis
Where studies were multi‐arm studies that randomly assigned participants to more than one type of IOL, we considered data from the relevant study arms in the analyses by calculating the relevant point estimate and measure of variability for each main category of IOL (i.e., non‐blue light filtering and blue‐light filtering). We considered the intervention groups of relevance to be all those that could be included in a pair‐wise comparison of intervention groups that, if investigated alone, would meet the criteria for including studies in the review.
Where appropriate, we performed a meta‐analysis for primary or secondary outcomes, or both. When we included fewer than three RCTs in a meta‐analysis, we used a fixed‐effect model. When we included three or more RCTs in a meta‐analysis, we used a random‐effects model.
As there was adequate consistency between individual study results for a pooled result to provide a good summary of the trial findings (i.e. effects in the same directions, I2 < 60%, or a Chi2 test P value > 0.10), we pooled data.
For adverse events, including intraoperative and postoperative complications, we generated tabulated results summaries.
Subgroup analysis and investigation of heterogeneity
We did not perform any subgroup analyses for prognostic factors (i.e., gender and age) at baseline for the primary outcome measure, as there was not a sufficient number of studies (considered two studies per subgroup or more) to perform these analyses.
Sensitivity analysis
We had planned to perform a sensitivity analysis on the primary outcome measure, to assess the effect of excluding studies that: (i) had a high risk of bias (due to lack of allocation concealment or incomplete outcome data or lack of masking), (ii) were unpublished and (iii) were industry‐funded. We were not able to perform a sensitivity analysis on the primary outcome measure as there were too few studies to permit this analysis.
Summary of findings
We prepared a ‘Summary of findings’ table for each comparison to summarise the results of our analyses, using the formats described in Chapter 11 of the Cochrane Handbook for Systematic Reviews of Interventions (Schünemann 2011). We followed the GRADE Working Group approach to grade the certainty of evidence. Outcomes include:
mean change in number of letters of distance BCVA from baseline BCVA in intervention and control groups after 12 months of follow‐up;
proportion of participants who lost 15 or more letters of distance BCVA from baseline BCVA in intervention and control groups after six months of follow‐up;
mean change in contrast sensitivity from baseline in intervention and control groups after six months of follow‐up;
proportion of eyes with a measurable loss of colour discrimination from baseline in intervention and control groups after six months of follow‐up;
proportion of eyes that developed late‐stage AMD in intervention and control groups after three years of follow‐up;
proportion of eyes that developed any AMD in intervention and control groups after one year of follow‐up;
proportion of participants with adverse events with a probable causal link with the study intervention after six months of follow‐up.
Results
Description of studies
Results of the search
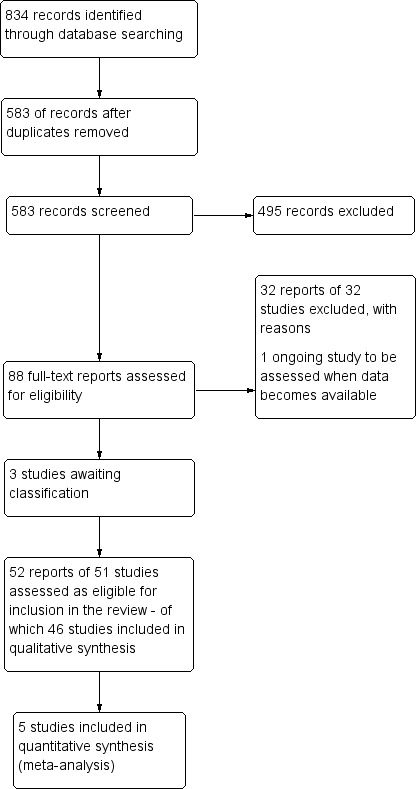
The electronic searches yielded a total of 834 references (Figure 1). The Cochrane Information Specialist removed 251 duplicate records and we screened the remaining 583 reports for potential inclusion in the review. We obtained 88 full‐text reports or conference abstracts that appeared to meet the pre‐defined inclusion criteria, based upon the abstract screening process. We considered a total of 52 reports of 51 studies to be suitable for inclusion in the review and these are summarised in the Characteristics of included studies. We excluded 32 reports of 32 studies; see Characteristics of excluded studies for details. We categorised one study as ongoing, see Characteristics of ongoing studies, and three studies are still currently awaiting categorisation: Ji 2013 is pending translation to English and currently we are unable to source two Chinese papers (Li 2009; Shi 2008). See Characteristics of studies awaiting classification for details.
1.
Study flow diagram
Included studies
Types of studies
Of the 51 included studies, 12 consisted of conference abstracts and 39 were full‐text articles. The individual study designs differed across the included studies, and involved:
the unit of randomisation being the participant, with bilateral implantation of a randomly allocated IOL type (i.e. blue‐light filtering or non‐blue‐light filtering), where the unit of analysis for inter‐group comparisons was the study eye (Caporossi 2007), the average of both eyes (Caporossi 2009; Hayashi 2006), both eyes without apparent statistical adjustment (Marshall 2005), or was unclear (Cionni 2003; Walter 2005). One study, involving bilateral IOL implantation only reported non‐ocular outcomes, and thus the unit of analysis was the participant (Espindle 2005). For the study where one eye was included in the analysis (Caporossi 2007), the method of selection was the dominant eye, although it was not stated whether this was a pre‐planned or post hoc selection.
the unit of randomisation being the participants, unilateral implantation of a randomly allocated IOL type with inter‐group comparisons (Bandyopadhyay 2016; Brøndsted 2015; Brøndsted 2017; Espíndola 2012a; Falkner Radler 2008; Kim 2011b; Leibovitch 2006; Monnet 2009; Neumaier‐Ammerer 2010; Pandita 2007; Schmoll 2014; Ueda 2006; Wang 2010; Yuan 2004);
a paired‐eye design, whereby one eye randomly received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL for intra‐individual comparisons (Bhattacharjee 2006; Cristobal 2005; Hahsler 2005; Kara Júnior 2006; Kara Junior 2011; Mester 2008a; Raj 2005; Rocha 2007; Schmack 2012; Schmidinger 2008; Wirtitsch 2009);
a combination of bilateral and unilateral IOL implantations, where one eye per individual was used for inter‐group comparisons (Cuthbertson 2009; Vuori 2006) or no further information was provided regarding the unit of analysis (Barisic 2007; Hyunseok 2007; Kennis 2004; Kim 2011a).
Additionally, in a number of studies, there was lack of a clear description relating to whether IOL allocation was bilateral or unilateral (Aose 2006; Behrens‐Baumann 2005; Brøndsted 2014; Cui 2009; Hahsler 2004; Kuchenbecker 2004; Nolan 2009; Rocha 2006a; Rocha 2006b; Soriano 2006; Ueda 2005; Yamaguchi 2009; Yamaguchi 2011).
For studies where one eye was randomised to one intervention group and the fellow eye was randomised to another intervention group, we noted that the analyses reported in these studies did not describe taking into account the non‐independence of eyes by using paired‐eye analysis methods. For most studies where bilateral IOL implantation was performed, data were inappropriately analysed as independent observations, without taking into account the relative non‐independence of eyes. In an attempt to incorporate studies adopting clustered or paired designs in our meta‐analyses, wherever possible, we contacted the authors of studies to obtain relevant data relating to within‐person differences or within‐person clustering for our prespecified outcome measures.
Types of participants
We included 51 RCTs in which the participants were adults (i.e. at least 18 years of age), where a blue‐light filtering IOL was compared with an equivalent type of non‐blue‐light filtering IOL. Together, these studies considered the outcomes of IOL implantation in over 5000 eyes. Based upon data reported in the studies, the number of participants in each trial ranged from 13 to 300. The follow‐up period of the studies ranged from one month to five years after cataract surgery.
The studies were conducted in 17 different countries: one in Australia (Leibovitch 2006), six in Austria (Falkner Radler 2008; Hahsler 2004; Hahsler 2005; Neumaier‐Ammerer 2010; Schmidinger 2008; Wirtitsch 2009), one in Belgium or Switzerland (unclear) (Kennis 2004), four in Brazil (Espíndola 2012a; Kara Júnior 2006; Kara Junior 2011; Rocha 2007), three in China (Cui 2009; Wang 2010; Yuan 2004), one in Croatia (Barisic 2007), three in Denmark (Brøndsted 2014; Brøndsted 2015; Brøndsted 2017), one in England (Cuthbertson 2009), one in Finland (Vuori 2006), one in France (Monnet 2009), four in Germany (Kuchenbecker 2004; Mester 2008a; Schmack 2012; Walter 2005), four in India (Bandyopadhyay 2016; Bhattacharjee 2006; Pandita 2007; Raj 2005), one in Ireland (Nolan 2009), two in Italy (Caporossi 2007; Caporossi 2009), five in Japan (Aose 2006; Hayashi 2006; Ueda 2006; Yamaguchi 2009; Yamaguchi 2011), two in Korea (Kim 2011a; Kim 2011b), one in Scotland (Schmoll 2014) and two in the USA (Espindle 2005; Marshall 2005). Investigators of eight studies did not report in which country the trial had been conducted (Behrens‐Baumann 2005; Cionni 2003; Cristobal 2005; Hyunseok 2007; Rocha 2006a; Rocha 2006b; Soriano 2006; Ueda 2005).
For all trials, an inclusion criterion was a clinical indication for cataract surgery. In one study (Falkner Radler 2008), participants had a diagnosis of vitreoretinal pathology, including diabetic vitreous haemorrhage, macular hole, epiretinal membrane or persisting macula oedema, with coexisting significant cataract. One trial (Schmoll 2014), described a group of 'control' participants not undergoing cataract surgery; we did not include data from these participants in our analyses. In one trial, all participants were moderate red–green anomalous trichromats (Raj 2005).
Several studies excluded participants with intraoperative complications (Bhattacharjee 2006; Caporossi 2007; Caporossi 2009; Cristobal 2005; Cuthbertson 2009; Espíndola 2012a; Kara Junior 2011; Kennis 2004; Kim 2011a; Mester 2008a; Monnet 2009; Pandita 2007; Raj 2005; Rocha 2007; Schmack 2012; Wang 2010; Yamaguchi 2009; Yamaguchi 2011), postoperative complications (Bhattacharjee 2006; Brøndsted 2015; Caporossi 2007; Caporossi 2009; Cristobal 2005; Kennis 2004; Kim 2011a; Pandita 2007; Raj 2005; Schmack 2012; Yamaguchi 2009; Yamaguchi 2011), incomplete follow‐up (Espíndola 2012a; Kara Junior 2011; Wang 2010) and/or reduced actual (Kara Júnior 2006) or anticipated (Wirtitsch 2009) postoperative visual acuity. Some trials indicated that no participants developed intraoperative or postoperative complications (Brøndsted 2015; Caporossi 2007; Caporossi 2009; Espíndola 2012a; Raj 2005; Yamaguchi 2009) but most studies did not report on how many participants were excluded due to such effects, which may have affected our ability to report upon all potential adverse events from the interventions.
Types of interventions
All included trials compared at least one blue‐light filtering IOL to at least one non‐blue‐light filtering IOL. In one study, all participants underwent phacoemulsification and IOL implantation, followed by a vitreo‐retinal procedure (Falkner Radler 2008).
Table 2 summarises the specific IOLs used in each trial. Most studies used one type of blue‐light filtering IOL and compared this directly with a non‐blue‐light filtering IOL, although some studies considered multiple IOL types. One trial did not report the IOLs investigated in the study (Yuan 2004).
1. Details of the intraocular lenses (IOLs) used as interventions in each study.
| Study | Blue‐light filtering IOL name(s)a (Manufacturer) | Non‐blue‐light filtering IOL name(s)a (Manufacturer) |
| Aose 2006 | YA‐60BB (Hoya) | AcrySof SA60AT (Alcon) or AcrySof MA60BM (Alcon) or VA‐60BB (Hoya) |
| Bandyopadhyay 2016 | AcrySof Natural SN60AT (Alcon) or PC4406 (Optech) | AcrySof SA60AT (Alcon) |
| Barisic 2007 | AcrySof Natural (Alcon) | AcrySof MA60BM (Alcon) |
| Behrens‐Baumann 2005 | YA‐60BB (Hoya) | VA‐60BB (Hoya) |
| Bhattacharjee 2006 | AcrySof Natural SN60AT (Alcon) | AcrySof SA60AT (Alcon) |
| Brøndsted 2014 | Not reported | Not reported |
| Brøndsted 2015 | AcrySof IQ SN60WF (Alcon) | AMO ZCBOO (Abbott Medical Optics) |
| Brøndsted 2017 | AcrySof IQ SN60WF (Alcon) | AMO ZCBOO (Abbott Medical Optics) |
| Caporossi 2007 | AcrySof Natural SN60AT (Alcon) or AcrySof IQ SN60WF (Alcon) | Sensar AR40e (Abbott Medical Optics) or Tecnis Z9000 (Abbott Medical Optics) or Sofport L161AO (Bausch & Lomb) |
| Caporossi 2009b | AcrySof Natural SN60AT (Alcon) or AcrySof IQ SN60WF (Alcon) | Sensar AR40e (Abbott Medical Optics) or Tecnis Z9000 (Abbott Medical Optics) |
| Cionni 2003 | AcrySof SB30AL (Alcon) | AcrySof SA30AL (Alcon) |
| Cristobal 2005 | AcrySof Natural SN60AT (Alcon) | AcrySof SA60AT (Alcon) |
| Cui 2009 | AcrySof Natural SN60AT (Alcon) or AcrySof IQ SN60WF (Alcon) | Tecnis Z9001 (Abbott Medical Optics) |
| Cuthbertson 2009 | AcrySof Natural SN60AT (Alcon) or AcrySof IQ SN60WF (Alcon) | Tecnis Z9000 (Abbott Medical Optics) or Cee On Edge (Abbott Medical Optics) or Akreos AO (Bausch & Lomb) or Akreos Adapt (Bausch & Lomb) |
| Espindle 2005 | AcrySof Natural (Alcon) | AcrySof single‐piece (Alcon) |
| Espíndola 2012a | AcrySof Natural SN60AT (Alcon) | Akreos Fit (Bausch & Lomb) or Akreos AO (Bausch & Lomb) or AcrySof SA60AT as described in the methods (but appears to be inadvertently described as the MA60AC in the reporting of the results) |
| Falkner Radler 2008 | AcrySof Natural (Alcon) or AF‐1 UY (Hoya) | AcrySof single‐piece (Alcon) or AF‐1 UV (Hoya) |
| Hahsler 2004 | SN60 (Alcon) | SA60 (Alcon) |
| Hahsler 2005 | YA (Hoya) or SN60 (Alcon) | VA (Hoya) or SA60 (Alcon) |
| Hayashi 2006 | YA‐60BB (Hoya) | VA‐60BB (Hoya) |
| Hyunseok 2007 | AcrySof Natural SN60AT (Alcon) | Tecnis ZA9003 (Abbott Medical Optics) |
| Kara Junior 2011 | AcrySof Natural SN60AT (Alcon) | AcrySof SA60AT (Alcon) |
| Kara Júnior 2006 | AcrySof Natural SN60AT (Alcon) | AcrySof MA30AC (Alcon) |
| Kennis 2004 | AcrySof Natural SN60AT (Alcon) | Tecnis Z9000 (Pfizer) or Opti‐Edge (Abbott Medical Optics) |
| Kim 2011a | AcrySof IQ SN60WF (Alcon) | OII Biovue3 (BioVue) or YA60BBR (Hoya) |
| Kim 2011b | AcrySof IQ SN60WF (Alcon) | Tecnis Z9003 (Abbott Medical Optics) |
| Kuchenbecker 2004 | YA‐60BB (Hoya) | VA‐60BB (Hoya) |
| Leibovitch 2006 | AcrySof Natural SN60AT (Alcon) | AcrySof single‐piece SA60AT (Alcon) |
| Marshall 2005 | AcrySof Natural IOL SB30AL (Alcon) (the current marketed version of this lens is the SN60AT) | AcrySof SA30AL (Alcon) |
| Mester 2008a | AF‐1 UY (Hoya) | AF‐1 UV (Hoya) |
| Monnet 2009 | AcrySof SN60AT (Alcon) | AcrySof MA60AC (Alcon) or AcrySof SA60AT (Alcon) |
| Neumaier‐Ammerer 2010 | AF1 UY (Hoya) or AcrySof SN60AT (Alcon) | AF1 UV (Hoya) or AcrySof SA60AT (Alcon) |
| Nolan 2009 | AcrySof Natural SN60AT (Alcon) | AcrySof SA60AT (Alcon) |
| Pandita 2007 | AcrySof SN60AT (Alcon) or AcrySof SN60WF (Alcon) | AcrySof SA60AT (Alcon) |
| Raj 2005 | AcrySof Natural SN60AT (Alcon) | AcrySof SA60AT (Alcon) |
| Rocha 2006a | AcrySof IQ (Alcon) or AcrySof Natural (Alcon) | Sensar (Abbott Medical Optics) |
| Rocha 2006b | AcrySof IQ (Alcon) or AcrySof Natural (Alcon) | Sensar (Abbott Medical Optics) |
| Rocha 2007 | AcrySof IQ (Alcon) or AcrySof SN60AT (Alcon) | Sensar AR40 (Allergan) |
| Schmack 2012 | Oculaid PC 440Y Orange Series (Ophtec BV) | Oculaid PC 430Y Elite Series (Ophtec BV) |
| Schmidinger 2008 | AF‐1 UY (Hoya) | AF‐1 UV (Hoya) |
| Schmoll 2014 | AcrySof SN60WF (Alcon) | Tecnis ZCB (Abbott Medical Optics) |
| Soriano 2006 | AcrySof SN60AT (Alcon) or AcrySof SN60WF (Alcon) | Sensar (Abbott Medical Optics) |
| Ueda 2005 | ENV‐13 (Menicon) | ES‐13 (Menicon) |
| Ueda 2006 | YA‐60BB (Hoya) | VA‐60BB (Hoya) |
| Vuori 2006 | AcrySof Natural SN60AT (Alcon) | AcrySof SA60AT (Alcon) |
| Walter 2005 | AF‐1 YA‐60BB (Hoya) | AF‐1 UV‐60BB (Hoya) |
| Wang 2010 | AY‐1 UY (Hoya) or Arium Matrix Model 4000 (Medennium) | MC611MI (HumanOptics) |
| Wirtitsch 2009 | YA‐60BB (Hoya) | VA‐60BB (Hoya) |
| Yamaguchi 2009 | AcrySof SN60WF (Alcon) or AcrySof SN60AT (Alcon) or Py60AD (Hoya) | Tecnis Z9003 (Abbott Medical Optics) |
| Yamaguchi 2011 | AcrySof SN60WF (Alcon) or AcrySof SN60AT (Alcon) or Py60AD (Hoya) | Tecnis Z9003 (Abbott Medical Optics) |
| Yuan 2004 | Not reported (Hoya) | Not reported (not reported) |
aDetails of the interventions are provided as per the details available in the included studies. bCaporossi 2009, reported two‐year follow‐up data for four out of five of the intervention groups from the Caporossi 2007 study (data from the Sofport L161AO group were not provided, although no explanation was provided).
Primary outcome
As a frequent measure of visual function, distance best‐corrected visual acuity (BCVA) was reported, in various forms and in varying degrees of detail, in many of the included studies.
Six studies (Bhattacharjee 2006; Caporossi 2009; Kennis 2004; Mester 2008a; Schmack 2012; Vuori 2006) presented data that we judged to be potentially relevant to the primary outcome, defined as the change in distance BCVA, and considered as a continuous variable. The methods adopted to assess BCVA involved quantification on an Early Treatment of Diabetic Retinopathy Study (ETDRS) chart under photopic conditions (Caporossi 2009; Mester 2008a; Schmack 2012), Snellen chart under photopic conditions (Kennis 2004; Vuori 2006), or was not reported (Bhattacharjee 2006).
In our protocol, we prespecified that we would obtain data between baseline and 12 months of follow‐up for this outcome measure, but that we would accept measures between six and 18 months of follow‐up, and that if studies did not report the change in distance BCVA, we would utilise data reported at the end of the follow‐up period. The trial designs of the six studies were single‐eye comparisons (Caporossi 2009; Vuori 2006), paired‐eye comparisons (Bhattacharjee 2006; Mester 2008a; Schmack 2012) and a clustered design including where data from more than one eye of some participants were included (Kennis 2004). We attempted to contact the authors of studies utilising paired‐eye and clustered designs, to obtain relevant information relating to within‐person clustering or within‐person differences, or both, to be able to include these data in a meta‐analysis. Each of the six studies reported BCVA data at the end of the follow‐up period, rather than the change from baseline. For one study (Kennis 2004), the unit of measure for distance BCVA was not defined in the paper; for all other studies, the unit of measure was in LogMAR.
Several studies reported data relating to distance BCVA that were not directly relevant to the primary outcome, due to:
the postoperative follow‐up period being less than six months (Aose 2006; Bandyopadhyay 2016; Brøndsted 2015; Caporossi 2007; Cristobal 2005; Cui 2009; Cuthbertson 2009; Falkner Radler 2008; Hayashi 2006; Kim 2011a; Kim 2011b; Kuchenbecker 2004; Neumaier‐Ammerer 2010; Pandita 2007; Rocha 2007; Schmidinger 2008; Ueda 2006; Walter 2005; Wang 2010; Wirtitsch 2009);
the postoperative follow‐up period being in excess of 18 months (Espíndola 2012a: 24 months);
-
data being presented in an alternative format:
Nolan 2009: reported distance BCVA as a 'visual acuity rating' (VAR) at 12 months after surgery, which could not be incorporated in our statistical analysis of this outcome. In this study, it was reported that "similar improvements in acuity were observed in (both intervention groups) over the time course of the study";
Barisic 2007: measured distance BCVA categorically as the number of eyes with BCVA of 0.8, 0.9 or 1.0 decimal acuity after six months of follow‐up, which could not be included in the statistical analysis;
a lack of quantitative data within the publication (Aose 2006; Barisic 2007; Caporossi 2007; Cionni 2003; Cui 2009; Kim 2011a; Kim 2011b; Leibovitch 2006; Marshall 2005).
Secondary outcomes
Proportion of eyes with late‐stage AMD (neovascular AMD or geographic atrophy)
One trial (Kara Junior 2011) reported data relevant to the proportion of eyes with late‐stage AMD (being neovascular AMD or geographic atrophy) at three‐years of follow‐up (with an acceptable follow‐up range of between two and four years).
Proportion of eyes with any stage of AMD
For the outcome involving the proportion of eyes with any stage of AMD, as defined by the study investigators at 12 months (with an acceptable follow‐up range of between six and 18 months), there were two relevant studies (Kara Junior 2011; Mester 2008a). Kara Junior 2011 examined macular findings, determined by optical coherence tomography (OCT) analysis and retinal examination by a masked retinal specialist, at five years of follow‐up and reported "no significant clinical or OCT findings with respect to AMD in any case", in the 25 individuals participating in this paired‐eye trial. The OCT used in this study was a Stratus OCT, with central retinal thickness quantified using the Stratus OCT Reading Software (version 4.1, Carl Zeiss Meditec, Incorporated). In Mester 2008a, also a paired‐eye trial, where participants were followed up for 12 months postoperatively, it was reported that "there were no pathologic findings on fundus examination in any eye at any follow‐up visit." As there were no eyes that developed AMD, of any stage, in any of the intervention groups, in either of the studies, meta‐analysis was not possible for this outcome.
Proportion of eyes with structural macular change
Four studies (Falkner Radler 2008; Marshall 2005; Mester 2008a; Ueda 2005) presented data that were considered potentially relevant to the outcome relating to the proportion of eyes with a finding of a pathological structural change at the macula, as detected by clinical observation, OCT or retinal fundus photography at 12 months (with an acceptable follow‐up range of between six and 18 months).
In the Falkner Radler 2008 study, it was reported that "one patient (in the blue‐light filtering IOL group) had a cystoid macular oedema at nine months after surgery." In the Marshall 2005 study, the same IOLs were bilaterally implanted; the relative non‐independence of eyes from a given participant did not appear to be factored into the statistical analysis. In this trial, it was reported that at six months of follow‐up, six eyes in the blue‐light filtering IOL group had developed cystoid macula oedema and six eyes required secondary surgical intervention; none of the occurrences were considered IOL‐related. In addition, in the non‐blue‐light filtering IOL group, three eyes developed cystoid macula oedema and three eyes required secondary surgical intervention; none of the occurrences were considered IOL‐related.In the paired‐eye Mester 2008a trial, no pathological findings were identified in the blue‐light filtering or non‐blue‐light filtering IOL groups. For the Ueda 2005 study, being an Association for Research in Vision and Ophthalmology (ARVO) conference abstract, the number of eyes assigned to each treatment group, from the 31 participants recruited, was not provided; we attempted to contact the study authors for this information, but were not successful; data from this study could thus not be included in the review for this outcome. In the conference abstract, the authors reported that in the blue‐light filtering IOL group, cystoid macular oedema was evident in 25% of participants at three months of follow‐up, and 9% of participants at 12 months of follow‐up. In the non‐blue‐light filtering IOL group, it was reported that cystoid macular oedema was present in 28% of participants at three months of follow‐up, and 17% of participants at 12 months of follow‐up. The type of OCT used in the study was not reported.
Effect on distance BCVA (logMAR)
For the effect on distance BCVA, measured in logMAR and considered as a dichotomous outcome (being the proportion of eyes that experienced loss of 15 or more letters from baseline BCVA) at six months postoperatively (with an acceptable follow‐up range of three to nine months), there were two studies reporting relevant data (Leibovitch 2006; Schmack 2012). Neither of these studies excluded participants on the basis of intraoperative and/or postoperative complications. In both studies, there were no cases of a loss of distance BCVA in either intervention group; as such, a meta‐analysis was not feasible for this secondary outcome.
Contrast sensitivity
In relation to effects on contrast sensitivity, many of the included studies reported data, in various forms and with varying degrees of detail. Nine studies (Caporossi 2009; Falkner Radler 2008; Kennis 2004; Leibovitch 2006; Mester 2008a; Pandita 2007; Schmack 2012; Wang 2010; Yuan 2004) presented data that we considered potentially relevant to this outcome, defined as the effect on the contrast sensitivity function, measured in log Contrast Threshold (%), and considered as a continuous outcome using the mid‐range of the available spatial frequencies (between six and 12 cycles/degree), under photopic conditions, as determined by various contrast acuity charts, at six months (with an acceptable follow‐up range of three to nine months). Of these potentially relevant trials, five studies (Caporossi 2009; Kennis 2004; Pandita 2007; Wang 2010; Yuan 2004) did not provide details relating to measures of variability for this outcome; we attempted to contact the study authors for this information, but this was not successful, and thus we were unable to include data from these trials. One trial (Falkner Radler 2008) reported changes to contrast acuity, from baseline, measured using the Pelli Robson chart, quantified in log contrast sensitivity, at three months postsurgery. The trial by Leibovitch 2006 reported photopic contrast sensitivity data at six‐months postoperatively (i.e. at the study endpoint) using the Pelli‐Robson chart; although the spatial frequency was not specified, we considered these data relevant to the review and incorporated this information in our analyses. Both the Mester 2008a and Schmack 2012 trials were paired‐eye studies, reporting data at 12 cycles/degree after six months of follow‐up; we contacted the authors of both studies to provide information relating to the means and standard deviations of the within‐pair differences in contrast sensitivity at follow‐up, and for P‐values from the repeated measures ANOVA or paired samples t‐tests; however we did not receive this information, and thus could not incorporate data from these trials in a meta‐analysis.
Reaction time
One study (Schmoll 2014) included a figure (box and whisker plot) that reported data relating to reaction time, as a cognitive outcome variable, at three months of follow‐up. The study authors stated that "Both lenses had an identical mean choice reaction time improvement; Mann–Whitney U testing showed no significant difference in lens effect (P=0.272)."
Overall satisfaction
One study (Barisic 2007) reported on the proportion of people who were overall satisfied with their visual outcome after six months. The authors stated that "high patient satisfaction was noticed since 96.7% of patients would implant (the) AcrySof Natural IOL again (Figure 6). Only one patient would not implant this lens again due to the fact that other people could see a yellow »shine« in his eye. Out of six patients having AcrySof Natural IOL in one eye and a standard AcrySof IOL in other eye, three patients were more satisfied with AcrySof Natural IOL, two didn't notice any difference and one was more satisfied with AcrySof MA60BM IOL."
There were no relevant extractable data for outcomes relating to the following secondary outcomes.
The effect on colour discrimination, measured as the proportion of eyes that had a measurable loss of colour discrimination from baseline using the Farnsworth‐Munsell 100‐hue colour test score under phototopic conditions, at six months of follow‐up. Several studies considered colour vision, but some only included subjective‐reported outcomes (Barisic 2007; Cristobal 2005), did not provide quantitative data in the required format (Behrens‐Baumann 2005; Bhattacharjee 2006; Cionni 2003; Kuchenbecker 2004; Neumaier‐Ammerer 2010; Schmack 2012; Vuori 2006; Walter 2005; Wang 2010; Wirtitsch 2009), used an alternative test to quantify it (i.e., the Ishihara test (Falkner Radler 2008) and/or Farnsworth D‐15 test (Marshall 2005; Raj 2005)), or quantified it at an alternative time‐point (Kara Junior 2011).
The effect on average macular pigment optical density (MPOD) measured as the proportion of eyes that had a significant increase in MPOD at six months of follow‐up. One study considered MPOD measures (Nolan 2009). This trial reported that "average MPOD across the retina increased significantly with time (after 3 months) in the ANIOL (blue‐light filtering) group (repeated‐measures, general linear model, P < 0.05), but remained stable in the AIOL (non‐blue‐light filtering) group (repeated‐measures, general linear model, P > 0.05)." Although the authors analysed the within‐group trend for change in MPOD separately for each group, they did not report the change from baseline in MPOD between groups. This outcome should be considered in the context that it is unclear, from the available information about this study, whether this was a pre‐planned or post‐hoc analysis.
The effect on daytime alertness, considered as the proportion of participants who had reduced daytime alertness measured using the Epworth Sleepiness Score, at six months of follow‐up. One study, Brøndsted 2015, reported on subjective sleep quality, measured using the Pittsburgh Sleep Quality Index (PSQI). The study authors reported that "subjective sleep quality assessed by the PSQI questionnaire was not affected by the surgery (mixed‐model ANOVA, F64 = 0.91, P = 0.345) or by IOL type (mixed‐model ANOVA, F63 = 2.04, P = 0.158) (Table 5). The number of poor sleepers was not affected by surgery (Chi‐square test, X2 = 0.03, P = 0.856) (Table 5)." Brøndsted 2017, also reported on subjective sleep quality, using the PSQI. The study authors reported that subjective sleep quality was improved, as the time of wakefulness after sleep onset had improved by five minutes (95% CI, 1 to 10) for the entire population, while sleep efficiency had increased by two percentage points (95% CI, 0.42 to 3.65) although exclusively, for the participants allocated to blue‐blocking IOLs. However, it should be noted that the results of the "Morningness‐eveningness questionnaire", listed as a secondary outcome measure on the clinicaltrials.gov entry for this study, were not reported.
