

Abstract
Background & Objectives:
Refractive Errors (RE) are responsible for major portion of the treatable visual impairment and avoidable blindness in the world. The prevalence of RE varies with age, gender, ethnicity, geographical locations and also from time to time due to progresse in eye care services. We aimed to study the prevalence of RE and assess their patterns among Saudi adults of Arar city, the capital of Northern Border Region of Saudi Arabia.
Methods:
This is a cross-sectional, population-based study. A total number of 966 Saudi adults aged 16 to 39 years were enrolled. The patterns of their RE were studied through auto-refraction evaluation.
Results:
The prevalence of RE was 45.8%. The most frequent type of RE was myopia in 24.4%, followed by hyperopia 11.9% and astigmatism in 9.5% cases. Ages and genders significantly affect the prevalence of the different patterns of RE (0.033 and 0.012, respectively).
Conclusion:
The prevalence of RE in Arar city is slightly lower than that previously published in the same targeted age group. Myopia is the main RE. More awareness programs, especially among young adults are recommended for better outcomes.
Keywords: Ametropia, Astigmatism, Emmetropia, Hyperopia, Myopia, Refractive error, Visual impairment
Abbreviations: RE: Refractive Error, SE: Spherical Equivalent, VA: Visual Acuity, VI: Visual Impairment
INTRODUCTION
When the parallel rays of light coming from infinity are focused on the retina with the accommodation of the eye at rest it indicates the normal refractive status of the eye called as emmetropia. An emmetropic eye will therefore make a clear image of the distant object without any internal adjustment of its optics. If the rays of light with accommodation of the eye at rest are not focused exactly on the retina the condition indicates an error of refraction, which is referred to as ametropia.1 Refractive error (RE) is classified into myopia, hyperopia and astigmatism. In myopia with accommodation relaxed, light rays from an object at infinity are focused in front of retina and in hyperopia behind the retina while as in astigmatism the light rays do not focus at a single point because of variations in the curvature of the cornea or lens at different meridians.2
RE can be treated by optical methods like corrective glasses and contact lenses or surgical methods like LASIK (laser-assisted in situ keratomileusis) or PRK (photorefractive keratectomy).
Lack of knowledge and awareness about RE3, non-recognition of the problem at personal or family level, as well as at community and public health level; economic and social barriers and availability and affordability of eye health services are the main reasons for RE to remain uncorrected.4,5 RE have serious impact on economy of many countries of the world.6,7 Many studies conducted abroad indicate that the prevalence of RE exhibits significant variation across geographic, racial, age, gender and ethnic boundaries, which has an enormous impact on the strategies utilized in addressing the problem of RE.8,9 This is more likely in people living in countries with limited resources and poor access to the eye care services. Studies conducted in some parts of Saudi Arabia indicate that RE are among the leading causes of VI.10-12 In Saudi Arabia, RE were studied considering either mainly the pediatric population13-16 or particular population groups like students undergoing higher education.17
Although a large number of studies pertaining to RE have been conducted in many parts of the world, the comparison of the data remains difficult owing to lack of consistency in methods and definitions used for identifying and measuring RE. However, prevalence and patterns of RE in Arar city have not been studied yet. The data from the current study shall fill the gap to evaluate the current state of the problem in Arar city with better guidelines for the future strategies to overcome the burden of RE.
METHODS
This cross-sectional, population-based study was conducted from January 1st, 2018 to September 1st, 2018. A sample from the general population was randomly collected at screening camps held in the main shopping mall of Arar city where a temporary eye clinic was installed for three consecutive days. Persons with any previous history of refractive surgery were excluded from this study. The participants were further evaluated at the Central Hospital of Arar city. Visual Acuity (VA) was tested on VA Auto Chart Projector (TOPCON ACP-8; Japan) and refraction without cyloplegia was performed on auto-refractor (Topcon KR-8900; Japan).
