

Abstract
This paper reviews economic aspects of selected HIV/non-communicable disease (NCD) service delivery integration programs to assess the efficiency of integration in limited capacity settings. We define economies of scope and scale and their relevance to HIV/NCD integration. We summarize the results of a systematic review of cost and cost-effectiveness studies of integrated care, which identified 12 datasets (9 studies) with a wide range of findings driven by differences in research questions, study methods, and health conditions measured. All studies were done in Africa and examined screening interventions only. No studies assessed the cost of integrated, long-term disease management. Few studies estimated the cost-effectiveness of integrated screening programs. The additional cost of integrating NCD screening with HIV care platforms represented a 6%−30% increase in the total costs of the programs for non-cancer NCDs, with cervical cancer screening costs dependent on screening strategy. We conducted 11 key informant interviews to uncover perceptions of the economics of HIV/NCD integration. None of the informants had hard information about the economic efficiency of integration. Most expected integrated care to be more cost-effective than current practice, though a minority thought that greater specialization could be more cost-effective. In the final section of this paper, we summarize research needs and propose a “minimum economic dataset” for future studies. We conclude that, while integrated HIV/NCD care has many benefits, the economic justification is unproven. Better information on the cost, cost-effectiveness, and fiscal sustainability of integrated programs is needed in order to justify this approach in limited-resource countries.
Keywords: cost, cost-effectiveness, HIV/NCD integration
Introduction
Integrated care for HIV/AIDS and non-communicable diseases (NCDs) is defined in this Supplement, entitled “Research to Guide Practice: Enhancing HIV/AIDS Platform to Address Non-Communicable Diseases in sub-Saharan Africa”, as the coordination, co-location, or simultaneous delivery of HIV services (including antiretroviral drug treatment [ART]) and screening and/or treatment for various NCDs among people living with HIV/AIDS.1 The literature on HIV/NCD integration has focused predominately on cardiovascular disease risk reduction, cancer screening and treatment, and management of comorbid mental health disorders.2 A number of investigators have argued that integrated care has the potential to improve both HIV and NCD health.3 This potential has become a desiderata in light of limited domestic and external funding to address rising NCD and HIV burdens.4 However, numerous salient questions remain before integrated care can be recommended as standard practice, especially in very resource-constrained, endemic or hyperendemic African countries. These questions include what scope of services and at what level integration should be attempted in order to achieve technical, productive, and allocative efficiency.5 Impacts on health outcomes and cost per patient of integrated services need to be evaluated to suggest how to best preserve donor and public sector investments and develop fiscally sustainable solutions.
Optimistic assumptions have been made about the possible economies of scope and scale that are achievable with integrated chronic disease care, and preliminary data presented here suggest this optimism may be warranted. Conversely, there is evidence of economic inefficiency when providing complex care for multiple morbidity in resource limited settings.6 Assumptions about achieving greater efficiencies in delivering quality integrated chronic care have not been sufficiently evaluated. In this paper, we review the economic principles that make integration of HIV/NCD care attractive in theory, summarize the limited literature on the cost and cost-effectiveness of integrated HIV/NCD care, and present the perspectives of various global and national stakeholders on the economics of integration. We then propose a research agenda and a minimum economic dataset for future studies of HIV/NCD integration.
The economics of integration: economies of scale and scope
The economic rationale for integrating NCD and HIV care stems from maximizing efficient health production through economies of scale and scope. Both kinds of efficiencies are theoretically possible to achieve through integration of HIV and NCD services. These efficiencies are measured by means of the “unit cost,” defined as the total expenditure to produce one unit of a product or service. Unit costs combine fixed costs (which are unchangeable in less than one year, such as facilities) and variable costs (which are changeable within one year, such as most labor or consumable supplies).
Economies of scale are depicted with a U-shaped curve (Figure 1). Economies of scale in health care delivery may arise from: spreading fixed costs (facilities, equipment) over more treatment cases; learning by doing, such as increased experience or repetition of treatments; lowering supply input prices through bargaining power, purchasing in bulk, strengthening supply chains; and creating opportunities for specialization. Diseconomies may arise from over-crowded clinics, longer wait times, and disenrollment; and from provider burnout due to expanding the range of services offered in a very constrained setting. Recent studies have found larger HIV prevention and treatment programs are associated with decreased unit costs across multiple countries and programs.7,8
Figure 1.
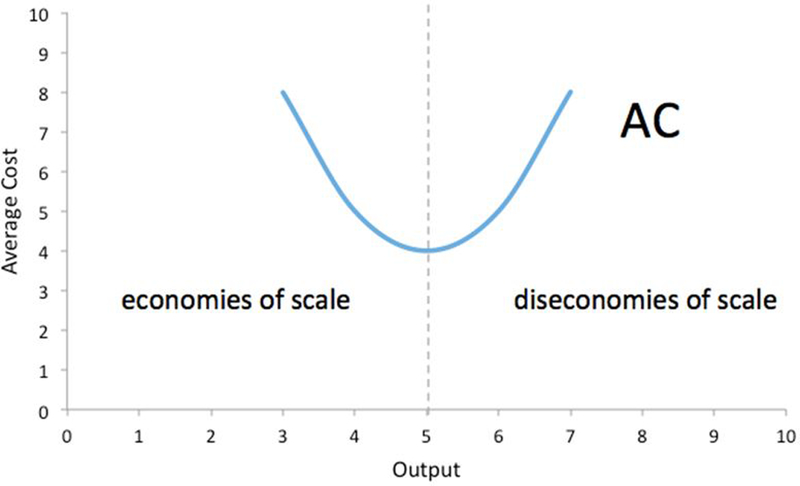
Economies of Scale
As the number of outputs grow, the average unit cost (AC in the figure) decreases as production rises until the point of highest production efficiency. As production rises past this point the average unit cost increases, providing diseconomies of scale.