One study (Espindle 2005) only reported quality‐of‐life outcomes, and did not describe any vision‐related outcomes.
Adverse effects
We have summarised data relating to adverse effects in relation to:
intraoperative complications (Bandyopadhyay 2016; Barisic 2007; Caporossi 2007; Cui 2009; Cuthbertson 2009; Espíndola 2012a; Falkner Radler 2008; Kim 2011a; Kim 2011b; Leibovitch 2006; Marshall 2005; Monnet 2009; Pandita 2007; Raj 2005; Schmidinger 2008; Vuori 2006);
eyes that required neodymium‐doped yttrium aluminium garnet (Nd:YAG) capsulotomy following cataract surgery (Barisic 2007; Caporossi 2009; Espíndola 2012a; Marshall 2005; Monnet 2009; Vuori 2006; Wang 2010; Yamaguchi 2011); and
postoperative complications (Bandyopadhyay 2016; Barisic 2007; Brøndsted 2015; Caporossi 2007; Cui 2009; Falkner Radler 2008; Hayashi 2006; Kara Junior 2011;Kim 2011a; Kim 2011b; Leibovitch 2006; Marshall 2005; Monnet 2009; Schmidinger 2008; Wang 2010;Yamaguchi 2011).
As summarised in Table 3, a total of 16 studies reported on intraoperative complications. Together, these studies considered a total of 1815 eyes (15 RCTs), with overall very few intraoperative complications described with either type of IOL. Marshall 2005 described one case of IOL dislocation during surgery with a blue‐light filtering IOL. Monnet 2009 reported that two (blue‐light filtering IOLs) were placed with one haptic in the capsular bag and one haptic outside the capsular bag; we excluded outcomes from these two participants from the analyses.
2. Adverse effects: intraoperative complications.
| Study |
Study population: number of participants (number of eyes) |
Number of intraoperative complication(s) | Details of intraoperative complication(s) |
| Bandyopadhyay 2016 | Blue‐light filtering IOLs: n = 65 (65); this group combined individuals assigned to 2 different blue‐light filtering IOLs Non‐blue‐light filtering IOL: n = 33 (33) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Barisic 2007 | Blue‐light filtering IOL: n = 30 (60) Non‐blue‐light filtering IOL: n = 30 (60) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Caporossi 2007 | Blue‐light filtering IOL: n = 50 (100); this group combined individuals assigned to 2 different blue‐light filtering IOLs Non‐blue‐light filtering IOL: n = 75 (150); this group combined individuals assigned to 3 different non‐blue‐light filtering IOLs |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Cui 2009 | Blue‐light filtering IOL: n = 39 (41) Non‐blue‐light filtering IOL: n = 18 (20) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Cuthbertson 2009 | Overall: n = 31 (31) | Not reported | One participant developed endophthalmitis and was removed from the trial, being replaced (after re‐randomisation) by another individual. There was one anterior capsular rim tear and one posterior capsule tear without vitreous loss. No details were provided in relation to which group(s) the adverse events occurred in. |
| Espíndola 2012a | Blue‐light filtering IOL: n = 27 (27) Non‐blue‐light filtering IOL: n = 52 (77) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Falkner Radler 2008 | Blue‐light filtering IOL: n = 30 (30) Non‐blue‐light filtering IOL: n = 30 (30) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Kim 2011a | Blue‐light filtering IOL: n = ? (42) Non‐blue‐light filtering IOL: n = ? (26) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Kim 2011b | Blue‐light filtering IOL: n = 23 (23) Non‐blue‐light filtering IOL: n = 16 (16) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Leibovitch 2006 | Blue‐light filtering IOL: n = 9 (9) Non‐blue‐light filtering IOL: n = 10 (10) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Marshall 2005 | Blue‐light filtering IOL: n = 150 (300) Non‐blue‐light filtering IOL: n = 147 (294) |
Blue‐light filtering IOL: n = 1 Non‐blue‐light filtering IOL: none |
There was one case of lens dislocation during surgery in the blue‐light filtering IOL group, in a case in which a posterior capsule rupture had occurred during cataract extraction. |
| Monnet 2009 | Blue‐light filtering IOL: n = 19 (19) Non‐blue‐light filtering IOL: n = 40 (40); this group combined individuals assigned to 2 different non‐blue‐light filtering IOLs. |
Blue‐light filtering IOL: n = 2 Non‐blue‐light filtering IOL: none |
In the blue‐light filtering IOL lens group "two IOLs were placed with 1 haptic in the capsular bag and 1 haptic outside the capsular bag; these 2 patients were also excluded from the final statistical analysis." |
| Pandita 2007 | Blue‐light filtering IOL: n = 73 (73); this group combined individuals assigned to 2 different blue‐light filtering IOLs. Non‐blue‐light filtering IOL: n = 36 (36) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Raj 2005 | Blue‐light filtering IOL: n = 30 (30) Non‐blue‐light filtering IOL: n = 30 (30) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Schmidinger 2008 | Blue‐light filtering IOL: n = 31 (31) Non‐blue‐light filtering IOL: n = 31 (31) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
| Vuori 2006 | Blue‐light filtering IOL: n = 19 (25) Non‐blue‐light filtering IOL: n = 18 (27) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Not applicable |
IOL: intraocular lens
As summarised in Table 4, the time period for reporting postoperative complications or Nd:YAG capsulotomies, or both, ranged from eight weeks to five years of follow‐up. In total, these trials considered more than 1700 eyes (19 RCTs). The risk ratio (RR) of a postoperative complication in the blue‐light filtering IOL group was RR 2.24 (95% CI 0.93 to 5.38), although there was no probable causal link with the intervention. The most common postoperative complication in both intervention groups was the need for a Nd:YAG capsulotomy.
3. Adverse effects: postoperative complications and Nd:YAG capsulotomies.
| Study | Study population: number of participants (number of eyes) | Number of postoperative complication(s) | Details of postoperative complication(s) |
| Bandyopadhyay 2016 | Blue‐light filtering IOLs: n = 65 (65); this group combined individuals assigned to 2 different blue‐light filtering IOLs. Non‐blue‐light filtering IOL: n = 33 (33) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at four weeks of follow‐up |
| Barisic 2007 | Blue‐light filtering IOL: n = 30 (60) Non‐blue‐light filtering IOL: n = 30 (60) |
Blue‐light filtering IOL: n = 3 eyes Non‐blue‐light filtering IOL: n = 4 eyes |
Although the study authors reported that "there were no postoperative complications", n = 3 eyes from the blue‐light filtering IOL group and n = 4 eyes from the non‐blue‐light filtering IOL group required Nd:YAG capsulotomy at six months of follow‐up. |
| Brøndsted 2015 | Blue‐light filtering IOL: n = 38 (38) Non‐blue‐light filtering IOL: n = 35 (35) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at six months of follow‐up. |
| Caporossi 2007 | Blue‐light filtering IOL: n = 50 (100); this group combined individuals assigned to 2 different blue‐light filtering IOLs. Non‐blue‐light filtering IOL: n = 75 (150); this group combined individuals assigned to three different non‐blue‐light filtering IOLs. |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at two months of follow‐up |
| Caporossi 2009 | Blue‐light filtering IOL: n = 50 (100); this group combined individuals assigned to 2 different blue‐light filtering IOLs Non‐blue‐light filtering IOL: n = 50 (100); this group combined individuals assigned to 2 different non‐blue‐light filtering IOLs |
Blue‐light filtering IOL: n = 1 for Nd:YAG capsulotomy Non‐blue‐light filtering IOL: n = 1 for Nd:YAG capsulotomy |
This study reports the two‐year follow‐up data for a subset of participants from Caporossi 2007. The study authors reported that "patients who underwent a capsulotomy before two‐year follow‐up (two patients) were excluded as it was not possible to perform aberrometric analysis. Two Nd:YAG laser capsulotomies were required in two patients who had AcrySof SN60AT IOL (blue‐light filtering IOL) and Tecnis Z9000 IOL (non‐blue‐light filtering IOL) implantation." |
| Cui 2009 | Blue‐light filtering IOL: n = 39 (41); this group combined individuals assigned to 2 different blue‐light filtering IOLs. Non‐blue‐light filtering IOL: n = 18 (20) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at two months of follow‐up |
| Espíndola 2012a | Blue‐light filtering IOL: n = 27 (27) Non‐blue‐light filtering IOL: n = 52 (77) |
Blue‐light filtering IOL: none for glaucoma or Nd:YAG capsulotomy Non‐blue‐light filtering IOL: none for glaucoma or Nd:YAG capsulotomy |
The study authors reported that "at two years after surgery, all lenses were well centered and there was no evidence of posterior capsule opacity or glaucoma." |
| Falkner Radler 2008 | Blue‐light filtering IOL: n = 30 (30) Non‐blue‐light filtering IOL: n = 30 (30) |
Blue‐light filtering IOL: n = 3 eyes Non‐blue‐light filtering IOL: n = 1 eye |
Blue‐light filtering IOL: n = 1 postoperative iris capture, n = 1 spontaneously reabsorbed vitreous haemorrhage, n = 1 cystoid macular oedema at nine months after surgery Non‐blue‐light filtering IOL: n = 1 postoperative iris capture |
| Kim 2011b | Blue‐light filtering IOL: n = 23 (23) Non‐blue‐light filtering IOL: n = 16 (16) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at eight weeks of follow‐up |
| Hayashi 2006 | Blue‐light filtering IOL: n = 38 (38) Non‐blue‐light filtering IOL: n = 36 (36) (In both groups, data were obtained from both eyes and averaged) |
Glare symptoms Blue‐light filtering IOL: n = 3 participants Non‐blue‐light filtering IOL: n = 2 participants Cyanopsia Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Postoperative complications (as measured by participant report of glare symptoms and cyanopsia) at three months after surgery One participant was reported to have a clinically significant epiretinal membrane in the macula (it is unclear which group the participant belonged to) |
| Kara Junior 2011 | Blue‐light filtering IOL: n = 30 (30) Non‐blue‐light filtering IOL: n = 30 (30) |
"Three patients required neodymium:YAG laser capsulotomy for posterior capsule opacification," however group allocations were not specified. | Three participants (although this was not distinguished by the IOL intervention) at five years of follow‐up |
| Kim 2011a | Blue‐light filtering IOL: n = 23 (23) Non‐blue‐light filtering IOL: n = 16 (16) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at eight weeks of follow‐up |
| Leibovitch 2006 | Blue‐light filtering IOL: n = 9 (9) Non‐blue‐light filtering IOL: n = 10 (10) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at six months of follow‐up |
| Marshall 2005 | Blue‐light filtering IOL: n = 150 (300) Non‐blue‐light filtering IOL: n = 147 (294) |
Blue‐light filtering IOL: n = 12 Non‐blue‐light filtering IOL: n = 6 |
At six months of follow‐up, in the blue‐light filtering IOL group, six eyes developed cystoid macula oedema and six eyes required secondary surgical intervention; none of the occurrences were considered IOL‐related. At six months of follow‐up, in the non‐blue‐light filtering IOL group, three eyes developed cystoid macula oedema and three eyes required secondary surgical intervention; none of the occurrences were considered IOL‐related. The study authors stated that "no Nd:YAG capsulotomy was performed in the first‐eye subgroup in either the test or control groups throughout the study period." |
| Monnet 2009 | Blue‐light filtering IOL: n = 19 (19) Non‐blue‐light filtering IOL: n = 40 (40); this group combined individuals assigned to 2 different non‐blue‐light filtering IOLs. |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at three months of follow‐up |
| Schmidinger 2008 | Blue‐light filtering IOL: n = 31 (31) Non‐blue‐light filtering IOL: n = 31 (31) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at three months of follow‐up |
| Wang 2010 | Blue‐light filtering IOL: n = 80 (80); this group combined individuals assigned to 2 different blue‐light filtering IOLs. Non‐blue‐light filtering IOL: n = 38 (38) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
None at 3 months of follow‐up |
| Vuori 2006 | Blue‐light filtering IOL: n = 19 (25) Non‐blue‐light filtering IOL: n = 18 (27) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
The study authors stated that "in the biomicroscopic examination (at one month postoperatively) the posterior capsule appeared clear in all test eyes." |
| Yamaguchi 2011 | Blue‐light filtering IOL: n = ? (120); this group combined individuals assigned to 3 different blue‐light filtering IOLs. Non‐blue‐light filtering IOL: n = ? (30) |
Blue‐light filtering IOL: none Non‐blue‐light filtering IOL: none |
Reported at one month of follow‐up |
IOL: intraocular lens
Funding sources
Thirty‐six of the 51 included studies did not report their source of funding. Four trials (Espindle 2005; Marshall 2005; Mester 2008a; Nolan 2009) were funded by an IOL manufacturer, three trials (Bhattacharjee 2006; Brøndsted 2017; Brøndsted 2015) received philanthropic funding and eight trials (Cuthbertson 2009; Espíndola 2012a; Falkner Radler 2008; Kara Junior 2011; Rocha 2006a; Schmoll 2014; Ueda 2005; Wirtitsch 2009) reported receiving no funding.
Seventeen of the 51 included studies did not report potential conflicts of interest. Thirty‐one studies reported an absence of any conflict of interest (Aose 2006; Bandyopadhyay 2016; Bhattacharjee 2006; Brøndsted 2014; Brøndsted 2015; Caporossi 2007; Caporossi 2009; Cui 2009; Cuthbertson 2009; Espíndola 2012a; Falkner Radler 2008; Hayashi 2006; Kara Júnior 2006; Kara Junior 2011; Kim 2011a; Kim 2011b; Mester 2008a; Monnet 2009; Neumaier‐Ammerer 2010; Pandita 2007; Raj 2005; Rocha 2006b; Rocha 2007; Schmack 2012; Schmidinger 2008; Schmoll 2014; Ueda 2005; Wang 2010; Wirtitsch 2009; Yamaguchi 2009; Yamaguchi 2011). Three studies (Espindle 2005; Marshall 2005; Nolan 2009) declared that one or more of their authors were employees of the IOL manufacturer that funded the trial.
Excluded studies
We excluded 32 studies from the review, after assessing full‐text reports. The reasons for excluding these studies are detailed in the Characteristics of excluded studies table. Sixteen trials (Alexander 2014; Alfonso 2007; Cionni 2006; Feng 2016; Hammond 2010; Hayashi 2009; Lak 2007; Lavric 2014; Munoz 2012; Nagai 2015; Nishi 2013; Rodriguez‐Galietero 2005a; Shpak 2012; Sun 2007; Wen 2012; Wohlfart 2007) adopted a non‐randomised method for allocating interventions. Twelve trials (Chen 2013; Chiosi 2006; Cunha 2010; Gavris 2006; Mayer 2005; Mayer 2006; Mester 2008b; Mester 2008c; Muller 2005; Nakamura 2006; Rodriguez‐Galietero 2005b; Stopyra 2012 did not specify adopting a randomised method to allocate interventions. Four trials (Clarke 1989; Gibson 2008; Kraff 1985; Tognetto 2003) did not meet the criteria for the type(s) of interventions being considered in this review.
As detailed in the Characteristics of studies awaiting classification, we categorised one study (Ji 2013) as 'awaiting classification', pending its translation to identify whether it meets the inclusion criteria for the review. We were unable to source two full‐text reports of studies (Li 2009; Shi 2008).
We categorised one study (Nishi 2015) as ongoing.
Risk of bias in included studies
Figure 2 and Figure 3 summarise the risk of bias assessments for studies included in this review. We have also provided information on risk of bias for individual studies are also provided in the Characteristics of included studies. We did not judge any of the 51 included studies to have a low risk of bias in all seven domains. We considered most studies to have an unclear risk of bias in at least four domains and approximately two‐thirds of the included studies to have a high risk of bias in the domains relating to ‘blinding of participants and personnel (performance bias)’ and ‘blinding of outcome assessment (detection bias)’. The vast majority of studies did not adequately describe their selection bias, ‘random sequence generation’ and ‘allocation concealment’ processes. The three studies that we considered to have the least overall risk of bias (Hayashi 2006; Pandita 2007; Wirtitsch 2009), which we judged as ‘low’ risk in five of the seven domains, did not report quantitative data that could be included in the analysis for any of the prespecified outcomes.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
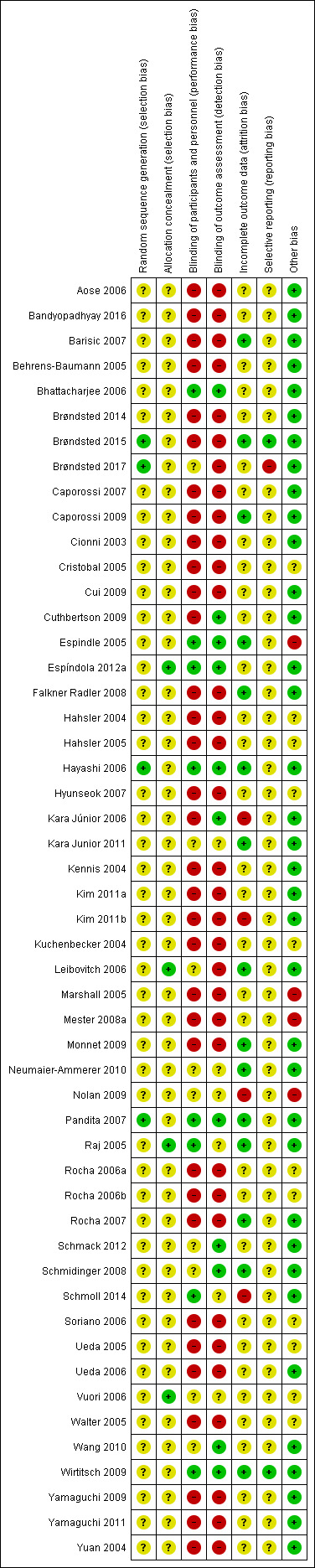
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Although all of the included studies were reported to be randomised, only four trials (Brøndsted 2015; Brøndsted 2017; Hayashi 2006; Pandita 2007), clearly detailed the method for generating a random sequence allocation, and we judged them as having a low risk of bias in this domain. Four trials did not describe how the randomisation sequence was generated, but reported an appropriate method to conceal the allocation sequence (Espíndola 2012a; Leibovitch 2006; Raj 2005; Vuori 2006). We considered that none of the 51 studies adequately reported both how the randomisation sequence was generated and how allocation was concealed.
Blinding
With regard to performance bias, eight studies clearly specified masking study participants and study personnel (Bhattacharjee 2006; Espindle 2005; Espíndola 2012a; Hayashi 2006; Pandita 2007; Raj 2005; Schmoll 2014; Wirtitsch 2009). For eight trials (Brøndsted 2017; Kara Junior 2011; Neumaier‐Ammerer 2010; Nolan 2009; Schmack 2012; Schmidinger 2008; Vuori 2006; Wang 2010), the study reports stated that the trials were 'double‐blind' or that participants and personnel were masked, but no details were provided with regard to how this was achieved. We therefore judged the potential risk of performance bias to be unclear in these trials. Leibovitch 2006 reported that participants were masked to the intervention, but there was no mention of whether personnel were masked. We therefore judged the risk of performance bias in this study as unclear. For the other 34 trials, the design was either an ‘open label’ trial (Behrens‐Baumann 2005; Kuchenbecker 2004; Monnet 2009; Walter 2005), 'patient‐masked only' (Cionni 2003; Marshall 2005), or there was no information provided in relation to how masking may have been performed for study participants and personnel (Aose 2006; Bandyopadhyay 2016; Barisic 2007; Brøndsted 2014; Brøndsted 2015; Caporossi 2007; Caporossi 2009; Cristobal 2005; Cui 2009; Cuthbertson 2009; Falkner Radler 2008; Hahsler 2004; Hahsler 2005; Hyunseok 2007; Kara Júnior 2006; Kennis 2004; Kim 2011a; Kim 2011b; Mester 2008a; Rocha 2006a; Rocha 2006b; Rocha 2007; Soriano 2006; Ueda 2005; Ueda 2006; Yamaguchi 2009; Yamaguchi 2011; Yuan 2004); in the absence of reporting, we assumed that masking was not performed, which constituted a high potential risk of bias.
For masking of outcome assessors (detection bias), we judged a low risk of bias for 11 trials (Bhattacharjee 2006; Cuthbertson 2009; Espindle 2005; Espíndola 2012a; Hayashi 2006; Kara Júnior 2006; Pandita 2007; Schmack 2012; Schmidinger 2008; Wang 2010; Wirtitsch 2009). For six trials, the studies were described as 'double‐blind', but they did not provide any details with regard to how this was achieved. We therefore judged the potential risk of bias in this domain to be unclear (Kara Junior 2011; Neumaier‐Ammerer 2010; Nolan 2009; Raj 2005; Schmoll 2014; Vuori 2006). We judged the other 34 included studies to have a high risk of detection bias, due to being either open label, 'patient‐masked' only or providing no information with regard to the masking of the outcome assessors.
Incomplete outcome data
We judged 15 trials judged to have a low risk of attrition bias (Barisic 2007; Brøndsted 2015; Caporossi 2009; Espindle 2005; Falkner Radler 2008; Hayashi 2006; Kara Junior 2011; Leibovitch 2006; Monnet 2009; Neumaier‐Ammerer 2010; Pandita 2007; Raj 2005; Rocha 2007; Schmidinger 2008; Wirtitsch 2009), reporting that either there were no participants lost to follow‐up, or missing data of less than 20% (based upon a 20% attrition threshold, Schulz 2002), and relatively equal follow‐up in both groups with no obvious reason as to why loss to follow‐up should have been related to the outcome. In 32 studies, we judged the influence of attrition bias to be unclear, as follow‐up was either not clearly stated (Aose 2006; Bandyopadhyay 2016; Behrens‐Baumann 2005; Brøndsted 2014; Brøndsted 2017; Cionni 2003; Cui 2009; Hahsler 2004; Hahsler 2005; Hyunseok 2007; Kennis 2004; Kim 2011a; Kuchenbecker 2004; Rocha 2006a; Rocha 2006b; Soriano 2006; Ueda 2005; Ueda 2006; Vuori 2006; Walter 2005; Yuan 2004), participants were potentially excluded due to intraoperative and/or postoperative complications (Bhattacharjee 2006; Caporossi 2007; Cristobal 2005; Cuthbertson 2009; Espíndola 2012a; Mester 2008a; Schmack 2012; Wang 2010; Yamaguchi 2009; Yamaguchi 2011), or where there was relatively similar follow‐up in the intervention groups but less than 80% participant retention overall (Marshall 2005). Four studies were judged as having a high risk of attrition bias (Kara Júnior 2006; Kim 2011b; Nolan 2009; Schmoll 2014) as overall participant follow‐up was less than 80%.
None of the included studies specifically reported undertaking an intention‐to‐treat (ITT) analysis.
Selective reporting
For 48 of the 51 included studies, we could not judge whether there was selective outcome reporting due to lack of access to the study protocol or a clinical trials registry entry, so we classed them as being as unclear risk of reporting bias. We judged two trials as having a low risk of reporting bias, as the outcomes in the manuscript were consistent with the relevant clinical trials registry entry on clinicaltrials.gov (Brøndsted 2015; Wirtitsch 2009). We judged one trial as having a high risk of reporting bias, as results from the "morningness‐eveningness questionnaire", listed as a secondary outcome measure on the clinicaltrials.gov entry, were not reported in the publication (Brøndsted 2017).
Other potential sources of bias
For 36 of the 51 included trials we did not identify any other potential sources of bias (Aose 2006; Bandyopadhyay 2016; Barisic 2007; Behrens‐Baumann 2005; Bhattacharjee 2006; Brøndsted 2014; Brøndsted 2015; Brøndsted 2017; Caporossi 2007; Caporossi 2009; Cionni 2003; Cui 2009; Cuthbertson 2009; Espíndola 2012a; Falkner Radler 2008; Hayashi 2006; Kara Júnior 2006; Kara Junior 2011; Kennis 2004; Kim 2011a; Kim 2011b; Leibovitch 2006; Monnet 2009; Neumaier‐Ammerer 2010; Pandita 2007; Raj 2005; Rocha 2007; Schmack 2012; Schmidinger 2008; Schmoll 2014; Ueda 2006; Wang 2010; Wirtitsch 2009; Yamaguchi 2009; Yamaguchi 2011; Yuan 2004). We judged four studies as having a high risk of other bias as a result of them being funded by industry, by the companies that manufactured the investigated IOLs (Espindle 2005; Marshall 2005; Mester 2008a; Nolan 2009). We judged an unclear risk of other sources of bias for nine studies, where only abstracts were available (Hahsler 2004; Hahsler 2005; Hyunseok 2007; Kuchenbecker 2004; Rocha 2006a; Rocha 2006b; Soriano 2006; Ueda 2005; Walter 2005), as there was insufficient information provided to comprehensively judge this domain. For Vuori 2006, we judged the risk of other sources of bias to be unclear, as the sex distribution of the study groups at baseline was not reported, however the significance of this baseline imbalance was not clear. For Cristobal 2005, we judged the risk of bias in this domain also as unclear as there was no baseline information available for participants.
Effects of interventions
See: Table 1
Table 1 summarises the effects of the intervention (blue‐light filtering IOL) compared to the comparator (non‐blue‐light filtering IOL) for prespecified outcomes.
Primary outcome: effect on distance best‐corrected visual acuity (BCVA)
A total of six studies (Bhattacharjee 2006; Caporossi 2009; Kennis 2004; Mester 2008a; Schmack 2012; Vuori 2006), reported data relating to the effect on distance BCVA data within six and 18 months of follow‐up; as none of the studies reported the change in distance BCVA from baseline, we utilised data reported at the end of the follow‐up period.
Two trials were single‐eye intervention studies, with no unit‐of‐analysis issue (Caporossi 2009; Vuori 2006). Three trials (Bhattacharjee 2006; Mester 2008a; Schmack 2012), were paired eye studies that undertook inter‐eye comparisons; for these trials, we attempted to contact the study authors via email to obtain the mean and standard deviations of the within‐pair differences in BCVA at follow‐up, however no response was received after more than one month of the email; data from these trials were not included in the meta‐analysis, due to the potential for biased estimates of variance of the outcome. One trial (Kennis 2004), analysed data from 98 eyes of 71 participants without providing further details regarding the analysis approach; we had intended to contact the authors for details relating to the intra‐class correlation coefficient for the within‐person clustering of BCVA, however we could not find any contact details. As a result, we could not include data from this study in the meta‐analysis.
Given the differences in study designs, we undertook a meta‐analysis for the single‐eye trials (Caporossi 2009; Vuori 2006; Analysis 1.1; Figure 4). Pooling the results from these studies, which reported BCVA at 12 months (Caporossi 2009), and six months (Vuori 2006), of follow‐up, the effect on distance BCVA was not statistically significant between blue‐light filtering IOLs and non‐blue‐light filtering IOLs (MD: ‐0.01, 95% CI ‐0.03 to 0.02, P = 0.48; n = 131 eyes, studies: 2); the level of heterogeneity between the two studies was negligible (I2 = 0%). Similar findings were reported separately in the three paired‐eye trials (Bhattacharjee 2006; Mester 2008a; Schmack 2012), and in Kennis 2004, which did not provide specific details regarding the unit of analysis, but appeared to be in Snellen acuity (Analysis 1.2; Figure 5).
1.1. Analysis.
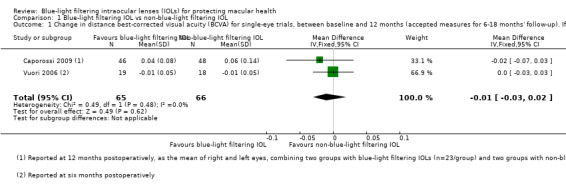
Comparison 1 Blue‐light filtering IOL vs non‐blue‐light filtering IOL, Outcome 1 Change in distance best‐corrected visual acuity (BCVA) for single‐eye trials, between baseline and 12 months (accepted measures for 6‐18 months' follow‐up). If studies did not report change in distance BCVA, we utilised data reported at the end of the follow‐up period..
4.

Forest plot of comparison 1. Blue‐light filtering IOL vs non‐blue‐light filtering IOL, outcome: 1.1 Change in distance best‐corrected visual acuity (BCVA), between baseline and 12 months (accepting measures for 6‐18 months' follow‐up. If change in distance BCVA not reported, we have utilised data reported at the end of the follow‐up period).
1.2. Analysis.
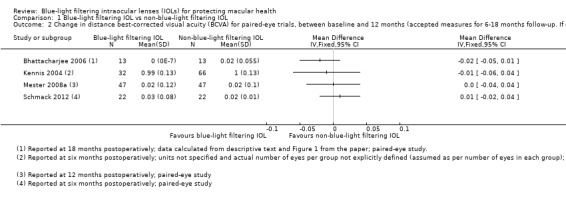
Comparison 1 Blue‐light filtering IOL vs non‐blue‐light filtering IOL, Outcome 2 Change in distance best‐corrected visual acuity (BCVA) for paired‐eye trials, between baseline and 12 months (accepted measures for 6‐18 months follow‐up. If change in distance BCVA was not reported, we utilised data reported at the end of the follow‐up period..
5.
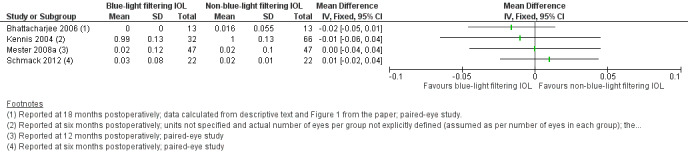
Forest plot of comparison 1. Blue‐light filtering IOL vs non‐blue‐light filtering IOL, outcome: 1.2 Change in distance best‐corrected visual acuity (BCVA) for paired‐eye trials, between baseline and 12 months (accepted measures for 6‐18 months' follow‐up. If change in distance BCVA was not reported, we utilised data reported at the end of the follow‐up period.
We assessed the certainty of the evidence for this outcome measure as 'moderate' using the GRADE approach.
Secondary outcome: effect on contrast sensitivity
Four trials (Falkner Radler 2008; Leibovitch 2006; Mester 2008a; Schmack 2012), reported data relating to the effect on contrast sensitivity, measured within three and nine months of follow‐up, in log Contrast Sensitivity, rather than log Contrast Threshold (%), as we had sought to capture. One study (Falkner Radler 2008), reported the change in contrast sensitivity from baseline, as measured using a Pelli Robson chart. For the remaining studies, (Leibovitch 2006; Mester 2008a; Schmack 2012), data were reported at the end of the follow‐up period. Leibovitch 2006 also used a Pelli Robson chart for measurement. Mester 2008a quantified contrast sensitivity using the Optec 6500 Contrast Sensitivity View‐In Tester (Stereo Optical Company). Schmack 2012 used a CSV‐1000 retroilluminated contrast sensitivity chart (Vector Vision).
Two trials (Falkner Radler 2008; Leibovitch 2006), were single‐eye intervention studies, with no unit‐of‐analysis issue, however we could not pool these data as standardised mean differences, because they represented change scores and final values respectively. As for the distance BCVA outcome, the two other trials (Mester 2008a; Schmack 2012), were paired eye studies that undertook inter‐eye comparisons; for these trials, we attempted to contact the study authors via email to obtain the mean and standard deviations of the within‐pair differences at follow‐up, however no response was received after more than one month of the email; we were therefore not able to include these data in a meta‐analysis.