The RE was classified using the Spherical equivalent (SE), which is the sum of the value of the sphere and half of the cylindrical value.18 Emmetropia was attributed to SE between -0.50 D and +0.50 D, myopia to SE ≤ -0.50 D, hyperopia to SE ≥ +0.50D and astigmatism to any cylindrical error of at least 0.5 D without reference to the axis. Myopia was further categorized as low (≥ −0.50 D and < −3.00 D), moderate (≥ −3.00 D and < −6.00 D) and high (≥ −6.00 D). Hyperopia was further categorized as low to moderate (≥ +0.50 D and < +3.00 D) and high (≥ +3.0 D) hyperopia. Astigmatism was further categorized as low to moderate (cylinder error of ≥ 0.50 D and < 3.00 D) and high (≥ 3.00 D) astigmatism. Simple myopic astigmatism was defined as plano sphere (<−0.5 D to < +0.5 D) and cylinder of ≥ −0.50 D, simple hyperopic astigmatism was defined as plano sphere (< −0.5 D to < +0.5 D) and cylinder of ≥ +0.50 D); compound myopic astigmatism was defined as sphere of ≥ −0.5 D and cylinder of ≥ −0.50 D, compound hyperopic astigmatism was defined as sphere of ≥ +0.5 D and cylinder of ≥ +0.50 D. Astigmatism was defined as mixed if the sphere was positive (> +0.5 D) and cylinder value was negative (> −0.50 D) or vice versa and the cylinder value was greater than a sphere.
Data Analysis
Data was revised, coded, entered, tabulated, and analyzed using SPSS version 20. Chisquare was used to study the significance of association. Statistical significance was kept constant at P<0.05.
This study was approved by the ethical committee of Deanship of Scientific Research, Northern Border University. Informed written consent was obtained from all participants involved in this study. Financial or any other compensations were not offered to any of the participants.
RESULTS
A total of 966 Saudi adults were enrolled in the current study [485 females (48.7%) and 481 males (51.3%)]. The mean age of the studied population was 27.48 (± 6.32) years with a range of 16-39 years old. The prevalence of RE was estimated to be 45.8%. The commonest type of RE was myopia (SE ≤-0.5D) in 24.4% followed by hyperopia (SE≥0.5D) in 11.9% and simple astigmatism (with SE between 0.5D and -0.5D) in 9.5% cases (Figure 1).
Fig.1.
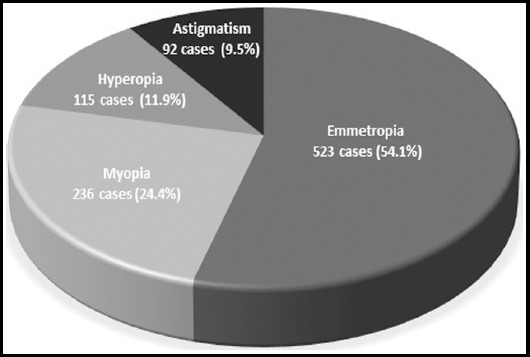
Refractive error among the studied population. Emmetropia was attributed to SE between -0.50D and +0.50D, myopia to SE ≤ -0.50D, hyperopia to SE ≥ +0.50D and astigmatism to any cylindrical error of ≤ -0.50D or ≥ +0.50D with SE in the emmetropia range without reference to the axis.
Regarding the genders of participants, there was a significant difference between the males and females in prevalence of RE (Table-I). Pertaining to the age (Table-II), myopia was found to be slightly more common in age group ≥ 25, while as hyperopia in >25 (p= 0.033). Grading of RE severity in the studied population is shown in Table-III. Cases with astigmatism were classified according to their SE (Table-I and II) and the commonest type was found to be the compound myopic astigmatism.
Table-I.
Pattern of refractive error in relation to gender.
| Type of refractive error | Total | Females | Males | P-value |
|---|---|---|---|---|
| Emmetropia | 523 (54.1%) | 240 (24.8%) | 283 (29.3%) | 0.0123* 17.93, 7 |
| Myopia | 67 (6.9) | 42 (4.3%) | 25 (2.6%) | |
| Hyperopia | 31 (3.2%) | 16 (1.7%) | 15 (1.6%) | |
| Simple myopic astigmatism | 76 (7.9%) | 32 (3.3%) | 44 (4.6%) | |
| Simple hyperopic astigmatism | 16 (1.7%) | 9 (0.9%) | 7 (0.7%) | |
| Compound myopic astigmatism | 166 (17.2%) | 101 (10.5%) | 65 (6.7%) | |
| Compound hyperopic astigmatism | 8 (0.8%) | 4 (0.4%) | 4 (0.4%) | |
| Mixed astigmatism | 79 (8.2%) | 41 (4.2%) | 38 (3.9%) | |
| Totals | 966 (100%) | 485 (50.2%) | 481 (49.8%) | |
Table-II.
