

Abstract
This study examined the associations between individual differences and posttraumatic growth, and coping strategies as mediators among 454 trauma-exposed American college students. Results showed that relational-interdependent self-construal, optimism, emotional expression, and social support seeking were associated with higher posttraumatic growth. Moreover, social support seeking and emotional expression partially mediated between relational-interdependent self-construal and posttraumatic growth, such that relational-interdependent self-construal was associated with posttraumatic growth through increased support seeking and emotional expression. However, the association between optimism and posttraumatic growth was partially mediated only by increased emotional expression, but not social support seeking. Findings imply that individual differences may facilitate posttraumatic growth through different coping mechanisms.
Keywords: emotional expression, optimism, posttraumatic growth, relational-interdependent self-construal, social support seeking
Research has found that it is common for people who have experienced negative events (e.g. diseases, accidents, and natural disasters) to report positive changes after those events (Schubert et al., 2016). Those perceived positive changes resulting from struggles with highly stressful events as posttraumatic growth (PTG; Calhoun and Tedeschi, 2013). PTG could be reflected in positive changes in self-perception, interpersonal relationships, and life philosophy; PTG has also been found predict higher well-being among trauma-exposed individuals (Ruini et al., 2014). According to Schaefer and Moos (1998), the degree to which people report PTG depends on a number of factors, including pre-trauma resources (e.g. individual differences and environmental resources), trauma characteristics (e.g. severity of exposure), and post-trauma factors (e.g. coping processes). Among these factors, little is known regarding the potential contributions of individual differences to PTG.
The potential roles of individual differences in coping and PTG
To adjust to the stressors brought from negative life events, people generally need to evaluate the impact of the events and available resources, plus engage in specific coping strategies to deal with the stressors. Such processes are found to be important predictors of adjustment outcomes, including PTG (Danhauer et al., 2013; Larsen and Berenbaum, 2015). According to the Stress and Coping model (Lazarus and Folkman, 1984), the person-environment relationship is dynamic and mutually reciprocal. Coping with stressors is therefore transactional such that people’s individual differences and their interplay with coping strategies could affect PTG. However, this question has not been well-addressed in the literature.
Previously, researchers have explored the associations between personality attributes and PTG. Extraversion, openness, agreeableness, and conscientiousness were associated with higher PTG in small-to-medium effect sizes (rs = 0.20–0.34; Măirean, 2016). Similarly, Owens (2016) found that higher extraversion, agreeableness, and conscientiousness were associated with higher PTG among trauma-exposed undergraduate students. This study aimed to examine the roles of two other individual differences (relational-interdependent self-construal (RISC) and optimism) in PTG, plus to explore whether coping strategies might mediate their relationships with PTG.
RISC, optimism, and PTG
RISC refers to the attribute that people are connected to others and define themselves by relationships, group memberships, or important roles in such relationships (Cross et al., 2000, 2011). People with high RISC tend to think and behave in ways that strengthen existing relationships (Cross et al., 2011) and engage in relationship supportive behaviors (e.g. self-disclosure). Previously, RISC has been found to be associated with higher life satisfaction (Heintzelman and Bacon, 2015), positive affect (King and Ganotice, 2015), and level of trust toward important others (Boucher, 2014; Morry et al., 2014). However, interpersonal trust and self-disclosure to others are associated with PTG (Ramos and Leal, 2013). It is noteworthy to explore whether RISC was associated with PTG, given a lack of empirical evidence in the literature.
Optimism is one of the most commonly studied intrapersonal coping resources (i.e. intrapsychic resources a person brings to the coping tasks) for predicting PTG. A meta-analysis found that optimism was moderately associated with higher PTG (r = 0.23) among different trauma-exposed populations in 27 studies (Prati and Pietrantoni, 2009). Another recent meta-analysis also found a moderate correlation between optimism and PTG among cancer patients (r = 0.27; Shand et al., 2015). Optimism is believed to facilitate well-being by helping people focus on the most important matters, disengaging from uncontrollable problems (Malinowski and Lim, 2015), plus promoting adaptive coping strategies (Hanssen et al., 2015). However, to the best of our knowledge, the mechanism between optimism and PTG has not been empirically confirmed, leaving this a knowledge gap to be explored.
