

Abstract
Background
While genetic counseling has expanded globally, Mexico has not adopted it as a separate profession. Given the rapid expansion of genetic and genomic services, understanding the current genetic counseling landscape in Mexico is crucial to improving healthcare outcomes.
Methods
Our needs assessment strategy has two components. First, we gathered quantitative data about genetics education and medical geneticists’ geographic distribution through an exhaustive compilation of available information across several medical schools and public databases. Second, we conducted semi‐structured interviews of 19 key‐informants from 10 Mexican states remotely with digital recording and transcription.
Results
Across 32 states, ~54% of enrolled medical students receive no medical genetics training, and only Mexico City averages at least one medical geneticist per 100,000 people. Barriers to genetic counseling services include: geographic distribution of medical geneticists, lack of access to diagnostic tools, patient health literacy and cultural beliefs, and education in medical genetics/genetic counseling. Participants reported generally positive attitudes towards a genetic counseling profession; concerns regarding a current shortage of available jobs for medical geneticists persisted.
Conclusion
To create a foundation that can support a genetic counseling profession in Mexico, the clinical significance of medical genetics must be promoted nationwide. Potential approaches include: requiring medical genetics coursework, developing community genetics services, and increasing jobs for medical geneticists.
Keywords: genetic counseling, Mexico, needs assessment
1. INTRODUCTION
In Latin America, lack of access to medical genetics services (Penchaszadeh, 2004) poses a tremendous challenge to fulfilling the objectives of the World Health Organization (WHO) Human Genomics in Global Health Initiative. This WHO initiative recognizes the impact of human genomics to achieve various public health goals including reducing health disparities and preventing, diagnosing, and treating genetic diseases (“[Link]). Previous studies on the status of genetic and genomic services in Latin American countries highlight several barriers to delivering services: a lack of proper education in medical genetics (Gandelman Horovitz, De Faria Ferraz, Dain, & Marques‐De‐Faria, 2013; Penchaszadeh, 2013; Rodas‐Pérez et al., 2015), low patient health literacy (Rodas‐Pérez et al., 2015), geographic distribution of providers (Gandelman Horovitz et al., 2013; Penchaszadeh, 2013), and difficulties obtaining diagnostic genetic testing (Gandelman Horovitz et al., 2013; Penchaszadeh, 2013; Rodas‐Pérez et al., 2015).
Some of these barriers persist in Mexico, an upper‐middle income country (“[Link]) with an estimated population size of 130 million inhabitants (“[Link]). In Mexico, medical education consists of 4–5 years of post‐secondary school training with an additional 3 years post‐medical school required to obtain specialized training in medical genetics (“[Link]). Board certification for medical genetics is provided by the Mexican Council for Genetics (CMGAC, in Spanish), currently listing 248 medical geneticists for the entire country (“Consejo Mexicano de Genetica[Link].C.,” n.d.). This equals to ~1 provider per 525,000 inhabitants, well below the US/UK standard of 1 per 100,000 (Hoskovec et al., 2018). In addition, the Mexican Society of Human Genetics (AMGH, in Spanish) provides professional and academic support to the genetics community (“[Link]).
Distribution of medical geneticists and the genetics infrastructure is highly concentrated in the capital, Mexico City (Kofman‐Alfaro & Zenteno, 2004). Even in Mexico City there is a reported lack of physician knowledge about the genetics specialty, and it is difficult to obtain diagnostic molecular testing (Kofman‐Alfaro & Zenteno, 2004). Currently available genomic testing facilities include academic institutions such as the National Autonomous University and the National Polytechnic Institute. There is also genetic testing available through the Ministry of Health via the National Institutes of Health, such as the National Institute of Genomic Medicine (INMEGEN, in Spanish), the National Cancer Institute, and the National Institute of Social Security (IMSS, in Spanish) (Jimenez‐Sanchez, Silva‐Zolezzi, Hidalgo, & March, 2008). These resources are all located in Mexico City. As such, patients that live in rural areas (22.2% of Mexico's population in 2010) are likely at a disadvantage compared to patients that live in urbanized areas of Mexico (“[Link]; Kofman‐Alfaro & Zenteno, 2004). Outside of Mexico City, there are a few scattered institutions that offer genetic testing services, but those are also located in urbanized areas (Jimenez‐Sanchez et al., 2008). These include the Autonomous University of Nuevo Leon (“[Link]) and the University of Guadalajara (“[Link]). Additionally, most of the current institutions offering genetic and genomic testing are involved in genomic research; few testing facilities exist for clinical purposes.
Access to diagnostic genetic testing is further challenged by a patient's access to health insurance. The Mexican health insurance system is fragmented into various programs that include single‐payer, private employer‐sponsored, government subsidies, and private insurances. As of 2015, there were over 20 million inhabitants (17.3%) who were uninsured and not affiliated to any health service (“[Link]). Uninsured and low‐income individuals are able to obtain healthcare services through the Seguro Popular and the National Institutes of Health (Kofman‐Alfaro & Zenteno, 2004; [Link]). Other major institutions offering healthcare insurance are IMSS and the Institute of Social Services and Security for Civil Servants (ISSSTE, in Spanish) ([Link]; [Link]). More than half of the population currently seeks services through the Seguro Popular or IMSS (“[Link]), both of which have limited genetics services and must care for patients from all over the country (10).
1.1. Genetics epidemiology of Mexico
The rarity of medical genetics services poses a public health concern (Kofman‐Alfaro & Zenteno, 2004) due to Mexico's genetic, environmental, and geographic diversity (Moreno‐estrada et al., 2014). In general, there is a lack of access to information about prevalence of genetic conditions in the country, but the prevalence of congenital anomalies and chromosomal abnormalities is estimated to be 5.3% (Christianson, Howson, & Modell, 2006) and is the second leading cause of infant mortality (8). Advanced maternal age, congenital disabilities, early‐onset cancer, and congenital malformations are all associated with genetic risks and are common indications for medical genetics and genetic counseling referrals in other parts of the world (Claus, Schildkraut, Thompson, & Risch, 1996; Hassold & Hunt, 2009; Heffner, 22004; Mcgirr, 2004; Ropers, 2008).The National Institute of Statistics and Geography (INEGI, in Spanish) documents the following regarding genetics‐related medical conditions or risks in the Mexican population (“[Link]): (a) births to mothers of advanced maternal age (over the age of 35) is estimated to be 10.1%, posing an increased risk for aneuploidy; (b) inherited or congenital disabilities involving impaired cognitive abilities, speech, motor skills, hearing, and sight, are reported to affect 16% of the population; (c) 14% of cancer deaths due to breast cancer occur in individuals between the ages of 25–44.