Economies of scope are efficiency gains that occur from producing several outputs together, producing cost savings by using proportionally fewer inputs than when the products are produced separately (Figure 2). Economies of scope can arise when producing multiple types of services reduces the unit costs, either through cost complementarity or sharing fixed costs like overhead and other indivisible resources.9 Economies of scope are already possible within HIV care as programs often include multiple different services. In programs that produce highly complementary services cost savings may even occur.10,11 For instance, some programs are clinically recommended to integrate, like HIV and tuberculosis screening of asymptomatic patients, and also do not require a large burden of extra inputs beyond what is needed for stand-alone programs.12,13 Finally, even if unit costs for integrated care are higher than for non-integrated care, HIV integration between HIV and general health services such as primary care and family planning can be cost-effective if joint production yields better health outcomes.
Figure 2.
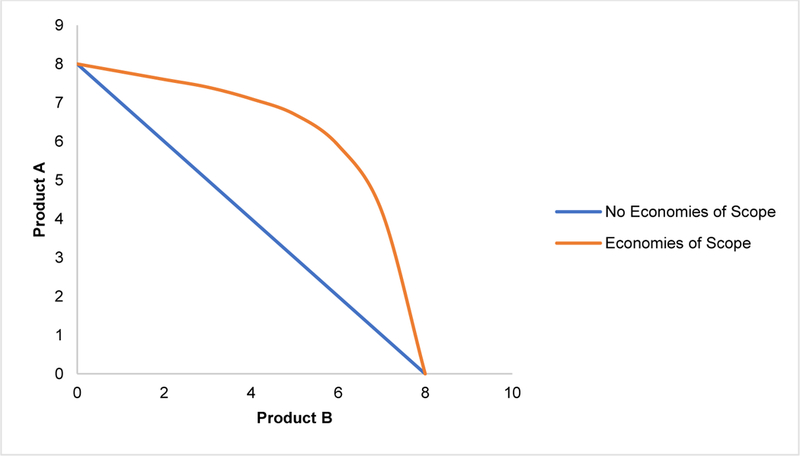
Economies of Scope
The lines show possible production possibility curves for two products while holding cost constant. The blue line shows the maximum possible goods produced for a certain cost if only products A or B are produced, or if some of both products are produced, with no economies of scope present. The orange line shows the maximum possible amount of Products A or B, or both, for a certain cost when economies of scope in production exist.
Review of Cost and Cost-effectiveness Studies of HIV/NCD Integration
Methods
We reviewed the current economic evidence for integrated HIV/NCD strategies in low and middle income countries (LMIC), focusing on the scope of conditions and countries addressed by this journal supplement. We conducted a systematic review following the Cochrane Collaboration14 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (see Supplemental Content Appendix A for search strategy and protocol).15 Briefly, we searched Medline, EMBASE, Global Health database and Econlit from January 1st, 2007 to March 1st, 2018 for studies that reported the results of integrated HIV/NCD care including economic outcomes. To obtain unpublished primary costing data, in early 2017, we surveyed colleagues to obtain a list of integrated HIV/NCD studies in progress and contacted the primary investigator. Four study groups responded to our request for primary costing data for integrated HIV/NCD treatment services [CDC-Malawi, Ampath, ICAP-Aga Khan, and Linkages].
Studies were eligible for inclusion if they reported cost data on the integration of NCD screening and/or care into HIV programs. NCD program terms included counseling, health promotion, screening, treatment and/or adherence monitoring. NCDs were defined as hypertension, diabetes, hyperlipidemia, cervical cancer screening and/or depression, within HIV programs, with an economic evaluation in at least one low- or middle-income country. Data were extracted by two independent reviewers. We used the Drummond Checklist to score the quality of the economic evaluation.16 Unit cost data for integrated services were abstracted from the cost analyses. All cost data were adjusted to 2013 USD to facilitate comparison across studies.
Findings of the Review
Our search strategy identified 896 abstracts for review. Data extraction forms were completed for 22 full-text articles, of which 12 reports (nine studies) met the inclusion criteria (see Appendix A, figure 1). Current evidence on the cost of HIV/NCD integration is limited to integrated screening within HIV programs in Sub-Saharan Africa. Five studies included cervical cancer screening (including dysplasia), four included cardiometabolic screening and one screened for depression. No studies clearly evaluated the costs of integrating NCD care (treatment, adherence, retention) within an HIV program. Most of the cervical cancer screening programs were facility-based, while the cardiometabolic screening were all community-based. All but one study took a provider prospective. One study took a societal perspective by incorporating costs outside the health system such as patient time and transport. Only three studies (all of cervical cancer screening) reported effectiveness outcomes (Table 1).