Pattern of refractive errors in relation to age groups.
| Type of refractive error | Total | ≥25 yrs. | >25 yrs. | P-value |
|---|---|---|---|---|
| Emmetropia | 523 (54.1%) | 293 (30.3%) | 228 (23.6%) | 0.033* 15.17 , 7 |
| Myopia | 67 (6.9) | 37 (3.8%) | 30 (3.1%) | |
| Hyperopia | 31 (3.2%) | 11 (1.1%) | 20 (2%) | |
| Simple myopic astigmatism | 76 (7.9%) | 34 (3.5%) | 32 (3.3%) | |
| Simple hyperopic astigmatism | 16 (1.7%) | 7 (0.7%) | 9 (0.9%) | |
| Compound myopic astigmatism | 166 (17.2%) | 76 (7.9%) | 90 (9.3%) | |
| Compound hyperopic astigmatism | 8 (0.8%) | 3 (0.3%) | 5 (0.5%) | |
| Mixed astigmatism | 79 (8.2%) | 33 (3.4%) | 46 (4.8%) | |
| Totals | 966 (100%) | 485 (50.2%) | 481 (49.8%) | |
Table-III.
Severity of refractive errors in relation to gender and age groups.
| RE | Severity | Totals | Females | Males | P-value | ≥25 yrs. | >25 yrs. | P-value |
|---|---|---|---|---|---|---|---|---|
| Myopia | Mild | 162(68.5%) | 132(55.9%) | 30(12.7%) | <0.0001 | 77 (32.6%) | 85(35.9%) | 0.0003 |
| Moderate | 60 (25.4%) | 15 (6.3%) | 45 (19.1%) | 46 (19.5%) | 14(5.9%) | |||
| Severe | 16 (6.7%) | 12 (5%) | 4 (1.7%) | 11 (4.6%) | 5 (2.1%) | |||
| Totals | 236 (100%) | 159(64.4%) | 77 (35.6%) | 134(56.8%) | 102(43.2%) | |||
| Hyperopia | Low to moderate | 93 (79.9%) | 48 (41.3%) | 45 (38.6%) | 1 | 31 (29.6%) | 62 (50.3%) | 1 |
| High | 22 (19.1%) | 11 (9.5%) | 11(9.5%) | 7 (6.1%) | 15 (13%) | |||
| Totals | 115 (100%) | 59 (51.3%) | 56 (48.7%) | 38 (33%) | 77(67%) | |||
| Astigmatism | Low to moderate | 324 (94%) | 147(42.6%) | 177(57.4%) | 0.652 | 175(50.7%) | 139(49.3%) | 0.068 |
| High | 21 (6%) | 11 (3.2%) | 10 (2.8%) | 7 (2%) | 14 (4%) | |||
| Totals | 345 (100%) | 158(45.8%) | 187(54.2%) | 182(52.8%) | 153(47.2%) |
Cases with SE≤-0.5D were classified according to the cylindrical correction to simple myopia (cylinder>-0.5D and <0.5D), compound myopic stigmatism (cylindrical correction≤-0.5D) and mixed myopic stigmatism (cylindrical correction≥0.5D) (Table-IV).Cases with SE≥0.5D were classified according to the cylindrical correction to simple hyperopia (cylinder>-0.5D and <0.5D), compound hyperopic stigmatism (cylinder≥0.5D) and mixed hyperopic stigmatism (cylinder≤-0.5D) (Table-V).
Table-IV.
Classification of cases with SE≤-0.5D among the studied population.
| SE and cylindrical lenses | Number of cases |
|---|---|
| Simple myopia (cylinder>-0.5D and <0.5D) | 67 (28.4%) |
| Compound myopic stigmatism (cylinder≤-0.5D) | 166 (70.3%) |
| Mixed myopic stigmatism (cylinder≥0.5D) | 3 (1.3%) |
| Total | 236 (100%) |
Table-V.