1.2. The role of genetic counselors
The roles of a medical geneticist and of a genetic counselor are complementary, not equivalent. For example, in the United States, when medical geneticists work in the same clinical environment as a genetic counselor, the medical geneticist is more involved in the diagnosis, physical examination, and medical management of the patient. The genetic counselor takes a family history, performs a risk assessment, educates patients about the benefits and limitations of genetic testing, facilitates decision making and provides psychosocial support to the patient (ACGC, 2015).
Genetic counseling is a well‐established profession in nearly 30 countries throughout the world and across various economic income groups (“[Link]): high‐income (Canada, The United States, The European Union, Australia, New Zealand, Taiwan, Japan, Singapore, South Korea, Israel, Saudi Arabia), upper‐middle income (South Africa, Malaysia, Cuba), and lower‐middle income (India, Indonesia, Philippines) (Abacan et al., 2019). In these countries, genetic counselors serve an integral role, either independently or alongside physicians, as part of the medical team.
Mexico, an upper‐middle income country, has yet to adopt genetic counseling as a separate profession. Currently, medical geneticists provide genetic counseling services in Mexico, but geographic location of patients and their access to healthcare can present obstacles to receiving care. Utilization of genetic counseling as a separate profession has the potential to help address these issues of limited access and availability of genetics services in Mexico by providing an additional type of healthcare provider available to patients in the public sector.
Given the expansion of genetic testing and precision health approaches worldwide, understanding the current practices, policies, and needs of genetic services in Mexico is critical to improving healthcare outcomes and allowing patients and families to benefit from genetic advancements within Mexico. This includes understanding the need for genetic counseling services (including via telemedicine) and the future potential for a separate profession of genetic counselors. No studies to date assess the genetic counseling landscape in Mexico, including any assessing the need for and feasibility of utilizing a separate genetic counseling profession. As such, we set out to describe the current state of genetic counseling services and potential need for genetic counseling as a separate profession in Mexico.
2. MATERIALS AND METHODS
2.1. Editorial policies and ethical considerations
This study was reviewed and approved by Stanford University's Institutional Review Board. All subjects elected to participate in the study after providing full informed consent.
2.2. Study design
This study is a mixed methodology needs assessment of the status of genetic counseling in Mexico. First, based on a review of scholarly literature and internet resources, we describe the current status of education in genetics and genetics providers’ geographic distribution in Mexico. Second, we interviewed key informants about the current state of genetics practice and views towards a genetic counseling profession in Mexico.
2.3. Quantitative analysis
2.3.1. Number of genetics‐related courses in medical schools
Information about the name and number of medical school programs in each Mexican state was obtained through the Mexican Association of Faculties and Schools of Medicine (AMFEM, in Spanish). The curricula for each medical school program was accessed from the school website and reviewed for presence of genetics‐related courses. Courses were determined to be genetics‐related if the title of the course included the words genética or genómica (genetics or genomics). Only required courses were considered. The number of enrolled students in each medical program for 2017 was obtained through the annual report of Mexico's National Association of Universities and Institutions of Higher Education (ANUIES, in Spanish). The total number of students enrolled in a required genetics‐related course was calculated for each state. The total number of students specifically enrolled in a required medical/clinically focused genetics course was calculated for each state as well.
2.3.2. Number of medical geneticists
Information regarding the concentration of medical geneticists per state in Mexico was gathered using four public sources: (a) CMGAC, which lists all active members which are board certified medical geneticists in the country and the state they are employed in; (b) Doctoralia (“Doctoralia,” [Link]), an online website for advertising medical geneticists that individuals may use to locate a medical geneticist in their state; (c) Infogen (“Infogen,” n.d.2008), a portal where individuals can access contact information for medical geneticists in their regions and (d) Seccion Amarilla (“Seccion Amarilla,”[Link]), a public online directory of various services and practices, including medical genetics practices.
The number of medical geneticists in Doctoralia was found by using the search term “genetistas” (geneticists) and documenting the state of employment for individuals listed. The number of medical geneticists in Seccion Amarilla was found by using the search term “medicos genetistas” (medical geneticists) and documenting the state of employment for each medical geneticist listed. The 2015 state population census information was obtained from INEGI (Supplementary material 1). The medical geneticists listed for each state were compared across all four sources to avoid double counting. The number of unique medical geneticists per state was then compared to the state population size, and the number of geneticists per 100,000 people was calculated. This method of analysis was used because reports from the United States and the United Kingdom predict the number of genetic counselors required to meet the demands of their populations is at least one provider per 100,000 people (Hoskovec et al., 2018). The number of total physicians per state was obtained from INEGI's State Statistics Yearbooks of 2017 (Supplementary material 2). The number of total physicians per 100,000 people was calculated for comparison to the number of medical geneticists.
2.4. Qualitative analysis
2.4.1. Participants
Participants over the age of 18 with the ability to interview in either English or Spanish were considered key informants if they were professionals in education, clinicians, or laboratory scientists who trained and currently worked in a medical genetics‐related capacity in Mexico. Each Mexican state was assigned to one of the regions of genetic diversity (North, Central East, Central West, South, and South East) identified by Moreno‐estrada et al., (2014). Key informants in these five distinct genetic regions of Mexico were targeted, to account for genetic diversity in the population.