Table 1a.
Unit cost data for integrated cardiometabolic HIV/NCD programs (2013 USD)
| Study (year conducted) |
Program | NCD Component | Personnel | Country | n (population) |
Integrated Unit Costa |
Unit cost allocated to NCDa (%)b |
Quality* |
|---|---|---|---|---|---|---|---|---|
|
SEARCH Collaboration |
Blood pressure, diabetesg | |||||||
| (2011)18 | 5 day community health campaign HTCc | Mobilizers and counselors | Uganda | 2282 (parish) | $39.10 | $2.49 (6%) | + | |
| (2013–2014)19 | 2 week hybrid (community and home-based) campaign HTCc | Mobilizers and counselors | Uganda, Kenya | 4505 (national) | $20.10 | $1.14 (6%) | ++ | |
| (2014)20 | 6 day community-led health campaign HTCc | Village leaders, mobilizers, counselors | Uganda | 1584 (parish) | $5.81i | Not Reported | ++ | |
| SMART 3 (2011)22 | 4 week home vs 1-day mobile campaign HTCd | Blood pressure, diabetesg | Counselors | Lesotho | 2563 (district) | $16.68 (home) 18.33 (mobile) |
Not Reported | + |
| Bophelo! (2009)21 | 10 month mobile HTC at workplace HTCe | Blood pressure, diabetes, dyslipidemia, hemoglobin, obesityg | Counselors | Namibia | 5734 (district) | $65.72 | $12.31 (19%) | + |
| Linkages (2015)17 | 1 month Home-based HTCf | Blood pressure, diabetes, dyslipidemia, obesity, depression, smokingh | Mobilizers, nurse and counselors | South Africa | 570 (district) | $13.30J | $3.95 (30%)J | ++ |
Per person screened
% NCD total = (NCD unit cost)/(Integrated Unit Cost)
Includes CD4 testing cost for positive identified cases, malaria rapid test. 2011 and 2014 campaign included rapid PCR-based TB sputum testing
Includes CD4 testing cost for positive identified cases, clinical tuberculosis, family planning
Includes rapid hepatitis B, syphilis and clinical tuberculosis
Includes CD4 testing cost for positive identified cases
point of care glucose level
point of care glucose, lipid test, PHQ9 screen and risk factor (including smoking) questionnaire
scaled estimate based projected costs using governmental resources without SEARCH support; does not specify if CD4 testing cost included. Overall operating estimate
operational costing model, removing research-related costs and assuming task-shifting from professional counselors to lay staff (community care workers)
We used the Drummond Checklist in creating guidelines to assess the quality of economic evaluation (Supplement: Table S1) A score was assigned to each study to measure quality of economic analysis as follows:
- 1–8 Drummond checkmarks
- 9–12 Drummond checkmarks
- >12 Drummond checkmarks.
HTC – HIV testing and counseling
There was limited evidence of the cost or cost-effectiveness of integration among non-cancer NCDs, including hypertension, diabetes, and associated risk factors, in HIV.17–22 All four studies identified were community-based HIV testing programs. While the absolute costs of screening varied widely depending on the site, we provide the amount attributable to NCD screening in both absolute terms and percentage terms (Table 1; (NCD unit cost)/(Integrated Unit Cost)). The estimated additional per-person cost of adding NCD screening to a non-facility program ranged from 6–30% of total HTC program costs (Table 1).17–19,22
The SEARCH platform in Kenya and Uganda (a multiphase integrated HIV/NCD community-based screening campaign with home-based follow-up) was one of the largest integrated programs studied. The attributable cost for hypertension and diabetes screening was USD 1.14 (or 6%), on top of a cost for HIV counseling and testing of USD 20.10. A majority of costs were counted as fixed, and personnel represented 50% of total costs.19 De Beer et al evaluated a mobile van-based integrated program in South Africa with an additional NCD screening cost of USD 12.31 (19% of the total screening cost of USD 65.72) and an additional time burden of 15 minutes (~20% of program time).21
The Linkages study, a prospective study of home-based HIV testing and linkage to care in South Africa, estimated the cost per NCD screening to be USD 3.95 (30%) for a total cost of USD 13.31 for an integrated HIV/NCD screening program.17 The NCD component of Linkages included screening for hypertension, diabetes, tobacco consumption, hyperlipidemia and depression, providing the broadest integrated screening services in the studied settings.23 There was a 15–20% decrease in the number of clients able to be screened per day with integration, based on a time assessment.
