

Abstract
Erector spinae plane (ESP) block is a recently described regional anaesthesia/analgesia technique. Although there is stil no consensus on its mechanism, the published case series seem to promise a new block for both chronic and acute pain. In this case report, the use of ESP block in 47-year-old female patient scheduled for bilateral segmental mastectomy surgery is presented. ESP was formerly reported for rib fracture, bariatric surgery, open abdominal surgery and breast implant surgery. To the best of our knowledge, no article has been published for ESP block in breast cancer surgery including axillary dissection.
Keywords: Analgesia, breast cancer, operations, regional anaesthesia
Introduction
Erector spinae plane (ESP) block was first described by Forero et al. (1). Since then, there have been several articles regarding its use in postoperative analgesia in different surgical procedures (1, 2). The simplicity and safety compared with thoracic epidural or bilateral paravertebral blocks are the advantages of this new technique (4). Although there is still not enough clear data over its analgesic range, it was documented that ESP block prevents both visceral and somatic pain in several case reports including breast implant surgery (5–7). Here, we present a successful ESP block for postoperative analgesia in a patient underwent bilateral segmental mastectomy.
Case Presentation
A 47-year-old woman (64 kg, 168 cm), was admitted to the hospital for bilateral malignant breast cancer surgery. She had no significant medical history and her American Society of Anesthesiologists score was I. After written informed consent was obtained from the patient, bilateral ESP block was planned for postoperative regional analgesia in addition to the multimodal therapy. Induction of anaesthesia was performed using propofol 2 mg kg−1, fentanyl 100 μg and rocuronium 0.5 mg kg−1. Anaesthesia was maintained by remifentanil infusion at the rate of 0.08 μg kg−1 min−1 and 1% sevoflurane. The procedure comprised left segmental mastectomy, left axillary dissection and right segmental mastectomy for fibroadenoma extraction. The patient received 1 g paracetamol and a further dose of fentanyl during the operation. Before the end of anaesthesia, bilateral ESP block was performed in the lateral decubitus position at T4 transverse process level using 10-MHz linear ultrasound probe (Logic E book XP General Electrics, USA). The probe was located 3 cm lateral to T1 spinous process in longitudinal parasagittal orientation and the scan from T1 to T5 revealed the erector spinae, rhomboid major and trapezius muscles posterior and superficial to the transverse processes. An 8 cm, 21-gauge needle (BRAUN Stimuplex A®, Germany) was inserted using out-of-plane technique at level of T4 transverse process. The injections were applied after the confirmation of location by hydrodissection developed anterior to erector spinae muscle with 1–2 mL of local anaesthetic solution (Figure 1). For the block, 10 mL of 0.25% bupivacaine and 5 mL of 0.5% lidocaine diluted to a 20 mL mixture was used on each side. Following tracheal extubation, the patient was transferred to the post-anaesthetic care unit (PACU). Pain was measured using numeric rating scale (NRS) (‘0’ representing ‘no pain’, ‘10’ representing ‘worst pain imaginable’) and it was <3 in PACU. The patient’s modified Aldrete’s score was 10 and she was transferred to the general ward. She did not need any rescue analgesic during the first 18 hours postoperatively. Oral diclofenac sodium 75 mg three times a day was prescribed for analgesia, and the patient was discharged with NRS <4.
Figure 1.
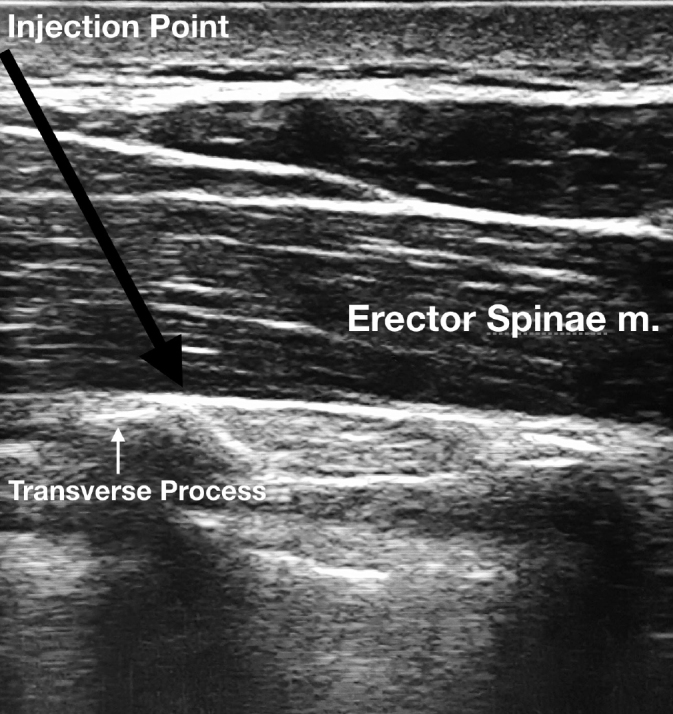
Ultrasound-guided Erector Spinae Block Performance at the T4 Level
Discussion
Successful ESP blocks have been used in major abdominal surgery, neuropathic pain, pneumothorax and breast implant surgeries (1, 7–9). Although the mechanism of analgesic efficacy of ESP block remains unclear, previous cadaver models have demonstrated that deposition of local anaesthetic deep (anterior) to the erector spinae muscle reaches the paravertebral space through connective tissues and ligaments (4). Radiological imaging of a cadaver model has shown that ESP leads to widespread sensory block between C7 and T8 when it is applied at the level of T5. This area was our target field for bilateral partial resections and left axillary dissection that reaches the posterolateral chest wall. Axillary dissection may lead to damage to the thoracodorsal, long thoracic, intercostobrachial nerves and axillary soft tissue, which causes acute and chronic postoperative pain after mastectomy (10, 11). Zocca et al. (12) described ultrasound-guided serratus plane block for post-mastectomy pain syndromes and emphasised the importance of pain management following surgery for breast cancers. However, he has questioned the variations of the thoracodorsal, long thoracic and intercostobrachial nerves as the reason for inadequate analgesia in 2 patients with the serratus anterior plane block. We propose that ESP block may be an alternative and useful choice for postoperative analgesia in breast cancer surgeries, especially those including axillary dissection. Since ESP has an effect on the dorsal, ventral and communicant ramus of spinal nerve roots, it is similar to paravertebral block or thoracic epidural block, without the complications attributed to these two major methods (4). In addition, it is easy to perform in intubated patients with fewer complications because the needle insertion point is at a distant location to important anatomical structures.
