

Abstract
Background
To explore the association of MRI‐diagnosed severe lumbar spinal stenosis with occupation.
Methods
Occupational data were collected by questionnaire and all participants underwent spine MRI scans using the same protocol. Central lumbar spinal stenosis (LSS) was graded qualitatively. Those with severe LSS (>two‐thirds narrowing) were compared with the controls with lesser degrees of stenosis or no stenosis.
Results
Data were available for 722 subjects, mean age 70.1 years. 239 (33%) cases with severe LSS were identified. Factory/construction workers had an almost four‐fold increased risk of severe LSS after adjustment for age, sex, smoking, and walking speed amongst those aged <75 years (OR 3.97, 95%CI 1.46‐10.85). Severe LSS was also associated with squatting ≥1 h/day (OR 1.76, 95%CI 1.01‐3.07) but this association became non‐significant after adjustment.
Conclusion
Further research is needed but this study adds more evidence that occupational factors are associated with an increased risk and/or severity of degenerative disease of the lumbar spine.
Keywords: factory and construction workers, Lumbar spinal stenosis (LSS), MRI, occupation, occupational exposures
1. INTRODUCTION
Occupational physical activity is associated with osteoarthritis at several different anatomical sites.1, 2, 3, 4 The risk of hip osteoarthritis, for example, is increased amongst agricultural workers5, 6, 7 and that of knee osteoarthritis amongst miners and floor layers.8, 9, 10 Regarding the spine, there has been evidence for some time that physical workplace exposures are associated with an increased risk of low back pain.1, 11, 12, 13, 14, 15, 16 However, most epidemiological studies have involved reporting of symptoms alone and have not included an investigation of spinal structural changes with occupation.
Lumbar spinal stenosis (LSS), defined as a narrowing of the lumbar canal with encroachment of neural structures by surrounding bone and soft tissue, is thought to be a degenerative condition of the spine.17, 18 When severe, symptoms of LSS include neurogenic claudication causing leg pain that increases in intensity with walking speed and distance traveled. These symptoms cause impaired mobility at older ages so that LSS is the most common indication for spinal surgery among people aged >65 years.19, 20
Epidemiological research to define risk factors for LSS has been hampered in the past by lack of reliable clinical or x‐ray criteria. In current clinical practice, magnetic resonance imaging (MRI) has become the preferred diagnostic tool, given that it allows the detection of minute changes of the intervertebral discs and ligaments.21, 22 To date however, there has been limited research to explore the contribution of occupation to structural changes in the spine as investigated by MRI. Therefore, we investigated the prevalence of LSS using spinal MRI in a population sample of adults who had undertaken a range of different occupations, as part of the Wakayama Spine Study. The objective of this analysis was to determine occupational risk factors for severe LSS.
2. MATERIALS AND METHODS
2.1. Participants
The Wakayama Spine Study assessed a sub‐cohort from the Research on Osteoarthritis/Osteoporosis Against Disability (ROAD) study, a large‐scale, prospective study of bone and joint disease among population‐based cohorts in Japan. The detailed profile of the ROAD study is described elsewhere.23 In brief, individuals were recruited from resident registrations in three communities: an urban region in Itabashi, Tokyo; a mountainous region in Hidakagawa, Wakayama; and a coastal region in Taiji, Wakayama. In total, 3040 people (1061 men and 1979 women) consented to take part in a clinical and genetic study approved by the ethics committees of the University of Tokyo and the Tokyo Metropolitan Institute of Gerontology. Participants completed an interviewer‐administered questionnaire that consisted of 400 questions about factors such as demographics, lifestyle and occupation, and they underwent anthropometric measurements and assessments of physical performance.
The Wakayama Spine Study involved a subset of ROAD participants from Hidakagawa and Taiji provinces. Participants were recruited if they had no contraindications to undergo MRI scanning (eg, sensitive implanted devices including pacemakers, claustrophobia) and provided written, informed consent.24 Everyone underwent lumbar spine MRI in a mobile unit (Excelart 1.5 T; Toshiba; Tokyo, Japan). The participants were positioned supine, with pillows if needed. The imaging protocol was as follows: axial images were obtained on T2‐weighted fast spin echo (repetition time: 4000 ms/echo, echo time 120 ms, field of view: 180 × 180 mm) (Figure 1).
Figure 1.