Classification of cases with SE≥0.5D among the studied population.
| SE and cylindrical lenses | Number of cases |
|---|---|
| Simple hyperopia (cylinder>-0.5D and <0.5D) | 31 (26.9%) |
| Compound hyperopic stigmatism (cylinder≥0.5D) | 8 (6.9%) |
| Mixed hyperopic stigmatism (cylinder≤-0.5D) | 76 (66%) |
| Total | 115 (100%) |
DISCUSSION
This study has evaluated the patterns and prevalence of RE in Arar city. The prevalence of RE was estimated to be 45.8%. The commonest type of RE was myopia (SE ≤-0.5D) in 24.4% followed by hyperopia (SE≥0.5D) in 11.9% and simple astigmatism (with SE between 0.5D and -0.5D) in 9.5% cases. Both genders and age groups of participants showed significant effect on patterns and prevalence of the different RE types.
No definite published data regarding the prevalence of RE is avaliable in Saudi Arabia. The published data were based only on school children and adolescents.19 The prevalence of RE in Saudi adults of Arar city is 45.8% which is lower than the prevalence of RE (72.2%) among female students of Medicine and Pharmacy Schools in Quassin University as reported by Albatanony.20 Another study from Quassim estimated the prevalence of RE as 58.6% among the male medical students of Qassim University.17 This higher prevalnce may be due to faulty abuse of vision during prolonged hours of studying among the medical students Kumar et al.,21 and Basu et al., 22 In an another study conducted in Riyadh19, the prevealence of RE among adolescents (12-20 years) was estimated to be 55.5% which is also higher than the present prevelence. In the nearby country Jordan, the prevalence of RE among adult population aged (17-40 years) was estimated to be around 60% (Mallen et al, 2005).23 Internationally, the prevalence in USA was reported to be around 72% in civilain population aged above 12 years (Vitale et al., 2008).24 This higher prevalence in USA may be due to the elderly age group (above 40 years) in their study.
In the current study myopia was the commonest type of RE. This is in accordance with some recent studies conducted in KSA17,19 and abroad.25,26 In Europe the greatest burden of RE is due to myopia.27 While other data showed higher prevalence of astigmatism.28,29 Higher prevalence of hyperopia is usually seen in studies targeting elder age groups than our study age range.27,30 However, all these differences regarding the prevalence of the different patterns of RE may be related to the difference in the studied populations, methods of study and ages of the studied groups.
As regards the effect of age on the patterns of RE, our data showed that myopia was more prevalent among participants aged <25 years, while hyperopia was more dominant in the elderly participants. This is in line with the previously published data.17,25-27,30
Regarding gender the current results had found that myopia was more common in females. This is in accordance with the other studies as Katz et al. (1997)31 and Czepita et al. (2007).32
CONCLUSION
To the best of our knowledge, this is the first research focused on RE of Saudi adult population to evaluate the current state of health service and to plan properly according to our results for better control of the problem in Northern Border Region. The vital epidemiological data on prevalence and patterns of RE from this study are important for planning and improvement of screening and rehabilitation programs for better outcomes of the cases of refractive errors in Arar.
Acknowledgements
We express gratitude to the Deanship of Scientific Research, Northern Border University for supporting this project.
Footnotes
Grant Support & Financial Disclosures: This study was funded by Deanship of Scientific Research, Northern Border University.
Author’s Contribution
MURP, EE: Conception, design and/or analysis and interpretation of data and Drafting the article or revising it critically for important intellectual content and final approval of the version to be published.