For cervical cancer screening among HIV-positive women on ART, two studies explored the cost of integrating several cervical cancer screening methods into existing HIV treatment programs. For visual inspection with acetic acid (VIA) the cost ranged from USD 3.24–3.67, Papanicolaou smear (Pap) cost USD 8.17–24.08, and human papillomavirus (HPV) testing costs ranged from USD 17.92–54.34.24,25 Three studies reported additional costs ranging from USD 18 – 26 per visit per person receiving integrated cervical cancer screening (PAP or VIA) within HIV testing and counseling (Sexual Reproductive Health/HTC strategies).26–28A number of cervical cancer screening strategies indicated a higher proportion of fixed costs compared to HIV services, since cervical cancer screening may depend heavily on staff and capital costs. However, in these instances, staff salaries were reported as fixed costs that could possibly change with more creative staffing arrangements, such as task-sharing.11,26–28 Variable costs for Pap testing included cytology, transport, and specimen collection.24,27
Few studies estimated cost effectiveness. In one instance in rural Zambia, integrated HIV-cervical cancer screening with enhanced counseling (including motivational interviewing and linkage to care) was more cost-effective compared with a non-integrated standard of care which included stand-alone HIV-testing and referral to other services.26 This finding relied heavily on model assumptions of projected treatment costs and morbidity/mortality based on the study’s 6-month outcome (HTC and cervical cancer uptake). From the societal perspective, integrating cervical cancer screening within an HIV treatment program in Kenya may be cost-saving; Vodicka et al. found decreased costs of cervical cancer screening strategies in an integrated platform compared to stand-alone through reductions in overhead costs, patient transport and time burden.25 Based on the same costing analysis, Zimmermann et al projected lifetime societal costs ranging from USD 192–218 by integrated varying screening and preventative cryotherapy in an HIV treatment program, with around 17 years projected life expectancy.29
In sum, the increased unit cost of the non-cancer NCD screening integrated with HIV care platforms ranged from USD 1.14 to 12.31, representing a 6%−30% increase in the total costs. Cervical cancer screening costs ranging from USD 3.24 to 54.34 depending on screening strategy. This review did not identify an economic evaluation of integrating NCD care services following screening in an HIV program. An additional evidence gap is the lack of studies estimating the cost of facility-based integration for non-cancer NCDs, given the reality that management of NCDs is usually facility-based. Lastly, few studies coupled costs with outcomes data to estimate efficiency and benefit; only one study provided a measure of improved health outcomes from cervical cancer screening.
This review has numerous limitations. For the non-cancer NCD integration studies, significant differences in study design and reporting limit the ability to compare programmatic costs across time and settings. The studies reviewed did not allow a direct comparison of integrated programs with programs that provided all components of integrated care separately. Other limitations included vague reporting on quantities and prices, unclear methods of time allotment for NCD integration, and limited data on efficacy and adjustments for differential timing of screening activities. The scope of the review focused on a limited number (5) of disease conditions. Future work would expand this search to a broader range of diseases.
Qualitative Assessment of Economics of HIV/NCD Integration
To better understand the expectations about the cost-effectiveness of integrated HIV/NCD care with the reality we found in the literature, we conducted a small number of focused interviews to explore the understanding and perceptions of the economics of HIV/NCD integration with key interested parties. The purpose was to inquire about the most likely sources of economies of scale and scope from using an integrated model, if at all, and learn of any first-hand observations regarding the existence of such efficiencies in service delivery.
Methods
We conducted semi-structured, in-depth interviews with 11 individuals specializing in HIV program implementation, HIV/NCD integration and/or economics from a variety of backgrounds, including: ministry of health (n=2), donors (2), in-country implementers (2), policy advisor (1), and academics/researchers focused on HIV (2) and health economics (2). Respondents worked in Kenya, Malawi, South Africa, Swaziland, and globally. We asked the respondents ten questions (Supplemental Content Appendix B) about integration of HIV/NCDs, initially to ascertain their perspectives and knowledge, and then to learn more about their understanding and impressions of the economic aspects of integration. Responses were transcribed and thematically analyzed to identify notable similarities and differences across respondents.
Results
Half of the respondents had direct experience integrating HIV/NCD services. Settings for this experience ranged from minimal NCD screenings conducted at HIV clinics to more complex integration of NCD and HIV, including treatment services. Most experiences were basic screening of NCDs within a vertical HIV program. Among the respondents, hypertension was most commonly screened for, followed by diabetes and cervical cancer. Treatment was often provided through referrals to other health facilities, not at the HIV clinic.
According to respondents, the three most common challenges facing national health programs trying to integrate HIV and NCDs were funding streams, drug procurement for medical management of NCDs, and monitoring and evaluation systems. Country level managers and ministry officials reported struggling to make services and chronic care more accessible for patients because they had to work around vertical funding streams. A related challenge was the cost of NCD treatment itself. The cost to procure the range of medications needed to treat cardiovascular disease, diabetes, and cancer far exceeded health budget lines. Moreover, there was a concern that NCD expenses would compete with other health needs. However, respondents consistently mentioned screening as a cost-effective intervention.
Respondents showed a clear understanding of cost effectiveness by providing an accepted definition, but responses varied about its importance in guiding the appropriateness of integrated care. Several respondents (donors, ministries of health, and health economists) indicated that program cost-effectiveness was of primary importance. Their view was that decision makers with limited funds need to be responsible and prioritize where healthcare funds are spent, such as what to screen and when. Others reported that cost is just one of many factors that must be considered. Some offered an ethical rationale for providing NCD treatment.
