

Abstract
About 10% of the parents reported that their children are allergic to one drug and the betalactam antibiotics are the most frequently suspected. Even if most of the adverse events following antibiotic prescriptions to children are considered allergic, after a full allergy work-up only a few of the suspected reactions are confirmed. For this reason, many children are incorrectly labelled as “allergic” and this represents an important challenge for the choice of the antibiotic therapy in these “labelled” children, who are frequently improperly deprived of narrow-spectrum antibiotics because considered as allergic. When an allergic reaction is suspected a precise diagnosis and a choice of a safe and effective alternative is essential for the future antibiotic option. In the light of this, the main aim of this paper is to try to provide a practical approach to managing the individuals who have reported adverse reactions to antibiotics. (www.actabiomedica.it)
Keywords: antibiotic allergy, betalactam, drug adverse reaction, hypersensitivity reactions, children, skin test, specific IgE, basophil activation test, drug provocation test
Introduction
Data on the prevalence and incidence of antibiotic hypersensitivity reactions (DHRs) are limited, especially in paediatric age and varies around the world (1).
About 10% of the parents reported that their children are allergic to drugs and betalactams (BLs) are the most frequently suspected (2). A prospective study conducted in children and adolescents showed that the rate of adverse drug reactions (ADR) was 10.9% in hospitalized children, 1% in outpatients, and the hospitalizations rate for adverse drug reactions was 1.8% (3). Antibiotics are significantly overused (4) and all classes can be associated with a certain predictable rate of adverse reactions (1). Nowadays, multiple drug-resistant infections are becoming more common (1). Thus, an effective antibiotic stewardship program is important and urgent (5). So, physicians, should be correctly informed on the risks of avoiding certain classes of antibiotics, like narrow-spectrum penicillins, when these are the drugs of choice (1). Physicians should be able to safely and efficiently evaluate and/or refer individuals with reported antibiotic adverse reaction and know when to perform diagnostic testing, drug challenge, or desensitization (6).
Many children are incorrectly labelled as “allergic” (1). The choice of antibiotic therapy in such children represents an important challenge (7). They commonly receive second-line broad spectrum antibiotics and this increases the risk for infection caused by Clostridium difficile, methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococcus (8). Furthermore, these patients have a prolonged hospital stay, and adverse effects related to second-line antibiotic use (8). This may lead to increase health-care utilization and costs (8,9). Li et al. showed that penicillin allergy was associated with 1.82- to 2.58-fold increase in total antibiotic cost (10).
This review aimed to provide a practical approach in managing the clinical care of individuals who have reported an adverse reaction to antibiotics.
Practical management
Step 1. Make a correct diagnosis
A key point for the management of antibiotic allergy is to establish a correct diagnosis (11).
The first step is to consider that ADRs are classified as type A (predictable by the properties of the drug, and including the toxic side effects, which are dose-dependent and non-immune-mediated) and type B reactions which are unpredictable, not dose-dependent and frequently immune-mediated (11-13). Type B reactions comprise both quick-onset reactions, such as anaphylaxis, bronchospasm, urticaria, angioedema, gastro-intestinal symptoms and late-onset reactions, such as maculopapular exanthema, contact eczema and severe cutaneous adverse reactions (SCARs) including drug reaction with eosinophilia and systemic symptoms (DRESS), Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN) (11-13). Antibiotics trigger type B reactions that should be differentiated from signs/symptoms due to an infectious disease, simultaneously administered drugs, food and airborne allergens, or functional mechanisms (14-21).
In adults, most of ADRs (about 80%) are type A reactions, while type B reactions comprise about 10%-–15% of all ADRs (13), while in children, the opposite is true (22). Immunological reactions were classified by Gell and Coombs (types I-IV) and later by Pichler who refined type IV (T-cell-mediated) in type IVa (Monocytic inflammation), IVb (Eosinophilic inflammation), IVc (T cells) and IVd (Neutrophilic inflammation) (23).
Most of the adverse events following antibiotic prescriptions are considered as allergic, but after a full allergic work-up only a few of the suspected reactions can be confirmed (2, 7, 11, 24). Ponvert et al. (25) in their twenty years’ experience, found that only 15.9% of 1431 children with suspected allergy to BLs antibiotics were found to be allergic. Caubet et al. (14) showed that the most frequent cause of a benign skin rush during BLs treatment in children, was a viral infection (69.5%) while only 6.8% of children had a positive drug provocation test (DPT) to BLs. Similar results were found by Zambonino et al. (26) that found only 7.9% of 783 patients with suspected allergy to BLs had drug allergy.
A recent paper by Vyles D et al. (27) confirmed the importance of a precise classification and definition of a penicillin adverse reaction. They found that no children with suspected penicillin allergic reaction categorized as low-risk with their allergy questionnaire have a true penicillin allergy (27).
Many studies have showed that penicillin skin testing is useful in increasing BLs use (when indicated by the antibiotic stewardship), and in reducing the use of alternative antibiotics as fluoroquinolones, glycopeptides and other second-line broad spectrum agents, with consequent and relevant cost saving (8, 28, 29). So, many reports called for an incorporation antibiotic allergy-testing program in antimicrobial stewardship (30-32). Raja et al. (33) found that penicillin skin test is useful in adult emergency department for ruling out penicillin allergy. This strategy although useful, appears unfeasible in paediatric emergency department because it is time consuming and costly (27).