The data from the single‐eye trials are presented in Analysis 1.3 and Figure 6. Contrast sensitivity was considered as the change from baseline at three months (Falkner Radler 2008), and the study endpoint value at six months of follow‐up (Leibovitch 2006). Similar findings were reported in the results of the two paired‐eye trials (Mester 2008a; Schmack 2012; Analysis 1.4; Figure 7).
1.3. Analysis.
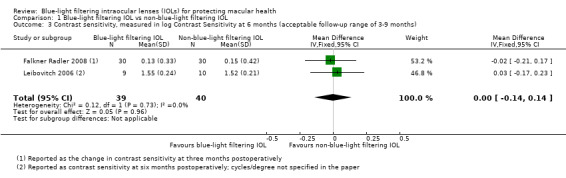
Comparison 1 Blue‐light filtering IOL vs non‐blue‐light filtering IOL, Outcome 3 Contrast sensitivity, measured in log Contrast Sensitivity at 6 months (acceptable follow‐up range of 3‐9 months).
6.

Forest plot of comparison 1. Blue‐light filtering IOL vs non‐blue‐light filtering IOL, outcome: 1.2 Effect on photopic contrast sensitivity function, measured in log Contrast Threshold (%) using the mid‐range of the available spatial frequencies (between 6‐12 cycles/deg) at 6 months (with an acceptable follow‐up range of 3‐9 months).
1.4. Analysis.
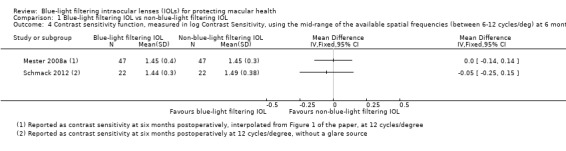
Comparison 1 Blue‐light filtering IOL vs non‐blue‐light filtering IOL, Outcome 4 Contrast sensitivity function, measured in log Contrast Sensitivity, using the mid‐range of the available spatial frequencies (between 6‐12 cycles/deg) at 6 months (acceptable follow‐up range of 3‐9 months; logCT).
7.

Forest plot of comparison 1. Blue‐light filtering IOL vs non‐blue‐light filtering IOL, outcome: 1.4 Contrast sensitivity function, measured in log Contrast Sensitivity, using the mid‐range of the available spatial frequencies (between 6‐12 cycles/deg) at 6 months (acceptable follow‐up range of 3‐9 months) [logCT].
We assessed the certainty of the evidence for this outcome measure as 'low' using the GRADE approach.
Secondary outcome: effect on colour vision
As previously reported, we were unable to extract any relevant data for the effect on colour discrimination, measured as the proportion of eyes that had a measurable loss of colour discrimination from baseline using the Farnsworth‐Munsell 100‐hue colour test score under phototopic conditions, at six months of follow‐up; thus, we could not perform a meta‐analysis.
Although the potential effect of the intervention on colour vision was considered in several studies, the ability to include this information was limited by the use of subjective‐reported outcomes (Barisic 2007; Cristobal 2005), quantitative data not being provided in the required format (Behrens‐Baumann 2005; Bhattacharjee 2006; Cionni 2003; Kuchenbecker 2004; Neumaier‐Ammerer 2010; Schmack 2012; Vuori 2006; Walter 2005; Wang 2010; Wirtitsch 2009), quantification with an alternative colour vision test (Ishihara (Falkner Radler 2008), and/or Farnsworth D‐15 test (Marshall 2005; Raj 2005)), or examination at a different follow‐up time point (Kara Junior 2011).
While most individual studies that considered effects on colour vision reported no significant difference between IOL interventions, Wang 2010 reported that "performance on rack 3 of the FM 100‐hue test, which contains blue disks, resulted in significantly higher mean total error scores in the yellow (blue‐light filtering) IOL group than in the other 2 IOL (photochromic and clear IOL) groups. The differences were statistically significant under mesopic (30 lux) conditions, under which photochromic IOL and clear IOL remained colorless." These findings are consistent with the findings of Neumaier‐Ammerer 2010, who concluded that "patients with yellow tinted IOLs made statistically significantly more mistakes in the blue range under dim light than patients with clear IOLs."
Secondary outcome: development of late stage age‐related macular degeneration (AMD)
We obtained data on the development of late‐stage AMD from one trial, Kara Junior 2011. In this paired‐eye study, which involved the recruitment of 30 people (60 eyes), of which 25 people (50 eyes) completed the study, there were no cases of late‐stage AMD at the five year follow‐up time point.
We assessed the certainty of the evidence for this outcome measure as 'very low' using the GRADE approach.
Secondary outcome: development of any stage of AMD
Two small trials (Kara Junior 2011; Mester 2008a), both being of a paired‐eye (intra‐individual) design, involving the recruitment of a total of 77 participants, reported data relating to the development of any stage of AMD in 144 eyes. The postoperative follow‐up period for these studies was five years (Kara Junior 2011), and 12 months (Mester 2008a). In both studies, there were no participants (in either the intervention of comparator groups) who developed AMD over the nominated follow‐up periods.
We assessed the certainty of the evidence for this outcome measure as 'very low' using the GRADE approach.
Secondary outcome: development of a pathological change at the macula
Three studies (Falkner Radler 2008; Marshall 2005; Mester 2008a), involving a total of 404 people (748 eyes), reported outcomes relating to the development of pathological changes at the macula, where the unit of analysis was the study eye. In Falkner Radler 2008, a single‐eye trial, one eye developed a cystoid macular oedema (CME) at nine months of follow‐up; this eye had received a blue‐light filtering IOL. Of note, in this study participants had a diagnosis of vitreoretinal pathology, including diabetic vitreous haemorrhage, macular hole, epiretinal membrane, or persisting macula oedema, with coexisting significant cataract. In Marshall 2005, both eyes received the same treatment and were analysed independently; at six months of follow‐up there were six eyes (from a total of 300 eyes) that had developed a pathological change at the macula (CME) in the blue‐light filtering IOL group and three eyes (from a total of 294 eyes) that had developed CME in the non‐blue‐light filtering IOL group. In Mester 2008a, which was a paired‐eye trial, no eyes developed a pathological macula change over the follow‐up period. Pooling the results from these three trials (Analysis 1.5; Figure 8), the proportion of eyes with a finding of a pathological structural change at the macula was not statistically different between blue‐light filtering IOLs and non‐blue‐light filtering IOLs (Peto odds‐ratio: 2.21, 95% CI 0.63 to 7.68, P = 0.21, n = 808 eyes, studies: 3); the level of heterogeneity between the three studies was negligible (I2 = 0%).
1.5. Analysis.
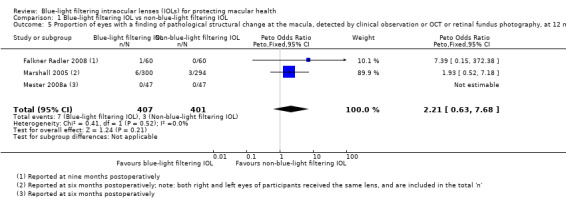
Comparison 1 Blue‐light filtering IOL vs non‐blue‐light filtering IOL, Outcome 5 Proportion of eyes with a finding of pathological structural change at the macula, detected by clinical observation or OCT or retinal fundus photography, at 12 months (acceptable follow‐up range of 6‐18 months).
8.
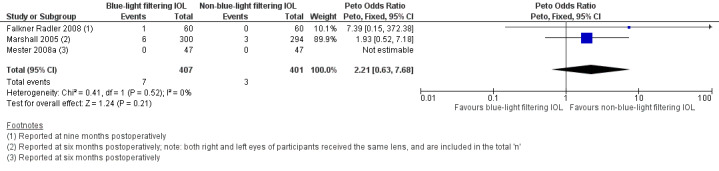
Forest plot of comparison 1. Blue‐light filtering IOL vs non‐blue‐light filtering IOL, outcome: 1.5 Proportion of eyes with a finding of pathological structural change at the macula, detected by clinical observation or optical coherence tomography or retinal fundus photography, at 12 months (acceptable follow‐up range of 6‐18 months).
In addition, in Hayashi 2006, it was reported that "one participant had a clinically significant epiretinal membrane in the macula" and was excluded from the analysis; they did not specify the time point at which this was identified or the intervention group of the participant.
Secondary outcome: effect on distance BCVA, considered as a dichotomous outcome
For the outcome relating to the proportion of participants who lost 15 or more letters of distance BCVA from baseline after six months of follow‐up, two small trials involving a total of 41 people (63 eyes) reported relevant data (Leibovitch 2006; Schmack 2012). In both Leibovitch 2006 (a single‐eye study) and Schmack 2012 (a paired‐eye study), there were no eyes that lost 15 or more letters of distance BCVA from baseline BCVA in either IOL intervention group.
We assessed the certainty of the evidence for this outcome measure as 'very low' using the GRADE approach.
Secondary outcome: effect on reaction time
We obtained data on the effect on reaction time, considered as the proportion of participants who had reduced reaction times, after six months of follow‐up (with an acceptable follow‐up range of three to nine months), from one study (Schmoll 2014). In this single‐eye trial involving a total of 59 eyes, there were no individuals that had a reduction in reaction time in either IOL intervention group at three months of follow‐up. However, this outcome should be viewed in the context that it is unclear from the study methodology whether the trial was sufficiently powered to detect a difference in reaction time between the study groups.
Secondary outcome: level of satisfaction with visual outcome
We obtained data on the level of patient satisfaction with the visual outcome at six months after cataract surgery from one trial (Barisic 2007). In this parallel‐group trial involving 60 participants, the authors reported bilateral IOL implantation of the same IOL type, except for six participants where a blue‐light filtering IOL was implanted in one eye and a non‐blue‐light IOL was implanted in the fellow eye. The study authors reported that: "high patient satisfaction was noticed since 96.67 % of patients would implant AcrySof Natural IOL again. Only one patient would not implant this lens again due to the fact that other people could see yellow »shine« in his eye. None of the patients reported any colour perception disturbances in photopic or mesopic conditions. Out of six patients having AcrySof Natural IOL in one (eye) and standard AcrySof IOL in (the) other eye, three patients were more satisfied with (the) AcrySof Natural IOL, two of them didn't notice any difference and one of them was more satisfied with AcrySof MA60BM IOL. There was no difference in colour perception under photopic and mesopic conditions between the two eyes."
Secondary outcome: proportion of participants with adverse events with a probable causal link with the study interventions after six months of follow‐up
There were no relevant data relating to the proportion of participants with adverse events with a probable casual link with the study interventions after six months of follow‐up. One study, Hayashi 2006, which reported outcomes at three months postoperatively, described that three out of 38 participants with blue‐light filtering IOLs and two out of 36 participants with non‐blue‐light filtering IOLs reported symptoms of glare; no participants in either group reported symptoms of cyanopsia.
Discussion
Intraocular lenses (IOLs) that selectively limit the transmission of shorter‐wavelength visible light, termed blue‐light filtering IOLs, have been suggested to have a potential role in protecting the macula and possibly attenuating the development and/or progression of AMD (Beatty 1999; Bernstein 2010). While the rationale for blue‐light filtering ophthalmic lenses is scientifically plausible, there has been academic debate with regard to the relative merit of these ophthalmic devices for providing protection to macular health and function (Downes 2016; Downie 2017; Lee 2012; Mainster 2011; Symes 2012). To date, it has been unclear whether blue‐light filtering IOLs confer any potential clinical benefits over non‐blue‐light filtering IOLs, with respect to aspects such as distance BCVA, contrast sensitivity and the development of macular pathology. Further, the potential negative effects of blue‐light filtering IOLs on functional parameters, such as colour discrimination, daytime alertness and reaction times (as a cognitive outcome variable), have been raised.
Summary of main results
The primary objective of this review was to assess the effects of blue‐light filtering IOLs with respect to providing protection to macular health and function, in adults undergoing cataract surgery.
We identified 51 eligible RCTs for inclusion, in which more than 3325 participants (involving more than 5000 eyes) were randomised to receive either a blue‐light filtering IOL or a non‐blue‐light filtering IOL. Based upon details provided in the included studies, the number of participants in each trial ranged from 13 to 300. The post‐surgical follow‐up period ranged from four weeks to five years. Overall, the studies' methods were not well reported, and we judged many of the 'Risk of bias' domains to be unclear. We judged the risk of performance bias and detection bias to be high in most of the included studies. We did not judge any studies to be at low risk across all 'Risk of bias' domains.
For all of the efficacy outcomes where relevant quantitative data were available, namely distance BCVA as a continuous outcome (six trials), distance BCVA as a dichotomous outcome (two trials), contrast sensitivity (four trials), development of late‐stage AMD (one trial), development of any stage of AMD (two trials), development of a pathological change at the macula (four trials), change in reaction time (one trial) and the level of patient satisfaction with the visual outcome (one trial), there was no significant difference between the outcomes reported for blue‐light filtering IOLs versus non‐blue‐light filtering IOLs. We were able to perform meta‐analyses for outcomes relating to BCVA as a continuous outcome (two trials) and contrast sensitivity (two trials); both analyses showed no significant differences between the two types of IOLs.
For safety outcomes, being intraoperative and postoperative complications, there was also no significant difference between the outcomes reported for blue‐light filtering IOLs versus non‐blue‐light filtering IOLs.
Thus, based upon the current, best‐available clinical data, the evidence surrounding whether blue‐light filtering IOLs provide greater protection to macular health than non‐blue‐light filtering IOLs is inconclusive.
Overall completeness and applicability of evidence
The trials included in this review were conducted in 17 countries. However, apart from one trial conducted in Australia (Leibovitch 2006), all of the included studies were undertaken in the Northern hemisphere. The trials evaluated the interventions in predominantly white and Asian populations. As it is currently unclear whether the risk of AMD is increased by exposure to sunlight (Chalam 2011; Sui 2013), the significance of there having been relatively less research undertaken in the Southern hemisphere on the generalisability of these findings is uncertain.
The trials in this review enrolled participants who required cataract surgery due to age‐related lenticular opacities. It is therefore unclear whether the reported findings are generalisable to younger populations requiring cataract surgery for different clinical indications (e.g., post‐trauma, congenital cataract, etc.). A further consideration is that the length of postsurgical follow‐up in the majority of trials was less than one year, with only one small study (Falkner Radler 2008), involving 60 participants, considering macular health at five years of postsurgical follow‐up. There is therefore currently insufficient evidence to determine whether blue‐light filtering IOLs confer longer‐term benefits to macular health or prevent the development and/or progression of AMD over extended time periods, or both.
As summarised in Table 2, the included studies used a variety of different IOLs. Some of these IOLs were aspheric and others adopted a spherical design; it is possible that differences in a range of vision‐related outcomes (e.g., BCVA, contrast sensitivity) may be related to the optical design of the IOL, rather than the presence or absence of a blue‐light filtering chromophore. As there were not a sufficient number of studies to consider the potential influence of optical design in our analyses, we are unable to ascertain the potential impact of this factor on the reported outcomes.
Due to differences in measurement technique, periods of follow‐up, data presentation (e.g. no unit of error, graphical presentation only), or a combination of some or all of these factors, we were unable to extract relevant data relating to whether blue‐light filtering IOLs affect colour perception, MPOD or reaction time (as a cognitive outcome variable). Thus, the effect of blue‐light filtering IOLs, compared with non‐blue‐light filtering IOLs, on these outcomes remains unclear.
In relation to the reporting of adverse events, including intraoperative and postoperative complications, the study designs of several trials potentially precluded the identification of all relevant cases. Approximately one‐third of the studies in the review excluded participants with intraoperative complications. Twelve studies excluded participants with postoperative complications, three trials excluded participants with incomplete follow‐up, one trial excluded participants with reduced postoperative visual acuity and one trial excluded participants with an anticipated reduced visual acuity. As data relating to excluded participants were not consistently available, it is therefore possible that the actual number of adverse events (due to both interventions) has been underestimated.
Differences in clinical trial design also posed a challenge for analysing the data. Although many of the included studies were single‐eye trials, there were several trials that adopted either a paired‐eye design, bilateral implantation of the same IOL where the unit of analysis was the study eye, or a combination of bilateral and unilateral IOL implantations where one eye per individual was used for inter‐group comparisons and no further information was provided regarding the unit of analysis. In these instances, we attempted to contact the study authors for further information to permit the inclusion of data from these studies into the relevant meta‐analyses, but did not receive the required information. We were thus unable to pool potentially relevant data from these studies in our meta‐analyses.
Quality of the evidence
Overall, we graded the evidence relating to the prespecified outcomes as being of moderate, low and very low certainty. The most frequent reason for downgrading, which was relevant to the primary outcome (change in distance BCVA considered as a continuous outcome) and several secondary outcomes (distance BCVA considered as a dichotomous outcome, contrast sensitivity, proportion of eyes developing AMD and/or macular pathology, rate of intraoperative complications and rate of postoperative complications), was due to risks of bias (particularly as we judged most of the trials to have uncertain or high risk of bias in the domains relating to performance bias and detection bias).
We downgraded the certainty of evidence (to low) for the effect on contrast sensitivity, as data derived from two small trials, both of which we judged to have a high risk of bias in relation to the blinding of outcome assessors, and indirectness (they did not specify spatial frequency).
We downgraded the certainty of evidence to very low for the effects on distance BCVA (considered as a dichotomous outcome) and proportion of eyes that developed any‐stage or late‐stage AMD, due to factors relating to imprecision (e.g. unknown risk of bias in multiple domains).
Potential biases in the review process
We followed the standard methodological procedures recommended by Cochrane in order to minimise potential biases, and were unable to identify any potential biases in the review process.
Agreements and disagreements with other studies or reviews
A previous meta‐analysis (Zhu 2012), compared functional outcomes (as related to postoperative BCVA, contrast sensitivity and colour vision, as well as postoperative visual quality assessment and adverse visual events) with blue‐light filtering IOLs compared with UV‐filtering IOLs. Consistent with our findings, this study, which included 15 RCTs, found that there were no significant differences in postoperative mean BCVA, contrast sensitivity or overall colour vision between the two types of IOLs. Based upon pooling the data from three studies, which included both single‐eye trials and paired‐eye trials, Zhu 2012 reported that colour vision with blue‐light filtering IOLs was significantly reduced in the blue‐light spectrum under mesopic light conditions (SMD = 0.74, 95% CI 0.29, 1.18; P = 0.001). We suggest that the results of this meta‐analysis should be interpreted with caution, since it appears that the authors did not adjust for the within‐person clustering of eyes, which could potentially have resulted in biased estimates of standard errors and as a result, a biased P‐value. We acknowledge that, in the present review, we did not consider the effect of short‐wavelength absorbing IOLs on visual performance at scotopic light levels; this was considered beyond the scope of the present review, but is a relevant direction for future evaluation of the effects of these devices.
A recent systematic review (Lawrenson 2017) that considered the effects of blue‐light filtering spectacle lenses on visual performance, macular health and the sleep‐wake cycle, concluded that a lack of high‐quality evidence was identified to support the use of blue‐blocking spectacle lenses for the general population to improve visual performance or sleep quality, alleviate eye fatigue or conserve macular health. These findings, relating to outcomes measuring visual performance and macular health with spectacle lenses, are consistent with the outcomes reported for IOLs in the present review.
Authors' conclusions
Implications for practice.
Based upon our consideration of the current, best‐available clinical research evidence, this systematic review shows, with moderate certainty (using the GRADE approach), that there is no clinically meaningful difference in short‐term (three to 18 months postoperative) BCVA with blue‐light filtering and non‐blue‐light filtering IOLs. With regard to effects on other visual performance measures, based upon available data, our findings suggest that there is no clinically meaningful difference in short‐term (three to six months postoperative) contrast sensitivity with the two interventions, although there was a low level of certainty for this outcome due to a small number of included studies and their inherent risk of bias. There were no relevant data relating to the proportion of participants with adverse events with a probably casual link with the study interventions after six months of follow‐up.
Whether blue‐light filtering IOLs preserve macular health or alter the risks associated with the development and progression of AMD, or both, are currently unclear (i.e. there was very low‐certainty evidence); the use of blue‐light filtering IOLs for this specific purpose, in clinical practice, is therefore speculative and claims regarding macular protection are not currently justified by the best available evidence. Due to an insufficient number of studies reporting on these outcomes or variability in the methods used to quantify the outcome(s), or both, we were unable to ascertain with any certainty whether blue‐light filtering IOLs have any significant effects on MPOD, colour discrimination, daytime alertness, reaction time or patient satisfaction.
Implications for research.
The question relating to whether blue‐light filtering IOLs protect macular health is a global public health issue. AMD is one of the leading causes of visual impairment worldwide, and effective methods for preventing its development and progression would be anticipated to have substantial benefits in terms of decreasing the individual and community burden of the disease.
The present review, which considered the best‐available research evidence relating to the potential benefits of blue‐light filtering IOLs for protecting macular health, showed that there is insufficient evidence to support the prescription of these devices for the purpose of preserving macular integrity and altering the risks associated with the development or progression of AMD. This largely reflects that many studies only considered vision performance measures (e.g. BCVA and contrast sensitivity) over relatively short postoperative follow‐up periods (i.e. up to 12 months). There is therefore currently a need for adequately‐powered, well‐designed, long‐term (i.e., over several years) clinical trials to evaluate whether blue‐light filtering IOLs are beneficial for preserving macular integrity. Ideally, future trials should consider whether the extent of environmental blue‐light exposure and/or the degree of blue‐light attenuation within the IOL affects clinical outcomes. Furthermore, there is a need for trials to investigate whether the potential benefit of a blue‐light filtering IOL differs between individuals with a healthy macula at baseline, versus those with early‐stage macular disease or a known risk of disease development (e.g., genetic risk factors or tobacco‐smoking risk factors for AMD); this information could be used to inform whether the potential benefits of blue‐light filtering IOL are stratified by patient population.
A further consideration relates to the design of future clinical trials in this field. Many of the included RCTs excluded participants who experienced intraoperative or postoperative complications. In order to ensure the accuracy of the reported outcome data and to reduce the potential for an underestimation of adverse effects from the interventions, we recommend that future trials describe the outcomes for all randomised participants, using an intention‐to‐treat analysis approach. Furthermore, to enable the outcomes reported in different studies to be more readily compared (and pooled in meta‐analyses, as appropriate), an agreed set of outcomes, known as a 'core outcome set', as recommended by the COMET initiative (Prinsen 2014), would be valuable. Such an approach would be useful for outcomes such as for colour discrimination, where there is still uncertainty about the potential effects of blue‐light filtering IOLS, and where we observed significant heterogeneity between studies in relation to its measurement and reporting. Another example where an agreed set of core outcomes would be advantageous relates to the detection of changes in macular integrity. With the advent of non‐invasive, high‐resolution retinal imaging modalities, such as optical coherence tomography (OCT), it may be possible to define a range of meaningful surrogate outcome measures that could have greater sensitivity for detecting changes to macular health than traditional retinal fundus photography.
Another area requiring consideration by future clinical trial researchers relates to the adoption of appropriate statistical approaches for analysing paired‐eye and bilateral eye studies. None of the included studies reported appropriate methods for considering within‐patient correlations, which may have resulted in biased estimates of effects in these studies.
The results of this review therefore encourage the conduct of future high‐quality research, factoring in the points described, to assess the effects of blue‐light filtering IOLs compared with non‐blue‐light filtering IOLs for providing long‐term protection to macular health and function.
Acknowledgements
Cochrane Eyes and Vision (CEV) created and executed the electronic search strategies. The methods section of this protocol includes some text from a standard template prepared by CEV. We thank Jennifer Evans and Anupa Shah for their assistance during the writing of the review. We thank Sharon Bentley, Catey Bunce, John Lawrenson, Ruth Hogg and Ana Quartilho for comments on the protocol, review or both. We thank the following translators: Covadonga Bascarán for translating a Spanish study (Cristobal 2005), Justin Wormald for translating a Russian study (Shpak 2012), Wu Taixiang and Hsin‐Wen Wu for translating the following Chinese studies (Chen 2013; Sun 2007; Wen 2012), Alex Schuster for translating the following German studies (Mayer 2006; Mester 2008b), Piotr Kanclerz for translating the following Polish papers (Lak 2007; Stopyra 2012).
Appendices
Appendix 1. CENTRAL search strategy
#1 [mh Cataract] #2 [mh "Cataract Extraction"] #3 [mh "Lens, Crystalline"] #4 cataract* #5 [mh "Lenses, Intraocular"] #6 [mh "Lens Implantation, Intraocular"] #7 (intraocular lens* or intra ocular lens* or IOL*) #8 [mh Phacoemulsification] #9 pha?oemulsif* #10 (phaco or phako) #11 (ECCE or MISICS or SICS) #12 [mh Capsulorhexis] #13 capsulor?hexis #14 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 #15 MeSH descriptor: [Retina] explode all trees #16 MeSH descriptor: [Retina] explode all trees #17 MeSH descriptor: [Retinal Pigments] explode all trees #18 retina* near/3 (damage* or phototoxic* or photoprotect*) #19 MeSH descriptor: [Retinal Degeneration] explode all trees #20 MeSH descriptor: [Retinal Neovascularization] this term only #21 MeSH descriptor: [Choroidal Neovascularization] this term only #22 MeSH descriptor: [Macula Lutea] explode all trees #23 maculopath* #24 (macula* or retina* or choroid*) near/3 degener* #25 (macula* or retina* or choroid*) near/3 neovasc* #26 AMD or ARMD or CNV #27 #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 #28 #14 or #27 #29 [mh filtration] #30 (blue near/2 light*) #31 (blue near/3 filter*) #32 (blue near/3 block*) #33 (OptiBlue or AcrySof Natural) #34 (AF‐1 or PC 440Y or SN60AT or SN6OAT or YA60BB) #35 yellow near/4 (intraocular or IOL*) #36 #29 or #30 or #31 or #32 or #33 or #34 or #35 #37 #28 and #36
Appendix 2. MEDLINE Ovid search strategy
1. randomized controlled trial.pt. 2. (randomized or randomised).ab,ti. 3. placebo.ab,ti. 4. dt.fs. 5. randomly.ab,ti. 6. trial.ab,ti. 7. groups.ab,ti. 8. or/1‐7 9. exp animals/ 10. exp humans/ 11. 9 not (9 and 10) 12. 8 not 11 13. exp cataract/ 14. cataract extraction/ 15. cataract$.tw. 16. exp lens crystalline/ 17. exp lenses intraocular/ 18. lens implantation intraocular/ 19. (intraocular lens$ or intra ocular lens$ or IOL$).tw. 20. phacoemulsification/ 21. pha?oemulsif$.tw. 22. (phaco or phako).tw. 23. ECCE.tw. 24. (MISICS or SICS).tw. 25. capsulorhexis/ 26. capsulor?hexis.tw. 27. or/13‐26 28. exp Retina/ 29. exp Retinal Pigments/ 30. (retina$ adj3 (damage$ or phototoxic$ or photoprotect$)).tw. 31. (photochemical adj2 damage$).tw. 32. exp retinal degeneration/ 33. retinal neovascularization/ 34. choroidal neovascularization/ 35. exp macula lutea/ 36. maculopath$.tw. 37. ((macul$ or retina$ or choroid$) adj3 degener$).tw. 38. ((macul$ or retina$ or choroid$) adj3 neovasc$).tw. 39. (AMD or ARMD or CNV).tw. 40. or/28‐39 41. 27 or 40 42. Filtration/ 43. (blue adj2 light$).tw. 44. (blue adj3 filter$).tw. 45. (blue adj3 block$).tw. 46. (OptiBlue or AcrySof Natural).tw. 47. (AF‐1 or PC 440Y or SN60AT or SN6OAT or YA60BB).tw. 48. (yellow adj4 (intraocular or IOL$)).tw. 49. or/42‐48 50. 41 and 49 51. 12 and 50
The search filter for trials at the beginning of the MEDLINE strategy is from the published paper by Glanville 2006.
