

Abstract
Aim:
Studies have been done in diversified population, demonstrating the uniqueness of frontal sinus; data related to the Indian population are less. Thus, the present study was aimed to determine the frontal sinus measurement and to assess its forensic application in the Indian population.
Materials and Methods:
A total of 400 individuals with Indian origin (21–30 years) were included in the study. The digitized posteroanterior skull radiographs were obtained and was transferred to Adobe® CS4 extended to measure the dimensions of frontal sinus and orbit for 12 parameters.
Statistical Analysis:
A descriptive statistical analysis was performed.
Results:
The descriptive statistics showed the presence of bilateral frontal sinus in 87.7% and bilateral absence in 8.0% of the individuals and the absence of left and right frontal sinus in 3.3% and 1%, respectively. Maximum population showed high asymmetry index (64.7%); the right side frontal sinus (height, 59.3% and width, 40.8%) was superior to the left side in both males and females. The partial septa among the Indian population were absent for maximum population (55.2%), and supraorbital cells of the frontal sinuses were present on both sides among the Indian population.
Conclusion:
The observation of the present study suggests that the frontal sinus is highly asymmetrical and unique to the individual and hence can be effectively used in personal identification method in forensic anthropology.
Keywords: Frontal sinus, human identification, Indian population, posteroanterior view, radiograph
INTRODUCTION
The personal identification of human remains is of vital importance in forensic investigation such as anthropologic, medical and dental forensic studies especially in cases where soft tissues of human remains become putrid or burnt and DNA analysis cannot be carried out. Several methods such as biometric recognition, cheiloscopy, palatoscopy, poroscopy, DNA typing and finger printing are used for identification of individuals. One of the unique and reliable methods in individual identification is assessment of frontal sinus, because the morphology of frontal sinus is unique to individual.[1]
Anatomically, the frontal sinuses are two pneumatic cavities covered by mucosa, which is embryonically developed from an ethmoidal cell, situated in the posterior part of superciliary arcs, between the internal and external cortical bones of the frontal bone. They are seldom symmetrical; in general, there is a septum between both, which usually deviates from the midline.[2] They are not visible at birth, but begin their development during the second year of life. Radiographically, they become evident at 5 or 6 years of age and continue to grow slowly until puberty and completely developed by approximately 20 years of age.[3,4] The morphology remains practically unchanged during one's entire adult life.
In forensic medicine, the use of frontal sinus radiographs in identifying human skeletal remains is now increasingly applied and accepted technique. In particular, the low frequency of frontal sinus aplasia may be considered a highly significant morphological characteristic for establishing a positive and reliable identification of an individual based on the comparison of antemortem and postmortem radiographs.
Although various studies have been done in diversified population, studies in this regard among the Indian population are limited. In the present study, the variability of frontal sinus pattern among the Indian population was observed and its relative applications in the field of forensic sciences were assessed.
MATERIALS AND METHODS
After obtaining institutional ethical clearance, the digitized posteroanterior (PA) cranial radiographs of 400 healthy adults (200 males and 200 females) of Indian origin aged between 21 and 30 years were observed. The intention of limiting the sample to young adults was based on the fact that frontal sinuses complete their development by approximately 20 years and remain stable. With old age, the walls become thin and appear to be larger.[5,6] Individuals with a history of orthodontic treatment or orthognathic surgery, trauma or any surgery of the skull, any systemic disturbance or hereditary facial asymmetry were excluded from the study. After obtaining thorough clinical history from the individuals, written consent was obtained and PA digital radiographs were taken following standard manufacture's instruction using Kodak 8000 digital panoramic system imagining machine using an exposure of 84 KVP and time of 1.00 s at 10 mA. All radiographs were taken by the same radiologist to overcome any technical error. The radiographic images were saved as high-resolution JPEG file. The digitized radiographs were analyzed using Adobe® Photoshop® CS4 extended software and the dimensions of frontal sinus and orbit for 12 parameters were measured using Ribeiro's method[7] [Figure 1].
Figure 1.