Recommendation. Not label a child as allergic to antibiotics without an accurate diagnostic work-up that starts with a precise description of the index reaction and his classification in Type A or Type B reaction.
Step 2: find a safe and effective alternative
Betalactams
BLs are the antibiotics that most frequently cause allergic reactions in childhood (2). The prevalence of self-reported reactions in children varies from 1.7% to 5.2% (7, 34). A study of 2,375,424 children and adults in Southern California showed that prevalence of allergy to penicillin was 7.9% (34). An European study show that the 0.21% of unselected paediatric outpatients demonstrate positive test for antibiotic allergy and 6.8% of children attending ED for suspected BLs hypersensitivity are allergic (35).
Penicillins are the first line therapy in most paediatric respiratory infections according to many guidelines (36-40). For these reasons when a correct diagnosis of penicillin allergy is done it should be given an alternative well tolerated but equally effective agent. It is important to consider that other classes of antibiotics have limited efficacy for these infection (39, 40). Many studies have found that the avoidance of cephalosporin in penicillin allergy patients causes an increased risk of adverse events, suboptimal treatment of infection and treatment failures (41, 42).
All BLs have a structure that consist in a 4-membered BL ring that in penicillins is attached to a 5-membered thiazolidine ring (44). The side chain distinguishes different penicillins (34, 43, 44). Cephalosporins have a 6-membered sulfur-containing dihydrothiazine ring and two side chains (R1 and R2) (44). Carbapenems (e.g. Imipenem, meropenem) in the 5-member thiazolidine ring contain a carbon double bound instead of sulphur and have a side chain that distinguishes the different carbapenems (44). Monobactams comprise the BL ring without an attached 5- or 6-membered sulphur ring (34, 43, 44) (Fig. 1).
Figure 1.
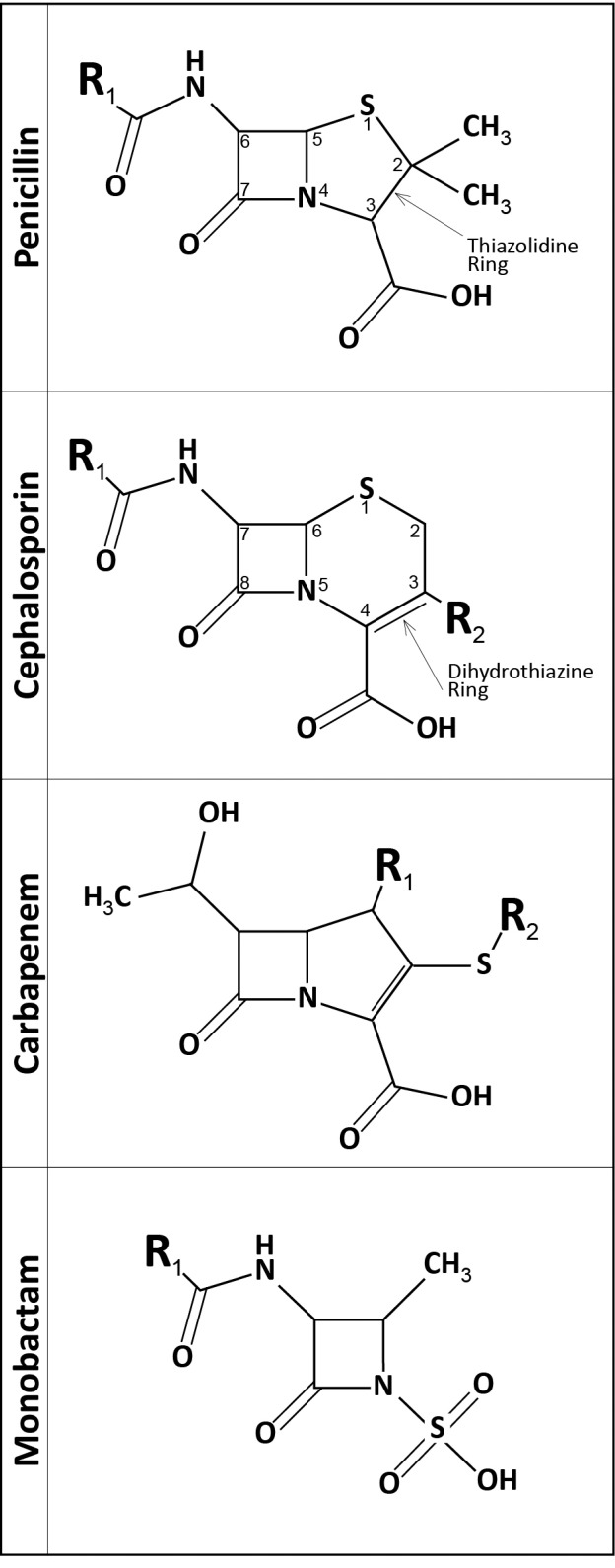
Betalactams chemical structures. “R” indicates side chains
The BL ring, the thiazolidine/ dihydrothiazine rings and the side chains are all potentially immunogenic (28, 38, 39). In the last ten years, the role of side-chain structures as antigenic determinants was widely accepted particularly in hypersensitivity reaction to amoxicillin and cephalosporin (28, 39, 45, 46). Cross-reactivity between BLs seems to be more closely related to side chain identity or similarity than to the central BL ring (34, 43, 44). However, shared epitopes from other parts of the molecule also account for cross-reactivity (34, 43, 44). For instance, ampicillin and cephalexin share an identical side chain with an amino group, as amoxicillin and cefadroxil (40) (Fig. 2). In early studies, cross-reactivity between penicillin and first and early (introduced before 1980) second-generation cephalosporins has been reported to occur in up to 10% of patients, while for the third-generation ones the rate is lower (2-3% of patients allergic to penicillin) (34, 44). Recent data indicate that the actual rate of cross-reactivity is probably less than 1% (43, 47). The degradation process of cephalosporin leads to a fragmentation of the BL ring as well as the thiazinic group but the R1 side-chain structure of cephalosporins usually remains intact and this is the main factor for cross reactivity between cephalosporins and penicillin (34, 43). The antigenic role of the R2 side-chain is still debated (43). Romano et al. demonstrated that patients with cephalosporin allergy commonly tolerated a cephalosporin with different R1/R2 side chain (48).