Some respondents indicated that NCD treatment is often not funded because is it not considered cost effective. There was a general belief that there would initially be higher costs to integrate treatment and care for patients with HIV/NCD comorbidity. Among the additional costs mentioned were staff training, tools, supplies, treatment, monitoring systems, and laboratory tests. The up-front costs were expected to be high for service design and training, while full service integration was expected to eventually cause costs to fall.
Nearly all respondents suggested that integration could be done efficiently and cost-effectively, if certain conditions are met. For instance, careful budget planning is necessary to support the rollout of integration, and the most effective integration model probably varies for each setting. An alternative point of view emerged suggesting that integration does not necessarily lead to efficiency; rather, that specialization leads to efficiency gains. Arguments for this viewpoint pointed to more challenging workflow for integrated service delivery. Most respondents cautioned that integration is complex and multilayered and must be examined in context for costs and cost-effectiveness to be demonstrated.
Respondents’ perceptions of the literature were consistent with the findings of our review that there is a serious shortage of data demonstrating cost effectiveness or cost savings from integration. One donor indicated that much of the cost data they use to prioritize funding is outdated, and the field is changing rapidly, even within two to three years. There is a need for primary cost data from a variety of countries and settings, including clinical services, commodities, and lab services.
Respondents made suggestions:
Longitudinal data would be valuable to look at the long-term costs and benefits of HIV/NCD treatment.
Data is needed on who pays for NCD treatments and how much; patient costs as well as program costs must be collected.
There is a need to compare NCD treatment costs within an integrated system to a standalone system.
Purchasing NCD and HIV treatment drugs together may provide economies of scale.
What are the critical gaps in knowledge on the economics of HIV/NCD integration?
Our systematic review has highlighted the divergence of methods and findings within the small literature on the cost and cost-effectiveness of integrated care. To address the knowledge gaps related to the economics of integration and encourage consistency and comparability in future research, we have proposed a minimum economic dataset (Table 2) for any economic evaluation of integrated care, and a set of research questions for understanding the economics of HIV/NCD integration. Ideally these data would become part of routine epidemiological studies and program evaluations and these research questions would be integrated into HIV outcomes research. Evaluation of economies of scale and scope require reporting of program size, breakdown of costs, and size and cost of comparable standalone programs, as comparators. In the absence of comparable standalone programs, economies of scope will be difficult to measure.
Table 2.
Recommendations for minimum economic dataset to be collected in studies of HIV/NCD integration
| Major components | Scale economies | Scope economies | Efficiency |
|---|---|---|---|
| Personnel | Size of program (clients) | Total cost of HIV care alone | Number of cases screened/yr |
| Equipment | Number of staff | Total cost of NCD care alone | Proportion aware of NCDs |
| Drugs and other consumables | Quantities of resources | Total cost of HIV + NCD care | Proportion on NCD treatment |
| Indirect (overhead) costs | Breakdown fixed/variable costs | Proportion with controlled NCD | |
| Patient out-of-pocket costs | Size of HIV program (clients) | (Comparison of NCD and HIV outcomes) | |
| Payer information | Size of HIV + NCD program (clients) |
This review has addressed the efficiency of delivering clinical services using integrated (as compared to non-integrated) care models. Cost-effectiveness analysis (CEA) is a flexible approach that can be used to assess various means by which to deliver the same types of services for NCDs. Cost-effectiveness ratios for process outcomes or intermediate clinical outcomes (e.g., cost per case of cervical dysplasia detected) are probably adequate for this sort of CEA; it may not be necessary to extrapolate to long-term outcomes (like deaths or DALYs averted from CVD or cancer) if the efficiency of producing certain services is the policy question.
As a separate problem, related to but outside the scope of this review, we know very little about cost-effective approaches to managing NCDs in PLHIV, whose risk profile is in some cases dramatically different than the general population. CVD risk provides a useful example here. Analyses conducted for Disease Control Priorities, 3rd Edition, and other publications have produced recommendations for screening and medical management of CVD risk factors in LMIC populations.30 Key lessons learned from these analyses are, (1) that baseline level of risk matters greatly in determining whether specific treatments are cost-effective, and (2) that combination therapy is generally preferred to focusing on single risk factors like blood pressure or cholesterol.30
Unfortunately, because the CVD risk profile of PLHIV is not comparable to the general population, existing guidelines may recommend care that is not cost-effective. PLHIV may be considered to have higher risk of CVD due to inflammatory effects of the virus itself, although in the African context PLHIV are (currently) a relatively young and cardio-metabolically healthy group compared to the general population. Reflecting these uncertainties, the development and validation of CVD risk calculators in PLHIV remains an active area of research.31 Further, the impact of ART itself on NCD risk is not well understood;32 it is plausible that viral suppression may reduce inflammation and hence reduce some risks (such as the risk of vascular disease or cervical dysplasia),33 while some ART regimens may precipitate mood disorders or induce metabolic derangements that increase risk of vascular disease.34
Given all these uncertainties, it would be perilous simply to apply the conclusions of CEAs conducted on CVD interventions in the general population to the HIV population. CEAs that assess CVD management strategies among HIV-affected populations, particularly African populations, are urgently needed. These studies should generally be modeling long-term outcomes (e.g., measured in deaths or DALYs) rather than process and intermediate outcomes.