Appendix 3. Embase Ovid search strategy
1. exp randomized controlled trial/ 2. exp randomization/ 3. exp double blind procedure/ 4. exp single blind procedure/ 5. random$.tw. 6. or/1‐5 7. (animal or animal experiment).sh. 8. human.sh. 9. 7 and 8 10. 7 not 9 11. 6 not 10 12. exp clinical trial/ 13. (clin$ adj3 trial$).tw. 14. ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw. 15. exp placebo/ 16. placebo$.tw. 17. random$.tw. 18. exp experimental design/ 19. exp crossover procedure/ 20. exp control group/ 21. exp latin square design/ 22. or/12‐21 23. 22 not 10 24. 23 not 11 25. exp comparative study/ 26. exp evaluation/ 27. exp prospective study/ 28. (control$ or prospectiv$ or volunteer$).tw. 29. or/25‐28 30. 29 not 10 31. 30 not (11 or 23) 32. 11 or 24 or 31 33. exp cataract/ 34. exp cataract extraction/ 35. exp lens/ 36. exp lens implant/ 37. exp lens implantation/ 38. (intraocular lens$ or intra ocular lens$ or IOLS).tw. 39. phacoemulsification/ 40. pha?oemulsif$.tw. 41. (phaco or phako).tw. 42. ECCE.tw. 43. (MISICS or SICS).tw. 44. capsulorhexis/ 45. capsulor?hexis.tw. 46. or/33‐45 47. exp Retina/ 48. Visual Pigment/ 49. (retina$ adj3 (damage$ or phototoxic$ or photoprotect$)).tw. 50. (photochemical adj2 damage$).tw. 51. exp retina degeneration/ 52. retina neovascularization/ 53. subretinal neovascularization/ 54. exp retina macula lutea/ 55. maculopath$.tw. 56. ((macul$ or retina$ or choroid$) adj3 degener$).tw. 57. ((macul$ or retina$ or choroid$) adj3 neovasc$).tw. 58. (AMD or ARMD or CNV).tw. 59. or/47‐58 60. 46 or 59 61. blue light/ 62. (blue adj2 light$).tw. 63. (blue adj3 filter$).tw. 64. (blue adj3 block$).tw. 65. (OptiBlue or AcrySof Natural).tw. 66. (AF‐1 or PC 440Y or SN60AT or SN6OAT or YA60BB).tw. 67. (yellow adj4 (intraocular or IOL$)).tw. 68. or/61‐67 69. 60 and 68 70. 32 and 69
Appendix 4. LILACS search strategy
cataract OR phacoemulsification OR IOL eye OR retina OR macula and light OR blue OR yellow OR block and filter
Appendix 5. ISRCTN search strategy
"( Condition: eye AND Interventions: (light OR blue OR yellow OR block) AND filter )"
Appendix 6. ClinicalTrials.gov search strategy
cataract OR phacoemulsification OR IOL eye OR retina OR macula | (light OR blue OR yellow OR block) AND filter
Appendix 7. ICTRP search strategy
cataract OR phacoemulsification OR IOL eye OR retina OR macula = Condition AND (light OR blue OR yellow OR block) AND filter = Intervention
Appendix 8. Data on study characteristics
| Primary items | Other items | |
| Methods | ||
| Study design | E.g. Parallel group RCT, paired‐eye RCT, cluster RCT, cross‐over RCT, or other design. | Exclusions after randomisation Losses to follow up How missing data were handled e.g. available case analysis, imputation methods Reported power calculation (Y/N), including sample size and power Unusual study design/issues (as required) |
| Unit of randomisation/unit of analysis | e.g. One eye included in study, two eyes included in study, both eyes received same treatment, or two eyes included in study, eyes received different treatments. | |
| Participants | ||
| Country | Setting Equivalence of baseline characteristics |
|
| Total number of participants | ||
| Number (%) of men and women | ||
| Average age and age range | ||
| Inclusion criteria | ||
| Exclusion criteria | ||
| Interventions | ||
| Intervention (n = ) Comparator (n = ) |
· Number of people randomised to each group · Intervention name |
|
| Outcomes | ||
| Primary and secondary outcomes as defined in study reports | Details of outcomes Length of follow up and intervals at which outcomes assessed |
Planned/actual length of follow up |
| Notes | ||
| Date conducted | Specify dates of recruitment of participants | Trial registration details Full study name: (if applicable) Author's name and contact details (email, mailing address) Were trial investigators contacted? |
| Sources of funding | ||
| Declaration of interest | ||
Data and analyses
Comparison 1. Blue‐light filtering IOL vs non‐blue‐light filtering IOL.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Aose 2006.
| Methods |
Study design: RCT Study grouping: parallel group; no further details provided Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group 1
Non‐blue‐light filtering IOL group 2
Non‐blue‐light filtering IOL group 3
Inclusion criteria: not reported Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL 1
Non‐blue‐light filtering IOL 2
Non‐blue‐light filtering IOL 3
|
|
| Outcomes | Refractive error, visual acuity, IOL tilt, IOL decentration, intraocular pressure, corneal endothelial cell loss and aqueous flare at three months postoperatively | |
| Identification |
Sponsorship source: Funding sources: none Declaration of interest: none for all authors Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Date study conducted: not reported First author's name: M Aose Institution: Ophthalmology, Dokkyo University School of Medicine, Tochigi, Japan Email: not reported Address: not reported |
|
| Notes | ARVO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting, participants and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting, the outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Bandyopadhyay 2016.
| Methods |
Study design: RCT Study grouping: parallel group, with 1 eye per participant randomised to 1 of the interventions Exclusions after randomisation: none apparent Losses to follow‐up: none apparent How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1 ‐ yellow
Blue‐light filtering IOL group 2 ‐ orange
Non‐blue‐light filtering IOL group
Inclusion criteria: people with senile cataract Exclusion criteria: people having anomalies or guttata in the corneal endothelium; receiving any ocular treatment within 1 month prior to commencement of the study; taking any medication that can produce somnolence or who are drug addicts or alcoholics; with retinopathies or any other ocular pathology; with any other condition including psychiatric abnormalities that could alter the results; whose pupils were not dilating well with mydriatics Comparison of study groups at baseline: no significant baseline differences |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1 ‐ yellow
Blue‐light filtering IOL 2 ‐ orange
Non‐blue‐light filtering IOL
|
|
| Outcomes | BCVA and contrast sensitivity (photopic and mesopic) at one month postoperatively intraoperative complications, and postoperative complications at one month after surgery |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: none Country: India Setting: tertiary care hospital in Kolkata, West Bengal, Eastern India Comments: Date study conducted: enrolments from 1 August 2014‐31 January 2015 Trial registration number: not provided Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Sabayaschi Bandyopadhyay Institution: Department of Ophthalmology, R. G. Kar Medical College Email: sabyasachi.bandyopadhyay@yahoo.com Address: Department of Ophthalmology, R. G. Kar Medical College, 1 Khudiram Bose Sarani, Kolkata 700 004, India |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in the absence of reporting, participants and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting, assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not clearly stated |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Barisic 2007.
| Methods |
Study design: RCT Study grouping: parallel group, with bilateral IOL implantation of same IOL type, except for six participants where a blue‐light filtering IOL (AcrySof Natural) was implanted in one eye and a non‐blue‐light IOL (AcrySof MA60BM) was implanted in the other eye. Exclusions after randomisation: none apparent Losses to follow‐up: none apparent How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people having bilateral cataract surgery Exclusion criteria: people with glaucoma, retinal, or any other severe ocular pathology Comparison of study groups at baseline: "There were no significant differences between the two investigated groups regarding age, gender and ocular pathology." |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Distance UCVA, measured as the proportion of eyes with UCVA < 0.8 decimal acuity or > 0.8 decimal acuity, after six months Distance BCVA, measured categorically as the number of eyes with BCVA of 0.8, 0.9 or 1.0 decimal acuity, after six months Proportion of people, reported as a dichotomous, who were overall satisfied with their visual outcome (i.e., would have the same type of IOL implanted again), after six months Adverse events:
|
|
| Identification |
Sponsorship source: Funding source: not reported Declaration of interest: not reported Country: Croatia Setting: University Department of Ophthalmology, General Hospital Sveti Duh, Zagreb, Croatia, and Eye Clinic Svjetlost, Zagreb, Croatia Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Ante Barisic Institution: University Department of Ophthalmology, General Hospital Sveti Duh, Zagreb, Croatia Email: not reported Address: University Department of Ophthalmology General Hospital Sveti Duh Zagreb, Croatia |
|
| Notes | Population Unit of error (SD/SEM) not detailed for age of participants at baseline Interventions For the intervention, the manuscript states that: "In six patients AcrySof Natural IOL was implanted in one eye and AcrySof MA60BM IOL in other eye," however no further details were reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided about masking; we assume that in absence of reporting, participants and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking; we assume that in absence of reporting, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: complete reporting for n = 60 participants is implied from the data; from the number of eyes presented in Figures 1, 2 and 3 |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Behrens‐Baumann 2005.
| Methods |
Study design: RCT Study grouping: parallel group Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Overall
Inclusion criteria: not reported Exclusion criteria: people with amblyopia or abnormal Ishihara test Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Colour recognition and contrast sensitivity (mesopic and photopic); time point not specified in the abstract | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Wolfgang Behrens‐Baumann MD Institution: not reported Email: not reported Address: not reported |
|
| Notes | AAO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details. |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "open label investigation," Judgement comment: study is described as "open label" |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: study is described as "open label" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Bhattacharjee 2006.
| Methods |
Study design: RCT Study grouping: parallel group, with inter‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL). Exclusions after randomisation: participants with intraoperative complications were excluded from the analysis; no further details were supplied. Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people ≥ 60 years with good general and ocular health having bilateral age‐related cataracts with a potential visual acuity of 20/40 or better, indicating cataract extraction and IOL implantation (in both eyes), and who agreed to have surgery in both eyes within a maximum interval of 60 days and were willing to complete a schedule of postoperative follow‐ups. Exclusion criteria: people with pre‐existing systemic disease such as diabetes or hypertension, ocular disease, such as uveitis, or who failed the Farnsworth Munsell 100‐Hue test prior to surgery. To avoid the skew deviation of the results, people with an intraoperative complication such as hyphema, zonular rupture, or posterior capsule were also excluded. Comparison of study groups at baseline: no group differences for the 26 eyes (13 participants) that were reported. However, we are unable to judge any potential group difference for participants who were excluded due to intraoperative complications. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Distance BCVA, colour perception and contrast sensitivity at 18 months postoperatively | |
| Identification |
Sponsorship source: Funding sources: Sri Kanchi Sankara Health Educational Foundation, Beltola, Guwahati, Assam, India Declaration of interest: no author had a financial or proprietary interest in any material or method mentioned. Country: India Setting: Sri Sankaradeva Nethralaya Beltola, Assam, India Comments: Date study conducted: June‐August 2003 Trial registration number: not reported Contacting study investigators: we emailed the study authors on 1 September 2017 for the means and standard deviations of the within‐pair differences in distance BCVA at follow‐up; no response was received. As a result, we could not incorporate these data in a meta‐analysis. Corresponding author's name: Harsha Bhattacharjee, MS, Medical Director Institution: Sri Sankaradeva Nethralaya Beltola, Assam, India Email: ssnghy1@sify.com Address: Harsha Bhattacharjee, MS, Medical Director SriSankaradeva Nethralaya Beltola, Guwahati 781028, Assam, India |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "On random selection basis in each patient" Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "patient‐masked, examiner‐masked" Judgement comment: clearly states that participants and personnel were not aware of which intervention was received, but surgeon was not masked |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement comment: clearly states that study was "examiner‐masked" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: appears "patients with an intra‐operative complication... were also excluded" so not intention‐to‐treat and no indication of how many participants were excluded on these grounds |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Brøndsted 2014.
| Methods |
Study design: RCT Study grouping: parallel group, with bilateral IOL implantation (although no further details provided) Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people with cataract and no other significant diseases Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Short wavelength chromatic pupillometry, measured using the consensual pupil reaction Circadian rhythm, assessed by direct activity measurements (actigraphy) and by questionnaires (Pittsburgh Sleep Quality Index and Morningness Eveningness Questionnaire) |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for the review Corresponding author's name: Adam Elias Brøndsted Institution: University of Copenhagen Email: not reported Address: not reported |
|
| Notes | ARVO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as "randomised" but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting on this patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting on this outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Brøndsted 2015.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: the publication states that "preoperative and postoperative complications with an impact on visual acuity, including ruptured capsule, nucleus drop, and postoperative corneal oedema, led to exclusion." However, no participants developed postoperative complications leading to exclusion. Losses to follow‐up: a total of 76 participants were enrolled from screening 267 candidates; 73 participants were randomised (n = 35 to a non‐blue‐light filtering IOL and n = 38 to a blue‐light filtering IOL) "because oneparticipant changed her mind regarding the operation and one participant dropped out after the baseline examination and another participant was excluded at the day of the operation because of posterior capsule rupture. Further, one participant found the study procedures too comprehensive and dropped out after the first control visit, producing a final number of 72 participants at the three‐week postoperative visit." How missing data were handled: not reported Reported power size calculation? yes |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: all patients who were referred for bilateral senile cataract surgery to the Department of Ophthalmology, Rigshospitalete Glostrup, Denmark and provided written informed consent Exclusion criteria: ophthalmological disease with an expected effect on the retina, optic disc, or cornea, including advanced AMD, glaucoma, diabetic retinopathy, corneal dystrophy, ocular trauma, and recurrent uveitis; people with severe systemic disease, including diabetes, cancer of any kind, and known sleep disturbances; people with preoperative and postoperative complications with an impact on visual acuity, including ruptured capsule, nucleus drop, and postoperative corneal oedema Comparison of study groups at baseline: there were no significant inter‐group differences at baseline. Participants were similar in terms of age, sex, distance BCVA, cataract severity and circadian type. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Activation of intrinsic photosensitive ganglion cells using post‐illumination pupil response (PIPR) to blue light from 10‐30 s after light exposure as a surrogate measure, before surgery, and at two days and three weeks post‐surgery. Circadian rhythm analysis using actigraphy and 24‐h salivary melatonin measurements before, and at 3 weeks after surgery Objective and subjective sleep quality, as determined by actigraphy and the Pittsburgh Sleep Quality Index before, and at 3 weeks postsurgery |
|
| Identification |
Sponsorship source: Funding sources: the study was funded by the Danish Association of the Blind and the Velux Foundation. Declaration of interest: the author(s) have no proprietary or commercial interest in any materials discussed in this article. Country: Denmark Setting: Department of Ophthalmology, Rigshospitalete Glostrup, Denmark Comments: Date study conducted: not reported Trial registration number: clinicaltrials.gov (NCT01686308) Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Adam Elias Brøndsted, MD Institution: Department of Ophthalmology, Rigshospitalet, Glostrup, Denmark Email: adelbr01@regionh.dk Address: Henrik Ibsens Vej 2, 4.tv, 1813 Frederiksberg C, Denmark |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was performed on the day of the surgery using automated, computerized block‐randomization lists" |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Because of the different colors of the blue‐blocking and neutral IOLs, it was not possible to keep the investigator masked to IOL type." Judgement comment: Participants were masked but not the "investigator". |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: whether the "same physician (A.E.B)" who examined all particpants was masked or unmasked is not stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: 72 of the 76 participants enrolled completed the study |
| Selective reporting (reporting bias) | Low risk | Judgement comment: main outcome measures are as specified in the relevant entry on clinicaltrials.gov |
| Other bias | Low risk | Judgement comment: no other risks of bias identified |
Brøndsted 2017.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant contributing to the analyses Exclusions after randomisation: "One participant was excluded at the day of surgery due to posterior capsule rupture" (although group allocation is not described). Losses to follow‐up: "The first eye in 76 participants was recruited for the study. Of these, 72 participants completed the three‐week follow‐up and 67 completed the one‐year follow‐up (31 allocated to neutral IOL and 36 allocated to blue‐blocking IOL). One participant was excluded at the day of surgery due to posterior capsule rupture, one participant dropped out and one participant changed her mind regarding the surgery. Three participants declined participation in the one‐year follow‐up and two participants did not respond to the invitation letter or to telephone calls." Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people with bilateral, age‐related cataract eligible for cataract surgery according to the local guidelines. Only the first eye, that is the eye first scheduled for cataract surgery, was included in the study although both eyes were scheduled for surgery. Exclusion criteria: any eye disease with an expected effect on the retina, optic nerve or cornea including advanced AMD, glaucoma, diabetic retinopathy, corneal dystrophy, ocular trauma or recurrent uveitis. People with severe systemic disease, including diabetes, cancer of any kind and known sleep disturbances. Comparison of study groups at baseline: not reported. Note: it is stated that "One participant was excluded at the day of surgery due to posterior capsule rupture" (although group allocation is not described). |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | The main outcome was the intrinsic activation of photosensitive retinal ganglion cells estimated by quantitation of the postillumination pupil response to blue light based on consensual pupil response measurements at one year after surgery. Circadian rhythm, measured by 24‐h melatonin profiles and actigraphy at one year after surgery Self‐evaluated sleep quality, measured using the Danish version of the Pittsburgh Sleep Quality Index (PSQI) at three weeks postoperative and one year after surgery |
|
| Identification |
Sponsorship source: Funding sources: the study was funded by the Danish Association of the Blind and the Velux Foundation. Declaration of interest: not reported Country: Denmark Setting: Department of Ophthalmology, Rigshospitalete Glostrup, Denmark Comments: Date study conducted: not reported Trial registration number: clinicaltrials.gov (NCT01686308) Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Adam Elias Brøndsted, MD Institution: Department of Ophthalmology, Rigshospitalet, Glostrup, Denmark Email: adelbr01@regionh.dk Address: Henrik Ibsens Vej 2, 4.tv, 1813 Frederiksberg C, Denmark |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Computerized block randomization lists" Judgement comment: Computer generated list |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Randomized to implantation" Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Masking of the participants" Judgement comment: "Participants were masked but it is unclear whether study personnel were masked." |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting on this patients and personnel were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "The first eye in 76 participants was recruited for the study. Of these, 72 participants completed the 3‐week follow‐up and 67 completed the 1‐year follow‐up (31 allocated to neutral IOL and 36 allocated to blue‐blocking IOL). 1 participant was excluded at the day of surgery due to posterior capsule rupture, one participant dropped out and one participant changed her mind regarding the surgery. Three participants declined participation in the 1‐year follow‐up and two participants did not respond to the invitation letter or to telephone calls." Judgement comment: missing data < 20% |
| Selective reporting (reporting bias) | High risk | Judgement comment: results of the "Morningness‐eveningness questionnaire", listed as a Secondary Outcome Measure on the clinicaltrials.gov entry are not reported |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Caporossi 2007.
| Methods |
Study design: RCT Study grouping: parallel group, where both eyes of each participant were randomised to the same type of intervention Exclusions after randomisation: participants with intraoperative complications, IOL tilt or decentration were excluded from the analyses; however, no participant had these complications Losses to follow‐up: none How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1 ‐ SN60AT (Alcon)
Non‐blue‐light filtering IOL group 1 ‐ Tecnis Z9000 (AMO)
Blue‐light filtering IOL group 2 ‐ SN60WF (Alcon)
Non‐blue‐light filtering IOL 2 ‐ Sensar AR40e (AMO)
Non‐blue‐light filtering IOL 3 ‐ Sofport L161AO (Bausch & Lomb)
Inclusion criteria: people aged between 50 and 80 years, bilateral cataracts, potential acuity better than 0.2 logMAR units, preoperative corneal spherical aberration (Z04) values between 0.1 and 0.25μm at 5‐mm pupil diameter, and IOL power between +18.00 and +24.00 diopters (D) Exclusion criteria: people were excluded if any of the following conditions were present: corneal astigmatism ≥ 1.00 D, surgical complications, IOL tilt and decentration estimated by retroillumination, glaucoma, amblyopia, corneal pathology, history of uveitis, diabetic retinopathy, pseudoexfoliation syndrome, macular pathology, and previous intraocular surgery. People using topical medications (apart from lubricants) and taking systemic steroids also were excluded. Comparison of study groups at baseline: there were no statistically significant differences among the groups in terms of participant age (P > 0.05). |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Non‐blue‐light filtering IOL 1
Blue‐light filtering IOL 2
Non‐blue‐light filtering IOL 2
Non‐blue‐light filtering IOL 3
|
|
| Outcomes | BCVA, contrast sensitivity (mesopic and photopic), corneal abberations and wavefront spherical aberration of the whole eye, at two months postoperatively intraoperative complications and postoperative complications at two months postoperatively |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: "the authors have no proprietary interest in the materials presented herein" Country: Italy Setting: Department of Ophthalmology and Neurosurgery at the University of Siena, Italy Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: authors contacted on 14th August 2017, Re: Table 2 – whether units of error show SD or another unit (as not specified in the paper); no response was received Corresponding author's name: Gianluca Martone, MD Institution: Department of Ophthalmology and Neurosurgery at the University of Siena, Italy Email: gianlucamartone@unisi.it Address: Gianluca Martone, MD Dipartimento di Scienze Oftalmologiche e NeurochirurgicheUniversità degli Studi di Siena, Viale Bracci 1, 53100 Siena, Italy |
|
| Notes | Data reported in this study for the SN60AT, SN60WF, Sensar AR40e, Tecnis Z900 participants (n = 100 people, n = 200 eyes) is the same as for the Caporossi 2009 paper (which reports later follow‐up time points for these participants). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: participants were masked to which IOL they received; however, there is no comment regarding other personnel, so we assume that in the absence of this information, the study personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: we assume that in absence of reporting, the outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: participants with “surgical complications, IOL tilt and decentration estimated by retroillumination” were excluded, but the paper also states that “no intraoperative or postoperative complications were recorded in the study. In particular no cases of significant IOL decentration and tilt developed during the follow‐up. Further, for the 125 participants enrolled in the study, none of the 125 patients dropped out of the study.” |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Caporossi 2009.
| Methods |
Study design: RCT Study grouping: parallel group, where both eyes of each participant were randomised to the same type of intervention (as per the Caporossi 2007 study) Exclusions after randomisation: 2‐year follow‐up data from participants in the Caporossi 2007 study Losses to follow‐up: none at 2 months postoperatively, 6 participants (12 eyes) at 1 year postoperatively and 11 participants (22 eyes) at 2 years postoperatively How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1 ‐ SN60AT (Alcon)
Non‐blue‐light filtering IOL group 1 ‐ Tecnis Z9000 (AMO)
Blue‐light filtering IOL group 2 ‐ SN60WF (Alcon)
Non‐blue‐light filtering IOL 2 ‐ Sensar AR40e (AMO)
Inclusion criteria: people aged between 50 and 80 years, bilateral cataracts, potential acuity > 0.2 logMAR units, preoperative corneal spherical aberration (Z04) values between 0.1 and 0.25 pm at 5 mm pupil diameter, and IOL power between + 18.00 and + 24.00 diopters (D) Exclusion criteria: people with any of the following present: corneal astigmatism of 1.00 D or more, surgical complications, IOL tilt and decent ration estimated by retroillumination, glaucoma, amblyopia, corneal pathology, history of uveitis, diabetic retinopathy, pseudoexfoliation syndrome, macular pathology, or previous intraocular surgery. People using topical medications (apart from lubricants) or systemic steroids Comparison of study groups at baseline: no statistically significant differences among groups in terms of age (P > 0.05) were noted. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Non‐blue‐light filtering IOL 1
Blue‐light filtering IOL 2
Non‐blue‐light filtering IOL 2
|
|
| Outcomes | BCVA, contrast sensitivity (mesopic and photopic), pupil size, corneal abberations and wavefront spherical aberration of the whole eye, at two months, one year and two years postoperatively Postoperative complications (Nd:YAG capsulotomies) at two years postoperatively |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: the authors have no proprietary interest in the materials presented herein. Country: Italy Setting: Department of Ophthalmology, University of Siena, Italy Comments: Date study conducted: surgeries performed between March 2004‐July 2005 Trial registration number: not reported Contacting study investigators: authors contacted on 14 August 2017 regarding distance BCVA and contrast sensitivity units of error (specifically, whether it is the SD or a different unit or error). We also asked for clarification with regard to why the longer‐term follow‐up data for individuals fitted with the Sofport L161AO lens (described in the earlier paper by Caporossi 2007, are not reported here). No response was received to the email, and as a consequence we could not incorporate these data in the meta‐analyses. Corresponding author's name: Gianluca Martone, MD Institution: Department of Ophthalmology, University of Siena, Italy Email: gianlucamartone@unisi.it Address: Gianluca Martone, MDVia Fontenuovu n.2O, 53100, Siena, Italy |
|
| Notes | Outcomes:We had already considered the rate of intraoperative complications in this group of participants in Caporossi 2007, so we did not extract the data again from this paper. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation was administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: we assume that in the absence of reporting, neither participants nor study personnel were masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: we assume that in the absence of reporting, the outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: participants with “surgical complications, IOL tilt and decentration estimated by retroillumination” were excluded, but the paper also states that “no intraoperative or postoperative complications were recorded" in the study. At two years postoperatively, 89 participants (178 eyes) out of 200 participants remained in the study; reasons for incomplete follow‐up are included (Table 2), and this is relatively equal across the four intervention groups. Although, note that the Caporossi 2007 paper, which reported baseline and two‐month follow‐up data for the same participants, included five lens types rather than four lens types (data relating to the Sofport L161AO lens are not included in this paper, without explanation). |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Cionni 2003.
| Methods |
Study design: RCT Study grouping: parallel group, where both eyes of each participant were randomised to the same type of intervention, but the unit of analysis was not reported Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: not reported Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Visual acuity, colour perception and contrast sensitivity; time point not reported | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: not reported Setting: not reported Comments: Date study conducted: not reported. Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Robert J Cionni, MD Institution: not reported Email: not reported Address: not reported |
|
| Notes | AAO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: study is described as "patient‐masked" only |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: study is described as "patient masked" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Cristobal 2005.
| Methods |
Study design: RCT Study grouping: parallel group, with inter‐eye comparison (i.e. 1 eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL). Exclusions after randomisation: participants with perioperative or postoperative complications were excluded, but no details were provided about these participants. Losses to follow‐up: people that did not attend follow up or did not use the indicated postoperative medications were excluded, but no details were provided about these participants. How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people requiring bilateral cataract surgery with an IOL implant Exclusion criteria: people who didn't attend follow‐up or didn't use the indicated postoperative medications; with systemic diseases that could influence visual function; with postoperative refractive error > 3.00 D; with perioperative or postoperative complications Comparison of study groups at baseline: no baseline information provided on the included participants |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Contrast sensitivity scores with CSV 1000E (®Vistech), for 3, 6, 12 and 18 cycles/degree at 2.6 meters, in scotopic conditions without glare at eight weeks postoperatively Colour vision errors with the Farnsworth test (25 colours) at eight weeks postoperatively participants' subjective measures of self visual function, including colour vision and glare at eight weeks postoperatively BCVA, in decimal scale, at eight weeks postoperatively |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: JA Cristobal Institution: Hospital Clínico Universitario Lozano Blesa, Zaragoza, España Email: not reported Address: not reported |
|
| Notes | Article in Spanish (translated to English for data extraction) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported, and "patients with perioperative or postoperative complications" were excluded from participation; details of those excluded on these grounds are not provided |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: no baseline information available on the included participants |
Cui 2009.
| Methods |
Study design: RCT Study grouping: parallel group, involving the randomisation of 57 people and 61 eyes, with no further details regarding treatment allocation Exclusions after randomisation: participants who were unable to understand or co‐operate with the contrast sensitivity examination were excluded, but no details were provided about these participants. Losses to follow‐up: participants who were lost to follow‐up were excluded, but no details were provided about these participants How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1
Blue‐light filtering IOL group 2
Non‐blue‐light filtering IOL group
Inclusion criteria: people were included who had age‐related cataract, underwent bilateral cataract surgery at the First Affiliated Hospital, Zhejiang University, ranged in age from 50–80 years, and had low degrees of spherical diopters (≤ 2.5 D) and astigmatism (≤ 1.0 D cylindrical) postoperatively. Exclusion criteria: a history of ocular diseases, such as corneal disease, glaucoma, uveitis, and retinal detachment; a history of systemic diseases, such as diabetes and hyperthyroidism Comparison of study groups at baseline: there was no significant difference in age, sex, laterality, or diopter (power) of the IOLs among the three groups at baseline. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Blue‐light filtering IOL 2
Non‐blue‐light filtering IOL
|
|
| Outcomes | BCVA, higher‐order aberrations, contrast sensitivity pre‐operatively and at one week, one month and two months postoperatively Intraoperative and postoperative complications at two months postoperatively |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: the authors have no proprietary or commercial interest in any materials discussed in this article. Country: China Setting: Department of Ophthalmology, First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Dinghua Lou, MD Institution: Department of Ophthalmology, First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China Email: ldh.96@hotmail.com Address: Department of Ophthalmology, First Affiliated Hospital, College of Medicine, Zhejiang University, 79 Qingchun Rd., Hangzhou, Zhejiang, China |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided in relation to masking |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided in relation to masking |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not clearly reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Cuthbertson 2009.
| Methods |
Study design: RCT Study grouping: parallel group, involving one eye per participant randomised to an intervention (being a mix of first and second eyes undergoing cataract surgery) Exclusions after randomisation: people with complicated surgery were excluded. One participant developed endophthalmitis and was removed from the trial, being replaced (after re‐randomisation) by another individual. Losses to follow‐up: One participant developed endophthalmitis and was removed from the trial, being replaced (after re‐randomisation) by another individual. There was one anterior capsular rim tear and one posterior capsule tear without vitreous loss. For the purposes of analysis of results, each of the six lens groups contained five participants. How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL
Overall
Inclusion criteria: people were recruited from cataract preassessment clinics, and informed consent was obtained. Any person over the age of 18 able to understand English and to give informed consent was eligible for inclusion in the trial. Exclusion criteria: exclusion criteria included coexistent ocular pathology, cylinder > 2 dioptres, complicated surgery and wheelchair‐bound patients. Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOLs
Non‐blue‐light filtering IOLs
|
|
| Outcomes | BCVA under standard photopic lighting conditions, contrast sensitivity (under mesopic (6 cd/m2) and photopic (65 cd/m2) conditions with and without glare (CST 1800 digital with Ginsberg Box, Vision Sciences Research Corporation), pupillometry, autorefraction, topography and wavefront analysis preoperatively, at two weeks and three months postoperatively | |
| Identification |
Sponsorship source: Funding sources: no financial support received Declaration of interest: no financial interests Country: England Setting: Department of Ophthalmology, Oxford Eye Hospital, West Wing, John Radcliffe Hospital Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: FM Cuthbertson Institution: Department of Ophthalmology, Oxford Eye Hospital Email: fcuthbertson@doctors.org.uk Address: Department of Ophthalmology, Oxford Eye Hospital, West Wing, John Radcliffe Hospital, Headley Way, Oxford OX3 9DUUK. |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: Assessor masked but no mention of participant masking |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The two observers carrying out the pre and postoperative assessments (FC and SD) were masked as to which lens the patient had received." Judgement comment: clearly states that the outcome assessors were masked to the lens allocation |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not explicitly reported. Participants with complicated surgery were excluded from the analysis. "One participant developed endophthalmitis and was removed from the trial, being replaced (after re‐randomisation) by another individual. There was one anterior capsular rim tear and one posterior capsule tear without vitreous loss. For the purposes of analysis of results, each of the six lens groups contained five patients." |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other source of bias |
Espindle 2005.
| Methods |
Study design: RCT Study grouping: parallel group, where both eyes of each participant were randomised to the same type of intervention Exclusions after randomisation: participants who were unable to understand or co‐operate with the contrast sensitivity examination were excluded, but no details were provided about these participants. Losses to follow‐up: of the 291 participants in the starting sample, 257 participants completed both a baseline HRQoL assessment and at least one of the two assessments following IOL implantation in the second eye and thus were eligible for the HRQoL analyses. Of the 34 ineligible participants, six failed to complete any of the three HRQoL assessments, 14 did not complete a baseline assessment, and 14 completed only a baseline assessment. 19 of the 34 ineligible participants had been implanted with the blue light–filtering IOL, while the other 15 had been implanted with the clear IOL. How missing data were handled: the primary analysis consisted of mean change to the third assessment or early termination, using the last observation carried forward approach to impute missing observations; if a score was missing at the third assessment, the score from the second assessment was carried forward, but no scores were carried forward from the baseline assessment. Analyses were also conducted on mean change to the second and third assessments without last observation carried forward to ensure the robustness of the findings. Reported power size calculation? yes |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people requiring bilateral extraction of age‐related cataracts with implantation of a posterior chamber IOL; aged ≥ 60 years of age, in good general and ocular health; expected to achieve at least 20/40 postoperative visual acuity, and passed both the Farnsworth D‐15 Panel Test and the Ishihara colour tests Exclusion criteria: people with alcoholism, Alzheimer’s disease, or terminal cancer; people with other eye conditions (including colour blindness or other colour‐vision deficiencies) or taking other medications that could interfere with the results to accurately measure any impact on colour vision and other outcomes postoperatively Comparison of study groups at baseline: as shown in Table 2, there were no treatment group differences at baseline with respect to age, ethnicity, or logMAR visual acuity lines in the first operative eye. However, there was a statistically higher percentage of women in the blue light–filtering IOL group than in the clear (non‐blue light filtering) IOL group. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | The primary treatment comparison analyses focused on the vision‐specific he 39‐item National Eye Institute Visual Functioning Questionnaire (NEI VFQ‐39) score, colour vision, and driving scales, and the generic 2‐item Short Form Health Survey (SF‐12) physical and mental component summary scales. Assessments were made at baseline before implantation in the first eye and 30‐60 days and 120‐180 days after implantation of the lens in the second eye. | |
| Identification |
Sponsorship source: Funding sources: Supported by Alcon Laboratories, Inc. Declaration of interest: Dr. Rajagopalan was employed at Alcon Laboratories, Fort Worth, Texas, USA, at the time this research was conducted Country: USA Setting: six clinical sites in the USA Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information provided for review Corresonding author's name: Derek Espindle, MA Institution: Mapi Values Email: derek.espindle@mapivalues.com Address: Derek Espindle, MA, 15 Court Square, Suite 620, Boston, Massachusetts 02108, USA |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation was administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Patients and HRQoL data collectors were masked to treatment;" Judgement comment: clearly states that participants and personnel not aware of which treatment was received |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Patients and HRQoL data collectors were masked to treatment; however, clinical investigators were not masked to treatment because the chromophore of the blue light–filtering IOL gives it a visible yellowish tint." Judgement comment: clearly stated that outcome assessors were masked, although investigators were not |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: missing data less than 20% (i.e., more than 80% follow‐up) and equal follow‐up in both groups and no obvious reason why loss to follow‐up should be related to outcome |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | High risk | Quote: "Supported by Alcon Laboratories, Inc. Dr. Rajagopalan was employed at Alcon Laboratories, Fort Worth, Texas, USA, at the time this research was conducted." Judgement comment: Industry funding and 1 author was an employee of the IOL manufacturer |
Espíndola 2012a.