A two‐phased recruitment approach was used. First, in an effort to use more general recruitment methods, individual email addresses were directly obtained through the American Society of Human Genetics (ASHG) public membership database (N = 14); Infogen (N = 25) (“2008); and university portals. Additional publicly available contact information (Appendix S1) was obtained through doing an online (Google) search of the listed medical geneticists in the CMGAC member list (N = 248). These databases were used to identify genetics professionals who were both medical geneticists (CMGAC, ASHG, Infogen, and universities) and non‐medical geneticists (ASHG and universities). Second, a snowball recruitment strategy (Valerio et al., 2016) was implemented to maximize subject participation. Participants were asked to voluntarily provide contact information for colleagues who might be interested in participating.
2.4.2. Semi‐structured interviews
A semi‐structured interview guide (Supplementary material 3) was developed by two genetic counselors (authors DB, KO), one of whom has been involved in genetic counselor education in the United States for nearly 20 years and is involved in international discussions about genetic counseling training. A health data scientist who has prior experience in population genetics and is from Mexico (author, ALP) provided feedback on the interview guide prior to its use. Participants were asked about their views and opinions regarding seven major topics: genetic counseling, medical genetics, genetic testing, impact of culture and religion on services, genetics education, creating a genetic counseling profession, and establishing a genetic counseling program.
Semi‐structured interviews were conducted by a single bilingual interviewer (DB) between November 2017 and March 2018, until data saturation was reached. Interviews were conducted remotely in a private facility in either English or Spanish, depending on the participant's preference. All interviews were audio recorded and transcribed in the language they were recorded. Transcripts in Spanish were not translated into English; only specific quotes used for publication were translated from Spanish to English. All three bilingual authors (DB, ALP, DH) reviewed any original quotes and the interpretations for accuracy prior to inclusion.
Transcripts were analyzed individually by thematic coding (Bradley, Curry, & Devers, 2007). A preliminary codebook was inductively developed using two transcripts. The codebook was then reviewed by two bilingual members of the analysis team (DB, author DH). Transcripts were re‐coded according to the revised codebook. An agreement test was performed until every code was agreed upon, and the codebook was finalized. These two investigators then co‐coded one additional transcript to test the final codebook. Following satisfactory co‐coding, four transcripts were individually coded by two members of the analysis team in an inter rater reliability test (Cohen, 1960), with a kappa value of 0.91, indicating “almost perfect agreement” (Cohen, 1960). Coding was subsequently completed independently by a single bilingual investigator (DB), and all final coded excerpts were reviewed and approved by DH. Thematic analysis was done by identifying response trends present in 10 or more transcripts (>50%). Final themes were reviewed and agreed upon by all members of the research team.
3. RESULTS
3.1. Current state of medical education in genetics and available medical geneticists
Figure 1 provides summary statistics on genetics education in medical schools across each state of Mexico, as well as the geographic distribution of medical geneticists in the country. We find that ~93% of medical students in Mexico are required to take a genetics‐related course as part of their curriculum. However, there is a lot of variation in what these courses may teach. Genetics‐related courses included: medical/clinical genetics, genetics/genomics, molecular genetics/molecular biology and genetics, genomic medicine/proteomics, molecular genetics laboratory, genetics and obstetrics, embryology and genetics, as well as genes and society (Supplementary material 4). When one looks specifically at required coursework focused on medical/clinical genetics, the numbers decrease such that ~46% of students are required to take a clinically focused genetics course. This means that ~63,000 students enrolled in physician training programs across Mexico in 2017 may not have received training in clinically applicable genetics content.
Figure 1.
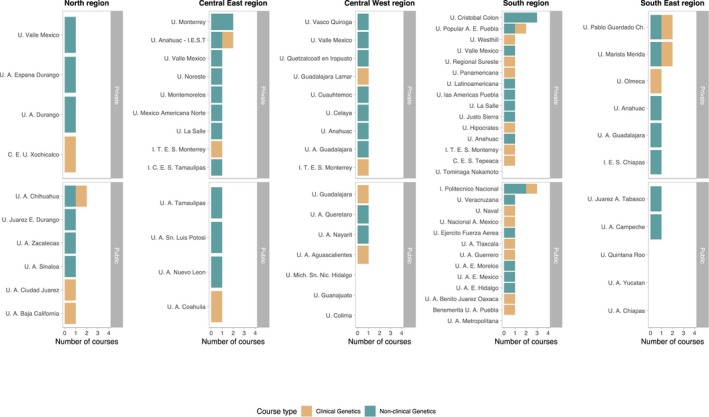
Genetics education. Number of students required to take a genetics‐related courses (excluding clinical genetics), curriculum from school websites, 2018. Number of students required to specifically take clinical genetics, curriculum from school websites, 2018
Figure 2 reflects the number of unique medical geneticists listed across four databases, meaning that there are more medical geneticists reported per state than are listed in CMGAC as registered board‐certified geneticists (Supplementary material 5). Based on the data from all databases, only Mexico City has at least 1 medical geneticist per 100,000 people. Nuevo Leon, Jalisco, Queretaro, Hidalgo, and Yucatan show a rate of 1 medical geneticist per 500,000 people. The remaining 26 states showed a rate lower than 1/500,000, with Baja California Sur, Colima, and Campeche having no medical geneticist.
Figure 2.
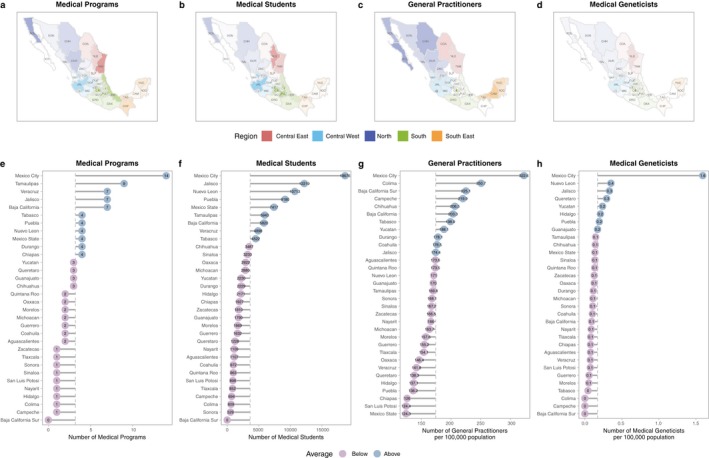
Medical programs and genetics workforce by state in the map (a,b,c,d) and lollipop plots (e,f,g,h). The panels show (a, b) Number of medical programs (AMFEM, 2017); (b, f) Total number of enrolled medical students (ANUIES, 2017); (c, g) Physicians by state (statistic yearbooks by state, INEGI 2017) (d, h) Unique medical geneticists from all four sources (CMGAC, Infogen, Seccion Amarilla, Doctoralia)
3.2. Participants
A total of 73 key informants were contacted for recruitment to participate in semi‐structured interviews. Ultimately, a total of 19 key informants from 10 different states participated in semi‐structured interviews that lasted between 30–120 min. Participants spanned each of the five regions of genetic diversity in the country (Figure 3). Participants worked in the public sector, private sector, or both. Seventeen of the 19 participants were clinical geneticists, 9 of whom also served as medical school educators throughout the country. One other participant was a non‐geneticist with an MD, PhD degree who worked in a clinical setting. The remaining participant had a PhD degree and participated in clinical research. All participants were directly involved in providing at least one of the following: diagnosis and management of genetic conditions and genetic counseling services.