REFERENCES
- 1.Khurana AK. Theory and Practice of Optics and Refraction. 2ndedition. Reed Elsevier India Pvt. Ltd; 2008. pp. 61–62. [Google Scholar]
- 2.Liesegang TJ, Gregory LS, Cantor LB. Basic and Clinical Science Course- Am Acad Ophthalmol. San Francisco: 2007. [Google Scholar]
- 3.Rosman M, Wong TY, Wong W, Wong ML, Saw SM. Knowledge and beliefs associated with refractive errors and undercorrection:the Singapore Malay Eye Study. Br J Ophthalmol. 2009;93(1):4–10. doi: 10.1136/bjo.2007.132506. doi:10.1136/bjo.2007.132506. [DOI] [PubMed] [Google Scholar]
- 4.Resnikoff S, Donatella P, Silvio PM, Gopal PP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bulletin of the World Health Organization. 2008;86:63–70. doi: 10.2471/BLT.07.041210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jeganathan VSERobin AL, Woodward MA. Refractive error in underserved adults:causes and potential solutions. Curr Opin Ophthalmol. 2017;28(4):299–304. doi: 10.1097/ICU.0000000000000376. doi:10.1097/ICU.0000000000000376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fricke TR, Holden BA, Wilson DA, Schlenther G, Naidoo KS, Resnikoff S, et al. Global cost of correcting vision impairment from uncorrected refractive error. Bull World Health Organ. 2012;90(10):728–738. doi: 10.2471/BLT.12.104034. doi:10.2471/BLT.12.104034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Smith TS, Frick KD, Holden BA, Fricke TR, Naidoo KS. Potential lost productivity resulting from the global burden of uncorrected refractive error. Bull World Health Organ. 2009;87(6):431e–437. doi: 10.2471/BLT.08.055673. doi:10.2471/BLT.08.055673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhao J, Pan X, Sui R, Munor SR, Spertudo RD, Ellwein LB. Refractive error study in children:Results from Shunyi District, China. Am J Ophthalmol. 2000;129:427–435. doi: 10.1016/s0002-9394(99)00452-3. [DOI] [PubMed] [Google Scholar]
- 9.Naidoo KS, Holden B, Sweeney D, Colvin M. Design of a blindness prevention reporting and planning tool utilising the results of a population based study of visual impairment in a health district in Kwazulu-Natal. Invest Ophthalmol Vis Sci. 2007;48(13):327. [Google Scholar]
- 10.Al-Shaaln FF, Bakrman MA, Ibrahim AM, Aljoudi AS. Prevalence and causes of visual impairment among Saudi adults attending primary health care centers in northern Saudi Arabia. Ann Saudi Med. 2011;31(5):473–480. doi: 10.4103/0256-4947.84624. doi:10.4103/0256-4947.84624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Parrey MU, Alswelmi FK. Prevalence and causes of visual impairment among Saudi adults. Pak J Med Sci. 2017;33(1):167–171. doi: 10.12669/pjms.331.11871. doi:10.12669/pjms.331.11871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tabbara KF, El-Sheikh HF, Shawaf SS. Pattern of childhood blindness at a referral center in Saudi Arabia. Ann Saudi Med. 2005;25(1):18–21. doi: 10.5144/0256-4947.2005.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Alrahili NHR, Jadidy ES, Alahmadi BSH, Abdula'al MF, Jadidy AS, Alhusaini A, et al. Prevalence of uncorrected refractive errors among children aged 3-10 years in western Saudi Arabia. Saudi Med J. 2017;38(8):804–810. doi: 10.15537/smj.2017.8.20412. doi:10.15537/smj.2017.8.20412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Al Wadaani FA, Amin TT, Ali A, Khan AR. Prevalence and pattern of refractive errors among primary school children in Al Hassa, Saudi Arabia. Glob J Health Sci. 2012;5(1):125–34. doi: 10.5539/gjhs.v5n1p125. doi:10.5539/gjhs.v5n1p125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Al-Rowaily MA. Prevalence of refractive errors among pre-school children at King Abdulaziz Medical City, Riyadh, Saudi Arabia. Saudi J Ophthalmol. 2010;24(2):45–48. doi: 10.1016/j.sjopt.2010.01.001. doi:10.1016/j.sjopt.2010.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Al-Tamimi ER, Shakeel A, Yassin SA, Ali SI, Khan UA. A clinic-based study of refractive errors, strabismus, and amblyopia in pediatric age-group. J Family Community Med. 2015;22(3):158–162. doi: 10.4103/2230-8229.163031. doi:10.4103/2230-8229.163031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Al-Rashidi SH, Albahouth AA, Althwini WA, Alsohibani AA, Alnughaymishi AA, Alsaeed AA, et al. Prevalence Refractive Errors among Medical Students of Qassim University, Saudi Arabia:Cross-Sectional Descriptive Study. Open Access Maced J Med Sci. 201819;6(5):940–943. doi: 10.3889/oamjms.2018.197. doi:10.3889/oamjms.2018.