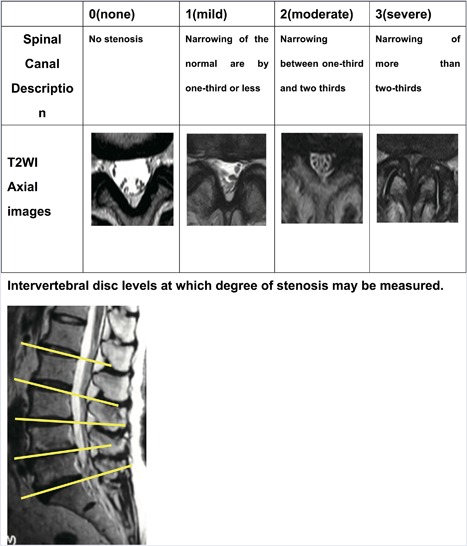
Qualitative central stenosis grading
2.2. Occupation and occupational activities
A lifetime occupational history was collected alongside details of seven types of specific work exposures: sitting on a chair for ≥2 h/day, standing for ≥2 h/day, kneeling for ≥1 h/day, squatting for ≥1 h/day, driving for ≥4 h/day, walking ≥3 km/day, walking upstairs 30 floors/day, climbing up slopes or steps for ≥1 h/day, and lifting loads weighing ≥10 kg at least once a week. For the current study, the information on occupational title and exposures was derived from the respondent's principal occupation (that in which the participant had worked for the longest duration).
2.3. Assessment of lumbar spinal stenosis
Despite the severity of symptoms that can result from LSS, there is to date no consensus as to how to define LSS radiologically using MRI scanning25 and a number of approaches have been suggested.26 For the current study, the severity of LSS on MRI scan was assessed qualitatively by one experienced orthopaedic surgeon (YI) following the methodology of Suri et al.18 The severity of the central canal stenosis was qualitatively graded on the axial images as: no spinal stenosis; mild spinal stenosis—a maximum of 1/3 narrowing; moderate spinal stenosis—narrowing between 1/3 to 2/3, and; severe spinal stenosis as more than 2/3 narrowing (Figure 1).
To confirm the reliability of this methodology, the observer re‐assessed a random sample of 50 of the MRI scans after a period of one month, blinded to the original rating, and achieved excellent intra‐observer reliability with a kappa of 0.82 (95%CI 0.77‐0.86). Moreover, inter‐observer variability was measured between the study observer and another experienced orthopaedic surgeon (KN) for a different sample of 50 MRI scans, achieving a kappa of 0.77 (95%CI 0.73‐0.82) for agreement. None of the included MRI scans were found to have LSS caused by tumor, nor inflammatory, or traumatic pathologies.
2.4. Statistical analysis
Participants’ demographic and lifestyle characteristics were summarized using means and standard deviations (SDs) and proportions (%) separately for those with severe LSS (cases) and those with lesser degrees of LSS or no LSS (controls). Differences in categorical and continuous characteristics between cases and controls were assessed using chi‐squared and t‐tests, respectively. The effects of type of occupation (using clerical/technical experts as a reference category), and occupational activities on severity of LSS were assessed using logistic regression modelling, before and after adjusting for demographic and lifestyle characteristics, and were summarized by odds ratios (ORs) and 95% confidence intervals (CIs).
As the main focus of this study was to explore the association between type of occupation and occupational activities with LSS, and many of the older participants had stopped working as much as 20‐30 years prior to their MRI scan, we repeated the analyses separately for those <75 and ≥75 years of age, allowing a decade after retirement.27
Statistical analyses were performed using Stata V.12.1 (StataCorp, College Station, TX).
3. RESULTS
Complete data were available for 722 participants (245 males, 477 females), mean age 70.9 years, range: 53‐93 years. To explore their representativeness, we compared the study population with the general population for a key characteristic known to be associated with osteoarthritis, body mass index (BMI). We found that the mean BMI of our participants was not significantly different from that of the general population of Japan (males: 23.71 (SD 3.41) vs 23.95 (2.64) kg/m2; females: 23.06 (3.42) vs 23.50 (3.69) kg/m2). In contrast however, we found that the study participants reported a lower prevalence of smoking and alcohol use than that reported by the general Japanese population, suggesting that they might live healthier lifestyles.
In total, 239 (33%) subjects were defined with severe LSS (cases) and the remaining 483 individuals were controls (Table 1). The cases were significantly older than the controls (cases: 74.1 (SD 9.2) years, controls: 69.4 (9.9) years, P < 0.001) but there were no differences in gender, BMI, smoking or alcohol.
Table 1.