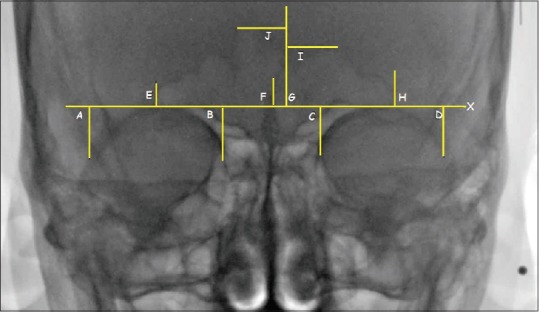
The photograph showing posteroanterior view of the frontal sinus and the orbit with the markings
Analysis of frontal sinus was also done using morphological characteristics as suggested by Yoshino et al., and the morphological characteristics suggested were area size, bilateral asymmetry, superiority of area size, outline of superior borders, partial septa and supraorbital cells.[8] This system assigns a class number to each morphological characteristic, and the frontal sinus patterns of a given person were formulated as a code number obtained by arranging the class numbers in each classification item as serial numbers.
Furthermore, in accordance with Yoshino's and Cameriere's methods, the parameters analyzed in our study were[3,8,9](1) the central septa, (2) the bilateral asymmetry index of height of frontal sinus (the smaller height of the frontal sinus × 100/the larger one of the frontal sinus), (3) the bilateral asymmetry index of the width of the frontal sinuses (the smaller width of the frontal sinus × 100/the larger one of the frontal sinus), (4) the height superiority of the side, (5) the width superiority of the side, (6) the outline of the upper border of the left frontal sinus, (7) the outline of the upper border of the right frontal sinus, (8) the number of partial septa of the left frontal sinus, (9) the number of partial septa of the right frontal sinus, (10) the supraorbital cell of the frontal sinus, (11) the ratio of the left frontal sinus width to the left orbital width and (12) the ratio of the right frontal sinus width to the right orbital width.
For measuring the dimensions of frontal sinus and orbit, a baseline X along the upper limit of both orbital cavities was drawn, and two lines (line I and J) pass through the highest point of the left frontal sinus and the right frontal sinus, respectively, on PA view. Eight lines were drawn perpendicular to the baseline at the specific points. Line H and E delineate the maximum lateral limit of the left frontal sinus and the right frontal sinus, respectively. Line G and F delineate the maximum central limit of the left frontal sinus and the right frontal sinus, respectively. Line D and A delineate the maximum lateral limit of the left orbital cavity and the right orbital cavity, respectively. Line C and B delineate the maximum central limit of the left orbital cavity and the right orbital cavity, respectively. The distances between line C and D and line A and B denote the left orbital width and the right orbital width, respectively. The distances between line G and H and line E and F denote the left frontal sinus width and the right frontal sinus width, respectively. The distances between line I and X and line J and X denote the left frontal sinus height and the right frontal sinus height, respectively.[1]
RESULTS
In this study, the overall percentage of bilateral frontal sinus presence was 87.7% and bilateral absence of frontal sinus was 8.0%, absence of left frontal sinus was 3.3% and absence of right was 1.0%. The percentage distribution and the classifications of 12 parameters assessed for frontal sinus are listed in Tables 1-7. To determine the reliability and reproducibility of frontal sinus measurements, intraobserver and interobserver variation was assessed for 50 samples and no significant difference was observed.
Table 1.
The classification of the central septa among the Indian population
| Classification | Number of samples (%) | Class number |
|---|---|---|
| Absent | 0 | 0 |
| Located in the midline | 112 (30.4) | 1 |
| Sloping to the left side of the midline | 123 (33.4) | 2 |
| Sloping to the right side of the midline | 83 (22.6) | 3 |
| Located in the left side of the midline | 18 (4.9) | 4 |
| Located in the right side of the midline | 9 (2.4) | 5 |
| Crossing the midline from upper left to lower right | 14 (3.9) | 6 |
| Crossing the midline from upper right to lower left | 9 (2.4) | 7 |
Table 7.
