

Abstract
Background and aim of the work: The spontaneous and simultaneous rupture of both quadriceps tendons is uncommon and has rarely been reported in medical literature. The current case involves a 62-years old man with bilateral atraumatic complete quadriceps tendon rupture. Aim of this study is to provide a systematic review of this case and a literature review of similar cases. Methods: We reviewed and analyzed this patient’s records. Initial x rays of both knees showed a bilateral patellar spur. Real time ultrasonography scan of both knees showed a complete tear of quadriceps. The repair has consisted on end to end Krackow sutures associated with bone suture to the proximal pole of the patella using patellar drill holes. We also researched the literature for bilateral simultaneous rupture of the quadriceps tendon. Results: The patient suffered only from seasonal asthma (receiving only inhaled corticosteroids) and he was overweight (BMI: 33,5), he did not do any type of sport, he was a biker. The patient was able to walk after 3 weeks with both knee cast. The patients had a 120° pain free range of motion in both knees 4 months after surgery. Conclusion: Simultaneous bilateral quadriceps tendon rupture is really very rare and these are generally reported as case presentation in the literature. This injury usually presents in middle aged people with a history of chronic illness. The general recommendation is to perform surgical intervention within 48-72 hours after injury. (www.actabiomedica.it)
Keywords: quadriceps, tendon, bilateral, rupture, patellar spur, ultrasonography
Introduction
Atraumatic acute bilateral rupture of both quadriceps tendons has been rarely reported in the literature and is usually observed in patients aged over 40 years (1); a male:female ratio of 6:1 has been recorded for this phenomenon (2). This extremely rare condition has been published in the literature with systemic diseases such as chronic renal failure (3), diabetes mellitus, rheumatoid arthritis, chronic tendinopathy, amyloidosis and long-term use of systemic or local corticosteroid injections (4). Degenerative changes associated with ageing and calcific tendinopathy has also been shown to be a factor with quadriceps tendon rupture. The most commonly reported mechanism is the sudden reflexive eccentric contraction of quadriceps, with the foot anchored to the ground and the knee flexed (5). Diagnosis iseasily suggested by inability to actively extend the knee butit is still often overlooked in the emergency (6). The general recommendation is to perform surgical intervention within 48-72 hours after injury because of only prompt surgical repair shown to result in good to excellent range of motion and return to sport in most studies (7). We report a case of a patient who has sustained of an acute bilateral quadriceps’ tendon tear. Accordingly, we present patient’s records, clinical examination, imaging data and the management employed.
Case report
The authors have obtained the patient’s informed consent for print and electronical publication of the case report. On 7th February 2008, at 8.30 p.m. a man aged 62 years was admitted to our hospital with pain and swelling in both knee and inability to walk. He fell down one step at home. Physical examination revealed anterior swelling and a gap in quadriceps tendon 2-3 cm above the patella in both knees. He reported pain level of an 8 on visual analogue scale. The patient was unable to actively extend his knee. The patient exhibited good general condition. He suffered only from seasonal asthma for whom he was receiving inhaled corticosteroids and he was overweight (BMI: 33,5), no other co-morbidities were noted. He did not do any type of sport, he was a biker. Initial x rays of both knees were obtained and showed a lowering of patella with a bilateral patellar spur (a bone prominence at the quadriceps tendon insertion point of the proximal pole (Fig. 1, 2, 3, 4). Acute bilateral quadriceps tendon rupture was evoked. The patient subsequently underwent ultrasonography scan (Fig. 5, 6) which confirmed simultaneous rupture of both quadriceps’ tendon 1-2 cm superior to the patella. Laboratory tests were normal. Hemostasis assessment, renal function, sugar level was all normal. Heparin was given in the emergency room and the patient was admitted to the orthopedics department. The next morning (14 hours from injury) the patient underwent surgery under spinal anesthesia. Preoperative antibiotic prophylaxis was given (2 grams cefazolin i.v). Both knees were prepared with routine cleaning and draping and a tourniquet was applied. Longitudinal skin incision was used for both knees. The quadriceps were visualized, revealing a full thickness rupture of both tendons 1-2 cm proximally the bone-tendon junction (Fig. 7, 8). The distal part of the tendon was reattached using Krakow’s sutures associated with bone suture to the proximal pole of the patella using patellar drill holes (we made Krackow point in the tendon stump, which is then passed through the patella using longitudinal bony tunnels). The knees were immobilized in a locking hinged knee brace for 6 weeks. On postoperative day one the patient was allowed to flex at 30 degrees with the brace. The patient was discharged on the second postoperative day. ROM was permitted to increase 10 degrees every 3 days to achieve 90° within 20 days. There were no postoperative complications. The patient was able to walk after 3 weeks with both knee brace in the extended position. The patients had a 120° pain free range of motion in both knees 4 months after surgery (Fig. 9, 10, 11). At 10 months he returned on the bike, the Lysholm Knee Scoring scale was applied to the patient, which showed 88 for the right knee and 94 for the left knee.
Figure 1.