Comparison of the demographic and lifestyle characteristics of cases with severe lumbar spinal stenosis as compared with controls
| Cases (N = 239) | Controls (N = 483) | P‐value | |
|---|---|---|---|
| Sex | |||
| Males | 82 (34.3%) | 163 (33.7%) | 0.881 |
| Females | 157 (65.7%) | 320 (66.3%) | |
| Mean age (years (SD)) | 74.1 (9.2) | 69.4 (9.9) | <0.001 |
| Mean BMI (SD) | 23.4 (3.5) | 23.1 (3.4) | 0.27 |
| Usual walking speed m/s (median (IQR)) | 5 (5‐7) | 5 (4‐6) | 0.001 |
| Current smoking status | |||
| Non‐smoker | 222 (92.9%) | 442 (91.5%) | 0.55 |
| Current smoker | 17 (7.1%) | 39 (8.1%) | |
| Any alcohol intake | |||
| None | 176 (73.6%) | 340 (70.4%) | 0.36 |
| Some alcohol | 63 (26.4%) | 143 (29.6%) |
Table 2 shows the associations between occupational group and occupational activities among cases as compared with controls. The results of the unadjusted analyses (Model 1) showed that Agricultural/Fishermen and Factory/Construction workers had a significantly higher risk of severe LSS when compared with the referent group of Clerical/Technical workers: Agricultural/Fishermen: OR 1.99, 95%CI 1.22‐3.26, Factory/Construction: OR 2.08, 95%CI 1.09‐3.96. Moreover, the risk of severe LSS was increased with kneeling ≥1 h/day (OR 1.56, 95%CI 1.04‐2.35), squatting ≥1 h/day OR 1.44, 95%CI 1.00‐2.08), and walking ≥3 h/day (OR 1.41, 95%CI 1.02‐1.95).
Table 2.
Comparison of the associations with occupational group and occupational activities between cases with severe lumbar spinal stenosis and controls without
| Model 1 | Model 2 | Model 3 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total N | Cases | Controls | OR | 95%CIs | P | OR | 95%CIs | P | OR | 95%CIs | P | |
| Occupational group | ||||||||||||
| Clerical/technical experts | 197 | 57 | 140 | Baseline | Baseline | Baseline | ||||||
| Agricultural/Fishermen | 105 | 47 | 58 | 1.99 | (1.22,3.26) | 0.01 | 1.37 | (0.82,2.30) | 0.23 | 1.35 | (0.79,2.28) | 0.27 |
| Factory/construction | 48 | 22 | 26 | 2.08 | (1.09,3.96) | 0.03 | 1.73 | (0.89,3.35) | 0.11 | 1.72 | (0.88,3.34) | 0.11 |
| Clinical/Housekeepers/Shop assistants/Hairdressers/Dressmakers | 207 | 63 | 144 | 1.07 | (0.70,1.65) | 0.74 | 1 | (0.65,1.56) | 0.98 | 0.92 | (0.58,1.45) | 0.71 |
| Teachers | 51 | 18 | 33 | 1.34 | (0.70,2.57) | 0.38 | 1.1 | (0.56,2.16) | 0.78 | 1.2 | (0.60,2.37) | 0.61 |
| Other/NA | 114 | 32 | 82 | 0.96 | (0.57,1.60) | 0.87 | 0.91 | (0.54,1.54) | 0.74 | 0.85 | (0.50,1.45) | 0.55 |
| Occupational activities | ||||||||||||
| Sitting | 347 | 109 | 238 | 0.86 | (0.63,1.18) | 0.35 | 1.01 | (0.73,1.39) | 0.97 | 1 | (0.72,1.39) | 0.99 |
| Standing | 574 | 199 | 375 | 1.43 | (0.96,2.14) | 0.08 | 1.2 | (0.79,1.81) | 0.4 | 1.22 | (0.80,1.85) | 0.36 |
| Kneeling | 115 | 48 | 67 | 1.56 | (1.04,2.35) | 0.03 | 1.44 | (0.95,2.19) | 0.09 | 1.43 | (0.94,2.17) | 0.1 |
| Squatting | 159 | 63 | 96 | 1.44 | (1.00,2.08) | 0.05 | 1.24 | (0.85,1.81) | 0.26 | 1.25 | (0.86,1.82) | 0.25 |
| Driving | 35 | 13 | 22 | 1.21 | (0.60,2.44) | 0.6 | 1.16 | (0.56,2.38) | 0.69 | 1.13 | (0.54,2.37) | 0.74 |
| Walking | 238 | 91 | 147 | 1.41 | (1.02,1.95) | 0.04 | 1.05 | (0.74,1.49) | 0.78 | 1.07 | (0.75,1.52) | 0.71 |
| Upstairs | 169 | 51 | 118 | 0.84 | (0.58,1.22) | 0.36 | 0.8 | (0.54,1.17) | 0.25 | 0.79 | (0.54,1.17) | 0.24 |
| Climbing | 94 | 38 | 56 | 1.44 | (0.92,2.25) | 0.11 | 0.9 | (0.56,1.44) | 0.65 | 0.92 | (0.56,1.50) | 0.73 |
| Lifting | 327 | 109 | 218 | 1.02 | (0.75,1.39) | 0.9 | 0.93 | (0.67,1.28) | 0.64 | 0.91 | (0.65,1.26) | 0.56 |
Model 1: Unadjusted OR; Model 2: Adjusted for age; Model 3: Adjusted for age, sex, BMI, smoking, usual walking speed.