Social support seeking and emotional expression as mediating coping strategies
We propose two mediators potentially explaining the associations between RISC/optimism and PTG. Research has suggested that people with higher levels of RISC are more likely to seek and receive social support from their significant others (Heintzelman and Bacon, 2015; Ringeisen and Buchward, 2008). Research has suggested that people with higher RISC are more likely to emotionally disclose deep feelings to their significant others (Do Couto and Hennig, 2015; Morry and Kito, 2009; Wills and Petrakis, 2018). We hence speculated that those higher in RISC may feel more comfortable seeking help and sharing emotional concerns with their significant others, as they tend to include significant others into their self-concept. Adding that social support seeking and emotional expression have been consistent predictors of PTG (Baillie et al., 2014; Larsen and Berenbaum, 2015; McDonough et al., 2014), this study expected that social support seeking and emotional expression would mediate the association between RISC and PTG.
Similarly, reviews have suggested that people with higher optimism tend to engage in more active coping (which includes social support seeking; Carver and Scheier, 2014; Nes and Segerstrom, 2006) and less avoidance (Dunn et al., 2011; Rauch et al., 2013). Seeing the future in a more positive light, higher levels of optimism may also facilitate people to perceive more social support from others. That may encourage them to actively seek social support from important others. Costello (1998) also found that optimism was associated with decreased use of denial and thoughts suppression when dealing with distress, implying that optimism might facilitate emotional expression. Given that the mediating roles of social support seeking and emotional expression in the association between optimism and PTG have not been examined, this study aimed to fill this knowledge gap in testing this mediation hypothesis.
Hypotheses
Based on the above rationales, this study examined the following hypotheses. First, RISC, optimism, social support seeking, and emotional expression would be associated with higher PTG. Second, the associations between the individual differences (i.e. optimism and RISC) and PTG were hypothesized to be mediated by social support seeking and emotional expression. Specifically, RISC and optimism were hypothesized to be associated with more frequent social support seeking and emotional expression, which in turn would be associated with higher PTG.
Method
Recruitment and participants
Students from psychology classes were invited to participate and sign up for this study on an online subject pool system. Upon consent, participants were directed to a link to access to the anonymous survey. The survey took about 25 minutes to complete. Participants included 454 undergraduate students (mean age = 22.9, standard deviation (SD) = 5.45, 82% female) from a large southwestern university. The sample was racially diverse, having 20.3% Asian/Pacific Islander, 12.8% African American, 26.5% Caucasian, 35.3% Hispanic/Latino, and 5.1% self-defined in other racial groups. The study was approved by the Institution Review Board.
Measures
Posttraumatic growth
The Posttraumatic Growth Inventory (PTGI; Tedeschi and Calhoun, 1996) was used to measure participants’ positive changes as a result of negative events they had experienced. This scale was reliable and valid among college students in the United States (Mohr and Rosén, 2017). On a 6-point scale (0 = I did not experience this change, 5 = I experienced this change to a very great degree), a sample item was “I changed my priorities about what is important in life” (α = .96). A higher mean score of the 21 items indicated higher levels of PTG (Taku and McDiarmid, 2015).
RISC
A 11-item scale was used to assess a person’s tendency to include significant others in his or her own self-definition (Cross et al., 2000). The scale was reliable and valid among college students (Heintzelman and Bacon, 2015). Participants reported how they agreed with the items on a 7-point Likert-type scale (1 = strongly disagree, 7 = strongly agree). A sample item was “When I think of myself, I often think of my close friends or family also” (α = .89). A higher mean score of all items indicated a higher level of RISC.
Social support seeking
The four items from the Use of Emotional Support and the Use of Instrumental Support subscales from the Brief Coping Orientation to Problems Experienced (COPE; Carver, 1997) was used to measure participants’ frequency of seeking social support when dealing with negative life events. This scale was valid and reliable among college students (Deatherage et al., 2014). On a 4-point Likert-type scale (1 = I haven’t been doing this at all, 4 = I’ve been doing this a lot), a sample item was “I’ve been getting comfort and understanding from someone” (α = .88). A higher mean score indicated more frequent support seeking from others.
Optimism
The Revised Life Orientation Test (LOT-R; Scheier et al., 1994) was used to measure participants’ optimism. This scale was reliable and valid among college students (Renshaw et al., 2016). Respondents indicated their level of agreements with the statements on a 5-point scale (0 = strongly disagree, 4 = strongly agree). A sample item was “Overall, I expect more good things to happen to me than bad” (α = .79). A higher mean score of the items indicated a higher level of optimism.
Emotional expression
Participants also completed the emotional expression subscale (eight items) from the Emotional Approach Coping Scale (EAC; Austenfeld and Stanton, 2004) on a 4-point scale (1 = I usually don’t do this at all, 4 = I usually do this a lot). A higher mean score of the items (e.g. “I take time to express my emotions,” α = .96) indicated more frequent use of emotional expression for coping with stress. The scale was reliable among college students and positively associated with adjustment outcomes (Juth et al., 2015). The Cronbach’s alpha was .96 in this sample.