Figure 2.
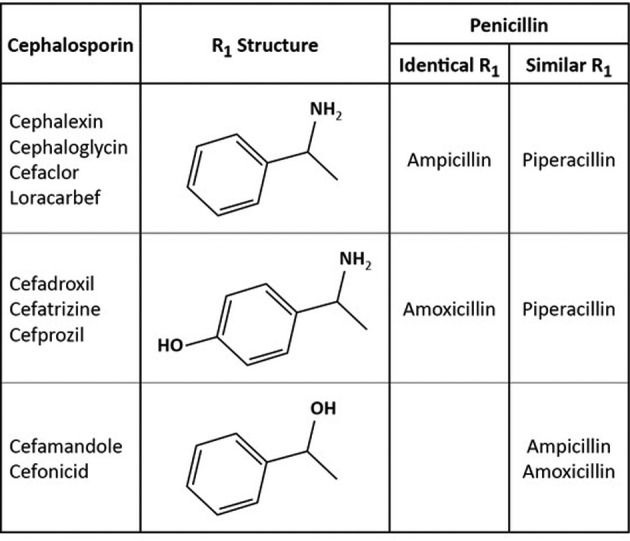
Penicillin and Cephalosporin side chains (R1): identical or similar structure. Modified by Zagursky RJ and, Pichichero ME (38).
Every patient reporting a suggestive history or who have a diagnosis of penicillin allergy may receive cephalosporins, especially the third generation, as a replacement, with the exception of those showing R1 side-chain similarity (34, 36, 43, 45, 47). It is still debated if in these occasions, a skin test should precede the administration of cephalosporin through a graded challenge (42). In figure 3 were listed many of the major drugs used nowadays and whether the R1 or R2 side chains are identical or similar.
Figure 3.

Comparison of penicllins and cephalosporins side chain. Bolded R1 or R2 (gray cell) indicate total identical R1/R2 side chain; regular R1 or R2 indicate only in part identical R1/R2 side chain; bolded r1 or r2 indicate total similar r1/r2 side chain; regular r1 or r2 indicate only in part similar r1/r2 side chain. Modified by Zagursky RJ and, Pichichero ME (38)
Prospective studies on carbapenems and monobactams suggest that cross reactivity with penicillins/cephalosporins is very unlikely or absent (34, 43, 44, 49), with the exception of ceftazidime which shares an identical R1 side chain with aztreonam (50).
Recommendations:
- Third generation cephalosporins can be used in patients with mild nonimmediate penicillin allergy. In case of SCARs, antibiotic class avoidance is the preferred management (11, 45).
- In patients with immediate reactions to penicillins who required cephalosporins, it is useful to perform skin tests with a cephalosporin of second or third generation with different side chains and if negative, administer the drug in a gradual and controlled challenge (34, 43-45, 47).
- In patients with immediate reactions to cephalosporins who required cephalosporin or penicillins, it is useful to perform skin tests with a cephalosporin or penicillins with different side chains and if negative, administer the drug in a gradual and controlled challenge (34, 43-45, 47).
- Subjects allergic to penicillin who required carbapenems or monobactams should undergo skin tests and when negative, the drug should be administered in a gradual and controlled challenge (11, 43-45, 51).
Non-betalactam antibiotics
The prevalence of allergic reactions to non-betalactam antibiotics (NBLs) is estimated to be 1-3% of the general population and represents about 10% of the DHRs in children (47). Viral infections can provoke skin eruptions such as maculopapular exanthemas that is also the most common symptom of allergic reactions to NBLs (51). Therefore, it is difficult to differentiate DHRs from skin symptoms due to infections (51). The main classes involved in NBLs DHRs in children are sulphonamides, macrolides, glycopeptides, aminoglycosides and quinolones (1, 52). There is a lack of studies on hypersensitivity reactions to NBLs (52).
Macrolides. Macrolides are classified according to the number of carbon atoms in their lactone ring: 14 membered (e.g. erythromycin, clarithromycin), 15 membered (azithromycin), and 16 membered (spiramycin, rokitamycin, josamycin) (52). Hypersensitivity reactions to macrolides occur in 0.4% to 3% of treatments (53). DHRs to azithromycin appear to be more frequent than to clarithromycin (54). Allergy to macrolides is difficult to diagnose because of poor standardization of skin tests as well as lack of accurate in vitro tests (1, 55). In a study by Mori at al. on sixty-four children with a history of hypersensitivity reactions to clarithromycin, the sensitivity and specificity of intradermal test (IDT) to clarithromycin at the concentration of 0.5 mg/ml were 75% and 90%, respectively (56). In children, few data are available on non-irritant concentrations, therefore the interpretation of a positive skin test result to macrolides is uncertain (1, 57). Thus, DPT is the only reliable diagnostic test (52, 55), even in the absence of any standardized protocol for macrolides. It should be taken into account that anaphylactic reactions can be induced by the systemic administration of allergens including drugs (51), and foods (58, 59) during challenge tests. So, challenges should be performed under medical surveillance by trained personnel and materials for treating anaphylaxis should be available (51).