AP e lateral Radiographs of right knee demonstrating a proximal patellar pole spur (with arrow)
Figure 2.

AP e lateral Radiographs of right knee demonstrating a proximal patellar pole spur (with arrow)
Figure 3.

AP e lateral Radiographs of left knee demonstrating a proximal patellar pole spur (with arrow)
Figure 4.

AP e lateral Radiographs of left knee demonstrating a proximal patellar pole spur (with arrow)
Figure 5.
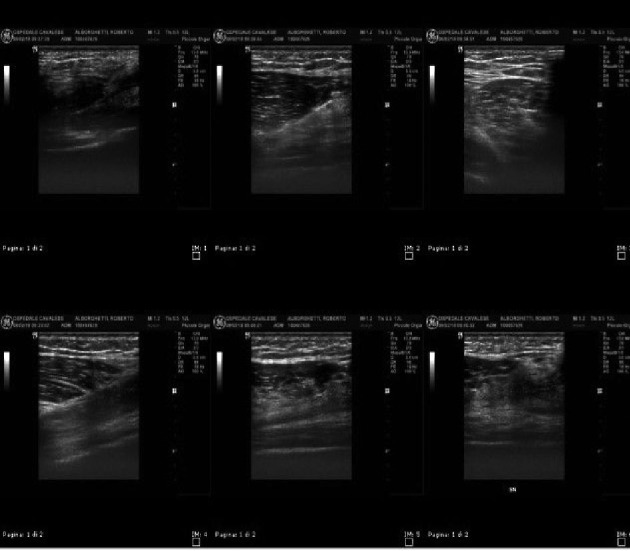
Ultrasonography scan of both knees showing a complete tear of both quadriceps’ tendons
Figure 6.
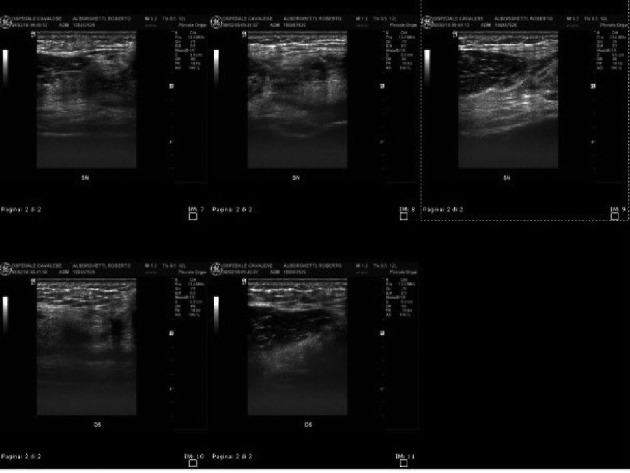
Ultrasonography scan of both knees showing a complete tear of both quadriceps’ tendons
Figure 7.