In this case local anaesthetic injection was applied bilaterally and total 100 mg bupivacaine and 200 mg lidocaine, which were used under advised toxic levels for these drugs, were used in total 40 ml volume. Local anaesthetic toxicity should always be considered as a severe complication for regional anaesthetic techniques, especially for bilateral injections as the one we performed in this case. Although there is still not enough clear data over local analgesic dose in ESP block, De Cassai suggested 3.6 mL of local anaesthetic for each targeted dermatome and he proposed the application of high volume and low concentration formula for plane blocks (13). Therefore, in this case local anaesthetics were diluted and used in a greater volume to reach the adequate spread of sensorial block.
Conclusion
To the best of our knowledge, this is the first description of the use the ESP block used for segmental mastectomy and further controlled clinical trials may better reveal the advantages and the disadvantages of this block.
Footnotes
Informed Consent: Written informed consent was obtained from patient who participated in this case.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept – O.S.; Design – O.S.; Supervision – O.S., S.T.; Resources – O.S.; Materials – O.S.; Data Collection and/or Processing – O.S.; Analysis and/or Interpretation – O.S., S.T.; Literature Search – O.S.; Writing Manuscript – O.S., S.T.; Critical Review – O.S., S.T.; Other – O.S.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The Erector Spinae Plane Block: A Novel Analgesic Technique in Thoracic Neuropathic Pain. Reg Anesth Pain Med. 2016;41:621–7. doi: 10.1097/AAP.0000000000000451. [DOI] [PubMed] [Google Scholar]
- 2.Tulgar S, Senturk O. Ultrasound guided Erector Spinae Plane block at L-4 transverse process level provides effective postoperative analgesia for total hip arthroplasty. J Clin Anesth. 2018;44:68. doi: 10.1016/j.jclinane.2017.11.006. [DOI] [PubMed] [Google Scholar]
- 3.Yamak EA, García DS, Fajardo-Pérez M. Erector spinae plane block for analgesia after lower segment caesarean section: Case report. Rev Esp Anestesiol Reanim. 2018;65:284–6. doi: 10.1016/j.redar.2017.11.006. [DOI] [PubMed] [Google Scholar]
- 4.Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. 2017;42:372–6. doi: 10.1097/AAP.0000000000000581. [DOI] [PubMed] [Google Scholar]
- 5.Forero M, Rajarathinam M, Adhikary SD, Chin KJ. Erector spinae plane block for the management of chronic shoulder pain: a case report. Can J Anaesth. 2018;65:288–93. doi: 10.1007/s12630-017-1010-1. [DOI] [PubMed] [Google Scholar]
- 6.Chin KJ, Adhikary S, Sarwani N, Forero M. The analgesic efficacy of pre-operative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017;72:452–60. doi: 10.1111/anae.13814. [DOI] [PubMed] [Google Scholar]
- 7.Bonvicini D, Giacomazzi A, Pizzirani E. Use of the ultrasound-guided erector spinae plane block in breast surgery. Minerva Anestesiol. 2017;83:1111–2. doi: 10.23736/S0375-9393.17.12015-8. [DOI] [PubMed] [Google Scholar]
- 8.Restrepo-Garces CE, Chin KJ, Suarez P, Diaz A. Bilateral continuous erector spinae plane block contributes to effective postoperative analgesia after major open abdominal surgery: a case report. A A Case Rep. 2017;9:319–21. doi: 10.1213/XAA.0000000000000605. [DOI] [PubMed] [Google Scholar]
- 9.Ueshima H, Otake H. Erector spinae plane block provides effective pain management during pneumothorax surgery. J Clin Anesth. 2017;40:74. doi: 10.1016/j.jclinane.2017.04.016. [DOI] [PubMed] [Google Scholar]
- 10.Andersen KG, Aasvang EK, Kroman N, Kehlet H. Intercostobrachial nerve handling and pain after axillary lymph node dissection for breast cancer. Acta Anaesthesiol Scand. 2014;58:1240–8. doi: 10.1111/aas.12393. [DOI] [PubMed] [Google Scholar]
- 11.Kulhari S, Bharti N, Bala I, Arora S, Singh G. Efficacy of pectoral nerve block versus thoracic paravertebral block for postoperative analgesia after radical mastectomy: a randomized controlled trial. Br J Anaesth. 2016;117:382–6. doi: 10.1093/bja/aew223. [DOI] [PubMed] [Google Scholar]
- 12.Zocca JA, Chen GH, Puttanniah VG, Hung JC, Gulati A. Ultrasound-guided serratus plane block for treatment of postmastectomy pain syndromes in breast cancer patients: a case series. Pain Pract. 2017;17:141–6. doi: 10.1111/papr.12482. [DOI] [PubMed] [Google Scholar]
- 13.De Cassai A, Tonetti T. Local anesthetic spread during erector spinae plane block. J Clin Anesth. 2018;48:60–1. doi: 10.1016/j.jclinane.2018.05.003. [DOI] [PubMed] [Google Scholar]