It has been suggested that macrolide allergies are unlikely to be a class allergy (1, 60). However, cross reactivity may occur between different macrolides, at least regarding anaphylaxis (61).
Aminoglycosides. Aminoglycosides are classified in two groups: (A) streptidine group: e.g., streptomycin; (B) desoxystreptamine group: e.g. amikacin, gentamicin, tobramycin, neomycin (60). Aminoglycosides hypersensitivity is uncommon except for some risk groups such as patients with cystic fibrosis (52). Contact dermatitis from topical aminoglycosides is the most frequent clinical manifestation, since neomycin, gentamicin and tobramycin are widely used as cream, ointment, and eye or ear drops (60, 62). Anecdotal cases of positive skin prick test to tobramycin, gentamicin, and streptomycin (63) have been observed. However, in vivo tests are not validated for the diagnosis of immediate reactions to aminoglycosides (51). Patch tests with reading at 72 and 96 hours have been performed for the diagnosis of non-immediate reactions (64).
Cross-reactivity between aminoglycosides is common (50%) (1, 65), so aminoglycosides should be avoided in patients with a diagnosis of hypersensitivity (60).
Sulphonamides. Cotrimoxazole is frequently used for prophylaxis and eradication of opportunistic infection in serious diseases, such as AIDS or hematologic malignancies, and for community infections in same regions of the world (47).
Sulfonamides are most commonly associated with non-immediate manifestations, such as maculopapular rashes, and SCARs (66, 67). Among antibiotics, sulfonamides have the more frequent cause of benign rash and of SYS/TEN (1). Most allergic sulfonamide-associated adverse reactions appear to be T-cell-mediated (1). The rash rate is even higher in individuals with active untreated or acutely treated HIV infection with low CD4 T-cell counts (67).
The best management strategy in a patient with sulfonamide hypersensitivity is to use a different drug, but in some clinical settings, especially in patients with HIV infection or hematologic malignancies, where no equally effective alternative exists (52).
In case of mild or moderate non-immediate reactions (without mucosal signs or systemic symptoms) different strategies have been proposed (60). It is possible to continue cotrimoxazole administration at the same doses, to discontinue the drug over a few months, usually 6 months, and then cotrimoxazole can be resumed after a graded challenge or a “desensitization” protocol (47). A meta-analysis involving 268 adults with HIV infection and mild or moderate hypersensitivity reactions to cotrimoxazole found that the desensitization protocol was the most beneficial for preventing severe skin reactions, when it is performed after 6 months of drug discontinuation (68).
Glycopeptides. Vancomycin, a glycopeptide, has been often used in infections with BL resistant Gram-positive organisms or in BL allergic patients (52, 60).
The most common hypersensitivity reaction associated with vancomycin is the red man syndrome (RMS) (52, 60). Vancomycin causes a variety of DHRs; nonimmediate DHRs are more common than immediate one, with linear IgA bullous dermatosis being most frequent (69).
In patients with suggestive clinical history, positive immediate-reading IDTs (0.1 mg/ml or lower dilution) may identify immediate hypersensitivity reactions, and positive patch tests (at concentration of 0.005%) delayed hypersensitivity reactions (52).
Severe RMS can mimic IgE-mediated anaphylaxis and requires immediate diagnosis and management (60). In contrast to true allergic hypersensitivity reactions, slowing the infusion rate of vancomycin to 500 mg given over one hour usually reduces the chance of developing RMS (60). There are few studies regarding the effectiveness of antihistamines as premedication to prevent RMS (60).
Despite its chemical affinity, no cases of RMS and very few cases of allergic reactions were reported with teicoplanin (70) in children with previous reactions to vancomycin. However, when possible, an alternative drug should be used or a desensitization protocol should be performed (51).
Quinolones. Quinolones can be classified according to their generation: first (e.g. nalidixic acid), second (e.g. ciprofloxacin), third (levofloxacin), and fourth (1).
In Spain, quinolones are the third cause of confirmed DHR, after anti-inflammatory drugs and BLs, having an increase in incidence from 0.53% in 2005 to 5.96% in 2009 (71). A paediatric study on ciprofloxacin involving 16,184 patients ≤17 years, gave an estimated risk of 0.046 suspected DHRs every 100 patients (72). The rate of allergic and non-allergic anaphylaxis between immediate hypersensitivity reactions to quinolones are similar among different quinolones (52). Allergic reactions to quinolones can be immediate or delayed (73). Anaphylaxis and maculopapular exanthema are respectively the most frequent clinical entities (73).
Skin prick tests and IDTs are not recommended for the diagnosis of hypersensitivity to quinolones because they can induce direct mast cells activation, leading to false positive results (1, 73). DPT remains the reference standard for the diagnosis even if not without risk (1, 52, 73). Cross-reactivity between quinolones is difficult to predict due to the small number of patients included in the few published studies (73). Some studies in adults showed that the level of cross-reactivity can be important (52, 73). Patients with hypersensitivity to quinolones should avoid these drugs and when quinolones are the only therapeutic option, desensitization is necessary (73). Cross-reactions between quinolones, BLs and neuromuscular blocking agents have been also described (74).