Previous experience of traumatic events
Participants’ experience of different types of traumatic events was measured by the Vrana–Lauterbach Traumatic Events Scale—Civilian (Lauterbach and Vrana, 1996). We measured whether the participants had experienced the particular types of events listed and how traumatic they currently felt for those events (on a 7-point scale, 1 = not at all traumatic, 7 = severely traumatic) (refer to Table 1). This scale was shown to be valid in college samples such that those having experienced more traumatic events reported more psychological symptoms (Boals and Ruggero, 2016).
Table 1.
Participants’ exposure to traumatic events (N = 454).
| Frequency (%) | ||
|---|---|---|
| Number of types of traumatic events experienced | ||
| 1–2 types | 323 (71.1) | |
| 3–4 types | 108 (23.8) | |
| 5 types or more | 23 (5.1) | |
| Types of traumatic events | Experienceda | Rated as most traumatica |
| Witnessed a serious accident (e.g. industrial, farm, car, fire, and explosion) | 111 (24.4) | 52 (11.5) |
| Been in a natural disaster (e.g. tornado, hurricane, flood, and earthquake) | 261 (57.5) | 107 (23.6) |
| Been a victim of violent crime (e.g. rape, robbery, and assault) | 63 (13.9) | 40 (8.8) |
| Been a victim of either physical or sexual abuse as a child | 53 (11.7) | 33 (7.3) |
| Had unwanted sexual experiences involving threat or use of force as an adult | 30 (6.6) | 19 (4.2) |
| Been in a relationship that involved being abused physically or otherwise | 59 (13.0) | 37 (8.1) |
| Witnessed someone being mutilated, seriously injured, or violently killed | 18 (4.0) | 7 (1.5) |
| Been in a serious danger of losing life or being seriously injured | 54 (11.9) | 36 (7.9) |
| Received news of mutilation, injury, or unexpected death of someone close to you | 121 (26.7) | 87 (19.2) |
| Had traumatic experiences like these that you feel you can’t tell anyone | 36 (7.9) | 25 (5.5) |
| Other very traumatic events (e.g. medical surgery, changing religion, parents getting divorced, and hospitalized due to illness) | 149 (32.8) | 135 (29.7) |
Participants might select more than one type of traumatic events if applicable, thus the total frequencies did not add up to the sample size (N = 454).
Analytic plan
Descriptive statistics (including means and SDs) and bivariate correlations of the major variables were computed. Missing data were found in less than 2% in the major psychological variables and therefore were imputed by an expectation–maximization algorithm in SPSS 22.0. Path analyses (conducted by AMOS 22.0) were used to evaluate the fitness of the hypothesized model with observed variables and maximum likelihood estimation method. A satisfactory model fit was indicated by a chi-square value with a non-significant p-value (Kelloway, 1998), a root mean square error of approximation (RMSEA) ⩽ 0.08 (Steiger, 1990), and a comparative fit index (CFI) and incremental fit index (IFI) ⩾ 0.95 (Hu and Bentler, 1999). With a relatively large sample size (N = 454), we did not use the statistical significance for the chi-square as the primary indicator to evaluate the model fit, as chi-square was sensitive to sample size.
To ensure the stability of the path coefficient estimates, the mediation model analysis was also supplemented with 2000 bootstrap replications. Significance of the indirect effects was examined by the 95% bias-corrected confidence intervals (CIs) after bootstrapping. CIs were computed based on the 2000 estimates of the indirect effect bootstrap samples. The highest and lowest 2.5% of the indirect effect estimates determined the CIs. A significant indirect effect was supported if the 95% CIs did not include zero. Kline (2011) recommended that 20 observations per parameter would provide sufficient statistical power for the path analysis. With 19 parameters in the model (G*Power 3.1.2), a sample of 454 was able to detect small-to-medium effect sizes at a power of .80 (using p = .05 as the significance level).
Results
Prior traumatic experience
Participants’ prior exposure to traumatic events was different, with the most commonly experienced events as being in a natural disaster (e.g. tornado, hurricane, flood, or earthquake; 57.5%), witnessing a serious accident (24.4%), being in an abusive relationship (13%), and being in serious danger of losing life (11.9%). Among the participants, 28.9% had experienced more than two types of negative events (Table 1).