Figure 3.

Participant distribution across the five genetically diverse regions of Mexico: North, Central West, Central East, South, and South East. One participant is employed in two regions
3.3. Themes identified
Overall, there were four major themes identified in participants’ responses: (a) the current state of medical genetics services; (b) impact of education on medical genetics practice; (c) patient features that impact provision of medical genetics; and (d) views towards a genetic counseling profession and program. Table 1 provides an executive summary of perceived barriers to medical genetics and genetic counseling services and establishing a genetic counseling profession. Table 2 presents a sample quote for each theme and the identified sub‐themes.
Table 1.
Executive summary of perceived barriers to medical genetics and genetic counseling services and establishing a genetic counseling profession
| Barriers to medical genetics services | Barriers associated with genetics education | Barriers associated with patient features | Barriers to establishing a GC program and profession |
|---|---|---|---|
|
|
|
|
Table 2.
Themes, sub‐themes, and sample quotes from respondents
| 1. The current state of medical genetics services | |
|
1.1 Medical geneticists provide genetic counseling 1.2 Shortage of medical geneticist jobs and regional distribution issues 1.3 High number of missed visits because patients cannot afford travel or cost of services 1.4 Limited genetic testing options |
“... for example at the [public sector] it [the wait list for an appointment] can be three months to almost a year. We have had various cases of patients who are fighting the waitlist, especially in regional hospitals. Since there are very few cities with medical geneticists, (patients) take a long time to get to us, and they have to cross half of the country to arrive at this service.” |
| 2. Impact of education about medical genetics practice | |
|
2.1 Physicians receive limited genetics training 2.2 Courses not required for all medica students 2.3 Courses often non‐clinical in focus and/or taught by non‐clinicians 2.4 Lack of education about medical genetics leads to limited referrals 2.5 Medical geneticists desire more GC training for themselves |
“The main barrier is that many medical students in the country do not take clinical genetics. So, a limiting factor that we have even outside of the institution is that the physician does not have the awareness to refer patients to genetics, even for malformations.” |
| 3. Patient features that impact provision of medical genetics | |
|
3.1 Low health‐literacy 3.2 “Magical” beliefs 3.3 Lack of preventative healthcare culture 3.4 No perceived significant impact of religion on acceptance of services |
“In Mexico we do not have a preventative medicine culture. This is to say, we do not treat symptoms until they are at advanced stages, and so I think that genetics is a very important change beyond a family or individual level, but more at a level of the health sector.” |
| 4. Views towards a genetic counseling profession and program | |
|
4.1 Positive attitudes overall 4.2 Concern about impact on medical geneticist workforce and workflow 4.3 All agreed classroom and rotation based teaching feasible 4.4 Recommended GC training involve a 2 years masters for health professionals |
“The demand for genomic diagnostic testing is increasing and so the results will have to be managed and explained by people who have the capacity, and medical geneticists will not be able to do all of that. So, I think that is one of the things that will catalyze this… that could catalyze it.” |
Additional quotes provided in Supplementary material 6.
3.3.1. The current state of clinical genetics services
In agreement with previous reports, all participants described that genetic counseling services in Mexico are currently offered through board certified medical geneticists, the majority of whom are located in Mexico City. Additionally, several participants mentioned that certain genetic conditions may only be seen in specific institutions. These two factors are perceived as impacting the provision of genetics services in Mexico, requiring many patients to travel long distances, and some patients may even be referred out‐of‐state to be seen by a genetics subspecialist even if there is an in‐state medical geneticist available. The shortage of medical geneticists in Mexico, particularly in the public sector where patients without private health insurance or ability to pay the out of pocket cost of a private genetics consultation are frequently seen, results in long waiting times from many weeks to over a year. Participants shared concerns that such a long waiting period prolongs the diagnosis of a patient, prevents timely medical management, and discourages patients from seeking care. Patients of low socioeconomic status may lack the resources required for travel and lodging to receive care. In these cases, participants stated that patients will typically go without a medical genetics consultation.
The lack of access to genetic and genomic testing for molecular diagnoses was described as a barrier to medical genetics services. In general, participants agreed that although genetic testing is available in Mexico, the types of tests available are limited. Several participants mentioned a lack of comprehensive clinical genetic testing laboratories that offer a full catalog of next generation sequencing tests in Mexico. According to their responses, many of the genetic tests they need to order must be done internationally, which increases the cost of genetic testing. As a result, they feel that very few patients have a confirmed molecular diagnosis because of the cost of genetic testing. Participants describe time intensive efforts to identify more cost‐effective testing alternatives for their patients, such as identifying research protocols that will perform the testing for free and writing to authors of published research papers to try and obtain free genetic testing for their patients.
3.3.2. Impact of genetics education on medical genetics practice
We elicited several concerns about the current education system for medical genetics and genetic counseling. First, participants perceive there is a lack of non‐genetics provider knowledge about the specialty and roles of medical genetics providers. Participants expressed worry that medical genetics is rarely a required course, may focus on basic molecular genetics rather than clinically relevant concepts, and may be taught by non‐physician basic scientists (for example a biologist or chemist) rather than a medical geneticist.