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Althomali TA. Relative Proportion of Different Types of Refractive Errors In Subjects Seeking Laser Vision Correction. Open Ophthalmol J. 2018;12:53–62. doi: 10.2174/1874364101812010053. doi:10.2174/1874364101812010053. eCollection 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Alsaqr A, Abu Sharha A, Fagehi R, Almutairi A, Alosaimi S, Almalki A, et al. The visual status of adolescents in Riyadh, Saudi Arabia:a population study. Clin Ophthalmol. 2018;12:965–972. doi: 10.2147/OPTH.S162319. Published online 2018 May 22. doi:10.2147/OPTH.S162319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Batanony MA. Refractive Errors among Saudi Medical and Pharmacy Female Students:A Questionnaire Survey Study. J Adv Med Pharmac Sci. 2016;7(1):1–8. Article no.JAMPS.24633. [Google Scholar]
- 21.Kumar N, Jangra B, Jangra MS, Pawar N. Risk factors associated with refractive error among medical students. Int J Community Med Public Health. 2018;5(2):634–638. doi:10.18203/2394-6040.ijcmph20170241. [Google Scholar]
- 22.Basu M, Ray S, Mazumdar M, Gupta AK, Sengupta P, Chatterjee S. Refractive Errors and its Determinants among Medical Students of Kolkata:A Descriptive Study. Int J Prev Pub Health Sci. 2016;2(1) doi:10.17354/ijpphs/2016/20. [Google Scholar]
- 23.Mallen EA, Gammoh Y, Al-Bdour M, Sayegh FN. Refractive error and ocular biometry in Jordanian adults. Ophthalmic Physiol Opt. 2005;25(4):302–309. doi: 10.1111/j.1475-1313.2005.00306.x. [DOI] [PubMed] [Google Scholar]
- 24.Vitale S, Ellwein L, Cotch MF, Ferris FL, 3rd, Sperduto R. Prevalence of refractive error in the United States, 1999-2004. Arch Ophthalmol. 2008;126(8):1111–1119. doi: 10.1001/archopht.126.8.1111. doi:10.1001/archopht.126.8.1111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Foster PJ, Jiang Y. Epidemiology of myopia. Eye (Lond) 2014;28(2):202–208. doi: 10.1038/eye.2013.280. doi:10.1038/eye.2013.280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gomez-Salazar F, Campos-Romero A, Gomez-Campana H, Cruz-Zamudio C, Chaidez-Felix M, Leon-Sicairos N, et al. Refractive errors among children, adolescents and adults attending eye clinics in Mexico. Int J Ophthalmol. 2017;10(5):796–802. doi: 10.18240/ijo.2017.05.23. doi:10.18240/ijo.2017.05.23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Williams KM, Verhoeven VJ, Cumberland P, Bertelsen G, Wolfram C, Buitendijk GH, et al. Prevalence of refractive error in Europe:the European Eye Epidemiology (E(3)) Consortium. Eur J Epidemiol. 2015;30(4):305–315. doi: 10.1007/s10654-015-0010-0. doi:10.1007/s10654-015-0010-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Prema R, George R, Sathyamangalam Ve R, Hemamalini A, Baskaran M, Kumaramanickavel G, Catherine M, et al. Comparison of refractive errors and factors associated with spectacle use in a rural and urban South Indian Population. Indian J Ophthalmol. 2008;56(2):139–144. doi: 10.4103/0301-4738.39119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ferraz FH, Corrente JE, Opromolla P, Padovani CR, Schellini SA. Refractive errors in a Brazilian population:age and sex distribution. Ophthalmic Physiol Opt. 2015;35(1):19–27. doi: 10.1111/opo.12164. doi:10.1111/opo.12164. [DOI] [PubMed] [Google Scholar]
- 30.Pan CW, Wong TY, Lavanya R, Wu RY, Zheng YF, Lin XY, et al. Prevalence and risk factors for refractive errors in Indians:the Singapore Indian Eye Study (SINDI) Invest Ophthalmol Vis Sci. 2011;52(6):3166–3173. doi: 10.1167/iovs.10-6210. doi:10.1167/iovs.10-6210. [DOI] [PubMed] [Google Scholar]
- 31.Katz J, Tielsch JM, Sommer A. Prevalence and risk factors for refractive errors in an adult inner city population. Invest Ophthalmol Vis Sci. 1997;38(2):334–340. [PubMed] [Google Scholar]
- 32.Czepita D, Mojsa A, Ustianowska M, Czepita M, Lachowicz E. Role of gender in the occurrence of refractive errors. Ann Acad Med Stetin. 2007;53(2):5–7. [PubMed] [Google Scholar]