Intraoperative pictures of both knees
Figure 8.
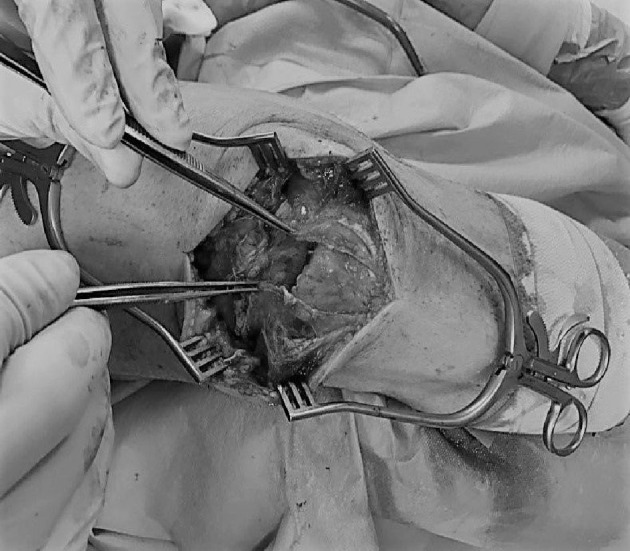
Intraoperative pictures of both knees
Figure 9.

Primary healed scar with full knee extension and full knee flexion at 4 months after operative.
Figure 10.

Primary healed scar with full knee extension and full knee flexion at 4 months after operative.
Figure 11.

