

Abstract
Cryoprobe transbronchial lung biopsy (TBLB)/transbronchial lung cryobiopsy (TBLC) is increasingly being described as an alternative to surgical lung biopsy and provides larger lung biopsy samples as compared with conventional TBLB in patients with diffuse parenchymal lung diseases. The technique for cryoprobe TBLB procedure has not yet been standardized, and various authors describe different modalities. However, the use of an artificial airway (rigid bronchoscope or endotracheal tube) is preferred for airway protection. In addition, the use of an occlusion balloon provides safety to prevent excessive bleeding. The exclusive use of rigid bronchoscopy may limit the widespread adoption of this diagnostic modality. We describe a method to perform cryoprobe TBLB with exclusive use of a flexible bronchoscope and utilization of Arndt endobronchial blocker as an occlusion balloon. The procedure was performed in two patients under moderate conscious sedation. Adequate lung biopsies were obtained in both the cases without any complications. This modality may allow safe performance of cryoprobe TBLB with a flexible bronchoscope. Herein, we describe the technical and procedural considerations of this modality.
KEY WORDS: Bronchoscopy, cryotherapy, transbronchial lung biopsy
INTRODUCTION
The use of cryoprobe transbronchial lung biopsy (cryoprobe TBLB)/transbronchial lung cryobiopsy (TBLC), is being increasingly reported for performing bronchoscopic lung biopsy in patients with diffuse parenchymal lung diseases. Studies have reported cryoprobe TBLB yield, similar to surgical lung biopsy.[1] Guidelines on patient selection and technical aspects of this modality are yet not standardized, and a variety of modalities have been described.[2] Exclusive use of a flexible bronchoscope may allow the performance of this procedure, but without the use of an occlusion balloon, this may be associated with unpredictable severe bleeding.[3,4] Some authors have reported the use of single flexible bronchoscope while others have used two flexible bronchoscopes in sequential manner or rendezvous method.[4] Artificial airway management options during the procedure include supraglottic airway, endotracheal tube, or rigid bronchoscope. The use of rigid bronchoscope and a bronchial blocker during the procedure may be preferable to provide airway protection in case of unpredictable bleeding.[5] However, requirement of rigid bronchoscopy and general anesthesia limits the widespread adoption of this diagnostic modality, due to the lack of rigid bronchoscopy expertise at majority of centers. Development of a modality to allow safe and efficacious performance of this procedure with flexible bronchoscopy has the potential to promote widespread utilization of this procedure. We herein describe a novel approach of cryoprobe TBLB under moderate sedation flexible bronchoscopy and use of Arndt endobronchial blocker as the occlusion balloon.
TECHNIQUE
Equipment
The required equipment includes a therapeutic flexible bronchoscope (channel diameter preferably 2.8 mm or greater), 1.9 mm diameter flexible cryoprobe, Cryostation with gas (cryogen) cylinder, Arndt blocker, small diameter flexible bronchoscope in case of difficult nasal negotiation of Arndt blocker using the therapeutic bronchoscope, and airway resuscitation equipment. The operator should be well experienced in handling the airway and performing bronchoscopic endotracheal intubation if there is any need during the procedure.
Patient preparation and procedure
A patient was asked to report fasting to the bronchoscopy suite, and a written informed consent for the procedure was obtained. No premedication was administered. Topical anesthesia included five sprays of 10% lignocaine to the pharynx, and 3 ml of lignocaine gel was instilled into each of the nostrils. Five milliliter of 2% lignocaine was instilled transtracheally using cricothyroid puncture with a 22G cannula. Initial intravenous sedation included a bolus administration of combination of midazolam (2 mg) and fentanyl (75 μg).