Interviewees expressed that, because of a lack of physician knowledge across the medical system, patients are not appropriately referred to medical geneticists. Participants report this creates the illusion that there are not many patients requiring genetics services, leading to hospital administrators believing genetics is not a necessary specialty area. Additionally, participants mentioned spending a significant portion of their workdays recruiting patients throughout their hospitals and educating other physicians on when to refer to medical genetics services.
Finally, the majority of interviewees stated that they did not receive formal training in genetic counseling during their own genetics specialty training, and expressed a desire for more psychosocial training of their own. Specific areas mentioned are to provide guidance for how to approach sensitive situations, help with delivering difficult information, and to allow them to develop their own counseling style.
3.3.3. Perceived patient features that impact the provision of medical genetics
Patient health literacy and cultural beliefs were discussed by many participants as challenges that impacted genetic counseling services. Several participants mentioned their patients having “magical beliefs” about congenital malformations and genetic conditions, which makes it difficult to counsel about the scientific etiology. Patients were also seen as resistant to being seen in genetics consultations because they lacked overall knowledge about what genetics is. They often did not understand the importance of going to a genetics consultation and either did not attend their appointments, or presented with resistance to the care being offered. Participants shared that these misunderstandings about medical genetics were enhanced by the fact that patients expressed a desire for a cure, not a diagnosis. According to interviewees, this disregard for a diagnosis stems from the overall lack of preventative healthcare culture in Mexico. They expressed that a patient's lack of appreciation for how a diagnosis can help inform medical management makes it difficult for them to advocate for their services.
The topic of placing blame on a family member was another barrier that participants cited as affecting the way medical genetics and genetic counseling services were accepted by patients. Some interviewees stated that when their patients are told their child might have a genetic condition, they have a tendency to place blame on the other parent, or fear that blame may be placed on themselves. This deep‐rooted perceived association between genetic conditions and a person at fault often prevents patients from pursuing a genetics consultation and genetic testing.
Finally, in terms of religious beliefs and their impact on genetic counseling and genetic testing services, participants mentioned that the majority of their patients are practicing Catholics. While a small subset of participants mentioned that some patients might refuse prenatal diagnostic services due to religious beliefs about pregnancy termination, most medical geneticists in our study felt religious beliefs did not impact patient care.
3.3.4. Views towards a genetic counseling profession and program
Almost all participants expressed positive attitudes towards a genetic counseling profession and the majority mentioned being able to envision a genetic counselor working in Mexico in the future. All participants agreed that genetic counselors were needed in every state, but would be particularly useful in rural settings where medical geneticists are not easily accessible, and rates of consanguinity are higher. Perceived roles for genetic counselors included serving as physician extenders by allowing them to see more patients. Additionally, participants expressed that genetic counselors would be especially valuable at this time, due to increasing demands for genetic and genomic testing. Some felt that genetic counselors would have a larger capacity to discuss testing and interpret results than geneticists currently do.
However, participants also mentioned physician attitudes and professional climate could pose barriers to establishing a separate genetic counseling profession in Mexico. Based on the perceived institutional lack of appreciation and awareness of the medical genetics specialty, there is a severe shortage of medical geneticist jobs in Mexico; new graduates can go long periods of time without being employed, and new graduates must sometimes educate hospital administrators on the importance and benefits of having a medical genetics service. Interviewees mentioned that other new graduates may find work as physicians outside of the medical genetics specialty, or pursue an industry or research position. In light of the current professional climate, participants expressed concern that the utilization of a separate genetic counseling profession at this time could either worsen the unemployment rate for geneticists, or genetic counselors themselves would be unemployed as well.
The majority of interviewees expressed that if a genetic counseling profession were to be established, it would be best to train existing health professionals due to their experience and knowledge. There was no clear consensus among participants’ answers regarding what type of healthcare professional would be the ideal candidate. Interviewees mentioned a master's degree as the ideal level of study because the time frame (2 years) is more focused than a bachelor's degree, and students would ideally already have a background in a health‐related field. All participants agreed that medical geneticists would be willing and able to provide course education and clinical training to genetic counseling students.
4. DISCUSSION
Our study found that the current status of medical genetics and genetic counseling services in Mexico is similar to previous reports on Latin America (Gandelman Horovitz et al., 2013; Penchaszadeh, 2013; Rodas‐Pérez et al., 2015). Our mixed methods approach showed consistencies between qualitative reports and publicly available data about medical school genetics training and the geographic distribution and numbers of medical geneticists. Several barriers to genetic counseling services were identified: geographic distribution of medical geneticists, lack of access to diagnostic tools, patient health literacy and cultural beliefs, and education in medical genetics and genetic counseling. Despite these barriers, participants reported generally positive attitudes towards a genetic counseling profession. The main perceived obstacles to creating a separate genetic counseling profession included worry about how creating a new pool of genetics professionals would impact the current workforce and workflow for geneticists. When broken down, a common theme unifying the identified barriers around genetic service delivery and perceived barriers to creating a separate genetic counseling profession is the lack of professional and public appreciation for the importance of medical genetics in the country.
To improve healthcare outcomes and advance medical genetics practices in Mexico, our study participants suggested that nation‐wide appreciation of genetics must be increased. An integral part of achieving this is to increase the genetics workforce in the country. Reports from the United States and the United Kingdom predict the number of genetic counselors needed to meet the demands of their populations are at least one provider per 100,000 people (Hoskovec et al., 2018). Our study data shows that only Mexico City is calculated to have the requisite workforce implying a massive unmet need. In fact, three states (Baja California Sur, Colima, and Campeche) appear to have zero practicing medical geneticists, and if one looks at data from the CMGAC alone, the numbers increase to six states (Baja California Sur, Colima, Campeche, Coahuila, Nayarit, and Tabasco) that currently do not have a practicing medical geneticist. This implies over 8 million people in Mexico do not have a genetics provider in their state.