| Methods |
Study design: RCT Study grouping: parallel group, with two study groups (non‐blue‐light filtering IOL vs different non‐blue‐light filtering IOL, n = 25 eyes each per comparison; non‐blue‐light filtering IOL vs blue‐light filtering IOL, n = 27 eyes each per comparison) Exclusions after randomisation: participants with incomplete follow‐up were excluded from the analyses Losses to follow‐up: participants with incomplete follow‐up were excluded from the analyses How missing data were handled: not reported Reported power size calculation? yes |
|
| Participants |
Baseline characteristics Blue‐light filtering IOLs
Non‐blue‐light filtering IOL
Inclusion criteria: people with visually significant bilateral cataract; people with no history of glaucoma Exclusion criteria: people with any ocular disease, such as corneal opacities or irregularity, dry eye, amblyopia, anisometropia, retinal abnormalities, surgical complications, IOL tilt, previous or current use of medications known to cause colour‐vision deficiencies, or incomplete follow‐up Comparison of study groups at baseline: paired eye study; no group differences reported and "no eye had intraoperative complications" |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOLs
|
|
| Outcomes | The primary outcome measures were contrast sensitivity (photopic and mesopic) and blue‐on‐yellow perimetry values (mean deviation and pattern standard deviation), at two years postoperatively Safety outcomes were the rate of intraoperative complications and the proportion of participants requiring capsulotomy at two years postoperatively |
|
| Identification |
Sponsorship source: Funding sources: no specific financial support Declaration of interest: no potential conflicts of interest for any authors Country: Brazil Setting: Study conducted in Ophthalmology Department of the University of São Paulo, São Paulo, Brazil Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Rodrigo F. Espíndola Institution: Ophthalmology Department of the University of São Paulo, São Paulo, Brazil Email: rodrigo166@uol.com.br Address: Rodrigo F. EspíndolaPraça das Hortências, 70 ‐ Itu (SP) ‐ 13301‐689 ‐ Brazil |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Low risk | Quote: "Sequenced and sealed envelopes containing the first type of IOL (Akreos AO or Akreos Fit; SN60AT or MA60AC) were prepared before surgery. An unscrubbed observer in the operating room opened the envelopes and assigned each patient." Judgement comment: clearly states how the intervention allocation was concealed |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "All patients and observers were masked about the IOL type implanted." Judgement comment: clearly states that all participants and observers were masked to the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The observers who conducted the postoperative visual evaluations did not have access to the randomization code or information about the surgical procedures." Judgement comment: clearly states that outcome assessors were masked |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "All patients completed 24 months of follow‐up." Judgement comment: although the paper states "All patients completed 24 months of follow‐up", an exclusion criterion was that "Patients with surgical complications or incomplete follow‐up were excluded". Although "there were no eyes with intraoperative complications," it is unclear whether follow‐up was 100‐percent for all participants as this was an exclusion criterion. |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Falkner Radler 2008.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant contributing to the analyses Exclusions after randomisation: none apparent Losses to follow‐up: none How missing data were handled: not reported; all participants were reported to complete the final study visit Reported power size calculation? yes |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: diagnosed vitreoretinal pathologic features, including diabetic vitreous haemorrhage, macular hole, epiretinal membrane, or persisting macula oedema, and coexisting significant cataract; the need for combined surgery, namely pars plana vitrectomy, phaco‐emulsification, and IOL implantation; age > 50 years Exclusion criteria: pseudophakia on the non‐study eye; the need for silicone oil tamponade; optic atrophy Comparison of study groups at baseline: "Patients’ baseline demographic data were comparable between both IOL groups (p>0.05, t test)." |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Intraoperative conditions for the surgeon, the functional outcome of the surgery (as related to BCVA, contrast sensitivity, colour vision and glare effects), complication rates (intraoperative and postoperative ) and vitreo‐retinal diagnoses, at seven days, one month and three months of follow‐up | |
| Identification |
Sponsorship source: Funding sources: none Declaration of interest: none for all authors Country: Austria Setting: the Ludwig Boltzmann Institute of Retinology and Biomicroscopic Laser surgery, Department of Ophthalmology, Rudolf Foundation Clinic, Vienna, Austria Comments: Date study conducted: 14 October 2004‐March 2006 Trial registration number: ClinicalTrials.gov NCT00537992 Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Christiane I. Falkner‐Radler Institution: The Ludwig Boltzmann Institute of Retinology and Biomicroscopic Lasersurgery Department of Ophthalmology, Rudolf Foundation Clinic Email: christiane.falkner‐radler@wienkav.at Address: The Ludwig Boltzmann Institute of Retinology and Biomicroscopic Laser Surgery, Department of Ophthalmology Rudolf Foundation Clinic, Juchgasse 25, A‐1030, Vienna, Austria |
|
| Notes | Interventions In all cases, phacoemulsification (scleral tunnel or clear corneal incision) and IOL implantation were followed by a vitreoretinal procedure. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Quote: "The patients included were assigned randomly to receive 30 clear UV‐filter IOLs (clear IOL group) and 30 yellow‐ blue light–filter IOLs (yellow IOL group)." Judgement comment: not reported how allocation was administered. Assignment is described as "random" but without further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information on masking; we assume that in the absence of reporting, patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "A masked statistical analysis for the questionnaire responses and the other main outcome parameters, namely mean differences between three‐month postoperative and baseline values for distance visual acuity (DVA), near visual acuity (NVA), contrast sensitivity, color vision, and glare effect for each IOL group was performed." Judgement comment: no information was provided in relation to the masking of outcome assessors (only the statistician); we assume that in the absence of reporting, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "No patient was lost to follow‐up, and all patients completed the three‐month postoperative follow‐up examination." Judgement comment: no participants were lost to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to a protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Hahsler 2004.
| Methods |
Study design: RCT Study grouping: parallel group study, with no further details relating to the allocation of the interventions Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: not reported Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Preoperative and postoperative findings were obtained regarding colour discrimination (using the Farnsowrth panel D‐15 test) and contrast perception (Pelli‐Robson contrast / sensitivity test); the time point for follow‐up was not reported. | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: Austria Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information provided for review First author's name: B Hahsler Institution: not reported Email: not reported Address: not reported |
|
| Notes | Conference abstract, in German | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient information to judge other sources of bias |
Hahsler 2005.
| Methods |
Study design: RCT Study grouping: parallel group, with inter‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL) Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
Inclusion criteria: not reported Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Functional acuity contrast test and contrast sensitivity; follow‐up period not reported | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: Austria Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors contacted for more information about abstract; no additional information provided for review First author's name: B Hahsler Institution: not reported Email: not reported Address: not reported |
|
| Notes | Conference abstract, in German | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient information in abstract to assess other potential sources of bias |
Hayashi 2006.
| Methods |
Study design: RCT Study grouping: parallel group, with bilateral implantation of the same intervention in both eyes, and data averaged between eyes for analyses Exclusions after randomisation: one participant was excluded due to an epi‐retinal membrane (the group assignment was not reported) Losses to follow‐up: of the 80 people enrolled, six were excluded from the analysis; four did not appear for a follow‐up examination because of scheduling conflicts, one refused the examination, and one had a clinically significant epiretinal membrane at the macula. Thus, 74 participants (92.5%) completed the examinations and remained in the analysis. How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: admission for bilateral cataract surgery Exclusion criteria: pathology of the cornea, retina or optic nerve; a history of ocular surgery or inflammation; a pupillary diameter < 6.0 mm after mydriasis; eyes scheduled for extracapsular cataract extraction; eyes of patients with diabetes; patients who anticipated any difficulty in follow‐up. Comparison of study groups at baseline: "No statistically significant difference was found between the groups (at baseline) regarding age, the ratio of men to women, manifest spherical equivalent, keratometric cylinder or pupillary diameter." |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Visual acuity, contrast visual acuity with and without a glare source under photopic (100 cd/m2) and mesopic (slightly higher luminance than typically used ‐ 5 cd/m2) conditions at two weeks and three months after surgery using the contrast sensitivity accurate tester The incidence of participants who noted cyanopsia at three months after surgery |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: "The authors have no proprietary interest in any of the materials described in this article" Country: Japan Setting: Hayashi Eye Hospital, 4‐7‐13 Hakataekimae, Hakata‐ Ku, Fukuoka 812, Japan Comments: Date study conducted: 3 November 2004‐20 April 2005 Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for the review Corresponding author's name: Ken Hayashi Institution: Hayashi Eye Hospital Email: hayaski‐ken@hayashi.or.jp Address: Hayashi Eye Hospital, 4‐7‐13 Hakataekimae, Hakata‐ Ku, Fukuoka 812, Japan |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The clinical research coordinator generated a code using a random number table." Judgement comment: the randomisation sequence was generated using a random number table by the research co‐ordinator. |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: method of allocation concealment not specified |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Patients and examiners were masked to the randomisation." Judgement comment: clearly stated that participants and personnel not aware of which treatment received |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Patients and examiners were masked to the randomisation. The surgeon, who was also the data analyst, did not participate in any of the examinations or in the data collection." Judgement comment: clearly stated that outcome assessors were masked |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "Of the 80 patients enrolled, six were excluded from the analysis; four did not appear for a follow up examination because of scheduling conflicts, one refused the examination, and one had a clinically significant epiretinal membrane in the macula. Thus, 74 patients (92.5%) completed the examinations and remained in the analysis." Judgement comment: missing data less than 20% (i.e., more than 80% follow‐up) and relatively equal follow‐up in both groups and no obvious reason why loss to follow‐up should be related to outcome |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other source of bias |
Hyunseok 2007.
| Methods |
Study design: RCT Study grouping: parallel group, involving 48 eyes from 42 individuals Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: not reported Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Wavefront analysis by iTrace (Tracey technologies), and contrast sensitivity test at three months post‐surgery | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors contacted for more information about abstract; no additional information provided for review. First author's name: Ahn Hyunseok MD Institution: not reported Email: not reported Address: not reported |
|
| Notes | AAO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient detail in abstract to judge whether other sources of bias are present |
Kara Junior 2011.
| Methods |
Study design: RCT Study grouping: parallel group, with paired‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL) Exclusions after randomisation: participants with incomplete follow‐up were not included in the analyses. Losses to follow‐up: during the five‐year study period, five participants were lost to follow‐up; therefore, 25 participants were considered in the analyses How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people with visually significant bilateral cataract and no history of colour vision deficiency were eligible for inclusion in the study. Exclusion criteria: ocular disease such as corneal opacity or irregularity, dry eye, amblyopia, anisometropia, glaucoma, retinal abnormalities; surgical complications; IOL tilt; previous or current use of medications known to cause colour‐vision deficiencies; incomplete follow‐up Comparison of study groups at baseline: paired‐eye trial, however participants who had surgical complications were excluded, and no details were provided about whether there were exclusions due to intraoperative complications. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | The primary outcome measures were contrast sensitivity, colour vision and macular findings at five years after surgery. | |
| Identification |
Sponsorship source: Funding sources: no funding sources listed Declaration of interest: "No author has a financial or proprietary interest in any material or method mentioned." Country: Brazil Setting: Ophthalmology Department, University of Sao Paulo, Sao Paulo, Brazil Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors contacted not contacted; no additional information used for review Corresponding author's name: Marcony R. Santhiago, MD Institution: Cole Eye Institute, Cleveland Clinic Email: marconysanthiago@hotmail.com Address: Cole Eye Institute Cleveland Clinic 1700 East 13th Street Apartment 15W, Cleveland, Ohio 44114, USA |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement comment: described as “double‐masked” with no information on who was masked |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement comment: described as “double‐masked” with no information on who was masked |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: missing data less than 20% (i.e., more than 80% follow‐up), equal follow‐up in both groups (as paired‐eye study) and no obvious reason why loss to follow‐up should be related to outcome |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other source of bias |
Kara Júnior 2006.
| Methods |
Study design: RCT Study grouping: parallel group, with inter‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL) Exclusions after randomisation: 46 patients had cataract surgery; 27 patients met the prespecified inclusion criteria Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: 46 patients had cataract surgery under similar preoperative conditions using the same phacoemulsification technique with a Legacy 20000 machine and NeoSoniX system (Alcon Laboratories, Inc.) and were randomised. 27 patients met the following inclusion criteria: visual acuity better than 20/40 in both eyes at least 1 year after surgery, stable intraocular pressures (IOP) throughout the 1‐year interval, and no signs or symptoms of glaucoma. Exclusion criteria: not reported Comparison of study groups at baseline: paired‐eye study; no significant inter‐group differences. Participants potentially excluded due to the nature of the inclusion criteria, and details about such participants are not included. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Blue‐yellow perimetry values at one year of follow‐up | |
| Identification |
Sponsorship source: Funding sources: not reported. Declaration of interest: no author had a financial or proprietary interest in any materials or methods mentioned. Country: Brazil Setting: cataract and glaucoma clinics of a medical school associated with a public hospital in Brazil Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for this review Corresponding author's name: Juliana Lopes Jardim, MD Institution: Hospital das Clinicas de Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil Email: Not reported Address: Juliana Lopes Jardim, MDAvenida Dr.Ene ´as de Carvalho Aguiar, 255, CEP: 05403‐000, São Paulo‐SP, Brazil |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The observers who conducted the postoperative visual evaluations did not have access to the randomization code or information about the surgical procedures." Judgement comment: clearly stated that outcome assessors were masked |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Judgement comment: 46 participants randomised, but only 27 included in analyses at one year |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Kennis 2004.
| Methods |
Study design: RCT Study grouping: parallel group, involving 71 people and 98 eyes (but with no further details) Exclusions after randomisation: participants with intraoperative or postoperative complications and posterior capsule opacification were excluded, but no information provided in relation to whether participants were excluded on these grounds. Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL 1
Non‐blue‐light filtering IOL 2
Inclusion criteria: people from 55‐85 years of age who had clinically significant cataract Exclusion criteria: people with ocular pathology other than cataract, neurologic or other disease known to affect contrast sensitivity (e.g. high hyperopia (> +6.0 D), high myopia (> −6.0 D), keratometric cylinder greater than 1.5 D). people with intraoperative or postoperative complications and posterior capsule opacification. Comparison of study groups at baseline: there were no statistically significant differences between groups, with respect to age, mean preoperative refractive error and best‐corrected spectacle acuity, at baseline. However, participants with intraoperative of postoperative complications and posterior capsule opacification were excluded. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL 1
Non‐blue‐light filtering IOL 2
|
|
| Outcomes | BCVA, pupil size and contrast sensitivity under mesopic and photopic conditions (with and without glare), at six months of follow‐up | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: Belgium or Switzerland (unclear which) Setting: eye hospital Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: we attempted to contact the study authors emailed on 1 September 2017 for information relating to the intra‐class correlation coefficient for the within‐person clustering of BCVA; we could not identify a contact email address for any of the authors, as this was not provided on this paper or identifiable from an extensive internet search. As a result we could not include these data in any meta‐analyses. Corresponding author's name: H. Kennis Institution: Department of Ophthalmology, University Hospital, Leuven Email: not reported Corresponding author's address: H. Kennis Dienst Oogziekten UZ Leuven Kapucijnenvoer 33B‐3000 Leuven |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not explicitly reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Kim 2011a.
| Methods |
Study design: RCT Study grouping: parallel group, involving 52 people and 68 eyes (participants received a mixture of unilateral IOL implantation and bilateral IOL implantation) Exclusions after randomisation: participants with poor co‐operation, complicated cataracts and any negative events resulting from cataract surgery were excluded from the study; no details about these participants were provided. Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1
Non‐blue‐light filtering IOL
Blue‐light filtering IOL group 2
Inclusion criteria: people who underwent cataract surgery and IOL implantation with otherwise normal eye findings Exclusion criteria: people with diabetes mellitus, poor co‐operation, glaucoma (diagnosed by intraocular pressure, visual field exam, optic nerve morphology, and retinal nerve fibre layer findings), complicated cataracts and any negative events resulting from cataract surgery Comparison of study groups at baseline: there were no significant differences among the three IOL groups with respect to visual acuity and spherical equivalence in the preoperative and postoperative phases. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Non‐blue‐light filtering IOL
Blue‐light filtering IOL 2
|
|
| Outcomes | Frequency doubling technique ‐ Humphrey matrix pattern standard deviation and mean deviation at two months of follow‐up | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no potential conflict of interest relevant to this article was reported Country: Korea Setting: Department of Ophthalmology and Visual Science, The Catholic University of Korea College of Medicine, Seoul, Korea Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Choun‐Ki Joo, MD, PhD Institution: Department of Ophthalmology and Visual Science, The Catholic University of Korea College of Medicine, Seoul, Korea Email: ckjoo@catholic.ac.kr Corresponding author's address: Choun‐Ki Joo Department of Ophthalmology and Visual ScienceSeoul St. Mary’s Hospital 505 Banpo‐dong, Seocho‐gu, Seoul 137‐040, Korea |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not explicitly reported. "Any negative events resulting from cataract surgery were excluded from the study," so it was not an intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Kim 2011b.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: not reported Losses to follow‐up: 11 eyes were excluded because participants refused to receive SD‐OCT imaging or receive follow‐up examinations. How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people who were undergoing phacoemulsification due to simple cataracts at the Department of Ophthalmology, Severance Hospital, Yonsei University College of Medicine, between February and September 2009. Exclusion criteria: conditions affecting retinal nerve fibre layer (RNFL) thickness measurements, such as diabetic retinopathy, glaucoma, degenerative or exudative retinopathy, optic nerve drusen, peripapillary atrophy and tilted disc syndrome; history of previous ocular surgery; vitreous opacity Comparison of study groups at baseline: "The participant characteristics are summarized in Table 1. There was no statistically significant difference between the two groups with respect to preoperative demographic findings." |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Peripapillary retinal nerve fibre layer thickness, measured using a Cirrus SD‐OCT, before and eight weeks after cataract surgery | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: "The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this paper." Country: Korea Setting: Department of Ophthalmology, Severance Hospital, Yonsei University College of Medicine Comments: Date study conducted: February 2009‐September 2009 Trial registration number: not reported Contacting study investigators: study authors contacted on 20 July 2016 with regard to the content of Tables 1‐10 (which were not provided in the main text or as supplementary material). Tables provided by Dr Kim via email (20 July 2016); Dr Kim was contacted again by email on 1 August 2016 regarding Table 2, which should report BCVA data, but does not (we asked whether it was possible to obtain these data, but no response was received). Corresponding author's name: Chan Yun Kim, MD, PhD Institution: Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine Email: kcyeye@yuhs.ac Corresponding author's address: Institute of Vision Research, Department of Ophthalmology Yonsei University College of Medicine, 134 Shinchon‐dong, Seodaemun‐gu, Seoul, 120–752, Korea |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information on masking. In the absence of reporting, assume patients and personnel were not masked |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking. In the absence of reporting, assume outcome assessors were not masked |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Judgement comment: missing data for 11/50 participants (22%) and unequal follow‐up between groups (n=23 eyes in blue‐light filtering IOL group, n=16 in clear IOL group) |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other source of bias |
Kuchenbecker 2004.
| Methods |
Study design: RCT Study grouping: parallel group, involving 15 participants (number of eyes not reported) Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: Non‐amblyopic patients between 60 and 80 years, with "inconspicuous" colour recognition (Ishihara) Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Visual acuity and contrast sensitivity at six weeks postoperatively | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: Germany Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors contacted to obtain further details about the abstract; no additional information provided for review First author's name: J Kuchenbecker Institution: Universitäts‐Augenklinik Magdeburg Email: not reported Corresponding author's address: not reported |
|
| Notes | Conference abstract, in German | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: study is described as open label |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: study is described as open label |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient information to judge other sources of bias |
Leibovitch 2006.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: one of the SN60 (blue‐light filtering) IOL participants was excluded early in the study as he refused to be operated on his other eye. Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people with age‐related cataracts requiring extraction, but an otherwise normal ocular examination. Exclusion criteria: people with other ocular pathologies, high hyperopia or myopia (6.00 D), or neurological diseases and patients using medications with a possible influence on contrast sensitivity or colour vision. Comparison of study groups at baseline: no significant differences, other than a difference in distribution by sex. A total of 10 participants were randomised to each group but one was dropped from the SN60 group (as they refused to be operated on the other eye). |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Distance BCVA (measured using a Snellen chart), contrast sensitivity (Pelli–Robson contrast sensitivity chart) and colour perception (Farnsworth–Munsell D‐15 panel test) at one, three and six months postoperatively The postoperative change in distance BCVA, considered as a dichotomous outcome, was interpreted from the reporting of the study results, "Preoperative BCVA in both groups ranged between 20/30 and 20/200. Postoperative BCVA after six months in the SN60 group was 20/20 or better in all eyes, except 1 (11%), which had a BCVA of 20/30. Postoperative BCVA in the SA60 group was 20/20 or better in all eyes." Intraoperative complications and postoperative complications at six months of follow‐up |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: Australia Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Igal Leibovitch Institution: Department of Ophthalmology and Visual Sciences, Royal Adelaide Hospital Email: leiboigal5@yahoo.com.au Corresponding author's address: Dr Dinesh Selva Department of Ophthalmology and Visual Sciences Royal Adelaide Hospital North Terrace Adelaide 5000 South Australia, Australia |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Low risk | Quote: "The patients were randomised to receive one of the two lenses by drawing a blank envelope for each patient out of a box of 20 envelopes. A note in each envelope stated whether an SA60 or SN60 lens would be implanted." Judgement comment: opaque envelopes used for allocation |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "All patients were operated by a single surgeon (GP) and were unaware of the type of IOL implanted." Judgement comment: Participants are reported to be masked, but there is no mention of whether personnel were masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: missing data is not explicitly described, but there appears to be 100% participant retention at six months |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Marshall 2005.
| Methods |
Study design: RCT Study grouping: parallel group, where both eyes were implanted with the same type of IOL and both eyes were used in the analyses (considered as independent samples) Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: all eyes that received a test or control IOL and had at least one postoperative examination were included in the postoperative analyses. Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people had to be healthy adults older than 60 years who had bilateral age‐related cataracts. people had to be willing and able to wait at least 30 days (but no more than 60 days) between cataract extraction procedures and had to successfully pass the Ishihara colour test and Farnsworth‐Munsell D‐15 colour perception test preoperatively. Exclusion criteria: people with retinal abnormalities, glaucoma, diabetic retinopathy, and previous or current use of medications known to cause colour‐vision deficiencies. Comparison of study groups at baseline: there were no statistically significant differences between the test and control groups in terms of age, sex, or race (Table 1). |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | People were examined 1‐2 days, 7‐14 days, 30‐60 days, 120‐180 days, and 330‐420 days after the first procedure. Screening for IOL implantation in the fellow eye was performed at the 30‐ to 60‐day postoperative examination. Distance BCVA was determined at all postoperative evaluations using the standard Snellen chart. Contrast sensitivity was evaluated at the 30‐ to 60‐day and at the 120‐ to 180‐day postoperative examinations using the CSV‐ 1000E contrast sensitivity unit (Vector Vision) calibrated to assure 85 cd/m2 luminance, under photopic and mesopic conditions. Colour perception was measured at the 30‐ to 60‐day and at the 120‐ to 180‐day postoperative examinations, using the Farnsworth‐Munsell D‐15 colour perception test. Clinical observations of the operative eyes and the IOLs were recorded at each postoperative examination. The occurrence of hyphema, hypopyon, pupillary block, cystoid macular edema, infection or endophthalmitis, retinal detachment, and secondary surgical intervention was noted, as was the presence of IOL tilt, decentration, or dislocation. At all visits through 120 to 180 days, posterior capsule opacification was graded subjectively by slitlamp biomicroscopy as none, clinically nonsignificant, clinically significant, or clinically significant requiring neodymium: YAG (Nd:YAG) laser posterior capsulotomy, using pre‐established criteria. |
|
| Identification |
Sponsorship source: Funding sources: sponsored by Alcon Laboratories, Inc. Declaration of interest: Drs. Cionni, Lehmann, and Maxwell are consultants to Alcon. No author has a financial or proprietary interest in the materials and methods mentioned Country: USA Setting: multicentre USA clinical trial Comments: Date study conducted: September 2000‐December 2001 Trial registration number: not reported Contacting study investigators: study authors contacted on 1 September 2017 for details relating to the intra‐class correlation for the within‐person clustering, for the outcome measures of: BCVA, proportion of people with cystoid macular oedema at six months, intraoperative complications, and postoperative complications; no response was received after more than one month. First author's name: John Marshall, PhD Institution: Department of Ophthalmology GKT, The Rayne Institute, St. Thomas’ Hospital, London Email: june.spacey@kcl.ac.uk Corresponding author's address: John Marshall Department of Ophthalmology GKT The Rayne Institute, St. Thomas’ Hospital London SE1 7EH, England |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: study described as 'patient‐masked' only, and thus personnel were not masked |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: study described as 'patient‐masked' only |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: although 150 participants implanted with natural IOL and 147 with control (bilateral) only those eyes that had at least 1 postoperative examination were included in the analyses which dropped the numbers to 135 and 127 for BCVA and 109 and 102 for colour. |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | High risk | Quote: "Philadelphia, Pennsylvania, USA, June 2002. Sponsored by Alcon Laboratories, Inc. Drs. Cionni, Lehmann, and Maxwell are consultants to Alcon. No author has a financial interest." Judgement comment: study was sponsored by Alcon Laboratories, and Drs Cionni, Lehmann and Maxwell were consultants to Alcon |
Mester 2008a.