Primary healed scar with full knee extension and full knee flexion at 4 months after operative.
Discussion
Simultaneous bilateral quadriceps tendon rupture is really very rare and usuallyreported as case presentation in the literature (8). The first reported case of simultaneous bilateral rupture of quadriceps tendons had been by Stener and Palmer in 1949 (9). Thes injury usually present in middle aged with a history of chronic illness (chronic renal failure, systemic lupus erythematosus, rheumatoid arthritis, diabetes mellitus, gout, long term corticosteroid use, obesity) that degenerate the intra-tendinous structure of the knee (10). Many cases of bilateral ruptures in athletes consuming anabolic agent have been also reported in literature (11). Moreover, direct corticosteroid injections and fluoroquinolone use have all been associated with increased risk of tendon rupture (11) Though fluoroquinolone use has most commonly affected the Achilles tendon, cases involving quadriceps tendons have also been described (12). In our case there was only history of inhaled corticosteroids and an increased BMI (13). Pain, cracking sensation, active knee extension defect and palpable supra-patellar defect are the typical signs and found in about 60% of patients (2). Accordingly, Siwek and Rao (14) in 1981 showed that 28% of ruptures had not been initially diagnosed. Therefore, clinical examination is crucial and allows for rapid diagnosis, which is critical for optimal therapeutic management (5). Anterior posterior and lateral radiograph of knee can objectify supra-patellar soft tissue defect, joint effusion, patella baja or avulsion fragment (15). It has also been suggested that the presence of a patella spur, a bony prominence at the QT tendon insertion point of the proximal pole may be associated with ruptures (16). Ultrasonography has proven to be a better modality than radiographs for the diagnosis if QT ruptures and can further differentiate between partial and complete tears as well as tear location (17). Magnetic resonance has greater sensitivity and specificity than US, however it is more expensive, time consuming and limited by its availability (18). The MRI scan is indicated when there is uncertainty regarding diagnosis and helps differentiate between a partial and complete tear. Although several techniques have been described including end-to-end suture, transosseus patellar tunnels or anchor fixation and also graft augmentation, there is a paucity of literature on the treatment of high-grade quadriceps tendon tears (19). Wenz at al have shown that either technique, compared to simple end-to-end sutures and patellar drilling holes, had no influence on the final outcome (20). Both Anchor suture techniques and transosseus sutures repair techniques do not show any difference in terms of clinical outcomes (21). After surgery walking was permitted protected with a brace keeping the knee extended for 4 to 6 week and not before 3-5 week (in bilateral simultaneous cases), which helps protect the reconstruction a mobilization of 0-30° have reported good functional results, always with complete motion recovery but in mono-lateral cases (22).
Conclusion
Both simultaneous quadriceps tendon rupture is extremely rare but however it must be considered in emergency if the patient has also a little traumatism of both knees associated to active extension deficiency, especially if it is over 40 years old, man, obese and with associated co-morbidities. Imaging should not substitute a good clinical examination. A missed diagnosis may lead to delayed repair, which could be problematic due to significant quadriceps retraction. General recommendation is to perform surgical intervention within 48-72 hours after injury, that allows optimal functional results.
References
- 1.Clayton RAE, Court-Brown CM. The epidemiology of muscolo-skeletal tendinous and ligaments injury. Injury. 2008;39:1338–44. doi: 10.1016/j.injury.2008.06.021. [DOI] [PubMed] [Google Scholar]
- 2.Ilian DI, Tejwani N, Kerschner M, Leibman M. “Quadriceps tendon rupture”. J Am Acad Orthop Surg. 2003;11:192–200. doi: 10.5435/00124635-200305000-00006. [DOI] [PubMed] [Google Scholar]
- 3.Y. Lee, B. Kim, J.-H. Chung, J. Dan. “Simultaneous bilateral quadriceps tendon rupture in patient with chronic renal failure”. Knee Surgery and Related Research. 2011;23(4):244–247. doi: 10.5792/ksrr.2011.23.4.244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.M.K. Shah. “Simultaneous bilateral rupture of quadriceps tendons: analysis of risk factors and associations”. Southern Medical Journal. 2001;95(8):860–866. [PubMed] [Google Scholar]