One approach to address the lack of accessibility to genetics providers in Mexico is to increase the genetics workforce in a clinical setting. Genetic counseling as a separate profession could help realize this goal. Previous studies show that implementing genetic counseling services in specialty settings, such as oncology departments, can increase patient referrals and improve patient compliance with medical management guidelines (La Verde et al., 2016). Improving compliance with medical management guidelines is especially important for the Mexican population because our study found that participants perceive some of their patients do not fully understand the value of preventative care and often do not proactively seek management. Additionally, an increased presence of genetics providers in a clinical setting could enhance public awareness of genetics and increase patient health literacy, because more patients would be exposed to a genetics professional.
A complementary approach is to implement community genetics services across the country. This would require a baseline assessment and ongoing monitoring of the health statuses of different communities throughout the country (Kaye et al., 2001). Based on these assessments, appropriate population‐based services as well as public education models can be implemented. Community genetics services have the potential to improve the overall health of a population by providing a first line approach to identifying individuals at risk of having a genetic condition themselves or of having children affected by genetic conditions (WHO, 2010). Because of this, the WHO has issued a report calling for the implementation of community genetics services in low and middle‐income countries, such as Mexico (WHO, 2010). Additionally, providing community genetics services can help meet the needs of a unique and vulnerable population. Patients living in rural settings with limited access to medical services are traditionally individuals with limited health literacy and poorer health than individuals in urban areas (Douthit, Kiv, Dwolatzky, & Biswas, 2015). These individuals would greatly benefit from community outreach education projects.
To maximize the benefits of increasing the genetics workforce in clinical and community settings, clinicians in specialties outside of genetics must both appreciate the benefit of a genetics consultation and have the tools required to make appropriate referrals when necessary. Therefore, increasing medical genetics training is another crucial component of improving the status of medical genetics and genetic counseling services in Mexico. The current lack of clinically applicable genetics training in Mexico creates a domino effect that decreases public and professional appreciation for the profession and practice. If Mexico required that all medical schools offer clinical/medical genetics as a required course and that maintenance of credentials included continuing medical education around genetics, the issue of lack of knowledge about the medical relevance of genetics among the medical community could be addressed at its core.
Other countries in Latin America have faced similar education issues to Mexico. In Cuba, when it was recognized that a gap in genetics knowledge among their physicians could negatively impact the health of their population, medical genetics became a requirement for all medical students (Cruz, 2013). Additionally, Cuba introduced genetic counseling training programs to make genetic counseling services more accessible and help improve health indicators in the country. The decrease in the national infant mortality rate in Cuba from 7.2 in 2000, to 4.9 in 2011 is largely attributed to the downstream effects of creating of a genetic counseling profession in the country (Cruz, 2013). A similar approach was taken in the Philippines, which like Mexico, is a country where mid‐level providers are not a large component of the healthcare infrastructure (Laurino & Padilla, 2013). To help address the health needs of their population and expand genetics services, they recognized the need for a mid‐level provider such as a genetic counselor and implemented a 2‐year genetic counseling masters training program in 2011 (Laurino & Padilla, 2013; Ormond et al., 2018).
To implement an independent genetic counseling profession in Mexico, thought must be put into what type of training would best suit the current infrastructure. Our study participants agree that the most appropriate way to train genetic counselors in Mexico would be to offer a 2‐year Masters training program, similar to the approach taken in the Philippines and other countries (e.g., Indonesia, Japan, Malaysia) (Ormond et al., 2018). Furthermore, they suggest the training program focus on individuals who have a background in a health‐related field. There is significant variation across different countries and training programs about whether genetic counseling trainees must have prior health‐related training and experience or are accepted with scientific bachelor's degrees (Ormond et al., 2018).
In addition to considering what prerequisites students should have and what type of training program would be most appropriate, consideration should be given to how genetic counselors would be incorporated into the workplace. In some countries, particularly ones where there are not many genetic counselors and services are less accessible; genetic counselors serve more general roles and receive referrals for conditions across a wide‐spectrum (Ormond et al., 2018). In countries where the profession is more developed, genetic counselors serve specialized roles in departments such as oncology, perinatology, and cardiology ([Link]). Discussions regarding what their particular roles would be should also occur.
One widespread concern among participants is that genetic counselors would not be able to perform their jobs due to the lack of accessibility of genetic testing in Mexico. In countries where genetic counseling is well established (e.g. US, UK, Canada, Australia), the profession was established at a time when genetic testing was far more limited than it is now. Presently, genetic counselors serve many roles beyond the scope of genetic testing: risk assessments based on family history, explanation of referral reason, facilitate decision making, provide emotional support, identification of patient resources, and patient follow‐up (ACGC, 2015). In countries such as the US, UK, Canada, and Australia, genetic counselors often work independently from, or in consultation with, medical geneticists (Ormond et al., 2018). Overall, genetic counselors across the globe serve to increase accessibility to genetics services. Due to this, and despite concerns, medical geneticists in Mexico express positive attitudes towards a genetic counseling profession in Mexico.
The incorporation of genetic counselors into medical practice is becoming increasingly relevant as the genomic era continues to expand globally. In fact, participants add that, despite current limitations in genetic testing, the genomic era is present in Mexico now more than ever. This is further supported by the launch of several efforts in the past two decades, such as the creation of INMEGEN, to establish a national platform of genomic medicine in the country with the hope of improving healthcare outcomes (Jimenez‐Sanchez et al., 2008). However, increasing the availability and accessibility of genomic technology without having the necessary number of appropriately trained medical providers to educate patients about the implications of genetic testing and obtain informed consent goes against the ethical recommendations set forth by the American College of Medical Genetics and ASHG (ACOG, 2008; Botkin et al., 2015). In the current genomic setting, genetic counselors would be an important addition to the workforce due to their specialized training in ethics, capacity to understand and deliver genomic information, and ability to educate other health providers about genomic medicine (Middleton et al., 2017).