Correlation analysis and path analyses
As hypothesized, RISC, optimism, social support seeking, and emotional expression were positively correlated with PTG (rs = 0.24–0.43, ps < .001) (Table 2). Path analyses were conducted to examine whether emotional expression and social support seeking mediated the relationships between individual differences variables (optimism and RISC) and PTG. The proposed model showed a good fit in predicting PTG (model 1: χ2(4) = 11.05, p = .026, CFI = 0.98, IFI = 0.98, RMSEA = 0.06). All proposed paths were statistically significant except for the path from optimism to social support seeking (β = 0.06, p > .05). Specifically, the direct effects from optimism to PTG (β < .01, and p < .01) and from RISC to PTG (β = 0.13, p > .05) were still significant after considering the mediators. To test a more parsimonious model, we tested another model with the removal of the path from optimism to social support seeking. This revised model showed a good fit in predicting PTG (model 2: χ2(5) = 12.85, p = .025, CFI = 0.98, ILI = 0.98, RMSEA = 0.06) with a non-significant chi-square change from the hypothesized model (Δχ2(1) = 1.80, p > .05) and hence considered as the final model (Figure 1). The associations among the variables did not change even after controlling for current distress due to the stressful event (significant demographic variable). The overall model explained 29% of variance in PTG.
Table 2.
Descriptive statistics and correlations among major variables (N = 454).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. PTG | – | |||||||
| 2. Gendera | −.11* | – | ||||||
| 3. Prior traumatic eventsa | .05 | −.02 | – | |||||
| 4. Current distressa | .13** | −.11* | .41*** | – | ||||
| 5. RISC | .28*** | −.04 | −.04 | .05 | – | |||
| 6. Optimism | .24*** | .10* | −.02 | −.11* | .19*** | – | ||
| 7. Social support seeking | .43*** | −.08 | .03 | .10* | .28*** | .11* | – | |
| 8. Emotion expression | .39*** | −.14** | .01 | .02 | .20*** | .22*** | .39*** | – |
| Mean | 3.09 | 1.13 | 2.10 | 3.20 | 5.11 | 2.37 | 2.57 | 2.56 |
| SD | 1.18 | 0.34 | 1.29 | 1.92 | 1.13 | 0.74 | 0.84 | 0.84 |
| Cronbach’s α | .96 | N/A | N/A | N/A | .89 | .80 | .88 | .96 |
PTG: posttraumatic growth; RISC: relational-interdependent self-construal; SD: standard deviation; N/A: not applicable.
Gender: female (1) and male (2); prior traumatic events: number of prior traumatic events experienced; current distress: current distress due to the most traumatic event.
p < .05; ** p < .01; *** p < .001.
Figure 1.
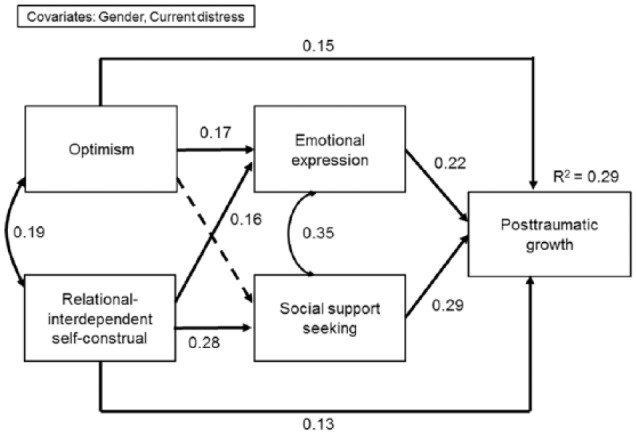
A path model illustrating the relationships among individual differences (relational-interdependent self-construal and optimism), coping strategies (emotional expression and social support seeking), and posttraumatic growth.
Values shown are standardized path coefficients. Solid lines represent significant paths in the hypothesized model (all ps < .01). The broken line indicates a non-significant path in the hypothesized model (p > .05), which was removed from the final model.
Partial mediation effects of emotional expression and social support seeking were supported. Specifically, the indirect effects from optimism to PTG via emotional expression (β = 0.04, p < .001), from RISC to PTG via emotional expression (β = −0.04, p < .001), and from RISC to PTG via social support seeking (β = 0.08, p < .001) were statistically significant (Figure 1). Results from bootstrapping supported the presence of a partial mediation effect, as both the indirect effect from optimism to PTG via emotional expression (β = 0.04, p = .001; 95% CI = 0.02, 0.06) and indirect effects from RISC to PTG via emotional expression and social support seeking (β = 0.12, p = .001; 95% CI = 0.09, 0.15) were greater than zero in the 95% CIs. These results suggested that RISC was associated with PTG through increased emotional expression and social support seeking, whereas optimism was associated with PTG through increased emotional expression only. After bootstrapping, the direct effects from optimism to PTG (β = 0.15, p = .001, 95% CI = 0.08, 0.21) and from RISC to PTG (β = 0.13, p = .001, 95% CI = 0.07, 0.18) were also found to be significant, suggesting that optimism and RISC still contributed to the variance of PTG significantly after considering the mediators.