Conclusion
Antibiotic hypersensitivity is a frequent problem for physicians in particular for the future use of antibiotics. Firstly, it should be determined if the reaction associated with antibiotic intake was a type A or Type B reaction. In case of a Type B reaction, it is mandatory an appropriate diagnostic work-up for ascertaining the causal role of the drug. This is the first step for a correct management of antibiotic allergy. It is important not to “label” a child as allergic without an appropriate diagnostic work-up. When a diagnosis of antibiotic allergy is done, the second step is to find a safe and effective alternative. Unfortunately, the allergic work-up and the evaluation of cross reactivity is well structured only for BLs. Up to now, evidences on diagnostic tests for NBL allergy in children are limited.
Conflict of interest:
None to declare
References
- 1.Macy E, Romano A, Khan DJ. Practical management of antibiotic hypersensitivity in 2017. Allergy Clin Immunol Pract. 2017;5:577–86. doi: 10.1016/j.jaip.2017.02.014. [DOI] [PubMed] [Google Scholar]
- 2.Gomes ER, Brockow K, Kuyucu S, et al. ENDA/EAACI Drug Allergy Interest Group. Drug hypersensitivity in children: report from the pediatric task force of the EAACI Drug Allergy Interest Group. Allergy. 2016;71:149–61. doi: 10.1111/all.12774. [DOI] [PubMed] [Google Scholar]
- 3.Clavenna A, Bonari M. Adverse drug reactions in childhood: a review of prospective studies and safety alerts. Arch Dis Child. 2009;94:724–8. doi: 10.1136/adc.2008.154377. [DOI] [PubMed] [Google Scholar]
- 4.Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-2011. JAMA. 2016;315:1864–73. doi: 10.1001/jama.2016.4151. [DOI] [PubMed] [Google Scholar]
- 5.Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin infect Dis. 2016;62:e51–77. doi: 10.1093/cid/ciw118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jeffres MN, Narayanan PP, Shuster JE, Schramm GE. Consequences of avoiding belactams in patients with belactam allergies. J Allergy Clin Immunol. 2016;137:1148–53. doi: 10.1016/j.jaci.2015.10.026. [DOI] [PubMed] [Google Scholar]
- 7.Trubiano JA, Grayson ML, Thursky KA, Phillips EJ, Slavin MA. How antibiotic allergy labels may be harming our most vulnerable patients. Med J Aust. 2018;208:469–70. doi: 10.5694/mja17.00487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sacco KA, Bates A, Brigham TJ, et al. Clinical outcomes following inpatient penicillin allergy testing: A systematic review and meta-analysis. Allergy. 2017;72:1288–96. doi: 10.1111/all.13168. [DOI] [PubMed] [Google Scholar]
- 9.Sousa-Pinto B, Cardoso-Fernandes A, Araùjo L, et al. Clinical and economic burden of hospitalization with registration of penicillin allergy. Ann Allergy Asthma Immunol. 2018;120:190–4. doi: 10.1016/j.anai.2017.11.022. [DOI] [PubMed] [Google Scholar]
- 10.Li M, Krishna KA, Razaq S, et al. A real-time prospective evaluation of clinical pharmaco-economic impact of diagnostic label of “penicillin allergy” in UK teaching hospital. J Clin Pathol. 2014;67:1088–92. doi: 10.1136/jclinpath-2014-202438. [DOI] [PubMed] [Google Scholar]
- 11.Trubiano JA, Cosby AS, Grayson ML, et al. The 3 Cs of antibiotic allergy-classification, cross-reactivity and collaboration. J Allergy Clin Immunol Pract. 2017;5:1532–42. doi: 10.1016/j.jaip.2017.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Johansson SG, Bieber T, Dahl R, et al. Revised nomenclature for allergy for global use: report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Allergy Clin Immunol. 2004;113:832–6. doi: 10.1016/j.jaci.2003.12.591. [DOI] [PubMed] [Google Scholar]
- 13.Thien FCK. Drug hypersensitivity. Med J Aust. 2006;185:333–8. doi: 10.5694/j.1326-5377.2006.tb00591.x. [DOI] [PubMed] [Google Scholar]
- 14.Caubet JC, Kaiser L, Lemaìtre B, et al. The role of penicillin in benign skin rushes in childhood: a prospective study based on drug rechallenge. J Allergy Clin Immunol. 2011;127:218–22. doi: 10.1016/j.jaci.2010.08.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Caimmi S, Caimmi D, Bernardini R, et al. Perioperative anaphylaxis: epidemiology. Int J Immunopathol Pharmacol. 2011;24(3):S21–6. doi: 10.1177/03946320110240s304. [DOI] [PubMed] [Google Scholar]
- 16.Gomez MB, Torres MJ, Mayorga T, et al. Immediate allergic reactions to betalactam: facts and controversies. Curr Opin Allergy Clin Immunol. 2004;4:261–6. doi: 10.1097/01.all.0000136764.74065.15. [DOI] [PubMed] [Google Scholar]