After adjustment for age (Model 2), none of the statistically significant associations with occupational title or activity were retained and similarly attenuated effects were seen after full adjustment for age, sex, BMI, smoking, and usual walking speed (Model 3).
Table 3 presents the stratified analysis by age using 75 years as a cut‐point. Among the participants aged ≥75 years, no statistically significant associations were seen for severe LSS and any occupational group or exposure, with or without adjustment for sex, BMI, smoking, and usual walking speed (Models 1 or 2) (Figure 2). However, the analyses among the younger subjects (aged <75 years) showed a stronger association between severe LSS in factory/construction workers compared with the referent group (OR 4.38, 95%CI 1.66‐11.59) (Model 1), an effect which was robust to adjustment for age, sex, BMI, smoking, and usual walking speed (OR 3.97, 95%CI 1.46‐10.85) (Model 2). Additionally, severe LSS was associated with squatting ≥1 h/day (OR 1.76, 95%CI 1.01‐3.07) in the unadjusted analyses but this association became non‐significant after adjustment (Model 2).
Table 3.
Comparison of the associations with occupational group and occupational activities between cases with severe lumbar spinal stenosis and controls with no severe stenosis, stratified by age
| <75 years | > = 75 years | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||||||
| OR | 95%CIs | P | OR | 95%CIs | P | OR | 95%CIs | P | OR | 95%CIs | P | |
| Occupational group | ||||||||||||
| Clerical/technical experts | Baseline | Baseline | Baseline | Baseline | ||||||||
| Agricultural/Fishermen | 1.79 | (0.73,4.41) | 0.2 | 1.49 | (0.59,3.79) | 0.4 | 1.22 | (0.63,2.37) | 0.55 | 1.17 | (0.59,2.31) | 0.65 |
| Factory/construction | 4.38 | (1.66,11.59) | <0.001 | 3.97 | (1.46,10.85) | 0.01 | 0.83 | (0.34,2.06) | 0.69 | 0.79 | (0.32,1.97) | 0.61 |
| Clinical/Housekeepers/Shop assistants/Hairdressers/Dressmakers | 0.92 | (0.51,1.66) | 0.79 | 0.85 | (0.46,1.58) | 0.61 | 1.19 | (0.61,2.32) | 0.62 | 0.96 | (0.47,1.96) | 0.91 |
| Teachers | 1.34 | (0.48,3.75) | 0.57 | 1.55 | (0.54,4.43) | 0.41 | 0.91 | (0.37,2.21) | 0.83 | 0.97 | (0.39,2.45) | 0.95 |
| Other/NA | 1.26 | (0.65,2.45) | 0.49 | 1.1 | (0.55,2.19) | 0.79 | 0.6 | (0.26,1.36) | 0.22 | 0.54 | (0.23,1.24) | 0.14 |
| Occupational activities | ||||||||||||
| Sitting | 0.77 | (0.49,1.21) | 0.27 | 0.75 | (0.47,1.19) | 0.22 | 1.23 | (0.78,1.93) | 0.38 | 1.32 | (0.82,2.11) | 0.25 |
| Standing | 1.4 | (0.82,2.39) | 0.21 | 1.4 | (0.81,2.42) | 0.23 | 0.95 | (0.49,1.84) | 0.87 | 0.93 | (0.47,1.86) | 0.85 |
| Kneeling | 1.44 | (0.78,2.65) | 0.24 | 1.26 | (0.67,2.35) | 0.47 | 1.54 | (0.87,2.74) | 0.14 | 1.49 | (0.83,2.69) | 0.18 |
| Squatting | 1.76 | (1.01,3.07) | 0.05 | 1.51 | (0.85,2.69) | 0.16 | 1 | (0.61,1.64) | 1 | 0.97 | (0.58,1.61) | 0.9 |
| Driving | 1.28 | (0.44,3.71) | 0.65 | 1 | (0.33,3.04) | 1 | 1.03 | (0.39,2.68) | 0.96 | 1.37 | (0.50,3.75) | 0.54 |
| Walking | 1.07 | (0.62,1.86) | 0.8 | 1.01 | (0.58,1.77) | 0.97 | 1.11 | (0.71,1.73) | 0.65 | 1.15 | (0.72,1.83) | 0.56 |
| Upstairs | 0.77 | (0.44,1.35) | 0.36 | 0.69 | (0.38,1.24) | 0.21 | 0.84 | (0.50,1.40) | 0.49 | 0.89 | (0.52,1.51) | 0.67 |
| Climbing | 1.22 | (0.37,3.98) | 0.74 | 1.13 | (0.33,3.85) | 0.85 | 0.93 | (0.56,1.55) | 0.78 | 0.91 | (0.53,1.57) | 0.74 |
| Lifting | 1.15 | (0.73,1.81) | 0.55 | 1.08 | (0.66,1.75) | 0.76 | 0.74 | (0.47,1.15) | 0.18 | 0.76 | (0.48,1.21) | 0.24 |
Model 1: Unadjusted OR; Model 2: Adjusted for age, sex, BMI, smoking, usual walking speed.