Discussion
Researchers proposed that the associations between coping processes and PTG could vary based on people’s individual differences (Vázquez et al., 2014). This was an early attempt to explore how optimism and RISC may associate with PTG through coping mechanisms. Social support seeking partially mediated between RISC and PTG; emotional expression partially mediated both the associations between optimism and PTG and between RISC and PTG.
Optimism and PTG: mediated by emotional expression but not social support seeking
Consistent to a previous review (Prati and Pietrantoni, 2009), our findings indicated that optimism was associated with PTG. We contributed to the literature by revealing one of the possible mechanisms through which optimism facilitates PTG. It has been assumed that optimism is always associated with people’s well-being through approach coping strategies (Carver and Scheier, 2014), which was consistent with our findings that optimism was positively correlated with both emotional expression and social support seeking. However, to look at it more deeply, our mediation model suggested that optimism could facilitate PTG only through increasing emotional expression, but not through social support seeking.
Scholars have also suggested that optimistic individuals tend to match their coping strategies with the characteristics of the situations using more problem-focused coping (e.g. seeking social support) for controllable stressors and adaptive emotional-focused coping for uncontrollable stressors (e.g. trauma) (Bonanno et al., 2011; Carver and Scheier, 2014; Nes and Segerstrom, 2006). It is possible that optimistic individuals learn to incorporate emotional expression into goal pursuit in the context of trauma adjustment. Consistent with this, Costello (1998) also found that social support seeking did not mediate between optimism and posttraumatic stress symptoms among people exposed to Hurricane Andrew. Extending from our findings, more research is warranted to examine whether optimism facilitates PTG through increased emotional approach coping strategies rather than interpersonal approach coping strategies.
RISC and PTG: mediated by social support seeking and emotional expression
To the best of our knowledge, this was one of the first studies indicating that RISC was associated with PTG. Our mediation model also suggested that that RISC was associated with more social support seeking and emotional expression, which further facilitated PTG. Previously, Du and King (2013) have found that relational self was related to external locus of hope from family and friends, which in turn predicted adjustment outcomes (e.g. life satisfaction). Another study found that those greater in RISC experienced great higher self-confidence when significant others (e.g. close relationship partners) were primed during the experiment (Gabriel et al., 2007). Such self-confidence may motivate people to emotionally disclose deeper feelings to their significant others, making them worrying less about the events’ potential consequences (Do Couto and Hennig, 2015; Morry and Kito, 2009; Wills and Petrakis, 2018). RISC may function as a facilitator for both interpersonal and emotional approach coping strategies, which could result in more PTG. As an extension from this study, future research could also explore the other mediating coping variables between RISC and PTG, plus examine whether training people’s skills in seeking support could increase their PTG. Given that RISC could be primed through experiments (Gabriel et al., 2007), it is worth exploring whether reminding people about their significant others through interventions may facilitate their willingness to seek social support and express trauma-related emotions.
Limitations
This study had several limitations. First, this study tested the mediation model based on cross-sectional data, which limited the exploration of temporal relationships between the variables. Examining the longitudinal relationships between individual differences, changes in coping variables, and PTG at multiple time points (e.g. cross-lagged panel design) was recommended for future studies. Second, similar to other studies recruiting undergraduate populations (Moore et al., 2017; Owens, 2016), this sample consisted of more females than males. It could only provide a limited variability to examine whether gender plays a significant role in PTG-related processes. However, we believed our sample provided the cultural and trauma-event-related variabilities to examine novel hypotheses as a valuable first step. Third, the mediation model only explained a moderate proportion of variance in PTG, implying that other important variables may need to be considered. Studies have suggested that centrality of the traumatic event (higher PTG among people incorporated the event into personal identity) and coping flexibility (higher PTG among those who could flexibly use different types of coping strategies) are also important determinants of PTG (Kunz et al., 2018; Wamser-Nanney et al., 2018). Considering those may explain additional variance in PTG.