- 17.Keighley CL, Saunderson RB, Kok J, Dwyer DE. Viral exanthems. Curr Opin Infect Dis. 2015;28:139–50. doi: 10.1097/QCO.0000000000000145. [DOI] [PubMed] [Google Scholar]
- 18.Caffarelli C, Cuomo B, Cardinale F, et al. Aetiological factors associated with chronic urticaria in children: a systematic review. Acta Derm Venereol. 2013;93:268–72. doi: 10.2340/00015555-1511. [DOI] [PubMed] [Google Scholar]
- 19.Caffarelli C, Dascola CP, Peroni D, et al. Airway acidification in childhood asthma exacerbations. Allergy Asthma Proc. 2014;35:51–6. doi: 10.2500/aap.2014.35.3740. [DOI] [PubMed] [Google Scholar]
- 20.Caffarelli C, Coscia A, Baldi F, et al. Characterization of irritable bowel syndrome and constipation in children with allergic diseases. Eur J Pediatr. 2007;166:1245–52. doi: 10.1007/s00431-006-0410-y. [DOI] [PubMed] [Google Scholar]
- 21.Macy E, Ho NJ. Multiple drug intolerance syndrome: prevalence, clinical characteristics, and management. Ann Allergy Asthma Immunol. 2012;108:88–93. doi: 10.1016/j.anai.2011.11.006. [DOI] [PubMed] [Google Scholar]
- 22.Lange L, Koningsbruggen SV, Rietschel E. Questionnaire-based survey of life time prevalence and character of allergic drug reactions in German children. Pediatr Allergy Immunol. 2008;19:634–8. doi: 10.1111/j.1399-3038.2007.00702.x. [DOI] [PubMed] [Google Scholar]
- 23.Demoly P, Adkinson NF, Brockow K, et al. International Consensus on drug allergy. Allergy. 2014;69:420–37. doi: 10.1111/all.12350. [DOI] [PubMed] [Google Scholar]
- 24.Har D, Solensky R. Penicillin and betalactam hypersensitivity. Immunol Allergy Clin N Am. 2017;37:643–62. doi: 10.1016/j.iac.2017.07.001. [DOI] [PubMed] [Google Scholar]
- 25.Ponvert C, Perrin Y, Bados-Albiero A, et al. Allergy to betalactam antibiotics in children: results of a 20-year study based on clinical history, skin and challenge test. Pediatr Allergy Immunol. 2011;22:411–8. doi: 10.1111/j.1399-3038.2011.01169.x. [DOI] [PubMed] [Google Scholar]
- 26.Zambonino MA, Corzo JL, Muñoz C, et al. Diagnostic evaluation of hypersensitivity reaction to beta-lactam antibiotics in a large population of children. Pediatr Allergy Immunol. 2014;25:80–7. doi: 10.1111/pai.12155. [DOI] [PubMed] [Google Scholar]
- 27.Vyles D, Adams J, Chiu Asriani , et al. Allergy test in children with low-risk penicillin allergy symptoms. Pediatrics. 2017;140:e20170471. doi: 10.1542/peds.2017-0471. [DOI] [PubMed] [Google Scholar]
- 28.King EA, Challa S, Curtin P, et al. Penicillin skin testing in hospitalized patients with beta lactam allergies: effect on antibiotic selection and cost. Ann Allergy Asthma Immunol. 2016;117:67–71. doi: 10.1016/j.anai.2016.04.021. [DOI] [PubMed] [Google Scholar]
- 29.Blumenthal KG, Wickner PG, Hurwitz S, et al. Takling inpatient penicillin allergies: assessing tools for antimicrobial stewardship. J Allergy Clin Immunol. 2017;140:154–61 e6. doi: 10.1016/j.jaci.2017.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program guidelines by the Infectious Disease Society of America and The Society of Healthcare Epidemiology of America. Clin Infect Dis. 2016;62:e51–77. doi: 10.1093/cid/ciw118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Banks TA, Ressner RA, Gada SM. Antibiotic reclamation: penicillin allergy, antibiotic stewaedship and the allergist. Ann Allergy Asthma Immunol. 2015;115:451–2. doi: 10.1016/j.anai.2015.08.008. [DOI] [PubMed] [Google Scholar]
- 32.Trubiano JA, Thursky KA, Stewardson AJ, et al. Impact of an integrated antibiotic allergy testing program on antimicrobial stewardship: a multicenter evaluation. Clin Infect Dis. 2017;65:166–74. doi: 10.1093/cid/cix244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Raja AS, Lindsell , Bernstein JA, et al. The use of penicillin skin testing to assess the prevalence of penicillin allergy in an emergency department setting. Ann Emerg Med. 2009;54:72–7. doi: 10.1016/j.annemergmed.2008.12.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mirakian R, Leech SC, Krishna MT, et al. Standards of Care Committee of the British Society for Allergy and Clinical Immunology. Management of allergy to penicillins and other beta-lactams. Clin Exp Allergy. 2016;45:300–27. doi: 10.1111/cea.12468. [DOI] [PubMed] [Google Scholar]
- 35.Marrs T, Fox AT, Lack G, du Toit G. The diagnosis and management of antibiotic allergy in children: Systematic review to inform a contemporary approach. Arch Dis Child. 2015;100:583–8. doi: 10.1136/archdischild-2014-306280. [DOI] [PubMed] [Google Scholar]