After administration of local anesthesia and ensuring that the patient was sedated, a thin video bronchoscope (Olympus P-190, channel diameter: 2.0 mm, outer diameter: 4.2 mm) was initially utilized, and the loop of the Arndt Blocker was secured at the distal end of the video bronchoscope [Figure 1a]. The bronchoscope and the Arndt blocker were then simultaneously introduced through one nostril [Figure 1b], and following negotiation of the vocal cords, the blocker was released into the distal bronchus intermedius, by loosening the loop, and scope was slightly withdrawn. An assistant held the blocker in place at the nostril and confirmed the intactness of inflation and deflation of the blocker. Next, an adult therapeutic video bronchoscope (Olympus BF-1T180, channel diameter: 3.0 mm, outer diameter: 6.0 mm) was introduced through the other nostril [Figure 2a]. The video bronchoscope was positioned proximal to the Arndt blocker; inflation of blocker was confirmed, and then, it was deflated [Figure 2b]. The flexible bronchoscope was then advanced into right lower lobe posterior basal segment (the segment to be biopsied). A 1.9-mm flexible cryoprobe (length: 900 mm, ERBE, Germany) was inserted through the bronchoscope working channel and advanced till resistance was felt. Fluoroscopy was not used. Once resistance was appreciated, the probe was withdrawn by 2 cm, and the foot pedal switch of Cryostation was activated for 5 s. The flexible bronchoscope and cryoprobe were forcefully withdrawn as a single unit while holding the cryoprobe fixed at the biopsy channel entry port. Immediately, the second assistant inflated the Arndt blocker to occlude the right lower lobe basal segments and stabilized the blocker at the nostril so that it does not get displaced. As soon as the bronchoscope with the biopsy attached at the cryoprobe tip was withdrawn, the probe was thawed, and the biopsy sample was preserved in fixative for pathological analysis. The bronchoscope was immediately re-inserted to look for correct positioning of blocker and look for any bleeding. The balloon was deflated after 45–60 s and no significant bleeding occurred. Three biopsy pieces were obtained in a similar fashion, and after ruling out ongoing bleeding, the Arndt blocker was removed. Subsequently, the flexible bronchoscope was removed after performing bronchial toileting. The size of biopsy pieces ranged from 6 to 9 mm and was similar to the biopsies we obtain using rigid bronchoscopic cryoprobe TBLB.[2] The procedure was performed in two patients, and no complications occurred. Thoracic ultrasound was performed on site in both the patients following biopsy and excluded pneumothorax.
Figure 1.
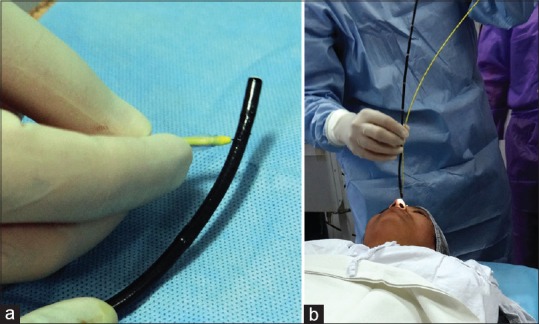
(a) The distal loop of the Arndt blocker is being secured around the flexible bronchoscope. (b) The Arndt blocker secured along the bronchoscope is being introduced through one nostril for placement in the bronchus
Figure 2.

(a) The Arndt blocker and a therapeutic flexible bronchoscope are introduced through separate nostrils for performance of the lung biopsy. (b) The inflation of the balloon is confirmed before obtaining cryoprobe transbronchial lung biopsy
DISCUSSION
We describe an alternative modality for performance of cryoprobe TBLB using flexible bronchoscopy. Studies have reported major bleeding with flexible bronchoscopic cryoprobe TBLB performed without the use of a bronchial blocker.[3] Alternatively, there are also descriptions of the use of a rigid bronchoscope to provide a secured airway during the procedure without the use of a occlusion balloon.[3] However, in our opinion, the use of an occlusion balloon is essential during cryoprobe TBLB. In ideal settings and to maximize procedural safety, rigid bronchoscope as the ventilation conduit, use of an occlusion balloon-like Fogarty balloon catheter to provide tamponade following biopsy, and general anesthesia is preferable, and this allows for a controlled environment to perform the procedure. However, there are concerns that requirements of rigid bronchoscopy and general anesthesia may seriously limit the widespread adoption of this modality. Therefore, development of modalities to simplify the procedure (like performance under flexible bronchoscopy) and simultaneously ensuring safety (herein the use of an Arndt blocker) are important. There is a need to standardize the procedural technique for transbronchial lung cryobiopsy to optimize yield and ensure patient safety. The Expert Statement from the Cryobiopsy Working Group (India) on safety and utility of lung cryobiopsy is an important step toward standardization of this new and exciting procedural technique in pulmonary diagnostics.