| Methods |
Study design: RCT Study grouping: parallel group, with paired‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL). Exclusions after randomisation: 51 patients were screened and enrolled in the study. Four participants were not treated as specified in the study protocol and were excluded. Thus, 47 participants were randomised to treatment Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL
Inclusion criteria: Bilateral cataract for which phacoemulsification and posterior IOL implantation were planned in both eyes. No prior ophthalmic surgical procedures. Age from 50‐80 years, inclusive. Bilateral potential visual acuity of 0.5 (20/40 Snellen) or better as estimated by the surgeon. No known colour‐vision deficiency. Normal colour‐vision test results on Ishihara plates. Surgery in both eyes performed by same surgeon within six weeks. Suitable for study participation according to the judgment of the clinical investigator Exclusion criteria: congenital ocular abnormalities. Inadequate visualisation of the fundus. IOL power calculation < +10.0 diopters (D) or > +30.00 D. Astigmatism > 2.5 D. intraoperative complications (e.g. capsule rupture, bleeding). Participation in another study at the same time or 14 days before enrolment in the study. People with a history of uveitis and current intraocular inflammation, uncontrollable glaucoma, proliferative diabetic retinopathy, or retinal detachment Comparison of study groups at baseline: the preoperative parameters for screened and enrolled participants were similar for the two IOL types, with no statistically significant differences in age; sex; UCVA; BCVA; IOP; corneal topography; photopic, mesopic, or scotopic pupil diameter; axial length; or endothelial cell density. It should be noted that participants with intraoperative complications were excluded, and no data were provided in relation to these potential exclusions, although the authors did state that "no serious ocular adverse events occurred during the study,” and "there were no pathologic findings on fundus examination in any eye at any follow‐up visit." |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Uncorrected and BCVA, pupil size, contrast vision (Early Treatment Diabetic Retinopathy Study (ETDRS) chart), functional acuity contrast test (photopic, mesopic, mesopic with glare), and colour discrimination (Farnsworth‐Munsell 100‐hue test, photopic and mesopic) at six and 12 months postoperatively | |
| Identification |
Sponsorship source: Funding sources: supported by Hoya, Frankfurt, Germany. Declaration of interest: no author has a financial or proprietary interest in any material or method mentioned Country: Germany Setting: five clinical ophthalmology centres in Germany Comments: Date study conducted: March 2005‐May 2007 Trial registration number: not reported Contacting study investigators: study authors contacted on 1 September 2017, regarding:
No response was received from the authors after more than one month, and as a result we could not incorporate these data in our meta‐analyses. First author's name: Ulrich Mester, MD Institution: Department of Ophthalmology Bundesknappschaft’s Hospital Email: sek‐augen@kksulzbach.de Corresponding author's address: Ulrich Mester Department of Ophthalmology Bundesknappschaft’s Hospital An der Klinik 10, G‐66280 Sulzbach Germany |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provide on masking. We assume that in absence of reporting on this patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting on this outcome, assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Fifty‐one patients were screened and enrolled in the study. Four patients were not treated as specified in the study protocol and were excluded. Thus, 47 patients were randomised to treatment arm 1‐1 (operation sequence: yellow IOL, clear" Judgement comment: missing data < 20%, intra‐individual comparative study, however no information is provided on four participants treated off protocol and excluded from the analysis. |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry. |
| Other bias | High risk | Quote: "Supported by Hoya, Frankfurt, Germany." Judgement comment: the study was funded by the IOL manufacturer. |
Monnet 2009.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: Two IOLs in Group 3 (blue‐light filtering IOL group) were placed with one haptic in the capsular bag and one haptic outside the capsular bag; these two participants were also excluded from the final statistical analyses. Losses to follow‐up: one participant in Group 2 (one of the two non‐blue‐light filtering IOL groups) was lost to follow‐up and was not included in the final statistical analyses. How missing data were handled: it appears that missing data were excluded from the analysis. Reported power size calculation? yes |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL (Group 3)
Non‐blue‐light filtering IOL1 ‐ MA60AC (Group 1)
Non‐blue‐light filtering IOL2 ‐ SA60AT (Group 2)
Inclusion criteria: people ≥ 60 years, of either sex, of any race, and scheduled for cataract surgery; in good general and ocular health, willing to attend all postoperative visits, and expected to achieve postoperative visual acuities of 20/40 or better Exclusion criteria: people with a history of uveitis, uncontrolled diabetes, diabetic retinopathy, Sjogren syndrome, trauma to the operative eye, use of anti‐inflammatory medications for any reason, use of topical prostaglandin analogues for ocular hypertension or glaucoma, bleeding tendencies, congenital ocular abnormality, or a nonfunctioning fellow eye. people with intraoperative complications including capsule tears, significant anterior chamber hyphema, zonule rupture, or out‐of‐the‐bag IOL implantation. people at risk for intraoperative complications by virtue of pseudoexfoliation syndrome or poor pupil dilation (6.0 mm). people having multiple planned procedures (i.e. cataract and trabeculectomy or corneal transplantation), except those having concurrent relaxing keratotomy for astigmatism correction. Comparison of study groups at baseline: no statistically significant differences between groups in any parameter at baseline, but no data reported for those participants who appear to be excluded from the analyses (n = 1 participant from Group 2, and n = 2 participants from Group 3, but all of Group 2 were included in the demographic data). |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL (Group 3)
Non‐blue‐light filtering IOL1 ‐ MA60AC (Group 1)
Non‐blue‐light filtering IOL2 ‐ SA60AT (Group 2)
|
|
| Outcomes | Postoperative evaluations were performed at one week, one month and three months. All visits included assessment of distance BCVA after manifest refraction, cells, flare, and adverse events. The primary objective of the study was to compare postoperative inflammation (presence of anterior chamber cells and flare) between the three IOL models. Anterior chamber cells were initially graded on a 5‐point scale (0‐4); however, because all eyes were graded 0 or 1, except for 1 eye that was graded 2, values were dichotomised into 2 categories: (1) cell or (2) no cell. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no author has a financial or proprietary interest in any material or method mentioned Country: France Setting: Service d’Ophtalmologie, Universite ´Paris Descartes Hospital Cochin, Paris, France Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Antoine P. Brezin, MD, PhD Institution: Universite ´ Paris Descartes, Assistance Publique Hopitaux de Paris, Hopital Cochin, Service d’Ophtalmologie Email: antoine.brezin@cch.aphp.fr Corresonding author's address: Antoine P. Brezin Universite ´ Paris Descartes, Assistance Publique Hopitaux de ParisHopital Cochin, Service d’Ophtalmologie 27 rue du Faubourg Saint‐Jacques 75014 Paris, France |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned in a 1:1:1 ratio to receive one of the IOL models according to a randomization list." Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "single‐center unmasked 3‐month study" Judgement comment: study is described as "unmasked" |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "single‐center unmasked 3‐month study" Judgement comment: study is described as "unmasked" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: missing data < 20% (i.e. more than 80% follow‐up) and equal follow‐up in the intervention groups |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Neumaier‐Ammerer 2010.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: not reported Losses to follow‐up: of the 80 participants (80 eyes) enrolled, 76 (95%) completed the study. Four participants (5%) did not attend the final follow‐up visit. How missing data were handled: it appears that missing data were excluded from the analysis Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1
Non‐blue‐light filtering IOL group 1
Blue‐light filtering IOL group 2
Non‐blue‐light filtering IOL group 2
Inclusion criteria: people with no history of ocular surgery or ocular pathology, such as corneal disorders, uveitis, disorders of the vitreous body or retina, glaucoma, or amblyopia Exclusion criteria: people with known colour deficiencies or problems concentrating Comparison of study groups at baseline: there were no statistically significant differences between IOL groups in pre‐operative age, cataract stage, visual acuity, contrast sensitivity, or colour perception. However, not all of the baseline data were reported, as it excluded four participants who did not complete the study. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Non‐blue‐light filtering IOL 1
Blue‐light filtering IOL 2
Non‐blue‐light filtering IOL 2
|
|
| Outcomes | People were examined postoperatively at one week and eight weeks. Every visit included anterior and posterior segment evaluation, intraocular pressure, corrected distance visual acuity and corrected near visual acuity. Contrast sensitivity was measured with Pelli‐Robson charts and the 1000E contrast sensitivity unit (CSV‐1000E, Vector‐Vision) with a constant test luminance level of 85 candelas/ m2. Contrast sensitivity with glare was assessed using the halogen glare test on the contrast sensitivity unit. Corrected distance visual acuity and the Pelli‐Robson test were evaluated at three light intensities (1000 lux, 100 lux, and 10 lux) to simulate day‐light and twilight. Colour discrimination was tested with the Roth 28 Hue Test. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no author has a financial or proprietary interest in any material or method mentioned Country: Austria Setting: Ludwig Boltzmann Institute of Retinology and Biomicroscopic Laser‐Surgery, Department of Ophthalmology, Rudolf Foundation Clinic, Vienna, Austria Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Beatrix Neumaier‐Ammerer, MD Institution: Department of Ophthalmology, Rudolf Foundation Hospital, Ludwig Boltzmann Institute for Retinologie and Biomicroscopic Laser surgery Email: beatrix.neumaier‐ammerer@wienkav.at Corresponding author's address: Beatrix Neumaier‐Ammerer Department of Ophthalmology, Rudolf Foundation Hospital, Ludwig Boltzmann Institute for Retinologie and Biomicroscopic Lasersurgery Juchgasse 25, A‐1030 Vienna, Austria |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "randomised (envelope method)" Judgement comment: insufficient information regarding "envelope method" |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "double‐blind study" Judgement comment: described as “double masked” with no information on who was masked |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "prospective randomised double‐blind study" Judgement comment: described as “double blind” with no information on who was masked |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "Of the 80 patients (80 eyes) enrolled, 76 (95%) completed the study." Judgement comment: high participant retention (95%) |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Nolan 2009.
| Methods |
Study design: RCT Study grouping: parallel group, involving 42 participants; it does not state whether the IOLs were unilaterally or bilaterally implanted Exclusions after randomisation: one participant from the AIOL group withdrew after Visit 1 (V1), two after Visit 2 (V2), and two after Visit 4 (V4) (n = 5 withdrawals in total). Three participants from the ANIOL group withdrew after V1, two after V2, and two after V4 (n = 7 withdrawals in total). The reasons for withdrawal were as follows: illness (non‐ocular); participant deceased; logistics of transport; and not interested in participating further Losses to follow‐up: Of the 42 participants recruited, 30 attended all study visits (one week before surgery, one week after surgery, and three, six, and 12 months after surgery: V1, V2, V3, V4, and V5, respectively) How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group (ANIOL group)
Non‐blue‐light filtering IOL group (AIOL group)
Inclusion criteria: people scheduled for cataract surgery at Waterford Regional Hospital Exclusion criteria: pre‐operative logMAR visual acuity of less than 0.5 (the minimum required for reliable measurement of MPOD) and those with any evidence of macular disease Comparison of study groups at baseline: groups were similar in age (P = 0.370) and sex distribution. The mean BMI was higher in the AIOL group compared with the ANIOL group (P = 0.017) |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL (ANIOL)
Non‐blue‐light filtering IOL (AIOL)
|
|
| Outcomes | The spatial profile of MPOD (i.e. at 0.25°, 0.5°, 1.0°, and 1.75° eccentricity) was measured with customised heterochromatic flicker photometry (cHFP) one week before and one week after surgery, and at three, six, and 12 months after surgery. Serum concentrations of lutein and zeaxanthin were measured at each study visit. BCVA, reported as a "Visual Acuity Rating" at 12 months postoperatively. |
|
| Identification |
Sponsorship source: Supported in full by Alcon Laboratories Inc., Fort Worth, Texas. Disclosure: "J.M. Nolan, Alcon Laboratories Inc. (F); P. O’Reilly, Alcon Laboratories Inc. (F); J. Loughman, Alcon Laboratories Inc. (F); J. Stack, Alcon Laboratories Inc. (F); E. Loane, Alcon Laboratories Inc. (F); E. Connolly, Alcon Laboratories Inc. (F); S. Beatty, Alcon Laboratories Inc. (F) The publication costs of this article were defrayed in part by page charge payment. This article must therefore be marked “advertisement” in accordance with 18 U.S.C. §1734 solely to indicate this fact." Country: Ireland Setting: Waterford Regional Hospital, Ireland Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information provided for review Authors name: John M. Nolan Institution: Macula Pigment Research Group, Waterford Institute of Technology, Cork Road, Waterford, Ireland Email: jnolan@wit.ie Address: Macula Pigment Research Group, Waterford Institute of Technology, Cork Road, Waterford, Ireland |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "The trial was conducted in a double‐blind, randomised, controlled fashion." Judgement comment: described as “double blind” with no information on who was masked |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement comment: described as “double blind” with no information on who was masked |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "Forty‐two patients were recruited. The patients were randomised to receive either the AIOL (n = 21) or the ANIOL (n = 21) implant as a lens replacement in their cataract surgery. Of the 42 patients recruited, 30 attended all study visits (one week before surgery, one week after surgery, and three, six, and 12 months after surgery: V1, V2, V3, V4, and V5, respectively). One patient from the AIOL group withdrew after V1, two after V2, and two after V4 (n = 5 withdrawals in total). Three patients from the ANIOL group withdrew after V1, two after V2, and two after V4 (n = 7 withdrawals in total). The reasons for withdrawal were as follows: patient illness (non‐ocular); patient deceased; logistics of transport; and not interested in participating further." |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | High risk | Quote: "Supported in full by Alcon Laboratories Inc., Fort Worth, Texas... The publication costs of this article were defrayed in part by page charge payment. This article must therefore be marked “advertisement” in accordance with 18 U.S.C. §1734 solely to indicate this fact." Judgement comment: industry funding (Alcon Laboratories), who manufactured the interventions |
Pandita 2007.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: not reported Losses to follow‐up: 109 patients, from 120 randomised, completed the three‐month follow‐up. Of 120 participants (eyes), three were transferred to a distant destination, one developed cystoid macular edema, one became seriously ill, one died, two returned at the five‐month follow‐up, and three refused to return. How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Non‐blue‐light filtering IOL group
Blue‐light filtering IOL group 1 (SN60AT)
Blue‐light filtering IOL group 2 (SN60WF)
Inclusion criteria: people aged 50‐70 years and scheduled for phacoemulsification for uncomplicated senile cataracts with in‐the‐bag implantation of an AcrySof IOL. Exclusion criteria: complicated cataract, coexisting ocular pathology, glaucoma, axial length greater than 25.0 mm, nondilating pupils, history of intraocular surgery, laser therapy, retinopathy, optic nerve or macular diseases, refusal or unable to maintain follow‐up, diabetes with or without retinopathy, preoperative and postoperative astigmatism greater than 1.5 diopters (D), residual posterior capsule plaque, postoperative best corrected visual acuity (BCVA) 20/25, and posterior capsule opacification. Eyes with intraoperative complications such as posterior capsule tear, zonular dialysis, or uveal manipulation. Comparison of study groups at baseline: there was no statistically significant difference in visual acuity, age, and sex ratio between the three groups. Only 109 of the 120 randomised participants are included in the analysis and reported in baseline characteristics. |
|
| Interventions |
Intervention characteristics Non‐blue‐light filtering IOL
Blue‐light filtering IOL 1
Blue‐light filtering IOL 2
|
|
| Outcomes | The main outcome measure was the difference in contrast sensitivity between IOLs at each spatial frequency. Contrast sensitivity, measured using the CSV‐1000E contrast sensitivity chart test face (Vector Vision) at three, six, 12, and 18 cycles per degrees (cpd) under photopic conditions (85 cd/m2) and mesopic conditions (2.7 cd/m2) with 4.0 mm and 6.0 mm fixed central apertures, with and without glare, at three months postoperatively. The outcome measure was distance BCVA, measured at three months postoperatively. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no author has a financial or proprietary interest in any material or method mentioned Country: India Setting: ladevi Cataract IOL Research Centre, Ahmedabad, India Comments: Date study conducted: December 2005‐February 2006 Trial registration number: not reported Contacting study investigators: trials authors contacted on 14 August 2017 regarding contrast sensitivity unit of error (specifically, whether it was the SD or a different unit or error); no response was received to this email. As a result, we could not incorporate these data in a meta‐analysis. Corresponding author's name: Dr Abhay R Vasavada Institution: Iladevi Cataract Research Centre, Raghudeep Eye Clinic Email: icirc@abhayvasavada.com Corresponding author's address: Abhay R. Vasavada Iladevi Cataract IOL Research Centre Raghudeep Eye Clinic, Gurukul Road, Memnagar, Ahmedabad–380 052, India |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Computer‐generated random numbers" Judgement comment: computer generated list used to assign interventions |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "triple‐masked trial (neither participant nor investigator responsible for patients was aware of IOL type)" Judgement comment: clearly stated that participants and personnel not aware of which treatment received |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Judgement comment: clearly stated that outcome assessors were masked |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "The drop‐out was 11 of 120 patients (9.2%)." Judgement comment: missing data less than 20% (i.e., more than 80% follow‐up) and equal follow‐up in both groups and no obvious reason why loss to follow‐up should be related to outcome. |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Raj 2005.
| Methods |
Study design: RCT Study grouping: parallel group, with paired‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL) Exclusions after randomisation: eyes with intraoperative complications such as posterior capsule tear, zonular dialysis, or uveal manipulation that could lead to postoperative cystoid macular oedema were also excluded. However, none of the patients were excluded because of intraoperative manipulations. Losses to follow‐up: all participants maintained their follow‐up schedule, and none of the participants dropped out of the study. How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people > 50 years of age with a congenital colour deficiency and senile bilateral uncomplicated cataracts with a visual acuity of > 20/200 on the Snellen visual acuity chart with all types of cataract: nuclear (type 1), cortical (types 2 and 3), posterior subcapsular (type 4), or mixed cataracts and all grades of cataract (in a nuclear sclerosis grading system from 1‐5) Exclusion criteria: people with mature cataracts, traumatic cataracts, glaucoma, history of intraocular surgery, laser therapy, retinopathy, or optic nerve or macular diseases; who refused to or were unable to maintain follow‐up; with diabetes with or without retinopathy; and those on medications such as chloroquine, digitalis, and indomethacin. Eyes with intraoperative complications such as posterior capsule tear, zonular dialysis, or uveal manipulation that could lead to postoperative cystoid macular oedema Comparison of study groups at baseline: paired‐eye study. All participants were moderate red–green anomalous trichromats. However, those randomised but excluded from the analysis were not adequately described. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | The main outcome measure was to detect an increase in the error scores on the Ishihara plates and an increase in the number of diametrical crossings in the circular diagram on the D‐15 test after implantation of AcrySof Natural IOL (blue‐light filtering IOL), at one month, three months and six months postoperatively. | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no author has a financial or proprietary interest in material or method mentioned. Country: India Setting: Iladevi Cataract IOL Research Centre, Raghudeep Eye Clinic Comments: Date study conducted: December 2002‐February 2004 Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author's name: Abhay R Vasavada, MS, FRCS Institution: Iladevi Cataract IOL Research Centre, Raghudeep Eye Clinic Corresponding author's mail: shailad2@sancharnet.in Address: Abhay R Vasavada Iladevi Cataract IOL Research Centre Raghudeep Eye Clinic Gurukul Road, Memnager Ahmedabad 380 052, India |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Low risk | Quote: "the circulating nurse in the operation theater opened 1 of the 30 preprepared envelopes containing 2 options:" Judgement comment: random assignment with pre‐prepared envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "neither participant nor the investigator responsible for the patients knew the eye assigned." Judgement comment: clearly stated that participants and personnel not aware of which treatment received |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "double‐masked trial (neither participant nor the investigator responsible for the patients knew the eye assigned to the test IOL)." Judgement comment: although it states that the trial was "double‐masked" with respect to participants and investigators being masked, it is unclear whether outcome assessors were also masked. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: even though it states in exclusion criteria section "Eyes with intraocular complications... were also excluded" in the Results section it states "none of the patients was excluded because of intraocular manipulations." No participant dropout |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Rocha 2006a.
| Methods |
Study design: RCT Study grouping: parallel group trial involving a total of 120 eyes, with no further details provided Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1
Non‐blue‐light filtering IOL group
Blue‐light filtering IOL group 2
Inclusion criteria: not reported Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Blue‐light filtering IOL 2
Non‐blue‐light filtering IOL
|
|
| Outcomes | Distance BCVA, contrast sensitivity (Pelli–Robson chart, Optec® 6500, performed under photopic and mesopic conditions, with and without glare) and wavefront abberation analysis (total root mean square and mean higher order abberations), at 30 and 90 days postoperatively. | |
| Identification |
Sponsorship source: Funding sources: none Declaration of interest: none Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: K M Rocha Institution: not reported Email: not reported Address: not reported |
|
| Notes | ARVO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in the absence of reporting on this, patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in the absence of reporting on this, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient information within abstract to judge other potential sources of bias |
Rocha 2006b.
| Methods |
Study design: RCT Study grouping: parallel group, involving a total of 60 people and 120 eyes, with no further details regarding how data were analysed Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1
Non‐blue‐light filtering IOL
Blue‐light filtering IOL group 2
Inclusion criteria: not reported Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Blue‐light filtering IOL 2
Non‐blue‐light filtering IOL
|
|
| Outcomes | Total and high‐order wavefront aberrations and contrast sensitivity at 30 and 90 days postoperatively | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review Corresponding author;s name: Karolline M Rocha, MD Institution: not reported Corresponding author's email: not reported Address: not reported |
|
| Notes | AAO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting on this, patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting on this, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient information to judge other potential sources of bias from the abstract |
Rocha 2007.
| Methods |
Study design: RCT Study grouping: parallel group, involving 60 participants (120 eyes) with paired‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL) Exclusions after randomisation: not reported Losses to follow‐up: one participant was lost at the 60‐day follow‐up visit because of unrelated health problems. How missing data were handled: wavefront measurement for a 5‐mm pupil diameter was not acquired in 13 eyes with either decentered IOLs, capsular constriction, or a small capsulorhexis. 35 eyes in AcrySof IQ group, 36 eyes in AcrySof SN60AT group, and 34 eyes in the Sensar AR40 group completed all follow‐up examinations. Although specifics of how missing data were handled is not described. Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1
Non‐blue‐light filtering IOL group
Blue‐light filtering IOL group 2
Inclusion criteria: people with visually significant bilateral senile cataracts, no other ocular diseases, corneal astigmatism less than 2.0 diopters (D), and potential acuity better than 0.2 logarithm of the minimum angle of resolution units (Guyton‐Minkowsky Potential Acuity Meter; MARCO Ophthalmic, Inc., Jacksonville, FL) Exclusion criteria: people with glaucoma, retinal pathologic features, corneal opacities or irregularities, dry eye, amblyopia, anisometropia, intraoperative complications, and decentration between pupil and IOL more than 0.4 mm, estimated by retroillumination and digital photos Comparison of study groups at baseline: there were no statistically significant differences in age, preoperative simulated mean keratometry, and axial length across study groups. Unclear whether baseline characteristics excludes some participants (15 eyes). It should also be noted that participants with intraoperative complications were excluded, and no data are provided in relation to these potential exclusions. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Non‐blue‐light filtering IOL
Blue‐light filtering IOL 2
|
|
| Outcomes | Participants were examined before surgery and at one, seven, 15, 30, and 90 days after surgery. The main outcome measures were spherical aberration and depth of focus (by means of distance‐corrected near and intermediate visual acuity) at 90 days after surgery. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: the authors have no financial interest in the technology described. Country: Brazil Setting: Department of Ophthalmology, Paulista School of Medicine, Federal University of São Paulo Comments: Date study conducted: February 2005‐October 2005 Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Karolinne Maia Rocha, MD Institution: Department of Ophthalmology, Paulista School of Medicine, Federal University of São Paulo, São Paulo, Brazil Email: karolinne@oftalmo.epm.br Corresponding author's address: Karolinne Maia Rocha Rua 3 de Maio, 130/124, São Paulo–SP, 04044‐020 Brazil |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: missing data less than 20% (i.e., more than 80% follow‐up) and equal follow‐up in both groups and no obvious reason why loss to follow‐up was related to outcome |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Schmack 2012.
| Methods |
Study design: RCT Study grouping: parallel group, with paired‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL) Exclusions after randomisation: baseline characteristics exclude those potentially excluded post‐randomisation for various reasons including intraoperative and postoperative complications, and no details are provided about these potential participants. Losses to follow‐up: three participants were lost to follow‐up because of private reasons (n = 2) and non‐study‐related medical reasons (n = 1). How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people who were sequentially admitted for bilateral cataract phacoemulsification with implantation of an IOL between April 2007 and November 2007; aged ≥ 50 years who were likely to complete all study visits and had a potential postoperative corrected distance visual acuity (CDVA) of 0.30 or better (logMAR). Exclusion criteria: people with active or previous ocular disease of the cornea, iris, retina, or optic nerve with potential impact on the visual acuity; colour vision deficiency; intraocular inflammation (iritis or uveitis); monocular status; history of intraocular surgery; uncontrolled systemic disease; diabetes mellitus; neurologic disease; and unavailable for follow‐up. People with a preoperative cycloplegic pupil diameter of 5.0 mm or less and surgical or postoperative complications, including vitreous loss, capsule tears, or prolonged intraocular inflammation. Comparison of study groups at baseline: participants received one each of a orange (blue‐light filtering) and clear (UV‐filtering) IOL. Baseline characteristics exclude those potentially excluded postrandomisation for various reasons including intraoperative and postoperative complications. There were no statistically significant differences in uncorrected distance visual acuity, corrected distance visual acuity, or contrast sensitivity with or without glare between the two IOL groups. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Participants were evaluated at the time of enrolment (two days before surgery) and one month, three months, and six months after surgery for each eye. Primary outcome measures were corrected distance visual acuity under scotopic (1 candela (cd)/m2) and photopic (85 cd/m2) conditions, colour vision, and contrast sensitivity with and without glare. Uncorrected distance visual acuity (UDVA) and patient satisfaction were defined as secondary outcome measures. The UDVA was tested under photopic conditions only. The postoperative change in distance BCVA, considered as a dichotomous outcome, was interpreted from the reporting of the study results in Tables 2 and 3, which provides the range of BCVA values and indicates that there were no individuals with a loss of BCVA of at least three lines, in any of the study groups. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no author has a financial or proprietary interest in any material or method mentioned Country: Germany Setting: Department of Ophthalmology, Ruhr University, Bochum, Germany Comments: Date study conducted: April 2007‐November 2007 Trial registration number: not reported Contacting study investigators: study authors were emailed on 1 September 2017, for information regarding:
No response was received after at least one month of contacting the authors, and as a result these data were not able to be included in our meta‐analyses. First author's name: Ingo Schmack, MD Institution: Department of Ophthalmology, Ruhr University Email: ingo.schmack@kk‐bochum.de Corresponding author's address: Ingo Schmack Department of Ophthalmology, Ruhr University In der Schornau 23‐25, 44892 Bochum, German |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Eye was randomised before IOL implantation using an envelope technique." Judgement comment: trial is described as "randomised" and used "envelope technique" to conceal allocation but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "double‐blind randomised masked fashion." Judgement comment: described as “double blind” with no specific information on whether participants and personnel were masked |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The individual who was responsible for the follow‐up examinations and data acquisition was blinded and not aware of which IOL was implanted in the eye being evaluated." Judgement comment: clearly stated that outcome assessors were masked |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: reports the number (22 patients) who completed the study not how many were excluded post‐randomisation for "surgical or postoperative complications" |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Schmidinger 2008.
| Methods |
Study design: RCT Study grouping: parallel group, with paired‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL) Exclusions after randomisation: of the 31 participants (enrolled), one was excluded because of subjectively disturbing vitreous floaters and two because of previously undetected macular drusen Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people with no history of corneal disorders, no abnormal pupil reaction, no sign of inflammation, no opacification of optic media apart from cataract, and no retinal disorders. Exclusion criteria: people with systemic disease or those having treatment known to affect colour perception. Based on specular microscopy, patients with evident signs of macular alteration or other ocular disease after surgery. Comparison of study groups at baseline: all participants had a similar cataract grade in both eyes. Baseline age was reported for 28 of the 31 participants. It should be noted that "patients with evident signs of macular alteration or other ocular disease after surgery were not included in the study", however "no intraoperative or postoperative complications or adverse events occurred." |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Distance BCVA, colour contrast sensitivity (measured using heterochromic flicker), central and peripheral tritan colour contrast sensitivities (measured using the Moorfields Vision System, CH Electronics) at three months postoperatively. The primary outcome measure was colour contrast sensitivity for short wavelengths of visible light at three months postoperatively. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no author had a financial or proprietary interest in any material or method mentioned Country: Austria Setting: Medical University of Vienna, Department of Ophthalmology, Vienna, Austria Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Gerald Schmidinger, MD Institution: Department of Ophthalmology, Medical University of Vienna Email: gerald.schmidinger@meduniwien.ac.at Corresponding author's address: Gerald Schmidinger Department of Ophthalmology, Medical University of Vienna Waehringer Guertel 18‐20, A‐1090 Vienna, Austria |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "double‐blind study" Judgement comment: study is described as "double‐blind" without specific information on how participants and personnel were masked |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The investigator performing the test was blind to the type of IOL implanted." Judgement comment: clearly stated that outcome assessors were masked |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Judgement comment: missing data less than 20% (i.e., more than 80% follow‐up) and no obvious reason why loss to follow‐up should be related to outcome |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Schmoll 2014.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: in all, 108 participants were recruited (including 21 age‐matched "control" participants, who did not receive an IOL and were not included these analyses), of whom 80 completed the study. Of the 28 who did not, 26 voluntarily declined to attend for the second test appointment, one had uncontrolled glaucoma and one required intercurrent hospital admission for an exacerbation of chronic obstructive pulmonary disease. Losses to follow‐up: as described above How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: participants were voluntarily recruited from routine cataract assessment clinics after providing informed consent. Participants were included regardless of whether they were being assessed for first‐ or second‐eye cataract surgery, or as controls. Exclusion criteria: participants unable to read the N48 test display on the reaction time task, those diagnosed with Parkinson’s Disease or dementia, any intercurrent illness requiring hospital admission, any previous ophthalmic history involving retinal damage including proliferative diabetic retinopathy, diabetic macular oedema, exudative AMD, central retinal artery or vein occlusion, and retinal detachment surgery. Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Choice reaction time (CRT) and the Epworth Sleepiness Score (ESS), at three months postoperatively | |
| Identification |
Sponsorship source: Funding sources: not commissioned Declaration of interest: no competing interests Country: Scotland Setting: St Johns Hospital, Livingston, United Kingdom Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Dr Conrad Schmoll Institution: Princess Alexandra Eye Pavilion Email: conradschmoll@gmail.com Corresponding author's address: Conrad Schmoll Princess Alexandra Eye Pavilion 45 Chalmers Street, Edinburgh EH3 9HA, UK |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "prospective randomised" Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Participants undergoing first‐eye cataract surgery were randomised to receive either a blue‐blocking IOL (Alcon Acrysof SN60WF) or a UV‐blocking IOL (AMO Tecnis ZCB00), and were masked as to which IOL type had been implanted. Study protocol dictated that participants undergoing second‐eye cataract surgery would receive an identical lens to their previous one. These patients had not been issued with information cards after their first‐eye surgery and were therefore unaware of which lens type they received." Judgement comment: participants were reported to be masked; although personnel were reported to be masked, this is not anticipated to significantly affect the study outcomes as most outcome measures were participant‐reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement comment: unclear whether outcome assessors were masked |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "108 participants were recruited, of whom 80 completed the study. Of the 28 who did not, 26 voluntarily declined to attend for the second test appointment, one had uncontrolled glaucoma and one required intercurrent hospital admission for an exacerbation of chronic obstructive pulmonary disease." Judgement comment: overall follow‐up < 80%, and follow‐up in each group not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Soriano 2006.
| Methods |
Study design: RCT Study grouping: parallel group, involving a total of 120 eyes (and an unspecified number of participants) Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1
Non‐blue‐light filtering IOL group
Blue‐light filtering IOL group 2
Inclusion criteria: not reported Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Non‐blue‐light filtering IOL
Blue‐light filtering IOL 2
|
|
| Outcomes | Near visual acuity, wave‐front analysis and pupil diameter at 60 days postoperatively | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information provided for review First author's name: Eduardo S Soriano, MD Institution: not reported Email: not reported Corresponding author's address: not reported |
|
| Notes | AAO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "randomised prospective study" Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information on masking. We assume that in absence of reporting on this, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient information provided within abstract to judge other potential sources of bias |
Ueda 2005.
| Methods |
Study design: RCT Study grouping: parallel group, involving 31 participants (although the number of eyes is not reported) Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people with cataract aged 40 to 80 years Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | The mean fluorescein transmittance in vitreous by vitreous fluorophotometry, the cystoid macular oedema by fluorescence angiography, and the thickness of fovea by optical coherence tomography at three months and 12 months postoperatively | |
| Identification |
Sponsorship source: Funding sources: none Declaration of interest: none for all authors Country: not reported Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: T Ueda Institution: Ophthamology, Showa University, Tokyo, Japan Email: not reported Corresponding author's address: not reported |
|
| Notes | ARVO conference abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient information provided within abstract to judge other potential sources of bias |
Ueda 2006.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL
Inclusion criteria: 26 cataractous eyes of 26 patients scheduled for phacoemulsification and acrylic IOL implantation were enrolled in this study. The criteria used in this study were completely normal ophthalmic examination after pupil dilation, including visual acuity ≥ 20/30, intraocular pressure 21 mm Hg, no prior automated perimetry experience, and no family history of glaucoma Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Mean deviation and pattern standard deviation on frequency doubling perimetry (24‐2 threshold) at three months postoperatively | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: Japan Setting: Department of Ophthalmology, Nara Medical University Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Tetsuo Ueda, MD Institution: Department of Ophthalmology, Nara Medical University, Japan Email: tueda@naramed‐u.ac.jp Corresponding author's address: Tetsuo Ueda Department of Ophthalmology Nara Medical University, 840, Kashihara‐shi Nara, 634‐8522, Japan |
|
| Notes | None. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Quote: "IOL implanted intraoperatively was randomly selected from clear (VA60BB, HOYA) and yellow‐tinted lenses (YA60BB, HOYA), which only differed by color." Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Vuori 2006.
| Methods |
Study design: RCT Study grouping: parallel group, involving 37 people (52 eyes) Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: in the photographic analysis, two eyes of one participant in the Acrysof Natural IOL group were excluded because of a very lightly pigmented fundus Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: white patients scheduled for phacoemulsification and IOL implantation Exclusion criteria: hereditary colour vision defects; medications that might affect colour vision, such as ethambutol; any medication for epilepsy; amiodarone; digitalis; anti‐inflammatory drugs; diabetes; any other ocular pathology except cataract Comparison of study groups at baseline: no apparent group differences, although this was not explicitly stated and sex of participants was not given |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Colour vision (measured using Standard pseudoisochromatic plates, part 2, (SPP2) (Ichikawa et al. 1983) and the FarnsworthMunsell 100‐hue test (FM 100) (Farnsworth 1957)) and visibility of the retinal nerve fibre layer, from retinal fundus photography at one to six months postoperatively | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: Finland Setting: Department of Ophthalmology, Turku University Hopsital, Turku, Finland Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Marja‐Liisa Vuori, MD Institution: Department of Ophthalmology Turku University Hospital, Kiinamyllynkatu 4–8, 20520 Turku, Finland Email: marja‐liisa.vuori@tyks.fi Corresponding author's address: Marja‐Liisa Vuori Department of Ophthalmology Turku University Hospital Kiinamyllynkatu 4–820520 Turku, Finland |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Low risk | Quote: "Sealed envelopes containing the code for the planned IOL type were used for randomization. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement comment: described as “double blind” with no information on who was masked |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Judgement comment: described as “double blind” with no information on who was masked |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: results suggest no participants were lost to follow‐up; although this is not explicitly stated |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: sex distribution between study groups at baseline is not reported; the significance of this baseline imbalance is not clear |
Walter 2005.