Figure 2.
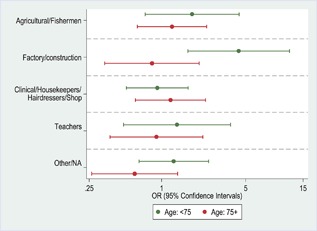
Comparison of the adjusted associations (OR and 95%CIs) among cases with severe LSS, as compared with controls without, among people from the different occupational, stratified by age
4. DISCUSSION
The results of this study suggest that severe LSS, assessed by MRI scan, was associated with heavy manual work particularly in the Factory/Construction industries. The strength of the association was strongest among individuals aged <75 years in whom the risk was increased almost four‐fold, even after adjustment for age, gender, BMI, smoking, and usual walking speed. We also tried to identify which specific occupational activities might be implicated in severe LSS. The exposures that were implicated were: kneeling ≥1 h/day, squatting ≥1 h/day and walking ≥3 h/day, but none of these showed statistically significant associations after full adjustment for participants’ characteristics.
It is noteworthy that these significant associations with agricultural/construction work were found among an older cohort of adults (mean age >70 years, range 53‐93 years), among whom we found a high prevalence of LSS changes on MRI scan (only 5/722, 0.7% had no central canal stenosis). Because of the high prevalence of changes, our comparisons were between the 239 cases with ”severe” LSS (defined as narrowing ≥two‐thirds) and the 483 “controls” amongst whom the prevalence of no LSS was only 5/483 (1%), the remainder being mild LSS 132/483 (27%) and moderate LSS 346/483 (72%). In consequence, the comparison was across the spectrum of severity rather between those with and without LSS. If occupation is a risk factor for onset of LSS we would have expected to see even larger effects were the control population free of stenosis on MRI scan.
There are other limitations that need to be considered. First, the participants in this study were a population sample but were not selected at random. When we explored their representativeness, we found that they had BMI similar to that of the general population but that the participants might have healthier lifestyles (lower levels of smoking and alcohol) than the background population. This may limit the generalizability of these findings and more research is required.
Second, the study design did not allow recruitment of elderly institutionalized adults as volunteers needed to be sufficiently healthy to participate, attend for physical function tests and undergo an MRI scan. As LSS is one of the common causes of impaired mobility in older people and immobility may lead to institutionalization, this may have created a bias, but if so, the effect would have been likely to reduce the estimated prevalence of LSS. The effect of this on the current findings would only be biased if we believe that those who previously performed certain occupations were more likely to be institutionalized than those previously employed in others, which seems unlikely.
In this study, ascertainment of occupational exertional exposures was by direct inquiry rather than being inferred from job title, a method that is well recognized to perform poorly in the absence of a job exposure matrix. The information is dependent upon recall, which may be subject to bias. Moreover, we analyzed data relative to the occupation which was held for the longest period of time during each participant's working lifetime (the principal occupation) which may not accurately represent an entire working life experience of exposures.
It is a strength of this study that all MRI scans were performed in the same scanner using one protocol. Moreover, all scans were assessed by one highly‐trained orthopaedic surgeon (YI). In addition, considerable efforts were made to guarantee the reliability of the assessments by the observer, including inter‐observer and intra‐observer studies with a sample of 5% of the MRI scans, both of which suggested a very good level of reliability (kappa >0.7 in both studies).
Occupations involving physical loading activities have been implicated in the causal pathway of osteoarthritis at other anatomical sites, particularly the knee and hip joints.28, 29 Back pain and degenerative changes at the cervical and lumbar spine have also been reported since the 1950s, implicating both occupational exposures such as heavy lifting and whole‐body vibration, and exposures outside work.1, 8, 30 LSS is a degenerative spinal condition and therefore, it is not unexpected that heavy manual work might be associated with its occurrence and/or severity.