Arndt blocker appears to be an ideal blocker in the setting of flexible bronchoscopic cryoprobe TBLB as it is relatively stiff and self-retaining. Therefore, the chances of displacement are less, and maneuverability is easier in case of displacement.[6] In addition, the blocker can be left in place and fixed at nose for a longer time if bleeding is significant and subsequently removed later. This technique requires preferably two assistants along with the primary operator, one for stabilizing and other for inflating the Arndt blocker. We recommend administration of moderate sedation during the procedure to optimize patient comfort and also minimize coughing as that has the potential to increase the likelihood of blocker displacement following cryoprobe TBLB. Another potential addition can be the use of fluoroscopy to confirm the position of freezing the cryoprobe.
Nonetheless, there are certain pertinent issues that need to be highlighted. Cryoprobe TBLB represents an advanced bronchoscopic procedure. This should be performed by a trained operator who is well versed with handling of an unstable airway and performing emergent endotracheal intubation if the need arises. The potential problem with this technique is the absence of an airway conduit (endotracheal tube or rigid bronchoscope) which can be problematic in case of displacement of blocker and bleeding from the biopsied segment. Achievement of lung isolation is a key step in the management of significant airway bleeding, and this can be problematic in the absence of a protected airway. Another unlikely possibility is that in the absence of airway conduit, there is a risk of injury to bronchial or upper airway mucosa by the sticking of the frozen cryoprobe while it is withdrawn along with biopsy piece and flexible bronchoscope. This can be minimized by performing a quick withdrawal of the cryoprobe after biopsy. Furthermore, there are chances of Arndt blocker displacement as the patient may start coughing in response to bleeding in the distal airway.
Although we inserted the second therapeutic bronchoscope through the nostril, oral route may be preferred by certain operators as the risk of tissue getting lost in the nasal cavity on bronchoscope withdrawal may be greater owing to the smaller size of the nasal passage. We used two bronchoscopes with this method (one of which is a 4.2-mm bronchoscope for placement of the blocker), although a single bronchoscope may suffice in many patients. One also needs a trained team with intubation skills, experienced to handle bleeding emergencies in the airways, and more trained bronchoscopy attendants. These requirements might be a hurdle for disseminating this useful modality. Performance of multilobar and upper lobe biopsy can also prove challenging with this method.
CONCLUSION
We have described a modality for performance of cryoprobe TBLB under flexible bronchoscopy with the use of an Arndt endobronchial blocker without an airway conduit. The safety and feasibility of this modality needs further evaluation in large and multicenter studies and comparison with rigid bronchoscopic cryoprobe TBLB techniques to establish its safety and utility. However, at present, we recommend that this novel technique should only be used by operators experienced in airway management and handling of a bleeding airway and preferably with existing experience with performing cryoprobe TBLB.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Dhooria S, Mehta RM, Srinivasan A, Madan K, Sehgal IS, Pattabhiraman V, et al. The safety and efficacy of different methods for obtaining transbronchial lung cryobiopsy in diffuse lung diseases. Clin Respir J. 2018;12:1711–20. doi: 10.1111/crj.12734. [DOI] [PubMed] [Google Scholar]
- 2.Madan K, Mittal S, Gupta N, Hadda V, Mohan A, Guleria R. Cryoprobe transbronchial lung biopsy: How we do it? Lung India. 2018;35:520–2. doi: 10.4103/lungindia.lungindia_52_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dhooria S, Sehgal IS, Bal A, Aggarwal AN, Behera D, Agarwal R, et al. Transbronchial lung biopsy with a flexible cryoprobe during rigid bronchoscopy: Standardizing the procedure. Lung India. 2016;33:248–9. doi: 10.4103/0970-2113.177463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dhooria S, Bal A, Sehgal IS, Aggarwal AN, Behera D, Agarwal R, et al. Transbronchial lung biopsy with a flexible cryoprobe:First case report from India. Lung India. 2016;33:64–8. doi: 10.4103/0970-2113.173066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Madan K, Mehta S, Gupta N, Hadda V, Mohan A, Guleria R. Pneumomediastinum and extensive subcutaneous emphysema after cryoprobe transbronchial lung biopsy. Ann Am Thorac Soc. 2016;13:2101–3. doi: 10.1513/AnnalsATS.201605-395LE. [DOI] [PubMed] [Google Scholar]
- 6.Culp WC, Jr, Kinsky MP. Sequential one-lung isolation using a double arndt bronchial blocker technique. Anesth Analg. 2004;99:945–6. doi: 10.1213/01.ANE.0000132697.22933.8C. [DOI] [PubMed] [Google Scholar]