We identify four major research needs in this area for LMICs. First, a range of additional economic evaluations are needed. They include: i) costing of multiple models of integrated strategies with linkage across levels of the treatment cascade; ii) cost-effectiveness analyses that compare standard care to integrated care, preferably using multi-site, longitudinal clinical and epidemiological studies; iii) microeconomic studies that can generate production functions across different types of facilities to demonstrate economies of scope and scale; and iv) methodological advances that incorporate those supply-side characteristics into existing health economic evaluations.
A second major need is better longitudinal data on NCD risk and outcomes in PLHIV. Third, studies are needed that assess the interactions of multiple NCDs. Fourth, from a technical standpoint, the methods, data sources, and assumptions of the HIV and NCD economic modeling communities need to be harmonized and standardized. Economic analysis from integration of HIV services with other chronic diseases, such as tuberculosis, may be a useful guide for NCD-HIV integration economic studies.
Conclusions
Economic evaluation of new service delivery models can guide countries seeking to offer efficient and effective HIV programs. The differentiated service delivery model that offers care to PLHIV who are stable on ART with suppressed viral loads will be an important test case of cost-effectiveness, especially when the goal is integration with community and other primary health care. How to manage the long-term chronic care needs for both HIV-positive and HIV-negative persons in a financially sustainable manner presents clear choices among care sites, populations reached, and services provided. Economic assessment of optimal services and policy packages will be most useful when it is fine-tuned to the population needs and projected resources available, incorporating the most cost-effective interventions, settings, and regions. Until such assessments are more widely available on a more comprehensive basis, the notion that integrated care for HIC and NCDs is cost-effective is more theory than reality.
Beyond economic assessment of integrated service delivery models, it is useful to take a step back and question how to best serve and meet population-wide needs. Even when integrated service delivery models are demonstrated to be cost-effective, they may not be affordable in the near-term. Many countries are only beginning to identify and provide NCD services to their populations in need. The scale and scope of those services will remain very limited until new funding sources are in place. Universal health coverage provides the framework for countries to choose a chronic care service model that best suits their choice of health system platforms, while also aiming to provide those services to the whole population. Integrated delivery within HIV services programs may be understood best as a temporary response to a funding model in transition.
Supplementary Material
Table 1b.
Unit cost data for integrated cervical cancer HIV/NCD programs
| Study (year conducted) |
Program | NCD Component | Personnel | Country | n (population) |
Integrated Unit Costa |
Unit cost allocated to NCDa (%)b |
Quality* |
|---|---|---|---|---|---|---|---|---|
| Right to Care (2013)27 | 12 month mobile clinic service HTC, SRHc | Pap smear, blood pressure | Primary care nurse and counselor | South Africa | 1,296 (district) | $76.03 | Not reportedf | + |
| Integra initiative11,28 (2010–2011) | Multi-country evaluation of varying models of HTC, HIV treatment, FP and PNC integration | Pap smear or VIA | Unspecified | Kenya and Swaziland | 40 health facilities (country) | Not reportede, | $26.29 (not reported) | ++ |
| Pap smear screen with integrated SRH and enhanced follow-up and partner testing26 | 6 week randomization with varying outreach HTC, HIV treatment, SRHd | Pap smear^ | Nurse | Zambia | 2043 (Urban Clinics) | $112.00 ** | Not reportedg | + |
| Comparison of cervical cancer screening24 | HIV treatment program | VIA, HPV, Pap smear^ | Primary care nurse | South Africa | Various inputs from tertiary public hospital (country) | Not reported** | VIA $3.67h
Pap $8.17h HPV $54.34h Colposcopic biopsy $67.71h |
+++ |
| Comparison of cervical cancer screening | HIV treatment program | |||||||
| (2014)25 | VIA, HPV, Pap smear | Nurse | Kenya | 148 (district) | Not reported | VIA $3.24i HPV $17.92i Pap $24.08i Hybrid $30.5i |
+ | |
| (2014)29 | Preventative cryotherapy, VIA, HPV, Pap smear^ | Nurse | Kenya | Various inputs from tertiary public hospital (country) | Not reported** | Lifetime costs reportedj | +++ | |
Per person screened
% NCD total = (NCD unit cost)/(Integrated Unit Cost)
Includes clinical tuberculosis, family planning, STI and candidiasis symptom screen
Includes HTC, family planning, STI care and treatment, TB testing, CD4 testing, ART, psychosocial support, partner referral
Overall mean unit cost per service $18.73 for HTC, $74.21 for HIV treatment across all models of integration
Average variable cost of Pap smear per person estimated $6.94; attributable fixed (and total) costs not reported
Cost per client cervical cancer screening estimated at $18.00 at vertical reference clinic site, were assumed not variable at integrated clinic sites and costs were not included in technical efficacy.
Functional Limit scenario represents the maximum number of procedures estimated to be possible. Alternate caseload reported is ‘study statistic scenario’ – as observed during the validation study.