- 36.Wald ER, Applegate KE, Bordley C, et al. Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics. 2013;132:e262–80. doi: 10.1542/peds.2013-1071. [DOI] [PubMed] [Google Scholar]
- 37.Esposito S, Cohen R, Domingo JD, et al. Do we know when, what and for how long to treat? Pediatr Infect Dis J. 2012;31:e78–e85. doi: 10.1097/INF.0b013e318255dc5b. [DOI] [PubMed] [Google Scholar]
- 38.Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131:e964–99. doi: 10.1542/peds.2012-3488. [DOI] [PubMed] [Google Scholar]
- 39.Marchisio P, Bellussi L, Di Mauro G, et al. Acute otitis media: from diagnosis to prevention. Summary of the Italian Guideline. Int J Pediatr Otorhinolaryngol. 2010;74:1209–16. doi: 10.1016/j.ijporl.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 40. Dossier 254/2015 – Otite media acuta in età pediatrica. Linea guida regionale Emilia Romagna. Accessed at http://assr.regione.emilia-romagna.it/it/servizi/pubblicazioni/dossier/doss254 . [Google Scholar]
- 41.Jeffres MN, Narayanan PP, Shuster JE, Schramm GE. Consequences of avoiding beta-lactams in patients with beta-lactam allergies. J Allergy Clin Immunol. 2016;137:1148–53. doi: 10.1016/j.jaci.2015.10.026. [DOI] [PubMed] [Google Scholar]
- 42.Macy E, Blumenthal KG. Are cephalosporin safe for use in penicillin allergy without allergy evaluation? J Allergy Clin Immunol Pract. 2018;6:82–9. doi: 10.1016/j.jaip.2017.07.033. [DOI] [PubMed] [Google Scholar]
- 43.Zagursky RJ, Pichichero ME. Cross-reactivity in β-lactam allergy. J Allergy Clin Immunol. 2018;6:72–81. doi: 10.1016/j.jaip.2017.08.027. [DOI] [PubMed] [Google Scholar]
- 44.Romano A, Gaeta F, Poves MFA, Valluzzi RL. Cross-Reactivity among beta-lactams. Curr Allergy Asthma Rep. 2016;16:24. doi: 10.1007/s11882-016-0594-9. [DOI] [PubMed] [Google Scholar]
- 45.Blanca M, Romano A, Torres MJ, et al. Update on the evaluation of hypersensitivity reactions to betalactams. Allergy. 2009;64:183–93. doi: 10.1111/j.1398-9995.2008.01916.x. [DOI] [PubMed] [Google Scholar]
- 46.Pichichero ME, Zagursky RJ. Penicillin and cephalosporin allergy. Ann Allergy Asthma Immunol. 2014;112:404–12. doi: 10.1016/j.anai.2014.02.005. [DOI] [PubMed] [Google Scholar]
- 47.Joint Task Force on Practice Parameter. American Academy of Allergy, Asthma and Immunology. American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology. Drug allergy: an update practice parameter. Ann Allergy Asthma Immunol. 2011;105:259–73. doi: 10.1016/j.anai.2010.08.002. [DOI] [PubMed] [Google Scholar]
- 48.Romano A, Gaeta F, Valluzzi RL, et al. IgE mediated Hypersensitivity to cephalosporins: cross-reactivity and tolerability of alternative cephalosporins. J Allergy Clin Immunol. 2015;136:685–93. doi: 10.1016/j.jaci.2015.03.012. [DOI] [PubMed] [Google Scholar]
- 49.Gaeta F, Valluzzi RL, Alonzi C, et al. Tolerability of aztreonam and carbapenems in patients with IgE-mediated hypersensitivity to penicillins. J Allergy Clin Immunol. 2015;135:972–6. doi: 10.1016/j.jaci.2014.10.011. [DOI] [PubMed] [Google Scholar]
- 50.Frumin J, Gallagher JC. Allergic cross-sensitivity between penicillin, carbapenems and monobactam antibiotics; what are the chances? Ann Pharmacother. 2009;43:304–15. doi: 10.1345/aph.1L486. [DOI] [PubMed] [Google Scholar]
- 51.Caffarelli C, Franceschini F, Caimmi D, et al. SIAIP position paper: provocation challenge to antibiotics and non-steroidal anti-inflammatory drugs in children. Ital J Pediatr. 2018;44:147. doi: 10.1186/s13052-018-0589-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kuyucu S, Mori F, Atanaskovic-Markovich M, et al. Hypersensitivity reactions to non beta lactam antibiotics in children: an extensive review. Ped Allergy Immunol. 2014;25:534–43. doi: 10.1111/pai.12273. [DOI] [PubMed] [Google Scholar]
- 53.Araujo L, Demoly P. Macrolides allergy. Curr Pharm Des. 2008;14:2840–2862. doi: 10.2174/138161208786369812. [DOI] [PubMed] [Google Scholar]
- 54.Barni S, Butti D, Mori F, et al. Azithromicin Is More Allergenic Than Clarithromycin in Children With Suspected Hypersensityvity Reactions to Macrolides. J Investig Allergol Clin Immunol. 2015;25:128–32. [PubMed] [Google Scholar]
- 55.Cavkaytar O, Karaatmaca B, Yilmaz EA, Sekerel BE, Soyer O. Testing for clarithromycin hypersensitivity: a diagnostic challenge in childhood. J Allergy Clin Immunol Pract. 2016;4:330–2. doi: 10.1016/j.jaip.2015.09.015. [DOI] [PubMed] [Google Scholar]
