

Abstract
We present a rare case of spontaneous regression in a typical lung carcinoid. A 20-year-old woman with an abnormal shadow on a chest radiograph was admitted to our hospital. Computed tomography revealed a smooth nodule in the left S1 + 2 segment. At the 6-month follow-up, the nodule had regressed without treatment. At the 2-year follow-up, the tumor reappeared in the same place as before. We performed left upper lobectomy via 4-port thoracoscopic surgery. A pathological examination revealed a typical carcinoid. Lung carcinoids can spontaneously regress; long-term follow-up is important for timely detection of tumor reappearance.
Keywords: Lung carcinoid, Spontaneous regression, Recurrence, Thoracoscopic surgery
Introduction
Spontaneous regression (SR) is the partial or complete disappearance of primary or metastatic tumor tissue in the absence of treatment [1]. It occurs approximately once in every 60,000–100,000 cancer cases and is less common in non-small cell lung carcinoma than other tumor types [2]. Herein, we present a rare case in which a typical carcinoid spontaneously regressed; however, thoracoscopic surgery was required after 30 months due to the reemergence of the tumor.
Case report
A 20-year-old woman was referred to our hospital for the evaluation of an abnormal shadow in a periodic chest radiograph examination. She had no anamnesis, and her physical examination was unremarkable. At our hospital, a chest radiograph showed a round mass shadow in the left middle lung field (Fig. 1), and chest computed tomography (CT) showed a nodule 1.9 cm in diameter in the left S1 + 2 segment (Fig. 2a). The tumor border was clear and smooth. The clinical diagnosis was a hamartoma or other benign tumor; the cause could not be identified. Six months after diagnosis, the tumor nodule shadow had regressed (Fig. 2b) spontaneously.
Fig. 1.
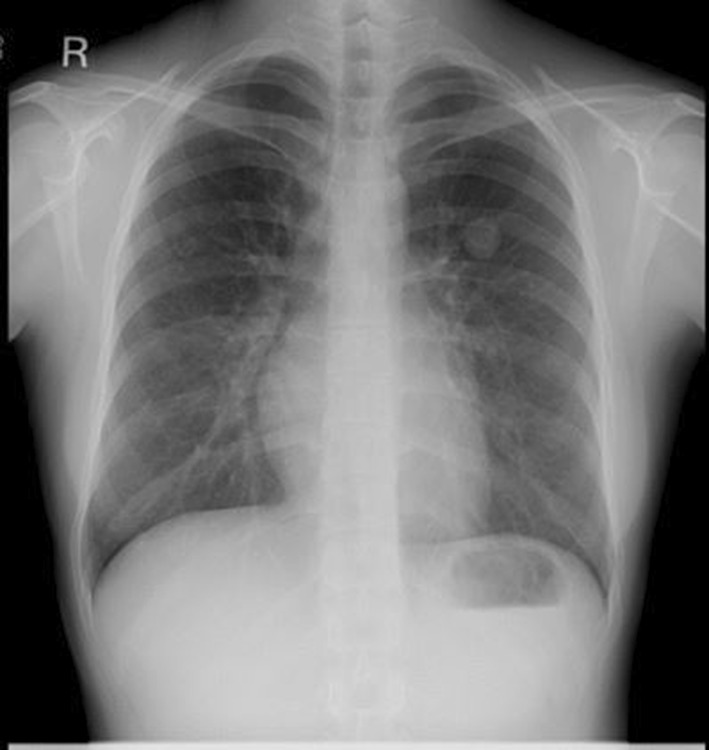
Initial chest radiograph showing a round mass shadow in the left middle lung field. R right
Fig. 2.