| Methods |
Study design: RCT Study grouping: parallel group, involving 29 people (58 eyes), where both eyes received the same type of IOL but no further details are provided in relation to the statistical approach Exclusions after randomisation: not reported Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: non‐amblyopic bilateral cataract patients aged 60‐80 years with inconspicuous (normal) colour recognition test (Ishihara) Exclusion criteria: not reported Comparison of study groups at baseline: not reported |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Visual acuity, contrast sensitivity and colour vision at six weeks and four and a half months postoperatively | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: Germany Setting: not reported Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: S Walter Institution: Universitäts‐Augenklinik Magdeburg, Germany Email: Not reported Corresponding author's address: not reported |
|
| Notes | Conference abstract, in German | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: study described as open label |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment:study described as open label |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Unclear risk | Judgement comment: insufficient information within abstract to judge other potential sources of bias |
Wang 2010.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: randomised participants were excluded from the baseline data on the basis of intraoperative complications and no details about these potential exclusions were provided. Losses to follow‐up: participants who were "unable to attend for follow‐up visits" (i.e., those with incomplete follow‐up) were excluded from the analyses. No details were provided in relation to those participants potentially excluded on these grounds. How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL 1 ‐ yellow
Non‐blue‐light filtering IOL
Blue‐light filtering IOL 2 ‐ photochromic
Inclusion criteria: this study enrolled consecutive eyes that had cataract surgery with IOL implantation from November 2008‐June 2009. The inclusion criteria were senile cataract, no previous ophthalmic surgery, a potential visual acuity of 0.5 or better, and no colour vision deficiency. Exclusion criteria: people with congenital ocular abnormalities, glaucoma, proliferative diabetic retinopathy, retinal detachment, inflammatory signs, IOL power calculation < +10.00 diopters (D) or > +30.00 D, astigmatism greater than 2.00 D, intraoperative complications (e.g., posterior capsule rupture, bleeding), abnormal pupil reaction, or unable to attend the follow‐up visits. Comparison of study groups at baseline: there were no significant differences in the demographic data reported for the three IOL groups. Randomised participants were excluded from the baseline data on the basis of intraoperative complications and no details about these potential exclusions were provided. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1 ‐ yellow
Non‐blue‐light filtering IOL
Blue‐light filtering IOL 2 ‐ photochromic
|
|
| Outcomes | Postoperative visits were scheduled at one day, one week, and one and three months. Outcomes were the postoperative uncorrected distance visual acuity, contrast sensitivity (testing using an Optec 6500 device (Stereo Optical Co.) at spatial frequencies of 1.5, 3.0, 6.0, 12.0, and 18.0 cycles per degree (cpd) and under photopic (85 candelas (cd)/m2), mesopic (3 cd/m2), photopic with glare (135 lux), and mesopic with glare (28 lux) lighting conditions), contrast vision (under 400 lux, 30 lux and 5 lux at 100%, 25%, and 5% contrast), hue discrimination (using the Farnsworth‐Munsell (FM) 100‐hue test under outdoor daylight conditions and indoor mesopic conditions), and the Catquest‐9SF patient questionnaire (which includes subjective evaluation of glare, halo and colour‐vision perception), at three months postoperatively. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no author has a financial or proprietary interest in any material or method mentioned Country: China Setting: Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University; Beijing Ophthalmology Visual Sciences Key Laboratory, Beijing, China Comments: Date study conducted: November 2008‐June 2009 Trial registration number: not reported Contacting study investigators: authors contacted on 14 August 2017 regarding the contrast sensitivity outcome unit of error (Figure 1); no response was received to this email and, as a result, we could not include these data in the meta‐analysis First author's name: Jun Wang, MD Institution: Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Beijing Ophthalmology Visual Sciences Key Laboratory Email: prince909090@163.com Corresponding author's address: Jun Wang Beijing Tongren Eye Center, Beijing Tongren Hospital Capital Medical University, Beijing Ophthalmology Visual Sciences Key Laboratory, Number 2 Chongnei Street, Bejing, China 100730 |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Judgement comment: described as “double blind” with no information on whether participants and personnel were masked |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The physician who conducted the follow‐up examinations and collected the data was not aware which IOL had been implanted in the eye being evaluated." Judgement comment: clearly states that outcome assessors were masked |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported, and participants with intraoperative complications were excluded, without specifying which groups these individuals were assigned to |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Wirtitsch 2009.
| Methods |
Study design: RCT Study grouping: parallel group, involving 24 people (48 eyes), with paired‐eye comparison (i.e., one eye received a blue‐light filtering IOL and the fellow eye received a non‐blue‐light filtering IOL) Exclusions after randomisation: all included participants completed the scheduled vision tests and questionnaire Losses to follow‐up: none How missing data were handled: not applicable Reported power size calculation? yes |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL
Overall
Inclusion criteria: participants were recruited from a continuous cohort who presented with bilateral age‐related cataract in the outpatient centre of the Department of Ophthalmology, Hietzing Hospital, Vienna. Exclusion criteria: amblyopia; pseudoexfoliation syndrome; primary or secondary glaucoma; ocular hypertension; uveitis; diabetes; history of intraocular surgery; laser treatment; retinal pathology; other relevant ophthalmic diseases. People with medication known to potentially cause ophthalmologic side effects; with an expected postoperative visual acuity less than 1.0 (20/20); congenital colour vision anomaly; ocular surface disease; ametropia of more than 3 diopters; with nicotine or alcohol abuse Comparison of study groups at baseline: intra‐individual comparison (no group differences) |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Contrast acuity (measured at illumination levels of 500, 5, and 0.5 lux and contrast levels of 100%, 50%, 25%, 12.5%, and 6.25%), colour vision (assessed using the Lanthony desaturated D‐15 test, the Lanthony new colour test (Munsell chroma 2 and 4), and an anomaloscope), blue/yellow foveal threshold (using short‐wave automated perimetry) and the subjective visual impression of participants (evaluated using a questionnaire) at three months postoperatively The main outcome measures were contrast acuity, colour vision, and foveal threshold. |
|
| Identification |
Sponsorship source: Funding sources: "This study did not receive any financial support." Declaration of interest: "The authors have no proprietary interest in any of the materials or equipments mentioned in this study." Country: Austria Setting: Department of Ophthalmology, Hietzing Hospital, Vienna, Austria Comments: Date study conducted: surgery performed between December 2005 and February 2007 Trial registration number: clinicaltrials.gov NCT0061278 Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Matthias G. Wirtitsch Institution: Department of Ophthalmology, Hietzing Hospital Email: matthias.wirtitsch@wienkav.at Corresponding author's address: Department of Ophthalmology, Hietzing Hospital Wolkersbergenstrasse 1, 1130 Vienna, Austria |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Quote: "The first eye was randomly assigned to receive a multipiece acrylic foldable IOL: either a Hoya AF‐1 (UY) YA‐60BB (both blue and UV light filter) or a Hoya AF‐1 (UV) VA‐60BB (only UV light filter) (both IOLs from Hoya Medical Europe, Frankfurt/ Main, Germany). The contralateral eye received the other IOL." Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "Patients and examiner were masked for IOL assignment." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Study testing was performed in 1 single test session 90 plus/minus 10 days after surgery of the second eye by the same experienced and masked examiner." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "All included patients completed the scheduled vision tests and questionnaire." |
| Selective reporting (reporting bias) | Low risk | Judgement comment: all outcomes listed in trials registry (clinicaltrials.gov NCT 00612781) are reported |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Yamaguchi 2009.
| Methods |
Study design: RCT Study grouping: parallel group, involving 92 people (120 eyes), but with no further details regarding the allocation of interventions Exclusions after randomisation: not reported. Participants could have been potentially excluded on the basis of intra‐ and postoperative complications, however no details were provided about any potential exclusions on these grounds. Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1 (SN60WF)
Non‐blue‐light filtering IOL group (aspheric ZA)
Blue‐light filtering group 2 (SN60AT)
Blue‐light filtering IOL group 3 (Hoya Py60AD)
Inclusion criteria: consecutive eyes of patients who had cataract extraction and implantation of an acrylic IOL at Keio University Hospital between October 2007 and December 2008. People with significant senile cataract and a postoperative visual acuity better than 20/20 were eligible for inclusion in the study. Exclusion criteria: people with previous or coexisting ocular pathology and intraoperative or postoperative complications Comparison of study groups at baseline: the authors state "there were no significant differences between the groups in age, IOL power, or postoperative pupil diameters under photopic and mesopic conditions (P > 0.05, Mann‐Whitney U test)." However, participants could have been potentially excluded on the basis of intraoperative and postoperative complications. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Non‐blue‐light filtering IOL
Blue‐light filtering IOL 2
Blue‐light filtering IOL 3
|
|
| Outcomes | The main outcome was the postoperative higher‐order aberrations (HOAs) of the cornea and whole eye (measured under photopic and mesopic conditions), measured at one month postoperatively. Other outcomes were corrected distance visual acuity, and pupil diameter under photopic and mesopic conditions, measured at one month postoperatively. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: no author has a financial or proprietary interest in any material or method mentioned. Country: Japan Setting: Keio University Hospital, Tokyo, Japan Comments: Date study conducted: October 2007‐December 2008 Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Takefumi Yamaguchi, MD Institution: Keio University School of Medicine, Japan Email: yama19770614@hotmail.com Corresponding author's address: Takefumi Yamaguchi Keio University School of Medicine Shinanomachi 35, Shinjuku‐ku, Tokyo, Japan. |
|
| Notes | Data presented in this paper for the blue‐light filtering IOLs (SN60WF and SN60AT), and the non‐blue‐light filtering IOL(Tecnis ZA9003) appear the same as in the Yamaguchi 2011 paper. The data for the PY‐60 AD (Hoya) blue‐light filtering IOL appear different. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Exclusion criteria included previous or coexisting ocular pathology and intraoperative or postoperative complications." Judgement comment: whether incomplete outcome data is relevant is unclear as patients with intraoperative or postoperative complications were excluded |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Yamaguchi 2011.
| Methods |
Study design: RCT Study grouping: parallel group, involving 92 people (120 eyes), but with no further details regarding the allocation of interventions Exclusions after randomisation: not reported. Participants could have been potentially excluded on the basis of having complications during cataract surgery or postoperatively. The authors do state that "no eyes had any postoperative complication", but no details were provided in relation to potential intraoperative complications. Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group 1 (SN60WF)
Non‐blue‐light filtering IOL group
Blue‐light filtering IOL group 2 (SN60AT)
Blue‐light filtering IOL group 3 (PY60AD)
Inclusion criteria: people with significant senile cataract and postoperative visual acuity better than 20/20 were eligible for inclusion in the study. Exclusion criteria: people with previous or coexistent ocular pathology and complications during cataract surgery or postoperatively Comparison of study groups at baseline: the authors state that "there was no significant difference in the average IOL powers, age, and postoperative refraction, astigmatism, and pupil diameters under photopic and mesopic conditions between the three types of aspheric and one type of spherical IOLs (Kruskal–Wallis test, p > 0.05)" for those eligible to participate. However, those with intraoperative complications were excluded, and there is no details about these potential events/participants. Also, some participants received bilateral implants but there was no description of first eye versus second eye. |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL 1
Non‐blue‐light filtering IOL
Blue‐light filtering IOL 2
Blue‐light filtering IOL 3
|
|
| Outcomes | Contrast sensitivity, higher‐order aberrations of the whole eye, and pupil diameter under photopic and mesopic conditions were measured one month postoperatively. Higher‐order aberrations were decomposed into Zernike coefficients, calculated according to individual pupil diameter. The correlation between higher‐order aberrations and contrast sensitivity was evaluated. | |
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: the authors report no conflicts of interest in this work Country: Japan Setting: Keio University Hospital, Japan Comments: Date study conducted: October 2007‐December 2009 Trial registration number: not reported Contacting study investigators: study authors not contacted; no additional information used for review First author's name: Takefumi Yamaguchi Institution: Department of Ophthalmology, Keio University School of Medicine Email: yama19770614@hotmail.com Corresonding author's address: Takefumi Yamaguchi Department of Ophthalmology Keio University School of Medicine Shinanomachi 35, Shinjuku, Tokyo, Japan |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: trial is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: trial is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, patients and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Exclusion criteria were previous or coexistent ocular pathology and complications during cataract surgery or postoperatively." Judgement comment: completeness of outcome data is unclear as participants with complications during cataract surgery were potentially excluded from the analysis |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
Yuan 2004.
| Methods |
Study design: RCT Study grouping: parallel group, with one eye per participant randomised to one of the interventions Exclusions after randomisation: a total of 60 participants were originally randomised; the blue‐light filtering IOL group included 27 individuals (12 men, 15 women; as three patients were non‐compliant). No further details were provided. Losses to follow‐up: not reported How missing data were handled: not reported Reported power size calculation? no |
|
| Participants |
Baseline characteristics Blue‐light filtering IOL group
Non‐blue‐light filtering IOL group
Inclusion criteria: people with senile cataract Exclusion criteria: not reported Comparison of study groups at baseline: there was no significant difference in visual acuities (0.80–1.02) between the yellow UV and ordinary UV IOL groups (P > 0.05) (note: it was unclear if this was at baseline or postoperative) |
|
| Interventions |
Intervention characteristics Blue‐light filtering IOL
Non‐blue‐light filtering IOL
|
|
| Outcomes | Visual acuity, spatial contrast sensitivity (Stereo Optical, Chicago, Illinois, U.S.A.), colour vision (FM‐100, Munsell, New Windsor, New York, U.S.A.), and subjective sensation at one week to six months postoperatively Participants were questioned about photophobia and cyanopsia. |
|
| Identification |
Sponsorship source: Funding sources: not reported Declaration of interest: not reported Country: China Setting: Tianjin Medical University Eye Center Comments: Date study conducted: not reported Trial registration number: not reported Contacting study investigators: authors contacted on 14 August 2017 regarding the contrast sensitivity outcome unit of error; no response was received to this email, and as a result we could not include these data in the meta‐analysis First author's name: Zhaoxu Yuan, MD, PhD Institution: Medical Research Building, Scottand White Hospital Email: zyuan@tamu.edu Corresponding author's address: Zhaoxu Yuan Medical Research Building, Scottand White Hospital 702 SW HK Dodgen Loop, Temple, TX, USA 76504 |
|
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Judgement comment: not reported how list was generated. Study is described as “randomised” but with no further details |
| Allocation concealment (selection bias) | Unclear risk | Judgement comment: not reported how allocation administered. Study is described as “randomised” but with no further details |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, participants and personnel were not masked. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Judgement comment: no information provided on masking. We assume that in absence of reporting on this, outcome assessors were not masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Judgement comment: follow‐up not reported, although three participants in the blue‐light blocking IOL group were reported to be "non‐compliant" and appear to have been excluded from the analyses |
| Selective reporting (reporting bias) | Unclear risk | Judgement comment: no access to protocol or trials registry entry |
| Other bias | Low risk | Judgement comment: no other apparent sources of bias |
AAO: American Academy of Ophthalmology AMD: age‐related macular degeneration ARVO: Association for Research in Vision and Ophthalmology BCVA: best‐corrected visual acuity BMI: body mass index D: dioptre HRQoL: health‐related quality of life IOL: intraocular lens RCT: randomised controlled trial UCVA: uncorrected visual acuity
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Alexander 2014 | Not a RCT |
| Alfonso 2007 | Not a RCT |
| Chen 2013 | Does not appear to be a RCT |
| Chiosi 2006 | Does not appear to be a RCT |
| Cionni 2006 | Not a RCT |
| Clarke 1989 | Not a blue‐light filtering IOL |
| Cunha 2010 | Does not appear to be a RCT |
| Feng 2016 | Does not appear to be a RCT |
| Gavris 2006 | Does not appear to be a RCT |
| Gibson 2008 | Not a blue‐light filtering IOL |
| Hammond 2010 | Not a RCT |
| Hayashi 2009 | Not a RCT |
| Kraff 1985 | Not a blue‐light filtering IOL |
| Lak 2007 | Does not appear to be a RCT |
| Lavric 2014 | Does not appear to be a RCT |
| Mayer 2005 | Does not appear to be a RCT |
| Mayer 2006 | Does not appear to be a RCT |
| Mester 2008b | Does not appear to be a RCT |
| Mester 2008c | Does not appear to be a RCT |
| Muller 2005 | Does not appear to be a RCT |
| Munoz 2012 | Not a RCT |
| Nagai 2015 | Not a RCT |
| Nakamura 2006 | Does not appear to be a RCT |
| Nishi 2013 | Not a RCT |
| Rodriguez‐Galietero 2005a | Does not appear to be a RCT |
| Rodriguez‐Galietero 2005b | Does not appear to be a RCT |
| Shpak 2012 | Does not appear to be a RCT |
| Stopyra 2012 | Does not appear to be a RCT |
| Sun 2007 | Does not appear to be a RCT |
| Tognetto 2003 | Not a blue‐light filtering IOL |
| Wen 2012 | Does not appear to be a RCT |
| Wohlfart 2007 | Not a RCT |
IOL: intraocular lens RCT: randomised controlled trial
Characteristics of studies awaiting assessment [ordered by study ID]
Ji 2013.
| Methods | Awaiting translation |
| Participants | Awaiting translation |
| Interventions | Awaiting translation |
| Outcomes | Awaiting translation |
| Notes | Awaiting translation |
Li 2009.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Unable to source paper |
Shi 2008.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | Unable to source paper |
Characteristics of ongoing studies [ordered by study ID]
Nishi 2015.
| Trial name or title | The CLOCK‐IOL colour (Cataract surgery and circadian biological rhythm among Japanese older people with cataract in Nara, Kansai Region: Influence of Intraocular Lens Implantation) study |
| Methods | Parallel group, open‐label, RCT |
| Participants | Patients diagnosed as having cataracts in Nara Medical University Hospital (Japan), according to the following inclusion and exclusion criteria Inclusion criteria
Exclusion criteria
|
| Interventions | Phacoemulsification with a small incision and implantation of an IOL. Participants will be randomly allocated to the clear or blue‐blocking IOL group in a ratio of 1:1. In the clear IOL group, a clear spherical IOL (SA60AT, Alcon, Fort Worth, USA) will be implanted. In the blue‐blocking, IOL group, a spherical blue‐blocking IOL (SN60AT) or an aspherical blue‐blocking IOL (SN60WF, Alcon, Fort Worth, USA) will be implanted in a randomly allocated 1:1 ratio. |
| Outcomes |
Primary outcomes The primary outcomes are mortality and the incidence of CVD, cancer and AMD after surgery Secondary outcomes The secondary outcomes are:
|
| Starting date | As detailed in UMIN Clinical Trials Registry (UMIN ID: UMIN000014680), the recruitment status on 26 February 2018 was 'Open public recruitment', with the anticipated trial start date listed as 28 July 2014 |
| Contact information | Tomo Nishi Nara Medical University School of Medicine Department of Ophthalmology 840 Shijo‐cho, Kashiharashi, Nara, Japan, 634‐8521 Email: tomon@naramed‐u.ac.jp |
| Notes | None |
AMD: age‐related macular degeneration BMI: body mass index IOL: intraocular lens RCT: randomised controlled trial
Differences between protocol and review
After discussion with the editorial base it was decided to redefine the scope of the search strategy to fulfil the stated objectives of the review. Therefore the search strategy has been re‐designed to reflect this amendment. Medline now contains Epub Ahead of Print records so PubMed is not being searched.
Contrast sensitivity has been expressed as log Contrast Sensitivity, as reported by the study authors, rather than log Contrast Threshold (%).
Contributions of authors
Review: LED drafted the initial review, with substantial input, discussion and editing from LB and PRK. All of the statistical analyses were confirmed by LB. All authors provided final approval of the review.
Protocol: LED drafted the initial protocol, with substantial input, discussion and editing from LB and PRK. All authors provided final approval of the protocol.
LED is the guarantor of the review.
Sources of support
Internal sources
The University of Melbourne, Australia.
Australian Catholic University, Australia.
External sources
-
National Health and Medical Research Council (NHMRC), Australia.
This review is undertaken as part of a 2015 NHMRC Translating Research Into Practice (TRIP) Fellowship (APP1091833, CIA: Dr Laura Downie).
-
National Institute for Health Research (NIHR), UK.
- Richard Wormald, Co‐ordinating Editor for Cochrane Eyes and Vision (CEV) acknowledges financial support for his CEV research sessions from the Department of Health through the award made by the NIHR to Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology for a Specialist Biomedical Research Centre for Ophthalmology.
- This review was supported by the NIHR, via Cochrane Infrastructure funding to the CEV UK editorial base.
The views expressed in this publication are those of the authors and not necessarily those of the NIHR, NHS, or the Department of Health.
Declarations of interest
Laura Downie: none known Ljoudmila Busija: none known Peter Keller: none known
New
References
References to studies included in this review
Aose 2006 {published data only}
- Aose M, Matsushima H, Nagata M, Matui E, Obara Y, Yoshida S, et al. Characteristics of different types of hydrophobic acrylic intraocular lenses and clinical evaluation during early postoperative period. Investigative Ophthalmology and Visual Science 2006; Vol. 47:ARVO E‐abstract 610.
Bandyopadhyay 2016 {published data only}
- Bandyopadhyay S, Saha M, Chakrabarti A, Sinha A. Effect on contrast sensitivity after clear, yellow and orange intraocular lens implantation. International Ophthalmology 2016;36(3):313‐8. [DOI] [PubMed] [Google Scholar]
Barisic 2007 {published data only}
- Barisić A, Dekaris I, Gabrić N, Bosnar D, Lazić R, Martinović ZK, et al. Blue light filtering intraocular lenses in phacoemulsification cataract surgery. Collegium Antropologicum 2007;31(Suppl 1):57‐60. [PubMed] [Google Scholar]
Behrens‐Baumann 2005 {published data only}
- Behrens‐Baumann W, Walter S, Muller S, Kuchenbecker J, Lindner H. Comparison of two lOLs: Hoya AF‐ I (UV) VA6013B vs. AF‐1 (UY) YA‐60BB. American Academy of Ophthalmology. 2005:185.
Bhattacharjee 2006 {published data only}
- Bhattacharjee H, Bhattacharjee K, Medhi J. Visual performance: comparison of foldable intraocular lenses. Journal of Cataract and Refractive Surgery 2006;32(3):451‐5. [DOI] [PubMed] [Google Scholar]
Brøndsted 2014 {published data only}
- Brøndsted AE, Sander B, Haargaard B, Lund‐Andersen H, Jennum P, Gammeltoft S, et al. The effect of neutral and blue‐blocking intraocular lenses on circadian photoentrainment. Investigative Ophthalmology and Visual Science 2014; Vol. 55, issue 13:4184.
Brøndsted 2015 {published data only}
- Brøndsted AE, Sander B, Haargaard B, Lund‐Andersen H, Jennum P, Gammeltoft S, et al. The effect of cataract surgery on circadian photoentrainment: a randomized trial of blue‐blocking versus neutral intraocular lenses. Ophthalmology 2015;122(10):2115‐24. [DOI] [PubMed] [Google Scholar]
Brøndsted 2017 {published data only}
- Brøndsted AE, Haargaard B, Sander B, Lund‐Andersen H, Jennum P, Kessel L. The effect of blue‐blocking and neutral intraocular lenses on circadian photoentrainment and sleep one year after cataract surgery. Acta Opthalmologica 2017;95(4):344‐51. [DOI] [PubMed] [Google Scholar]
Caporossi 2007 {published data only}
- Caporossi A, Martone G, Casprini F, Rapisarda L. Prospective randomized study of clinical performance of 3 aspheric and 2 spherical intraocular lenses in 250 eyes. Journal of Refractive Surgery 2007;23(7):639‐48. [DOI] [PubMed] [Google Scholar]
Caporossi 2009 {published data only}
- Caporossi A, Casprini F, Martone G, Balestrazzi A, Tosi GM, Ciompi L. Contrast sensitivity evaluation of aspheric and spherical intraocular lenses 2 years after implantation. Journal of Refractive Surgery 2009;25(7):578‐90. [DOI] [PubMed] [Google Scholar]
Cionni 2003 {published data only}
- Cionni RJ. Clinical study results of the AcrySof Natural intraocular lens. American Academy of Ophthalmology. 2003:130.
Cristobal 2005 {published data only}
- Cristobal JA, Sierra J, Martin J, Rodriguez NA, Ascaso J. Intraocular lenses with blue light filter. Archivos de la Sociedad Espanola de Oftalmologia 2005;80(4):245‐9. [DOI] [PubMed] [Google Scholar]
Cui 2009 {published data only}
- Cui H, Hu R, Zhang Y, Lou D. Comparison of pseudophakic visual quality in spherical and aspherical intraocular lenses. Canadian Journal of Ophthalmology 2009;44(3):274‐8. [DOI] [PubMed] [Google Scholar]
Cuthbertson 2009 {published data only}
- Cuthbertson FM, Dhingra S, Benjamin L. Objective and subjective outcomes in comparing three different aspheric intraocular lens implants with their spherical counterparts. Eye 2009;23(4):877‐83. [DOI] [PubMed] [Google Scholar]
Espindle 2005 {published data only}
- Espindle D, Crawford B, Maxwell A, Rajagopalan K, Barnes R, Harris B, et al. Quality‐of‐life improvements in cataract patients with bilateral blue light‐filtering intraocular lenses: clinical trial. Journal of Cataract and Refractive Surgery 2005;31(10):1952‐9. [DOI] [PubMed] [Google Scholar]
Espíndola 2012a {published data only}
- Espíndola RF, Santhiago MR, Kara‐Júnior N. Effect of aspherical and yellow tinted intraocular lens on blue‐on‐yellow perimetry. Arquivos Brasileiros de Oftalmologia 2012;75(5):316‐9. [DOI] [PubMed] [Google Scholar]
Falkner Radler 2008 {published data only}
- Falkner CI, Binder S. UV‐filter IOL versus yellow blue light‐filter IOL in combined cataract surgery with vitrectomy: a prospective randomized clinical trial. Investigative Ophthalmology and Visual Science ARVO E‐abstract 1484.
- Falkner‐Radler CI, Benesch T, Binder S. Blue light‐filter intraocular lenses in vitrectomy combined with cataract surgery: results of a randomized controlled clinical trial. American Journal of Ophthalmology 2008;145(3):499‐503. [DOI] [PubMed] [Google Scholar]
Hahsler 2004 {published data only}
- Hahsler B, Lackinger B, Klemen U. Contrast sensitivity in IOL with blue light filter: a comparison of SN60 and SA60. Klinische Monatsblatter fur Augenheilkunde 2004;221(Suppl 1):S15‐6. [Google Scholar]
Hahsler 2005 {published data only}
- Hahsler B, Lackinger B, Klemen U. Contrast sensitivity in IOL with blue filter: SN 60/SA 60, HOYA‐YA/HOYA‐VA on the F.A.C.T. test facility. Klinische Monatsblatter fur Augenheilkunde 2005;222(Suppl 1):S8. [Google Scholar]
Hayashi 2006 {published data only}
- Hayashi K, Hayashi H. Visual function in patients with yellow tinted intraocular lenses compared with vision in patients with non‐tinted intraocular lenses. British Journal of Ophthalmology 2006;90(8):1019‐23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hyunseok 2007 {published data only}
- Hyunseok A, Kim SW, Kim EK, Lee AY, Kim T. Comparison of an aspherical IOL with a spherical IOU wavefront analysis and visual quality. American Academy of Ophthalmology. 2007:210.
Kara Júnior 2006 {published data only}
- Kara‐Júnior N, Jardim JL, Oliveira Leme E, Dall'Col M, Susanna R Jr. Effect of the AcrySof Natural intraocular lens on blue‐yellow perimetry. Journal of Cataract and Refractive Surgery 2006;32(8):1328‐30. [DOI] [PubMed] [Google Scholar]
Kara Junior 2011 {published data only}
- Kara‐Junior N, Espindola RF, Gomes BA, Ventura B, Smadja D, Santhiago MR. Effects of blue light‐filtering intraocular lenses on the macula, contrast sensitivity, and color vision after a long‐term follow‐up. Journal of Cataract and Refractive Surgery 2011;37(12):2115‐9. [DOI] [PubMed] [Google Scholar]
Kennis 2004 {published data only}
- Kennis H, Huygens M, Callebaut F. Comparing the contrast sensitivity of a modified prolate anterior surface IOL and of two spherical IOLs. Bulletin de la Societe Belge d'Ophtalmologie 2004;2004(294):49‐58. [PubMed] [Google Scholar]
Kim 2011a {published data only}
- Kim JY, Choi JA, Na KS, Joo CK. The effect of yellow tinted intraocular lenses on the result of frequency doubling perimetry after cataract surgery. Korean Journal of Ophthalmology 2011;25(1):29‐32. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2011b {published data only}
- Kim JH, Kim NR, Lee ES, Rho S, Kang SY, Kim CY. Influence of blue light‐filtering intraocular lenses on retinal nerve fiber layer measurements by spectral‐domain optical coherence tomography. Current Eye Research 2011;36(10):937‐42. [DOI] [PubMed] [Google Scholar]
Kuchenbecker 2004 {published data only}
- Kuchenbecker J, Muller S, Walter S, Lindner H, Behrens‐Baumann W. The comparison of two intraocular lenses: Hoya AF‐1 (UV) VA‐60BB and AF‐1 (UY) YA‐60BB ‐ preliminary results. Klinische Monatsblatter fur Augenheilkunde 2004;221(Suppl 5):S11‐2. [Google Scholar]
Leibovitch 2006 {published data only}
- Leibovitch I, Lai T, Porter N, Pietris G, Newland H, Selva D. Visual outcomes with the yellow intraocular lens. Acta Ophthalmologica Scandinavica 2006;84(1):95‐9. [DOI] [PubMed] [Google Scholar]
Marshall 2005 {published data only}
- Marshall J, Cionni RJ, Davison J, Ernest P, Lehmann R, Maxwell WA, et al. Clinical results of the blue‐light filtering AcrySof Natural foldable acrylic intraocular lens. Journal of Cataract and Refractive Surgery 2005;31(12):2319‐23. [DOI] [PubMed] [Google Scholar]
Mester 2008a {published data only}
- Mester U, Holz F, Kohnen T, Lohmann C, Tetz M. Intraindividual comparison of a blue‐light filter on visual function: AF‐1 (UY) versus AF‐1 (UV) intraocular lens. Journal of Cataract and Refractive Surgery 2008;34(4):608‐15. [DOI] [PubMed] [Google Scholar]
Monnet 2009 {published data only}
- Monnet D, Tépenier L, Brézin AP. Objective assessment of inflammation after cataract surgery: comparison of 3 similar intraocular lens models. Journal of Cataract and Refractive Surgery 2009;35(4):677‐81. [DOI] [PubMed] [Google Scholar]
Neumaier‐Ammerer 2010 {published data only}
- Neumaier‐Ammerer B, Felke S, Hagen S, Haas P, Zeiler F, Mauler H, et al. Comparison of visual performance with blue light‐filtering and ultraviolet light‐filtering intraocular lenses. Journal of Cataract and Refractive Surgery 2010;36(12):2073‐9. [DOI] [PubMed] [Google Scholar]
Nolan 2009 {published data only}
- Nolan JM, O'Reilly P, Loughman J, Stack J, Loane E, Connolly E, et al. Augmentation of macular pigment following implantation of blue light‐filtering intraocular lenses at the time of cataract surgery. Investigative Ophthalmology and Visual Science 2009;50(10):4777‐85. [DOI] [PubMed] [Google Scholar]
Pandita 2007 {published data only}
- Pandita D, Raj SM, Vasavada VA, Vasavada VA, Kazi NS, Vasavada AR. Contrast sensitivity and glare disability after implantation of AcrySof IQ Natural aspherical intraocular lens: prospective randomized masked clinical trial. Journal of Cataract and Refractive Surgery 2007;33(4):603‐10. [DOI] [PubMed] [Google Scholar]
Raj 2005 {published data only}
- Raj SM, Vasavada AR, Nanavaty MA. AcrySof Natural SN60AT versus AcrySof SA60AT intraocular lens in patients with color vision defects. Journal of Cataract and Refractive Surgery 2005;31(12):2324‐8. [DOI] [PubMed] [Google Scholar]
Rocha 2006a {published data only}
Rocha 2006b {published data only}
Rocha 2007 {published data only}
- Rocha KM, Soriano ES, Chamon W, Chalita MR, Nosé W. Spherical aberration and depth of focus in eyes implanted with aspheric and spherical intraocular lenses: a prospective randomized study. Ophthalmology 2007;114(11):2050‐4. [DOI] [PubMed] [Google Scholar]
Schmack 2012 {published data only}
- Schmack I, Schimpf M, Stolzenberg A, Conrad‐Hengerer I, Hengerer FH, Dick HB. Visual quality assessment in patients with orange‐tinted blue light‐filtering and clear ultraviolet light‐filtering intraocular lenses. Journal of Cataract and Refractive Surgery 2012;38(5):823‐32. [DOI] [PubMed] [Google Scholar]
Schmidinger 2008 {published data only}
- Schmidinger G, Menapace R, Pieh S. Intraindividual comparison of color contrast sensitivity in patients with clear and blue‐light‐filtering intraocular lenses. Journal of Cataract and Refractive Surgery 2008;34(5):769‐73. [DOI] [PubMed] [Google Scholar]
Schmoll 2014 {published data only}
- Schmoll C, Khan A, Aspinall P, Goudie C, Koay P, Tendo C, et al. New light for old eyes: comparing melanopsin‐mediated non‐visual benefits of blue‐light and UV‐blocking intraocular lenses. British Journal of Ophthalmology 2014;98(1):124‐8. [DOI] [PubMed] [Google Scholar]
Soriano 2006 {published data only}
- Soriano ES, Rocha KM, Nose W, Monmoto M, Chalita MR, Chamon W. Correlation between near vision and pupil size in aspheric and spherical IOLs. American Academy of Ophthalmology. 2006:209.