The classification of ratio of width of unilateral frontal sinus to unilateral orbit among the Indian population
| Range of ratio | Number of sample (%) | Class number | |
|---|---|---|---|
| Left | Right | ||
| ≥1.0 | 52 (14.1) | 56 (15.2) | 0 |
| 1.0-0.9 | 26 (7.1) | 48 (13.0) | 1 |
| 0.9-0.8 | 41 (11.1) | 41 (11.2) | 2 |
| 0.8-0.7 | 74 (20.1) | 65 (17.7) | 3 |
| 0.7-0.6 | 58 (15.8) | 63 (17.1) | 4 |
| 0.6-0.5 | 62 (16.9) | 45 (12.2) | 5 |
| 0.5-0.4 | 27 (7.3) | 29 (7.9) | 6 |
| 0.4-0.3 | 13 (3.5) | 15 (4.1) | 7 |
| 0.3-0.2 | 1 (0.3) | 2 (0.50) | 8 |
| <0.2 | 14 (3.8) | 4 (1.1) | 9 |
The central septa were classified based on their location [Table 1], which showed 33.4% of population with central septa sloping to the left side of the midline followed by 30.4% showing central septa located in the midline and 22.6% of population with central septa sloping to the right side of the midline. In the present study the asymmetry index of bilateral sinus areas and the ratio (the unilateral frontal sinus area to the unilateral orbital area) were replaced with the asymmetry indices of bilateral sinus dimensions, and the ratio (width of the unilateral frontal sinus to the unilateral orbit) respectively. The superiority of area size was substituted for the unilateral superiority of dimensions. Maximum population showed high asymmetry index (64.7%) ranged between 100 and 80 [Table 2]. In the study, the right side frontal sinus (height, 59.3% and width, 40.8%) was superior to the left side in both males and females [Table 3]. The classification of the outline of the upper border of the frontal sinus among the Indian populations showed scalloped with two arcades on the left side (33.7%) and scalloped with three arcades on the right side (31.5%) [Table 4]. Partial septa among the Indian population were absent for maximum population (55.2%) [Table 5]. Supraorbital cells of the frontal sinuses present on both sides were 53.5% of the Indian population [Table 6]. The ratios of the width of the unilateral frontal sinus to the unilateral orbit were classified into ten grades, showing maximum population 17.7% class number 3 [Table 7].
Table 2.
The asymmetry index of height and width of bilateral frontal sinuses among the Indian population
| Range of asymmetry index | Number of sample (%) | Class number | |
|---|---|---|---|
| Height | Width | ||
| 100-80 | 238 (64.7) | 2215 (58.4) | 1 |
| 80-60 | 101 (27.4) | 108 (29.3) | 2 |
| 60-40 | 10 (2.7) | 27 (7.3) | 3 |
| 40-20 | 2 (0.6) | 1 (0.4) | 4 |
| <20 | 17 (4.6) | 17 (4.6) | 5 |
Table 3.
The classification of the height and width superiority of the side among the Indian population
| Classification | Number of sample (%) | Class number | |
|---|---|---|---|
| Height | Width | ||
| The left frontal sinus superior over the right one | 144 (39.3) | 150 (40.8) | 1 |
| The right frontal sinus superior over the left one | 219 (59.3) | 212 (57.6) | 2 |
| The equivalent between bilateral frontal sinus | 5 (1.4) | 6 (1.6) | 3 |
Table 4.
The classification of the outline of the upper border of the frontal sinus among the Indian population
| Outline of upper border | Number of sample (%) | Class number | |
|---|---|---|---|
| Left | Right | ||
| Absent | 13 (3.5) | 4 (1.1) | 00 |
| Scalloped with 1 arcade | 91 (24.7) | 83 (22.6) | 1 |
| Scalloped with 2 arcades | 124 (33.7) | 114 (31) | 2 |
| Scalloped with 3 arcades | 84 (22.83) | 116 (31.5) | 3 |
| Scalloped with 4 arcades | 40 (10.9) | 36 (9.8) | 4 |
| Scalloped with 5 arcades | 10 (2.72) | 9 (2.4) | 5 |
| Scalloped with 6 arcades | 4 (1.1) | 2 (0.5) | 6 |
| Scalloped with 7 arcades | 2 (0.55) | 4 (1.1) | 7 |
Table 5.
The classification of the number of the partial septa among the Indian population
| Classification | Number of sample (%) | Class number | |
|---|---|---|---|
| Left | Right | ||
| Absent | 223 (60.6) | 203 (55.2) | 0 |
| 1 partial septum | 96 (26.1) | 128 (34.8) | 1 |
| 2 partial septum | 40 (10.9) | 28 (7.6) | 2 |
| 3 partial septum | 9 (2.4) | 9 (2.4) | 3 |
Table 6.