Additional research is needed to assess the unmet needs regarding genetic counseling in Mexico. Future studies could focus on specific regions in the country, such as each region of genetic diversity, to determine if there is a difference in needs between regions and what those differences are. This could be done through a qualitative study assessing patient perspectives including their understanding, beliefs, perceived unmet needs, and attitudes towards genetics services. The data obtained from such a study would allow genetic service providers to be aware of the specific needs of the population they are serving and give them an opportunity to tailor their approach appropriately. Additionally, the current body of literature could be enriched by studies reporting on the burden of different genetic conditions and concerns in the country. This information can benefit potential genetic counseling training programs by providing common conditions and concerns that should be taught as part of the curriculum. It would also benefit providers by quantifying the prevalence of genetic conditions and allowing them to provide more accurate risk assessments for patients.
We recognize that a limitation of this study is that qualitative data from semi‐structured interviews was self‐reported. However, claims regarding medical geneticist distribution and genetics education in the country were supported by quantitative analysis of data obtained from public databases. Another limitation is that the semi‐structured interviews were done on a voluntary basis. As such, participants in the study could have been individuals who are more likely to favor a genetic counseling profession in Mexico and more eager to effect change in the country, thus creating a sampling bias (Norris, 1997). To address this, interviews were conducted until data saturation was reached and participants were selected from each identified region of genetic diversity in the nation to account for diversity in patient populations.
5. CONCLUSION
To support the utilization of a genetic counseling profession in Mexico, the significance of medical genetics must be promoted nationwide to both patients and healthcare providers. Potential approaches include: (a). Increasing the number of medical geneticists employed in the public sector (b). Developing physician knowledge of genetics by requiring a clinically focused genetics course in all medical school programs and (c). Development of a pipeline of community genetics services to improve preventative healthcare awareness and genetic health literacy in the population (d). Implementation of a 2‐year Master's degree level genetic counseling training program to introduce additional genetics professionals into the workforce and address current population health needs as well as ethical dilemmas presented by an expanding genomic landscape.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
Supporting information
ACKNOWLEDGEMENTS
Research reported in this publication was partially supported via funds from the National Society of Genetic Counselors (NSGC) international special interest group and the National Human Genome Research Institute (NHGRI) under grant number U41HG009649. CDB is a Chan Zuckerberg Biohub Investigator. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors also wish to thank Dr. Louanne Hudgins for thoughtful review and comments on earlier drafts of this paper.
Bucio D, Ormond KE, Hernandez D, Bustamante CD, Lopez Pineda A. A genetic counseling needs assessment of Mexico. Mol Genet Genomic Med. 2019;7:e668 10.1002/mgg3.668
REFERENCES
- Abacan, M. , Alsubaie, L. , Barlow‐Stewart, K. , Caanen, B. , Cordier, C. , Courtney, E. , … Guan, Y. (2019). The global state of the genetic counseling profession. European Journal of Human Genetics, 27(2), 183‐197. 10.1038/s41431-018-0252-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- ACGC . (2015). Practice‐based competencies for genetic counselors. Accreditation Council for Genetic Counseling, 1–9.
- ACOG (2008). ACOG committee opinion No. 410: Ethical issues in genetic testing. Obstetrics and Gynecology, 111(6), 1495–1502. 10.1097/AOG.0b013e31817d252f [DOI] [PubMed] [Google Scholar]
- Asociacion Mexicana de Genetica Humana . (n.d.). Retrieved from http://www.amgh.org.mx
- Botkin, J. R. , Belmont, J. W. , Berg, J. S. , Berkman, B. E. , Bombard, Y. , Holm, I. A. , … McInerney, J. D. (2015). Points to consider: Ethical, legal, and psychosocial implications of genetic testing in children and adolescents. American Journal of Human Genetics, 97(1), 6–21. 10.1016/j.ajhg.2015.05.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bradley, E. H. , Curry, L. A. , & Devers, K. J. (2007). Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Services Research, 42(4), 1758–1772. 10.1111/j.1475-6773.2006.00684.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christianson, A. , Howson, C. P. , & Modell, B. (2006). March of Dimes. Retrieved from http://www.marchofdimes.com/aboutus/15796_19306.asp [Google Scholar]
- Claus, E. B. , Schildkraut, J. M. , Thompson, W. D. , & Risch, N. J. (1996). The genetic attributable risk of breast and ovarian cancer. Cancer, 77(11), 2318–2324. 10.1002/(SICI)1097-0142(19960601)77:11<2318:AID-CNCR8>3.0.CO;2-Z [DOI] [PubMed] [Google Scholar]
- Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological Measurement, 20(1), 37–46. 10.1177/001316446002000104 [DOI] [Google Scholar]
- Consejo Mexicano de Genetica A.C. (n.d.). Retrieved from https://www.cmgac.org.mx
- Cruz, A. L. (2013). An overview of genetic counseling in Cuba. Journal of Genetic Counseling, 22(6), 849–853. 10.1007/s10897-013-9635-x [DOI] [PubMed] [Google Scholar]
- Departamento de Genetica‐ Facultad de Medicina y Hospital Universitario, UANL . (n.d.). Retrieved from http://genetica-uanl.mx/Servicios2.html
- Doctoralia . (n.d.). Retrieved from https://www.doctoralia.com.mx
- Douthit, N. , Kiv, S. , Dwolatzky, T. , & Biswas, S. (2015). Exposing some important barriers to health care access in the rural USA. Public Health, 129(6), 611–620. 10.1016/j.puhe.2015.04.001 [DOI] [PubMed] [Google Scholar]