Although there have been many studies of low back pain and occupation,11, 12, 13, 14, 15, 16 we found little published evidence about LSS and occupation. One study which explored LSS using lumbar spine radiographs reported that men who did heavy manual work had smaller anteroposterior foraminal diameters than men whose work involved less physical labor but that, paradoxically, the mean anteroposterior foraminal diameters were wider in female farm workers than in other women.31 Another study explored hospitalizations for back disorders by industrial classification using population census data linked with hospital registry data.32 Data on LSS were only available amalgamated with spondylosis and back‐pain syndromes in the category “other common back disorders.” In this category, agricultural workers and animal caretakers had a considerably higher rate of hospital admissions (age‐standardized risk ratio (SRR) 388 for men and 304 for women). Among women, mail carriers and sorters (SRR 237) were also at high risk and, among men, assemblers, assembly line workers, and other occupations in iron and metal work (SRR 192).32
We found one other MRI study, in which Mariconda and colleagues assessed LSS among 120 patients aged 40‐84 years, all of whom had LBP.33 The investigators estimated occupational lifetime exposures from self‐reported questionnaires. LSS, (defined as a dural sac cross‐sectional area of less than 100 mm2) was not associated with any occupational exposure in the age‐adjusted univariate analyses. However, in the multivariate backward logistic regression model, manual materials handling was found to be associated with LSS, albeit with wide confidence intervals (OR 4.76 1.24‐18.20, P = 0.023). Paradoxically, exposure to occupational awkward postures was associated with a protective effect (OR 0.54, 0.29‐1.01, P = 0.054).
Taken together with previous findings, the current study offers new epidemiological evidence to suggest an association between LSS confirmed on MRI scanning and physical work exposures. However, this finding will require investigation in other populations and suggests that additional laboratory or ergonomic investigation of the workplace risks is needed.
Our finding that the associations of LSS with occupation become attenuated at older ages (≥ 75 years) is not surprising. Many Japanese industries have an age of retirement before age 65 years.25 Given that this was an older cohort, age 53‐93 years, many participants would have stopped work some years before their MRI scan. The effects of age, survival, BMI, and other factors (eg, non‐occupational physical activity) would intuitively play a greater role in determining an individual's measured risk of LSS as time since stopping work increases.
In any study of occupation, the healthy worker effect is of relevance, particularly when participants are selected for inclusion from within the workplace as, of course, workers who are least healthy are those most unable to attend work. We do not believe that this effect will have paid a significant part in the current study given that this was a community study in which all participants reported upon their lifetime occupational exposure. If anything, we would expect that those with most severe back pain symptoms would have self‐selected themselves into more desk‐based and sedentary types of work during their lifetimes, attenuating the association between exposure and effect. Alternatively however, it could be conjectured that Japanese workers in rural settings might have difficulty finding alternative employment or that the Japanese work culture encourages workers to continue in manual work despite troublesome back symptoms. Either way, the findings of the current study suggest an impact of heavy manual tasks on the risk of LSS and it will be important to determine if these findings are replicated in other workforces.
In conclusion, we present the first population study describing the association of heavy manual work with severe LSS, particularly among people aged <75 years at the time of the MRI scan. According to our results, the risk appears strongest in those from the factory and construction industries but it would be important to understand what aspects of these jobs are specifically associated and undertake research to explore how best to prevent any adverse impacts. This finding needs replication in other cohorts but could have implications for countries that define and compensate “industrial injuries.”
AUTHORS' CONTRIBUTION
All authors worked collectively to develop the protocols and methods described in this paper. YI, SM, KN, NO were the principal investigators responsible for the fieldwork in the Wakayama Spine Study. GN performed the statistical analysis. YI, CC, and KWB contributed to the analysis and interpretation of results. YI wrote the report. All authors read and approved the final report. They agreed to be accountable for all aspects of this paper.
FUNDING
Grant sponsor: Grants‐in‐Aid for Scientific Research; Grant number: B20390182, B23390357, C20591737, C20591774 and C22591639. Grant sponsor: Young Scientists: Grant number: A18689031. Grant sponsor: Exploratory Research from the Japanese Ministry of Education, Culture, Sports, Science and Technology; Grant number: 19659305. Grant sponsor: Grants‐in‐Aid from the Ministry of Health, Labour and Welfare: Grant number: H17‐Men‐eki‐009, H18‐Choujyu‐037, and H20‐Choujyu‐009. Grant sponsor: Research Aid from the Japanese Orthopaedic Association (JOA‐Subsidized Science Project Research): Grant number:2006–1 and 2010‐2. Grant sponsor: A grant from the Japanese Orthopaedics and Traumatology Foundation, Inc.; Grant number: 166. Grant sponsor: the 2012 Wakayama Medical Award for Young Researchers. Grant sponsor: Grant‐in‐Aid for the Promotion of joint International Research from Japan Society for the Promotion of Science; Grant number:15KK0316.