The classification of supra-orbital cells of the frontal sinuses among the Indian population
| Classification | Number of sample (%) | Class |
|---|---|---|
| Absent | 60 (16.3) | 0 |
| Present in the left side | 47 (12.8) | 1 |
| Present in the right side | 64 (17.4) | 2 |
| Present in the both side | 197 (53.5) | 3 |
DISCUSSION
In 1895, Zuckerkandl was the first to note asymmetry of the frontal sinus.[10] Later, Schuller observred in his study that no two persons have identical frontal sinus including monozygotic twins.[11] This was confirmed by Asherson who examined 74 twins (monozygotic and dizygotic) and found frontal sinus to be always different.[12] Reliability of the frontal sinus in identification using two radiographs of the same person was tested by Kullman et al. in 99 individuals.[13] These above-mentioned data suggest frontal sinus being unique to individual, and hence in the present study, we chose frontal sinus as a parameter for assessment and its applicability in forensic science among the Indian population.
The percentage of bilateral frontal sinus absence in our study group was 8.0% (32 persons), the left frontal sinus absence was 3.3% (13 persons) and the right frontal sinus absence was 1.0% (04 persons), whereas the Chinese Han population showed 33% bilateral and 12.6% unilateral absence and the Turkish population showed 3.8% bilateral and 0.8% unilateral absence as compared to the Northern Ireland population which showed 10% bilateral and 2% unilateral absence.[1,9,14] Schuller has emphasized that the presence of metopic suture is associated with the absence of frontal sinuses.[2] The frontal sinus shape is largely determined by the interaction of three factors such as endocrinal, mechanical and factors inherent in the mucus membrane.[15]
We also noted the absence of frontal sinus, which was greater in females when compared to males (male: 4% and female: 12%), and this finding is similar to the findings of the Turkish (male: 1.3% and female: 5%) population, Japanese population (male: 13% and female: 23%) and Alaskan Eskimos (male: 25% and female: 36%).[4]
The central septa in our study showed maximum population (33.4%) sloping toward the left side of the midline, which was in contrast to the study done by Tang et al. on the Chinese Han population which showed maximum population (22.4%) slop located toward the right side of the midline. Taniguchi et al. made combined use of the central septum pattern of the deviation and the frontal sinus pattern and achieved a classification of 204 different types; this classification has a high efficiency for exclusion and suggesting possible usefulness to establish a systemic identification procedure.[16] The central septa parameters show good variability in our samples and can be applied to personal identification.
The outline of the frontal sinus is irregular, and the dimensions of the frontal sinus are more convenient for being exactly measured. We found that the morphology of each frontal sinus of both males and females was different and asymmetrical. Maximum population showed high asymmetry index (64.7%), ranging between 100 and 80, thus confirming the finding of various studies done in the past. Asymmetry for the frontal sinus of both sides is a rule because of the unequal reabsorption of the dipole during sinus development.[14]
In the study, the right side (height, 59.3% and width, 40.8%) frontal sinus was superior to the left side in both males and females, which is in contrast to the study done by Tang et al., where the left frontal sinus was superior over the right one. The existence of one side larger than the other is due to their independent development and the larger sinuses may cross the midline and even overlap the other.[14]
The classification of the outline of the upper border of the frontal sinus among the Indian populations showed scalloped with two arcades on the left side (33.7%) whereas the right side showed scalloped with three arcades (31.5%) followed by scalloped with two arcades (31%). Similar results were found in the Chinese Han population. This finding was in contrast to the Italian population (scalloped with two arcades: 12% left; smooth: 40% right). A previous study has shown that sinus is generally larger in males, although, in females, the scalloped arcades of upper border are smaller and more numerous.[15]
Partial septa among the Indian population were absent for maximum population (55.2%), which was in accordance with the results obtained among the Chinese Han population and Italian population.[1,14]
Supraorbital cells of the frontal sinuses were present on both sides among the Indian population. Similar results were found among the Chinese Han population whereas contrasting results were observed in the Italian population, which showed the absence of supraorbital cells in frontal sinus.[14]
The ratios of the width of the unilateral frontal sinus to the unilateral orbit showed maximum population (20.1% left and 17.7% right) class number 3 and minimum population showed class 8. The present study observed that the majority of the parameters were similar to the Chinese Han population. This is probably because both Indian and Chinese Han population belong to Caucasoid race.
CONCLUSION
The use of frontal sinus radiographs in identifying human skeletal remains is now increasingly applied and accepted technique in forensic anthropology. In particular, the low frequency of frontal sinus aplasia may be considered a highly significant morphological characteristic for the positive identification of an individual in a given population. Digitalized storage of morphological characteristic of frontal sinus of every individual of a defined population will be a big boon in the field of forensic sciences. The methodology used in the present study is simple, cost effective method in providing high accuracy in human identification using frontal sinus. Norms should be laid down by the governing bodies to store all the records of every individual which could help in his/her identification in medico-legal cases and mass disasters. Present study showed different morphology of frontal sinus in each individual thus proving uniqueness in forensic identification if ante mortem record exists.