Spontaneous regression and reappearance of the tumor. a Initial computed tomography (CT) scan showing a nodule 1.9 cm in diameter in the left S1 + 2 segment. b CT scan at 6 months. c CT scan at 2 years. d CT scan at 2.5 years
The patient underwent chest radiography each year, and the chest radiograph at the 2-year follow-up showed a mass shadow, which we investigated further using CT. It showed a nodule 1.4 cm in diameter in the same place as before (Fig. 2c). Six months later, the tumor had increased in size (Fig. 2d). To remove and diagnose the tumor, left upper division segmentectomy via 4-port thoracoscopic surgery was performed. Intraoperative rapid diagnosis of a frozen tumor section indicated a carcinoid tumor; hence, we also performed lingular division segmentectomy with ND2a-1 lymph node dissection.
The postoperative course was good with no complications. A pathological examination revealed a typical carcinoid with no lymph node metastasis (Fig. 3). The patient has remained disease-free for 42 months after the surgery.
Fig. 3.

Carcinoid tumor showing monotonous round cells with finely granular chromatin arranged in an organized pattern. There was no necrosis or mitotic cells. a Hematoxylin and eosin, × 10. b Hematoxylin and eosin, × 40
Discussion
The case demonstrates two key points. First, SR can occur in lung carcinoid cases. Eberson and Cole defined SR as a complete or partial disappearance of all or at least some relevant parameters of a soundly diagnosed malignant disease [3]. SR is rare in thoracic malignancies: a literature review by Kumar et al. found only five instances of SR in true primary thoracic malignancies [4]. There are several reports of SR of gastric and pelvic neuroendocrine tumors in the English literature, but only two reports of SR of lung carcinoid tumors [5, 6]. In the present case, the tumor initially disappeared without treatment and then reappeared approximately 2 years later.
Second, it is important to follow the patient even if the tumor has seemingly disappeared. In a case reported in 2017, a spontaneously regressed endobronchial carcinoid tumor followed for 2 years did not recur [6]. Also reported was partial SR of a metastatic lung adenocarcinoma within a month of diagnosis [7]. However, in our case, the tumor reappeared approximately 2 years after its almost complete disappearance.
Conclusion
Lung carcinoids can spontaneously regress. However, long-term follow-up is required even if the tumor is no longer evident.
Acknowledgements
We would like to thank Editage (http://www.editage.jp) for English language editing.
Abbreviations
- CT
Computed tomography
- SR
Spontaneous regression
Author contributions
HM: drafted and revised the manuscript. AS: revised the manuscript. HM: revised the manuscript. TI: revised the manuscript. HN: revised the manuscript.
Funding
The authors did not receive any funding for this report.
Conflict of interest
The authors have no conflicts of interest to disclose.
Informed consent
Written informed consent was obtained from the patient for publication of this article and accompanying images.
References
- 1.Everson TC, Cole WH. Spontaneous regression of cancer: preliminary report. Ann Surg. 1956;144:366–380. doi: 10.1097/00000658-195609000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cole WH. Efforts to explain spontaneous regression of cancer. J Surg Oncol. 1981;17:201–209. doi: 10.1002/jso.2930170302. [DOI] [PubMed] [Google Scholar]
- 3.Everson TC, Cole WH. Spontaneous regression of malignant disease. J Am Med Assoc. 1959;169:1758–1759. doi: 10.1001/jama.1959.03000320060014. [DOI] [PubMed] [Google Scholar]
- 4.Kumar T, Patel N, Talwar A. Spontaneous regression of thoracic malignancies. Respir Med. 2010;104:1543–1550. doi: 10.1016/j.rmed.2010.04.026. [DOI] [PubMed] [Google Scholar]
- 5.Luosto R, Koikkalainen K, Sipponen P. Spontaneous regression of a bronchial carcinoid tumour following pregnancy. Ann Chir Gynaecol Fenn. 1974;63:342–345. [PubMed] [Google Scholar]
- 6.Venkatram S, Sinha N, Hashmi H, et al. Spontaneous regression of endobronchial carcinoid tumor. J Bronchol Intervent Pulmonol. 2017;24:70–74. doi: 10.1097/LBR.0000000000000232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Haruki T, Nakamura H, Taniguchi Y, et al. Spontaneous regression of lung adenocarcinoma: report of a case. Surg Today. 2010;40:1155–1158. doi: 10.1007/s00595-009-4195-2. [DOI] [PubMed] [Google Scholar]