ACKNOWLEDGMENTS
The sponsors had no role in study design, data collection, data analysis, data interpretation, or in the writing of the report. The authors wish to thank Mrs. Tomoko Takijiri and other members of the Public Office in Hidakagawa Town, and Mrs. Tamako Tsutsumi, Mrs. Kanami Maeda, and other members of the Public Office in Taiji Town, for their assistance in locating and scheduling participants for examinations. The corresponding author had full access to all the data and had the final decision to submit for publication.
ETHICS APPROVAL AND INFORMED CONSENT
This study was performed in Hidakagawa Clinic and the center of Taijicho Tamokuteki Center, Wakayama, Japan. All participants provided written informed consent, and the study was conducted with the approval of ethical committees of the University of Tokyo and the Tokyo Metropolitan Institute of Gerontology (no.5).
DISCLOSURE (AUTHORS)
The authors declare no conflicts of interest.
DISCLOSURE BY AJIM EDITOR OF RECORD
Rodney Ehrlich declares that he has no conflict of interest in the review and publication decision regarding this article.
DISCLAIMER
None.
Ishimoto Y, Cooper C, Ntani G, et al. Factory and construction work is associated with an increased risk of severe lumbar spinal stenosis on MRI: A case control analysis within the wakayama spine study. Am J Ind Med. 2019;62:430–438. 10.1002/ajim.22957
Institution at which the work was performed: Wakayama Medical University.
REFERENCES
- 1. Lawrence JS. Rheumatism in coal miners. III. Occupational factors. Br J Ind Med. 1955; 12:249–261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Waldron HA, Cox M. Occupational arthropathy: evidence from the past. Br J Ind Med. 1989; 46:420–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Hadler NM, Gillings DB, Imbus HR, et al. Hand structure and function in an industrial setting. Arthritis Rheum. 1978; 21:210–220. [DOI] [PubMed] [Google Scholar]
- 4. Yoshimura N, Nishioka S, Kinoshita H, et al. Risk factors for knee osteoarthritis in Japanese women: heavy weight, previous joint injuries, and occupational activities. J Rheumatol. 2004; 31:157–162. [PubMed] [Google Scholar]
- 5. Jensen LK. Hip osteoarthritis: influence of work with heavy lifting, climbing stairs or ladders, or combining kneeling/squatting with heavy lifting. Occup Environ Med. 2008; 65:6–19. [DOI] [PubMed] [Google Scholar]
- 6. Croft P, Coggon D, Cruddas M, et al. Osteoarthritis of the hip: an occupational disease in farmers. BMJ. 1992; 304:1269–1272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Johansson H, Vala CH, Odén A, et al. Low risk for hip fracture and high risk for hip arthroplasty due to osteoarthritis among Swedish farmers. Osteoporos Int. 2018; 29:741–749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Muraki S, Akune T, Oka H, et al. Association of occupational activity with radiographic knee osteoarthritis and lumbar spondylosis in elderly patients of population‐based cohorts: a large‐scale population‐based study. Arthritis Rheum. 2009; 61:779–786. [DOI] [PubMed] [Google Scholar]
- 9. O'Reilly SC, Muir KR, Doherty M. Occupation and knee pain: a community study. Osteoarthr Cartil. 2000; 8:78–81. [DOI] [PubMed] [Google Scholar]
- 10. Yoshimura N, Kinoshita H, Hori N, et al. Risk factors for knee osteoarthritis in Japanese men: a case‐control study. Mod Rheumatol. 2006; 16:24–29. [DOI] [PubMed] [Google Scholar]
- 11. Riihimäki H, Wickström G, Hänninen K, Mattsson T, Waris P, Zitting A. Radiographically detectable lumbar degenerative changes as risk indicators of back pain. A cross‐sectional epidemiologic study of concrete reinforcement workers and house painters. Scand J Work Environ Health. 1989; 15:280–285. [DOI] [PubMed] [Google Scholar]
- 12. Kuh DJ, Coggon D, Mann S, et al. Height, occupation and back pain in a national prospective study. Br J Rheumatol. 1993; 32:911–916. [DOI] [PubMed] [Google Scholar]
- 13. Coggon D, Ntani G, Walker‐Bone K, et al. Epidemiological differences between localised and non‐localised low back pain. Spine (PhilaPa 1976). 2016; 42:1. [Google Scholar]