- 56.Mori F, Barni S, Pucci N, et al. Sensivity and specificity of skin tests in the diagnosis of clarithromicin allergy. Ann Allergy Asthma Immunol. 2010;104:417–9. doi: 10.1016/j.anai.2010.03.010. [DOI] [PubMed] [Google Scholar]
- 57.Broz P, Harr TH, Hecking C, et al. Non irritant intradermal skin test concentration of ciprofloxacin, clarithomycin, and rifampicin. Allergy. 2012;67:647–52. doi: 10.1111/j.1398-9995.2012.02807.x. [DOI] [PubMed] [Google Scholar]
- 58.Caglayan Sozmen S, Povesi Dascola C, Gioia E, Mastrorilli C, Rizzuti L, Caffarelli C. Diagnostic accuracy of patch test in children with food allergy. Pediatr Allergy Immunol. 2015;26:416–22. doi: 10.1111/pai.12377. [DOI] [PubMed] [Google Scholar]
- 59.Caffarelli C, Ricò S, Rinaldi L, Povesi Dascola C, Terzi C, Bernasconi S. Blood pressure monitoring in children undergoing food challenge: association with anaphylaxis. Ann Allergy Asthma Immunol. 2012;108:285–6. doi: 10.1016/j.anai.2012.02.001. [DOI] [PubMed] [Google Scholar]
- 60.Sànchez-Borges M, Thong B, Blanca M, et al. Hypersensitivity reaction to non beta-lactam antimicrobial agents, a statement of the WAO special committee on drug allergy. World Allergy Organ J. 2013;6:18. doi: 10.1186/1939-4551-6-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Mori F, Pecorari L, Pantano S, et al. Azithromycin anaphylaxis in children. Int J Immunopath Pharmacol. 2014;27:121–6. doi: 10.1177/039463201402700116. [DOI] [PubMed] [Google Scholar]
- 62.Galli E, Neri I, Ricci G, et al. Consensus Conference on Clinical Management of pediatric Atopic Dermatitis. Ital J Pediatr. 2016;42:26. doi: 10.1186/s13052-016-0229-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Bensaid B, Rozieres A, Nosbaum A, Nicolas J, Berard F. Amikacin-induced drug reaction with eosinophilia and systemic symptoms syndrome: delayed skin test and ELISPOT assay results allow the identification of the culprit drug. J Allergy Clin Immunol. 2012;130:1413–4. doi: 10.1016/j.jaci.2012.05.042. [DOI] [PubMed] [Google Scholar]
- 64.Belloni Fortina A, Romano I, Peserico A, Eichenfield LF. Contact sensitization in very young children. J Am Acad Dermatol. 2011;65:772–9. doi: 10.1016/j.jaad.2010.07.030. [DOI] [PubMed] [Google Scholar]
- 65.Liippo J, Lammintausta K. Positive patch test reactions to gentamicin show sensitization to aminoglycosides from topical therapies, bone cements, and from systemic medication. Contact Dermatitis. 2008;59:268–72. doi: 10.1111/j.1600-0536.2008.01419.x. [DOI] [PubMed] [Google Scholar]
- 66.Schnyder B, Pichler WJ. Allergy to sulfonamides. J Allergy Clin Immunol. 2013;131:256–7. doi: 10.1016/j.jaci.2012.10.003. [DOI] [PubMed] [Google Scholar]
- 67.Chantachaeng W, Chularojanamontri L, Kulthanan K, Jongjarearnprasert K, Dhana N. Cutaneous adverse reactions to sulfonamide antibiotics. Asian Pac J Allergy Immunol. 2011;29:284–9. [PubMed] [Google Scholar]
- 68.Lin D, Li WIK, Rieder MJ. Cotrimoxazole for prophylaxis or treatment of opportunistic infections of HIV/AIDS in patients with previous history of hypersensitivity to cotrimoxazole. Cochrane Database Syst Rew. 2007;CD005646 doi: 10.1002/14651858.CD005646.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Minhas JS, Wickner PG, Long AA, Banerji A, Blumenthal KG. Immune-mediated reactions to vancomycon: A systemic case review and analysis. Ann Allergy Asthma Immunol. 2016;116:544–53. doi: 10.1016/j.anai.2016.03.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Khurana C, de Belder MA. Red man syndrome after vancomycin: potential cross reactivity with teicoplanin. Postgrad Med J. 1999;75:41–3. doi: 10.1136/pgmj.75.879.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Blanca-Lòpez N, Andreu I, Torres Jaèn MJ. Hypersensitivity reactions to quinolones. Curr Opin Allergy Clin Immunol. 2011;11:285–91. doi: 10.1097/ACI.0b013e3283489bc3. [DOI] [PubMed] [Google Scholar]
- 72.Abiodun Adefurin A, Sammons H, Jacqz-Aigrain E, Choonara I. Ciprofloxacin safety in paediatrics: a systematic review. Arch Dis Child. 2011;96:874–80. doi: 10.1136/adc.2010.208843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Doña I, Moreno E, Pérez-Sánchez N, et al. Update on Quinolone Allergy. Curr Allergy Asthma Rep. 2017;17:56. doi: 10.1007/s11882-017-0725-y. [DOI] [PubMed] [Google Scholar]
- 74.Rouzaire P, Nosbaum A, Mullet C, et al. Immediate allergic hypersensitivity to quinolones associates with neuro muscular blocking agents. J Allergy Clin Immunol in Practice. 2013;1:273–9. doi: 10.1016/j.jaip.2013.02.007. [DOI] [PubMed] [Google Scholar]