Societal prospective, including direct non-medical (patient transport, expenses) and indirect costs (loss earnings, child/elderly care, patient wait time). Per-screening cost estimates for standalone services also reported.
Markov model used to project health outcomes and costs by varying cervical cancer screening strategy. With roughly equal life expectancy (~17), preventative cryotherapy lifetime societal costs were $97.07, compared to other cervical cancer screening platforms ($192.17-$218.64). Unclear source for treatment costs assumptions for cryotherapy, colposcopy and LEEP.
We used the Drummond Checklist in creating guidelines to assess the quality of economic evaluation (Supplement: Table S1) A score was assigned to each study to measure quality of economic analysis as follows:
- 1–8 Drummond checkmarks
- 9–12 Drummond checkmarks
- >12 Drummond checkmarks.
Cost effectiveness reported by integrated outreach platform and comparative cervical screening strategy 24,26,29
VIA – visual inspection with acetic acid, Pap - Papanicolaou smear, HPV – human papillomavirus, CEA- cost-effectiveness analysis, PNC- prenatal care, FP – family planning, HTC – HIV testing and counseling
Table 3–
Economics Research Questions
| 1. | What is the existing economic evidence for integrated HIV/NCD strategies in LMICs with regards to cost and impact? |
| 2. | What are the most common challenges facing national health program efforts to integrate HIV and NCDs treatment and care? |
| 3. | What are the gaps in data and how can longitudinal data be used to look at the long-term costs/benefits of NCD treatment? |
| 4. | What are the critical gaps in knowledge on the economics of HIV/NCD integration? |
| 5. | What is the ideal minimum economic dataset and what variables should be captured in an economic evaluation of integrated care? |
| 6. | How can cost-effectiveness analyses (CEAs) be used to evaluate the integration of HIV/NCD care? |
| 7. | What information is needed to assess the interactions of multiple NCDs, including interactions between CVD, cancer, and mental health risks over time? |
| 8. | Is it feasible to harmonize and standardize HIV and NCD economic models, and their methods, data sources, and assumptions? |
| 9. | Do current economic assessments and available data support the integration of HIV/NCD programs and care? |
Acknowledgments
FINANCIAL SUPPORT: Fogarty International Center, National Institutes of Health
Sources of Support
RTI International
Footnotes
Conflict of Interest
Authors report no conflicts of interest, as per AIDS guidelines.
CDC Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
DISCLAIMER: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. government.
References
- 1.Njuguna B Models of Integration of HIV and Non-Communicable Disease Care in Sub Saharan Africa: Lessons Learned and Evidence Gaps. AIDS. 2018(32(1).). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Duffy M, Ojikutu B, Andrian S, Sohng E, Minior T, Hirschhorn LR. Non-communicable diseases and HIV care and treatment: models of integrated service delivery. Trop Med Int Health. 2017;22(8):926–937. [DOI] [PubMed] [Google Scholar]
- 3.Rabkin M, El-Sadr WM. Why reinvent the wheel? Leveraging the lessons of HIV scale-up to confront non-communicable diseases. Glob Public Health. 2011;6(3):247–256. [DOI] [PubMed] [Google Scholar]
- 4.Nugent R A Chronology of Global Assistance Funding for NCD. Glob Heart. 2016;11(4):371–374. [DOI] [PubMed] [Google Scholar]
- 5.Palmer S, Torgerson DJ. Economic notes: definitions of efficiency. BMJ. 1999;318(7191):1136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.McPhail SM. Multimorbidity in chronic disease: impact on health care resources and costs. Risk Manag Healthc Policy. 2016;9:143–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marseille E, Dandona L, Marshall N, et al. HIV prevention costs and program scale: data from the PANCEA project in five low and middle-income countries. BMC Health Serv Res. 2007;7:108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Siapka M, Remme M, Obure CD, Maier CB, Dehne KL, Vassall A. Is there scope for cost savings and efficiency gains in HIV services? A systematic review of the evidence from low- and middle-income countries. Bull World Health Organ. 2014;92(7):499–511AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ickovics JR. “Bundling” HIV prevention: integrating services to promote synergistic gain. Prev Med. 2008;46(3):222–225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sweeney S, Obure CD, Maier CB, Greener R, Dehne K, Vassall A. Costs and efficiency of integrating HIV/AIDS services with other health services: a systematic review of evidence and experience. Sex Transm Infect. 2012;88(2):85–99. [DOI] [PubMed] [Google Scholar]
- 11.Obure CD, Guinness L, Sweeney S, Initiative I, Vassall A. Does integration of HIV and SRH services achieve economies of scale and scope in practice? A cost function analysis of the Integra Initiative. Sex Transm Infect. 2016;92(2):130–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hyle EP, Naidoo K, Su AE, El-Sadr WM, Freedberg KA . HIV, tuberculosis, and noncommunicable diseases: what is known about the costs, effects, and cost-effectiveness of integrated care? Journal of acquired immune deficiency syndromes (1999). 2014;67 Suppl 1:S87–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bell JC, Rose DN, Sacks HS. Tuberculosis preventive therapy for HIV-infected people in sub-Saharan Africa is cost-effective. AIDS. 1999;13(12):1549–1556. [DOI] [PubMed] [Google Scholar]