Implications
This study had strong implications to advance our understanding in how pre-trauma and post-trauma factors contribute to PTG. Future studies may extend to understand how the interplay between these individual differences and coping strategies contribute to people’s PTG (Jayawickreme and Blackie, 2014). For example, the linkage between RISC and self-compassion (i.e. being discerning and gentle toward oneself in face of hardship or perceived inadequacy) was examined. RISC was associated with different aspects of self-compassion (e.g. self-kindness, less self-judgment, and mindfulness; Akin and Eroglu, 2013), whereas self-compassion was found to be associated with more cognitive processing and higher PTG (Wong and Yeung, 2017).
Even though optimism is generally regarded as a relatively stable individual characteristic, researchers have found that optimism could be enhanced in medium effect size through psychological interventions (Hedge’s g = 0.41; Malouff and Schutte, 2017). Based on our findings, increasing optimism may facilitate more frequent emotional expression, which in turn enhances PTG. Similarly, how PTG can be enhanced through interventions has received growing empirical attentions. A recent meta-analysis evaluated the effects of 12 randomized controlled trials of psychosocial interventions on PTG among trauma-exposed populations. It found that those interventions increased people’s PTG in medium effect sizes (Roepke, 2015). Accumulating these findings could help to tailor interventions based on people’s individual characteristics to maximize their PTG in the long run.
Footnotes
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Akin A, Eroglu Y. (2013) Self-compassion and relational-interdependent self-construal. Studia Psychologica 55: 111–121. [Google Scholar]
- Austenfeld JL, Stanton AL. (2004) Coping through emotional approach: A new look at emotion, coping, and health-related outcomes. Journal of Personality 72: 1335–1364. [DOI] [PubMed] [Google Scholar]
- Baillie SE, Sellwood W, Wisely JA. (2014) Posttraumatic growth in adults following a burn. Burns 40: 1089–1096. [DOI] [PubMed] [Google Scholar]
- Boals A, Ruggero C. (2016) Event centrality prospectively predicts PTSD symptoms. Anxiety, Stress, & Coping 29: 533–541. [DOI] [PubMed] [Google Scholar]
- Bonanno GA, Pat-Horenczyk R, Noll J. (2011) Coping flexibility and trauma: The Perceived Ability to Cope with Trauma (PACT) scale. Psychological Trauma: Theory, Research, Practice, and Policy 3: 117–129. [Google Scholar]
- Boucher HC. (2014) The relational-interdependent self-construal and positive illusions in friendship. Self and Identity 13: 460–476 [Google Scholar]
- Calhoun LG, Tedeschi RG. (2013) Posttraumatic Growth in Clinical Practice. New York: Routledge. [Google Scholar]
- Carver CS. (1997) You want to measure coping but your protocol’s too long: Consider the brief cope. International Journal of Behavioral Medicine 4: 92–100. [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF. (2014) Dispositional optimism. Trends in Cognitive Sciences 18: 293–299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costello NL. (1998) Emotional expression and trauma: Relationships to optimism, coping, neuroendocrine, and immune system functioning. Dissertation Abstracts International: Section B: The Sciences and Engineering 59: 0868. [Google Scholar]
- Cross SE, Bacon PL, Morris ML. (2000) The relational-interdependent self-construal and relationships. Journal of Personality and Social Psychology 78: 791–808. [PubMed] [Google Scholar]
- Cross SE, Hardin EE, Gercek-Swing B. (2011) The what, how, why, and where of self-construal. Personality and Social Psychology Review 15: 142–179. [DOI] [PubMed] [Google Scholar]
- Danhauer SC, Case LD, Tedeschi RG, et al. (2013) Predictors of posttraumatic growth in women with breast cancer. Psycho-oncology 22: 2676–2683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deatherage S, Servaty-Seib HL, Aksoz I. (2014) Stress, coping, and internet use of college students. Journal of American College Health 62: 40–46. [DOI] [PubMed] [Google Scholar]
- Do Couto L, Hennig KH. (2015) Multiple facets of women’s relational orientation and their role in the relationship formation process. Personality and Individual Differences 77: 137–142. [Google Scholar]
- Du H, King RB. (2013) Placing hope in self and others: Exploring the relationships among self-construals, locus of hope, and adjustment. Personality and Individual Differences 54: 332–337. [Google Scholar]