- 5.Wassim Zribi, Mohamed Zribi, Ahmed Recam Guidara, Mohamed Ben Jemaa, Ameur Abid, Abdessalem Naceur, Hassib Keskes. “Spontaneous and simultaneous complete bilateral rupture if quadriceps tendon in a patient receiving hemodialysis: A case report and literature review” World Journ Orthop. 2018 September 18;9(9):180–184. doi: 10.5312/wjo.v9.i9.180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Badr Ennaciri, Eric Montbarton, Emmanuel Beaudouin. “Surgical management of acute quadriceps tendon rupture (a case report with literature review”. Pan African Medical Journal. 2015;22:1–4. doi: 10.11604/pamj.2015.22.243.7533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Prasad Ellanti, Andrew Moriarty, Matthew Nagle, Tom McCharty. “Outcomes after quadriceps tendon repair in patients over 80 years of age”. Muscle, Ligaments and Tendons Journal. 2016;6(2):224–227. doi: 10.11138/mltj/2016.6.2.224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Maffulli N, Del Buono A, Spiezia F, Longo UG, Denaro V. “Light microscopic histology of quadriceps tendon ruptures”. Int Orthop. 2012;36(11):2367–2371. doi: 10.1007/s00264-012-1637-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sevan Sivacioglu, Ahmet Salduz, Ufuk Ozturk, Serkan Bayram, Fevzi Birisik. “Simultaneous bilateral quadriceps tendon rupture in a patient with diffuse idiopathic skeletal hyperostosis after minimal trauma: eight-year follow-ip”. Case reports in Orthopedics. 2018 February;2018:1–5. doi: 10.1155/2018/5047138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lewis AC, Purushotam B, Power DM. “Bilateral simultaneous quadriceps tendon rupture in a bodybuilder”. Othopedics. 2005;28:701–702. doi: 10.3928/0147-7447-20050701-23. [DOI] [PubMed] [Google Scholar]
- 11.V. Ristic’, M. Malianovic’, I. Popov, V Harhaji, V. Milankov. “Quadriceps tendon injuries”. Medical Review. 2013;66(3-4):121–125. doi: 10.2298/mpns1304121r. [DOI] [PubMed] [Google Scholar]
- 12.Stinner DJ, Orr JD, Hsu JR. “Fluoroquinolone-associated bilateral patellar tendon rupture: a case report and review of the literature”. Mil Med. 2010;175:457–459. doi: 10.7205/milmed-d-09-00142. [DOI] [PubMed] [Google Scholar]
- 13.Mohamed Omar, Philipp Haas, Max Ettinger, Christian Krettek, Maximilian Petri. “Simultaneous Bilateral Quadriceps Tendon Rupture following use of long-term low-dose nasal corticosteroid application”. Case Rep Orthop. 2013 Jul:1–5. doi: 10.1155/2013/657845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Siwek CW, Rao JP. “Ruptures of the extensor mechanism of the knee joint”. J Bone Joint Surg Am. 1981;63:932–937. [PubMed] [Google Scholar]
- 15.Haneko K, Demouy EH, Brunet ME, Benzian J. “Radiographic diagnosis of quadriceps tendon rupture: analysis of diagnostic failure”. J Emerg Med. 1994;12(2):225–229. doi: 10.1016/0736-4679(94)90703-x. [DOI] [PubMed] [Google Scholar]
- 16.Prasad Ellanti, Andrew Moriarty, Nikita Wainberg, Cliodhna Ni Foghlu, Tom Mc Carthy. “Association between patella spurs and quadriceps tendon ruptures”. Muscle, Ligaments and Tendons Journal. 2015;5(2):88–91. [PMC free article] [PubMed] [Google Scholar]
- 17.La S, Fessel DP, Femino JE, Jacobson JA, Jamadar D, Hayes C. “Sonography of partial-thickness quadriceps tendon tears with surgical correlation”. J Ultrasound Med. 2003;22:1323–1329. doi: 10.7863/jum.2003.22.12.1323. [DOI] [PubMed] [Google Scholar]
- 18.Swamy GN1, Nanjan SK, Yalapa S, Bishnoi A, Pickering SA. “Is ultrasound diagnosis reliable in acute extensor tendon injuries of the knee?”. Acta Orthop Belg. 2012;78(6):764–770. [PubMed] [Google Scholar]
- 19.Jorge Chahla, Nicholas N. DePhilippo, Mark E. Cinque, M.S Nicholas, I. Kennedy, George F. Lebus, Filippo Familiari, Gilbert Moatsche, Robert F. LaPrade. “Open repair of quadriceps tendon with suture anchors and semitendinous tendon allograft augmentation”. Arthr Techn. 2017;6(6 (December)):2071–2077. doi: 10.1016/j.eats.2017.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wenzi ME, Kirchner R, Seide K, Strametz S, Jurgens C. “Quadriceps tendon ruptures-is there a complete functional restitution?”. Injury. 2004;35(9):922–926. doi: 10.1016/S0020-1383(03)00261-4. [DOI] [PubMed] [Google Scholar]
- 21.Stefan Plesser, Mohammad Keilani, Gyoergy Vekszler, Timothy Hasenoehrl, Stefano Palma, Martin Reschl, Richard Crevenna, Stefan Hajdu, Harald Kurt Widhalm. “Clinical outcomes after treatment of quadriceps tendon ruptures show equal results independent of suture anchor or transosseus repair technique used – A pilot study”. PLoS One. 2018;13(3) doi: 10.1371/journal.pone.0194376. Supplementary materials S1 Table: pone.0194376. Published online 2018 Mar 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lighthart WA, Cohen DA, Levine RG, Parks BG, Boucher HR. “Suture anchor versus suture through tunnel fixation for quadriceps tendon rupture: a biomechanical study”. Orthopedics. 2008;31:441. doi: 10.3928/01477447-20080501-18. [DOI] [PubMed] [Google Scholar]