- 14.JPT H Cochraine Handbook for Systematic Reviews of Interventions. 2011. [Google Scholar]
- 15.Shamseer LMD, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart L. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P). BMJ. 2015(2;349(jan02 1)):g7647. [DOI] [PubMed] [Google Scholar]
- 16.Drummond MJT. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ. 1996((7052):275). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Golovaty ISM, Van Heerden A, Van Rooyen H, Celum C, Barnabas R. A Cost Evaluation of Integrating Non-communicable Disease Screening into Home-based HIV Testing and Counseling. Paper presented at: HIV R4P Conference; 18–19 October 2016, 2016; Chicago. [Google Scholar]
- 18.Chamie G, Kwarisiima D, Clark TD, et al. Leveraging rapid community-based HIV testing campaigns for non-communicable diseases in rural Uganda. PLoS One. 2012;7(8):e43400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chang W, Chamie G, Mwai D, et al. Implementation and Operational Research: Cost and Efficiency of a Hybrid Mobile Multidisease Testing Approach With High HIV Testing Coverage in East Africa. Journal of acquired immune deficiency syndromes (1999). 2016;73(3):e39–e45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kabami J, Chamie G, Kwarisiima D, et al. Journal of the International AIDS Society. 2017;20(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.de Beer I, Chani K, Feeley FG, de Wit Rinke TF, Sweeney-Bindels E, Mulongeni P. Assessing the costs of mobile voluntary counseling and testing at the work place versus facility based voluntary counseling and testing in Namibia. Rural and remote health. 2015;15(4):3357. [PubMed] [Google Scholar]
- 22.Labhardt ND, Motlomelo M, Cerutti B, et al. Home-based versus mobile clinic HIV testing and counseling in rural Lesotho: a cluster-randomized trial. PLoS Med. 2014;11(12):e1001768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Van Heerden ABR, Norris S, Micklesfield L. Integrating non-communicable disease (NCD) screening and referral to care into home HIV testing and counseling in rural KwaZulu-Natal, South Africa: Burden of disease. International AIDS Conference; 18 – 22 July 2016; Durban, South Africa. [Google Scholar]
- 24.Lince-Deroche N, Phiri J, Michelow P, Smith JS, Firnhaber C. Costs and Cost Effectiveness of Three Approaches for Cervical Cancer Screening among HIV-Positive Women in Johannesburg, South Africa. PLoS One. 2015;10(11):e0141969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vodicka EL, Babigumira JB, Mann MR, et al. Costs of integrating cervical cancer screening at an HIV clinic in Kenya. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2017;136(2):220–228. [DOI] [PubMed] [Google Scholar]
- 26.Hewett PC, Nalubamba M, Bozzani F, et al. Randomized evaluation and cost-effectiveness of HIV and sexual and reproductive health service referral and linkage models in Zambia. BMC public health. 2016;16:785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schnippel K, Lince-Deroche N, van den Handel T, Molefi S, Bruce S, Firnhaber C. Cost evaluation of reproductive and primary health care mobile service delivery for women in two rural districts in South Africa. PLoS One. 2015;10(3):e0119236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Obure CD, Sweeney S, Darsamo V, et al. The Costs of Delivering Integrated HIV and Sexual Reproductive Health Services in Limited Resource Settings. PLoS One. 2015;10(5):e0124476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Zimmermann MR, Vodicka E, Babigumira JB, et al. Cost-effectiveness of cervical cancer screening and preventative cryotherapy at an HIV treatment clinic in Kenya. Cost effectiveness and resource allocation : C/E. 2017;15:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Prabhakaran D, Anand S, Watkins D, et al. Cardiovascular, respiratory, and related disorders: key messages from Disease Control Priorities, 3rd edition. Lancet. 2018;391(10126):1224–1236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Krikke M, Hoogeveen RC, Hoepelman AI, Visseren FL, Arends JE. Cardiovascular risk prediction in HIV-infected patients: comparing the Framingham, atherosclerotic cardiovascular disease risk score (ASCVD), Systematic Coronary Risk Evaluation for the Netherlands (SCORE-NL) and Data Collection on Adverse Events of Anti-HIV Drugs (D:A:D) risk prediction models. HIV Med. 2016;17(4):289–297. [DOI] [PubMed] [Google Scholar]
- 32.Patel P Non-communicable Diseases among Persons Living with HIV in Low- and Middle-Income Countries: A Systematic Review of Cardiovascular Disease, Cervical Cancer, Depression, and Diabetes. AIDS. 2018;32(1). [Google Scholar]
- 33.Bekolo CE, O’Bryan G, Tchago FE, Nangue C, Bekoule PS, Kollo B. Integrating Cervical Cancer Screening with HIV Care in Cameroon: Comparative Risk Analysis of Cervical Disease in HIV-Infected Women Receiving Antiretroviral Therapy to Women in the General Population. PLoS One. 2016;11(2):e0149152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nou E, Lo J, Grinspoon SK. Inflammation, immune activation, and cardiovascular disease in HIV. AIDS. 2016;30(10):1495–1509. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.