- Dunn J, Occhipinti S, Campbell A, et al. (2011) Benefit finding after cancer: The role of optimism, intrusive thinking and social environment. Journal of Health Psychology 16: 169–177. [DOI] [PubMed] [Google Scholar]
- Gabriel S, Renaud JM, Tippin B. (2007) When I think of you, I feel more confident about me: The relational self and self-confidence. Journal of Experimental Social Psychology 43: 772–779. [Google Scholar]
- Hanssen MM, Vancleef LMG, Vlaeyen JWS, et al. (2015) Optimism, motivational coping and well-being: Evidence supporting the importance of flexible goal adjustment. Journal of Happiness Studies 16: 1525–1537. [Google Scholar]
- Heintzelman SJ, Bacon PL. (2015) Relational self-construal moderates the effect of social support on life satisfaction. Personality and Individual Differences 73: 72–77. [Google Scholar]
- Hu L, Bentler PM. (1999) Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling 6: 1–55. [Google Scholar]
- Jayawickreme E, Blackie LE. (2014) Posttraumatic growth as positive personality change: Evidence, controversies and future directions. European Journal of Personality 28: 312–331. [Google Scholar]
- Juth V, Dickerson SS, Zoccola PM, et al. (2015) Understanding the utility of emotional approach coping: Evidence from a laboratory stressor and daily life. Anxiety, Stress, & Coping 28: 50–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelloway EK. (1998) Using LISREL for Structural Equation Modeling a Research Guide. Thousand Oaks, CA: SAGE. [Google Scholar]
- King RB, Ganotice FA. (2015) Does family obligation matter for students’ motivation, engagement, and well-being? It depends on your self-construal. Personality and Individual Differences 86: 243–248. [Google Scholar]
- Kline RB. (2011) Methodology in the Social Sciences (Principles and Practice of Structural Equation Modeling) (3rd edn). New York: The Guilford Press. [Google Scholar]
- Kunz S, Joseph S, Geyh S, et al. (2018) Coping and posttraumatic growth: A longitudinal comparison of two alternative views. Rehabilitation Psychology 63: 240–249. [DOI] [PubMed] [Google Scholar]
- Larsen SE, Berenbaum H. (2015) Are specific emotion regulation strategies differentially associated with posttraumatic growth versus stress? Journal of Aggression, Maltreatment & Trauma 24: 794–808. [Google Scholar]
- Lauterbach D, Vrana S. (1996) Three studies on the reliabilities and validity of a self-report measure of posttraumatic stress disorder. Assessment 3: 17–25. [Google Scholar]
- Lazarus RS, Folkman S. (1984) Stress, Appraisal and Coping. New York: Springer. [Google Scholar]
- McDonough MH, Sabiston CM, Wrosch C. (2014) Predicting changes in posttraumatic growth and subjective well-being among breast cancer survivors: The role of social support and stress. Psycho-Oncology 23: 114–120. [DOI] [PubMed] [Google Scholar]
- Măirean C. (2016) The relationship between secondary traumatic stress and personal posttraumatic growth: Personality factors as moderators. Journal of Adult Development 23: 120–128. [Google Scholar]
- Malinowski P, Lim HJ. (2015) Mindfulness at work: Positive affect, hope, and optimism mediate the relationship between dispositional mindfulness, work engagement, and well-being. Mindfulness 6: 1250–1262. [Google Scholar]
- Malouff JM, Schutte NS. (2017) Can psychological interventions increase optimism? A meta-analysis. Journal of Positive Psychology 12: 594–604. [Google Scholar]
- Mohr D, Rosén LA. (2017) The impact of protective factors on posttraumatic growth for college student survivors of childhood maltreatment. Journal of Aggression, Maltreatment & Trauma 26: 756–771. [Google Scholar]
- Moore AA, Overstreet C, Kendler KS, et al. (2017) Potentially traumatic events, personality, and risky sexual behavior in undergraduate college students. Psychological Trauma: Theory, Research, Practice, and Policy 9: 105–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morry MM, Kito M. (2009) Relational-interdependent self-construal as a predictor of relationship quality: The mediating roles of one’s own behaviors and perceptions of the fulfillment of friendship functions. Journal of Social Psychology 149: 205–222. [DOI] [PubMed] [Google Scholar]
- Morry MM, Hall A, Mann S, et al. (2014) A longitudinal investigation of the friendship model of relational interdependent self-construal. Journal of Social Psychology 15: 401–422. [DOI] [PubMed] [Google Scholar]