However the study has certain limitation like we did not categorize the participants region wise to know if any difference is observed between each region of India. This was pooled sample from all parts of the country. Larger sample size will allow us to categorize and compare if any difference exists, which will add up to the existing data. Further using conventional radiographs have certain limitations like causing vertical angle distortion, might also alter the reading, but we have taken care of this by standardizing the technique.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Tang JP, Hu DY, Jiang FH, Yu XJ. Assessing forensic applications of the frontal sinus in a Chinese Han population. Forensic Sci Int. 2009;183:104.e1–3. doi: 10.1016/j.forsciint.2008.10.017. [DOI] [PubMed] [Google Scholar]
- 2.Jose MP, Ralmundo NA, Jose MV, Patick M, Ana CT. Anatomoical variations of the frontal sinus. Int J Morphol. 2008;26:803–8. [Google Scholar]
- 3.Cameriere R, Ferrante L, Mirtella D, Rollo FU, Cingolani M. Frontal sinuses for identification: Quality of classifications, possible error and potential corrections. J Forensic Sci. 2005;50:770–3. [PubMed] [Google Scholar]
- 4.Belaldavar C, Kotrashetti VS, Hallikerimath SR, Kale AD. Assessment of frontal sinus dimensions to determine sexual dimorphism among Indian adults. J Forensic Dent Sci. 2014;6:25–30. doi: 10.4103/0975-1475.127766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tatlisumak E, Ovali GY, Asirdizer M, Aslan A, Ozyurt B, Bayindir P, et al. CT study on morphometry of frontal sinus. Clin Anat. 2008;21:287–93. doi: 10.1002/ca.20617. [DOI] [PubMed] [Google Scholar]
- 6.Cristiane RR, Nader N. Anatomo-radiological and morphometrical study of the frontal sinus in humans. Braz J Morphol Sci. 2004;21:53–6. [Google Scholar]
- 7.Ribeiro Fde A. Standardized measurements of radiographic films of the frontal sinuses: An aid to identifying unknown persons. Ear Nose Throat J. 2000;79:26–8. 30, 32-3. [PubMed] [Google Scholar]
- 8.Yoshino M, Miyasaka S, Sato H, Seta S. Classification system of frontal sinus patterns by radiography. Its application to identification of unknown skeletal remains. Forensic Sci Int. 1987;34:289–99. doi: 10.1016/0379-0738(87)90041-7. [DOI] [PubMed] [Google Scholar]
- 9.Cameriere R, Ferrante L, Molleson T, Brown B. Frontal sinus accuracy in identification as measured by false positives in kin groups. J Forensic Sci. 2008;53:1280–2. doi: 10.1111/j.1556-4029.2008.00851.x. [DOI] [PubMed] [Google Scholar]
- 10.Zuckerkendl E. Paris: G. Masson; 1895. Anatomy of the frontal sinuses. In: Pathological Normal Anatomy of the Nasal Fans and their Annexes Pneumatics; pp. 349–61. [Google Scholar]
- 11.Schuller A. A note on the identification of skulls by X-ray pictures of the frontal sinuses. Med J Aust. 1943;1:554–7. [Google Scholar]
- 12.Asherson N. London: Lewis; 1965. Identification by Frontal Sinus Prints: A Forensic Medical Pilot Survey. Iillustrated ED. [Google Scholar]
- 13.Kullman L, Eklund B, Grundin R. Value of the frontal sinus in identification of unknown persons. J Forensic Odontostomatol. 1990;8:3–10. [PubMed] [Google Scholar]
- 14.Aydinlioǧlu A, Kavakli A, Erdem S. Absence of frontal sinus in Turkish individuals. Yonsei Med J. 2003;44:215–8. doi: 10.3349/ymj.2003.44.2.215. [DOI] [PubMed] [Google Scholar]
- 15.Buckland-Wright JC. A radiographic examination of frontal sinuses in early British populations. Man New Series. 1970;5:512–7. [Google Scholar]
- 16.Taniguchi M, Sakoda S, Kano T, Zhu BL, Kamikodai Y, Fujita MQ, et al. Possible use of nasal septum and frontal sinus patterns to radiographic identification of unknown human remains. Osaka City Med J. 2003;49:31–8. [PubMed] [Google Scholar]