Ueda 2005 {published data only}
- Ueda T, Taguchi Y, Tsukahara M, Yamamoto Y, Koide R. Retinal light damage control by blue light‐absorbing intraocular lens. Investigative Ophthalmology and Visual Science 2005; Vol. 46:ARVO E‐abstract 808.
Ueda 2006 {published data only}
- Ueda T, Ota T, Yukawa E, Hara Y. Frequency doubling technology perimetry after clear and yellow intraocular lens implantation. American Journal of Ophthalmology 2006;142(5):856‐8. [DOI] [PubMed] [Google Scholar]
Vuori 2006 {published data only}
- Vuori ML, Mantyjarvi M. Colour vision and retinal nerve fibre layer photography in patients with an Acrysof Natural intraocular lens. Acta Ophthalmologica Scandinavica 2006;84(1):92‐4. [DOI] [PubMed] [Google Scholar]
Walter 2005 {published data only}
- Walter S, Kuchenbecker J, Muller S, Behrens‐Baumann W. A comparison of two intraocular lenses: Hoya AF‐1 (UV) VA‐60BB and AF‐1 (UY) YA‐60BB ‐ preliminary results. Klinische Monatsblatter fur Augenheilkunde 2005;222(Suppl 6):S7‐8. [Google Scholar]
Wang 2010 {published data only}
- Wang H, Wang J, Fan W, Wang W. Comparison of photochromic, yellow, and clear intraocular lenses in human eyes under photopic and mesopic lighting conditions. Journal of Cataract and Refractive Surgery 2010;36(12):2080‐6. [DOI] [PubMed] [Google Scholar]
Wirtitsch 2009 {published data only}
- Wirtitsch MG, Schmidinger G, Prskavec M, Rubey M, Skorpik F, Heinze G, et al. Influence of blue‐light‐filtering intraocular lenses on color perception and contrast acuity. Ophthalmology 2009;116(1):39‐45. [DOI] [PubMed] [Google Scholar]
Yamaguchi 2009 {published data only}
- Yamaguchi T, Negishi K, Ono T, Torii H, Dogru M, Yamaguchi K, et al. Feasibility of spherical aberration correction with aspheric intraocular lenses in cataract surgery based on individual pupil diameter. Journal of Cataract and Refractive Surgery 2009;35(10):1725‐33. [DOI] [PubMed] [Google Scholar]
Yamaguchi 2011 {published data only}
- Yamaguchi T, Negishi K, Ohnuma K, Tsubota K. Correlation between contrast sensitivity and higher‐order aberration based on pupil diameter after cataract surgery. Clinical Ophthalmology 2011;5(1):1701‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Yuan 2004 {published data only}
- Yuan Z, Reinach P, Yuan, J. Contrast sensitivity and color vision with a yellow intraocular lens. American Journal of Ophthalmology 2004;138(1):138‐40. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Alexander 2014 {published data only}
- Alexander I, Cuthbertson FM, Ratnarajan G, Safa R, Mellington FE, Foster RG, et al. Impact of cataract surgery on sleep in patients receiving either ultraviolet‐blocking or blue‐filtering intraocular lens implants. Investigative Ophthalmology and Visual Science 2014; Vol. 55, issue 8:4999‐5004. [DOI] [PMC free article] [PubMed]
Alfonso 2007 {published data only}
- Alfonso JF, Fernández‐Vega L, Baamonde MB, Montés‐Micó R. Prospective visual evaluation of apodized diffractive intraocular lenses. Journal of Cataract and Refractive Surgery 2007;33(7):1235‐43. [DOI] [PubMed] [Google Scholar]
Chen 2013 {published data only}
- Chen C, Du WJ, Shen LT, Wei QH. Comparison of the contrast vision after implanting photochromic, yellow or clear intraocular lenses. International Eye Science 2013;13(5):931‐3. [Google Scholar]
Chiosi 2006 {published data only}
- Chiosi F, Greenstein VC, Braunstein RE, Holopigian K, Seiple W, Sparrow JR. Does a "yellow" tinted IOL adversely affect scotopic and photopic visual performance?. Investigative Ophthalmology and Visual Science 2006; Vol. 47:ARVO E‐abstract 304.
Cionni 2006 {published data only}
- Cionni RJ, Tsai JH. Color perception with AcrySof natural and AcrySof single‐piece intraocular lenses under photopic and mesopic conditions. Journal of Cataract and Refractive Surgery 2006;32(2):236‐42. [DOI] [PubMed] [Google Scholar]
Clarke 1989 {published data only}
- Clarke MP, Yap M, Weatherill JR. Do intraocular lenses with ultraviolet absorbing chromophores protect against macular oedema?. Acta Ophthalmologica 1989;67(5):593‐6. [DOI] [PubMed] [Google Scholar]
Cunha 2010 {published data only}
- Cunha JP, Paiva T, Castanheira‐Dinis A. The eye, the intraocular lens and the circadian rhythm. Journal of Sleep Research 2010;19:189. [Google Scholar]
Feng 2016 {published data only}
- Feng X, Xu K, Hao Y, Qi, H. Impact of blue‐light filtering intraocular lens implantation on the quality of sleep in patients after cataract surgery. Medicine 2016;95(51):e5648. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gavris 2006 {published data only}
- Gavris M, Horge I, Marian N, Popa D, Olaru G, Stepan E. Our experience with Acrysof Natural intraocular lens. Oftalmologia 2006;50(3):94‐8. [PubMed] [Google Scholar]
Gibson 2008 {published data only}
- Gibson GA, Davies LN, Wolffsohn JS. Cognitive and visual function in phakic and pseudophakic eyes: an intraocular lens filter study. Investigative Ophthalmology and Visual Science 2008:ARVO E‐ abstract 3342.
Hammond 2010 {published data only}
- Hammond BR Jr, Renzi LM, Sachak S, Brint SF. Contralateral comparison of blue‐filtering and non‐blue‐filtering intraocular lenses: glare disability, heterochromatic contrast, and photostress recovery. Clinical Ophthalmology 2010;4:1465‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hayashi 2009 {published data only}
- Hayashi K, Masumoto M, Hayashi H. All‐distance visual acuity in eyes with a nontinted or a yellow‐tinted diffractive multifocal intraocular lens. Japanese Journal of Ophthalmology 2009;53(2):100‐6. [DOI] [PubMed] [Google Scholar]
Kraff 1985 {published data only}
- Kraff MC, Sanders DR, Jampol LM, Lieberman HL. Effect of an ultraviolet‐filtering intraocular lens on cystoid macular edema. Ophthalmology 1985;92(3):366‐9. [DOI] [PubMed] [Google Scholar]
Lak 2007 {published data only}
- Lak D, Lubinski W, Sylwestrzak Z, Szych Z, Karczewicz D. Comparative assessment of the course of age‐related macular degeneration in patients after phacoemulsification cataract surgery with implantation of AcrySof Natural SN 60 at and AcrySof SA 60 at lenses. Annales Academiae Medicae Stetinensis 2007;53(Suppl 1):43‐7. [PubMed] [Google Scholar]
Lavric 2014 {published data only}
- Lavric A, Pompe MT. Do blue‐light filtering intraocular lenses affect visual function?. Optometry and Vision Science 2014;91(11):1348‐54. [DOI] [PubMed] [Google Scholar]
Mayer 2005 {published data only}
- Mayer S, Wirbelauer C, Haberle H, Pham DT. Contrast vision after IOL implantation with or without blue light filter. Klinische Monatsblatter fur Augenheilkunde 2005;222(Suppl 1):S8. [Google Scholar]
Mayer 2006 {published data only}
- Mayer S, Wirbelauer C, Pham DT. Functional results after intraocular lens implantation with or without blue light filter: an intraindividual comparison. Klinische Monatsblätter für Augenheilkunde 2006;223(2):142‐6. [DOI] [PubMed] [Google Scholar]
Mester 2008b {published data only}
- Mester U, Kaymak H. The aspheric blue light filter IOL AcrySof IQ compared to the AcrySof SA60AT: influence of IOL power, pupil diameter, and corneal asphericity on postoperative spherical aberration. Der Ophthalmologe 2008;105(11):1029‐35. [DOI] [PubMed] [Google Scholar]
Mester 2008c {published data only}
- Mester U, Kaymak H. Comparison of the AcrySof IQ aspheric blue light filter and the AcrySof SA60AT intraocular lenses. Journal of Refractive Surgery 2008;24(8):817‐25. [DOI] [PubMed] [Google Scholar]
Muller 2005 {published data only}
- Muller V, Langenbeck J, Muller M, Tetz MR. Intra‐ and interindividual comparison of spherical, aspherical, clear and yellow intraocular lenses (IOL). Klinische Monatsblatter fur Augenheilkunde 2005;222(Suppl 7):S18. [Google Scholar]
Munoz 2012 {published data only}
- Muñoz G, Belda‐Salmerón L, Albarrán‐Diego C, Ferrer‐Blasco T, Fernández‐Porrero A. Contrast sensitivity and color perception with orange and yellow intraocular lenses. European Journal of Ophthalmology 2012;22(5):769‐75. [DOI] [PubMed] [Google Scholar]
Nagai 2015 {published data only}
- Nagai H, Hirano Y, Yasukawa T, Morita H, Nozaki M, Wolf‐Schnurrbusch U, et al. Prevention of increased abnormal fundus autofluorescence with blue light‐filtering intraocular lenses. Journal of Cataract and Refractive Surgery 2015;41(9):1855‐9. [DOI] [PubMed] [Google Scholar]
Nakamura 2006 {published data only}
- Nakamura T, Kiuchi Y, Fukui K, Harada J, Fujimoto M. Improving contrast sensitivity with the Acryl‐Foldable yellow intraocular lens. Investigative Ophthalmology and Visual Science 2006; Vol. 47:ARVO E‐abstract 302.
Nishi 2013 {published data only}
- Nishi T, Taketani F, Ueda T, Ogata N. Comparisons of amplitude of pseudoaccommodation with aspheric yellow, spheric yellow, and spheric clear monofocal intraocular lenses. Clinical Ophthalmology 2013;7:2159‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rodriguez‐Galietero 2005a {published data only}
- Rodríguez‐Galietero A, Montés‐Micó R, Muñoz G, Albarrán‐Diego C. Blue‐light filtering intraocular lens in patients with diabetes: contrast sensitivity and chromatic discrimination. Journal of Cataract and Refractive Surgery 2005;31(11):2088‐92. [DOI] [PubMed] [Google Scholar]
Rodriguez‐Galietero 2005b {published data only}
- Rodríguez‐Galietero A, Montés‐Micó R, Muñoz G, Albarrán‐Diego C. Comparison of contrast sensitivity and color discrimination after clear and yellow intraocular lens implantation. Journal of Cataract and Refractive Surgery 2005;31(9):1736‐40. [DOI] [PubMed] [Google Scholar]
Shpak 2012 {published data only}
- Shpak AA, Maliugin BE, Fadeeva TV. The effect of yellow filter intraocular lens on the macula after cataract phacoemulsification in patients with age macular degeneration. Vestnik Oftalmologii 2012;128(4):48‐51. [PubMed] [Google Scholar]
Stopyra 2012 {published data only}
- Stopyra W. Evaluation of colour vision according to type of implanted artificial foldable intraocular lens. Klinika Oczna 2012;114(4):266‐9. [PubMed] [Google Scholar]
Sun 2007 {published data only}
- Sun K, Huang Y, Luo S, Lu Q, Zhang W, Xie J, et al. The clinical investigation of early visual function in cataract patients after implantation with aspheric intraocular lens. Eye Science 2007;23(1):43‐7. [PubMed] [Google Scholar]
Tognetto 2003 {published data only}
- Tognetto D, Toto L, Sanguinetti G, Cecchini P, Vattovani O, Filacorda S, et al. Lens epithelial cell reaction after implantation of different intraocular lens materials: two‐year results of a randomized prospective trial. Ophthalmology 2003;110(10):1935‐41. [DOI] [PubMed] [Google Scholar]
Wen 2012 {published data only}
- Wen HM, Han LC, Cong RC, Li HX. Compare the pseudophakic accommodation of three type monofocal intraocular lens implantation eyes. International Eye Science 2012;12(7):1311‐3. [Google Scholar]
Wohlfart 2007 {published data only}
- Wohlfart C, Tschuschnig K, Fellner P, Weiss K, Vidic B, El‐Shabrawi Y, et al. Visual function with blue light filter IOLs. Klinische Monatsblätter für Augenheilkunde 2007;224(1):23‐7. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Ji 2013 {published data only}
- Ji HL, Xiao W, Pu W. Mesopic visual quality after three kinds of aspheric acrylic monofocal intraocular lenses. International Eye Science 2013;13(8):1609‐12. [Google Scholar]
Li 2009 {published data only}
- Li HW, Guo HK, Zhang HY, Jin HY, Chen YL, Liu MY. Comparative analysis of visual quality after aspheric intraocular lens implantation. International Journal of Ophthalmology 2009;9(11):2092‐6. [Google Scholar]
Shi 2008 {published data only}
- Shi D, Zhang JS. Impact of different intraocular lens design on the wave‐front aberration of pseudophakic eyes. International Journal of Ophthalmology 2008;8(1):71‐3. [Google Scholar]
References to ongoing studies
Nishi 2015 {published data only}
- Nishi T, Saeki K, Obayashi K, Miyata K, Tone N, Tsujinaka H, et al. The effect of blue‐blocking intraocular lenses on circadian biological rhythm: protocol for a randomised controlled trial (CLOCK‐IOL colour study). BMJ Open 2015;5(5):e007930. [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Baatz 2008
- Baatz H, Darawsha R, Ackermann H, Scharioth GB, Ortueta D, Pavlidis M, et al. Phacoemulsification does not induce neovascular age‐related macular degeneration. Investigative Ophthalmology and Visual Science 2008;49(3):1079‐83. [DOI] [PubMed] [Google Scholar]
Beatty 1999
- Beatty S, Boulton M, Henson D, Koh HH, Murray IJ. Macular pigment and age related macular degeneration. British Journal of Ophthalmology 1999;83(7):867‐77. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bernstein 2010
- Bernstein PS, Delori FC, Richer S, Kujik FJ, Wenzel AJ. The value of measurement of macular carotenoid pigment optical densities and distributions in age‐related macular degeneration and other retinal disorders. Vision Research 2010;50(7):716‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
Boettner 1962
- Boettner EA, Walter JR. Transmission of the ocular media. Investigative Ophthalmology and Visual Science 1962;1:766‐83. [Google Scholar]
Boulton 2001
- Boulton M, Rozanowska M, Rozanowski B. Retinal photodamage. Journal of Photochemistry and Photobiology. B, Biology 2001;64(2‐3):144‐61. [DOI] [PubMed] [Google Scholar]
Bressler 1994
- Bressler NM, Silva JC, Bressler SB, Fine SL, Green WR. Clinicopathologic correlation of drusen and retinal pigment epithelial abnormalities in age‐related macular degeneration. Retina 1994;14(2):130‐42. [PubMed] [Google Scholar]
Brockmann 2008
- Brockmann C, Schulz M, Laube T. Transmittance characteristics of ultraviolet and blue‐light‐filtering intraocular lenses. Journal of Cataract and Refractive Surgery 2008;34(7):1161‐6. [DOI] [PubMed] [Google Scholar]
Casparis 2012
- Casparis H, Lindsley K, Kuo IC, Sikder S, Bressler NM. Surgery for cataracts in people with age‐related macular degeneration. Cochrane Database of Systematic Reviews 2012, Issue 6. [DOI: 10.1002/14651858.CD006757.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chalam 2011
- Chalam KV, Khetpal V, Rusovici R, Balaiya S. A review: role of ultraviolet radiation in age‐related macular degeneration. Eye Contact Lens 2011;37(4):225‐32. [DOI] [PubMed] [Google Scholar]
Chew 2009
- Chew EY, Sperduto RD, Milton RC, Clemons TE, Gensler GR, Bressler SB, et al. Risk of advanced age‐related macular degeneration after cataract surgery in the Age‐Related Eye Disease Study: AREDS report 25. Ophthalmology 2009;116(2):297‐303. [DOI] [PMC free article] [PubMed] [Google Scholar]
Coleman 2008
- Coleman H, Chan C, Ferris FL. Age‐related macular degeneration. Lancet 2008;372(9652):1835‐45. [DOI] [PMC free article] [PubMed] [Google Scholar]
Congdon 2004
- Congdon N, O'Colmain B, Klaver CC, Klein R, Munoz B, Friedman DS, et al. Causes and prevalence of visual impairment among adults in the United States. Archives of Ophthalmology 2004;122(4):477‐85. [DOI] [PubMed] [Google Scholar]
Covidence [Computer program]
- Veritas Health Innovation. Covidence. Melbourne, Australia: Veritas Health Innovation, accessed 19 September 2017.
Deeks 2011
- Deeks JJ, Higgins JP, Altman DG editor(s). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Downes 2016
- Downes SM. Ultraviolet or blue‐filtering intraocular lenses: what is the evidence?. Eye 2016;30(2):215‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Downie 2014a
- Downie LE, Keller PR. Nutrition and age‐related macular degeneration: research evidence in practice. Optometry and Vision Science 2014;91(8):821‐31. [DOI] [PubMed] [Google Scholar]
Downie 2014b
- Downie LE, Cheng AS, Vingrys AJ. Color vision deficits in intermediate age‐related macular degeneration. Optometry and Vision Science 2014;91(8):932‐8. [DOI] [PubMed] [Google Scholar]
Downie 2017
- Downie LE. Blue‐light filtering ophthalmic lenses: to prescribe, or not to prescribe?. Ophthalmic and Physiological Optics 2017;37(6):640‐3. [DOI] [PubMed] [Google Scholar]
Ferris 2005
- Ferris FL, Davis MD, Clemons TE, Lee LY, Chew EY, Lindblad AS, et al. A simplified severity scale for age‐related macular degeneration: AREDS Report No. 18. Archives of Ophthalmology 2005;123(11):1570‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gin 2011
- Gin TJ, Luu CD, Guymer RH. Central retinal function as measured by the multifocal electroretinogram and flicker perimetry in early age‐related macular degeneration. Investigative Ophthalmology and Visual Science 2011;52(12):9267‐74. [DOI] [PubMed] [Google Scholar]
Glanville 2006
- Glanville JM, Lefebvre C, Miles JN, Camosso‐Stefinovic J. How to identify randomized controlled trials in MEDLINE: ten years on. Journal of the Medical Library Association 2006;94(2):130‐6. [PMC free article] [PubMed] [Google Scholar]
Ham 1976
- Ham WT Jr, Mueller HA, Sliney DH. Retinal sensitivity to damage from short wavelength light. Nature 1976;260:153‐5. [DOI] [PubMed] [Google Scholar]
Ham 1978
- Ham WT Jr, Ruffolo JJ Jr, Mueller HA, Clarke AM, Moon ME. Histologic analysis of photochemical lesions produced in rhesus retina by short‐wave‐length light. Investigative Ophthalmology and Visual Science 1978;17(10):1029‐35. [PubMed] [Google Scholar]
Ham 1984
- Ham WT Jr, Mueller HA, Ruffolo JJ Jr, Millen JE, Cleary SF, Guerry RK, et al. Basic mechanisms underlying the production of photochemical lesions in the mammalian retina. Current Eye Research 1984;3(1):165‐74. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011a
- Higgins JP, Altman DG, Sterne JAC editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011b
- Higgins JPT, Deeks JJ, Altman DG (editors). Chapter 16: Special topics in statistics. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Holz 2013
- Holz FG, Pauleikhoff D, Spaide RF, Bird AC. Age‐related Macular Degeneration. Berlin: Springer‐Verlag, 2013. [Google Scholar]
Jonas 2014
- Jonas JB, Bourne RR, White RA, Flaxman SR, Keeffe J, Leasher J, et al. Visual impairment and blindness due to macular diseases globally: a systematic review and meta‐analysis. American Journal of Ophthalmology 2014;158(4):808‐15. [DOI] [PubMed] [Google Scholar]
Klein 1992
- Klein R, Klein BE, Linton KL. Prevalence of age‐related maculopathy. The Beaver Dam Eye Study. Ophthalmology 1992;99(6):933‐43. [DOI] [PubMed] [Google Scholar]
Klein 1998
- Klein R, Klein BE, Jensen SC, Cruickshanks KJ. The relationship of ocular factors to the incidence and progression of age‐related maculopathy. Archives of Ophthalmology 1998;116(4):506‐13. [DOI] [PubMed] [Google Scholar]
Klein 2005
- Klein RJ, Zeiss C, Chew EY, Tsai JY, Sackler RS, Haynes C, et al. Complement factor H polymorphism in age‐related macular degeneration. Science 2005;308(5720):358‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lawrenson 2017
- Lawrenson JG, Hull CH, Downie LE. The effect of blue‐light blocking spectacle lenses on visual performance, macular health and the sleep‐wake cycle: a systematic review of the literature. Ophthalmic and Physiological Optics 2017;37(6):644‐54. [DOI] [PubMed] [Google Scholar]
Lee 2012
- Lee RM, Lam FC, Liu CS. Blue‐blocking intraocular implants should be used routinely during phacoemulsification surgery ‐ No. Eye 2012;26:1400‐1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Liu 1989
- Liu IY, White L, LaCroix AZ. The association of age‐related macular degeneration and lens opacities in the aged. American Journal of Public Health 1989;79(6):765‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Luu 2013
- Luu CD, Dimitrov PN, Wu Z, Ayton LN, Makeyeva G, Aung KZ, et al. Static and flicker perimetry in age‐related macular degeneration. Investigative Ophthalmology and Visual Science 2013;54(5):3560‐8. [DOI] [PubMed] [Google Scholar]
Mainster 1978
- Mainster MA. Solar retinitis, photic maculopathy and the pseudophakic eye. Journal of the American Intra‐Ocular Implant Society 1978;4(3):84‐6. [DOI] [PubMed] [Google Scholar]
Mainster 1986
- Mainster MA. The spectra, classification, and rationale of ultraviolet‐protective intraocular lenses. American Journal of Ophthalmology 1986;102(6):727‐32. [DOI] [PubMed] [Google Scholar]
Mainster 2005
- Mainster MA. Intraocular lenses should block UV radiation and violet but not blue light. Archives of Ophthalmology 2005;123(4):550‐5. [DOI] [PubMed] [Google Scholar]
Mainster 2006
- Mainster MA. Violet and blue light blocking intraocular lenses: photoprotection versus photoreception. British Journal of Ophthalmology 2006;90(6):784‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mainster 2010
- Mainster MA, Turner PL. Blue‐blocking IOLs decrease photoreception without providing significant photoprotection. Survey of Ophthalmology 2010;55(3):272‐89. [DOI] [PubMed] [Google Scholar]
Mainster 2011
- Mainster MA, Turner PL. Blue‐blocking IOLs vs. short‐wavelength visible light: hypothesis‐based vs. evidence‐based medical practice. Ophthalmology 2011;118(1):1‐2. [DOI] [PubMed] [Google Scholar]
Margrain 2004
- Margrain TH, Boulton M, Marshall J, Sliney DH. Do blue light filters confer protection against age‐related macular degeneration?. Progress in Retinal and Eye Research 2004;23(5):523‐31. [DOI] [PubMed] [Google Scholar]
Ng 2014
- Ng SM, Lindsley K, Akpek EK. Omega‐3 and omega‐6 polyunsaturated fatty acids for dry eye syndrome. Cochrane Database of Systematic Reviews 2014, Issue 3. [DOI: 10.1002/14651858.CD011016] [DOI] [PMC free article] [PubMed] [Google Scholar]
Norren 1974
- Norren DV, Vos JJ. Spectral transmission of the human ocular media. Vision Research 1974;14(11):1237‐44. [DOI] [PubMed] [Google Scholar]
Owen 2003
- Owen CG, Fletcher AE, Donoghue M, Rudnicka AR. How big is the burden of visual loss caused by age related macular degeneration in the United Kingdom?. British Journal of Ophthalmology 2003;87(3):312‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Parish 1998
- Parish CA, Hashimoto M, Nakanishi K, Dillon J, Sparrow J. Isolation and one‐step preparation of A2E and iso‐A2E, fluorophores from human retinal pigment epithelium. Proceedings of the National Academy of Sciences of the United States of America 1998;95(25):14609‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pascolini 2012
- Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. British Journal of Ophthalmology 2012;95(5):614‐8. [DOI] [PubMed] [Google Scholar]
Prinsen 2014
- Prinsen CA, Vohra S, Rose MR, King‐Jones S, Ishaque S, Bhaloo Z, et al. Core Outcome Measures in Effectiveness Trials (COMET) initiative: protocol for an international Delphi study to achieve consensus on how to select outcome measurement instruments for outcomes included in a ‘core outcome set’. Trials 2014;15:247. [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rudnicka 2012
- Rudnicka AR, Jarrar Z, Wormald R, Cook DG, Fletcher A, Owen CG. Age and gender variations in age‐related macular degeneration prevalence in populations of European ancestry: a meta‐analysis. Ophthalmology 2012;119(3):571‐80. [DOI] [PubMed] [Google Scholar]
Sarks 1999
- Sarks SH, Arnold JJ, Killingsworth MC, Sarks JP. Early drusen formation in the normal and aging eye and their relation to age related maculopathy: a clinicopathological study. British Journal of Ophthalmology 1999;83(3):358‐68. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schulz 2002
- Schulz KF, Grimes DA. Sample size slippages in randomised trials: exclusions and the lost and wayward. Lancet 2002;359(9308):781‐5. [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Higgins JP, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and ‘Summary of findings' tables. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Snell 1998
- Snell RS, Lemp MA. Clinical Anatomy of the Eye. Oxford: Blackwell Science, 1998. [Google Scholar]
Sui 2013
- Sui GY, Liu GC, Liu GY, Gao YY, Deng Y, Wang WY, et al. Is sunlight exposure a risk factor for age‐related macular degeneration? A systematic review and meta‐analysis. British Journal of Ophthlamology 2013;97(4):389‐94. [DOI] [PubMed] [Google Scholar]
Symes 2012
- Symes RJ, Cuthbertson FM. Blue‐blocking intraocular implants should be used routinely during phacoemulsification surgery‐‐yes. Eye 2012;26(11):1397‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Thornton 2005
- Thornton J, Edwards R, Mitchell P, Harrison RA, Buchan I, Kelly SP. Smoking and age‐related macular degeneration: a review of association. Eye 2005;19(9):935‐44. [DOI] [PubMed] [Google Scholar]
Van Norren 2007
- Norren D, Kraats J. Spectral transmission of intraocular lenses expressed as a virtual age. British Journal of Ophthalmology 2007;91(10):1374‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wald 1945
- Wald G. Human vision and the spectrum. Science 1945;101(2635):653‐8. [DOI] [PubMed] [Google Scholar]
Wong 2014
- Wong WL, Su X, Li X, Cheung CM, Klein R, Cheng CY, et al. Global prevalence of age‐related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta‐analysis. Lancet Global Health 2014;2(2):e106‐16. [DOI] [PubMed] [Google Scholar]
Wu 2013
- Wu Z, Ayton LN, Guymer RH, Luu CD. Intrasession test‐retest variability of microperimetry in age‐related macular degeneration. Investigative Ophthalmology and Visual Science 2013;54(12):7378‐85. [DOI] [PubMed] [Google Scholar]
Yang 2006
- Yang Z, Camp NJ, Sun H, Tong Z, Gibbs D, Cameron DJ, et al. A variant of the HTRA1 gene increases susceptibility to age‐related macular degeneration. Science 2006;314(5801):992‐3. [DOI] [PubMed] [Google Scholar]
Youssef 2011
- Youssef PN, Sheibani N, Albert DM. Retinal light toxicity. Eye 2011;25:1‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zhu 2012
- Zhu XF, Zou HD, Fu YF, Sun Q, Zhao NQ. Comparison of blue‐light filtering IOLs and UV light‐iltering IOLs for cataract surgery: a meta‐analysis. PloS One 2012;7(3):e33013. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Downie 2015
- Downie LE, Busija L, Keller PR. Blue‐light filtering intraocular lenses (IOLs) for protecting macular health. Cochrane Database of Systematic Reviews 2015, Issue 11. [DOI: 10.1002/14651858.CD011977] [DOI] [PMC free article] [PubMed] [Google Scholar]