- Nes LS, Segerstrom SC. (2006) Dispositional optimism and coping: A meta-analytic review. Personality and Social Psychology Review 10: 235–251. [DOI] [PubMed] [Google Scholar]
- Owens GP. (2016) Predictors of posttraumatic growth and posttraumatic stress symptom severity in undergraduates reporting potentially traumatic events. Journal of Clinical Psychology 72: 1064–1076. [DOI] [PubMed] [Google Scholar]
- Prati G, Pietrantoni L. (2009) Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis. Journal of Loss and Trauma 14: 364–388. [Google Scholar]
- Ramos C, Leal I. (2013) Posttraumatic growth in the aftermath of trauma: A literature review about related factors and application contexts. Psychology, Community and Health 2: 43–54. [Google Scholar]
- Rauch SA, Defever E, Oetting S, et al. (2013) Optimism, coping, and posttraumatic stress severity in women in the childbearing year. Psychological Trauma: Theory, Research, Practice, and Policy 5: 77–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Renshaw TR, Eklund KR, Bolognino SJ, et al. (2016) Bidimensional emotional health in college students: A comparison of categorical and continuous analytic approaches. Journal of Psychopathology and Behavioral Assessment 38: 618–694. [Google Scholar]
- Ringeisen T, Buchward P. (2008) It matters who you turn to: The relational self-construal and communal coping. In: Buchward P, Ringeisen T, Eysenck M. (eds) Stress and Anxiety—Application to Life Span Development and Health Promotion. Berlin: Logos, pp. 75–86. [Google Scholar]
- Roepke AM. (2015) Psychosocial interventions and posttraumatic growth: A meta-analysis. Journal of Counsulting and Clinical Psychology 83: 129–142. [DOI] [PubMed] [Google Scholar]
- Ruini C, Albieri E, Vescovelli F. (2014) Posttraumatic growth, psychological well-being, and distress. In: Martin CR, Preedy VR, Patel VB. (eds) Comprehensive Guide to Post-Traumatic Stress Disorder. Cham: Springer, pp. 1–19. [Google Scholar]
- Schaefer JA, Moos RH. (1998) The context for posttraumatic growth: Life crises, individual and social resources, and coping. In: Tedeschi RG, Park CL, Calhoun LG. (eds) Posttraumatic Growth: Positive Changes in the Aftermath of Crisis. Mahwah, NJ: Lawrence Erlbaum Associates, pp. 99–101. [Google Scholar]
- Scheier MF, Carver CS, Bridges MW, et al. (1994) Revised life orientation test. Journal of Personality and Social Psychology 67: 1063–1078. [DOI] [PubMed] [Google Scholar]
- Schubert CF, Schmidt U, Rosner R. (2016) Posttraumatic growth in populations with posttraumatic stress disorder: A systematic review on growth-related psychological constructs and biological variables. Clinical Psychology and Psychotherapy 23: 469–486. [DOI] [PubMed] [Google Scholar]
- Shand LK, Cowlishaw S, Brooker JE, et al. (2015) Correlates of post-traumatic stress symptoms and growth in cancer patients: A systematic review and meta-analysis. Psycho-Oncology 24: 624–634. [DOI] [PubMed] [Google Scholar]
- Steiger JH. (1990) Structural model evaluation and modification: An interval estimation approach. Multivariate Behavioral Research 25: 173–180. [DOI] [PubMed] [Google Scholar]
- Taku K, McDiarmid L. (2015) Personally important posttraumatic growth in adolescents: The effect on self-esteem beyond commonly defined posttraumatic growth. Journal of Adolescence 44: 224–231. [DOI] [PubMed] [Google Scholar]
- Tedeschi RG, Calhoun LG. (1996) The Posttraumatic Growth Inventory: Measuring the positive legacy of trauma. Journal of Traumatic Stress 9: 455–471. [DOI] [PubMed] [Google Scholar]
- Vázquez C, Pérez-Sales P, Ochoa C. (2014) Posttraumatic growth: Challenges from a cross-cultural viewpoint. In: Fava GA, Ruini C. (eds) Increasing Psychological Well-being in Clinical and Educational Settings: Interventions and Cultural Contexts. New York: Springer Science+Business Media, pp. 57–74. [Google Scholar]
- Wamser-Nanney R, Howell KH, Schwartz LE, et al. (2018) The moderating role of trauma type on the relationship between event centrality of the traumatic experience and mental health outcome. Psychological Trauma: Theory, Research, Practice, and Policy 10: 499–507. [DOI] [PubMed] [Google Scholar]
- Wills L, Petrakis M. (2018) The self in motherhood: A systematised review of relational self-construal and well-being in mothers. Advances in Mental Health 17: 72–84. [Google Scholar]
- Wong CCY, Yeung NCY. (2017) Self-compassion and posttraumatic growth: Cognitive processes as mediators. Mindfulness 8: 1078–1087. [Google Scholar]