- 14. Yang S, Kim W, Choi KH, et al. Influence of occupation on lumbar spine degeneration in men: the Korean National Health and Nutrition Examination Survey 2010–2013. Int Arch Occup Environ Health. 2016; 89:1321–1328. [DOI] [PubMed] [Google Scholar]
- 15. Jang T‐W, Ahn Y‐S, Byun J, et al. Lumbar intervertebral disc degeneration and related factors in Korean firefighters. BMJ Open. 2016; 6:e011587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Hangai M, Kaneoka K, Kuno S, et al. Factors associated with lumbar intervertebral disc degeneration in the elderly. Spine J. 2008; 8:732–740. [DOI] [PubMed] [Google Scholar]
- 17. Katz JN, Harris MB. Clinical practice. Lumbar spinal stenosis. N Engl J Med. 2008; 358:818–825. [DOI] [PubMed] [Google Scholar]
- 18. Suri P, Rainville J, Kalichman L, et al. Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis? JAMA. 2010; 304:2628–2636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Deyo RA, Mirza SK, Martin BI, et al. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010; 303:1259–1265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Ciol MA, Deyo RA, Howell E, et al. An assessment of surgery for spinal stenosis: time trends, geographic variations, complications, and reoperations. J Am Geriatr Soc. 1996; 44:285–290. [DOI] [PubMed] [Google Scholar]
- 21. Bischoff RJ, Rodriguez RP, Gupta K, et al. A comparison of computed tomography‐myelography, magnetic resonance imaging, and myelography in the diagnosis of herniated nucleus pulposus and spinal stenosis. J Spinal Disord. 1993; 6:289–295. [DOI] [PubMed] [Google Scholar]
- 22. Jia LS, Shi ZR. MRI and myelography in the diagnosis of lumbar canal stenosis and disc herniation. A comparative study. Chin Med J (Engl). 1991; 104:303–306. [PubMed] [Google Scholar]
- 23. Yoshimura N, Muraki S, Oka H, et al. Cohort profile: research on Osteoarthritis/Osteoporosis against disability study. Int J Epidemiol. 2010; 39:988–995. [DOI] [PubMed] [Google Scholar]
- 24. Ishimoto Y, Yoshimura N, Muraki S, et al. Prevalence of symptomatic lumbar spinal stenosis and its association with physical performance in a population‐based cohort in Japan: the Wakayama Spine Study. Osteoarthritis Cartilage. 2012; 20:1103–1108. [DOI] [PubMed] [Google Scholar]
- 25. Steurer J, Roner S, Gnannt R, Hodler J; LumbSten Research Collaboration. Quantitative radiologic criteria for the diagnosis of lumbar spinal stenosis: a systematic literature review. BMC Musculoskelet Disord. 2011; 12:175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hughes A, Makirov SK, Osadchiy V. Measuring spinal canal size in lumbar spinal stenosis: description of method and preliminary results. Int J Spine Surg. 2015; 9:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Gendell M. Trends in retirement age in four countries, 1965–1995. Mon Labor Rev. 1998; 121:20–30. [Google Scholar]
- 28. Harris EC, Coggon D. HIP osteoarthritis and work. Best Pract Res Clin Rheumatol. 2015; 29:462–482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Martin KR, Kuh D, Harris TB, et al. Body mass index, occupational activity, and leisure‐time physical activity: an exploration of risk factors and modifiers for knee osteoarthritis in the 1946 British birth cohort. BMC Musculoskelet Disord. 2013; 14:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Mahbub H, Laskar S, Seikh F, et al. Prevalence of cervical spondylosis and musculoskeletal symptoms among coolies in a city of bangladesh prevalence of cervical spondylosis and musculoskeletal symptoms among coolies in a city of Bangladesh. J Occup Health. 2006; 48:69–73. [DOI] [PubMed] [Google Scholar]
- 31. Vanharanta H, Heliovaara M, Korpi J, et al. Occupation, work load and the size and shape of lumbar vertebral canals. Scand J Work Environ Heal. 1987; 13:146–149. [DOI] [PubMed] [Google Scholar]
- 32. Leino‐Arjas P, Kaila‐Kangas L, Notkola V, et al. Inpatient hospital care for back disorders in relation to industry and occupation in Finland. Scand J Work Environ Heal. 2002; 28:304–313. [DOI] [PubMed] [Google Scholar]
- 33. Mariconda M, Galasso O, Imbimbo L, et al. Relationship between alterations of the lumbar spine, visualized with magnetic resonance imaging, and occupational variables. Eur Spine J. 2007; 16:255–266. [DOI] [PMC free article] [PubMed] [Google Scholar]