- Gandelman Horovitz, D. D. , De Faria Ferraz, V. E. , Dain, S. , & Marques‐De‐Faria, A. P. (2013). Genetic services and testing in Brazil. Journal of Community Genetics, 4(3), 355–375. 10.1007/s12687-012-0096-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hassold, T. , & Hunt, P. (2009). Maternal age and chromosomally abnormal pregnancies: What we know and what we wish we knew. Current Opinion in Pediatrics, 21(6), 703–708. 10.1097/MOP.0b013e328332c6ab.Maternal [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heffner, L. J. (2004). Advanced maternal age – how old is too old? New England Journal of Medicine, 351(19), 1927–1929. 10.1056/nejmp048087 [DOI] [PubMed] [Google Scholar]
- Hoskovec, J. M. , Bennett, R. l. , Carey, M. E. , DaVanzo, J. E. , Dougherty, M. , Hahn, S. E. , … Wicklund, C. A. (2018). Projecting the supply and demand for certified genetic counselors: A workforce study. Journal of Genetic Counseling, 27(1), 16–20. 10.1007/s10897-017-0158-8 [DOI] [PubMed] [Google Scholar]
- Human Genomics in Global Health: about WHO’s human genomics in global health initiative . (n.d.). Retrieved from http://www.who.int/genomics/about/en/
- Infogen . (n.d.). Retrieved from http://infogen.org.mx
- Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado . (n.d.). Retrieved from https://www.gob.mx/issste
- Instituto Mexicano del Seguro Social . (n.d.). Retrieved from https://www.gob.mx/imss
- Instituto Nacional de Estadistica y Geografia (INEGI) . (n.d.). Retrieved from http://www.inegi.org.mx
- Jimenez‐Sanchez, G. , Silva‐Zolezzi, I. , Hidalgo, A. , & March, S. (2008). Genomic medicine in Mexico: Initial steps and the road ahead. Genome Research, 18(8), 1191–1198. 10.1101/gr.065359.107 [DOI] [PubMed] [Google Scholar]
- Kaye, C. I. , Laxova, R. , Livingston, J. E. , Lloyd‐Puryear, M. A. , Mann, M. , McCabe, E. R. B. , & Therrell, B. L. (2001). Integrating genetic services into public health – guidance for state and territorial programs from the National Newborn Screening and Genetics Resource Center (NNSGRC). Public Health Genomics, 4(3), 175–196. 10.1159/000051179 [DOI] [PubMed] [Google Scholar]
- Kofman‐Alfaro, S. , & Zenteno, J. C. (2004). Genetic services in Mexico City. Public Health Genomics, 7(2–3), 142–145. 10.1159/000080785 [DOI] [PubMed] [Google Scholar]
- La Verde, N. , Corsi, F. , Moretti, A. , Peissel, B. , Dalu, D. , Girelli, S. , … Manoukian, S. (2016). A targeted approach to genetic counseling in breast cancer patients: The experience of an Italian local project. Tumori Journal, 102(1), 45–50. 10.5301/tj.5000407 [DOI] [PubMed] [Google Scholar]
- Laurino, M. Y. , & Padilla, C. D. (2013). Genetic counseling training in the Philippines. Journal of Genetic Counseling, 22(6), 865–868. 10.1007/s10897-013-9587-1 [DOI] [PubMed] [Google Scholar]
- Mcgirr, E. M. (1968). The genetics of congenital malformations. 61(April),385–389.
- Middleton, A. , Marks, P. , Bruce, A. , Protheroe‐Davies, L. K. , King, C. , Claber, O. , … Boyes, L. (2017). The role of genetic counsellors in genomic healthcare in the United Kingdom: A statement by the Association of Genetic Nurses and Counsellors. European Journal of Human Genetics, 25(6), 659–661. 10.1038/ejhg.2017.28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moreno‐Estrada, A. , Gignoux, C. R. , Fernández‐lópez, J. C. , Zakharia, F. , Sikora, M. , Contreras, A. V. , & Silva‐zolezzi, I. (2014). The genetics of Mexico recapitulates Native American substructure and affects biomedical traits. NIH Public Access, 344(6189), 1280–1285. 10.1126/science.1251688 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Society of Genetic Counselors‐ genetic counselors by specialty . (n.d.). Retrieved from https://www.nsgc.org/page/specialty-areas
- Norris, N. (1997). Error, bias and validity in qualitative research. Educational Action Research, 5(1), 172–176. 10.1080/09650799700200020 [DOI] [Google Scholar]
- Ormond, K. E. , Laurino, M. Y. , Barlow‐Stewart, K. , Wessels, T. M. , Macaulay, S. , Austin, J. , & Middleton, A. (2018). Genetic counseling globally: Where are we now? American Journal of Medical Genetics, Part C: Seminars in Medical Genetics, 178, 98–107. 10.1002/ajmg.c.31607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Penchaszadeh, V. B. (2004). Genetic services in Latin America. Public Health Genomics, 7(2–3), 65–69. 10.1159/000080773 [DOI] [PubMed] [Google Scholar]
- Penchaszadeh, V. B. (2013). Genetic testing and services in Argentina. Journal of Community Genetics, 4(3), 343–354. 10.1007/s12687-012-0093-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodas‐Pérez, C. , Clarke, A. , Powell, J. , Thorogood, M. , Rodas‐Perez, C. , Clarke, A. , … Thorogood, M. (2015). Challenges for providing genetic counselling in Colombian genetic clinics: The viewpoint of the physicians providing genetic consultations. Journal of Community Genetics, 6(3), 301–311. 10.1007/s12687-015-0237-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ropers, H. H. (2008). Genetics of intellectual disability. Current Opinion in Genetics and Development, 18(3), 241–250. 10.1016/j.gde.2008.07.008 [DOI] [PubMed] [Google Scholar]
- Salud Seguro Popular . (n.d.). Retrieved from http://www.seguropopular.org
- Seccion Amarilla . (n.d.). Retrieved from https://www.seccionamarilla.com.mx
- The World Bank: World Bank Country and Lending Groups . (n.d.). Retrieved from https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
- Universidad de Guadalajara‐ estudios citogenéticos constitucionales y adquiridos . (n.d.). Retrieved from http://www.udg.mx/es/servicios/catalogo/estudios-citogen-ticos-constitucionales-y-adquiridos
- Universidad Nacional Autonoma de Mexico, Facultad de Medicina, Division de Estudios de Posgrado . (n.d.). Retrieved from http://www.sidep.fmposgrado.unam.mx:8080/fmposgrado/programas/genmed.pdf
- Valerio, M. A. , Rodriguez, N. , Winkler, P. , Lopez, J. , Dennison, M. , Liang, Y. , & Turner, B. J. (2016). Comparing two sampling methods to engage hard‐to‐reach communities in research priority setting. BMC Medical Research Methodology, 16(1), 1–11. 10.1186/s12874-016-0242-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO . (2010). Community genetics services: report of a WHO consultation on community genetics in low and middle income countries. 1–4.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials